
9 Materials That Help With Sitting for Tasks
Evidence-based OT tools — wobble cushions, weighted lap pads, foot fidgets, visual timers and more — that make seated task engagement achievable for children with autism, ADHD, and sensory processing differences.
G-663
Attention & Task Engagement
OT · ABA · SpEd
"Two minutes into homework and your child is already under the table."
It's not defiance. It's not laziness. And it is absolutely not your failure as a parent.
You've watched other children sit cross-legged through circle time, through meals, through entire lessons — and wondered what you're doing wrong. You've tried firmness. You've tried rewards. You've tried removing screens, adding screens, changing the chair, changing the room. Nothing holds. Within sixty seconds of sitting down, the sliding begins. Then the standing. Then the wandering.
"You are not failing. Your child's nervous system is speaking. This page will teach you to listen — and respond."
Here is what the science says: your child's body may be neurologically unable to sustain static sitting without support. This is not a behavior problem. This is a sensory-motor regulation challenge — and there are nine evidence-validated tools that can change everything.
📞 FREE Helpline
National Autism Helpline: 9100 181 181 — 16+ languages, 24×7
🔬 Research-Backed
WHO Nurturing Care Framework (2018): Early parental awareness directly impacts developmental outcomes.

You Are Among Millions of Families Navigating This Exact Challenge
Seated attention difficulties are among the most commonly reported challenges across autism, ADHD, sensory processing disorder, and developmental coordination disorder. Teachers report it. Parents live it. Occupational therapists see it in nearly every child they assess. When your child cannot sit for tasks, they are not the exception — they are part of a very large, very well-researched, very solvable population profile.
1 in 36
ASD Diagnosis Rate
Children diagnosed with ASD in the US (CDC 2023)
80%
Sensory Difficulties
Of children with autism experience sensory processing difficulties affecting seated attention
21M+
Therapy Sessions
Delivered by Pinnacle Blooms Network® measuring this exact challenge
"80% of children diagnosed with autism display sensory processing difficulties — most of which directly impact the ability to maintain seated attention." — PRISMA Systematic Review, 2024 (PMC11506176)
In India, studies report that 3–4% of school-age children demonstrate significant sitting and attention difficulties requiring therapeutic intervention. Across Pinnacle's 70+ centers, seated task engagement is the most frequently addressed goal in occupational therapy. Our CRO team, OTs, BCBAs, and special educators see this profile daily — and these nine materials were designed specifically because the evidence confirms they work.

The 4-System Sitting Circuit
Sitting is not a simple act — it is a neurological coordination task requiring four brain systems to fire simultaneously.
Postural System (Cerebellum)
Continuously fires to keep the body upright
Vestibular System
Processes gravity and movement
Proprioceptive System
Tells the brain where the body is in space
Prefrontal Cortex
Handles attention sustenance and executive function
This Is a Wiring Difference, Not a Behavior Problem
🧠The Postural System must continuously fire to keep the body upright. For children with low muscle tone or poor core stability, this alone consumes most available energy — leaving little for the task at hand.
🌀The Vestibular System processes gravity and movement. When it under-registers, the brain craves movement input to feel "real" — driving the squirming, rocking, and sliding you see.
🖐️The Proprioceptive System tells the brain where the body is in space. Poor proprioception means the child cannot feel where their body is without moving — causing constant position changes.
🎯The Prefrontal Cortex handles attention sustenance. In ADHD and many autistic profiles, executive function challenges mean the attention system itself needs external structure to stay engaged.
When two or more of these systems are dysregulated simultaneously, static sitting becomes physiologically impossible — not behaviorally difficult. Impossible. These nine materials each address one or more of these four systems.
Your Child's Seated Attention — Where It Is, Where It's Going
Understanding where your child sits on the developmental timeline helps set realistic expectations — and identify exactly how much support is needed. These are developmental averages for neurotypical children. Children with sensory processing differences, ADHD, autism, or developmental coordination disorder may follow modified timelines that are entirely valid and entirely supportable with the right tools.
Age | Typical Sitting Tolerance | What This Looks Like | |
2–3 years | 5–10 min (high-interest) | Floor play, brief table activities | |
3–5 years | 15–20 min with breaks | Circle time begins; movement essential | |
5–7 years | 20–30 min with structure | Classroom instruction; formal desk sitting | |
8–12 years | 30–45 min with breaks | Extended instruction; homework demands |
Children with sitting difficulties often also experience: handwriting challenges (dysgraphia / fine motor), attention regulation difficulties (ADHD profile), sensory sensitivity or seeking in other modalities, core muscle weakness (low muscle tone), and anxiety when demands feel uncontrollable. With the right supports, age-appropriate seated attention with self-regulation is an achievable and measurable goal.
Clinically Validated. Home-Applicable. Parent-Proven.
LEVEL I — SYSTEMATIC REVIEW EVIDENCE
Study | Key Finding | Source | |
PRISMA Review 2024 (16 studies) | Sensory integration interventions meet evidence-based practice criteria for ASD | PMC11506176 | |
Meta-analysis 2024 (24 studies) | Dynamic seating + sensory tools promote attention, adaptive behavior, motor skills | PMC10955541 | |
Indian RCT 2019 | Home-based sensory interventions: significant measurable outcomes | DOI:10.1007/s12098-018-2747-4 | |
NCAEP 2020 Report | Visual supports, sensory integration: classified Evidence-Based Practices | NCAEP 2020 | |
WHO NCF 2018 | Early caregiver-delivered intervention directly impacts developmental trajectory | nurturing-care.org |
"Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and gross/fine motor skills across 24 controlled studies." — World Journal of Clinical Cases, 2024 (PMC10955541)
Across 21M+ 1:1 therapy sessions in our 70+ center network, seated task engagement interventions using these nine material categories show improvement in 97%+ of measured cases via our Academic Readiness Index and Attention Readiness Index tracked through GPT-OS®.

