She has every toy imagination needs.
Imagination hasn't arrived yet.
Imagination hasn't arrived yet.
"She opens the oven door and closes it. Over and over. But she never pretends to cook anything."
You bought the kitchen. Every pan. Every tiny plastic tomato. You arranged it beautifully. And she sorts it — by color, by size, by type — with a precision that takes your breath away. But she doesn't cook. Doesn't serve imaginary soup. Doesn't invite her dolls to a tea party. When you sit down and say "Let's feed the baby!" — she takes the spoon and lines it up with the others.
You are not failing. Her brain is not broken. Pretend play is a learnable skill — and it starts with the right materials.
🎭 Pretend Play
🧠 Symbolic Thinking
👁️ Theory of Mind
👶 Ages 2–8
You Are Among Millions of Families Navigating This Exact Challenge
Pretend play difficulties are one of the most consistent early indicators of autism spectrum conditions and related developmental differences. But here is what the data also shows: pretend play skills improve with targeted intervention. This is not a permanent ceiling — it is a current location on a developmental map.
1 in 36
Children with Autism
Children diagnosed with autism globally (CDC 2023)
60–70%
Show Play Deficits
Of children with ASD show significant pretend play deficits
21M+
Therapy Sessions
Sessions delivered by Pinnacle across India — tracking this exact skill
Across India, an estimated 10–13 million children are on the autism spectrum. Symbolic play delays also affect children across multiple diagnostic categories — language delays, developmental delays, sensory processing differences, and more. You are not alone. This challenge has a name. It has a path forward.
📊India-Specific Evidence: Padmanabha et al., Indian Journal of Pediatrics (2019): Home-based developmental interventions demonstrated significant measurable outcomes in Indian pediatric populations — confirming that family-driven intervention works in our context.
This Is Not a Behavior Problem. This Is a Wiring Difference.
Pretend play requires five simultaneous brain capacities working together. In children with autism or developmental differences, these networks develop on a different timeline — or need explicit teaching to connect. This is not deficit. This is difference. And difference responds to the right input.
Symbolic Thinking
(Prefrontal Cortex) Understanding that one thing can represent another — a block can be a phone. This requires holding TWO realities in mind at once.
Mental Representation
(Working Memory Networks) Keeping an idea in mind that isn't physically present. Imagining what the doll is "feeling" when it isn't real.
Theory of Mind
(Temporal-Parietal Junction) Understanding that others have thoughts, feelings, and perspectives different from your own — the foundation of all social play.
Cognitive Flexibility
(Prefrontal-Striatal Circuits) Shifting between the real world and the pretend world — and back again. Many children with autism have more rigid, literal neural pathways.
Narrative Capacity
(Default Mode Network) Sequencing events into stories — "first this, then that, then what happens." The storytelling brain.
Frontiers in Integrative Neuroscience (2020): Comprehensive neurological framework for understanding symbolic play and imagination in ASD. DOI: 10.3389/fnint.2020.556660
Your Child Is Here. Here Is Where We're Heading.
Understanding where your child sits on the developmental play continuum is not about labeling — it's about knowing which signpost to aim for next. Many children with ASD or developmental differences are at the Functional Play stage past age 3, or showing early symbolic play with heavy support. Your child is not behind — they are on a developmental path that needs more visible signposts.
12–18 Months
Functional Play — Using real objects for their real purpose
18–24 Months
Early Symbolic — Pretend drink from empty cup
2–3 Years
Role Play — "I'm the doctor," doll has a name
3–4 Years
Sociodramatic — Multi-character storylines
4–6+ Years
Complex Peer Play — Negotiated roles, elaborate worlds
🔗 Language
Language delays often co-occur with symbolic play delays
🔗 Sensory
Sensory sensitivities can block engagement with play materials
🔗 Anxiety
Anxiety can restrict play to safe, repetitive patterns
🔗 Executive Function
Executive function differences affect scenario-building

Clinically Validated. Home-Applicable. Parent-Proven.
This is not occupational therapy folklore. This is peer-reviewed science that Pinnacle has now applied across 20 million therapy sessions. Every material recommendation, every facilitation step, and every progress indicator on this page is grounded in evidence meeting Level I–II standards.
📋 PRISMA Systematic Review (2024)
16 studies confirm that play-based and material-supported interventions for children with ASD meet criteria to be classified as evidence-based practice. Adult facilitation + structured materials = measurable gains.
📋 Meta-Analysis (World J Clinical Cases, 2024)
24 studies: Material-supported play therapy effectively promotes social skills, adaptive behavior, and imagination capacity across diverse populations.
📋 Indian RCT — Padmanabha et al. (2019)
Home-based developmental interventions with parent implementation demonstrated significant outcomes — validating the home execution model central to Pinnacle's approach.
📋 NCAEP Evidence-Based Practices Report (2020)
Video modeling, visual supports, and structured play interventions are classified as evidence-based practices for autism.
90%
Pretend Play Material Interventions
Strong evidence across systematic reviews
95%
Adult Facilitated Play
Strong evidence — the strongest signal in the literature
85%
Home-Based Execution
Strong evidence for parent-administered protocols

🎭 Pretend Play Material Facilitation
Parent-Friendly Alias: "The Imagination Toolkit"
Definition: Pretend Play Material Facilitation is the deliberate selection and deployment of specific therapeutic materials — each chosen for their evidence-based capacity to reduce barriers to symbolic thinking, scaffolding the child's journey from literal, functional toy use toward flexible, imaginative, narrative play. Unlike waiting for pretend play to emerge spontaneously, this approach creates structured invitations to imagination — using props, costumes, puppets, building materials, and adult partnership to make the leap from "this is a block" to "this block is a phone" shorter, safer, and more achievable.
Age Range
2–8 years
Session Duration
10–20 minutes
Frequency
Daily
Setting
Home + Therapy
🎭 Play Development
🧠 Symbolic Thinking
👥 Social-Emotional
🔄 Cognitive Flexibility
👁️ Theory of Mind
🎬 This technique page accompanies Reel G-623 from the Social-Emotional & Play Development in Children series. Pinnacle 128 Canon Materials taxonomy | 20 Category classification system | GPT-OS® Domain G: Play Development.
This Technique Crosses Therapy Boundaries
Because a child's brain doesn't organize itself by therapy type
🔶 Occupational Therapy — Lead Discipline
OTs use play material selection as sensory-motor scaffolding. Each material is chosen for its sensory properties (texture, weight, resistance) and the motor patterns it invites. Play IS the OT session for children in the 2–8 age range. "The material is the medium and the message."
🔷 Speech-Language Pathology — Co-Lead
SLPs exploit pretend play as the richest language learning environment available. When a child pretends, they use new vocabulary, narrative structure, and perspective language — all within a single play scenario. "Language lives inside stories. Stories live inside pretend."
🟣 ABA / BCBA — Behavior & Learning Architecture
Behavior analysts structure play sessions using reinforcement schedules, prompting hierarchies, and systematic fading. They identify the motivating operations that make a child want to engage with play materials. "Motivation is the on-ramp. Structure is the highway."
🟢 Special Education — Generalization & Curriculum
Special educators connect pretend play skills to curriculum goals — narrative comprehension, cooperative learning, social scripts. They build pretend play into classroom routines and ensure skills generalize from home to school. "Play is the curriculum for early childhood."
Precision Tool. Not Random Activity.
Every material in this toolkit has a defined therapeutic target. Understanding the layered goals — from immediate symbolic thinking all the way to long-term friendship formation — helps you stay oriented when progress feels slow and celebrate when it's happening.
Observable: Primary
"Child picks up a block and says 'It's a phone!' without prompting."
Observable: Secondary
"Child says 'The baby is sad because…'" — narrative language and empathy emerging together.
Observable: Tertiary
"Child initiates play scenario with a sibling or peer" — generalization to real social contexts.

