
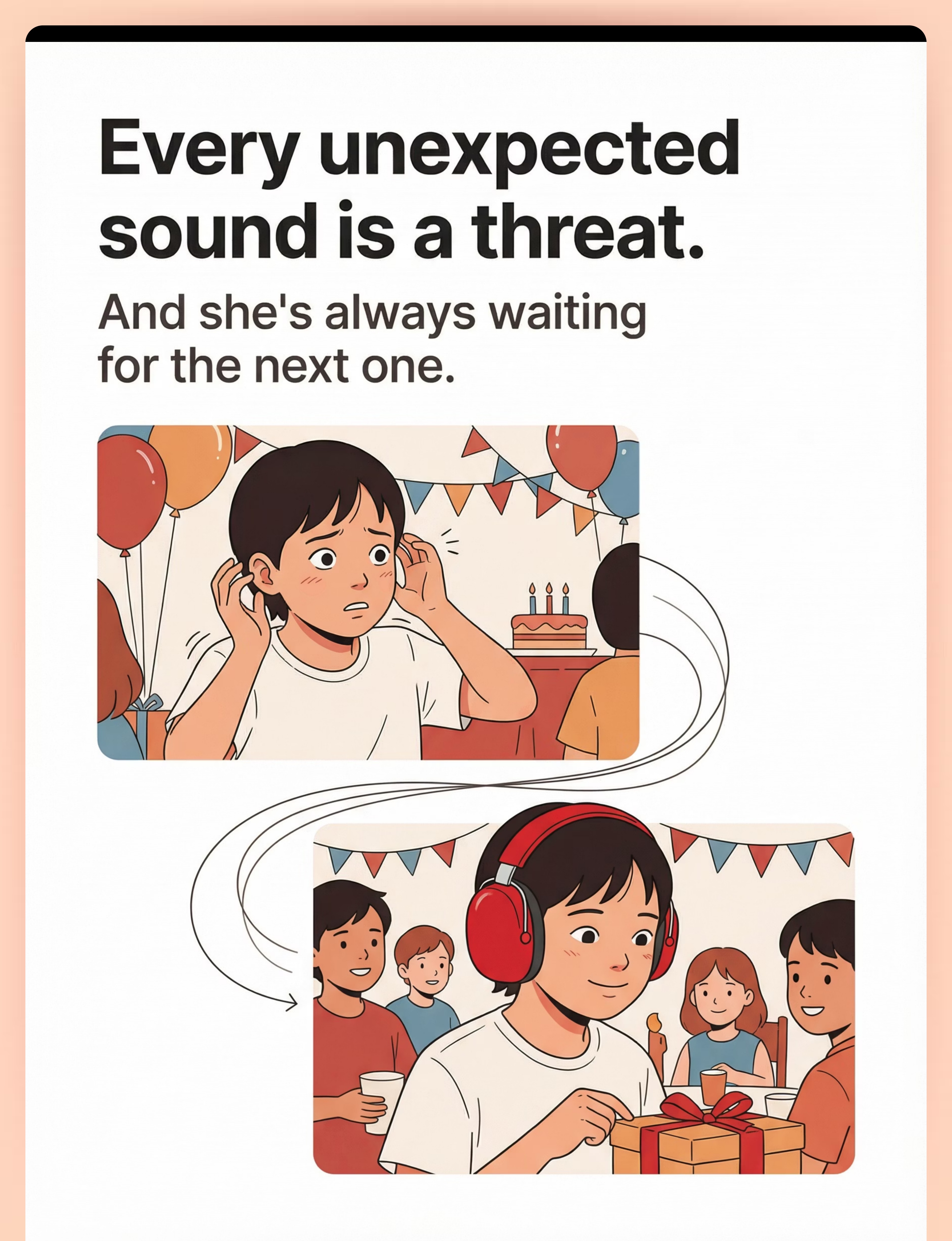
"She's not afraid of the sounds. She's afraid they might happen."
It's 7:15 AM. Your daughter is standing at the front door, frozen. She won't step outside because a dog somewhere in the neighborhood might bark without warning. Yesterday, a car horn on the walk to school sent her into twenty minutes of screaming. Last week, a balloon pop at a birthday party ended the party — for her. She lives in a state of permanent readiness for the next unexpected sound. Her hands hover near her ears. Her shoulders never drop. Even in silence, she is not calm — she is waiting.
Auditory Startle Desensitization Protocol — a structured, 9-material intervention to address both the extreme startle response and the anticipatory anxiety that steals your child's ability to exist in the world without fear.
You are not failing. Your child's nervous system is genuinely treating every unexpected sound as a threat. This is a wiring difference, not a behavior choice. And it can be addressed.
Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev

You Are Among Millions.
Across India and around the world, millions of families navigate the daily reality of auditory startle sensitivity. You are not alone — and the science behind your child's experience is well-documented, studied, and addressable.
80%
Children with Autism
of children diagnosed with autism exhibit sensory processing difficulties, with auditory over-responsivity among the most functionally limiting. Source: PRISMA Systematic Review, 2024 — PMC11506176
1 in 6
Startle Sensitivity
children with sensory processing differences display clinically significant exaggerated startle responses to unexpected sounds. Source: SPD Foundation Research Database
18M+
Families in India
families in India alone navigate auditory sensory challenges daily. Globally, this number exceeds 90 million. Source: WHO Global Report on Developmental Disabilities, 2024
You are not the only parent who has left a restaurant in tears, declined a birthday party invitation, or watched your child brace for impact in silence. Your child's experience is documented, studied, and — most importantly — addressable.
India-Specific Context: In India's dense urban and festival-rich environments — Diwali crackers, temple bells, traffic horns, street vendors — auditory startle sensitivity creates daily functional limitations that many Western clinical protocols fail to address. This protocol is designed for Indian realities.

The Alarm That Won't Turn Off
Understanding what's happening in your child's brain is the first step toward helping them — and toward releasing yourself from the belief that this is a parenting failure.
The Startle Reflex Circuit
Every human has an acoustic startle reflex — a brainstem-level protective response. Sound enters the ear and reaches the brainstem in under 10 milliseconds. Cochlea → Auditory Nerve → Brainstem — the startle reflex circuit fires before conscious thought is possible.
The Amygdala is the threat detection center — in these children, it is chronically overactivated. The Prefrontal Cortex — the "it's just a dog bark" rational override — remains underconnected, unable to reassure the alarmed amygdala in time.
What's Different in Your Child
Three things are altered in children with auditory startle hyperresponsivity:
- Lowered Threshold: Sounds that wouldn't trigger a startle in others activate the reflex. A pen dropping. A cough. A quiet door closing.
- Amplified Response: When the startle fires, it fires at maximum intensity — not a flinch but a scream, a cry, a full-body jolt.
- Failed Habituation: Typical nervous systems learn to stop startling to repeated sounds. Your child's system doesn't habituate — the 100th balloon pop is as terrifying as the first.
The amygdala has learned that unexpected sounds equal danger and now maintains constant surveillance: hypervigilance. Your child isn't just reacting to sounds — they're living in chronic anticipatory fear. The sound is the trigger, but the anticipation is the prison.
Key Insight: This is not a behavior problem. This is a neurological wiring pattern where the acoustic startle circuit is calibrated to a lower threshold, higher amplitude, and failed habituation — compounded by amygdala-driven anticipatory threat monitoring. It can be recalibrated. Frontiers in Integrative Neuroscience, 2020 — DOI: 10.3389/fnint.2020.556660

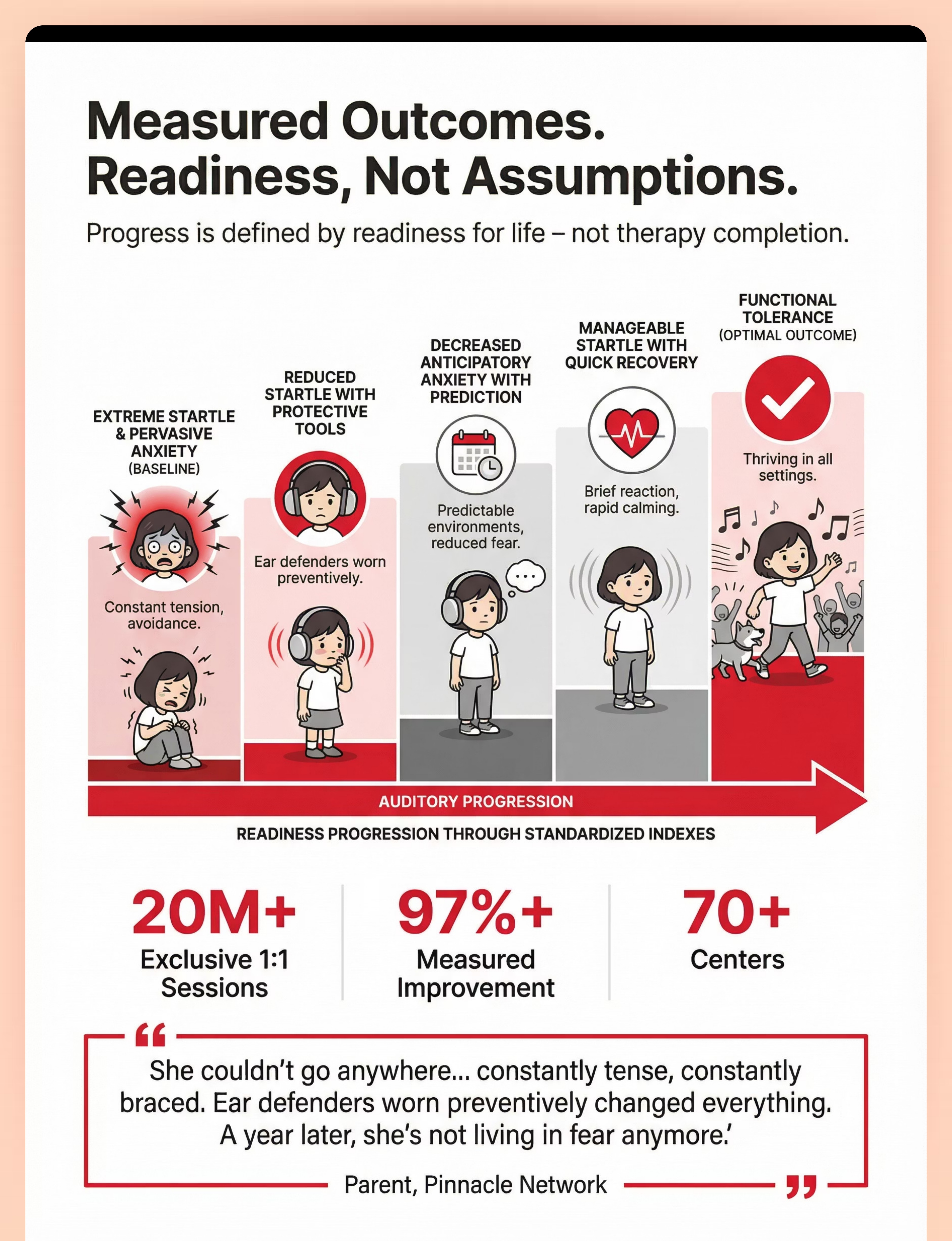
Your Child Is Here. Here Is Where We're Heading.
Understanding where your child sits on the developmental timeline — and what the trajectory looks like with and without intervention — gives you both clarity and urgency.
The 2–4 year window is the critical challenge zone: auditory modulation is still developing, and startle sensitivity frequently becomes functionally limiting. Anticipatory anxiety emerges here. Without intervention, avoidance patterns entrench and expand — school bells, announcements, classrooms, and social gatherings all become triggers by ages 6–12.
Age | Typical Development | Startle-Sensitive Child | |
0–6 mo | Normal Moro reflex to loud sounds | Exaggerated Moro; difficulty settling after sounds | |
6–12 mo | Begins habituating to household sounds | Continues startling to familiar sounds; no habituation | |
1–2 yrs | Explores sound-making toys; tolerates moderate noise | Avoids sound toys; distress in noisy environments | |
2–4 yrs ★ | Auditory modulation develops; distinguishes safe vs. threatening sounds | CHALLENGE ZONE: Functional limitation; anticipatory anxiety emerges | |
4–6 yrs | Participates in noisy group activities | Avoids group activities; school bells become triggers | |
6–12 yrs | Fully manages unexpected sounds with brief startle | Without intervention: entrenched avoidance, social isolation, anxiety comorbidity |
Auditory startle hyperresponsivity commonly co-occurs with: general auditory over-responsivity (50–70%), anxiety disorders (40–60%), tactile defensiveness (30–50%), and attention difficulties (25–40%). WHO CCD Package — PMC9978394 | UNICEF MICS Developmental Monitoring Indicators

