
When Staying Upright Takes All Their Concentration
9 Clinically Validated Materials That Build Balance from the Ground Up
"My daughter is six years old and she still can't ride a bike. Not because she doesn't want to — she desperately wants to be like her friends. But she can't balance. She falls off playground equipment that other kids climb without thinking. She trips over nothing. The PE teacher mentioned she's 'clumsy.' She's started refusing to try things because she's embarrassed about falling. Her doctor said her ears are fine and there's nothing medically wrong. So why does my daughter act like gravity is her enemy?"
You are not failing. Your child's vestibular system is speaking. Balance can be built — with the right materials, the right approach, and the right guidance.
Sensory Solutions Series — Episode 90
Vestibular Processing + Motor Development
Ages 2–12 Years
Consortium Validated
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System. | Powered by GPT-OS®

02 — You Are Not Alone: The Numbers Behind Balance Difficulties
What feels isolating is, in fact, one of the most common sensory-motor challenges in pediatric development. These numbers reflect millions of families navigating the exact same path.
80%
Children with Autism
display sensory processing difficulties including vestibular and balance challenges. PRISMA Systematic Review, Children, 2024 — PMC11506176
1 in 6
Children Affected
experience developmental coordination difficulties including poor balance, representing millions of families worldwide. Meta-analysis, World J Clin Cases, 2024 — PMC10955541
18.5M+
Children in India
are estimated to experience neurodevelopmental differences where balance and motor challenges are a common feature. WHO/UNICEF Global Estimates; ICMR data
"You are among millions of families navigating this exact challenge. What feels isolating is, in fact, one of the most common sensory-motor difficulties in pediatric development."

03 — This Is a Wiring Difference, Not a Behaviour Choice
Understanding what is happening inside your child's brain is the first step to helping them. Balance is not a single skill — it is a neurological symphony.
Three Systems, One Balance Output
Your child's brain must simultaneously process three streams of information to stay upright:
- Vestibular Input — Inner ear → brainstem: where is the head in space?
- Proprioceptive Input — Muscles/joints → spinal cord → brain: where is the body positioned?
- Visual Input — Eyes → visual cortex → integration: what does the space look like?
All three streams must integrate in the cerebellum and brainstem to produce the automatic muscle adjustments that keep us upright.
What This Means for Your Child
When any of these systems is under-responsive, over-responsive, or poorly integrated, balance suffers. Your child isn't clumsy. Your child's brain is processing spatial information differently — and this can be addressed, because the vestibular system responds to structured input.
"The vestibular system is the oldest sensory system in the human brain. It develops before birth. And it can be strengthened at any age through appropriate input."
Research: Frontiers in Integrative Neuroscience (2020) — Neurological basis for sensory-based interventions.DOI: 10.3389/fnint.2020.556660 →

04 — Your Child Is Here. Here Is Where We're Heading.
Understanding where balance milestones fall in development helps you see your child's current position — and the achievable goal ahead.
2–18 Months
Head control, independent sitting, pulling to stand, and first independent steps. The vestibular foundation is being laid.
18 Months – 3 Years
Running, kicking, tiptoe walking, brief one-foot stands, tricycle riding. ⚠️ Challenge Zone begins here.
3–5 Years
Hopping, walking a balance beam, pedalling a bicycle, skipping, catching a ball. ⚠️ Primary challenge zone for vestibular difficulties.
5–7 Years
Riding a bicycle without training wheels, complex playground use. 🎯 Target milestone for this intervention.
7–12 Years
Sports participation, complex motor coordination, full peer physical play. 🏆 Long-term goal.
Balance difficulties commonly co-occur with: low muscle tone (hypotonia), developmental coordination disorder (DCD/dyspraxia), sensory processing differences, gravitational insecurity, vestibular hypo/hyperresponsivity, and autism spectrum-related motor differences.
WHO Care for Child Development Package — implemented across 54 countries.PMC9978394 → | WHO/UNICEF CCD Package →
05 — Clinically Validated. Home-Applicable. Parent-Proven.
This is not experimental. Vestibular-based balance intervention is among the most extensively researched approaches in paediatric occupational therapy, with evidence spanning decades and continents.
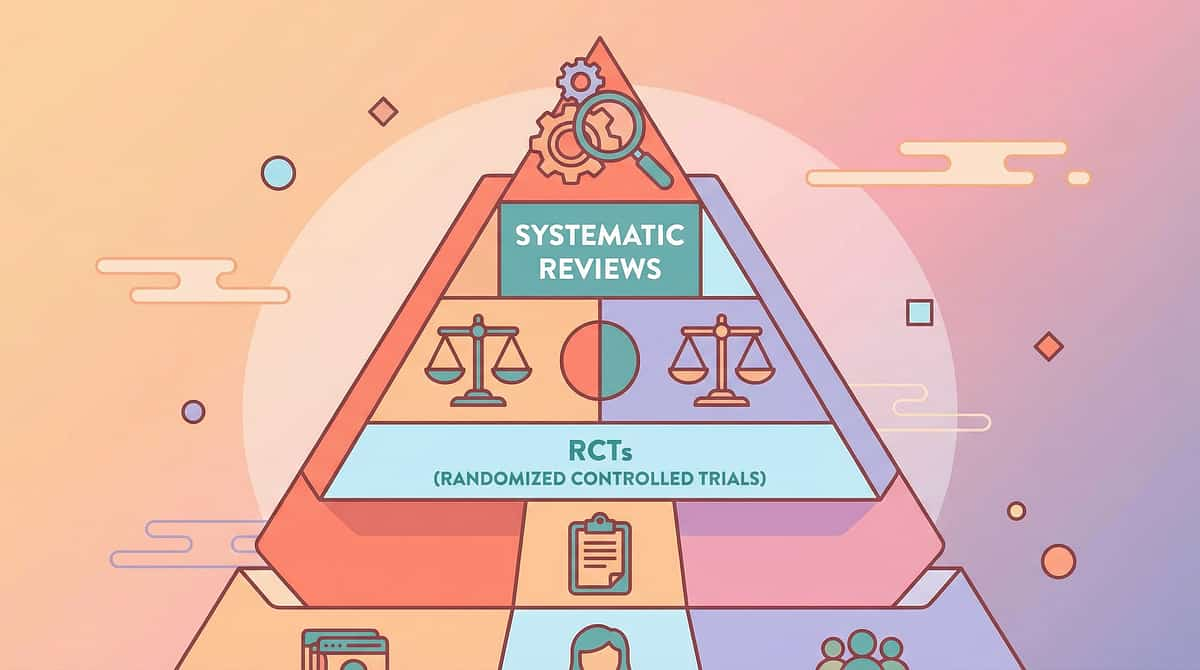
⬛ LEVEL I–II EVIDENCE — Supported by systematic reviews, meta-analyses, and randomised controlled trials.
Finding 1 — PRISMA Systematic Review (2024)
Across 16 articles (2013–2023), confirms sensory integration intervention meets evidence-based practice criteria for children with ASD, including vestibular and balance components. PMC11506176 →
Finding 2 — Meta-Analysis (World J Clin Cases, 2024)
Across 24 studies, demonstrates sensory integration therapy effectively promotes motor skills, adaptive behaviour, and sensory processing. PMC10955541 →
Finding 3 — Indian RCT (Indian Journal of Pediatrics, 2019)
Home-based sensory interventions demonstrate significant outcomes in Indian paediatric populations. DOI: 10.1007/s12098-018-2747-4 →
Finding 4 — NCAEP (2020)
Sensory integration is classified among evidence-based practices for children with autism by the National Clearinghouse on Autism Evidence and Practice. NCAEP 2020 Report →
"This is not experimental. Vestibular-based balance intervention is among the most extensively researched approaches in paediatric occupational therapy, with evidence spanning decades and continents."

