9 Materials That Help With Pica Behavior
"She ate the foam from her mattress. She found the batteries." — You can't look away for one second. The fear is constant. The danger is real. These 9 clinically validated materials are the answer.
D-419
Behavioral Safety
Oral-Motor
Ages 2–12

Why They Eat Things That Aren't Food: The Neuroscience
The Oral Sensory System
The trigeminal nerve is one of the most powerful sensory pathways in the human nervous system. In children with sensory processing differences, this system may be chronically under-responsive, demanding constant, intense oral input to achieve regulation. The brain broadcasts: "Feed me MORE sensation."
Pica as Sensory Seeking
The child's insular cortex — which processes interoceptive signals like hunger and satiety — may not accurately distinguish between "I need food" and "I need intense oral input." The mouth becomes the primary regulatory tool.
Pica as Behaviour Without Awareness
In many children, the behaviour is automatic — triggered by sensory states below the threshold of conscious awareness. The child does not "decide" to eat paper. The nervous system compels it.
The Nutritional Link
Iron and zinc deficiencies dysregulate dopamine reward pathways, which can intensify non-food cravings at a neurochemical level. This is why blood panels matter — medical assessment is a non-negotiable parallel track.
"This is a wiring difference, not a behaviour choice. The intervention must address the wiring." — Pinnacle NeuroDev Paediatrics & OT Consortium

Your Child Is Here. Here Is Where We're Heading.
Pica is clinically defined as the persistent eating of non-nutritive substances beyond 18–24 months at a developmentally inappropriate age. By age 2, most children have learned food/non-food discrimination. When this learning hasn't occurred — or is overridden by sensory need — pica persists, and the stakes of non-intervention rise sharply with age and motor capability.
Birth–6 mo
Oral reflexes present — developmentally normal
6–18 mo
Mouthing for exploration — normal
18–24 mo
Food/non-food discrimination develops; mouthing fades
2–5 yrs
Pica ZONE — persistent mouthing is clinically significant here
5–12 yrs
Target: resolution through structured multi-modal intervention
Pica Most Commonly Co-occurs With:
Autism Spectrum Disorder
Intellectual Disability
Iron / Zinc Deficiency
OCD Patterns
Sensory Processing Disorder (Oral)

Clinically Validated. Home-Applicable. Parent-Proven.
★★★★☆ Level II–III Evidence
Multi-modal intervention for pica is supported by RCTs, systematic reviews, and clinical consensus. The evidence base spans sensory integration, discrimination training, and caregiver-delivered protocols — all validated for home application within a nurturing care framework.
Study | Key Finding | Source | |
PRISMA Systematic Review (2024) | Sensory integration intervention meets evidence-based practice criteria for ASD | PMC11506176 | |
World J Clin Cases Meta-analysis (2024) | SI therapy effectively promotes adaptive behaviour across 24 studies | PMC10955541 | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based sensory interventions show significant outcomes in Indian paediatric population | DOI:10.1007/s12098-018-2747-4 | |
NCAEP Report (2020) | Response interruption, redirection, and discrimination training are EBPs for autism | NCAEP 2020 | |
WHO NCF (2018) | Caregiver-delivered intervention within nurturing care framework produces measurable outcomes | PMC9978394 |
"Multi-modal intervention addressing oral sensory needs, environmental safety, discrimination training, and behavioural replacement achieves measurable pica reduction in the majority of cases when individualised to function."

Pica Behaviour Intervention: What It Is
🛡️ D-419
Ages 2–12
8–16 Week Primary Intervention
"Meeting the mouth's need safely — while keeping your child out of danger."
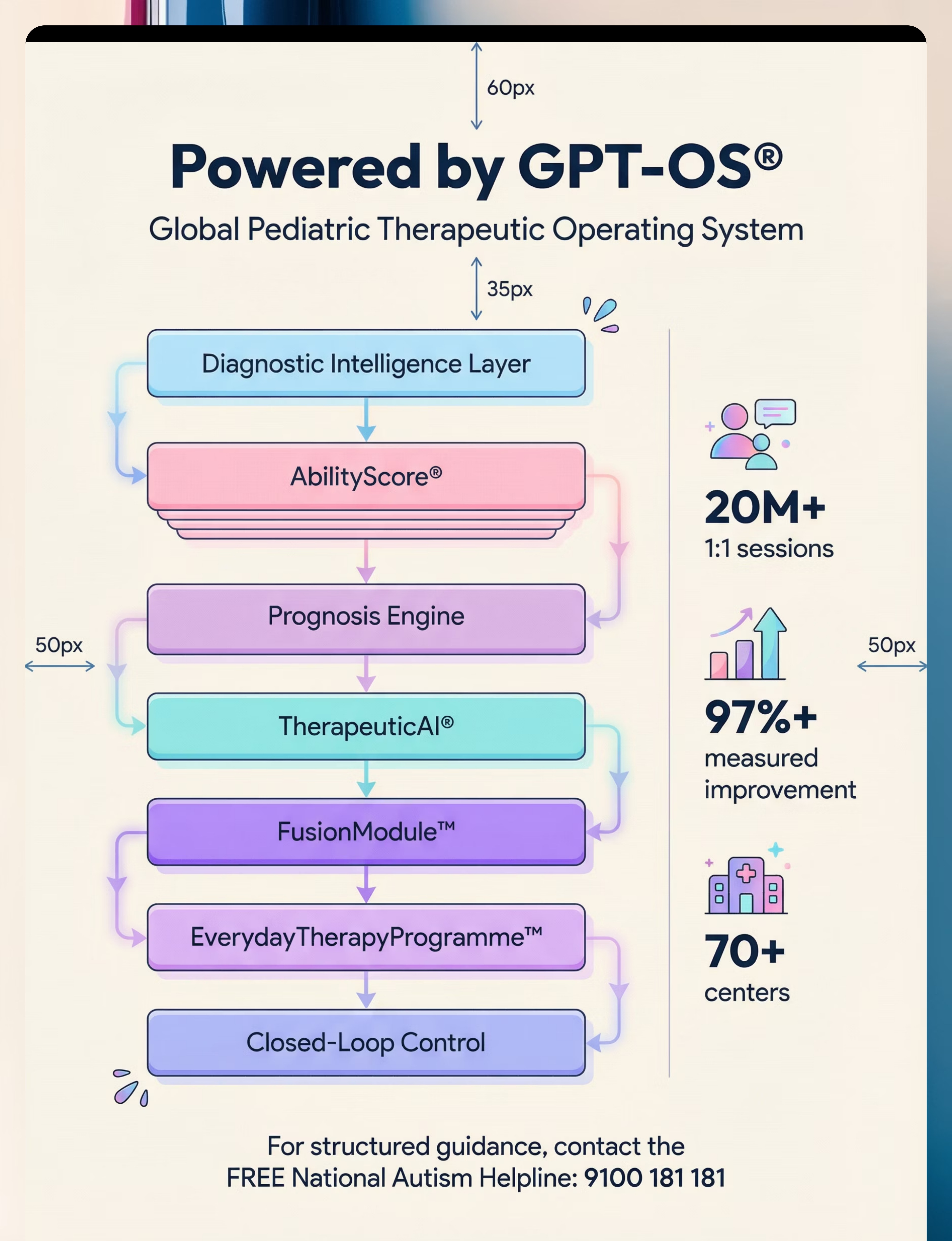
Pica Behaviour Intervention is a structured, multi-layered clinical approach that simultaneously addresses every dimension of the challenge. This is not a single technique — it is a coordinated framework, governed by GPT-OS® FusionModule™, that unifies OT, ABA, SLP, NeuroDev Paediatrics, and family coaching into one coherent intervention.
