
"Every afternoon, my child runs straight to the bathroom. They've held it for seven hours."
School Bathroom Refusal isn't stubbornness. It's a nervous system under siege — and there are nine proven ways to help.
🟢 E-503 | School Bathroom Refusal
Ages 5–14
Toileting Anxiety
Sensory Processing
School Functioning
"You are not failing. Your child's nervous system is speaking — in the only language it knows."
— Pinnacle Blooms Consortium | OT • SLP • ABA • SpEd • NeuroDev
FREE National Autism Helpline | Available in 16+ languages | 24×7

What's Happening in Your Child's Brain & Body
This is a wiring difference. Not a behaviour choice.
The Science
Auditory Hypersensitivity: The auditory cortex over-amplifies sudden loud sounds. Automatic flushes reach 85–100dB — equivalent to a motorcycle. For children with hyperacusis, this triggers a genuine threat response via the amygdala, activating the fight-flight-freeze cascade.
Psychogenic Urinary Retention: When anxiety activates, the sympathetic nervous system tenses the pelvic floor and external urethral sphincter. This is neurological, not volitional — the child literally cannot void even when the bladder is full.
Interoceptive Dysfunction: Many children with autism and ADHD have reduced interoceptive awareness — they don't register bladder signals until urgency is extreme, leaving insufficient time to overcome avoidance barriers.
Paruresis Mechanism: Social anxiety triggers the same sympathetic cascade — fear of being heard, seen, or judged physically prevents urination. Classified by the ICS as a functional voiding disorder.
For Parents: Plain English
"Their body isn't being stubborn. It is responding to perceived danger — real danger, to their nervous system."
The bathroom sounds that seem normal to us are physically painful to auditory-sensitive children
The freeze response that prevents voiding is involuntary — not willpower failure
Body signals that say "I need to go" arrive late or not at all in many children with neurodevelopmental differences
The shame from accidents compounds the neurological fear into a reinforced avoidance cycle
DOI: 10.3389/fnint.2020.556660 | ICS Pediatric Voiding Guidelines | ADAA Paruresis Clinical Framework
Where This Sits in Development
Your child is here. Here is the path forward.
Ages 2–3
Toilet training begins; core interoceptive awareness develops
Ages 3–5
Home bathroom independence; body signal recognition emerges
Ages 5–7 ← Your child may be here
School transition challenge zone — structured environments with shared, busy bathrooms
Ages 7–10
Generalisation to multiple settings; peer social awareness intensifies
Ages 10–14
Independence and privacy needs peak; anxiety-driven avoidance peaks without intervention
Ages 14+
Adult functioning patterns establish — chronic avoidance can persist without treatment
🎯This technique's zone: Ages 5–14 | School Bathroom Generalisation. School bathroom refusal peaks at ages 5–12 — coinciding with entry into structured environments, increased peer social awareness, and development of avoidance patterns that can become chronic without intervention.
Comorbidities to Watch
Constipation
School stool avoidance frequently co-occurs
UTIs
Urinary tract infections from chronic holding
School Avoidance
Bathroom anxiety as gateway condition
Social Anxiety
Paruresis and fear of being heard or judged
Sensory Processing
SPD amplifies all avoidance barriers
PMC9978394 | WHO/UNICEF CCD Package (2023) | ICS Pediatric Continence Guidelines 2024
The Evidence Behind These Interventions
Clinically validated. Home-applicable. Consortium-tested.
🏆 LEVEL II–III EVIDENCE
Multi-disciplinary consensus
Controlled studies
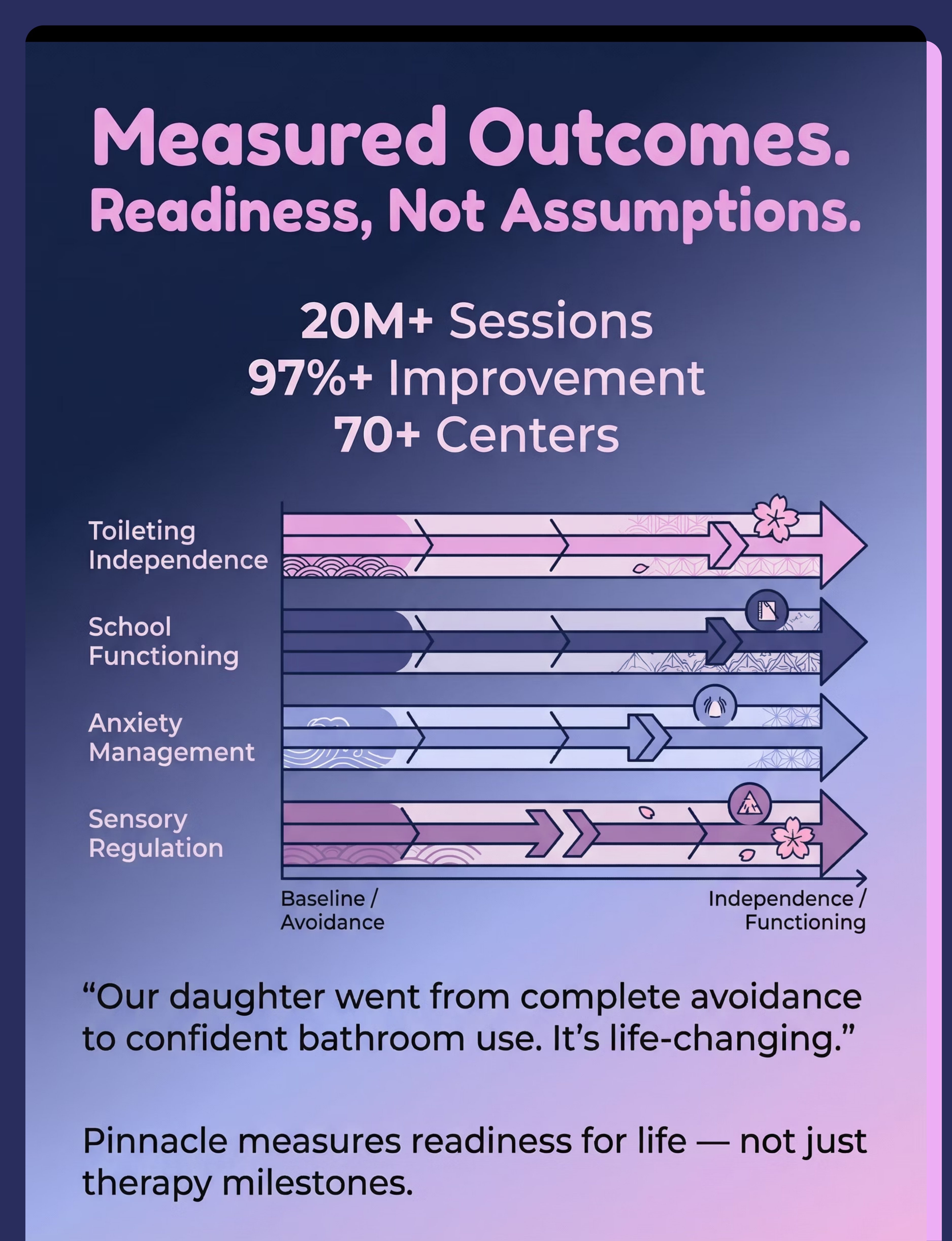
20M+ real-world outcomes
1
Sensory Modification Interventions (OT Evidence Base)
PRISMA Systematic Review (2024) — 16 studies, 2013–2023: Sensory integration intervention meets criteria as evidence-based practice for children with ASD, including functional daily living skill generalisation.
PMC11506176
2
Gradual Exposure / Systematic Desensitisation (ABA + Psychology)
Exposure-based interventions for specific phobias and anxiety in children: strong evidence across multiple RCTs. Avoidance maintenance of fear is a foundational behavioural principle.
ADAA Evidence Base | NCAEP 2020 Report
3
Timed Voiding Protocols (Medical / OT)
International Continence Society: Timed voiding reduces urinary urgency, improves bladder function, and prevents overflow accidents. Evidence-based in paediatric urology literature.
ICS Pediatric Guidelines 2024
4
Social Stories & Visual Supports (ABA / SLP)
NCAEP (2020): Social narratives classified as evidence-based practice for autism. Reduces anxiety around predictable transitions and environments.
NCAEP Evidence-Based Practices Report 2020
5
Home-Based Delivery
Indian Journal of Pediatrics RCT (2019): Home-based sensory and behavioural interventions demonstrate significant outcomes for Indian paediatric populations.
DOI: 10.1007/s12098-018-2747-4 (Padmanabha et al.)
"This is not experimental. These interventions have decades of evidence, internationally validated guidelines, and real-world proof across 20 million Pinnacle therapy sessions."
PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | ICS 2024 | DOI:10.1007/s12098-018-2747-4