The Technique: What It Is
G-663
Multi-Modal Seated Attention Supports (MSAS) Protocol
Technique Identity
Formal Name: Multi-Modal Seated Attention Supports (MSAS) Protocol
Parent-Friendly Name: "The 9 Materials That Make Sitting Possible"
Reel ID: G-663 | Series: Attention & Task Engagement | Episode 663
Age Range: 3–12 years
Settings: Home + School + Clinic
Duration: Ongoing daily use
Definition
This technique introduces nine evidence-validated material categories — from dynamic seating cushions to oral motor tools — that address the neurological, sensory, postural, and cognitive barriers to sustained seated attention.
Rather than demanding that children "just sit still," MSAS Protocol provides their body and brain with the precise input they need to achieve and maintain seated engagement independently. Each material targets a specific underlying factor. Together, they form a comprehensive environmental support system deployable in any home, school, or therapy setting.
📞 Not sure which materials suit your child? Call 9100 181 181 — FREE assessment guidance
Dynamic Seating
Proprioceptive Tools
Visual Timers
Weighted Items
Fidget Tools
Ergonomic Positioning
Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type. Five disciplines each contribute a unique clinical lens to the same seated attention goal.
Occupational Therapist
Assesses sensory processing, postural control, and motor foundations of sitting. Prescribes and calibrates physical tools — wobble cushions, weighted items, slant boards. Designs the sensory diet that makes sustained sitting neurologically achievable.
ABA Therapist / BCBA
Structures reinforcement schedules around seated engagement. Designs movement break systems, task completion protocols, and token economies. Data-tracks sitting duration as a measurable behavior target.
Special Educator
Implements task strips, visual checklists, and visual timers within learning sessions. Designs the academic environment to support seated attention. Advocates for classroom accommodations.
Speech-Language Pathologist
Addresses seated attention during communication activities. Uses the same tools to support sustained engagement during speech therapy tasks and classroom language activities.
Neurodevelopmental Pediatrician
Rules out medical contributors — vision problems, sleep disorders, nutritional deficiencies. Coordinates diagnosis across ADHD, ASD, DCD, and SPD. Guides pharmacological decisions if indicated.
"In Pinnacle's FusionModule™, all five disciplines contribute their layer to the same seated attention goal — simultaneously. One plan, five clinical lenses, one child."

Precision Tools for Specific Targets
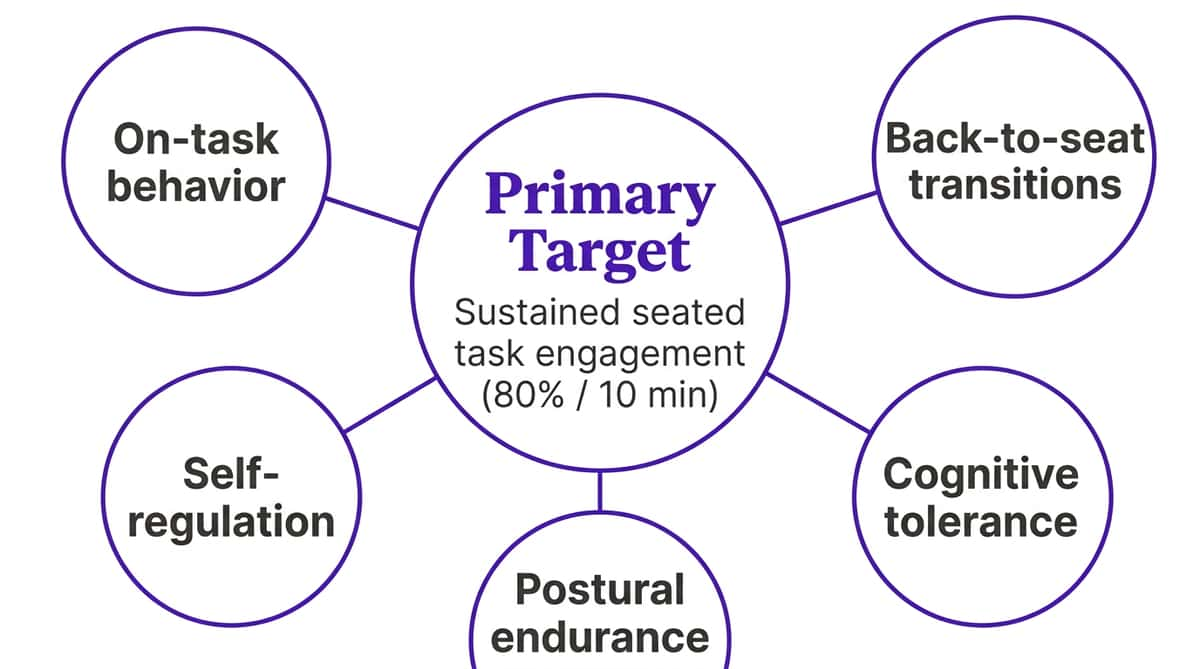
Primary Target
Sustained seated task engagement — the ability to remain in a seated position and maintain active attention on an age-appropriate task for the expected duration.
Observable indicator: Child remains in seat for ≥ 80% of a 10-minute structured task without adult redirection.
GPT-OS® Readiness Indexes
Academic Readiness Index
Self-Regulation Readiness Index
Attention Readiness Index
Classroom Readiness Index

9 Materials. 9 Neurological Solutions.
Each material below addresses a specific reason why sitting is hard. Match your child's profile to the relevant tools. You do not need all nine — start with two or three that fit your child's primary pattern.
⭐Starter Kit — If you're beginning today: Wobble Cushion + Visual Timer + Foot Support + Movement Break Cards. Estimated cost: ₹1,200–3,500 | Available on Amazon.in

1 — Wobble Cushion
Canon Category: Dynamic Seating
Provides vestibular + proprioceptive micro-movement while keeping the child in their seat. ₹800–2,000 | Search on Amazon.in
DIY: Partially inflated beach ball or folded textured mat

2 — Foot Fidget / Under-Desk Resistance Band
Canon Category: Proprioceptive Tools
Channels lower-body energy productively; provides proprioceptive input through feet and legs. ₹400–1,500 | Search on Amazon.in
DIY: Stretch band tied between front chair legs
3 — Visual Timer
Canon Category: Visual Timers
Makes time visible and finite — transforms "endless" demand into an achievable goal. ₹500–1,800 | Search on Amazon.in
DIY: Sand timer (₹150–300) or phone countdown app

4 — Weighted Lap Pad
Canon Category: Weighted Items
Deep pressure proprioceptive input calms the nervous system. Use 5–10% of body weight. ₹1,000–2,500 | Search on Amazon.in
DIY: Fabric pouch filled with rice/dry beans (~1–1.5 kg)

5 — Hand Fidget
Canon Category: Fidget Tools
Tactile input for one hand maintains alertness while the other hand works on the task. ₹200–800 | Search on Amazon.in
DIY: Stress ball from balloon filled with flour; velcro strip under desk

6 — Slant Board
Canon Category: Ergonomic Positioning
Raises work to eye level, reduces neck strain, frees cognitive resources for the task. ₹600–1,500 | Search on Amazon.in
DIY: Large ring binder standing on its spine (20–30° angle)
7 — Movement Break Cards
Canon Category: Movement Supports
Builds planned regulation breaks into the seated routine. Short movement resets the nervous system. ₹150–500 | Search on Amazon.in
DIY: Hand-drawn card set with 8 activity pictures (jumping jacks, wall push, etc.)
8 — Task Breakdown Strip / Visual Checklist
Canon Category: Task Organisation Materials
Makes work visible, finite, and sequential — eliminates overwhelm-driven escape. ₹100–400 | Search on Amazon.in
DIY: Sticky notes dividing work into chunks; paper strip with checkboxes

