"They Start Upright. Then, Slowly, They Melt."
It's homework time. You've set up the desk, put out the pencils. Your child sits down, back straight. Thirty seconds later, their chin is resting on the table. Three minutes in, they're half off the chair, one arm draped like a flag with no wind. You say "sit up." They try — hold it for two seconds — and collapse again.
9 Materials That Help With Sitting Upright — When they slump, lean, and can't hold themselves up.
Pinnacle Blooms Network®
OT-POST-SIT · Episode F-579
Postural Control Series

You Are Among Millions of Families Navigating This Exact Challenge
Postural control deficit — the clinical name for what you see — is among the most prevalent yet least-discussed challenges in pediatric development. When a child cannot sit upright, it isn't laziness, defiance, or inattention. It is a neuromotor reality: their trunk muscles, vestibular system, and proprioceptive feedback loops are working at a disadvantage.
1 in 6
Children Affected
Experience motor coordination difficulties affecting sitting posture and daily function
40–80%
ASD / Hypotonia / DCD
Display significant postural control deficits impacting school participation
3×
More Energy Used
Energy expenditure for a child with low postural tone to maintain seated position vs. a typically developing peer
In India alone, an estimated 8–12 million children between ages 3–12 experience clinically significant postural control difficulties. In your child's classroom, they are almost certainly not alone.
Research: PMC11506176 · PMC10955541 · DOI: 10.12998/wjcc.v12.i7.1260 · AOTA Postural Control Position Paper

This Is Not Laziness. This Is Neuroscience.
The Postural Control System
Vestibular System (inner ear) — detects head position relative to gravity. Sends continuous signals: "You are tilting. Correct."
Proprioceptive System (muscles + joints) — reports body position: "Core muscles, activate now."
Cerebellum — integrates both signals and coordinates automatic micro-corrections every 50–200 milliseconds.
Core Muscle Network — abdominals, back extensors, hip flexors, paraspinals — must sustain low-level tonic contraction all day.
What This Means for Your Child
"Imagine sitting on a boat that rocks slightly, all day. By lunchtime, your back would ache and your attention would collapse. That is what your child experiences on a stable chair — because to their nervous system, the chair is unstable. They are not choosing to slouch. They are exhausted."
In children with hypotonia, weak core, or sensory processing differences, one or more of these links is underperforming. The vestibular signal may be weak. The proprioceptive feedback delayed. The muscles undertoned. This is a wiring difference, not a behavior choice.
The good news: neural pathways can be trained. Core muscles can be strengthened. Sensory systems can be calibrated. And in the meantime — the right materials make sitting possible while that development happens.

Your Child Is Here. Here Is Where We're Heading.
According to the WHO Care for Child Development Package (2023), independent seated posture with appropriate endurance is a foundational prerequisite for school readiness. Children who enter formal schooling without adequate postural control spend cognitive resources on staying upright instead of learning.
Birth – 6 Months
Head control develops
12 Months
Sits briefly, then independently
18 Months – 3 Years
Floor play, sustained sitting
⚠ 5–7 Years
Challenge Zone — postural demands peak at school entry
12 Years
Full desk-work endurance expected
Common Co-occurring Challenges: Hypotonia · Developmental Coordination Disorder (DCD) · Autism Spectrum Disorder · Sensory Processing Disorder · Down Syndrome · ADHD · Fine motor delays. With the right supports and a consistent strengthening program, children routinely progress from unable to hold position to independent age-appropriate seated endurance within 8–24 weeks.
Research: WHO CCD Package (2023) · PMC9978394 · UNICEF MICS indicators

