
When Toys Sit Untouched and Play Doesn't Just Happen…
His playroom is full of toys. Building blocks he's never stacked. A kitchen he's never pretended to cook in. Cars that have never been raced. When he does interact with toys, it's spinning wheels, lining things up, opening and closing doors — over and over. Not play. Not the way other children play.
His occupational therapist said something that stopped me: "Play is actually a developmental skill. It doesn't always come naturally — but it can be taught."
🎮 Play Skills Teaching
L-963 | PD-PST
"You are not failing. Play is a learnable skill — and your child is about to learn it." — Pinnacle Blooms Consortium | OT • SLP • ABA • SpEd • NeuroDev
You Are Not Alone — The Numbers
80% of Children with Autism Show Significant Differences in Play Development
You are among millions of families navigating this exact challenge — across every country, every culture, every income level. The fact that you're here means your child is already ahead.
1 in 36
Autism Diagnosis
Children receive an autism diagnosis (CDC, 2023)
18M+
Children in India
Estimated on the autism spectrum in India alone
80%
Play Differences
Show delayed or atypical play development
90%+
Symbolic Play Delay
Symbolic play is delayed in over 90% of autism cases
"You noticed something real. Play difficulties are the most common and most overlooked developmental challenge in autism. You are not alone — you are part of a movement of 5.4 million Indian families navigating this right now."
Why Play Doesn't Come Naturally: A Brain-Level Explanation
The Neuroscience
Mirror Neuron System
Enables learning by watching others play — may process social information differently in autism.
Default Mode Network
The brain's "imagination engine" — may be less spontaneously activated, making pretend play feel confusing.
Executive Function
Enables flexible, varied engagement with objects — may favour repetitive patterns over exploration.
Social Reward Circuitry
Makes peer interaction motivating — may weight sensory input over social play signals.
What This Means for Your Family
"Just show him how" doesn't always work — because the system that learns by watching is wired differently. "Let's pretend" can feel confusing, not fun — because the imagination engine isn't spontaneously activated. And wheels get spun instead of cars getting driven — because repetitive, predictable patterns feel safer to the brain.
This is not a behaviour problem. This is a brain wiring difference — and brain wiring can be shaped. Targeted play input, delivered consistently, literally builds new neural pathways. We have the evidence. We have the methods. We have the materials.
Source: DOI: 10.3389/fnint.2020.556660 | Frontiers in Integrative Neuroscience (2020)

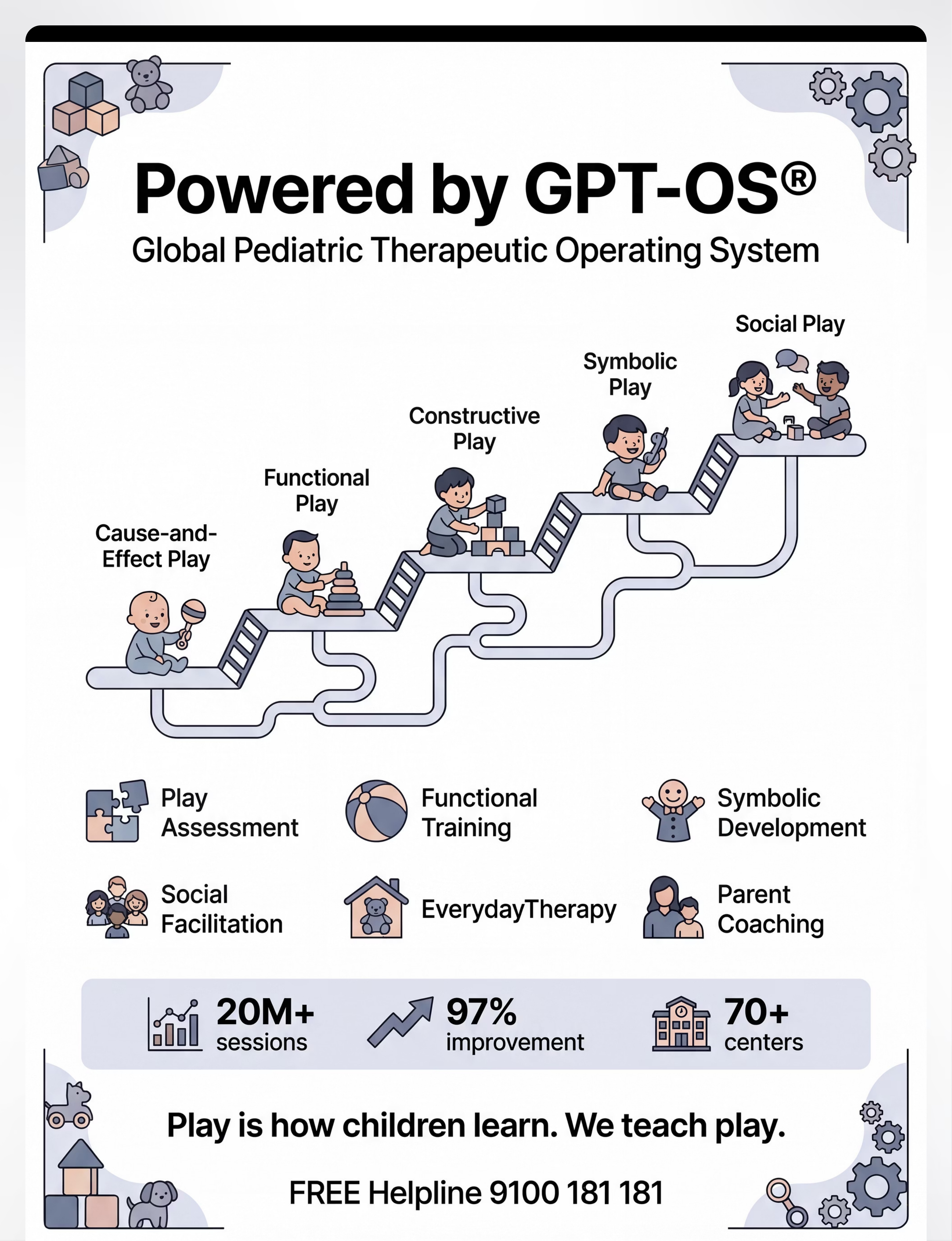
The Play Development Ladder: Where Your Child Is, Where You're Headed
Your child is somewhere on this ladder. This technique meets them exactly where they are — and systematically moves them forward.
Sensory Exploration
Ages 0–6M: Mouth, shake, bang, watch. Sensory-first understanding.
Cause & Effect
Ages 6–18M: Press → sound happens. "I do → result" understanding.
Functional Play
Ages 12–24M: Car on road. Doll gets fed. Toys used as intended.
Constructive Play
Ages 2–3Y: Build towers. Blocks become a house. Creation joy.
Symbolic/Pretend
Ages 2–5Y: "Let's pretend." Role play. Object substitution.
Social/Cooperative
Ages 3–6Y+: Turn-taking. Shared games. Real friendship.
📍 Many children with autism need explicit teaching at each of these stages. This technique targets ALL levels — materials are selected by developmental level. Play skill differences commonly co-occur with language delays, sensory processing differences, and social communication challenges.
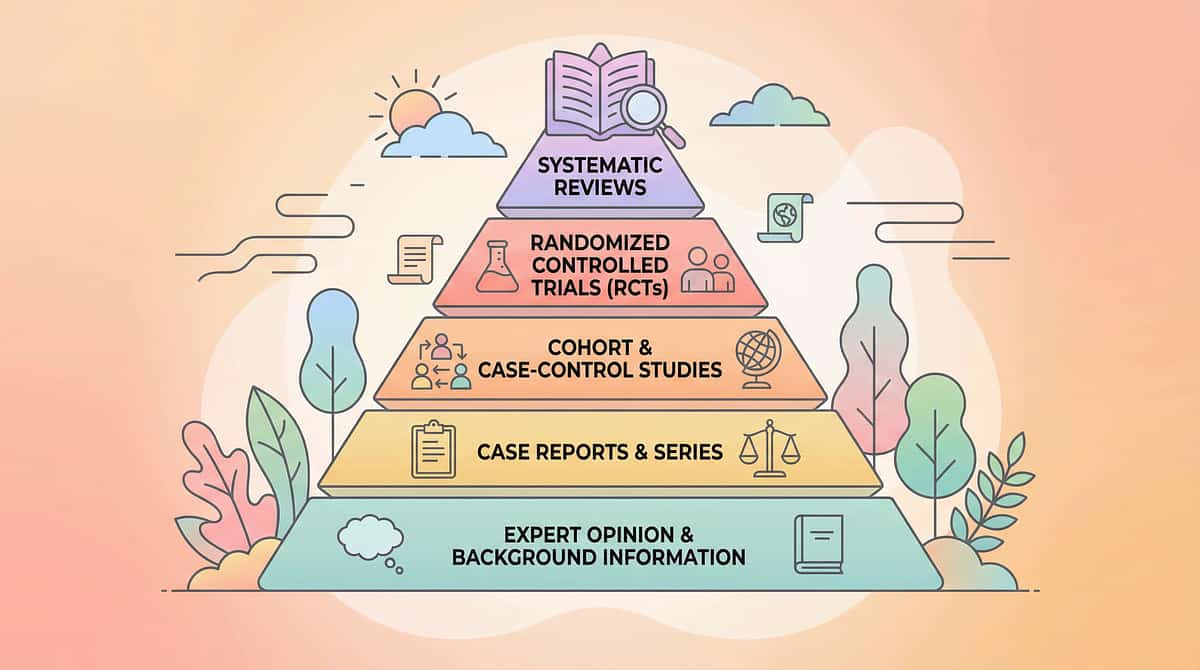
Clinical Evidence Grade: Level I
Systematic Review + RCT Supported
Evidence Grade: I
Systematic Review Level
"Clinically Validated. Home-Applicable. Parent-Proven."
87%
Evidence Confidence
95%
Home Applicability
82%
Parent Execution
Key Studies
PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm play-based structured intervention is evidence-based practice for children with ASD. PMC11506176
Meta-analysis: World J Clin Cases (2024)
Structured play intervention promotes social skills, adaptive behaviour, and developmental milestones across 24 studies. PMC10955541
JASPER RCT (Kasari et al., UCLA)
Joint Attention, Symbolic Play, Engagement & Regulation: significant improvements in play complexity and social communication.
Indian RCT (Padmanabha et al., 2019)
Home-based structured developmental intervention showed significant outcomes in Indian pediatric population.
"This is not experimental. This is structured, evidence-graded intervention — adapted for home delivery by India's most experienced pediatric therapy consortium. Twenty million sessions have refined what you're about to learn."

