
9 Materials That Help With Self-Help Skills
Evidence-based occupational therapy materials to build self-help skills and daily living independence in children with autism and developmental differences — with clinical guidance from Pinnacle's 70+ center consortium.
OT-ADL · Daily Living
Ages 3–12
L-979 · GPT-OS®

The Recognition Moment
Still doing everything for them?
"It's 7:42 AM. School starts at 8:15. My son has been standing at the door for six minutes while I button his shirt — the same shirt he could not button yesterday, or the day before, or last year. He's seven. He knows his multiplication tables. He can tell you every dinosaur that walked this planet. But he cannot button his shirt. And this morning, I realized I've stopped trying to teach him. I just… do it. Because there's no time. Because trying ends in tears — his and mine."
You are not failing. Your child's nervous system is wired differently, not defectively.
Self-help skills — dressing, feeding, toileting, grooming — are the hardest skills to teach because they require your child's motor planning, fine motor control, sensory processing, and sequencing ability to all work together at the same time. This page gives you the 9 materials that make that possible.
Domain
Occupational Therapy · Daily Living Skills · Functional Independence
Age Band
3–12 years · Consortium Lead: Pediatric OT
Code
L-979 · GPT-OS® Technique Library
Built by Mothers. Engineered as a System. — Pinnacle Blooms Consortium®

You Are Not Alone
Millions of families are navigating this exact challenge.
Children Diagnosed
Children in India diagnosed with autism or developmental differences
Motor Planning Difficulties
Of children with ASD demonstrate motor planning difficulties affecting daily self-care
Families Affected
Of families report self-care independence is their primary daily living concern
Globally, over 78 million children have a developmental condition affecting their ability to perform self-care tasks independently. In India, this translates to more than 8 million families navigating daily battles over dressing, feeding, brushing teeth, and toileting — tasks other families take for granted.
Self-help skill delays are not parenting failures. They are neurological realities with neurological solutions. The gap between what your child cognitively understands and what their motor system can execute is called dyspraxia — a motor planning difficulty. It is documented, researched, and most importantly: addressable.
📖 PRISMA Systematic Review (2024): 80% of children with ASD display motor planning and sensory processing difficulties affecting ADL performance. References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260

What's Happening in Your Child's Brain
The science of "they know what to do but can't make their body do it"
The Praxis Network
Your child's brain uses a praxis network to plan and execute motor sequences:
Premotor Cortex
Plans the movement sequence
Basal Ganglia
Selects and initiates the right pattern
Cerebellum
Coordinates timing and precision
Somatosensory Cortex
Reads tactile feedback from hands
Motor Execution
The button gets buttoned
In children with motor planning differences, this signal chain has gaps. The intent is there. The knowledge is there. The motor execution breaks down between planning and doing.
What This Means for You
"He WANTS to button his shirt. He KNOWS how a button works. His hands just won't do what his brain is telling them to do."
This is not stubbornness. This is not laziness. This is a praxis gap — a real, measurable, neurological difference in how motor sequences are organized and executed.
What creates the praxis gap:
- Proprioceptive processing differences (poor body-position awareness)
- Tactile discrimination difficulty (can't feel where fingers are in space)
- Motor memory formation challenges (repetition doesn't "stick" as fast)
- Sensory overload (textures, sounds, sensations during self-care are overwhelming)
The 9 materials on this page directly compensate for each of these gaps.
📖 Frontiers in Integrative Neuroscience (2020): Praxis network dysfunction is neurologically documented in ASD and DCD populations. Reference: DOI: 10.3389/fnint.2020.556660
Developmental Timeline
Your child is here. Here is where we're heading.
Age 1–2
Participates in dressing — arms through sleeves, socks off
Age 2–4
Removes simple clothing; spoon use (messy); emerging dressing independence; elastic waist management
Age 4–6
Independent dressing except complex fasteners; toileting independent; spoon/fork proficiency
Age 5–9
Fastener mastery begins — buttons, zippers; grooming emerging; handwashing independent; shoe tying
Age 9–12
Full self-care independence across all ADL domains
Children with developmental differences may be functioning 2–4 years behind this timeline. A 7-year-old may have the self-care capacity of a 3–4 year old. This gap is not permanent — it is a developmental waypoint.
What Commonly Co-Occurs with Self-Help Skill Delays: Developmental Coordination Disorder (DCD/Dyspraxia), Sensory Processing Disorder, Autism Spectrum Disorder (ASD), ADHD (executive function affecting task initiation and completion), and Hypotonia (low muscle tone affecting grip and coordination).
"Your child is not behind. Your child is on a different timeline that requires a different approach."
📖 WHO Care for Child Development (CCD) Package: Age-specific evidence-based ADL milestones implemented across 54 countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)
Evidence Base
Clinically validated. Home-applicable. Parent-proven.
Level II — Strong Evidence
Study | Finding | Source | |
PRISMA Systematic Review (2024), 16 studies | OT and sensory integration interventions are evidence-based practice for adaptive behavior in ASD children | PMC11506176 | |
Meta-analysis (World J Clin Cases, 2024), 24 studies | OT interventions significantly improve social skills, adaptive behavior, and motor function | PMC10955541 | |
WHO CCD Package Implementation (2023) | Home-based structured ADL programs across 54 LMICs show significant independence gains | PMC9978394 | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based OT interventions in Indian children produced significant functional outcomes | DOI: 10.1007/s12098-018-2747-4 | |
NCAEP Evidence-Based Practices Report (2020) | Visual supports and task analysis are classified as evidence-based practices for autism | NCAEP 2020 |
1. Task Analysis
Breaking complex skills into visible, teachable steps
2. Adapted Equipment
Modifying tools and environment to reduce barriers
3. Systematic Instruction
Backward chaining, prompting hierarchies, reinforcement schedules
Every material on this page has a documented mechanism of action. This is not trial-and-error. This is precision pediatric occupational therapy, home-delivered.

What It Is · Technique L-979
Self-Help Skills Development via Adapted Materials & Structured Teaching
Formal Name: Activities of Daily Living (ADL) Intervention with Adapted Equipment and Task Analysis
Parent-Friendly Alias: "The Independence Kit" — the tools that turn 'I can't' into 'I did it myself'
Self-help skill development is a structured occupational therapy approach that uses specialized materials, visual supports, adapted equipment, and systematic teaching methods to build children's capacity to care for themselves independently. It addresses the core domains of dressing, feeding, oral hygiene, toileting, and grooming — the foundational self-care tasks that determine whether a child can function independently in home, school, and community settings.
Unlike traditional "watch and copy" instruction, this approach matches teaching method to the child's neurological profile — using visual task analysis for children who can't hold sequences in memory, adapted equipment for children whose motor system creates barriers, and motivation systems for children who disengage from challenging tasks.
📅 Age Range
3–12 years
⏱️ Session Duration
10–20 minutes per skill practice
🔄 Frequency
Daily — every morning and evening is therapy
🎯 Material Categories
Visual Supports · Adaptive Equipment · Practice Tools · Motivation Supports

Who Uses This Technique
This technique crosses every therapy boundary — because independence does too.
Pediatric OT (Primary Lead)
Assesses motor planning, fine motor, and sensory processing; designs task analysis; recommends adapted equipment; trains parents in backward chaining and prompting hierarchies.
ABA / BCBA
Designs reinforcement schedules; implements token economies for self-care routines; uses backward chaining and prompt fading systematically; tracks independence data.
Special Educator
Embeds ADL goals into IEP/ITP; coordinates with home and school; teaches functional life skills in classroom context; supports generalization across settings.
NeuroDev Pediatrics
Identifies underlying motor planning disorders (DCD, dyspraxia); assesses for hypotonia, proprioceptive processing; coordinates medical support for sensory sensitivities.
"The brain doesn't organize by therapy type. Buttoning a shirt requires motor planning (OT), sequencing (SpEd), reinforcement for persistence (ABA), and sensory tolerance (NeuroDev). Teaching it requires all of us." — Pinnacle Blooms Consortium Clinical Lead
The Pinnacle FusionModule™ coordinates these disciplines into a single converged therapeutic pathway — so your child receives the right input from the right specialist at the right moment. 📞 9100 181 181 (FREE · 24×7 · OT + ABA + SpEd + NeuroDev)
Precision Targets
Every material on this page hits a specific ring.
🎯 Primary Targets
- Independence in dressing, feeding, oral hygiene, toileting, and grooming
- Motor planning for multi-step self-care sequences
- Fine motor precision for fasteners, utensils, and grooming tools
- Sequencing ability for routine completion without adult prompting
🔶 Secondary & Tertiary Targets
- Self-esteem and self-efficacy ("I can do it myself")
- Frustration tolerance during challenging motor tasks
- School participation and social inclusion
- Caregiver burden reduction
✅ Observable Progress Indicators
- Child initiates a step without being told
- Meltdowns during self-care decrease in frequency or duration
- Child completes a routine with fewer prompts than last week
- Child says "I did it" or "I can do it"
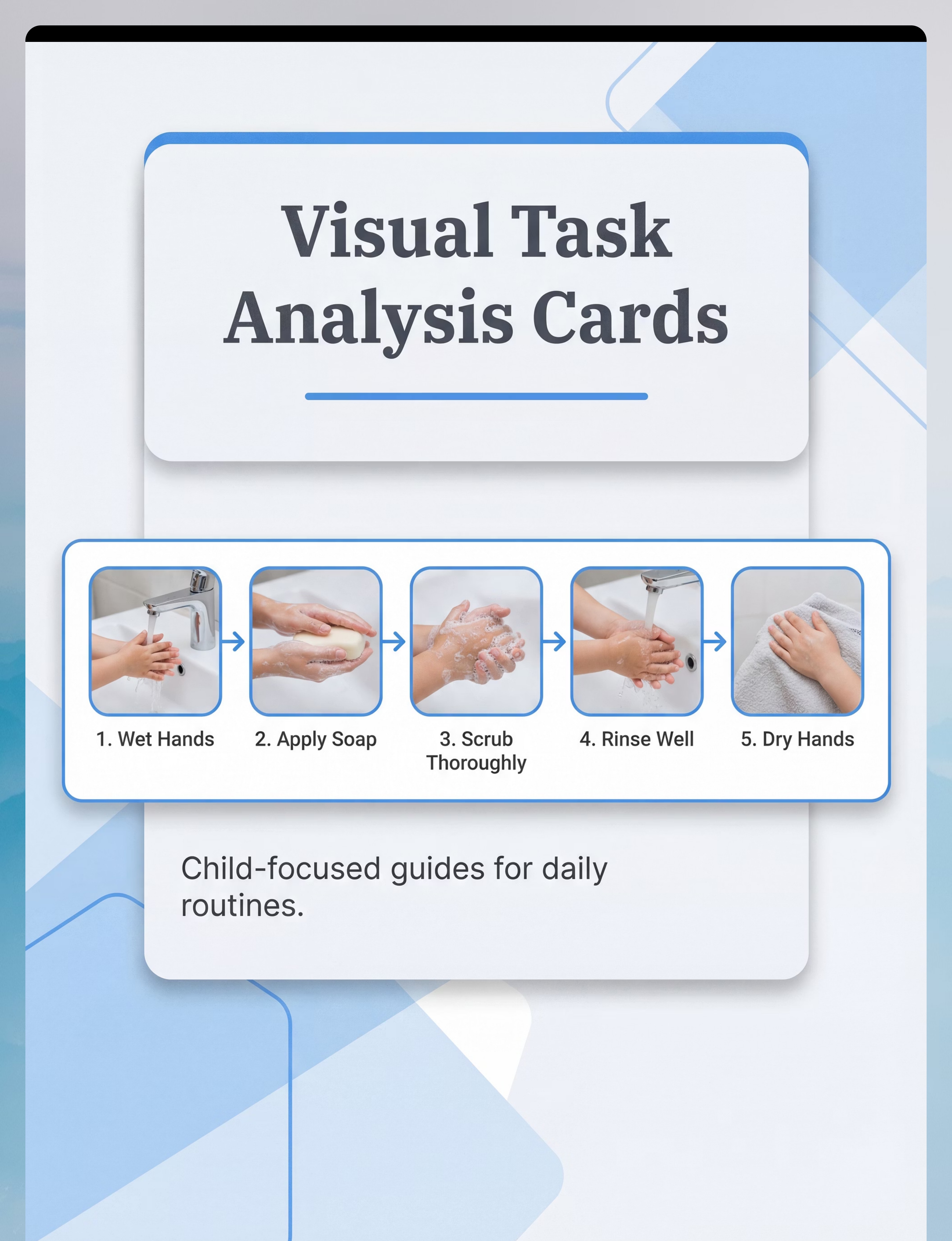
Material 1 of 9
📋 Visual Task Analysis Cards & Self-Care Sequence Strips
🏅 Most Essential — Start Here
Visual Supports
What It Does
Externalizes the multi-step sequence the child's motor planning system struggles to hold internally. Each step is shown as a photograph, arranged left-to-right, posted at point of use — so the visual leads the child through the routine instead of the parent's voice.
Why It Works
Children with motor planning difficulties cannot hold a 7-step handwashing sequence in working memory while simultaneously executing the physical steps. The card eliminates that working memory demand entirely.
Price Range
₹200–600 (printed sets) | ₹0 (DIY with phone + printer)
Where to Get It
DIY Alternative: Photograph YOUR bathroom, YOUR toothbrush, YOUR child's clothes. Print. Laminate with clear tape. Specificity to your home environment is actually superior to generic printed sets.

