
The Blender Makes Her Scream. The Hand Dryer Is Torture. Birthday Parties End Under the Table.
The vacuum cleaner, the toilet flushing, the dogs barking, the fire alarm — sounds that other children don't even notice cause your child genuine pain. She covers her ears constantly. She refuses to go places. People tell you she's being dramatic. She's not. The sounds actually hurt her. Her nervous system turns up the volume on everything.
You are not failing. Your child's nervous system is speaking.
This page gives you 9 materials that help make the sound world bearable — backed by clinical research, used across 70+ Pinnacle Blooms centers, and designed for you to start at home today.
Sensory Solutions Series — Episode A-031
Age Band: 2–12 Years
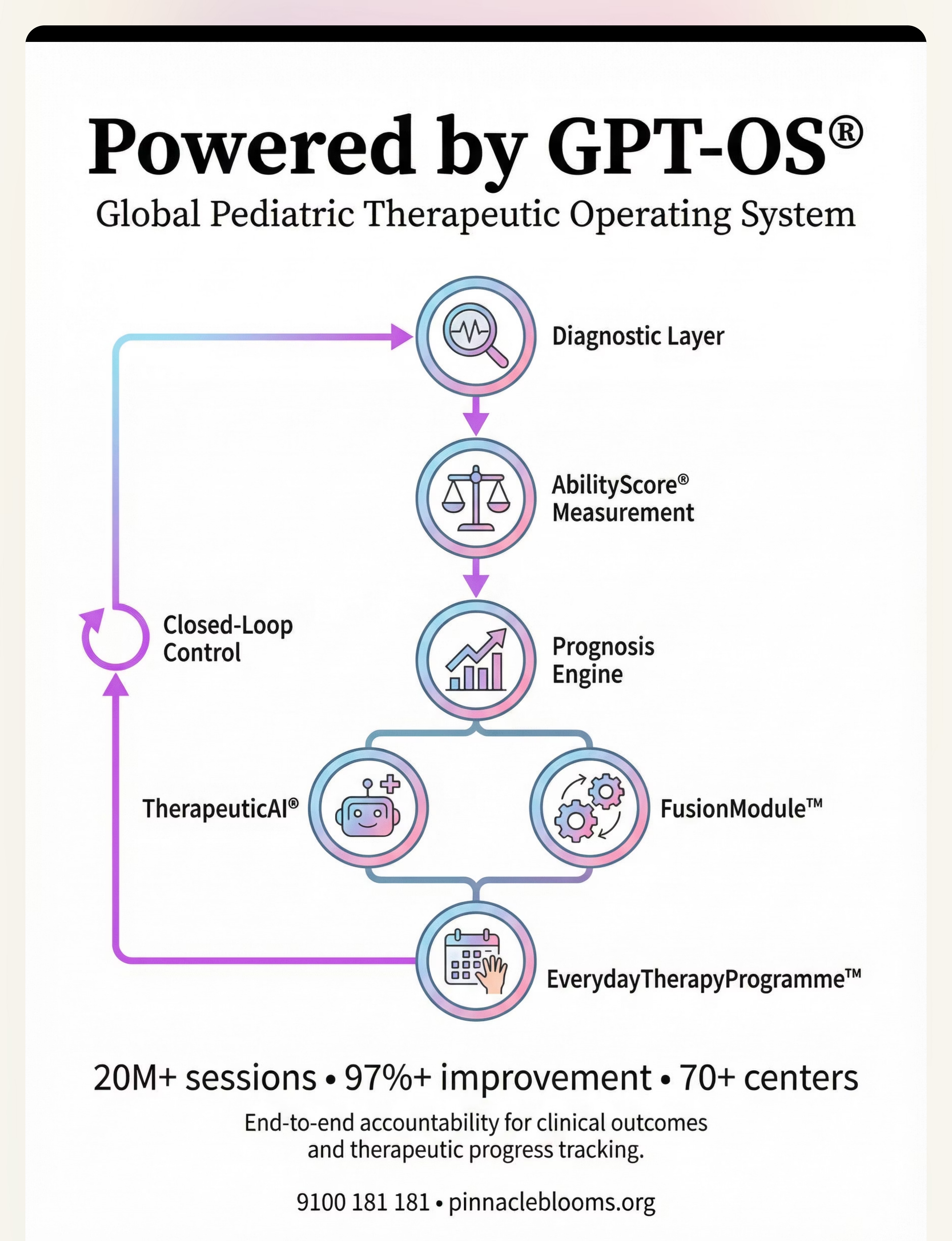
Pinnacle Blooms Network® — Built by Mothers. Engineered as a System. Powered by GPT-OS®

You Are Among Millions.
Sound sensitivity — clinically termed auditory over-responsivity — is one of the most common sensory processing differences in children. It is recognized by the WHO, documented across UNICEF developmental frameworks, and addressed by every major pediatric therapy discipline. This is not rare. This is not unusual. This is a well-understood neurological pattern with evidence-based interventions.
80%
Sensory Difficulties
of children diagnosed with autism experience sensory processing difficulties, including auditory over-responsivity
1 in 6
Primary Concern
children with sensory processing differences show clinically significant auditory over-responsivity
54
Countries
have implemented the WHO Care for Child Development Package, validating caregiver-led sensory interventions
Sources: PRISMA Systematic Review, Children (2024) | PMC11506176 · Meta-analysis, World Journal of Clinical Cases (2024) | PMC10955541 · PMC9978394 | WHO/UNICEF CCD Package (2023)
The Volume Control Is Set Too High.
What's Happening in Your Child's Brain
Auditory over-responsivity occurs when the brain's sound processing system registers everyday sounds more intensely than typical. Think of it as the brain's volume control stuck at maximum — sounds that register at "3" for most people come in at "8" or "9" for your child.
The nervous system amplifies incoming sound. The somatosensory and auditory cortex process sound input at a higher gain. Background sounds that most brains automatically filter — the hum of lights, distant traffic, a ticking clock — remain loud and salient.
The startle response is heightened. Unexpected sounds trigger the fight-or-flight system disproportionately. Even moderate sounds create a threat response.
Auditory fatigue accumulates. Processing everything at high volume is exhausting. Your child becomes progressively more sensitive as the day goes on. Morning tolerance dissolves into afternoon meltdowns — not from behavior, but from cumulative auditory overload.
Anxiety amplifies sensitivity. Anticipating potentially loud sounds keeps the nervous system in a state of vigilance, which further increases sensitivity. Sound and anxiety feed each other in a relentless cycle.
This is a wiring difference, not a behavior choice. The distress is real. The discomfort is genuine. The avoidance is protective, not manipulative.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660

Your Child Is Here. Here Is Where We're Heading.
Sound sensitivity follows a recognizable developmental trajectory. Understanding where your child sits on this timeline helps you anticipate challenges and celebrate progress in context.
0–6 Months
Startle responses to loud sounds emerge as a typical developmental milestone
6–12 Months
Sound localization develops; some infants show early signs of auditory sensitivity
1–2 Years
Sound preferences and aversions become more apparent; covering ears may begin
2–4 Years ★
Common emergence zone: Sound sensitivity becomes clinically significant — avoidance behaviors crystallize, specific triggers identified, social participation affected
4–7 Years
School entry creates new sound challenges — cafeterias, assemblies, bells, fire drills, playground noise
7–12 Years
Self-awareness emerges; child may develop anxiety, avoidance patterns, or compensatory strategies
Comorbidity Awareness: Sound sensitivity commonly co-occurs with tactile over-responsivity, visual sensitivity, anxiety disorders, ADHD, and broader sensory processing differences. A comprehensive sensory evaluation may reveal related patterns.
References: WHO Care for Child Development (CCD) Package | PMC9978394 | UNICEF MICS indicators

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I–II
Supported by Systematic Reviews & RCTs
PRISMA Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria for children with ASD
Meta-Analysis (2024)
24 studies demonstrate sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills
Indian RCT (2019)
Padmanabha et al. validates home-based sensory interventions with significant outcomes in Indian pediatric population
80%
Confidence Level
Strong evidence base with active ongoing research
PubMed: PMC11506176 · PMC10955541 · DOI: 10.1007/s12098-018-2747-4 · DOI: 10.3389/fnint.2020.556660

ACT II: KNOWLEDGE TRANSFER
The Technique: What It Is
Technique Profile
Formal Name: Auditory Sensory Modulation Materials Intervention
Parent-Friendly Alias: "9 Materials That Help With Sound Sensitivity"
Canon Code: SEN-AUD-OVER
Age Range: 2–12 years
Setting: Home + Therapy + School + Community
Duration: Ongoing daily use with graduated exposure protocols
Definition
A multi-material, environment-modification approach to managing auditory over-responsivity in children. This technique introduces 9 categories of tools — from immediate protection (noise-reducing headphones, earplugs) to environmental management (white noise, quiet spaces) to professional intervention (therapeutic listening programs) — that together create a layered strategy for making the sound world bearable.
Each material addresses a different aspect of the sound challenge: some reduce volume, some increase predictability, some provide retreat, some build tolerance. Used together and personalized to your child's specific triggers, they transform daily environments from sources of distress to spaces of managed participation.
This Technique Crosses Therapy Boundaries
Because the brain doesn't organize by therapy type, this toolkit draws expertise from multiple disciplines. Each professional brings a unique lens to your child's sound sensitivity.
Occupational Therapist (OT) — Primary Lead
Conducts comprehensive sensory processing evaluation. Administers Sensory Profile assessments. Designs personalized auditory desensitization programs. Implements therapeutic listening protocols. Guides material selection (NRR ratings, headphone fit, earplug sizing).
Speech-Language Pathologist (SLP)
Addresses auditory processing as it impacts language comprehension. Works on listening skills in managed sound environments. Collaborates on communication strategies for the child to express sound distress.
Board Certified Behavior Analyst (BCBA)
Conducts functional assessment of sound-avoidance behaviors. Designs reinforcement schedules for graduated sound exposure. Creates behavioral protocols for headphone/earplug use and addresses anticipatory anxiety.
NeuroDevelopmental Pediatrician & Special Educator
Rules out medical causes of hyperacusis, evaluates comorbid conditions, coordinates IEP/504 plan accommodations for sound sensitivity, and implements classroom modifications.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) | DOI: 10.1080/17549507.2022.2141327
This Is Not a Random Activity. It's a Precision Toolkit.
Every material in this toolkit targets specific, measurable outcomes across three levels of developmental impact.
The primary target is reducing the intensity of sound input reaching your child's nervous system and building tolerance for environmental sounds. Observable indicators include reduced ear-covering frequency, fewer meltdowns in noisy environments, and willingness to enter previously-avoided spaces. Secondary targets include anxiety reduction, increased social participation, and environmental adaptability. Long-term tertiary gains cascade into self-regulation, emotional regulation, daily living independence, and academic performance.
Reference: Meta-analysis (World J Clin Cases, 2024) — PMC10955541