Clinically Validated. Home-Applicable. Parent-Proven.
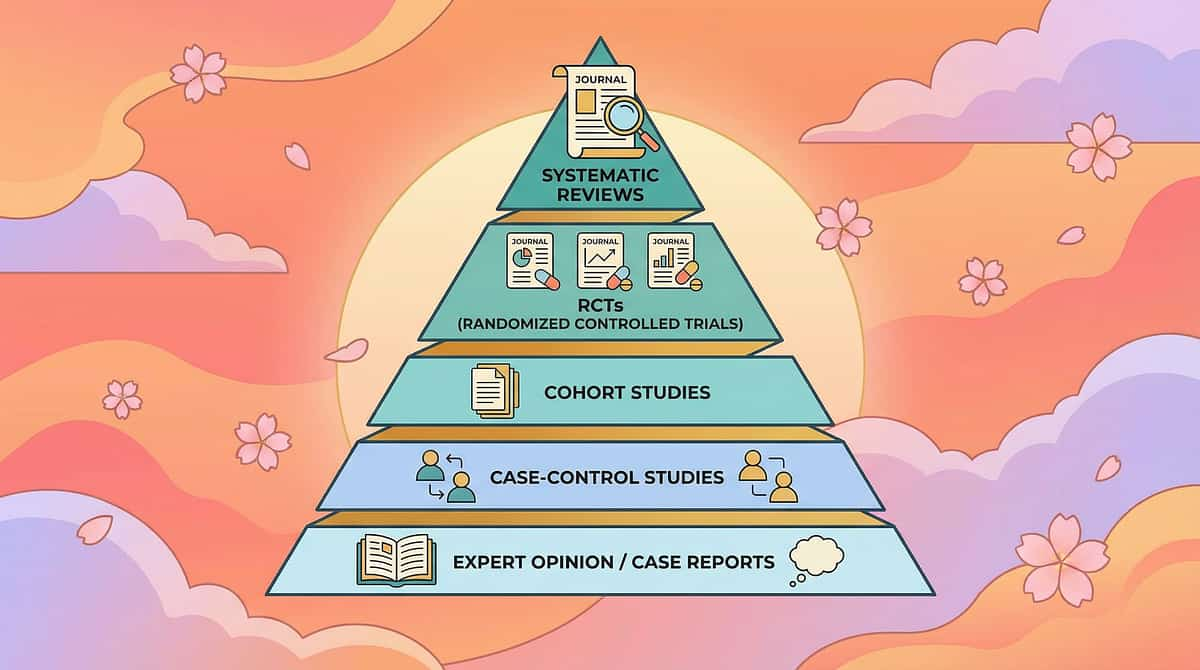
LEVEL II EVIDENCE
Supported by Systematic Reviews & Controlled Studies
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria as evidence-based practice for children with ASD. Auditory modulation interventions demonstrated improvement in sound tolerance and reduced startle amplitude. PMC11506176
Meta-Analysis, World J Clin Cases (2024)
24 studies covering sensory integration therapy across social skills, adaptive behavior, sensory processing, and motor skills. Individually-administered sessions showed maximum effectiveness for auditory processing targets. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Indian Pediatric RCT (2019)
Home-based sensory interventions in Indian children demonstrated significant outcomes when parents received structured protocols. Safety monitoring confirmed parent-administered auditory desensitization is safe with proper guidance. Padmanabha et al., Indian J Pediatrics — DOI: 10.1007/s12098-018-2747-4
Acoustic Startle Research
Exaggerated acoustic startle and habituation failure documented in auditory over-responsivity populations. Desensitization protocols reduce startle amplitude by 40–60% over 8–12 week periods with controlled exposure. SPD Foundation | AOTA Clinical Practice Guidelines
20M+
Exclusive 1:1 Sessions
Pinnacle Blooms Network therapy sessions tracked via GPT-OS® standardized measurement
97%+
Measured Improvement
Across sensory processing interventions at 70+ centers nationwide

The Technique: What It Is
SEN-AUD-STR
Age 3–12 Years
Home + School + Community
Formal Name: Auditory Startle Desensitization Protocol with Protective Buffering & Predictability Enhancement
Parent-Friendly Name: "Sound-Proofing Your Child's World — Then Slowly Opening It Up"
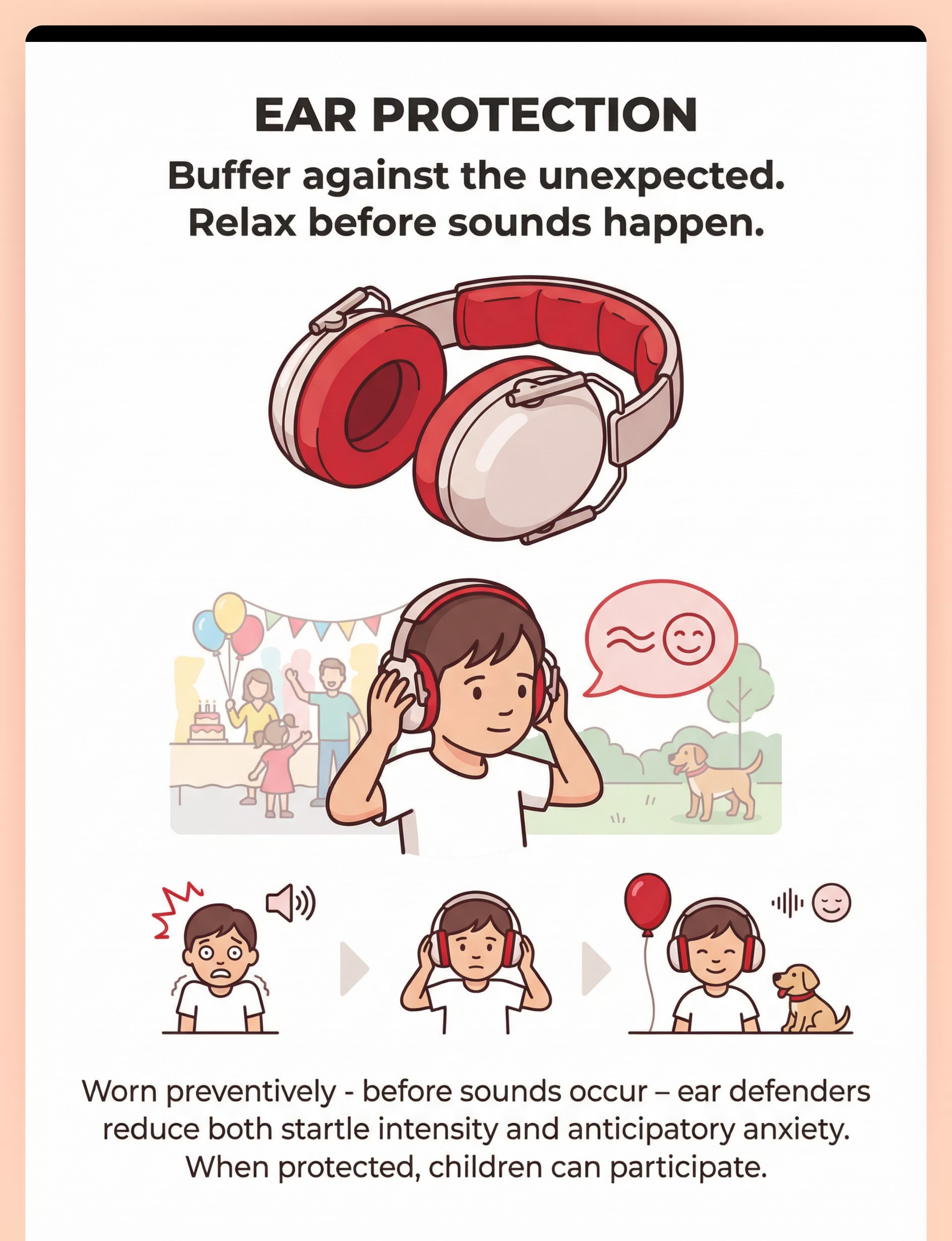
A multi-material intervention protocol that addresses extreme startle responses to sudden, unexpected sounds through three parallel strategies: (1) protective buffering using ear defenders and white noise to reduce startle intensity and anticipatory anxiety, (2) predictability enhancement using verbal warnings, visual schedules, and safe space planning to transform unexpected sounds into expected ones, and (3) gradual tolerance-building using controlled sound exposure, calming anchor objects, and breathing regulation to recalibrate the acoustic startle reflex over time.
Canon Materials (9)
- Noise-Reducing Ear Defenders
- White Noise / Sound Machines
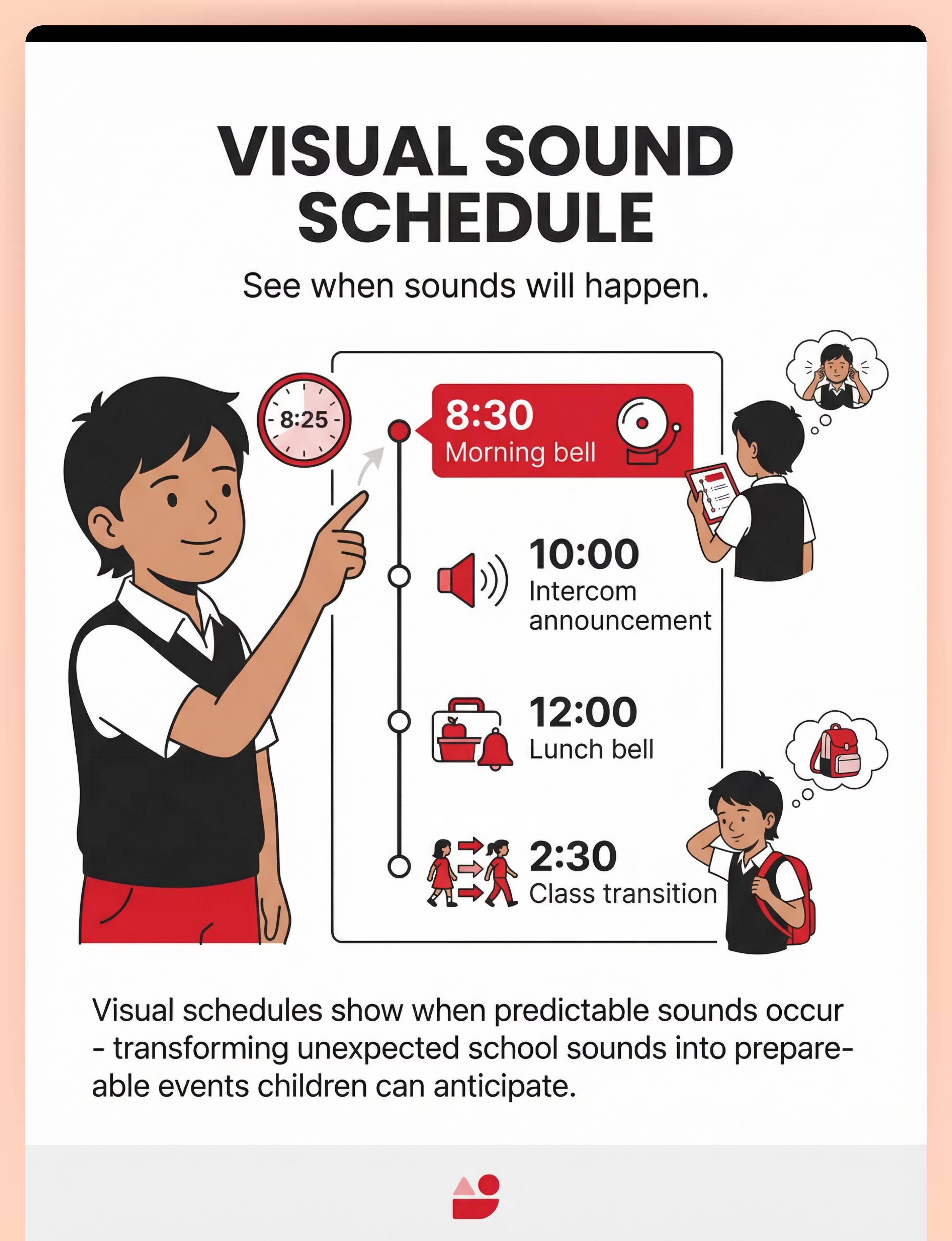
- Visual Schedule System
- Calm-Down Kit
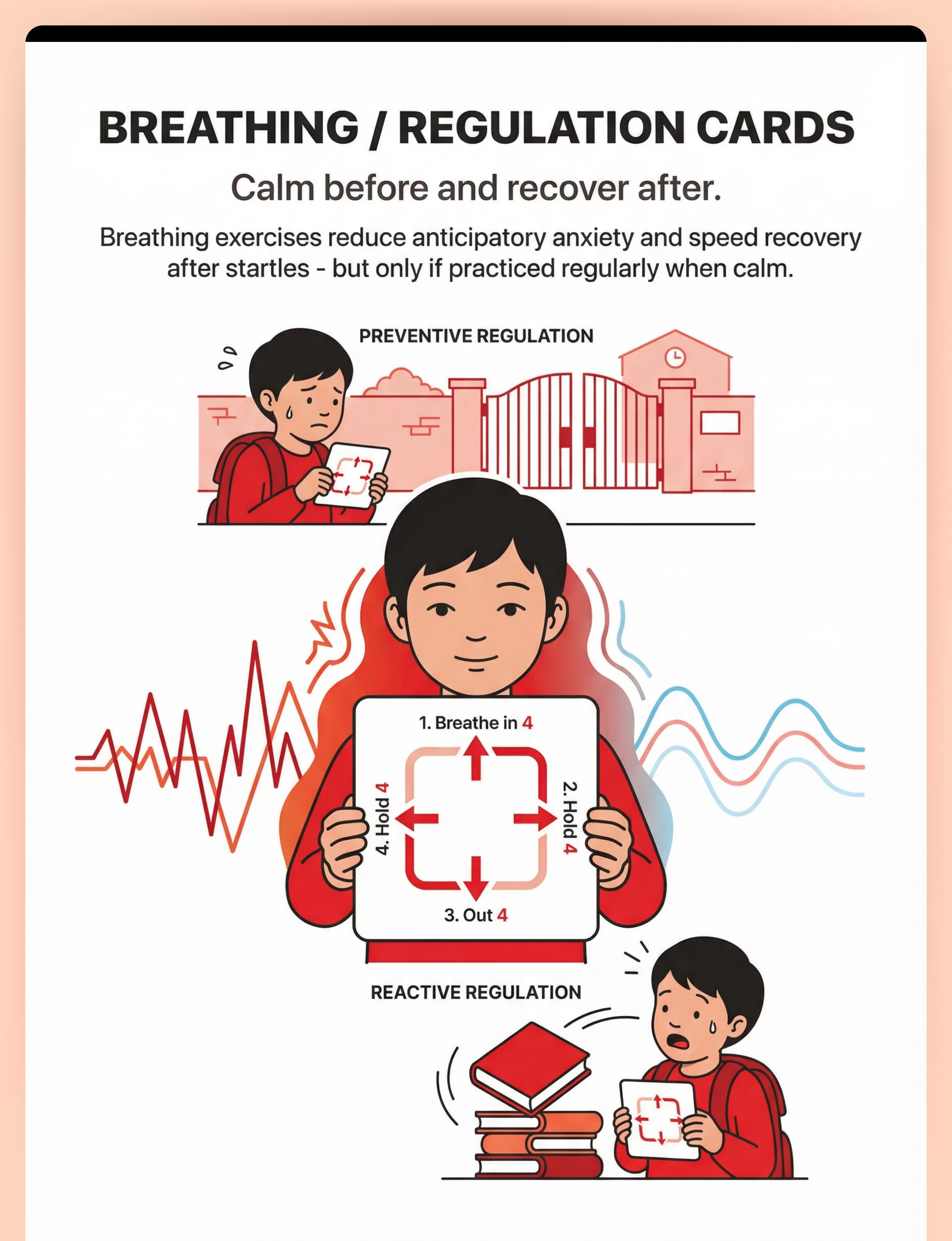
- Breathing / Relaxation Tools
- Fidget Tool Set
- Transition / Comfort Objects
- Sensory Tent / Calm-Down Space
- Sensory & Calming Apps
Domains & Categories
- Sensory Regulation & Nervous System Modulation
- Sleep (cross-deployed)
- Visual Supports & Schedules
- Emotional Regulation & Coping
- Behavior Support
- Technology & Apps
Session Guidance
- Protection: Ongoing, daily integration
- Prediction: Embedded in daily life
- Exposure: 5–15 min structured sessions
- Frequency: Daily across all environments

