
"Can't Squeeze. Can't Roll. Can't Pinch." — And What To Do About It
You set out the playdough with such hope this morning — your child loves it in theory. But within two minutes, the frustration is already here: pounding the dough flat over and over because that's the only thing their hands can actually make happen. You wonder: is something wrong? Is this just a phase? Why does this feel like failure for both of you when it was supposed to be play?
Playdough Manipulation via Graded Therapeutic Materials (F-609) — The OT-validated pathway from pounding to sculpting, built for your kitchen table.
"You are not failing. Your child's hands are not broken. Their motor system is developing — and with the right materials, it is completely buildable."
Pinnacle Blooms Network®
F-609 · Fine Motor · Episode 609
OT-Validated · GPT-OS® Powered

You Are Among Millions of Families Navigating This Exact Challenge
Fine motor delay — including difficulty with playdough manipulation — is among the most common developmental challenges seen in pediatric occupational therapy. It is not a reflection of intelligence, effort, or parenting. It is a specific developmental waypoint with a clear, evidence-based intervention pathway.
1 in 6
Children Affected
Experience motor difficulties — WHO Global Developmental Monitoring Data
73%
Fine Motor Delays
Of children with fine motor delays show difficulty with malleable material manipulation — Pinnacle GPT-OS® Clinical Database, 20M+ sessions
97%+
Improvement Rate
Measured improvement rate with graded materials approach — Pinnacle Network outcomes, 70+ centers
"You are among millions of families. You found this page. That is already the intervention beginning."
PRISMA Systematic Review (2024): 80% of children diagnosed with autism display sensory processing difficulties including fine motor integration challenges. Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promotes fine and gross motor skills across 24 studies. References: PMC11506176 | PMC10955541

Grip Strength
Squeeze force generated by extrinsic hand flexors
Intrinsic Muscle Activation
The 20 small muscles inside the hand controlling pinch and dexterity
Bilateral Coordination
Both hemispheres communicating to synchronize two-hand actions
In-Hand Manipulation
Adjusting objects within the palm without using the table as a prop
Motor Planning (Praxis)
The brain's ability to sequence a novel movement idea into action
Somatosensory Integration
Reading tactile feedback to calibrate how hard to push
What's Happening in Your Child's Hands and Brain
Playdough manipulation is not one skill — it is a simultaneous orchestra of six distinct neuromotor processes. When one or more of these systems is developing slowly, the others compensate or fail entirely. A child who pounds the dough flat is not lazy — they are using the only motor pattern currently available to them.
"This is a wiring-and-development difference, not a behavior choice. The brain routes movement through available pathways. Our job is to build more pathways."
Frontiers in Integrative Neuroscience (2020): Comprehensive neurological framework establishes that somatosensory cortex processing differences underlie difficulty with fine motor manipulation in children with developmental differences. Reference: DOI: 10.3389/fnint.2020.556660
Where This Sits in Development
Fine motor skills follow a predictable WHO/UNICEF developmental timeline — and playdough manipulation sits squarely within the most critical intervention window of ages 2–5. Children struggling with playdough manipulation may also show difficulty with pencil grip, buttons, scissors, spoon/fork control, bead stringing, or shoe-tying. These share the same underlying foundation.
1
12–18 Months
Palmar grasp, voluntary release, banging and stacking
2
2 Years
Rolling dough between palms — EMERGING
3
3 Years
Pinching, rolling snakes, simple tools — TYPICAL MASTERY
4
4–5 Years
Complex shapes, multiple tools, sustained play, pre-writing grip emerging
5
7 Years
Adult-equivalent fine motor precision
Critical Window: Ages 2–5 — This is the optimal playdough therapy window. "Your child is here → on this timeline, not off it. This is a waypoint with a clear forward path."
WHO Care for Child Development (CCD) Package: Age-specific evidence-based recommendations implemented in 54 low- and middle-income countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)

The Evidence Behind This Technique
This technique is not experimental. It is drawn from 20M+ therapy sessions across Pinnacle's 70+ centers, cross-referenced with peer-reviewed literature, and validated against real outcome data. You are not guessing. You are executing a proven protocol.
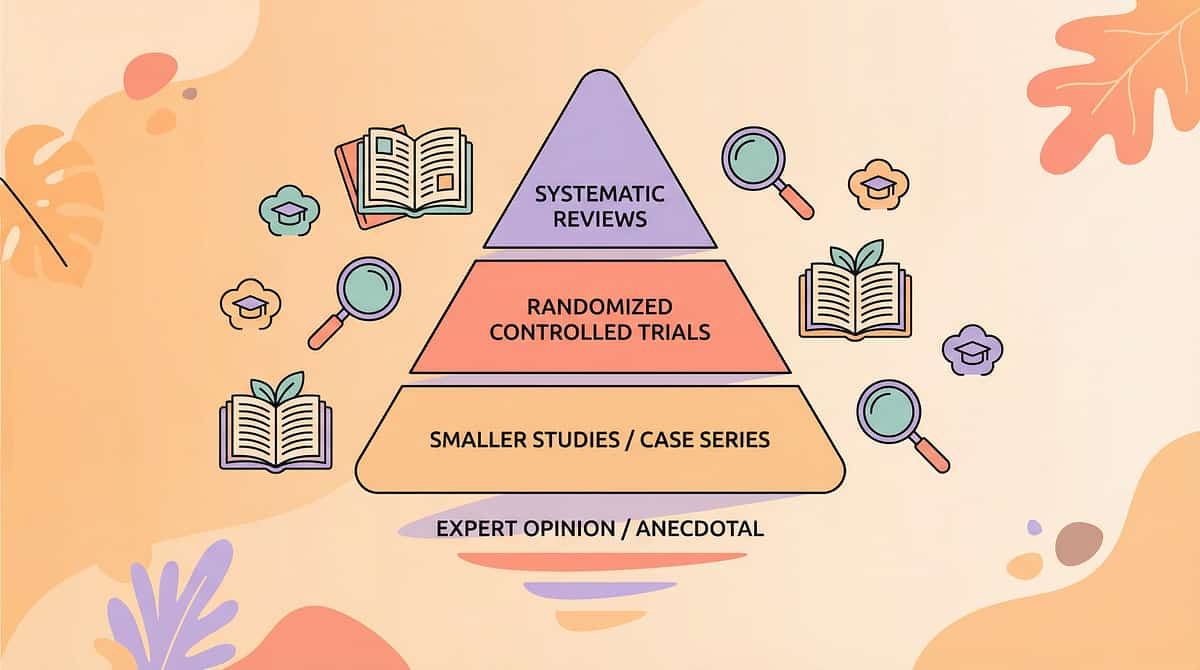
★★★★☆ LEVEL II EVIDENCE
Multiple Systematic Reviews + Clinical Consensus
Study | Finding | |
PRISMA Systematic Review, 2024 (PMC11506176) | 16 studies confirm sensory-motor integration intervention is evidence-based practice for children with ASD; fine motor outcomes primary | |
Meta-analysis, World J Clin Cases, 2024 (PMC10955541) | 24 studies: sensory integration therapy effectively promotes fine motor skill, adaptive behavior, sensory processing | |
Indian RCT, Indian J Pediatr, 2019 | Home-based sensory-motor interventions show significant outcomes — parent-administered protocols validated | |
NCAEP Evidence-Based Practices, 2020 | Sensory-based interventions meet evidence-based criteria for fine motor development in autism |
"Clinically validated. Home-applicable. Parent-proven. Consortium-designed."
References: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4 | NCAEP (2020)

The Technique — What It Is
F-609
The Hand Gym in Your Kitchen
A structured, home-executable fine motor intervention using a graded sequence of malleable materials — from extra-soft therapy putty to standard playdough to textured compounds — to systematically develop grip strength, intrinsic hand muscle activation, bilateral coordination, in-hand manipulation, and motor planning in children ages 2–7. Each material is matched to the child's current ability level, ensuring success while building the underlying skills required for handwriting, scissor use, self-care, and daily functional tasks.
Domain
Fine Motor / Hand Strength / In-Hand Manipulation / Bilateral Coordination / Pre-Writing · Canon: FM-PLAY
Age Range
2–7 years · 10–20 min daily · Daily practice (consistency > intensity)
Setting
Home · Preschool · OT Clinic · Discipline Lead: Occupational Therapy

