9 Materials That Help With Sensory Fine Motor
F-616 | Pinnacle Blooms Network® — When hands need to feel in order to learn how to move. Evidence-based guidance for families, caregivers, and therapists.
OTSLPABASpEdNeuroDev
CRO

"She stared at her fingers the whole time. Every. Single. Button."
It's 7:43 AM. School bus in four minutes. Your daughter is hunched over her shirt, forehead furrowed, eyes locked on her fingers trying to push a button through its hole. She squeezes too hard. The button pops back out. She stares harder — as if looking away for one second would make her hands forget what they're doing. You reach over. She pulls away. She needs to see her hands to make her hands work.
Her occupational therapist called it "sensory fine motor dysfunction." But what you called it this morning was Tuesday.
You are not failing. Your child's hands need to feel in order to learn how to move. That is a neurological truth — and it is trainable.
Technique F-616Fine Motor DevelopmentBuilt by Mothers. Engineered as a System.
You Are Not Alone in This
When your child needs to watch their hands just to button a shirt, grip a crayon, or pick up a raisin — you're seeing a specific and documented neurological pattern. You are among millions of families navigating exactly this.
80%
Sensory Impact
of children diagnosed with autism experience sensory processing difficulties that directly affect fine motor function. PRISMA Systematic Review, 2024 (PMC11506176)
1 in 6
Global Prevalence
children globally show sensory processing differences significant enough to affect daily activities including hand use and manipulation. STAR Institute, 2023
21M+
Sessions Documented
therapy sessions delivered by Pinnacle Blooms Network® document the sensory-motor connection — the most rigorously observed pattern in Indian pediatric OT. GPT-OS® Real-World Evidence Database

The Neuroscience of "Hands That Can't Feel"
Understanding what's happening in your child's brain is the first step to helping their hands learn to work.
The Tactile Pathway
When your child's fingertips touch a button, receptors in the skin fire signals upward — through the spinal cord, through the brainstem, to the thalamus, and finally to the somatosensory cortex. This is where the brain decides: "What am I touching? How hard? What shape?"
What's Different in Sensory Fine Motor Dysfunction
For some children, this pathway exists — but the brain's processing of those signals is inefficient. The information arrives distorted, delayed, or muted. The brain compensates: it turns to the eyes to do what touch should be doing automatically.
The Proprioceptive System
Receptors in muscles and joints tell the brain: "How hard am I gripping? Where are my fingers in space?" When this system is under-responsive, children grip too hard (can't feel when "enough" is enough) or too soft (objects slip away unnoticed).
The Critical Insight
This is not a behavior problem. This is not laziness. This is a wiring difference — specifically, how efficiently the brain processes and integrates tactile and proprioceptive input. Neural pathways are plastic. They can be trained.
"Your child isn't fighting the button. Their brain is missing the sensory map that would make the button findable by touch alone." — Pinnacle Blooms OT Consortium

The Developmental Map: Where Your Child Is, Where They're Going
Sensory fine motor development follows a predictable arc. Knowing where your child sits on this map helps you intervene at exactly the right moment — when neural plasticity returns are highest.
0–18 Months
Tactile exploration through mouthing, grasping, banging. Proprioceptive system developing through whole-body movement.
18 Months–3 Years
Refined grasp development. Child begins using tools (spoon, crayon). Tactile discrimination emerging — identifying objects by feel.
3–5 Years — Typical Emergence Zone
By age 4–5, most children perform simple fine motor tasks WITHOUT constant visual monitoring. Tactile feedback should guide manipulation.
🔴 Challenge Zone — Maximum Intervention Impact
Children with sensory fine motor differences remain visually dependent beyond typical age. They grip inconsistently. They avoid or seek intense tactile input. This is where F-616 intervenes.
5–8 Years — With Intervention
Sensory-guided fine motor develops. Visual dependence reduces. Grip modulation improves. Participation in school tasks, self-care, and play expands dramatically.
8–10 Years — Automaticity Target
Fine motor performed without conscious monitoring. Writing, fastening, tool use become background processes, freeing attention for content and connection.

Clinically Validated. Home-Applicable. Parent-Proven.
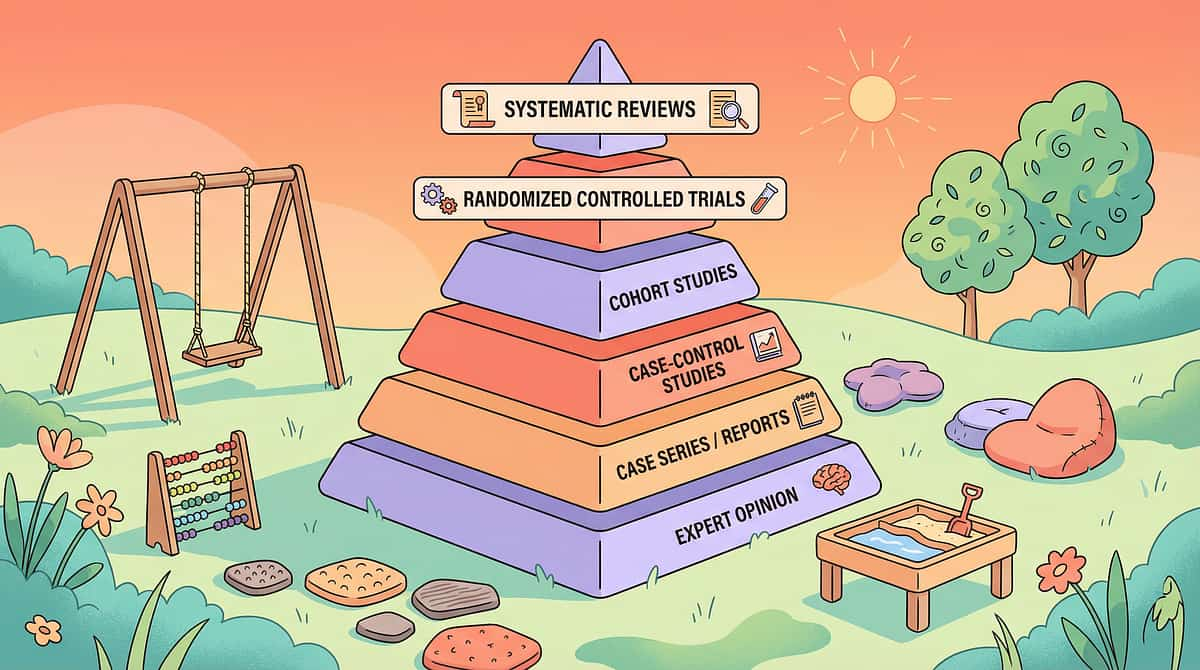
The intervention approach behind F-616 is not experimental. It is grounded in systematic reviews, randomized controlled trials, and over 20 million documented therapy sessions.
PRISMA Systematic Review (2024)
16 articles, 2013–2023 | PMC11506176 — "Sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD, with demonstrated improvements in sensory processing, fine motor skills, social participation, and adaptive behavior."
Meta-Analysis — World J Clin Cases (2024)
24 studies reviewed | PMC10955541 — "Sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and gross/fine motor skills — with significant effect sizes across outcome domains."
Indian RCT — Padmanabha et al. (2019)
Indian Journal of Pediatrics — "Home-based sensory interventions demonstrated significant outcomes in Indian pediatric populations — validating the clinical approach for family-administered protocols." DOI: 10.1007/s12098-018-2747-4
"This technique is supported by systematic review evidence. It is internationally validated, India-tested, and designed for your home."

