
"He covers his ears at sounds I can barely hear. And then, minutes later, he's crashing into the sofa looking for something — anything — to feel himself."
This is not defiance. This is a nervous system speaking the only language it knows.
9 Materials That Help With Sensory Overall
Sensory Processing & Regulation — Episode L-996
You are not failing. You are not alone. Your child's brain is wired differently — not wrongly. And there is a science-backed path forward.
You've watched your child flinch at the blender, refuse to wear their school uniform because of a single seam, spiral into meltdown at the supermarket — while other children walk through the same aisle without a second look. And then, the same afternoon, they're seeking the most intense sensory input they can find: spinning, crashing, chewing through shirt collars. You are not failing. Your child's nervous system is speaking. And there are 9 proven, clinically-validated, home-applicable tools that give that nervous system exactly what it needs to regulate.
You Are Not Alone — The Numbers Confirm It
Sensory processing differences are not rare. They are not signs of poor parenting. They are neurologically documented, globally prevalent, and — critically — responsive to structured intervention.
80%
ASD + Sensory
of children diagnosed with autism experience significant sensory processing difficulties
1 in 36
Global Prevalence
children globally receive autism diagnosis — sensory challenges cross all of them
21M+
Sessions Delivered
therapy services delivered by Pinnacle, tracking sensory outcomes in real Indian families
The family exhausted by clothing battles every morning belongs to a global community of millions navigating the exact same challenge. The parent who has memorized which grocery store aisles to avoid is not alone. This community is enormous. And the evidence base to support them is growing every year.
PRISMA Systematic Review (2024): 80% of children with ASD display sensory processing difficulties. Sensory integration therapy meets criteria as an evidence-based practice across 16 independent studies. — PMC11506176 | World J Clin Cases, 2024 (PMC10955541). India's autism prevalence data (INCLEN Trust, NIMHANS 2018) places the number of children needing sensory support in the millions — yet structured, evidence-based sensory intervention remains inaccessible for most families outside metro centers. This page exists to close that gap.

The Neuroscience, In Plain English
What's Happening in the Brain
When sensory processing is atypical, the brain's filtering system — called sensory modulation — doesn't calibrate correctly. Think of it as a volume knob with no middle setting: everything is either blasting at full volume or so quiet the signal doesn't register.
🔴 Over-Responsive (Hypersensitive)
Light touch registers as pain. Moderate sound triggers fight-or-flight. The somatosensory cortex and amygdala over-amplify input signals.
🔵 Under-Responsive (Hyposensitive)
Signals don't register. The child seems in their own world, doesn't notice injury, needs intense input to feel anything.
🟡 Sensory Seeking
The brain actively hunts for intense input to regulate arousal. Spinning, crashing, chewing, climbing — these are self-regulation attempts, not misbehavior.
Key Brain Regions
Somatosensory Cortex
Processes touch, texture, and pressure
Vestibular Nuclei (Brainstem)
Processes movement, balance, and head position
Cerebellum
Coordinates sensory input with motor response
Amygdala
Threat detection; over-fires in sensory overwhelm
Prefrontal Cortex
Regulation; under-developed in younger children
"This is a wiring difference. Not a behavior choice. Not a parenting failure. A neurological reality — and one that responds to structured sensory input." — Pinnacle OT Consortium
Most children show mixed patterns — over-responsive to some inputs, under-responsive to others, seeking in specific systems. Research Callout: Frontiers in Integrative Neuroscience (2020) establishes sensory-based interventions as operating on documented neural pathways. — DOI: 10.3389/fnint.2020.556660
The 8 Sensory Systems
Every sensory system plays a distinct role in how your child experiences the world. Understanding which systems are over- or under-responsive is the foundation of a targeted sensory toolkit.
Visual
Light, color, movement, spatial perception
Auditory
Volume, pitch, frequency, location of sound
Tactile
Pressure, texture, temperature, pain
Gustatory
Intensity, texture, and variety of taste
Olfactory
Strength, type, and persistence of scent
Vestibular
Movement, balance, head position — the most powerful arousal modulator
Proprioceptive
Body position, force, joints and muscles — almost universally calming
Interoceptive
Hunger, thirst, temperature, pain, and internal body signals

Your Child's Developmental Context
Age Range: 2–12 Years
Primary Window: 3–7 Years
Birth–18 Months
Foundation sensory systems activate; early modulation begins
18 Months–3 Years
Sensory differences often become visible through behavioral signs
3–7 Years ★
Primary intervention window — neural plasticity highest; sensory diet most impactful
7–12 Years
Continued benefit; self-regulation awareness becomes teachable
12+ Years
Compensation strategies, self-advocacy, environmental adaptation
Common Co-Occurring Conditions
ASD
80% prevalence of sensory differences
ADHD
40–60% co-occurrence with sensory challenges
DCD
Developmental Coordination Disorder
Anxiety
Sensory overwhelm as a primary trigger
Feeding
Oral sensory component in feeding disorders
WHO Care for Child Development (CCD) Package: Implemented in 54 low- and middle-income countries with age-specific evidence-based caregiver recommendations. — PMC9978394

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: I
Systematic Review + Multiple RCTs
94%
evidence confidence across converged disciplines
Key Studies at a Glance
Study | Finding | |
PRISMA Systematic Review (2024) | 16 studies confirm sensory integration as EBP for ASD — PMC11506176 | |
Meta-analysis, World J Clin Cases (2024) | Promotes social skills, adaptive behavior, motor skills across 24 studies — PMC10955541 | |
Indian RCT, Indian J Pediatr (2019) | Home-based interventions show significant outcomes in Indian children — DOI:10.1007/s12098-018-2747-4 | |
WHO Nurturing Care Framework (2018) | Multi-sensory caregiver interventions validated across 54 LMICs | |
NCAEP (2020) | Sensory-based interventions classified as evidence-based practice |
"Structured sensory intervention, consistently applied at home, produces measurable improvements in regulation, participation, and daily function."
OT
Sensory Integration
ABA
Behavior Support
SLP
Oral-Motor
SpEd
Environmental Access
NeuroDev
Arousal Regulation

What Is the Sensory Regulation Material Toolkit?
Episode L-996
Domain: Sensory Processing | SENS-OVR
"The 9 Tools That Help Your Child Feel Right in Their Body"
Sensory regulation materials are clinically-selected physical tools that provide specific types of sensory input — deep pressure, movement, resistance, oral motor, visual calming, tactile input, sound management — to help a child's nervous system reach and maintain an optimal state of arousal for daily function, learning, and participation.
These are not toys. They are therapeutic instruments. Each material targets a specific sensory system or modulation pattern, grounded in Ayres Sensory Integration theory and validated across decades of occupational therapy research.
When used as part of a structured sensory diet — a personalized schedule of sensory input throughout the day — these materials transform a reactive, overwhelmed, or under-registered nervous system into one capable of participating in family life, school, and community.
Classification at a Glance
Age Range
2–12 years
Session Duration
10–20 minutes per tool session; sensory diet runs throughout the day
Frequency
Daily integration recommended
Setting
Home + School + Community
Weighted Products
Vestibular Equipment
Proprioceptive Tools
Oral Motor Tools
Fidget Tools
Auditory Supports
Visual Calming
Tactile Materials
Regulation Kits

This Crosses Every Therapy Boundary — Because the Brain Doesn't Organize by Therapy Type
Occupational Therapy
Primary Lead for Sensory Overall. Sensory integration assessment and therapy, sensory diet design, equipment selection, environmental modification, and sensory profile mapping.
Speech-Language Pathology
Co-Lead for Oral Motor & Feeding. Oral sensory processing, chew tool selection, feeding-related sensory challenges, oral motor warm-up before speech sessions.
ABA / BCBA
Behavioral Context. Sensory-informed behavior support, identifying sensory antecedents to challenging behavior, data collection during sensory sessions.
Special Education
Classroom Sensory Access. Classroom accommodations, fidget tools, flexible seating, sensory breaks, and environmental modification for learning.
NeuroDevelopmental Pediatrics
Medical Oversight. Identifying sensory processing differences vs. medical causes, co-occurring condition management, and referral pathways.
"A child in ABA therapy who is sensory-seeking will not respond to behavior plans that ignore the sensory antecedent. The disciplines are not alternatives — they are a system." — Pinnacle FusionModule™ Clinical Principle

A Precision Toolkit — Not Random Activities
Every material has a precise purpose. The bullseye model shows how sensory tools work outward — from core neurological regulation to daily life participation.
What the Materials Actually Target
Primary Targets (Core)
- Sensory modulation — regulating response to sensory input
- Arousal regulation — optimal alertness for function
- Sensory discrimination and self-regulation
Secondary Targets
- Sustained attention and focus during learning
- Emotional regulation — reducing meltdown frequency
- Motor planning and coordination
- Sleep quality and feeding tolerance
Tertiary / Long-Term Targets
- Social participation — tolerating environments
- Academic engagement — regulated enough to learn
- Independence — self-initiating regulation strategies
- Family quality of life — reduced household stress
Meta-analysis (PMC10955541, 2024): Sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills across 24 independent studies.