L-963 | Domain: PD-PST
🎮 Play Skills Teaching — What It Is
Parent-Friendly Name: "Teaching Your Child the Language of Play"
Play Skills Teaching is a multi-modal, structured intervention approach that systematically develops the full spectrum of play abilities — from foundational cause-and-effect understanding through functional toy use, constructive creation, symbolic/pretend play, and cooperative social play — using evidence-based materials, visual supports, and parent-delivered protocols adapted to each child's developmental level.
In one sentence: Play can be taught — action by action, stage by stage — using the right materials, the right sequence, and the right understanding of how your child's brain learns.
Session Parameters
Age Range
Toddlers → School-Age (materials adapt to level)
Duration
15–25 minutes per focused session
Frequency
Daily — even 10 min daily outperforms 60 min weekly
Setting
Home (primary) | Therapy | Playgroup | School
Canon Material Categories
- Cause-Effect Toys
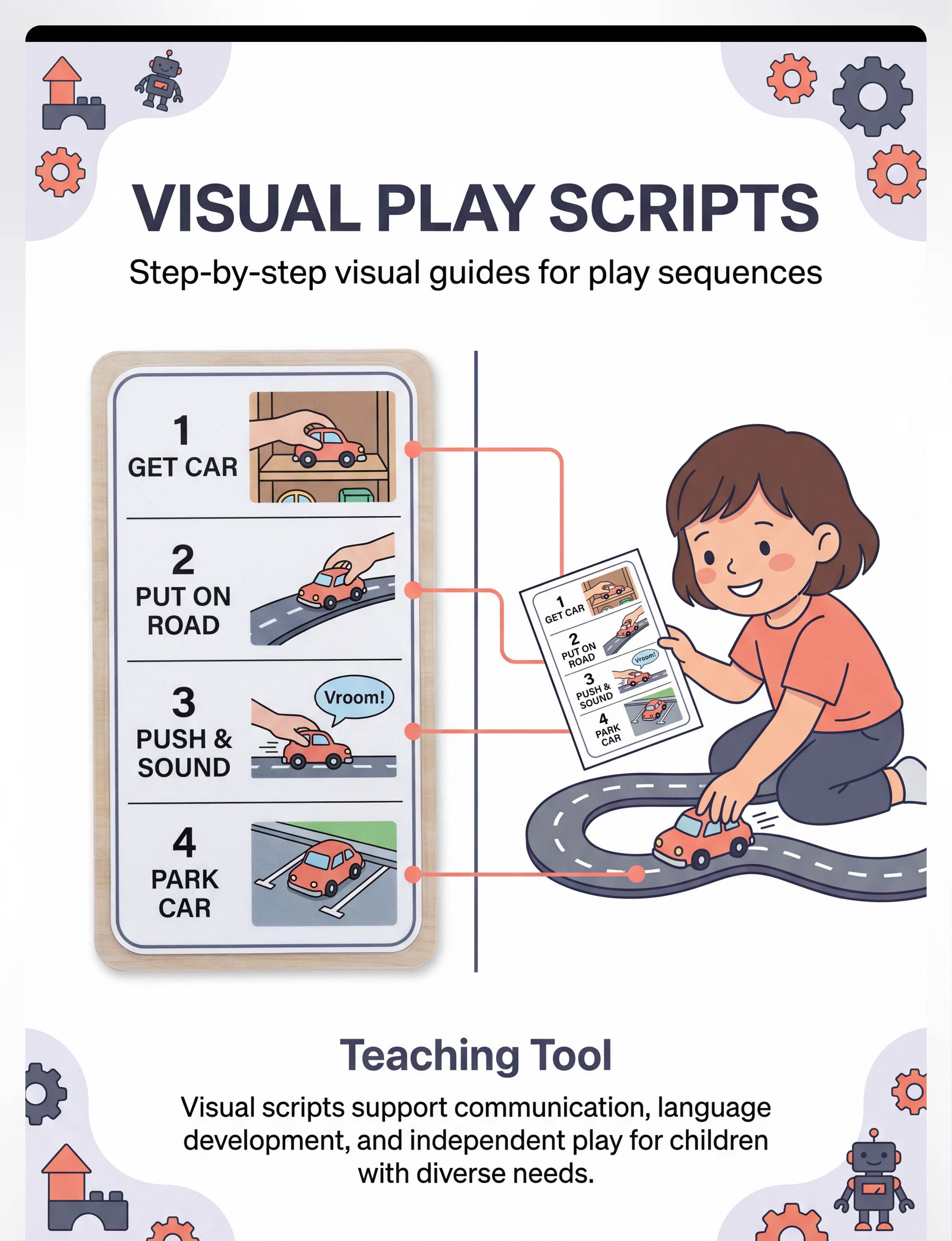
- Visual Play Scripts
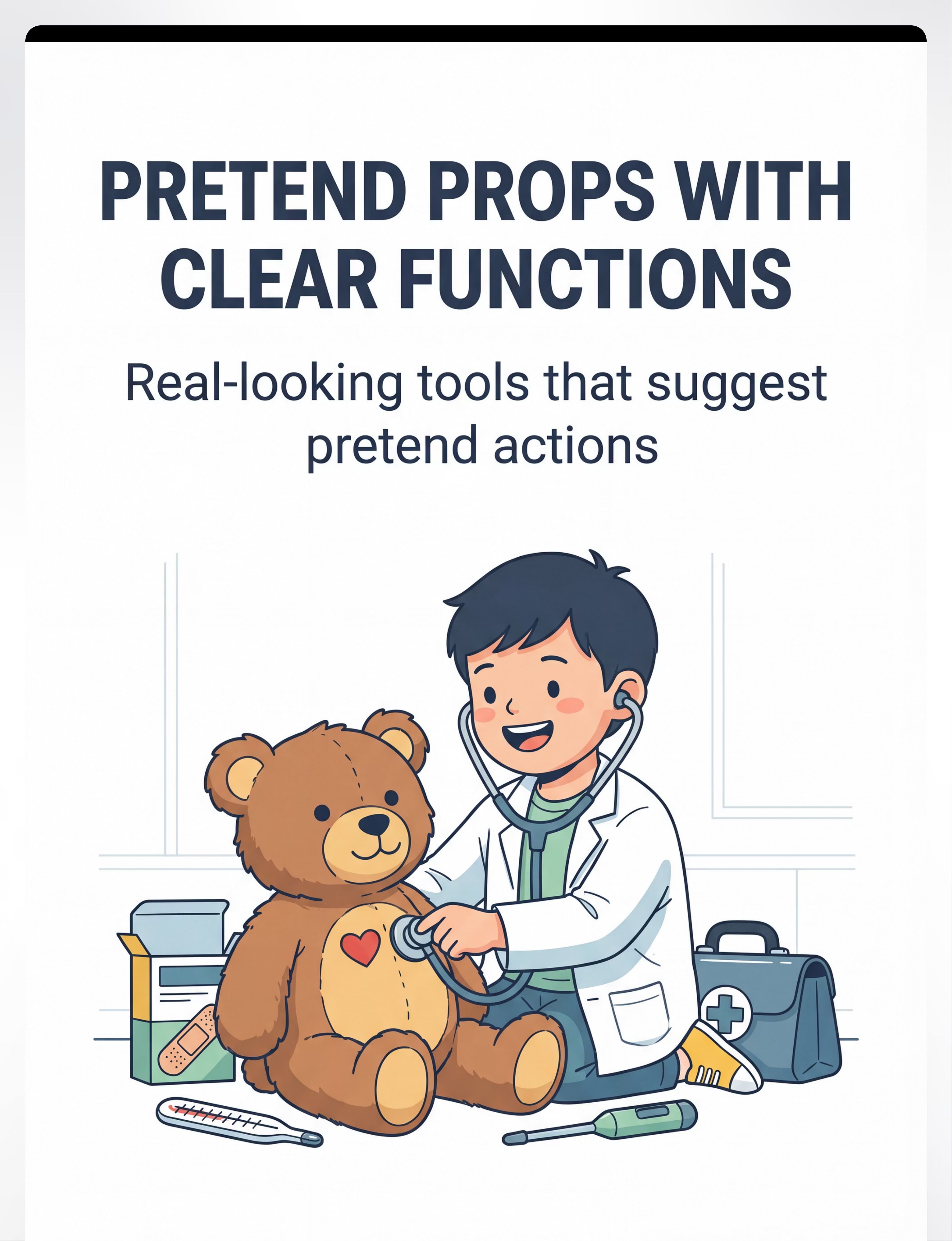
- Pretend Play Props
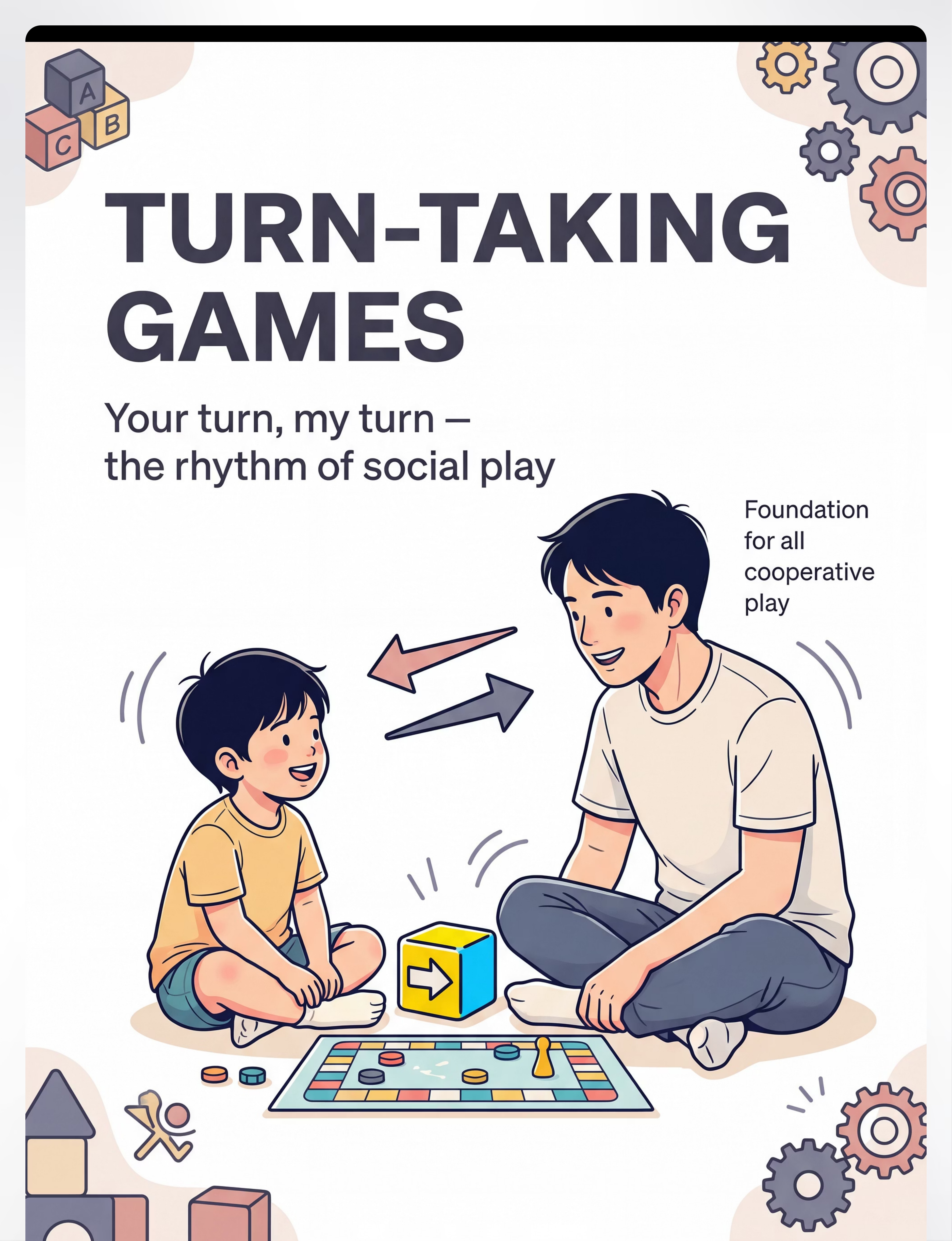
- Turn-Taking Games
- Constructive Materials
- Social Story Books
- Video Models
- Peer Play Supports
- Single-Scheme Play Sets