Sensory Fine Motor Integration — The Technique
F-616Ages 3–1015–30 min sessions4–5× weekly
Sensory Fine Motor Integration is an evidence-based occupational therapy approach that combines tactile (touch) and proprioceptive (deep pressure/force/position) sensory input with deliberate fine motor practice. Rather than treating the hands as purely mechanical tools, this approach recognizes that skilled hand function depends on the brain accurately receiving and interpreting sensory information from the fingers, joints, and muscles.
When a child cannot feel what their hands are doing with precision — whether due to under-responsiveness, over-responsiveness, or discrimination difficulty — fine motor control suffers despite adequate strength. The intervention provides enhanced sensory experiences while practicing fine motor tasks, training the brain to use sensory input for motor guidance.
This Technique Crosses Every Therapy Boundary
The brain doesn't organize by therapy type. Sensory fine motor challenges are observed, addressed, and monitored by every discipline in the Pinnacle Consortium — each through a specialized lens.
🧩 Occupational Therapy (Primary Lead)
OTs evaluate the full sensory profile — tactile discrimination, proprioceptive processing, sensory seeking vs. avoiding patterns — and design individualized sensory-motor programs. The 9 materials on this page are core OT tools. Ayres Sensory Integration® | AOTA Sensory Processing Framework
🗣️ Speech-Language Pathology
Oral motor parallels sensory fine motor. SLPs working on feeding, articulation, and oral sensory tolerance apply the same tactile discrimination principles to the mouth and face. Coordinated OT-SLP planning addresses children with both hand and oral sensory differences.
📊 Applied Behavior Analysis (ABA/BCBA)
ABA practitioners design reinforcement schedules that make sensory fine motor practice rewarding and repeatable. Token economies, behavioral momentum, and shaping procedures all apply here. BACB Ethical Guidelines | NCAEP EBP (2020)
📚 Special Education
SpEd teachers integrate sensory fine motor supports into classroom routines — adapted writing tools, textured grips, sensory warm-ups before academic tasks, and accommodation plans. They observe carryover from home-based work and adjust expectations accordingly.
"The sensory-motor connection doesn't belong to any one profession. It belongs to the child." — Pinnacle Blooms Multi-Disciplinary Consortium

Precision Intervention: What Exactly Gets Better
Challenge Now | Intermediate Indicator | Target Outcome |
Must watch hands constantly | Occasional visual check only | Independent tactile monitoring |
Grips too hard / breaks things | Notices when grip is excessive | Auto-calibrated grip modulation |
Drops objects unexpectedly | Improved retention, occasional drops | Reliable, appropriate grip |
Avoids messy/textured materials | Tolerates with support | Comfortable engagement |
Weak fine motor endurance | Improved duration before fatigue | Age-appropriate sustained fine motor |