Your Sound Sensitivity Toolkit — 9 Materials, 3 Categories
These 9 materials form a comprehensive, layered approach to managing your child's sound sensitivity. They range from immediate protection to long-term systemic support, and every family can start with at least some of them today.
Category 1
Immediate Protection
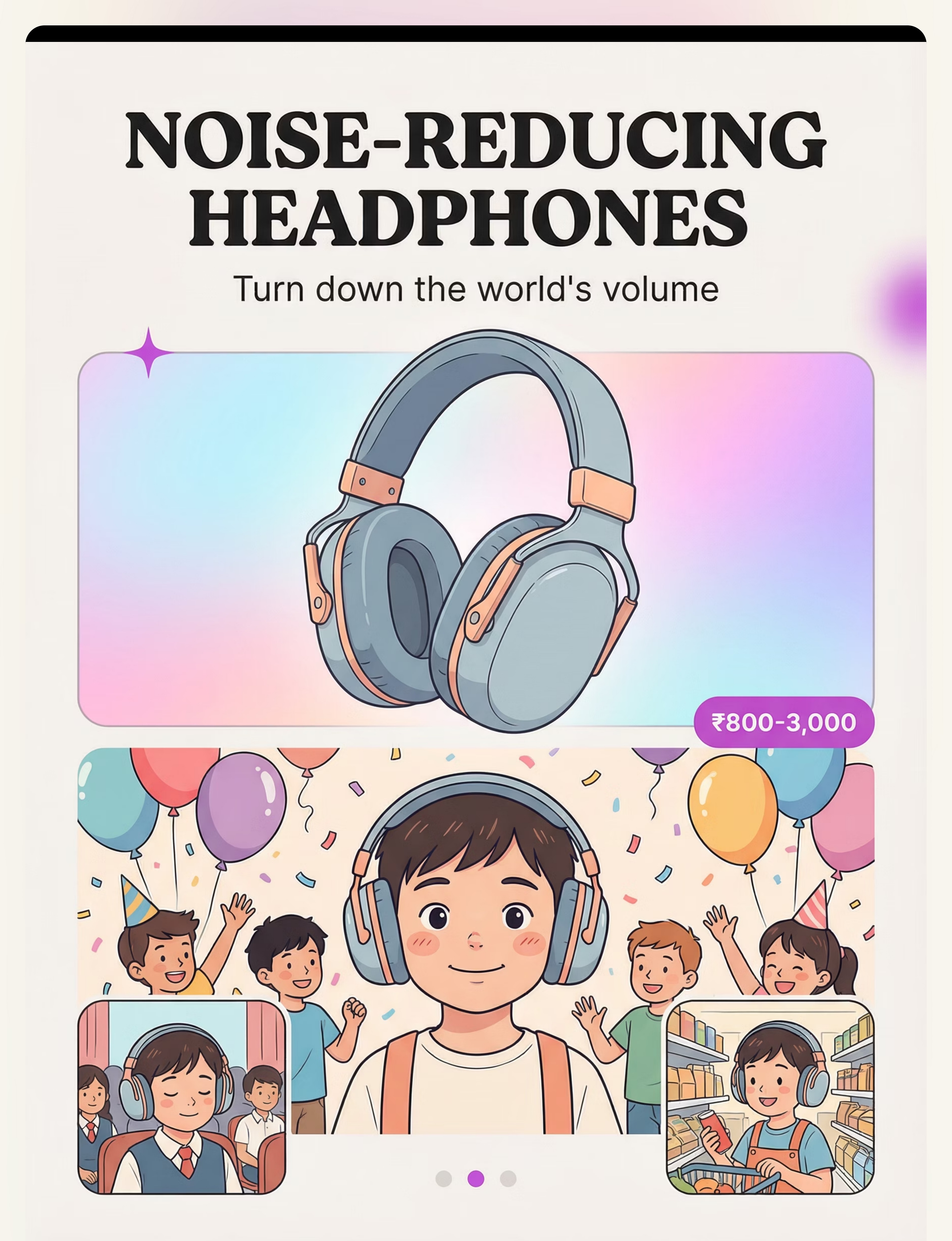
Noise-Reducing Headphones · Noise-Canceling Headphones · Filtered Earplugs
Noise-Reducing Headphones · Noise-Canceling Headphones · Filtered Earplugs
Category 2
Environmental Management
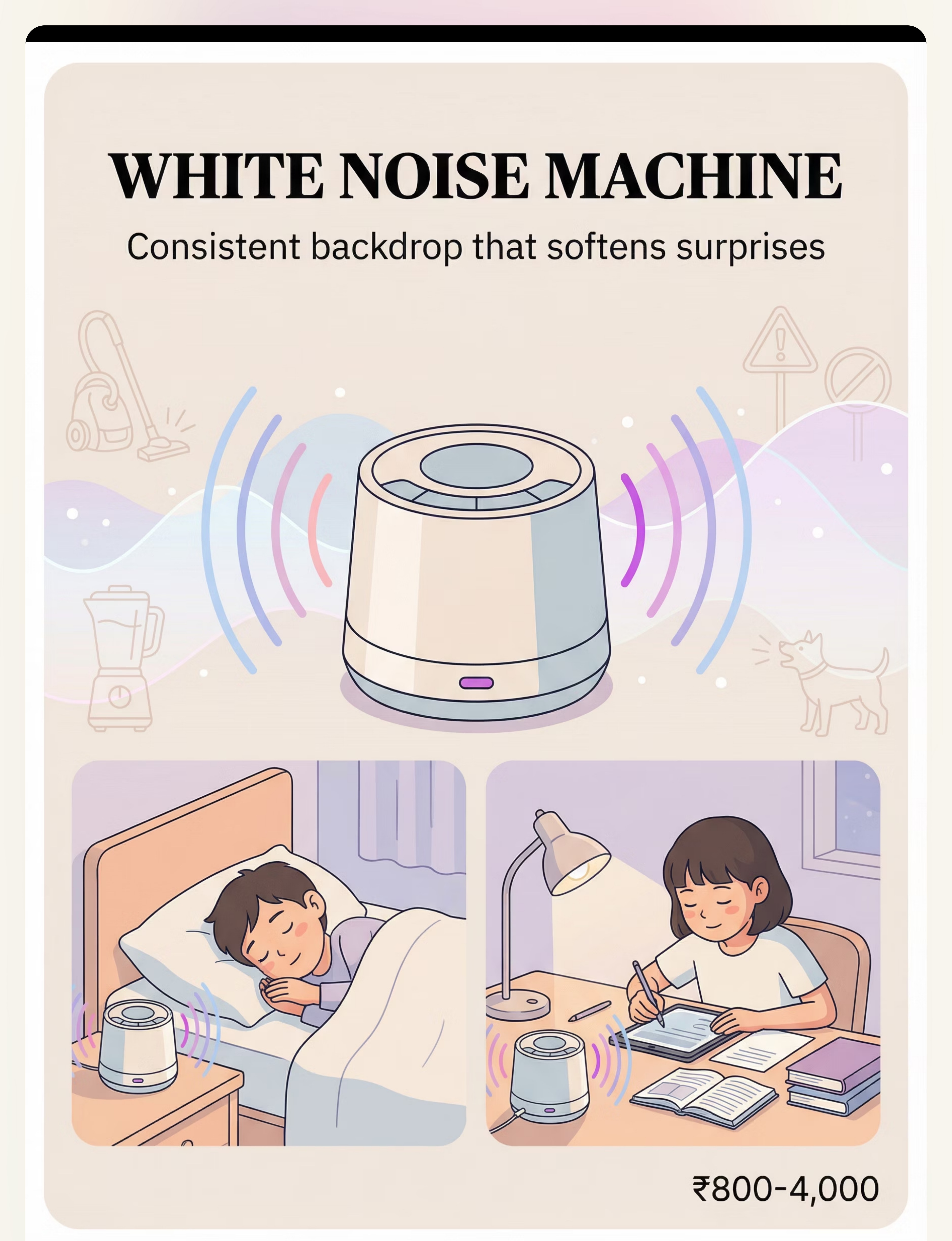
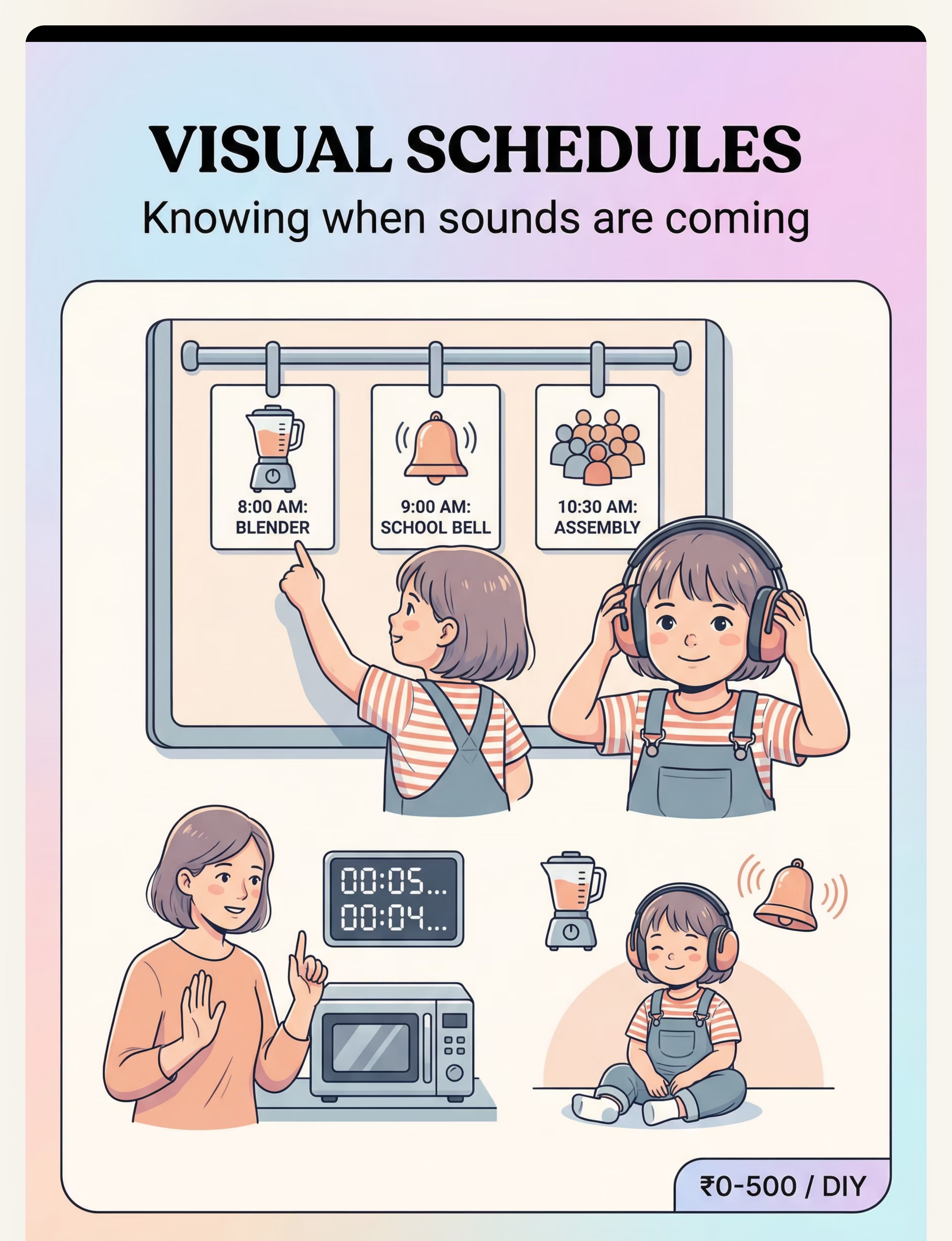
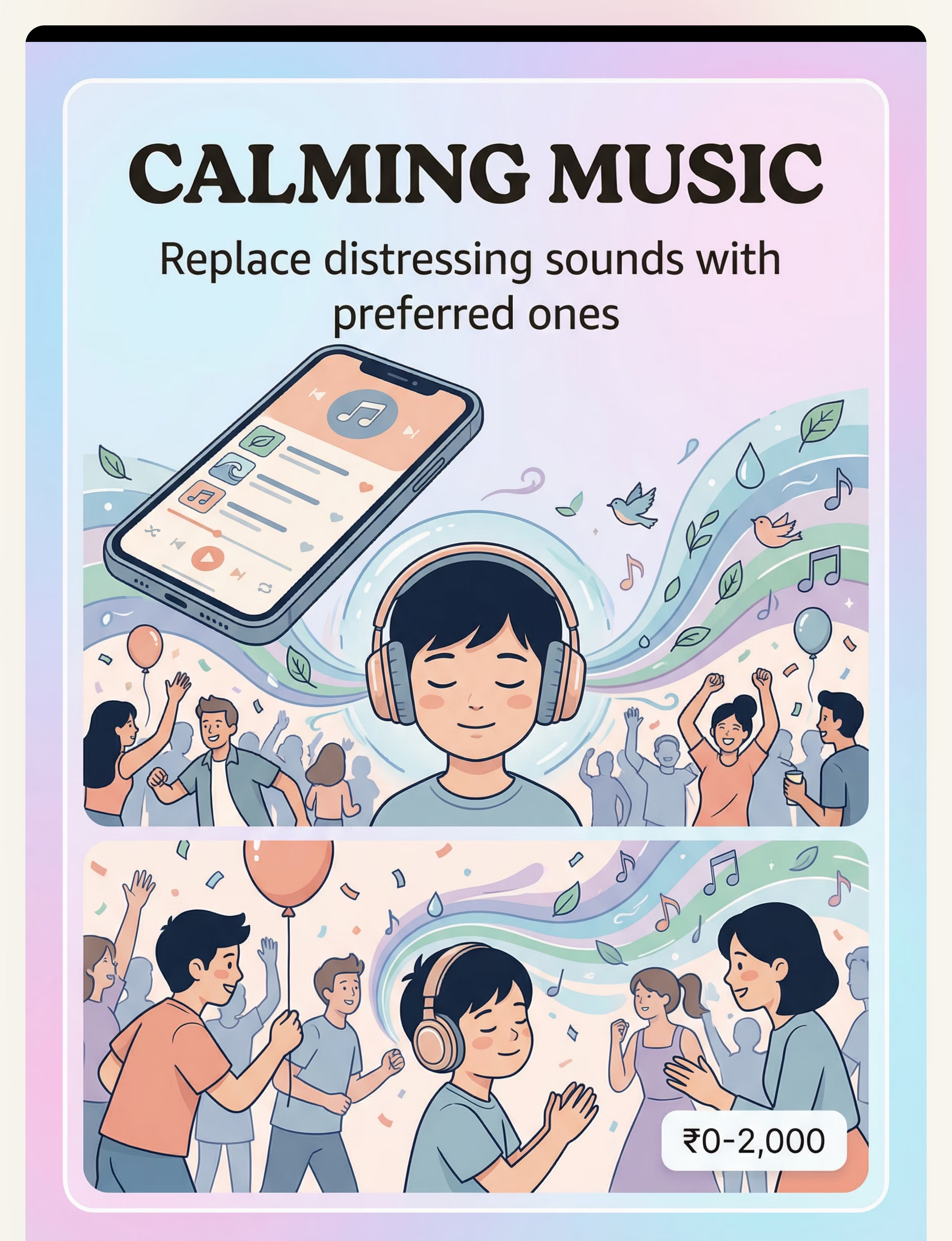
White Noise Machine · Visual Schedules · Calming Music & Soundscapes
White Noise Machine · Visual Schedules · Calming Music & Soundscapes
Category 3
Systemic Support
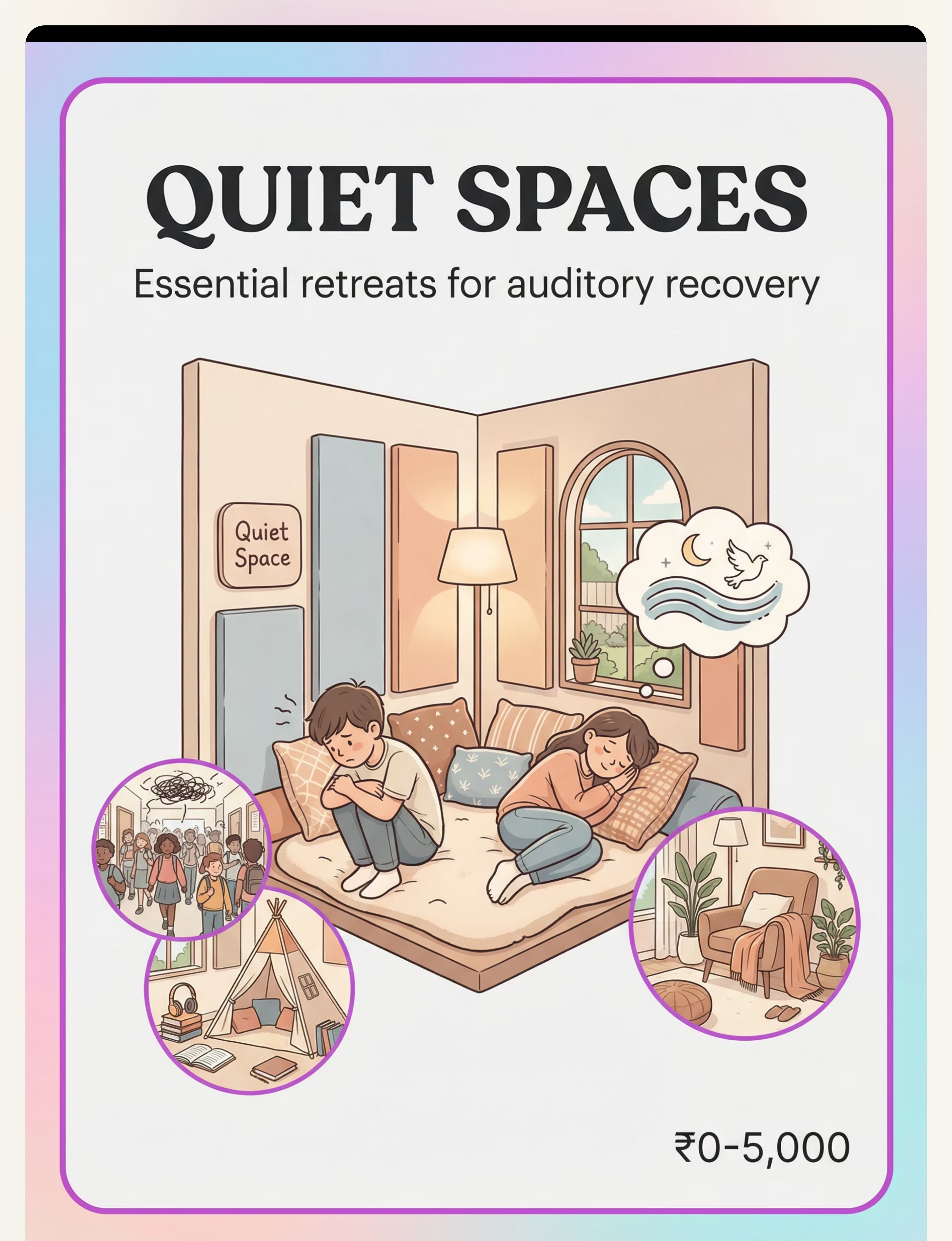
Quiet Spaces · Therapeutic Listening · Nervous System Regulation Tools
Quiet Spaces · Therapeutic Listening · Nervous System Regulation Tools
# | Material | Price (INR) | Priority | |
1 | Noise-Reducing Headphones / Ear Defenders | ₹800–3,000 | ESSENTIAL — Start here | |
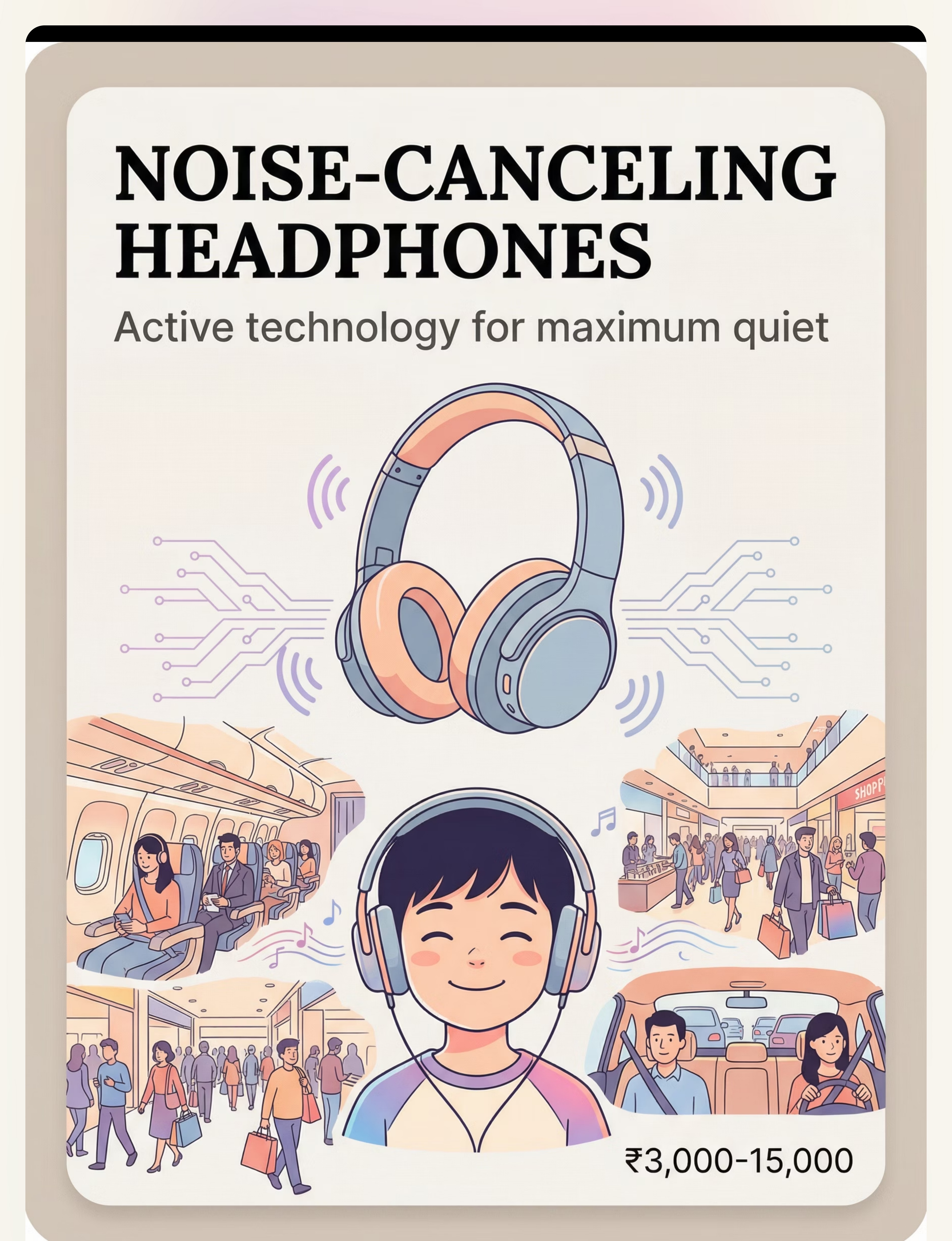
2 | Noise-Canceling Headphones | ₹3,000–15,000 | Maximum protection | |
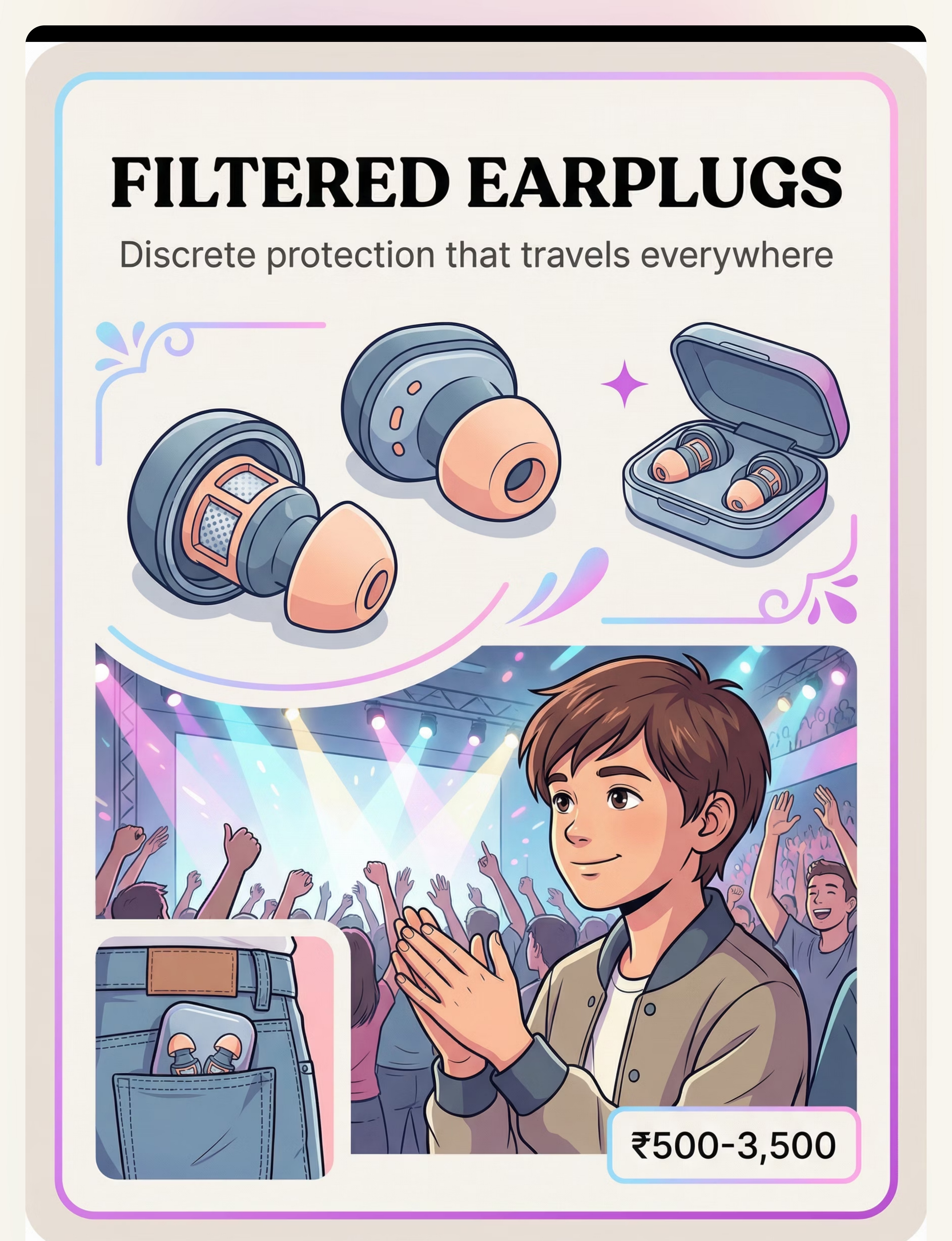
3 | Filtered Earplugs | ₹500–3,500 | Discrete, portable | |
4 | White Noise Machine / Sound Masking | ₹800–4,000 | Home/sleep/study | |
5 | Visual Schedules / Sound Warnings | ₹0–500 (DIY) | Reduces anxiety | |
6 | Calming Music / Preferred Soundscapes | ₹0–2,000 | Substitution strategy | |
7 | Quiet Spaces / Sensory Retreats | ₹0–5,000 | Essential retreat | |
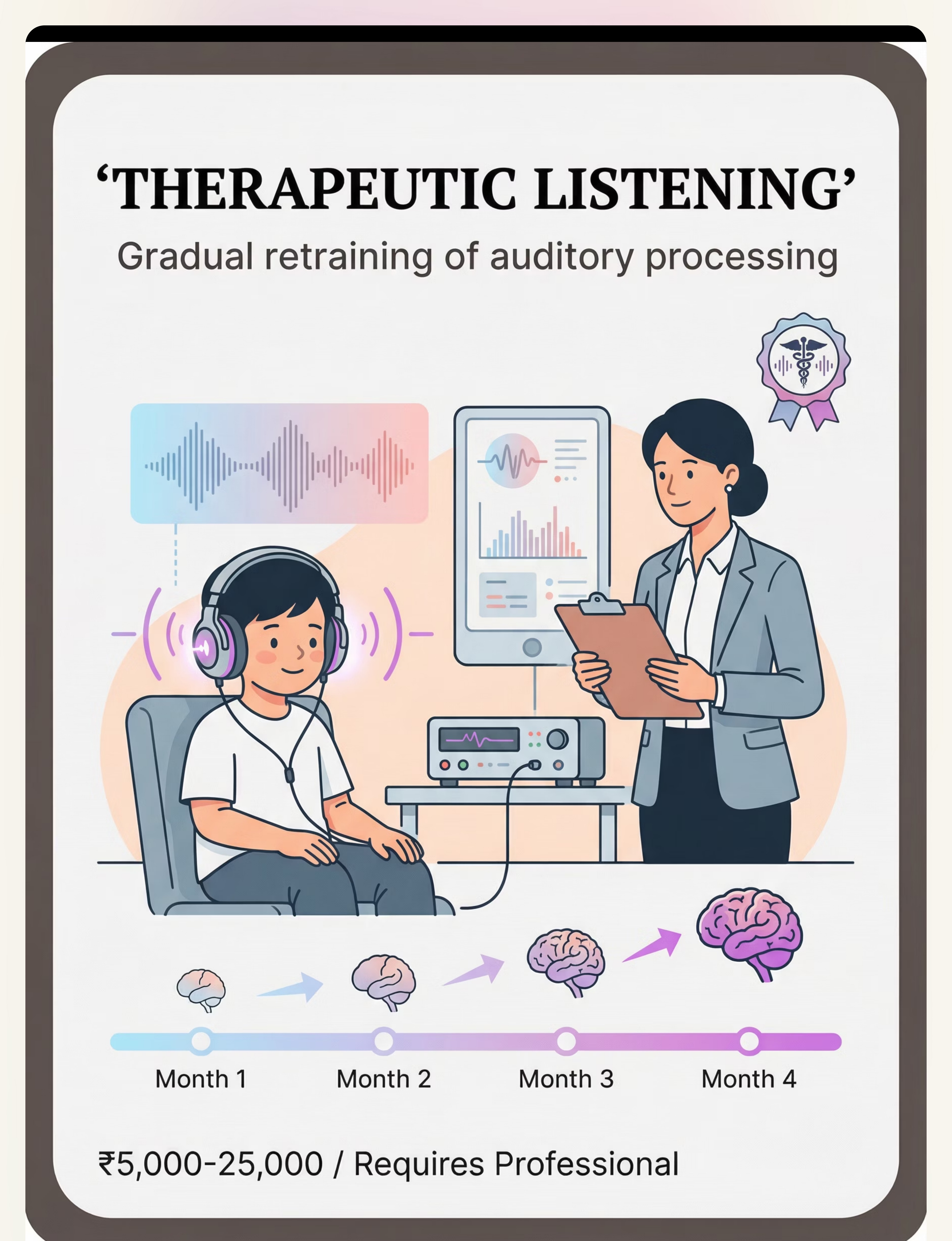
8 | Therapeutic Listening Programs | ₹5,000–25,000 | Requires professional | |