06 — Balance Building Through Vestibular-Motor-Sensory Integration Materials
Parent-Friendly Alias: "The 9 Tools That Teach Your Child's Brain to Balance"
Definition: Poor balance in children refers to difficulty maintaining postural stability during static positions (standing still, sitting upright) and dynamic activities (walking, running, climbing, riding). Balance is a complex neurological function requiring integration of vestibular input, proprioceptive input, visual input, and coordinated motor responses.
This technique introduces 9 categories of therapeutic materials — each targeting a different component of the balance system — that families can use at home under guidance to progressively build their child's vestibular processing, postural control, core strength, proprioceptive awareness, and sensory-motor integration.
Domain
Vestibular Processing / Motor Development / Sensory Integration / Postural Control
Code
VEST-BAL-MOT
Age Range
2–12 years
Setting
Home + Therapy + Outdoor + School
Frequency
Daily balance activities, 10–20 minutes

07 — This Technique Crosses Therapy Boundaries
Because the brain doesn't organise by therapy type, balance intervention draws on multiple disciplines working in concert. Here is who does what — and why it matters for your child.
Occupational Therapist (OT) — Primary Lead
OTs trained in sensory integration (Ayres SI) assess vestibular processing, design graded sensory-motor activities, prescribe materials, and monitor integration. They address balance as a sensory processing function — building the vestibular system's ability to detect, interpret, and respond to movement.
Physical Therapist (PT)
PTs address the musculoskeletal and biomechanical components of balance — core strength, ankle stability, postural alignment, and gross motor coordination. While OT works on the sensory processing side, PT works on motor execution. Together, they address balance comprehensively.
ABA Therapist (BCBA/RBT)
ABA contributes reinforcement strategies, motivation systems, and systematic desensitisation for balance-avoidant children. Pairing and shaping procedures build willingness and tolerance when a child refuses balance activities due to fear or negative history.
Special Educator
Special educators integrate balance materials into classroom-based activities, ensuring gross motor practice generalises to school settings — PE participation, playground access, and physical classroom activities.
"When your child's OT works on vestibular processing and your PT strengthens their core simultaneously, the combined effect is greater than either alone. This is why Pinnacle's FusionModule™ coordinates all disciplines into a single converged pathway."
Adapted UNICEF/WHO Nurturing Care Framework (2022).DOI: 10.1080/17549507.2022.2141327 →

08 — Precision Targets — This Is Not Random Play, It's a Precision Tool
Every balance activity targets specific neurological and physical systems. Understanding these targets helps you measure real progress.
Primary targets are the direct neurological outcomes of vestibular intervention. Secondary targets build the physical infrastructure that supports balance. Tertiary targets are the real-world functional gains — the playground participation, the social confidence, the sport-readiness — that emerge when the primary and secondary targets are addressed consistently.
Meta-analysis (World J Clin Cases, 2024): SI therapy effectively promoted social skills, adaptive behaviour, sensory processing, and motor skills across 24 studies.PMC10955541 →