The Technique: What It Is
Formal Name
School Bathroom Refusal — Sensory-Environmental Modification + Graduated Anxiety Reduction Protocol
💡Parent-Friendly Alias:"The School Bathroom Safety Kit"
A multi-modal intervention approach addressing the sensory, anxiety, interoceptive, and environmental factors that prevent children from using school bathrooms safely and independently. Unlike single-strategy approaches, this evidence-based framework addresses all layers simultaneously — the environment (accommodations), the body (sensory tools), the mind (anxiety management), and the system (timed voiding, gradual exposure).
What it is not: This is not about forcing, tricking, or pressuring a child into a bathroom that feels unsafe. It is about systematically creating the conditions under which bathroom use becomes genuinely manageable — and eventually automatic.
Domain Badges
Sensory Processing
Auditory and olfactory modification
Anxiety Management
Graduated exposure and relaxation
School Functioning
Accommodation and inclusion frameworks
Interoceptive Awareness
Body signal recognition and timed schedules
Clinical Taxonomy: Domain Code: GI-SBREF | Age Band: 5–14 years | Setting: School + Home + Therapy + Medical | Frequency: Daily environmental supports + structured practice sessions
Who Uses This Technique
This technique crosses therapy boundaries — because the child's nervous system doesn't divide itself by discipline.
🔴 Occupational Therapy (Lead Discipline)
Sensory modulation, interoceptive awareness, environmental adaptation, pelvic floor relaxation techniques, activity of daily living (ADL) skill generalisation across settings.
🔵 Behavioural Therapy / ABA-BCBA
Gradual exposure hierarchy design, reinforcement systems for approach behaviour, functional behaviour assessment of avoidance, timed voiding schedule implementation.
🟡 Paediatric Psychology
Cognitive-behavioural techniques for anxiety, paruresis-specific treatment, trauma processing if applicable, school refusal intervention integration.
🟢 Special Education (SpEd)
504 Plan and IEP accommodation facilitation, school staff training, bathroom pass systems, classroom seating modifications for discrete exit.
🟣 Neurodevelopmental Paediatrics
UTI monitoring, bladder health assessment, constipation management, referral to paediatric urology, medical documentation for school accommodations.
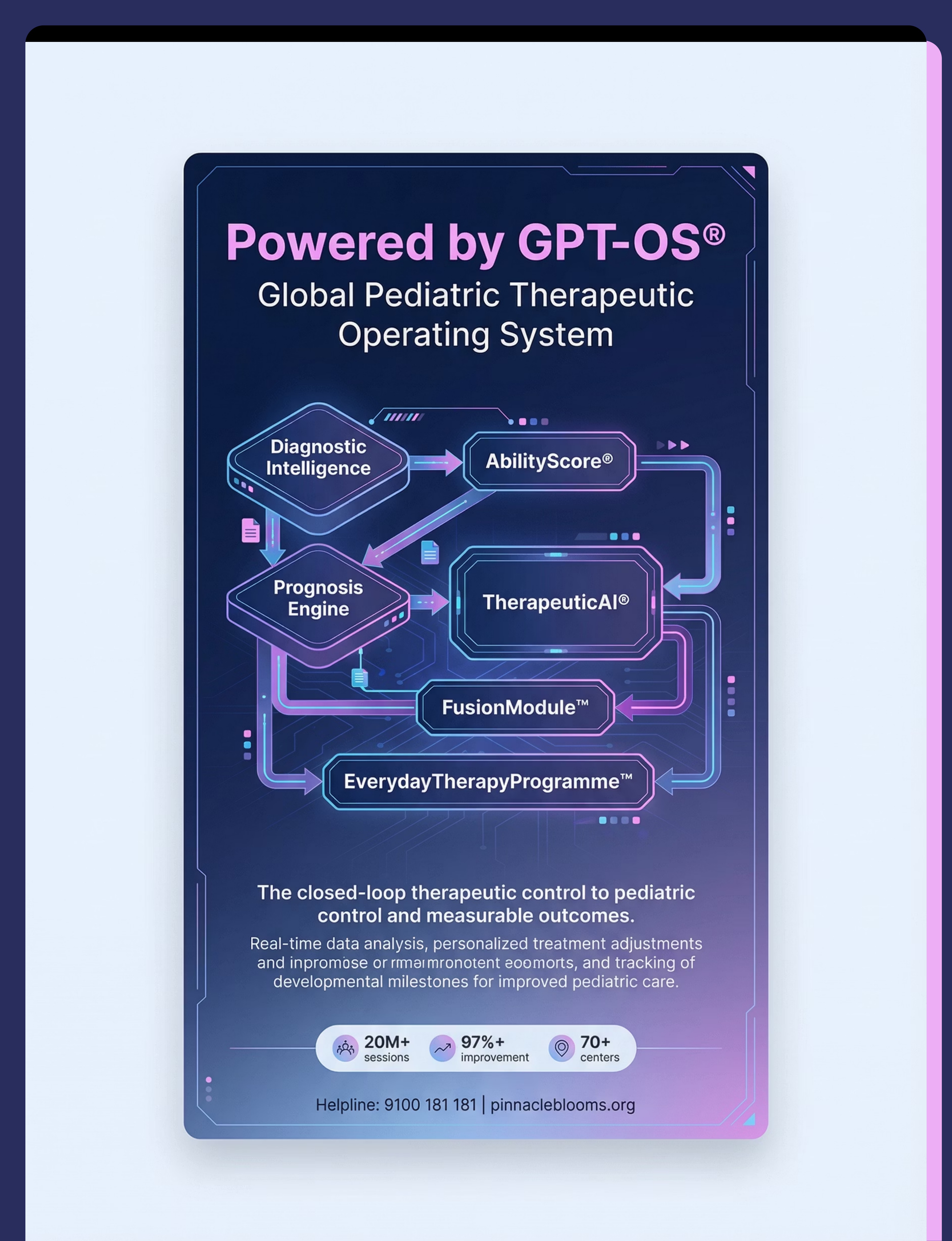
"At Pinnacle, our FusionModule™ coordinates all five disciplines into a single converged plan. Your child isn't seeing five specialists with five different approaches — they're receiving one unified therapeutic pathway."
For disciplinary coordination guidance, call 9100 181 181 — FREE, 24×7

9 Materials That Help With School Bathroom Refusal
9 materials. One mission: making school bathrooms usable. These are drawn from the Pinnacle 128 Canon Materials™ taxonomy — the consortium's clinically validated, cross-disciplinary library of therapeutic tools.
1
Noise-Cancelling Headphones / Ear Defenders
Canon: Sensory Processing Tools
2
Automatic Flush Sensor Covers
Canon: Sensory Processing Tools / Adaptive Equipment
3
Bathroom Social Story & Visual Sequence Cards
Canon: Visual Supports / Social Narratives
4
Portable Sensory Regulation Kit
Canon: Sensory Processing Tools / Portable Regulation Aids
5
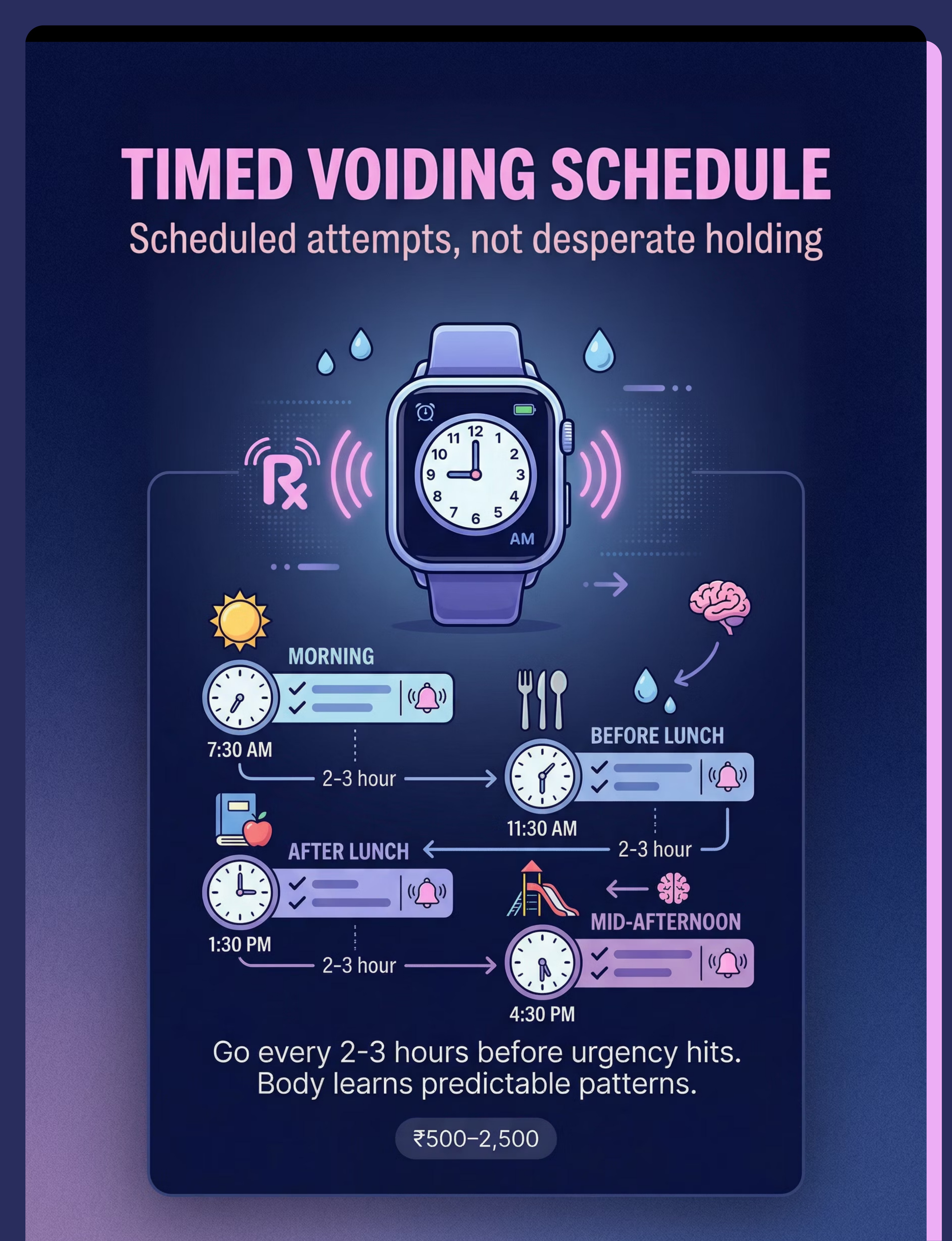
Timed Voiding Reminder Watch
Canon: Scheduling & Time Management Tools
6
School Bathroom Accommodation Request Documentation Kit
Canon: Educational Support Materials / Advocacy Tools
7
Relaxation & Body Awareness Tools
Canon: Regulation & Self-Calming Tools
8
Gradual Exposure Program Materials
Canon: Behavioural Intervention Tools / Reinforcement Systems
9
Medical Evaluation & Bladder Health Monitoring Kit
Canon: Medical/Health Documentation Tools
Material 1: Noise-Cancelling Headphones / Ear Defenders
Sensory Processing Tools
Canon Category 1 of 9
Why This Material Works
Blocks the 85–100dB assault of hand dryers and automatic flushes that trigger auditory overwhelm. One tool can transform an unbearable space into a usable one. For children with hyperacusis or auditory hypersensitivity, the bathroom is genuinely painful — not uncomfortable. Headphones directly interrupt the amygdala threat response before it can cascade into full avoidance.
Price Range: ₹1,500–6,000
DIY Option: Foam earplugs (₹50–200) as starter alternative
Where to Find
Search for noise-cancelling headphones for children on Amazon.in — look for models with NRR 25dB or higher, lightweight construction, and adjustable headbands suitable for children aged 5–14.
How to Introduce
01
Let child handle and try headphones during play time — no bathroom involved
02
Wear headphones at home during noisy situations to build familiarity
03
Introduce headphones as part of bathroom kit before any school practice