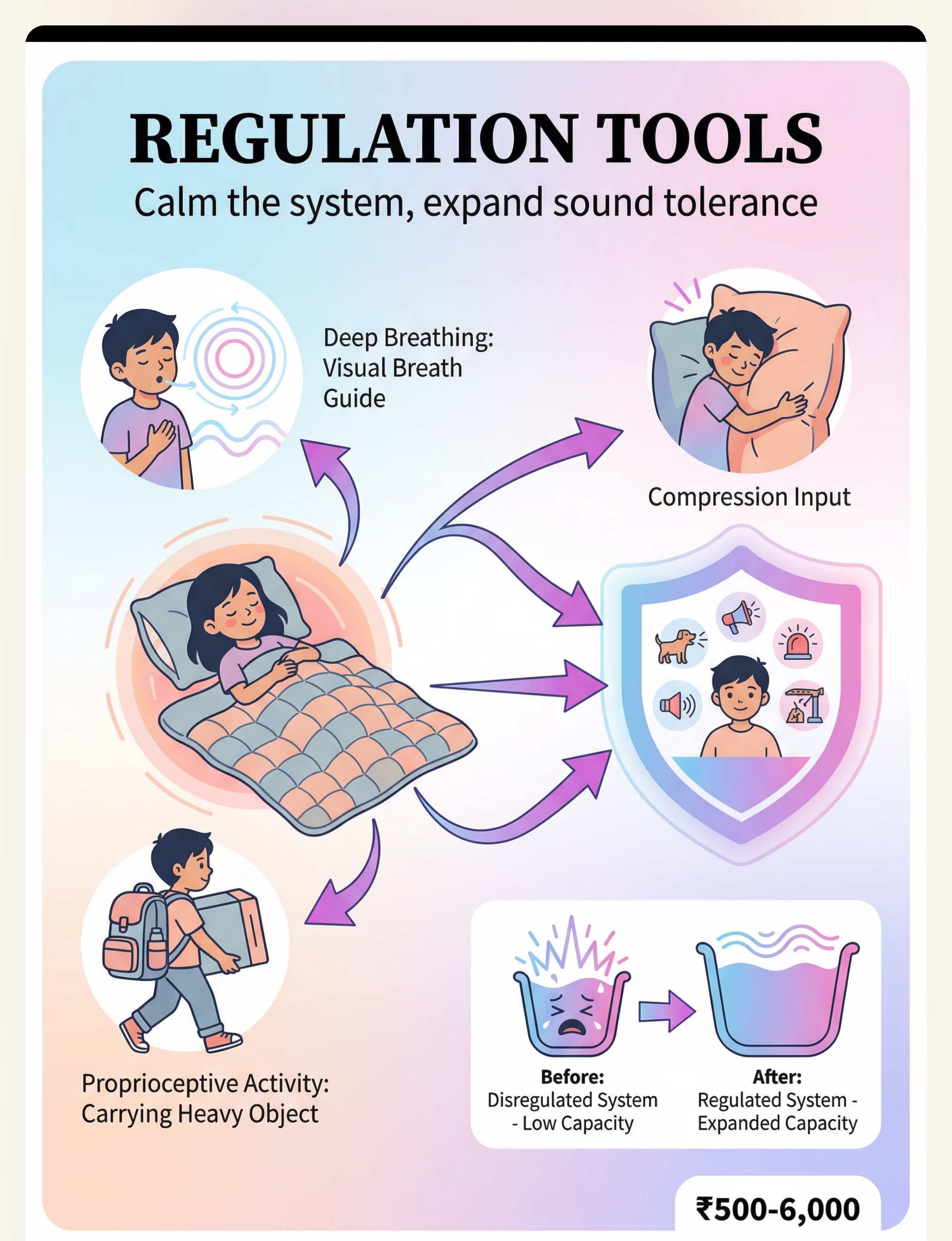
9 | Nervous System Regulation Tools | ₹500–6,000 | Expands tolerance |
"Pinnacle Recommends" Starting Kit: Begin with noise-reducing headphones, verbal warnings before anticipated sounds, and a quiet retreat space. These three alone transform daily functioning. Essential starters: ₹800–3,500.
Every Family Can Start Today — Regardless of Budget
The WHO Nurturing Care Framework (2018) emphasizes context-specific, equity-focused interventions. The CCD Package implemented across 54 low- and middle-income countries demonstrates that household-material-based interventions are effective. Your home has what you need to start.
Buy This
- Noise-reducing headphones (₹800+) — Purpose-built NRR-rated protection
- Noise-canceling headphones (₹3,000+) — Active noise cancellation technology
- Filtered earplugs (₹500+) — Reduce volume while preserving speech clarity
- White noise machine (₹800+) — Consistent, calibrated sound masking
- Therapeutic listening (₹5,000+) — Professionally modulated recordings
Make This (Zero Cost)
- Ear protection: Construction ear muffs, pool noodle over headband for softer pressure
- White noise: Fan running in room, white noise apps on phone, air purifier, running water
- Visual schedules: Hand-drawn picture schedules, verbal warnings, countdown timers on phone
- Calming music: Phone/tablet with music apps, nature sounds apps, child's favorite calming music
- Quiet spaces: Designate a quiet corner, add soft furnishings, tent or blanket fort
- Regulation tools: Tight hugs, heavy blankets, calm-down breathing, consistent routines
⚠️Therapeutic listening is NOT DIY-able. It requires specific modulated recordings and professional guidance.
Reference: PMC9978394 | WHO NCF Handbook (2022)