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level II–III
Systematic Reviews + RCTs + Clinical Consensus
🔬 Systematic Review 2024
PRISMA review of 16 studies (2013–2023) confirms sensory integration and postural support interventions meet criteria for evidence-based practice in children with ASD and motor challenges.
PMC11506176
📊 Meta-Analysis 2024
Across 24 studies, sensory integration therapy effectively promoted motor skills, adaptive behavior, and participation in pediatric populations.
World J Clin Cases · PMC10955541
🏥 Indian RCT 2019
Home-based sensory and postural interventions demonstrated significant functional outcomes in Indian pediatric populations — validating home execution.
Indian J Pediatr · DOI: 10.1007/s12098-018-2747-4
🌍 WHO/UNICEF Framework
WHO Care for Child Development Package: implemented across 54 LMICs; household-material-based interventions demonstrated efficacy for postural and motor development.
PMC9978394 · WHO NCF 2018
These 9 materials are deployed across Pinnacle Blooms Network's 70+ centers, informing 20M+ exclusive 1:1 therapy sessions. The GPT-OS® Postural Control Readiness Index tracks outcomes with a 97%+ improvement rate across network families.

The Sitting Upright Kit — What This Technique Is
The Postural Support Material Toolkit for Seated Stability is a curated set of 9 evidence-based therapeutic tools that address postural control deficits in children — the inability to maintain an erect, stable seated posture against gravity without external support or compensatory strategies.
Dynamic Engagement
Unstable surfaces automatically activate core muscles throughout every session
Static Positioning
Structural aids create biomechanically correct alignment from hips to head
Sensory Activation
Proprioceptive and vestibular stimulation "wakes up" the postural system
Environmental Optimization
Ergonomic adjustments remove biomechanical barriers to good posture
Occupational Therapy
Ages 3–12
10–30 min sessions
Daily use
Postural Control
Core Stability

This Technique Crosses Therapy Boundaries
The brain doesn't organize by therapy type — and neither does postural control. Every discipline in the care team plays a distinct and essential role in helping a child sit upright.
Occupational Therapist (Primary Lead)
OTs assess muscle tone, sensory processing, seating biomechanics, and core strength. They select appropriate materials, design graded home programs, and monitor Postural Control Readiness Index progression.
Physical Therapist (Co-Lead)
PTs assess gross motor foundations, muscle strength, and movement quality. They design the core strengthening exercise component and work in tandem with OTs on progressive postural challenges.
ABA Therapist / BCBA
Uses behavioral strategies to increase tolerance for postural positions, implement reinforcement schedules for sitting duration goals, and embed postural work within behavioral intervention sessions.
Special Educator
Implements classroom postural supports as accommodations; communicates biomechanical needs to school teachers; ensures the seating environment supports full learning access.
NeuroDev Pediatrician
Evaluates underlying neurological and musculoskeletal contributors; coordinates multidisciplinary approach; guides medical management where indicated.
At Pinnacle Blooms Network, postural intervention is never a solo discipline. Our FusionModule™ coordinates OT, PT, ABA, SpEd, and medical inputs into a single converged therapeutic pathway.
This Isn't a Random Activity. It's a Precision Tool.
Every material in this kit targets a specific layer of the postural control system — from deep core engagement to full academic participation.
When core muscles activate automatically and the vestibular-proprioceptive loop is calibrated, cognitive resources once spent on fighting gravity are freed entirely for learning. Fine motor tasks improve. Mealtime participation improves. Self-regulation improves. Posture is the gateway skill.
Research: PMC10955541 · AOTA Postural Control Position Statement