Material 2: Automatic Flush Sensor Covers
Sensory Processing Tools
Adaptive Equipment
Canon Category 2 of 9
Why This Material Works
Stops the sudden, startling flush-while-seated that triggers lasting bathroom fear. When a toilet flushes unexpectedly beneath a child, the shock response is profound — and memorable. Each traumatic flush reinforces avoidance. The sensor cover hands control back to the child: the flush happens when they decide. And control is the antidote to fear.
Price Range: ₹200–600
DIY Option: Post-it notes (₹30–50) cover sensors in an emergency — the principle is identical to the commercial version
Where to Find
Search for toilet sensor covers or automatic flush sensor covers on Amazon.in. Choose reusable adhesive versions that fit standard commercial sensor positions. Carry several — stalls vary.
Implementation Tip
Practise placing the cover at home first so the child can do it independently and confidently before they need to do it at school. Make it a ritual: "Cover first, then sit."
Material 3: Bathroom Social Story & Visual Sequence Cards
Visual Supports
Social Narratives
Canon Category 3 of 9
Why This Material Works
Anxiety feeds on uncertainty. Personalised social stories address specific fears, provide coping scripts, and reduce the unpredictability that triggers avoidance. When a child knows exactly what will happen — and has read their own story about handling it — the bathroom becomes predictable. Predictability reduces the threat signal. NCAEP (2020) classifies social narratives as an evidence-based practice for autism.
Price Range: ₹200–800 (or free DIY)
DIY Option: Create at home using photos of the actual school bathroom, printed on cardstock. Personalisation beats production value — photos of their bathroom are more therapeutically effective than generic illustrations.
Where to Find
DIY Social Story Components
01
Photos of the actual school bathroom (entrance, stall, flush button)
02
Simple sentences describing each step in first person: "I walk in. I find my stall."
03
A coping script: "If I feel scared, I breathe. I have my kit. I am safe."
04
A positive ending: "I did it! I used the bathroom and came back to class."

Material 4: Portable Sensory Regulation Kit
Sensory Processing Tools
Portable Regulation Aids
Canon Category 4 of 9
Why This Material Works
Addresses smell overwhelm, anxiety regulation, and visual focus challenges simultaneously. School bathrooms are olfactorily overwhelming environments for sensory-sensitive children. The portable kit gives a child agency: they enter the bathroom equipped — not defenceless. Having tools in hand activates the prefrontal cortex's sense of control, reducing the amygdala's threat response before it can cascade.
Price Range: ₹300–1,000 (assembled kit)
DIY Option: Small ziplock bag with lavender cotton ball, a rubber band fidget, and a printed focus card (₹50)
Where to Find
Kit Contents (Recommended)
Scent Override
Lavender cotton ball or roll-on balm
Fidget
Rubber band or small squeeze toy
Visual Focus Card
Laminated breathing card or calming image
Sensor Covers
2–3 post-its or commercial covers

Material 5: Timed Voiding Reminder Watch (Vibrating Alarm Watch)
Scheduling & Time Management Tools
Canon Category 5 of 9
Why This Material Works
Bypasses faulty interoceptive signals by imposing a regular schedule. For children with interoceptive dysfunction — particularly those with autism or ADHD — bladder signals simply don't arrive reliably until urgency is overwhelming. By the time they feel the need, avoidance barriers are at their peak. A timed schedule interrupts this cycle: the child goes every 2–3 hours before urgency hijacks avoidance. The schedule, not the sensation, drives behaviour.
Price Range: ₹500–2,500
DIY Option: Silent alarm on child's phone / teacher-triggered bathroom reminder schedule (₹0)
Where to Find
Recommended School Schedule
1
7:30 AM
Bathroom before school (home)
2
10:00–10:30 AM
Scheduled school attempt (break time)
3
12:30–1:00 PM
Scheduled school attempt (lunch)
4
3:00–3:30 PM
Scheduled school attempt (mid-afternoon)
5
4:00 PM+
Bathroom on arrival home

Material 6: School Bathroom Accommodation Request Documentation Kit
Educational Support Materials
Advocacy Tools
Canon Category 6 of 9
Why This Material Works
Private bathroom access, schedule modifications, sensory tools permitted — schools can and must accommodate. Yet without a formal written request, verbal accommodation conversations rarely result in action. Parents need to know exactly what to ask for, in the precise language that school systems respond to, backed by medical documentation. This kit provides that structure. In India, children with neurodevelopmental differences are entitled to reasonable accommodations under the Rights of Persons with Disabilities Act (RPWD 2016).
Price Range: ₹0–500 (documentation and template printing)
DIY Option: Free — downloadable template letters and accommodation checklists
Key Accommodations to Request
Private bathroom access (nurse's room or staff bathroom)
Scheduled bathroom times every 2–3 hours
Permission to use headphones for bathroom trips
Non-verbal bathroom request system (signal card)
Classroom seating near door for discrete exit
Towel paper instead of hand dryer
Material 7: Relaxation & Body Awareness Tools (Breathing Cards / Biofeedback Toys)
Regulation & Self-Calming Tools
Canon Category 7 of 9
Why This Material Works
Psychogenic urinary retention — when the body cannot void because of anxiety — is resolved through parasympathetic activation. The key mechanism: slow, controlled breathing directly relaxes the pelvic floor musculature and external urethral sphincter. This is the physiological antidote to the sympathetic freeze that prevents voiding. Breathing exercises are not a comfort measure — they are a direct clinical intervention for the retention mechanism itself.
Price Range: ₹200–800
DIY Option: Pinwheel for slow-exhale breathing practice (₹30–100); printed breathing cards (₹0)
Breathing Protocol for Bathroom Use
🗣"Breathe with me. In through your nose... 1, 2, 3, 4. Hold... 2. Out through your mouth... 1, 2, 3, 4, 5, 6. Perfect. Your body is safe here."
Pelvic Release Cues
"Imagine warm water flowing from a waterfall"
"Let your belly go soft. Let your bottom be loose."
Run the tap — auditory cue for voiding reflex