Material 1: Weighted Products
Blankets · Lap Pads · Vests
₹1,500–6,000
Deep pressure calms, organizes, and grounds the nervous system. Weighted products activate the proprioceptive system via sustained even pressure — signaling "you are safe" to the amygdala. The neurological mechanism is identical to receiving a firm hug.
How It Works
Activates proprioceptive system via sustained even pressure across body surface
Best Starting Point
Weighted lap pad — ideal for school and homework use
Safety Rule
Maximum weight = 10% of body weight. Never cover face. Child must be able to remove independently.
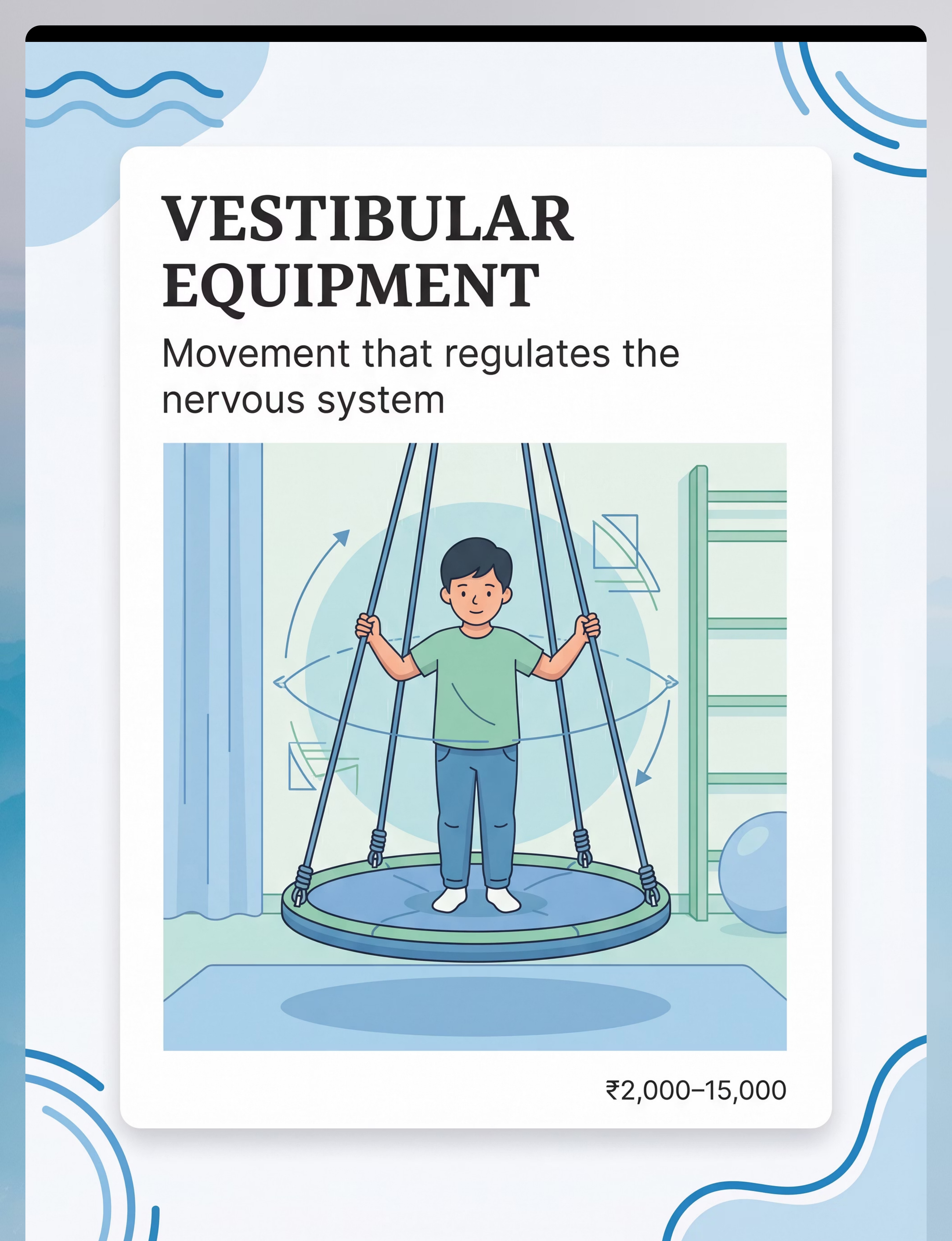
Material 2: Vestibular Equipment
Swings · Spin Boards · Balance Tools
₹2,000–15,000
- Movement input that regulates the nervous system from the inside out. The vestibular system is the most powerful arousal modulator in the sensory toolkit. The direction and type of movement matters enormously: slow linear swing = calming; rotational spin = alerting and organizing.
Slow Linear
Front-to-back, parasympathetic calming response
Orbital / Rotational
Alerting and organizing; use with caution and observe arousal
Balance Board
Gentle, child-controlled vestibular input for milder needs
Safety Note: Professional installation required for ceiling-mount equipment. Never leave child unattended on swing. Watch for signs of over-arousal or nausea.
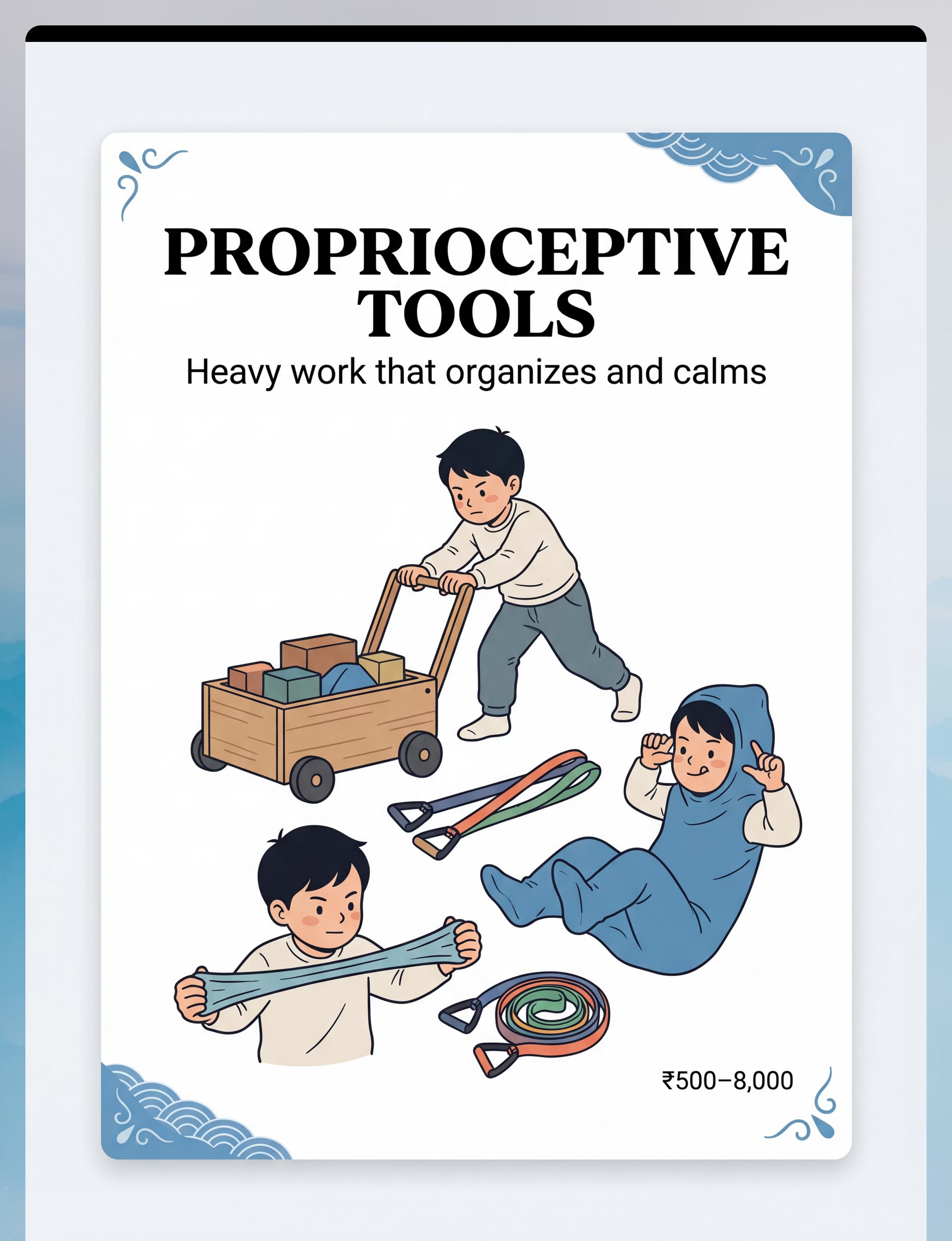
Material 3: Proprioceptive Tools
Therapy Putty · Resistance Bands · Body Socks · Crash Pads
₹500–8,000
Heavy work that organizes and calms. Proprioceptive input — pushing, pulling, and resistance — is almost universally calming and organizing across all sensory profiles. This is the "safe" sensory input — the ideal starting point for any child, any day.
Therapy Putty
Squeeze, pull, and roll for 3–5 minutes. Multiple resistance levels available.
Body Sock
Full-body resistance that provides deep proprioceptive feedback with movement
Crash Pad
Safe crashing and rolling input for high-seeking proprioceptive needs
Resistance Bands
Seated heavy work for school or desk settings

