
Writing Starts Long Before the Pencil
She's four years old. She reaches for the crayon and wraps her whole fist around it. When she tries to draw a circle, it comes out as a jagged loop that doesn't close. She presses so hard the crayon snaps — or so lightly the mark disappears. The tracing workbooks sit untouched because they trigger tears. Kindergarten is eight months away, and you've just been told she "needs to work on pre-writing skills."
You are not failing. Your child's hands are asking for a foundation that hasn't been built yet — and building it is entirely possible.
F-606 | Fine Motor & Handwriting Readiness
Age Band: 2–6 Years
Pinnacle Blooms Network®

ACT I — UNDERSTANDING
You Are Among Millions of Families Navigating This Exact Challenge
Pre-writing skill difficulties are among the most common concerns that bring families to occupational therapists globally. In India, where academic writing demands begin as early as age 3 in competitive preschool environments, the urgency families feel is real, documented, and shared by millions. What you're experiencing at home is happening in millions of homes across 70+ countries where Pinnacle families live.
1 in 5
Children Affected
Show pre-writing skill delays requiring intervention before age 6
43%
OT Referrals
Children referred to OT for handwriting show foundational pre-writing deficits — not letter-practice deficits
85%
Addressable at Home
Of fine motor delays are addressable through consistent home-based intervention with the right materials
📊India-Specific Context: With Class 1 entry requiring letter writing by age 5–6, and competitive preschool assessments evaluating drawing and tracing skills, Indian families face earlier pre-writing pressure than global averages. GPT-OS® data from 20M+ sessions shows fine motor and pre-writing interventions are among the top 3 most requested disciplines at Pinnacle centers.

ACT I — UNDERSTANDING
The Architecture of a Handwriting-Ready Hand
The Muscle Reality
Your child's hand contains 19 intrinsic muscles — small muscles housed entirely within the hand that control the fine, precise movements of each finger independently. These muscles are genuinely underdeveloped at birth and build strength through resistive, repetitive use across the first five years of life. A child who cannot maintain consistent pencil pressure is not being lazy — their intrinsic muscles are literally not yet strong enough for the task being demanded.
The Grasp Progression
- Age 1–2: Palmar/fist grasp (whole hand)
- Age 2–3: Digital pronate grasp (fingers on top, arm-driven)
- Age 3.5–4: Static tripod (3-finger hold, wrist movement)
- Age 4.5–6: Dynamic tripod (3-finger, finger-driven ← THE TARGET)
The Visual-Motor Connection
Pre-writing requires the eyes and hands to operate as a synchronized system — the visual cortex must perceive where the line should go, transmit that to the motor cortex, which executes the movement with precision. This visual-motor integration is its own developmental pathway, separate from both vision and hand strength, requiring specific activities to develop.
ACT I — UNDERSTANDING
Where Pre-Writing Sits in Development
Pre-writing skills are not a single ability — they are a cascade. Each stroke type depends on the physical and neural foundations built by the previous one. A child who cannot yet draw a consistent vertical line is not ready to copy a square, regardless of chronological age. The sequence is developmental, not academic.
1
Age 1–2
Scribble with fist
2
Age 2–2.5
Vertical line imitation
3
Age 3
Horizontal line + Circle imitation
4
Age 4
Cross (+) and Square imitation
5
Age 5–6
Triangle and Diamond imitation
Commonly Co-Occurring: Fine motor and pre-writing delays frequently appear alongside low muscle tone (hypotonia), developmental coordination disorder (DCD/dyspraxia), autism spectrum differences, attention challenges (ADHD), and sensory processing differences. A delay in pre-writing is never "just" a handwriting problem — it's a window into the whole child's neurodevelopment.

ACT I — UNDERSTANDING
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I–II | Systematic Review + RCT Support. These are not creative suggestions. They are the clinical tools that occupational therapists deploy daily across Pinnacle's 70+ centers, now documented and structured for home execution.
PRISMA Systematic Review (2024)
PMC11506176 — 16 studies (2013–2023) confirm sensory-motor and fine motor interventions meet evidence-based practice criteria. Home-based implementation shows outcomes equivalent to clinic-based when properly structured.
Meta-Analysis (2024)
PMC10955541 — Across 24 studies, sensory integration and fine motor approaches effectively promote motor skills, adaptive behavior, and academic readiness. Effect size: moderate-to-strong across fine motor outcomes.
Indian RCT (2019)
DOI:10.1007/s12098-018-2747-4 — Padmanabha et al.: Home-based sensory-motor interventions by trained parents demonstrated statistically significant motor outcomes in Indian children.
WHO/UNICEF CCD Package (2023)
PMC9978394 — Implemented across 54 low- and middle-income countries: caregiver-delivered, material-supported motor activities produce measurable developmental gains, even without clinical-grade equipment.

ACT II — KNOWLEDGE TRANSFER
The Technique: What It Is
Formal Name: Pre-Writing Skill Development Through Material-Based Intervention
Parent-Friendly Alias: Building Writing-Ready Hands Before the Pencil
Parent-Friendly Alias: Building Writing-Ready Hands Before the Pencil
Pre-writing skills are the foundational physical, neurological, and visual-motor abilities that must exist before a child can successfully learn to form letters and numbers. This intervention uses 9 specific therapeutic materials to systematically build: (1) intrinsic hand strength, (2) grasp development from fist → tripod, (3) bilateral coordination, (4) wrist positioning, (5) visual-motor integration, and (6) stroke formation in developmental sequence. The goal is not to teach writing — it is to build the hands and neural systems that make writing learnable.
📂 Domain
Fine Motor Development / Pre-Writing / Handwriting Readiness
📋 Code & Age
F-606 | Age: 2–6 years | 15–20 min daily | 6–8 week programme
🏷 Canon Materials
Playdough & Putty | Tools & Manipulatives | Writing Surfaces | Sensory Materials | Template Materials

ACT II — KNOWLEDGE TRANSFER
Who Uses This Technique
"This technique crosses therapy boundaries because the brain does not organize by therapy type. A child's hand needs strength (OT), structure (ABA), sequence (SpEd), and context (NeuroDev) — simultaneously."
Occupational Therapy 🏆 PRIMARY LEAD
OTs assess hand strength, grasp maturity, wrist positioning, visual-motor integration, and stroke formation. They design the entire progression from foundational hand strengthening through material selection, grading resistance and complexity. All 9 materials in this series come from OT clinical practice.
Special Education
SpEd teachers apply pre-writing interventions in classroom settings. They track stroke formation sequence, identify students needing OT referral, and adapt writing curricula to developmental readiness rather than chronological age. Often the first professionals to flag delays.
ABA / BCBA
Behavior analysts structure pre-writing as a behavioral chain, applying task analysis, discrete trial training, and reinforcement schedules to each material interaction. They track baseline grasp maturity and set specific mastery criteria (e.g., tripod hold for 80% of trials across 3 sessions).
Pediatric Neurodevelopment
Neurodevelopmental pediatricians assess underlying conditions (hypotonia, DCD, ASD, ADHD) driving pre-writing delays. They determine whether motor delays are isolated or part of a broader neurodevelopmental profile and set the clinical context for intervention intensity.
ACT II — KNOWLEDGE TRANSFER
What This Technique Targets
Research (PMC10955541) documents motor skills, adaptive behavior, and academic readiness as concurrent outcomes of this intervention. The center target — functional pencil readiness — is observable: child holds a short writing tool with a 3-finger tripod grasp and produces intentional, controlled strokes matching at least 3 developmental shapes appropriate for age.

ACT II — KNOWLEDGE TRANSFER
9 Materials. 9 Foundations. Start With What You Have.
Every one of these materials has a ₹0 version. The therapeutic value lies in how you use them — not in what they cost. Begin with what you already own.