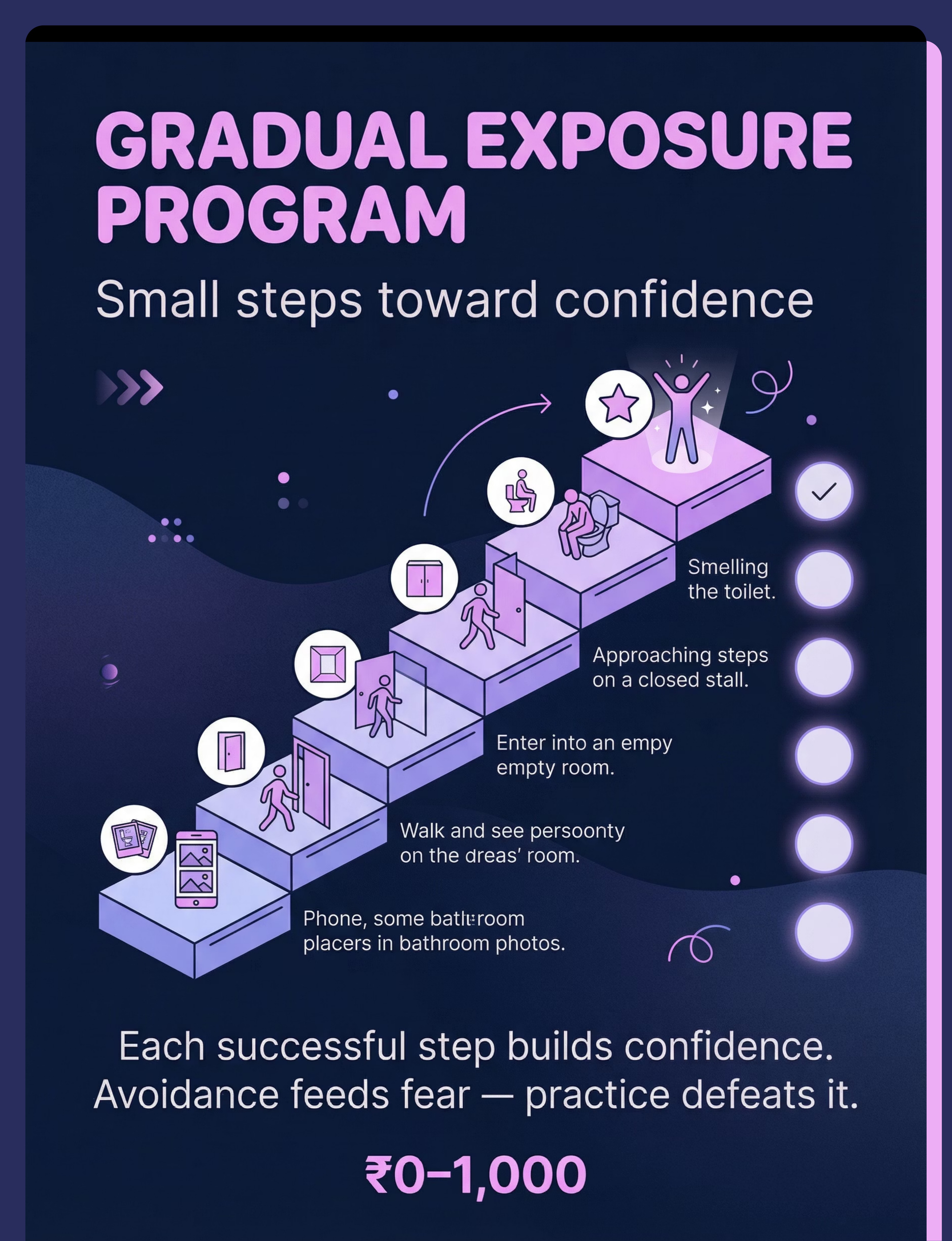
Material 8: Gradual Exposure Program Materials
Behavioural Intervention Tools
Reinforcement Systems
Canon Category 8 of 9
Avoidance feeds fear — only gradual, rewarded practice defeats it. A structured exposure hierarchy with a celebration system transforms a terrifying challenge into manageable steps. The ABA principle is clear: approach behaviour must be reinforced immediately, specifically, and enthusiastically to overcome the competing pull of avoidance relief.
Pinnacle Canon Products
The Rosette Imprint Reward Jar — ₹589
Canon: Reinforcement Menus
Canon: Reinforcement Menus
1800+ Reward Stickers — ₹364
Canon: Reinforcement Menus
Canon: Reinforcement Menus
DIY Option: Hand-drawn sticker chart and verbal praise (₹0) — immediate, specific praise is the most powerful reinforcer
Why Graduated Exposure Works
01
Each small step reduces the fear response slightly through habituation
02
Immediate reinforcement pairs the bathroom with positive outcomes
03
The child's sense of mastery and confidence grows step by step
04
Over weeks, approach behaviour replaces avoidance as the dominant response
Key principle: Progress through the exposure hierarchy only after 3 consecutive successful sessions at each step. Never skip levels.

Material 9: Medical Evaluation & Bladder Health Monitoring Kit (Voiding Diary + Symptom Log)
Medical/Health Documentation Tools
Canon Category 9 of 9
Why This Material Is Non-Negotiable
Chronic holding causes measurable physical damage — UTIs, bladder muscle stretch, reduced contractility, and a constipation cascade that worsens urinary symptoms. Medical monitoring is essential, not optional. Without a voiding diary, parents and clinicians are guessing. With systematic data, patterns emerge: which days are worst, what preceded a UTI, whether holding duration is decreasing. This data guides clinical decisions and strengthens school accommodation requests.
Price Range: ₹1,000–5,000 per consultation (plus free symptom tracking printables)
DIY Option: Printed voiding diary and symptom log (₹0) — the data, not the format, is what guides treatment
What to Track Daily
Times child used bathroom at school
Times child attempted but couldn't void
Holding complaints throughout the day (yes/no)
Any UTI symptoms (burning, frequency, odour, fever)
Fluid intake during school hours
Bowel movement frequency (constipation directly affects bladder)
For medical coordination, call 9100 181 181 — FREE, 24×7

DIY & Substitute Options: Every Family Can Start Today
Regardless of budget. WHO/UNICEF Equity Principle: No child's access to therapeutic support should depend on purchasing power.
Material | Clinical-Grade (Buy) | Zero-Cost DIY (Make/Use) | Why It Works | |
Noise-Cancelling Headphones | ₹1,500–6,000 | Foam earplugs from pharmacy ₹50 | Same principle: reduce auditory input | |
Flush Sensor Covers | ₹200–600 | Post-it sticky notes ₹30 | Sensor blocked = no automatic flush | |
Social Story Cards | ₹200–800 | Phone photos + printed script ₹0 | Photos of THEIR bathroom are more effective | |
Portable Sensory Kit | ₹300–1,000 | Ziplock bag + lavender cotton ball ₹50 | Function (scent, fidget, focus) is identical | |
Timed Voiding Watch | ₹500–2,500 | Teacher-coordinated reminder ₹0 | Schedule, not technology, is the active ingredient | |
Accommodation Documentation | ₹0–500 | Free template letters ₹0 | Document, print, submit — no cost required | |
Breathing/Relaxation Tools | ₹200–800 | Pinwheel + printed card ₹30 | The breath technique, not the tool, is therapeutic | |
Exposure + Reward System | ₹364–589 (stickers) | Hand-drawn chart + verbal praise ₹0 | Immediate specific praise is the most powerful reinforcer | |
Medical Voiding Diary | ₹1,000–5,000 (consult) | Printed symptom log ₹0 | The data, not the format, guides treatment |
💡Zero-Cost Starter Pack — ₹100–150 total: Foam earplugs • Post-it notes (5–6) • Photo-based social story printed at ₹5/page • Lavender cotton ball in small container • Accommodation letter (template below) • Pinwheel for breathing • Teacher bathroom reminder schedule • Hand-drawn brave chart • Voiding diary from free online template. Full starter pack. Same evidence base.
PMC9978394 | WHO/UNICEF CCD Package: Household-material-based intervention efficacy demonstrated across 54 LMICs.