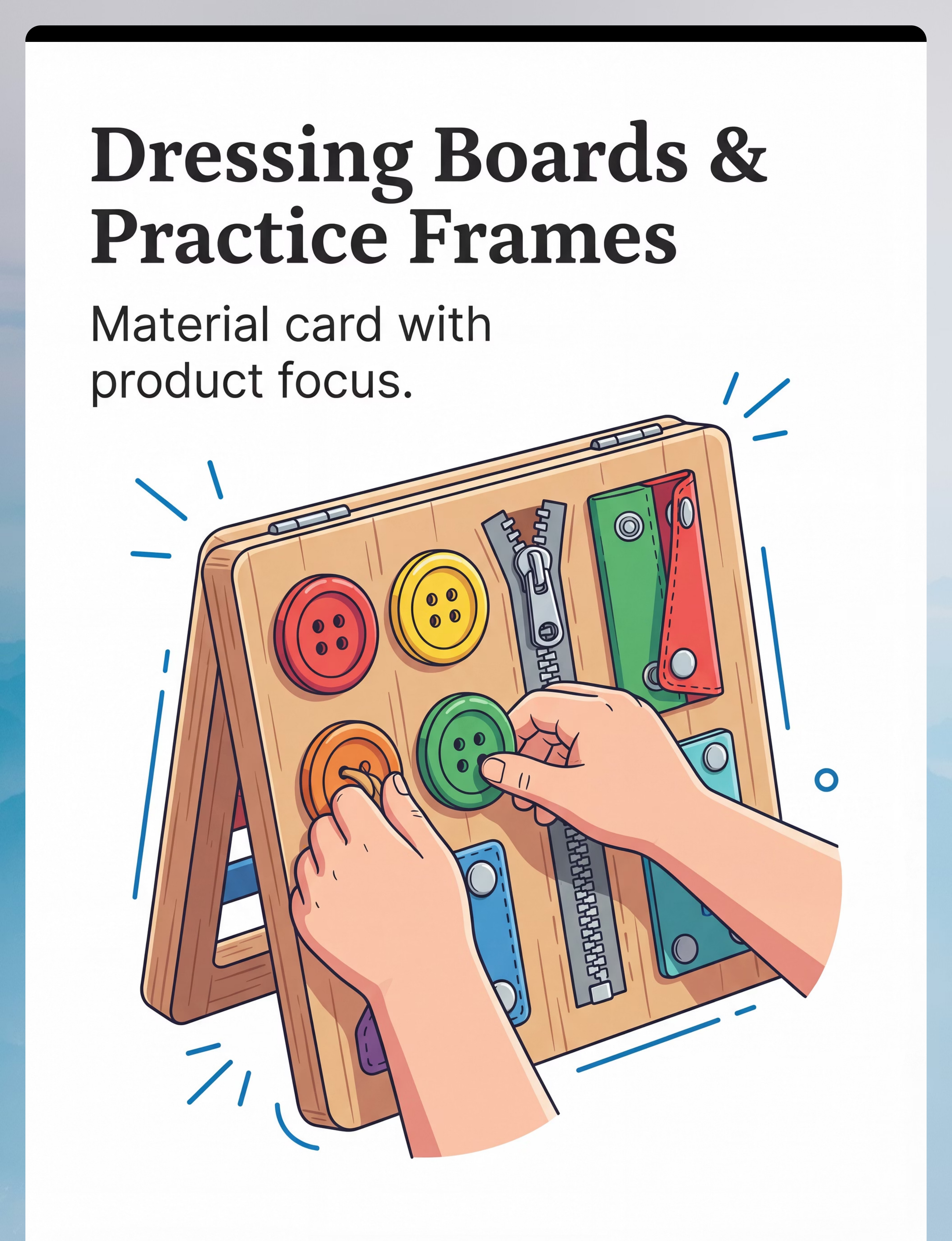
Material 2 of 9
🪡 Dressing Boards & Fastener Practice Frames
Fine Motor
Dressing Practice Tools
What It Does
Isolated fastener practice in a stable, non-moving frame eliminates the confounding factors of actual clothing — fabric movement, awkward angles, and time pressure. This builds motor memory before real-world application.
When a child tries to button a shirt while wearing it, they face an unstable fabric surface, an awkward shoulder angle, and the social pressure of getting out the door on time. The dressing board removes all three barriers simultaneously.
The Clinical Principle
Motor memory forms best when the task is simplified to its core components. Master the button in isolation first; transfer to the real garment second. Each step builds on the last — this is systematic motor learning, not wishful repetition.
Price Range
₹400–1,500
Where to Get It
DIY: Stretch fabric with buttonholes over cardboard. Sew on large buttons. Attach a zipper strip. Add Velcro sections. Cost: scraps. Time: 30 minutes.

Material 3 of 9
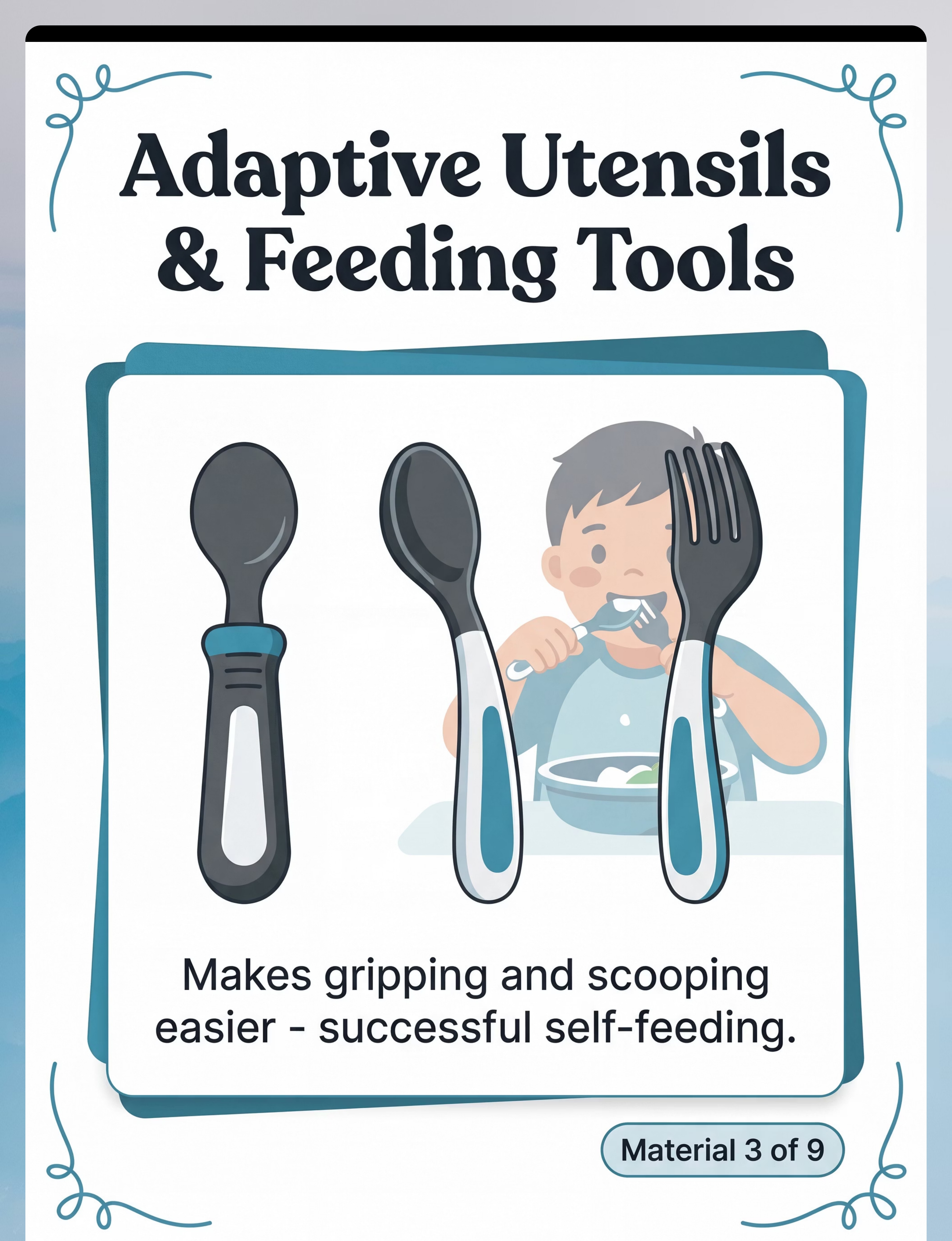
🥄 Adaptive Utensils & Feeding Equipment
Adaptive Equipment
Feeding Tools
What It Does
Built-up handles, weighted barrels, angled spoon heads, and suction bowls reduce the grip strength, wrist rotation, and coordination demands of self-feeding — making success achievable now while skills develop. The child experiences independence before mastery is complete.
The Mechanism of Action
- Built-up handles — reduce grip strength demand; compensate for low tone
- Weighted barrels — increase proprioceptive feedback; reduce tremor effect
- Angled spoon heads — eliminate wrist rotation requirement
- Suction bowls — remove bowl stabilization from the task demand equation
Price Range
₹300–1,200
Where to Get It
DIY: Wrap existing spoon handles with foam pipe insulation (hardware store, ₹50). Tape securely. Place non-slip shelf liner under bowl. Same compensation, near-zero cost.

