
"Almost 4. Still in diapers. You've tried everything."
It's another morning of wet sheets, another failed attempt at the potty, another meltdown when you even mention the bathroom. You've bought the character underwear, the sticker charts, the reward candies — and your child still doesn't seem to notice when they're wet. Their cousins trained by 2, preschool admission requires toilet training, and every well-meaning relative asks the question you dread.
Toilet Training Readiness — Building the Foundation, Not Just the Behavior. You are not failing. Your child's developmental systems are not yet synchronized for this skill — and that is something we can address, systematically and compassionately.
Pinnacle Blooms Consortium®
Occupational Therapy Lead
ABA · SLP · SpEd · NeuroDev
Age 18m–7yr
Domain E: Self-Care
WHO Nurturing Care Framework (2018): Early identification of developmental gaps and informed parental response directly determines long-term functional outcomes.

You Are Among Millions of Families Navigating This Exact Challenge
1 in 3
Children with Developmental Differences
Experience significant toilet training delays beyond typical age. Toileting difficulty is among the most common referral reasons to pediatric OT worldwide.
80%
Of Children with Autism
Display sensory processing differences that directly impact toileting readiness. PRISMA systematic review, 24 studies, 2024 | PMC11506176
4–6 yrs
Actual Typical Age
For reliable toilet independence in children with neurodevelopmental differences. American Academy of Pediatrics — expanded readiness framework
In India alone, an estimated 18 million children are navigating toileting delays associated with developmental variation. This is a clinical challenge — not a parenting failure.
PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | AAP Toilet Training Guidelines (2023)
What's Happening in Your Child's Brain
Toilet training requires the convergence of six distinct developmental systems. When any one of these systems has a gap, training falters — not because the child is stubborn, but because the required infrastructure isn't yet complete. This is a wiring difference, not a willpower problem.
Physiological Maturity
Bladder capacity, sphincter muscle control, bowel regularity. Cannot be forced — must develop biologically.
Interoceptive Awareness
The brain's ability to feel internal body states: fullness, urgency, wetness. Many children with ASD genuinely cannot feel what neurotypical children feel.
Motor Skills
Walking to the bathroom, sitting balanced on a potty, managing clothing, wiping. Each is a discrete motor task.
Cognitive Sequencing
Following a 7-step routine, connecting sensation to action, understanding cause and effect.
Communication
Signaling the need before it becomes urgent. Requires language OR an alternative communication system.
Emotional Readiness
Willingness to engage, absence of phobia, tolerance of the novel sensory environment of the bathroom.
Frontiers in Integrative Neuroscience (2020): Neurological basis for sensory processing differences in ASD, including interoceptive hypo-sensitivity. DOI: 10.3389/fnint.2020.556660

Where This Sits in Development
Toilet Training in the WHO/AAP Developmental Framework
Children with sensory processing differences, ASD, motor delays, or communication challenges typically need 12–36 additional months and modified approaches. This is not regression — it is a different developmental trajectory requiring targeted support. Toilet training delays commonly co-occur with: Autism Spectrum Disorder, Sensory Processing Disorder, Intellectual Disability, Cerebral Palsy, ADHD, Language Delays, and Constipation/GI issues. Nighttime dryness frequently follows daytime mastery by 2–3 years in all children.
WHO Care for Child Development (CCD) Package (2023) | UNICEF MICS developmental monitoring indicators | PMC9978394