ACT II — KNOWLEDGE TRANSFER
Materials 7–9: The Final Three Foundations
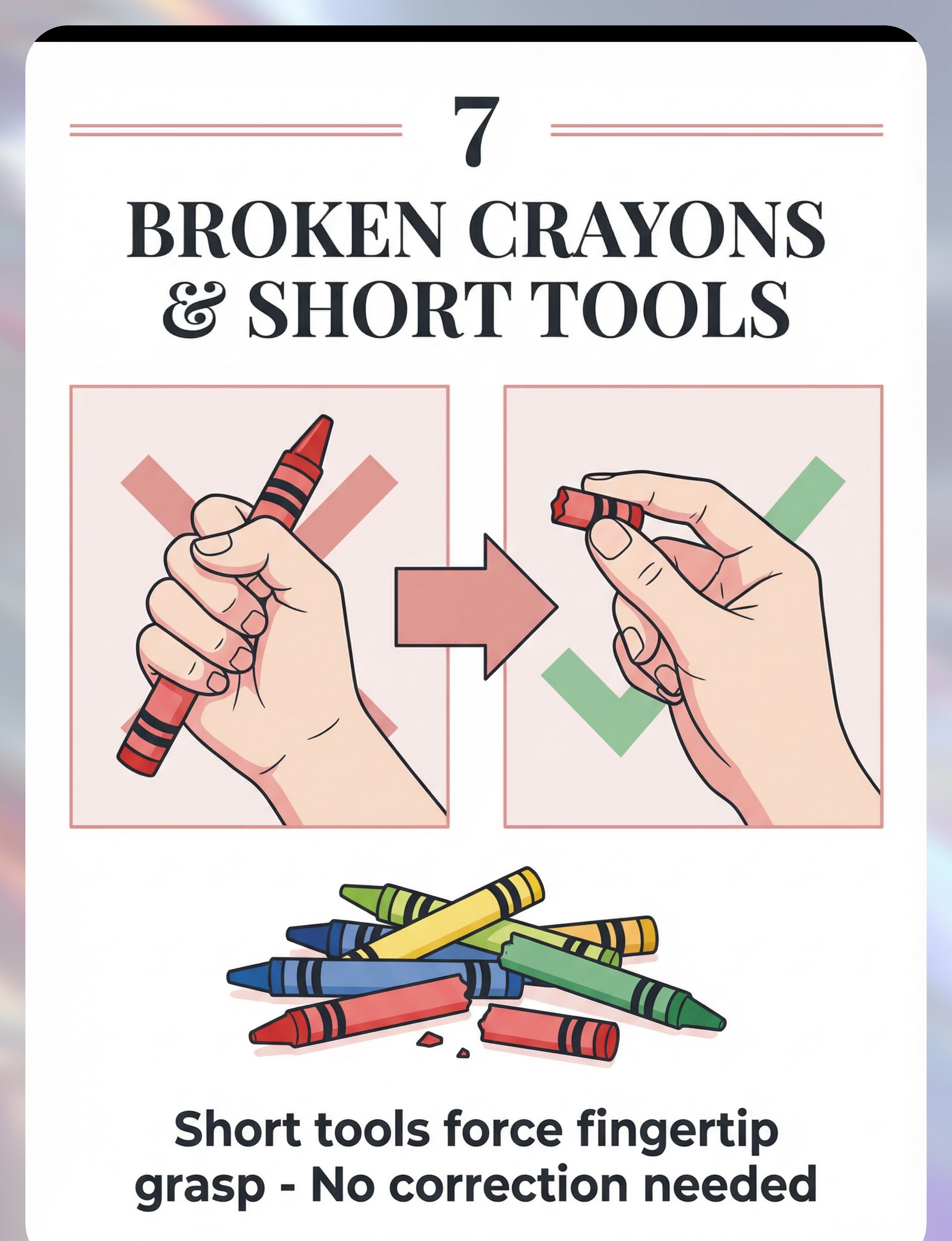
M7 — Broken Crayons / Short Writing Tools
🎯Builds: Tripod grasp (forced by tool length)
💰 DIY: ₹0 — break your existing crayons into 1–2 inch pieces
🔑 Replace ALL full crayons with broken pieces. The short length physically prevents fist grip — fingertip grasp is the only option.
💰 DIY: ₹0 — break your existing crayons into 1–2 inch pieces
🔑 Replace ALL full crayons with broken pieces. The short length physically prevents fist grip — fingertip grasp is the only option.
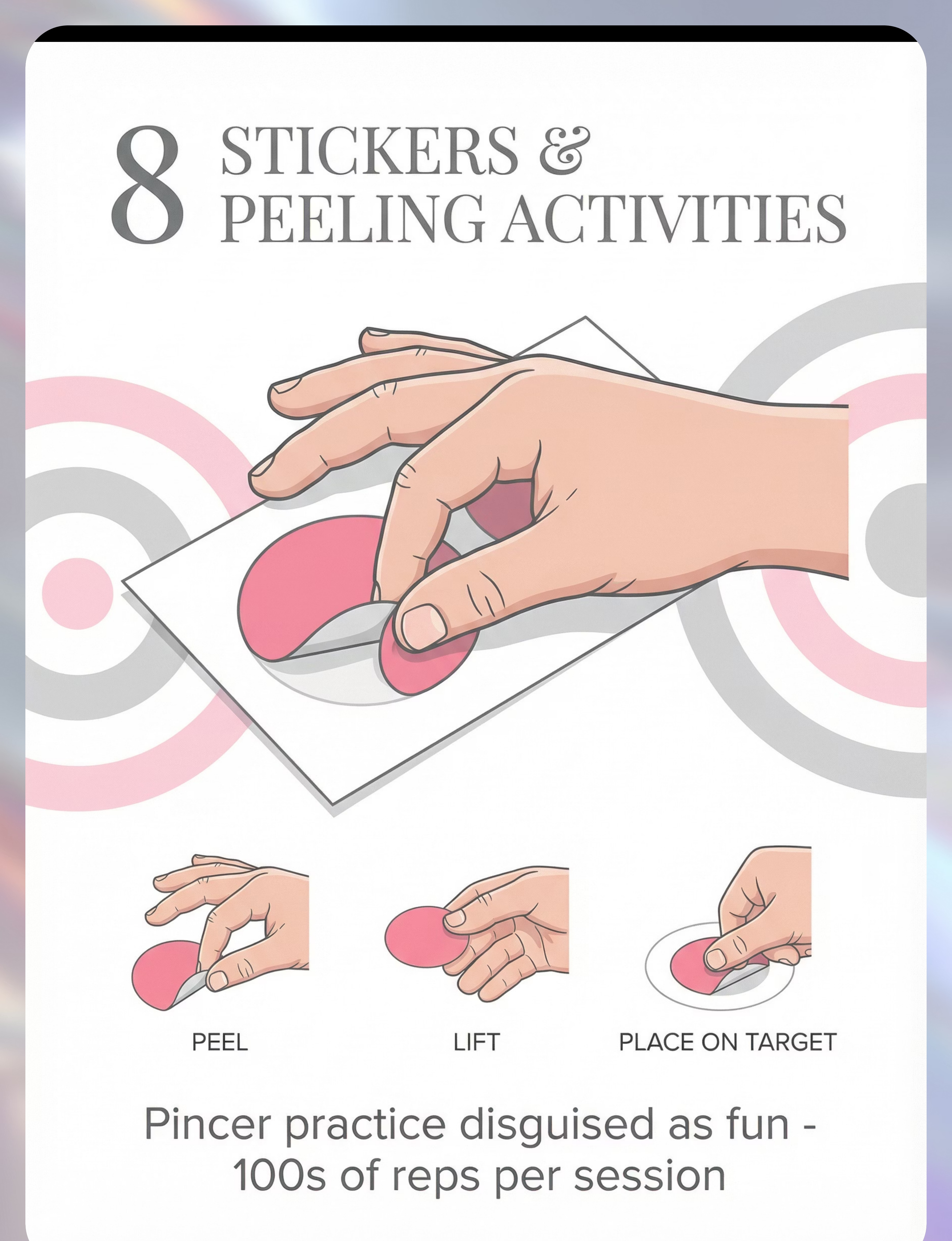
M8 — Stickers & Peeling Activities
🎯Builds: Pincer grasp, in-hand manipulation, bilateral coordination
💰 DIY: ₹0 (price labels, tape strips) | Sticker sheets: ₹50–200
🔑 Peel and place with precision. Pinnacle Recommends: 1800+ Reward Stickers →
💰 DIY: ₹0 (price labels, tape strips) | Sticker sheets: ₹50–200
🔑 Peel and place with precision. Pinnacle Recommends: 1800+ Reward Stickers →
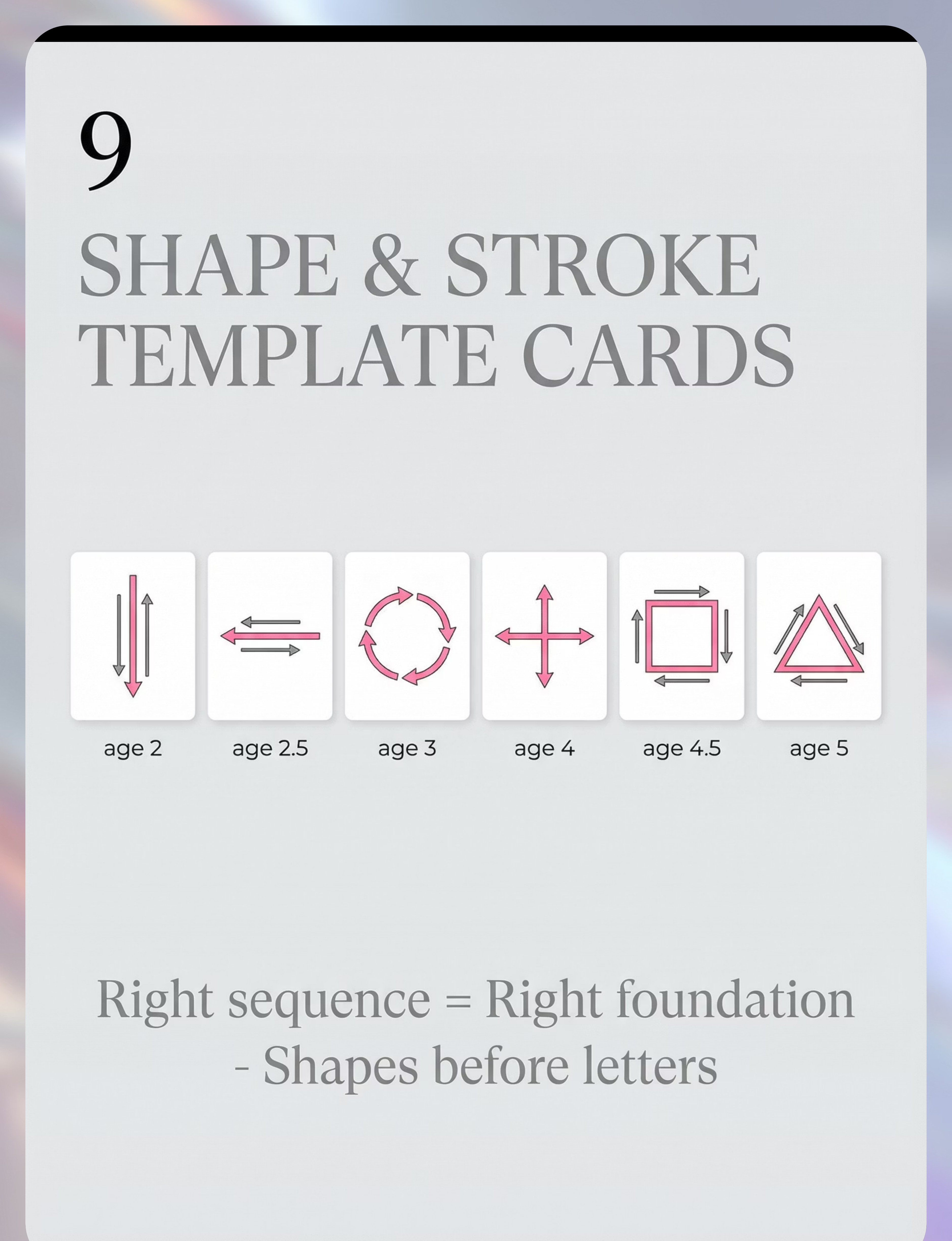
M9 — Shape & Stroke Template Cards
🎯Builds: Stroke sequence knowledge, visual model, copy skills
💰 DIY: ₹0 (draw shapes on cardstock + laminate) | Commercial: ₹150–400
🔑 Follow sequence: line → circle → cross → square → triangle. Never skip ahead.
💰 DIY: ₹0 (draw shapes on cardstock + laminate) | Commercial: ₹150–400
🔑 Follow sequence: line → circle → cross → square → triangle. Never skip ahead.
🏁Zero-Budget Starter Kit Today: (1) Break 2 crayons into 1-inch pieces. (2) Tape paper to the wall at eye height. (3) Find kitchen tongs + cotton balls. (4) Make playdough: 2 cups flour + 1 cup salt + 1 cup water + 1 tbsp oil. Cost: ₹0. Impact: Begins building the foundation today. Questions? Call FREE Helpline 9100 181 181 — 24×7, 16+ languages.
ACT II — KNOWLEDGE TRANSFER
Every Material Has a ₹0 Version. Zero Economic Barrier.
WHO/UNICEF Nurturing Care Framework (2018) establishes equity as a core principle: every child, regardless of family income, deserves access to evidence-based developmental intervention. These substitutes are not compromises — they apply the same sensory and motor principles using materials already in your home.
Material | Clinical Version | Household Substitute & Why It Works | |
Therapy Putty | Commercial graded putty ₹200–800 | Homemade playdough: 2c flour + 1c salt + 1c water + 1tbsp oil. Make stiffer for more resistance. Same resistive input to intrinsic muscles. | |
Tongs/Tweezers | Therapy tweezers ₹100–400 | Kitchen tongs, salad tongs, clothespins, chopsticks. Same tripod finger isolation — three fingers squeezed on tool. | |
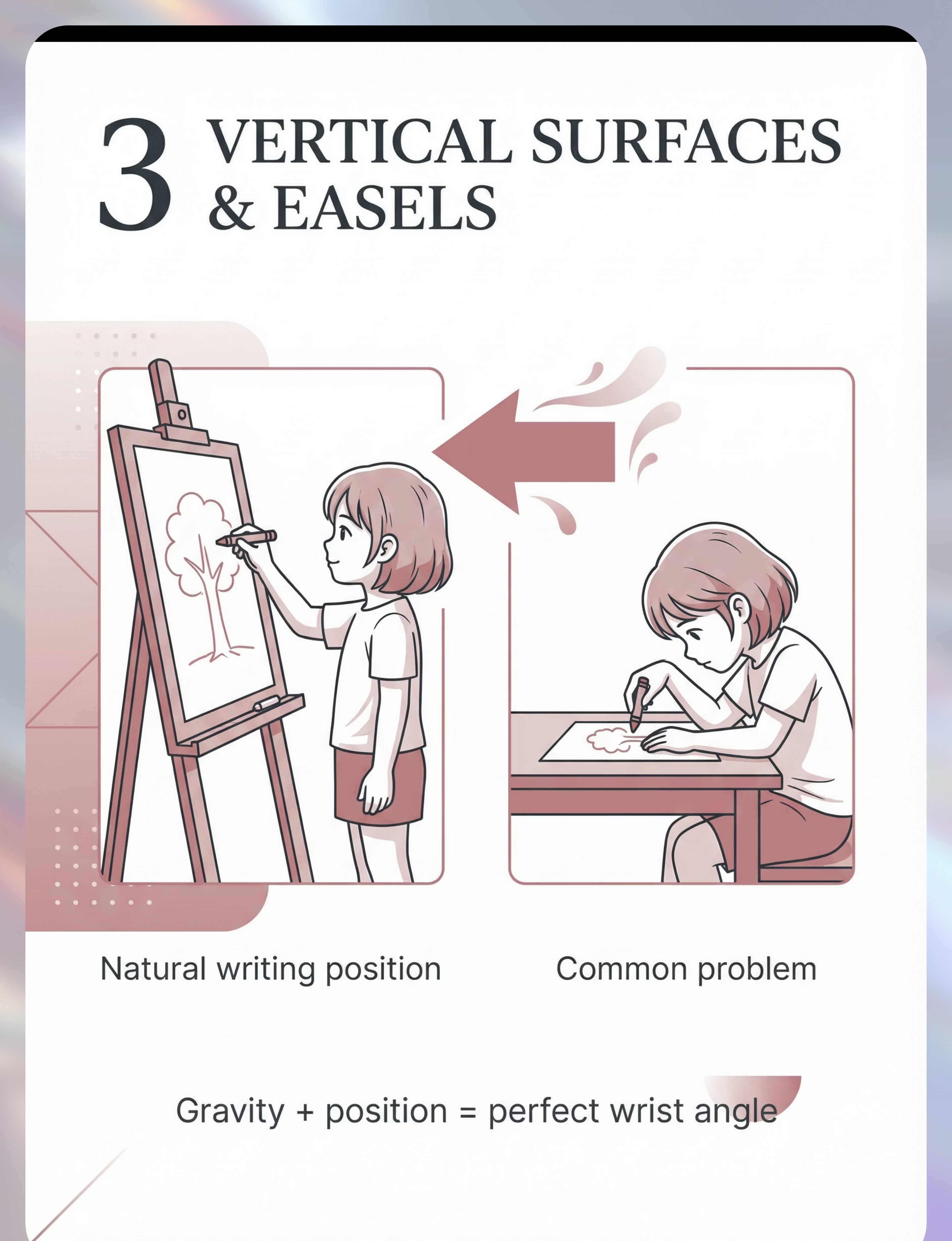
Vertical Surface | Children's easel ₹500–2,000 | Paper + masking tape + wall. Shower wall (bath crayons). Gravity creates the same wrist extension pattern automatically. | |
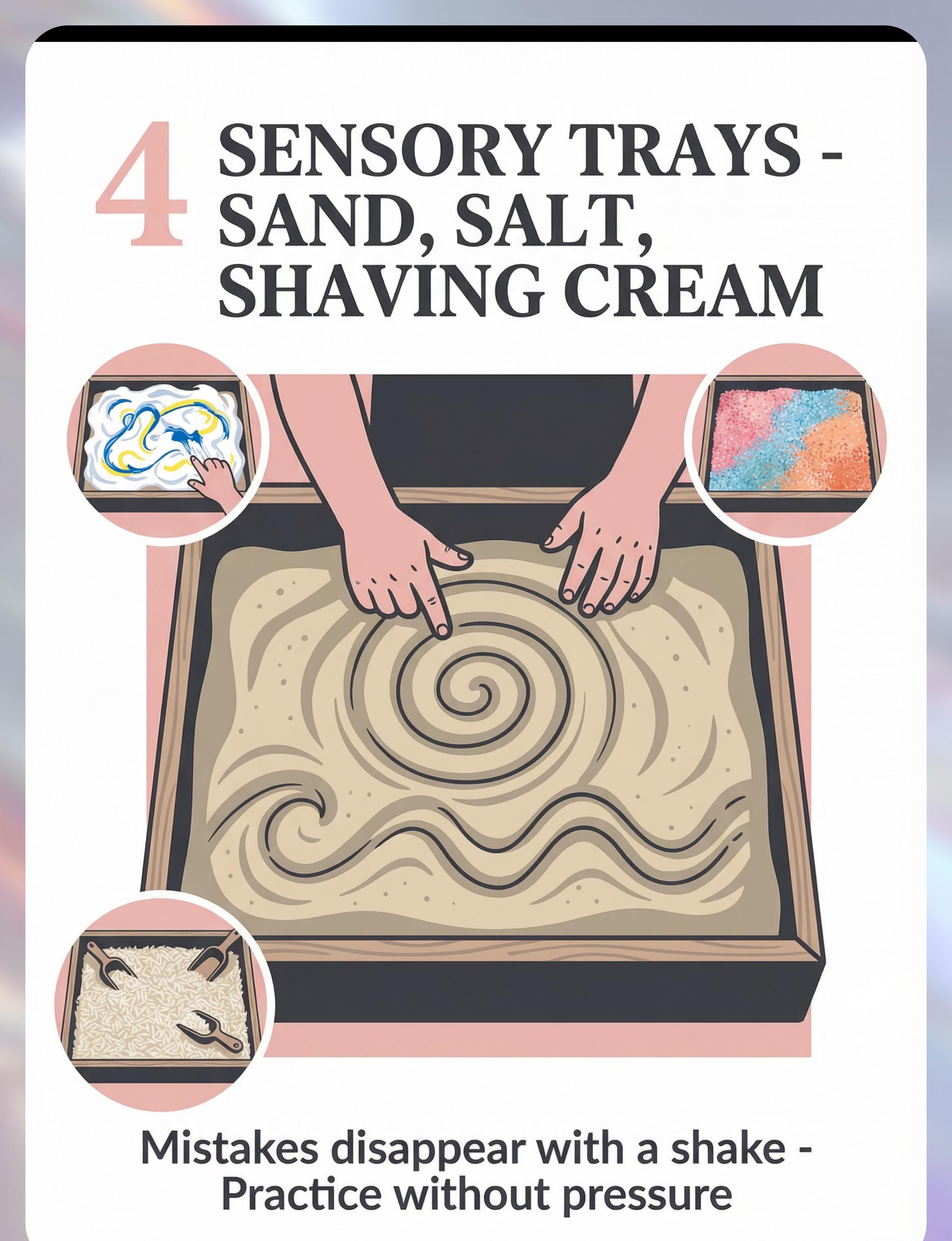
Sensory Tray | Kinetic sand + tray ₹300–600 | Kitchen baking tray + table salt. Add food coloring for visual contrast. Rice works too. Same proprioceptive feedback from finger drag. | |
Lacing Cards | Commercial lacing set ₹200–500 | Cardboard + hole punch + shoelace or thick yarn with taped end. Identical bilateral coordination demand. | |
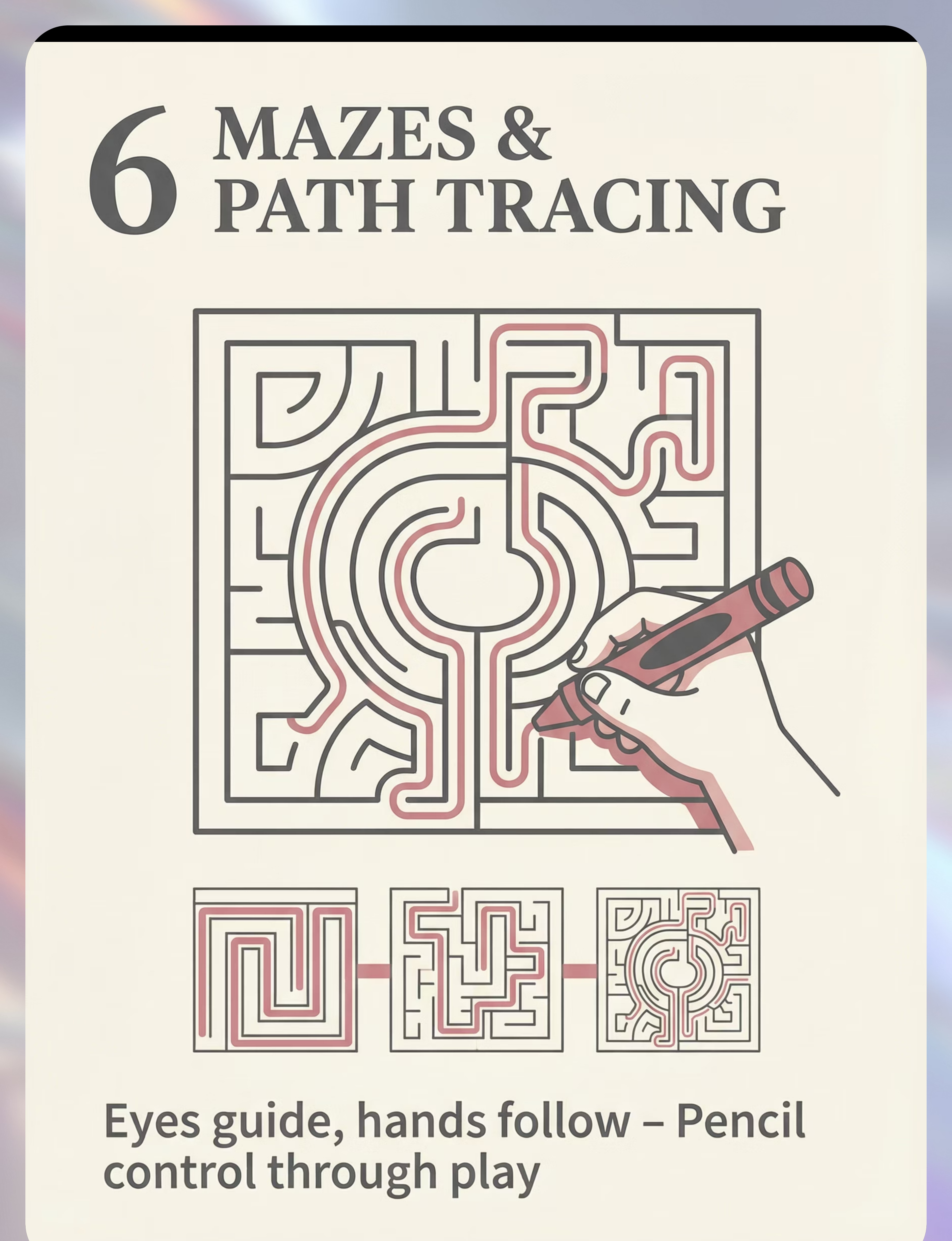
Mazes | Maze workbooks ₹100–300 | Draw paths on A4 paper (wide lanes first, narrow over time). Print free PDFs online. Identical visual-motor control demand. | |
Broken Crayons | Golf pencils ₹50–100 | Break existing crayons into 1–2 inch pieces. Short length physically prevents fist grip — fingertip grasp is the only option. | |
Stickers | Sticker sheets ₹50–200 | Price sticker labels, masking tape strips, old magazine address labels, Post-it notes. Same pincer grasp peel-and-place action. | |
Shape Templates | Commercial cards ₹150–400 | Draw shapes on cardstock with arrows showing stroke direction. Laminate with contact paper for dry-erase reuse. Same visual model function. |
"A broken crayon in the hands of a parent who understands why it matters is more powerful than an expensive grip aid used without therapeutic intent." — Pinnacle OT Consortium

