
Room Full of Toys. Still Says "I'm Bored."
Self-entertainment is not about having enough toys. It is a skill — involving ideation, initiation, and sustained engagement.
🌸 Pinnacle Blooms Consortium
G-629 | Play Development
Ages 3–12

"My son is seven. He cannot entertain himself. Not for five minutes. Not even two. The moment I step away — to cook, to use the bathroom — he's right there. 'Mommy, what should I do?' He has a room full of Legos, puzzles, books, art supplies. He won't touch any of it unless I'm sitting right there with him. If I say 'Go play,' he just stands there looking lost. His four-year-old sister disappears into her room for an hour. He can't do that. Is this anxiety? Is this something he never learned? Is something wrong with him — or with me?"
You are not failing. Your child's nervous system is learning a skill it simply hasn't mastered yet.
This experience is more common than most parents realize. What looks like defiance or disinterest is almost always a genuine developmental skill gap — one that responds beautifully to the right structured support. G-629 is built exactly for this moment.
🌸Pinnacle Blooms Consortium | G-629 | Play Development Domain | Ages 3–12 — Episode 629 of the Social-Emotional & Play Development Series. WHO Nurturing Care Framework (2018): Parental awareness and early identification directly determine developmental outcomes.
You Are Among Millions of Families Navigating This Exact Challenge
1in36
Children with Autism
In India are on the autism spectrum — independent play skills are a core challenge (CDC ADDM 2023; INCLEN 2021).
80%
Children with ADHD
Struggle with self-initiated, sustained independent engagement, according to a 2024 PRISMA Systematic Review (PMC11506176).
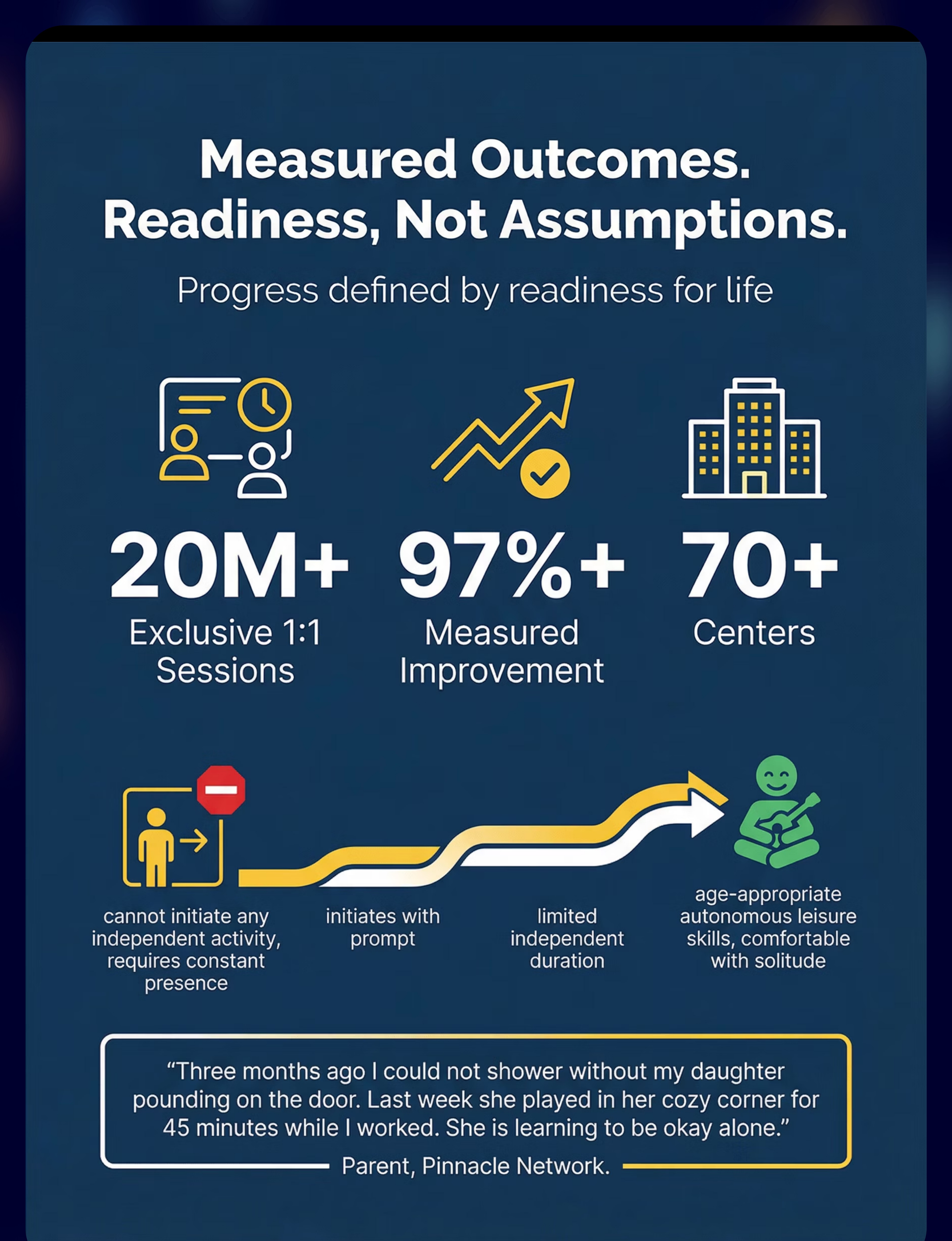
20M+
Therapy Sessions
Delivered by Pinnacle Blooms Network® — informing these evidence-based strategies across 70+ countries.
Self-entertainment is the capacity to occupy oneself meaningfully without adult direction. It is not a personality trait — it is a developmental skill built from five underlying capacities: ideation (thinking of what to do), initiation (starting without a prompt), sustained attention (staying engaged), emotional regulation (tolerating aloneness), and intrinsic motivation (finding satisfaction in solo activity). When children struggle here, one or more of these capacities is underdeveloped. This is not parental failure. This is a skill gap — and skill gaps can be addressed with the right tools.
🌍 Across 70+ countries, Pinnacle GPT-OS® has measured this exact challenge in children aged 3–12. It is among the top 10 most-reported parental concerns in our network — and among the most addressable.
Self-Entertainment Across Development: A WHO/UNICEF Milestone Map
1–2 Years
Solitary play with parent visible nearby. Foundation stage. 15–30 min baseline.
3–4 Years
Play with check-ins in familiar space. Building stage. 30–45 min target.
5–6 Years
Independent in self-selected activities. Consolidating stage. 45–60+ min.
7–9 Years ★
TARGET ZONE. Extended hours — autonomous leisure with occasional check-ins.
10–12 Years
Mastery. Full autonomous leisure across settings and activities.
⭐If your child is 7–12 and functioning at the 1–2 year zone, this is not a crisis — it is a skill gap. The same neural pathways that typical children build through natural play experience can be built through structured support. This is what the 9 materials in this guide address.
ADHD
Initiation + sustained attention difficulties are neurological
Autism Spectrum
Ideation + flexibility across activities
Anxiety
Tolerance of aloneness + self-regulation
Dev. Delays
Match activities to developmental (not chronological) age
WHO Care for Child Development (CCD) Package: Age-specific evidence-based caregiver guidance implemented in 54 low- and middle-income countries. | UNICEF MICS indicators for developmental monitoring across 197 countries. PMC9978394

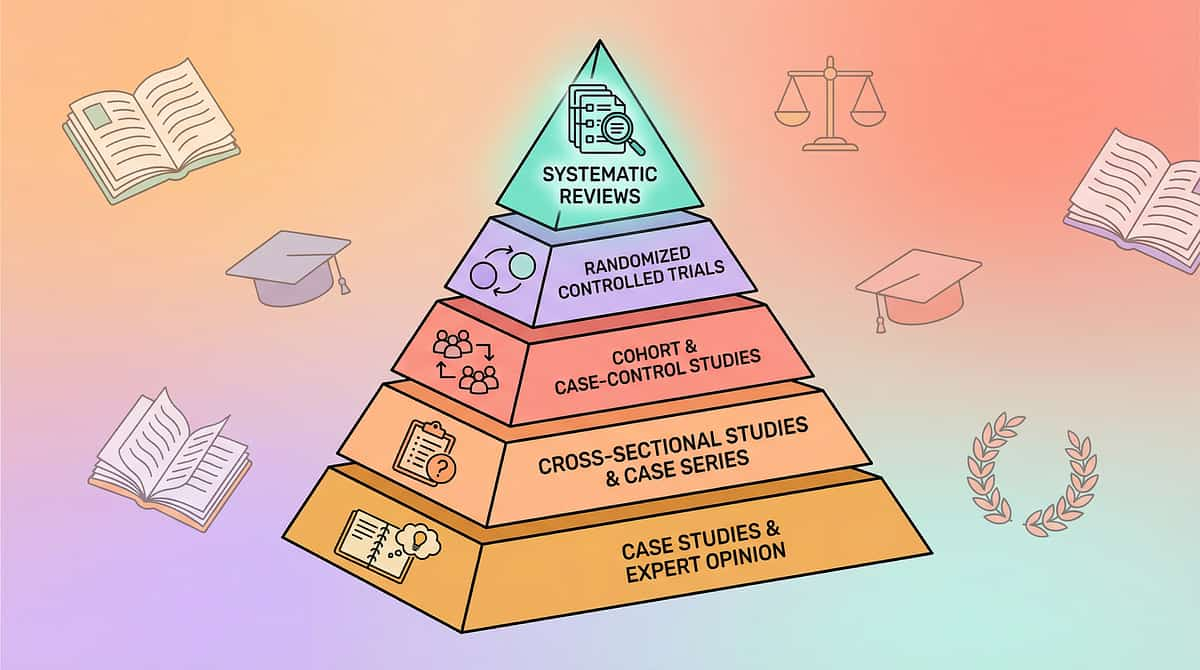
The Evidence Behind This Approach
⬡ LEVEL II EVIDENCE
Systematic Review + RCT
Clinically Validated
Home-Applicable
📚 Systematic Review (2024)
16 peer-reviewed articles (2013–2023) confirm structured material-based interventions for independent play meet evidence-based practice criteria. Effect sizes moderate to large for initiation and sustained engagement outcomes. PMC11506176
📚 Meta-Analysis (2024)
24 studies confirm structured play interventions promote social skills, adaptive behavior, and sustained engagement capacity in pediatric populations. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
📚 Indian RCT (2019)
Home-based structured interventions by trained parents demonstrated significant outcomes comparable to clinic-based delivery. Parent-as-therapist model validated for India-specific populations. Padmanabha et al., Indian J Pediatr | DOI: 10.1007/s12098-018-2747-4
📚 WHO/UNICEF (2023)
Care for Child Development package: structured caregiver-delivered activities improve developmental outcomes across 54 LMICs. Home environment quality is the strongest predictor of independent skill development. PMC9978394
Clinically validated. Home-applicable. Parent-proven. 20M+ sessions. 97%+ measured improvement.