The Evidence Behind This Approach
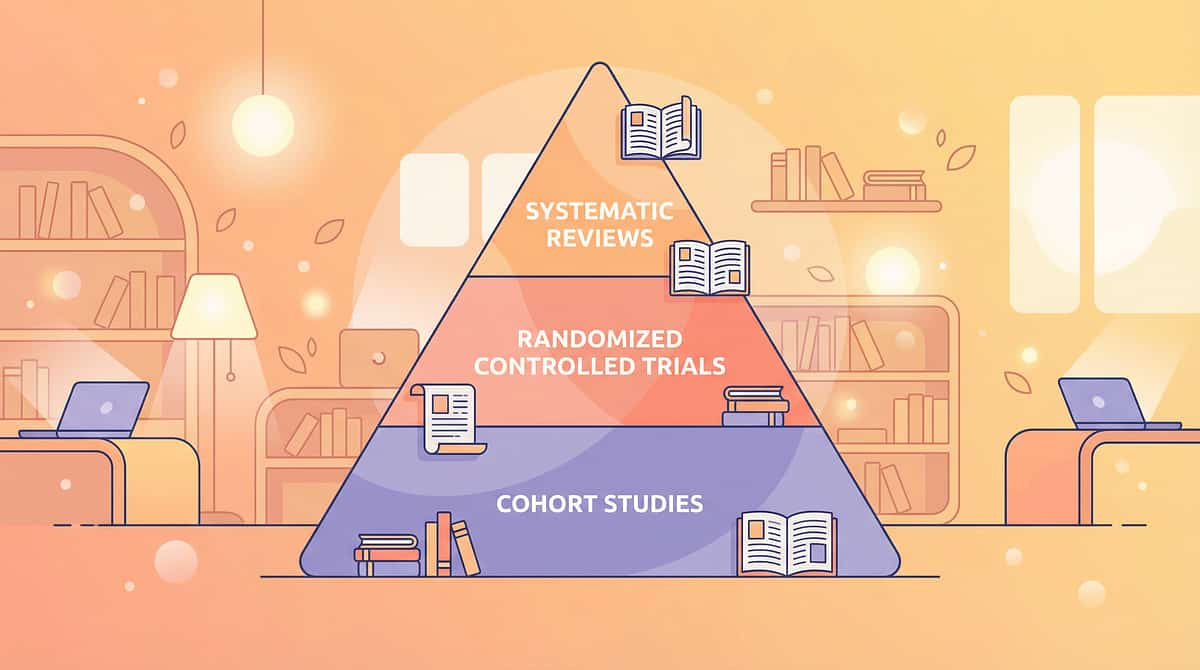
🛡️ LEVEL II EVIDENCE
RCTs + Systematic Reviews
Multi-Country Clinical Data
The multi-component readiness approach to toilet training — addressing sensory awareness, motor skills, visual supports, behavioral reinforcement, and environmental adaptation — is supported by convergent evidence across occupational therapy, applied behavior analysis, and developmental pediatrics.
Study | Finding | Source | |
PRISMA Review 2024, 16 studies | Sensory integration intervention meets EBP criteria for ASD | PMC11506176 | |
Meta-analysis 2024, 24 studies | SI therapy effectively improves adaptive behavior & self-care skills | PMC10955541 | |
Indian RCT, Padmanabha 2019 | Home-based sensory interventions show significant measurable outcomes | DOI:10.1007/s12098-018-2747-4 | |
NCAEP 2020 | Visual supports & behavioral reinforcement are EBP for autism | NCAEP Report | |
AAP Clinical Report 2023 | Readiness-based approach superior to age-based approach | AAP Pediatrics |
The Bottom Line: Clinically validated. Home-applicable. Parent-proven. The 9 materials in this guide address the specific readiness gaps that cause toilet training to fail.
The Technique: What It Is
Multi-Component Toilet Training Readiness Intervention
"Building Readiness, Not Forcing Timelines"
Domain E: Self-Care
Age: 18m–7yr
Setting: Home + Clinic
Definition
Toilet training readiness intervention is a systematic, multi-domain approach that builds the six underlying developmental foundations required for successful toilet training: physiological maturity, interoceptive body awareness, motor skills, cognitive sequencing, communication ability, and emotional willingness.
Rather than repeating failed training attempts with more pressure or different rewards, this approach identifies which of the six systems needs development and targets it directly — using specific materials and techniques matched to each gap.
Who It's For
Children aged 18 months–7 years who have not responded to conventional toilet training approaches, particularly those with ASD, sensory processing differences, developmental delays, motor challenges, communication delays, or significant toileting anxiety.
Who Uses This Technique
This technique crosses therapy boundaries — because the body doesn't organize by therapy type.
Occupational Therapist (Primary Lead)
Assesses all 6 readiness domains. Identifies sensory processing gaps (interoception, tactile sensitivity). Adapts environment, materials, and clothing. Addresses motor skills for bathroom independence.
ABA/BCBA Therapist
Designs reinforcement schedules. Creates data collection systems. Implements scheduled sits and token economy. Addresses behavioral resistance and anxiety.
Special Educator
Develops visual schedules and social stories. Supports sequencing in the classroom. Coordinates home-school consistency. Adapts academic expectations during training.
Speech-Language Pathologist
Establishes toileting communication method (verbal or AAC). Supports signaling needs. Creates social stories with appropriate language level.
NeuroDev Pediatrician
Rules out medical contributors (constipation, UTI, anatomical issues). Manages co-occurring medical needs. Guides readiness assessment from developmental medicine perspective.
When toilet training fails despite consistent effort, it almost always means one or more of these disciplines hasn't been involved yet. 📞 9100 181 181 — FREE, 16+ languages, 24x7
What This Technique Targets
Primary Target
Independent, Child-Initiated Toileting Across Settings
Observable: Child recognizes urge → goes to bathroom independently → completes sequence → returns to activity without accidents.
Secondary Targets
- Interoceptive Body Awareness — Child can reliably feel bladder fullness and bowel signals before emergency urgency
- Toileting Sequence Mastery — Child follows the 7-step routine without prompting
- Clothing Independence — Child manages elastic-waist clothing without adult assistance during toilet transitions
Tertiary Developmental Gains
Self-Regulation
Toileting routines build body regulation skills that transfer to other self-care domains.
Communication
Establishing a reliable toilet signal often accelerates broader communication development.
School & Social Readiness
Toilet independence is prerequisite for preschool, play dates, and normative social participation.
Family Wellbeing
Reduced parent stress, increased child confidence, normalization of family routines.

The 9 Primary Materials
What You Need: Evidence-Backed Clinical Tools
These 9 materials address the specific readiness gaps that make toilet training fail. Each one is an evidence-backed clinical tool — not a gimmick.

1. Potty Training Doll with Wetting Feature
Teaches the complete toileting sequence through play, removing all performance pressure. The child is the helper — not the trainee. ₹800–2,500 | Amazon.in

2. Moisture-Sensing Training Underwear
Restores the sensory feedback loop that diapers eliminate, helping the brain connect sensation to wetness. ₹300–800/pack | Amazon.in

3. Visual Sequence Cards for Toileting
Posts each of the 7–9 steps at child height in the bathroom, eliminating cognitive load. The child simply follows the pictures. ₹100–400 | Amazon.in

The 9 Materials, Continued

4. Potty Chair with Sensory Supports
Removes vestibular fear and fall-in anxiety. Appropriately sized so feet touch the floor. Can be positioned anywhere. ₹500–2,000 | Amazon.in

5. Social Stories / Toilet Training Books
Books preview the toileting journey, normalize the experience, address fears, and model success through relatable characters. Essential for children who need preparation before new experiences. ₹150–500 | Amazon.in

6. Visual Timer
Externalizes the potty schedule — the timer says it's time, not the parent. Dramatically reduces power struggles. Visual timers give children predictability and a concrete endpoint. ₹300–1,200 | Amazon.in

The 9 Materials: Final Three
7. Toilet Targets / Potty Games
Transforms toileting from a demand into a game. Gamified elements activate intrinsic motivation and break the cycle of resistance. ₹100–600 | Amazon.in