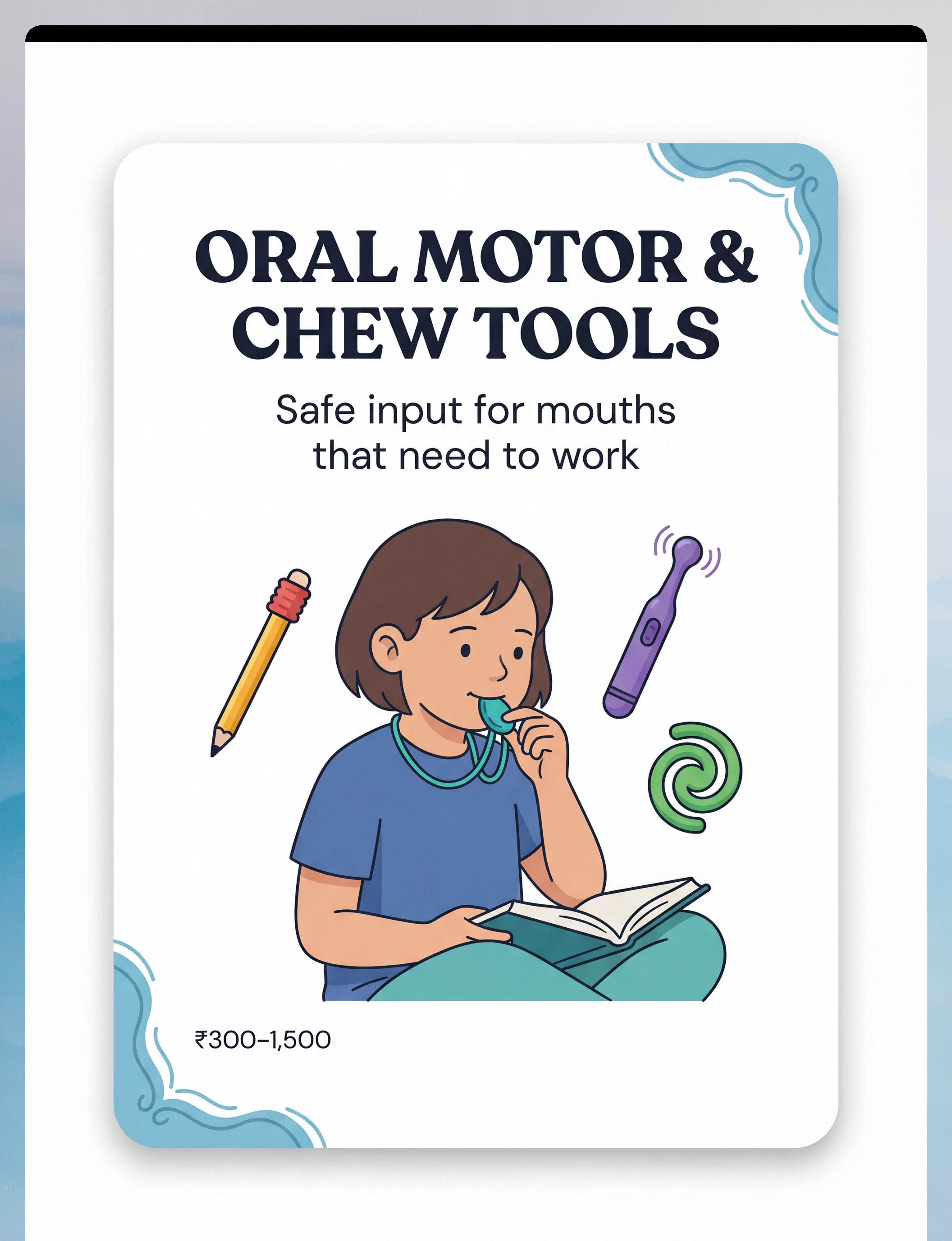
Material 4: Oral Motor & Chew Tools
Chew Necklaces · Pencil Toppers · Vibrating Oral Tools
₹300–1,500
Safe input for mouths that need to work. The mouth has more sensory receptors per cm² than almost any other body region — making oral proprioception a powerful and reliable regulator. Chew tools channel this need safely, reducing mouthing of clothing, pencils, and other non-food items.
Chew Necklace
Worn throughout the day; different resistance levels for different needs
Pencil Topper
Discreet school-appropriate option; replaces pencil-chewing
Vibrating Oral Tool
Introduce slowly; allows child to control — alerting and organizing
Safety Critical: Food-grade silicone only. Inspect for wear at every use. Replace immediately if any pieces are separating. Never use on infants without OT guidance.
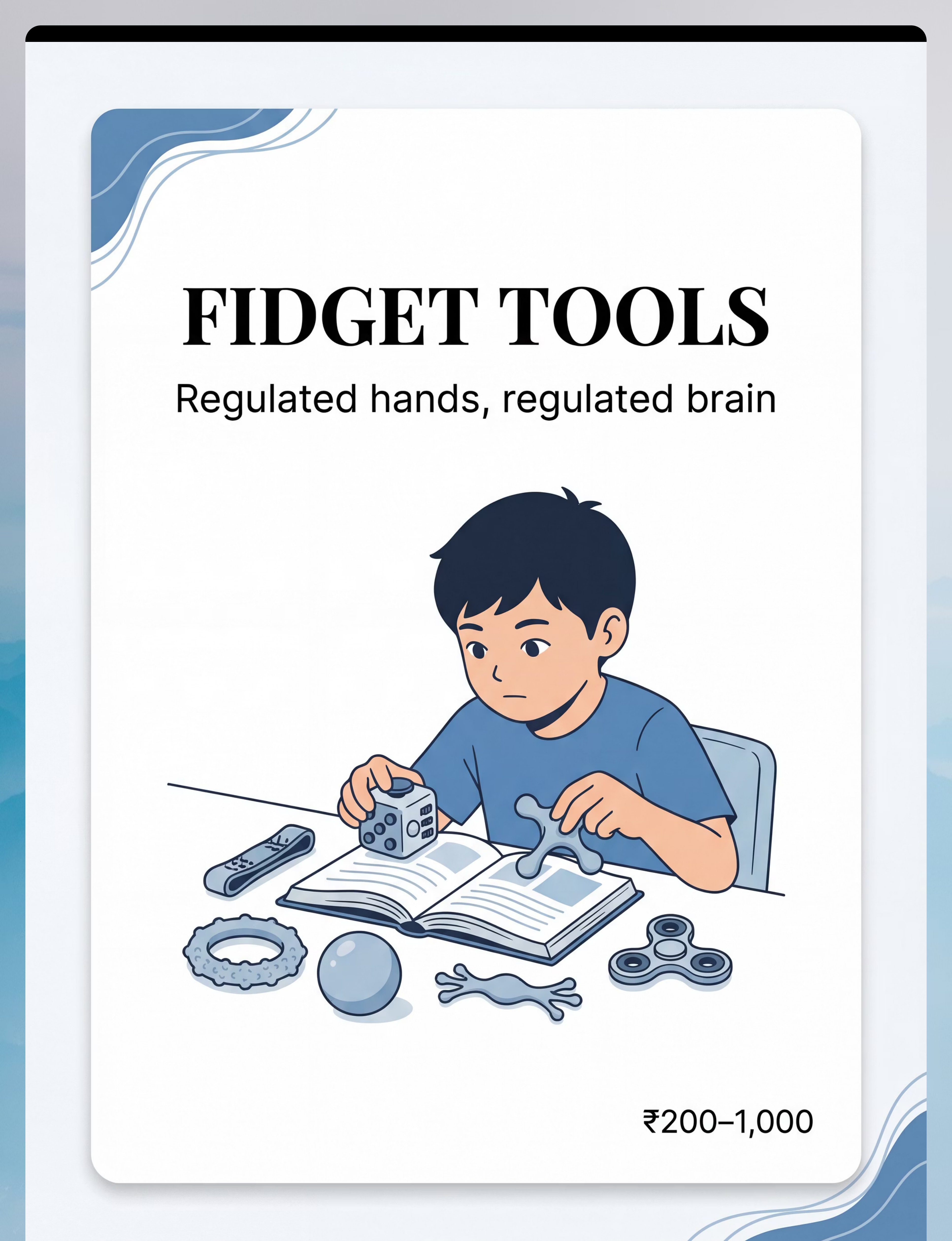
Material 5: Fidget Tools
Fidget Cubes · Textured Toys · Stretchy Bands · Putty
₹200–1,000
Regulated hands → regulated brain. Manual sensory input during cognitive tasks improves arousal regulation without competing for attention — when the right fidget is matched to the sensory need. The wrong fidget becomes a distraction; the right one becomes invisible, quietly organizing the nervous system throughout a task.
Fidget Cube
Multiple textures and actions; rotates through sensory input types
Textured Toy
Tactile proprioceptive input; held in non-dominant hand
Stretchy Band
Chair-leg band allows leg movement while seated; school-appropriate
Putty
Quiet, non-visual, resistance-based — excellent for classroom use
Classroom fidgets must be quiet and non-visually distracting. Introduce at home first to establish the function before bringing to school.

Material 6: Auditory Tools
Noise-Reducing Headphones · White Noise Machine · Ear Protection
₹800–5,000
Managing sound for sensitive ears. For auditory over-responders, unpredictable sound triggers an amygdala-based threat response — fight, flight, or freeze — before conscious awareness even registers the source. Noise reduction removes the trigger; white noise provides a predictable auditory background that allows the brain to relax its constant environmental scanning.
Noise-Reducing Headphones
Use proactively before entering challenging environments — not only in response to distress
White Noise Machine
Turn on before sessions begin; introduce at low volume and adjust upward gradually
Key Principle
Proactive use prevents escalation. Reactive use manages crisis. Always aim for prevention.