⚠️ Safety First: Before You Begin
Read this before starting. Every intervention has safety gates.
1
🔴 RED LINE — Stop and Seek Medical Attention Immediately If:
- Fever with urinary symptoms (possible kidney infection from UTI)
- Blood in urine
- Severe abdominal pain
- Inability to urinate for 8+ hours despite trying
- Significant constipation (fewer than 3 bowel movements per week for extended period)
- Child in acute distress or panic when approaching bathroom
→ These require same-day medical evaluation, not therapy materials.
2
🟠 AMBER — Modify Your Approach, Consult Before Proceeding:
- Child has history of traumatic bathroom experience (teasing, assault, witnessed accident)
- Avoidance is associated with broader school refusal
- Severe anxiety affecting multiple areas of functioning
- Multiple UTIs in past 3 months (bladder damage monitoring needed)
- Child becomes hysterical (not just reluctant) when exposure is attempted
→ Professional guidance is needed before home programme. Call 9100 181 181 for assessment.
3
🟢 GREEN — Proceed With Home Programme:
- Child is medically stable (no active UTI, no fever)
- Avoidance is school-specific (uses bathroom normally at home)
- Child can discuss the issue without acute distress
- Parent/caregiver is consistent and available to support the programme
Critical Safety Rules
❌ NEVER force
Never force a child physically or verbally into a bathroom that feels unsafe — this increases fear and can cause trauma
❌ NEVER punish
Avoidance is a symptom, not defiance — punishment worsens the neurological fear response
❌ NEVER restrict fluids
Restricting fluids causes dehydration and worsens UTI risk — never manage bathroom needs this way
✅ DO approach collaboratively
Gradual, collaborative process with the child as partner
✅ DO ensure regulated state
Child should be fed, rested, and regulated before any exposure practice
✅ DO celebrate all attempts
Celebrate every attempt regardless of voiding outcome — the approach is the win
DOI: 10.1007/s12098-018-2747-4 | Pinnacle clinical safety protocols | ICS Pediatric Continence Safety Standards
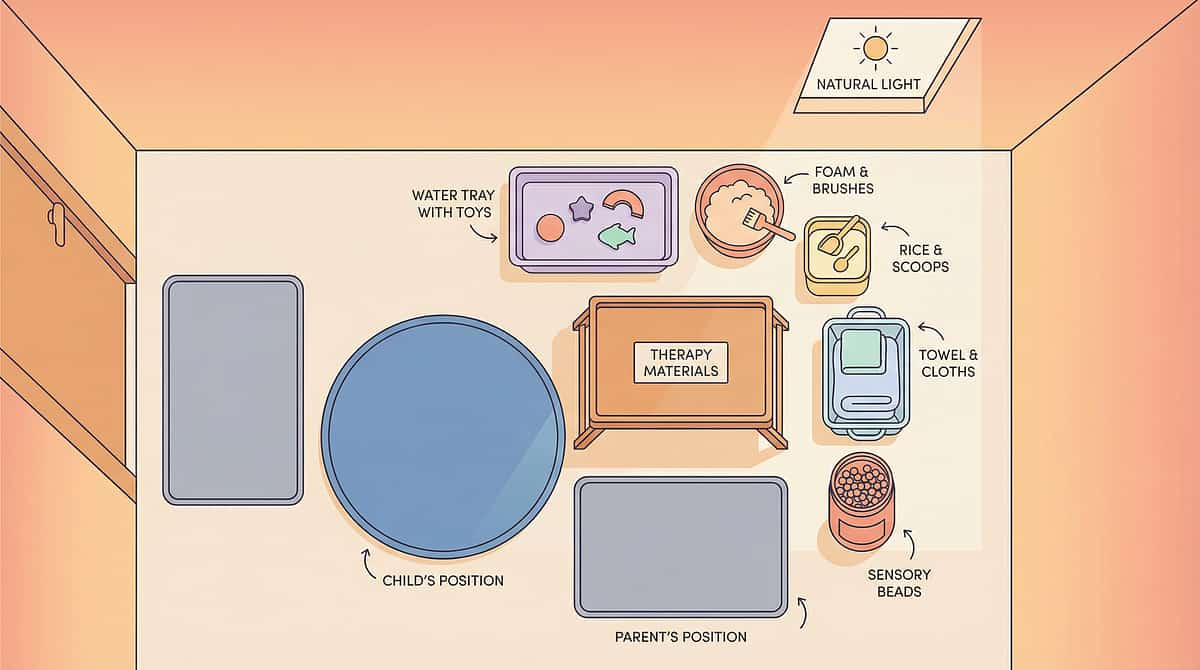
Set Up Your Space
The right environment is 50% of the intervention. This card covers two environments — your home bathroom (practice space) and the school bathroom (target space).
Home Bathroom — Practice Setup
Purpose: Build skills and confidence in a safe, controllable environment before transferring to school.
01
Remove rushing — schedule practice at non-urgent times (not when child genuinely needs to go)
02
Reduce sensory load — turn off harsh fans if tolerated; dim lights if needed
03
Add sensory support — place calming scent item, fidget in pocket before entering
04
Visual schedule — laminated bathroom sequence card at child's eye level
05
Parent position — just outside door (not inside), available but not hovering
06
Visual timer — showing "5 minutes" so child knows when practice ends
Atmosphere: Calm, low-demand, no performance pressure. "We're just practising — no pressure to go."
School Bathroom — Environmental Analysis
Before implementing school strategies, assess these factors and request corresponding accommodations:
Factor | What to Check | Accommodation to Request | |
Flush type | Automatic? | Manual-flush bathroom or sensor cover permission | |
Hand dryer | Present? | Paper towel permission; headphone use | |
Privacy | Lock working? Door gaps? | Stall assessment or private bathroom access | |
Crowd timing | Busiest times? | Early/late break permission | |
Distance | From classroom? | Nearest-bathroom seat assignment | |
Noise level | Echo level? | Headphone permission for bathroom trips |
Setup Principle: Modify the environment to remove barriers BEFORE practising exposure.
PMC10955541 | Environmental setup as core sensory integration principle; Ayres Sensory Integration Theory

Is Your Child Ready? Readiness Check
The best session is one that starts right. Run this 60-second check before every practice session.
# | Check | ✅ Go | ⚠️ Modify | ❌ Postpone | |
1 | Child has eaten in last 2 hours | Fed | Hungry but not distressed | Not eaten today | |
2 | Emotional state | Calm/content | Slightly anxious | Upset, crying, or post-meltdown | |
3 | Recent bathroom success | Used bathroom today | No recent use but not distressed | Held all day + uncomfortable | |
4 | Sleep last night | 8+ hours | Some disruption | Significant sleep loss | |
5 | Recent negative bathroom experience | None | Minor discomfort | UTI, accident, or distressing event today | |
6 | Willingness | Accepting with support | Reluctant but engaged | Refusing and escalating |
✅ GO (4–6 greens)
Proceed with planned session at planned difficulty level
⚠️ MODIFY (2–3 greens, no reds)
Use an easier step in the exposure hierarchy; reduce pressure; shorter duration
❌ POSTPONE (any red)
Don't push today. Do a comfort activity instead. Log the postponement — it's data, not failure.
"Postponing when your child isn't ready is expert parenting. Pushing when the child isn't ready sets progress back weeks."

Step 1: The Invitation
Step 1 of 6
⏱ 30–60 seconds
Never a command. Always an invitation.
Before ANY bathroom attempt, the child must be doing a preferred activity (calm baseline) and NOT currently in urgent need. Practice should never equal desperation. The child must be aware this is "practice time" — not a surprise.
🗣"Hey [child's name], it's our bathroom practice time. We're not going to rush. You have your [headphones/sensory kit/cards] ready. We're just going to walk toward the bathroom together. That's the only goal today. Ready?"
What Acceptance Looks Like
Eye contact or nod
Picks up their sensory kit willingly
Follows toward bathroom without acute distress
What Resistance Looks Like
Physical pulling away or running
Verbal refusal ("No! I don't want to!")
Crying or escalating anxiety
If Resistance → Modify:"Okay, no problem. Let's just look at the bathroom photos on your card instead today."
ABA Pairing Principle: Before any demand can be placed, the parent must be paired with positive experiences. The invitation must feel safe, not threatening.
ABA Pairing Principle: Before any demand can be placed, the parent must be paired with positive experiences. The invitation must feel safe, not threatening.

Step 2: The Engagement
Step 2 of 6
⏱ 1–3 minutes
The sensory kit goes on. The bathroom gets closer.
The child prepares their sensory regulation tools before approaching the bathroom — not inside it. This sequence is important: equipping before entering means the child enters already regulated, not scrambling for tools under stress.
🗣"Let's get your [headphones/earplugs] on. Check — lavender ready? Fidget in pocket? Your bathroom card? Perfect. You're equipped. Let's walk."
Material Introduction Sequence
1
Headphones/earplugs on — before entering, not inside
2
Flush sensor covers in pocket (child holds them — ownership)
3
Sensory kit accessed (lavender, fidget)
4
Visual card in hand for reference
Child Response | Meaning | Action | |
Handles materials calmly | Engagement | Continue — proceed toward bathroom | |
Touches materials but stalls | Tolerance | Allow 60 seconds; gentle encouragement | |
Refuses to take materials | Avoidance signal | Step back; practise handling materials at neutral location |
🗣"I can see you're being so brave picking up your kit. That's real courage."
Key principle: Reinforce the approach behaviour — NOT the voiding outcome.