09 — Your 9-Material Balance Toolkit: Clinically Selected, Home-Ready
Each material targets a different component of the balance system. Start with one, build progressively. Prices are in Indian Rupees (₹).
# | Material | Price Range (₹) | Canon Category | Link | |
1 | Balance Boards & Wobble Boards | ₹500–3,000 | Gross Motor & Movement | ||
2 | Therapy Swings (Vestibular Input) | ₹2,000–15,000 | Professional Therapy Equipment | ||
3 | Balance Beams & Walking Paths | ₹500–4,000 | Gross Motor & Movement | ||
4 | Core Strengthening Equipment | ₹400–2,500 | Gross Motor & Movement | ||
5 | Stepping Stones & Obstacle Courses | ₹600–3,500 | Gross Motor & Movement | ||
6 | Proprioceptive Input Tools | ₹500–3,000 | Sensory Regulation | ||
7 | One-Legged Balance Practice Tools | ₹400–1,800 | Gross Motor & Movement | ||
8 | Visual-Vestibular Integration Activities | ₹300–2,000 | Sensory Regulation | ||
9 | Graduated Gross Motor Challenges | ₹500–5,000 | Gross Motor & Movement |
Total Investment Range: ₹300–15,000 — start with one material, build progressively.
Pinnacle Recommends — Essential Starters (total under ₹1,500):
1. Balance board or balance cushion (₹500–800)
2. DIY balance beam — tape line on floor (₹0)
3. Regular playground swing use (₹0 — free at any park)
1. Balance board or balance cushion (₹500–800)
2. DIY balance beam — tape line on floor (₹0)
3. Regular playground swing use (₹0 — free at any park)
10 — Every Family Can Start Today, Regardless of Budget
The WHO Nurturing Care Framework emphasises context-specific, equity-focused interventions. The CCD Package, implemented across 54 low- and middle-income countries, demonstrates that household-material-based interventions achieve meaningful outcomes. PMC9978394 →
Buy This | Make This (₹0) | Why It Works | |
Balance board (₹500–3,000) | Couch cushions, plank on a half-round dowel, folded towels under a board, pillows | Same principle: unstable surface activates vestibular-motor integration | |
Therapy swing (₹2,000–15,000) | Playground swing, hammock, blanket swing between two adults, spinning on parent's lap | Same vestibular input — linear, rotational, and orbital movement | |
Balance beam (₹500–4,000) | Tape line on floor, rope laid straight, curb walking (supervised), chalk line on pavement | Same dynamic balance challenge — narrowed path forces precise centre-of-gravity control | |
Core equipment (₹400–2,500) | Wheelbarrow walking, Superman pose, crawling games, sitting on pillow while playing | Same core engagement — any activity maintaining posture against gravity | |
Stepping stones (₹600–3,500) | Pillows on floor, paper plates, chalk circles on pavement, carpet squares | Same weight-shifting and single-leg balance demand | |
Proprioceptive tools (₹500–3,000) | Backpack filled with books, heavy carrying, wheelbarrow walks, deep pressure hugs | Same proprioceptive input from muscles and joints during resistance work | |
Balance pods (₹400–1,800) | Flamingo stance during teeth brushing, hopscotch, kicking games | Same single-leg stance practice | |
Visual-vestibular tools (₹300–2,000) | Eyes-closed balance (briefly, safely), play catch while on pillow, track flashlight while walking a line | Same sensory integration challenge | |
Graduated equipment (₹500–5,000) | Progression plan: stand 3 sec → 5 sec → 10 sec → on cushion → eyes closed | Same progressive challenge principle |
When is clinical-grade material non-negotiable? If your child has significant vestibular dysfunction, gravitational insecurity, or has been prescribed specific equipment by an OT/PT, use the recommended clinical-grade materials. DIY substitutes work well for general balance building but may not provide the precise graded input required for clinical-level intervention.

11 — Safety Gate: Read This Before Any Balance Activity
Vestibular input is powerful. Before beginning any balance activity, work through this traffic-light safety system carefully. Your child's safety — physical and emotional — is the foundation of every session.
🔴 DO NOT PROCEED IF:
- Child has a known inner ear infection or active ear condition
- Child shows signs of illness (fever, nausea, dizziness unrelated to activity)
- Child has had a recent head injury or concussion (physician clearance required)
- Child has an undiagnosed seizure condition — get medical clearance first
- Child is in severe emotional distress, post-meltdown, or dysregulated
🟡 MODIFY AND MONITOR IF:
- Child has gravitational insecurity — start at floor level only, child-directed pace
- Child has low muscle tone — ensure adequate support and shorter sessions
- Child has a history of motion sickness — start with very gentle, brief input
- Child is fatigued or has had a long therapy day — reduce intensity and duration
🟢 PROCEED WHEN:
- Child is calm, alert, fed, and rested
- Environment is clear of hard/sharp obstacles with soft landing surfaces
- Adult supervision is present throughout
- Materials are age-appropriate and stable
- Child is willing (not forced) to participate
Critical Safety Notes: Weighted items (vests, pads) should never exceed 5–10% of the child's body weight. Watch for vestibular overload signs: nausea, pallor, disorientation, excessive sweating, or distress — stop immediately if any appear. Never force a child through an activity they resist. Protect against public embarrassment and celebrate effort above all else.
Indian Journal of Pediatrics RCT (2019): Home-based sensory intervention safety protocols established for parent-administered sessions.DOI: 10.1007/s12098-018-2747-4 →

12 — Your Balance Practice Space: Set Up for Success
The environment is not a background detail — it is a core component of vestibular intervention. A well-prepared space enables focus, maximises safety, and signals to your child that something intentional and enjoyable is about to happen.
Your Setup Checklist
- ✅ Clear area: minimum 2m × 2m open floor space
- ✅ Soft surface: exercise mat, thick carpet, or grass
- ✅ Support nearby: wall, sturdy furniture, or adult hands within reach
- ✅ Bright, even lighting — child needs to see floor and equipment clearly
- ✅ Low ambient noise — auditory distractions compete for processing bandwidth
- ✅ Comfortable temperature — sweating or shivering diverts sensory attention
- ✅ Removed: hard-edged furniture, sharp corners, slippery rugs
- ✅ Barefoot preferred for maximum proprioceptive feedback, or non-slip socks
- ✅ Visual timer visible to child — builds routine and transition predictability
- ✅ Data sheet ready for post-session recording
Parent Positioning
Position yourself at the child's side, slightly behind — within arm's reach at all times. Not behind (child can't see you). Not in front (blocks their path). At the side, ready to stabilise without hovering.
Your calm, confident presence regulates your child's nervous system. If you are anxious about the activity, your child will feel it. Breathe. You are prepared.
Sensory Integration Theory (Ayres): Environmental setup is a core principle. Meta-analysis confirms 1:1 structured environment sessions are most effective.PMC10955541 →

13 — The Best Session Is One That Starts Right
A quick pre-session readiness check takes less than two minutes and dramatically improves outcomes. Never skip it. The data from this check guides your decision to go, modify, or postpone — and all three are valid choices.
# | Readiness Indicator | Yes / No | |
1 | Child has eaten within the last 2 hours (not hungry, not just fed) | ☐ | |
2 | Child has slept adequately (not overtired) | ☐ | |
3 | Child is in a regulated emotional state (no recent meltdown, tantrum, or crying) | ☐ | |
4 | Child is not ill (no fever, nausea, ear pain, headache) | ☐ | |
5 | Child shows willingness or neutral response to the activity invitation | ☐ | |
6 | Environment is set up per Card 12 | ☐ | |
7 | Safety checks from Card 11 are all clear | ☐ |
🟢 All Yes → GO
Proceed to Step 1: The Invitation.
🟡 1–2 No → MODIFY
Choose ONE material only. Shorter session (5 minutes). Lower challenge. More support. Still proceed if child is willing.
🔴 3+ No or Resisting → POSTPONE
Gentle rocking, deep pressure, or preferred quiet activity instead. Try again tomorrow. Postponing is not failure — it is clinical wisdom.