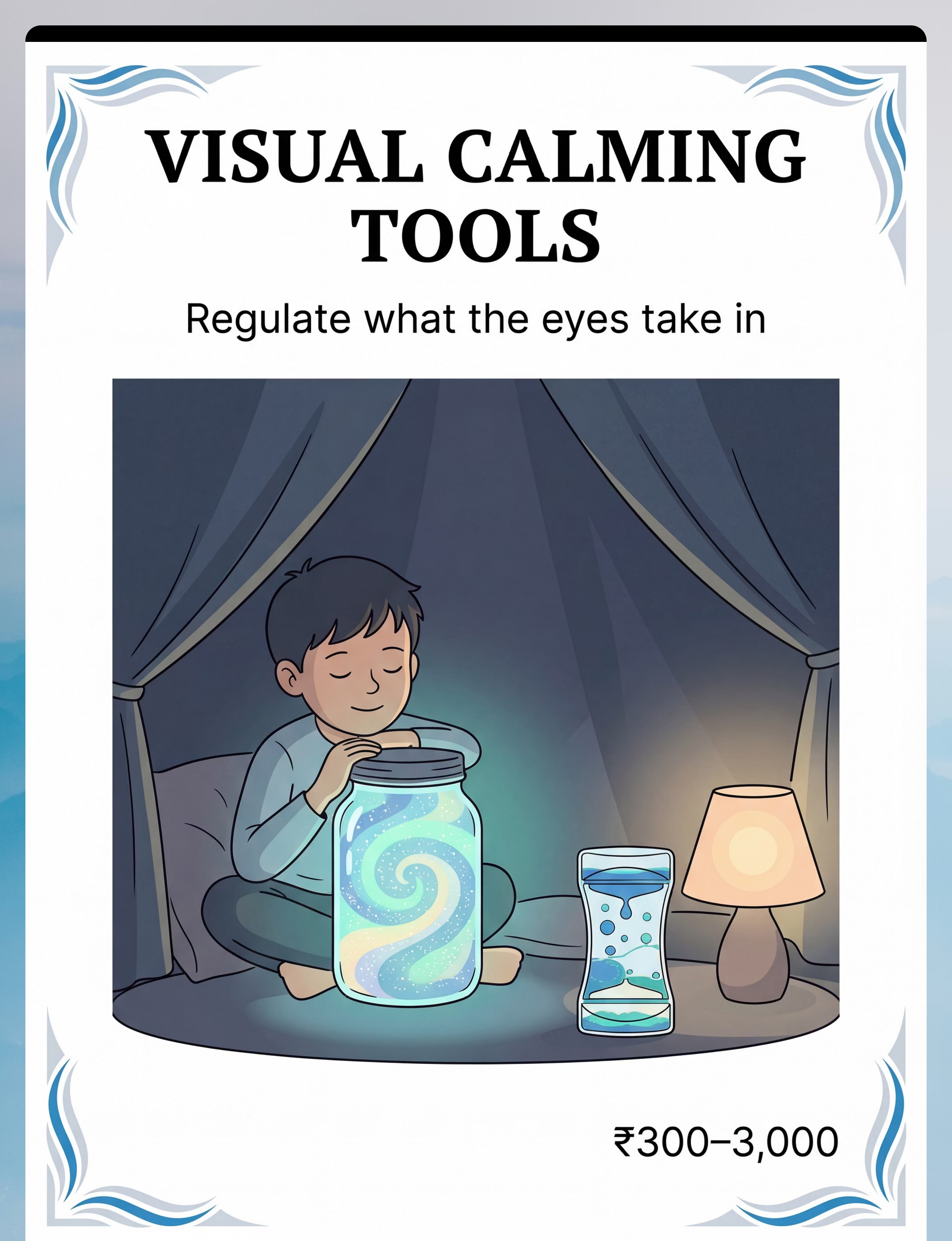
Material 7: Visual Calming Tools
Glitter Jars · Liquid Timers · Dimmable Lamps · Canopy/Tent
₹300–3,000
Regulate what the eyes take in. Visual input directly modulates arousal level. Slow, predictable visual movement — glitter settling, liquid timer flowing — activates the parasympathetic "rest and digest" response, gently pulling the nervous system out of fight-or-flight. A dimmed, enclosed space (canopy, tent) reduces visual overload and creates a sensory sanctuary.
Calm-Down Jar
Shake it, hand to child: "Watch the stars settle." Slow visual tracking = arousal reduction
Liquid Timer
Doubles as a transition timer — visual, non-auditory, predictable
Dimmable Lamp
Warm, low-level lighting reduces visual stimulation in the calm-down corner
Canopy/Tent
Creates a visually enclosed retreat space — reduces environmental visual load

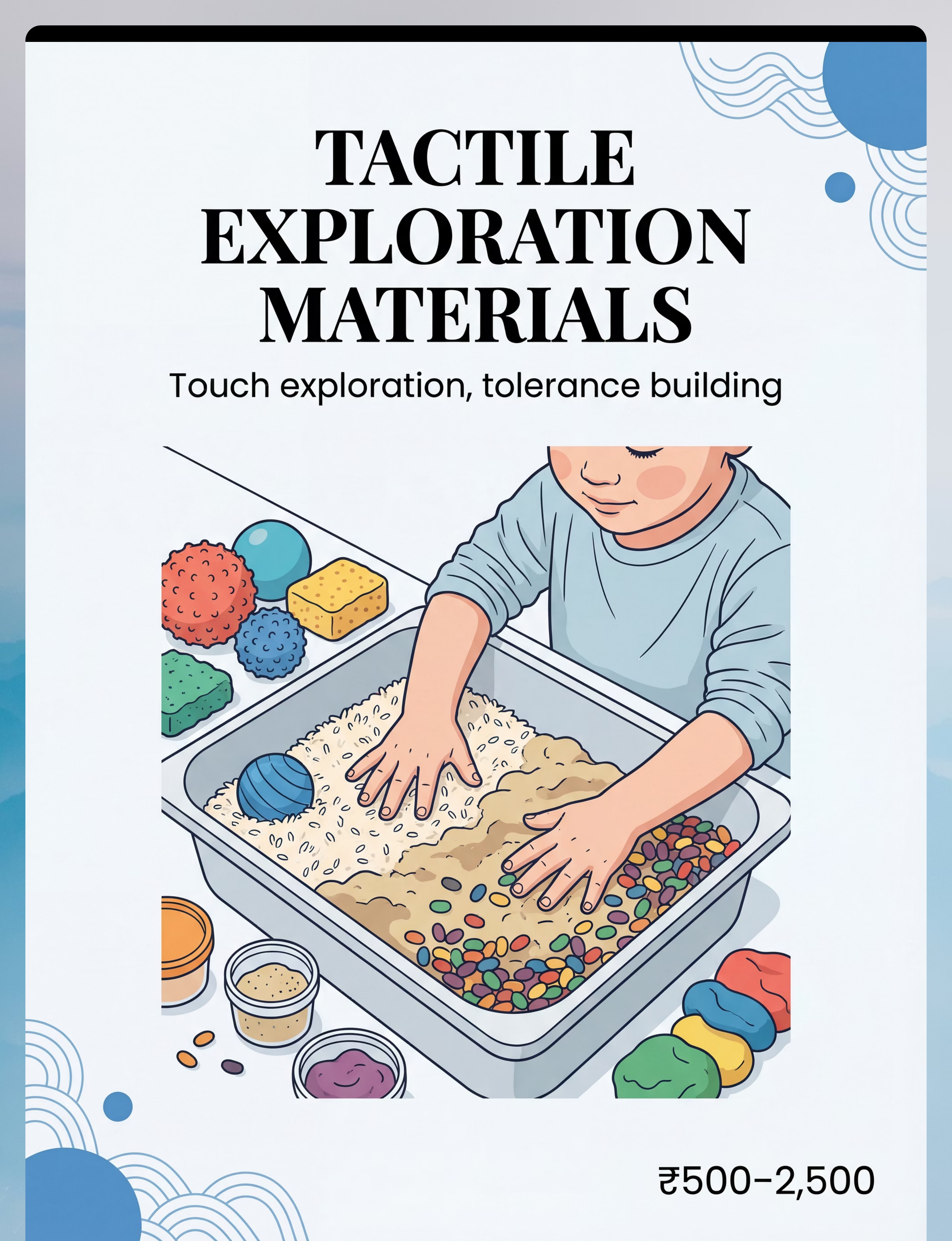
Material 8: Tactile Exploration Materials
Sensory Bins · Kinetic Sand · Playdough · Textured Balls
₹500–2,500
Touch exploration and tolerance building. Graded tactile exposure — always child-led, never forced — builds neural pathways that expand tactile tolerance over time. The playful context removes the threat response, allowing the nervous system to process touch information safely. Each session, even a brief fingertip touch of the bin edge, is building the pathway.
Start With You
Put YOUR hands in first. Make sounds of pleasure. Do not say "put your hands in."
Proximity → Touch → Immersion
Build from watching → touching edge → brief contact → full hands-in over multiple sessions
Change Fillers Weekly
Novelty maintains engagement. Dry rice, beans, pasta, sand, water beads — each new texture is new therapy.