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type
Occupational Therapist (OT) — Primary Lead
The OT leads sensory integration assessment and intervention. They evaluate the child's auditory modulation profile, determine startle thresholds, design the sensory diet incorporating ear protection and white noise, implement gradual desensitization hierarchies, and monitor changes using standardized Sensory Profile-2 measures.
Board Certified Behavior Analyst (BCBA) — Secondary
The BCBA addresses the behavioral dimensions: avoidance behaviors, escape responses, anticipatory anxiety behaviors, and reinforcement systems for tolerance-building. They design the gradual exposure hierarchy using ABA principles with behavior-analytic precision and data-driven progress tracking.
Clinical Psychologist — Secondary
The psychologist addresses the anxiety component — particularly anticipatory anxiety, hypervigilance, and potential comorbid anxiety disorders. For older children (6+), they may integrate cognitive behavioral approaches and guide systematic desensitization while addressing family anxiety dynamics.
NeuroDevelopmental Pediatrician — Tertiary
The pediatrician rules out underlying auditory or neurological conditions, evaluates comorbidities, and may consider pharmacological support for severe anxiety components. They provide medical clearance, audiological referral, and ongoing developmental monitoring.
Special Educator — Supporting
The special educator implements accommodations in school: visual sound schedules, exit plans, ear protection permission, and classroom sound management. They bridge clinic recommendations to classroom execution — a critical link often overlooked.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) — DOI: 10.1080/17549507.2022.2141327

Precision Targeting — Not a Random Activity
Every element of this protocol is aimed at a specific clinical outcome. Understanding the targets helps you measure what's changing — and celebrate the right milestones.
🎯 Primary: Startle Modulation
Child's startle response decreases from extreme (screaming, crying, 10+ min recovery) → moderate (brief flinch, 30-sec recovery) → manageable (notices sound, immediate return to activity).
🔵 Secondary: Anxiety & Participation
Child relaxes in previously avoided environments; shoulders drop; hands move away from ears. Child attends events previously refused; duration of participation increases.
🟢 Tertiary: Whole-Family Impact
Self-regulation capacity builds. Social participation with peers increases. Parental stress decreases. Nighttime hypervigilance reduces — sleep onset and maintenance improve.
Reference: Meta-analysis, World J Clin Cases, 2024 — PMC10955541
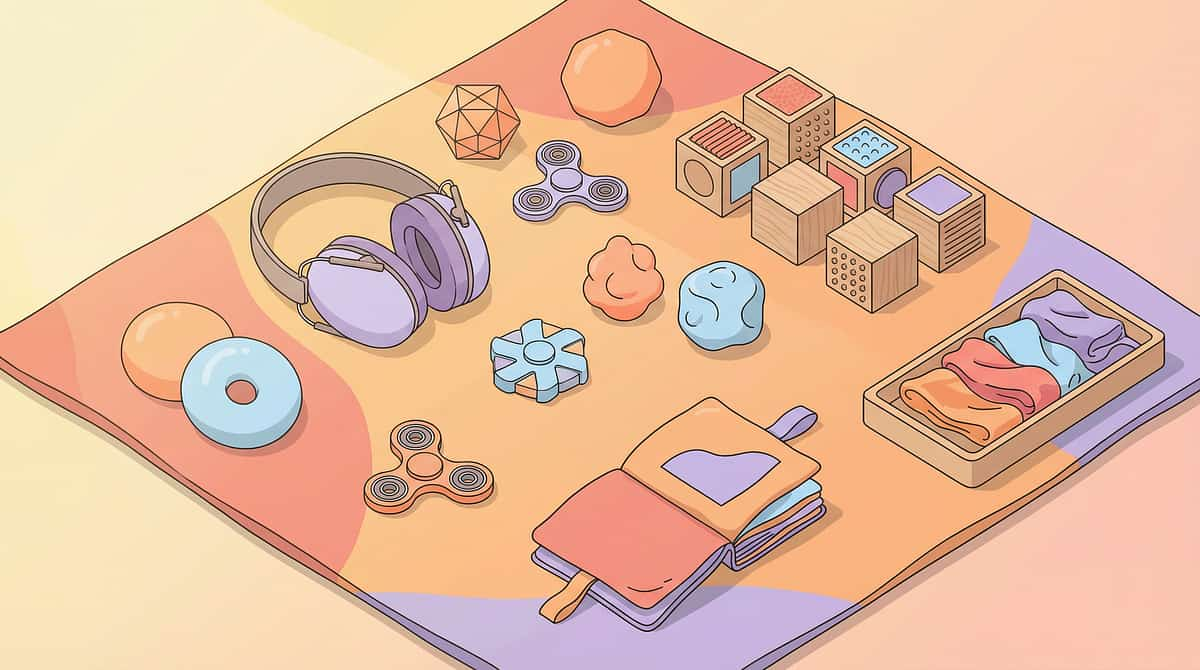
Your 9-Material Toolkit — Everything You Need
Material 1 of 9

Noise-Reducing Ear Defenders
Canon: Noise-Reducing Headphones / Ear Defenders
Category: Sensory Regulation & Nervous System Modulation
Product: SNOWIE SOFT Noise Cancellation Ear Muffs for Children (NRR 22+)
Price: ₹1,000–5,000
Purchase:Amazon.in
Key: Passive noise reduction preferred. Child-sized, adjustable, comfortable for extended wear. ✓ Pinnacle Recommends
Category: Sensory Regulation & Nervous System Modulation
Product: SNOWIE SOFT Noise Cancellation Ear Muffs for Children (NRR 22+)
Price: ₹1,000–5,000
Purchase:Amazon.in
Key: Passive noise reduction preferred. Child-sized, adjustable, comfortable for extended wear. ✓ Pinnacle Recommends
Material 2 of 9

White Noise / Sound Machine
Canon: White Noise / Sound Machines
Category: Sleep (cross-deployed to Sensory Regulation)
Product: Babelio White Noise Machine — portable, multiple sound options
Price: ₹0–3,000 (free apps available)
Purchase:Amazon.in
Key: Portable for use across environments. Pink/brown noise options for children who find white noise harsh.
Category: Sleep (cross-deployed to Sensory Regulation)
Product: Babelio White Noise Machine — portable, multiple sound options
Price: ₹0–3,000 (free apps available)
Purchase:Amazon.in
Key: Portable for use across environments. Pink/brown noise options for children who find white noise harsh.
Material 3 of 9

Sound Recordings (Digital)
Canon: Sensory & Calming Apps
Category: Technology & Apps
Product: Free — Freesound.org, YouTube sound libraries, custom recordings
Price: ₹0
Access:Freesound.org | YouTube
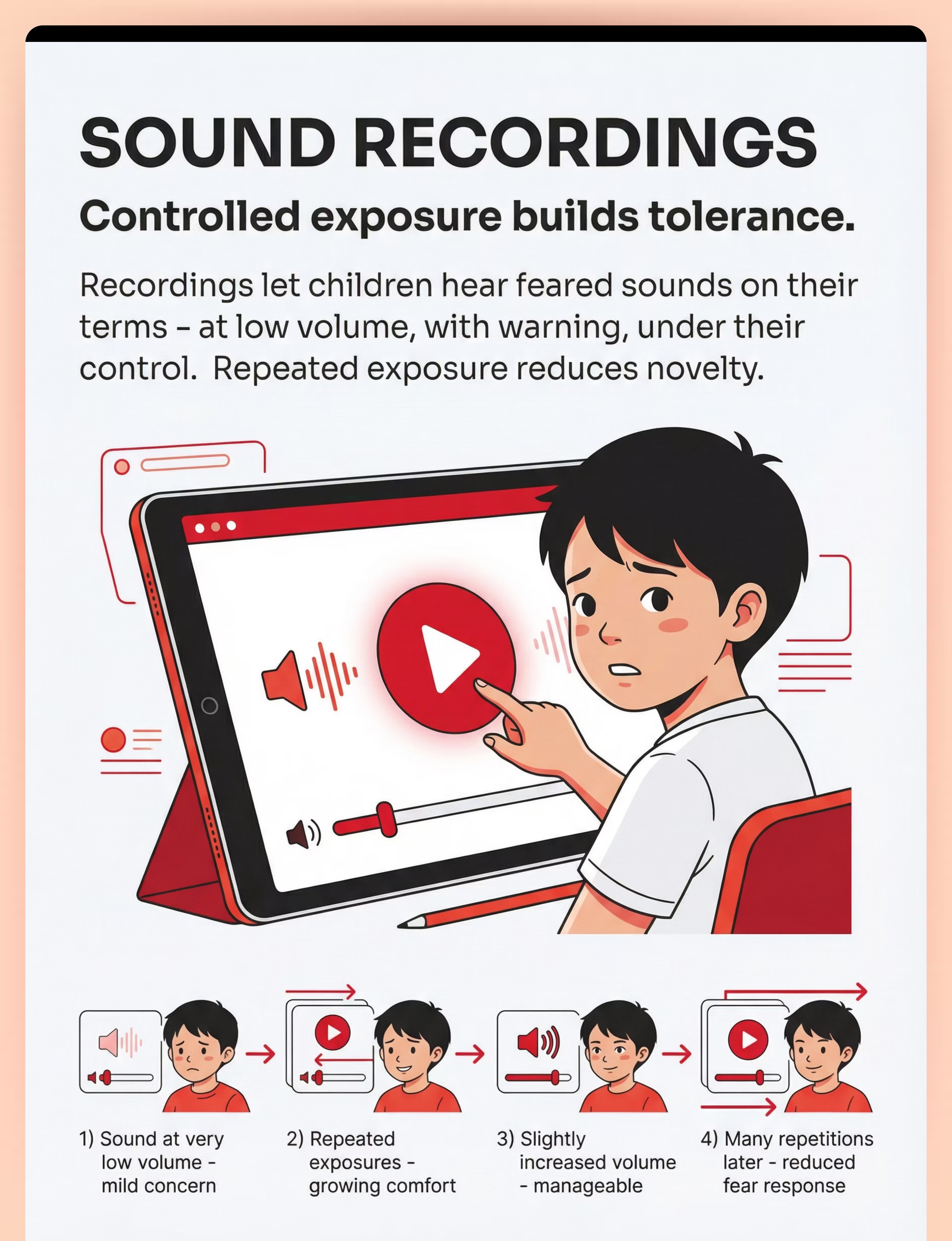
Key: Recordings of specific feared sounds (dog barks, balloon pops, thunder, bells). Volume-controllable playback is essential for safe, graduated exposure.
Category: Technology & Apps
Product: Free — Freesound.org, YouTube sound libraries, custom recordings
Price: ₹0
Access:Freesound.org | YouTube
Key: Recordings of specific feared sounds (dog barks, balloon pops, thunder, bells). Volume-controllable playback is essential for safe, graduated exposure.

Your 9-Material Toolkit — Materials 4–6
Material 4 of 9

Visual Schedule System
Canon: Visual Schedule System
Category: Visual Supports & Schedules
Product: SNOWIE SOFT Schedule Planning Chart / Little Minds at Work Daily Routine Chart
Price: ₹0–500
Purchase:Amazon.in
Key: Customizable to include sound events in the child's day — the school bell at 10:00, the cooker at 6:00 PM, the temple bells on Sunday morning.
Category: Visual Supports & Schedules
Product: SNOWIE SOFT Schedule Planning Chart / Little Minds at Work Daily Routine Chart
Price: ₹0–500
Purchase:Amazon.in
Key: Customizable to include sound events in the child's day — the school bell at 10:00, the cooker at 6:00 PM, the temple bells on Sunday morning.
Material 5 of 9

Calm-Down Kit / Self-Regulation Toolbox
Canon: Calm-Down Kit / Self-Regulation Toolbox
Category: Emotional Regulation & Coping
Product: Calming Corner Self-Management Toolbox
Price: ₹200–2,000
Purchase:Amazon.in
Key: A portable collection of the child's most effective calming tools. Should be immediately accessible — never locked away or out of reach during high-risk moments.
Category: Emotional Regulation & Coping
Product: Calming Corner Self-Management Toolbox
Price: ₹200–2,000
Purchase:Amazon.in
Key: A portable collection of the child's most effective calming tools. Should be immediately accessible — never locked away or out of reach during high-risk moments.
Material 6 of 9
Breathing / Relaxation Tools
Canon: Breathing / Relaxation Tools
Category: Emotional Regulation & Coping
Product: Yoga Poses Flash Cards / Visual Breathing Cards (downloadable free)
Price: ₹0–500
Key: Square breathing, star breathing, balloon breathing visuals. Practice these when calm so the skill is available during stress. The breathing card becomes a portable anchor during startle recovery.
Category: Emotional Regulation & Coping
Product: Yoga Poses Flash Cards / Visual Breathing Cards (downloadable free)
Price: ₹0–500
Key: Square breathing, star breathing, balloon breathing visuals. Practice these when calm so the skill is available during stress. The breathing card becomes a portable anchor during startle recovery.