G-629 | 9 Materials That Help With Self-Entertainment
🎯 Play Development
🧠 Executive Function
🕐 Ages 3–12
⏱ 10–45 min daily
🏠 Home-primary
Self-entertainment (also: independent play, solitary play, self-directed leisure) is the capacity to engage oneself in meaningful, satisfying activity without external direction or constant adult companionship. It is not about having the right toys. It requires five underlying skills working together:
Ideation
Thinking of what to do — generating an activity idea without adult suggestion
Initiation
Starting without being told — overcoming the inertia of beginning
Sustained Attention
Continuing when it gets boring — tolerating the dip in engagement
Emotional Regulation
Tolerating the experience of being alone — felt safety in solitude
Intrinsic Motivation
Finding satisfaction in the activity itself — internal reward independent of external praise
💬"This is the guide for parents whose child stands in a room full of toys and says 'I'm bored.' It's not about the toys — it's about building the skill to use them alone."
The Pinnacle Consortium Multi-Discipline Approach
"The brain doesn't organize by therapy type — and neither do we."
🟠 Occupational Therapy — Primary Lead
OTs assess sensory, motor, and executive function barriers to independent play. They prescribe specific material types, session structure, and environmental modifications. For G-629, OT designs the activity bin system, play space setup, and sensory regulation supports.
🟣 Applied Behavior Analysis (ABA/BCBA)
BCBAs build the reinforcement architecture — defining what earns rewards, shaping independent play duration from 2 to 45 minutes, and fading external motivation as intrinsic satisfaction develops. Token economy and prompt-fading protocols are ABA contributions.
🔵 Special Education (SpEd)
Special educators design visual supports — activity menus, choice boards, visual schedules — that make the "what to do" question answerable without adult input. They also build academic and pre-academic activities within the independent play repertoire.
🟢 NeuroDev Pediatrics
NeuroDev doctors evaluate and manage underlying ADHD, anxiety, or developmental conditions creating the neurological basis for self-entertainment challenges. Medication management and developmental monitoring are NeuroDev contributions.
🌸Validated by the Pinnacle Blooms Network® Multi-Disciplinary Consortium — CRO | OT | SLP | ABA | SpEd | NeuroDev | WHO/UNICEF-Aligned
Precision Targets: What Each Layer of This Intervention Addresses
Each layer of G-629 addresses a different dimension of the self-entertainment skill chain. The bullseye model ensures no barrier is left unaddressed — from the moment of initiation at the core, out to long-term life independence at the periphery.
Target | Currently Absent | Emerging | Developing | Mastered | |
Initiation | Cannot start without adult | Starts with visual prompt | Starts independently from bin | Generates own play ideas | |
Duration | Abandons in under 1 min | 2–5 min with support | 10–20 min structured | 30–60+ min flexible | |
Ideation | "I don't know what to do" | Uses choice board | Selects from menu | Generates novel ideas | |
Regulation | Distress when alone | Tolerates 2–3 min | Comfortable 10–15 min | Comfortable extended time |
Meta-analysis (World J Clin Cases, 2024): Structured play interventions promote adaptive behavior, social skills, sensory processing, and motor skills across 24 studies. | PMC10955541
Materials 1–3: Ideation & Initiation Foundations

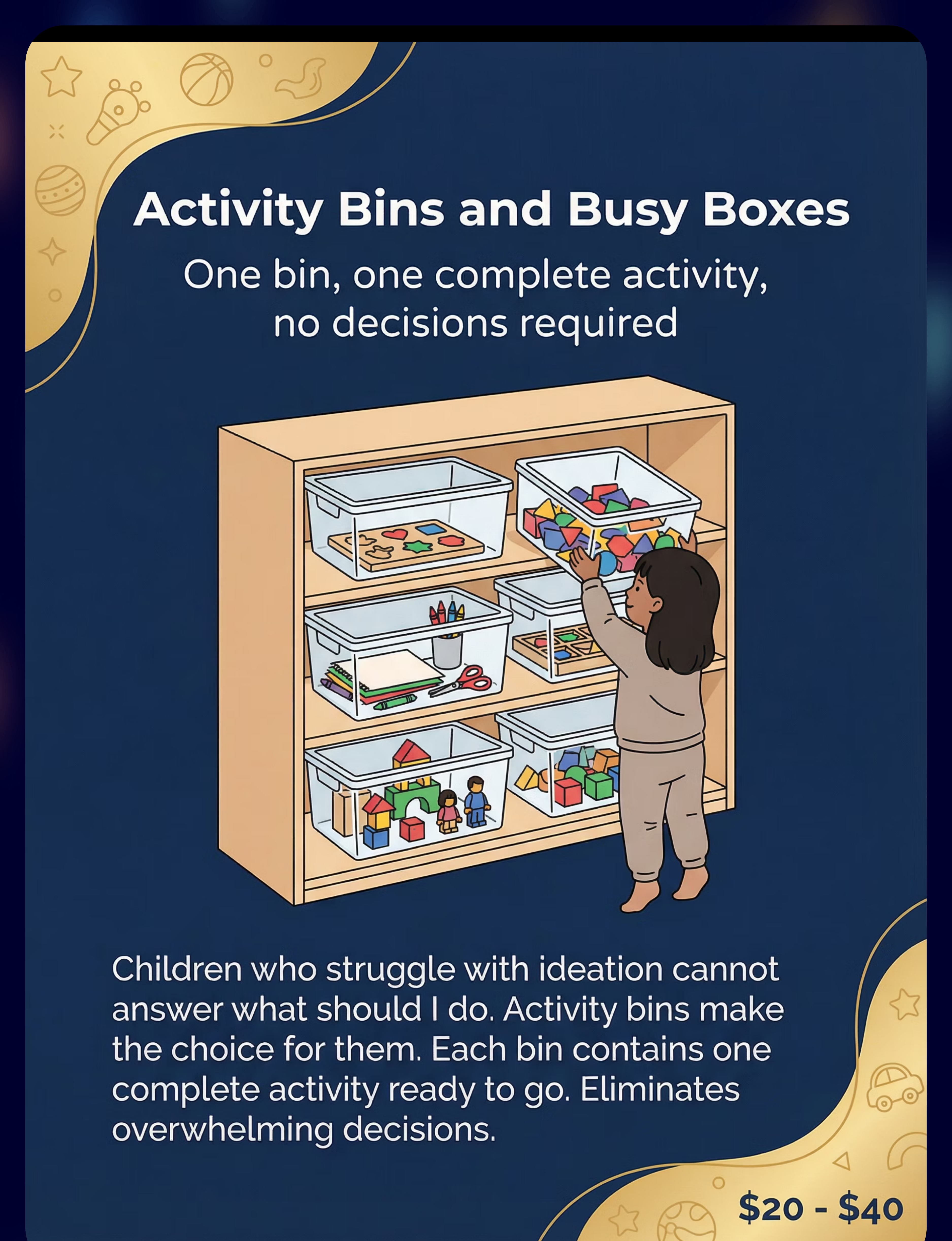
Material 1 — Activity Bins & Busy Boxes
🎯Eliminates ideation barrier — one bin = one complete activity. Clear lidded containers, each pre-loaded with one complete activity (puzzle, art supplies, building set). Child picks a bin. The decision is made. The question "What should I do?" has a physical answer.
Price: ₹200–1,000 (bins) + activity contents | Category: Problem-Solving Toys / Sorting Activities
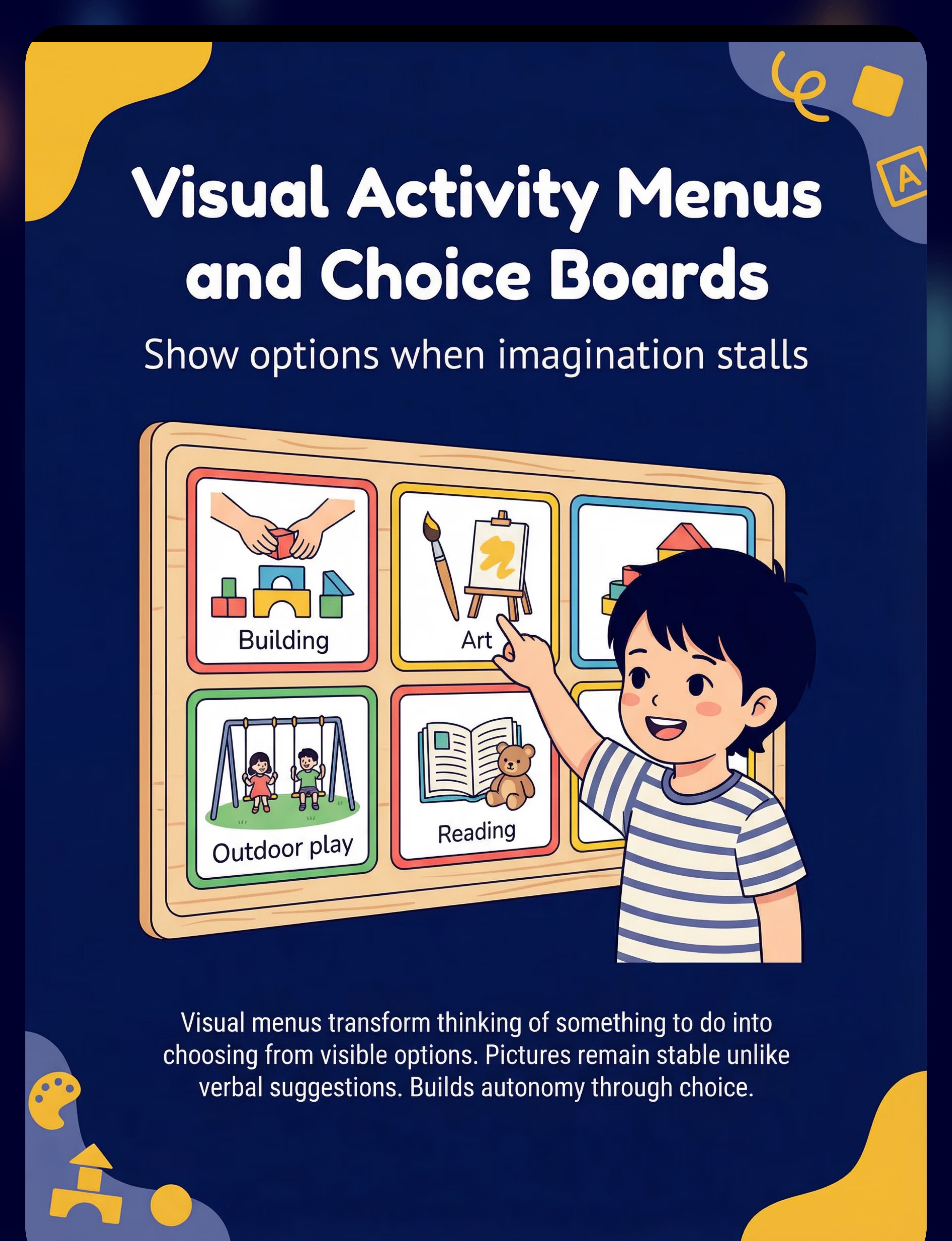
Material 2 — Visual Activity Menus & Choice Boards
🎯Externalizes ideation — shows options when imagination stalls. Picture-based boards showing 8–10 activity options. Transforms "thinking of something to do" (abstract) into "pointing to something to do" (concrete). Essential for children with autism, ADHD, and language delays.
Price: ₹100–500 | Category: Matching Games / Visual Support Materials