8. Easy-Access Clothing / Elastic Waist Outfits
Many "toilet training failures" are actually fine motor failures. Elastic waistbands that pull down in under 3 seconds remove this barrier entirely. ₹200–600/outfit | Amazon.in
9. Reward System / Reinforcement Materials
Immediate, specific, consistent reinforcement bridges the gap between "not motivated enough" and "habit formed." External rewards are temporary scaffolding — they get the behavior started. ₹100–500 | ₹589 Amazon.in🟢Pinnacle Recommends
Complete Kit Cost: ₹2,350–8,900 for full setup. Essential Starter (4 items): Potty chair + Visual sequence cards + Timer + Training underwear ~ ₹1,200–4,400
DIY & Zero-Cost Substitutes
WHO/UNICEF equity principle: Every family — regardless of income — can access this intervention today. The therapeutic mechanism is in the principle — sensory feedback, visual predictability, play-based learning, reinforcement timing — not in the brand of product.
Material | Buy It (₹) | Make It (₹0) | |
Potty Training Doll | ₹800–2,500 | Any doll or stuffed animal + pretend play. Feed water, pretend it wets, practice the full routine with zero performance pressure. | |
Visual Sequence Cards | ₹100–400 | Draw or print pictures for each step. Laminate with tape. Post at child eye-level. Free templates at Pinterest or Teachers Pay Teachers. | |
Visual Timer | ₹300–1,200 | Sand timer (₹50 at any stationery shop) or smartphone countdown timer visible to child. | |
Training Underwear | ₹300–800 | Regular cotton underwear. Less wetness protection, but provides full sensory feedback. Start during low-risk times. | |
Potty Chair | ₹500–2,000 | Lower regular toilet seat with foam pool noodle as bumper, add step stool for foot support. Functional as a bridge. | |
Social Story | ₹150–500 | Write 8–10 simple sentences about YOUR child's bathroom, YOUR potty, YOUR routine. Add photos. Read every day. Often more effective than commercial books. | |
Reward Chart | ₹100–500 | Draw a grid on paper. Any star sticker from a ₹10 stationery pack. The chart is the ritual — the sticker is secondary. |
When the Clinical Product Is Non-Negotiable: If the child has significant sensory over-responsiveness to wet sensation — proper moisture-sensing underwear is recommended. If the child has vestibular insecurity — a proper potty chair with stable base matters.

Safety First: Before You Begin
🔴 RED — STOP. Consult a Professional If:
- History of painful toileting, constipation, or encopresis — medical evaluation first
- Phobia-level response to the bathroom (severe panic, self-injurious behavior)
- Cannot sit unsupported for more than 30 seconds
- Blood in stool or urine, or signs of urinary tract infection
- Previous traumatic toileting experience creating ongoing distress
🟡 AMBER — MODIFY. Proceed with Extra Care If:
- Strong gag or vomit response to bathroom smells — desensitization first
- Significant fine motor delays — clothing management needs OT support
- Currently in a period of emotional regression (new sibling, school change, illness)
- Uses augmentative communication — establish toilet signal first
🟢 GREEN — PROCEED. Safe to Start When:
- Medical factors have been addressed (especially constipation)
- Child is not acutely ill
- At least 30 minutes without time pressure for first attempts
- You are emotionally regulated — children co-regulate with their caregivers
The Absolute Red Line: Never use shame, punishment, or emotional withdrawal as toilet training "motivation." Research is unambiguous: punishment during toilet training causes anxiety, withholding, constipation, toilet phobia, and regression. It makes training take longer, not shorter.

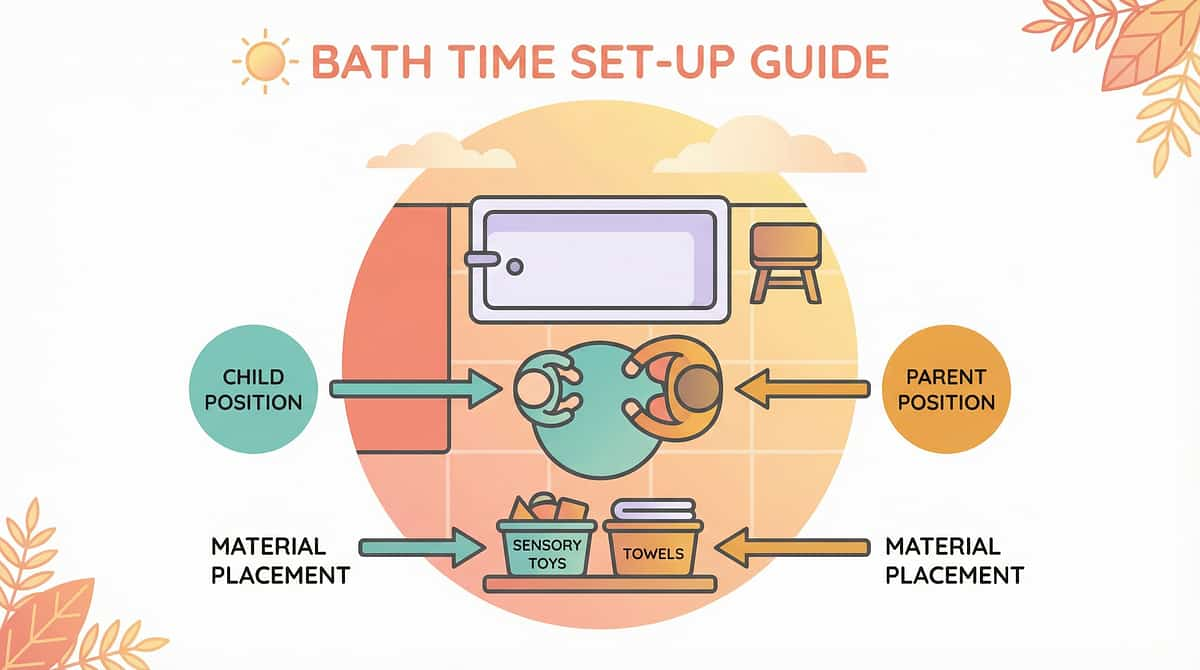
Set Up Your Space
The right environment prevents 80% of session failures. A few intentional changes to your bathroom dramatically increase the probability of every session succeeding.
Remove From the Space
- Distracting toys (sessions are purposeful, not playtime)
- Strong air fresheners (can be sensory aversive)
- Other children during initial training stages
- Time pressure — never when rushing
Add to the Space
- Visual sequence cards at 90–100cm height (child eye-level seated)
- Potty chair on non-slip mat, feet touching floor
- Timer visible from potty position
- Reward materials within reach but out of immediate sight
- Warm (not cold) bathroom temperature — cold rooms increase sensory resistance
Potty Chair Position Check
- Both feet flat on floor when seated (most critical factor)
- Child's bottom supported on seat without tension
- No risk of tipping or instability
- Child can get on/off independently (with support as needed)
Sensory Environment
Lighting: Soft or natural preferred. Avoid harsh fluorescent during early training.
Sound: White noise machine or gentle music can mask the echo that frightens some children.
Privacy: Door partially open or fully closed based on child preference.
SI Theory (Ayres): Environmental setup is a core intervention principle. PMC10955541: Individual 1:1 structured environment sessions most effective.