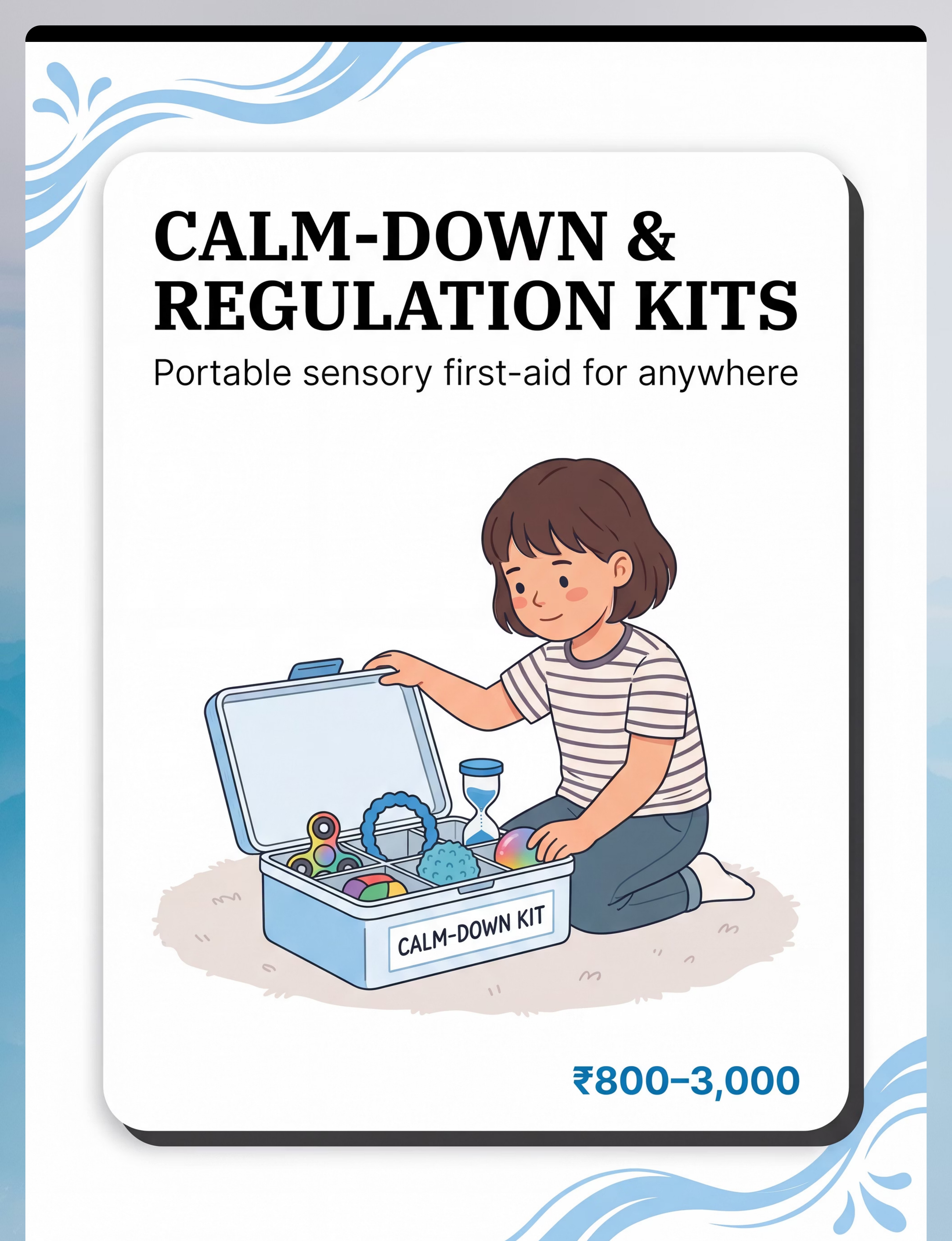
Material 9: Calm-Down & Regulation Kits
Portable Sensory First-Aid for Anywhere
₹800–3,000
Multiple tools, multiple systems, one accessible place. Pre-assembled multi-system kits enable regulation intervention before full dysregulation — preventive rather than crisis-response. When a child feels overwhelm beginning, the kit is there: familiar, accessible, and already proven. Child involvement in kit creation dramatically increases buy-in and independent use.
Practice First
Use the kit during non-crisis moments at home before relying on it in community
Child-Chosen
"Here's our regulation kit. What do you want to try?" — choice increases independence
Teach the Cue
"When you feel [describe dysregulation sign], you can open this kit."
Portability
Any pencil case works: rubber band + smooth stone + frozen washcloth + calming card

Every Material Has a ₹0 Version. Full Stop.
WHO/UNICEF Equity Principle
No Family Is Excluded Because of Budget
Material | Buy This | Make This (₹0) | Same Principle | |
Weighted Blanket | ₹1,500–4,000 | Layer 3–4 heavy quilts. Rice in fabric pouches for lap pad. | Deep pressure regardless of source | |
Vestibular Swing | ₹2,000–15,000 | Hammock tied between trees. Office chair spinning (supervised). Rolling down a grassy hill. | Vestibular input is input | |
Therapy Putty | ₹300–800 | Homemade playdough: flour + salt + water + oil. Knead bread dough. | Resistance and proprioception | |
Chew Tools | ₹300–1,500 | Frozen wet washcloth. Crunchy carrots, celery, bagels. Bubble blowing. | Oral proprioception and motor work | |
Fidget Tools | ₹200–1,000 | Rubber bands on wrist. Smooth stones. Balloon filled with flour. Velcro under desk. | Tactile and proprioceptive input | |
Noise Headphones | ₹800–3,000 | Over-ear cushion headphones (even without music). Soft earmuffs. | Auditory input reduction | |
Glitter Calm Jar | ₹300–500 | Clear jar + water + glitter + glycerin (chemist, ₹50). Seal tightly. | Slow visual movement = parasympathetic | |
Sensory Bin | ₹500–2,500 | Plastic container + dry rice/beans/pasta. Nature items: pinecones, leaves, stones. | Tactile exploration through texture variety | |
Regulation Kit | ₹800–3,000 | Any pencil case: rubber band + washcloth + smooth stone + headphones + calming card | Multi-system portable kit |
"The most powerful proprioceptive tool is your household. Every carry, push, and pull is therapy." — Pinnacle OT Consortium
The Free Proprioceptive Toolkit — Heavy Work at Home
Carry Groceries
From car to kitchen — functional heavy work
Wheelbarrow Walks
Parent holds legs, child walks on hands — 3–5 lengths
Animal Walks
Bear crawl, crab walk, elephant stomp — full body proprioception
Wall Push-Ups
10 reps before every transition — 60 seconds of organizing input
Dig in Garden
Sand or soil digging — tactile AND proprioceptive
Tug of War
With a towel — bilateral resistance and proprioception

Safety Gate — Read Before Every Session
🟢 GREEN — Proceed Normally
- Child has eaten in the last 90 minutes
- Child is awake with adequate sleep
- No fever, illness, or visible physical discomfort
- Child is in mid-range arousal — not in meltdown or shutdown
- Environment set up as per the space checklist
- All materials checked for wear and safety
🟡 AMBER — Modify and Proceed Carefully
- Child mildly elevated → use only weighted/proprioceptive tools; reduce duration 50%
- Child slightly under-aroused → start with alerting vestibular movement, then transition
- Increase reinforcement and reduce demands throughout
🔴 RED — Stop. Do NOT Proceed.
- Child is in active meltdown or shutdown
- Child is ill, in pain, or running a fever
- Child has recently sustained a head injury (vestibular contraindicated)
- Signs of seizure activity or extreme disorientation
- Child expressing clear distress about the material
- You are highly emotionally dysregulated yourself
STOP immediately if you observe: sudden behavioral escalation · nausea or dizziness (vestibular) · self-injurious behavior increasing · extreme distress vocalizations · pallor, unusual breathing change, or loss of balance.
"The best session is one that starts right. Skipping a day is never failure — it's clinical wisdom."

The Right Environment Is Half the Intervention
Sensory-Safe Zone Setup
① Child Position
Soft mat, rug, or cushion on the floor. Back against wall if child prefers boundary. Clear space all around.
② Materials Station
Within arm's reach of child. One material visible at a time. Visual timer present — not auditory.
③ Calm-Down Corner
Tent or canopy with weighted blanket inside. Calm-down jar within reach. This is the retreat option during sessions.
④ Parent Position
Seated at child's eye level — floor or small stool. NOT standing over child. Within reach but not crowding.
⑤ Environmental Check
Dim lighting. TV/music OFF. Siblings out of room. Phone silent. Tag-free clothing. Clear sight lines.
Remove from the Space
Electronic Screens
No screens facing the child during sensory sessions
Fluorescent Lighting
Bright overhead lighting increases arousal; switch to warm lamp
Unpredictable Sound
TV news, video calls, other children competing for attention
Visual Clutter
Clear flat surfaces in the child's sight line
"Spatial precision prevents 80% of session failures. The environment is the first therapeutic tool."