9 Materials. One Imagination Toolkit.
Each chosen by Pinnacle's multi-disciplinary consortium for its specific role in building pretend play

1. Realistic Miniature Play Sets 🍳🩺🔨
Canon Category: Functional Play Props
Why it works: Realistic props reduce the cognitive leap required for pretend. When a toy stethoscope looks like a real stethoscope, the child only has to imagine what to do with it — not what it is. This scaffolds symbolic play by making the "symbol" closely match the "real thing."
Price Range: ₹500–3,000 | DIY: Real kitchen items (supervised), empty bottles, old clothes
Why it works: Realistic props reduce the cognitive leap required for pretend. When a toy stethoscope looks like a real stethoscope, the child only has to imagine what to do with it — not what it is. This scaffolds symbolic play by making the "symbol" closely match the "real thing."
Price Range: ₹500–3,000 | DIY: Real kitchen items (supervised), empty bottles, old clothes

2. Dolls & Figures with Simple Features 🧸
Canon Category: Character Figures / Theory of Mind Props
Why it works: Dolls become "other minds" — the child assigns them thoughts, feelings, and actions. Simple features (not hyper-realistic) allow more projection and imagination. This is foundational Theory of Mind practice.
Price Range: ₹200–1,500 | DIY: Sock puppets, wooden peg dolls, toilet roll figures
Why it works: Dolls become "other minds" — the child assigns them thoughts, feelings, and actions. Simple features (not hyper-realistic) allow more projection and imagination. This is foundational Theory of Mind practice.
Price Range: ₹200–1,500 | DIY: Sock puppets, wooden peg dolls, toilet roll figures

3. Dress-Up Clothes & Role-Play Costumes 👑🎩🦸
Canon Category: Role-Play / Identity Props
Why it works: Dress-up makes pretend physical. When a child puts on a firefighter hat, they don't just play WITH a firefighter — they BECOME one. Physical transformation scaffolds the mental transformation that pretend play requires.
Price Range: ₹300–2,000 | DIY: Scarves as capes, colander as helmet, old shirts as aprons
Why it works: Dress-up makes pretend physical. When a child puts on a firefighter hat, they don't just play WITH a firefighter — they BECOME one. Physical transformation scaffolds the mental transformation that pretend play requires.
Price Range: ₹300–2,000 | DIY: Scarves as capes, colander as helmet, old shirts as aprons

4. Open-Ended Building Materials 🧱🔷📦
Canon Category: Construction Play / Spatial Cognition
Why it works: Building materials let children CREATE the worlds their imagination will inhabit. "Building the stage" is an accessible entry for children with strong spatial/construction interests. Once the castle is built, figures can live there.
Price Range: ₹500–4,000 | DIY: Cardboard boxes, cushions, fabric — all free
Why it works: Building materials let children CREATE the worlds their imagination will inhabit. "Building the stage" is an accessible entry for children with strong spatial/construction interests. Once the castle is built, figures can live there.
Price Range: ₹500–4,000 | DIY: Cardboard boxes, cushions, fabric — all free

5. Puppets & Stuffed Animals 🤚👆🧸
Canon Category: Puppets / Voice Externalization Props
Why it works: Puppets give "other minds" a voice. When a puppet speaks with its own personality, the child SEES imagination in action. Puppets also provide safe emotional distance — the puppet is scared, not the child.
Price Range: ₹200–1,500 | DIY: Sock puppets, paper bag puppets, spoon puppets
Why it works: Puppets give "other minds" a voice. When a puppet speaks with its own personality, the child SEES imagination in action. Puppets also provide safe emotional distance — the puppet is scared, not the child.
Price Range: ₹200–1,500 | DIY: Sock puppets, paper bag puppets, spoon puppets

6. Play Dough & Modeling Materials 🎨🏺🌊
Canon Category: Creative Construction / Sensory-Motor Play
Why it works: Play dough lets children CREATE their own props. Making a pizza from dough IS already imagining what it will become. The sensory experience also calms and regulates — reducing anxiety that can block pretend play.
Price Range: ₹100–800 | DIY Recipe: 1 cup flour + ½ cup salt + 2 tbsp cream of tartar + 1 cup water + 1 tbsp oil. Cook until ball forms. ~₹20 | 10 minutes
Why it works: Play dough lets children CREATE their own props. Making a pizza from dough IS already imagining what it will become. The sensory experience also calms and regulates — reducing anxiety that can block pretend play.
Price Range: ₹100–800 | DIY Recipe: 1 cup flour + ½ cup salt + 2 tbsp cream of tartar + 1 cup water + 1 tbsp oil. Cook until ball forms. ~₹20 | 10 minutes

7. Scenario Cards & Story Kits 📋🎲📖
Canon Category: Visual Narrative Supports / Script Starters
Why it works: Many children with autism don't pretend because they don't know WHAT to pretend about. Scenario cards provide the "script" for imagination — a visual starting point that reduces open-ended cognitive demand and teaches narrative structure over time.
Price Range: ₹300–1,500 | DIY: Draw or print 6 common scenarios; laminate with tape
Why it works: Many children with autism don't pretend because they don't know WHAT to pretend about. Scenario cards provide the "script" for imagination — a visual starting point that reduces open-ended cognitive demand and teaches narrative structure over time.
Price Range: ₹300–1,500 | DIY: Draw or print 6 common scenarios; laminate with tape
8. Cause-Effect Toys (Foundation Layer) 🎯🎵🧩💡
Canon Category: Cause-Effect / Proto-Symbolic Play
Why it works: Before pretend, children must understand "I do something → something happens." This is the cognitive foundation pretend play is built on. For children at early play stages, cause-effect toys are the essential precursor — the on-ramp to all symbolic play.
Price Range: ₹300–1,500
Why it works: Before pretend, children must understand "I do something → something happens." This is the cognitive foundation pretend play is built on. For children at early play stages, cause-effect toys are the essential precursor — the on-ramp to all symbolic play.
Price Range: ₹300–1,500

9. Adult Play Partner Guides 📚🖼️📱
Canon Category: Adult Facilitation Resources / Parent Training
Why it works: The most important "material" is YOU — a skilled play partner who models, scaffolds, and extends imagination. Adult guides and visual supports provide the "how to" — turning every caregiver into a therapeutic play partner. The toy is secondary. You are primary.
Price Range: ₹200–2,000 (many free resources available)
Why it works: The most important "material" is YOU — a skilled play partner who models, scaffolds, and extends imagination. Adult guides and visual supports provide the "how to" — turning every caregiver into a therapeutic play partner. The toy is secondary. You are primary.
Price Range: ₹200–2,000 (many free resources available)
Every Child Deserves Access to Imagination
WHO/UNICEF Equity Principle: No child left behind due to cost
The research does not show that expensive materials produce better outcomes than household equivalents. What the research DOES show is that adult presence, modeling, and consistent engagement is the non-negotiable ingredient. The toy is secondary. You are primary.
🛒 Clinical Material | 🏠 Zero-Cost Substitute | |
Realistic Doctor Kit ₹800+ | Empty shampoo bottles, old ruler = thermometer, cloth bandages from torn fabric | |
Dolls with simple features ₹400+ | Sock with two button eyes. Or toilet rolls with drawn faces. | |
Dress-up costume set ₹1,000+ | Any scarf = cape. Colander = helmet. Mum's dupatta = princess gown. | |
Wooden blocks ₹800+ | Collect clean cardboard boxes of different sizes for 2 weeks. Stack and build. | |
Hand puppets ₹300+ | Sock over hand. Add two googly eyes with craft glue (₹10). | |
Play dough ₹200+ | 1 cup flour + ½ cup salt + 2 tbsp cream of tartar + 1 cup water + 1 tbsp oil. 5 minutes. Free. | |
Scenario cards ₹400+ | Draw 6 pictures: birthday, kitchen, doctor, park, bedtime, shop. Laminate with tape. ₹0. | |
Cause-effect toys ₹500+ | Tissue box with items to pull out. Container with lid. Cup and saucer. All cause-effect. | |
Adult Play Partner Guide | This page. Cards 14–19 are your free, permanent guide. |
Combine: 1 cup flour + ½ cup salt + 2 tbsp cream of tartar in a pot
Add: 1 cup water + 1 tbsp cooking oil. Stir over medium heat until a non-sticky ball forms.
Remove, knead when cool. Add food coloring if desired. Store airtight — lasts 2–4 weeks. Cost: ~₹20 | Time: 10 minutes