ACT II — KNOWLEDGE TRANSFER
Safety First: Before You Begin
🔴 DO NOT PROCEED IF:
- Child is in active meltdown, tantrum, or severe dysregulation
- Child has open skin wounds on hands (salt/putty will irritate)
- Child has known wheat/gluten allergy (homemade playdough contains flour — use gluten-free version)
- Session is more than 30 minutes from last meal
- You are stressed or unable to remain patient — the child will sense it
- Therapy putty or playdough shows signs of mold (discard and remake)
🟡 PROCEED WITH MODIFICATION IF:
- Child has sensory hypersensitivity to textures — introduce at child's edge, never force
- Child has significantly low muscle tone — use softest putty, shorter sessions (5 min)
- Child has attention challenges — use 5-minute rotation across materials
- Child had a poor sleep night — reduce demands, use child's preferred material only
🟢 PROCEED WHEN:
- Child is alert, regulated, recently fed, within a familiar routine
- You have 15–20 uninterrupted minutes
- Materials are prepared and accessible before the child sits down
- You are in a calm, patient state
⚠️CHOKING HAZARD: Small objects used with tweezers (beads, small pom poms), broken crayon pieces, and small stickers are choking hazards. Always supervise children under 4 years. STOP IMMEDIATELY IF child shows distress, gagging, allergic reaction, attempts to ingest non-food materials, or hands show redness, swelling, or pain.