1
Safe Sensory Alternatives
Provide safe oral-sensory alternatives to meet the needs driving non-food ingestion
2
Environmental Modification
Modify the environment to reduce access to dangerous items
3
Discrimination Training
Explicitly teach food vs. non-food through repeated, reinforced behavioural practice
4
Behaviour Replacement
Replace the behaviour with functionally equivalent, safe alternatives
5
Medical Monitoring
Monitor medical status as an essential parallel track — always running alongside the behavioural work

The Consortium Behind Your Child's Safety Plan
Pica does not respect therapy boundaries. It is simultaneously a sensory, behavioural, medical, and developmental challenge. The only effective response is a simultaneous, coordinated one. Here are the five disciplines working together on your child's safety plan.
Occupational Therapist (OT)
Sensory profile assessment; oral sensory diet design; chew tool selection; full-body sensory regulation plan
Speech-Language Pathologist (SLP)
Oral-motor assessment; oral tone and coordination; feeding safety evaluation; communication of needs as alternative to pica
Behavioural Analyst (BCBA / ABA)
Functional Behaviour Assessment to identify pica's function; discrimination training; replacement behaviour protocol; reinforcement systems
Special Educator (SpEd)
Food/non-food discrimination across environments; school coordination; visual support systems
NeuroDev Paediatrician
Medical evaluation; nutritional deficiency testing (iron, zinc); GI monitoring; medication assessment if compulsive component present
"The brain doesn't organise itself by therapy type. Pica is a sensory, behavioural, medical, and developmental challenge simultaneously. The only effective response is a simultaneous, coordinated one." — Pinnacle FusionModule™ Clinical Principle

What This Targets — Specifically
Effective pica intervention works in three concentric rings, moving from the most urgent safety goals outward to long-term developmental independence. Understanding what each ring means helps you measure progress accurately and celebrate every step.
Primary Target Indicators
- Zero dangerous ingestion for 30+ consecutive days
- Child redirects own mouthing impulse to safe chew tool
- No emergency room visits or poison control calls
Secondary & Tertiary Indicators
- Child spontaneously reaches for chew necklace when oral urge arises
- Child correctly sorts items as "food" / "not food" in novel contexts
- Caregiver supervision needs reduce progressively over weeks
- Parent reports reduced anxiety and increased confidence

9 Materials That Help With Pica Behaviour
Clinically mapped by the Pinnacle Consortium. Canon-classified. Home-deployable. Every family can access at least one option from each category today.
1
1 — Safe Chew Tools
Oral Sensory Alternatives
2
2 — Environmental Modification
Safety Supplies
3
3 — Oral-Motor Exercise Tools
Therapeutic Exercise
4
4 — Discrimination Training
Behavioural Sorting Materials
5
5 — Replacement Behaviour Tools
ABA Redirection Systems
6
6 — Sensory Diet Tools
Full-Body Regulation
7
7 — Medical Monitoring Supplies
Clinical Necessity
8
8 — Safe Texture Alternatives
Sensory Substitution
9
9 — Supervision & Monitoring Systems
Caregiver Infrastructure

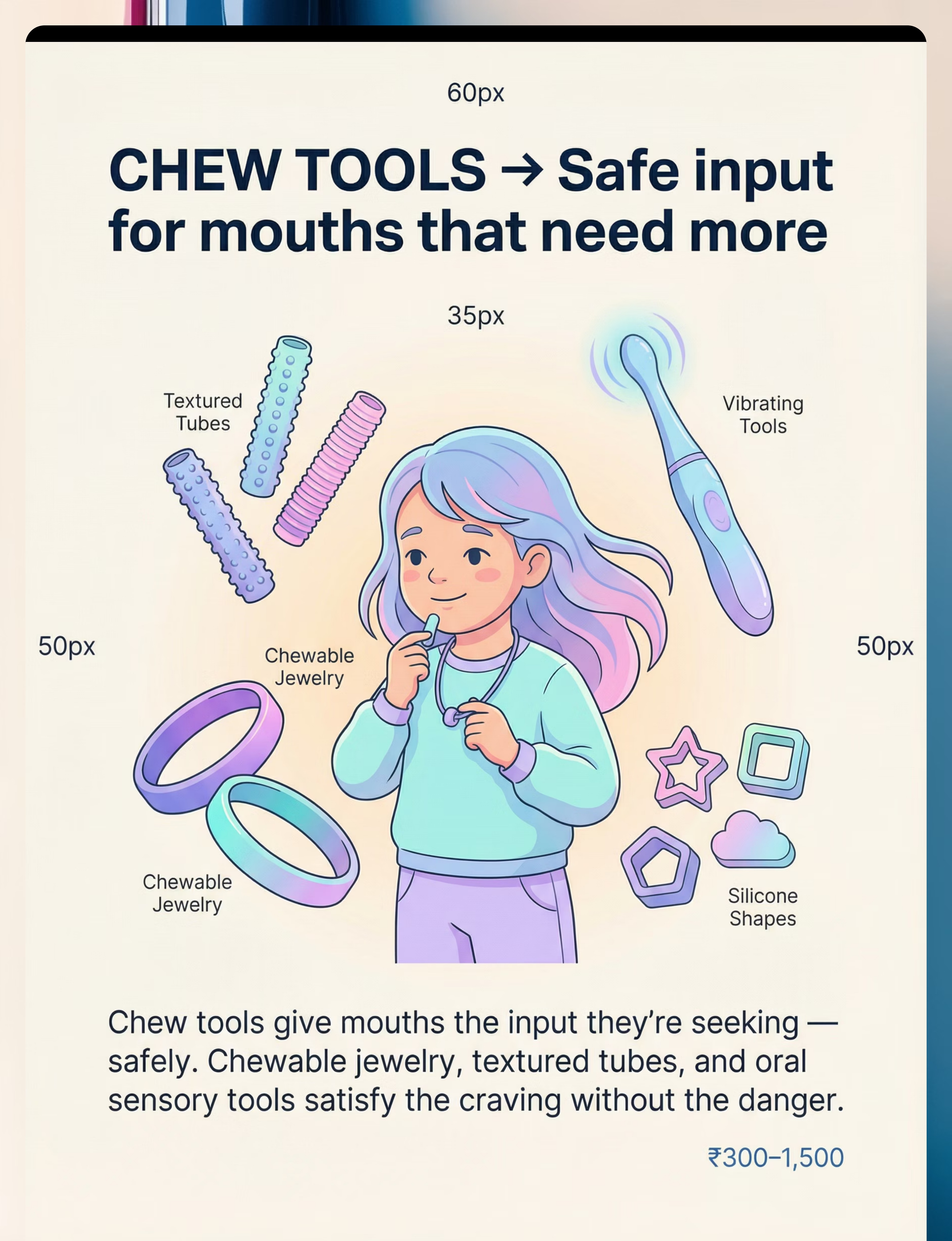
Material 1 — Safe Chew Tools & Oral Sensory Alternatives
Canon: Oral Sensory Tools
Primary Material
₹300–1,500
Pica's most common driver is oral sensory seeking — the mouth is desperately seeking input that food alone doesn't provide. Safe chew tools provide the exact proprioceptive, textural, and resistive oral input the nervous system demands, through materials that cannot cause choking, poisoning, or obstruction. When the mouth has a safe, always-available outlet that truly satisfies the craving, the drive toward dangerous non-food items decreases measurably.