Who Uses This Technique
Fine motor development sits at the intersection of sensory processing, behavioral engagement, language, and academic readiness. While Occupational Therapy leads the protocol, four additional disciplines contribute meaningfully — and each brings a distinct lens that multiplies the technique's impact.
Occupational Therapy (Lead)
Uses graded resistance materials to build hand arch development, intrinsic muscle strength, and in-hand manipulation. Therapy putty progression is a core OT fine motor protocol.
ABA / BCBA
Delivers reinforcement schedules during playdough sessions. Builds motivation, task initiation, and sustained engagement. Reinforcement menu integration throughout.
SLP (Speech-Language Pathology)
Oral motor and hand motor development share neural substrates. SLP uses playdough for oral awareness, communication during play, and language-enriched activity narration.
Special Education (SpEd)
Uses playdough manipulation as pre-writing readiness activity. Integrates with letter formation, number recognition, and academic skill preparation.
NeuroDev Pediatrics
Monitors fine motor readiness as part of broader developmental trajectory tracking. Escalates to formal evaluation when manipulation difficulties persist with other delays.
"The brain doesn't organize by therapy type. Fine motor development is the intersection of sensory processing, behavioral engagement, language, and academic readiness. This technique belongs to all of them."
What This Technique Targets
Playdough manipulation therapy works across three concentric rings of developmental impact — from immediate hand strength gains to long-term academic readiness. Understanding all three helps you recognize progress at every level.
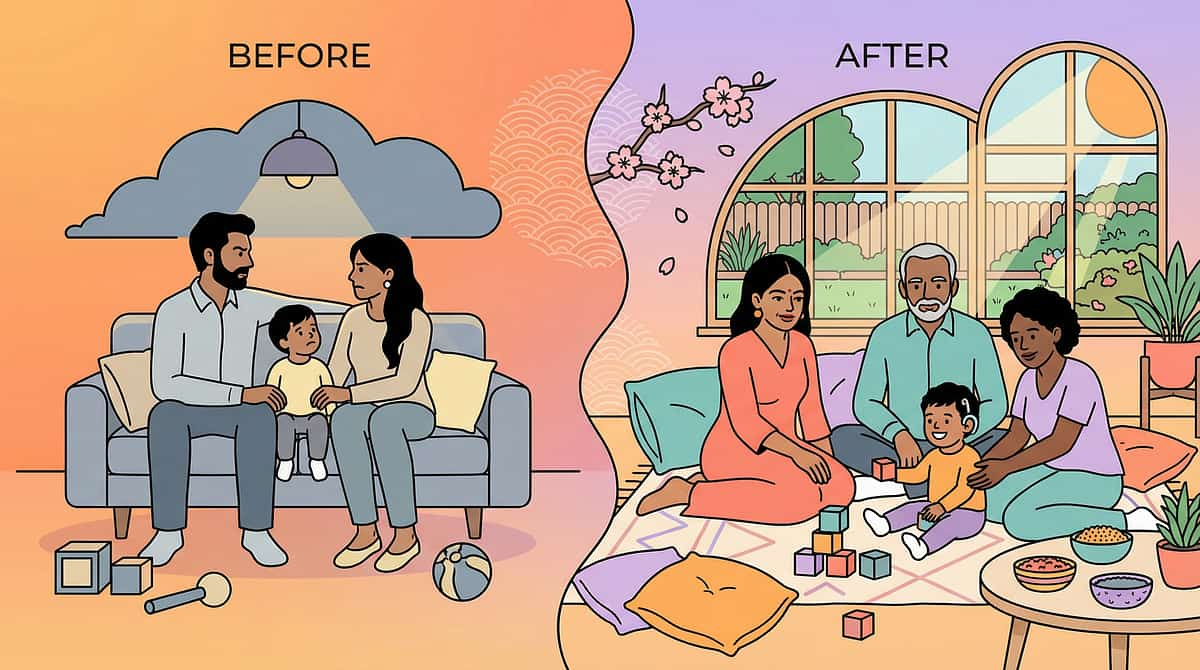
Before (Baseline)
- Child pounds dough flat — only available pattern
- Fatigues in under 2 minutes
- Hands you the dough: "you do it"
- Uses two hands for every single action
After 8 Weeks (Observable Gains)
- Rolls balls and snakes independently
- Uses cutters with minimal assistance
- Sustains play for 10+ minutes
- Attempts finger-isolation activities
Meta-analysis (PMC10955541): Sensory integration therapy promotes fine motor skills (primary), adaptive behavior (secondary), social skills (tertiary) across 24 studies.

Material 1: Therapy Putty / Graded Resistance Putty
Canon: Fine Motor / Hand Strengthening
Start Here
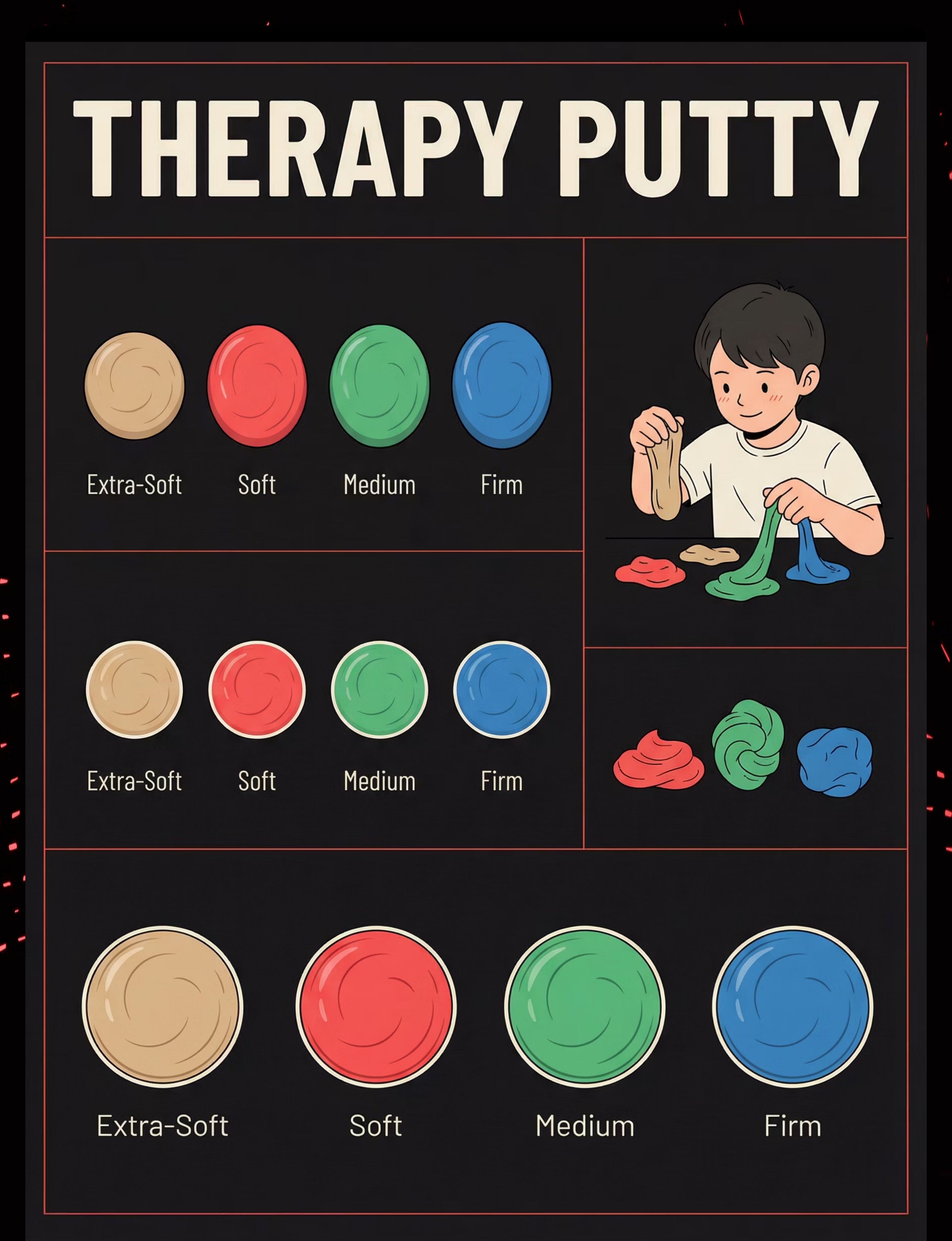
Therapy putty is the clinical gold standard for building grip strength and intrinsic hand muscle activation. Its precision-graded resistance levels — from Extra-Soft to Extra-Firm — allow you to match the exact challenge level to your child's current capacity, ensuring every squeeze is therapeutic without causing frustration or failure.
Extra-Soft (Tan/Yellow)
Entry level — for children who cannot squeeze standard playdough at all
Soft (Red)
Building phase — child can squeeze but fatigues within 2 minutes
Medium (Green)
Consolidation — child manipulates but lacks precision or endurance
Firm / Extra-Firm (Blue)
Mastery level — significant resistance for advanced hand strengthening
Price Range: ₹400–1,200 | 🔗Search Amazon.in: "therapy putty for children hand strengthening"
Pinnacle Recommends: Start at Extra-Soft or Soft for children who cannot squeeze standard playdough. Never begin with resistance that causes immediate failure.
Materials 2–5: Tools, Motivators, Guides & Extruders
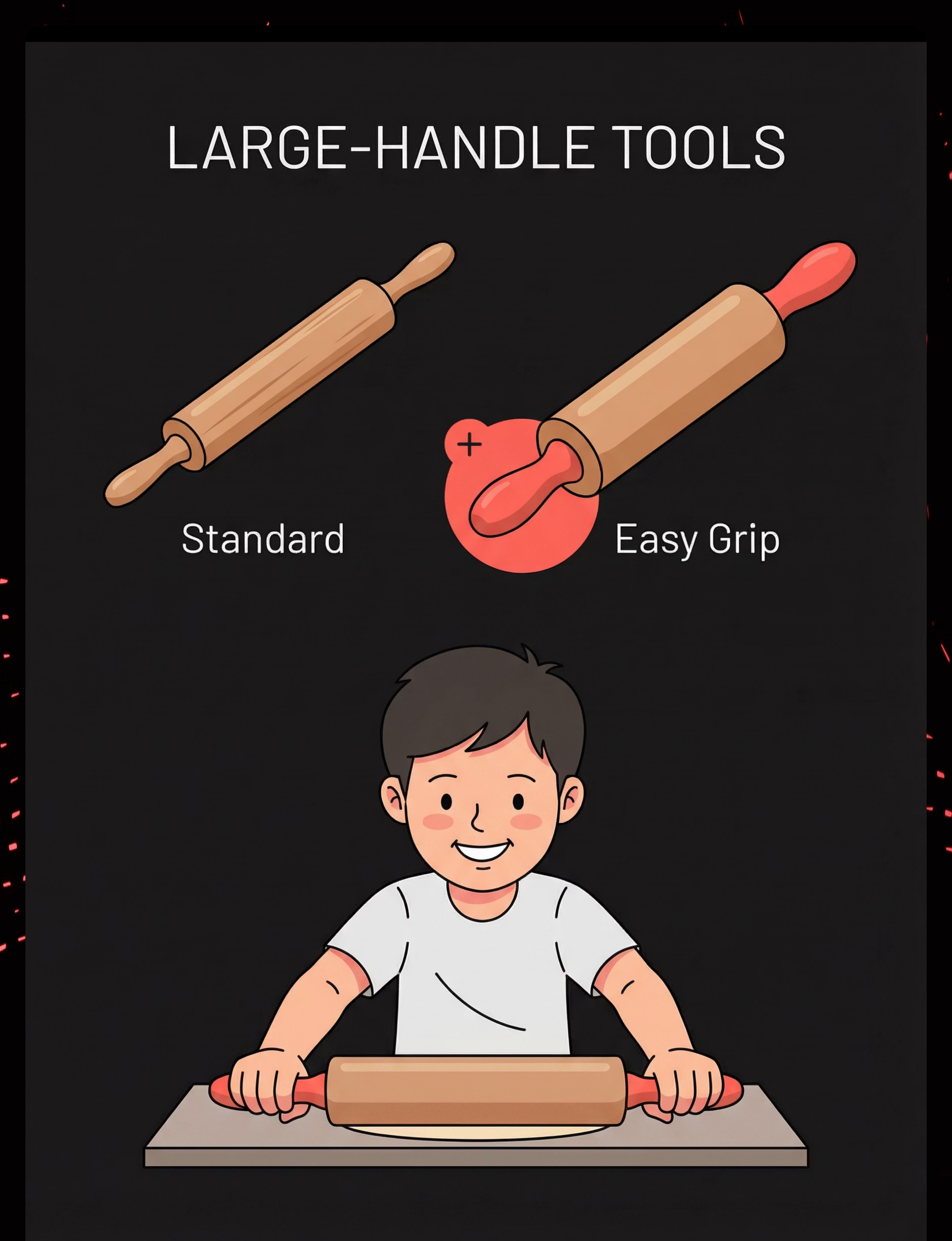
Material 2: Large-Handle Playdough Tools
Canon: Fine Motor Tools / Adaptive Grip · Price: ₹300–800
Chunky-grip rollers, wide-base cutters, and easy-press extruders. Handles should fill the child's palm — not require fingertip grip. This single design principle determines whether a tool builds strength or builds frustration.
Material 3: Hide-and-Find Objects
Canon: Fine Motor / Motivational Materials · Price: ₹100–400
Coins, small figurines, and large beads pressed into the putty become a treasure hunt — disguising hand strengthening as pure play. Every squeeze, dig, and pull is therapeutic action. Household items are entirely appropriate.
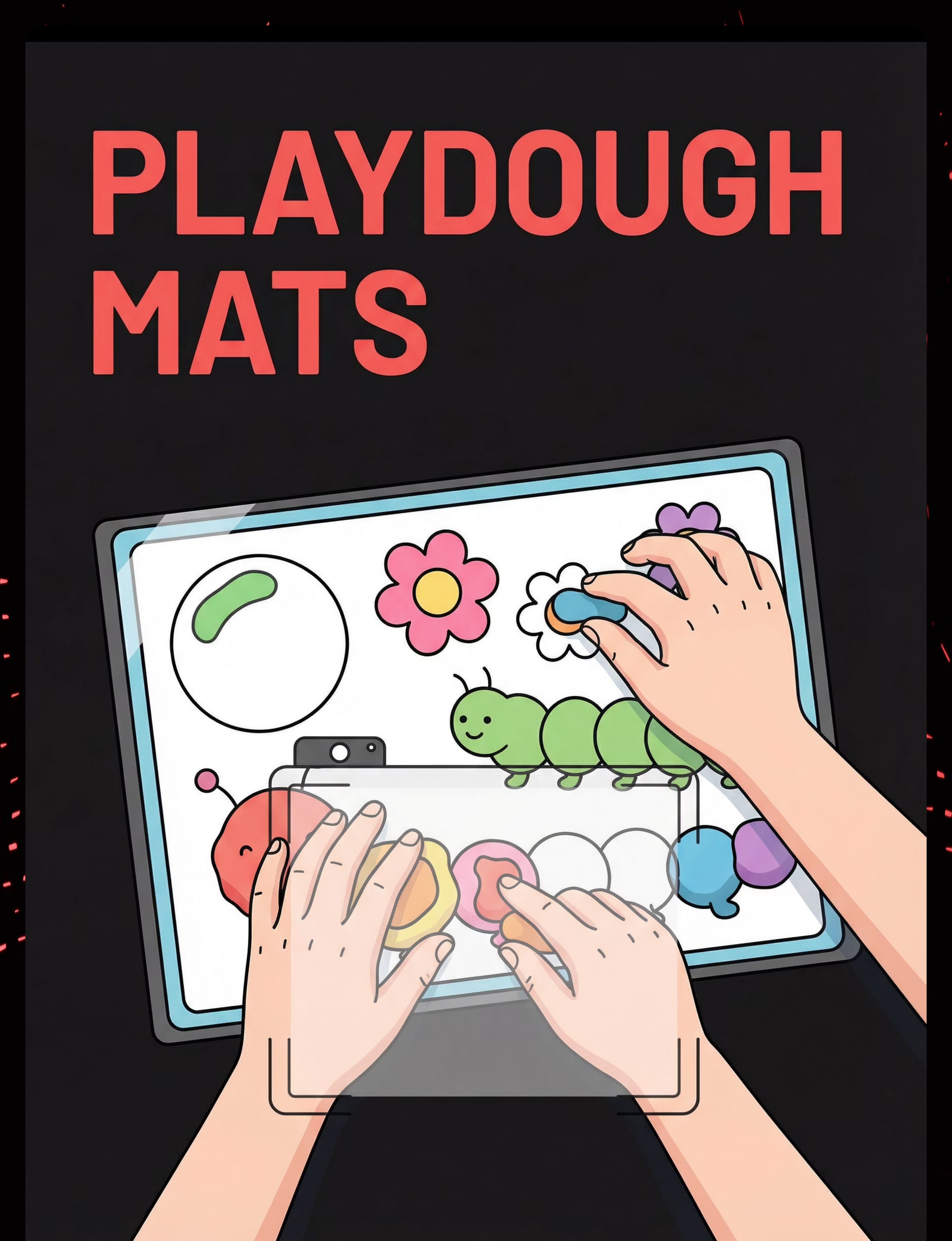
Material 4: Playdough Mats / Visual Guides
Canon: Visual Supports / Fine Motor Structure · Price: ₹200–600
Laminated A4/A5 mats with outlined shapes, characters, and letters give the child a clear visual goal. Free printable mats are available online — laminate at a local print shop for ₹10–20.
Material 5: Playdough Extruder / Press
Canon: Fine Motor Tools / Bilateral Press · Price: ₹200–700
The easy-press mechanism with multiple disc shapes builds bilateral hand strength dramatically. The dramatic visual output — spaghetti strands, star shapes — provides immediate, intrinsically motivating reward. Free alternative: garlic press from your kitchen.