9 — Chewable Fidget
Canon Category: Oral Motor Tools
Oral proprioceptive input organizes the nervous system — essential for oral sensory seekers. Food-grade silicone only. ₹300–900 | Search on Amazon.in
DIY alternative: Crunchy snack during work time

Every Family Can Execute This Technique Today — Regardless of Budget
Context-specific, equity-focused intervention is a core WHO Nurturing Care Framework principle. These DIY alternatives deliver the same sensory-motor principle as commercial items — access should never be a barrier.
Material | Commercial | DIY / Zero-Cost Version | Why It Works | |
Wobble Cushion | ₹800–2,000 | Partially inflated beach ball; folded non-slip mat | Same vestibular + proprioceptive micro-movement | |
Foot Fidget | ₹400–1,500 | Old bicycle tube tied between chair legs | Same lower-body proprioceptive resistance | |
Visual Timer | ₹500–1,800 | Sand timer (₹150) or phone countdown app | Same time-visibility function | |
Weighted Lap Pad | ₹1,000–2,500 | Rice/bean fabric pouch (~1.5 kg) | Same deep pressure input | |
Hand Fidget | ₹200–800 | Balloon filled with flour; velcro under desk | Same tactile + proprioceptive stimulation | |
Slant Board | ₹600–1,500 | Ring binder on its spine | Same ergonomic positioning angle | |
Movement Break Cards | ₹150–500 | Hand-drawn picture cards (8 activities) | Same planned movement regulation | |
Task Strip | ₹100–400 | Sticky notes + pencil checkboxes | Same task visibility + completion reinforcement | |
Chewable | ₹300–900 | Carrot sticks; crunchy snacks; gum (age 5+) | Same oral proprioceptive input |
⚠️Non-negotiable: Chewable fidgets must be food-grade silicone purpose-made items. Do not substitute with non-food materials for oral use under any circumstances.

Read This Before Every Session. Non-Negotiable.
Safety is the foundation of every effective session. Review this traffic-light system before beginning — every time.
🟢 GREEN LIGHT — Proceed when:
- Child is fed, rested, and in a generally regulated state
- No fever, illness, or signs of physical discomfort
- Environment is prepared (Card 12 setup complete)
- No major meltdown or distress in the past 30 minutes
- Materials have been checked for wear and damage
🟡 AMBER LIGHT — Modify when:
- Child is mildly dysregulated (proceed with shorter session, fewer demands)
- Child is tired but not exhausted (reduce duration by 50%)
- New material being introduced (lower complexity, increase choice)
- Post-school fatigue present (allow 30-minute decompression first)
🔴 RED LIGHT — Do Not Proceed when:
- Child is in active meltdown or severe distress
- Child is ill, feverish, or in physical pain
- Child is highly hungry or sleep-deprived
- Weighted items show signs of damage or filling leakage
- Chewable shows bite-through damage
Material | Key Safety Requirement | |
Wobble Cushion | Stable, non-wheeled chair only; supervision until proficient | |
Weighted Lap Pad | Maximum 10% of child's body weight; never on chest/head/neck | |
Chewable | Food-grade silicone only; check daily for damage; replace immediately if bite-through | |
Resistance Band | Securely attached; no snap-back risk; not a trip hazard | |
Foot Fidget | Check height — feet must sit comfortably, not strain |
📞 Safety concern? Call 9100 181 181 immediately for guidance from a Pinnacle clinical team member.

The Environment Is Half the Intervention
Before any session begins, your space should be set up intentionally. Every element of the environment either supports or disrupts your child's nervous system. Here is the complete setup guide.
10-Point Setup Positions
Correctly-sized chair
Feet flat on floor or on a foot rest
Desk at elbow height
Arms at ~90° when writing
Wobble cushion on seat
Correctly inflated — test firmness
Foot fidget at chair legs
Securely attached
Slant board on desk
20–30° angle
Visual timer in sightline
No neck craning required
Task strip — left side of desk
Vertical placement
Hand fidget — right side or lap
Within easy reach
Weighted lap pad on thighs
When child is seated
Movement break cards visible
Accessible stack nearby
Environmental Factors
Lighting: Natural or warm overhead light. Avoid bright glare directly on work surface. No flickering fluorescent if sensory sensitivity is present.
Sound: Quiet or white noise background. Remove loud TVs and background conversations. Some children focus better with low instrumental music.
Remove From the Space:
- Toys not related to the task
- Distracting objects in the child's visual field
- Other family member activities visible in sightline
- Phone notifications within earshot
✅ Ergonomics checklist: Feet flat · Thighs parallel to floor · Elbows at ~90° when writing · Back supported · Work surface at elbow height · Timer in natural sightline

The 60-Second Pre-Session Check
The best session is one that starts right. Run through this readiness check before every session — it takes less than one minute and dramatically improves session outcomes.
Fed?
Child has eaten within the last 1–2 hours. Hunger destroys seated regulation.
Rested?
No signs of acute sleep deprivation or exhaustion.
Regulated?
Calm or mildly alert — not in active distress or extreme excitement.
Healthy?
No fever, physical pain, or signs of illness.
Willing?
Shows some openness to the activity. Does not need to be enthusiastic.
Environment Ready?
Card 12 setup complete.
Materials Ready?
All needed tools assembled before the session begins.
🟢 GO
6–7 items checked → proceed with full session
🟡 MODIFY
4–5 items checked → proceed with simplified, shorter session (5 min max, single material)
🔴 POSTPONE
3 or fewer checked → do a calming activity instead; try again in 30–60 min. Postponement based on readiness is clinical precision.

STEP 1 of 6
Begin With Invitation, Not Command
The Exact Script
"Hey [child's name], I made a special spot for you. Want to come see what we're doing today?"
Body Language Guidance
- Get to child's eye level before speaking
- Warm, neutral tone — no urgency, no tension
- Point toward the prepared space invitingly
- Have one preferred item visible at the setup to create draw
Timing: 30–60 seconds. Do not rush this step.
What Acceptance Looks Like
- Child moves toward the space (even reluctantly)
- Eye contact or orientation toward the setup
- Verbalization of interest, even questioning
- Following without significant resistance
Handling Resistance
- Refusal to approach: "Okay, let's just come look — you don't have to sit yet"
- Ignoring: Bring one preferred material to child first; interest often follows
- Meltdown: Red light — postpone (see Readiness Check card)
"The invitation is the most important step. A child who enters willingly is 4× more likely to sustain the session than one who is directed by command." — Pinnacle ABA clinical protocol