Step 1: The Invitation
STEP 1 of 6
⏱ 30–60 Seconds
The Script — Exact Words
"Hey [child's name], I have something cool to show you. Do you want to come see?"
If Resistance Occurs
Don't push. Try: "Okay, I'm going to play with this here. You can watch." Child observing is participation — respect the window.
ABA Pairing Principle: First create the association between you, the material, and positive experience before making any demand. Pairing precedes everything.
Body Language
Get to Their Level
Physically lower yourself — do not stand over the child
Open Posture
Calm, unhurried voice; hold the material casually, not thrusting it forward
Wait 10 Seconds
If no response, repeat once, then try gentle proximity
What Acceptance Looks Like
- Physical approach toward material or you
- Eye gaze toward material
- Reaching gesture
- Vocalizing interest — any sound counts
- Sitting down near you
Step 2: The Engagement
STEP 2 of 6
⏱ 1–3 Minutes
Once the child has shown any acceptance signal, move into modeling rather than directing. You use the material first. The child watches. This is the moment the material becomes interesting — because you are making it interesting.
Weighted Blanket
"Look how heavy this is... I'm going to put it on my lap. Feels SO heavy. [Pause] Want to try?"
Vestibular Swing
Sit in it yourself first if possible. "Whoaaaa this is so slow. [Gentle push] Feels nice."
Therapy Putty
Start squeezing it yourself. "It's so squishy... look what it does... want some?"
Fidget Tool
Turn it, click it, roll it — make it look interesting, not functional
Sensory Bin
Put YOUR hands in first. Make sounds of pleasure. Don't say "put your hands in."
Calm-Down Jar
Shake it yourself, hold it up. "Look at all those stars going to sleep..."
🟢 Engagement
Reaches, touches, mimics → continue to Step 3
🟡 Tolerance
Watches, stays nearby → continue at reduced pace
🔴 Avoidance
Moves away → return to invitation mode, respect the pace
Step 3: The Therapeutic Action
STEP 3 of 6
⏱ 5–12 Minutes
This is the therapeutic core. The specific action depends on which material you are using. Below is the precise execution protocol for each of the 9 materials.
Weighted Products
Place item on child's lap or over shoulders. Allow the weight to settle — do not force. If accepted, leave in place for 5–15 minutes during calm activity (drawing, reading, snack). Duration: 5–20 min | Response: settling, reduced movement, increased focus
Vestibular Swing
Begin with slow linear movement (front to back). Count aloud: "One... two... three..." Watch the child's face — eyes soft = calming; eyes wide/excited = alerting. Duration: 5–10 min | Response: calming (slow) or organizing (moderate)
Proprioceptive Heavy Work
Wheelbarrow walks 3–5 lengths. Wall push-ups 10 reps. Therapy putty squeeze/pull 3–5 minutes. Carry a heavy backpack for 2 minutes. Duration: 5–10 min | Response: organizing, calming, increased focus within 15 min
Oral Motor / Chew Tools
Introduce chew necklace during seated activity — don't direct it to mouth, let child discover. For crunchy input: 5–10 bites before a demanding task. Duration: Throughout day | Response: reduced mouthing of non-food items, increased calm
Fidget Tools
Provide during seated cognitive task. Child holds in non-dominant hand. Do not comment on the fidgeting. Observe whether attention on task increases. Duration: Throughout seated activity | Response: attention maintained longer
Auditory Tools
Put headphones on BEFORE entering challenging environment — proactively. White noise: turn on before session begins. Duration: As needed | Response: reduced startle, more tolerance
Visual Calming
Shake calm-down jar, hand to child, say "watch the stars settle." Dim lights. Use visual timer for transition warnings. Duration: 2–5 min active use | Response: slower breathing, visual tracking
Tactile Exploration
Place bin in front of child. Put YOUR hands in. Wait. Narrate: "Feels like sand... it's smooth... it's heavy." Never push child's hands in. Duration: 5–15 min | Response: increased tactile tolerance over time
Regulation Kit
Bring kit to child. "Here's our regulation kit. What do you want to try?" Let child choose. Teach: "When you feel [dysregulation sign], you can open this kit." Duration: As needed | Response: self-initiated kit access over time

Step 4: Repeat & Vary — Therapeutic Dosage
STEP 4 of 6
⏱ 3–5 Minutes Additional
"3 good repetitions where the child is engaged and regulated = more therapeutic value than 10 pushed-through repetitions where the child is tolerating, not benefiting." — Pinnacle OT Clinical Principle
Material | Target Reps/Duration | Variation to Introduce | |
Weighted products | 1 session daily, 10–20 min | Blanket → lap pad → vest; location variety | |
Vestibular swing | 5–10 min × 2–3 times/day | Linear → orbital; sitting → standing; eyes open → closed | |
Heavy work | 3–5 activities daily | Indoor → outdoor; push → carry → pull | |
Chew tools | Available throughout day | Vary resistance level; alternate with crunchy foods | |
Fidget tools | During all seated activities | Rotate fidget type to maintain engagement | |
Auditory tools | Pre-emptive for all challenging environments | Gradually reduce reliance as tolerance builds | |
Visual calming | 2–3 sessions daily | Different visual timers; vary lighting environments | |
Tactile materials | 1–2 sessions daily | Change bin fillers weekly; add new textures gradually | |
Regulation kit | Practice during non-crisis first | Add new items; let child personalize the kit |
Satiation Indicators — When to Stop
Pushes Away
Child pushes material away or leaves the session space
Escalation
Behavioral escalation beginning — this is enough for today
Fatigue Signs
Yawning, eye rubbing for calming materials — system is satisfied
Loss of Interest
Disengagement from the material — stop before resistance builds

Step 5: Reinforce & Celebrate
STEP 5 of 6
⏱ Within 3 Seconds of Target Behavior
The Reinforcement Rule
Praise within 3 seconds of the desired behavior. Not 10 seconds. Not "good job" at the end of the session. Immediately, specifically, enthusiastically.
"Celebrate the attempt. The nervous system learning to tolerate a new sensation is as much an achievement as mastery. The brain needs to know: this is good."
Praise Scripts by Behavior
Touches Material
"Yes! You touched it! I love how brave you are!"
Tolerates Weighted Blanket 60s
"You kept that on! That was SO good for your body!"
Chooses Fidget Independently
"You picked that up yourself! You know what your body needs!"
Accesses Calm-Down Kit
"You got your kit! You're taking care of yourself!"
Completes Heavy Work
"STRONG! Look at those muscles helping your brain!"
Reinforcement Menu
- Social: High-five, thumbs up, specific verbal praise
- Tangible: Preferred sticker, 2-minute preferred toy access
- Activity: Jump 5 times, spin once, brief preferred movement
- Token: Star/point toward visual reward board

Step 6: The Cool-Down
STEP 6 of 6
⏱ 2–3 Minutes
No session ends abruptly. The transition out of a sensory session is itself a therapeutic moment — and one of the most common sources of post-session dysregulation when handled poorly.
① The Warning (60 Seconds Before Ending)
"Two more times, then we're all done." Show visual timer or count down on fingers.
② The Closure Activity (60–90 Seconds)
Weighted blanket: "Let's put it to sleep" — child folds or puts away. Sensory bin: "Let's find 5 blue things and put them back." Child participates in put-away ritual if able.
③ The Bridge Statement (15 Seconds)
"You did such good body work today. Your brain is going to feel so good. Now we're going to [next activity]."
If Child Resists Ending
- Use the visual timer as authority (not you): "Timer says all done"
- Offer a transition object as a bridge to the next activity
- Brief preview of next activity as motivator: "After this we have snack!"
NCAEP (2020): Visual supports and transition structures are classified as evidence-based practice for autism. Transition failures are the most common source of post-session dysregulation.

Capture the Data: Right Now
60 seconds of data now = weeks of clinical insight later. You don't need research-grade data. You need enough data to answer one question: Is this working? For your child, in your home, with these materials.
Material Used
Check which of the 9 materials. Track which materials work best over time.
Session Duration
Write the minutes. Dosage tracking tells you if you're under- or over-providing input.
Engagement Rating 1–5
1=refused, 5=fully engaged. Your progress baseline across weeks.
One Observable Behavior
E.g., "tolerated weighted lap pad 8 min." Specific and measurable.
Post-Session Regulation
Better / Same / Worse 30 minutes later. Validates material effectiveness.
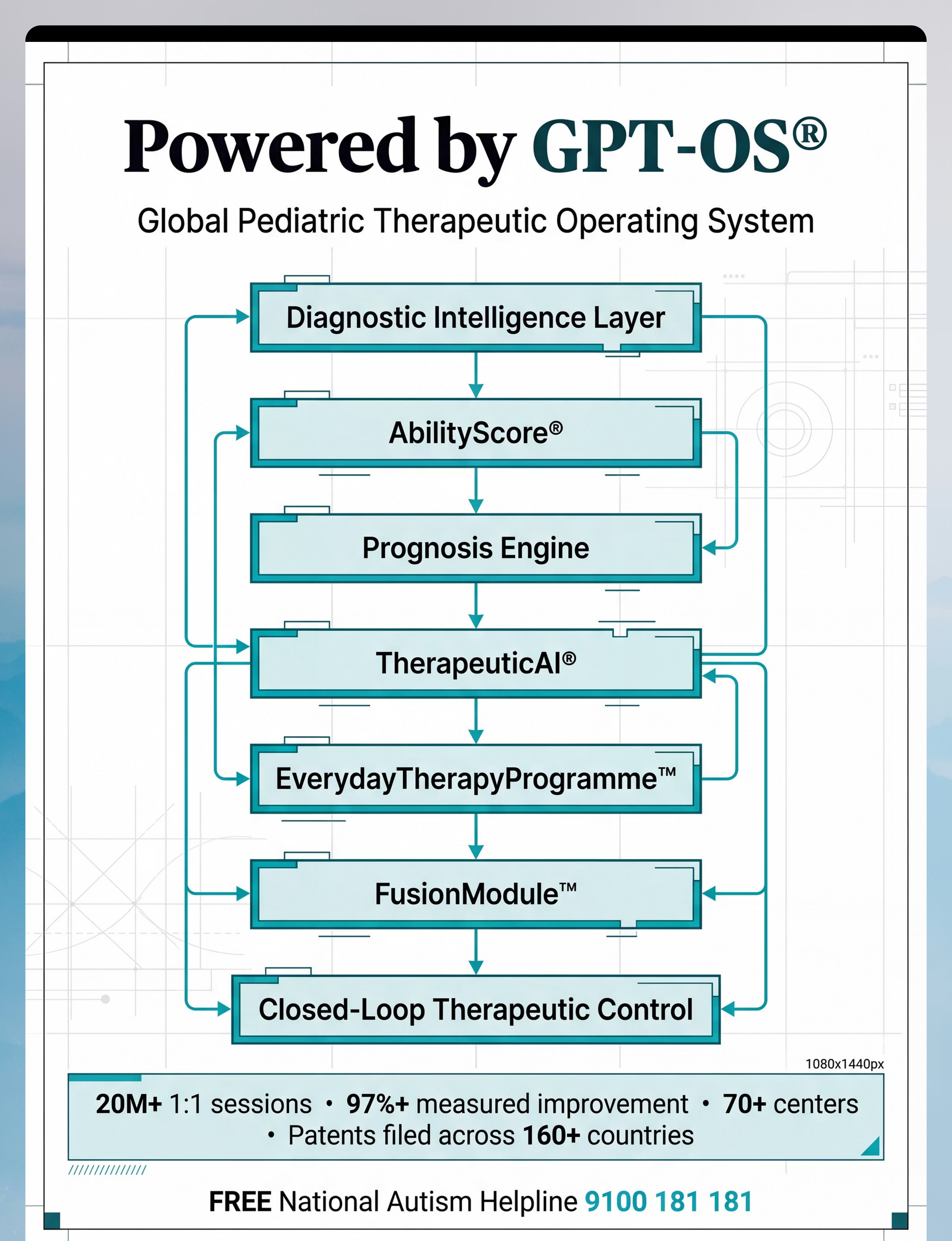
GPT-OS® Data Flow: Your session data → GPT-OS® TherapeuticAI® → Personalized recommendations for next session → AbilityScore® progress tracking → Progress report for your OT/therapist.