What to Source
- Chewable silicone necklaces and bracelets (multiple resistance levels)
- Chew tubes — textured: bumpy, ridged, smooth
- Chewable pencil toppers (discreet for school use)
- Vibrating oral-sensory tools
- Food-grade silicone chewables in shape variations
- Textured teething toys rated for older children's bite force
⚠️ Safety Note
Inspect chew tools weekly for bite damage. Replace immediately when worn. Match resistance level to child's bite strength — too soft breaks; too hard causes jaw fatigue.
💡 DIY Zero-Cost Version
Any food-grade silicone kitchen tool (not sharp, not breakable into small pieces) can be temporarily repurposed as a chew surface. A frozen damp cloth provides intense oral input. Always confirm non-toxicity before any DIY oral tool.

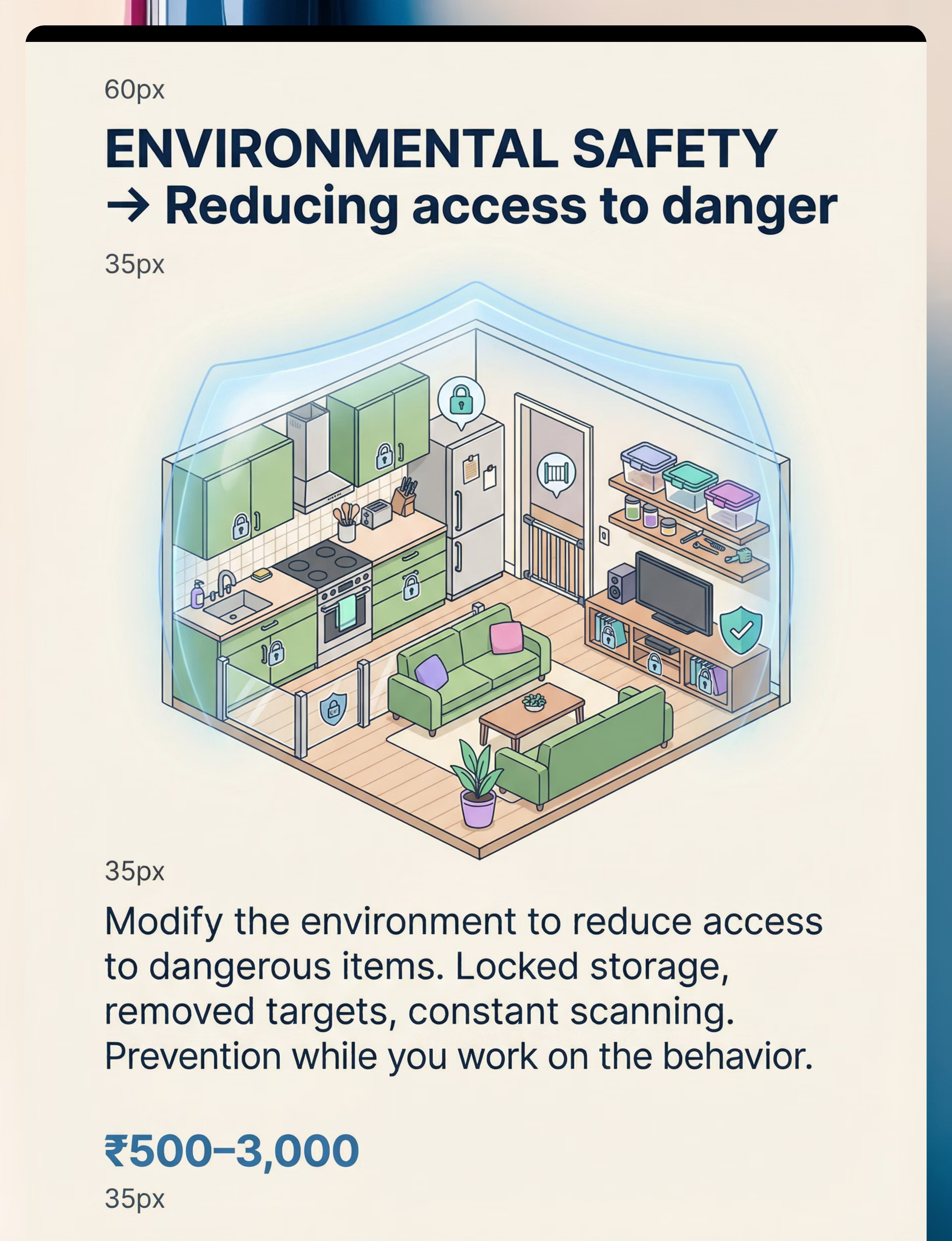
Material 2 — Environmental Modification Supplies
Canon: Environmental Safety
Safety-Critical
₹500–3,000
While behavioural and sensory interventions work over time, the environment must become the first line of defence. Environmental modification does not treat pica — it prevents the dangerous ingestion that makes treatment possible. A child cannot learn when they are in constant medical danger, and a parent cannot implement interventions while simultaneously conducting emergency room visits.
What to Source
- Childproof cabinet and drawer locks (multi-pack)
- Locking storage containers for cleaning supplies, medications, batteries
- Heavy-duty trash cans with locking lids
- Baby gates for high-risk areas (bathrooms, utility rooms, kitchens)
- Cord covers and outlet protectors (fabric and electrical targets)
- Furniture anchors (to prevent access to items behind furniture)
⚠️ Safety Note
Environmental modification buys time but does not replace supervision. Children with pica consistently find items caregivers didn't anticipate. Conduct room-by-room audits quarterly.
💡 DIY Zero-Cost Version
Rope ties through cabinet handles, heavy furniture blocking access to specific areas, and removing all pica-target items from accessible locations cost nothing and can be implemented today.