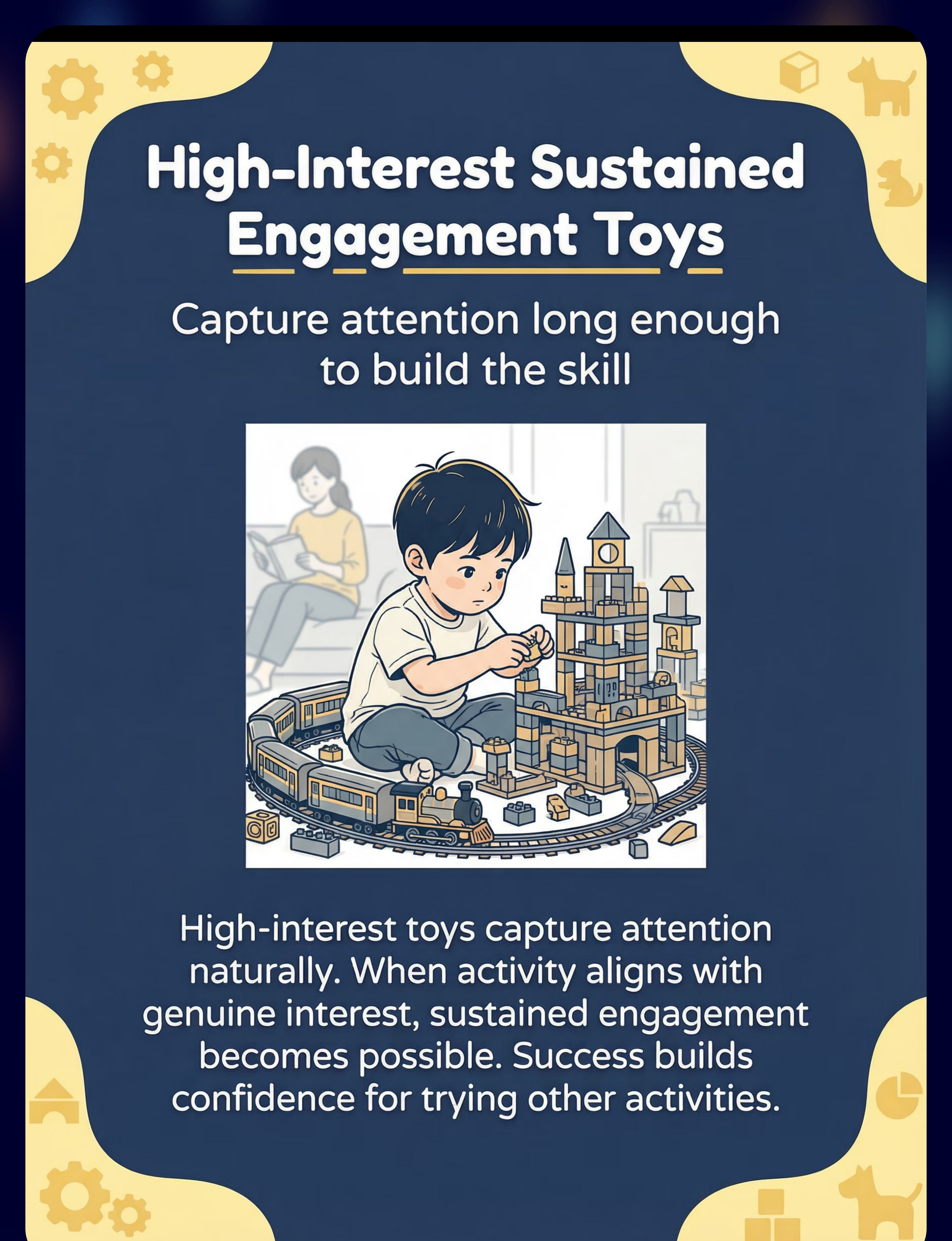
Material 3 — High-Interest Sustained Engagement Toys
🎯Leverages intrinsic motivation — attention follows genuine interest. NOT "good toys in general" — items specifically matched to YOUR child's special interest. Trains, Lego, animals, art supplies calibrated to their specific fascination. When activity aligns with interest, sustained engagement becomes neurologically possible.
Price: ₹500–5,000 (varies by interest)

Materials 4–6: Time, Regulation & Creativity

Material 4 — Independent Play Timers & Visual Schedules
🎯Makes "how long" visible — transforms undefined alone-time into a finite, predictable experience. Visual countdown timers (Time Timer or similar) show remaining time as a shrinking color segment. "Play until the timer shows green" is survivable. "Go play alone" (undefined duration) is not — especially for anxious children.
Price: ₹500–2,500 | Active Pinnacle Product: Reinforcement Menu Set — ₹589 (supports reward + timer integration)
Material 5 — Sensory & Fidget Tools for Self-Regulation
🎯Regulates first — engagement becomes possible only when the nervous system is settled. Fidget toys, weighted lap pads, chew tools, wiggle cushions. For children who cannot engage because they cannot regulate, these tools meet nervous system needs so attention can land on activity.
Price: ₹200–1,500