Material 4 of 9
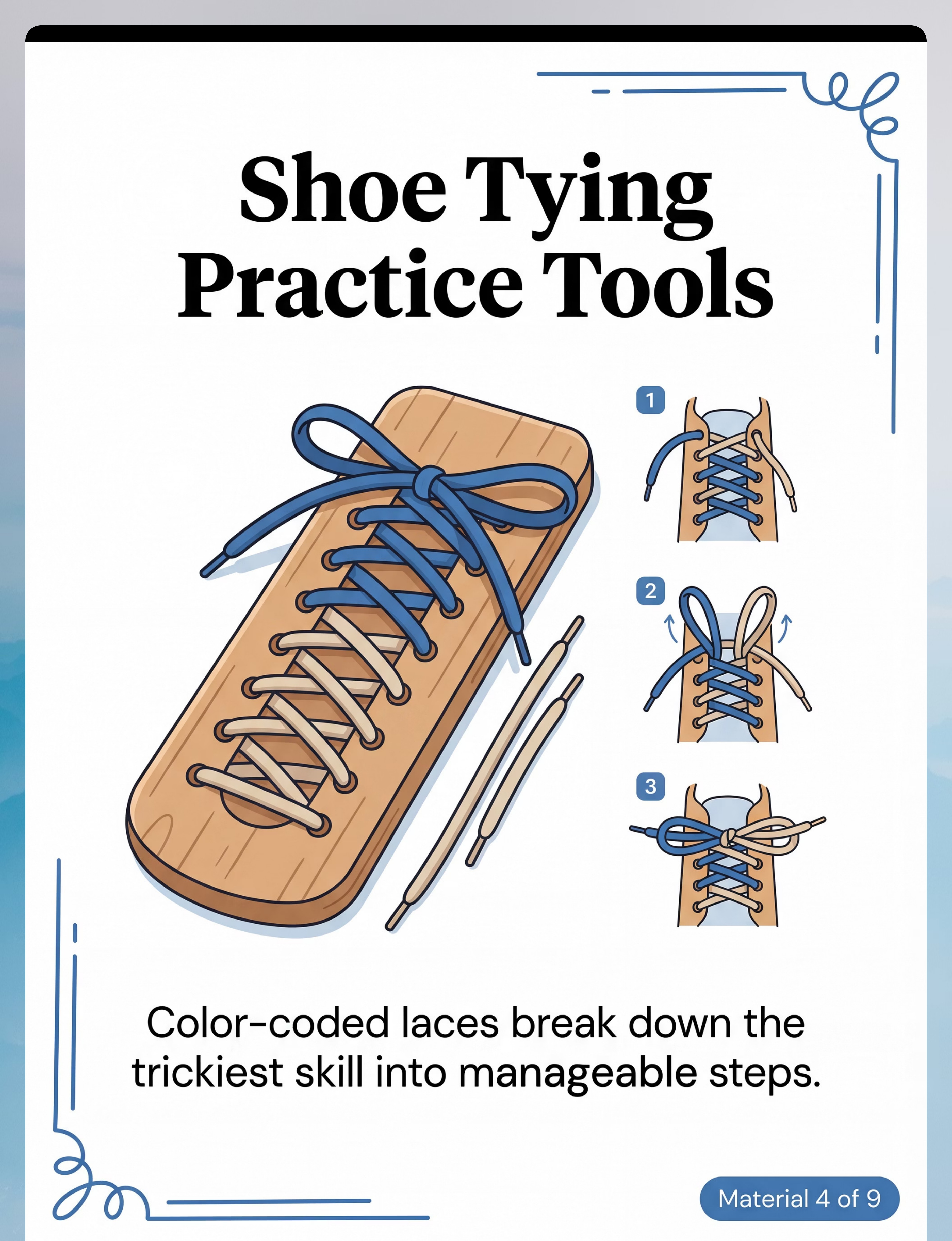
👟 Shoe Tying Practice Tools & Lacing Trainers
Fine Motor
Bilateral Coordination
What It Does
Breaks shoe tying — the most complex ADL motor sequence — into isolated components. Shoe tying requires bilateral coordination, sequential motor planning, and sustained attention simultaneously. Color-coded laces reduce working memory demands by making each lace visually distinct.
Clinical Reality: Shoe tying is genuinely the hardest ADL fine motor skill. If it hasn't responded to structured teaching in 2 years, switch to elastic no-tie laces or Velcro shoes for independence NOW. Revisit when other fine motor skills have developed. Independence matters more than the method.
Price Range
₹200–800
Where to Get It
DIY: Take an old shoe. Mount it at an accessible angle with tape on a table. Use two different colored shoelaces. Same practice, same result.
Material 5 of 9
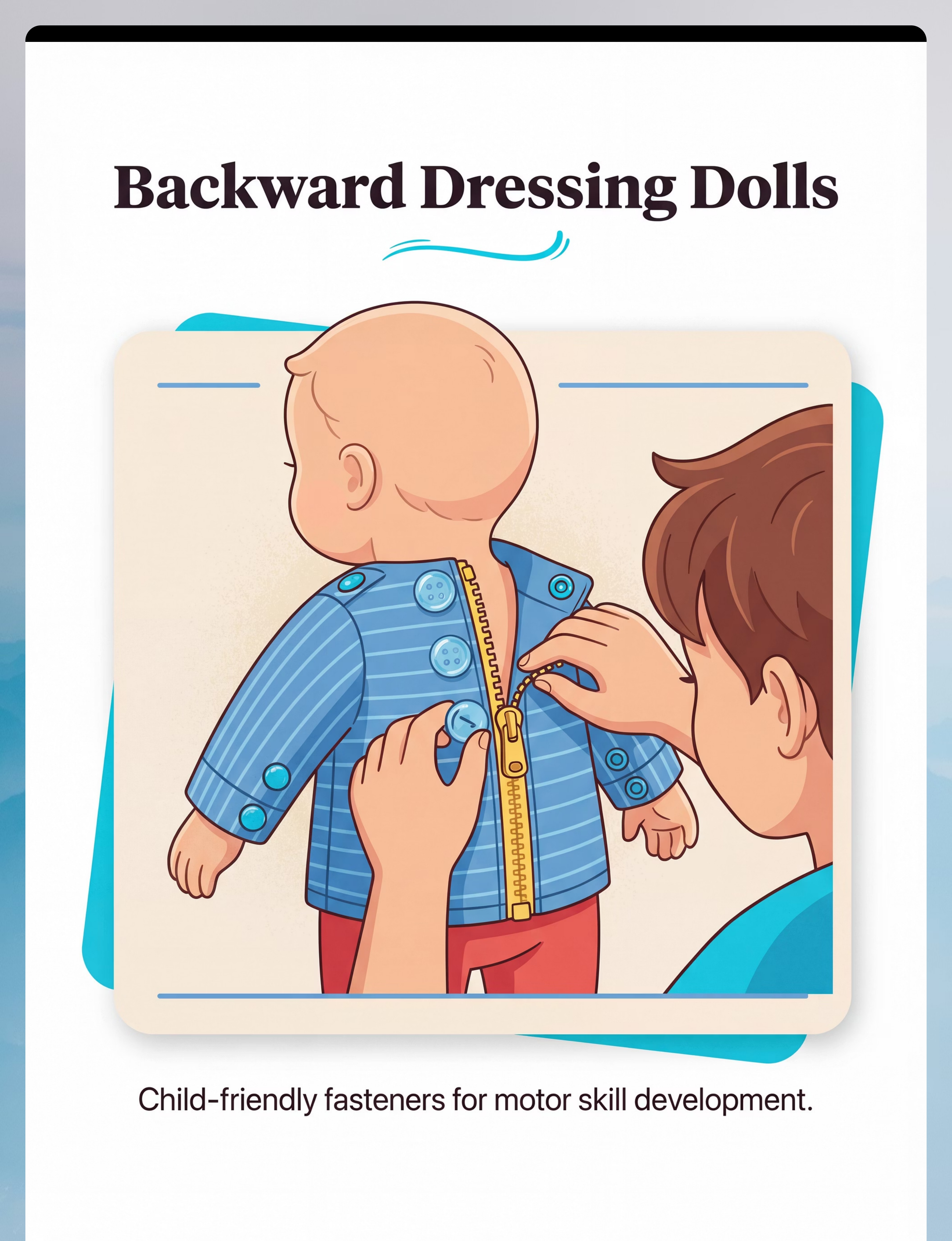
🪆 Backward Dressing Dolls & Self-Help Skill Toys
Practice Toys
Dressing Skills
What It Does
Provides a visible, external practice context. The child can see what their hands are doing, creating motor learning that isn't possible when dressing their own body — where visibility is extremely limited. The doll enables backward chaining in a play context, making practice feel like a game.
The Visibility Advantage
When a child dresses themselves, they cannot see their own shirt collar, the back of their waistband, or their fingers on a button at chest level. On a doll, every movement is fully visible — dramatically accelerating the motor learning loop.
Using It with Backward Chaining
Complete all steps on the doll except the last. Let the child complete the final step. Celebrate. Next session, child does the last two steps. Each session, one more step is added from the end.
Price Range
₹400–1,500
Where to Get It
DIY: Use a large stuffed animal. Dress in actual toddler clothes. Real buttons, real zippers — identical motor practice at a fraction of the cost.