ACT III: THE EXECUTION
Is Your Child Ready? The Readiness Check
Complete this checklist before every session. The best session is one that starts right. Three good attempts beat ten forced ones in building the neural pathway.
Fed and Watered
Child has eaten and had fluids within last hour — not starving, not immediately post-large-meal.
Rested & Regulated
Not showing fatigue or hypersensitivity. Baseline calm state — not in active meltdown, high arousal, or post-incident recovery.
Timing Opportunity
One of the high-probability windows: upon waking, 15–20 min after eating, before bath, before bed.
Your Emotional State
You are regulated. Not stressed, rushed, or emotionally activated about toileting.
🟢 6–7 Checked: GO
Proceed to Step 1: The Invitation
🟡 4–5 Checked: MODIFY
Use simplified version — doll play only, or a casual bathroom visit with no expectation
🔴 3 or Fewer: POSTPONE
Not today. Do a connecting, positive activity instead. Tomorrow is another opportunity.
Step 1: The Invitation
30–60 Seconds
Bringing the child into the bathroom through a playful, low-demand, choice-based opening. No command. No announcement. An invitation.
For Doll-Play Children
"Hey! [Child's name] — want to help [Doll's name] try the potty? The doll has to go!"
For Children Past Doll-Play
"The timer just went — bathroom time! Race you to the bathroom?"
For Non-Verbal / AAC Users
Show toilet symbol card → point to bathroom → use child's established signal.
Body Language
- Kneel to child's eye level
- Relaxed face, gentle smile
- Open posture — no blocking, no steering
- Move toward bathroom yourself (model the direction)
Resistance Response
If child refuses: Do not push. "OK, maybe later." Return to activity. Retry at next scheduled window. Forced entry creates avoidance.
Step 2: The Engagement
1–3 Minutes
Deepening the interaction by introducing the therapeutic material. Reinforcement begins here — before any production is expected.
For Doll-Based Practice (Materials 1–3)
Give child the potty doll. "Let's help baby practice!"
Child 'feeds' doll from bottle → "Oh no! Baby's wet! Let's check!"
Child helps doll follow visual sequence: pants down → sit → wait → wipe → pants up → flush → wash hands
For Direct Potty Practice
Show visual sequence cards: "Let's follow the pictures"
Child approaches potty chair, explores it (no demand to sit yet if new)
Set visual timer: "We'll sit until the red is gone" (2–3 minutes)
Reinforcement Cue: Praise every engagement behavior, not just production. Walked to bathroom ✓ "Amazing! You came right away!" — Sat on potty ✓ "Brilliant sitting! Body's thinking!" — Stayed for timer ✓ "You did it! Timer's done!"

Step 3: The Therapeutic Action
3–8 Minutes — The Session Core
If Gap is INTEROCEPTIVE AWARENESS
Moisture-sensing underwear worn during training windows. Immediately and neutrally point out wetness: "You're wet! Your body is telling you something — let's listen." Body awareness ritual: "Put hand on tummy. Any feelings? Pressing? Moving? That's your body talking!"
If Gap is COGNITIVE SEQUENCING
Visual sequence cards are the primary tool. Child points to each card as they complete it. Velcro version: child moves each completed step to "Done" column. Narrate in parallel: "Pants down — first! Sit — next! Wait — timer's counting!"
If Gap is EMOTIONAL/ANXIETY
Potty doll practice: no expectation on child, all practice through the doll. Gradual exposure: Week 1, just visiting bathroom. Week 2, sitting clothed. Week 3, unclothed with no expectation to produce. Read toilet training social story book during seated doll play.
If Gap is MOTIVATION
Timer as external authority: "The timer says — not me!" Toilet targets: "Try to sink the target!" Special potty-only toy (available ONLY during potty sits). Immediate reward upon any success attempt.
Child Response | Meaning | Action | |
Engaged, compliant | Ideal — continue | Reinforce every step | |
Tolerating but passive | Acceptable — build from here | Reduce demand, increase reinforcement | |
Escalating distress | Stop immediately | End session positively, try doll play |