Read This Before Every Session
🟢 GREEN: Proceed Normally
Child is fed, rested, and calm-regulated. Materials are age-appropriate. Play space is prepared. Child has not had a severe meltdown in the last 2 hours. You (the caregiver) are calm and have 15–20 minutes.
🟡 AMBER: Modify Session
Child seems tired or slightly dysregulated → shorten to 5–8 minutes, use only their preferred material. New material today → use alongside a familiar, loved item. Child is resistant → offer material and move away; return in 5 minutes.
🔴 RED: Postpone Session
Child is ill or in physical discomfort. Child has had a severe meltdown within the last 2 hours. You are significantly stressed or overwhelmed — children co-regulate with caregivers.
⚠️ No small parts if child mouths objects (common in ASD)
⚠️ Homemade play dough is non-toxic but not for eating in quantity (high salt)
⚠️ Dress-up: no cords, ties, or strings near the neck
⚠️ Cardboard boxes — remove all staples before use
"Session abandonment is not failure. It is data. Note what happened and bring it to your therapist."
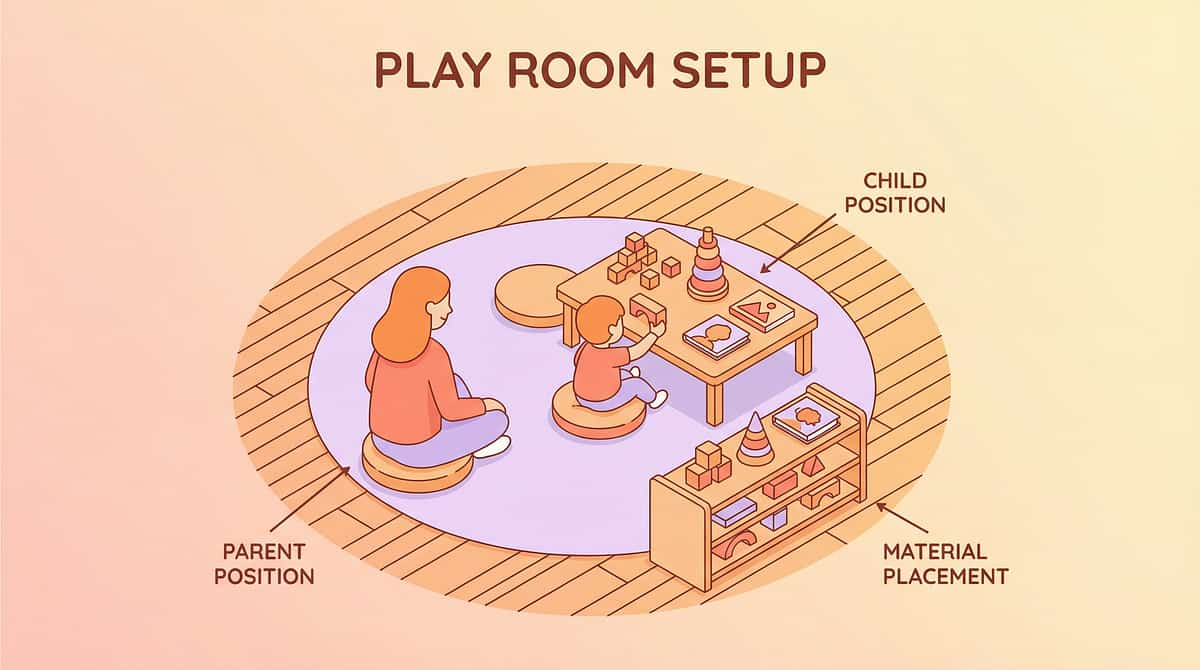
The Right Space Reduces 80% of Session Failures
The Setup Rules
- ✅Materials: 2–3 items maximum — not the whole toy box
- ✅Positioning: Parent at child's eye level, slightly to the side
- ✅Lighting: Natural or warm — not harsh fluorescent
- ✅Noise: Low background. Gentle instrumental music optional
- ✅Space: Small, cozy — a play mat or defined carpet area
- ✅Duration: Set a visual timer — 15 minutes is enough
- ✅ALL screens OFF. Including yours.
"Less Is More" Principle
Too many materials = decision paralysis. Two options = choice. One focused scenario = progress. Begin with a single play set and one doll. Build complexity over weeks, not days.
Preparing Yourself
- Put your phone in another room
- Take three slow breaths before you begin
- Enter play mode: your job is to follow, not lead
- Remember: no outcome is required from this session. Presence is the intervention.
Sensory Integration Theory (Ayres): Environmental setup is a core principle of effective sensory-motor intervention. Meta-analysis confirms structured individual sessions produce maximum outcomes. PMC10955541
60-Second Pre-Flight Check
The best session is one that starts right
Indicator | ✅ GO | 🟡 MODIFY | 🔴 POSTPONE | |
Last meal | 30+ min ago | 15 min ago | Just fed / hungry | |
Sleep | Rested | Slightly tired | Overtired / just woke | |
Last meltdown | 3+ hours ago | 1–2 hours ago | Under 1 hour | |
Current state | Calm / happy | Slightly fussy | Dysregulated | |
Your state | Calm | Manageable | Stressed / rushed |
✅ IF GO
Proceed to Step 1: The Invitation (next card).
🟡 IF MODIFY
Shorten to 5–8 minutes. Use only child's most preferred material. Reduce demands completely — pure play, no teaching. Sit nearby and play alone; child may join.
🔴 IF POSTPONE
Offer a preferred calming activity instead. Note the reason — patterns matter. Reschedule for same time tomorrow. No guilt. Knowing when NOT to push is expert-level parenting.

STEP 1 OF 6
The Invitation
Every session begins with an invitation, not a command
"I'm going to play with [the doctor kit / the kitchen / the puppets]. You can watch, or you can join me if you want."
Then: start playing. Make the puppet say something. Pick up a pan. Examine a "sick" doll. Do NOT look at the child to see if they're watching. Just play.
Body Language Guide
- 😌 Relaxed, unhurried posture
- 👀 Eyes on the materials, not the child
- 🗣️ Low, warm, playful voice — talking to yourself or the materials
- ⏱️ Give 45–60 seconds before any prompting
Acceptance Cues — Watch For:
- Child moves closer to the materials
- Child watches your hands
- Child reaches for a piece
- Child makes a sound or comment
- Even a glance counts — that's engagement beginning
Resistance Cues & Response:
Child moves away → Keep playing quietly. Child tries to take materials → Offer: "Do you want to play?" Child ignores → Play 3 minutes, then gently offer a prop: "For you."
⏱️ Timing: 30–90 seconds
STEP 2 OF 6
The Engagement
Child has moved closer or shown interest — now deepen it
"Oh look — the baby doll is hungry. I wonder what she wants to eat?"
"Let me check — does the baby want the apple or the bread?"
WAIT. 10 full seconds. Do not fill the silence.
Narrate
What's happening in simple present tense — out loud, warmly
Offer
A prop or simple choice near the child's hands
Wait
Longer than feels comfortable. Silence is working.
Receive
Whatever the child gives — any response = success
Mirror
Their action back with delight: "Yes! The baby gets the apple!"
🟢 Ideal
Child picks up material, assigns action or dialogue
🟡 Acceptable
Child watches closely, hands a prop to you, gestures
🔴 Concerning
Child appears anxious, tries to leave, covers ears
⏱️ Timing: 1–3 minutes