5 Therapy Disciplines. One Goal: Teaching Your Child to Play.
Occupational Therapy (OT) — Primary Lead
Builds sensory-motor foundations of play. Selects developmentally-appropriate materials; develops fine/gross motor skills for play execution. "OT builds the body's capacity to engage with toys."
Speech-Language Pathology (SLP)
Language and communication within play. Narrating play, joint attention scaffolding, play scripts, requesting during play. "Play IS language. SLP turns play into dialogue."
Applied Behaviour Analysis (ABA)
Teaching play behaviours systematically. Task analysis, reinforcement schedules, prompt hierarchies, data collection. "ABA turns play into measurable, teachable steps."
Special Education (SpEd)
Integrating play into learning routines. Play-based curriculum, IEP play goals, peer integration planning. "SpEd ensures play skills transfer to school."
Neurodevelopmental Pediatrics
Medical monitoring and developmental staging. Diagnosing play-level delays; coordinating multi-disciplinary approach. "NeuroDev ensures the whole child is developing."
"The brain doesn't organize by therapy type. Play skills cross every discipline because play IS how children develop across every domain. That's why Pinnacle deploys a unified consortium approach — not isolated specialties."

Precision Targeting: What Play Skills Teaching Develops
Observable Behaviour Indicators
Target | "Before" Indicator | "After" Indicator | |
Functional Play | Spins toy car wheels; doesn't drive | Pushes car on road, makes vroom sounds | |
Pretend Play | Confused by "let's pretend" | Feeds doll, uses toy stethoscope | |
Constructive Play | Lines up blocks; doesn't stack | Builds towers, structures, with pride | |
Turn-Taking | Grabs toys, can't wait | Passes toy, waits, re-engages | |
Peer Play | Plays beside, not with | Makes eye contact, shares materials |