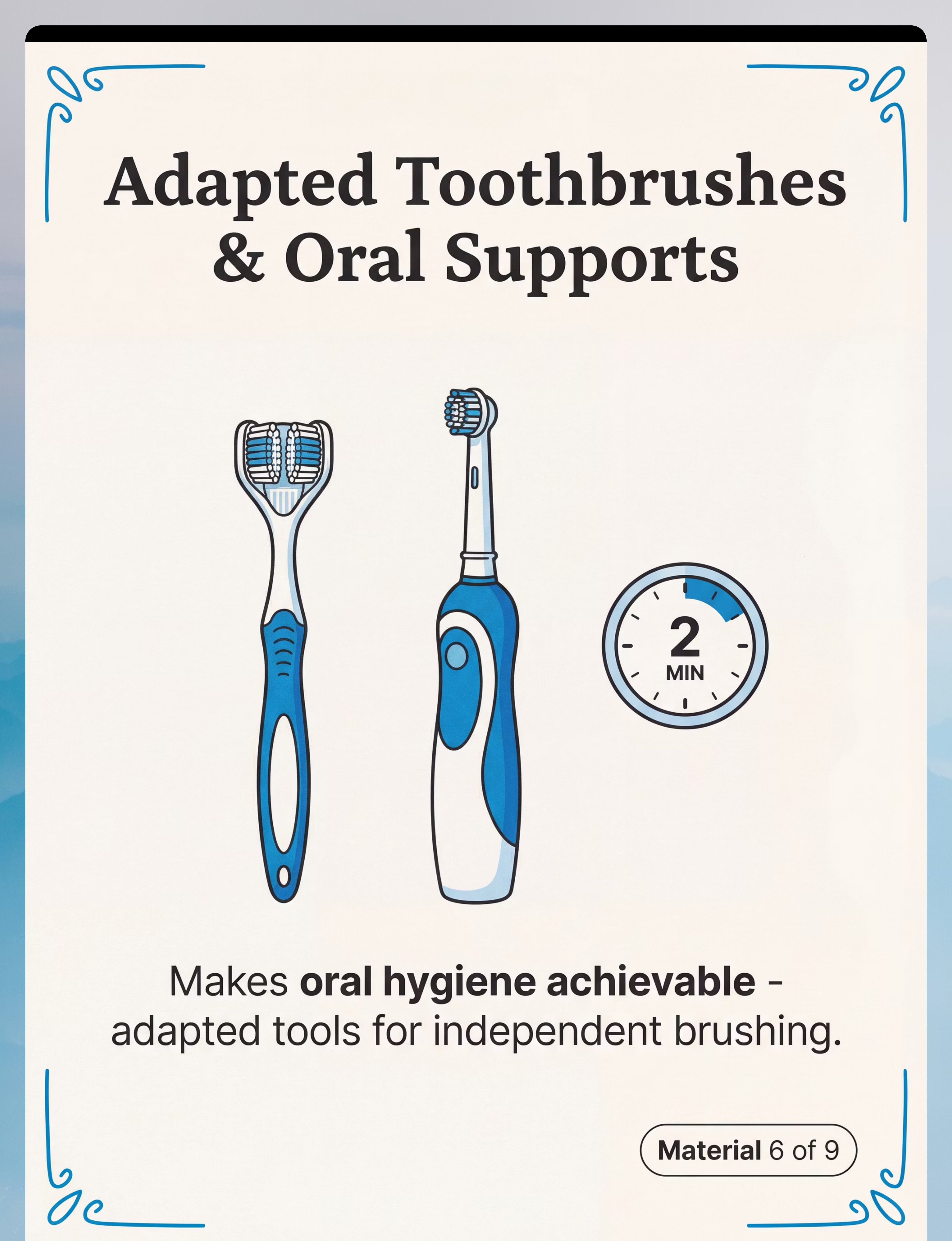
Material 6 of 9
🪥 Adapted Toothbrushes & Oral Hygiene Supports
Adaptive Equipment
Oral Hygiene
What It Does
Three-sided toothbrushes brush all tooth surfaces simultaneously — eliminating the motor planning demand for sequence coverage. Electric toothbrushes provide the movement; the child only positions the brush. Large handles compensate for grip weakness. Together, these adaptations reduce a 7-step oral hygiene sequence down to 2 steps.
For Sensory-Sensitive Children
Toothbrushing aversion this severe usually indicates genuine sensory hypersensitivity. Do not force brushing. Begin oral desensitization: touch toothbrush → lips only → inside lips → dry brush (no paste) → water only → then toothpaste. This process may take 4–8 weeks before any brushing is possible.
Price Range
₹200–1,000
Where to Get It
DIY: Electric toothbrush from any pharmacy (₹150). Wrap handle with rubber bands for grip. Two-minute sand timer from craft store (₹30). Total cost under ₹200.
Monitor toothpaste amount — children who swallow must use training toothpaste (fluoride-free).

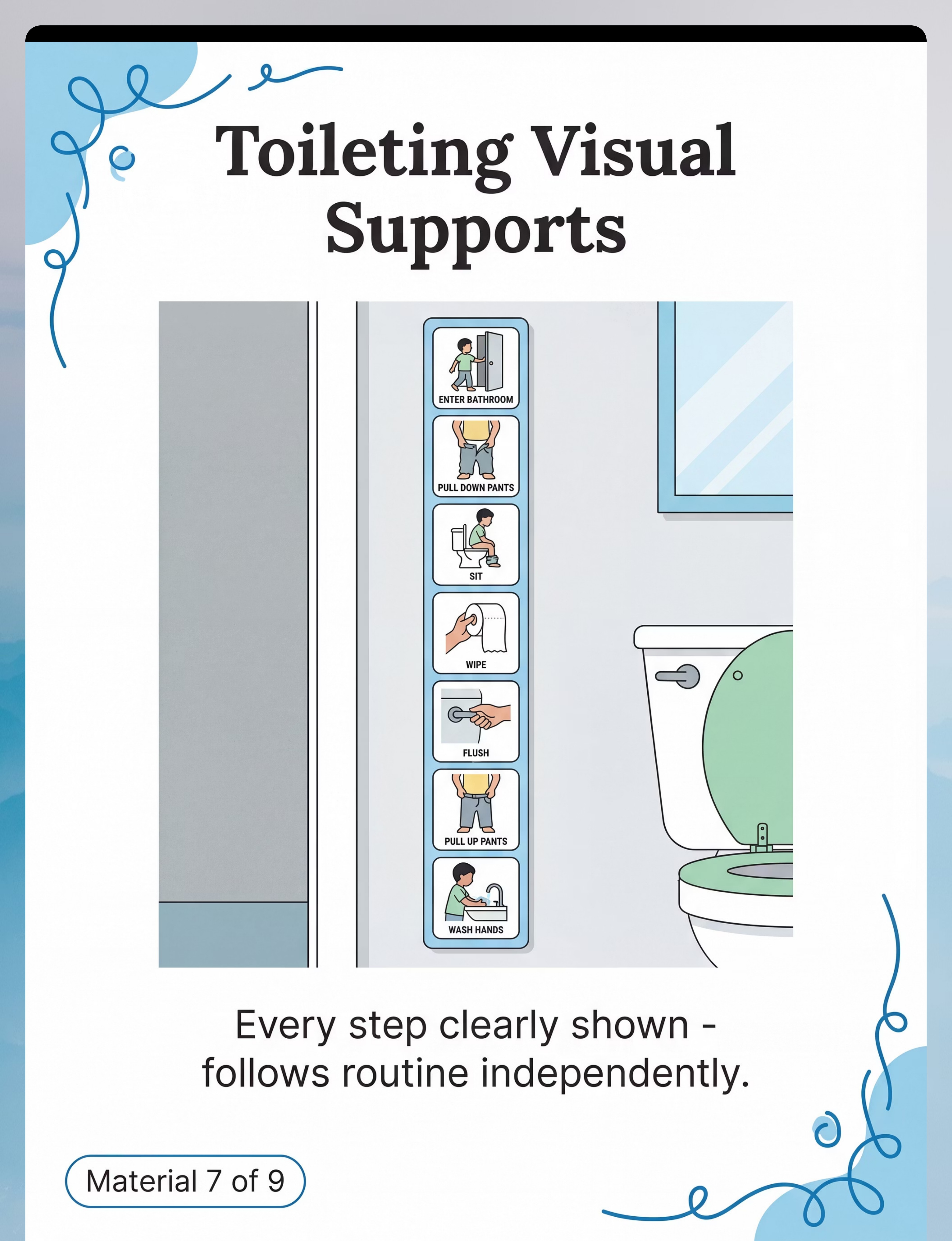
Material 7 of 9
🚽 Toileting Visual Supports & Bathroom Sequence Strips
Visual Supports
Toileting Aids
What It Does
The 14-step toileting sequence — enter → pants down → sit → wait → wipe → flush → pants up → handwash → dry → exit — is impossible to hold in working memory while executing the physical steps simultaneously. Posted at child's eye level, this visual strip eliminates verbal prompting entirely and builds true, lasting independence.
Placement Matters
Post inside the bathroom door at the child's eye level. The strip should be visible from the toilet position. Use real photographs of your bathroom (not generic clipart) for maximum relevance and comprehension.
Price Range
₹100–400 (printed) | ₹0 (DIY with photos of your bathroom)
Where to Get It
DIY: Print any toileting picture sequence from the internet. Laminate with clear tape. Tape inside your bathroom door. Ready in under 10 minutes.