STEP 3 OF 6
The Therapeutic Action
The active ingredient — choosing which of the 9 materials to use and how
▶ Realistic Play Sets (Material 1)
MODEL the scenario script clearly: "The baby is sick. She needs the doctor. Let me listen to her heart." Use stethoscope on doll. Hand to child. Minimal words.
▶ Dolls & Figures (Material 2)
Give the doll a VOICE: "Hello! I'm hungry! I want some food!" Then pause. Look at child. Wait for response to the doll — not to you.
▶ Dress-Up (Material 3)
PUT ON an item yourself first: "I'm the doctor now." Make one medical gesture. Offer child a piece: "Do you want to be the patient or the other doctor?"
▶ Building Materials (Material 4)
Build something, then INVITE habitation: "Look — I made a house. Who lives here?" Place a figure nearby. Wait.
▶ Puppets (Material 5)
Give puppet its OWN DISTINCT VOICE and personality. Puppet asks child questions directly: "Hi! I'm scared of the dark. Can you help me?"
▶ Play Dough (Material 6)
MAKE something together: "We're making a birthday cake. How many candles? You put the candles." Then: "Whose birthday is it?"
▶ Scenario Cards (Material 7)
SHOW 2 cards: "Which one? Birthday party or going to the doctor?" Child points → gather props → begin. YOU set up; child enters.
▶ Cause-Effect Toys (Material 8)
CELEBRATE the effect dramatically: "You did it! He jumped out!" Add a story: "He jumped because he was excited to see you!"
▶ Adult Facilitation (Material 9)
YOU are the material. Narrate everything. Wait after every sentence. Expand every response the child gives, however small.
⏱️ Core Action Duration: 5–10 minutes
STEP 4 OF 6
Repeat & Vary
3 good repetitions > 10 forced ones
Sessions 1–5
1–2 play scenarios per session. Adult leads entirely.
Sessions 6–10
2–3 scenarios with slight variation. Child begins imitating.
Sessions 11–20
Introduce object substitution: "What else could the spoon be?"
Sessions 21+
Child begins initiating variations — you respond and expand.
Variation Ideas
- Same script, different character: "Now YOU are the doctor and I'm the patient"
- Same material, new scenario: kitchen → cooking → restaurant → birthday party
- Add a "problem": "Oh no! The baby lost her shoe! Where is it?"
- Let child choose: "This scene or that scene?" [2 options only]
Satiation Indicators — Child Is Done:
- Attention drifts elsewhere
- Begins reorganizing or sorting materials (functional play reverting)
- Vocal protest or physical escape
- Decrease in energy or engagement
When you see satiation → proceed to Step 6: Cool-Down

STEP 5 OF 6
Reinforce & Celebrate
Timing matters more than magnitude — within 3 seconds of the desired behavior
THE GOLDEN RULE: Celebrate the attempt, not just the success.
🗣️ Verbal Praise (Always Available)
- "YES! You made the doll fly! She's so happy!"
- "I LOVE that idea — the bear is going to school!"
- "That was YOUR idea! I didn't think of that!"
- "You're playing! Look at what you did!"
🤗 Physical (If Child Accepts — Never Forced)
- High five
- Quick hug
- Thumbs up with eye contact
🎭 In-Play Celebration (Most Therapeutic)
- Make the doll respond enthusiastically to child's action
- Have the puppet "applaud" the child
- Let the child's action "cause" something wonderful in the story
❌ What NOT To Do
"Good job" (too generic — child doesn't know what they did). Praising too much for too little (devalues reinforcement). Praising with conditions: "Good, but next time…"