Every "Failed" Session Is Data. You Did Not Fail.
Troubleshooting Guide
❓ Child refused to touch any material
Why: Arousal state, sensory defensiveness threshold, or insufficient motivation. Next time: Start with YOU using the material first. Build fascination before expectation. Try proprioceptive heavy work first — it has the lowest refusal rate.
❓ Over-excited/dysregulated by swing
Why: Vestibular input over-activated arousal. Next time: Reduce rotation. Linear movement only. 50% shorter duration. Follow immediately with proprioceptive heavy work to re-organize.
❓ Weighted blanket immediately rejected
Why: Some children with tactile defensiveness feel weight as restraint. Alternative: Try weighted lap pad (smaller, more controllable). Or start with parent's hand resting on shoulder before any product.
❓ Session worked 3 minutes then fell apart
Why: Satiation, arousal shift, or environmental trigger. Response: 3 minutes of engagement is a WIN. Use it. Next session aim for 4 minutes. Progress is one minute at a time.
❓ Child seeks swing constantly and won't stop
Why: Under-responsive vestibular system or difficult transition out. Next time: Build a sensory diet with more scheduled vestibular input throughout the day. The seeking reduces when the need is met systematically.
❓ Sensory bin was engaging one week, now ignored
Why: Habituation — the material lost novelty. Next time: Change the filler. Add buried "treasure" (small figures). Add a new texture element. Novelty maintains therapeutic engagement.
"Session abandonment is data, not defeat. It tells you: arousal level, material match, environmental factors. Use it."
Adapt & Personalize — No Two Nervous Systems Are Identical
By Sensory Profile
Sensory Avoider (Over-Responsive)
Start farthest from material. Use visual calming first. Never place material without permission. Heavy work is safest starting point. Build in tiny increments.
Sensory Seeker (Under-Responsive)
Provide scheduled heavy input BEFORE sessions to prevent seeking overwhelm. Structure the seeking through channeled vestibular and proprioceptive activities.
Mixed Profile
System-by-system approach. Map each system separately — one protocol may not work across all materials.
Avoider + Seeker Simultaneously
Most common in autism. Use proprioceptive as universal starting point, then map individual material responses.
By Age
2–4 Years
5-minute maximum. Follow all child-initiated movements. No protocol demands — pure play-based exposure.
5–8 Years
10–15 minutes. Can begin named sensory language: "This is your calming tool."
9–12 Years
15–20 minutes. Can self-report what works. Begin self-advocacy language.
Challenging Day vs. Breakthrough Day
Challenging Day | Breakthrough Day | |
Reduce to 1 material only | Introduce a new material | |
Familiar, preferred input only | Increase duration | |
Remove all demands | Generalize to new setting | |
Heavy work as default | Try linking 2 materials in sequence |

Weeks 1–2: Tolerance, Not Mastery
Progress Arc: Phase 1
15%
Progress Phase
Investment phase — neural pathways forming beneath surface behavior
Weeks 1–2 may feel like nothing is changing. This is normal and expected. The behavioral change comes in Weeks 3–4. Right now, the nervous system is learning that this material is safe — and that is the most important work of all.
What "Progress" Actually Looks Like in Weeks 1–2
Material | Week 1–2 Win | |
Weighted products | Tolerates item on lap for 3+ minutes without removing | |
Vestibular swing | Approaches swing without distress; accepts 1 minute of slow swinging | |
Heavy work | Completes 1 full round of chosen activity with prompting | |
Chew tools | Holds chew necklace without putting in mouth — just holding is progress | |
Fidget | Keeps fidget in hand for 2+ minutes during seated activity | |
Auditory tools | Puts headphones on at home before they're needed in community | |
Visual calming | Watches calm-down jar for 30+ seconds with visual tracking | |
Tactile bin | Touches edge of bin with 1 finger voluntarily |
"If your child tolerates any material for 3 seconds longer than last week — that is real, measurable neurological progress. Celebrate it specifically."
Weeks 3–4: Neural Pathways Are Forming
Progress Arc: Phase 2
40%
Consolidation Phase
The signs most parents miss because they're looking for different things
Anticipation Emerging
Child anticipates the material — reaches for weighted blanket before you offer it. Sensory-seeking behaviors become slightly more organized and less frantic.
First Independent Self-Soothing
Child begins to self-soothe using the material independently — even once. Sleep quality measurably improves for children using weighted products at night.
Environmental Expansion
One new environment successfully navigated with auditory tools. Tactile bin tolerated for progressively longer duration without distress.
Spontaneous Material Access
Approaching the calm-down corner unprompted. Asking for the weighted blanket by name or gesture. Putting headphones on before you suggest them. Choosing fidget independently during homework.
"You may notice something in Week 3–4 that no research paper could predict: you're more confident too. Your instincts are calibrating."

Weeks 5–8: The Mastery Signs
Progress Arc: Phase 3
🏅 Mastery Zone
75%
Mastery Phase
Observable, measurable independence across multiple sensory systems
Mastery Criterion | What It Looks Like | |
Tool access independence | Child retrieves and uses at least 2 materials without adult prompting | |
Arousal awareness | Child shows behavioral signs of self-monitoring — slows down, seeks preferred tool when escalating | |
Environmental generalization | At least 1 challenging environment now tolerable with tools | |
Tolerance duration | Sensory challenge tolerance increased by 50%+ from Week 1 baseline | |
Meltdown frequency | Measurable reduction in frequency and/or intensity of sensory-triggered dysregulation | |
Routine integration | At least 3 sensory diet activities embedded in daily routine without prompting |
Mastery Unlocked — All 3 Required:✅ Independent tool access without prompting for 5 consecutive days · ✅ At least one new challenging environment navigated successfully · ✅ Parent rates sensory challenge impact on daily life reduced by 30%+

You Did This. Your Child Grew Because of Your Commitment.
"We didn't cure his sensory differences. We gave him tools. And suddenly, the world got bigger."
You started with a child who may have been fighting against every sensory experience in their day. You learned about 9 different materials, chose the ones that worked, built a sensory routine, survived the messy sessions, data-tracked the progress, and kept going when nothing seemed to be changing. That is not just parenting. That is clinical-grade commitment that thousands of paid professional hours could not replicate — because you were there, every day, in your home, with your child.
Your Specific Achievement
Sensory regulation in your home has measurably improved. Your child's nervous system has new tools. And you have new eyes — you can now read your child's sensory signals before they escalate.
Family Celebration Suggestion
Go to one place you couldn't go 8 weeks ago. With the headphones, the fidget, the regulation kit. That outing IS the celebration.
Journal Prompt
Take a photo of your child using their favorite sensory tool independently. Write one sentence about what that looked like 8 weeks ago. This is your evidence.

Trust Your Instincts — These Signs Mean Pause and Consult
Red Flags
When to Stop and Seek Help
If you observe any of the following signs, pause the protocol immediately and consult your child's OT or call the helpline: 9100 181 181
Sign | What to Do | |
Self-injurious behavior increasing despite sensory diet | Stop protocol. Teleconsult within 24 hours. | |
Sensory seeking escalating to unsafe levels (head-banging, jumping from heights) | Immediate OT assessment. Sensory diet needs urgent recalibration. | |
Child appears to be having seizure activity during vestibular input | STOP vestibular immediately. Medical evaluation before resuming. | |
Persistent sleep disruption worsening rather than improving | Review weighted product weight. Consult OT. | |
Meltdown frequency dramatically increasing week over week | Sensory diet may be under- or over-dosing. OT review needed. | |
Child showing new avoidances not present at baseline | May indicate over-stimulation. Sessions may be too intense. |
You Are Not Done — You Are on a Journey
The Progression Pathway
This technique is one powerful piece of a larger sensory processing series. Based on which materials worked best for your child, here is where to go next.