ACT II — KNOWLEDGE TRANSFER
The Right Environment Prevents 80% of Session Problems
Table Setup Checklist
- Table height: Child's elbows at surface when seated — feet flat on floor or footrest
- Chair: Firm, stable, feet supported — no swivel chairs, no floor seating
- Lighting: Bright, natural preferred. No shadows on work surface.
- Wall above table: Paper taped at child's eye-level for vertical work
- Materials: Pre-arranged before child sits — not retrieved during session
- Reinforcers: Preferred item visible but withheld (creates motivation)
- Distractors removed: Screens off, toys not visible
- Data tracker: Simple tally sheet + pen at parent's side
Parent Positioning
Sit at the child's non-dominant side (if right-handed child, sit to their left). This allows visual modeling while allowing the child's dominant hand full range of motion. Never sit directly opposite — it creates a confrontational dynamic.
Session Rhythm
- 0:00–2:00 — Invitation and warm-up
- 2:00–5:00 — Material 1 engagement
- 5:00–8:00 — Material 2 engagement
- 8:00–13:00 — Core therapeutic activity
- 13:00–17:00 — Repeat, vary, reinforce
- 17:00–19:00 — Cool-down + data capture

ACT III — EXECUTION
Is Your Child Ready? Pre-Session Readiness Check
The best session is one that starts right. A perfect 8-minute session beats a forced 25-minute struggle every time. Complete this 60-second check before every session.
Indicator | ✅ GO | 🔄 MODIFY | ⏸ POSTPONE | |
Feeding | Fed within last 2 hrs | Slightly hungry — offer snack first | Very hungry or just ate — wait 30 min | |
Sleep | Normal night's sleep | Slightly tired — shorten to 10 min | Overtired or unwell — skip today | |
Emotional state | Calm, engaged, approachable | Slightly fussy — preferred material only | Active meltdown or severe distress | |
Body awareness | Sitting steadily, alert eyes | Low arousal — 2 min movement first | Seeking intense movement only | |
Prior session | 6+ hrs since last session | 3–6 hrs — same materials, lower demand | Less than 3 hrs — too close, skip |
✅ All/Most GREEN
GO: Proceed to Step 1 — The Invitation
🔄 Mix Green/Amber
MODIFY: Use highest-preferred material, reduce session to 8 minutes
⏸ Any RED
POSTPONE: Do a regulation activity instead. "Not ready" is valid data.

ACT III — STEP 1
Step 1: The Invitation
Timing: 1–2 minutes. Every pre-writing session begins with an invitation, not a demand. The child chooses to engage — your job is to make engagement irresistible through presentation, not pressure.
"I have something really cool to show you. Come see what I found." [Place the playdough / tongs + pom poms in child's sight line — do NOT announce it as therapy] "I'm going to make a little worm. Want to try?" [Begin working with the material yourself — modeling without demand]
Body Language Guidance
- Sit at child's level or slightly below
- Open, relaxed posture — no forward lean or anxious expression
- Make the material look genuinely interesting to you
- If child approaches: DO NOT immediately prompt — let them observe for 10–15 seconds
Acceptance Cues vs. Resistance Signs
Acceptance: Eye contact with material, moves closer, imitates your action unprompted, vocalizes toward material.
Resistance: If child turns away — work quietly yourself; many return within 2 minutes. If child pushes material away — accept gracefully: "That's okay." Try a different material. If child says "no" — honor it. Try again in 10 minutes.