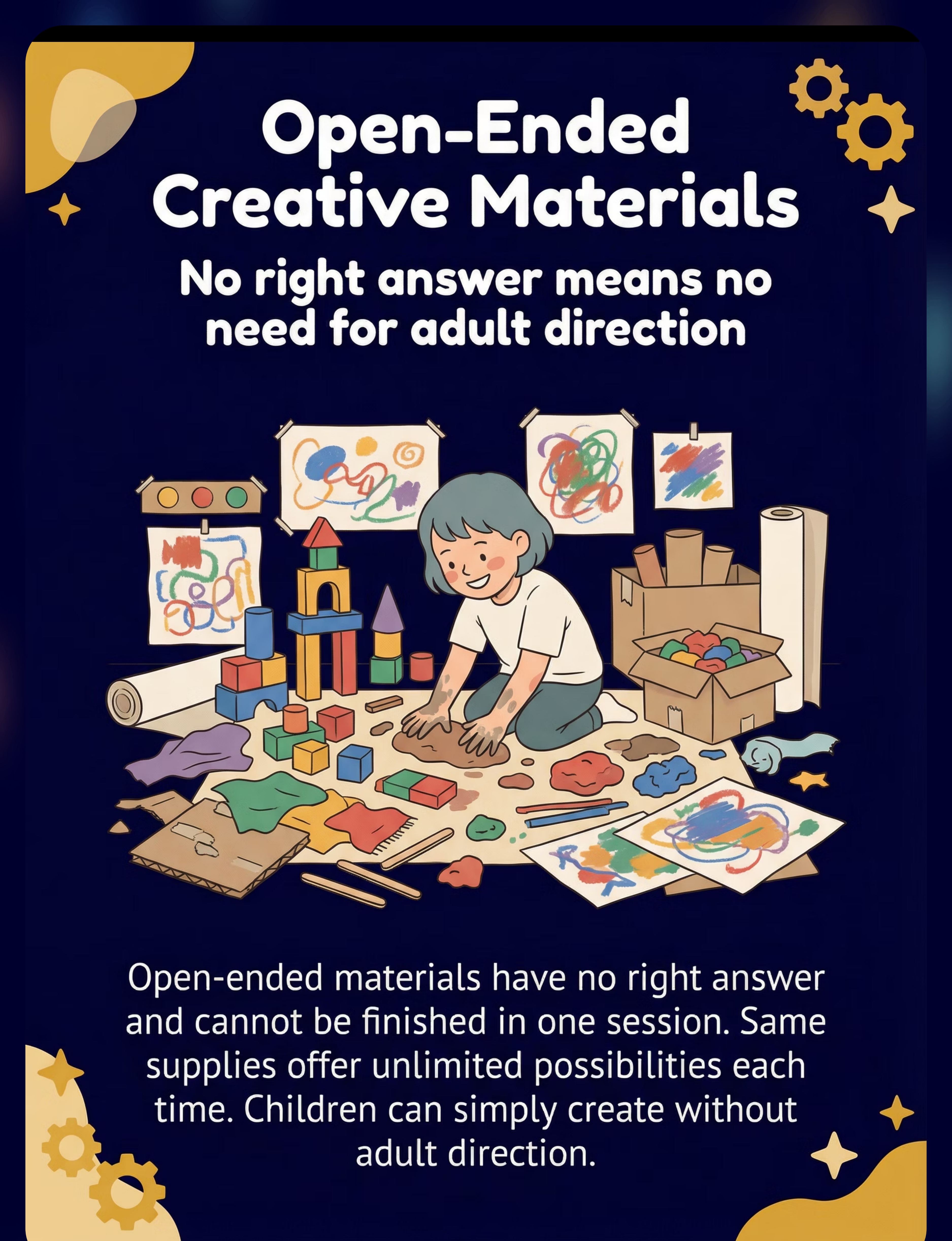
Material 6 — Open-Ended Creative Materials
🎯No right answer = no adult needed to give the right answer. Art supplies, blocks, loose parts, play dough. These have no "finish" and no "wrong answer" — children can just make things without instruction, goal, or adult direction. Renewably engaging session after session.
Price: ₹300–2,000
Materials 7–9: Audio, Space & Reward

Material 7 — Audiobooks & Music Players with Child Control
🎯Fills silence without screens — audio companionship children control themselves. Simple child-operated audio players, story cubes, or controlled tablets in audio-only mode. Reduces anxiety of aloneness. Pairs with any physical activity. Builds sustained attention through narrative engagement.
Price: ₹1,000–4,000

Material 8 — Cozy Independent Play Space Design
🎯Environment communicates "you can be here alone" — architectural support for internal self-direction. A defined, contained, comfortable play corner, tent, or nook. Low shelving for bins, floor cushions, soft lighting. The space becomes a cue: "When I'm here, I play independently."
Price: ₹1,000–5,000 (wide range, fully DIY possible)

Material 9 — Reward Systems & Reinforcement Tools
🎯External motivation while intrinsic satisfaction develops — temporary scaffolding, not permanent management. Token boards, sticker charts, marble jars. Provide external motivation while children discover that independent play can be satisfying on its own. Evidence-based ABA reinforcement principles.
Price: ₹100–500 | Active Pinnacle Product: Reinforcement Menu Set — ₹589
GPT-OS® Canon Material Classification: 128 clinically validated material categories across 12 developmental domains. Product database sourced from 20M+ session evidence base.

Every Material Has a ₹0 Version — WHO/UNICEF Equity Principle in Action
"No family should be unable to support their child's development because of cost. Every technique here has a complete household-item version that works on the same therapeutic principle." — Pinnacle Blooms Consortium Clinical Team
Material | Buy This | Make This (₹0) | Same Principle | |
Activity Bins | Clear lidded containers ₹200–500 | Old dabbas, shoe boxes, plastic bags | One container = one activity, decision removed | |
Visual Menu | Printed choice board ₹100–300 | Photos of toys on paper, drawn pictures | Pictures stable, verbal suggestions disappear | |
Visual Timer | Time Timer ₹800–2,000 | Kitchen timer (sound only), phone timer app (free) | Makes duration visible and finite | |
Sensory Fidget | Commercial fidget set ₹300–800 | Rolled sock, dry rice in sealed bag, rubber band on wrist | Hands occupied, regulatory input delivered | |
Creative Materials | Art supply set ₹500–1,000 | Pencil + old newspaper, mud/sand outdoors, sticks and stones | Open-ended, no right answer, no adult needed | |
Play Space | Play tent ₹1,500–3,000 | Corner defined by furniture, sheet over table, rug boundary | Spatial cue: "I can be here alone" | |
Reward System | Token board ₹200–500 | Stones in a jar, drawn sticker chart, pasta pieces | Visual progress, immediate reinforcement |
🌍This guide works in Mumbai apartments and rural Telangana villages. The therapeutic principle — not the product price — drives outcomes. Pinnacle serves families across all economic contexts. WHO Nurturing Care Framework (2018) | CCD Package implementation across 54 LMICs | PMC9978394

⚠️ Pre-Session Safety Gate — Read Before Every Session
🔴 RED — Do Not Proceed If:
- Child is in active meltdown, severe distress, or post-seizure state
- Child is unwell, overtired, or significantly hypoglycemic
- Materials contain small parts and child is under 3 or mouthing is present — substitute age-appropriate alternatives
- Child has known latex allergy — avoid latex fidgets and rubber bands
- Play space is not childproofed (sharp furniture edges, unstable shelving, electrical hazards)
🟡 AMBER — Modify Session If:
- Child is mildly irritable or had a difficult day — reduce duration, increase support
- Child is over-excited (very high arousal) — use calming sensory input first, then proceed
- New material being introduced — present passively first, no demands for 1–2 sessions
- Sibling present and creating distraction — either include or separate spaces
🟢 GREEN — Proceed When:
- Child is calm, alert, and fed (not hungry)
- Space is prepared and materials accessible
- Parent is patient and unhurried — sessions scheduled for low-pressure time windows
- Visual supports are in place and child understands the routine
🛑STOP IF YOU SEE: Self-injurious behavior escalating during the session | Child severely dysregulated (aggression, panic, inconsolable distress) | Signs of physical discomfort (choking, allergic response, fall). Indian Journal of Pediatrics RCT (2019) | DOI: 10.1007/s12098-018-2747-4

The Independent Play Space Setup — Before the Session Begins
Define the Play Zone
Corner, rug, tent, or nook. Child-specific, not general family space. The physical boundary creates psychological safety.
Place Activity Bins at Child Height
Accessible without adult help. 4–6 bins visible, others in rotation storage. Accessibility removes all friction from the ideation-to-action loop.
Post Visual Activity Menu at Eye Level
In the play zone. Pictured options only. Menu must be visible from child's seated play position.
Place Visual Timer — Pre-Set Short
Visible from play position. Start SHORT — 2–3 minutes for new users. The defined endpoint makes aloneness survivable.
Remove Primary Distractions
TV off, screens away from play zone. Minimize sibling access initially. A clear environment supports a clear mind.
Parent Positions 2–5 Meters Away
Visible to child but engaged in a separate task. Do not hover. Your visible calm is the child's regulatory anchor.
Space Notes: Natural light preferred. Warm LED for reading/art areas. Quiet preferred initially — no TV or screen audio competing. Comfortable temperature — neither too warm (drowsy) nor too cold (distracting). Sensory Integration Theory (Ayres) | PMC10955541