Step 4: Repeat & Vary
Across Multiple Sessions
Within One Session
- 1–3 good reps per session (never push to satiation)
- 3 good reps > 10 forced reps — this is the therapeutic dosage principle
- Vary within principle: sometimes doll, sometimes direct, sometimes book reading in bathroom
Across Days
- Every day, multiple times at scheduled windows
- Typical schedule: upon waking, 15–20 min after breakfast, 15–20 min after lunch, before bath, before bed
- Goal: repetition until automatic (procedural memory formation)
Variation Levels
Level 1 — Foundational
Doll play only → Book reading in bathroom → Casual bathroom visits
Level 2 — Emerging
Visual cards + timer sits → Moisture-sensing underwear during home time
Level 3 — Progressing
Full sequence with visual cards → All training in underwear → Child points to toilet symbol spontaneously
Level 4 — Advancing
Fading visual card prompts → Child-initiated attempts → Generalization to other bathrooms
Step 5: Reinforce & Celebrate
Within 3 Seconds of Behavior
The Timing Principle: Reinforcement delivered within 3 seconds is 10× more powerful than reinforcement delivered 30 seconds later. The brain makes the connection: behavior → consequence. Delay breaks that connection.
Tier 1 — Social Reinforcement
"YES! You sat on the potty! I'm SO proud of you!" High-energy, specific, immediate. Most sustainable long-term. Works for children who value social connection.
Tier 2 — Token Economy
One sticker on chart immediately after each successful sit. After 5 stickers → preferred activity or small tangible reward. Sticker Chart — ₹364🟢Pinnacle Recommends
Tier 3 — Immediate Tangible
Small preferred item from the "Potty Prize Box" — opened only in the bathroom after success. Reward Pack — ₹589🟢Pinnacle Recommends
The Celebration Principle: When actual production occurs for the first time — Make it a MOMENT. Dance, high-five, let the child see your genuine joy. This moment will anchor the behavior. Never:🚫 Reward for "not having accidents" (creates anxiety) 🚫 Delay reward until end of day 🚫 Take away earned rewards for subsequent failures
Step 6: The Cool-Down
2–3 Minutes
No session ends abruptly. The bathroom experience should end on a positive, predictable, child-controlled note — every time. This prevents post-session dysregulation and builds positive bathroom associations.
"Two more seconds on the potty, then all done!"→ 2 more seconds pass →"Timer's done! All done potty time! Let's wash hands — your turn to squirt the soap!"
Closing Ritual (Same Every Time — Predictability Is Therapeutic)
Child participates in putting down toilet lid (if able)
Hands washed together (make it sensory fun — warm water, foam soap)
Dry hands with their special towel
Child puts their sticker on the chart immediately
Exit bathroom together → "Now what do you want to do?"
Transition to Next Activity: Always have a preferred activity waiting: "First potty, THEN [favorite activity]." This makes the bathroom a gateway to good things, not just a demand. 📞Helpline: 9100 181 181
Capture the Data: Right Now
60 seconds of data now saves hours of guessing later. Capture within 60 seconds of session end.
The 3-Point Tracker
Attempt
□ Child came to bathroom (with help / independently) □ Child sat on potty (clothed / unclothed / refused) □ Child sat for timer (yes / partially / no)
Production
□ Urine ✓ □ Bowel movement ✓ □ No production □ Accident after Engagement: 1—2—3—4—5
Notes
What worked? What didn't? Any patterns noticed? Any resistance triggers identified?
Why This Data Matters
- Identifies highest-success times of day (guides schedule)
- Shows whether resistance is increasing or decreasing (trend)
- Reveals if accidents have a pattern (specific times, after certain activities)
- Provides objective evidence of progress when "nothing seems to be working"
GPT-OS® Integration
Parents in EverydayTherapyProgramme™ enter data directly into GPT-OS®. TherapeuticAI® analyzes patterns and adjusts recommendations at each session.

What If It Didn't Go as Planned?
Session abandonment is not failure — it's data. Every difficulty points to a specific cause with a specific solution.
"My child refused to enter the bathroom"
Cause: Bathroom may have negative associations from previous pressure. Environmental sensitivity. Solution: Go back to doll play outside the bathroom. Use desensitization: visit bathroom for a fun unrelated activity first. Gradually increase comfort before potty expectations return.
"My child sat but immediately got up"
Cause: Sensory discomfort (cold seat, instability), lack of meaningful activity during sit, uncertainty about expectations. Solution: Add padded seat cover. Use visual timer. Introduce special potty-only book or toy. Reduce sit duration to 60 seconds initially.
"My child had an accident 5 minutes after getting off the potty"
Cause: Child cannot yet feel pre-elimination urge (interoceptive gap). Extremely common and medical, not behavioral. Solution: Neutral response: "You're wet! Body needed to go!" Increase frequency of scheduled sits. Add moisture-sensing underwear.
"My child had a meltdown when I mentioned potty time"
Cause: Accumulated negative associations. Anticipatory anxiety is now driving resistance. Solution: STOP all direct potty attempts for 1–2 weeks. Rebuild positive bathroom associations through indirect methods. Consult OT if anxiety is severe. Call 9100 181 181.
"We were making progress, then suddenly regressed"
Cause: Environmental change (new sibling, school transition, illness), or natural consolidation plateau. Solution: Identify the stressor. Reduce expectations temporarily. Maintain the routine without pressure. Regression is the brain consolidating — it's normal and temporary.
"Nothing at all is working despite 6+ months of consistent effort"
This is the signal for professional evaluation, not more effort at home. Book an AbilityScore® assessment. Targeted professional intervention + home program is far more effective. 📞9100 181 181

Adapt & Personalize
No two children's readiness gaps are identical. Personalize this protocol based on your child's sensory profile.
Sensory SEEKER
Seeks input, high threshold, doesn't notice wet. Approach: Maximize sensory feedback. Moisture-sensing underwear during all waking hours. Cold water hand wash for sensory alerting before sits. More physical engagement during bathroom time.
Sensory AVOIDER
Over-responsive, bathroom is overwhelming. Approach: Minimize sensory input. Padded warm potty seat. White noise to mask echoes. Potty chair placed outside bathroom initially. Very gradual desensitization.
MIXED Profile
Some seeking, some avoiding — varies by sensation type. Approach: Map individual sensory responses. OT sensory profile assessment recommended. Address highest-barrier sensory channel first.
Dimension | Easier (Struggling) | Current Protocol | Harder (Mastery Near) | |
Session location | Outside bathroom | In bathroom | Any bathroom | |
Sitting requirement | Clothed, 30 sec | Unclothed, 3 min | Unclothed, 5 min | |
Sequence steps | 3 steps | 7 steps | Full independent routine | |
Prompt level | Hand-over-hand | Point to card | Self-directed | |
Reward frequency | Every attempt | Every success | Intermittent |