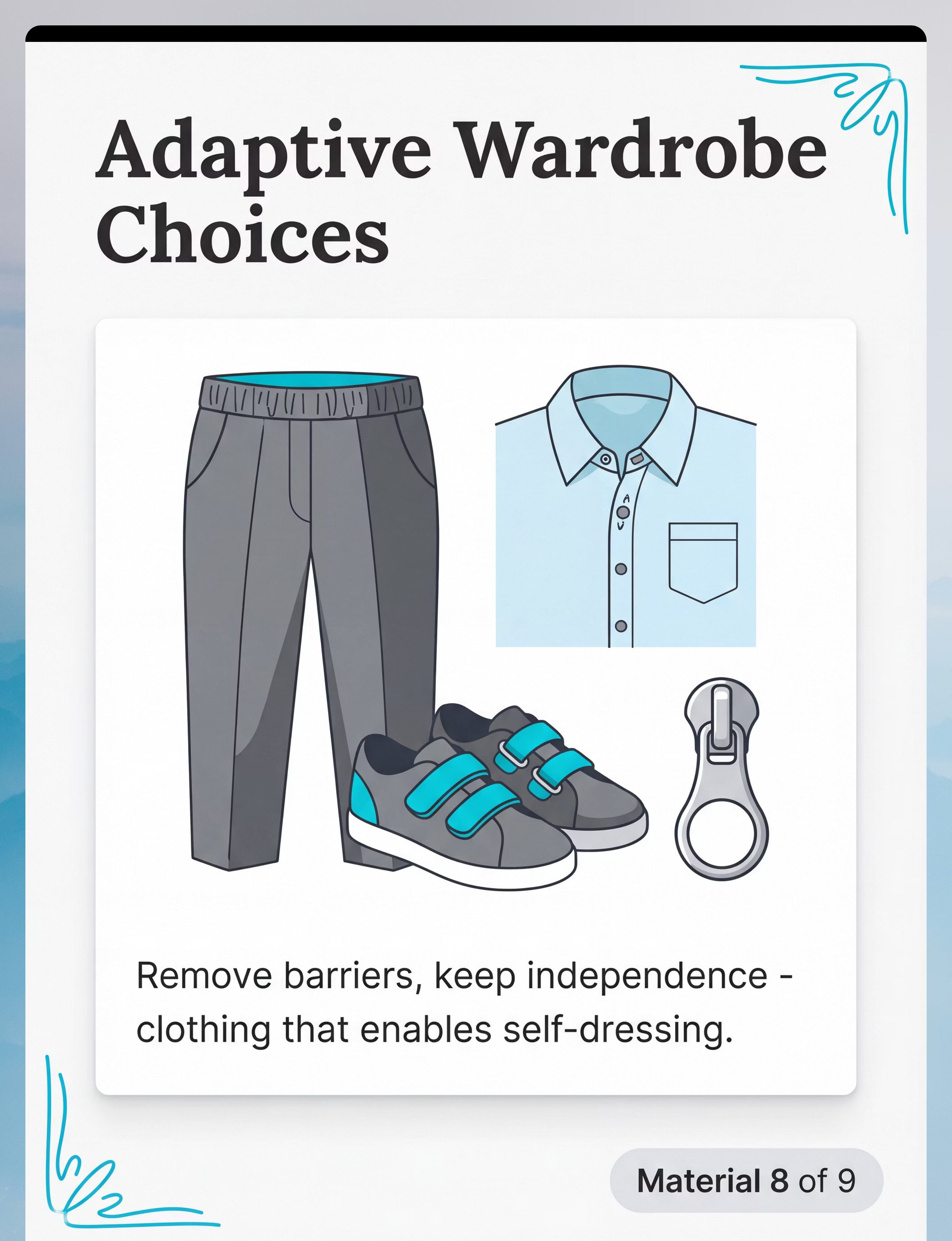
Material 8 of 9
👕 Clothing Adaptations & Adaptive Wardrobe Choices
Adaptive Equipment
Clothing Modifications
What It Does
Removes unnecessary fine motor barriers from the clothing itself. Magnetic closures, Velcro substitutes, elastic waistbands, and zipper pulls reduce the number of motor planning demands in getting dressed — preserving independence without requiring mastery of complex fasteners.
This is not "giving up." This is meeting the child where they are today while building skills for tomorrow. A child who dresses independently in adaptive clothing is building self-efficacy, confidence, and the foundational routine that fastener mastery will eventually upgrade.
Adaptation Menu
- Magnetic closures — replace buttons on shirts entirely
- Velcro under buttons — buttons become decorative; Velcro does the work
- Elastic waistbands — eliminate all fastener demands for pants/skirts
- D-ring zipper pull — ribbon loop makes zipper graspable
- Tagless, seamless fabrics — reduce sensory triggers during dressing
Price Range
₹200–2,000 (adaptations) | ₹1,000–5,000 (adaptive clothing)
Where to Get It

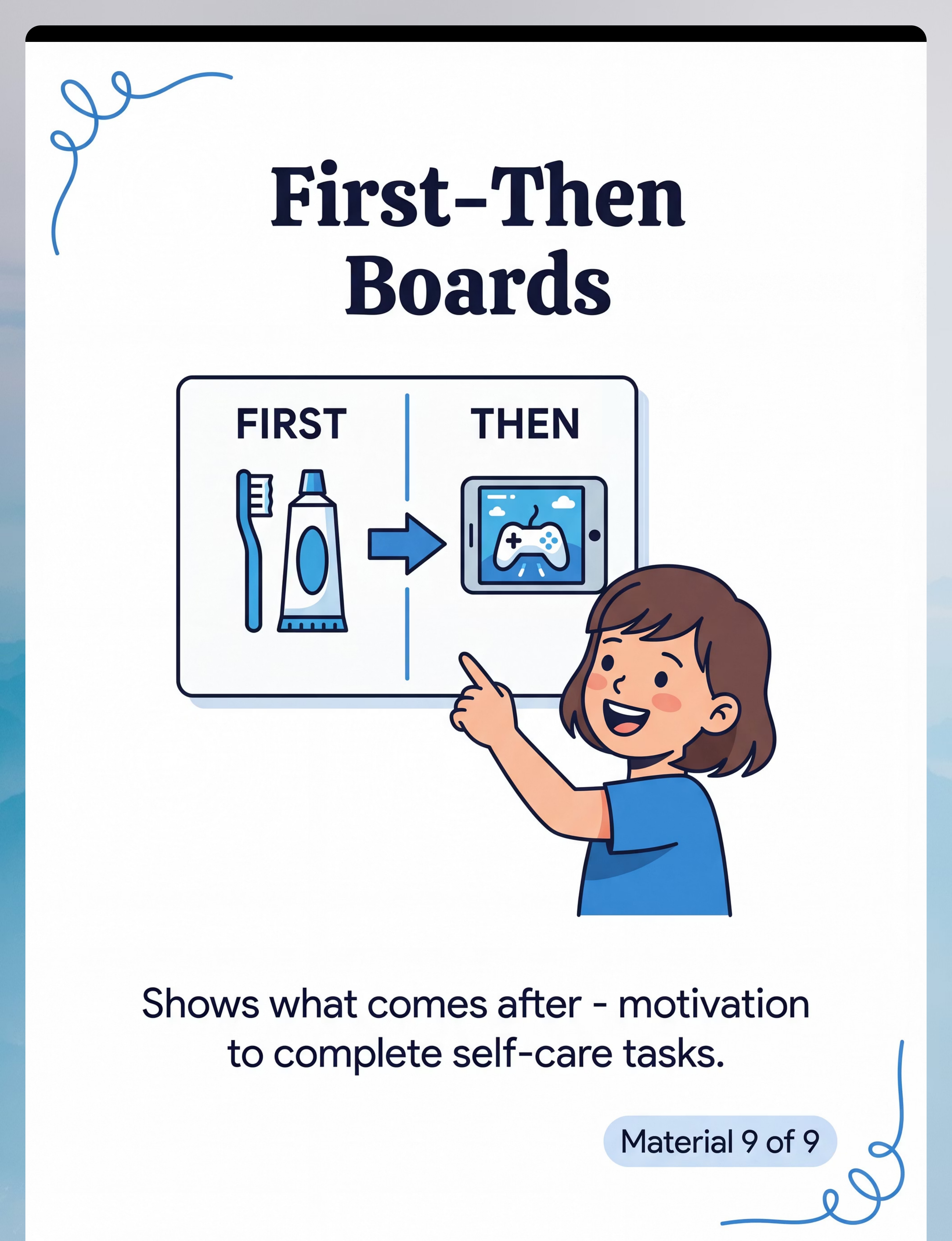
Material 9 of 9
📋 First-Then Boards & Motivation Supports for Self-Care
Reinforcement Menus
Motivation Systems
What It Does
Makes the reward for completing a difficult self-care task concrete and visible — not abstract ("you'll feel good") but immediate and specific ("finish brushing → iPad for 10 minutes"). When children can SEE the reward before they begin, persistence through hard tasks becomes neurologically possible.
This is documented ABA science. You are not bribing your child. You are scaffolding a skill until intrinsic motivation — "I can do it myself!" — replaces extrinsic reward. That transition typically happens at weeks 6–10 for established routines.
Price Range
₹100–400 | ₹0 (printable templates)
DIY: Two sections of cardboard. Write "FIRST" and "THEN." Draw or print pictures. Attach with Velcro or hold up. Starts working immediately.
Canon Direct Products
Rosette Imprint Reward Jar — ₹589
Canon Direct Link — Every completed self-care step earns a marble in the jar. Full jar = preferred activity.
1800+ Reward Stickers — ₹364
Canon Direct Link — Sticker chart for ADL milestone celebration. Morning routine chart sticker for each complete day.
📞 Need help choosing the right materials for your child? Call 9100 181 181 — FREE OT guidance, 24×7

DIY & Substitute Options
Every material on this page has a ₹0 version.
Per WHO/UNICEF equity principles: No family's economic situation should determine whether their child learns independence.
Material | BUY (Amazon.in) | DIY (Today, at Home) | |
Visual Task Analysis Cards | Printed laminated sets ₹200–600 | Photograph YOUR bathroom, YOUR toothbrush, YOUR child's clothes. Print. Laminate with clear tape. Specificity to your home is actually superior. | |
Dressing Boards | Montessori frames ₹400–1,500 | Stretch fabric with buttonholes over cardboard. Sew on large buttons. Attach a zipper strip. Add Velcro. Cost: scraps. Time: 30 minutes. | |
Adaptive Utensils | Built-up handle sets ₹300–1,200 | Wrap existing spoon handles with foam pipe insulation (hardware store, ₹50). Tape securely. Non-slip shelf liner under bowl. | |
Shoe Tying Tools | Practice boards ₹200–800 | Old shoe mounted at accessible angle. Two different colored shoelaces. Same practice, same result. | |
Dressing Dolls | Practice dolls ₹400–1,500 | Large stuffed animal dressed in actual toddler clothes. Real buttons, real zippers — identical motor practice. | |
Adapted Toothbrush | Three-sided brushes ₹200–1,000 | Electric toothbrush from any pharmacy (₹150). Wrap handle with rubber bands for grip. Two-minute sand timer (₹30). | |
Toileting Visuals | Printed strips ₹100–400 | Print any toileting sequence from internet. Laminate with clear tape. Tape inside bathroom door. | |
Adaptive Clothing | Magnetic shirts ₹1,000–5,000 | Sew Velcro under all buttons. Choose elastic-waist pants. Add D-ring zipper pull with ribbon (₹10). | |
First-Then Boards | Commercial boards ₹100–400 | Two sections of cardboard. "FIRST" and "THEN." Draw or print pictures. Works immediately. |
"When you can't buy it, make it. When you make it with photos of your home, it may work better than the purchased version." — Pinnacle Blooms OT Consortium