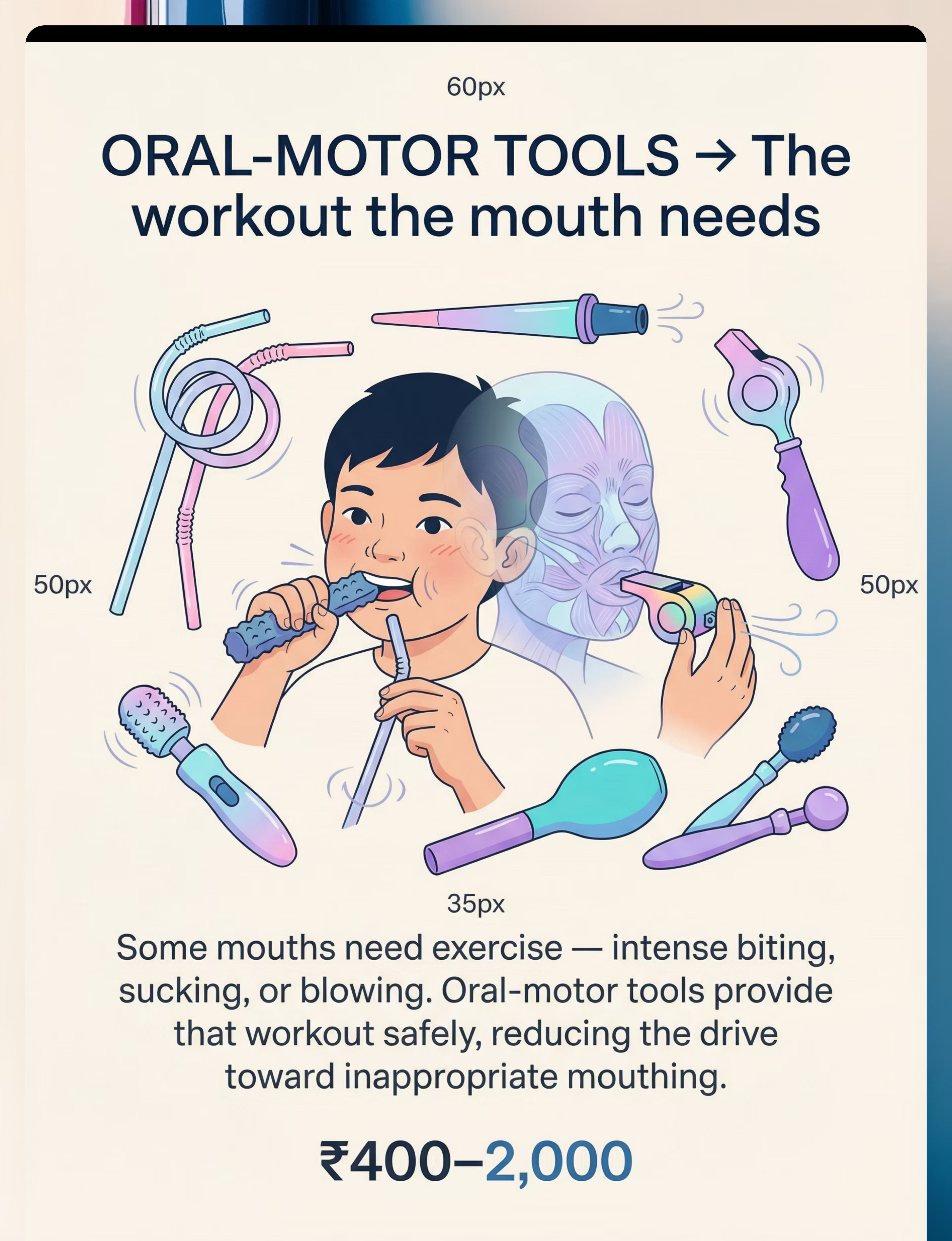
Material 3 — Oral-Motor Exercise Tools
Canon: Oral-Motor Tools
Therapeutic Exercise
₹400–2,000
Some pica is driven not by sensory seeking alone, but by oral-motor needs — the mouth requires structured exercise, resistance, and motor challenge that typical eating doesn't provide. Therapeutic oral-motor tools deliver this "workout" safely. When the oral musculature receives the exercise it needs, the urgent drive toward inappropriate mouthing decreases because the neurological demand has been satisfied.
What to Source
- Therapeutic chew tools with graduated resistance levels (light / medium / firm)
- Therapeutic straws — narrow, long, or textured for intense sucking work
- Blow toys: party horns, blow-bubbles, kazoos, whistles
- Vibrating oral-motor tools (electronic vibration targets jaw / tongue)
- Oral massage wands (Z-Vibes or equivalents)
- Chewy food options for structured meal-time oral work (jerky, dried fruit, bagels)
⚠️ Safety Note
Oral-motor tools should be introduced under SLP or OT guidance. Incorrect tool selection can cause jaw fatigue or reinforce the wrong patterns.
💡 DIY Zero-Cost Version
Thick smoothies through thin drinking straws provide intense sucking work at zero cost. Blowing bubbles with soap and water. Chewing raw carrot sticks or celery for structured oral-motor input at mealtimes.