Materials 6–9: Rolling, Texture, Isolation & Bilateral Games
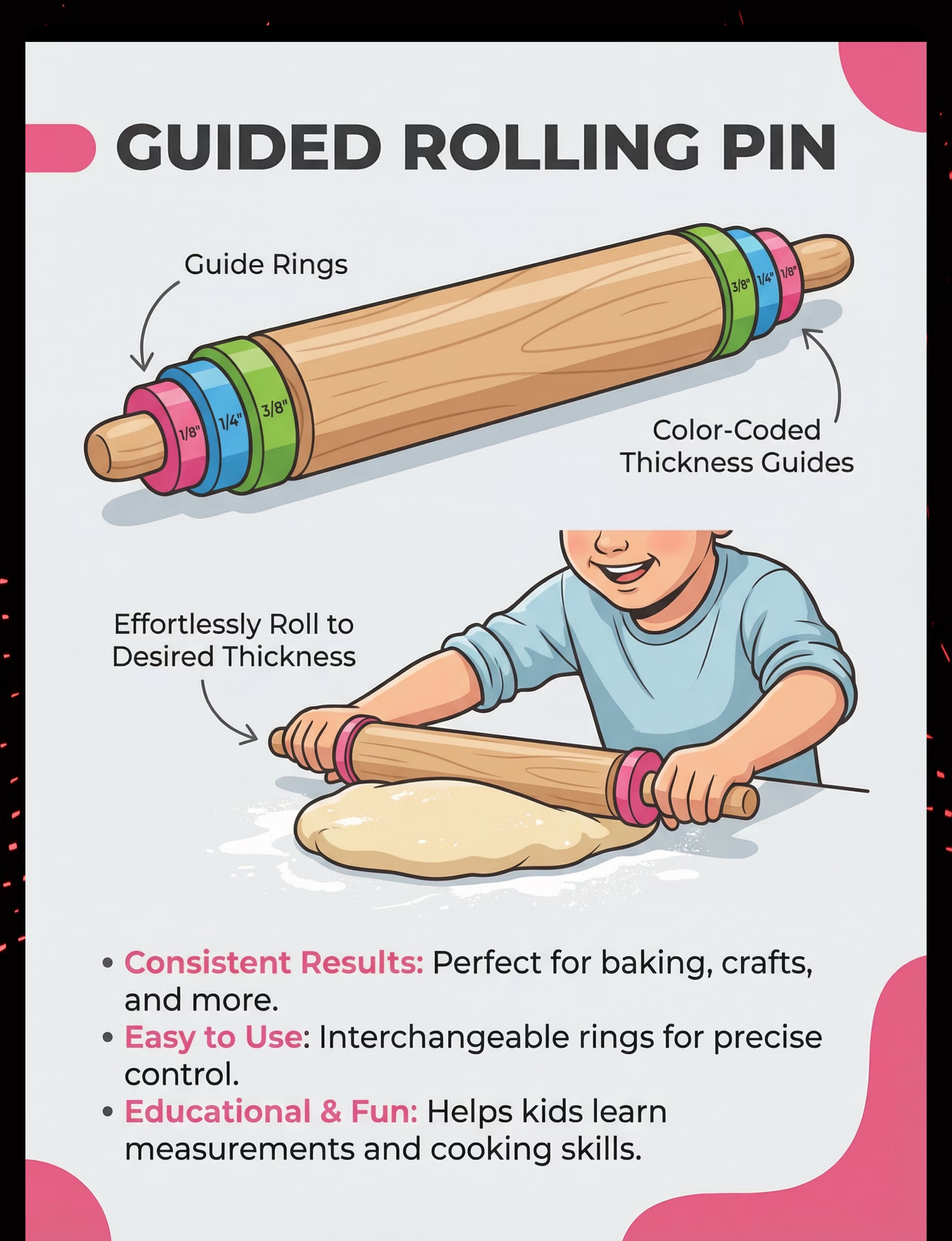
Material 6: Rolling Pin with Guide Rings
Canon: Fine Motor Tools / Pressure Control · Price: ₹300–800
Adjustable thickness guide rings (color-coded) remove the guesswork from pressure calibration, allowing the child to focus entirely on the bilateral rolling action. The pin rests on the guides when dough reaches the right thickness — immediate, satisfying feedback.
Material 7: Textured Materials / Loose Parts
Canon: Sensory / Manipulative Materials · Price: ₹100–500 (or ₹0)
Buttons, shells, googly eyes, pipe cleaners, pasta shapes, and beads create pressing, inserting, and combining demands that activate intrinsic hand muscles deeply. Fully sourceable from your kitchen, craft drawer, and nature walks.
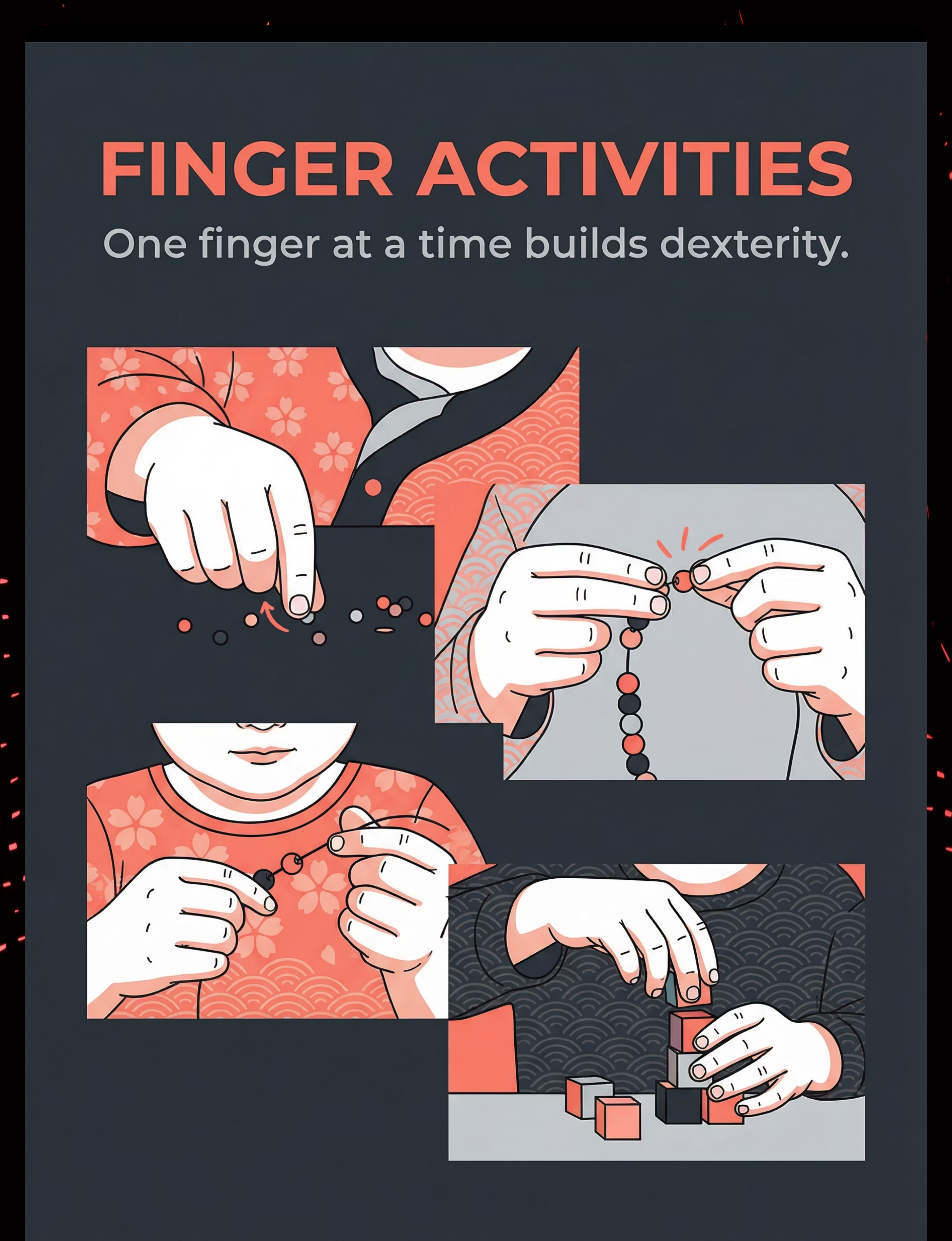
Material 8: Finger Isolation / Pinch Pot Setup
Canon: Fine Motor / Finger Dexterity · Price: ₹0–200
Activity-based — requires only playdough plus a structured activity sequence. No purchase required. Builds individual digit control and thumb isolation — the precise finger dexterity that underlies pencil grip and pincer grasp.
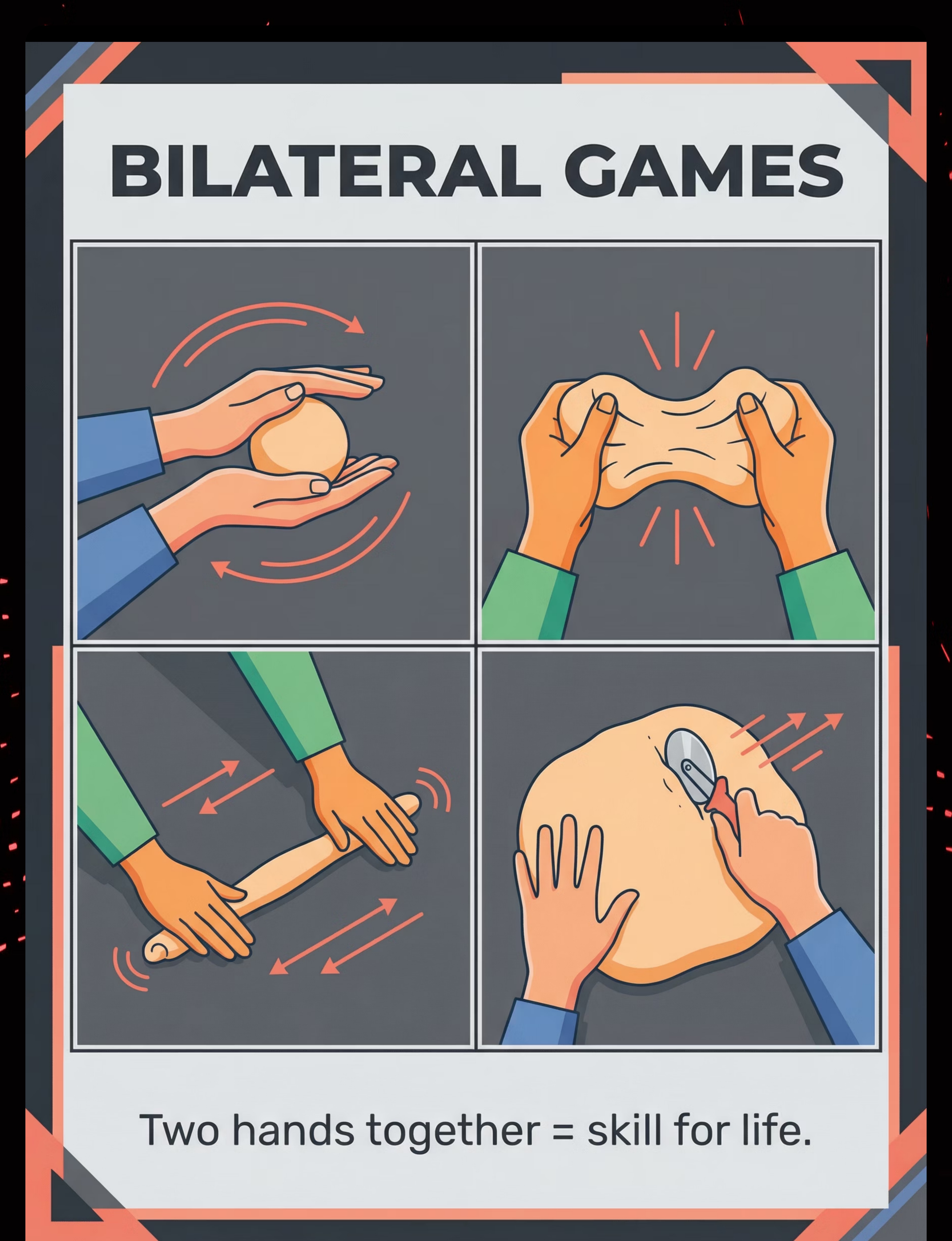
Material 9: Bilateral Coordination Games Setup
Canon: Bilateral Motor / Hand Coordination · Price: ₹0–200
Activity-based structured two-hand exercises using standard playdough. No additional purchase required. Builds the neurological bridge between hemispheres — the foundation for every functional two-hand task from handwriting to tying shoes.