Protect First. Always.
Before introducing any sound sensitivity materials, review these safety guidelines carefully. Protection should never cause additional distress or create new risks.
🔴 STOP IF
- Child shows signs of ear infection or unrelated ear pain — see physician immediately
- Earplugs or headphones cause pain or pressure discomfort
- Child cannot hear their own name when wearing protection (safety risk)
- Any signs of hearing loss — seek audiological evaluation
- Child becomes MORE distressed when using a specific tool
🟡 CAUTION
- Earplugs for children under 7: choking hazard, fit issues — use over-ear protection instead
- Noise-canceling headphones may create uncomfortable "pressure" sensation — test first
- White noise should be comfortable background, NOT loud — place away from child's head
- Weighted items: use 5–10% body weight guideline only
- Therapeutic listening: ONLY under professional OT guidance
🟢 SAFE TO PROCEED
- Child is fed, rested, and in a reasonably regulated state
- Protection materials fit comfortably
- Child can still hear speech and safety-critical sounds
- Quiet retreat space is accessible
- Caregiver is present and attentive
"Ear defenders are not avoidance — they're accommodation. They allow participation that would otherwise be impossible. Like glasses for vision, they're a tool that helps the child access their environment. Never withhold ear protection as punishment."
Reference: Padmanabha et al., Indian J Pediatr (2019) — DOI: 10.1007/s12098-018-2747-4
Before Sound Protection Begins, the Environment Must Be Right
Home Sound Audit
Kitchen: Identify appliance sounds (blender, mixer, microwave beep, exhaust fan). These are predictable — add them to a visual schedule.
Bathroom: Hand dryer alternatives at home (towels). Toilet flush warning. Exhaust fan sound level check.
Living Areas: TV volume baseline. Doorbells and phone ringtones — can these be softened? Sibling noise patterns.
Bedroom — The Sanctuary: This should be the quietest room. Add soft furnishings (carpet, curtains, pillows) that absorb sound. White noise machine positioned away from head. Ear defenders within arm's reach.
Quiet Space Setup
- Choose a corner or small room with minimal external noise
- Soft lighting (no harsh fluorescents that hum)
- Comfortable seating (beanbag, cushions, soft mat)
- Sound-absorbing materials (thick curtains, carpet, pillows)
- Ear defenders stored here, always accessible
- Calming music device available
- "Quiet Space" sign visible
Rule: This space is NEVER used as punishment. It is ALWAYS accessible. Share this page with your child's teacher and request quiet space access at school, including fire drill accommodation protocols.
Reference: Sensory Integration Theory (Ayres) — Environmental setup is a core principle. | PMC10955541