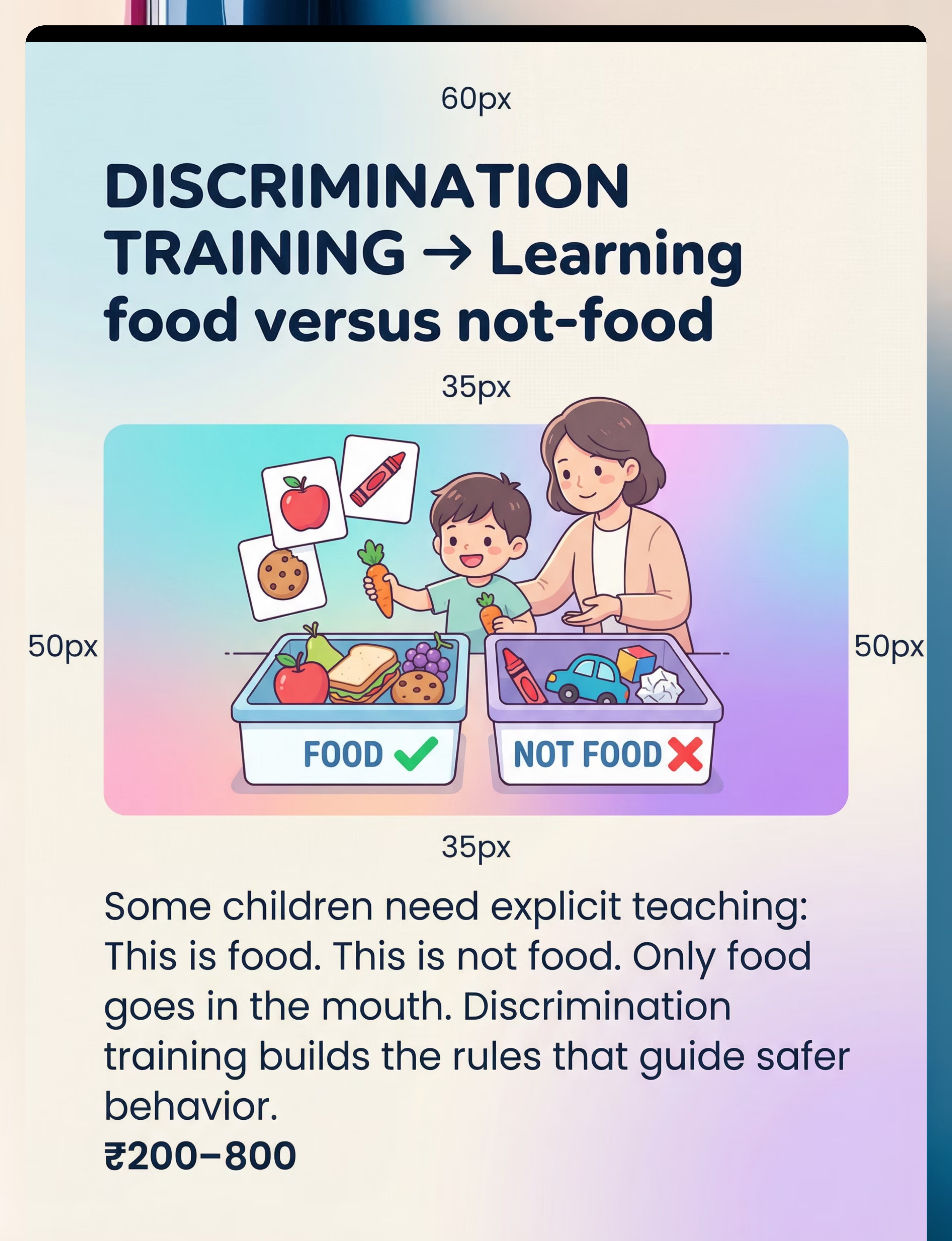
Material 4 — Discrimination Training Materials
Canon: Sorting Activities / Categorisation
Behavioural Training
₹200–800
Many children with pica have not learned — or cannot consistently apply — the rule that "only food goes in the mouth." Discrimination training is explicit, structured teaching of the food/not-food rule through repeated practice, immediate feedback, and across multiple contexts. It builds the cognitive framework that governs safe oral behaviour.
What to Source
- Food/not-food picture card sets (printable or commercial)
- Sorting bins or mats labelled "FOOD ✓" and "NOT FOOD ✗"
- Visual rules poster: "Only food goes in the mouth" — laminated, posted at child height
- Category sorting games (adapt commercial sorting toys)
- Social stories featuring food/not-food scenarios
- Practice items: real or toy food alongside safe non-edible objects
Active Product Matches
Lattooland Rainbow Sorting Activity Set for Toddlers — adaptable for food/not-food discrimination practice.
Brainy Bug Resources Flashcards — category sorting foundation for building discrimination skills.
💡 DIY Zero-Cost Version
Draw and laminate two boxes on A4 paper — "FOOD ✓" and "NOT FOOD ✗." Use actual household items to practise sorting: apple → food box, pen → not food box. Run 5-minute practice sessions twice daily.
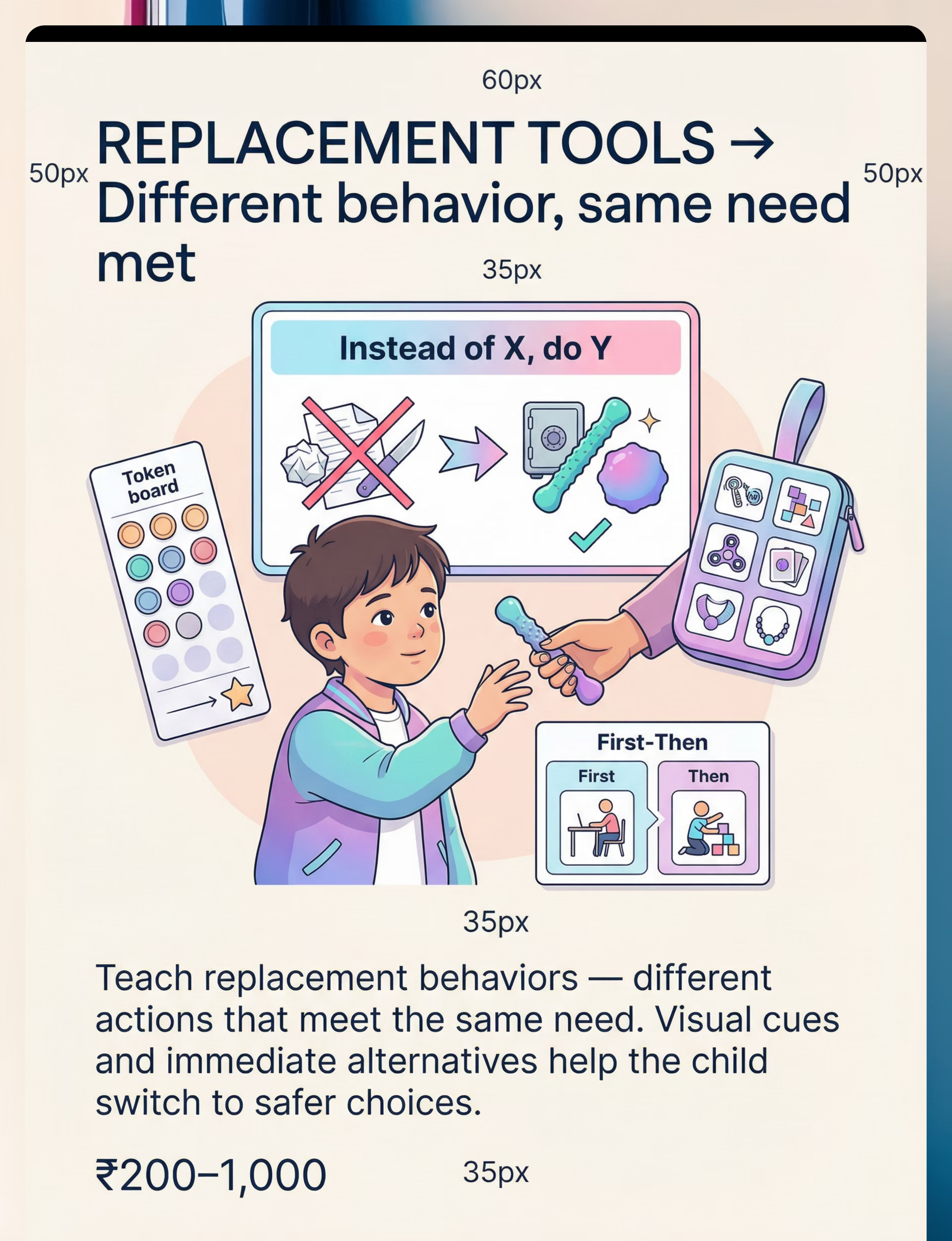
Material 5 — Replacement Behaviour & Redirection Tools
Canon: Reinforcement Menus
ABA Behavioural Tools
₹200–1,000
The function of pica — sensory input, attention, escape, or automatic behaviour — does not disappear when the dangerous behaviour is blocked. The need must be redirected to a functionally equivalent, safe alternative. Replacement behaviour tools make the "switch" immediate and visible: visual cue cards show "Instead of that → chew this." Reinforcement systems reward every successful redirect.