The 60-Second Pre-Session Assessment
"The best session is one that starts right."
Check | Yes → | No → | |
✅ Fed within the last 2 hours? | Proceed | Feed first, wait 20 min | |
✅ Slept adequately last night? | Proceed | Reduce duration by half | |
✅ Calm or mildly alert (not over-excited)? | Proceed | Sensory cool-down first | |
✅ No active illness or pain indicators? | Proceed | Postpone to next session | |
✅ No meltdown in last 30 minutes? | Proceed | Postpone — recovery time needed | |
✅ Play space is set up and ready? | Proceed | Set up first (Card 12) | |
✅ Parent is patient and unhurried? | Proceed | Reschedule — parent state transfers to child |
🟢 6–7 Checks
GO — Proceed to the Invitation step
🟡 4–5 Checks
MODIFY — Shorter session, more support, parent stays closer
🔴 0–3 Checks
POSTPONE — Do a calming activity instead, try again in 2–4 hours
ABA Antecedent Manipulation Principles: Setting events and pre-session conditions are the strongest predictors of session outcome quality.
Step 01 of 06 — The Invitation
ACT III: Execution
Duration: 30–60 seconds
Style: Playful, low-demand
The Principle: Every independent play session begins with an invitation, not a command. "Go play" is a command with no structure. The invitation opens a door without pushing the child through it.
💬 "Hey [child's name], I set up your play corner! Your [favorite material] is in your bin. The timer is ready — it's just [X] minutes. When the timer ends, I'll come see what you made. I'll be right here [gesture toward parent zone]."
Body Language That Works
- Get to child's physical level (crouch or sit)
- Warm smile, relaxed face — your regulation is their regulator
- Walk WITH child to the play space for the first weeks
- Do NOT follow them in — point from the doorway
When Resistance Appears
Child says "I don't want to" or begins to follow you. Response: "I know it feels hard to start. Let's just pick ONE bin together." Offer choice of 2 bins. Then EXIT. Resistance is information — not failure.
ABA Pairing Procedures: Establishing motivating operations before demand placement. OT "Just-Right Challenge" principle: matching task demand to current capacity.

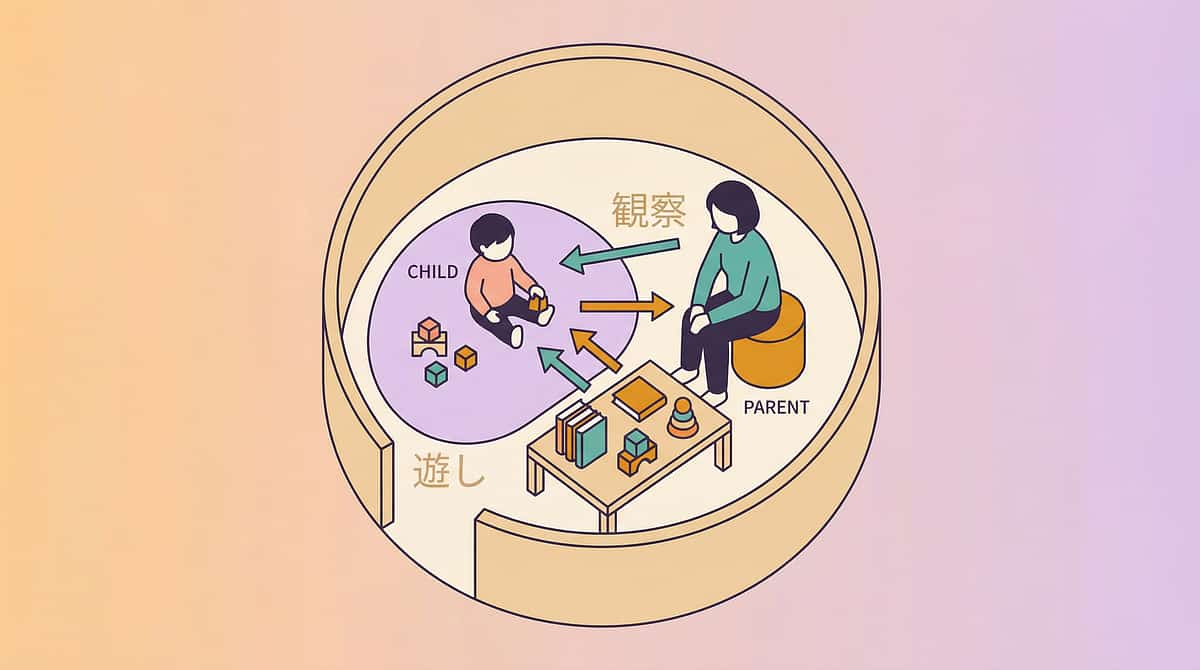
Step 02 of 06 — The Engagement
Duration: 1–3 minutes
Observe from distance. Intervene minimally.
The Principle: The child is now in the play space. Your job is to NOT join, NOT redirect, NOT ask "What are you making?" The presence of your observation — without intervention — teaches the child that independent play is possible even when you're watching.
Child focuses 60+ seconds
Full engagement. Stay in your zone — do nothing. This is the skill building in real time.
Child glances toward parent
Checking safety. Make brief eye contact, smile, look away — do NOT call out. Brief eye contact = "You're safe."
Child appears "stuck" (looking around)
Menu needed. Wait 30 seconds. If no movement, silently point to activity menu. No words — gesture only.
Child brings activity to parent
Seeking attention. Admire briefly (10 seconds), redirect: "Can you take that back to your corner and keep going?"
Parent Protocol During This Phase: Engage in your own task (phone, book, cooking from kitchen doorway) — visibly busy. Resist the urge to comment. Allow the bin to be "wrong" or "boring" — frustration tolerance builds through managed frustration, not rescue. Systematic review (Children, 2024) | PMC11506176

Step 03 of 06 — The Therapeutic Action
Duration: 2–15 minutes (timer-dependent)
The Active Therapeutic Window
This is the phase where independent play actually HAPPENS. The child engages with material, the timer counts down, and the skill of self-entertainment is being built — repetition by repetition, session by session, minute by minute. Each minute of independent engagement is a neural repetition strengthening the initiation and attention circuits.
If Primary Barrier Is... | Lead With This Material | |
"I don't know what to do" (ideation) | Activity Bins + Visual Menu | |
"I won't start" (initiation) | High-Interest Toy + Reward System | |
"I can't stay" (attention) | Visual Timer + Sensory Tool | |
"I'm scared to be alone" (regulation) | Audiobook + Cozy Space | |
"It's not worth it" (motivation) | Reward System + High-Interest Toy |
Week 1–2
2–3 minutes independent
Week 3–4
5–7 minutes independent
Week 5–8
10–15 minutes independent
Month 3+
20–45 minutes as skill develops
Meta-analysis (2024): 40-minute therapy sessions show maximum effectiveness. Home sessions 10–20 minutes; core active engagement occupies 40–60% of session time. | PMC10955541

Step 04 of 06 — Repeat & Vary
Across sessions, not within a session
Dosage Principle
The Principle: Therapeutic skill-building requires repetition. Daily short sessions beat weekly long sessions. The variation principle prevents satiation — the same bin feels fresh after a week away. Five sessions of 5 minutes is more therapeutically valuable than one session of 25 minutes.
Daily Practice
Standard dosage — even 5 minutes on school days counts toward skill consolidation
Weekend Long Sessions
Aim for current maximum tolerance + 2 minutes to gently advance the baseline
Skip Protocol
If 3 consecutive days missed, restart at shorter duration. Never treat a miss as failure — restart gently
Strategy | How It Works | |
Bin Rotation | 15–20 bins total, only 4–5 visible at a time, rotate weekly. Same bins feel new after 2 weeks away. | |
Menu Refresh | Update activity menu monthly. Photograph new activities, retire overdone ones. | |
Theme Days | "Train Tuesday" (special interest), "Art Thursday" (open-ended), "Build Saturday" (construction). | |
Novelty Injection | Once per week, introduce one new material — place it in play space before child wakes up. |
Sensory integration therapy dosage research: 2–3 sessions per week for 8–12 weeks as clinical standard. | General SI literature

Step 05 of 06 — Reinforce & Celebrate
⭐ Most Powerful Moment
Timing: Within 10 seconds of timer completing
The ABA Principle: The reinforcement delivers the message: "Being alone and playing independently was worth it." The timing, specificity, and warmth of this moment determines whether the behavior repeats. This single step is the most powerful in the entire protocol.
💬 "[Child's name], YES! You played all by yourself for [X] minutes! I saw you working with your [activity]. That was AMAZING independent play. Here's your [token/sticker/marble] — AND I am so proud of you."
Within 10 Seconds
Not 2 minutes later when you've finished your task. Timing is everything in behavioral reinforcement.
Be Specific
Name what they did: "I saw you building the whole tower alone." Specificity amplifies the impact of praise.
Be Enthusiastic
Your genuine joy is the primary reinforcer. Children read emotional authenticity immediately.
Token + Verbal Together
Both together while skill is building. Token fades later; verbal praise continues always.
Celebrate the Attempt, Not Just the Success: If the child managed 1 minute when the timer was set for 3 minutes — that is still reinforceable. "You tried! You stayed for 1 whole minute! Tomorrow we'll try 2." ABA Reinforcement Principles | BACB Ethical Guidelines
Step 06 of 06 — The Cool-Down
Duration: 2–3 minutes
Closes the Session Properly
The Principle: No session ends abruptly. The cool-down transitions the child from independent play back to family engagement, reinforces the routine structure, and prevents the "abandonment" feeling that can undermine next session buy-in.
Resisting the Ending
Child says "No, I want to keep playing!" — This is actually positive (independent play was enjoyable). Response: "I love that you want to keep going! We'll do it again tomorrow. For now, [transition to next activity]."
Post-Session Parent Check-In (30 seconds)
Ask yourself: What worked? What struggled? Adjust tomorrow's session accordingly — shorter, longer, different bin, different timer setting. Micro-adjustments compound over weeks.
Visual timer and transition support: Visual supports classified as evidence-based practice for autism (NCAEP Evidence-Based Practices Report, 2020).