Step 3: The Therapeutic Action
Step 3 of 6
⏱ 3–10 minutes
The active ingredient. Every successful step rewires the fear response.
Progress through the graduated exposure hierarchy over days and weeks — never skip levels. Move to the next step only after 3 consecutive successful sessions at the current step.
Step | Action | Success Criterion | |
1 | Look at photos of school bathroom | Views without distress | |
2 | Walk past school bathroom (after school, empty) | Passes without panic | |
3 | Look inside from doorway (empty bathroom) | Peeks in without avoidance | |
4 | Enter empty bathroom briefly (30 seconds) | Enters, exits calmly | |
5 | Stand inside for increasing durations (1–5 min) | Remains calm for 5 min | |
6 | Enter bathroom stall (not using toilet) | Opens/closes stall | |
7 | Sit on toilet, clothed (empty bathroom) | Sits for 2 min | |
8 | Attempt voiding in empty bathroom | Any output = success | |
9 | Use bathroom during quiet school times | Morning/late break | |
10 | Use bathroom during typical break times | Independent use |
📍Identify your child's current step: Start one step below the last successful attempt.
Execution Errors to Avoid
❌ Skipping steps
Moving to next step before 3 consecutive successes — current step is not yet mastered
❌ Practising under urgency
Always practise when bladder is comfortable — urgency amplifies avoidance
❌ Parental anxiety
Child mirrors parent's nervous system state — regulate yourself first
NCAEP 2020 | Gradual exposure evidence base | ABA graduated approach principles
Step 4: Repeat & Vary
Step 4 of 6
⏱ 3–5 min per session | Daily practice
3 good practice sessions are worth more than 10 forced ones.
Dosage Guidelines
Frequency
Daily bathroom practice sessions or school bathroom attempt
Duration
5–15 minutes per session
Progression
Move to next exposure step after 3 consecutive successful sessions
Schedule
Timed voiding every 2–3 hours in parallel
Variation Options (to maintain engagement)
Child Profile | Variation | |
Sensory Seeker | Allow exploration of bathroom tiles, handle textures | |
Sensory Avoider | Minimal time, maximum sensory supports | |
Anxiety-driven | Extra social story review before entering | |
Interoceptive differences | Timed voiding regardless of urgency feeling |
Satiation Indicators (enough for today)
Child becomes oppositional where previously cooperative
Anxiety escalating rather than reducing
Somatic complaints increase (headache, stomach ache)
"Scheduled attempts at comfortable times create practice without pressure. Never wait until desperation — that's when avoidance is strongest."

Step 5: Reinforce & Celebrate
Step 5 of 6
⏱ Within 3 seconds of target behaviour
Celebrate the attempt. Not just the success.
Bathroom avoidance is maintained by fear. Bathroom approach behaviour must be reinforced immediately, specifically, and enthusiastically to overcome the competing pull of avoidance relief. Every tiny step deserves recognition.
Verbal Praise Scripts
For approaching:"You walked toward the bathroom even though it felt scary. That's real courage."
For entering:"You went inside! Your body was nervous and you did it anyway. I'm so proud."
For attempting:"You tried to use the bathroom. Whether anything came out or not — that attempt is huge."
For voiding:"You did it! You used the school bathroom. That's the bravest thing."
Reinforcer Type | Example | Pinnacle Product | Cost | |
Social | Specific verbal praise, hug, high-five | — | Free | |
Activity | Extra screen time, special game | — | Free | |
Token | Sticker on chart → reward at 10 stickers | 1800+ Reward Stickers | ₹364 | |
Tangible | Small prize from reward jar | Rosette Reward Jar | ₹589 |
The step practised in today's session — however small — is progress. Avoidance is the enemy, not the child.

Step 6: The Cool-Down
Step 6 of 6
⏱ 2–3 minutes
No session ends abruptly. The cool-down locks in the gains.
Transition the child from therapeutic engagement back to relaxed baseline. Prevents post-session dysregulation and consolidates the positive experience in memory. Abrupt endings can undo the calming work of the session itself.
🗣"Two more breaths, then we're all done with practice. [Breathe together.] Excellent. Let's put everything away. You were so brave today."
1
Verbal transition warning: "One more minute, then we're done"
2
Visual timer: Set to 60 seconds — child watches countdown
3
Sensory kit put-away ritual: Child puts items back in pouch (builds ownership and pride)
4
Regulation activity: 2 minutes of preferred calming activity (drawing, quiet book, favourite toy)
5
Debrief (for verbal children): "What was the hardest part? What felt okay?"
If child resists ending: This is positive — they're no longer avoidant of the activity! Gently honour the engagement while maintaining the routine.
Post-Session Body Check
Is child regulated and calm? ✅ → Proceed to data capture (next card)
Still anxious or dysregulated? → Extra regulation support before resuming normal activities
Visual timers and transition supports are classified as evidence-based practice for autism. NCAEP Evidence-Based Practices Report (2020)

Capture the Data: Right Now
60 seconds of data now saves hours of guessing later. Record these data points immediately after each session while the information is fresh.
Data Point | What to Record | Format | |
Date & Time | When did practice happen | dd/mm/yyyy + time | |
Exposure Step # | Which step in the hierarchy (1–10) | Number | |
Duration in Bathroom | How long child stayed | Minutes/seconds | |
Voiding Outcome | Yes / No / Attempted | Y/N/A | |
Anxiety Level | 1 (calm) to 5 (very distressed) | Rating 1–5 |
School Day Voiding Log (Daily)
School Bathroom Uses
Times child used bathroom at school
Attempted, Couldn't Void
Times child tried but retention occurred
Holding Complaints
Yes/no — any reports of discomfort during school day
UTI Symptoms
Any burning, frequency, odour, or fever today
Tracking Options
GPT-OS® App Tracker
Most powerful — links to AbilityScore® dashboard for personalised recommendations
Printable PDF Sheet
A4 tracking sheet — download, print at home, keep in child's folder
Simple Tally Card
Backpack card — note each bathroom attempt/success during the school day
"Parents who track their child's progress show 3× greater adherence to home programmes and see measurable outcomes 40% faster." — Pinnacle Clinical Outcomes Database
For data interpretation help, call 9100 181 181 — FREE, 24×7
BACB Data Collection Standards | Cooper, Heron & Heward (Applied Behavior Analysis, 8th ed.)

What If It Didn't Go as Planned?
Most sessions don't go perfectly. The technique needs adjusting — not you. Here are the most common problems and their evidence-based fixes.
Problem 1: Child refused to approach the bathroom at all
Why: Current starting step may be too demanding. Fear has not been reduced enough at a lower level.
Fix: Back up to photos/talking about bathroom only. Re-establish comfort at lower step before re-attempting.
Problem 2: Child got to the bathroom but couldn't void despite trying
Why: Classic psychogenic retention — anxiety-locked pelvic floor. Not wilful.
Fix: Increase relaxation practice at home. Run tap water. Practise when less urgent. Do NOT comment on failure to void — only praise the attempt.
Problem 3: Child used bathroom successfully once, then refused for a week
Why: Normal two-steps-forward, one-step-back pattern. Fear is not linear.
Fix: Return to last successful step. Reduce demand. Wait for readiness check. This is progress, not regression.
Problem 4: Timed voiding schedule isn't working — school won't cooperate
Why: Accommodation has not been formally requested. Verbal requests are often not actioned.
Fix: Submit formal written accommodation request (Material 6). Reference medical necessity. Involve school nurse or special educator.
Problem 5: Child developed new UTI during programme
Why: Holding behaviour has not yet reduced enough. Bladder still vulnerable.
Fix: Medical treatment first. Resume programme after UTI resolves. Request urgent school accommodation for private bathroom.
Problem 6: Relaxation techniques don't seem to help
Why: Techniques haven't been practised enough at home to automatise under anxiety.
Fix: Practise relaxation techniques DAILY at home — NOT in the bathroom — until automatic. Only then introduce during bathroom practice.
Problem 7: Child is more distressed now than when we started
Why: Exposure too fast; step gradient too steep; or undisclosed trauma component.
Fix: STOP home programme. Consult professional (OT/psychology). Call 9100 181 181 for teleconsultation guidance.
"Session abandonment is not failure — it's data. Every 'no' tells you where the work needs to happen next."
Adapt & Personalise
Your child is unique. Their protocol must be too.
⬅ Easier (use on difficult days or after regression)
Photos only — no actual bathroom exposure
Enter bathroom with parent for social comfort
Shorten duration targets by 50%
Add extra preferred item to sensory kit
Remove voiding pressure entirely — just practise presence
➡ Harder (use when child is ready to progress)
Attempt during slightly busier bathroom times
Reduce sensory supports by one item
Increase duration before leaving
Add voiding attempt requirement
Try a new bathroom (generalisation)
Child Profile Modifications
Profile | Modification | |
Auditory Hypersensitivity | Start with headphones always on; fade gradually over weeks | |
Anxiety/Paruresis dominant | Prioritise relaxation training; private bathroom longer before exposure to shared | |
Interoceptive differences (ADHD/Autism) | Timed voiding is essential; don't rely on body signals | |
Trauma history | Work with therapist; do not attempt exposure without professional guidance | |
Younger children (5–7) | Shorter sessions (3–5 min), more parent presence, simpler explanations, more tangible rewards | |
Older children (11–14) | Privacy is paramount; less parent visible presence; peer-relevant rewards | |
Bowel avoidance concurrent | Address both urination AND defecation avoidance; constipation worsens urinary symptoms |
Sensory Intensity Scale
Level 1
Empty bathroom, headphones, parent present
Level 2
Empty bathroom, headphones, parent outside
Level 3
Empty bathroom, earplugs only, parent outside
Level 4
Bathroom during quiet time, all supports
Level 5
Bathroom during typical time, minimal supports

Week 1–2: What to Expect
Foundation Phase
Progress: ~15%
Progress in weeks 1–2 looks tiny. It isn't. The foundations being laid now are why months 2–3 will accelerate.
✅ What You May See
Reduced resistance to discussing the bathroom (willingness to talk = neural progress)
Child handles sensory kit materials without protest
School accommodation request submitted
One or two successful scheduled bathroom attempts at quiet times
Child places sensor cover on toilet at home without distress
❌ What You Will Not See Yet
Independent school bathroom use (this takes 6–12 weeks)
Complete elimination of anxiety (calibrate for reduction, not elimination)
Perfect voiding every session (partial success counts)
Milestones to Celebrate This Week
"Child sat in bathroom for 2 minutes today without distress" ← This is huge.
"School agreed to try scheduled bathroom times" ← This is movement.
"Child used their flush sensor cover at home unprompted" ← This is ownership.
This week will feel slow. The fear that nothing is working is normal — and incorrect.
PMC11506176 | Sensory integration outcomes emerge across 8–12 week timelines; early phase focuses on tolerance and participation.