9 Evidence-Selected Play Teaching Materials
Mapped to the Pinnacle 128 Canon Materials System. Shop or Make.
Cause-and-Effect Toys
Clinical Role: Foundation for intentional play — play's first lesson
Price Range: ₹300–2,000
★ Recommends: Dyomnizy Educational Memory Game with Lights & Sound — ₹519
DIY: Light switches, doorbells, wind-up toys, bubble blowing
Price Range: ₹300–2,000
★ Recommends: Dyomnizy Educational Memory Game with Lights & Sound — ₹519
DIY: Light switches, doorbells, wind-up toys, bubble blowing
Single-Scheme Functional Play Sets
Clinical Role: One play action mastered at a time
Price Range: ₹200–1,000 per set
★ Recommends: Kidology Pull Out Spike Toy — ₹380
DIY: Car + fabric road, doll + comb, toy phone
Price Range: ₹200–1,000 per set
★ Recommends: Kidology Pull Out Spike Toy — ₹380
DIY: Car + fabric road, doll + comb, toy phone
Visual Play Scripts / Sequence Cards
Clinical Role: Step-by-step visual play guidance
Price Range: ₹0–500 (largely homemade)
★ Recommends: Brainy Bug Resources Flashcards — ₹305
DIY: Photo sequence strips, laminated icon cards, velcro step trackers
Price Range: ₹0–500 (largely homemade)
★ Recommends: Brainy Bug Resources Flashcards — ₹305
DIY: Photo sequence strips, laminated icon cards, velcro step trackers
Pretend Play Props with Clear Functions
Clinical Role: Realistic props scaffold symbolic play
Price Range: ₹300–2,500 per set
★ Recommends: A Visit to the Hospital Activity + Sticker Book — ₹199
DIY: Also search: "doctor kit toy India" | "play kitchen set India"
Price Range: ₹300–2,500 per set
★ Recommends: A Visit to the Hospital Activity + Sticker Book — ₹199
DIY: Also search: "doctor kit toy India" | "play kitchen set India"
Turn-Taking Games and Toys
Clinical Role: Social play rhythm foundation
Price Range: ₹200–1,500
★ Recommends: SHINETOY Shut The Box Classic Game — ₹428
DIY: Ball rolling, block tower (alternate adding), coin flip games
Price Range: ₹200–1,500
★ Recommends: SHINETOY Shut The Box Classic Game — ₹428
DIY: Ball rolling, block tower (alternate adding), coin flip games
Constructive Play Materials
Clinical Role: Building and creating — visible competence
Price Range: ₹300–3,000
★ Recommends: Lattooland Rainbow Sorting Activity Set — ₹628
DIY: Cardboard boxes, plastic cups, egg carton structures
Price Range: ₹300–3,000
★ Recommends: Lattooland Rainbow Sorting Activity Set — ₹628
DIY: Cardboard boxes, plastic cups, egg carton structures
Social Story Books About Play
Clinical Role: Making invisible play rules visible
Price Range: ₹200–800 or Free (homemade)
★ Search: "social story autism play India" | "how to play with friends book"
DIY: Photo books of your child + their toys in play sequences
Price Range: ₹200–800 or Free (homemade)
★ Search: "social story autism play India" | "how to play with friends book"
DIY: Photo books of your child + their toys in play sequences
Video Models of Play
Clinical Role: Visual learning for visual learners
Price Range: ₹0 (YouTube) | ₹500–1,000 (subscription)
★ Resources: YouTube: "play skills autism video model" | GPT-OS® video library
DIY: Record 2-minute play sequences on your phone
Price Range: ₹0 (YouTube) | ₹500–1,000 (subscription)
★ Resources: YouTube: "play skills autism video model" | GPT-OS® video library
DIY: Record 2-minute play sequences on your phone
Play Partner Supports / Peer Play Guides
Clinical Role: Preparing both sides of the play interaction
Price Range: ₹100–500 or Free (homemade)
★ Recommends: 1800+ Reward Stickers — ₹364
DIY: Script cards, turn-taking visuals, peer information sheets
Price Range: ₹100–500 or Free (homemade)
★ Recommends: 1800+ Reward Stickers — ₹364
DIY: Script cards, turn-taking visuals, peer information sheets
Essential Kit
₹1,200–2,000: Cause-effect toy + blocks + turn-taking game + sticker rewards
Full Kit
₹5,000–10,000: All 9 categories with recommended products
Zero-Cost Option
Household items + homemade scripts + YouTube videos

Every Material Has a Zero-Cost Version. Every Family Can Start Today.
WHO/UNICEF Equity Principle: Evidence-based intervention must be accessible regardless of geography or income.
Material | 🛒 Clinical Option | 🏠 Home Substitute | Why It Works | |
Cause-Effect Toys | Light-up musical toy ₹500+ | Light switch ON/OFF, doorbell, bubble wand | Same neural principle: action → predictable result | |
Single-Scheme Sets | Commercial toy car set ₹300 | Bottle cap as car, cloth as road | Same functional scheme, different object | |
Visual Scripts | Printed laminated cards ₹200 | Photos on phone, drawn sequence on paper | Visual sequencing works regardless of medium | |
Pretend Props | Doctor kit ₹500 | Ruler as thermometer, cup as stethoscope | Realistic-enough props trigger pretend action | |
Turn-Taking Games | Board game ₹400 | Rock-paper-scissors, ball rolling | Explicit turn structure is what matters | |
Constructive Materials | Magnetic tiles ₹800 | Cardboard boxes, plastic cups, dried pasta | Stacking + creating principle is universal | |
Social Story Books | Commercial ₹300 | 6-photo sequence on your phone | Story structure, not production quality | |
Video Models | Commercial app ₹500 | 90-second phone video of parent playing | Modelling works regardless of camera quality | |
Peer Play Supports | Printed script cards ₹200 | Handwritten index cards | The words and structure matter, not the format |
"The science works with household items. Pinnacle's clinical protocols have been adapted for families across 70 countries — including those with no access to therapy materials. Your kitchen, your living room, and five minutes of intentional engagement are enough to begin."
When clinical materials are non-negotiable: Consult your Pinnacle therapist if your child has oral motor seeking needs, severe sensory hypersensitivity, or shows no response to household substitutes after 2 weeks.

Safety Gate: Read Before Every Session
🔴 RED — Do NOT Proceed
Stop the session if your child shows any of the following:
- Active illness, fever, or pain (sensory thresholds altered)
- Post-meltdown state (nervous system not regulated)
- Signs of extreme fatigue or hunger
- Severe emotional dysregulation (crying, screaming, self-injuring)
- Recent traumatic experience related to play (forced play)
- Medical contraindication from treating physician
Action: Postpone session. Do a calming activity instead. Call 9100 181 181 if repeated episodes of distress.
🟢 GREEN — Safe to Proceed
Begin when all of these are true:
- Child is fed (within 2 hours), not hungry
- Child is rested (not immediately post-nap)
- Child is in a regulated, calm-alert state
- Environment is prepared (see Setup card)
- You are emotionally ready — not rushed, not anxious
- Materials are safe: no sharp edges, appropriate for child's oral stage
🟡 AMBER — Modify and Proceed
Child seems slightly tired → shorten session to 5–7 minutes
Low motivation today → use higher-preference materials
Transitioning from difficult activity → allow 10-min regulated break first
New material being introduced → use extra modelling, reduce expectation
Material Safety: No pieces smaller than 3cm for children who mouth objects. No toxic paints. No balloon fragments. Screens: maximum 15 minutes followed by active play. EMERGENCY: 9100 181 181 (24×7)

The Play Space Setup: 5 Minutes of Preparation = 20 Minutes of Success
Spatial precision prevents 80% of session failures. Five minutes of setup is the highest-leverage investment you can make before any play session begins.
Environment Checklist
- Lighting: natural/warm — NOT fluorescent overhead
- Sound: quiet — background music optional (instrumental, soft)
- Temperature: comfortable — not too warm
- TV off, siblings in another area initially
- 15–25 minutes blocked — no interruptions
Parent State Check
- Phone on silent and face-down
- You feel calm — not rushed, not anxious
- Door closed or visual barrier in place
- Materials pre-staged (not rummaging mid-session)
- Your energy is warm and playful, not clinical
The 60-Second Pre-Flight Check
The best session is one that starts right.
Observable Indicator | GO ✓ | MODIFY ◐ | POSTPONE ✗ | |
Eye contact available | Easy | Effortful | Absent | |
Body: calm-alert state | Regulated | Slightly elevated | Dysregulated | |
Responding to name | Yes | Delayed | No | |
Active stim behaviour | Absent | Mild | Intense | |
Verbal/vocal baseline | Typical | Reduced | Silent or elevated | |
Last meal: within 2 hours | ✓ | >2 hours | >4 hours | |
Last meltdown: >2 hours ago | ✓ | 1–2 hours | <1 hour |
7 ✓ — Start Session
Proceed to Step 1: The Invitation
4–6 ✓ — Modify
Use easier materials, shorter duration (see Adapt card)
<4 ✓ — Postpone
Calming activity instead; reattempt in 30 minutes
Calming bridge activities: Deep pressure (hugs/squeezes), rhythmic movement (rocking), proprioceptive input (carrying heavy bag), sensory snack, quiet co-reading. Do NOT force the play session — forced sessions set back progress.
Parent self-check: Am I calm? Am I rushed? Your nervous system co-regulates with your child's.
Parent self-check: Am I calm? Am I rushed? Your nervous system co-regulates with your child's.
Step 1 of 6 — 15%
The Invitation
Every Session Begins with an Invitation, Not a Command
What to Say (pick one, warmly, at child's eye level)
"Want to play?"
"[Child's name], come play with me."
"Look what I have — [hold up preferred toy]."
[For non-verbal child]: Hold toy toward child; wait 10 seconds.
Acceptance Cues ✓
- Moves toward material
- Makes eye contact with material or you
- Reaches for toy
- Increases vocalisation or pointing
- Smiles or shows positive affect
Resistance Cues ⚠️
- Turns body away
- Returns to preferred stim
- Cries or vocalises distress
The Magnet Principle: If resistance occurs, don't push. Put toy down. Play with it enthusiastically near the child until curiosity brings them closer. Allow 30–90 seconds.