Your 9-Material Toolkit — Materials 7–9
Material 7 of 9

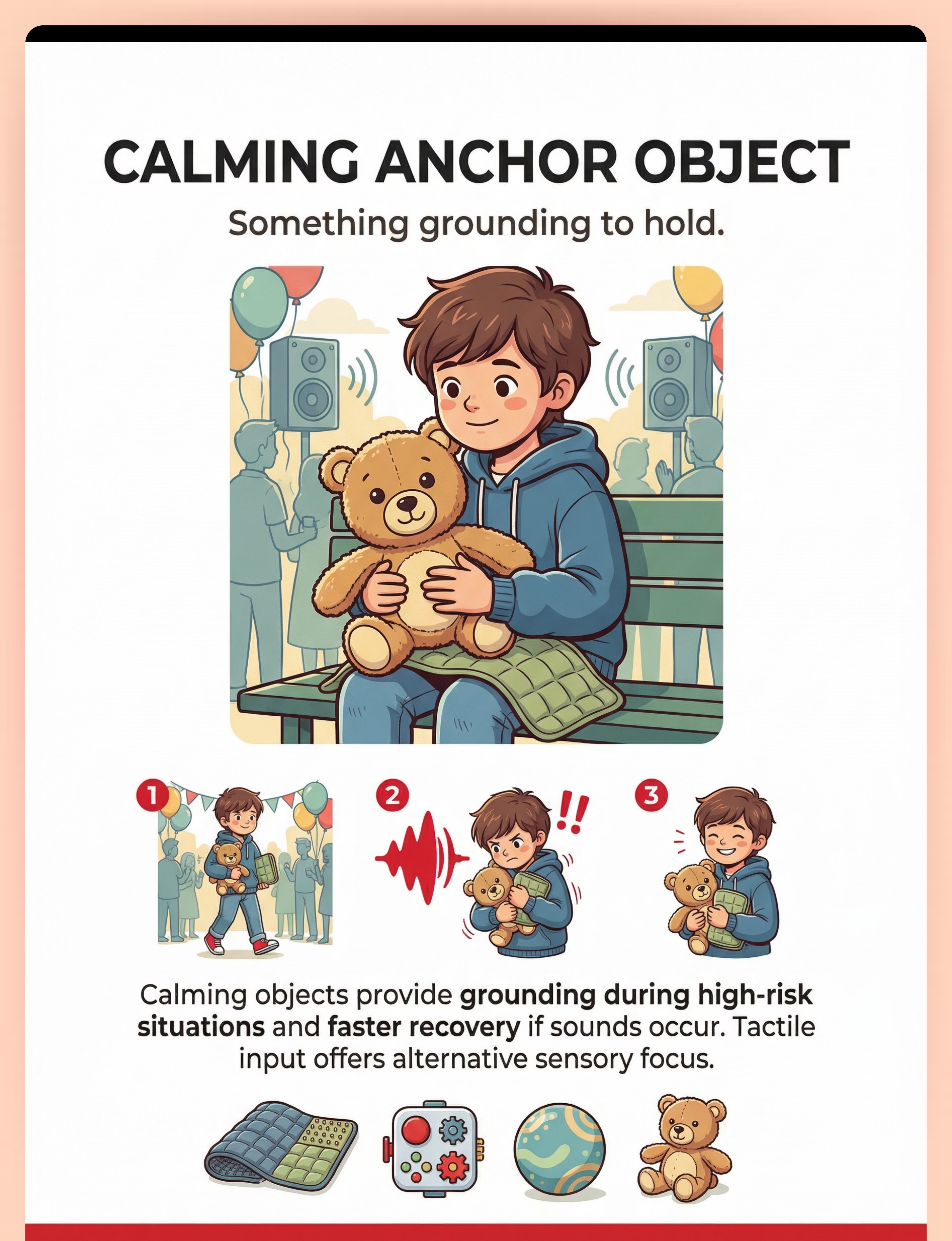
Fidget / Calming Anchor Object
Canon: Fidget Tool Set + Transition Objects / Comfort Items
Category: Sensory Regulation & Behavior Support
Product: Pop It Fidget, stress ball, soft stuffed animal, weighted lap pad
Price: ₹200–2,000
Purchase:Amazon.in
Key: A familiar tactile object in the child's hands provides grounding during high-risk sound environments. The child chooses their anchor — it must be theirs.
Category: Sensory Regulation & Behavior Support
Product: Pop It Fidget, stress ball, soft stuffed animal, weighted lap pad
Price: ₹200–2,000
Purchase:Amazon.in
Key: A familiar tactile object in the child's hands provides grounding during high-risk sound environments. The child chooses their anchor — it must be theirs.
Material 8 of 9

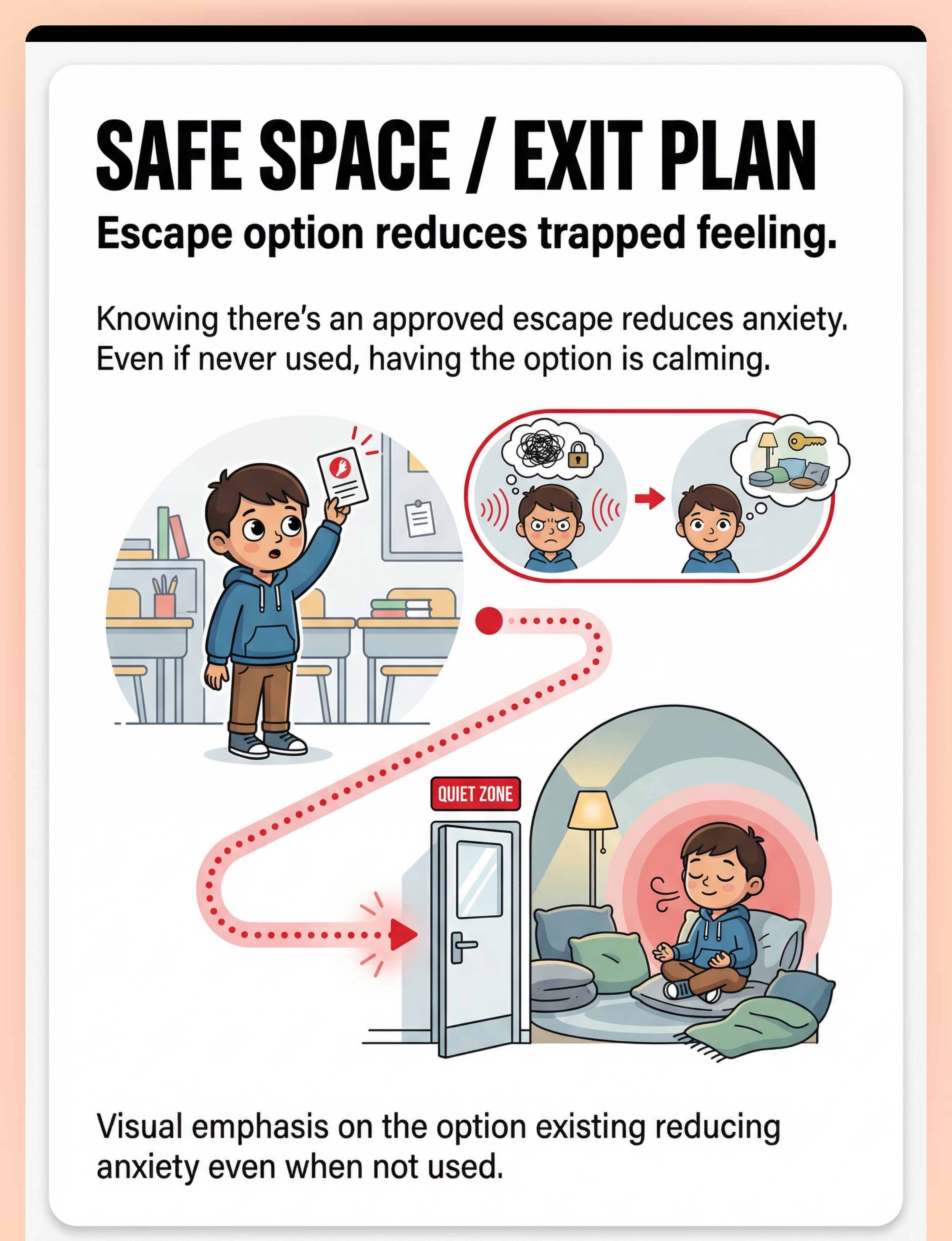
Sensory Tent / Calm-Down Space
Canon: Sensory Tent / Hideaway / Calm-Down Space
Category: Sensory Regulation & Nervous System Modulation
Product: Toyshine Foldable Play Tent / designated quiet corner with cushions
Price: ₹0–2,000
Key: Genuinely quiet space the child can retreat to. Pre-approved exit plan. The child must know this space is always available — never removed as a consequence.
Category: Sensory Regulation & Nervous System Modulation
Product: Toyshine Foldable Play Tent / designated quiet corner with cushions
Price: ₹0–2,000
Key: Genuinely quiet space the child can retreat to. Pre-approved exit plan. The child must know this space is always available — never removed as a consequence.
Material 9 of 9
Visual Schedule & Calming Apps
Canon: Visual Schedule & Organization Apps + Sensory & Calming Apps
Category: Technology & Apps
Product: Free apps for white noise, breathing exercises, visual schedules
Price: ₹0
Access:App recommendations → materials.pinnacleblooms.org
Key: Technology-based tools bridge home and school. A visual schedule app can be shared with teachers. A calming app can travel in a pocket.
Category: Technology & Apps
Product: Free apps for white noise, breathing exercises, visual schedules
Price: ₹0
Access:App recommendations → materials.pinnacleblooms.org
Key: Technology-based tools bridge home and school. A visual schedule app can be shared with teachers. A calming app can travel in a pocket.
Total Investment: ₹0–5,000. Many materials are free or made from household items. No family is excluded from starting today.