DIY & Substitute Options — Every Family Can Start Today
WHO/UNICEF Equity Principle
Context-Specific · Accessible to All
Every family can execute this technique today — regardless of budget. The therapeutic principle is what matters, not the brand. WHO/UNICEF equity-focused interventions are designed to reach every family through context-specific adaptation.
Clinical Material | DIY / ₹0 Substitute | Why It Works | |
Therapy Putty (Extra-Soft) | Homemade playdough: 2 cups flour + 1 cup salt + ½ cup water + oil. For softer: more oil + less flour | Same resistance principle — adjust texture toward child's ability level | |
Graded Resistance Levels | Refrigerate (firmer) vs. microwave briefly (softer). Different flour ratios for batch variety | Temperature and formula control resistance just like commercial grading | |
Large-Handle Tools | Wrap foam pipe insulation around existing handles. Use large kitchen spoons, potato mashers | Diameter is the key variable — palm fill vs. fingertip grip | |
Playdough Mats | Print coloring pages, laminate. Draw outlines on laminated card | Visual guide principle identical — target shape is what matters | |
Extruder Press | Garlic press. Colander pressed into dough. Cup with hole-punched bottom | All create same extrusion motor pattern | |
Loose Parts | Kitchen: pasta shapes, straws, blunted toothpicks. Nature: leaves, shells, twigs, seeds | Same pressing, inserting, combining motor demands |
Important Caveat: When commercial therapy putty is non-negotiable — if your child requires precise resistance grading (hypotonia, severe low muscle tone) or has a latex allergy, clinical-grade putty is strongly preferred. Consult your Pinnacle OT. Free guidance: 9100 181 181
WHO NCF (2018): Emphasizes context-specific, equity-focused interventions. CCD Package implemented across 54 LMICs using household-material-based protocols. References: PMC9978394 | WHO NCF Handbook (2022)
Safety First — Before You Begin
Clinical precision in safety checks protects your child and ensures every session builds trust rather than eroding it. Run this full check before every session. It takes under 60 seconds.
🔴 DO NOT PROCEED
- Open cuts, wounds, or active skin infections on hands
- Severe latex allergy (check putty packaging)
- Acute illness (fever, respiratory distress)
- Post-meltdown dysregulation state
- Any material contains known allergens
🟡 MODIFY FIRST
- Hungry or overtired → Feed/rest first, shorten session
- Tactile defensiveness → Start with tools only, never force contact
- Previously rejected playdough → Use hide-and-find as entry point
- Hypotonia → Extra-Soft only, 3–5 minute sessions maximum
🟢 ALL CLEAR
- Child is fed, rested, regulated
- Materials are non-toxic, age-appropriate, non-allergenic
- Environment is prepared
- You have 15–20 uninterrupted minutes
STOP SESSION IMMEDIATELY if: Hands turn white or red (vascular response) · Child crying or rigid · Gagging or mouthing materials · Extreme hand pain complaints.
Helpline: 9100 181 181 — Free National Autism Helpline · 16+ languages · 24x7
Helpline: 9100 181 181 — Free National Autism Helpline · 16+ languages · 24x7
Indian Journal of Pediatrics RCT (2019): Home-based sensory-motor intervention safety protocols established for parent-administered sessions. Reference: DOI: 10.1007/s12098-018-2747-4