14 — Step 1: The Invitation (Not a Command)
Step 1 of 6
"Hey [child's name], look what I found! This wobble board — want to see what happens when you stand on it? I'll be right here. Let's try it together."
Body Language Guidance
Kneel to the child's level. Smile. Relaxed posture. Hold the material yourself first — demonstrate it is safe. Step on the balance board yourself, wobble dramatically, laugh. Make it inviting, not instructional. You are not delivering a lesson; you are playing.
What Acceptance Looks Like
- Child approaches the material
- Child watches with interest
- Child touches or steps towards the equipment
- Child asks questions or requests to try
- Child copies your demonstration
What Resistance Looks Like — and How to Respond
- Child turns away → Don't push. Leave the material visible. Return to it later.
- Child says "no" → "That's okay. It'll be here when you're ready." Engage with a preferred activity nearby.
- Child shows fear → Start at absolute floor level. Sit on the balance board instead of standing. Hold the child's hands while they touch the swing.
Timing: 30–60 seconds. The invitation is brief. You are reading the child's response, not delivering a lesson.

15 — Step 2: The Engagement Deepens
Step 2 of 6
"See how it wobbles? That wobble is teaching your body something. Your brain is learning to keep you steady. Watch what happens when I move my arms... Want to try? I'll hold your hands."
How you introduce each material shapes the child's first neural association with that experience. Make it curious, not instructional.
Balance Boards
Place on carpet/mat first. Show the child you can stand on it. Wobble. Laugh. Show it is not dangerous before the child ever touches it.
Therapy Swings
Sit in the swing yourself (if size allows). Push gently. Show the motion is controlled and enjoyable.
Balance Beams
Walk the tape line yourself. Wobble intentionally. Show the child it is perfectly okay to step off.
Stepping Stones
Hop stone to stone yourself. Make it a game. Exaggerate your effort and enjoyment.
Reinforcement Cue: When the child makes ANY approach toward the material — verbal praise immediately: "You looked right at it! You're so brave for trying!" Timing matters: within 3 seconds of the behaviour.
Timing for this step: 1–3 minutes. | PMC11506176: Sensory integration intervention with structured material introduction meets evidence-based practice criteria.

16 — Step 3: The Core Balance Activity
Step 3 of 6
This is where the therapeutic work happens. Each material has its own protocol. Quality of engagement always outweighs quantity of repetitions.
1
Balance Boards
Child stands with both feet. Hold adult's hands initially. Goal: maintain position for 5 seconds. Progress: release one hand → both → shift weight side to side → catch a soft ball while balancing.
2
Therapy Swings
Child sits in swing. Parent pushes gently — linear (back-and-forth) motion first. Goal: 1 minute without distress. Progress: increase amplitude → add rotational component → change positions.
3
Balance Beams
Child walks tape line on floor (no height). Goal: 2 metres without stepping off. Progress: narrower line → actual beam on floor → low raised beam → walk backwards → carry an object.
4
Stepping Stones
Child steps from stone to stone (pillows on floor). Goal: cross 5 stones without touching the floor. Progress: increase distance between stones → vary heights → add timing challenges.
5
Core Equipment
Child sits on therapy ball while playing with a toy. Goal: maintain seated balance for 2 minutes. Progress: bouncing gently → reaching for objects → prone on ball while doing a puzzle.
Common Execution Errors:❌ Holding too tightly (they can't learn if you are doing it for them). ❌ Moving too fast through progressions. ❌ Continuing past the child's engagement window. ✅ Provide MINIMAL support — enough to prevent injury, not enough to prevent wobble. Let them wobble. Wobble IS the therapeutic input.
Meta-analysis (World J Clin Cases, 2024): Core therapeutic action occupies 40–60% of session time for maximum effectiveness.PMC10955541 →

17 — Step 4: Repeat and Vary — 3 Good Reps Are Worth More Than 10 Forced Ones
Step 4 of 6
Target Repetitions by Material
- Balance board standing: 3–5 attempts of 5–10 seconds each
- Swing sessions: 1–3 minutes continuous, 2–3 rounds with breaks
- Balance beam crossing: 3–5 crossings
- Stepping stone navigation: 3–5 runs through the course
- Core ball sitting: 2–3 minutes continuous, 2–3 rounds
Variation Options to Maintain Engagement
- Change the material — alternate between two materials within one session
- Add a game element — "Can you stand on the board while I count to 10?"
- Change the sensory challenge — eyes open → eyes looking at a fixed target → eyes tracking a moving object
- Add music — balance activities with rhythm: marching, swaying, dancing on unstable surfaces
- Involve siblings — make it a family challenge
Satiation Indicators — when the child has had enough: Quality of balance attempts decreasing, increasing distractibility, requesting to stop, or physical fatigue signs. Respect the child's engagement window every time.
"3 good repetitions where the child is engaged and trying are worth more than 10 forced repetitions where the child is resistant and unhappy."

18 — Step 5: Celebrate the Attempt, Not Just the Success
Step 5 of 6
Specific, immediate praise is the fuel that drives neurological learning. Generic praise fades. Specific praise anchors the behaviour.
For an Attempt
"You stepped on the board! That was brave!"
For Effort
"Look at you wobbling and staying on! Your brain is learning right now!"
For Duration
"Five whole seconds! Last time it was three! You're getting stronger!"
For Recovery
"You wobbled and caught yourself! That's exactly what balance is!"
Timing Rule: Within 3 seconds of the behaviour. Immediate, specific, enthusiastic. Not generic "good job" — specific to what the child just did.
Reinforcement Menu Options
- Verbal praise (always — the primary reinforcer)
- High five / fist bump / secret handshake
- Sticker on a balance progress chart
- 2 minutes of preferred activity after balance practice
- "Balance champion" badge on the fridge
- Tell the other parent or grandparent what the child achieved today

19 — Step 6: The Gentle Landing
Step 6 of 6
"Two more tries on the board, then we're all done for today. All done! Great balance work today. Let's put the board away together."
The cool-down is not an afterthought. It is a neurological reset that consolidates the vestibular input the child has just received and signals a safe, predictable end to the session.
Transition Warning
Give a 2-attempt warning before ending. Children with vestibular and sensory processing differences need predictable endings. Surprise endings spike anxiety.
Cool-Down Activity (1–2 minutes)
Lie flat on the floor in "snow angel" position with deep breaths. Or gentle seated rocking — arms wrapped around knees, rocking side to side (calming vestibular input). Or deep pressure: firm hug, weighted lap pad, lying under a heavy blanket for 1 minute.
Material Put-Away Ritual
Child participates in cleanup. This creates a predictable end boundary and delivers proprioceptive input (carrying, pushing materials back). It also builds responsibility and routine.
If the child resists ending: "I know you want to keep going! That means you're having fun. We'll do it again tomorrow. Right now, let's [preferred transition activity]." Visual supports (timers) are evidence-based practice for autism per NCAEP (2020). NCAEP Evidence-Based Practices Report →