Every Parent Can Start Today — Regardless of Budget
The most important thing is that you begin. Every single strategy in this protocol has a zero-cost alternative that works on the same clinical principle.
Buy This | Make This (₹0) | Same Principle | |
Child ear defenders (₹1,500) | Adult industrial hearing protection (₹200–400); cotton balls as temporary measure | Physical sound reduction buffer | |
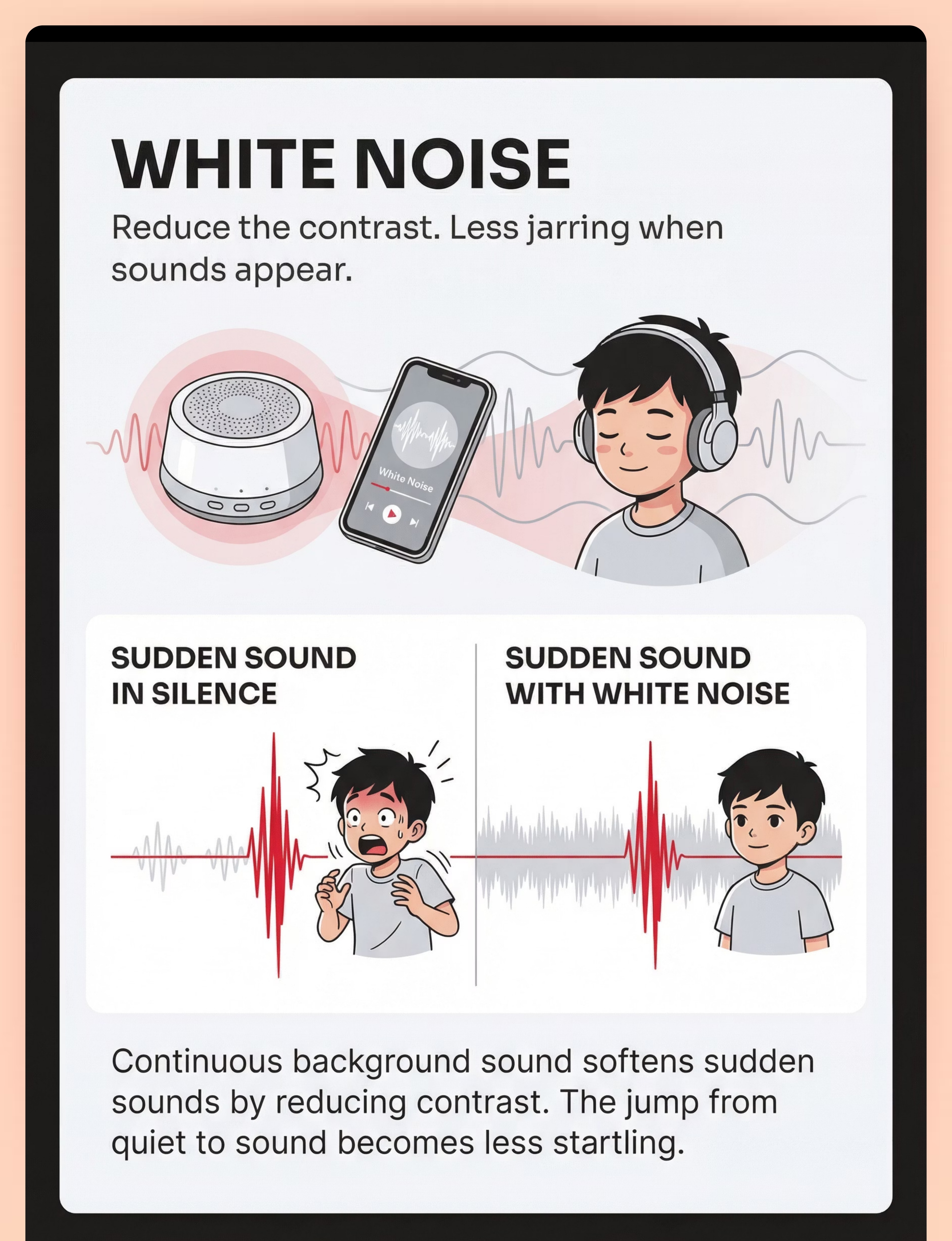
White noise machine (₹2,000) | Free white noise app; table fan; running water; TV on low static | Continuous background sound reduces sudden sound contrast | |
Sound recordings (₹0) | Record feared sounds on your phone; YouTube "dog barking sound effect" | Controlled, voluntary, repeatable exposure | |
Visual schedule (₹500) | Draw daily timeline on paper with clock faces showing when loud sounds happen | Visual prediction of sound events | |
Breathing cards (₹300) | Draw a square on paper: "Breathe in 4, Hold 4, Out 4, Hold 4." Laminate with clear tape. | Visual breathing cue available during stress | |
Calm-down space (₹1,500) | Any quiet corner with a blanket over chairs, a pillow, and the child's comfort object | Protected quiet retreat space | |
Calming anchor object (₹500) | Any existing stuffed animal, smooth stone from the garden, familiar soft fabric | Grounding tactile input during high-risk situations |
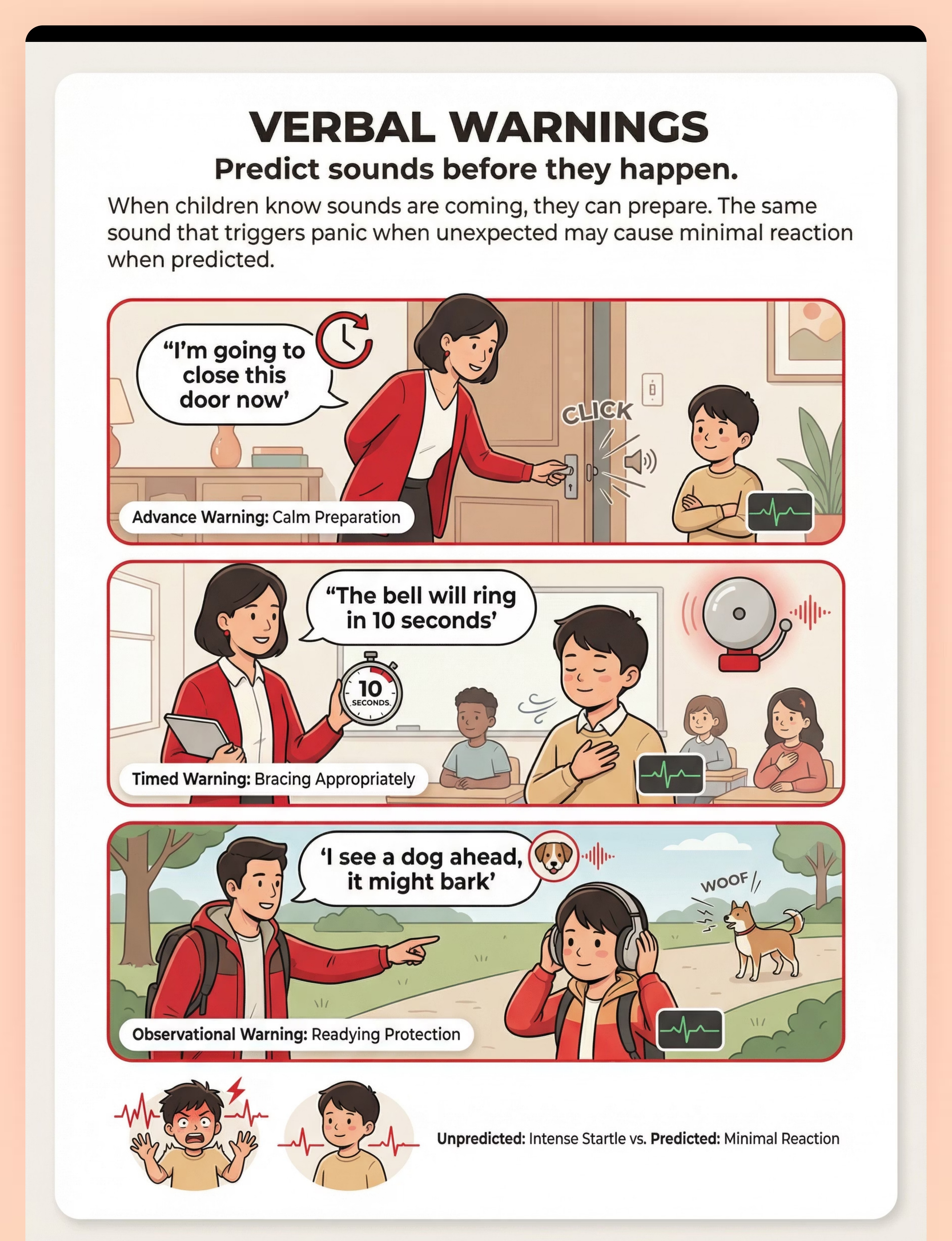
Start Giving Verbal Warnings Today
"I'm going to close this door." "The cooker will whistle in 2 minutes." "I'm going to turn on the mixer." Begin this practice right now — it costs nothing and begins recalibrating your child's nervous system immediately.
Download a Free White Noise App
Play it in the background during high-risk times — cooking, car rides, crowded outings. The continuous sound fills the sonic landscape and reduces the contrast of sudden sounds.
Designate One Quiet Corner
Any room, any corner. A cushion, a blanket, the child's favorite object. Name it together. "This is your quiet space. It's always here for you." That sentence alone reduces anticipatory anxiety.
When Clinical-Grade Materials Are Non-Negotiable: For structured desensitization programs, professional guidance from an OT or psychologist is strongly recommended. DIY exposure done incorrectly can increase fear rather than reduce it. WHO Nurturing Care Framework — PMC9978394

Read This Before You Begin. Every Time.
The safety framework for this protocol is not a formality — it is the difference between building tolerance and building fear. Follow this traffic-light system before every session.
🔴 RED — DO NOT PROCEED IF:
- Child is in acute distress, meltdown, or panic — this is NOT the time
- Child has ear infection, ear pain, or recent ear surgery — consult physician first
- Child has seizure disorder triggered by auditory stimuli — requires medical supervision
- You are planning forced exposure (holding child in place while playing feared sounds) — this is NEVER appropriate and WILL worsen the condition
- Child is expressing extreme despair about their sound sensitivity — seek immediate professional support
🟡 AMBER — PROCEED WITH MODIFICATION:
- Child is tired, hungry, or mildly dysregulated → protective strategies only, skip exposure work
- Child had a difficult startle experience within the last 2 hours → focus on calming and recovery
- Unsure about volume for sound recordings → start MUCH quieter than you think necessary
🟢 GREEN — PROCEED:
- Child is calm, fed, rested, and genuinely regulated
- Environment is prepared, materials accessible, quiet space designated
- You are calm and patient — your anxiety transmits directly to your child
- You have reviewed the specific strategy you're implementing today
MATERIAL SAFETY: Ear defenders: child must still hear safety-critical information (fire alarms). White noise: 50–60 dB max — never louder than a speaking voice. Sound recordings: NEVER play at full volume. Start at minimum. Child controls playback. Calm-down space: well-ventilated, no strangulation hazards, child can exit easily at all times.
THE ABSOLUTE RED LINE: Stop immediately and seek professional help if you see: sound sensitivity suddenly worsening without explanation; child developing new fears to previously tolerated sounds; complete social withdrawal; self-injurious behavior in response to sounds; significant sleep disruption lasting more than 2 weeks. Padmanabha et al., Indian J Pediatr, 2019 — DOI: 10.1007/s12098-018-2747-4

The Right Environment Prevents 80% of Session Failures
Before a single strategy begins, the physical environment must be prepared. A correct setup turns a challenging session into a successful one.
For Protective Strategy Sessions
- Child Position: Comfortable seating (floor cushion, beanbag, familiar chair) — NOT restrained or trapped
- Parent Position: Beside or in front — never behind (behind = unpredictable)
- Ear Defenders: Within child's arm reach — they put them on themselves when possible
- White Noise: 1–2 meters from child, playing at low volume before session begins
- Calming Object: Already in child's hands or lap
- Exit Path: Clear, unobstructed path to the quiet zone. Child knows the route.
REMOVE: Silence phones, close windows to traffic, turn off appliances that beep randomly.
For Gradual Exposure Sessions
- Child Position: Comfortable, relaxed, in control
- Playback Device: In CHILD'S hands — they press play, they control volume
- Volume Control: Start at minimum. If device has 1–10 scale, start at 0.5–1
- Parent Position: Beside child, calm, matter-of-fact. Do NOT show anxiety.
- Comfort Object: In child's other hand
- Breathing Card: Visible, posted or held
- Exit Option: Quiet zone clearly available — child knows they can stop anytime
Lighting: Natural, warm — avoid fluorescent. Time of Day: Mid-morning or early afternoon — when child is most regulated. NEVER immediately before or after transitions.

The Best Session Is One That Starts Right
The readiness check is not optional. A session started with a dysregulated child teaches the brain that these materials and strategies are associated with distress — the opposite of what you're building.
1
Child is genuinely calm
Not just "not crying" — genuinely relaxed. Shoulders loose. Breathing normal. Hands not hovering near ears.
2
Basic needs are met
Child has eaten within the last 2 hours. Adequate sleep last night. No significant sleep disruption.
3
No recent startle incidents
No significant startle events in the last 1–2 hours. No upcoming transitions, appointments, or stressors within the next 30 minutes.
4
Parent is fully present
Not rushed, stressed, or distracted. Your calm is the child's permission to try. Materials are prepared and accessible.
✅ All GREEN → GO
Proceed with today's planned strategy: protection, prediction, or exposure.
⚠️ 1–2 AMBER → MODIFY
Protective strategies only today. Skip exposure work. Practice breathing in a calm, no-pressure context.
🛑 Any RED → POSTPONE
Today is not a session day. That's data, not failure. Offer the calming object. Try again tomorrow.
"Pushing through when the child isn't ready doesn't build tolerance — it builds fear. The most valuable session is sometimes the one you don't do."

Step 1 of 6
The Invitation — Not a Command
What to Say
"Hey [child's name], I have your special sound helpers ready. Would you like to try your ear protectors on? You can take them off whenever you want."
For exposure sessions:
"[Child's name], remember how we've been practicing listening to sounds? Want to play our sound game today? You're the boss — you press the buttons."
Body Language
- Crouch to child's eye level
- Open posture — no crossed arms
- Calm, warm voice — slightly slower than normal speech
- Genuine smile, not performative
- Hold materials at child's level, not thrust forward
What Acceptance Looks Like
- Child reaches for the ear defenders
- Child moves toward the materials
- Child nods, even slightly
- Child says "okay" or equivalent
- Child allows you to place ear defenders near them
What Resistance Looks Like
- Child turns away, pulls back, or says no
- Child's body tenses
- Child puts hands over ears preemptively
- Child begins to cry or protest
If Resistance: DO NOT PUSH. Say: "That's okay. They'll be here when you're ready. Want to hold your [comfort object] instead?" Offer calming alternatives. Try again later or tomorrow.
ABA Pairing Principle: Establish motivating operations before demand placement. 30–60 seconds.
Step 2 of 6
The Engagement — Deepening Interaction
For Protective Strategies
Once the child has accepted ear defenders:
- Let them adjust for comfort — show how to loosen/tighten
- "How does that feel? Good? Let's see how quiet things get."
- Snap your fingers at normal volume: "See? Much quieter, right? You have your sound shield on."
- If using white noise: "Listen to this — it's like rain/ocean/fan. It fills up the quiet so surprise sounds are smaller."
For Exposure Sessions
Once the child is holding the device:
- "Here's our sound game. Remember, YOU decide. Press play when you're ready. I'll be right here."
- Volume confirmed at minimum. Child controls play/pause.
- First play: "There it is! You heard it and you're okay. Well done. Want to hear it again?"
- Do NOT increase volume in the same session unless the child is clearly comfortable and asks for more.
Engagement vs. Tolerance vs. Avoidance
Engaged: Child is curious, reaching for device, asking questions, smiling. Continue — this is exactly what you want.
Tolerating: Child is allowing the activity but showing tension (tight grip, shallow breathing). Continue at current level — do not push further.
Avoiding: Child is pulling away, going quiet, freezing, or escalating. STOP. End the session gently.
Reinforcement Cue
When the child willingly engages — immediate, specific praise:
- "You pressed play all by yourself! That was brave."
- "You're wearing your ear protectors like a champion."
Timing: 1–3 minutes. Reference: PMC11506176 — structured material introduction meets evidence-based practice criteria.