ACT III — STEP 2
Step 2: The Engagement
Timing: 2–4 minutes. The child is now present. This step deepens engagement by introducing the therapeutic element of the material without naming it as therapy. The child should be experiencing play — you are experiencing therapy delivery.
Playdough
"Let's see who can make the longest snake." → Introduces bilateral rolling and intrinsic strength building.
Tongs / Tweezers
"Can you move all the yellow ones to this bowl before I move all the blue ones?" → Competition framing creates motivation; tripod grasp is the hidden therapeutic target.
Vertical Surface
"Can you make it rain on my house? Draw raindrops." → Vertical surface; wrist extension achieved automatically.
Sensory Tray
"Drive your finger-car along this road without going off the sides." → Stroke path, directional pressure, tactile feedback.
Lacing Cards
"I need your help sewing this back together. Can you put the lace through each hole?" → Bilateral coordination framed as helping.
Mazes
"Help the mouse get to the cheese — but the pencil can't touch the walls." → Visual-motor control through play motivation.
Reinforcement timing: Deliver praise at the first instance of the target behavior (tripod contact, maintained grasp, stroke completion): "I love how you're using these three fingers — exactly right." Be specific, not generic.
ACT III — STEP 3
Step 3: The Therapeutic Action
Timing: 8–12 minutes — this is the core of the session. Research (PMC10955541) shows core therapeutic action occupies 40–60% of effective session time.
Phase A — Hand Preparation (3–4 min)
Use Playdough or Therapy Putty first in every session. The resistive input activates intrinsic hand muscles and proprioceptive awareness needed for all subsequent fine motor activities. Roll 10 snakes between palms → make 10 small balls with fingertips only → pinch off pieces to hide 3 objects → pull putty apart and push together.
Phase B — Grasp Development (2–3 min)
Immediately following hand preparation, introduce tongs/tweezers or broken crayons while intrinsic muscles are activated and warm. Transfer 10 objects with tongs focusing on 3-finger hold — OR draw freely with broken crayons on vertical surface.
Phase C — Stroke Practice (4–5 min)
Using the sensory tray or maze/path tracing, practice the next stroke in the developmental sequence. Always: vertical → horizontal → circle → cross → square → triangle. NEVER skip ahead. Master each stroke before introducing the next. Model first with your own finger. Name the stroke: "Down, all the way down."

ACT III — STEP 4
Step 4: Repeat & Vary
Timing: 3–5 minutes.Dosage Principle: 3 quality repetitions performed with engagement and correct form are worth more than 10 forced repetitions with resistance and compensation. This is the Pinnacle doctrine for pre-writing skill building.
Repetition Targets Per Session
- Playdough squeezing: 10–15 reps
- Tong transfers: 15–20 objects
- Vertical surface strokes: 5–8 attempts at target shape
- Sensory tray strokes: 8–12 traces
- Lacing: 1 complete card OR 6–8 holes
- Mazes: 2–3 complete paths
- Sticker peel-place: 10–15 stickers
Variation Without Leaving the Target
- Change color of playdough (not resistance)
- Change objects being transferred (not the tongs)
- Change medium in sensory tray (sand → salt → shaving cream)
- Change maze difficulty up OR down based on success rate
- Change sticker size (larger = easier, smaller = harder)
Satiation Indicators — Move On When:
- Child uses material non-functionally (throwing, smearing)
- Decreasing quality of execution over last 3 repetitions
- Vocal protest or physical withdrawal from material
- Loss of eye contact with task

ACT III — STEP 5
Step 5: Reinforce & Celebrate
The ABA Reinforcement Rule: Timing matters more than magnitude. Reinforcement delivered within 3 seconds of the target behavior is 4× more effective than reinforcement delivered after a delay.
✅ What TO Say — Be Specific
- "I love how you held the crayon with just those three fingers!" (reinforcing grasp, not drawing quality)
- "You went ALL the way down — that's a perfect line!" (reinforcing stroke direction)
- "Your hand stayed inside the path the whole time!" (reinforcing visual-motor control)
- "You found all three things in the putty — your fingers are so strong!" (reinforcing effort + strength)
❌ What NOT to Say
- "Good job" — too generic; child doesn't know what behavior earned it
- "That's beautiful!" — judges the product, not the process; discourages risk-taking
- "Almost! Try again." — correction mid-activity kills motivation
Celebrate the attempt, not just the success. A child who engages with therapy putty for 2 minutes despite disliking the texture deserves the same celebration as a child who produces a perfect circle. Reinforcement options: verbal praise + high five | token/sticker chart | Rosette Imprint Reward Jar ₹589 → | brief access to preferred toy (1–2 min) after session.

ACT III — STEP 6
Step 6: The Cool-Down
The Rule: No session ends without a 2-minute cool-down transition. Abrupt endings cause post-session dysregulation — the child doesn't understand the shift and protests or melts down.
Warning 1 — 2 Minutes Before End
"We have 2 more — then we're all done." [Hold up 2 fingers visually]
Warning 2 — 1 Minute Before
"One more, then we'll put everything away."
Closing Ritual
"All done! You worked so hard today. Let's put the [material] back together." [Child participates in material put-away — fine motor skill in itself]
Transition Statement
"Now we're going to [name preferred next activity]. Time for [activity]."
Cool-Down Activities (1–2 min)
- Heavy work — push materials together firmly with both hands (proprioceptive calming)
- Hand washing — sensory routine, signals transition
- Deep pressure — press palms together firmly 5×
- Child places materials in container independently
If Child Resists Ending
Do NOT extend the activity — this teaches that protesting gets more time. Stay calm: "I know you want more. We're all done now. [Preferred activity] is next." Redirect immediately to the transition. Extending the session trains protest behavior.

ACT III — DATA
Capture the Data: Right Now
The 60-Second Post-Session Data Rule: Data captured immediately after session is 10× more accurate than data recalled later. This is your child's progress record. 60 seconds now saves hours of guessing in 4 weeks.
Field 1 — Session Rating
1 — Did not engage | 2 — Tolerated briefly | 3 — Engaged partially | 4 — Engaged fully | 5 — Requested more
Field 2 — Grasp Quality Observed
Fist grip throughout | Mixed grip | Tripod moments observed | Consistent tripod/near-tripod | N/A (non-pencil activity)
Field 3 — Today's Best Moment
One sentence: "She held the tong with three fingers for 5 transfers." or "He drew a line from top to bottom without lifting."
"60 seconds of data now saves hours of guessing later." — Pinnacle OT Consortium
ACT III — TROUBLESHOOTING
What If It Didn't Go As Planned?
"Session abandonment is not failure — it is data." Here are the most common obstacles and exactly what to do next.
Child refused every material and left the table
Why: Child was not in a regulated or motivated state. Next time: Pair each material with something the child loves (playdough + hide their favorite small toy inside). Never force return to table — this creates negative associations. Try again in 2 hours or tomorrow.
Child used fist grip despite correction
Why: Verbal correction alone doesn't rewire motor habits. Next time: STOP verbal corrections entirely. Change the tool — use broken crayon only. Fist grip is physically impossible on a 1-inch piece. The tool does the correcting. Your voice does the celebrating.
Child could only scribble — couldn't imitate the stroke shown
Why: The stroke targeted is above their current developmental level. Next time: Drop back to the previous developmental stroke. If they can't copy a circle, go back to horizontal lines. If they can't copy horizontal, stay on vertical. Master each before advancing.
Child became distressed when hands touched sensory tray
Why: Tactile defensiveness — the tactile processing system over-registers sensory input. Next time: Start with indirect contact (use a tool in the tray, not bare hand). Gradually decrease tool length over sessions. Never force direct contact — gradual habituation works; forced contact backfires.
Child only did one material for 2 minutes then ran away
Why: Attention capacity and/or intrinsic motivation was low. 2 minutes IS a legitimate session for some children. Next time: Accept the 2 minutes. Celebrate it. Build from there: "We did playdough for 2 minutes — that's our record. Tomorrow let's try 2 minutes AND tongs."
Session went great but no change in grasp quality
Why: Grasp change is a multi-week outcome, not a session-level outcome. Next time: Trust the process. Document grasp quality each session. You will see the shift across weeks, not days.
Child keeps wanting to eat the playdough
Why: Oral seeking behavior — common in younger children and sensory seeking profiles. Next time: Use salt dough (the salt taste is aversive and discourages eating). Alternatively, use commercially sealed therapy putty. Provide an oral motor item (chewy tube) at the same time.

ACT III — ADAPT
Adapt & Personalize: Every Child Is Different
No two children respond identically to these materials. Here is how to adjust the technique for your child's specific profile. Each material has three levels — start where your child succeeds and build from there.
Material | EASIER | STANDARD | HARDER | |
Putty/Dough | Extra-soft dough, large pieces | Standard commercial playdough | Therapy putty medium/firm resistance | |
Tongs | Large kitchen tongs + large pom poms | Medium tongs + medium objects | Tweezers + small beads | |
Vertical Surface | Large paper, whole arm movement | A4 paper, crayon/marker | Small paper, short crayon | |
Sensory Tray | Finger only, wide paths | Stylus (chopstick), medium paths | Pencil, narrow paths | |
Lacing | 4 large holes, stiff lace | 8 holes, semi-flexible lace | 12 holes, flexible thread, pattern | |
Mazes | Finger tracing, finger-wide path | Crayon, pencil-wide path | Pencil, hair-thin path | |
Stickers | Large stickers, easy peel | Medium stickers | Small dot stickers, precise placement |
For Autism
Use preferred themes for all activities. Provide visual schedule before session. Use consistent materials and sequence.
For Hypotonia
Emphasize putty phase. Vertical surface is essential. Shorten sessions to 8–10 min; quality over duration.
For Sensory Avoiding
Begin with tools — no direct texture contact. Gradually decrease tool length. Build contact tolerance slowly over weeks.
For ADHD
Rotate materials every 3 minutes. Use visual timer. Keep sessions to 10 minutes max; multiple short sessions daily preferred.

ACT IV — PROGRESS ARC
Weeks 1–2: What to Expect
Most parents expect visible handwriting improvement within 2 weeks. The evidence says: early-phase outcomes are about participation, not performance. This is when the neural foundations are beginning to form — not when you see them.
✅ Observable Progress in Weeks 1–2
- Child tolerates sessions — even 3–5 minutes is normal
- Reduced resistance to specific materials (familiarity effect)
- Increased duration of material contact by even 30 seconds per session
- Spontaneously approaching the materials (motivation building)
- First observable moments of non-fist contact with writing tools
❌ What Is NOT Expected Weeks 1–2
- Grasp change — too early; motor patterns take 4–6 weeks minimum
- Stroke imitation improvement — foundational strength not yet built
- Reduced frustration during writing tasks at school — hasn't generalized yet
Parent Emotional Preparation
Weeks 1–2 may feel like "nothing is working." This is the most common drop-out window for home intervention programmes. Parents who persist through weeks 1–2 with consistent, brief sessions see consolidation by weeks 3–4. Data tip: Count session duration. If it increased from 3 minutes to 5 minutes — that is measurable, real, valid progress.