60 Seconds of Data Now Saves Hours of Guessing Later
Data Point | How to Record | Example | |
Duration | Minutes of independent engagement before seeking parent | "7 minutes" | |
Prompt Level | 0 = Independent | 1 = Visual prompt only | 2 = Verbal | 3 = Physical | "Level 1 — pointed to menu" | |
Material Used | Which bin/activity led the session | "Puzzle bin + timer" | |
Regulation Quality | 1 (distressed) → 5 (calm and engaged) | "Rating 4 — one check-in glance at 3 min" | |
Termination | Self-ended / Timer ended / Parent ended / Distress ended | "Timer ended — child wanted to continue" |
📊 GPT-OS® Digital Tracker
Log today's session in the GPT-OS® Parent Dashboard — tracks progress curves, flags regression, celebrates milestones across your child's full profile.
⬇️ Printable PDF Tracker
Download the G-629 Home Tracking Sheet — 8-week printable tracker with visual progress graph. No device required.
ABA Data Collection Standards: Continuous measurement (frequency, duration) as standard behavioral intervention practice. | BACB Guidelines + Cooper, Heron & Heward (ABA, 8th Ed.)

Session Abandonment Is Not Failure — It's Data
"Most sessions don't go perfectly in weeks 1–4. This card addresses the 7 most common challenges for G-629."
❌ Child Immediately Followed Me Out of the Play Space
Why: The independent play routine is not yet established. The habit of following is stronger than the new instruction. Fix: Decrease timer to 1 minute. Walk child back silently. Try 5 times in one day — repetition builds the routine. Use physical boundary (baby gate) if needed in early weeks.
❌ Child Ignored the Visual Menu and Said "I Don't Know"
Why: Choice board images don't yet have meaning, or there are too many options. Fix: Reduce to 3 options maximum. Use photos of YOUR CHILD'S actual toys (not stock images). Point to each with child until one gets a reaction. Use hand-over-hand to help with first selection.
❌ Child Played 2 Minutes Then Screamed When Timer Ended
Why: Abrupt transition without warning. Timer ending = loss of something enjoyable. Fix: Give a 1-minute warning before timer ends. Celebrate this as success: "You played for 2 minutes AND you loved it — that's amazing!"
❌ Child Destroyed the Play Space or Threw Materials
Why: Frustration from activity being too hard, OR dysregulation during alone time. Fix: Simplify activities in bins. Add sensory regulation support before session. Reduce duration to 1 minute. Clean up together without punishment.
❌ Child Cried the Entire Session, Clearly Distressed
Why: Anxiety about separation — being alone feels genuinely unsafe to this child. Fix: Back up significantly. Start with parent INSIDE the play space, gradually moving out over weeks. Consider referral to anxiety-focused therapy alongside this technique.
❌ Child Only Wanted One Bin and Refused All Others
Why: This is actually progress — the child is engaging! Restricted preference is normal early behavior. Fix: Honor this for now. Use the preferred bin as the foundation. Introduce ONE new bin per week alongside the preferred one.
❌ Everything Worked at Home but Not at Grandparent's House
Why: The skill is not yet generalized across environments. It's learned in one context. Fix: Share the Family Guide (Card 37) with grandparents. Recreate the identical setup — same bins, same timer, same space — at the new location. Generalization follows environmental similarity.
ABA Troubleshooting: Functional analysis principles applied to session-level problem solving. Antecedent modification strategies from behavioral literature.

No Two Children Are Identical — Calibrate to YOUR Child
⬅ EASIER: Guided
Reduce timer to 1–2 minutes. Parent sits inside play zone reading own book. Only 2 bin options visible. High-interest material only. Add comfort object. Parent narrates from adjacent room: "I can hear you playing!"
↔ STANDARD: Weeks 3–8
As described in Steps 1–6. 5–15 minute sessions. 4–6 bin options. Parent in adjacent room. Timer + menu + reward system all active simultaneously.
HARDER: Extended ➡
Increase duration to 20–45 min. Parent in different room (not visible). Child selects from full menu independently. Introduce less-preferred activities. Reduce token frequency. Different locations.
Child Profile | Key Adaptation | |
ADHD — High Sensory Seeking | Add movement breaks between bins. Wiggle cushion in play space. Audiobook for background stimulation. | |
Autism — Restricted Interests | Build initial sessions ENTIRELY around special interest. Expand repertoire gradually from that foundation. | |
Anxiety — Aloneness Fear | Never use absence/disappearance as technique. Remain visible. Use photos of parent as proxy comfort object. | |
Developmental Delay | Match bin activities to developmental age (not chronological). 3-year-old bins for a 7-year-old at 3-year developmental level. |
Individualized intervention planning: Core principle across OT (sensory profile-based), ABA (function-based), and SpEd (IEP-based) clinical practice.

Week 1–2: Calibrating Expectations
ACT IV: Progress Arc
15% — You Are Here
Observable Indicator | What It Means | |
Child enters play space without crying | Huge. The routine is beginning to form. | |
Child picks up a bin without adult direction | Ideation beginning to emerge. | |
Child stays 2–3 minutes before seeking parent | Tolerance baseline established. | |
Child glances at timer (even anxiously) | The timer is becoming a coping tool. | |
Child doesn't resist clean-up at session end | Routine is taking hold. |
"In weeks 1–2, you may feel like this isn't working. The sessions are short. The child is still asking for you. You're still having to prompt. This is entirely normal — and entirely expected. Skill-building looks like nothing is happening right before it starts happening. Stay consistent."
Systematic review (Children, 2024): Structured independent play interventions show outcome emergence across 8–12 week timelines. | PMC11506176
Week 3–4: The Neural Pathways Are Forming
40% — Week 3–4 Zone
Child Anticipates the Session
They bring their preferred bin to the play corner before you've set up. This means the routine has been encoded at the neural level.
Resistance at Start Decreases
Fewer "I don't want to" moments. The new behavior is becoming the expected behavior. The path of least resistance is shifting.
Duration Extends Spontaneously
The timer ends at 5 minutes and the child keeps playing for another 2 minutes before noticing. This is generalization beginning — the skill is becoming self-sustaining.
Glances Toward Parent Decrease
The child is less anxious about parental proximity. Trust in their own ability to be alone — and to be okay — is building session by session.
Milestone: You may notice you're more confident too. Most parents at week 3–4 report feeling less guilty about stepping away, and more able to enjoy their brief alone-time. Your capacity for self-care is also a therapeutic variable. Neuroplasticity evidence: Synaptic strengthening through repeated structured input follows predictable timelines.
If sessions at current duration are easy for 3 consecutive days → increase timer by 2 minutes. Never rush — let the child lead the pace of advancement.
Week 5–8: When the Skill Begins to Own Itself
⭐ Mastery Emerging
75% — Week 5–8 Zone
✅ Duration
Child sustains independent play for 20+ minutes consistently — not just on best days. Measured across at least 3 observation sessions.
✅ Initiation
Child moves to play space independently within 2–3 minutes of routine cue, without adult prompt. The cue alone is enough.
✅ Ideation
Child selects activity from menu without adult involvement; occasionally skips menu and goes directly to preferred activity.
✅ Generalization
Independent play skill appears in at least one NEW setting — grandparent's home, after-school program, or clinic waiting room.
✅ Regulation
Child tolerates being in play zone with parent not visible for 5+ minutes without distress. Aloneness is no longer threatening.
Mastery Badge Unlock: When ALL 5 criteria are met on 3 consecutive observation days → G-629 MASTERY achieved → proceed to G-630 Turn-Taking Skills. Important — Mastery ≠ Completed: Continue 3–4 sessions per week indefinitely to prevent regression. Skills not practiced slowly erode. PMC10955541 | BACB Standards