Set Up Your Space — The Therapeutic Environment
Environmental structure is a core principle of Sensory Integration intervention. How you arrange the physical space directly impacts your child's posture, attention, and fine motor output. This setup takes five minutes and makes every session more effective.
The Setup Checklist
- ☐ Child's feet flat on floor, hips at 90°, elbows at table height
- ☐ Non-slip silicone mat under work area
- ☐ Only today's 2–3 materials visible — not the whole collection
- ☐ Visual timer set to session duration (10–15 min)
- ☐ Reinforcement jar/sticker chart in child's line of sight
- ☐ All screens off — bilateral attention required
- ☐ You are seated beside the child, not across from them
Environment Details That Matter
Position: Sit beside your child — not opposite. This enables hand-over-hand assist without confrontational positioning and allows you to model actions naturally.
Lighting: Bright natural light preferred. Good lighting reduces visual strain during fine motor work.
Sound: Low-level background music acceptable. Avoid TV or high-stimulation audio. This activity requires bilateral attention.
Temperature: Room temperature. Cold hands reduce dexterity. Warm dough slightly if stored in a cool place.
Distractions: Screens off, loud toys away, pets out of the room for the session duration.
Sensory Integration Theory (Ayres): Environmental structure is a core principle of SI intervention. Meta-analysis confirms individually structured sessions are most effective. Reference: PMC10955541

Is Your Child Ready? — The Pre-Session Readiness Check
The best session is one that starts right. A 7-minute successful session builds more neural adaptation than a 20-minute forced one. This 60-second readiness check is the single highest-leverage thing you can do before every session.
Indicator | YES ✅ → Action | NO ❌ → Action | |
Fed in last 2 hours? | Proceed | Feed first (15 min) | |
Rested (not overtired)? | Proceed | Shorten session to 5 min | |
No recent meltdown (60+ min ago)? | Proceed | Postpone to tomorrow | |
Body calm (no running/spinning)? | Proceed | 5 min heavy work first (carry books, push chair) | |
No illness signs today? | Proceed | Postpone | |
Interested when shown materials? | Proceed | Use hide-and-find entry (highest motivation) | |
Hands clean and uninjured? | Proceed | Check and treat if needed |
🟢 5+ YES: Full Session
Proceed to Step 1 — The Invitation at full protocol
🟡 3–4 YES: Modified
Softest material only · Shorten to 7 min · High reinforcement rate
🔴 Under 3: Postpone
Alternative calming activity today. Try again tomorrow. No session.

Step 1 of 6 — The Invitation (30–60 Seconds)
Step 1
OT Principle: Pairing + Just-Right Challenge
The child's choice to approach the material is itself the first therapeutic success. Never present playdough as a demand. Present it as a discovery. The invitation is not about compliance — it is about building the motivating operation that makes everything that follows possible.
Parent Script (Exact Words)
"Hey, I found something special. Look what I have — want to see if there's a treasure hiding in here?"
For a child who previously rejected playdough:
"I hid something for you. Can you find it?" (Press a small figurine INTO the putty before showing child. Mystery = motivation.)
Body Language Guidance
- Kneel or sit to child's eye level — do not stand over them
- Hold material at child's eye level, not extending toward them
- Smile, relaxed, curious energy — not eager-expectant energy
- Child reaches → success. Child looks away → wait 5 seconds and re-present
If Child Resists
- "No" → Don't force. "OK, I'll leave it here. Let me know."
- Ignores → Play with it yourself, narrate: "Ooh, it's so squishy..."
- Walks away → Postpone. Use a preferred activity today.

Step 2 of 6 — The Engagement (1–3 Minutes)
Step 2
Match Material to Entry Point
Material introduction must match where the child actually is — not where you hope they are. Over-challenging the entry point is the single most common cause of session failure. When you match correctly, even one squeeze of putty becomes a genuine therapeutic win.
Never Succeeded With Playdough
Present Extra-Soft therapy putty. Say: "This one is super squishy — give it one squeeze and see what happens." If child squeezes, even slightly: IMMEDIATE specific praise — "Yes! You squeezed it! I felt it move!"
Can Squeeze But Struggles With Manipulation
Present Soft putty + hide-and-find setup. Say: "I think there's a dinosaur hiding in here. Can you find him?" All searching behavior — squeezing, digging, pulling — equals productive therapeutic action and deserves praise.
Can Manipulate But Fatigues Quickly
Present playdough mat. Say: "Can you make a circle for this caterpillar's body? Just one — right here." One achievable goal at a time. Celebrate each completion before introducing the next.
Reinforcement Schedule — Begin Now: First contact with material → Verbal praise · Any squeeze, pinch, or pull → Praise + possible sticker · 30 seconds of sustained engagement → Praise. Watch for avoidance cues (pulling back, "done," hands on lap) and immediately pivot to easier material.
PMC11506176: Structured material introduction with immediate reinforcement meets evidence-based criteria for sensory-motor intervention.
Step 3 of 6 — The Therapeutic Action (5–10 Minutes)
Step 3
Execute 2–3 Actions Per Session · Rotate
The core of every session. Execute 2–3 of these nine therapeutic actions, rotating across sessions to maintain novelty and comprehensively develop all target skills. The nine actions address every primary and secondary target identified in the clinical protocol.
Graded Resistance Squeezing
Ball of putty in dominant hand. "Squeeze as hard as you can." Then non-dominant. Target: 5–10 squeezes per hand. Progress resistance when no fatigue shows.
Hide-and-Find Treasure Hunt
Press 3–5 objects into putty. "Find all 5 dinosaurs!" Squeezing, pulling, digging — all therapeutic. Child doesn't know they're exercising.
Mat-Guided Creation
Place laminated mat. Assign one element. Verbal and hand-over-hand guidance for rolling. One success = one celebration.
Extruder Press (Bilateral Strength)
Load extruder. "Push it down hard — watch what comes out!" Both hands on extruder simultaneously. Dramatic visual output = immediate reward.
Guided Rolling (Bilateral Coordination)
Rolling pin with guides. "Roll it until the rings touch — flat as a pancake!" Both hands on pin simultaneously. Guide rings handle pressure calibration automatically.
Finger Poking and Isolation
Flat disc on mat. "Poke a hole with just your pointer finger." Progress to: pinky, ring finger, middle finger in sequence.
Pulling Apart (Bilateral Opposition)
"One hand here, one hand there — PULL!" Dough tear requires bilateral effort. Celebrate the tear. Repeat with firmer material progressively.
Loose Parts Construction
"Can you make a hedgehog? Press these sticks in for spines." Pressing, inserting, combining — all intrinsic muscle activation disguised as creation.
Pinch Pot Creation
"Push your thumb right in the middle — make a bowl." Thumb isolation. Progress: squeeze sides up, add texture detail with finger pokes.
PMC10955541: Core therapeutic action occupies 40–60% of effective session time. 40-minute clinic sessions → 10–20 minutes home equivalent.
Common Execution Errors — And How to Fix Them
Even experienced parents encounter these patterns. Recognizing them quickly — and knowing the clinical correction — turns a derailed session into a teaching moment for both of you.
Error Observed | Why It Happens | Clinical Correction | |
Child uses table to support rolling instead of palm | Insufficient intrinsic hand strength at current level | Place dough on silicone mat first; guide palms together under the dough | |
Both hands do the same action instead of coordinating | Bilateral development stage — one hemisphere leading | Give verbal label: "This hand HOLDS. This hand ROLLS." Repeat consistently. | |
Child immediately asks adult to do it for them | History of failure → learned helplessness → parent rescue as coping | Reduce resistance by one level. Hand-over-hand assist (your hands over theirs). Praise: "YOU did that — I just helped." | |
Session ends after 2 minutes due to fatigue | Intrinsic muscles working at maximum capacity — this is correct | End on success, not depletion. 5 good minutes beats 15 forced minutes. Build endurance session by session. |
Session Abandonment is Not Failure: "A terminated session is data. It tells you exactly what needs adjustment." Log it on your tracker (Step 6) and use it to calibrate tomorrow's session.