ACT IV — PROGRESS ARC
Weeks 3–4: Consolidation Signs
Between weeks 3–4, the repetition accumulated in weeks 1–2 begins to manifest as observable change. Most parents miss these signals because they're watching for dramatic improvement rather than the subtle consolidation behaviors that are actually the real evidence of progress.
🧠 Anticipation
Child goes to the material storage area independently before the session — they remember and expect the activity. This signals positive associative memory forming.
🤲 Grasp Emergence
First spontaneous moments of 3-finger grip on broken crayons or tongs — even brief (2–3 seconds) — indicate the motor pattern is beginning to encode.
📐 Intentional Marks
Scribbles that begin to show directionality — lines that go more consistently in one direction, circles that are more consistently round. The child is starting to control.
⏱ Session Tolerance
Sessions extend naturally to 12–15 minutes without behavioral resistance — the child is no longer fighting the demand level.
🔁 Generalization Seeds
Child spontaneously uses tripod-like grip on other objects (forks, toothbrush) — the pattern is bleeding into daily life.
If you're seeing 3+ of the above signals, begin increasing session demands: add 1 new material from the 9, advance one level on the difficulty slider, and increase session duration by 5 minutes. By week 4, your own confidence as session facilitator will also have increased — and your child reads your confidence. It becomes part of the therapy.

ACT IV — PROGRESS ARC
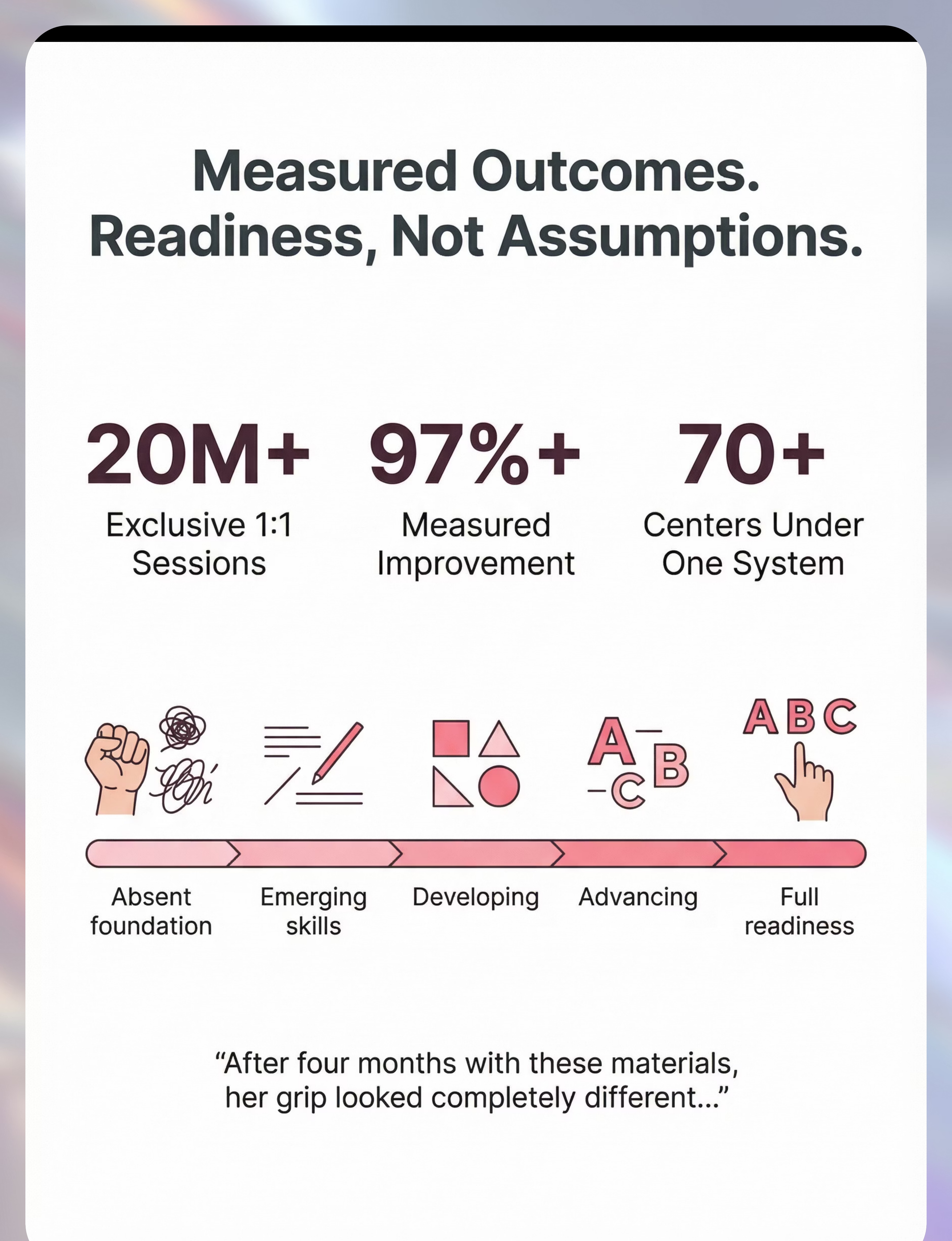
Weeks 5–8: Mastery Indicators
The Mastery Phase — what "Ready for the Pencil" actually looks like. These are the clinical criteria that Pinnacle OTs use to determine when a child is ready to advance to formal pencil work and letter formation.
Grasp
Consistent tripod or quadrupod grasp on short writing tool for 80%+ of writing tasks across 3 consecutive sessions
Stroke Sequence
Can imitate and independently produce all strokes up to developmental age (minimum: vertical + horizontal + circle for age 3; + cross + square for age 4–5)
Pressure Grading
Consistent pencil pressure — visible mark without crayon breaking, appropriate to surface
Hand Dominance
Clear consistent dominant hand preference established
Session Tolerance
20+ minute sessions with engagement and without behavioral resistance
Transfer to ADLs
Improved grip observed in daily activities — utensils, toothbrush, scissors attempt
If fewer than 4/6 mastery criteria are met by Week 8 → continue for 4 more weeks before advancing. If 5–6/6 are met → proceed to F-607 (Pencil Grip Problems) or begin letter formation instruction with an OT.
ACT IV — CELEBRATE
You Did This. Your Child Grew Because of Your Commitment.
Six to eight weeks ago, a 4-year-old was wrapping her fist around a crayon and making random marks that frustrated her. Today, she holds a broken crayon with three fingers, draws a circle that closes, and traces a path from left to right without lifting. Her hands are writing-ready — not because the kindergarten letter workbook finally clicked, but because you chose to build the invisible foundation first.
That is not small. That is the difference between a child who enters school ready and a child who spends years fighting a system whose prerequisite skills were never built. You are not just a parent running home therapy. You are a therapeutic partner in your child's neurodevelopment.
🎉Mark this milestone visibly. Frame one of the first controlled drawings your child made in week 1 next to one from week 8. The visual progression is the most powerful evidence document you have.
📝Journal prompt: Write one sentence today: "Before [date], [child's name] could not ________. Today, [he/she] ________." This is the data that matters most.
📝Journal prompt: Write one sentence today: "Before [date], [child's name] could not ________. Today, [he/she] ________." This is the data that matters most.

ACT IV — SAFETY
Red Flags: When to Pause and Seek Professional Support
Trust your instincts. If something feels wrong, pause. These five signals mean it's time to step beyond home-based intervention and bring in clinical support.
🚩 Hand Pain or Swelling After Sessions
What it looks like: Child guards hand, refuses touch, or shows visible swelling post-session.
Why it matters: May indicate hypermobility, joint laxity, or structural issue.
Action: Stop activities causing pain immediately. Consult pediatric OT within 2 weeks.
Why it matters: May indicate hypermobility, joint laxity, or structural issue.
Action: Stop activities causing pain immediately. Consult pediatric OT within 2 weeks.
🚩 Zero Grasp Progress After 8 Weeks
What it looks like: Fist grip remains 100% consistent despite tool modifications.
Why it matters: May indicate neurological differences, significant low muscle tone, or motor planning disorder.
Action: Request formal OT fine motor assessment. Do not continue pushing without professional input.
Why it matters: May indicate neurological differences, significant low muscle tone, or motor planning disorder.
Action: Request formal OT fine motor assessment. Do not continue pushing without professional input.
🚩 Extreme Distress Response to All Tactile Materials
What it looks like: Child screams, vomits, or shows extreme behavioral response to material contact.
Why it matters: Severe tactile defensiveness may be a sensory processing disorder requiring clinical sensory integration therapy.
Action: Discontinue texture-based materials. Seek SPD/sensory integration evaluation from qualified OT.
Why it matters: Severe tactile defensiveness may be a sensory processing disorder requiring clinical sensory integration therapy.
Action: Discontinue texture-based materials. Seek SPD/sensory integration evaluation from qualified OT.
🚩 Hand Preference Still Absent After Age 5
What it looks like: Child consistently switches hands mid-activity with no emerging dominance at age 5+.
Why it matters: Mixed laterality at age 5+ warrants neurological evaluation.
Action: Document the pattern and discuss with neurodevelopmental pediatrician.
Why it matters: Mixed laterality at age 5+ warrants neurological evaluation.
Action: Document the pattern and discuss with neurodevelopmental pediatrician.
🚩 Pre-Writing Delays + Regression in Other Areas
What it looks like: Losing previously acquired skills alongside the fine motor delay.
Why it matters: Developmental regression is always a clinical flag regardless of domain.
Action: Urgent — consult neurodevelopmental pediatrician. Do not wait.
Why it matters: Developmental regression is always a clinical flag regardless of domain.
Action: Urgent — consult neurodevelopmental pediatrician. Do not wait.
📞FREE Helpline: 9100 181 181 — 24×7, 16+ languages. Clinical guidance available. Escalation pathway: Home monitoring → Teleconsultation → Clinic evaluation → Specialist referral.
ACT IV — PATHWAY
The Progression Pathway: Your Position in the Fine Motor Journey
Pre-writing skill development (F-606) sits at the center of the fine motor journey — built on the foundations of hand strength and finger isolation, and leading forward into functional pencil grip and letter formation. Knowing where you are in the sequence helps you plan what comes next.
Grasp Mastered → F-607
Pencil Grip Problems — advance from pre-writing into functional pencil hold. View Technique →
Bilateral Gap → Lacing Track
Target: Simultaneous two-hand skilled use. Relevant for cutting, dressing, musical instruments.
Visual-Motor Gap → VMI Track
Target: Eye-hand coordination for copying, drawing, reading. Relevant for shape copying and maze completion.
Solid Foundation → F-608
Letter Formation — correct formation sequence, directional consistency, legible size and spacing.