The 9 Materials That Make Hands Learn to Feel
These are not toys. These are clinical tools graded for therapeutic use, validated by the Pinnacle OT Consortium across 20M+ therapy sessions. Each one delivers specific sensory input — tactile, proprioceptive, or combined — while requiring fine motor practice. Start with 2–3 materials. Build your home sensory toolkit progressively.
1. Therapy Putty & Resistive Doughs
Tactile / Proprioceptive Input. Resistance calibrates force-sensing. Hidden object excavation trains precision pinch. ₹300–800 | DIY: white glue + liquid starch.
2. Sensory Bins with Varied Textures
Tactile Exploration / Sensory Play. Rice, kinetic sand, water beads — each texture trains a different aspect of tactile processing. ₹200–600 | DIY: dal box + dry rice.
3. Vibrating Pens & Massagers
Vibration / Tactile Alerting. Activates touch receptors, priming hands for precise action before or during fine motor tasks. ₹400–1,200 | DIY: electric toothbrush handle.
4. Textured Pencil Grips
Writing & Fine Motor Tools. Ridged, bumpy surfaces give fingers ongoing position information — reducing visual dependence during writing. ₹100–400 | DIY: rubber band on pencil.
5. Weighted Wrist Cuffs
Proprioceptive / Weighted Supports. Added weight sends strong proprioceptive signals — the brain tracks limb position more precisely. ₹300–900 | DIY: rice-filled fabric pouch.
6. Tactile Discrimination Games
Sensory Discrimination / Cognitive-Motor. Mystery bags, texture matching — directly training the foundational ability for all skilled hand function. ₹150–500 | DIY: opaque bag + 5 objects.
7. Finger Paints & Messy Play
Messy Play / Tactile Tolerance. Hands learn to work THROUGH sensory challenge. Tolerance transfers to daily life textures. ₹100–350 | DIY: cornstarch + water = oobleck.
8. Squeeze & Pinch Tools
Resistance / Proprioceptive Play. Spray bottles, clothespins, tongs — calibrate "how hard is hard enough." ₹100–400 | DIY: spray bottle (₹50) + water.
9. Sensory Fidgets & Manipulation Toys
Sensory Self-Regulation / Portable Input. Dexterity improves as a byproduct of sensory regulation. ₹100–500 | DIY: smooth stone + rough stone + pompom.
Every Technique. Every Budget. Every Home.
"Effective sensory fine motor intervention does not require expensive equipment. It requires the right understanding of WHY each material works — and that knowledge costs nothing." — WHO Nurturing Care Framework Principle | Pinnacle OT Consortium
Material | Clinical Version | Home Substitute | Why It Works the Same |
Therapy Putty | ₹300–800 | White glue + liquid starch mixture | Same resistance principle; graded by starch ratio |
Sensory Bin | ₹200–600 | Plastic dal box + dry rice/lentils | Rice provides identical tactile discrimination training |
Vibrating Tool | ₹400–1,200 | Electric toothbrush handle on palm | Same vibration mechanism activating touch receptors |
Textured Grip | ₹100–400 | Rubber band wrapped around pencil | Contact texture provides same positional feedback |
Weighted Cuff | ₹300–900 | Rice-filled fabric pouch tied at wrist | Same proprioceptive deep pressure mechanism |
Tactile Game | ₹150–500 | Any opaque bag + household objects | Identical training of tactile discrimination pathways |
Messy Play | ₹100–350 | Cornstarch + water (oobleck) | Unique pressure-responsive texture; superior sensory complexity |
Squeeze Tool | ₹100–400 | Spray bottle (₹50) + water | Identical proprioceptive squeeze training |
Fidget | ₹100–500 | Smooth stone + rough stone + pompom | Multi-texture variety; complete sensory-motor training |

Read This Before Every Session
Safety is not a formality — it is the foundation of effective sensory intervention. Review this card before each session, especially in the first four weeks.
🔴 DO NOT PROCEED IF:
Child is in active meltdown or significantly dysregulated • Open skin wounds or eczema flare on hands • Joint hypermobility or hypotonia requiring OT clearance for weighted activities • Severe distress (self-injury, aggression) to tactile input in the past week • Child is ill, febrile, or in post-meltdown recovery (within 2 hours)
🟡 PROCEED WITH MODIFICATION:
Mildly tired: shorten to 5–10 minutes • Tactile defensive day: start with deep pressure only • New material: introduce only during calm moments • Water beads: choking hazard under age 4 — do not use unsupervised • Small hidden objects (beads, coins): choking hazard under age 3
🟢 OPTIMAL CONDITIONS:
Child is calm, alert, and recently fed ✅ Environment prepared — materials out, distractions removed ✅ Parent is regulated with 15–30 uninterrupted minutes ✅ Familiar materials first; new materials at end of session ✅ Child has agreed to engage (invitation, not command) ✅

The Environment Is Part of the Therapy
How you set up your space directly impacts your child's ability to engage, regulate, and benefit from sensory fine motor intervention. A prepared environment reduces sensory overload before the session even begins.
Child Position
Seated at low table, feet flat on floor or stool. Hips, knees, ankles at 90°. Table at elbow height. Good postural base = better fine motor performance.
Parent Position
Seated to child's right (or left if left-handed). Close but not hovering. Within arm's reach to model, not to correct.
Primary Material
On tray directly in front of child. One material at a time. Others out of sight. Reinforcement within parent's reach, NOT visible to child until earned.
Lighting & Sound
Natural light preferred. Warm artificial light acceptable. Avoid harsh fluorescent (increases sensory load). Quiet or gentle background hum only.
Cleanup Station
Wet wipes and small towel visible but not prominent. Child knowing cleanup is available reduces tactile-defensive anxiety about mess.
Remove from Space
❌ All screens (off, face down) ❌ Other toys ❌ Other children initially ❌ Strong smells ❌ Loud background noise
60-Second Pre-Session Readiness Assessment
The best therapy session starts with the right child state. Take 60 seconds right now. This matters more than which material you use.
Basic Needs Met
Child is fed (not hungry) and not thirsty.
Calm State
Not in post-meltdown window (≥2 hours since last major dysregulation).
Alert
Not drowsy, not hyper-aroused — in the optimal arousal window.
Not Ill
No fever, no pain, no post-illness fatigue.
Smooth Transition
Minimal resistance getting to the activity — child came willingly.
Parent Regulated
You are calm and have uninterrupted time for the session.
🟢 5–6 Ticked → GO
Full session as planned.
🟡 3–4 Ticked → MODIFY
Shorten to 10 minutes. Familiar material only. Skip new introductions.
🔴 0–2 Ticked → POSTPONE
This is not failure. It is data. A postponed session is a professionally sound decision.
"Pushing a session when your child is dysregulated doesn't build the skill — it builds a negative association with the material." — Pinnacle BCBA Consortium

Step 1: The Invitation
Step 1 of 6
Script option A:"Hey, I have something interesting for you. Want to see?" — Hold material behind your back or in closed hands. Reveal slowly. Let curiosity do the work.
Script option B (structured choice):"Time for hands work. Pick: [show two options in each hand]. Which one first?" — Choice creates agency. Agency creates buy-in.
Body Language Guidance
Sit at child's level — never stand over. Relaxed shoulders, soft face, no urgency. Present material on open palm — offering, not imposing. Match your energy to theirs: calm child → quiet invitation; activated child → slightly animated.
Timing
30–60 seconds maximum for invitation phase.
✅ Acceptance Cues
Child reaches toward material • Eye contact with material • Body leans forward • Any positive vocalization • Smile or brightened expression
🔄 Resistance Cues — What to Do
Child turns away → Wait 10–15 seconds, try alternate material. Child says no → Respect it: "Okay, I'll put it here. You can touch it whenever." Meltdown → Move to postpone protocol (Card 13).