Week 3–4: Consolidation Signs
Consolidation Phase
Progress: ~40%
The neural pathways are forming. Watch for these signals — they are the measurable markers of synaptic consolidation.
✅ Child initiates picking up their sensory kit without prompting
✅ Asks about timed voiding schedule ("Is it bathroom time?")
✅ Uses bathroom at school at least 1–2 times per week (even with accommodation)
✅ Relaxation breathing becoming familiar — uses it without full prompting
✅ Vocabulary about the fear emerging: "I was scared but I went anyway"
✅ Gradual reduction in post-school bathroom desperation
What School Cooperation Looks Like by Week 3–4
Scheduled bathroom times in place
Teacher/nurse aware without peer disclosure
Bathroom pass system functioning
Headphone/sensory tool permission confirmed
Progression Decisions
Increase intensity if: All week 1–2 milestones met + child tolerating current exposure step for 3 consecutive sessions
Stay at current level if: Progress is patchy — consolidate before advancing
When a child starts anticipating the practice routine positively, synaptic consolidation is occurring. This is the inflection point.

Week 5–8: Mastery Indicators
🏆 Mastery Phase
Progress: ~75%
The bathroom is no longer the enemy.
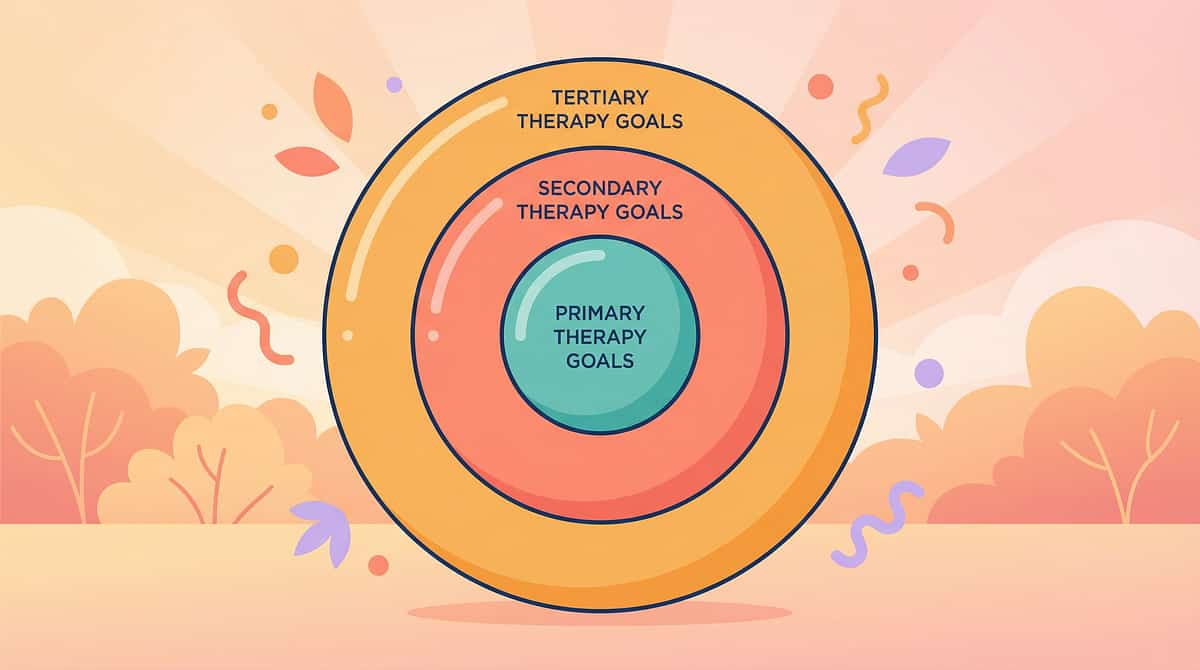
Mastery criteria are specific, observable, and measurable — not impressionistic. Use these to confirm your child has achieved the primary therapeutic target before beginning support fading.
Daily Use ✅
Uses school bathroom at least once per school day without acute distress
Voluntary Approach ✅
Approaches bathroom voluntarily with sensory supports when needed
Appropriate Intervals ✅
Holds urine for 3–4 hours — not all day
UTI Reduction ✅
UTI frequency has decreased (medical indicator)
Self-Communication ✅
Can communicate bathroom needs to teacher without excessive anxiety
Generalisation Indicators
Uses bathroom in at least one public/non-home location
Tolerates less-familiar bathrooms with sensory supports
Asks to go to bathroom at restaurants, shopping centres, family events
🏆Mastery Badge: School Bathroom Independence (Supported) — Child uses school bathroom daily with accommodation supports and minimal distress.
Pinnacle Toileting Independence Readiness Index: Emerging Independence
Pinnacle Toileting Independence Readiness Index: Emerging Independence
🎉 Celebrate This Win
You did this. Your child grew because of your commitment.
You watched your child in pain. Watched the UTIs, the accidents, the dehydration. You learned that this wasn't stubbornness — it was neurology. You built a sensory kit, submitted accommodation requests, practised breathing together, and celebrated every tiny step.
Weeks 5–8 ago, your child held it all day. Today, they used the school bathroom.
That is not a small thing. That is a transformation. That is your family's victory.
What Your Child Achieved
Neurological Courage
Overcame a genuine neurological fear response — not stubbornness, but real bravery
Lifelong Skills
Built self-regulation skills they will use for life, in classrooms, workplaces, and beyond
Self-Advocacy
Learned to advocate for their own needs and communicate with trusted adults
Bladder Health
Established bladder health habits that protect their body from long-term damage
Family Celebration Suggestions
Special Outing
A trip to your child's absolute favourite place — chosen by them
Document the Milestone
"Brave Chart Complete" photo — this record becomes your child's story of overcoming
Mastery Reward
The agreed-upon reward from your reward jar system — earned and celebrated

⚠️ Red Flags: When to Pause
Even in the progress zone — safety awareness continues. Watch for these signs and follow the escalation pathway.
🔴 Red Flag 1: Recurring UTIs (2+ in 3 months)
What it looks like: Frequent urination, burning, fever, foul odour
Why it matters: Chronic UTIs can cause kidney damage and permanent bladder dysfunction
Action: Urgent paediatrician visit. Do NOT continue home exposure without medical clearance. Request urgent school accommodation for private bathroom.
🔴 Red Flag 2: Severe Constipation (fewer than 3 BMs/week)
What it looks like: Abdominal pain, hard stools, soiling between attempts
Why it matters: Full bowel directly compresses the bladder, worsening urinary symptoms
Action: Paediatric consult. Dietary and medical management — often must be treated before bathroom programme succeeds.
🔴 Red Flag 3: School Avoidance Developing
What it looks like: Monday morning somatic complaints, refusal to attend, increasing general anxiety
Why it matters: Bathroom anxiety becoming a gateway to broader school refusal — a clinically complex and serious outcome
Action: Psychology consult. School counsellor involvement. Do not push bathroom programme while attendance is at risk.
🔴 Red Flag 4: Significant Regression After Progress
What it looks like: Return to complete refusal after multiple weeks of progress
Why it matters: May indicate a new stressor, a negative school bathroom experience, or undisclosed event
Action: Calm conversation with child. Consult therapist. Don't force exposure during regression.
🔴 Red Flag 5: Extreme Distress During Any Exposure Step
What it looks like: Panic attacks, vomiting from anxiety, acute meltdowns during bathroom practice
Why it matters: Traumatic exposure without adequate support worsens phobia
Action: STOP exposure programme. Professional support is required. Call 9100 181 181.