ACT IV — RELATED TECHNIQUES
Related Techniques in This Domain
You already have materials for some of these techniques if you've been working through F-606. Materials overlap is intentional — the Pinnacle system is designed for maximum efficiency with minimum cost.
F-603: Hand Strength Building
🟢 Foundation Level | Uses: Playdough, resistance activities
Build the strength that makes pre-writing possible
→ View Technique
Build the strength that makes pre-writing possible
→ View Technique
F-604: Finger Isolation
🟢 Foundation Level | Uses: Tweezers, pegs, pop toys
Train each finger to move independently
→ View Technique
Train each finger to move independently
→ View Technique
F-605: Scissor Skills
🟡 Core Level | Uses: Safety scissors, paper strips
Bilateral coordination in a graded snipping format
→ View Technique
Bilateral coordination in a graded snipping format
→ View Technique
F-607: Pencil Grip Problems ← NEXT
🟡 Core Level | Uses: Broken crayons, pencil grips, short pencils
Advance from pre-writing into functional pencil hold
→ View Technique
Advance from pre-writing into functional pencil hold
→ View Technique
F-608: Letter Formation
🟠 Advanced Level | Uses: Sand trays, templates, multisensory letter kits
Correct formation sequence, directional consistency
→ View Technique
Correct formation sequence, directional consistency
→ View Technique
F-610: Handwriting Legibility
🔴 Advanced Level | Uses: Lined paper, spacing tools, pacing guides
Size, spacing, and speed for academic writing
→ View Technique
Size, spacing, and speed for academic writing
→ View Technique
ACT IV — FULL MAP
Your Child's Full Developmental Map
Fine Motor (F-606) is one technique within the Fine Motor & Handwriting domain — itself one of 12 developmental domains that together constitute a child's complete developmental profile within GPT-OS®.
The FusionModule™ Principle: Pre-writing skill development does not exist in isolation. When a child's hands build strength and coordination through this programme, you will likely see ripple effects in: self-care (dressing buttons, utensil use), play (construction toys, drawing), and cognitive engagement (sustained attention during fine motor tasks). Therapeutic gains in one domain catalyze progress in adjacent domains.
🔗See your child's full developmental profile in GPT-OS® →
🔗See your child's full developmental profile in GPT-OS® →
ACT V — COMMUNITY
Families Who've Been Here: From Fear to Mastery
These three family vignettes are based on composite clinical narratives from Pinnacle center case documentation. Individual details anonymized. Outcomes representative of documented GPT-OS® case archives; individual results vary.
Priya, Hyderabad
"My son Arnav was 4.5 with a death grip on every crayon. His preschool teacher said he needed to work on 'pre-writing' before they could progress him. The OT gave us broken crayons, playdough, and paper taped to our bathroom wall. Week 7, I watched Arnav pick up a small crayon piece and hold it with three fingers — unprompted. He drew a circle that actually closed. His teacher messaged me saying 'something changed.' I cried."
Therapist: "Fist grip was the presenting behavior, but the root was inadequate intrinsic hand strength. Playdough built the strength. Broken crayons rewired the grip pattern. The wall vertical surface established wrist extension. Seven weeks. The sequence was the therapy."
David, Kerala
"Maya is 5 and was starting to fall behind in LKG. She couldn't draw a person — not even a circle with lines. Her eyes and hands weren't working together. Eight weeks of sensory tray practice, mazes starting with finger-wide paths, and lacing cards. Today she colors within lines and copies shapes. She's not the child avoiding the drawing table anymore. She's the child who asks when art time is."
Therapist: "Maya's core deficit was visual-motor integration. Sensory trays built the tactile feedback loop. Mazes trained the eyes-to-hand pathway. The lacing built bilateral coordination. All three were needed simultaneously."
Sita, Maharashtra
"Riya has autism. Getting her to do anything with a pencil triggered a meltdown. The framework changed everything. We started with just playdough — hidden toys inside, her favorite characters as stamps. No pencil, no demand to draw. Six weeks later, she was willingly picking up the broken crayons herself."
Therapist: "For children with ASD, the invitation and reinforcement architecture of this protocol is as critical as the materials themselves. We never demanded engagement with the writing tools. Pencil readiness emerged as a natural downstream outcome."
ACT V — COMMUNITY
You Don't Have to Figure This Out Alone
If only one caregiver implements this programme, the child receives intervention for ~1 hour/day. If both parents, grandparents, and the preschool teacher all understand the principles, the child receives therapeutic input across all waking hours. Community is not optional — it is the mechanism through which home-based intervention becomes transformational.
📱 WhatsApp Parent Community
Join the Pinnacle Fine Motor Parent Group — parents navigating pre-writing with children in the same age range. → Join WhatsApp Group
💬 Online Forum
Share questions, progress updates, and resource discoveries with families across India and 70+ countries. → Pinnacle Parent Forum
🤝 Peer Mentoring
Connect with a parent who has already completed this technique journey with their child. → Request a Peer Mentor
📍 Local Parent Meetups
Pinnacle centers across 70+ locations in India host monthly parent meetups organized by technique domain. → Find Nearest Center
"The parents in the Pinnacle Fine Motor group gave me the confidence to break crayons on purpose. That sounds small. It was transformative." — Parent, Pinnacle Bengaluru Center
📞 Helpline: 9100 181 181 — You can also call just to talk to someone who understands.
ACT V — PROFESSIONAL SUPPORT
Your Professional Support Team: Home + Clinic = Maximum Impact
"Every child who engages in home-based pre-writing intervention achieves significantly better outcomes when that home programme is supervised and calibrated by a clinical occupational therapist. Home and clinic are not alternatives — they are partners." — Pinnacle OT Consortium
Tier 1 — Free Consultation (Today)
📞National Autism Helpline: 9100 181 181
Available 24×7 in 16+ languages. Clinical guidance, material questions, session troubleshooting. No appointment required.
Available 24×7 in 16+ languages. Clinical guidance, material questions, session troubleshooting. No appointment required.
Tier 2 — Teleconsultation (This Week)
💻Book a Video Consultation →
One-on-one OT consultation via video. Therapist observes your session environment, assesses materials, and provides personalized protocol guidance. Available within 48 hours.
One-on-one OT consultation via video. Therapist observes your session environment, assesses materials, and provides personalized protocol guidance. Available within 48 hours.
Tier 3 — Center Assessment (Comprehensive)
🏥Find Nearest Center →
Full fine motor assessment: grasp analysis, visual-motor integration testing, hand strength measurement, AbilityScore® developmental baseline, and comprehensive OT programme design. 70+ centers across India.
Full fine motor assessment: grasp analysis, visual-motor integration testing, hand strength measurement, AbilityScore® developmental baseline, and comprehensive OT programme design. 70+ centers across India.
When calling or booking, request specifically: "I would like a Pediatric Occupational Therapy evaluation for pre-writing skill development including grasp assessment and visual-motor integration screening."
ACT V — RESEARCH
The Research Library: Deeper Reading for the Curious Parent
🔺 Level I — Systematic Reviews
PMC11506176 — PRISMA Systematic Review, Children (2024): 16 studies (2013–2023) confirm sensory-motor interventions meet evidence-based practice criteria. Home-based implementation equivalent to clinic-based when properly structured. → View on PubMed
PMC10955541 — Meta-Analysis, World J Clinical Cases (2024): Sensory integration therapy effectively promoted adaptive behavior and motor skills across 24 studies. Effect size moderate-to-strong for motor outcomes. → View on PubMed
🔺 Level II — Randomized Controlled Trials
DOI:10.1007/s12098-018-2747-4 — Padmanabha et al., Indian J Pediatrics (2019): Home-based sensory-motor interventions by trained parents in India demonstrated statistically significant motor outcomes. Validates cultural applicability. → View Study
PMC9978394 — WHO/UNICEF CCD (2023): Caregiver-delivered, material-supported motor activities produce measurable developmental gains across 54 LMICs — even without clinical-grade equipment. → WHO CCD Package
🔺 Level III — Expert Consensus
NCAEP (2020): Visual supports and structured routine intervention classified as evidence-based practices for autism. → NCAEP Report
AOTA Guidelines: Fine motor and handwriting development practice guidelines — foundational clinical framework for pre-writing skill sequencing. → AOTA
WHO NCF (2018): Five-component nurturing care model — the global policy framework underpinning this intervention. → nurturing-care.org