Step 2: The Engagement
Step 2 of 6
The child is exploring the material. Your role shifts from inviter to co-explorer. You're providing sensory-motor context without directing. The exploration IS the therapy.
Therapy Putty
"See what it does when you push it..." Model squeezing in your own hand first. Let child see. Offer putty. "Can you make it flat? Can you make it into a ball?"
Sensory Bin
"I wonder what's hiding in here..." Let hands explore before mentioning hidden objects. Discovery first — always.
Vibrating Tool
"This one does something interesting on your hand..." Try on YOUR hand first, visibly. Then offer. Never introduce vibration directly without modeling.
Mystery Bag / Tactile Game
"Close your eyes. Can your hands be detectives?" Gamify immediately. Detectives don't look — that's the whole point.
Step 3: The Therapeutic Action
Step 3 of 6
Every material has one therapeutic action — the specific movement or sensory experience that activates the target neural pathway. Below are the 9 therapeutic actions, one per material.
1 — Therapy Putty
Squeeze-pull-pinch cycle with eyes occasionally closed. Squeeze full fist (5 sec) → Pull apart → Pinch with index + thumb → Bury small object → Find it with fingers. 5–8 min. Progress to eyes-closed excavation.
2 — Sensory Bin
Hide-and-find with texture progression. Start with hands running through base material (30–60 sec), then: "Find the circle. Find everything smooth." Sort by texture category. 5–10 min. Resist letting child use eyes.
3 — Vibrating Tool
Pre-task vibration warm-up + during-task feedback. 30–45 sec on palm and fingertips BEFORE the fine motor task. Then immediately perform the task. Compare performance with and without vibration.
4 — Textured Grip
Sustained tool use with tactile monitoring, not visual monitoring. Cover the child's writing hand with a small cloth every few minutes — forcing reliance on grip texture, not vision. Gradually increase "covered" duration.
5 — Weighted Cuff
Fine motor task with added proprioceptive input. Start 50–100g on dominant wrist. Perform bead threading, button practice, stacking, or drawing. Observe grip modulation change. Remove and observe carryover effect.
6 — Tactile Discrimination Game
Eyes-closed identification, progressing to subtle differences. 5 objects in bag → identify each without looking. Progress to same objects + 2 new → then same category with subtle differences (smooth vs. rough coin).
7 — Messy Play
Graded texture exposure with fine motor task embedded. Dry → damp → wet/sticky. At each level: draw letters, find objects, make patterns — fine motor work IN the texture, not alongside it.
8 — Squeeze Tools
Functional squeeze-pinch with graded resistance. Water plants with spray bottle → hang drawings with clothespins → transfer with tongs. Make it purposeful — watering a real plant, hanging real artwork.
9 — Fidget
Pre-task sensory priming + movement-break integration. 2–3 min fidget before task (alerting). 1–2 min break every 8–10 min during sustained work. End of session: quiet fidget for regulation cool-down.

Step 4: Repeat & Vary
Step 4 of 6
"Three engaged repetitions are more therapeutically valuable than ten forced ones." Repetition drives neural pathway formation — but only when the child is actively processing the sensory input.
Material | Target Reps Per Session | Rest Between Reps |
Therapy Putty | 5–8 squeeze-pull cycles | 10 sec rest between cycles |
Sensory Bin | 2–3 find-and-sort rounds | Free explore between rounds |
Vibration warm-up | 1–2 warm-up rounds | Before each new task |
Tactile Discrimination | 3–5 identification attempts | Praise between each |
Weighted Cuff | 1 sustained activity | Remove and observe carryover |
Messy Play | 1 texture level per session | Progress texture level weekly |
Squeeze Tools | 10–15 squeezes per tool | Natural movement rest |
Variation Options to Maintain Engagement
- Change the hidden object (same bin, new hunt → novelty within structure)
- Change the grip texture (different putty resistance level → progressive challenge)
- Change the task (write letters → draw shapes → trace pictures, same textured grip)
- Change the timing (race the timer → slow motion → pause game)
- Change the body position (table → floor → standing at wall)

Step 5: Reinforce & Celebrate
Step 5 of 6
Timing matters more than magnitude. Immediate, specific, enthusiastic reinforcement within 0–3 seconds of the desired sensory-motor behavior is what drives repetition. Dopamine release tied to success signals is basic neuroscience.
"YES! Your fingers found it without looking — that's your hands learning to feel!"
"Did you feel how the putty pushed back? Your hands are getting smarter!"
"Look — you didn't even look at your fingers that time. Your hands knew!"
"I saw you squeeze just right! Not too hard, not too soft!"
Social Reinforcers
Specific praise, high five, thumbs up, brief dance celebration. Primary and most powerful for most children.
Token Reinforcers
Sticker on chart, point system, stamp on hand. Builds toward larger reward over multiple sessions.
Activity Reinforcers
2 minutes of preferred activity following therapeutic task. Natural reinforcers: "You found all 5! You decide what goes in the bin tomorrow."
"Celebrate the attempt, not just the success." The child who put their hand in the sensory bin for 2 seconds despite hating it — that deserves specific, named celebration.