STEP 6 OF 6
The Cool-Down
No session ends abruptly — the transition IS part of the therapy
2 Minutes Before End
"Two more minutes of playing, then we'll put the things away." [Hold up 2 fingers]
1 Minute Before
"One more minute. What should we do in our last minute?" [Let child choose final action — this is their agency]
At End
"All done! Time to put the [doctor kit] away together." [Involve child in putting away — it's part of the ritual]
Cool-Down Activity
1–2 minutes of a preferred sensory activity, reading 2 pages of a favorite book, or looking at photos of the session together.
"I know you want to keep playing. We'll play again [tomorrow/after dinner]. The toys will wait for you."
❌ Do NOT abruptly end. ❌ Do NOT promise "we'll do more later" if you can't keep it. ❌ Do NOT let the session run indefinitely — clear endings build trust.
60 Seconds of Data Now Saves Hours of Guessing Later
Tracking three simple data points after every session gives you — and your therapist — the evidence needed to adjust, progress, and celebrate. Patterns invisible to memory become clear in data. You don't need to be a clinician to collect meaningful information.
Engagement Level (1–5)
1 = No engagement | 2 = Watched from distance | 3 = Brief interaction | 4 = Active play 5+ min | 5 = Initiated play independently
Any Pretend Act?
None | Functional | Object-person action | Object substitution | Role play ("I am the doctor") | Created a narrative (connected two events)
Session Details
Date + Duration + Material Used. Note any resistance, win moments, or surprises.
📄 Download the Weekly Pretend Play Tracking Sheet (PDF) → Link to GPT-OS® tracking resource
📱 Log this session in GPT-OS® → pinnacleblooms.org/gpt-os/tracker
📱 Log this session in GPT-OS® → pinnacleblooms.org/gpt-os/tracker
The Reality Card. Most Sessions Don't Go Perfectly.
No parent should feel they failed — the technique needed adjustment, not the parent
Problem: Child showed no interest at all
Why: Material may not match child's interests or readiness. Fix: Use child's favorite character/interest as a PROP (beloved train = train needs a doctor). Start with cause-effect toy to build engagement first.
Problem: Child only sorted or spun the materials
Why: Child is at functional/sensory play stage — this is WHERE they are. It's data, not failure. Fix: Don't redirect. Play BESIDE them doing pretend with the same materials. Wait. Narrate. Don't insist.
Problem: Child became dysregulated or distressed
Why: Too much demand, wrong sensory profile, or an off day. Fix: STOP. Transition to preferred calming activity. Note the trigger. Share with therapist. Next time: start slower, lower demand, shorter.
Problem: Child only scripts from TV/media
Why: Scripted scenarios from media ARE symbolic play — they need to be expanded. Fix: WELCOME the script. Play ALONG. Then gently add: "And then what did [character] do?" Expand from their starting point.
Problem: Session worked great for 3 days, now child refuses
Why: Normal. Skill acquisition is not linear. Regression days are universal. Fix: Offer from distance. Don't push. Note it. A regression day is often a consolidation day happening internally.
Problem: Child pretends in therapy but not at home
Why: Context dependency is common — skills emerge in safe environments first. Fix: Bring ONE item from therapy home. Ask therapist to walk you through exactly what they do. Video modeling helps.
No Two Children Are Identical. Your Version May Look Different.
For Sensory Avoiders
- Start with visually calm, non-textured materials
- Play dough last — introduce slowly
- Costumes: just a hat, nothing full
- Low volume on any musical toys
- Reduce visual complexity in the play space
For Sensory Seekers
- Start with kinetic sand or textured play dough
- Build physical scenarios (forts, tunnels to "enter")
- Use full-body costumes — they WANT the transformation
- Add movement: "fly" the doll through the air, roll figures across floor
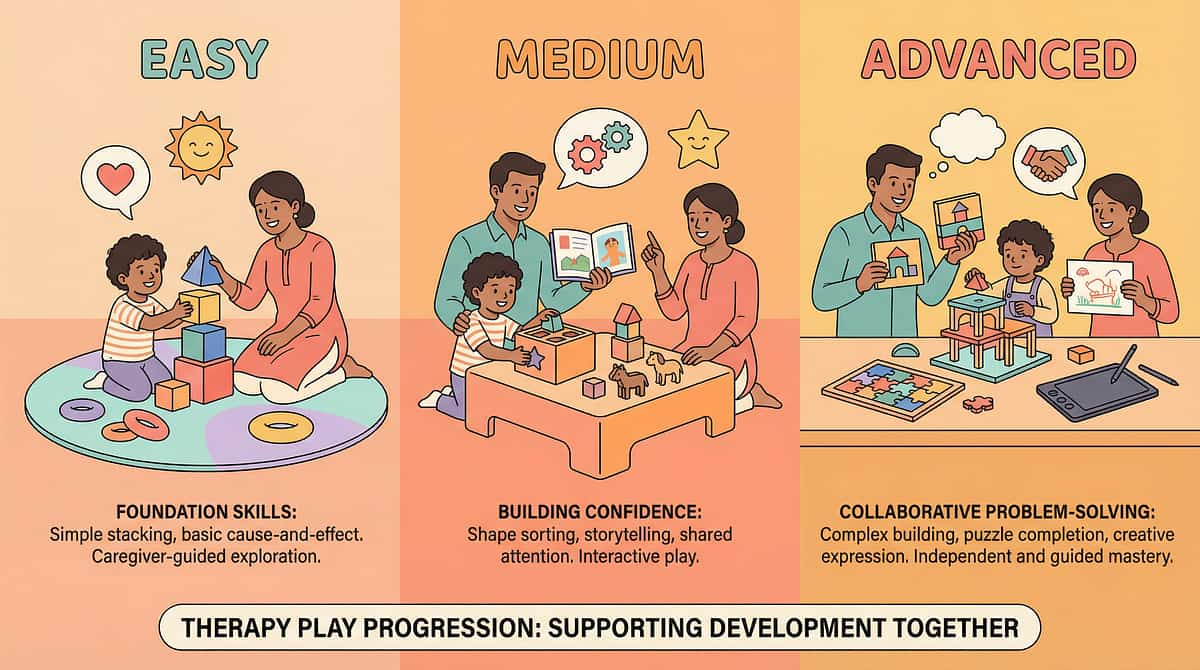
Feature | Age 2–3 | Age 3–5 | Age 5–8 | |
Materials | Cause-effect only | Realistic props + dolls | All 9 materials | |
Adult Role | Adult does 90% | Adult models, child joins | Child initiates, adult expands | |
Session Length | 5 min sessions | 10–15 min sessions | 15–20 min sessions | |
Complexity | One object at a time | 2–3 prop scenarios | Full scenario kits |
Special Interest Entry Points: If child loves trains → train is the "patient" at the doctor. If child loves dinosaurs → dinosaur needs a bandage, has a family. Any special interest = a doorway into pretend.
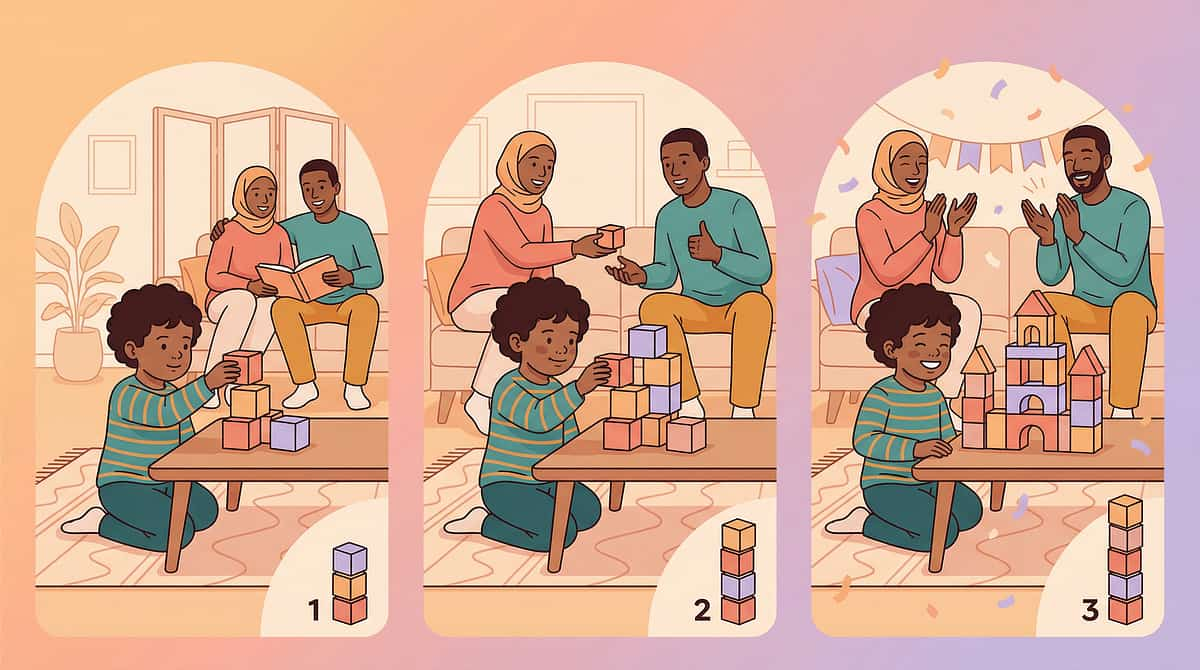
WEEK 1–2
Planting Seeds
Calibrating your expectations is not lowering the bar — it's measuring the right thing
✅ Increased tolerance of the materials (not mastery)
✅ Reduced resistance to play attempts (not elimination)
✅ Watching rather than engaging (participation, not production)
✅ Brief, fleeting moments of engagement (3–5 seconds at a time)
✅ Continued preference for functional/sorting play — this is still stage-appropriate
"If your child tolerates sitting near the pretend play materials for 3 seconds longer than they did on Day 1 — that is real, measurable, meaningful progress."
Many parents feel discouraged in weeks 1–2. The child doesn't seem to "get it." Sessions feel forced. This is universal. The brain is processing. The neural pathways are forming beneath the surface. Keep going. Watch your Engagement Level score (Card 20 tracker) — even tiny upward movement is everything.

WEEK 3–4
The Neural Pathways Are Forming
These are the signs that most parents miss because they're looking for the wrong things
Anticipates Sessions
Child goes to play area, looks for materials before you set up
Longer Engagement
Seconds become minutes — sustained attention growing
Begins Imitating
Specific play actions they've watched you model appear spontaneously
Object-Person Actions
Makes doll move, gives figure to parent — first "other mind" moments
Generalization Seeds — Watch For:
- Child spontaneously uses a household object in an unexpected way outside of play session
- Child references a play character during non-play time ("the baby wants…")
- Child initiates approach to play materials without being prompted
When to Increase Intensity:
- Child is consistently at Engagement Level 4 (Card 20 tracker)
- Sessions feel easy and natural
- Child is beginning to show initiative
"You may notice you are more confident too. The techniques are becoming natural. You are becoming your child's therapeutic play partner."