What to Source
- Visual cue cards: "Instead of [X], I can [Y]" — laminated, portable
- Portable alternative kit: chew tools and safe items in a belt pouch
- Token boards for reinforcing pica-free intervals
- First-Then boards: "First safe chew → Then [preferred activity]"
- Social stories about choosing safe alternatives
- Visual timer for reinforcing pica-free periods
⚠️ Critical Note
Replacement behaviours must be functionally equivalent to succeed. A replacement that doesn't meet the same sensory or behavioural need as the pica will not compete effectively with it.
💡 DIY Zero-Cost Version
Print visual cue cards from any home printer. A small ziplock bag with a chew tool clipped to a belt loop is a zero-cost "portable kit." Verbal praise is a zero-cost reinforcer that is always available.
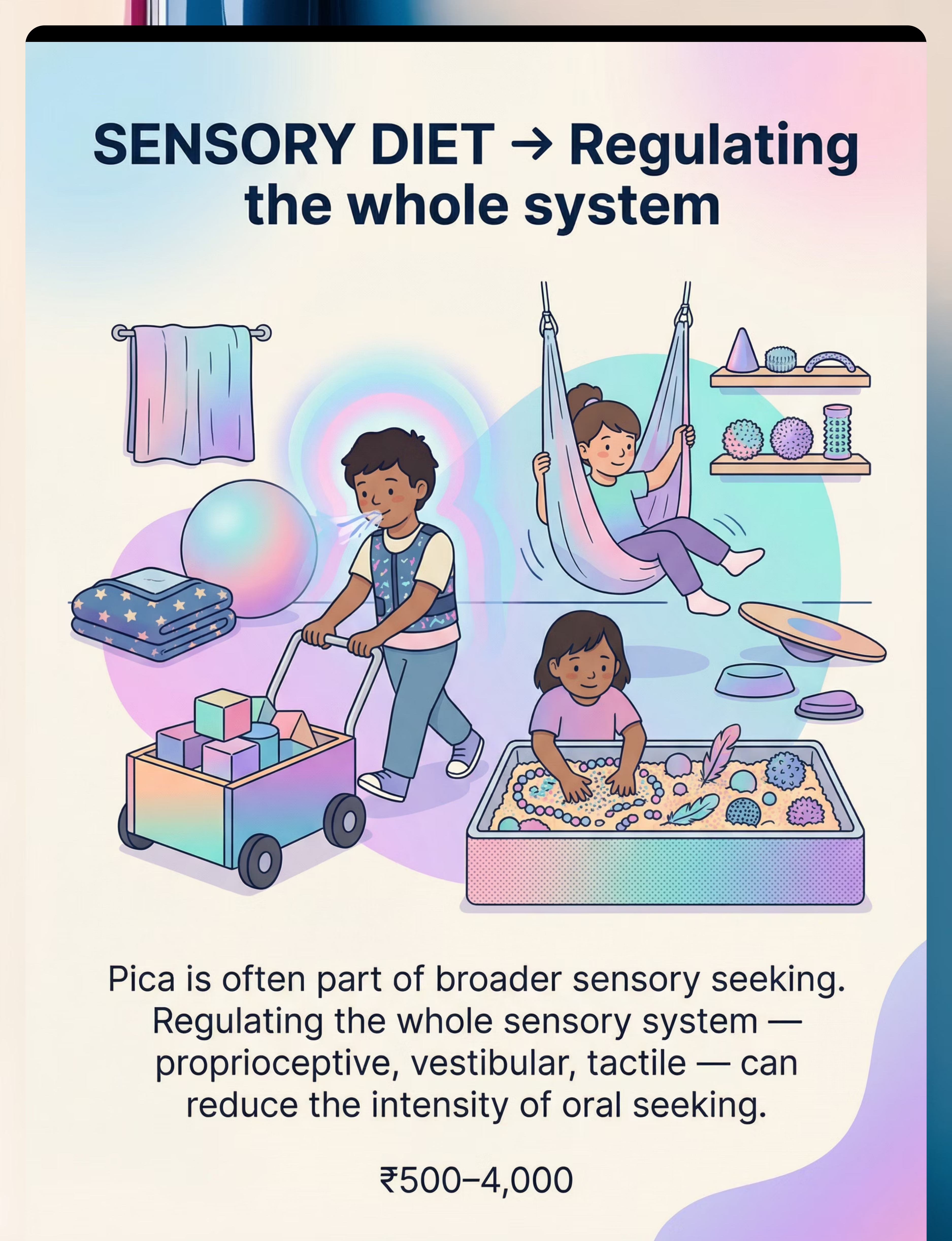
Material 6 — Sensory Diet Tools (Full Body)
Canon: Sensory Processing Tools
OT Sensory Diet
₹500–4,000
Pica is rarely an isolated oral behaviour. It almost always exists within a broader landscape of sensory dysregulation. When the entire sensory system — proprioceptive, vestibular, tactile — is chronically under-regulated, the mouth becomes the primary seeking outlet. A comprehensive sensory diet that addresses whole-body regulation reduces the intensity and urgency of oral seeking by meeting the nervous system's input needs through safer, broader channels.
What to Source
- Weighted blankets and weighted lap pads (deep pressure)
- Compression vest or body suit (proprioceptive grounding)
- Mini trampoline for indoor vestibular input
- Therapy balls (large Physio balls for rolling / bouncing)
- Sensory tactile bins: kinetic sand, water beads, rice bins (supervised)
- Body sock or lycra compression tunnel
- Heavy work tools: weighted bags, indoor push/pull cart
⚠️ Safety Note
Sensory diet design requires OT assessment. Incorrect intensity can dysregulate further rather than regulate. Start low, observe carefully.
💡 DIY Zero-Cost Version
Bear hugs, joint compressions, climbing stairs repeatedly, pushing a laundry basket, carrying groceries — heavy work is everywhere and costs nothing. A rolled-up yoga mat provides deep pressure. Sandpit play is outdoor proprioception.

Material 7 — Medical Monitoring & Nutritional Supplies
Canon: Medical Management Tools
Clinical Necessity
₹300–2,000+
Pica is a behavioural and medical condition. Iron and zinc deficiencies are directly associated with pica through dopaminergic pathway disruption. Non-food items consumed can cause poisoning, intestinal obstruction, parasitic infection, and dental damage. Medical monitoring is not optional — it is the parallel clinical track that runs alongside every behavioural intervention.