Step 6: The Cool-Down
Step 6 of 6
No session ends abruptly. The nervous system needs a transition signal — especially when it has been processing intense sensory input. An abrupt ending can trigger dysregulation. A 2–3 minute cool-down protects your child's regulation and sets up the next session positively.
Transition Warning Script
"Two more times, then all done." — Use exact number. Not "almost done." Children with sensory processing differences need precise transitions.
"One more. Then we put it away together." — "Together" is inclusion and reduces resistance.
Material Put-Away Ritual
Child participates in cleaning up materials. This is NOT a chore — it is a sensory transition activity and a self-regulation building moment: "Let's put everything back in its home."
Cool-Down Activities (Choose One)
- Deep pressure hands: Child presses palms flat on table, pushes down firmly 5 sec × 3 reps. Proprioceptive calming.
- Hand massage: Parent firmly squeezes child's hands — each finger, palm, back of hand.
- Wash hands ritual: Warm water for 30 seconds. Familiar routine signals session end.
- Putty squeeze-out: 5 slow deep squeezes, then putty in container. Completion ritual.
If Child Resists Ending
Don't escalate. Say: "I know, it's fun. One more minute." Set timer. Offer: "Tomorrow we'll start with this one."
Capture the Data: Right Now
60 seconds of data now. Hours of clarity later. Your observations immediately after a session are the most accurate you'll have. Don't wait until bedtime. Three data points. This is how we know the therapy is working.
Data Point 1 — Engagement Duration
"How many minutes did [child] actively engage with the material?" Target: working toward 10+ minutes of quality engagement.
Data Point 2 — Visual Dependence Score
0 = Constant visual monitoring (baseline) | 1 = Frequent checking | 2 = Occasional checking | 3 = Minimal or no checking (target). "How often did [child] look at hands when not needed?"
Data Point 3 — Sensory Tolerance Rating
1 = Refused / significant distress | 2 = Tolerated with support | 3 = Engaged willingly | 4 = Enthusiastic engagement / seeking the material.
Session Abandonment Is Not Failure. It Is Data.
Most sensory fine motor sessions — especially early ones — don't go perfectly. This is expected and documented. Here are the 7 most common difficulties with specific solutions.
Child completely refused to touch the material
Why: Normal for tactile-defensive children on first exposure. Next time: Model touching the material extensively before inviting child. Leave material out in the room for 2–3 days (passive exposure). Start with dry rice bin before putty.
Child touched briefly then immediately walked away
Why: Sensory threshold reached quickly — still successful engagement. Next time: Reduce session duration. Celebrate the brief engagement. Extend by 10–15 seconds each day. Brief + positive > long + negative.
Child used too much force and damaged the material
Why: Proprioceptive seeking — this is diagnostic information. Next time: Provide firmer putty resistance. Add weighted cuff. Introduce more-resistance squeeze tools. Contact Pinnacle — seeking may need specific sensory diet design. 📞9100 181 181
Child kept looking at hands despite encouragement
Why: Visual monitoring is still the primary feedback system — this is exactly what the technique addresses over time. Next time: This is the baseline. Continue. Track Visual Dependence Score. Reduction is gradual — weeks, not days.
Child became distressed and the session escalated
Why: Sensory input exceeded tolerance threshold, or timing was wrong. Next time: Review readiness check. Start with ONLY the most familiar, preferred sensory material. Contact Pinnacle if distress is severe or recurring.
Child engaged beautifully but shows no carryover to real life
Why: Carryover from therapeutic context to functional context takes 3–6 weeks. The pathway is building — it just hasn't generalized yet. Next time: Increase frequency. Create functional application opportunities (use textured grip for homework, not just session).
Parent lost patience and the session ended badly
Why: The most common and least discussed reality. Parents are humans. Next time: Shorter session. Script ready before starting. "Good enough" session > no session. Pinnacle has parent support resources at 9100 181 181.

No Two Children Are Identical. Neither Is Their Therapy.
F-616 is a flexible protocol, not a rigid script. Adapt the difficulty, materials, and intensity to match your child's sensory profile, age, and current developmental zone.
EASIER — Early Stage / Overwhelmed
Only dry textures (rice, beans) • No hidden objects initially — just exploration • 5 minutes maximum • Parent models extensively before child participation • Weight cuff at minimum (50g) • Only familiar, previously tolerated materials
CORE — Standard Protocol
Mix of dry and wet textures introduced progressively • Hidden objects with tactile identification • 15–20 minute sessions • Child leads with parent supporting • Medium putty resistance • Standard weighted cuff (100–150g)
HARDER — Progress / Sensory Seeking
Eyes-closed challenges for all tactile activities • Subtle difference discrimination (coins of different sizes) • Extended sessions (25–30 min) • Firm therapy putty • Weighted cuff 150–200g • Combine materials in same session
Sensory Profile Adaptations
Under-Responsive / Seeker: Firmer putty, higher resistance, add vibration before ALL tasks, heavier cuffs, more intense textures, longer sessions tolerated and beneficial.
Over-Responsive / Avoider: Start with deep pressure ONLY, graded exposure (dry → slightly textured → wet), child controls exposure level, shorter sessions, end before distress point.
Discrimination Difficulty: Prioritize tactile discrimination games above all others, eyes-closed challenges as soon as any tolerance is established, verbal description required: "What does it feel like? Rough or smooth? Round or flat?"
Age Adaptations
Ages 3–5: Shorter sessions (10–15 min), more playful framing, simpler hidden objects, parent co-participation throughout.
Ages 6–8: Introduce functional connection: "Same grip as your pencil at school."
Ages 8–10: Self-monitoring encouraged: "Did you need to look? Try again without looking."

Week 1–2: Building Trust, Not Mastery
Act IV: Progress
✅ What You WILL Likely See
Increased willingness to approach material on 2nd/3rd exposure • Reduced resistance (child stops running away, even if engagement is brief) • Parent increasing confidence with the protocol • First data patterns emerging (you'll see your baseline numbers) • Child beginning to anticipate the activity — this is massive
⚠️ What You Will NOT See Yet
Dramatic reduction in visual dependence during real-life tasks • Consistent grip modulation across contexts • Child willingly touching previously avoided textures in daily life • Carryover to school or other settings
"If your child tolerates sensory material for 3 seconds longer than last week — that is documented, measurable, clinically meaningful progress."