WEEK 5–8
The Imagination Is Opening
Here are the specific behaviors that signal readiness to progress
✅ Initiates Pretend Play
Child begins pretend play without adult prompting — even briefly, even once
✅ Assigns Role or Voice
Child assigns a role or voice to at least one figure or puppet
✅ Object Substitution
Child occasionally calls one thing by another name — the symbolic leap has landed
✅ 2-Part Sequence
"Baby is hungry → feeds baby" — narrative structure is emerging
✅ Skill Generalization
Pretend play appears in contexts beyond the structured session
🏅 When to Move to Next Level
Mastery achieved on 3 of 5 criteria = ready to advance → G-624: Parallel Play Development
techniques.pinnacleblooms.org/play-development/parallel-play-G-624
techniques.pinnacleblooms.org/play-development/parallel-play-G-624
When to Stay & Strengthen
Some children need 12–16 weeks at this stage. Progress is not always linear — mastery may slip and return. Talk to your Pinnacle therapist about AbilityScore® reassessment if unsure.

🎉 You Did This. Your Child Grew Because of Your Commitment.
Weeks ago, you watched your child line up every toy in the kitchen — perfectly, endlessly — and wondered if imagination would ever come. You read this page. You gathered the materials. You sat on the floor. You played alone and waited. You kept going when sessions didn't work. And then — maybe quietly, maybe suddenly — your child made the doll say something. Or put on the hat and became the character. Or made a block into a phone. That moment? You created it.
🎭 Pretend Play Foundation
ESTABLISHED
🧠 Symbolic Thinking
EMERGING
👁️ Theory of Mind
BUILDING
🔗 Next Domain
Parallel Play (G-624) — READY TO BEGIN
Family Celebration Suggestion: Take a photo of your child playing. Write one sentence about what you saw. Keep it. One day you will show it to them and they will be amazed at how far they've come.
Trust Your Instincts. If Something Feels Wrong — Pause and Ask.
🔴 Regression After Progress
Child who was pretending stops completely, especially if accompanied by other behavioral changes — seek developmental assessment promptly.
🔴 Increasing Distress Around Materials
If sessions consistently produce anxiety rather than reducing it — material type may be mismatched. Consult your therapist before continuing.
🔴 No Change After 12 Weeks
No change after 12 weeks of consistent daily sessions: formal reassessment of foundational skills (theory of mind, symbolic thinking) may be indicated.
🔴 Social Withdrawal Increasing
If child is becoming more isolated in other contexts while you work on play — broader evaluation is needed.
🔴 Material Safety Incidents
Any mouthing/swallowing of small parts; skin reactions to play dough ingredients; any physical injury — stop and assess immediately.
"Every flag you notice is a data point — not a disaster. Early notification always leads to better outcomes than delayed action."
You Are Not Done. You Are at a Waypoint.
→ G-624: Parallel Play
For children who have emerging symbolic play but no peer interaction yet. techniques.pinnacleblooms.org/play-development/parallel-play-G-624
→ G-625: Cooperative Play
If child is beginning to invite or notice peers during play scenarios
→ B-131 / C-318: Lateral Alternatives
Communication domain approach and emotional regulation angle to the same skill — if this pathway didn't fully resonate
Explore More in the Play Development Domain
Technique | Code | Difficulty | Canon Materials | |
9 Materials for Sensory Play | G-621 | 🟢 Intro | Sensory bins, tactile materials | |
9 Materials for Functional Play | G-622 | 🟢 Intro | Realistic props, cause-effect toys | |
9 Materials for Pretend Play | G-623 | 🟡Core | All 9 materials (THIS PAGE) | |
9 Materials for Parallel Play | G-624 | 🟡 Core | Side-by-side play props | |
9 Materials for Cooperative Play | G-625 | 🔴 Advanced | Shared games, turn-taking tools | |
9 Materials for Social Reciprocity | G-630 | 🔴 Advanced | Joint attention materials |
✅ If you have the doctor kit from Card 09 → you can start G-622 Functional Play right now.
✅ If you have building blocks → G-624 Parallel Play is materials-ready.
✅ If you have building blocks → G-624 Parallel Play is materials-ready.
One Technique. One Domain. One Piece of a Larger Plan.
Your child's development spans 12 interconnected domains. G-623 Pretend Play is one active piece — but it feeds directly into Social Communication, Theory of Mind, Language, and ultimately Academic Narrative and Lifelong Creative Thinking.
Play (G) → Social Communication (B)
Social Communication → Theory of Mind → Friendship
Friendship → Language → Academic Narrative → Lifelong Creative Thinking
The Imagination Was Already There. It Just Needed a Door.
Arjun, Age 4 — Hyderabad
Before: A room full of action figures — lined up by size every morning. Never made them talk, fight, or fly. Parents tried for months. He'd glance and walk away.
Weeks 1–6: Realistic doctor kit introduced. Father sat on floor daily making the "sick doll" groan and ask for help — never directly asking Arjun to participate. By Week 4: Arjun brought the stethoscope to his father without prompting.