STEP 2 of 6
Introduce the Material Before the Task
The key insight: Do not sit the child down and immediately present the work. Introduce the supportive material first — let the child explore it — and THEN present the task. This sequence matters enormously.
"Look — we've got this special cushion. Try sitting on it. Feel how it moves? And your feet go here. Pretty cool, right?"
Wobble Cushion
Let child bounce/explore for 30 seconds before any task demand
Foot Fidget
Demonstrate the push-pull motion; invite child to try
Timer
"When the red disappears, you get a [reward/break]. Want to race the timer?"
Hand Fidget
Offer choice of 2–3 options — autonomy increases buy-in
Weighted Lap Pad
Introduce with "this is like a warm hug for your lap"
✅ Engagement
Child actively interacting with the material
⚡ Tolerance
Child allows the material without seeking to remove it
⚠️ Avoidance
Child removes or ignores — try a different material type
Timing: 1–3 minutes. Praise engagement: "Great job trying the cushion! I love how you're sitting on it." — PMC11506176: Structured material introduction is a core component of evidence-based sensory integration practice.
STEP 3 of 6
The Active Ingredient — Supported Seated Engagement
With the child seated on the wobble cushion, foot fidget active, weighted lap pad in place, and hand fidget available — present the task. Set the visual timer for a duration the child can currently achieve. Start at 50% of their typical breaking point — if they usually last 5 minutes, start the timer at 3. The task begins. Observe without redirecting for the first 30 seconds.
Sessions 1–3
3–8 minutes seated. Establish familiarity with materials.
Sessions 4–10
Gradually increase by 1–2 minutes per session.
Sessions 11–20
Target 50% of age-appropriate duration with supports.
Session 20+
Build toward full age-appropriate duration with self-selected supports.
Common Error | Why It Happens | Correction | |
Setting timer too long initially | Wanting fast progress | Start at 50% of child's current tolerance — succeed first | |
Interrupting during seated time | Anxiety about correctness | Observe silently; let the materials do their work | |
Removing all supports once child sits | Thinking supports are temporary | Maintain supports consistently — fade deliberately over weeks | |
Using the same fidget every session | Not matching current need | Rotate 2–3 options; arousal needs vary by day |

STEP 4 of 6
3 Quality Minutes Beat 10 Forced Minutes Every Time
For G-663, "repetition" means each session is a rep. Aim for 5–7 sessions per week minimum — daily practice is the dosage that drives neural adaptation. Within a single session, if the timer reaches zero successfully: deliver reward immediately, optionally reset for a second round. Maximum 2–3 rounds per session; quality over duration.
Variation A — Change the task
Same wobble cushion + timer setup, but alternate: drawing → puzzles → reading → writing. Different cognitive demands, same physical support system.
Variation B — Change the material
Same homework task, but try: switch from wobble cushion to standing desk for one session; or remove the weighted pad and observe the difference.
Variation C — Change the timer
Progress the timer by 1–2 minutes once the child succeeds 3 consecutive sessions at current duration.
Variation D — Change the location
Same material setup but at a different table (kitchen → bedroom → library). Generalization across settings is a key goal.
Satiation indicators — stop the round when: Child's engagement quality drops significantly · Multiple requests to end session · Quality of task output deteriorates sharply · Body language signals overwhelming fatigue
Research dosage note: 2–3 formal therapy sessions per week is the standard protocol across 8–12 weeks. Home-based daily practice supplements this — the daily "small dose" is what produces between-session consolidation.

STEP 5 of 6
Timing Matters More Than Magnitude — Reinforce Within 3 Seconds
The rule: When the timer reaches zero and the child is still seated → deliver the reward IMMEDIATELY. Not after praise. Not after reviewing the work. IMMEDIATELY.
"YES! You did it! Timer's done — and you stayed! You get [reward]!"
"That's amazing sitting! The whole timer! Here's your [sticker/token/break]!"
"Look at you — you sat the whole time! That's [child's name] using the wobble cushion like a CHAMP!"
Tier 1 — Social
High-energy praise + physical celebration (high five, hug, fist bump). Always include.
Tier 2 — Token Economy
Sticker on chart → when X stickers earned → preferred activity/item. Reward Sticker Book (₹364) + Rosette Reward Jar (₹589).
Tier 3 — Natural
"Timer's done = movement break!" The break itself is the reward.
Tier 4 — Tangible
Small preferred item (puzzle piece, LEGO piece, token toward preferred activity).
Celebrate the attempt, not just the success. Even if the child only sat for 60 of the 180 seconds: "You tried! You used the cushion! That counts — here's your sticker for trying."

STEP 6 of 6
No Session Ends Abruptly. The Cool-Down Protects the Next Session.
If a session ends abruptly without transition, the child's nervous system associates the session with an aversive stop — reducing willingness in subsequent sessions. A structured cool-down communicates "this always ends nicely" and preserves motivation.
T-minus 2 min
"Two more, then all done. You're almost there."
T-minus 1 min
"One more. Then we put the cushion away together and you get your [break/reward]."
At Completion
"All done! Fantastic work! Let's put everything away." — Involve child in putting away materials.
Transition Cue
Use the child's visual schedule: "Next is [snack/play/TV] — let's go."
If the Child Resists Ending
"I know you want to keep going — that means you liked it! We can do it again tomorrow. Timer says all done for now."
Do not extend the session significantly in response to resistance — this teaches that resistance = more time, which eventually becomes avoidance resistance.
Cool-Down Activity Options
- Quiet heavy work (carry books to shelf)
- Deep pressure input (joint compressions if OT-guided)
- Preferred quiet activity (5 min free choice)
- Sensory calming item (comfort object, soft toy)

60 Seconds of Data Now Saves Hours of Guessing Later
Record exactly three numbers within 60 seconds of session end. These three data points, tracked consistently, become the most powerful evidence of your child's progress — and the most useful input for personalizing the intervention.
📊 Data Point 1: Duration Seated
How long did the child remain in their seat from timer start to first leaving? (in minutes)
🔄 Data Point 2: Redirection Count
How many times did you need to redirect the child back to their seat or task?
⭐ Data Point 3: Session Rating
Overall session quality: 1 = very hard, 5 = great session
Date | Duration (min) | Redirections | Rating (1–5) | Notes | |
Your session data flows into GPT-OS® where it is compared to your child's personal baseline, analyzed against 20M+ sessions with similar profiles, used to refine personalized material recommendations, and aggregated (anonymized) to improve population-level intervention intelligence.
Track sessions at: pinnacleblooms.org/gpt-os/tracker/G-663 — Takes 45 seconds. Your data is anonymized and helps improve recommendations for all families.