Step 2 of 6 — 30%
The Engagement
The Child is Interested. Now Deepen the Connection.
Deliver verbal praise within 3 seconds of any play-directed behaviour: "Yes! You touched the car!" Reinforcement begins the moment interest appears — not just when perfect play occurs.
Play Level | Presentation Approach | |
Cause-Effect | High contrast, close to child, activate it once first | |
Functional | Single action demonstrated; one prop at a time | |
Constructive | Place one block, then gesture to second; wait | |
Pretend | Act it out yourself with exaggeration and joy | |
Turn-Taking | Hold toy visibly, do your action, then pass clearly |

Step 3 of 6 — 45%
The Therapeutic Action
The Active Ingredient — Targeted Play Input by Material Type
🔵 Cause-Effect Toys
Child presses button/dial/lever. Parent waits for effect, then narrates: "You pressed it — music! Did you hear that?" Repeat until child initiates independently. Mastery: child activates and looks at parent to share delight.
🟠 Single-Scheme Play Sets
Parent models ONE action: push car forward on road. Child imitates. Parent adds ONE word: "Vroom!" Session stays with ONE scheme until mastered — 3 consecutive independent correct actions = mastery for that scheme.
🟢 Visual Play Scripts
Parent points to Step 1 of script: "First — get the car." Continue through script, pointing and narrating. Gradually fade pointing; child follows script independently.
🔴 Pretend Props
Parent models: "I'm the doctor! I'm checking teddy's heart — listen!" Child imitates. Build sequence: check → diagnose → bandage → "All better!" Exaggeration and delight are the therapeutic ingredients.
🟣 Turn-Taking Games
Establish visual turn marker (token, object). "My turn" [does action, returns marker]. "Your turn" [child does action, returns marker]. Minimum 3 complete exchanges = successful turn-taking session.
🟡 Constructive Play
Parent places first block. Waits. Child places second. Parent adds third. Build rhythm of co-construction. Name the creation together: "We're building a tower! How many blocks?"
Core therapeutic action = 5–10 minutes (40–60% of total session). Child must be engaged (not distracted). Parent is modelling, not directing. Language is simple and action-paired. Any approximation is celebrated.
Step 4 of 6 — 60%
Repeat & Vary
3 Good Repetitions > 10 Forced Ones
Material | Target Reps | Variation Strategy | |
Cause-Effect Toys | 5–10 activations | Different buttons, different toys with same principle | |
Single-Scheme Sets | 3–5 complete schemes | Same action, different toy (car → truck → train) | |
Visual Scripts | 2–3 full script runs | Different toy, same sequence structure | |
Pretend Props | 2–4 complete sequences | Different patient (teddy → parent → child) | |
Turn-Taking | 3–5 complete exchanges | Vary who goes first; vary the item passed | |
Constructive | 2–3 building sequences | Different height, different shape goal |
Too Easy
Child disengages — bored. Add complexity: new prop, extra step, new toy in same scheme.
Just Right ✓
Child is engaged, slightly stretched. STAY HERE — this is the therapeutic zone.
Too Hard
Child is frustrated or refusing. Reduce to simpler version of the same activity.
Satiation Indicators — When to Stop: Child turns body away repeatedly, stim behaviour increasing, eye contact reducing, frustrated vocalisation, "jelly" body (lying on floor). These are communication: "I'm done." Honour them. Move to Step 5.

Step 5 of 6 — 75%
Reinforce & Celebrate
Timing Is Everything: Reinforce Within 3 Seconds
🎉 "YES! You did it! Amazing playing!" (for first attempt at any new play action)
🌟 "You did that ALL BY YOURSELF!" (for independent play with no prompting)
🤝 "Perfect turn! You gave it to me — that's how friends play!" (for turn-taking)
🎭 "You're being the DOCTOR! That's pretending — you're brilliant!" (for pretend play)
Type | Examples | Use When | |
🗣️ Verbal | Enthusiastic praise, specific labelling | Every correct play action | |
🌟 Social | High five, hug, celebratory dance | Significant milestones | |
🎯 Token | Sticker chart, star token | For session goals (3 stars = preferred activity) | |
🍬 Tangible | Preferred food item (tiny) | When motivation is low; fade quickly | |
📱 Activity | Screen time, preferred toy/activity | Session completion reward |
"Celebrate the ATTEMPT, not just the success. A child who reaches toward the pretend stethoscope — even if they don't use it — deserves celebration. The nervous system learns that trying leads to joy. That's the loop we're building."

Step 6 of 6 — 90%
The Cool-Down
No Session Ends Abruptly. The Cool-Down Is Part of the Therapy.
The cool-down is not an afterthought — it's a therapeutic transition. Children who experience consistent, predictable endings develop greater session tolerance and arrive at the next session more regulated.
Cool-Down Activities (choose one)
- Deep pressure: firm hug or shoulder squeeze
- Rhythmic: gentle rocking or swaying together
- Proprioceptive: child carries the toy box to storage
- Sensory: favourite comfort object or soft toy
- Visual: look at a picture book together briefly
If Child Resists Ending
- Don't abruptly remove materials — this escalates
- "You can play again [after lunch / tomorrow]."
- Offer choice: "Which toy puts away first?"
- Use visual timer showing "5 more seconds"
- Honour the ending when it happens: "You stopped so well."

Capture the Data — Right Now
60 Seconds of Data Now = Weeks of Progress Insight Later
"Session abandonment is not failure — it's data. Everything your child did today tells you something."
Data Point 1: Engagement Duration
- Under 2 minutes
- 2–5 minutes
- 5–10 minutes
- 10–15 minutes
- 15+ minutes
Data Point 2: Play Level Reached Today
- Cause-effect (activated toy independently)
- Functional (used toy as intended)
- Constructive (built/created something)
- Pretend (used prop in pretend scenario)
- Turn-taking (2+ complete exchanges)
- Peer play (engaged with a play partner)
Data Point 3: Quality Rating
Overall session: 1 (very difficult) → 5 (excellent)
Child's mood at end: Same / Better / Worse than start
Any new behaviour observed: [Free text / voice note]
Why This Matters
Week 1 data baseline → Week 4 comparison → visible progress arc. Parents who track data report 3× higher confidence in their child's development and 2× better session consistency.
Use the GPT-OS® in-app tracker at pinnacleblooms.org/tracker or download the L-963 Play Skills Tracking Sheet PDF.
7 Common Play Session Challenges — and Exactly What to Do
"The technique needs adjustment. Not the parent."
Child won't touch the toy at all
Why: Material may be aversive, or motivation pairing hasn't happened yet.
Fix: Use the Magnet Principle — play enthusiastically yourself. Try 3 different materials. Check for sensory barriers (try covering sharp textures, reducing sound volume).
Fix: Use the Magnet Principle — play enthusiastically yourself. Try 3 different materials. Check for sensory barriers (try covering sharp textures, reducing sound volume).
Child grabs toy and returns to repetitive use (spinning, lining)
Why: Repetitive use is regulated and comfortable; new functional use requires more neural effort.
Fix: Join the repetitive play first for 30 seconds. Then model the functional use once. Don't stop — redirect gently with enthusiasm.
Fix: Join the repetitive play first for 30 seconds. Then model the functional use once. Don't stop — redirect gently with enthusiasm.
Child loses interest after 2–3 minutes
Why: Session duration exceeds current attention capacity.
Fix: Shorten to 2–3 minute blocks with brief sensory breaks between. Three 3-minute blocks > one 10-minute forced session.
Fix: Shorten to 2–3 minute blocks with brief sensory breaks between. Three 3-minute blocks > one 10-minute forced session.
Pretend play attempts get no response
Why: Symbolic thinking requires abstract processing — child may need more time at functional play stage first.
Fix: Drop back to single-scheme functional play for 2 more weeks. Pretend play builds on a solid functional foundation.
Fix: Drop back to single-scheme functional play for 2 more weeks. Pretend play builds on a solid functional foundation.
Turn-taking falls apart — child grabs or melts down
Why: Waiting is a learned skill that requires regulatory capacity.
Fix: Make the turn shorter (2 seconds → return). Provide a "waiting" object. Build tolerance in 2-second increments over days.
Fix: Make the turn shorter (2 seconds → return). Provide a "waiting" object. Build tolerance in 2-second increments over days.
Child plays alone with script but not with a partner
Why: Independent play before social play is developmental — this is actually progress.
Fix: Join parallel to child using identical material for several sessions before attempting coordinated play. Let child initiate the joint element.
Fix: Join parallel to child using identical material for several sessions before attempting coordinated play. Let child initiate the joint element.
Parent gets frustrated and session escalates
Why: Parental emotional state directly regulates child's state.
Fix: Stop the session. Say "All done" calmly. Reconnect after 15 minutes. Review which step in the protocol broke down. Call 9100 181 181 for coaching support.
Fix: Stop the session. Say "All done" calmly. Reconnect after 15 minutes. Review which step in the protocol broke down. Call 9100 181 181 for coaching support.
No Two Children Are the Same. Here's How to Adjust.
Easier Adjustments
- Single object only
- Hand-over-hand throughout
- 2-minute sessions only
- One word narration
- Parent initiates every time
- Same toy/material daily
Harder Adjustments
- Add 2nd scheme to sequence
- Fade all physical prompts
- Child leads the script
- Child generates new actions
- Child invites parent to play
- Rotate 3+ materials per session
Sensory Profile Variations
🔴 Sensory Seeker
Use high-feedback cause-effect toys; active constructive play; materials with strong tactile/proprioceptive input.
🔵 Sensory Avoider
Start with non-tactile materials (visual scripts, video models); introduce textures gradually; never force contact.
🟡 Variable (Mixed)
Morning sessions for tactile; afternoon for visual; rotate material types across the week.
Age/Level | Focus Area | Duration | |
Toddler (1–3) | Cause-effect → basic functional | 5–8 minutes | |
Early Preschool (3–4) | Single scheme → constructive | 8–12 minutes | |
Preschool (4–5) | Constructive → pretend → turn-taking | 12–18 minutes | |
School-age (5+) | Social play → peer play → cooperative games | 15–25 minutes |
"The fastest route to play skill development runs through your child's special interest. Trains → build train station → drive train → pretend to be conductor → play trains with sibling. The interest IS the bridge."