ACT IV: THE PROGRESS ARC
Week 1–2: What to Expect
15%
Progress Milestone
Early phase — building tolerance and positive associations
Watch For These Signs ✓
- Reduced bathroom resistance — child enters with less argument
- Doll play fluency — can guide doll through entire sequence unprompted
- Visual card recognition — can point to correct picture when you name the step
- Timer tolerance — stays on potty for 30+ seconds without escalating
- One spontaneous success — even if accidental: huge celebration
Not Expected Yet ✗
- Consistent production on the potty
- Child-initiated toileting
- Accident elimination
- Independence with the full sequence
The Micro-Progress That Matters
If your child tolerates the potty room for 3 seconds longer than last week — that is real, measurable, neurological progress. Don't dismiss small shifts.
Week 1–2 is the hardest. Stay consistent. The data you're collecting will show small improvements that may not be visible day-to-day. PMC11506176: SI intervention outcomes emerge across 8–12 week timelines.

Week 3–4: Consolidation Signs
40%
Progress Milestone
Synaptic consolidation phase — neural pathways strengthening
In Weeks 3–4, Watch For:
- Anticipatory behavior — Child goes to bathroom before you prompt
- Sequence initiation — Child begins pulling down pants without being prompted to the first step
- Generalization seeds — Child comments on others' toileting, applies knowledge to doll or sibling
- Increased sit tolerance — Sitting for full 3–5 minute timer without distress
- Regular scheduled successes — Production occurring at 1–3 scheduled sits per day
- Clothing competence building — Child managing elastic waistbands with decreasing assistance
What the Brain Is Doing
This is the synaptic consolidation phase. The neural pathway between "bathroom" → "routine" → "reward" is strengthening. The child's brain is beginning to automate what was previously effortful. You may notice the child seems more confident in the bathroom space.
Parent Milestone
You may notice you're more confident too. Your predictions of accident timing are improving. You're reading your child's pre-elimination signs. This bidirectional co-regulation is itself therapeutic.
When to Increase Intensity: If production is occurring at 2+ scheduled sits per day consistently → begin extending underwear wear time during lower-risk periods. 📞 Helpline: 9100 181 181

Week 5–8: Mastery Indicators
🏆 Mastery Badge Criteria
75%
Progress Milestone
Approaching full mastery — independent, generalized toileting emerging
Domain | Mastery Indicator | |
Interoception | Demonstrates pre-elimination awareness (goes BEFORE urgency) | |
Sequence | Completes full 7-step routine with maximum 1 verbal prompt | |
Initiative | Self-initiates potty trip at least once per day without external prompt | |
Production | Consistent success at 2+ scheduled sits AND 1+ self-initiated daily | |
Clothing | Manages elastic-waist clothing independently for toileting | |
Accidents | Fewer than 2 accidents per day at home during waking hours | |
Generalization | Success occurring in at least one setting other than primary home bathroom |
When 5 of 7 are checked → Mastery Level Reached. Next Level: Transition from potty chair to regular toilet → Begin nighttime training foundation → Public bathroom generalization program.
Celebrate This Win
You spent weeks building something the world often reduces to a simple "milestone." You learned to read your child's nervous system. You created a bathroom environment that felt safe. You delivered 50, 100, 200 consistent reinforcements. You absorbed the setbacks without making your child feel shame. You showed up, adjusted, and showed up again.
Your Child Grew Because of Your Commitment.
School Participation
Preschool and school access now open — a prerequisite achieved.
Family Wellbeing
Reduced caregiver burden, normalized family routines, restored confidence for everyone.
Child Self-Efficacy
Foundation for all other self-care independence skills — this mastery transfers everywhere.
📸 Take a photo. Write a date in your family record. This moment matters. Share your story on the Pinnacle parent community — your journey can help another family. → pinnacleblooms.org/community