Safety First
Pre-Session Safety Gate — Read Before Executing
🔴 DO NOT PROCEED IF:
- Child is in active meltdown or post-meltdown recovery (30-minute window)
- Child is running fever or is physically unwell
- Task analysis cards or practice boards have loose small parts (choking hazard for children under 4)
- Child has had a traumatic experience with this specific self-care task today
- Electric toothbrush or adaptive equipment has damaged/frayed components
🟡 MODIFY BEFORE PROCEEDING:
- Child appears tired, hungry, or emotionally dysregulated → Feed first, simplify the goal
- Child is showing sensory sensitivity in relevant body area → Use lightest approach; don't force tolerance
- Button or fastener practice is causing significant frustration → Shift to Velcro first
- Child resisted the last 3 sessions in a row → Conduct functional assessment before next session
🟢 SAFE TO PROCEED WHEN:
- Child is calm, alert, and recently fed
- Environment is prepared (see Setup Card)
- Practice materials are securely assembled — no loose parts
- Parent/caregiver has reviewed this session's specific goal
🛑 STOP SESSION IMMEDIATELY IF: Child shows signs of severe sensory overload (self-harm, vomiting, extreme distress), acute illness symptoms, or refuses to continue despite modification attempts.

Environment Setup
The right environment makes the difference between a session that works and one that doesn't.
Bathroom Setup
- Mirror at child's eye level — place sequence strip here
- Toothbrush in cup — same position every time
- Handwashing sequence strip beside sink at eye level
- Towel at child's reach — not the adult towel rack
- Visual timer on counter, visible from sink position
Bedroom / Dressing Area
- Dressing sequence strip posted at child's eye level on closet door
- Chair or bed for seated dressing — eliminates balance demand
- Clothes laid out in dressing order: underwear on top
- Dressing board on stable table for practice before real clothes
- First-Then board visible — motivating "then" visible before starting
Dining Area
- Non-slip placemat — bowl and plate cannot slide
- Adaptive utensils beside bowl — child's position only
- Food that matches skill level — practice scooping with appropriate foods
- Cup at manageable level — not adult-height positioning
WHAT TO REMOVE: Competing screens (unless in "then" position on First-Then board) · Other children who may distract · Time pressure whenever possible — morning routines are hardest; practice in afternoon · Adult items that look similar to children's items
💡Lighting: Bright and clear — children need to SEE what their hands are doing. Sound: Minimal background noise — distraction breaks sequencing. Temperature: Comfortable — sensory discomfort during dressing interferes with skill acquisition.

Readiness Check
60-Second Pre-Session Assessment
Check these 7 indicators before beginning every session:
1
Fed & Hydrated
Child has eaten in the last 1.5 hours and is not hungry
2
Rested
Not overtired — check for eye-rubbing, yawning, irritability
3
Calm Baseline
At emotional baseline — not recovering from any distress
4
No Active Illness
No fever, no unusual physical discomfort
5
Engagement Available
Makes eye contact, responds to name, shows some interest
6
Reinforcer Ready
You have the "then" item ready for First-Then board
7
Time Available
10–20 uninterrupted minutes — no imminent departure pressure
Checklist Result | Decision | Action | |
6–7 boxes checked | ✅ GO | Proceed with full session plan | |
4–5 boxes checked | ⚠️ MODIFY | Reduce to one skill, shorter duration, lighter materials | |
3 or fewer checked | 🛑 POSTPONE | Today is not a therapy day. Do a preferred activity instead. |
"The best session is one that starts right. Pushing through a 'no-go' state doesn't build skills — it builds resistance." — Pinnacle Blooms ABA/OT Integrated Protocol

Step 1 of 6
THE INVITATION
Timing: 30–60 seconds | Goal: Child approaches without resistance
"Hey, let's try something together. Look — I made you a special card that shows every step. You just have to look at the pictures."
"First we do [task], then you get [preferred item]. See? [show First-Then board]. Just this one thing, then you're free."
"I need your help testing something. Can you try putting on your shirt with this card? I want to see if it works."
✅ Acceptance Cues (child is ready)
- Looks at you or the materials
- Physically moves toward the task area
- Takes the visual card from you
- Stops current activity without severe protest
⚠️ Resistance Cues (modify the invitation)
- Turns away or covers ears
- Drops to floor
- Verbal "no" with rising distress
If Resistance: Do NOT raise demand. Try: "Okay, just come sit with me and look at the picture." Zero-demand proximity before task introduction.
Body Language for the Parent: Crouch to child's height. Calm, unhurried tone — your anxiety transmits. Show visual supports first, before mentioning the task. Position yourself beside the child, not in front.

Step 2 of 6
THE ENGAGEMENT
Timing: 1–3 minutes | Goal: Child interacts with materials
Introducing the Visual Task Analysis Card
Place the sequence strip where the task happens. Point to the FIRST step only — "Look, step one. Just step one." Do not narrate the whole sequence. Let child look, touch, and examine.
Introducing the Practice Tool
Place the dressing board or lacing trainer on the table without instruction. Let child explore for 30 seconds (natural curiosity activates engagement). Demonstrate ONE action. Offer: "Want to try?"
Introducing the Adaptive Utensil
Place adapted spoon beside regular spoon — let child choose. If child chooses regular, respect it and observe where breakdown occurs. If child chooses adapted, narrate: "That one has a big handle — easier to hold."
Reinforcement Cue: The moment the child makes ANY contact with the material — verbal praise immediately: "Great, you're looking at it. That's exactly right."

Step 3 of 6
THE THERAPEUTIC ACTION
Timing: 5–12 minutes | This is the skill-building core of the session
Visual Task Analysis Practice
- Child stands/sits at point of use (bathroom mirror, closet, sink)
- Parent points to Step 1: "What does that picture show?"
- Child looks at picture and performs step
- Parent points to Step 2; child looks and performs
- Continue through all steps — the visual strip leads, not verbal instruction
- Goal: Parent speaks as little as possible. The visual does the prompting.
Dressing Board — Backward Chaining
- Parent completes all steps except the LAST (child completes the final push)
- Child completes LAST step → IMMEDIATE celebration
- Next session: parent completes all but LAST TWO steps
- Each session, child does ONE MORE step from the end
- Every trial ends in success — this is the power of backward chaining
Adaptive Utensil Use
- Place appropriate food in high-rimmed bowl on suction mat
- Offer adapted spoon — let child grasp naturally
- Correct grip ONCE with gentle hand-over-hand guidance, then release
- Let child attempt the scoop → mouth arc without interruption
- Celebrate any independent attempt, regardless of spillage

Step 4 of 6
REPEAT & VARY
Timing: 3–5 minutes | Target: 3–5 quality repetitions
Dosage Principle: 3 good repetitions > 10 forced repetitions. Motor memory forms through quality, not volume. When the child is engaged and succeeding, neural pathways are forming. When they're resistant and forced, the pathways don't form — only avoidance does.
Skill | Reps/Session | Variation Strategy | |
Dressing board fasteners | 3–5 opens + closes | Vary starting position slightly each time | |
Handwashing sequence | 2–3 complete sequences | Vary the visual prompt detail (more/fewer pictures) | |
Adaptive utensil feeding | Full meal duration | Vary food texture within child's comfort zone | |
Shoe tying practice | 3–5 attempts | Alternate color-coded lace orientation | |
Toileting sequence | Natural frequency + visual | Never forced — follows biological need |
Variation Options to Maintain Engagement:
- Change the child's seated position slightly — different angle builds motor generalization
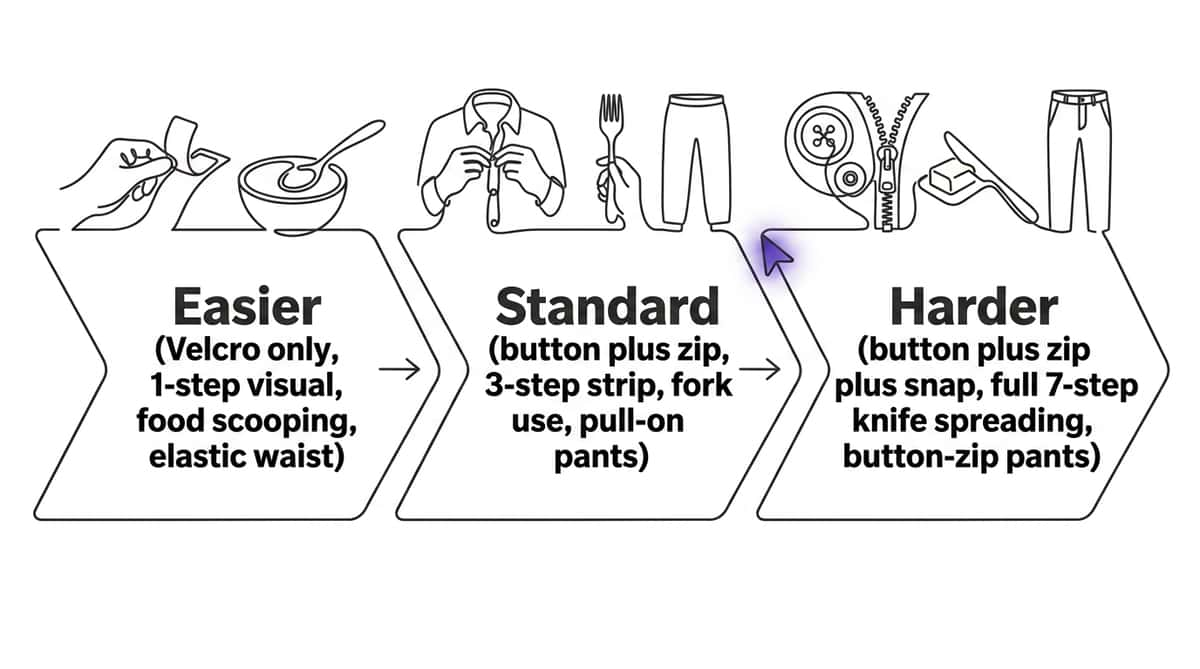
- Change task complexity by 5% up or down based on child's response
- Introduce a second visual card showing the same sequence differently
- Allow child to "teach" the parent one step — metacognitive boost
Step 5 of 6
REINFORCE & CELEBRATE
Timing: Immediate — within 3 seconds of desired behavior
The Reinforcement Rule: Immediate + Specific + Enthusiastic = Behavior Strengthens
"YES! You buttoned it yourself! You did it!"
"Look at you! You followed the card all the way through!"
"That was the hardest part and you did it — I'm so proud."
Natural Reinforcers (Always First Choice)
- "You get to choose today's breakfast because you dressed yourself"
- "Because you brushed your teeth, now you can have [preferred food]"
- "You are SO independent right now"
Social Reinforcers
- High five, fist bump, hug (if touch is welcome)
- Specific verbal praise from preferred adult
- Show Dad / Grandma / teacher what you did
Token Economy (Canon Direct Links)
Rosette Imprint Reward Jar — ₹589
Canon Direct Link — Every completed self-care step earns a marble. Full jar = preferred activity.
1800+ Reward Stickers — ₹364
Canon Direct Link — Morning routine chart sticker for each complete self-care day.
First-Then Delivery: Deliver the "then" item IMMEDIATELY upon task completion. No delay. Broken First-Then promises destroy the system within 2 attempts.