ACT III: THE EXECUTION
Is Your Child Ready? The Readiness Check
The best session is one that starts right. This 60-second pre-session readiness check ensures your child is in the optimal state for learning and can engage safely with the protocol.
✅ Biological Needs Met
Child has eaten recently and is not hungry. Child is reasonably rested and not overtired. No signs of illness (ear infection, headache, fever).
✅ Emotional Readiness
No recent meltdown or high-distress episode in the last 30 minutes. Child is in a reasonably regulated state and open to interaction.
✅ Environment & Materials
Environment is set up per the sound audit. Protection materials are charged, available, and within reach. Caregiver has 15–20 uninterrupted minutes.
1
All GREEN
GO. Begin with Step 1.
2
1–2 AMBER
MODIFY. Just introduce one protection tool calmly. No formal protocol.
3
Any RED
POSTPONE. Calming activity instead. Try again tomorrow. Postponing is not failure — it's clinical judgment.

Step 1: The Invitation
Duration: 1–2 minutes
"I have something that might help with the sounds. Want to see it?"
Every protocol begins with an invitation, not a command. Show the child the noise-reducing headphones (or chosen material) without placing them on the child's head. Let the child see, touch, and explore at their own pace.
What Acceptance Looks Like
- Reaches for the material
- Makes eye contact and approaches
- Nods or verbally agrees
- Allows you to place the material on or near them
What Resistance Looks Like
- Turns away or pushes material away
- Shows distress or anxiety
- Says "no" or shakes head
If Resistance:"That's okay. It will be here when you're ready." Place the material within view but don't push. Try again in a few hours or the next day. Pair the material with a preferred activity.
Reference: ABA Pairing Procedures + OT "Just-Right Challenge" principle

Step 2: The Engagement
Duration: 2–3 minutes
The child is now engaged. It's time to deepen the interaction and build the association between the protection tool and comfort.
Model First
Wear the headphones yourself. Smile. Show it's comfortable. Say: "These help make sounds softer. Let me show you..."
Gentle Placement
If child is willing, place headphones gently on child's head. Adjust fit carefully. Ask: "How does that feel? Is it comfortable?"
Demonstrate the Effect
Turn on a mildly challenging sound (soft music from a speaker) and show how the headphones reduce it. Narrate: "See? The headphones make the music quieter."
Read the Response
Engagement: Child keeps headphones on, looks interested → Continue. Tolerance: Neutral/uncertain → Keep duration short. Avoidance: Child removes headphones → End here gently.
Reinforcement Cue:"You're doing great trying something new!"