ACT IV — The Progress Arc
Week 1–2
Weeks 1–2: Tolerance and First Sparks
Foundation Phase — 15% Progress
What You Will See ✓
- Child tolerates materials being present without distress
- Brief glances at you while you model play (2–3 seconds)
- Single activations of cause-effect toy (then moves on)
- Reduced resistance to being in the play space
- ONE functional play action, inconsistently performed
What Is NOT Progress Yet ✗
- Spontaneous independent play (this comes later)
- Consistent performance across sessions
- Social engagement or asking for materials
- Pretend play of any kind (weeks away for many children)
"If your child tolerates the play space for 3 minutes longer than last week — that is real, measurable, clinically significant progress. The nervous system is reorganising. The neural pathways are forming. The work is happening."
Parent Milestones Week 1–2: Completed 5+ sessions (any duration) ✓ Identified child's highest-preference material ✓ Identified one successful reinforcer ✓ Set up consistent play space ✓ Tracking data (even rough notes) ✓

ACT IV — The Progress Arc
Week 3–4
Weeks 3–4: Anticipation and Neural Pathway Formation
Consolidation Phase — 40% Progress
Child moves toward play space (not just tolerates it)
Child reaches for specific preferred material
2–3 consecutive functional play actions with a single prompt
Increased session duration (2–3 minutes longer than Week 1)
FIRST SIGNS of anticipation: child looks toward materials tray
Parent may hear first play-related verbalisations ("car!", "vroom")
Reduced prompt intensity needed for familiar action
"When your child looks toward the play space before you've said anything — that's neural pathway formation in action. That casual glance is synaptic strengthening made visible. That's 3 weeks of daily work showing up as a behaviour."
Increase Intensity If: Child consistently completing all steps without prompts → child showing boredom → child initiating the play action independently for 3+ sessions. Action: Add next scheme / extend session by 5 minutes / introduce partner play element.

ACT IV — The Progress Arc
Week 5–8
Weeks 5–8: Mastery, Generalisation, and the Joy of Independent Play
🏆 Mastery Phase — 75% Progress
Functional Play Mastery
- Completes 3 functional play schemes independently (no prompts)
- Generalises scheme to 2+ different but related toys
- Sessions self-maintain for 10+ minutes without adult initiation
Constructive Play Mastery
- Initiates building independently when materials are present
- Shows creation to caregiver (sharing attention)
- Uses creation as setting for another play action
Pretend Play Mastery (if reached)
- Executes 2-step pretend sequence with realistic prop
- Assigns role to one other object (e.g., teddy is patient)
- Shows pretend delight (smile, laugh) during scenario
Turn-Taking Mastery
- Completes 5 turn exchanges without prompt or protest
- Waits through partner's turn with object or visual support
- Initiates "your turn" unprompted
Generalisation = True Mastery. Is the skill appearing in OTHER contexts? Child drives car at grandparent's house. Child takes turns with sibling during bath time. Child uses stethoscope in doctor's play at school. When mastery criteria are met across 3 sessions on 3 different days — you're ready for the next level.

🎉 You Did This.
Your Child Grew Because You Showed Up Every Day.
You committed to teaching play — the most fundamental skill a child can learn. You got on the floor. You modelled. You waited. You adapted. You tracked. And your child — your unique, brilliant child — responded.
🏆 Achievement Unlocked
"Play Skills Foundation" — [Child's name] can now: ___________________________
Date achieved: _______________ Witnessed by: _______________
Date achieved: _______________ Witnessed by: _______________
📸 Celebrate Tonight
Tell everyone at dinner what [child's name] did today. Name it specifically. "She pretended to feed the doll — for the first time ever. That's symbolic play. That's imagination. That happened in our house, today."
📱 Share Your Win
WhatsApp the Pinnacle parent community. Post with #PinnaclePlayWin #GPTOSKid. Call us: 9100 181 181 — we celebrate with you.

Clinical Guardrails: When to Pause and Seek Support
"Trust your instincts. If something feels wrong — pause and ask. That's not failure; that's clinical intelligence."
🚨 Flag | What It Looks Like | Why It Matters | Action | |
Regression | Child loses skills previously mastered | May indicate medical, sensory, or environmental stressor | Teleconsult within 48 hours | |
Self-injury during play | Hitting self, biting, head-banging with play materials | Functional play may be triggering; environment assessment needed | Call 9100 181 181 | |
Flat affect | Engages mechanically — no affect, no delight | May indicate emotional dysregulation or sensory shutdown | NeuroDev consult | |
Physical signs | Nausea, headache, tummy ache before/after sessions | Possible sensory-induced physical response | Pediatrician consult | |
No progress after 8 weeks | No observable change across any domain | Assessment for co-occurring challenges needed | Formal developmental assessment | |
Increasing anxiety | Anxiety about play space/materials increases weekly | Protocol needs significant modification | OT teleconsult |
"Red flags are not failures. They are information. The same instinct that brought you to this page is the instinct that will tell you when to reach out. We are here."

Your Child's Play Development GPS
Where You Were, Where You Are, Where You're Going
Before moving to L-964 (Pretend Play Development): Child should have solid cause-effect understanding AND at least 3 functional play schemes mastered independently across 3 sessions on 3 different days.
Lateral Alternatives: L-968: Sensory Play for Exploration | L-971: Floortime / Child-Led Play | L-974: Play-Based Language Development
Lateral Alternatives: L-968: Sensory Play for Exploration | L-971: Floortime / Child-Led Play | L-974: Play-Based Language Development

More Play Development Techniques at techniques.pinnacleblooms.org

🎯 L-961 — Cause-and-Effect Play
Level: Intro | Materials: Pop-up toys, busy boxes
The foundational play skill — action creates predictable result.
The foundational play skill — action creates predictable result.

🎯 L-962 — Functional Toy Use
Level: Core | Materials: Car sets, doll sets
Using toys as intended — the bridge to all higher play.
Using toys as intended — the bridge to all higher play.

🎯 L-964 — Pretend Play Development
Level: Next Level | Materials: Doctor kit, kitchen set
Symbolic thinking and imagination through structured props.
Symbolic thinking and imagination through structured props.

🎯 L-965 — Peer Play & Social Games
Level: Advanced | Materials: Board games, ball
Real social play with peers — turn-taking and joint engagement.
Real social play with peers — turn-taking and joint engagement.

🎯 L-966 — Cooperative Play Skills
Level: Advanced | Materials: Team games, building sets
Working together toward a shared goal — true cooperation.
Working together toward a shared goal — true cooperation.