What to Source
- Ingestion tracking log (paper or digital) — dates, items, estimated amounts
- Emergency medical information card (laminated) — child's name, condition, contact, poison control
- Nutritional supplements as medically prescribed (iron, zinc, multivitamin)
- Medical alert identification (bracelet or card)
- First aid supplies for oral injuries
- Poison control number accessible in every room: 1800-116-117 (India)
🚨 SEEK IMMEDIATE MEDICAL ATTENTION
For ingestion of any toxic substance, sharp object, or large material that could obstruct the digestive tract. Do not wait for symptoms to appear.
Poison Control India: 1800-116-117
💡 DIY Zero-Cost Version
A printed daily log sheet. An index card with emergency information laminated. A photo folder on your phone of items the child targets. All free. All essential.

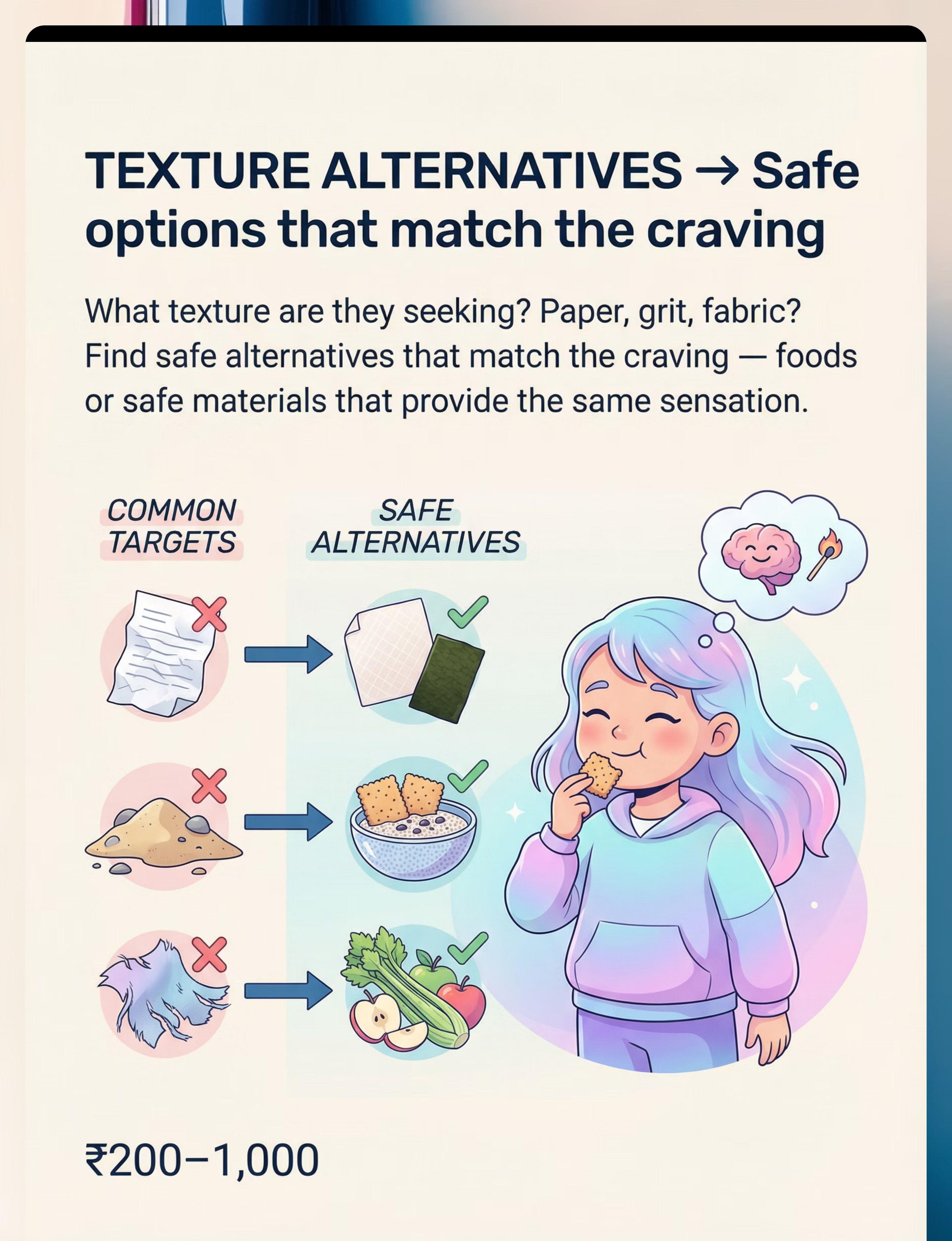
Material 8 — Safe Texture & Material Alternatives
Canon: Texture Alternatives
Sensory Substitution
₹200–1,000
Children with pica often seek specific textures, not just "something to eat." A child who eats paper is seeking fibrous texture. A child who eats dirt craves granular pressure and earthy taste-smell combinations. When you identify the specific sensory quality being sought and provide a safe alternative that matches it, you can redirect the behaviour without eliminating its neurological driver.
Paper Seekers
Rice paper (edible) or nori/dried seaweed — safe, fibrous, edible alternatives matching thin, fibrous texture
Dirt / Gravel Seekers
Textured crackers (ragi crackers, multigrain wafers), chia pudding, or oatmeal — for dense, grainy texture needs
Clay / Dough Seekers
Edible playdough (flour, salt, water) safely matches the texture and manipulation qualities of clay
Fabric / Thread Seekers
Safe fibrous snacks (celery, raw carrot), food-grade silicone texture mats for oral exploration without ingestion
⚠️ Safety Note: Texture matching works best when sensory texture is the primary pica driver. Functional assessment must confirm this before relying on this strategy alone. Always run a brief Functional Behaviour Assessment (FBA) in parallel.