Week 3–4: The Neural Pathways Are Beginning to Stabilize
40% Progress
In weeks 3–4, synaptic strengthening is measurably underway. You can't see it — but the OT measuring your child's data can. Here are the consolidation indicators to look for.
🔵 Child Anticipates the Activity
Reaches for the sensory bin without being prompted, or asks for the putty. The material has been linked to positive sensory experience in their neural map.
🔵 Engagement Duration Increases
Sessions that were 3 minutes are now 8–10 minutes. The child's sensory tolerance window has widened.
🔵 Tactile Tolerance Expands Slightly
The child who previously refused wet textures may now briefly touch wet sand. Not mastery — a beginning. Document it.
🔵 First Generalization Seed
You may notice your child using a slightly different grip on a spoon, or staring at their hands slightly less when buttoning. This is the therapy working.
🔵 Parent-Child Dynamic Shifts
You're reading your child's sensory cues more accurately. You're adjusting the session without thinking about it. This is co-regulation developing.

Week 5–8: Mastery Is Not Perfection. It Is Automatic.
75% Progress
Mastery criteria for F-616 are specific, observable, and measurable. Here is exactly what you are looking for — and what it means when you find it.
Mastery Indicator 1
Tactile discrimination task (mystery bag, 5–7 objects) with ≥80% accuracy across 3 consecutive sessions. Objects identified by touch WITHOUT visual confirmation.
Mastery Indicator 2
Grip modulation during prescribed fine motor task shows no more than 2 instances of breaking material or dropping objects across a 10-minute session.
Mastery Indicator 3
Child voluntarily engages with a previously avoided texture without significant distress across 3+ consecutive exposures — voluntary, unaided approach.
Mastery Indicator 4
Visual Dependence Score reaches consistent 2–3 during session AND at least one parent observation of reduced visual monitoring during a daily life task (buttoning, eating, writing).

You Did This.
Five to eight weeks ago, you watched your child stare at their fingers just to button a shirt. You felt helpless in the gap between what you saw and what you could do about it.
You did something about it. You set up a sensory bin on the kitchen table. You introduced therapy putty at breakfast. You played mystery bag before homework. You did the eyes-closed challenge after school. You recorded the data. You modified the approach when it wasn't working. You came back the next day.
Your child's hands are different now. Not perfect — different. More aware. More guided by feeling. More able. That difference was not random. It was yours.
✅ Achievement Summary
Sensory fine motor tolerance established for multiple materials • Tactile discrimination measurably improved • Visual dependence during manipulation reduced • Grip modulation showing consistent improvement • Parent-child sensory co-regulation: active and strengthening
🎉 Family Celebration Suggestion
Tonight: tell your child's story at dinner. Specifically. "Remember when you couldn't find the button without staring at your fingers? Look at you now." Name the specific change. Let them feel it.
Trust Your Instincts. If Something Feels Wrong, Pause and Ask.
Home-based practice is powerful. But some patterns warrant professional consultation — and recognizing them is part of being a skilled intervention partner for your child.
🚨 Extreme Tactile Reactions Persisting Beyond 4–6 Weeks
Child's distress response is NOT reducing over 4–6 weeks of consistent graduated exposure. Extreme reactions (severe crying, self-injury, aggression) at any sensory input. → Requires formal OT sensory processing evaluation.
🚨 Self-Injurious Sensory Seeking
Child seeking input to the point of injuring themselves (biting hands, head-banging for proprioception, scratching skin). → Requires immediate professional assessment.
🚨 Regression in Other Developmental Domains
Regression in communication, social engagement, or self-care skills while implementing this technique — may indicate sensory overload from the home program. → Needs clinical review.
🚨 Fine Motor Declining Despite 6–8 Weeks of Practice
Not plateau — decline. Performance getting measurably worse. → May indicate a different diagnosis requiring evaluation (DCD, neurological, vision).
🚨 Significant Sensory-Related School Refusal
Child refusing school or social activities primarily due to sensory fine motor anxieties. → Requires multi-disciplinary assessment.
You Are Not at a Destination. You Are on a Trajectory.
F-616 is one carefully positioned step in your child's fine motor development arc. Understanding what comes before and after helps you sequence intervention with confidence.
Path A — Bilateral Coordination
📍F-617 — Coordinating both hands together. Best for children who have established single-hand sensory awareness and are ready for two-hand coordination challenges.
Path B — Visual Motor Integration
📍F-618 — Integrating hand movement with visual tracking for handwriting, drawing, cutting. Best for children who have reduced visual dependence during tactile tasks.
Path C — Advanced Tactile Discrimination
📍F-619 — Distinguishing subtle texture and shape differences by touch alone. Best for children who have mastered basic tactile discrimination.
More Tools for the Sensory Fine Motor Journey
Domain: Fine Motor Development | Sensory-Motor Integration Cluster. If you have therapy putty and a sensory bin from F-616, you already own the primary materials for F-614, F-617, and A-207. Your toolkit grows efficiently.

F-614: Hand Strengthening Activities
Prerequisite. Materials: Therapy putty, resistance bands, squeeze toys. Build the physical foundation for sensory-motor work.

F-615: Tool Use Development
Core (before F-616). Materials: Scissors, tongs, utensils. Learning to use fine motor tools before adding sensory complexity.

F-617: Bilateral Coordination
Next Level (after F-616). Materials: Beading, bilateral drawing tasks. Coordinating both hands — requires established single-hand awareness.