9 Materials. One Complete Postural Support System.
Each material addresses a specific mechanism. Together, they form a complete toolkit that can be started today — at any budget.
Wobble Cushion
Dynamic Seating — Active sitting engages core muscles. Dynamic inflatable disc creates an unstable surface that continuously activates postural muscles.
₹400–1,200 · 🛒 Find on Amazon.in →
Therapy Ball Chair
Maximum Core Engagement — Ball surface with stabilizing frame; constant balance activates deep core stabilizers.
₹1,500–4,000 · 🛒 Find on Amazon.in →
Foot Rest / Foot Stool
Feet Support the Whole Posture Chain — Elevates feet to create 90° hip/knee/ankle alignment. Removes the #1 barrier to good posture.
₹300–1,500 · 🛒 Find on Amazon.in →
Slant Board
Bring Work Up, Keep Spine Tall — 20–30° angled work surface eliminates forward trunk collapse during reading and writing.
₹500–2,000 · 🛒 Find on Amazon.in →
Compression Vest / Core Garment
Sensory Input Activates Posture — Deep pressure input to trunk proprioceptively "wakes up" postural muscles.
₹800–3,000 · 🛒 Find on Amazon.in →
Resistance Band on Chair Legs
Leg Input Organizes the Whole Body — Elastic band between chair front legs provides proprioceptive foot/leg input that grounds the whole body.
₹100–400 · 🛒 Find on Amazon.in →
Wedge Cushion
Tilts Pelvis for Natural Alignment — Triangular foam wedge on seat; forward pelvic tilt creates automatic spinal stacking.
₹500–1,500 · 🛒 Find on Amazon.in →
Core Strengthening Equipment
Build the Strength Behind Posture — Therapy ball, balance board, scooter board — home program that develops permanent postural foundations.
₹500–3,000 · 🛒 Find on Amazon.in →
Proper Desk & Chair Setup
Furniture That Fits the Body — Age-appropriate, adjustable ergonomic furniture creates the biomechanical conditions for good posture.
₹2,000–15,000 · 🛒 Find on Amazon.in →

Every Family Can Start Today — Regardless of Budget
WHO Equity Principle
"Context-specific, equity-focused interventions." — WHO Nurturing Care Framework (2018). No child should wait for a package to arrive. Every one of these materials has a zero-cost equivalent that works on the same therapeutic principle.
Material | Clinical Option | Home Substitute (₹0) | |
Wobble Cushion | Inflatable disc cushion | Partially deflated bicycle inner tube folded flat under a pillow cover | |
Therapy Ball Chair | Ball + stabilizing frame | Fully inflated round balloon cushion; rolled yoga mat under regular cushion | |
Foot Rest | Adjustable footrest | Sturdy stack of textbooks taped together; wooden step stool | |
Slant Board | Commercial 20–30° board | Large hardcover encyclopedia/binder stood at an angle, rubber band at bottom | |
Compression Vest | Therapeutic compression garment | Snug-fitting lycra undershirt; light cloth bandage layer around torso | |
Resistance Band | Therapy elastic band | Old pantyhose/tights tied between chair legs | |
Wedge Cushion | Firm foam wedge | Folded firm pillow or rolled bath towel under back half of seat | |
Core Equipment | Therapy ball + balance board | Floor exercises: Superman, bird-dog, plank on yoga mat | |
Ergonomic Setup | Adjustable desk + chair | Cushions + book footrest; bring chair to kitchen table |
For compression garments: ensure proper fit — too tight is dangerous. For therapy balls: proper sizing is critical (hips/knees at 90°). When in doubt, a Pinnacle OT assessment will specify exact requirements.

Before You Set Up — Read This Card Completely
🔴 Do Not Proceed Without Professional Guidance
Child has known spinal abnormality, scoliosis, or orthopedic condition. Child uses a prescribed wheelchair or adaptive seating system. Compression garment: do not use with circulatory, cardiac, or severe tactile hypersensitivity without OT clearance. Therapy ball: do not use unsupervised with seizure disorders or significant balance impairment.
🟡 Proceed with Caution
Wobble cushion and therapy ball: supervise first 4–6 sessions. Resistance band: check for wear; ensure secure knot; replace when elasticity reduces. All equipment: never leave child unsupervised on dynamic seating during initial weeks.
🟢 General Session Readiness
Child is fed and rested. No fever, illness, or pain reported. Child is in a regulated state — not post-meltdown. Space is clear of tripping hazards.
STOP IMMEDIATELY if: Child reports pain, pressure, or discomfort · Skin redness under compression garment · Child becomes significantly more distressed than baseline · Equipment shows damage · Child slides off dynamic seating and is at fall risk.
Pinnacle Helpline: 9100 181 181 — FREE · 24×7 · 16 languages