Step 3: The Therapeutic Action
Duration: 5–15 minutes
Now use the protection in a real sound situation. Choose a mildly challenging sound environment the child currently avoids. Start with the least challenging, not the most.
Level 1: Home — Controlled
Turn on blender in kitchen while child wears headphones in the next room
Level 2: Home — Closer
Turn on blender while child is in the kitchen with headphones on
Level 3: Community — Brief
Quick grocery store trip with headphones (5 minutes only)
Level 4: Community — Extended
Full shopping trip with headphones and visual schedule
Level 5: Social
Attend part of a party or gathering with headphones and a quiet-space exit plan
Parent Script:"You're wearing your headphones. The sounds are softer now. You're safe. I'm right here."
Duration Guidance: Start with 5 minutes in a challenging environment. Increase by 2–3 minutes per session only if your child tolerates the current duration well. If the child shows escalating distress despite protection, retreat to a quiet space immediately — this level was too much today.
Step 4: Repeat & Vary
Duration: Across Multiple Sessions
3 good experiences are worth more than 10 forced ones.
Repetition Protocol
- Repeat the same level of exposure 3–5 times before moving to the next level
- Same time of day when possible (reduces variables)
- Same protection tool initially (build association: headphones = safety)
- Same preparation routine (visual schedule → choose protection → warning → exposure)
Variation Options (After 2 Weeks)
- Try different protection tools for the same environment
- Vary the duration slightly (5 min → 7 min → 10 min)
- Vary the sound source (blender → vacuum → TV volume)
- Introduce the "choice" protocol: let child choose between two protection options
Satiation Indicators (child has had enough): Increased fidgeting with the protection device, asking to leave or remove headphones, declining engagement, body tension or facial signs of fatigue. When you see satiation: Stop. Celebrate what was achieved. "You did amazing. We'll try again tomorrow."

Step 5: Reinforce & Celebrate
Duration: 30–60 seconds post-exposure
Celebrate the attempt, not just the success. Deliver reinforcement within 3 seconds of exposure completion. Be specific — not just "good job" but exactly what the child did.
"You wore your headphones and stayed at the store! That was brave. I'm so proud of you."
"You stayed at the birthday party for 20 minutes! That's amazing!"
"You told me when it was getting too loud instead of melting down. That's so grown-up."
Verbal Praise
Immediate, specific, enthusiastic
Physical Comfort
Hug, high-five (if child initiates)
Preferred Activity
5 minutes of favorite game/video
Visual Tracking
Token or sticker for chart
Critical Principle: A child who wears headphones to a birthday party for 5 minutes before needing to leave has not failed. They participated for 5 minutes more than they could have without the headphones. The attempt IS the success.

Step 6: The Cool-Down
Duration: 3–5 minutes
No session ends abruptly. The cool-down is a critical transition that protects the gains your child just made and teaches their nervous system that challenging sound environments have a safe ending.
1
Signal the Transition
"We're going to finish up now. Let's go to our quiet spot."
2
Move to Quiet Space
Go to the designated retreat you set up in the environment preparation step.
3
Remove Protection Gradually
Don't rush headphones off. Ask the child if they're ready. Offer calming input — weighted blanket, deep pressure hug, or preferred calm activity.
4
Narrate Recovery
"Your body is calming down. The sounds are soft here. You're safe. When you're ready, we'll move on. No rush."
If the child wants to KEEP wearing headphones and keep participating — that's success, not a problem. Let them continue if possible. The cool-down applies when the exposure was challenging and the child needs recovery time.
Reference: NCAEP Evidence-Based Practices Report (2020) — Visual supports and transition strategies

Capture the Data: Right Now
60 seconds of data now saves hours of guessing later. Record these 3 data points within 60 seconds of session end. Consistent tracking turns observations into patterns and patterns into progress.
1. Duration
How long did the child tolerate the sound environment with protection?
□ <2 min | □ 2–5 min | □ 5–10 min | □ 10–20 min | □ 20+ min
□ <2 min | □ 2–5 min | □ 5–10 min | □ 10–20 min | □ 20+ min
2. Distress Level
Child's peak distress during exposure (1–5 scale):
1 = Calm | 2 = Mild discomfort | 3 = Moderate distress | 4 = Needed to leave | 5 = Meltdown
1 = Calm | 2 = Mild discomfort | 3 = Moderate distress | 4 = Needed to leave | 5 = Meltdown
3. Protection Used
Which material(s) were used?
□ Ear defenders | □ Noise-canceling | □ Earplugs | □ White noise | □ Music | □ Other
□ Ear defenders | □ Noise-canceling | □ Earplugs | □ White noise | □ Music | □ Other
Optional Quick Notes: Sound trigger, environment, what helped, what didn't. Track with GPT-OS® for longitudinal analysis and personalized recommendations.
Reference: ABA Data Collection Standards — Cooper, Heron & Heward (Applied Behavior Analysis)

What If It Didn't Go as Planned?
Session abandonment is not failure — it's data. Every challenging session teaches you something about your child's specific profile. Here are the most common issues and their evidence-based solutions.
Child Refused Headphones
Why: They may feel uncomfortable, look unfamiliar, or the child associates them with forced sound exposure.
Fix: Leave headphones in child's play area. Model wearing them yourself. Let child play with them. Pair with preferred activity. Try again tomorrow with zero demand.
Fix: Leave headphones in child's play area. Model wearing them yourself. Let child play with them. Pair with preferred activity. Try again tomorrow with zero demand.
Headphones On, Still Melted Down
Why: Sound environment was too challenging, OR the headphones don't reduce sound enough.
Fix: Drop back one exposure level. Try higher-NRR headphones or noise-canceling. Reduce duration. Add white noise as secondary protection.
Fix: Drop back one exposure level. Try higher-NRR headphones or noise-canceling. Reduce duration. Add white noise as secondary protection.
Removed Headphones Mid-Exposure
Why: Discomfort (fit, pressure, heat), OR sound was no longer overwhelming (success!), OR child was overwhelmed by other stimuli.
Fix: Check fit. Ask why (if verbal). If sound was tolerable without — celebrate progress!
Fix: Check fit. Ask why (if verbal). If sound was tolerable without — celebrate progress!
Only Tolerates One Specific Pair
Why: Sensory children often attach to specific items. This is normal and functional.
Fix: Buy a backup pair of the SAME headphones. Gradually introduce similar alternatives over time.
Fix: Buy a backup pair of the SAME headphones. Gradually introduce similar alternatives over time.
"They Need to Learn to Deal With It"
Why: Misunderstanding of auditory over-responsivity as behavioral choice.
Fix: Share this page. Share the neuroscience explanation. Provide clinical documentation. This is a neurological difference, not a preference.
Fix: Share this page. Share the neuroscience explanation. Provide clinical documentation. This is a neurological difference, not a preference.

Adapt & Personalize: No Two Children Are Identical
EASIER
For bad days, early stages, younger children: Maximum protection (noise-canceling headphones). Recorded sounds first at low volume. Familiar environments only. 2–3 minute sessions. Heavy regulation input BEFORE exposure.
STANDARD
For typical sessions: Age-appropriate headphones or earplugs. Graduated real-world exposure per protocol. 5–15 minute sessions. Visual schedule for sound warnings. Cool-down afterward.
HARDER
For breakthrough days, older children: Reduce NRR rating. Extend duration. Introduce new sound environments. Practice self-advocacy: "I need my headphones please." Transition from protection to no protection for tolerable sounds.
Sensory Profile Variations
- Sound + Tactile sensitivity: Headphones touching ears may be an issue. Try over-ear styles with soft padding, or earplugs for children who tolerate in-ear sensation.
- Sound + Visual sensitivity: Quiet space should also be visually calm — dim lighting, minimal visual clutter.
- Sound + Anxiety: Address anticipatory anxiety. Visual schedules are CRITICAL. Consider parallel anxiety management intervention.