20 — 60 Seconds of Data Now Saves Hours of Guessing Later
Without data, you are guessing. With data, you are measuring. GPT-OS® uses your session records to detect patterns, recommend progressions, and personalise your child's next session automatically.
Data Point | How to Record | Example | |
Duration on balance board (longest hold) | Seconds | "8 seconds today (vs. 5 last time)" | |
Balance beam crossings (successful) | Tally out of attempts | "3/5 crossings without stepping off" | |
Level of support needed | Full → Partial → Minimal → Independent | "Partial support (one hand held)" | |
Child engagement | Scale 1 (refused) to 5 (enthusiastic) | "4 — engaged and willing" | |
Notable observations | Quick note | "Tolerated swing 2 min today. No nausea." |
Why this matters: GPT-OS® uses your data to detect patterns you cannot see, recommend when to progress or modify, predict your child's trajectory, and personalise the next session. Your 60 seconds of recording drives weeks of optimised intervention.
21 — Session Abandonment Is Not Failure — It's Data
Every difficult session tells you something clinically useful. Work through these problem-solution pairs before your next attempt.
Problem: Child refused the balance board
Why: Gravitational insecurity or negative past experience. Fix: Start at floor level — sit on the board instead. Place on thick carpet to reduce movement. Progress from touching → sitting → kneeling → standing over multiple sessions.
Problem: Child became nauseous or pale during swinging
Why: Vestibular overload. Fix: Stop immediately. Lie the child flat on their back. Provide deep pressure. Next session: reduce swing amplitude and duration by 50%. Always follow the child's lead.
Problem: Child engaged for 2 minutes then lost interest
Why: Satiation point reached — this is normal. Fix: 2 minutes of engaged practice is valuable! Switch material or end on a success note. Do not push for more.
Problem: Child fell and became upset or afraid
Why: The fall confirmed the child's fear. Fix: Comfort immediately. Validate: "That was scary. You're safe." Return to an easier challenge where success is guaranteed. Rebuild from there.
Problem: Child was distracted and wouldn't focus
Why: Environmental distractions or arousal level mismatch. Fix: Check environment (screens off, noise reduced). Try a more novel material. Assess arousal state — too high needs calming input first; too low needs alerting input first.
Problem: Child wanted to keep going and resisted ending
Why: The session was successful and motivating — a good problem. Fix: Still end on time. Over-practice leads to fatigue and diminishing returns. Use a visual timer consistently and promise tomorrow's session.
Emergency Guidance: If the child becomes severely distressed (prolonged crying, panic, vomiting): stop all activities, provide deep pressure and calm environment, and do not resume until you have consulted an OT.
22 — No Two Children Are Identical: Personalise for Yours
The standard protocol is a starting point, not a rigid prescription. Every child's vestibular system, emotional profile, and developmental stage is unique. Adjust accordingly.
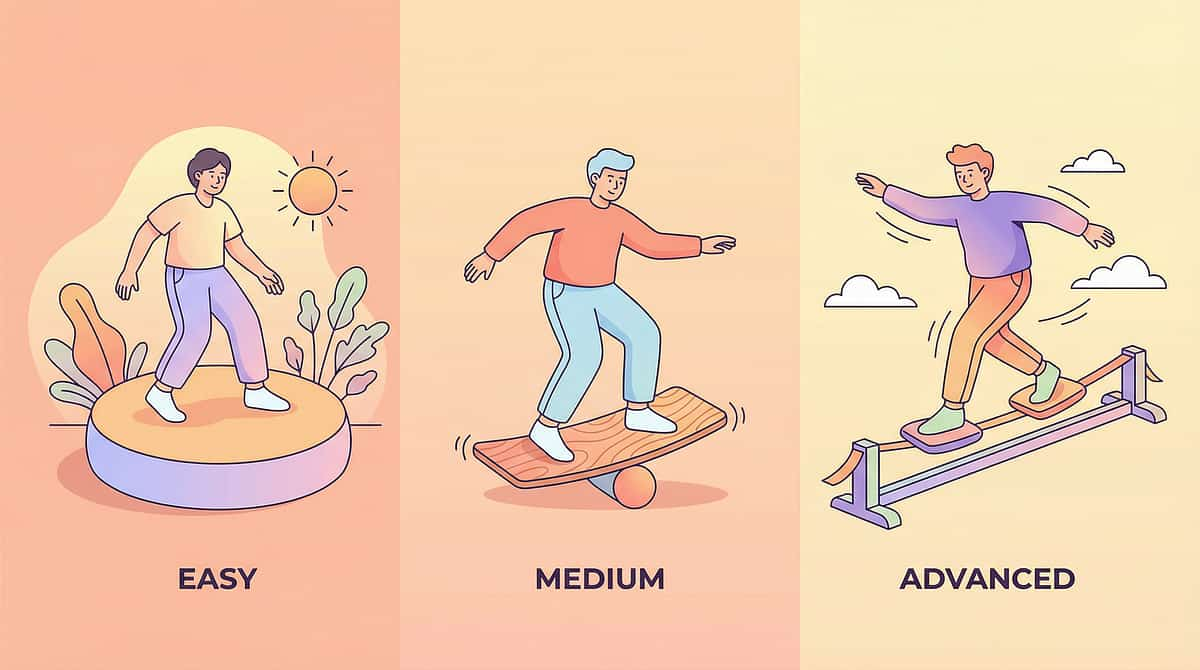
⬅️ Easier Modifications
All activities at floor level. Full adult physical support throughout. Single material per session. 5-minute maximum. Focus on tolerance, not performance. Child chooses which material to use. Stable surfaces before unstable.
Standard Protocol
Mixed materials per session. Partial support reducing over time. 10–15 minute sessions. Balance between challenge and success. Data tracking active throughout.
Harder Modifications ➡️
Unstable surfaces combined (board on mat, beam on cushion). Eyes-closed balance challenges. Dual-task balance (balance + catch, balance + count). Novel surfaces: grass, sand, gravel, slopes. Dynamic activities: riding, skating, sports drills.
Sensory Seeker (craves movement) | Sensory Avoider (fears movement) | |
More rotational input (spinning) | Linear input only (back-and-forth) | |
Faster swing speeds | Slow, controlled, child-paced | |
Higher challenge levels welcome | Floor-level only, gradual height increase | |
Challenge: overstimulation risk — set clear time limits | Challenge: engagement — use pairing and desensitisation |
Age Modifications: Ages 2–3: supported sitting/standing on cushions, parent-held swinging, tape lines. Ages 4–6: balance boards with support, low beams, stepping stones. Ages 7–9: independent board work, obstacle courses, bike progression. Ages 10–12: complex challenges, sports integration, advanced vestibular activities.