The Right Environment Makes the Technique. Set It Up Once, Use It Every Day.
The 4-Zone Setup
① Chair Setup: Place wobble cushion (or wedge) centered on seat. Tie resistance band between front chair legs at foot-height. Hips at ~90° when seated.
② Desk Setup: Position slant board for reading/writing. Desk height: elbows rest at 90° with shoulders relaxed. Clear work surface.
③ Foot Support: Footrest (or book stack) under the desk — feet rest flat, ankles at 90°.
④ Environment: Bright, non-flickering lighting. Quiet or low background music (no TV). Comfortable temperature. Remove all distractions.
Session Duration Guide
Start with 10–15 minutes at the properly set-up station. Increase by 5 minutes per week as tolerance builds.
Parent position: slightly behind and to the left — present, but not hovering. Your goal is to engage with the task content ("Wow, what are you drawing?"), not to watch the posture. The materials are watching the posture.
Lighting bright, no fluorescent flicker
Sound quiet or low background music
Temperature comfortable — hypotonic children are often cold-sensitive
Remove anything the child will reach for or be distracted by

The Best Session Is One That Starts Right. 60 Seconds Now Saves 30 Minutes Later.
A simple readiness check before every session dramatically increases success rate and protects the child's positive association with the postural station.
Indicator | ✅ GO | ⚠️ MODIFY | ❌ POSTPONE | |
Hunger | Fed within last 90 min | Mild hunger | Not eaten in 3+ hours | |
Sleep | Rested | Slightly tired | Overtired / just woken | |
Regulation | Calm, available | Slightly wound up | Post-meltdown, crying | |
Physical | No pain/illness | Mild cold | Fever, pain, ill | |
Time of Day | Optimal window | Neutral time | End-of-day depletion | |
Environment | Set up, quiet | Minor adjustments needed | Chaotic disruption |
If MODIFY
Seated on floor with back support against wall. Use only compression garment or resistance band. Reduce to 5-minute session.
If POSTPONE
Do 5 minutes of heavy work (pushing, carrying, wall push-ups) as sensory preparation, then reassess.
A cancelled session is not failure — it is data. Note the child's state and time of day. GPT-OS® pattern recognition identifies their optimal window over time.

Step 1 — The Invitation
Session Step 1
30–60 seconds
"Hey [child's name], it's time for your special sitting spot. Come show me how strong you are. Can you find your cushion?"
Body Language Guidance
Crouch to child's eye level — do not stand over them
Warm, calm tone — not urgent or stern
Point to the chair/cushion rather than leading by the hand
Smile — this is their special setup, not a punishment
The 10-Second Win Principle
Always start with a duration the child will definitely succeed at. A 10-second success is more valuable than a 10-minute battle. Add 10 seconds per successful session.
If the child resists: "Okay, let's start with just sitting for 10 seconds — that's it." Use a visual timer. Almost all children can succeed at 10 seconds.
What Acceptance Looks Like: child moves toward the chair, sits on the cushion, touches the resistance band, or shows curiosity about the setup. Even reluctant sitting is acceptable.

Step 2 — The Engagement
Session Step 2
1–3 minutes
How you introduce each material shapes whether the child experiences it as exciting or threatening. Use sensory, playful language — present these as superpower tools.
For Wobble Cushion
"Feel how the cushion moves? Your body is doing the work! Can you feel your tummy getting strong?"
For Resistance Band
"Push your feet against the band — like you're driving a rocket! Feel that?" Demonstrate by gently pressing your own hands against the band.
For Compression Vest
"This is your strong body suit. Let's put it on — squeeze, squeeze." Apply with gentle rhythmic pressure for extra proprioceptive benefit.
For Wedge Cushion
"Sit right at the front of the wedge — feel your bottom and your tummy both wake up?"
Reinforcement Cue: At the first moment the child is sitting upright on the material, say immediately: "I can see how strong and tall you are. Your spine is amazing right now."
Observation: Engagement signal = explores material; Tolerance signal = accepts passively (fine in early weeks); Avoidance signal = pushes away or removes vest — reduce duration and input intensity.