Step 4 of 6 — Repeat & Vary (3–5 Minutes)
Step 4
3 Good Reps > 10 Forced Reps. Always.
Sensory-motor skills build through consistent, motivated repetition — not exhaustion. A child who leaves the session wanting more will return tomorrow willing to do more. Satiation — the point where quality drops — is your signal to transition, not push harder.
Repetition Targets
Per action: 3–8 quality repetitions (not sets of 20)
Per session: 2–3 different actions from the nine
Golden Rule: 3 good reps > 10 forced reps. Always.
Satiation Indicators — Stop This Action When:
- Child looks away from material repeatedly
- Quality of manipulation decreases (less forceful)
- Child begins talking about something else
- Hands opening and dropping material
Variation Framework — Keep It Fresh
Same Material | Introduce Variation | |
Therapy putty squeezing | Switch dominant to non-dominant hand | |
Hide-and-find | Change hidden objects (coins → figurines → buttons) | |
Mat activity | Change mat theme (caterpillar → pizza → face) | |
Extruder | Change disc shape (circle → star → rectangle) | |
Rolling | Change guide thickness setting |
Sensory integration therapy dosage research: 2–3 sessions/week, 8–12 weeks is typical clinic protocol. Session-level: 3–8 quality repetitions per action optimizes neural pathway building.

Step 5 of 6 — Reinforce & Celebrate (Throughout Session)
Step 5
ABA Golden Rule: Within 3 Seconds · Specific · Enthusiastic
The timing and specificity of reinforcement determines what the brain encodes as worth repeating. "Good job" tells the brain nothing. "You squeezed that — your hands are getting so strong!" tells the brain exactly what skill to reinforce and consolidate.
"You SQUEEZED that! Your hands are getting so strong!"
"You found the dinosaur! You had to dig SO hard — I saw how hard you worked!"
"You rolled a SNAKE! Look at that snake you made with your own hands!"
"You used BOTH hands at the same time — that's exactly what strong hands do!"
Type | Example | Timing | |
Verbal praise | Specific script above | Within 3 seconds | |
Physical celebration | High five, shoulder squeeze | Immediately | |
Token economy | Sticker on chart | Per action completed | |
Reward Jar | Token to Rosette Reward Jar · ₹589 · Buy | End of session |
Celebrate the Attempt, Not Just the Success: If the child tries to squeeze and can't, praise the try: "You tried so hard — I saw your hands working!" Effort reinforcement sustains engagement through difficulty.

Step 6 of 6 — The Cool-Down (2–3 Minutes)
Step 6
End Every Session on a Win
Abrupt endings increase resistance to starting the next session. Predictable cool-down rituals regulate the nervous system, consolidate the session's emotional win, and build the habit architecture that makes daily practice sustainable.
If Child Resists Ending
Do NOT abruptly take material away. Say: "One more snake, then the dough goes to sleep in its box." Follow through once. Consistency prevents end-of-session battles from becoming habitual.
What to Avoid
- Abrupt endings → increases resistance to starting next session
- "Good job, now stop" → does not teach self-regulation
- Leaving materials out → reduces novelty of next session
NCAEP (2020): Visual supports and transition warnings are classified as evidence-based practices for autism. Predictable endings reduce post-session dysregulation.

Capture the Data — Right Now (Within 60 Seconds)
"60 seconds of data now saves hours of guessing later. When your OT asks 'what have you noticed?' — you will have the answer." Data collection is not extra work — it is the feedback loop that makes every session smarter than the last.
The 3-Field Tracker
Date: _______ · Material Used: _______ · Today's Best Moment: _______
Duration: ___ min · Start Mood: 😊😐😟 · End Mood: 😊😐😟
Resistance Level: Extra-Soft / Soft / Medium / Firm
Actions: ☐Squeeze ☐HideFind ☐Mat ☐Extruder ☐Roll ☐Poke ☐Pull ☐Loose ☐Pinch
Notable Observation: _______
Duration: ___ min · Start Mood: 😊😐😟 · End Mood: 😊😐😟
Resistance Level: Extra-Soft / Soft / Medium / Firm
Actions: ☐Squeeze ☐HideFind ☐Mat ☐Extruder ☐Roll ☐Poke ☐Pull ☐Loose ☐Pinch
Notable Observation: _______
Tracking Options
- 📱 GPT-OS® In-App Tracker: pinnacleblooms.org/gptos
- 🗓️ Simple paper chart — week grid, tally marks, mood faces
What the Data Reveals
- Which resistance level produces best engagement
- Which action sustains attention longest
- Mood pattern: frustrated start → satisfied end (neurological adaptation)
- When to increase resistance (3 sessions of no fatigue = time to progress)
ABA Data Collection Standards: Continuous measurement (frequency, duration) as standard behavioral practice. BACB Guidelines + Cooper, Heron & Heward (Applied Behavior Analysis, 8th ed.) · Helpline: 9100 181 181

What If It Didn't Go As Planned?
Most sessions don't go perfectly. That is completely normal — and completely workable. Each problem has a specific, clinically grounded fix. Your response in the difficult moment determines whether tomorrow's session is easier or harder.
Child refused to touch the material
Why: Resistance too high or texture aversive. Fix: Drop one resistance level. Hide an object first to introduce purpose before contact. Consistent refusal → consult OT re: tactile defensiveness protocol.
Child touched briefly, walked away after 2 minutes
Why: Fatigue (muscles working appropriately) or disengagement. Fix: 2-minute engagement is a WIN in early sessions. Celebrate it. Build to 5, then 10 minutes. Never extend by force.
Child only pounded and flattened — no other action
Why: Pounding is the one reliably achievable action at current strength level. Fix: This IS your baseline. Pounding IS the intervention today. Add hide-and-find to pounding to introduce new demand gradually.
Child became frustrated and cried
Why: Demand exceeded current capacity or poor antecedent conditions. Fix: End session with empathy. Reduce demand tomorrow. Check readiness indicators before starting next time.
Child asked me to do it for them every time
Why: History of failure → learned helplessness → parent rescue as coping. Fix: Reduce to softest resistance. Hand-over-hand assist — they are doing the work. Praise: "YOU did that, I just helped."
Ran out of ideas after 3 sessions
Why: Novelty is a natural motivator — it needs renewal. Fix: Rotate from the 9 materials systematically. New hidden objects, new mat theme, new extruder disc shape each session.

Adapt & Personalize — Matching the Protocol to Your Child
No two children arrive at the same difficulty for the same reason. Individualized adaptation is not optional — it is the core clinical principle. Use your child's sensory profile, diagnosis, and current ability level to select the right configuration.
🔴 Sensory Seeker
Seeks input, presses hard, loves heavy work. → Firm/Extra-Firm resistance. Deep pressure squeezing before fine manipulation. Bilateral pulling-apart with significant force. Heavy extruder pressing.
🔵 Sensory Avoider / Tactile Defensive
Avoids touching material. → Start with tools only. Introduce glove or barrier, then fingertip, then full hand — over days/weeks, not minutes. Never force exposure.
🟣 Autism / Predictability Needs
Same materials in same positions each session. Visual schedule showing today's sequence. Same verbal script each time. Changes introduced one at a time only.
🟡 Low Muscle Tone (Hypotonia)
Extra-Soft only. Supported seating (feet on floor, back supported). Very short sessions (3–5 min). Hand-over-hand for initial actions. Celebrate every micro-gain.
🟠 DCD (Developmental Coordination Disorder)
Visual guides (mats) essential. Break each action into verbal steps: "HOLD — SQUEEZE — TURN." Slow the pace. Model first, assist second, then independent.
🟢 Older Child (5–7 years)
Introduce functional goals: "Roll enough dough to make chapati." "Make letters from your name." Complexity and purpose accelerates motivation at this age.

Week 1–2: What to Expect — Foundation Laying
Progress: 15%
Foundation Laying Phase
Weeks 1–2 are NOT about beautiful creations. They are about the nervous system learning that playdough is safe, manageable, and worth engaging with. Progress at this stage is measured in seconds of tolerance and single successful squeezes — not in snakes and snowmen.
Observable Indicators You WILL See ✅
- Child tolerates material for 2–3 minutes (up from 30 seconds)
- Child accepts softer resistance without immediate refusal
- Child makes one or two successful squeezes independently
- Child stops asking you to "do it" as frequently
- Less frustration response when material "doesn't work"
What Is NOT Progress Yet (But Is Normal)
- Child still cannot roll a ball independently — normal
- Child still prefers pounding over fine manipulation — normal
- Sessions still end early — normal
- Child needs reinforcement for every action — normal
"If your child tolerates the material for 3 seconds longer than last week — that is measurable neural adaptation. That is real progress. The brain is changing. You can't see the wiring, but it is happening."
PMC11506176: Sensory integration intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation, not skill mastery.