Step 3 of 6
The Core Therapeutic Actions
Choose the strategy that matches your child's current stage. All three strategies run in parallel — protection and prediction are daily, while exposure is structured and gradual.
Strategy A: Protective Buffering
- Child wears ear defenders.
- Parent guides child into a mildly challenging sound environment (kitchen during cooking, garden where dogs may pass).
- If a sudden sound occurs: observe child's response. With protection, the startle should be reduced.
- After the sound: "You heard that and you were okay! Your ear protectors helped."
- Duration: 10–20 minutes of protected environmental exposure.
Strategy B: Predictability Enhancement
- Throughout the day, give verbal warnings before EVERY controllable sound: "I'm going to close this cabinet." "The washing machine will beep in 2 minutes."
- Review the visual sound schedule for school days: "At 10:00, the bell will ring. You know it's coming."
- Practice predictive scanning: "Look around — do you see anything that might make a sound? What about that dog? Good spotting!"
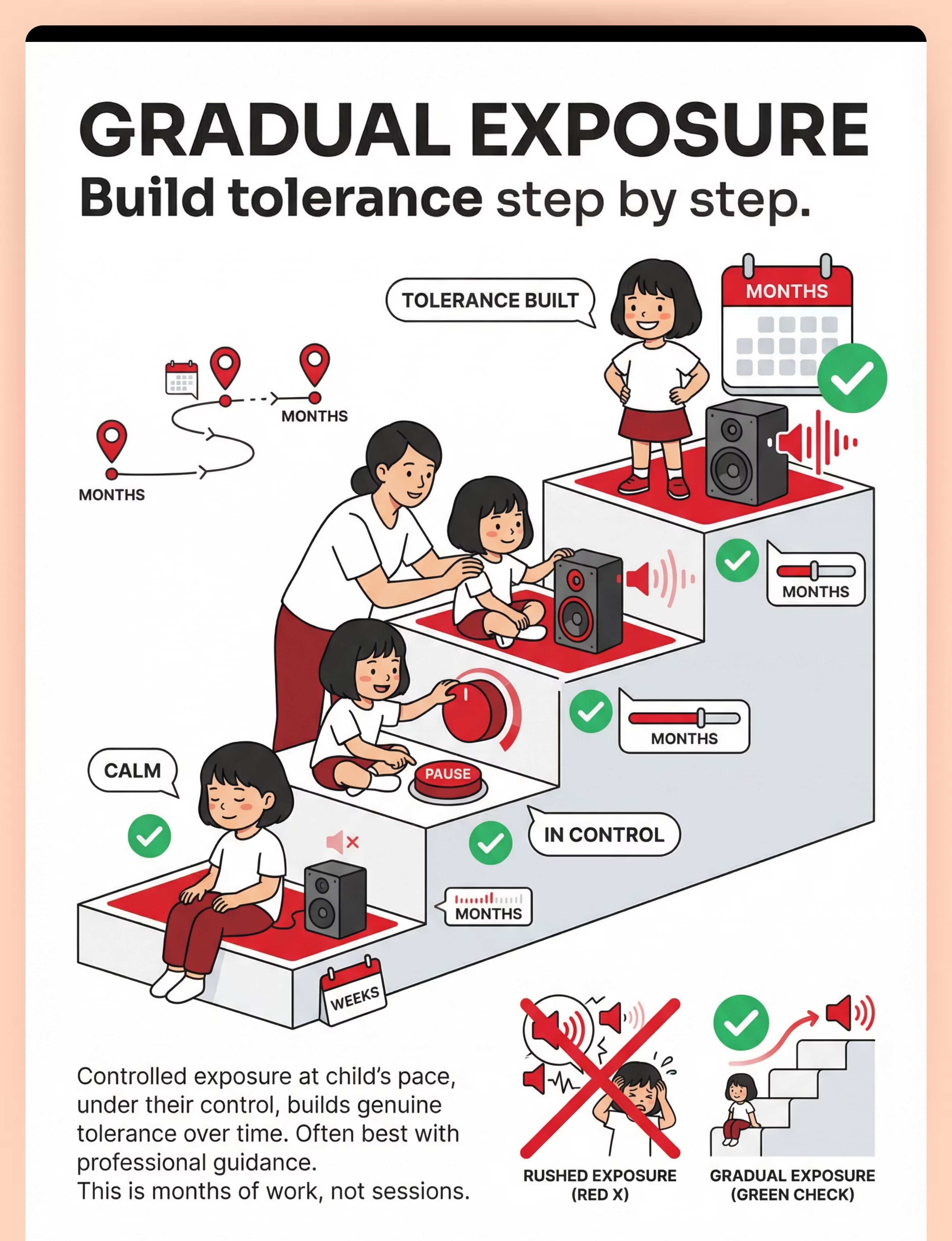
Strategy C: Gradual Exposure (Advanced — after weeks of A and B)
- Child holds device with feared sound recording. Volume at minimum. Child presses play.
- If calm: "Good! You heard that and you're fine. Want to hear it again?"
- Repeat 3–5 times at same volume.
- Do NOT increase volume today unless child specifically asks or appears completely unbothered.
- End on success. The session goal is not to push limits — it's to build a successful experience.
Child Response Spectrum:Ideal = engages with reduced anxiety. Acceptable = participates with visible tension but completes the activity. Concerning = escalates → STOP. End gently. This is data showing the step was too big. Reference: PMC10955541 — home sessions 10–20 minutes with core action occupying 40–60% of time.

Step 4 of 6
Repeat & Vary — Therapeutic Dosage
Protective Buffering
Duration-based, not repetition-based. 10–20 minutes of protected environmental exposure, daily if possible. Vary the environments: today the kitchen, tomorrow the park, next day a shop. Each new environment expands the child's functional world.
Prediction Practice
Embedded throughout the entire day — not a "session" but a lifestyle change. Every family member gives warnings. The visual schedule is checked every morning. This becomes household culture. Within 1–2 weeks, your child's body language will begin to change when you give warnings.
Gradual Exposure Dosage
- Target: 3–5 repetitions per session
- Same volume, same sound, same session
- Vary across SESSIONS (not within): different feared sounds on different days
- Week 1: Dog bark at volume 1, 3–5 reps daily
- Week 2: Same sound, same volume, but less warning before play
- Week 3: IF clearly comfortable, increase to volume 1.5
- The pace is the child's. Not yours.
Variation Options
- Different feared sounds (dog, bell, balloon, thunder — one per session)
- Different environments for protective strategy
- Different times of day for exposure
- Different calming objects as anchor (child chooses)
Satiation Indicators — When to Stop
- Child says "enough" or "done" (verbally or by gesture)
- Child's attention wanders significantly
- Child begins to escalate after initial calm
- Session has reached 15–20 minutes
"3 good repetitions are worth more than 10 forced ones."

Step 5 of 6
Reinforce & Celebrate — Within 3 Seconds
Reinforcement timing is clinical, not casual. The praise must come within 3 seconds of the desired behavior for the brain to associate the action with the positive outcome.
For Wearing Ear Protection
✓ "You wore your sound shields the entire walk! That's incredible."
✗ "Good job." — Too vague. The brain needs specific feedback to know what to repeat.
✗ "Good job." — Too vague. The brain needs specific feedback to know what to repeat.
For Tolerating a Sudden Sound
✓ "A dog barked and you just covered your ears — no screaming, no running. That's HUGE progress."
✗ "See, that wasn't so bad." — Dismissive of their genuine experience.
✗ "See, that wasn't so bad." — Dismissive of their genuine experience.
For Completing an Exposure Repetition
✓ "You pressed play three times all by yourself. You're in charge of those sounds now."
✗ "You need to do more next time." — Undermines the current success entirely.
✗ "You need to do more next time." — Undermines the current success entirely.
For Using a Breathing Card
✓ "You used your breathing square when that sound surprised you. Your body calmed down so fast."
Verbal Praise
Immediate, specific, enthusiastic
High-Five / Thumbs Up
Child's preferred physical celebration
Sticker Chart
"Sound bravery chart" visible in the home
Token Reward
Toward a chosen activity reward
Extra Story
At bedtime as session reward
"Celebrate the attempt, not just the success. A child who agreed to hold the ear defenders — even if they didn't put them on — just took a step."

Step 6 of 6
The Cool-Down — No Session Ends Abruptly
Abrupt endings dysregulate children who are already managing high sensory and emotional loads. The cool-down is a clinical step, not a courtesy.
Transition Warning
"Two more minutes, then we'll finish our sound practice for today." "One more time hearing the sound, then we're all done."
Remove/Set Aside Materials
Set aside exposure materials (tablet, recordings). Child keeps calming object if desired.
Calming Sensory Input
Soft music (predicted, not sudden), gentle rocking if child seeks movement, deep pressure hug if child consents.
Breathing Together
One round of square breathing together. "Great session today. You're getting stronger with sounds every time."
Material Put-Away Ritual
Let the child put their ear defenders in their designated spot. Let them turn off the white noise machine. Participation in the ritual gives closure and ownership.
Restore Choice
"Sound practice is done. What would you like to do now?" Give the child choice to restore sense of control after a challenging experience.
If Child Resists Ending: This is a positive sign — they're engaged. Allow 1–2 more minutes, then firmly but gently close: "We'll do more tomorrow. I promise."
Capture the Data — Right Now
60 seconds of data immediately after a session saves hours of guessing, prevents repeating unhelpful approaches, and gives your therapist the information they need to guide you accurately.
Data Point 1: Strategy Used
- ☐ Protective Buffering (ear defenders, white noise)
- ☐ Predictability Enhancement (warnings, schedule)
- ☐ Gradual Exposure (sound recordings)
- ☐ Combination
Data Point 2: Peak Response
- ☐ 5 — Extreme startle (screaming, running, >10 min recovery)
- ☐ 4 — Significant (crying, ear covering, 5–10 min recovery)
- ☐ 3 — Moderate (flinch, brief distress, 1–5 min recovery)
- ☐ 2 — Mild (notices sound, brief pause, <1 min recovery)
- ☐ 1 — Minimal (brief awareness, immediate return)
- ☐ 0 — No observable startle
Data Point 3: Anticipatory Anxiety
- ☐ High — Tense, scanning, hypervigilant throughout
- ☐ Medium — Some tension but redirectable
- ☐ Low — Appeared relaxed most of the session
- ☐ None — No anticipatory behaviors displayed
Data Point 4: Duration
Minutes of participation: ______
📥 Download Pinnacle Sound Sensitivity Tracker — PDF
📱 Log in GPT-OS® child developmental profile
📱 Log in GPT-OS® child developmental profile

Session Abandonment Is Not Failure — It's Data
Every problem has a clinical reason and a clinical fix. These six scenarios are the most common — read them before you interpret a difficult session as evidence that the protocol isn't working.
Child refused to wear the ear defenders
Why: New objects near ears can feel threatening. Ear defenders may feel too tight, too heavy, or too "different."
Fix: Let the child hold them, examine them, play with them without wearing them. Wear them yourself first. Put them on a stuffed animal. Try headband-style alternatives. Build familiarity over days before expecting wear.
Fix: Let the child hold them, examine them, play with them without wearing them. Wear them yourself first. Put them on a stuffed animal. Try headband-style alternatives. Build familiarity over days before expecting wear.
The sound recording caused a meltdown
Why: Volume was too high, child wasn't ready, or session was attempted when already dysregulated.
Fix: Start at a volume so low YOU can barely hear it. Ensure the child was in a fully green readiness state. Next session: lower volume, shorter duration, more calming support present.
Fix: Start at a volume so low YOU can barely hear it. Ensure the child was in a fully green readiness state. Next session: lower volume, shorter duration, more calming support present.
Child won't enter any environment, even with protection
Why: Anticipatory anxiety may be at clinical levels. Avoidance has been reinforced over time.
Fix: Start smaller — much smaller. Open a window for 1 minute instead of going outside. Watch a video of the feared environment before going there. Build toward the environment in micro-steps.
Fix: Start smaller — much smaller. Open a window for 1 minute instead of going outside. Watch a video of the feared environment before going there. Build toward the environment in micro-steps.
Verbal warnings seem to make things worse
Why: Warnings may be inadvertently communicating that the sound IS threatening. The warning voice may carry parental anxiety.
Fix: Deliver warnings casually: "Oh, I'm gonna close this" (casual) vs. "I need you to know that the door is going to close now" (anxious). The goal is information, not alarm.
Fix: Deliver warnings casually: "Oh, I'm gonna close this" (casual) vs. "I need you to know that the door is going to close now" (anxious). The goal is information, not alarm.
Child was calm during the session but melted down an hour later
Why: Delayed stress response. The child may have been masking or suppressing during the session, and the emotional load released later.
Fix: Add a longer decompression period after sessions. Reduce intensity next time. Watch for masking behaviors during sessions — frozen stillness, flat affect, or over-compliance are all signs.
Fix: Add a longer decompression period after sessions. Reduce intensity next time. Watch for masking behaviors during sessions — frozen stillness, flat affect, or over-compliance are all signs.
Three weeks in and no improvement
Why: This is a months-long process. 3 weeks is barely the beginning. Neural recalibration requires consistent, repeated, safe exposure over extended periods.
Fix: Continue. Review your data. Are the daily protection strategies in place? Is the prediction culture established? Small improvements compound. If no change after 8+ weeks, consult a professional OT or psychologist.
Fix: Continue. Review your data. Are the daily protection strategies in place? Is the prediction culture established? Small improvements compound. If no change after 8+ weeks, consult a professional OT or psychologist.
Adapt & Personalize — No Two Children Are Identical
The protocol is a framework, not a script. Use this guide to calibrate the approach for your child's unique profile, current state, and developmental stage.
← EASIER
For bad days, early stages, or younger children:
- Use only protective strategies — no exposure
- Shorter duration (5 minutes)
- More calming supports present simultaneously
- Stay in familiar, controllable environments only
- Parent provides all predictions — child doesn't need to self-scan yet
HARDER →
For good days, advanced stages, or older children:
- Gradual reduction of ear protection (one ear uncovered, then both briefly)
- Incrementally increase exposure session volume
- Introduce less predictable environments with protection
- Child begins self-warning (looking for sound cues independently)
- Practice recovery from unexpected sounds with breathing techniques
Ages 3–4 Years
Mostly protective strategies + prediction. Exposure is play-based (stuffed animal "hears" the sound first). Minimal demand. Maximum choice. The child is learning that these materials are friends, not threats.
Ages 5–7 Years
All three strategies. Visual schedules prominent. Begin exposure hierarchies with child control. Breathing card practice as a daily habit. Begin building the vocabulary of "my ears feel different."
Ages 8–12 Years
Add cognitive component — explain WHY they're doing each strategy. Self-monitoring. Self-advocacy for school accommodations. Older children can understand: "We're training your brain to feel safer around sounds."
Sensory Seeker–Avoider Mix: If your child seeks some sounds but avoids others, use the sounds they love as "bridge" experiences. If they love music but fear barking, play their favorite music very quietly in the background during exposure to a recorded bark. The positive association transfers.