Step 6 of 6
THE COOL-DOWN
Timing: 2–3 minutes | No session ends abruptly
Abrupt endings are associated with dysregulation and resistance to starting next time. The cool-down signals session completion without surprise, allows the child to integrate the sensory and motor experience, and maintains positive associations with self-care practice.
Transition Warning
"Two more times, then we're all done." Use a visual timer if needed.
Final Repetition
Complete final repetition with enthusiastic celebration.
Material Put-Away
Child participates in putting materials away — this is a therapeutic routine in itself.
Brief Calming Activity
60 seconds of preferred low-demand activity to transition out.
First-Then Delivery
Deliver the "then" item. Transition to next routine cue.
Post-Session Care for the Parent: This was hard. You sat through the resistance, the redirecting, the "no"s and the frustrations. That is therapeutic parenting — the most demanding discipline there is. You showed up. That matters.

Track Progress
60 seconds of data now saves hours of guessing later.
Field | What to Note | Time | |
Skill Practiced | Which specific skill (e.g., "buttoning shirt") | 5 seconds | |
Prompts Needed | 0 = independent, 1 = visual only, 2 = verbal, 3 = gesture, 4 = partial physical, 5 = full physical | 5 seconds | |
Child Response | 1 = refused/meltdown, 2 = resistant, 3 = tolerated, 4 = engaged, 5 = enthusiastic | 5 seconds |
Quick Tracking Formats
- Tally: Mark each completed step. Count at end of week.
- Independence Level: Rate 0–5 (full physical → fully independent)
- Duration: How long to complete the full routine without adult intervention
Why This Data Matters
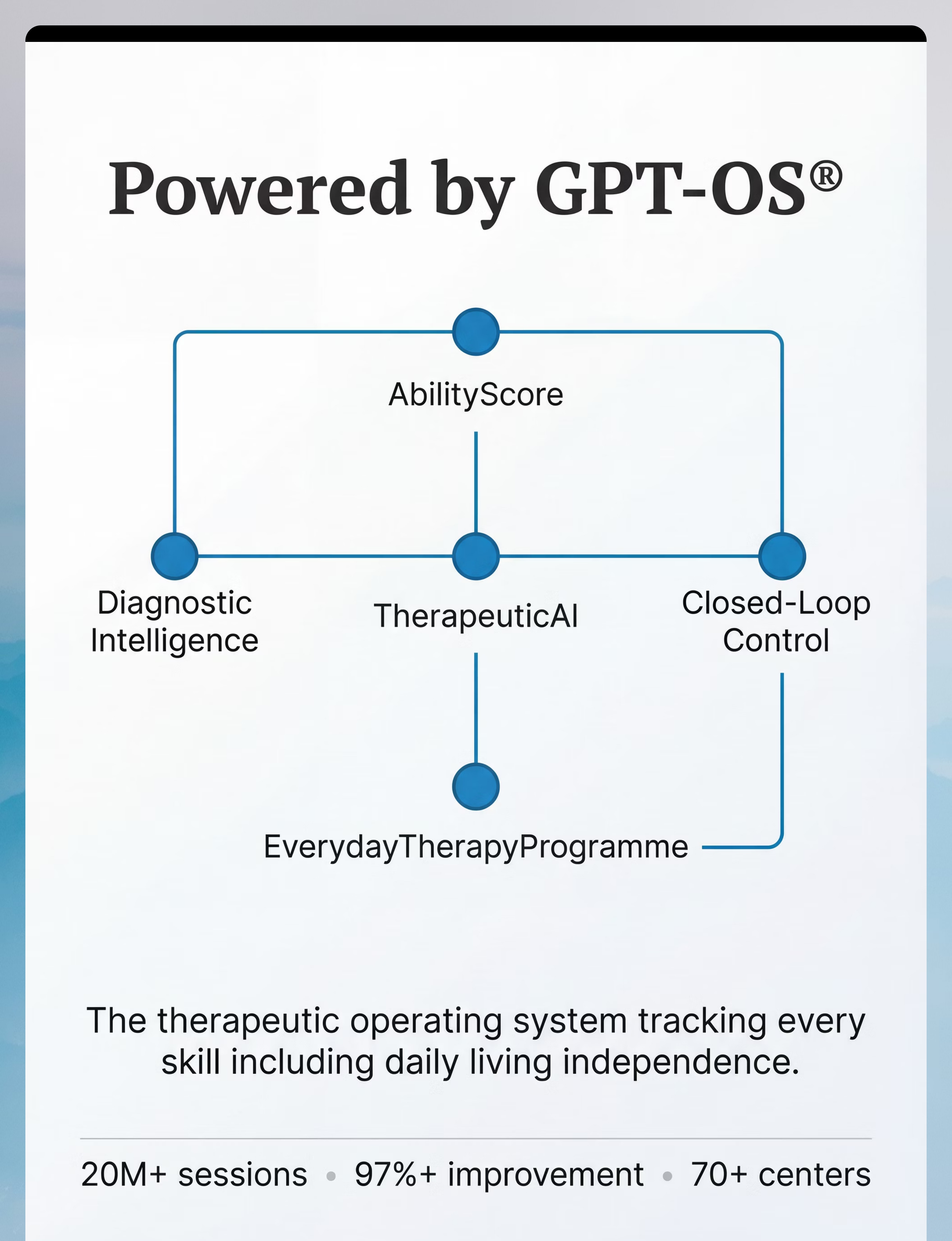
Your GPT-OS® therapist uses this data to adjust the prompting level, change materials, or escalate to clinic support. Without data, your OT is guessing. With data, your OT is precise.
Progress Indicator to Watch: When "Prompts Needed" decreases from 4 → 3 → 2 over 2–3 weeks: neural pathway formation confirmed. You're doing it right.

Troubleshooting
"That didn't work" has a fix.
⚠️ Child completely ignored the visual task analysis card
Why: Visual cards work only when the habit of looking at them is established first. The first 5–10 sessions build the "check the card" behavior.
Fix: Before the task, practice the habit: point to card → child looks → immediate praise. Repeat 5 times without performing any task step. Establish the looking behavior first.
Fix: Before the task, practice the habit: point to card → child looks → immediate praise. Repeat 5 times without performing any task step. Establish the looking behavior first.
⚠️ Dressing board practice fell apart at real clothes
Why: Transfer from isolated practice to real-world application requires explicit bridging. The board is a prerequisite, not a replacement for real-clothes practice.
Fix: After 3 board reps, immediately attempt the same fastener on actual clothing. Bridge the gap in the same session.
Fix: After 3 board reps, immediately attempt the same fastener on actual clothing. Bridge the gap in the same session.
⚠️ Child ate with fingers instead of adaptive utensil
Why: Fingers work better, feel familiar, and require no motor planning — it's the path of least resistance.
Fix: Guide spoon hand through ONE scoop with partial physical prompt, then release. Gradually increase the spoon-guided portion each session.
Fix: Guide spoon hand through ONE scoop with partial physical prompt, then release. Gradually increase the spoon-guided portion each session.
⚠️ Shoe tying practice ended in complete frustration
Why: Shoe tying requires bilateral coordination, sequential motor planning, and sustained attention simultaneously — it is the hardest ADL fine motor skill.
Fix: Stop tying practice entirely. Switch to elastic laces / Velcro shoes for independence NOW. Independence matters more than the method.
Fix: Stop tying practice entirely. Switch to elastic laces / Velcro shoes for independence NOW. Independence matters more than the method.
⚠️ Child severely distressed during toothbrushing
Why: The sensory experience (bristle texture, mint flavor, vibration) can be genuinely intolerable — not behavioral resistance.
Fix: Complete sensory desensitization: start with child touching toothbrush only. Next session: touching to lips. Next: inside lips. Build slowly toward teeth over 2–4 weeks.
Fix: Complete sensory desensitization: start with child touching toothbrush only. Next session: touching to lips. Next: inside lips. Build slowly toward teeth over 2–4 weeks.
⚠️ Toileting strip ignored; child still needs all prompts
Why: Environmental cues only work when child's attention is directed to them consistently — they don't work through passive exposure.
Fix: For 1 week, stand beside child and point to each step before they do it. Build the "look at strip" habit. Fade pointing as the habit forms.
Fix: For 1 week, stand beside child and point to each step before they do it. Build the "look at strip" habit. Fade pointing as the habit forms.
⚠️ First-Then board stopped working
Why: Reinforcer satiation — what was motivating last month may not motivate this month.
Fix: Survey the child's current preferences. Rotate reinforcers. Introduce choice: "Do you want [A] or [B] after brushing?" Novelty preserves motivational value.
Fix: Survey the child's current preferences. Rotate reinforcers. Introduce choice: "Do you want [A] or [B] after brushing?" Novelty preserves motivational value.