Week 3–4: Consolidation — Pathways Forming
Progress: 40%
Consolidation Phase
The child begins to anticipate the activity. Neural pathways built in weeks 1–2 are now strengthening. What required maximum effort now requires moderate effort. This is neuroplasticity made visible — and the moment parents first start to feel genuine confidence.
Consolidation Indicators
- Child walks toward materials unprompted on some days ✅
- Session duration increases to 7–10 minutes ✅
- Rolling action produces a recognizable snake (not just a pancake) ✅
- Child uses one hand for holding while other works ✅
- Child asks "what are we making today?" (goal-directed engagement) ✅
Spontaneous Generalization
- Reaching for playdough during free play
- Applying squeezing action to other objects (stress balls, orange juice, bread dough)
- Using two hands together for containers, socks, pulling activities
When to Increase Resistance
If child completes 3 consecutive sessions with NO fatigue at current resistance level → move to next level. Progress resistance ONE level at a time. Never skip levels.
"You may notice you're more confident too. You know what to say. You know how to set up. You've built the habit. That parent confidence is itself a therapeutic variable — your child reads it."
Week 5–8: Mastery — Skill Emergence
Progress: 75%
Skill Emergence Phase
Mastery is specific, observable, and measurable. Use these criteria to determine when your child has genuinely consolidated F-609 skills — and is ready to advance to the next technique in the series.
Ball Rolling
Rolls a ball between palms independently × 3 trials without table support
Snake Rolling
Rolls a snake 10cm long without table support × 3 trials
Minutes Sustained
Sustains playdough play for 10+ minutes independently
Mastery Badge Unlock Criteria: F-609 MASTERED when child meets 4 of 6 mastery criteria across 3 consecutive sessions at Soft resistance.
Generalization Signs
- Improved pencil grip observed by teacher ✅
- Opens twist caps and containers more easily ✅
- Scissor use emerging or improving ✅
- Button/zipper attempts increasing ✅
Ready to Progress To
- F-610: Scissor Skills (bilateral + fine motor in functional task)
- F-611: Bead Stringing Challenges (precision + sustained grip)
- F-615: Pre-Writing Readiness (direct handwriting preparation)
PMC10955541 | BACB mastery criteria standards. Mastery defined as consistent, independent, generalized performance across contexts.
🏆 Celebrate This Win — You Did This
In the past 5–8 weeks, you set up a kitchen table as a therapeutic space, showed up through the frustrated sessions, learned to read your child's readiness, adapted when things didn't work, and kept going. The child who couldn't squeeze playdough can now roll a snake. That is not a small thing. That is neural architecture that will support handwriting, scissors, buttons, and independence for life.
"You provided structured, graded, repeated sensory-motor input during a critical neuroplasticity window. You literally built new connections in your child's brain. The research calls this 'activity-dependent synaptic strengthening.' You call it playdough time."
Family Celebration Suggestion
Make something with the playdough together today — something your child chooses. Let them lead. Watch what their hands can do now. Take a photo. Print it. Put it up.
Journal / Photo Prompt
"Today I noticed my child doing _____________ with their hands that they couldn't do 8 weeks ago. The look on their face was _____________."
Parental self-efficacy research: Parent confidence is the strongest predictor of continued home intervention. Celebration rituals reinforce the commitment cycle.

Red Flags — When to Pause and Seek Professional Input
Knowing when to pause is as important as knowing how to continue. These specific warning signs warrant prompt professional attention — not alarm, but action. Trust your instincts: you know your child.
Red Flag | What It Looks Like | Why It Matters | Action | |
Pain during hand activities | Child pulls back, guards hands, cries when squeezing | May indicate joint hypermobility or pain condition | Stop all resistance. Consult OT + pediatrician | |
No improvement after 8 weeks daily | Zero generalization, same resistance struggles | May indicate hypotonia, DCD, or neurological factor | Book AbilityScore® Assessment | |
Regression after improvement | Skills reverse without illness explanation | May signal broader developmental concern | Teleconsult within 1 week | |
Hand asymmetry | Child refuses one hand, tremor visible | Neurological screening warranted | Pediatrician consult within 2 weeks | |
Severe tactile defensiveness | Full avoidance after 4+ weeks of graduated exposure | Sensory processing disorder requiring specialized SI therapy | OT sensory processing assessment |
01
Observe → Self-resolves in 3–4 days
Continue protocol with noted modification
02
Persists more than 1 week → Teleconsult
Call 9100 181 181 — Free · 16+ languages · 24x7
03
Significant red flag → Clinic Visit
Book AbilityScore® at nearest Pinnacle center: pinnacleblooms.org/centers
The Progression Pathway — Where You Go From Here
F-609 sits within a carefully architected developmental sequence. Knowing where you came from and where you're going helps you see each technique as one step in a coherent journey toward full fine motor independence.
Lateral Alternatives
If this approach didn't resonate with your child:
- F-620: Kinetic Sand Manipulation (similar motor demands, different texture)
- F-622: Wet Sponge Squeeze Protocol (resistive hand activities)
Long-Term Developmental Goals
- Functional Handwriting Readiness
- Self-Care Independence (buttons, zips, cutlery)
- Academic Tool Use (scissors, rulers, glue)
- Instrument and tool competency
WHO/UNICEF milestones framework + Pinnacle developmental cascade architecture across Domain F: Fine Motor.
Related Techniques in the Fine Motor Domain
With your F-609 materials — therapy putty, loose parts, mats, bilateral games — you can immediately begin F-607, F-608, and most of F-611. The investment you've made in materials serves multiple techniques across the domain.
Code | Technique | Level | Shared Materials | |
F-607 | Weak Grip Strength | 🟡 Intro | Therapy Putty | |
F-608 | Trouble with Pincer Grasp | 🟡 Intro | Therapy Putty, Loose Parts | |
F-609 | Playdough Manipulation ← YOU | 🟡 Core | All 9 Materials | |
F-610 | Scissor Skills | 🟠 Core+ | Bilateral setup, Mat guides | |
F-611 | Bead Stringing Challenges | 🟠 Core+ | Loose parts, Bilateral | |
F-615 | Pre-Writing Readiness | 🔴 Advanced | Mat guides, Rolling pin |
You Already Own Materials For These: With your F-609 kit, you can immediately begin F-607, F-608, and most of F-611. Browse the full domain: View All Fine Motor Techniques →
Your Child's Full Developmental Map
Fine motor is one of twelve developmental domains tracked by the Pinnacle GPT-OS® system. But notice how deeply it connects to the others: fine motor delay creates ripples across behavior, emotional regulation, communication, feeding, and academic readiness simultaneously.
Domain F Connects Directly To:
- D: Behavior — frustration regulation during tasks
- C: Emotional Regulation — achievement and self-efficacy
- B: Communication — writing, drawing expression
- J: Feeding — spoon, fork, cup use
The GPT-OS® Perspective
"This technique is one piece of a larger, personalized developmental plan. Your child's AbilityScore® maps progress across all 12 domains simultaneously."
📞 Book AbilityScore® Assessment: 9100 181 181
WHO NCF: Five components of nurturing care require holistic developmental monitoring. UNICEF 2025 indicators: 42 developmental metrics per country. References: WHO NCF (2018) | UNICEF 2025 Country Profiles
Families Who've Been Here — Real Stories
These outcome patterns represent the real journeys of families across Pinnacle's 70+ centers. Names are changed for privacy. Individual results vary. Every story here began exactly where you are now.
Rohan, Age 4 — Hyderabad
Before: Couldn't squeeze standard playdough at all. Hands so weak he could only pound flat. Preschool teacher flagged handwriting readiness. Playdough time always ended in crying — his and hers.
After Week 8: Rolling snakes and balls independently. Using cookie cutters with minimal assistance. Teacher reported improved pencil grip. Rohan now asks for playdough by name.
"The moment he rolled his first snake by himself — he looked at his own hands like he couldn't believe it. We both cried happy tears."
Timeline: Daily 10-minute sessions × 8 weeks. Extra-Soft → Soft → Medium progression.
Aanya, Age 3.5 — Bangalore
Before: Tactile defensive — wouldn't touch playdough at all. Would leave the room if playdough appeared on the table.
After Week 12: Using tools (not bare hands yet) to manipulate dough. Tolerates 8 minutes of tool-mediated activity. Beginning to touch dough with fingertip for hide-and-find games.
"We didn't rush the touching. We started with just looking. Then tools. Now she touches sometimes. The therapist said not to rush it — she was right."
Dev, Age 6 — Chennai (DCD Diagnosis)
Before: Could not coordinate two hands — would use one while the other hung at his side. Teacher frustrated with handwriting attempts.
After Week 10: Bilateral snake rolling mastered. Using rolling pin with both hands. Handwriting: improved grip pattern, beginning to form letters. School OT confirmed progress.
"Dev's core challenge was bilateral sequencing — the motor plan for 'left holds, right rolls.' Once we built that through playdough, the pencil transfer happened naturally." — Therapist's Notes
Cases are illustrative composites representing real outcome patterns. Individual results vary. · Helpline: 9100 181 181 · Free · 24x7

Connect With Other Parents
Intervention adherence is significantly higher when parents are embedded in a community of families navigating the same challenges. You don't have to figure this out alone — and you shouldn't.
Fine Motor Parent Community (WhatsApp)
Parents of children working on playdough manipulation, scissor skills, and handwriting readiness — sharing daily wins and real questions.
Pinnacle Parent Forum
Moderated by Pinnacle OTs. Question-answer, material sharing, progress celebrations. A safe, expert-backed space.
Local Parent Meetups
Find your nearest Pinnacle center's parent group for in-person connection with families in your city.
Peer Mentoring
"Connect with a parent who was exactly where you are 3 months ago." Your story is someone else's hope.
WHO NCF: Over 1,000 individuals from 111 countries contributed to the framework. Community engagement improves intervention outcomes. Parent networks: evidence-based adherence support.