Week 1–2: Progress Is Measured in Seconds, Not Transformations
Progress Arc — Week 1–2
~15% of Journey
✓ Child accepts wearing ear defenders
Even briefly — even holding them. Each second of contact is neural change.
✓ Family has begun verbal warning culture
"I'm going to..." is now part of daily household language. Every family member is participating.
✓ White noise is playing during at least one high-risk daily period
Kitchen, car, bedtime. The sonic landscape has changed.
✓ Child has visited the designated quiet space voluntarily at least once
They know where it is. They know it's theirs. That knowledge alone reduces anticipatory anxiety.
✓ First exposure session attempted
Even if only one 2-second play at minimum volume. That is a milestone. That is the beginning of recalibration.
Normal at This Stage: Child's startle response to real-world sounds may be UNCHANGED — that is expected. You are building infrastructure, not yet seeing results. What IS progress: willingness, cooperation, and seconds. Not yet expected: tolerating sudden sounds without reaction, attending birthday parties, anticipatory anxiety disappearing.

Week 3–4: The Neural Pathway Is Forming
Progress Arc — Week 3–4
~40% of Journey
Reaches for Ear Defenders Independently
Before entering feared environments. Without being reminded. This is internalization — the protective strategy has become the child's own.
Uses Calming Object Without Prompting
The anchor object has been incorporated into the child's self-regulation repertoire. They reach for it instinctively.
Verbal Warnings Visibly Reduce Tension
You give the warning and watch their shoulders drop. Their body is responding to prediction. The amygdala is beginning to trust that information is available.
Child May Begin Self-Warning
"Mama, I see a dog." Environmental scanning emerging. The child is becoming their own safety system — a profound developmental shift.
Recovery Time Has Decreased
From 15 minutes to 5–8 minutes after unexpected sounds. The nervous system is learning to return to baseline faster. This is measurable neurological change.
"You may notice you're more confident too. You're not avoiding outings as much. You're preparing instead of canceling. Your own anticipatory anxiety is decreasing alongside your child's."

Week 5–8: From Surviving Sounds to Managing Them
Progress Arc — Week 5–8
~75% of Journey
Mastery Criteria
- Startle response decreased in intensity: from screaming → flinch
- Recovery time under 2 minutes for most sounds
- Child uses protective tools independently
- Anticipatory anxiety significantly reduced — enters environments without prolonged negotiation
- Tolerates recorded feared sounds at moderate volume with minimal distress
- Exposure hierarchy progressed through 3+ levels
- Breathing/regulation strategies used independently during and after startle events
- School participation improved with accommodations in place
Generalization Indicators
- Child manages a real-world sudden sound using tools WITHOUT parental prompting
- Child attends a social event (party, restaurant, outing) with protection and participates for a meaningful duration
- Child's anxiety about sound environments decreased — agrees to go places with less pre-event distress
"Mastery Unlocked" Badge Criteria: When the child demonstrates functional tolerance across 3+ environments over 2 consecutive weeks, the Mastery Badge for Auditory Startle Modulation Level 1 is achieved in the GPT-OS® developmental profile.
You Did This. Your Child Grew Because of Your Commitment.
Eight weeks ago, your child couldn't walk to school without bracing for a dog bark. They couldn't attend a birthday party. They couldn't sit in the kitchen while you cooked. Every moment was haunted by the possibility of the next unexpected sound.
Today, they have a toolkit. Ear defenders that make them feel safe. Breathing exercises that help them recover. The ability to predict sounds before they happen. A quiet space that is theirs. And — slowly, steadily — a nervous system that is learning that not every unexpected sound is a threat.
"You are not just a parent. You are your child's first therapist, their safety net, their sound-proofer, and their courage-builder. This work you've done at home — every verbal warning, every breathing exercise, every gentle exposure — is clinical-grade intervention delivered with unconditional love."
Sound Bravery Certificate
Create one with your child's name, the date, and what they achieved. Frame it.
Take a Photo
At a place your child couldn't visit 8 weeks ago. Now they can. Document the transformation.
Write It Down
What your child could do today that they couldn't do before. Name every milestone, however small.
Tell Your Family
"Look what [child's name] achieved." Let everyone who loves this child witness their growth.

Red Flags: When to Pause and Seek Help
Trust your instincts. If something feels wrong, pause. The protocol is powerful, but some situations require more than a home-based approach.
🚩 Regression
Sound sensitivity significantly worsening despite 4+ weeks of consistent intervention — sounds that were previously tolerated are now triggering again. This is a signal to pause and consult.
🚩 Generalized Anxiety Expansion
Fear spreading from sounds to other sensory domains (now also afraid of lights, touch, movement) or to non-sensory fears. The anxiety has outgrown the auditory domain.
🚩 Self-Injurious Response
Child hitting their own ears, head-banging, scratching face, or engaging in other self-injurious behavior during or after startle events. Requires immediate professional evaluation.
🚩 Complete Social Withdrawal
Child refusing to leave the house/room entirely. Regression from partial participation to zero participation. The avoidance has become total.
🚩 Sleep Crisis
Unable to fall asleep or stay asleep for more than 2 consecutive weeks due to sound-related hypervigilance. Sleep deprivation compounds every sensory challenge.
🚩 Parent/Caregiver Burnout
You are experiencing significant anxiety, depression, or hopelessness related to managing this condition. Your wellbeing matters — seek support. You cannot pour from an empty vessel.
Minor Setbacks
Reduce intensity, return to earlier strategies, try again in a few days
Moderate Concerns
Teleconsultation via Pinnacle helpline: 9100 181 181
Significant Concerns
Comprehensive evaluation at nearest Pinnacle center
Urgent Concerns
NeuroDevelopmental Pediatrician evaluation for underlying conditions
Where You Were. Where You Are. Where You're Going.
Prerequisite Techniques
- ← A-043: Hums to Block Sound
- ← A-042: Cafeteria Sound Challenges
- ← General auditory over-responsivity awareness
Lateral Alternatives
- → A-046: Covers Ears Constantly
- → Music therapy approaches to auditory processing
- → Auditory Integration Therapy (professional-guided)
Next-Level Paths
Path A — Startle improving, generalize:
A-045: Voice Tone Sensitivity → Community sound exposure program
A-045: Voice Tone Sensitivity → Community sound exposure program
Path B — Specific sound phobias persist:
A-036: Hand Dryer Fear → A-037: Balloon Fear → A-041: Firework/Thunder Fear
A-036: Hand Dryer Fear → A-037: Balloon Fear → A-041: Firework/Thunder Fear
Path C — Anticipatory anxiety primary challenge:
Anxiety management (psychologist-led) → CBT for children 8+ → Mindfulness and body-scan interventions
Anxiety management (psychologist-led) → CBT for children 8+ → Mindfulness and body-scan interventions
Explore More Auditory Sensory Techniques
The materials you've gathered for A-044 are the foundation of an entire auditory sensory toolkit. Every related technique in this domain uses the same core materials — you're already equipped.
Technique | Level | Materials You Already Have | Key Overlap | |
A-036: Hand Dryer Fear | Intro | Ear defenders, exposure recordings | Protective buffering + gradual exposure | |
A-037: Balloon Fear | Intro | Ear defenders, gradual exposure | Impact sound desensitization | |
A-041: Firework/Thunder Fear | Core | White noise, ear defenders, safe space | Low-frequency sudden sound | |
A-042: Cafeteria Sound Challenges | Core | Ear defenders, visual schedule, calming object | Environmental participation | |
A-043: Hums to Block Sound | Intro | White noise, calming strategies | Self-generated sound masking | |
A-045: Voice Tone Sensitivity | Advanced | Exposure recordings, prediction strategies | Frequency-specific modulation | |
A-046: Covers Ears Constantly | Core | Ear defenders, gradual exposure, safe space | Chronic ear-covering behavior |
"You already own the materials for all 7 of these techniques." The investment you've made in this protocol unlocks an entire domain of auditory sensory work.

This Technique Is One Piece of a Larger Plan
Auditory startle modulation doesn't exist in isolation. When a child's sound sensitivity is addressed, the ripple effects touch nearly every domain of development.
→ Social (C)
Social participation increases as sound environments become manageable
→ Learning (D/J)
Classroom engagement and academic readiness improve when school bells and announcements no longer derail the day
→ Behavior (H)
Emotional regulation strengthens — the self-regulation tools built here transfer to all stress responses
→ Community (L)
Community integration expands — markets, temples, festivals, restaurants become accessible again
→ Family (K)
Family stress decreases, restriction decreases, and quality of life improves across the household
"Solving one challenge unlocks progress in many."
Real Families. Real Sound Sensitivity. Real Progress.
Priya, Mother — Hyderabad
Before:"Aarav couldn't go to the temple. The bells, the crowds, the sudden chanting — he would scream and try to run. We stopped going. We stopped going to restaurants. We stopped going to family gatherings. Our world shrank to our apartment."
After 4 months:"We started with ear defenders before every outing. I warned him about every sound I could predict. After 6 weeks, he would put them on himself and say 'ready, Amma.' After 3 months of gradual exposure with recordings, he attended his cousin's birthday party — with ear defenders — and stayed the whole time. He even blew out his own candle at his birthday."
"He went from a child who lived in fear to a child who carries his own toolkit."
Aisha, Mother — Mumbai
Before:"Zara couldn't be in the kitchen. A spoon dropping would send her under the table. The pressure cooker whistle was her worst enemy. Cooking dinner was a daily crisis."
After 3 months:"White noise in the kitchen changed everything instantly. Then I started warning: 'cooker in 2 minutes.' Then we practiced the cooker sound on my phone at low volume. Now she can be in the kitchen — not always happily, but she stays. She hears the cooker and says 'it's okay, it's the cooker.' That sentence from my child is worth everything."
From the Therapist's Notes: Both families demonstrate the three-layer approach: protection first (immediate anxiety reduction), prediction second (environmental mastery), exposure third (genuine tolerance building). The timeline — months, not weeks — is typical and expected. Neither child's startle response is eliminated, but it's managed. They have tools. That's the clinical definition of functional improvement. Note: Illustrative cases. Outcomes vary by child profile.
You Are Not a Solo Operator Anymore
The families navigating this challenge successfully are not doing it alone. Community is a clinical resource — peer knowledge, shared strategies, and the simple relief of being understood reduce parental anxiety and improve consistency.
Sound Sensitivity Parent Support Group
WhatsApp community for families navigating auditory startle, sound phobia, and auditory over-responsivity. Share strategies, ask questions, get peer support from parents who understand exactly what your mornings look like.
Pinnacle Parent Forum
Online community across all developmental challenges. Your experience helps others. When you share what worked, you save another parent months of searching. Join → pinnacleblooms.org/community
Local Parent Meetups
Monthly gatherings at your nearest Pinnacle center. Meet families navigating similar challenges. Children play together in sensory-friendly environments — a rare and precious gift. Find your local meetup → pinnacleblooms.org/events
Peer Mentoring
Connect 1:1 with a parent who has been through this journey. They know the terrain. Request a peer mentor through the helpline. 📞9100 181 181

Home + Clinic = Maximum Impact
The home protocol you're implementing is powerful. It becomes even more powerful when supported by a therapist who knows your child, can adjust the hierarchy, and can measure progress with clinical precision.
Services for Sound Sensitivity
- Occupational Therapy: Comprehensive Sensory Processing Evaluation, Auditory Modulation Assessment, individualized sensory diet, desensitization program design
- Psychological Support: Anticipatory anxiety evaluation, systematic desensitization, CBT for older children, family anxiety coaching
- Audiological Referral: Hearing evaluation, hyperacusis assessment, custom ear protection fitting
- NeuroDevelopmental Pediatrics: Medical evaluation, comorbidity assessment, medication consideration for severe anxiety
Find Your Support
🗺️ Find Your Nearest Pinnacle Center
70+ centers across India. Sensory-friendly environments. Trained multi-disciplinary teams.
70+ centers across India. Sensory-friendly environments. Trained multi-disciplinary teams.
📱Teleconsultation Available
Can't visit a center? Book a virtual session with a Pinnacle specialist. pinnacleblooms.org/teleconsult
Can't visit a center? Book a virtual session with a Pinnacle specialist. pinnacleblooms.org/teleconsult
📞FREE National Autism Helpline: 9100 181 181
Available 24/7 in 16+ languages. Ask anything. No commitment. Trained counselors who understand the Indian sensory landscape.
Available 24/7 in 16+ languages. Ask anything. No commitment. Trained counselors who understand the Indian sensory landscape.
"The most effective intervention combines professional clinical guidance with daily home execution. The techniques in this page are more powerful when supported by a therapist who knows your child."