Step 3 — The Therapeutic Action
Session Step 3
5–20 minutes
The child is seated on their postural support material, engaged in a meaningful task at the properly set-up desk. The therapeutic work is happening continuously and automatically — every moment they maintain position against gravity, core muscles are strengthening and postural endurance is building.
Feet flat on footrest
Not dangling
Hips at ~90°
Not slumped back
Knees at ~90°
Stable base of support
Work at elbow height
Not reaching up or hunching down
Head upright
Not propped on hand
Common Execution Errors
❌ Wobble cushion too soft — inflate more firmly ❌ Footrest too high — forces knees above hips ❌ Resistance band too high — reposition lower ❌ Desk too high — shoulders rise, elbows above 90°
Your Role During This Phase
Stay present but don't hover. Do not issue constant "sit up" reminders — the materials are doing that work. Engage with the task content. Watch for fatigue signs (sliding beginning, head drooping) — this marks the productive end of the session.

Step 4 — Repeat & Vary
Session Step 4
3–5 minutes across sessions
The 3 Good Reps Principle:Three sessions where the child maintains position for the full duration are worth more than ten sessions where they fight the setup. Quality of supported sitting > duration of struggling.
Therapeutic Dosage
Daily use during regular activities (meals, homework, desk work) — the primary dosage
Targeted sessions 3–5× per week for specific core strengthening exercises
1–3 meaningful activities per session in supported posture — not time-watching
Variation Schedule
Weeks 1–2
Wobble cushion only
Weeks 3–4
Add resistance band
Weeks 5–6
Add compression vest on challenging days
Weeks 7–8
Full toolkit; begin reducing one support to test independence
Satiation indicators — when to end: child begins sliding despite setup · drops head repeatedly · starts vocalizing distress · compliance drops significantly. End within 2–3 minutes with a cool-down, not abruptly.

Step 5 — Reinforce & Celebrate
Session Step 5
Within 3 seconds of success
The Golden Rule: Immediate. Specific. Enthusiastic. Within 3 seconds. Not: "Good job sitting today" (too vague, too late) Yes: "I saw you sitting tall for that entire story! That was your body getting SO strong right there!"
Sat for 10 seconds
"Ten whole seconds of strong sitting! Your spine is a superhero!"
Completed a full task seated
"You finished your whole drawing sitting tall. That's your core muscles working!"
Self-corrected posture once
"I saw you fix your sitting yourself — that's your body getting smarter every day."
New duration record
"That's the longest you've ever sat upright! Let's remember this moment."
Celebrate the attempt, not just the success. Progress is never linear. Regression days are normal and expected. Your consistent positive response is what builds the child's motivation to try again tomorrow. Reinforcement materials available at reward sticker charts ₹364 →