The Progression Pathway
You're not done — you're on a journey. Here's the map.
📍Your Current Position: E-503: School Bathroom Refusal (9 Materials) — Materials awareness and introduction
Prerequisites (What Came Before)
E-501: Encopresis and Soiling
Path A: School Bathroom Independence Deepening
E-505: Toileting Anxiety (if anxiety component is primary)
Deep-dive into Gradual Exposure Protocol (E-503-DD-02)
Sensory Regulation in Novel Environments technique
Path B: Toilet Training & Generalisation
E-504: Toilet Training Resistance (generalisation to other settings)
E-506: Public Bathroom Avoidance
Path C: Medical Management Integration
Functional Voiding Dysfunction protocol (medical/OT track)
Paediatric Urology consultation integration
Long-Term Goal
Full participation in school and community activities without bathroom-based limitation → School Functioning Readiness Index: Full Independence

Related Techniques in the Toileting Domain
More techniques in the Gastrointestinal & Toileting Domain (E-Series). You already have materials for several related techniques.
Technique | Code | Level | Materials You Already Have | |
Encopresis and Soiling | E-501 | Core | Sensory Kit ✓ | |
Nighttime Wetting | E-502 | Core | Visual Schedule ✓ | |
School Bathroom Refusal | E-503 | Core (You Are Here) | All 9 Materials | |
Toilet Training Resistance | E-504 | Foundation | Reward Jar ✓ | |
Toileting Anxiety | E-505 | Core | Social Stories ✓ | |
Public Bathroom Avoidance | E-506 | Advanced | Headphones ✓ |
"You already have materials for 4 related techniques in this domain."
Related Domains
Domain A: Sensory Processing
Domain C: Emotional Regulation
Domain B: Social Communication
Your Child's Full Developmental Map
This technique is one piece of a larger plan. Here's the whole picture. School bathroom refusal does not exist in isolation — it connects to sensory processing, emotional regulation, health, and academic participation.
Domain | Label | Status for This Child | |
A | Sensory Processing | 🔗 Connected to E-503 | |
B | Social Communication | — | |
C | Emotional Regulation | 🔗 Connected to E-503 | |
D | Behavioural Flexibility | — | |
E | Gastrointestinal & Toileting | 📍ACTIVE: E-503 | |
F | Motor Skills | — | |
G | Cognitive Development | — | |
H | Self-Care & Daily Living | 🔗 Connected to E-503 | |
I | Academic Readiness | 🔗 Connected (school functioning) | |
J | Social-Emotional Wellbeing | 🔗 Connected (anxiety impact) | |
K | Family Systems | 🔗 Connected (caregiver burden) | |
L | Medical & Health | 🔗 Connected (UTI, bladder health) |
Addressing school bathroom refusal through this multi-material framework moves multiple domains simultaneously. The technique you are implementing today is not a single fix — it is a systemic intervention.
WHO/UNICEF Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring. | UNICEF MICS indicators (42 per country, 197 countries).
Families Who've Been Here
From complete avoidance to confident bathroom use. These are real families.
Priya, Mother of 8-year-old Arjun — Hyderabad
Before (Month 0): "Arjun had not used the school bathroom in 14 months. He developed his third UTI of the year. His teacher called me twice a week about him holding himself in class. He refused to drink water. He was dehydrated by 1 PM every day. I was terrified."
Intervention: Noise-cancelling headphones + flush sensor covers + private nurse's bathroom accommodation + timed voiding schedule + gradual exposure with OT support.
After (Month 4): "He uses the school bathroom now. Not easily, not always, but he uses it. The UTIs stopped. He drinks water during school. He told me last week that 'the bathroom at school isn't so bad anymore.' I cried."
"From complete avoidance to 'not so bad' in four months. For us, that's everything."
Kavitha, Mother of 11-year-old Sneha — Bangalore
Before: "Sneha refused overnight field trips, school camps, sports days. Anything involving a non-home bathroom meant she stayed home. She was missing her entire school social life."
Intervention: Portable sensory kit + social story + graduated public bathroom exposure + peer-invisible accommodation (seat by door, teacher signal).
After: "She went on the school trip to Coorg. First overnight trip in four years. She called us from camp to say she used the bathroom there. She sounded so proud of herself."
From the therapist's notes: "Sneha's avoidance was primarily privacy and social anxiety-driven. Once the accommodation gave her a discrete exit and she had tools she trusted, the exposure work accelerated rapidly. The camp call was the clinical milestone I'd been working toward."
Outcomes vary. These are illustrative narratives based on aggregate Pinnacle centre outcomes. Individual progress depends on profile, anxiety severity, and support consistency.
Your Professional Support Team
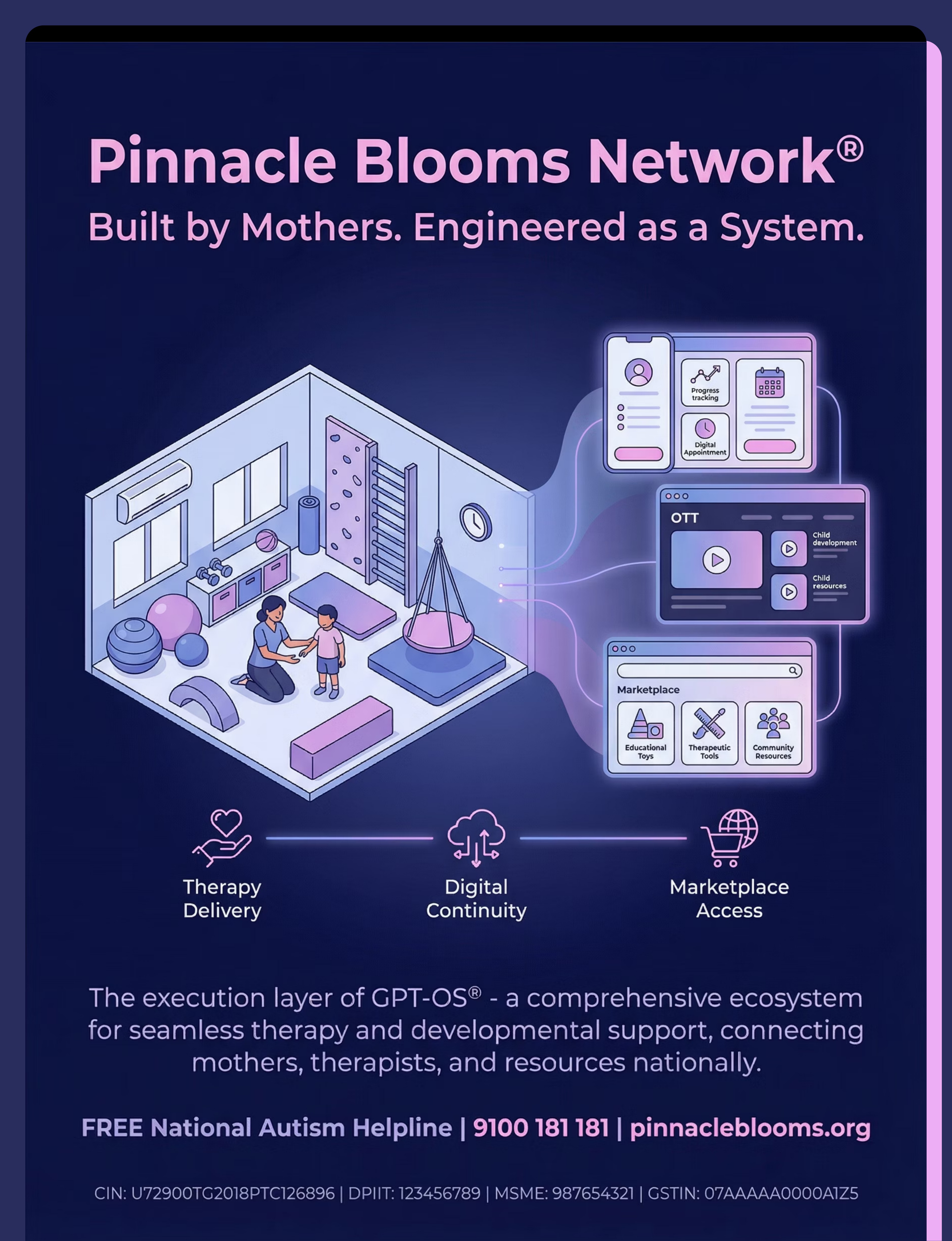
Home + Clinic = Maximum Impact. Your nearest Pinnacle centre brings all five disciplines together under one roof, coordinated through a single FusionModule™ plan.
Your Primary Concern | Specialist | Available At | |
Sensory overwhelm in bathroom | Paediatric Occupational Therapist | All centres | |
Anxiety / paruresis / exposure programme | ABA-BCBA + Paediatric Psychologist | Select centres | |
School accommodation support | Special Education Coordinator | All centres | |
UTI / bladder health | NeuroDevelopmental Paediatrician | All centres | |
Holistic plan coordination | FusionModule™ Multi-Disciplinary Team | All centres |
Teleconsultation — From Anywhere in India
Can't reach a centre? Our teleconsultation team brings Pinnacle expertise to your home. Same clinical quality. No travel required.
FREE National Helpline
📞9100 181 181
Available 24×7 | 16+ languages | First consultation guidance free
Available 24×7 | 16+ languages | First consultation guidance free
"This is not a call centre. These are therapists."
WHO NCF Progress Report (2023): 48% increase in countries adopting ECD policies. Primary healthcare as key platform for reaching all families.
Preview of 9 materials that help with school bathroom refusal Therapy Material
Below is a visual preview of 9 materials that help with school bathroom refusal therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!