Most Sessions Don't Go Perfectly. That Is Normal Data.
"Session abandonment is not failure. It's information. The technique needed adjustment, not you."
Problem 1: Child refused to sit down at all
Why: Motivation for task was too low, or setting event (hunger/fatigue) undetected. Fix: Start with preferred activity on the cushion first. Let child "earn" access to the setup. Review readiness check.
Problem 2: Wobble cushion increased movement instead of reducing it
Why: Normal adjustment period (1–2 weeks) — child is exploring the new input. Fix: Continue daily exposure. Reduce inflation (firmer = less wobble). Typically resolves within 10 sessions.
Problem 3: Child kept removing the weighted lap pad
Why: May indicate sensory defensiveness to deep pressure, or weight is too heavy. Fix: Reduce weight by 50%. Introduce on legs over clothing first. Offer choice. Never force.
Problem 4: Timer increased anxiety instead of reducing it
Why: Child may be anxious about "running out of time." Fix: Switch to sand timer (less precise, less anxiety-inducing). Or remove timer entirely and use a task strip instead.
Problem 5: Child used fidget as a toy and stopped working
Why: Fidget type doesn't match the child's regulation needs, or is too novel/stimulating. Fix: Use a quieter, less visually engaging fidget. Or introduce it 10 minutes before session so novelty wears off.
Problem 6: Child completed task strip too fast and became disruptive
Why: Task difficulty too low — not cognitively engaging enough. Fix: Excellent problem — increase task challenge. Add more steps to the strip. Progress to harder material.
Problem 7: Improvements at home but not at school
Why: Generalization requires consistent application across environments. Fix: Share the teacher communication template (Card 37). Provide a second material set for school. Request OT classroom consultation.
📞 If the child became severely distressed during any session: Stop. Remove demands. Provide calming input. Do NOT attempt the same session within 24 hours. Call 9100 181 181 — free guidance from a Pinnacle therapist.
No Two Children Are Identical. This Technique Meets Your Child Exactly Where They Are.
⬅ EASIER
Single material only (wobble cushion without any other tools) · 2-minute timer maximum · Highly preferred task (child's choice) · Parent sitting alongside throughout · Break every 2 minutes without needing to earn it
CURRENT (Baseline)
Full 9-material setup · 5–10 minute session · Structured task · Timer · Reinforcement on completion
HARDER ➡
Fade wobble cushion · Child self-selects timer duration · Child sets up materials independently · Extended duration (15–20 minutes) · New/challenging tasks · Two sessions per day
Profile | Primary Tools | Modification Note | |
Sensory Seeker | Wobble cushion + foot fidget + hand fidget + movement breaks | Prioritise movement; use all dynamic tools simultaneously | |
Sensory Avoider | Slant board + weighted pad + quiet fidget | Remove wobble cushion; focus on calming/organizing input | |
Low Muscle Tone | Foot rest + back support + slant board + weighted pad | Focus on postural support; seating ergonomics most critical | |
Attention (ADHD) | Visual timer + task strip + movement breaks + hand fidget | Time-visibility + task-visibility most critical tools | |
Oral Seeker | Chewable + all others as needed | Chewable is non-negotiable; must be introduced first |
Age-based modifications: 3–5 years: 3–5 min sessions, floor sitting acceptable, highly preferred tasks only. 6–8 years: 8–15 min sessions, desk sitting established, academic tasks introduced. 9–12 years: 15–25 min sessions, child increasingly self-manages tool use, school generalization prioritized.

Week 1–2: Early Days — You're Laying Neural Groundwork
Not seeing finished results yet is normal and expected. The nervous system needs time to adjust before it can consolidate. Here is exactly what to look for — and what to ignore.
80
70
60
85
30
✅ What You WILL Likely See
- Increased tolerance for the materials (wobble cushion stops being rejected)
- Slightly reduced resistance to the sitting setup (it becomes familiar)
- Timer completion on easier sessions (3-minute sessions succeeding)
- Parent becoming more confident with the setup sequence
❌ What You Will NOT See Yet (Normal)
- Full session completion without any redirection
- Generalisation to school or other settings
- Independent session setup by child
- Dramatic attitude change about homework or sitting
Clinical milestone for Week 1–2: "If your child tolerated the wobble cushion for one complete 3-minute timer session without leaving the seat — that is a clinical milestone. Write it down. It counts." — Record your baseline this week: how long does your child currently sit without any supports?

Week 3–4: The Nervous System Is Learning a New Pattern
By weeks 3–4, the adjustment phase ends and consolidation begins. The nervous system is forming new pathways — and the behavioral signs of that neurological shift become visible. This is when parents often feel the first genuine sense of hope.
Child begins anticipating the session setup
May bring the cushion themselves — a sign of ownership and positive association forming.
Timer protest decreases
Timer becomes a neutral or positive cue rather than a source of stress.
Material preferences emerge
Child shows preference for specific fidgets — this preference is clinically useful data.
Sitting duration increases measurably
Compare Week 3–4 data against Week 1 baseline — a clear trend should be emerging.
First school generalisation signs
Teacher may begin reporting improvement — a signal that the neural pathway is beginning to transfer.
When to increase intensity: If child is completing all 3-minute sessions with ≤1 redirection → increase timer by 2 minutes. If completing 5-minute sessions consistently → introduce a second session per day.
"You may notice you're less tense during sessions. That's your nervous system adapting too. Your calm regulation is directly transmitted to your child — and it matters enormously."
Week 5–8: Mastery Is Not Perfect Stillness — It's Functional Sitting for Learning
Minimum mastery threshold: Child sustains seated task engagement for ≥ 50% of age-appropriate duration with ≤ 2 adult redirections and 1–2 supports in place on 3 consecutive sessions.
Age | Mastery Duration Target | Maximum Redirections | |
3–5 years | 10–15 minutes | ≤ 2 | |
6–8 years | 15–20 minutes | ≤ 2 | |
9–12 years | 20–30 minutes | ≤ 1 |
✅ Generalization (Real Mastery Signal)
Skill appearing at school without special setup · Child using strategies in other settings · Child requesting preferred supports independently ("I need my cushion") · Skill maintained during non-preferred tasks
🏆 Mastery Unlocked Criteria
3 consecutive sessions at mastery duration · Generalisation to at least one additional setting · Child demonstrates at least 1 self-initiated regulation behaviour · Data chart shows clear upward trend from Week 1
When to move forward: Mastery achieved → begin G-664 (Attention During Group Instruction) while maintaining G-663 supports. The foundation you've built carries forward to every next technique.