ACT IV: THE PROGRESS ARC
Week 1–2: What to Expect
Progress looks like tolerance, not mastery. The first two weeks can feel slow. The nervous system is learning a new association: protection equals safety. Trust the process and continue capturing data.
What You May See
- Child begins to accept the headphones without resistance
- Reduced startle response when wearing protection
- Willingness to enter ONE previously-avoided space (with protection)
- Decreased time to calm after unexpected sound exposure
- Beginning to use the visual schedule to anticipate sounds
What You Will NOT See Yet
- Tolerance of sounds without protection
- Complete elimination of ear-covering behavior
- Ability to attend full events in noisy environments
- Independent use of strategies
Progress Indicator:"If your child tolerates the headphones for 30 seconds longer than last week — that is real, measurable, neurological progress."
15%
Progress Milestone
Foundation building — new neural associations forming

Week 3–4: Consolidation Signs
Neural pathways are forming. This is the phase where consistent effort begins to produce visible change. Look for these consolidation indicators that signal your child's nervous system is adapting.
Emerging Self-Awareness
Child asks for headphones before entering challenging environments — they're recognizing their own needs
Reduced Anticipatory Anxiety
Less anxiety about sounds, not just during sounds — the fear of the fear is decreasing
Extended Tolerance
Can stay in noisy environments 2–3x longer than Week 1 with protection in place
Unprotected Tolerance
May begin to tolerate some previously-triggering sounds without protection (e.g., microwave beep no longer triggers ear covering)
Proactive Coping
Requesting quiet space before meltdown (not after). Pointing to schedule before sound events. Showing reduced distress at specific familiar sounds.
When to Increase: If child consistently tolerates current level for 3+ sessions with distress level ≤2, consider moving to the next exposure level.
40%
Progress Milestone
Consolidation — visible behavioral changes emerging

Week 5–8: Mastery Indicators
The toolkit is working. These are the observable, measurable signs that your child has internalized the strategies and is building genuine auditory resilience.
Independent Access
Child independently accesses protection materials when needed without prompting
Multi-Environment
Can participate in 2+ previously-avoided environments with protection in place
Reduced Meltdowns
Meltdown frequency from sound triggers reduced by >50% from baseline
Strategy Generalization
Uses protection strategies in NEW environments and adapts strategy choice to situation
Self-Advocacy
Can verbalize or communicate sound distress ("It's too loud") instead of melting down
Maintenance Check: Remove the structured protocol for one week. If your child independently continues to use strategies and tolerance is maintained — mastery confirmed.
75%
Progress Milestone
Mastery — self-directed strategy use and generalization

You Did This. Your Child Grew Because of Your Commitment.
Five to eight weeks ago, your child's sound world was a source of constant distress. Birthday parties were impossible. The cafeteria was a war zone. Hand dryers triggered meltdowns. Fire drills were traumatic.
Today, your child has a toolkit. Headphones that turn down the volume. Visual schedules that remove the surprise. A quiet space that provides retreat. A nervous system that's building capacity.
You equipped your child with what the world wouldn't provide.
You learned the neuroscience. You set up the space. You executed the protocol — session after session. You captured the data. You adapted when things didn't work. You celebrated the attempts, not just the successes. From fear to function. That's your family's achievement.
📸Document this milestone. Take a photo of your child in an environment they couldn't access before. This is your evidence of change.
🎉Celebration suggestion: Let the child choose a family activity in a space they can now access with their toolkit — the party they can now attend, the restaurant they can now visit. Let THEM choose.
🎉Celebration suggestion: Let the child choose a family activity in a space they can now access with their toolkit — the party they can now attend, the restaurant they can now visit. Let THEM choose.

Red Flags: When to Pause and Seek Help
Trust your instincts. If something feels wrong, pause and ask. These red flags indicate the need for professional consultation rather than continuing the home protocol independently.
Increasing Sensitivity
Sound sensitivity is INCREASING despite 4+ weeks of consistent protection and accommodation. The nervous system should be stabilizing, not sensitizing.
New Triggers Emerging
Child develops NEW sound triggers that didn't exist before intervention — suggests possible sensitization from inappropriate exposure levels.
Physical Symptoms
Sensitivity accompanied by ear pain, hearing changes, or balance issues — may indicate a medical condition requiring audiological evaluation.
Escalating Anxiety
Anticipatory anxiety about sounds is increasing rather than decreasing. Psychological intervention may be needed alongside sensory strategies.
Complete Avoidance
Total avoidance of ALL sound environments despite maximum protection — may indicate a comorbid condition requiring comprehensive evaluation.
Reference: WHO NCF Progress Report 2018–2023 | Pinnacle clinical escalation protocols
The Progression Pathway: Your Child's Journey Map
Sound sensitivity intervention doesn't exist in isolation. It connects to a broader developmental journey with clear pathways forward based on your child's response and emerging needs.
Your current position is A-031: Sound Sensitivity Materials. Based on your child's progress and profile, your therapist can help you choose the next best step — whether that's a deep dive into ear protection selection, exploring therapeutic listening, or addressing co-occurring sensory differences like movement seeking or visual sensitivity.
Long-term developmental goal: Self-managed sensory regulation → Functional participation in all life environments → Independent self-advocacy.
Related Techniques in the Sensory Processing Domain
Your Sound Sensitivity Toolkit (headphones, visual schedules, quiet space, regulation tools) overlaps with materials needed for related sensory interventions. You already own materials for these techniques.

A-025: Light Touch Sensitivity
Difficulty: Intro
Uses: Weighted blanket, quiet space you already have
Uses: Weighted blanket, quiet space you already have

A-032: Movement Seeking
Difficulty: Core
Uses: Regulation tools from your existing toolkit
Uses: Regulation tools from your existing toolkit

A-033: Crashing & Bumping
Difficulty: Core
Uses: Deep pressure tools and regulation strategies
Uses: Deep pressure tools and regulation strategies

A-034: Difficulty With Transitions
Difficulty: Core
Uses: Visual schedules you've already created
Uses: Visual schedules you've already created

A-035: Visual Sensitivity
Difficulty: Intro
Uses: Quiet space, regulation tools
Uses: Quiet space, regulation tools

A-040: Anxiety + Sensory Processing
Difficulty: Advanced
Uses: All regulation tools from your kit
Uses: All regulation tools from your kit
Your Child's Full Developmental Map
This technique is one piece of a larger plan. The Pinnacle GPT-OS® system organizes child development into 12 interconnected domains. Sound Sensitivity sits in Domain A: Sensory Processing — but improvement here cascades into multiple other domains.
A: Sensory
★ Current focus
B: Motor Skills
Regulation improves motor planning
C: Communication
Sound tolerance enables listening and language
D: Social Skills
Group participation becomes possible
F: Emotional Regulation
Reduced sound-triggered dysregulation
J: Academic Readiness
School acoustic tolerance improves learning
Additional domains impacted: E: Adaptive Behavior · G: Cognitive Skills · H: Play Skills · I: Self-Care · K: Family Functioning · L: Community Participation
Reference: WHO/UNICEF Nurturing Care Framework (2018) — Five components of nurturing care require holistic developmental monitoring.
ACT V: COMMUNITY & ECOSYSTEM
Families Who've Been Here: Before and After
Before:"Birthday parties were impossible. The moment everyone sang Happy Birthday, she'd be under the table with her hands over her ears, crying. We stopped going. We stopped being invited."
After (8 weeks):"With her ear defenders and the warning that singing is coming, she sits at the table with the other kids. She still covers her ears sometimes. But she's THERE. She's participating. That's everything."
— Parent, Pinnacle Blooms Network
After (8 weeks):"With her ear defenders and the warning that singing is coming, she sits at the table with the other kids. She still covers her ears sometimes. But she's THERE. She's participating. That's everything."
— Parent, Pinnacle Blooms Network
Before:"School was a minefield. The cafeteria, assemblies, fire drills, even other kids shouting on the playground. Every afternoon was a meltdown waiting to happen."
After (12 weeks):"His teacher keeps backup headphones in the classroom. He knows to put them on before assembly. He goes to the quiet corner when he needs to. He hasn't been sent home for a meltdown in six weeks."
— Parent, Pinnacle Blooms Network
After (12 weeks):"His teacher keeps backup headphones in the classroom. He knows to put them on before assembly. He goes to the quiet corner when he needs to. He hasn't been sent home for a meltdown in six weeks."
— Parent, Pinnacle Blooms Network
"Sound sensitivity is one of the most impactful sensory challenges because it's invisible and constant. When families have the right tools and understand the neuroscience, the change in daily functioning is often dramatic. Protection is not avoidance — it's access."
— Pinnacle Blooms Therapist
Note: Illustrative cases; outcomes vary by child profile and consistency of implementation.

Connect With Other Parents
Your experience helps others. Their experience helps you. Isolation is the enemy of adherence. Every parent who connects with another parent stays in the program longer and gets better outcomes.
Parent Community — WhatsApp Group
Join families navigating sound sensitivity, tactile challenges, and sensory processing differences. Real-time support from parents who understand.
Online Forum
Share your journey, ask questions, find support at pinnacleblooms.org/community. A safe space for honest conversations.
Local Pinnacle Parent Meetups
Monthly gatherings at your nearest Pinnacle center. Connect with experienced parents in your city who've walked this path.
Peer Mentoring Program
Connect one-on-one with a parent who has navigated sound sensitivity successfully. Learn what worked, what didn't, and how they adapted.
Reference: WHO NCF Community Engagement Principles — "Over 1,000 individuals from 111 countries contributed to the framework."
Your Professional Support Team
Home + Clinic = Maximum Impact. When your child needs more than what home strategies can provide, these specialists bring the expertise to unlock the next level of progress.
Specialist | Seek If... | |
Occupational Therapist | Comprehensive sensory processing evaluation needed; therapeutic listening candidacy assessment; school consultation required | |
Audiologist | Hearing concerns; hyperacusis assessment; central auditory processing evaluation needed | |
Developmental Pediatrician | Comprehensive developmental evaluation; comorbid conditions (autism, ADHD); medication consideration for significant anxiety | |
Psychologist | Significant anxiety or phobia component; trauma history; behavioral patterns requiring psychological intervention |
📞 FREE Helpline
9100 181 181
24/7 · 16+ languages · No cost
24/7 · 16+ languages · No cost
🗺️ 70+ Centers
Find your nearest center at pinnacleblooms.org/centers
📱 Teleconsultation
For families in remote areas or 70+ countries served by Pinnacle
The Research Library: Deeper Reading
For the curious parent, clinician, or program lead who wants to explore the evidence base behind these recommendations. Every strategy on this page is anchored in peer-reviewed research.
Level I — Systematic Reviews & Meta-Analyses
PRISMA Systematic Review (2024): 16 articles from 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria. → PMC11506176
Meta-analysis, World J Clin Cases (2024): 24 studies — sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills. → PMC10955541
Level II — Randomized Controlled Trials
Padmanabha et al., Indian J Pediatr (2019): Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population. → DOI: 10.1007/s12098-018-2747-4
Level III — Framework & Guideline Reviews
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration treatment in ASD. → DOI: 10.3389/fnint.2020.556660
WHO Nurturing Care Framework (2018): Global standard for early childhood development. → nurturing-care.org
WHO/UNICEF CCD Package (2023): Care for Child Development across 54 countries. → PMC9978394
Additional Sources: NCAEP Evidence-Based Practices Report (2020) · SPD Foundation (spdfoundation.net) · AOTA sensory processing guidelines · Porges, S. — Polyvagal Theory · Miller, L.J. — Sensational Kids
How GPT-OS® Uses Your Data
Your consistent data tracking improves recommendations not just for your child, but for every child navigating sound sensitivity worldwide. Here's how the system learns and adapts.
What GPT-OS® Learns From Sound Sensitivity Data
- Which materials work best for which age groups and sensitivity profiles
- Optimal exposure progression timelines by severity level
- Trigger-specific intervention matching (sudden sounds vs. sustained noise vs. high-frequency)
- Predictive indicators: which children will respond to protection alone vs. requiring therapeutic listening
🔒 Anonymized
All personal data is anonymized in aggregate analysis
🔒 Consent-Based
Individual child data never shared without explicit consent
🔒 Protected
Indian IT Act and GDPR-equivalent protections applied
🔒 Parent Control
Full control — request data deletion at any time
Reference: Digital health + ASD systematic reviews (2024) — 21 RCTs, 1,050 participants demonstrate digital intervention efficacy
Watch the Reel: See the Materials in Action
Sensory Solutions Series — Episode 31
Auditory Over-Responsivity
In this Reel, a Pinnacle Blooms therapist demonstrates:
Immediate Protection
How noise-reducing headphones immediately change a child's experience, the difference between noise-reducing and noise-canceling headphones, and filtered earplugs in action for older children
Environmental Management
White noise machine setup for sleep and study, visual schedules for sound warnings, and the calm of a well-designed quiet space
Systemic Support
What therapeutic listening looks like in practice, and regulation tools that expand sound tolerance over time
Multi-modal learning: Watching a therapist demonstrate these materials reinforces what you've read through a different learning channel. Both together maximize your ability to execute at home.
Reference: NCAEP (2020) — Video modeling is classified as an evidence-based practice. Multi-modal learning improves parent skill acquisition.
Share This With Your Family
If only one parent knows this — it's limited. If everyone in the child's life knows — it's transformative. Consistency across caregivers multiplies impact.
👴👵 Explain to Grandparents
"Your grandchild's brain processes sounds differently. Loud sounds that you barely notice cause them real pain. This isn't drama. This isn't bad behavior. It's how their nervous system is wired.
Here's how you can help: always have their headphones accessible, warn before loud sounds, provide a quiet retreat space, and never force them to 'just deal with it.' Your understanding makes a massive difference."
👩🏫 Teacher Communication Template
A formatted letter for school explaining your child's sound sensitivity, requested accommodations (quiet space access, ear defender use, fire drill protocols, seating placement), and Pinnacle clinical contact for consultation.
Key accommodations to request:
- Quiet space access during the school day
- Permission to wear ear defenders in class
- Advance warning before fire drills when possible
- Preferential seating away from noise sources
Reference: PMC9978394 — WHO CCD Package emphasizes multi-caregiver training as critical for intervention generalization.