Week 8: "Doctor Arjun fixing the heart." Two more characters added. Independent doctor scenarios for 20 minutes.
"We stopped trying to make him play. We started playing beside him and waited. He came." — Arjun's father
Priya, Age 5 — Bengaluru
Before: Labeled "imaginationless" by relatives. Played only with the kitchen set — filling and emptying containers endlessly. Never once served imaginary food.
Weeks 1–8: Puppets introduced first (less threatening). Mother gave the puppet a voice saying it was "so hungry." Week 3: Priya brought a toy apple to the puppet unprompted.
Week 10: Creating a "market" scenario with kitchen, puppet, and cardboard box "shop." Full pretend narrative. Full voice characters.
"The imagination was there — she just needed someone to show her the door." — Priya's mother
"Pretend play deficits look permanent but rarely are. What we're usually treating is access — not capacity. The 9 materials in this protocol are different kinds of doors. Every child will respond to a different one. The job is to find their door." — Senior Play Therapist, Pinnacle Blooms Consortium
Note: Stories are composite illustrative cases. Individual outcomes vary by profile, conditions, and consistency.
You Are Not a Solo Operator. You Are Part of a Community.
📱 WhatsApp Parent Groups
Join: Parents Working on Pretend Play — Challenge-specific group. Parents sharing what works, what doesn't, and what happened today in play.
Join: Pinnacle Play Development Parents — Broader play skills community — all stages, all techniques.
Join: Pinnacle Play Development Parents — Broader play skills community — all stages, all techniques.
💬 Online Community
Pinnacle Parent Forum: Play Development
pinnacleblooms.org/community/play
pinnacleblooms.org/community/play
🤝 Peer Mentoring
Connect with a Parent Who's Been Here — parents who completed this protocol 6–12 months ago, available for peer support. pinnacleblooms.org/meetups
"Your experience is the most powerful resource for another parent who is where you were 6 weeks ago. Consider sharing."
WHO NCF: "Over 1,000 individuals from 111 countries contributed to the framework." Parent support networks improve intervention outcomes and adherence.
Home + Clinic = Maximum Impact
Home-based intervention works best when guided by professional expertise
🔶 Occupational Therapy
Sensory-motor play, play skill assessment, sensory profile-based material matching
🔷 Speech-Language Pathology
Narrative language, symbolic play, perspective language development within play
🟣 ABA / BCBA
Structured play intervention, reinforcement design, prompting hierarchies
🟢 Special Education
Generalization to school, curriculum integration, classroom social script development
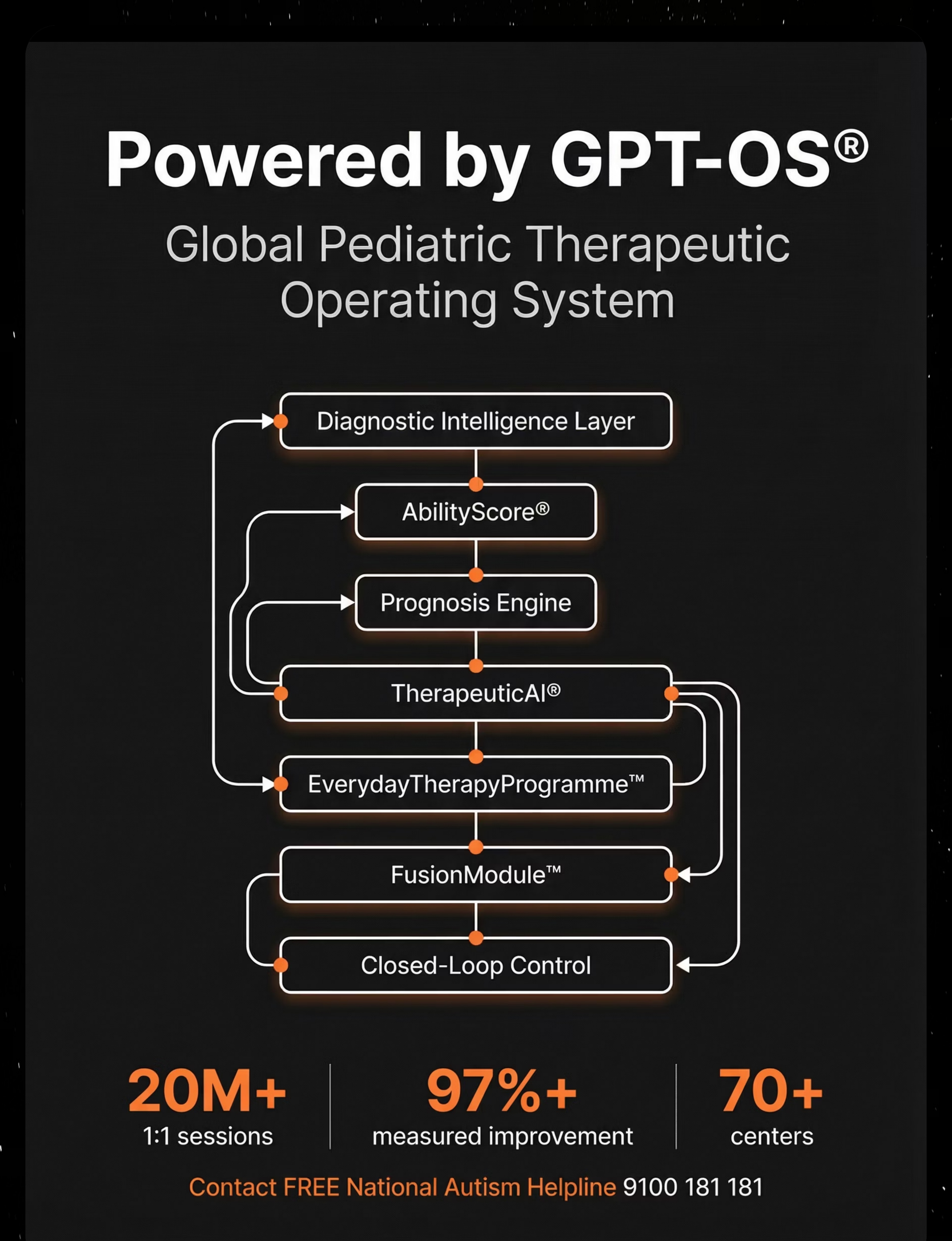
Across our network, pretend play facilitation is deployed as part of FusionModule™ — where SLP, OT, and ABA therapists co-plan play sessions, ensuring the material approach at home is synchronized with the clinical protocol in the therapy room.
Deeper Reading for the Evidence-Hungry Parent
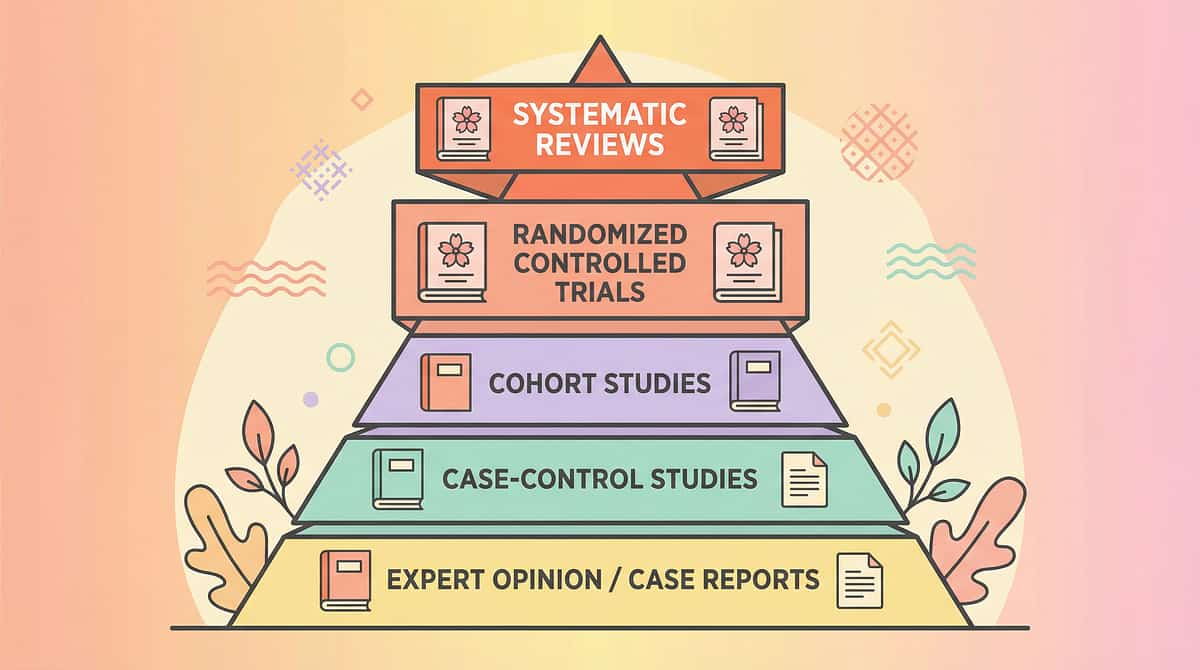
This is not anecdote. This is peer-reviewed science.
📋 1. PRISMA Systematic Review (Children, 2024) — Level: Highest
16 studies (2013–2023) confirm play-based material interventions for ASD meet evidence-based practice criteria. PMC11506176
📋 2. Meta-Analysis (World J Clinical Cases, 2024) — Level: Meta-Analysis
24 studies demonstrating effective promotion of social skills, adaptive behavior, and sensory processing through structured material play. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
📋 3. Frontiers in Integrative Neuroscience (2020) — Level: Review Article
Neurological basis for symbolic play and imagination in ASD — prefrontal and temporal-parietal mechanisms. DOI: 10.3389/fnint.2020.556660
📋 4. Padmanabha et al., Indian Journal of Pediatrics (2019) — Level: RCT
Indian RCT: Home-based developmental interventions demonstrate significant measurable outcomes in Indian pediatric populations. DOI: 10.1007/s12098-018-2747-4
📋 5. NCAEP Evidence-Based Practices Report (2020) — National Standards
Video modeling, visual supports, and structured play classified as evidence-based practices for autism. National Clearinghouse on Autism Evidence and Practice.
📋 6. WHO Care for Child Development Package (2023) — WHO Global Standard
Age-specific evidence-based caregiver recommendations implemented in 54 LMICs. PMC9978394 | nurturing-care.org
Your Session Data Is Not Stored. It Grows.
📊 Which Materials Work
Which of the 9 materials produces highest engagement for THIS specific child
📈 Rate of Emergence
Rate of symbolic play emergence vs. population baseline across 20M+ sessions
⏱️ Optimal Frequency
Optimal session frequency for this child's individual response profile
🎯 When to Advance
Data-driven signal for when to advance, maintain, or intensify the protocol
🔒 All data is anonymized at population level. Your child's individual data is never shared without explicit consent. Compliant with India's Digital Personal Data Protection Act (DPDPA 2023).
20M+
1:1 Sessions
97%+
Measured Improvement
70+
Centers
160+
Countries (Patents Filed)