Step 6 — The Cool-Down
Session Step 6
2–3 minutes
Why this step is non-negotiable: Abrupt endings to structured sessions are the #1 cause of resistance to starting the next session. A predictable cool-down tells the child's nervous system: "This ends safely. It's okay to start again tomorrow."
Warning — 2 minutes before end
"Two more minutes at your strong sitting spot, then we're all done." Show a visual timer counting down 2 minutes.
Final Activity Closure
"One more [drawing/page/puzzle piece], then we put away the cushion." Give a clear task endpoint, not just a time.
Material Put-Away Ritual
"Can you help me take the cushion off the chair? Let's put it in its special spot." Child involvement increases ownership and willingness to use it again.
Transition to Preferred Activity
"Strong sitting is done! Now it's time for [preferred activity]." The cool-down always transitions to something the child wants.
If the child resists ending: Do not extend the session. Acknowledge: "I know you want to keep going — we'll do this again [specific time tomorrow]." A visual schedule showing when the next session is helps enormously.
60 Seconds of Data Now Saves Hours of Guessing Later
Tracking three simple data points after every session reveals patterns invisible to daily observation — and drives GPT-OS® personalized recommendations for your child specifically.
📋 Session Duration
Total minutes of supported sitting. Example: "18 minutes"
⭐ Position Maintenance Rating
1–5 scale (1 = couldn't hold position, 5 = held entire session). Example: "3 — held for half, slid twice"
🛠 Materials Used Today
Checkboxes: ☑ Wobble cushion ☑ Footrest ☐ Compression vest
Optional (if you observed something notable): One sentence — "First time he self-corrected his posture without prompting!" or "Very tired today, only 8 minutes."
Why This Data Matters
Reveals optimal time-of-day window · Identifies best material combinations · Quantifies progress daily observation misses · Feeds GPT-OS® personalized recommendations
📥 Download F-579 Postural Support Weekly Tracker — PDF · pinnacleblooms.org/resources/F579-tracker →