ACT VI: THE CLOSE
Frequently Asked Questions
Will my child become dependent on headphones?
Protection is not dependency — it's accommodation. Many children naturally expand their tolerance over time. Some will always benefit from protection in certain environments, just as some people always need glasses. The goal is functional participation, not elimination of sensitivity.
Should I force my child into loud environments to "toughen them up"?
No. Forced exposure without protection can cause sensitization, trauma, anxiety, and loss of trust. Protect first. Gradual, supported, child-paced exposure with protection is the evidence-based approach. Never force; always invite.
Can sound sensitivity improve with age?
Some children show improvement as their nervous system matures. Others maintain sensitivity but become expert self-managers. Consistent accommodation and intervention optimize outcomes regardless of natural trajectory.
My child is sensitive to sounds BUT also makes a lot of noise. Is this contradictory?
Not at all. Self-generated sounds are predictable and controllable — the child's own humming or noise-making may actually be a coping strategy to mask unpredictable environmental sounds. This is "auditory self-regulation" and is common.
How do I handle fire drills at school?
Work with the school to provide advance warning, allow ear defenders during drills, assign a known staff member to the child during emergencies, and practice fire drill responses in a calm setting. These can be written into IEP/504 plans.
Is this the same as misophonia?
Not exactly. Auditory over-responsivity is about sound volume/intensity — sounds are too LOUD. Misophonia is about specific trigger sounds provoking strong emotional reactions regardless of volume. Some children have both. A professional can differentiate.
Are noise-canceling headphones safe for hearing?
Yes, when used appropriately. Ensure the child isn't also playing music at high volume through the headphones. The noise-canceling technology itself does not produce harmful sound levels. Follow manufacturer age recommendations.
At what age should I seek a formal evaluation?
If sound sensitivity significantly impacts daily functioning — avoidance of essential environments, frequent meltdowns from sounds, social isolation — at any age, seek evaluation. Earlier intervention allows earlier accommodation and better outcomes.

Your Next Step: Start Now
You've read the science. You've seen the evidence. You understand the neuroscience. You have the toolkit. Now act.
🟣 Start This Technique Today
Launch GPT-OS® guided session for Sound Sensitivity Materials — personalized to your child's age, sensitivity profile, and available materials
🔵 Book a Consultation
Connect with a Pinnacle OT specializing in auditory processing — in-center or teleconsultation available
📞 9100 181 181 (FREE)
📞 9100 181 181 (FREE)
⚪ Explore Next Technique
A-032: 9 Materials That Help With Movement Seeking — or browse the full Sensory Processing domain
Validated by the Pinnacle Blooms Consortium
Discipline Icons:🧠 OT · 🗣️ SLP · 📊 BCBA · 🎓 SpEd · 👩⚕️ NeuroDev · 🔬 CRO
Preview of 9 materials that help with sound sensitivity Therapy Material
Below is a visual preview of 9 materials that help with sound sensitivity therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Network® — India's Largest Autism Therapy Chain
Built by Mothers. Engineered as a System. Powered by GPT-OS®.
Built by Mothers. Engineered as a System. Powered by GPT-OS®.
"Every child with sound sensitivity deserves a world they can participate in. Every family deserves the tools and knowledge to make that possible. This page is one of 70,000+ evidence-based technique pages in the Pinnacle GPT-OS® library — the largest structured pediatric intervention knowledge base on Earth."
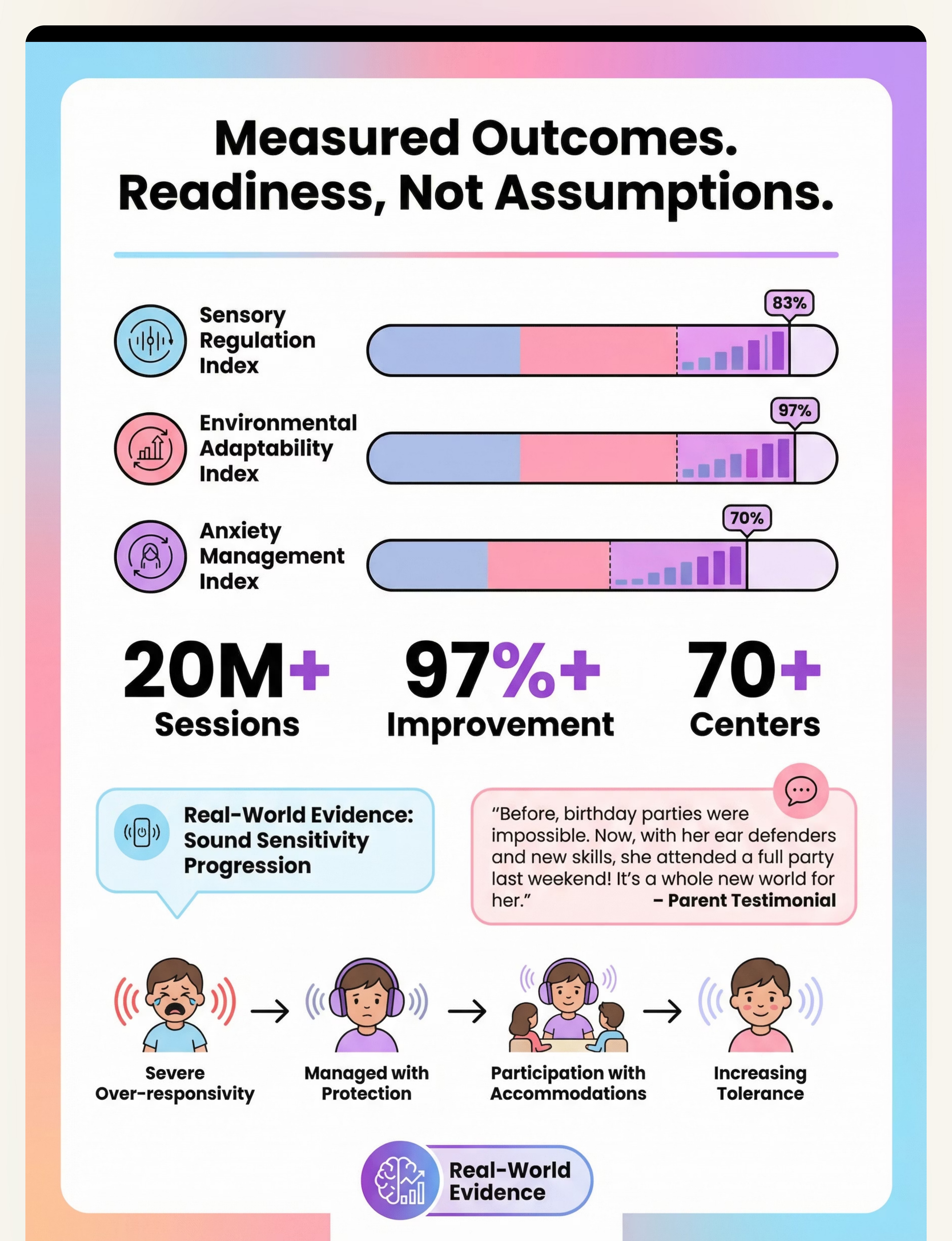
20M+
Therapy Sessions
Exclusive 1:1 sessions delivered
97%+
Improvement
Measured improvement rate
70+
Centers
Across India and growing
70+
Countries
Families served worldwide
Statutory Identifiers: CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed audiologist, occupational therapist, or healthcare provider. Persistent sound sensitivity may require comprehensive auditory processing evaluation. Therapeutic listening programs require professional supervision. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Sensory processing timelines vary significantly between children.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Global IP protection across 160+ countries. GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, and FusionModule™ are proprietary trademarks.