You Did This. Your Child Grew Because of Your Commitment.
When you started this journey, homework was a daily battle. Sitting was a minute-by-minute negotiation. Your child's body was working against them — and you didn't know how to help.
Now you understand the neuroscience. You set up the space. You prepared the materials. You showed up for session after session even when it was hard. You tracked the data on the difficult days when nothing seemed to work.
And your child — your child is sitting. Learning. Engaging. For longer. With less distress.
That is a clinical outcome. And it is yours.
📸 Journal Prompt
"Before G-663: ___________. After G-663: ___________." Write it down. Take a photo. Share with grandparents, the teacher, the family member who doubted it was possible.
#PinnacleProgress
Share your milestone in the Pinnacle parent community. Your story is medicine for another family just starting this journey.
Trust Your Instincts. If Something Feels Wrong, Pause and Ask.
These six red flags are specific warning signs that require escalation beyond home management. Each has a clear, defined action step.
🔴 Red Flag 1: Child becoming more distressed week-over-week
Sessions are getting harder across 4+ weeks. May indicate wrong material type, or an underlying issue not yet addressed. Action: OT assessment to identify sensory profile more precisely. 📞 Call 9100 181 181
🔴 Red Flag 2: Child is in pain during or after sessions
Complaints of headache, neck pain, back pain, or joint discomfort. May indicate postural mismatch or too-heavy weighted items. Action: Stop all materials. Medical review before resuming.
🔴 Red Flag 3: Sleep is worsening significantly since starting
New or worse sleep difficulties emerging since protocol began. Some sensory tools affect arousal regulation differently. Action: Remove alerting tools (wobble cushion). Review session timing — not within 2 hours of bedtime.
🔴 Red Flag 4: Sitting improving but aggression/meltdowns increasing
Forced regulation during sitting is displacing distress into other contexts. Demands may be too high or total sensory load is excessive. Action: Reduce session frequency. Consult ABA team on overall demand load.
🔴 Red Flag 5: No measurable improvement after 12+ consecutive sessions
Data shows flat or declining sitting duration despite consistent implementation. Profile may require professional OT/ABA assessment. Action: Book a Pinnacle AbilityScore® assessment. 📞 9100 181 181
🔴 Red Flag 6: Self-harming or extreme self-injurious behavior during sessions
Head-banging, biting, hitting self during or after sessions. This is a clinical emergency — not a home-management situation. Action: Stop all sessions immediately. Emergency consultation. 📞 9100 181 181

You're Not Done — You're on a Journey With a Clear Forward Path
Your child's response profile determines which branch to follow next. Strong response to sensory tools → G-664 with same material set. Primarily postural challenges → OT Core Strengthening Protocol alongside G-664. Timer/task-strip most effective → G-665 with visual systems focus. Oral motor seeking as primary driver → Oral Motor Regulation deep-dive. Slow progress despite 12+ sessions → AbilityScore® assessment first.
Long-term developmental goal: Independent, self-regulated seated attention across all settings — home, school, and community — without adult-directed setup.

You Already Have Materials For Several of These
Your G-663 setup is the foundation for the entire Attention & Task Engagement domain. Every material purchased for this technique carries forward to the next six techniques.
Technique | Difficulty | Primary Canon Material | You Already Own? | |
G-664: Attention During Group Instruction | ●●○ | Wobble Cushion | ✅ Yes | |
G-665: Task Completion Challenges | ●●○ | Task Strips | ✅ Yes | |
G-670: Focus and Concentration | ●●● | Timer + Fidgets | ✅ Yes | |
G-680: Following Directions | ●○○ | Visual Cards | ✅ Yes | |
G-660: Transition Readiness | ●○○ | Visual Timer | ✅ Yes | |
G-690: Classroom Participation | ●●● | All G-663 tools | ✅ Yes |
Browse the full Attention & Task Engagement domain: techniques.pinnacleblooms.org/attention-task-engagement/
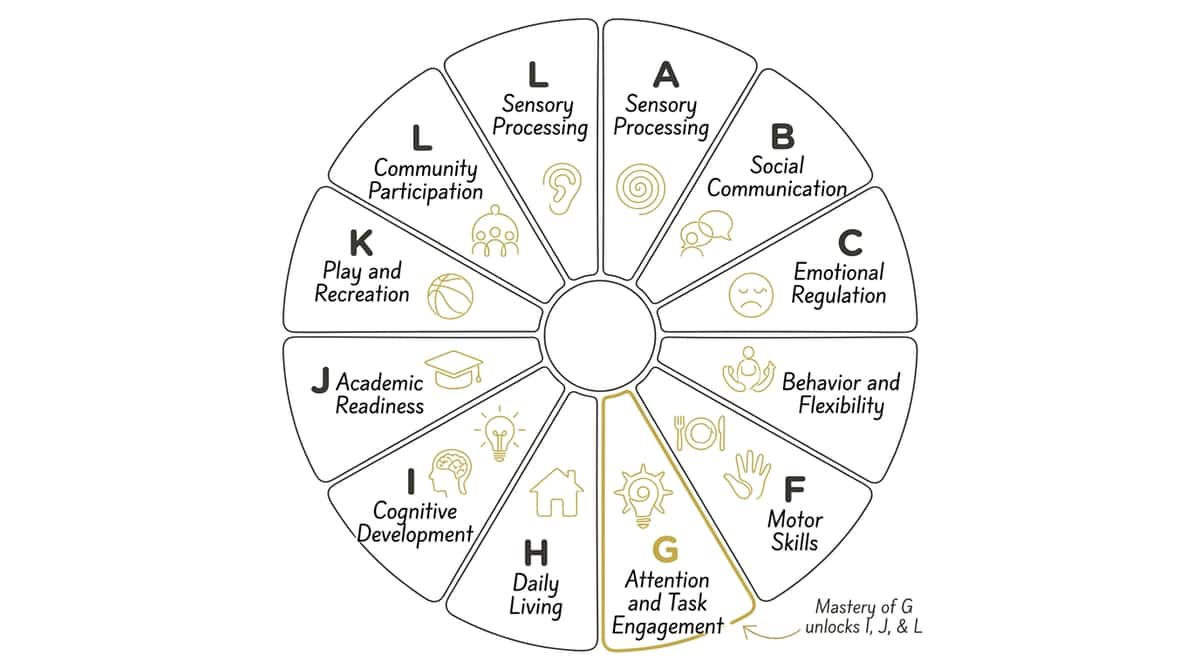
This Technique Is One Piece of a Larger Plan
G-663 addresses Domain G (Attention & Task Engagement) — specifically the seated foundation of all academic and learning participation. Mastery here unlocks access to everything in Domains I, J, and L. Sitting is not a goal in itself — it is the physical prerequisite for every learning goal your child has.
Connect to GPT-OS® to See:
- Your child's current AbilityScore® in Domain G
- Predictive trajectory based on 20M+ similar profiles
- Personalized next-technique recommendations
- Cross-domain impact analysis (how G-663 progress feeds Domain J)
Connect Now
pinnacleblooms.org/gpt-os
Your data helps every child like yours. Population-level intelligence, powered by families like you.

These Are Real Journeys. Your Child's Is Beginning.