F-618: Visual Motor Integration
Advanced (after F-616). Materials: Mazes, cutting activities, ball-tracking. Eye-hand coordination for handwriting and academic tasks.
One Technique. One Piece of a 12-Domain Plan.
F-616 sits within Domain F (Fine Motor Development) of GPT-OS® — which monitors your child's development across all 12 domains simultaneously. The sensory fine motor work you're doing connects outward to sensory processing, self-care, and academic readiness.
From the Families Who Walked This Path Before You
Act V: Community
Arjun, 6 Years, Hyderabad
Before: Arjun would snap every crayon within minutes. His preschool noted "destructive behavior." His OT observed he couldn't feel the force he was applying. He wasn't being aggressive — he was seeking proprioceptive feedback.
Intervention: Firm therapy putty + weighted cuff during writing. 8 weeks, daily 15-minute home sessions.
After (7 weeks): Crayons intact for the first time. Writing with two pressure levels. Mother's note: "He said to me: 'Mama, I can feel when it's enough now.'"
Priya, 8 Years, Bengaluru
Before: Refused to touch playdough, glue, or anything sticky. Tactile defensiveness so significant that school art class was daily distress.
Intervention: Gradual texture exposure. Week 1: dry rice. Week 3: damp sand. Week 5: finger paint with glove, then bare hands with choice. Week 7: playdough voluntarily picked up.
After (8 weeks): Participating in school art class. Mother: "She came home and told me she made a bird in art today. She was so proud. I cried in the car."
Krish, 5 Years, Mumbai
Before: Could not button shirt independently at age 5. Would stare at fingers the entire time, lose focus, give up. Morning routine: 25 minutes minimum.
Intervention: Textured pencil grip → tactile discrimination games (coins in bag) → textured button board. 6 weeks.
After (6 weeks): First independent shirt-buttoning without looking. Father's data note: "3 buttons. No looking. 45 seconds. I didn't believe it and made him do it again."
"The first time a parent sees their child button without looking, they often describe it as 'a miracle.' It isn't. It's eight weeks of neural pathway training, delivered at a kitchen table." — Pinnacle OT Senior Clinician
Isolation Is the Enemy of Adherence
The families in those vignettes didn't succeed alone. They had other parents who knew the exact feeling of a child staring at their fingers. They had communities that celebrated a 3-second improvement in sensory bin tolerance. You deserve that community too.
📱 Sensory Fine Motor WhatsApp Group
Share progress, ask questions, get peer support from families in the same domain. Real parents, real-time answers. → Join Group at pinnacleblooms.org/community
💻 Pinnacle Parent Community Forum
Structured discussion threads by technique, domain, and challenge type. Search F-616 for a dedicated thread with hundreds of family experiences. → pinnacleblooms.org/community
🤝 Peer Mentoring Program
Connect with an experienced parent who has completed this exact technique with their child. One-to-one guidance from someone who has lived it. → pinnacleblooms.org/mentoring
📍 Local Parent Meetups
Pinnacle Center-organized monthly parent meetings by city. Meet families navigating the same challenges in your community. → pinnacleblooms.org/centers
"If you've made it past week 4 with this technique, you have something irreplaceable to offer a parent on week 1. Consider sharing your journey — even one message in the WhatsApp group can change the trajectory of another family."
Home + Clinic = Maximum Impact
Home-based sensory fine motor practice is clinically validated and essential. But it works best when guided by professional assessment — particularly for children with complex sensory profiles or significant functional impact.
The Clinical Partnership Principle
"The parent is the intervention agent in the home. The OT is the architect of the intervention design. The most effective sensory fine motor outcomes occur when both roles are active, informed, and communicating weekly." — GPT-OS® Clinical Framework
📞 FREE National Autism Helpline
9100 181 181
16+ languages | 24×7 | No appointment needed. Start here for guidance on your next clinical step.
16+ languages | 24×7 | No appointment needed. Start here for guidance on your next clinical step.
🗺️ Find a Center
70+ centers across India. Sensory Integration OTs at all centers. → Find My Nearest Center at pinnacleblooms.org/centers
🎯 OT Matching
Pinnacle's GPT-OS® match engine connects you to the therapist best suited to your child's specific profile. → pinnacleblooms.org/match
📹 Teleconsultation
Not near a center? Video consultation with Pinnacle's OT team — same clinical expertise, delivered to your home. Available: Monday–Saturday, 9 AM – 8 PM IST. → pinnacleblooms.org/consult
Deeper Reading for the Curious Parent
"This page is built on this evidence. Not interpretation of it. The evidence itself."
PRISMA Systematic Review (2024)
16 studies, 2013–2023 | Children, MDPI. "Sensory integration intervention meets EBP criteria for children with ASD across sensory processing, fine motor, social, and adaptive domains."🔗 PMC11506176
Meta-Analysis — World J Clin Cases (2024)
24 studies reviewed. "Significant effect sizes across sensory processing, fine motor, gross motor, social skills, and adaptive behavior outcomes."🔗 PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT — Padmanabha et al. (2019)
Indian Journal of Pediatrics. "Significant outcomes in Indian pediatric populations — validating family-administered sensory protocols in South Asian contexts."🔗 DOI: 10.1007/s12098-018-2747-4
WHO/UNICEF CCD Package (2023)
Care for Child Development. "Caregiver-implemented developmental interventions across 54 LMICs show significant developmental impact — validating home-based protocol frameworks."🔗 PMC9978394
NCAEP Report (2020)
Evidence-Based Practices for Children, Youth, and Young Adults with Autism. "Video modeling, visual supports, and reinforcement procedures confirmed as EBP for autism."🔗 NCAEP (2020)