Session Abandonment Is Not Failure. It's Data.
Child refuses to sit on the wobble cushion
Root cause: Tactile or movement sensitivity — the new sensation feels threatening. Solution: Introduce cushion OFF the chair first. Normalize on the floor for 3–5 days, then transfer to chair.
Posture not improving after 2 weeks
Root cause: Materials may be mismatched to the child's underlying cause. Solution: Use the Support Selection Guide (Card 22). If no improvement in 4 weeks, book an OT assessment.
Child removes the compression vest immediately
Root cause: Tactile sensitivity — compression feels aversive to a sensory avoider. Solution: Start with the lightest garment, worn over a soft t-shirt. Begin with 2 minutes. Do not force.
Child slips off wobble cushion — safety issue
Root cause: Inflation too high or chair too big. Solution: Deflate slightly, check chair size. Consider switching to wedge cushion (static) if dynamic seating proves unsafe.
Child does well at home but collapses at school
Root cause: School furniture is adult-sized; no supports available in classroom. Solution: Bring portable supports to school. Request formal accommodation — Card 37 includes a teacher communication template.
Parent is exhausted by constant monitoring
Root cause: Setup is not yet automatic. Once equipment is in place, it does the work. Solution: Re-check setup against Card 12. If child can do a task while parent steps back 1–2 meters, the setup is correct.
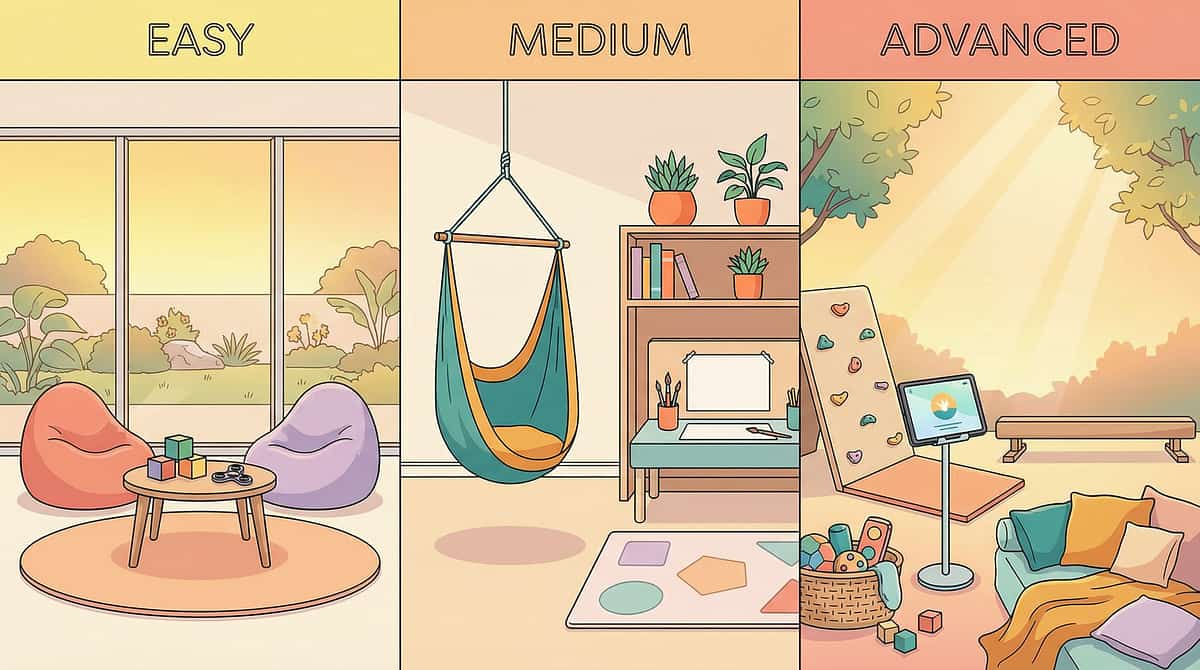
No Two Children Are Identical. Adjust Until It Fits.
Start where the child succeeds. Move right as strength builds.
🔵 Movement Seeker
Craves sensory input, can't sit still. Primary: Wobble cushion + therapy ball chair + resistance band (all three if tolerated). Movement need is met within the seated position.
🟢 Low Tone Child
Floppy, generally hypotonic. Primary: Compression vest + wedge cushion + therapy ball chair + core strengthening program. Proprioceptive input "wakes up" muscles.
🟡 Environmental Mismatch
Good days / bad chairs. Primary: Footrest + proper desk height + wedge cushion. Fix the furniture before adding dynamic elements — often dramatic improvement with ergonomic correction alone.
🔴 Sensory Avoider
Dislikes movement, strong tactile sensitivity. Primary: Wedge cushion (static) + footrest + desk height adjustment. Avoid wobble cushion initially. Prioritize static supports.
Age adjustments: Ages 3–5: Shorter sessions (5–10 min), floor seating may be preferable, playful framing. Ages 6–9: Standard protocol; school integration is key. Ages 10–12: Child-directed support selection; frame as "performance optimization."
Week 1–2: Progress Looks Small. It Is Not Small.
Tolerance Phase
~15% Progress
15%
Tolerance Phase
Week 1–2 progress indicator
What Progress Looks Like in Weeks 1–2
Accepts wobble cushion without removing it for increasing durations
Slightly reduced "sit up" reminders needed per session
Fewer chair exits before session goal duration
More willingness to start the next session
Compression vest tolerance building (if using)
What Is NOT Expected Yet
Independent maintenance without supports
Significant visible change without materials
Reduction in slumping at unsupported times
"If your child tolerates the wobble cushion 3 seconds longer than Day 1, that is a neural pathway forming. That is real progress."
The families who continue through this phase consistently report breakthrough moments in Weeks 4–6. Research confirms: sensory integration and postural intervention outcomes emerge across 8–12 week timelines. — PMC11506176

Week 3–4: Consolidation Signs
Consolidation Phase
~40% Progress
40%
Consolidation Phase
Week 3–4 progress indicator
These are the "neural pathway forming" indicators most parents miss because they're looking for the wrong things:
Anticipation
Child approaches the postural station without prompting — they've associated the setup with a positive experience.
Preference
Child requests the wobble cushion when it's not set up: "Where's my cushion?"
Spontaneous Self-Correction
Once or twice per session, the child corrects their own posture without being told.
Task Performance Improving
Handwriting quality improving because the stable base is freeing up fine motor capacity.
"In Weeks 3–4, you may notice something unexpected: you're more confident. You know how to set up the station. You know how to read the child's readiness. You're no longer guessing. That is a skill you've built."

Week 5–8: Mastery Indicators