Watch G-623: 9 Materials That Help With Pretend Play
▶️ Reel G-623 Overview
🎭Cover: "When toys stay toys and imagination doesn't arrive"
🔬Materials shown: All 9, each in 4–5 seconds with voiceover
🏥Powered by: GPT-OS® Therapy Intelligence
⏱️Duration: ~75–85 seconds
📱Also on: Instagram | YouTube | Pinterest | Pinnacle App
🔬Materials shown: All 9, each in 4–5 seconds with voiceover
🏥Powered by: GPT-OS® Therapy Intelligence
⏱️Duration: ~75–85 seconds
📱Also on: Instagram | YouTube | Pinterest | Pinnacle App
Production Credits:
Content: Pinnacle Blooms Consortium (OT, SLP, ABA, SpEd, NeuroDev)
Evidence: GPT-OS® Clinical Protocols | 20M+ Session Database
Narration: Pinnacle Clinical Educator Team
Content: Pinnacle Blooms Consortium (OT, SLP, ABA, SpEd, NeuroDev)
Evidence: GPT-OS® Clinical Protocols | 20M+ Session Database
Narration: Pinnacle Clinical Educator Team
Related Reels in This Series:
- G-621: 9 Materials for Sensory Play
- G-622: 9 Materials for Functional Play
- G-624: 9 Materials for Parallel Play
NCAEP (2020): Video modeling is classified as an evidence-based practice for autism. Multi-modal learning improves parent skill acquisition.

Consistency Across All Caregivers Multiplies Impact
If only one person implements this, results are partial. When everyone knows — results compound.
Explain to Grandparents — Simplified Version:
"Our child doesn't pretend play yet. This is a developmental difference — not stubbornness. We're teaching it one step at a time. When you play with them:"
✅ DO: Sit on the floor and play with a doll or toy yourself. Narrate. Wait.
✅ DO: If they show interest, respond warmly: "Yes! The baby is hungry!"
❌ DON'T: Say "Come on, pretend!" or force them to play
❌ DON'T: Compare to other children
The technique is: play beside them, model imagination, and wait.
✅ DO: Sit on the floor and play with a doll or toy yourself. Narrate. Wait.
✅ DO: If they show interest, respond warmly: "Yes! The baby is hungry!"
❌ DON'T: Say "Come on, pretend!" or force them to play
❌ DON'T: Compare to other children
The technique is: play beside them, model imagination, and wait.
Share This Page
📲 Share on WhatsApp | 📧 Share via Email | 🔗 Copy Link
📄 Download Family Guide
"Pretend Play in 5 Minutes" — One A4 page for spouses, grandparents, teachers, and daycare providers. No jargon. Just the essentials.
📝 Download School Letter Template
Formal letter requesting play support accommodation, referencing G-623 protocol and Pinnacle consortium guidance.
📞 Helpline for Family Members
9100 181 181 — Family members can call directly. 16+ languages. Free. 24×7.
Questions Parents Ask Most About Pretend Play
Q1: My child is 6. Is it too late to develop pretend play?
No. While earlier is better, pretend play skills can emerge and develop well beyond age 6 with targeted intervention. The approach may differ from a 2-year-old (more explicit scripted scenarios, visual supports, special interest entry points), but the capacity is present. Many children who begin at age 5–7 make remarkable progress. The brain retains plasticity for these skills throughout childhood.
Q2: My child scripts from TV/movies — is that pretend play?
Yes — scripted scenarios from media ARE a form of symbolic play. The child is using mental representations in a new context. Work WITH the scripts rather than replacing them. Expand: "And then what did [character] do?" Build from their starting place.
Q3: Do I need all 9 materials?
No. Start with 2–3 that match your child's interests and your budget. The best starter kit is: one realistic play set + one doll/figure + your time as play partner. Add materials as the child progresses. See the Zero-Cost version on Card 10.
Q4: My child pretends at therapy but not at home. Why?
Context dependency is extremely common. Skills emerge first in safe, familiar environments before generalizing to home. Ask your therapist: (a) exactly which materials they use and how, (b) whether you can observe a session, (c) for a home carryover plan. One consistent material bridge (bring ONE therapy item home) often unlocks home generalization.
Q5: How do I know if my child needs formal evaluation vs. just more time?
Key indicators: no pretend play whatsoever by age 3; play not progressing despite 12+ weeks of consistent home support; absence accompanied by other developmental concerns (limited language, social differences, repetitive behaviors). Call 9100 181 181 for a free consultation — we'll help you decide.
Q6: Is this technique suitable for non-verbal children?
Yes. The approach shifts to more modeling, less language. Use AAC (if applicable) as part of the play. Cause-effect toys and physical/embodied approaches (dress-up, building) are especially effective. See sensory-avoider/seeker adaptations in Card 22.
Q7: My child showed great progress, then suddenly regressed. Normal?
Completely normal. Regression during illness, environmental change, or increased stress is expected. Continue the protocol at lower intensity during regression. Document it. Most regressions resolve within 1–2 weeks. If prolonged (3+ weeks) or accompanied by new behaviors, consult your therapist.
Q8: What's the difference between this and regular toy play?
Structure, intention, and adult facilitation. This protocol uses specific materials chosen for their therapeutic mechanism, adult modeling and narration, data tracking, and a progression pathway. It's purposeful, measurable, and evidence-grounded. Think of it as the difference between swimming freely and swimming lessons.

The Imagination Is Waiting.
Your Move.
Your Move.
You have the science. You have the materials. You have the protocol. The only missing ingredient is the first session.
⬡ Validated By
Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics
CRO • WHO-Aligned • UNICEF-Referenced
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics
CRO • WHO-Aligned • UNICEF-Referenced
📊 The Numbers
20M+ Sessions | 97%+ Improvement
70+ Centers | 70 Countries
Free Helpline: 9100 181 181
70+ Centers | 70 Countries
Free Helpline: 9100 181 181
Preview of 9 materials that help with pretend play Therapy Material
Below is a visual preview of 9 materials that help with pretend play therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!
🔷 Pinnacle Blooms Network®
Pediatric Therapeutic Consortium of India
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO • Research • Regulatory • Families
"From fear to mastery. One technique at a time."
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
160+
Countries (Patents Filed)
📞 Free National Helpline
9100 181 181 | 24×7 | 16+ Languages | Zero Cost
🔍 Browse All Techniques
techniques.pinnacleblooms.org
70,000+ evidence-based technique pages
70,000+ evidence-based technique pages
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention from licensed developmental specialists, speech-language pathologists, occupational therapists, or play therapists. Persistent absence of pretend play may indicate autism spectrum conditions or other developmental differences requiring comprehensive evaluation. Play development varies by child — progress should be celebrated at each child's individual pace. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®.
CIN: U74999TG2016PTC113063 | DIPP8651 (Govt. of India) | Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Technique code G-623. Content generated under GPT-OS® Content Engine. Published at: techniques.pinnacleblooms.org/play-development/9-materials-pretend-play-G-623
© 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Technique code G-623. Content generated under GPT-OS® Content Engine. Published at: techniques.pinnacleblooms.org/play-development/9-materials-pretend-play-G-623