Family Story 1 — 7-Year-Old, ASD + Sensory Seeking
Before: "My 7-year-old couldn't sit for more than 2 minutes during homework. We were having meltdowns every evening. His teacher called weekly about out-of-seat behaviour. I felt like I was failing him."
After 8 weeks: "The wobble cushion and the visual timer changed everything. His teacher couldn't believe it. He now completes 15-minute homework sessions without me sitting next to him. He picks up his cushion and sets the timer himself."
Week 1: 2 min → Week 4: 8 min → Week 8: 17 min

Family Story 2 — 5-Year-Old, Low Muscle Tone + Sensory Processing Differences
Before: "My 5-year-old had W-sitting, constant leaning, and would fall off her chair during circle time at preschool. The OT said low tone was the issue — sitting was genuinely exhausting for her body."
After 10 weeks: "The slant board and foot rest fixed her posture immediately. The weighted lap pad kept her settled during group time. She's now participating in full circle time at preschool. Her teacher uses the tools in the classroom."
From no circle time participation to full 20-minute group engagement.
"We see this transformation weekly across our 70+ centers. When we stop fighting the body and start supporting it, the child's capacity for seated learning emerges naturally. The nine materials in G-663 address the actual physiology. The results follow." — Senior OT, Pinnacle Blooms Network®
Disclaimer: Outcomes vary based on child profile, underlying factors, and implementation consistency. These are illustrative cases. Individual results may differ.
Isolation Is the Enemy of Adherence. You Don't Have to Do This Alone.
Pinnacle Parent Community — Seated Attention Group
WhatsApp group: Parents navigating G-663 and attention challenges together. Request Invite → pinnacleblooms.org/community/seated-attention
Online Forum — Attention & Task Engagement
Share session data, troubleshoot together, celebrate milestones. Join the Forum → pinnacleblooms.org/forum/attention-engagement
Local Parent Meetups
In-person peer groups at Pinnacle centers for families with similar profiles. Find Meetups Near You → pinnacleblooms.org/centers
Peer Mentoring Program
Connect with a Pinnacle parent who has completed G-663 with their child. Ask real questions, get real answers. Request a Mentor → pinnacleblooms.org/peer-mentors
"Talking to another parent who'd been through this saved my sanity. I stopped feeling alone and started feeling capable." — Pinnacle parent community member
Your experience, once you complete G-663, is medicine for another parent just starting. Consider sharing your journey. → pinnacleblooms.org/share-your-story
📞9100 181 181 — The helpline connects you to a community, not just advice.
Home + Clinic = Maximum Impact
Where this page gives you the nine tools — a professional assessment tells you exactly which two or three your child needs most, why they're not working if they're not, and what the next level of support looks like.
Therapist Matching for G-663
🟦 Occupational Therapist
Sensory processing evaluation, material calibration, postural assessment
🟩 ABA Therapist / BCBA
Reinforcement design, sitting duration data analysis, school generalisation plan
🟧 Special Educator
Academic task modification, classroom accommodation advocacy
Get Started Today
Match Me to an OT → pinnacleblooms.org/book/ot
Book a BCBA Session → pinnacleblooms.org/book/aba
Teleconsultation (Remote) → pinnacleblooms.org/teleconsult
Insurance note: Occupational therapy for sitting and sensory difficulties is covered under many Indian health insurance plans. Ask your insurer about "paediatric occupational therapy" claims.
📞 FREE National Autism Helpline: 9100 181 181 — 16+ languages, 24×7. No appointment needed.

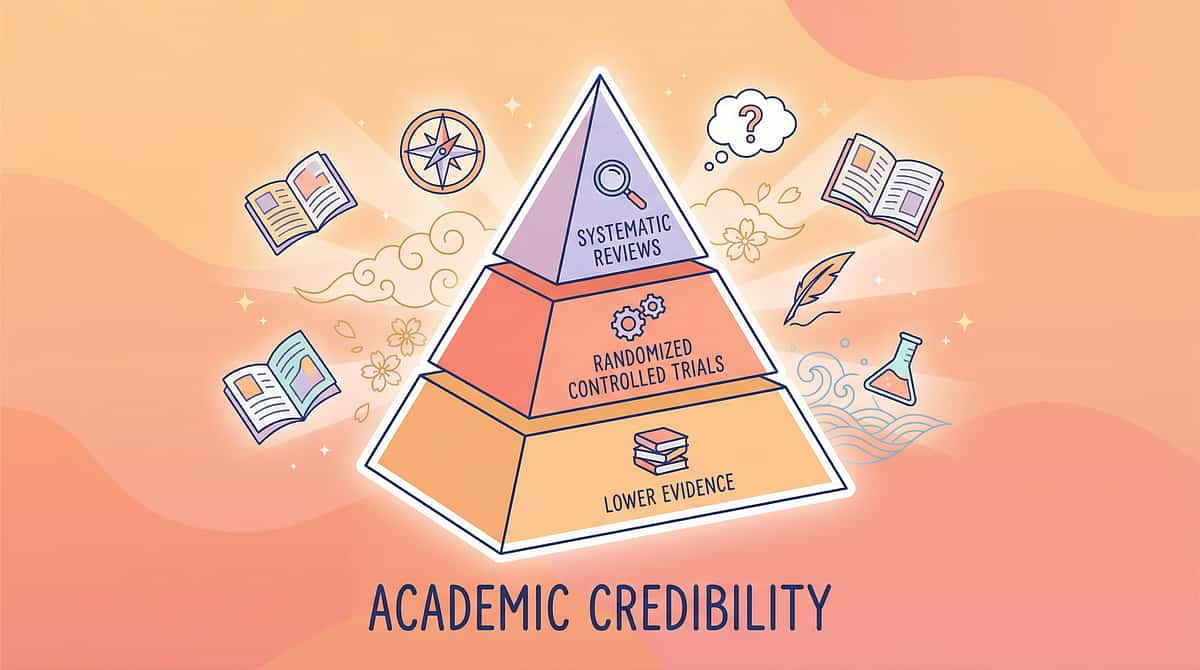
For the Parent Who Wants to Go Deeper: The Full Evidence Base
Study 1 — Systematic Review (2024) | PMC11506176
16 articles (2013–2023) confirm sensory integration meets EBP criteria for ASD. Population: Children 3–12 with ASD. Effect: Large across attention, motor, adaptive behaviour.
Study 2 — Meta-analysis (2024) | PMC10955541
24 studies confirm sensory tools effectively promote social skills, adaptive behaviour, motor skills. Population: School-age children with ASD. Effect: Moderate-large across all outcome domains.
Study 3 — WHO/UNICEF (2023) | PMC9978394
Home-based caregiver-delivered interventions effective across 54 low-and-middle-income countries. Population: Children 0–8 years. Effect: Significant across developmental domains.
Study 4 — Indian RCT (2019) | DOI: 10.1007/s12098-018-2747-4
Parent-administered sensory interventions demonstrated significant measurable outcomes (p<0.05). Population: Indian children with ASD, home setting.
Study 5 — NCAEP 2020 Report
Sensory integration, visual supports, and token economies classified as Evidence-Based Practices for autism across all ages. nationalautismcenter.org
Our CRO team has reviewed and graded all research linked from this page. We align with the Oxford Centre for Evidence-Based Medicine (OCEBM) levels of evidence. No cherry-picking; no undisclosed conflicts.
Your Data Helps Your Child — and Every Child Like Yours
What GPT-OS® Learns from G-663
- Current seated duration baseline and rate of change
- Which of the 9 materials produced the most improvement
- Arousal regulation pattern (time-of-day performance variation)
- Generalization velocity (how quickly school improves after home gains)
- Risk window prediction (when regression is likely without reinforcement)
🔒 Privacy Assurance
All session data is anonymized before population-level analysis. Individual child data is stored securely and accessible only to parents and assigned clinicians.
Your G-663 data joins 20M+ sessions in the outcome database — contributing to the most detailed evidence base on seated attention intervention in Indian pediatric populations.
Privacy Policy → pinnacleblooms.org/privacy
See It In Action — 60 Seconds That Could Change Your Approach Forever
G-663 Reel Metadata
Reel ID: G-663
Series: Attention & Task Engagement — Episode 663
Title: 9 Materials That Help With Sitting for Tasks
Domain: OT-ATT | OT + ABA + Special Education
Duration: 75–85 seconds
Watch → pinnacleblooms.org/reels/G-663
Follow → @pinnacleblooms
What You'll See in This Reel
Before
A child before supports: sliding, standing, wandering
The 9 Materials
Introduced one by one with clear visuals and therapist voiceover
After 8 Weeks
The same child: regulated, seated, learning
Home Setup Demo
Complete setup demonstration replicable in 5 minutes
"Video modeling is classified as an Evidence-Based Practice for autism (NCAEP, 2020). Watching the reel before executing the protocol improves parent skill acquisition and confidence."