23 — Weeks 1–2: Tolerance, Not Mastery
Progress Arc — Week 1–2
In the first two weeks, you are not looking for mastery. You are looking for tolerance — and tolerance is the first, essential neurological milestone.
15%
Progress Arc
Week 1–2 benchmark. The vestibular system is beginning to register new input. Neural pathways are being introduced — not yet strengthened. Think of it as planting seeds, not harvesting crops.
What You May See
- Child tolerates standing on the balance board for 3–5 seconds (vs. immediate refusal)
- Child sits in the swing without resistance
- Child attempts to walk the tape line, even if stepping off frequently
- Reduced resistance to balance activities generally
- Beginning to approach materials voluntarily
What Is NOT Progress Yet — Managing Expectations
- Independent balance (too early)
- Riding a bike or complex tasks
- Enjoyment or enthusiasm (tolerance comes first)
- Consistency (good days and bad days are entirely normal at this stage)
Parent Metric: "If your child tolerates the balance board for 3 seconds longer this week than last week — that is real, measurable, neurological progress."
PMC11506176: Sensory integration intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation.

24 — Weeks 3–4: The Brain Is Wiring
Progress Arc — Week 3–4
Something is shifting. You will begin to see it in small, observable moments — a spontaneous one-foot stance, less furniture-holding, a willingness to attempt what was previously refused.
40%
Progress Arc
Week 3–4 benchmark. Neural pathway formation is underway. The vestibular system is consolidating its new input patterns.
Consolidation Indicators
Child anticipates balance activities (asks for the board, requests the swing). Duration on unstable surfaces increasing — 10–15 seconds on board vs. 3–5 seconds in Week 1. Reduced need for physical support. Beginning to recover from small wobbles without stepping off.
Behavioural Signals of Neural Change
Spontaneous single-leg stance while waiting. Reduced furniture-holding at home. Attempting playground equipment previously avoided. Improved sitting posture — less slouching. These small daily-life changes are the real evidence of neurological progress.
When to Progress
If the child is consistently successful at the current level for 3+ sessions → increase challenge by one step. Not a jump — a step. Wider board → narrower. Two hands held → one. Flat surface → slight cushion underneath.
Parent Milestone: "You may notice you are more confident too. The anxiety around your child's balance is being replaced by data. You can see the change. Trust what you see."

25 — Weeks 5–8: Mastery Unlocked
Progress Arc — Week 5–8
75%
Progress Arc
Week 5–8 benchmark. Mastery criteria are within reach. The neural pathways are established and generalisation to daily life is beginning.
Mastery Criteria — Observable and Measurable
- Stands on balance board independently for 15+ seconds
- Walks balance beam (floor level) end to end without stepping off
- Tolerates 3+ minutes of swing time with visible enjoyment
- Stands on one foot for age-appropriate duration (3+ sec at age 3–4; 5+ sec at age 5–6; 10+ sec at age 7+)
- Navigates stepping stone course with minimal hesitation
- Attempts new physical challenges with willingness, not avoidance
Generalisation Indicators
The most meaningful progress is when balance improvements appear in daily life — not just during structured practice sessions.
- Balance improvements appearing in playground behaviour
- Improved bike riding, scooter attempts, or sports participation
- Walking on uneven surfaces (grass, sand, gravel) with less hesitation
- Reduced clumsiness in daily activities
- Physical confidence emerging in social settings
Maintenance Check: Does the balance improvement persist without the structured protocol? If yes — the neural pathways are established. Continue activities as play, not therapy.
PMC10955541: Mastery criteria derived from behavioural measurement standards across 24 studies.

26 — You Did This. Your Child Grew Because of Your Commitment.
Remember Card 01? That parent whose six-year-old couldn't ride a bike — who held onto furniture walking through the house, who was already deciding what she "can't do"?
"Week 1: held my hand to stand on the board for 3 seconds. Week 8: catching a ball while standing on it alone."
Look at your child now. Standing on a wobble board. Walking a beam. Swinging without fear. Attempting things that were impossible weeks ago. Every wobble, every session, every moment of patience — it built this.
Celebrate as a Family
Mark this milestone meaningfully. A balance beam crossing party. A "first bike ride" video. A stepping stone course with the whole family. Let the child see that THEY achieved something worth celebrating.
Document the Journey
Before and after. This documentation is not just memory — it is evidence. Evidence that your child can grow. Evidence you will need on the harder days ahead.
Share Your Win
Your experience helps other families who are at the beginning of this journey, searching for reassurance that progress is possible. Consider sharing in the Pinnacle community.