Red Flags: When to Pause
Clinical Guardrail — Trust Your Instincts
🔴 Constipation and Withholding
Child holding bowel movements for 3+ days, hard or painful stool, visible distress. Why it matters: Creates a fear-constipation-pain cycle. Requires pediatric medical management.
🔴 Complete Absence of Wet Awareness
After 6+ weeks of consistent moisture-sensing underwear, child shows zero response to wetness. Why it matters: May indicate significant interoceptive processing difference requiring OT specialist.
🔴 Escalating Bathroom Anxiety
Child's fear response is increasing despite gentle, consistent approach. Why it matters: Anxiety is forming, not reducing. Requires behavioral consultation or psychological support.
🔴 Pain During Urination or Defecation
Any expressed pain. Why it matters: Medical emergency — UTI, fissure, structural issue. Pediatrician same week.
🔴 No Progress After 3+ Months
Despite consistent, appropriate effort at home. Why it matters: The protocol has run its course at home. Professional assessment now — not in another 3 months.
Escalation Pathway: Self-resolve → Continue protocol (Cards 21–22) → Teleconsult: pinnacleblooms.org/teleconsult → Clinic: pinnacleblooms.org/centers → Emergency (pain, blood): Pediatrician same day. 📞FREE National Helpline: 9100 181 181 (24x7, 16+ languages)
The Progression Pathway
Your position on the Self-Care Development Map — and the forward paths available based on your child's response.
If Mastery Is Achieved
→ Progress to E-492: Hygiene Skills Development (handwashing independence, face washing, teeth brushing)
If Nighttime Dryness Is Next
→ Progress to E-495: Bedwetting / Nighttime Dryness Foundation
If Bowel Training Is Lagging
→ Explore E-498: Constipation and Withholding — Breaking the Cycle
If Sensory Issues Are Pervasive
→ Explore E-502: Sensory-Based Self-Care Challenges (comprehensive sensory approach)
Related Techniques in the Self-Care Domain
Domain E: Self-Care & Daily Living Skills
Cluster Position 491/520
Technique | Code | Difficulty | Materials You May Already Have | |
9 Materials for Dressing Readiness | E-490 | Core | Visual cards, timer ✓ | |
9 Materials for Hygiene Skills | E-492 | Core | Visual cards, reward system ✓ | |
Potty Chair Selection Guide | E-491-DD-04 | Intro | Potty chair ✓ | |
Creating Toileting Social Stories | E-491-DD-02 | Intro | Story books ✓ | |
Nighttime Dryness Foundation | E-495 | Advanced | Timer, reward system ✓ | |
Bowel Training for Withholding | E-498 | Advanced | Potty chair, timer ✓ |
Materials You Already Own → Immediately Applicable: If you have a reward chart, visual timer, and visual sequence cards from E-491, you already have the foundation for E-492 (Hygiene), E-493 (Sleep), and E-490 (Dressing). Browse all 520 Self-Care & Daily Living Techniques: techniques.pinnacleblooms.org/self-care
ACT V: THE COMMUNITY & ECOSYSTEM
Families Who've Been Here
These are clinical narratives — not marketing stories.
Arjun, 5 Years — BangaloreBefore: Non-verbal autism, completely diaper-dependent at age 5. Four failed training attempts over 18 months. Zero interoceptive awareness of bladder state.Intervention: Moisture-sensing underwear 4 hours daily, padded potty chair outside bathroom (Week 1), visual sequence cards, 90-minute scheduled sits.At 20 weeks: Initiating potty visits independently using AAC device's toilet symbol. At 6 months: fully daytime independent."We had given up. The OT found what was missing in 30 minutes — no one had ever checked if he could actually feel when he was wet. He couldn't. The moisture underwear changed everything."
Priya, 4.5 Years — HyderabadBefore: Severe toilet anxiety following a traumatic flush incident at age 3. Holding bowel movements for 5+ days, encopresis, screaming when brought near any bathroom.Intervention: 3 weeks doll play entirely outside bathroom. Social story with her own photos. Potty chair in living room. Medical constipation management in parallel.At 4 months: Using the bathroom without distress. At 6 months: nighttime dryness beginning to emerge."No one told us the constipation and the anxiety were feeding each other. Once we addressed both together, she stopped being scared."
All cases illustrative. Individual results vary by child profile, underlying condition, and intervention consistency. Qualitative research confirms peer narratives are the strongest motivator for home-based intervention adherence.

Connect With Other Parents
Isolation is the enemy of adherence. Families who connect with peer support maintain consistent home protocols far longer than those who go it alone.
Pinnacle Parent WhatsApp Group
For parents navigating toilet training delays, sensory-based toileting challenges, and daily living skills for children with developmental differences. → pinnacleblooms.org/parent-groups
Online Forum — Self-Care Domain
Peer discussion, progress sharing, question answering with community support and therapist moderation. → pinnacleblooms.org/forums/self-care
Peer Mentoring
Connect with a parent who has been through this journey and reached mastery. Request through your nearest Pinnacle center. → pinnacleblooms.org/peer-mentoring
Local Parent Meetups
In-person parent groups at 70+ Pinnacle centers across India. Find your nearest center and ask about their parent peer support schedule. → pinnacleblooms.org/centers
📞9100 181 181 — WHO NCF: Community engagement is a core principle. Parent support networks improve intervention outcomes and adherence.
Your Professional Support Team
Home + Clinic = Maximum Impact
Home-based intervention gets you to 70% of potential outcomes.
Home + Professional Guidance gets you to 97%+.
What a Pinnacle OT Brings
- Formal sensory processing assessment (interoceptive sensitivity testing)
- Motor skills evaluation (sitting balance, clothing management)
- Environmental modification consultation (your specific bathroom)
- GPT-OS® personalized intervention pathway
- EverydayTherapyProgramme™ home plan with weekly progression
Three Ways to Access Professional Support
🗺️ Find a Pinnacle Center
70+ centers across India. OT assessment for toilet training readiness at all centers. → Book Assessment
📱 Teleconsultation
Remote video consultation with a Pinnacle OT, available in 16+ languages. → Book Teleconsult | 📞9100 181 181 FREE, 24x7
📋 AbilityCore® Assessment
Maps all 6 readiness domains clinically and generates a precision intervention pathway through GPT-OS®. → Learn About AbilityScore®
The Research Library
Deeper reading for the evidence-seeking parent and professional.
Study | Type | Finding | Link | |
PRISMA Review 2024 — 16 studies, ASD | Systematic Review | SI intervention meets EBP criteria for ASD | PMC11506176 | |
Meta-analysis 2024 — 24 studies, SI therapy | Meta-analysis | SI therapy promotes adaptive behavior, motor & social skills | PMC10955541 | |
WHO CCD Package | International Guideline | Home-based caregiver interventions effective across 54 LMICs | PMC9978394 | |
Padmanabha et al, Indian J Pediatr 2019 | RCT (India) | Home-based sensory interventions show significant outcomes | DOI:10.1007/s12098-018-2747-4 | |
NCAEP 2020 Evidence-Based Practices | Policy Document | Visual supports, reinforcement, video modeling are EBP for autism | NCAEP.org | |
WHO Nurturing Care Framework 2018 | Global Framework | Responsive caregiving + early learning = long-term developmental outcomes | WHO NCF 2018 | |
AAP Clinical Report — Toilet Training 2023 | Clinical Guidelines | Readiness-based approach recommended over age-based approach | AAP Pediatrics |
How GPT-OS® Uses Your Data
GPT-OS® — Global Pediatric Therapeutic Operating System. When 20 million therapy sessions contribute data, GPT-OS® identifies patterns that no individual clinician could observe.
What GPT-OS® Learns from E-491 Data
- Which of the 6 readiness domains is the rate-limiting factor for your child specifically
- Optimal time windows for scheduled sits based on your child's pattern data
- Rate of progress trajectory → predicted mastery date
- Early detection of regression or resistance escalation patterns
Privacy Assurance
All data is governed by Indian IT Act privacy standards. Children are never identified by name in aggregate analysis. Parents control their data entirely.
System Components
AbilityScore® · Prognosis Engine · TherapeuticAI® · EverydayTherapyProgramme™ · FusionModule™ · Closed-Loop Therapeutic Control