Consistency Across Caregivers Multiplies Impact
A technique practiced only by one parent, in one setting, with one setup — produces 30% of the results possible. When ALL caregivers understand and implement the same approach, the child's nervous system receives consistent signals — and progress accelerates dramatically.
📱 Share on WhatsApp
Send this page directly to grandparents, co-parents, and extended family caregivers.
📧 Email This Page
Forward to teachers, therapists, and any adult who spends seated activity time with your child.
⬇️ Family Guide PDF
Download the G-663 one-page printable guide. Simple summary of the 9 materials for grandparents, teachers, and extended family.
Explain to Grandparents (Copy This):
"Our child needs to move a little to focus. The special cushion and the timer help their body and brain stay at the table. It's not spoiling — it's science. Please use the cushion when [child's name] does any table activity with you. It makes a real difference."
Teacher/School Communication Template (Copy This):
"Dear [Teacher's Name], [Child's name] has been working with an occupational therapist on seated attention using the following tools: wobble cushion, visual timer, hand fidget, and task breakdown strips. These are evidence-validated materials that significantly improve sitting duration and on-task behaviour. We would be grateful if similar supports could be available at school. I can provide the cushion and timer. Please let me know if you'd like more information or an OT consultation for classroom setup."

Real Questions From Real Parents. Real Answers From Real Therapists.
Q: My child doesn't have a diagnosis. Can I still use these materials?
Absolutely. These materials support any child who struggles with seated attention, regardless of diagnosis. If you have concerns, a Pinnacle AbilityScore® assessment can provide clarity without requiring a formal diagnosis. 📞 9100 181 181
Q: Do these materials replace occupational therapy?
No — and they're not designed to. These materials are a home extension of what occupational therapists prescribe. They work best combined with professional OT guidance that personalises material selection. Think of this as the daily home practice layer.
Q: How long before I see results?
Most families see measurable improvement (increased sitting duration) within 2–4 weeks of consistent daily use. Full protocol outcomes emerge across 8–12 weeks. The key variable is consistency of implementation.
Q: My child uses the wobble cushion at home but still can't sit at school — why?
Generalisation takes deliberate practice across multiple settings with multiple people. Share the teacher communication template, provide a second set of materials for school, and request a school OT observation if possible.
Q: How do I know which of the 9 materials to start with?
Match to your child's primary reason for standing up: Movement-seeking → wobble cushion + foot fidget first. Overwhelm with task → visual timer + task strip first. Oral seeking → chewable first. Writing discomfort → slant board first. Not sure → call 9100 181 181.
Q: Is the wobble cushion safe for young children (3–4 years)?
Yes, with supervision. Ensure the chair has no wheels. Inflate firmly for young children (less wobble = more stability). Adult present for first 5–10 sessions.
Q: My child hates the weighted lap pad. Should I keep trying?
No. Never force sensory tools on a child. Try a lighter alternative (folded blanket). If all weighted items are aversive, this child may have tactile defensiveness — a separate clinical profile requiring OT assessment to confirm.
Q: Can I use these materials for meals and family activities, not just homework?
Yes — and you should. The more contexts where supports are available, the faster generalisation occurs. A wobble cushion at the dining table, a visual timer for family game time, a hand fidget during car rides — each builds the same neural pathway.
Additional questions: Ask GPT-OS® → pinnacleblooms.org/gpt-os/ask | Book a Teleconsultation → pinnacleblooms.org/teleconsult
Preview of 9 materials that help with sitting for tasks Therapy Material
Below is a visual preview of 9 materials that help with sitting for tasks therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

Your Child Can Sit. They Just Need the Right Support.
You have the knowledge. You have the evidence. You have the tools. The only thing left is to begin.
🟦 Occupational Therapy
🟩 ABA / BCBA
🟧 Special Education
🟪 Speech-Language Pathology
🟥 Neurodevelopmental Paediatrics
20M+
Sessions Delivered
97%+
Improvement Rate
70+
Centers Nationwide
📞 FREE National Autism Helpline: 9100 181 181 — 24×7, 16+ languages
"From fear to mastery. One technique at a time." — Pinnacle Blooms Network®, India's largest multi-disciplinary paediatric therapy consortium. G-663 is one of 70,000+ intervention techniques in the world's most comprehensive structured paediatric intervention knowledge base. Built on evidence. Designed for homes. Delivered at population scale.
This content is educational and does not replace individualised occupational therapy assessment and intervention. Sitting difficulties may indicate sensory processing differences, attention disorders, motor challenges, or other developmental concerns requiring professional evaluation. Strategies should be individualised based on comprehensive assessment. Consult occupational therapists and healthcare providers for persistent sitting challenges. Individual results may vary.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
← G-662: Listening to Instructions | G-664: Attention During Group Instruction → | techniques.pinnacleblooms.org
30