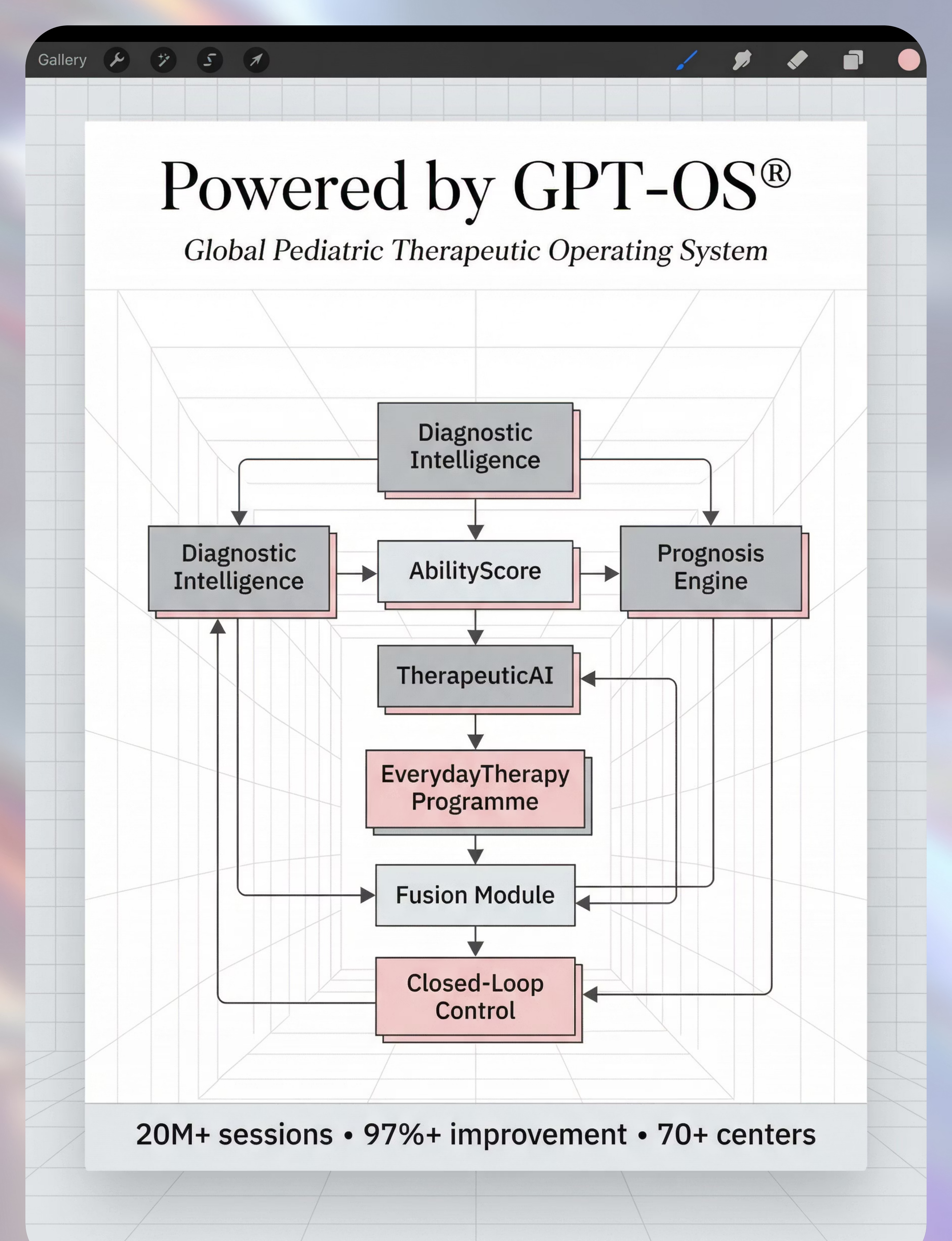
ACT V — GPT-OS®
How GPT-OS® Uses Your Data: Your Child's Progress, Personalized
Your data helps your child. Your data also helps every child like yours — through the anonymous, aggregated population intelligence that makes GPT-OS® recommendations more precise over time.
AbilityScore®
Tracks grasp baseline and development over time
TherapeuticAI®
Determines progression and next material selection
EverydayTherapy™
Designs your personalized home session structure
FusionModule™
Integrates OT + ABA + SpEd inputs holistically
Closed-Loop Control
Re-measures and re-calibrates based on your data
🔒 All data is encrypted, DPDPA-compliant (India Digital Personal Data Protection Act 2023), and never sold or shared with third parties. Anonymized, aggregated population data is used to improve recommendations for all families — your contribution helps the next parent who faces the same challenge.

ACT V — REEL
The Reel That Started This Journey
📹F-606 | 9 Materials That Help With Pre-Writing Skills
📂 Series: Fine Motor & Handwriting Development in Children | Episode 606
⏱ Duration: 75–85 seconds
📂 Series: Fine Motor & Handwriting Development in Children | Episode 606
⏱ Duration: 75–85 seconds
"Hi, I'm part of the Pinnacle Occupational Therapy Consortium. In this reel, I'm going to show you 9 materials that build the foundation your child needs before handwriting can succeed. These aren't expensive or complex. Several cost nothing. But they are the materials that OTs around the world use every day — and now you'll know exactly why."
What to Watch For
- The 9 materials demonstrated with actual children
- The grasp pattern visible on broken crayons vs. full crayons
- Wrist position comparison: vertical surface vs. flat table
- Sensory tray stroke practice — erasable, low-pressure
Related Reels in Series
- F-604: Finger Isolation
- F-605: Scissor Skills
- F-607: Pencil Grip Problems
Research: NCAEP (2020) — Video modeling classified as evidence-based practice for autism | Multi-modal learning improves parent skill acquisition.

ACT V — SHARE
Share This With Your Family: Consistency Across Caregivers Multiplies Impact
If only one caregiver implements this programme, the child receives intervention for ~1 hour/day. If both parents, grandparents, and the preschool teacher all understand the principles, the child receives therapeutic input across all waking hours. This is not optional for maximum impact — it is the mechanism through which home-based intervention becomes transformational.
📄 Explain to Grandparents
- Break the crayons — it's intentional and it works
- Paper should be on the wall, not always on the table
- Playdough is therapy — let them squeeze and roll it freely
- Don't correct the grip — change the tool instead
- Praise the effort and the fingers, not the picture quality
📋 Teacher / School Communication Template
"We are currently working on pre-writing skill development with [child's name] using an OT-directed home programme from Pinnacle Blooms Network (techniques.pinnacleblooms.org/fine-motor/pre-writing-skills-F-606). We are using broken crayons, vertical surface drawing, and sensory tray practice. It would be very helpful if [he/she] could use short crayons in class and work at the easel when possible. Thank you for partnering with us."

ACT VI — FAQ
Frequently Asked Questions
Questions we hear every day at Pinnacle centers — answered with clinical precision and parent-friendly language.
Q: My child is 4 and still uses a fist grip. Is it too late?
Not at all. The tripod grasp typically emerges between 3.5–4.5 years, but continues to develop and stabilize through age 6. Four years old is not late — it's the heart of the intervention window. The broken crayon modification alone often produces visible change within 3–4 weeks of consistent use.
Q: How many of the 9 materials do I need to start?
You need exactly one: broken crayons + paper taped to the wall. These are free and address the two most fundamental issues (grasp and wrist position). Add playdough in week 2. Add tongs in week 3. You do not need all 9 materials simultaneously — you build the toolkit gradually.
Q: My child has autism and refuses to touch playdough. What do I do?
Do not force tactile contact. Begin with tools (cookie cutter pressed into dough without touching it). Gradually move to touching through a thin plastic bag. Then to a fingertip touch for 1 second. Sensory tolerance is built through graduated exposure over weeks, not forced exposure in single sessions.
Q: How is this different from just giving more tracing worksheets?
Fundamentally different. Worksheets demand the output (letter tracing) without building the underlying capability (hand strength, grasp maturity, visual-motor integration). It is equivalent to demanding a child read before their visual processing system is ready. The 9 materials build the biological prerequisite. Worksheets require it. The sequence matters enormously.
Q: My child is in kindergarten and already behind. Is it too late?
Pre-writing foundational work is beneficial through age 7–8 for children with neurodevelopmental differences. A 6-year-old who has not mastered the pre-writing stroke sequence should begin where they are developmentally, not where the curriculum expects them to be chronologically.
Q: How do I know when to move from sensory trays to actual paper?
When the child can produce all strokes at their developmental level in the tray consistently (3 sessions in a row, same result) — with a tool (stylus or chopstick), not just finger — they are ready for paper. The paper version is more demanding: permanent marks, no erasing, higher pressure regulation required. Earn the paper; don't start with it.
Q: Can both parents run these sessions?
Ideally, both parents should understand the protocol — but one consistent primary facilitator per session is more effective. Consistency in session structure, material presentation, and reinforcement language matters more than who delivers it. Share this page with the other parent; use the simplified family guide from the Share card.
Q: How do I know if my child needs clinical OT beyond home materials?
Signs that clinical OT is needed: child is 5+ with consistent fist grip despite 8 weeks of intervention; zero progress in any domain after 8 weeks; severe tactile defensiveness making material engagement impossible; diagnosed condition (DCD, autism, hypotonia) without any clinical OT involvement. Call 9100 181 181 for guidance.
Preview of 9 materials that help with pre writing skills Therapy Material
Below is a visual preview of 9 materials that help with pre writing skills therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

ACT VI — START NOW
The Foundation Is Built One Session at a Time. Today Is Day One.
Every expert occupational therapist, every evidence-based study, and every family who has walked this path before you says the same thing: the foundation is built through consistent, brief, joyful sessions — not through pressure, worksheets, or waiting. You have everything you need to begin today.
🟢 Occupational Therapy
🟢 Speech-Language Pathology
🟢 Applied Behavior Analysis
🟢 Special Education
🟢 Neurodevelopmental Pediatrics
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | No appointment required
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System. "From fear to mastery. One technique at a time."
Every page on techniques.pinnacleblooms.org is authored by the Pinnacle Blooms Consortium — a multi-disciplinary team of Pediatric Occupational Therapists, Speech-Language Pathologists, ABA/BCBA Specialists, Special Educators, Neurodevelopmental Pediatricians, CRO professionals, and the parents and families who have walked this journey before you. 20 million therapy sessions. 97%+ measured improvement. 70+ centers.
This content is educational in nature and is intended to support — not replace — individualized professional assessment and intervention. It does not constitute medical advice, occupational therapy prescription, or clinical diagnosis. Persistent pre-writing difficulties may indicate underlying developmental conditions requiring formal evaluation. Always consult a licensed occupational therapist or neurodevelopmental pediatrician for comprehensive assessment and individualized programme design.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | techniques.pinnacleblooms.org | pinnacleblooms.org