Watch the Reel
🎬 REEL E-491
Series Episode 491
Domain E — Self-Care
"9 Materials That Help With Toilet Training Readiness"
A Pinnacle OT therapist introduces each of the 9 materials in 60 seconds — with a visual of each material and a one-line clinical insight. B-roll shows the doll play sequence, visual cards in a bathroom, a timer countdown, and a reward chart sticker placement.
"Toilet training readiness isn't about trying harder. It's about building the foundation. These 9 materials help build what's missing — sensory awareness, visual structure, comfort, and motivation. Building readiness, not forcing timelines."
→ When published at techniques.pinnacleblooms.org, the corresponding Instagram/YouTube Reel embeds here.
Also From This Series
← E-490
9 Materials That Help With Dressing Readiness
→ E-492
9 Materials That Help With Hygiene Skills Development
Why Video Matters
Video modeling is classified as an evidence-based practice for autism (NCAEP 2020). Watching a therapist demonstrate activates different learning pathways than reading. Use both — text for depth, video for demonstration.
Share This With Your Family
Consistency across all caregivers multiplies impact by 3–5×. The more people in your child's life who understand and apply this approach, the faster progress occurs.
Explain to Grandparents
"[Child's name] is working on toilet training with a special readiness approach from Pinnacle Blooms Network. The most important things you can do:
- Use the same visual cards (on bathroom wall) — point to them together
- Set the timer for potty sits — the timer says when, not you
- Praise every attempt, not just success
- NEVER show frustration or shame for accidents — just neutrally change clothes
- Same reward sticker on the chart after any production
The approach is working at home. Consistency from you makes it work everywhere."
Share This Page
Downloadable Resources
Includes: current protocol summary, visual cards set for school bathroom, reinforcement system, accident handling protocol, data collection sheet.
The complete protocol on one laminated page for fridge/bathroom door.
Frequently Asked Questions
My child is 4 years old and still in diapers. Is this a developmental emergency?
Age 4 in diapers, while outside the typical range, is not unusual for children with developmental differences or who have had repeated unsuccessful training attempts creating resistance. It is a signal that the standard approach isn't working and a professional readiness assessment would be valuable. Book a free consultation: 9100 181 181.
How do I know if failure is sensory-based or behavioral?
If your child genuinely doesn't notice wetness even when directly pointed out — that's interoceptive (sensory). If your child notices but refuses to act — that's more behavioral, often with an anxiety component. Many children have both. An OT assessment differentiates them clearly. The distinction matters because sensory approaches won't address behavioral resistance, and reward systems won't address genuine interoceptive unawareness.
Should I use diapers or training underwear during the day?
For building readiness — training underwear or no underwear during home training windows. Diapers signal to the brain that wetness is expected and handled externally; they actively work against interoceptive awareness. During outings or high-demand times, diapers are acceptable; the training window at home is the therapeutic window.
My child sits but nothing comes out, then has an accident 10 minutes later. What's happening?
This is an interoception gap — the child cannot yet feel pre-elimination urgency. This is extremely common and is neurological, not behavioral. Moisture-sensing underwear, body awareness prompts, and scheduled sits timed around natural patterns (post-meal, upon waking) are the solution. It typically improves over 4–8 weeks with consistent protocol.
We tried once and it was traumatic. How do we start again?
Start with a complete break from all direct potty expectations — 2–3 weeks minimum. Rebuild the bathroom as a neutral or positive space through indirect activities: tooth brushing, hand washing, reading a book in the bathroom for fun. Then begin with doll play only (outside bathroom if needed). Moving slowly now saves months of resistance later.
How is this different from standard potty training methods online?
Standard approaches assume the child has all 6 readiness domains intact and simply needs motivation and opportunity. This approach first assesses which domains are lagging and targets them specifically. Targeting the specific gap is far more efficient than repeating general strategies that assume what might be missing. → Ask GPT-OS® more questions
Preview of 9 materials that help with toilet training readiness Therapy Material
Below is a visual preview of 9 materials that help with toilet training readiness therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

Your Next Step: Start Now
You now know more about your child's toilet training readiness than 95% of parents who will struggle through this without support. The knowledge is in hand. The materials are identified. The protocol is clear. What happens next is up to you — and we're here every step of the way.
20M+
1:1 Sessions
Exclusive therapy sessions delivered across the Pinnacle Blooms Network®
97%+
Measured Improvement
Across enrolled children in the EverydayTherapyProgramme™
70+
Centers India
Specialist pediatric therapy centers across India, serving 70+ countries
Pinnacle Blooms Network® | E-491 | Toilet Training Readiness
🔵 OT · 🟣 ABA/BCBA · 🟢 SpEd · 🔴 SLP · 🟡 NeuroDev Pediatrics · ⚪ CRO
"From fear to mastery. One technique at a time."
This content is educational and informational. It does not replace individualized assessment and intervention from licensed occupational therapists, developmental pediatricians, or other qualified healthcare professionals. © 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2