27 — Trust Your Instincts: If Something Feels Wrong, Pause and Ask
Home-based intervention is powerful — and it works best when complemented by clinical oversight. Know when to escalate.
🚩 No improvement after 8 weeks of consistent practice
The child should show at least tolerance-level improvement. Absence of any change suggests the challenge may be more complex than home-based intervention alone can address.
🚩 Balance getting worse, not better
Regression may indicate an underlying condition (inner ear, neurological, or progressive) requiring medical evaluation. Do not delay.
🚩 Persistent nausea or vomiting with vestibular input
Some initial sensitivity is normal; persistent sickness is not. May indicate vestibular processing differences requiring specialist clinical-grade intervention.
🚩 Sudden onset of balance problems
If balance difficulties appeared suddenly (vs. always present), seek immediate medical evaluation to rule out neurological or inner ear pathology.
🚩 Balance difficulties with vision changes, headaches, or confusion
These combinations require urgent neurological assessment. Do not wait.
🚩 Severe anxiety or avoidance around all physical activity
The intervention should reduce avoidance, not increase it. If fear is escalating, the approach needs professional modification immediately.
28 — Your Child's Balance Journey: Where You Are, Where You're Going
This technique sits within a carefully mapped progression pathway. Knowing what came before — and what comes next — helps you see the full arc of your child's development.
The pathway is not linear for every child. Some will advance quickly through Path A to gravitational insecurity work; others will move laterally to coordination or motor planning. GPT-OS® uses your session data to recommend the optimal next step for your specific child.
29 — Related Techniques: You May Already Own the Materials
Balance materials overlap significantly with core strength, vestibular, and motor coordination tools. One toolkit, multiple interventions.
A-089: 9 Materials for Low Muscle Tone
Difficulty: Intro — Materials you already have: therapy ball, scooter board, bolsters ✅
A-091: 9 Materials for Gravitational Insecurity
Difficulty: Core — Materials you already have: therapy swings, balance boards ✅
A-092: 9 Materials for Movement Seeking Behaviour
Difficulty: Core — Materials you already have: stepping stones, obstacle courses ✅
A-088: 9 Materials for Coordination Problems
Difficulty: Core — Materials you already have: balance beams, visual tracking tools ✅
A-093: 9 Materials for Clumsiness
Difficulty: Intro — Materials you already have: multiple overlap materials ✅
A-094: 9 Materials for Motor Planning Difficulties
Difficulty: Advanced — Materials you already have: obstacle courses, graduated challenges ✅
30 — Balance Is One Piece of a Larger Plan
Better balance leads to better physical participation, which leads to better social access, which leads to better learning readiness. The vestibular foundation supports every domain of your child's development.
This technique addresses Domain A — Vestibular Processing / Balance / Postural Control. It is the sensory-motor foundation that supports every other domain in the wheel. When your child's balance improves, the ripple effects spread outward through communication, social participation, learning readiness, and daily life confidence.
GPT-OS® Connection: "This technique is one piece of your child's personalised developmental plan. GPT-OS® maps your child's profile across all 12 domains and recommends the optimal intervention sequence."
WHO/UNICEF Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring.WHO NCF →
31 — From Furniture-Holding to Bicycle-Riding: Real Families, Real Progress
These are anonymised stories from families within the Pinnacle Network. Individual outcomes vary by child profile. What is consistent is the direction of travel.
"She couldn't stand on one foot. She couldn't walk a straight line. She couldn't ride a bike — she wanted to so badly, but she just couldn't stay upright. We started with balance boards and therapy swings. It was slow at first, and she got frustrated. But we kept with it, little by little. After about eight months, she rode a bike around the block. No training wheels. I ran alongside her crying. Last week she tried a scooter for the first time. She wants to try roller skating next. The same child who held onto furniture when she walked across a room." — Parent, Pinnacle Network
"Our son would refuse to go to the playground. He'd say 'I'll just watch.' He was terrified of falling. We started with stepping stones at home — pillows on the floor. Then a tape line. Then a real balance beam at therapy. It took four months before he attempted the monkey bars. He didn't make it across — but he TRIED. That was the day everything changed. He stopped saying 'I can't' and started saying 'I'll try.'" — Parent, Pinnacle Network
From the Therapist's Notes: "Balance confidence doesn't follow a linear path. There are plateaus and setbacks. But the neurological trend, when measured objectively through the Vestibular Processing Index, is consistently upward. Parents often don't see the daily micro-progress — but the data shows it." — Pinnacle OT Clinical Lead
32 — You Are Not a Solo Operator: Join Families on the Same Journey
The challenges you are navigating — the frustration, the patience required, the setbacks, and the joy of watching your child grow — are shared by thousands of families in this network. Community does not just provide comfort; it provides actionable knowledge and lived-experience wisdom that no guide can fully replicate.
Balance and Motor Skills WhatsApp Group
Connect directly with parents navigating the same balance challenges. Share wins, ask questions, and receive peer support in real time.
Pinnacle Parent Community Forum
Longer-form discussions, technique questions, progress updates, and professional responses from Pinnacle's therapy team.
Local Parent Meetup
Find families in your city navigating similar journeys. In-person connection builds the support network that sustains long-term intervention.
"Your experience helps others. Consider sharing your journey — the parent searching tonight for 'why does my child keep falling' needs to hear that someone else's child fell too, and got up, and learned to balance."
33 — Home + Clinic = Maximum Impact
Home practice is most effective alongside professional guidance — not as a replacement for it. The combination of structured home sessions and clinic-based therapy produces outcomes neither achieves alone.
Your Professional Support Team
For balance and vestibular challenges, your primary match is a Paediatric Occupational Therapist with Sensory Integration (Ayres SI) training, supported by a Physical Therapist for gross motor strengthening and a BCBA for behavioural engagement strategies.
Relevant Pinnacle Services
- Occupational Therapy (Sensory Integration)
- Physical Therapy
- Gross Motor Programmes
- Sensory Processing Assessment
- EverydayTherapyProgramme™
- AbilityScore® Assessment
Find Your Support
Pinnacle operates 70+ centres across India, with teleconsultation available for families in all locations.
Occupational Therapy → | All Services →
34 — Deeper Reading for the Curious Parent
This technique's evidence base grades at Level I–II on the Oxford Centre for Evidence-Based Medicine scale — the highest levels of clinical confidence available in paediatric intervention research.
📚 Study 1 — PRISMA Systematic Review (2024)
16 articles (2013–2023) confirming sensory integration intervention as evidence-based practice for children with ASD. 80% of children with ASD display sensory processing difficulties. PMC11506176 →
📚 Study 2 — Meta-Analysis: SI Therapy Effectiveness (2024)
24 studies demonstrating sensory integration therapy promotes social skills, adaptive behaviour, sensory processing, and motor skills. PMC10955541 → | DOI: 10.12998/wjcc.v12.i7.1260
📚 Study 3 — Indian RCT: Home-Based Sensory Interventions (2019)
Randomised controlled trial demonstrating significant outcomes of home-based sensory interventions in Indian paediatric populations. DOI: 10.1007/s12098-018-2747-4 →
📚 Study 4 — WHO/UNICEF CCD Package
Age-specific caregiving recommendations implemented across 54 countries, demonstrating household-material-based intervention efficacy. PMC9978394 → | WHO Nurturing Care Framework →
📚 Study 5 — NCAEP Evidence-Based Practices Report (2020)
National classification of sensory integration and visual supports as evidence-based practices for autism. NCAEP Report →