⛔ Clinical Guardrails — Even in the Success Zone
"Trust your instincts. If something feels wrong — pause and ask."
Signal | What It May Indicate | Action | Escalation | |
Child becomes more anxious about aloneness over time, not less | Underlying anxiety disorder may require therapeutic focus | Teleconsult → Psychological assessment | Clinical priority | |
Self-injurious behavior during or after sessions | Session structure triggering dysregulation | STOP technique. Consult ABA/NeuroDev immediately | Urgent | |
Complete regression after a period of progress | Medical event, environmental stressor, or therapy mismatch | Review with Pinnacle therapist | High priority | |
Child's language or social skills appear to be regressing | Requires comprehensive developmental review | AbilityScore® reassessment | Clinical priority | |
No progress after 8 weeks of consistent implementation | Technique may not be addressing the primary barrier | Escalate to clinical assessment | Reassessment needed |

You Are Here — Where the Journey Goes Next
G-627
Age-Appropriate Play Skills
PREREQUISITE
PREREQUISITE
G-628
Independent Play
PREREQUISITE
PREREQUISITE
★ G-629 ★
SELF-ENTERTAINMENT
YOU ARE HERE
YOU ARE HERE
G-630
Adult-Dependent Play Reduction
NEXT LEVEL
NEXT LEVEL
G-631
Turn-Taking Games
ADVANCED
ADVANCED
If Your Child's Mastery Shows... | Next Recommended Technique | |
Strong independent play, ready for social expansion | G-630 Adult-Dependent Play Reduction → G-631 Turn-Taking Games | |
Good initiation but limited creativity | G-580 Open-Ended Play Skills | |
Strong self-entertainment, poor transitions | G-345 Transition Support Techniques | |
Excellent at home, fails at school | G-390 Generalization to Novel Settings |
G-629 contributes to: Leisure & Recreation Readiness Index + Autonomy Development Index + Independent Living Skills Readiness — three of the five GPT-OS® life-readiness indexes. Every minute your child spends playing independently is an investment in their autonomous adulthood.
Explore the Play Development Domain
You may already own the materials for several of these techniques.
Technique | Code | Difficulty | Materials You Have | |
9 Materials That Help With Age-Appropriate Play | G-627 | 🟢 Intro | Activity Bins ✓ | |
9 Materials That Help With Independent Play | G-628 | 🟢 Intro | Timers ✓ | |
Self-Entertainment (CURRENT) | G-629 | 🟡 Core | Full kit | |
Adult-Dependent Play Reduction | G-630 | 🟡 Core | Reward System ✓ | |
Turn-Taking in Play | G-631 | 🟡 Core | Game materials | |
Leisure Skill Development | G-628 | 🟡 Core | Most materials ✓ |
"You Already Own Materials For" Indicator: Based on your G-629 material kit → You have what you need for G-627, G-628, and G-630. Zero additional purchases required to begin these techniques immediately after mastering G-629.
G-629 Is One Piece of a Larger Plan
Your child's developmental landscape across all 12 GPT-OS® domains.
Your work on G-629 contributes to Domains G (Play) and L (Executive Function) simultaneously. The 5 underlying capacities built here — ideation, initiation, sustained attention, emotional regulation, intrinsic motivation — are cross-domain capacities that improve outcomes in communication, behavior, and academic readiness as well.
AbilityScore® tracks your child's progress across all 12 domains simultaneously, ensuring that G-629's gains integrate with gains from other active techniques into a unified developmental trajectory. WHO Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring. | WHO NCF (2018)
From the Pinnacle Network — Real Families, Real Outcomes
Illustrative clinical narratives. All identifying details changed. Outcomes reflect aggregate experience across Pinnacle's 70+ centers.
Kavya, 6 Years — Hyderabad
Before (Week 0): Kavya could not be in a room alone for 60 seconds. Her mother could not shower, cook, or make a phone call without Kavya following her, crying, or screaming. Diagnosed with ASD Level 1 with separation anxiety.
After (Week 8): Kavya plays independently in her cozy corner for 25–30 minutes on weekday mornings while her mother works from home. She selects her own activity bin, checks the timer, and brings her creations to show her mother when the timer ends.
"Three months ago I could not shower without her pounding on the door. Last week she played in her corner for 45 minutes while I worked. She came to show me what she'd made — but she didn't need me for the making." — Parent, Pinnacle Hyderabad
OT Lead Note: "Kavya's primary barrier was felt safety. We built her play space 18 inches from her mother's desk, gradually moved it to 3 feet, then 6 feet, then the adjacent room. The timer was her safety anchor — she could see the end. Anxiety responded to predictability, not instruction."
Rohan, 9 Years — Bengaluru
Before (Week 0): Rohan had ADHD (combined type). Each intervention worked for 2 days then stopped. Assessment revealed the real issue: initiation failure, not ideation or attention. He could list 20 things he wanted to do — he simply could not start any without an adult physically beginning alongside him.
After (Week 8): With the ABA-guided prompt-fading protocol (full physical → gestural → visual → independent), Rohan now initiates his Lego sessions independently. Duration: 35–40 minutes. He no longer needs an adult to "start" the activity for him.
"We tried everything and concluded he was incapable of playing alone. Now I watch him build for 40 minutes by himself. He just needed the right scaffold to get started." — Parent, Pinnacle Bengaluru

Isolation Is the Enemy of Adherence
Join 10,000+ families navigating the same journey.
💬 WhatsApp Parent Groups
Join the Independent Play & Self-Entertainment Parent Group — moderated by Pinnacle therapists. 5,000+ active parents sharing real-time strategies, wins, and support.
🌐 Online Forum
Pinnacle GPT-OS® Parent Community — search "G-629" for technique-specific threads. Find parents whose children share your child's profile and diagnosis.
👥 Peer Mentoring
Connect with a parent who has completed G-629 — matched by child age, diagnosis, and city. Real conversations, real experience, real encouragement.
📍 Local Parent Meetups
70+ centers across India host monthly parent circles. Find a Pinnacle parent group near you for in-person peer connection and therapist-facilitated support.
"Your experience helps others. If you've completed G-629, consider sharing your journey. One parent's story is another parent's lifeline." — WHO NCF: Community engagement is a core nurturing care principle. | WHO NCF Community Engagement Principles

Home + Clinic = Maximum Impact
Professional guidance multiplies what you're already doing at home.
🟠 OT Assessment
Identify the exact underlying barrier (ideation/initiation/attention/regulation) — which determines which of the 9 materials matters most for YOUR child's specific profile.
🟣 ABA Consultation
Build the precise reinforcement schedule that matches your child's motivation profile. Prompt-fading protocols calibrated to current baseline and target duration.
🟢 NeuroDev Review
Evaluate whether ADHD medication, anxiety management, or other medical supports would accelerate progress. Medical optimization enables therapeutic gains.
🔵 SpEd Input
Design visual supports (menus, schedules) calibrated to your child's language and comprehension level. Materials that match the child's developmental language are used independently.
🌸Pinnacle Consortium Disciplines: OT | SLP | ABA/BCBA | Special Education | NeuroDev Pediatrics | CRO
The Evidence Behind G-629 — For the Curious Parent
📚 Study 1 — 2024 Systematic Review | Level I Evidence
"Structured independent play interventions for children with autism and ADHD: 16 articles confirm evidence-based practice status for initiation and sustained engagement outcomes." PMC11506176 — Read on PubMed
📚 Study 2 — 2024 Meta-Analysis | Level I Evidence
"Sensory integration and play-based therapy across 24 studies: effective promotion of adaptive behavior, social skills, and self-directed engagement." PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
📚 Study 3 — Indian RCT, 2019 | Level II Evidence
"Parent-delivered home-based structured interventions in Indian pediatric populations: significant outcomes comparable to clinic-based delivery." Padmanabha et al., Indian J Pediatr | DOI: 10.1007/s12098-018-2747-4
📚 Study 4 — WHO/UNICEF, 2023 | Implementation Evidence
"Care for Child Development Package: structured caregiver activities improve developmental independence outcomes across 54 LMICs." PMC9978394
📚 Study 5 — NCAEP, 2020 | Level I Practice Guideline
"Visual supports, token economy systems, and video modeling classified as evidence-based practices for autism spectrum disorder." NCAEP Evidence-Based Practices Report 2020

From Your Living Room to the World's Largest Pediatric Therapy Intelligence System
What GPT-OS® Learns From G-629
- Which of the 9 materials produces fastest initiation gains in children of your child's profile
- Optimal timer starting duration by age, diagnosis, and baseline tolerance
- Correlation between sensory regulation tools and independent play duration
- Reinforcement schedules that produce fastest motivation transfer from external to internal
🛡️ Privacy Assurance
All data encrypted and anonymized. No identifying information shared. DPIIT-registered, MSME-certified, GSTIN-compliant. India Data Protection Bill 2023 compliant.
"Your Data Helps Every Child Like Yours": Each session you record contributes to the evidence base that improves GPT-OS® recommendations for every family on the platform. Your 5-minute data entry is a contribution to pediatric developmental science.
Digital health interventions for ASD: 21 RCTs, 1,050 participants confirm gamified digital health interventions show significant promise. | 2024 Meta-Analysis