Adapt & Personalize
No two children need the same version of this technique.
Sensory Profile Adaptations
Sensory Seeker | Sensory Avoider | |
Weighted utensils preferred | Light-touch utensils preferred | |
Firm hand-over-hand guidance helpful | Hands-off guidance preferred | |
Textured toothbrush (more input) | Extra-soft toothbrush (less input) | |
Tight elastic waistband feels good | Tagless, seamless, loose clothing | |
Enjoys water play during handwashing | Minimal water; dry afterward quickly |
Profile-Based Priority Starters
DCD / Dyspraxia Profile
Start with visual task analysis + dressing board. Motor planning is the primary barrier.
Sensory Processing Profile
Start with adapted toothbrush + adaptive clothing. Sensory tolerance is the primary barrier.
ABA / Behavioral Profile
Start with First-Then boards + token economy. Motivation and task initiation are primary barriers.
Low Muscle Tone Profile
Start with adaptive utensils + built-up handles. Strength and grip are primary barriers.

Week 1–2 Progress
Tolerance & First Steps
15%
Progress Arc
Weeks 1–2: Tolerance and initial engagement forming
Indicator | What It Looks Like | |
📍 Reduced resistance | Child argues less about starting — not zero, just less | |
📍 Visual card attention | Child glances at the strip 2–3 times during routine instead of ignoring it | |
📍 Increased tolerance | Dressing board practice extends from 30 seconds to 2 minutes without meltdown | |
📍 First independent attempt | Child tries one step without being physically prompted — even if unsuccessful |
If your child sat with the materials for 3 minutes longer than last week — that is real, measurable neural pathway formation. Document it. The invisible work is happening.
Weeks 1–2 are the hardest for parents because they don't look like progress. But underneath: sensory pathways are adapting, motor memories are beginning to form, and negative associations with self-care tasks are being slowly replaced by neutral or positive ones.

Week 3–4 Progress
Neural Pathways Forming
40%
Progress Arc
Weeks 3–4: Consolidation and synaptic strengthening underway
Signal | Clinical Meaning | |
🔶 Child approaches task with less prompting | Anticipatory behavior — brain is pattern-matching | |
🔶 Child references visual card spontaneously | "Check the visual" behavior is becoming habitual | |
🔶 Morning routine time decreasing | Motor memory reducing planning load = faster execution | |
🔶 Child shows awareness of own success | "I did it!" or reduced frustration at attempts | |
🔶 First generalization signs | Using skill in new context (school, grandparent's house) |
Repeated structured practice over 3–4 weeks is when synaptic strengthening becomes measurable in pediatric populations. The motor sequence is moving from effortful, conscious execution to more automatic processing. Sessions may seem "easier" suddenly — not because the child changed, but because the neural architecture supporting the skill is more robust.
When to Increase Intensity (Week 3–4 Decision Point)
- ✅ Child completes 3+ successful trials with only visual prompts → increase complexity by one step
- ✅ Child initiates the task 2+ times without prompting → practice in a new setting
- ✅ Child is bored with current challenge level → "just-right challenge" signal to progress

Week 5–8 Progress
Mastery Unlocking
75%
Progress Arc
Weeks 5–8: Mastery criteria being met across domains
Domain | Mastery Indicator | |
Dressing | Selects clothing, dresses completely, manages all fasteners in wardrobe within 8 minutes | |
Feeding | Self-feeds complete meal with chosen utensil with <20% spillage | |
Oral Hygiene | Completes full brushing sequence independently using visual card, minimal adult verification | |
Toileting | Toilets independently with visual support, requests help only for hygiene confirmation | |
Grooming | Follows handwashing sequence independently to WHO standard (20-second scrub) |
What to Do at Mastery: Document and celebrate · Begin fading the visual support (remove last step from strip, then second-to-last) · Introduce one new skill within the same domain · Update GPT-OS® tracker with mastery status.
Celebrate This Win
You did this.
Your child grew because of your commitment.
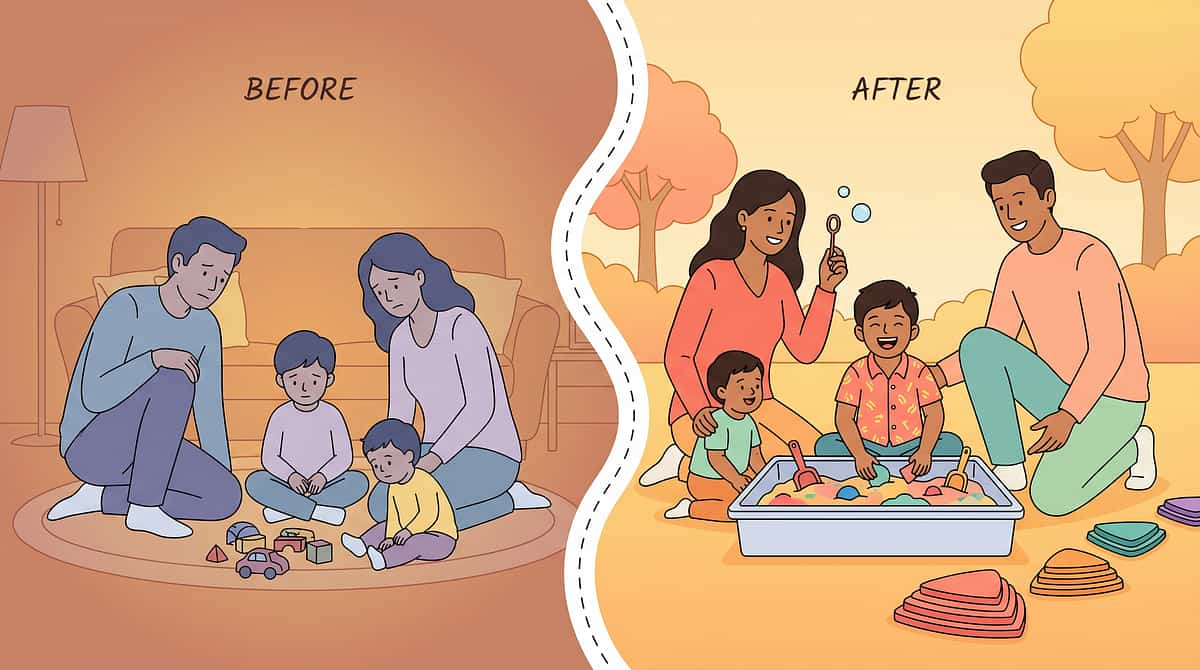
Five to eight weeks ago, you were doing everything for them. You buttoned their shirt, opened their lunchbox, wiped their mouth, brushed their teeth. Every morning was a negotiation with a child who wanted to do it themselves but couldn't — or who had stopped wanting to try.
And you kept going. You posted the visual cards. You assembled the dressing board. You sat beside them through the frustration and the failed attempts and the "I can't" moments.
These are not small victories. These are the foundation of a life of independence.

Red Flags — When to Pause
Even in the celebration zone — watch for these signals.
Flag | What It Looks Like | What It Might Mean | |
Regression after mastery | Skill previously mastered is no longer performed | Medical event, anxiety increase, sensory change, or environmental disruption | |
Intensifying sensory aversion | What was tolerated now causes severe distress | Sensory processing may have shifted; OT reassessment needed | |
Self-harm during self-care | Child harms self when unable to complete task | Frustration has exceeded capacity; intervention redesign required | |
Skill ceiling | No progress across 8+ weeks despite consistent practice | Underlying motor/sensory barrier may need clinical assessment | |
Extreme oral sensitivity | Toothbrushing remains impossible after desensitization protocol | Dental OT referral needed; possible oral hypersensitivity | |
Toileting withholding | Child is withholding bowel movements as result of toileting program | Pause all toileting work; medical consultation before resuming |
"Trust your instincts. If something feels wrong about how your child is responding, pause and ask. You know your child. We know the science. Together we protect them."
Your Progression Pathway
You are not done. You are at a waypoint.
If your child mastered... | Next priority is... | Technique | |
Dressing + toileting | Feeding independence | L-980 | |
Dressing + feeding | Grooming/hygiene | L-981 | |
All ADLs at home | Generalization to school | Contact Pinnacle for IEP support | |
All ADLs | Fine motor advancement | Domain K (Fine Motor) |
Related Cross-Domain Techniques: K-850 (Fine Motor Development) and K-851 (Motor Planning Foundations) feed directly into ADL work — prerequisite skills that accelerate everything on this page.
Related Techniques
More techniques in your child's independence journey
L-977 — Morning Routine Independence
🟡 Core
Uses Core Visual Supports from this page


Your Child's Full Developmental Map
One technique. One domain. One piece of a 12-domain life.
Your child's self-help skill development is not isolated. It feeds into and draws from every other domain:
Domain K → L
Fine motor progress enables fastener mastery → ADL independence
Domain A → L
Sensory processing gains reduce grooming aversion → ADL tolerance
Domain B → L
Communication growth enables "I need help" requests → ADL safety
Domain C → L
Emotional regulation reduces self-care meltdowns → ADL persistence
📞 Request a Full Developmental Assessment: 9100 181 181 | pinnacleblooms.org
Preview of 9 materials that help with self help skills Therapy Material
Below is a visual preview of 9 materials that help with self help skills therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!
Real Families · Real Independence
Documented at Pinnacle centers across India.
Arjun, Age 7 — Hyderabad
Before: Arjun's mother dressed him completely every morning. He required full physical assistance for toileting hygiene, brushing teeth, and eating breakfast with utensils. He was academically advanced but needed an aide for every self-care task at school. The gap between his cognitive ability and his functional independence was causing visible distress — he knew he was different from his peers.
Approach: Pinnacle OT designed task analysis cards for all morning routine steps, a dressing board for fastener practice, and an adaptive utensil kit. His ABA team implemented a token economy for morning routine completion.
After 11 weeks: Arjun dresses himself in approximately 9 minutes with visual card support. He brushes his teeth using the sequence strip. He self-feeds breakfast independently with an adaptive fork. The aide at school no longer assists him with toileting or feeding.
"I never thought I'd hear 'Mom, I did it myself!' about a shirt button. That was the day I cried the good kind of tears." — Arjun's mother
Meera, Age 5 — Bangalore
Before: Meera had such severe tactile sensitivities that toothbrushing was impossible — she would gag, scream, and physically fight any attempt. Her oral hygiene was a genuine medical concern. Dressing required over 45 minutes each morning due to sensory aversions and her difficulty managing elastic waistbands.
Approach: Sensory desensitization protocol with soft-bristle toothbrush; tagless adaptive clothing; backward chaining for dressing with visual support.
After 8 weeks: Meera tolerates toothbrushing with a soft-bristle brush for the full two minutes. Dressing is completed in 15 minutes with minimal assistance. She can pull her own elastic-waist pants on and off independently — critical for school toileting.
"It took eight weeks to go from me holding her down to brush her teeth to her standing at the sink doing it herself. Eight weeks changed her life." — Meera's mother