🎯 L-968 — Sensory Play for Engagement
Level: Parallel | Materials: Sand, water, kinetic
Sensory exploration as a gateway to play engagement.
Sensory exploration as a gateway to play engagement.
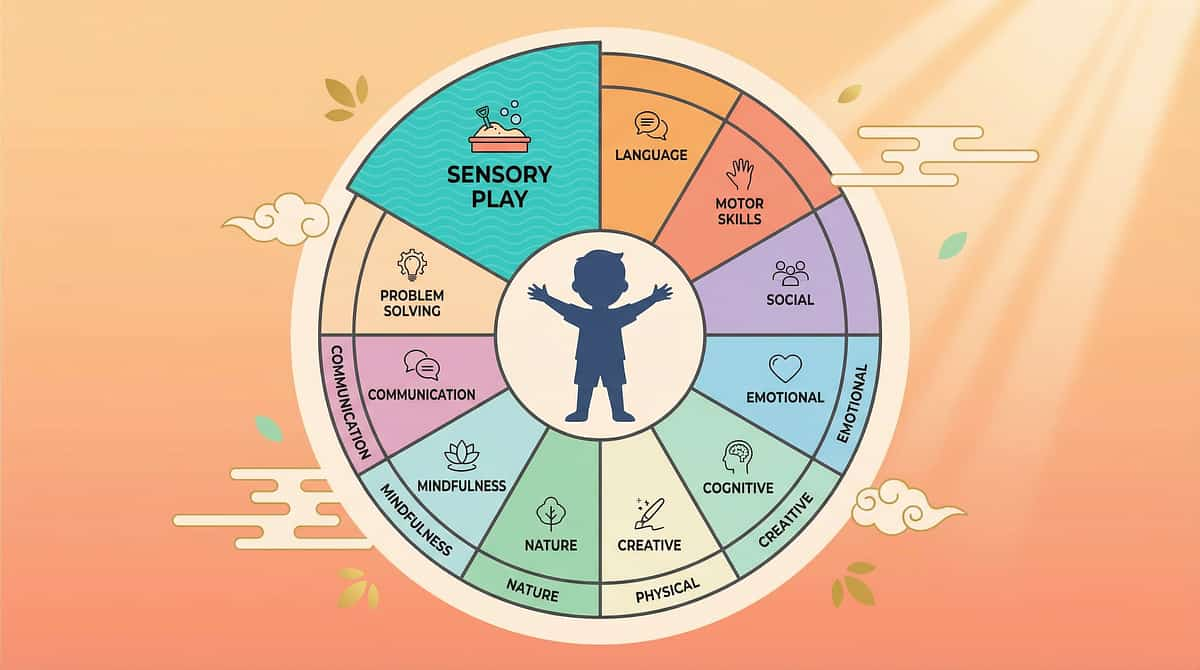
The Complete Developmental Picture: 12 Domains, One Child
"This technique is one piece of a larger plan. Your child is developing across all dimensions simultaneously."
Play Development Accelerates Every Domain
- Language (C): Play is language's developmental substrate
- Social skills (E): Peer play IS social skill training
- Cognitive function (D): Constructive and pretend play build executive function
- Emotional regulation (K): Co-regulated play builds self-regulation capacity
Teaching Play Teaches Everything
When you invest in play skills, you are simultaneously advancing language, social competence, cognitive flexibility, motor coordination, and emotional regulation. Play is not one domain — it is the vehicle through which all domains grow together.
View your child's full developmental profile at pinnacleblooms.org/profile via the GPT-OS® dashboard.
ACT V — Community & Ecosystem
Real Families. Real Play. Real Transformation.
Anonymised case narratives from Pinnacle Blooms Network. Individual outcomes vary based on child profile and intervention intensity.
Family Story 1 — Hyderabad
Before:"At three, my son had never really played. Toys were objects to spin or line up. He never pretended, never built anything on purpose, never played with other children. We'd given up on play."
After 8 weeks:"He builds elaborate block towers now. He pretends to cook and feeds his stuffed giraffe. Last month he played cars with another child for ten minutes — they were driving together, making sounds, taking turns. Real play. Real connection."
— Mother, 4-year-old boy | Therapist note: Entered at cause-effect level. Single-scheme sets for 3 weeks, visual scripts at Week 4, turn-taking games by Week 6. By Week 8: 7 independent functional play schemes. Parent coaching was the multiplier.
Family Story 2 — Bengaluru
Before:"She would sit at the edge of birthday parties watching other children play, trying to organise their toys into rows. Play felt like a foreign country she didn't have a visa for."
After:"She has a play script for her tea party set. It's laminated. She follows it herself. And last week — unprompted — she invited her younger cousin to join. She said: 'Teddy needs more tea. You pour.' I can't explain what that moment meant."
— Father, 5-year-old girl | Bengaluru

You Don't Have to Do This Alone.
18 Million Families Are Walking This Path.
WhatsApp Support Groups
Request the "Play Skills Teaching" parent group via Pinnacle Helpline: 9100 181 181 (say "WhatsApp play group"). Moderated by Pinnacle clinical team. Hindi + English + 14 regional languages.
Online Community
pinnacleblooms.org/community — Domain-specific forums for Play Development with parent-to-parent support across India and 70+ countries.
Local Parent Meetups
Organised quarterly by Pinnacle centers. Ask at your nearest center to join upcoming events in your city.
Peer Mentoring
Connect with a parent who is 3–6 months ahead of you on this journey. Request via helpline: "I'd like a peer mentor for play skills."
"Your experience helps others. When you share what worked — the material that clicked, the script that unlocked something — you accelerate another child's progress. This is collective intelligence. This is how GPT-OS® gets smarter for every family."
Home Practice + Professional Guidance = Maximum Impact
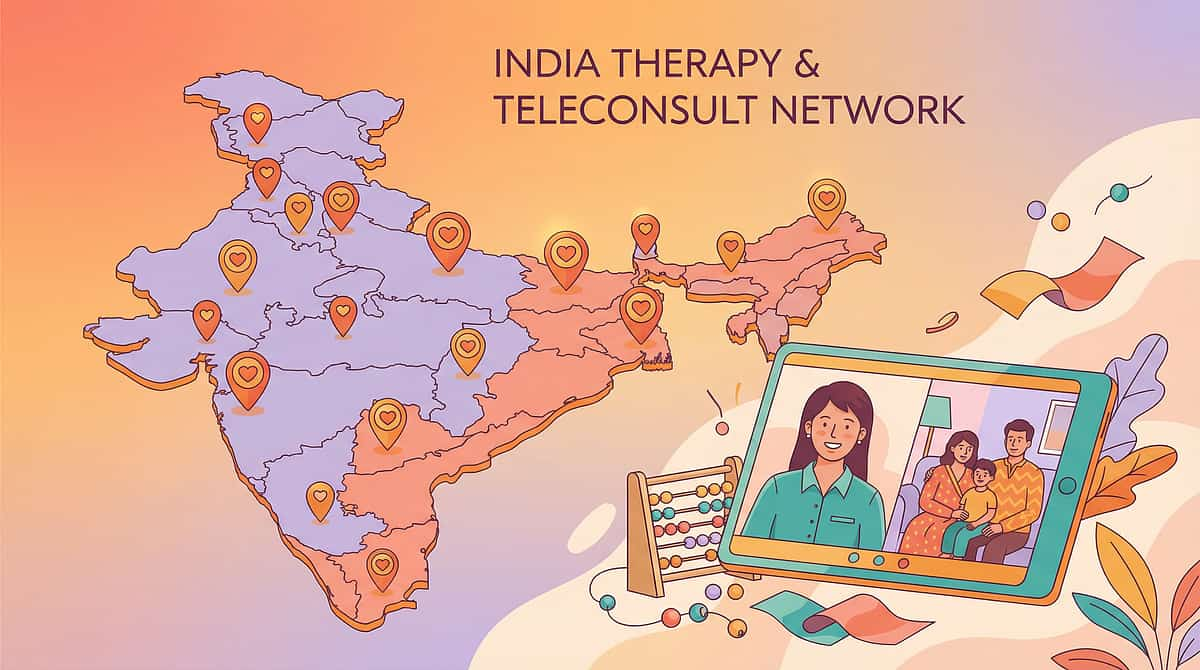
70+ Pinnacle Blooms Network Centers Across India
Find Your Center
Interactive locator showing 70+ Pinnacle centers across India. Auto-detected by browser location.
Filter by: OT | SLP | ABA | SpEd | NeuroDev
Visit: pinnacleblooms.org/centers
Teleconsultation — Available Nationally
FREE initial consultation for play skills assessment.
Book: pinnacleblooms.org/teleconsult | 9100 181 181
Book: pinnacleblooms.org/teleconsult | 9100 181 181
Service Matching
Your Need | Pinnacle Service | |
Comprehensive play assessment | OT Play Development Evaluation | |
Protocol setup + parent training | OT Home Programme (Play Focus) | |
Language through play | SLP Play-Based Language Therapy | |
Play skill behavioural support | ABA Play Skills Protocol | |
School integration of play | SpEd Inclusion Programme | |
Medical developmental oversight | NeuroDev Pediatrics | |
Remote families | Teleconsultation (all disciplines) |
Play-based OT/SLP intervention is claimable under many Indian insurance policies and state government schemes. Ask your Pinnacle center for documentation support.
The Evidence Base: For Parents Who Want to Go Deeper
Key Studies
PRISMA Systematic Review (2024) — PMC11506176
16 studies confirm play-based structured intervention as evidence-based practice for ASD; engagement and developmental outcomes measured.
Meta-analysis — World J Clin Cases (2024) — PMC10955541
Structured play intervention across 24 studies: significant improvement in social skills, adaptive behaviour, sensory processing.
JASPER Intervention — Kasari et al., UCLA
RCT-validated joint attention + symbolic play; improvements in play complexity and social communication.
WHO Care for Child Development (2023) — PMC9978394
Parent-delivered developmental intervention: multi-country evidence for home-based effectiveness.
Padmanabha et al. — Indian J Pediatr (2019)
Indian RCT: home-based developmental intervention; significant outcomes in Indian pediatric population. DOI: 10.1007/s12098-018-2747-4
Full bibliography: pinnacleblooms.org/research/play-skills
Your Sessions Are Generating Intelligence — For Your Child and 18 Million Others
What GPT-OS® Learns from L-963 Data
- Which of the 9 materials generates highest engagement for your child's profile
- Optimal session duration by age + sensory profile combination
- Technique sequencing: which play skill to develop next
- Parent confidence curve: when to introduce next complexity level
- Indian-population-specific patterns in play skill development trajectories
Privacy Assurance
- All data anonymised and encrypted
- No individual child identifiable in population analysis
- DPIIT registered: DIPP8651
- Compliant with Indian data protection standards
- You control your data: delete or export anytime
"When 50,000 families track L-963 sessions, GPT-OS® develops a precision map of what works, for whom, at which developmental stage — more powerful than any single research study. Your 60-second daily log is a contribution to the most comprehensive pediatric play development database on Earth."
Watch: 9 Materials That Help With Play Skills Teaching
▶ Play Video — L-963 Reel
Series: Developmental Play, Episode 963
Duration: 75–85 seconds
Domain: Play Development / PD-PST
Duration: 75–85 seconds
Domain: Play Development / PD-PST
Why Video Modeling Works
Video modeling is a classified evidence-based practice for autism (NCAEP, 2020). Watching this reel and then immediately attempting the material shown is a therapeutic act in itself. Let your child watch it with you — multiple viewings are encouraged and clinically beneficial.
Related Reels in This Series
- ← L-962: 9 Materials That Help With Functional Toy Use
- → L-964: 9 Materials That Help With Pretend Play Development
pinnacleblooms.org/reels/play-development/
Consistency Across All Caregivers Multiplies Impact by 3×
Play skills generalise when every caregiver speaks the same therapeutic language.
Share This Page
Link: techniques.pinnacleblooms.org/play-development/play-skills-teaching-L-963
Downloadable Resources
- 📥 "Teaching Play at Home — L-963 Family Guide" (1-page PDF)
- Available in Hindi, Telugu, Tamil, Kannada, Malayalam, Bengali, Marathi
- 📥 School Communication Letter for Play Skills Teaching
- pinnacleblooms.org/family-guides/L-963
"Explain to Grandparents" Version
[Child's name] is learning to play — specific skills: how to use toys on purpose, how to take turns, how to imagine. Every time you play with [child's name], follow these three rules:
- Get on the floor at their level.
- Copy what they do for 30 seconds.
- Add one new action — then wait.
That's it. You're doing therapy.
"When the Pinnacle OT, the parent, the grandparent, and the class teacher all use the same play language and the same visual scripts — the neural pathways form 3× faster. Consistency is the highest-leverage investment any family can make." — PMC9978394