Deeper Reading for the Curious Parent
The evidence behind this protocol is substantial, peer-reviewed, and internationally recognized. For parents, therapists, and program leads who want to go deeper:
PRISMA Systematic Review (2024) — Level I
Sensory integration intervention as evidence-based practice for ASD — 16 articles, 2013–2023. Auditory modulation interventions specifically demonstrated improvement in sound tolerance and reduced startle amplitude. PubMed: PMC11506176
Meta-Analysis, World J Clin Cases (2024) — Level I
Sensory integration therapy efficacy across 24 studies. Social skills, adaptive behavior, sensory processing, motor skills. Individually-administered sessions showed maximum effectiveness. PubMed: PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Indian Pediatric RCT (2019) — Level II
Home-based sensory interventions in Indian children — significant outcomes with parent-administered protocols. Safety monitoring confirmed parent-administered auditory desensitization is safe with proper guidance. DOI: 10.1007/s12098-018-2747-4
Frontiers in Integrative Neuroscience (2020) — Level III
Neurological framework establishing the basis for sensory processing interventions in ASD. Comprehensive mapping of startle reflex circuit, amygdala function, and prefrontal modulation. DOI: 10.3389/fnint.2020.556660
WHO Nurturing Care Framework (2018)
Early childhood development framework — responsive caregiving and early identification. Foundation for the home-execution approach in this protocol. nurturing-care.org
WHO Care for Child Development (CCD) Package
Implementation across 54 LMICs. Demonstrates household-material-based intervention efficacy in resource-variable settings — the foundation for the DIY alternatives in this protocol. PMC9978394
AOTA Clinical Guidelines
Auditory modulation and sensory processing. aota.org
SPD Foundation
Auditory startle hyperresponsivity research database. spdfoundation.net
NCAEP Report (2020)
Visual supports and video modeling as EBPs for autism.

Your Data Helps Every Child Like Yours
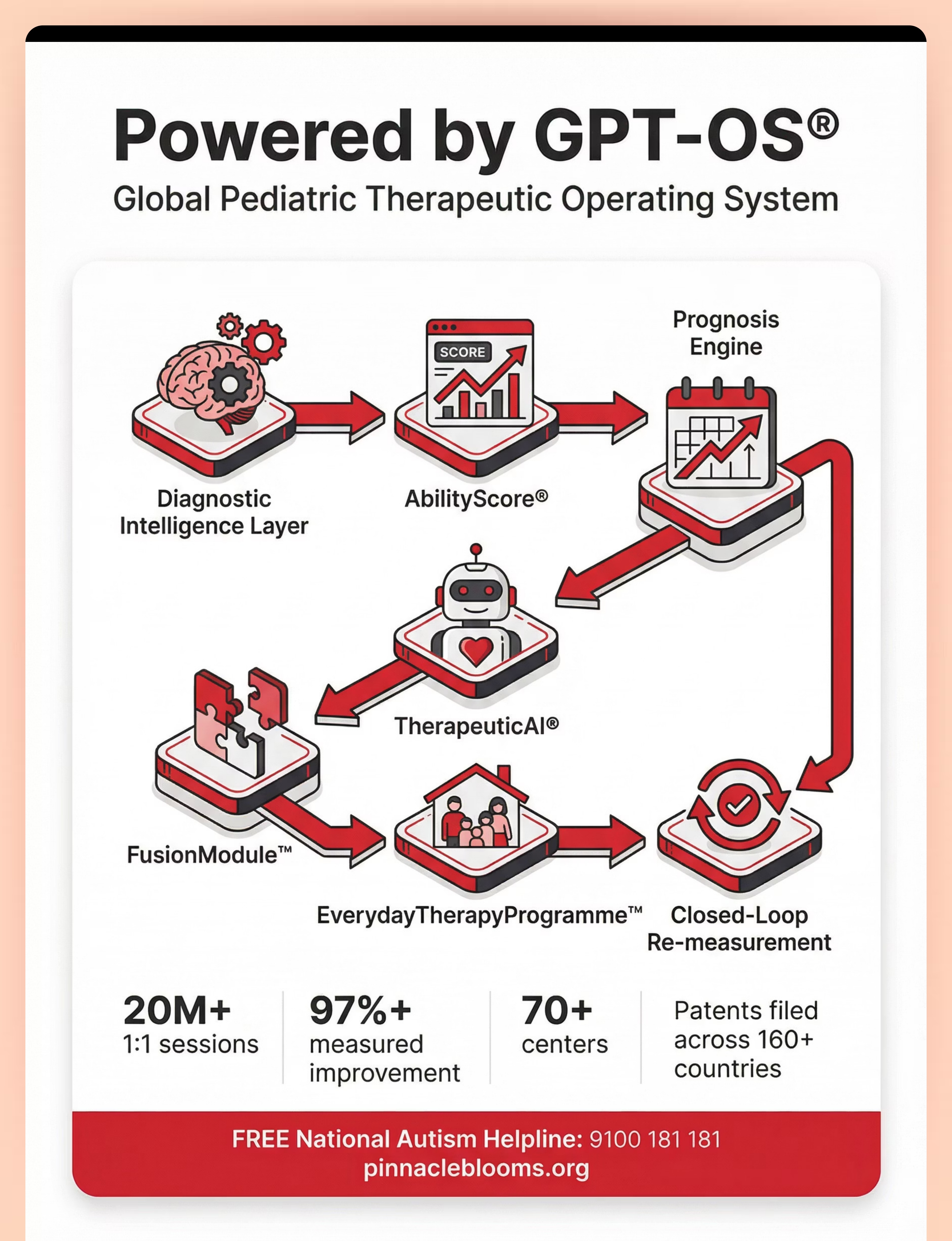
What GPT-OS® Learns from This Technique's Data
- Which protective tools are most effective for different startle profiles
- Optimal exposure progression rates — how fast to increase volume/complexity safely
- Prediction strategies with the highest anxiety-reduction impact
- Which age groups respond fastest to each strategy layer
- Environmental factors specific to India — festival seasons, monsoon thunder, urban vs. rural sound profiles — that affect outcomes
Privacy Assurances
- All data is anonymized and aggregated
- Individual child profiles are never shared with third parties
- Data stored under Indian data protection regulations
- Parents can request data deletion at any time
- GPT-OS® uses population-level patterns, not individual identification
"When you log your child's session, you're contributing to the largest pediatric therapy dataset in the world — 20M+ sessions across 70+ centers. Your data helps researchers, therapists, and families you'll never meet. That's the power of the Pinnacle network."
See It in Action
Reel A-044
Sensory Solutions Series — Episode 44
9 Materials That Help With Sudden Sound Reactions
Watch a Pinnacle OT specialist demonstrate each of the 9 materials with a child — explaining how each one addresses the startle response and the anticipatory anxiety beneath it. Seeing the materials in use with a real child transforms your confidence as a caregiver.
Domain: Sensory Processing → Auditory Over-Responsivity → Startle Response
Presenter: Pinnacle OT specialist with expertise in auditory sensory processing
Length: ~6 minutes
Presenter: Pinnacle OT specialist with expertise in auditory sensory processing
Length: ~6 minutes
Multi-Modal Learning: Research shows parent skill acquisition improves significantly with combined text + video instruction. This video reinforces the protocol you've just read through visual demonstration. NCAEP Evidence-Based Practices Report, 2020 — Video modeling as EBP for autism.

Consistency Across Caregivers Multiplies Impact
A child who receives verbal warnings from you but none from their grandparents, teacher, or second parent receives inconsistent prediction support — and their nervous system cannot consolidate safety. Share this page with everyone who cares for your child.
📱 Share via WhatsApp
Send this page to your spouse, grandparents, and anyone who cares for your child. The more consistently the strategies are applied, the faster the nervous system recalibrates.
📧 Share via Email
Include the full link for teachers, school counselors, and therapists. techniques.pinnacleblooms.org
📥 Download Family Guide PDF
A simplified 1-page summary: wear ear protection before noisy environments; warn before every predictable sound; keep the quiet space available; keep the calming object accessible; practice breathing when calm; never force exposure — let the child control the pace.
👴 Explain to Grandparents
"[Child's name] has a nervous system that overreacts to sudden sounds. It's not a behavior choice — it's a wiring difference. You can help by: (1) warning before you make sounds: 'I'm going to close this door'; (2) letting them wear their ear protectors without judgment; (3) not forcing them to 'get used to it' — that makes it worse. Ask them where their quiet space is. Follow their lead."
🏫 Teacher Communication Template
"Dear [Teacher], [Child's name] has auditory startle sensitivity. Recommended accommodations: (1) ear defenders permitted in classroom; (2) advance warning before school bells/announcements when possible; (3) designated quiet space for recovery; (4) break card system to exit to quiet area as needed. Contact: [parent phone] or Pinnacle Blooms helpline 9100 181 181."
Reference: WHO CCD Package — Multi-caregiver training is critical for intervention generalization. PMC9978394

Frequently Asked Questions
Is my child's extreme startle response a sign of autism?
Not necessarily. Exaggerated startle responses occur in children with ASD, Sensory Processing Disorder, anxiety disorders, PTSD, and sometimes in neurotypical children with heightened sensory sensitivity. An exaggerated startle response alone doesn't indicate autism, but it is one of many sensory processing differences common in autism. A comprehensive developmental evaluation — like Pinnacle's AbilityScore® assessment — can provide clarity.
Will my child grow out of this?
Some children's auditory modulation naturally improves with neurological maturation (particularly around ages 6–8). However, without intervention, many children develop entrenched avoidance patterns and anxiety that persist into adulthood. Intervention during the 3–8 year window produces the best outcomes. Even if the startle reflex remains somewhat exaggerated, learning management tools transforms the child's functional capacity entirely.
Isn't wearing ear defenders just avoidance? Won't it create dependence?
No. Ear defenders worn preventively ENABLE participation. A child who wears ear defenders to a party ATTENDS the party. A child without them stays home. Protection is a bridge — not a destination. Over time, with gradual exposure, the child needs less protection. But the protection allows them to be present in the environments where desensitization naturally occurs.
Can I do the gradual exposure myself, or do I need a therapist?
Mild-to-moderate startle sensitivity can be addressed at home following this protocol. For severe sound phobias — child is completely homebound, non-functional, or has comorbid anxiety disorders — professional guidance from an OT or psychologist experienced in systematic desensitization is strongly recommended. Exposure done incorrectly can increase fear.
My child is fine with LOUD sounds but panics at QUIET unexpected sounds. Is that possible?
Yes. This is the hallmark of startle hyperresponsivity — the trigger is unpredictability, not volume. A child may enjoy loud music (predicted, controlled) but panic at a pen dropping (unpredicted, uncontrolled). This distinction is critical for intervention: the strategies target unpredictability, not volume.
How long until we see real improvement?
Protection strategies often show immediate anxiety reduction. Prediction strategies show effect within 1–2 weeks. Genuine tolerance building through gradual exposure takes 2–6 months of consistent work. The startle reflex may always be somewhat more sensitive than typical, but the child's ability to manage it transforms completely.
Should I avoid all loud events like Diwali, weddings, and festivals?
Not forever. In the early stages, avoidance with occasional protected exposure is appropriate. As the child builds tolerance, attend WITH protection — ear defenders, white noise, safe space available, exit plan ready. The goal is not to avoid life — it's to equip your child to participate in life with appropriate support.
Didn't find your answer? 📞9100 181 181 — FREE National Autism Helpline | pinnacleblooms.org/teleconsult

You Know What To Do. Start Today.
"The window for intervention is now. Every day of consistent strategy application is a day of neural recalibration. The nervous system is not fixed — it is trainable."
🟥 Start This Technique Today
Download the free tracking sheet, gather your materials (even DIY versions), and begin with Strategy A: Protective Buffering. Put ear defenders on your child before the next outing. Give verbal warnings before the next sound you make. You can start RIGHT NOW.
🔵 Book a Consultation
Want professional guidance? Book a teleconsultation or visit your nearest Pinnacle center for a comprehensive sensory processing evaluation and personalized intervention plan.
📞9100 181 181 | pinnacleblooms.org/teleconsult
⬜ Explore Next Technique
Ready for more? Explore the next technique in the Auditory Sensory domain or browse all 70,000+ intervention techniques.
✅ Validated by Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev
20M+ Sessions | 97%+ Improvement | 70+ Centers
Preview of 9 materials that help with sudden sound reactions Therapy Material
Below is a visual preview of 9 materials that help with sudden sound reactions therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
The Pinnacle Promise
🏛️ Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
"From fear to mastery. One technique at a time."
A parent arrived on this page scared, confused, and exhausted. Now they understand the neuroscience, have a 9-material toolkit, know the step-by-step protocol, can track progress, know when to seek help, and are connected to a community of millions. The next technique awaits.
OT
Occupational Therapy
SLP
Speech-Language Pathology
ABA
Applied Behavior Analysis
SpEd
Special Education
NeuroDev
NeuroDevelopmental Pediatrics
Medical Disclaimer: This content is educational and informational. It does not replace assessment, diagnosis, or treatment by a licensed occupational therapist, psychologist, audiologist, or healthcare provider. Extreme startle responses, significant sound phobias, or pervasive anticipatory anxiety may require comprehensive professional evaluation and guided intervention including systematic desensitization. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Always consult a healthcare provider for your child's specific needs.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
ISO 13485 — Medical Device QMS | ISO/IEC 27001 — Information Security
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
ISO 13485 — Medical Device QMS | ISO/IEC 27001 — Information Security
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
📞 FREE National Autism Helpline: 9100 181 181 | 🌐pinnacleblooms.org | 📧care@pinnacleblooms.org
📞 FREE National Autism Helpline: 9100 181 181 | 🌐pinnacleblooms.org | 📧care@pinnacleblooms.org