Consistency Across Caregivers Multiplies Impact
One parent implementing this technique = good. The whole family = transformational.
📱 Share on WhatsApp
Send this guide directly to grandparents, co-parents, or family members who care for your child. Consistency requires shared understanding.
⬇️ Family Guide PDF
Download the G-629 Family Guide — a simple, printable 1-page summary for grandparents, teachers, and babysitters. No jargon, just clear instructions.
📋 School Template
Ready-to-send school communication template — share the visual timer and activity menu approach with teachers for consistent support during free-choice periods.
📖 "Explain to Grandparents" Version: "[Child's name] is learning to play independently. Their therapist has given us a system: bins with one activity each, a visual timer, and a reward when they finish. Please do NOT ask them what to do or sit with them during play time. Just stay nearby and come when the timer ends. Celebrate any independent time — even 1 minute is progress. Call 9100 181 181 if you have questions."
WHO CCD Package: Multi-caregiver training is critical for intervention generalization and maintenance. | PMC9978394

Frequently Asked Questions — Answered by the Pinnacle Consortium
Q1: My child plays on screens for hours. Why can't they do it without one?
Screens provide external engagement that requires no ideation, initiation, or tolerance of ambiguity. They're not a failure — they're evidence that the underlying attention capacity EXISTS. Start with the child's highest-interest non-screen activity and use it as the "gateway." Don't eliminate screens — use them strategically as rewards that reinforce non-screen independent play.
Q2: How long before I see real progress?
Most parents notice a qualitative shift in weeks 3–4. Measurable duration increase (2–3 minutes) typically appears in weeks 2–3. Meaningful independent sessions (15+ minutes) emerge in weeks 6–10 for most children. These timelines vary significantly by underlying diagnosis, starting baseline, and implementation consistency.
Q3: Is this appropriate for my non-verbal child?
Yes — with modification. Non-verbal children often benefit MORE from visual supports (menus, timers) because these bypass language. Activity bins and sensory tools are language-independent. Focus on high-interest and open-ended materials. The reward system can use non-verbal reinforcement (preferred activity, sensory input, physical affirmation).
Q4: My autistic child LOVES to play alone already. Is G-629 still relevant?
Partially. If your child engages contentedly in preferred solo activities, respect and celebrate that. G-629 is relevant if you want to expand the repertoire, if the preferred activity becomes a functional barrier, or if school requires broader independent engagement. Never pathologize healthy solitary engagement.
Q5: 6 weeks consistent, no progress. What's wrong?
This usually indicates a mismatch between the technique and the primary barrier. See the Troubleshooting and Adapt & Personalize cards. If you've tried all adaptations without progress, the child may have an unaddressed underlying condition requiring clinical assessment before home techniques can gain traction. Call 9100 181 181 for a free consultation.
Q6: Should I use all 9 materials simultaneously?
No. Start with the 2–3 that address your child's primary barrier. A typical starting kit: activity bins (address ideation) + visual timer (address regulation) + one high-interest item (address motivation). Add materials as the skill develops over weeks 3–8.
Q7: How is this different from "just leaving the child to figure it out"?
Profoundly different. "Leaving them to figure it out" assumes the skill is present but not applied. G-629 assumes the skill may be absent or underdeveloped — and provides the scaffolding that makes skill-building possible. The difference is between expecting a child to swim and teaching them to swim with floats that gradually come off.
Q8: Will my child always need these supports?
No. The goal is for supports to become unnecessary. Bins → free play. Timer → internal time sense. Menu → spontaneous ideation. Rewards → intrinsic satisfaction. Most children reduce their need for supports significantly by week 12+. Some children will benefit from reduced (not eliminated) supports long-term — and that's appropriate, not a failure.

You've Read the Evidence. You've Seen the Materials. You Have Everything You Need.
The only difference between a parent who transforms their child's development and one who doesn't is one decision: start today.
🧠 OT
Occupational Therapy — Primary Lead
💬 SLP
Speech Language Pathology
📊 ABA
Applied Behavior Analysis / BCBA
📚 SpEd
Special Education
👨⚕️ NeuroDev
NeuroDev Pediatrics
🌸Validated by the Pinnacle Blooms Network® Multi-Disciplinary Consortium | OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO
📞FREE National Autism Helpline: 9100 181 181 — 16 languages | 24×7 | No appointment | No cost | India's largest autism support network
Preview of 9 materials that help with self entertainment Therapy Material
Below is a visual preview of 9 materials that help with self entertainment therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.











Link copied!
🌸 The Pinnacle Promise
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
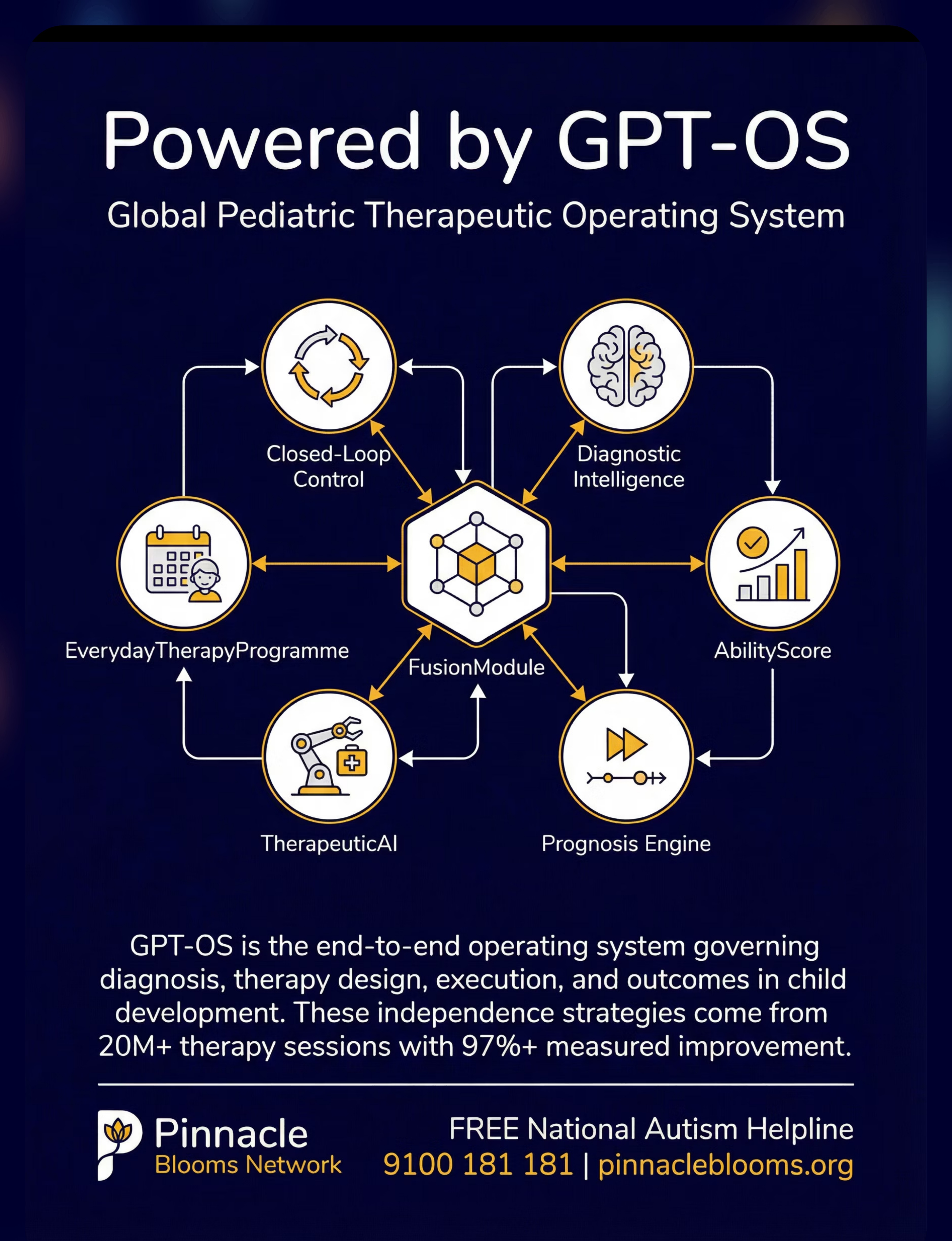
GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™
"From fear to mastery. One technique at a time."
Every page in the Pinnacle Techniques Library — all 70,000+ — is built on a single promise: that every parent, regardless of where they live, how much they earn, or how overwhelming their child's challenges feel, deserves the same quality of evidence-based intervention guidance that was previously available only to families with access to private specialist clinics.
G-629 is one of 70,000+ techniques. Each is sourced from 20M+ therapy sessions, validated by multi-disciplinary clinical teams, aligned with WHO/UNICEF global developmental standards, and designed for execution in the home — not just in the clinic.
↑ Return to Top
Back to The Recognition Moment — Card 01
→ Next Technique
G-630 Adult-Dependent Play Reduction
🏠 All Techniques
🌸 Main Site
📧care@pinnacleblooms.org | pinnacleblooms.org
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: UDYAM-TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention from licensed occupational therapists, behavioral therapists, psychologists, or physicians. Difficulty with independent play may indicate underlying attention, anxiety, developmental, or sensory processing differences requiring comprehensive evaluation. Each child develops at their own pace — progress should be celebrated relative to their own baseline, not compared to siblings or peers. Consult a qualified healthcare professional before implementing any therapy technique. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®. © 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, and Pinnacle Blooms Network® are registered trademarks.