ACT VI — The Close
Your Questions, Answered by the Pinnacle Consortium
My child is 7 — is it too late to teach play skills?
It is never too late. Play development can occur at any age when the right scaffolding and materials are provided. Older children often progress faster because they have more cognitive capacity to understand scripts and sequences. Contact us at 9100 181 181 for an age-specific assessment.
How long before I see results?
Most families observe first changes within 1–2 weeks of daily practice. Functional play actions typically emerge by weeks 3–4. Pretend play may take 8–12 weeks of consistent work. Progress is non-linear — track data (Card 20) to see what's actually happening beneath your perception.
Do I need to do all 9 materials?
No. Start with 1–2 materials matched to your child's current developmental play level. Add materials as your child progresses. The sequence in the materials card represents an effective developmental order, but adapt to your child.
My child loves YouTube but won't engage with physical toys — what do I do?
Use YouTube as the bridge. Find video models of the toys you want to introduce (search "playing with [toy name]"). Watch together. Then immediately offer the physical toy. The video-to-physical bridge is a legitimate clinical technique.
We have a weekly clinic session. Should I still do this at home?
Absolutely — this is the clinical recommendation. Weekly clinic sessions set the protocol; daily home sessions build the neural density. The research shows home-based practice is the primary driver of generalisation and maintenance. The clinic teaches; the home solidifies.
My child has no language yet — can they still learn play skills?
Yes. Play and language develop in parallel but are not dependent on each other. Visual scripts, video models, and gestural communication make play teaching fully accessible to non-verbal children. Your SLP and OT should be coordinating play and language goals together.
What if siblings don't know how to play with my child?
Brief sibling training — 5–10 minutes — on how to offer toys, wait for responses, and celebrate any engagement can transform sibling interactions. Contact the Pinnacle center for a "Sibling Support" session.
This feels overwhelming — where do I start?
Start with ONE material. Choose the one that best matches where your child currently is. Do ONE 10-minute session tomorrow. Call 9100 181 181 before or after — we'll coach you through it. The first session is always the hardest. Everything compounds from there.

Your Child's Play Journey Begins With One Session.
You Have Everything You Need. Start Today.
🎮 Start This Technique Today
Launch your first Play Skills session with GPT-OS® step-by-step guidance.
→ pinnacleblooms.org/start/L-963
📞 Book a Consultation
Speak with an OT, SLP, or ABA specialist. Free initial teleconsult available.
→ 9100 181 181 | pinnacleblooms.org/book
🗺️ Explore Next Technique
L-964: Pretend Play Development — the natural next step after this technique.
→ techniques.pinnacleblooms.org/L-964
✦ PINNACLE BLOOMS CONSORTIUM VALIDATED ✦
OT • SLP • ABA/BCBA • SpEd • NeuroDev • CRO • WHO/UNICEF-Aligned
20M+ Sessions | 97%+ Improvement | 70+ Centers
FREE National Autism Helpline: 9100 181 181 — Available in 16 languages | 24×7 | India + International
Preview of 9 materials that help with play skills teaching Therapy Material
Below is a visual preview of 9 materials that help with play skills teaching therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Network® was built by mothers, engineered as a system, and validated by twenty million therapy sessions. We exist for one purpose: to transform every home into a proven, scientific, 24×7, personalised, multi-sensory therapy centre — for every child, regardless of geography or income.
You've Completed
L-963 — Play Skills Teaching
Next Recommended
→ L-964: Pretend Play Development
"The imagination is not missing — it's waiting to be unlocked."
"The imagination is not missing — it's waiting to be unlocked."
Occupational Therapy
Sensory-motor foundations of play
Speech-Language Pathology
Language and communication within play
Applied Behaviour Analysis
Systematic play skill teaching
Special Education
Play skills transfer to school
Neurodevelopmental Pediatrics
Whole-child medical oversight
70+ Centers | 20M+ Sessions | 97%+ Improvement | Serving families from 70+ countries
FREE Helpline: 9100 181 181 | 16 Languages | 24×7
FREE Helpline: 9100 181 181 | 16 Languages | 24×7
techniques.pinnacleblooms.org | pinnacleblooms.org | care@pinnacleblooms.org
Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®. All rights reserved. Pinnacle Blooms Network® | GPT-OS® | AbilityScore® | TherapeuticAI® are registered trademarks.
Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®. All rights reserved. Pinnacle Blooms Network® | GPT-OS® | AbilityScore® | TherapeuticAI® are registered trademarks.
Medical Disclaimer: This content is educational and addresses play skill development for children with autism and developmental differences. Strategies should be adapted to your child's specific developmental level, interests, and needs in consultation with qualified therapists. This content does not replace professional developmental or therapeutic assessment and individualised intervention planning. Individual outcomes vary based on child's profile and intervention intensity.