35 — Your Data Helps Every Child Like Yours
Every 60-second session log you complete does more than track your child's progress. It enters a learning system that improves recommendations for every family in the Pinnacle Network.
What GPT-OS® Learns from Balance Data
- Optimal session duration for different age groups
- Which materials produce fastest balance improvements
- Which progression sequences maximise confidence
- Vestibular Processing Index trajectories that predict motor milestones
- When to recommend professional escalation vs. continued home practice
Privacy and Data Protection
- All data encrypted in transit and at rest
- Anonymised before population-level analysis
- Parent controls: view, download, or delete your data at any time
- Compliant with India's DPDP Act (2023) and international standards
- ISO/IEC 27001 aligned information security

36 — Watch: 9 Materials That Help With Poor Balance — Sensory Solutions #90
This Reel is presented by Pinnacle Blooms Network's Occupational Therapy team, specialising in vestibular processing, sensory integration, and motor development. Every material recommended has been clinically validated across thousands of therapy sessions.
Reel Details
Series: Sensory Solutions | Episode: 90 | Reel ID: A-090 | Duration: 60 seconds | Domain: Vestibular Processing + Motor Development + Sensory Integration
Multi-modal learning works: Video modelling is classified as an evidence-based practice for autism (NCAEP, 2020). Parents who combine video demonstration with written guides acquire practical skills significantly faster than those using text alone. Watch the Reel, then return to the step-by-step protocol in Cards 14–19.
37 — Consistency Across Caregivers Multiplies Impact
The sessions you run at home are only as powerful as the consistency that surrounds them. When grandparents, teachers, and other caregivers understand and support what you are building, the neurological gains compound.
For Grandparents and Family Members
"[Child's name] has difficulty with balance because of how their brain processes movement signals. We're using special balance tools at home — a wobble board, stepping stones, and swinging — to help their brain learn to balance better. It's working. Please: encourage them, don't push too hard, celebrate every attempt, and let them practise on the stepping stones when they visit."
For Teachers and School Staff
"Dear [Teacher], [Child's name] is working on balance and vestibular processing with guidance from Pinnacle Blooms Network. It would be helpful to: allow extra time for physical transitions, provide a stable chair option, encourage playground participation without pressure, and celebrate physical attempts. For more information: techniques.pinnacleblooms.org"
WHO CCD Package: Multi-caregiver training is critical for intervention generalisation and maintenance.PMC9978394 →

38 — Your Questions, Answered
These are the questions Pinnacle families ask most frequently. If yours is not here, call the FREE Helpline: 9100 181 181.
How long until I see improvement in my child's balance?
Most families notice tolerance-level changes within 2–3 weeks of consistent daily practice. Meaningful functional improvements typically emerge across 6–12 weeks. Track data (Card 20) and trust the trend, not individual sessions.
Can poor balance in children be fully corrected?
In most cases, balance can be significantly improved through consistent vestibular-motor intervention. The vestibular system responds to structured input at any age. The goal is functional balance for daily life participation — achievable for the vast majority of children.
My child is terrified of any balance activity. How do I start?
This is gravitational insecurity. Start at absolute floor level. Sit on the balance board. Use the child's preferred toy ON the balance equipment to create a reason to approach. Never force. Progress from proximity → touching → sitting → standing over multiple weeks.
Is this safe to do at home without a therapist?
The activities in this guide are designed for home implementation with appropriate safety precautions (Card 11). For children with significant vestibular dysfunction or complex profiles, initial assessment from a paediatric OT is recommended. Home practice is most effective alongside professional guidance.
How much should I spend on materials?
You can start with ₹0. Tape lines, pillows as stepping stones, and playground swings cost nothing. If investing, a balance board or cushion (₹500–800) provides the best value for home practice. Build your toolkit progressively as your child advances.
My child has autism. Are these materials appropriate?
Yes. 80% of children with ASD experience sensory processing differences including vestibular challenges. These materials are extensively researched in ASD populations specifically (PMC11506176, PMC10955541). Key adaptations: follow the child's lead, use visual supports, build predictable routines, and apply ABA reinforcement strategies — all covered in this guide.
Can siblings participate?
Absolutely. Sibling participation normalises the activities, provides social motivation, and creates natural play contexts. Make obstacle courses, balance challenges, and stepping stone races family activities.
When should I seek professional help instead of continuing at home?
See Card 27 (Red Flags). Specifically: no improvement after 8 weeks, worsening balance, persistent nausea, sudden onset of balance problems, or accompanying vision or neurological symptoms.

39 — From Reading to Doing: Your Child's Balance Journey Starts Now
You have the science. You have the materials list. You have the step-by-step protocol, the safety guidance, the troubleshooting framework, and the progress milestones. Everything you need is here.
The only remaining step is the first one. Lay down a tape line. Place some pillows on the floor. Call your child in. Demonstrate the wobble board yourself. Laugh. Invite them. Begin.
1
20M+ Sessions
Delivered across the Pinnacle Network
2
97%+
Measured improvement rate
3
70+ Centres
Across India
4
160+ Countries
Patents filed across the globe
Validated by the Pinnacle Blooms Consortium: OT • PT • SLP • ABA/BCBA • Special Education • NeuroDevelopmental Paediatrics • CRO
📞 FREE National Autism Helpline: 9100 181 181 — 24/7 • 16+ languages • pinnacleblooms.org
📞 FREE National Autism Helpline: 9100 181 181 — 24/7 • 16+ languages • pinnacleblooms.org
Preview of 9 materials that help with poor balance Therapy Material
Below is a visual preview of 9 materials that help with poor balance therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

40 — The Pinnacle Promise
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System. | Powered by GPT-OS®
OT | PT | SLP | ABA/BCBA | Special Education | NeuroDev Paediatrics | CRO
"From fear to mastery. One technique at a time."
A parent arrived on Card 01 scared, confused, and exhausted. By Card 40, they understand the science, have the materials, have executed the technique, tracked the data, and connected with a community of families on the same journey. The loop closes. A new one begins.
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist, physical therapist, or healthcare provider. Persistent balance difficulties, especially when impacting daily function or occurring with other motor, sensory, or developmental concerns, should be evaluated comprehensively. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606