Your 60 Seconds of Data Helps Every Child Like Yours
When 1,000 families track F-616 data, GPT-OS® can detect which specific material combination, sequence, and intensity produces optimal outcomes for children with specific sensory profiles. This improves recommendations for every future child.
From Visual Dependence Score
GPT-OS® tracks rate of visual independence development across thousands of children with similar sensory profiles. Your child's trajectory is compared against matched cohorts — flagging if progress is faster, typical, or slower than expected.
From Tolerance Rating
The texture tolerance curve predicts generalization timelines. GPT-OS® uses this to recommend when to introduce the next texture level, when to plateau, and when to escalate to clinical review.
From Engagement Duration
Session length data informs optimal future session planning — ensuring home programs remain within the child's optimal therapeutic window, not overtaxing or underserving.
See It Before You Do It
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Watching a model complete the technique before attempting it increases parent accuracy and child acceptance of the intervention.
📹 F-616: 9 Materials That Help With Sensory Fine Motor
Series: Fine Motor Development in Children | Episode 616 | Duration: 75–85 seconds | Available in 16+ languages (subtitled)
What the Reel Shows
- Therapist introduction: the sensory-motor connection in 60 seconds
- All 9 materials demonstrated on-camera with a child participant
- Before/after comparison: hands struggling vs. hands succeeding
- Clinical rationale for each material in plain language
- Subtitled in full for accessibility
"Here's something many parents don't realize: fine motor skills depend on sensory processing. Your child's hands don't just need strength and coordination — they need accurate sensory feedback to guide their movements. When that processing is inefficient, hands can't work automatically. They need eyes to compensate. That's exhausting. These 9 materials address this at the root." — Pinnacle OT Consortium Clinician
Subscribe: YouTube @PinnacleBlooms | Instagram @pinnacleblooms
Consistency Across Caregivers Multiplies Impact
If only one caregiver executes this technique, impact is limited to their presence. When both parents, grandparents, and teachers understand the approach, the child receives sensory-motor training throughout their entire day — not just in scheduled sessions.
For Grandparents & Family Members
"[Child's name] is working on helping their hands learn to feel what they're touching, so their fingers can work without their eyes watching all the time. Let them explore different textures without forcing it. If they use too much force — don't scold. It means their hands are still learning. Ask the parents which materials [child] is working with and do 5 minutes together when you visit."
Teacher Communication Template
Brief, professional template for sharing F-616 context with class teacher — accommodation language, specific classroom adaptations (textured grips, sensory warm-ups before academic tasks), what to look for and report back to parents.
Share This Page:

Questions Families Ask Most About F-616
Act VI: Take Action
Q1: How long before we see results in daily life (like buttoning)?
Functional carryover to daily life tasks typically appears between weeks 4–8. Sensory bin tolerance may improve within 2–3 weeks. Grip modulation in real tasks (writing, eating) typically follows at 4–6 weeks. Buttoning-specific carryover: 6–10 weeks with daily practice.
Q2: My child hates messy play. Should I skip that material?
No — but start with extreme gradualism. Dry sand → damp sand → finger paint (glove first, then bare hands). The trajectory from dry to messy typically takes 4–8 weeks. If your child shows extreme distress at ANY tactile material after 4 weeks, contact Pinnacle at 9100 181 181.
Q3: Can I do this without any purchased materials?
Yes. The most essential tools — sensory bin (any container + dry rice), tactile mystery bag (any opaque bag + household objects), homemade putty (glue + starch) — cost under ₹200. The technique's value is in the sensory input and fine motor practice, not the brand.
Q4: My child has both tactile defensiveness AND proprioceptive seeking. Which materials first?
Start with proprioceptive materials (therapy putty, weighted cuff, squeeze tools). Deep pressure is typically more tolerable for tactile defensive children than light touch. Once proprioceptive system is more organized (2–3 weeks), introduce gradual tactile exposure. Confirm with an OT for complex profiles.
Q5: How many materials should I use per session?
Maximum 2–3 materials per session. One primary (15–20 min) + one secondary (5–8 min) + optional brief fidget cool-down. Rotating which materials are primary across the week ensures all 9 are encountered weekly. Quality of sensory engagement > quantity of materials.
Q6: My child's school says they're too fidgety to concentrate. Is this related?
Almost certainly yes. Sensory-seeking children who lack adequate sensory input regulation seek it through movement and fidgeting — because their nervous system is looking for proprioceptive and tactile input. Sensory fine motor intervention at home directly addresses the underlying need, often reducing school-based fidgeting within 4–6 weeks.
Q7: At what point should we stop home sessions and rely only on clinic OT?
Never. Home and clinic are not alternatives — they are complementary. Add 15-minute daily home sessions to 2× weekly clinic OT and total therapeutic input increases by 85% — delivered in the setting where generalization matters most.
Q8: My child is neurotypical but shows some of these signs. Is this technique relevant?
Yes. Sensory processing differences exist on a spectrum in all populations. This technique is appropriate for any child showing the signs described in Card 2, regardless of diagnosis. If uncertain, contact Pinnacle at 9100 181 181 for a brief screening conversation.
Preview of 9 materials that help with sensory fine motor Therapy Material
Below is a visual preview of 9 materials that help with sensory fine motor therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

The Page Has Given You Everything. Now the Hands Need Practice.
You have the neuroscience. You have the 9 materials. You have the 6-step protocol. You have the progress timeline. You have the troubleshooting guide. You have the parent stories. The only thing between your child's hands and their next skill is 15 minutes and a shallow bin of rice.
🎯 Start This Technique Today
GPT-OS® guided session launcher. Personalized first session plan based on your child's AbilityScore®.
📞 Speak With a Pinnacle OT
Book consultation or call FREE Helpline 9100 181 181 | 16+ languages | 24×7
➡️ Explore the Next Technique
F-617: Bilateral Coordination — "Your next step after sensory fine motor awareness is established." techniques.pinnacleblooms.org/fine-motor/bilateral-coordination-F617
Validated by the Pinnacle Blooms® Multi-Disciplinary Consortium
Pediatric OT • Speech-Language Pathology • Applied Behavior Analysis • Special Education • Neurodevelopmental Pediatrics • CRO
"20M+ sessions • 97%+ measured improvement • 70+ centers • GPT-OS® powered"
"Built by Mothers. Engineered as a System." | "From fear to mastery. One technique at a time."
Pediatric OT • Speech-Language Pathology • Applied Behavior Analysis • Special Education • Neurodevelopmental Pediatrics • CRO
"20M+ sessions • 97%+ measured improvement • 70+ centers • GPT-OS® powered"
"Built by Mothers. Engineered as a System." | "From fear to mastery. One technique at a time."
← F-615: Tool Use Development (previous) | → F-617: Bilateral Coordination (next) | 🏠 techniques.pinnacleblooms.org
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7 | care@pinnacleblooms.org | pinnacleblooms.org