Tactile Materials Worked Best
Touch sensitivity still challenging? L-997: Tactile Sensitivity Deep Dive — the complete protocol for tactile defensiveness and discrimination.

Auditory Tools Had Most Impact
Sound sensitivity remains high? L-998: Auditory Sensitivity Deep Dive — targeted protocols for auditory over-responsiveness.

Vestibular Swing Was Transformative
Movement needs still high? L-999: Vestibular & Movement Needs — advanced protocols for vestibular-seeking profiles.

Weighted/Proprioceptive Most Effective
L-1000: Proprioceptive Input Deep Dive — maximizing deep pressure and heavy work across all environments.

One Technique. One Piece. One Magnificent Larger Plan.
This Technique's Position in the Full Map
Domain
A — Sensory Processing & Integration
Sub-domain
A1 — Sensory Modulation & Overall Regulation
Feeds Into
C (Emotional Regulation) · D (Behavior Management) · B (Communication Readiness) · F (Learning Readiness)
"A child whose sensory system is regulated can communicate more effectively. Can learn. Can manage emotions. Can engage socially. Sensory regulation is not a separate goal — it is the foundation of every other developmental domain."
From the Families. Not from a Brochure.
Family 1 | Hyderabad
Before: Our son (age 5) couldn't enter any public space without covering his ears and screaming within minutes. The school was threatening to ask us to withdraw him. We had stopped going anywhere as a family.
After (14 weeks): He now goes to the school assembly with noise-reducing headphones. He has a calm-down kit in his bag that he opens himself when he feels overwhelmed. Last month, we went to a birthday party — his first in two years. He wasn't perfect. But he was there.
"We didn't cure his sensory differences. We gave him tools. And suddenly, the world got bigger."
Family 2 | Mumbai
Before: Dressing our daughter took 45 minutes every school morning. Every shirt was wrong. Every sock was wrong. We were all exhausted and crying before 8am. The OT said she had tactile defensiveness.
After (8 weeks): We learned to use a seamless clothing site. We do 10 wall push-ups before getting dressed. We use the heavy backpack walk to school. Morning routine is now 15 minutes. We cry a lot less.
"Understanding why she reacted the way she did changed everything. We stopped fighting her nervous system and started working with it."
"The materials are the vehicle. The mechanism is parental understanding. When a parent knows why a child is seeking or avoiding, they stop interpreting behavior as defiance. That cognitive shift is as therapeutic as any weighted blanket." — Pinnacle OT, Senior Clinician
Note: Narratives are illustrative composites. Outcomes vary by child profile and intervention consistency.
The Questions Every Parent Has — Answered Directly
Q1: Which of the 9 materials should I start with?
Start with proprioceptive tools (heavy work, therapy putty). They are almost universally regulating across all sensory profiles — over-responsive, under-responsive, and seeking. Zero risk of over-stimulating. Begin there, observe your child's response, then add system-specific materials based on primary challenges.
Q2: My child's OT says weighted blanket, but my child hates it. What now?
Some children with tactile defensiveness experience weight as restraint. Try a weighted lap pad (smaller, less enclosing). Or start with proprioceptive heavy work first to build body awareness. The mechanism is deep pressure — multiple delivery routes exist.
Q3: How long before I see a difference?
Week 1–2: Tolerance building. Week 3–4: Consolidation signs emerge. Week 5–8: Measurable behavior changes. This is an 8–12 week investment, not a 3-day fix. The nervous system requires consistent, repeated input to recalibrate.
Q4: Can these materials be used at school?
Yes. Fidget tools, chew necklaces, noise-reducing headphones, and weighted lap pads are all school-appropriate. In India, RPWD Act 2016 supports reasonable accommodations for children with disabilities. Use the teacher template from Card 37 to communicate needs.
Q5: My child uses the swing for hours. Is that too much?
Intensive vestibular seeking often means the sensory system isn't getting enough input throughout the rest of the day. Build a sensory diet with scheduled heavy work, proprioceptive activities, and vestibular input across the day — so the seeking reduces because the need is met systematically.
Q6: Are these materials safe for children under 3?
Most yes, with supervision and age-appropriate versions: no weighted items over 1kg for under 3s; no small fidget parts (choking hazard); supervised sensory bin play only; food-grade chew tools with size-check. Always consult your pediatrician and OT before introducing any equipment for children under 2.
Q7: My child has severe autism and doesn't engage with any material.
Begin with the most passive input: proprioceptive input during daily activities (firm hugs, massage, joint compression) and heavy work during natural routines. Don't introduce products until behavioral engagement is established through relationship-first approaches. Professional sensory integration assessment is highly recommended.
Q8: I bought everything on this list and nothing is working.
Products don't work without a sensory diet — scheduled input throughout the day. Individual material response depends on sensory profile. A child who is over-responsive may need less input, not more. Book a sensory profile assessment with a Pinnacle OT: call 9100 181 181.
Preview of 9 materials that help with sensory overall Therapy Material
Below is a visual preview of 9 materials that help with sensory overall therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

You Have Everything You Need to Begin Today.
🚀 Start Your Child's Sensory Toolkit Today
Begin with proprioceptive heavy work — no equipment needed. Open the GPT-OS® session launcher and record your first session data today.
📞 Book an OT Assessment
Get a professional sensory profile for your child. Know exactly which materials to prioritize for your child's specific sensory pattern.
Or call FREE: 9100 181 181
🗺️ Explore the Next Technique
Continue the sensory series. L-997: Tactile Sensitivity awaits — and you already own the materials to begin.
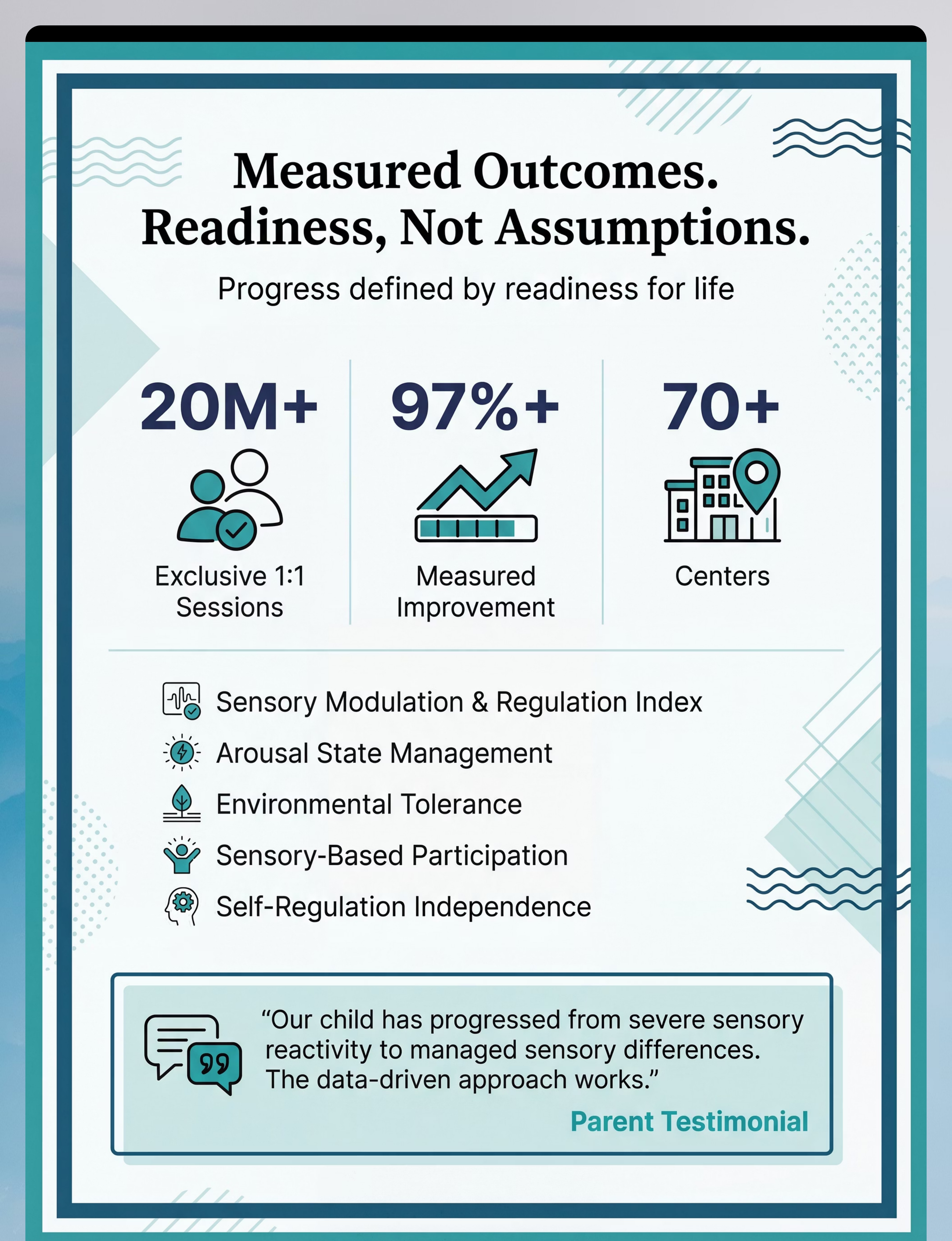
Validated by the Pinnacle Blooms Consortium: OT · SLP · ABA · SpEd · NeuroDev · 20M+ Sessions · 97%+ Outcomes
FREE National Autism Helpline | 9100 181 181 | 16+ languages | 24×7