Your Professional Support Team
Home practice and professional support are not alternatives — they are multipliers. Daily home sessions combined with weekly clinic sessions produce significantly better outcomes than either modality alone. Here's your full professional support map.
Specialist | Role With F-609 | How to Access | |
Pediatric OT | Hand function assessment, resistance grading prescription, therapy putty selection | Nearest Pinnacle center or teleconsult | |
BCBA/ABA | Reinforcement system design, session structure, engagement protocols | Via FusionModule™ at Pinnacle | |
NeuroDev Pediatrics | Developmental screening, muscle tone assessment, underlying condition identification | Via Pinnacle clinical team | |
SpEd Specialist | Pre-writing readiness assessment, school accommodation planning | Via Pinnacle education team |
📍 Center Locator
💻 Teleconsultation
For families more than 50km from a center: Book Teleconsult → or call 9100 181 181
📞 FREE Helpline
9100 181 181 · 16+ languages · 24x7 · Zero cost · Available from 70+ countries
WHO NCF Progress Report (2023): 48% increase in countries adopting ECD policies. Primary health care as key platform for reaching families with ECD interventions.
The Research Library — Evidence Foundation for F-609
Every technique in the Pinnacle 128 Canon is grounded in peer-reviewed evidence. F-609 draws from five converging streams of research — from systematic reviews to WHO/UNICEF frameworks — all pointing to the same conclusion: graded sensory-motor intervention works.
PMC11506176 (Children, 2024)
16 studies confirm sensory-motor integration intervention is evidence-based practice for fine motor development in children with ASD.
PMC10955541 (World J Clin Cases, 2024)
Meta-analysis of 24 studies demonstrates SI therapy promotes fine motor, gross motor, adaptive behavior, and social skills.
DOI: 10.1007/s12098-018-2747-4 (Indian J Pediatr, 2019)
Indian RCT validates parent-administered home-based sensory-motor protocols with significant outcome measures.
DOI: 10.3389/fnint.2020.556660 (Frontiers, 2020)
Establishes neurological basis: somatosensory cortex processing as the core mechanism in fine motor development differences.
How GPT-OS® Uses Your Session Data
Every session you log makes the system smarter for the next family navigating this exact challenge. You are not just helping your child — you are contributing to the world's largest pediatric intervention knowledge base.
What GPT-OS® Learns From Your F-609 Data
- Which resistance level produced best engagement by developmental age
- Which material sequence produces fastest bilateral coordination gains
- Which reinforcement schedule produces highest session adherence
- Predictors of readiness to advance to F-610 (Scissor Skills)
Privacy Assurance
All data is anonymized, aggregated, and stored under ISO 27001 standards. No individual child data is identifiable in population analysis. DPDP Act (India) compliant. Parent consent obtained at registration.
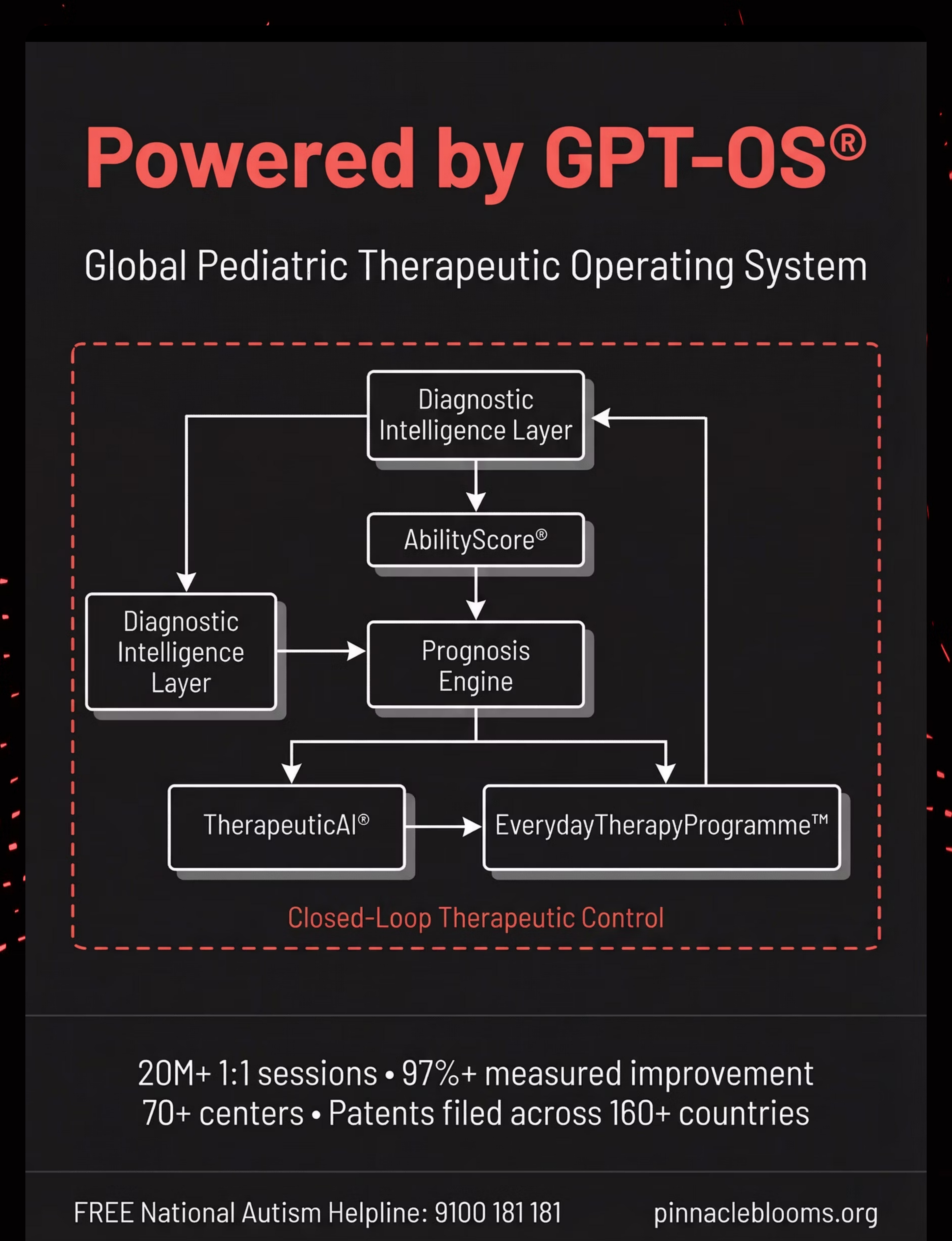
GPT-OS® Key Statistics
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centers · Patents filed across 160+ countries
Frequently Asked Questions
The most common questions parents ask after reading F-609 — answered with clinical precision and the warmth you deserve.
How long before I see results?
Most families see increased engagement and reduced resistance within 1–2 weeks of daily practice. Measurable skill gains (rolling, pinching) typically emerge at weeks 3–5. Full mastery: 8–12 weeks of consistent daily sessions. Consistency (daily, even 10 min) matters far more than duration.
My child is 7 — is it too late to start?
No. Fine motor skills respond to targeted input across the developmental window. At age 7, goals shift toward functional readiness (handwriting, scissors) rather than foundational strength, but the materials and protocol remain highly effective.
Do I need therapy putty or can I use regular playdough?
For children with significant weakness or frustration with standard playdough — therapy putty's precision grading is clinically preferred. For children with mild challenges, well-made homemade playdough (varying flour ratios) can be an effective start. See Card 12 for recipes.
My child hates the texture. Do I force it?
Never force direct contact. Start with tools only. Gradual, voluntary exposure — over days, not minutes — is the evidence-based approach. See the Sensory Avoider protocol in Card 25.
How do I know which resistance level to start with?
Simple test: if child cannot make an impression with one-handed squeeze → Extra-Soft. If child can squeeze but fatigues in 2 min → Soft. If child can manipulate but lacks precision → Medium.
Can I do this alongside clinic therapy?
Absolutely — and you should. Home daily sessions + clinic weekly sessions produce significantly better outcomes than clinic alone. Share your tracking data with your OT at each session.
My child is autistic — are there specific considerations?
Yes. Predictable structure is essential: same materials, same positions, same sequence, same verbal scripts each session. Changes introduced one at a time. Use special interests to motivate (hide their favorite characters). See Card 25 for full autism profile variation.
When should I stop and seek professional evaluation?
See Card 30 (Red Flags) for specific criteria. In general: if no improvement after 8 weeks of consistent daily practice, or if other fine motor areas are also significantly delayed. Free consultation: 9100 181 181
Preview of 9 materials that help with playdough manipulation Therapy Material
Below is a visual preview of 9 materials that help with playdough manipulation therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

Your Next Step — Start Today
You have read the science, learned the steps, understood the safety checks, and seen the stories of families who started exactly where you are. The technique is proven. The materials are accessible. The time is now. Every day of consistent practice is a day of neural pathway building.
🚀 Start This Technique Today
Launch the full F-609 GPT-OS® Session Guide and begin your child's first session with clinical support built in.
📞 Book a Consultation
FREE National Autism Helpline: 9100 181 181
16+ languages · 24x7 · No appointment needed
16+ languages · 24x7 · No appointment needed
🗺️ Explore the Next Technique
F-610: Scissor Skills — Building on Your F-609 Foundations. You already have the materials. You already have the habit.
Pinnacle Blooms Consortium · The Promise
"From fear to mastery. One technique at a time." Transforming every home into a proven, scientific, 24x7, personalized, multi-sensory, multi-disciplinary pediatric therapy center — powered by GPT-OS®, built by the world's largest consortium of pediatric therapeutic expertise.
Validated By
✅ OT · SLP · ABA/BCBA · SpEd · NeuroDev Pediatrics · CRO
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centers · Patents filed across 160+ countries
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centers · Patents filed across 160+ countries
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention from licensed occupational therapists or developmental specialists. Persistent fine motor challenges may indicate underlying conditions requiring professional evaluation. Individual results vary. If you have concerns about your child's development, please consult a qualified healthcare professional or contact our FREE National Autism Helpline: 9100 181 181.
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, FusionModule™ are registered trademarks/proprietary marks of Bharath Healthcare Laboratories Pvt. Ltd.
Site: techniques.pinnacleblooms.org · pinnacleblooms.org · care@pinnacleblooms.org · FREE National Autism Helpline: 9100 181 181
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, FusionModule™ are registered trademarks/proprietary marks of Bharath Healthcare Laboratories Pvt. Ltd.
Site: techniques.pinnacleblooms.org · pinnacleblooms.org · care@pinnacleblooms.org · FREE National Autism Helpline: 9100 181 181