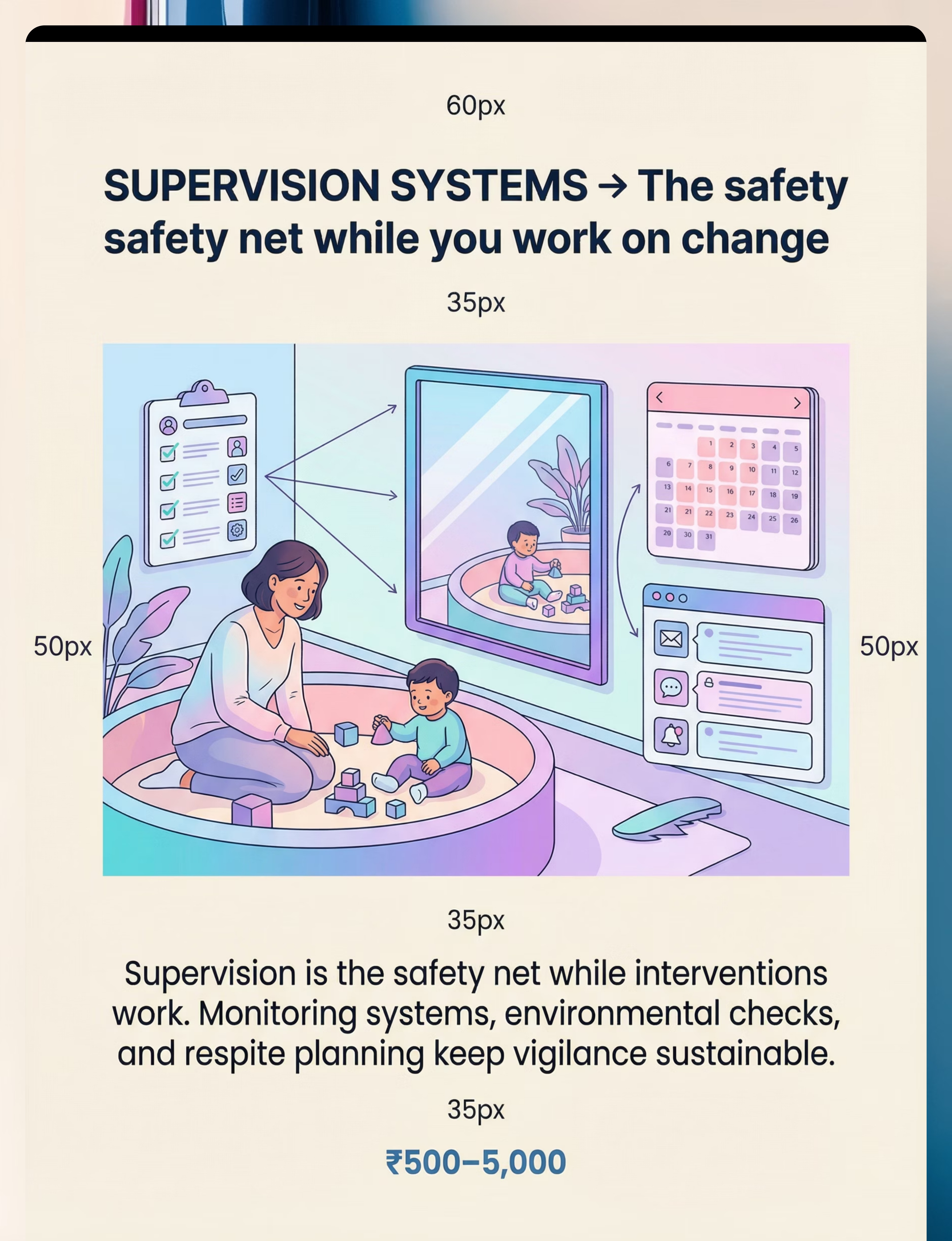
Material 9 — Supervision & Monitoring Systems
Canon: Safety Monitoring Systems
Caregiver Infrastructure
₹500–5,000
No intervention eliminates the need for supervision while it works. Supervision is not a failure of intervention — it is what keeps your child alive while the interventions take effect. The challenge is that no single caregiver can sustain constant vigilance indefinitely without systemic support. Monitoring systems extend your awareness, build in redundancy, and make sustainable vigilance possible.
What to Source
- Indoor monitoring cameras for high-risk zones (bathroom, bedroom, play area)
- Wall-mounted mirrors to extend visual field
- Environmental check checklists (morning, afternoon, evening scans)
- Communication logs between home and school
- School monitoring plan (shared with all staff)
- Respite care schedule — caregiver mental health is a clinical necessity
- Baby monitor for overnight pica risk
⚠️ Critical Note on Caregiver Fatigue
Supervision fatigue is real and documented. An exhausted caregiver is not a safe caregiver. Plan respite as you plan meals — non-negotiably. Your wellbeing is your child's safety.
💡 DIY Zero-Cost Version
Rearrange furniture so primary play areas are in direct sightlines from kitchen and work areas. Use physical barriers instead of electronic monitoring. Establish a neighbourhood/family "supervision rotation" for high-risk hours.
Every Family Can Start Today — Regardless of Budget
WHO/UNICEF equity principle: No child should wait for therapy because their family cannot access a shop. The science does not require a budget. It requires consistency, attention, and the right knowledge. All three are free.
Material | Commercial (₹) | DIY Zero-Cost Version | |
Chew Tools | ₹300–1,500 | Food-grade frozen damp cloth; silicone kitchen spatula (non-breakable) | |
Environmental Safety | ₹500–3,000 | Rope ties; furniture repositioning; remove all targets to locked room | |
Oral-Motor Exercise | ₹400–2,000 | Thick smoothies through thin straws; blowing bubbles; raw carrot sticks | |
Discrimination Training | ₹200–800 | Hand-drawn food/not-food sorting cards; household items as practice set | |
Replacement Tools | ₹200–1,000 | Printed visual cue cards; verbal praise; ziplock bag portable kit | |
Sensory Diet | ₹500–4,000 | Bear hugs; carrying heavy bags; stair climbing; outdoor sandpit | |
Medical Monitoring | ₹300–2,000+ | Paper log; phone photo folder; printed emergency card | |
Texture Alternatives | ₹200–1,000 | Kitchen items: rice paper, ragi crackers, chia seeds, raw vegetables | |
Supervision Systems | ₹500–5,000 | Mirror placement; furniture rearrangement; family rotation schedule |

🛑 Read This Before Any Pica Intervention
🚨 RED — IMMEDIATE MEDICAL EMERGENCY (Stop. Call. Go.)
If your child has ingested ANY of the following — act NOW, do not delay: Batteries (any type) • Cleaning products, bleach, disinfectants • Medications (prescription or OTC) • Sharp objects (glass, metal, pins, needles) • Large quantities of any non-food material • Paint chips (lead poisoning risk)
Poison Control India: 1800-116-117 — Nearest Emergency Department: Go immediately.
If your child has ingested ANY of the following — act NOW, do not delay: Batteries (any type) • Cleaning products, bleach, disinfectants • Medications (prescription or OTC) • Sharp objects (glass, metal, pins, needles) • Large quantities of any non-food material • Paint chips (lead poisoning risk)
Poison Control India: 1800-116-117 — Nearest Emergency Department: Go immediately.
🟡 AMBER — Modify or Consult
- Child has active infection, fever, or is unwell — postpone all sessions
- Child is in crisis (active meltdown, severe dysregulation) — provide safety, not protocol
- Unknown ingestion history — medical clearance before introducing any oral tools
- Severe oral motor impairment — SLP assessment before introducing chew tools
- OCD component suspected — psychology review before behavioural intervention alone
🟢 GREEN — Proceed Conditions
- Medical evaluation completed within last 3 months
- Blood panel (iron, zinc) reviewed by paediatrician
- Environmental modification audit completed
- All caregivers briefed on the plan
- Emergency information card prepared and posted

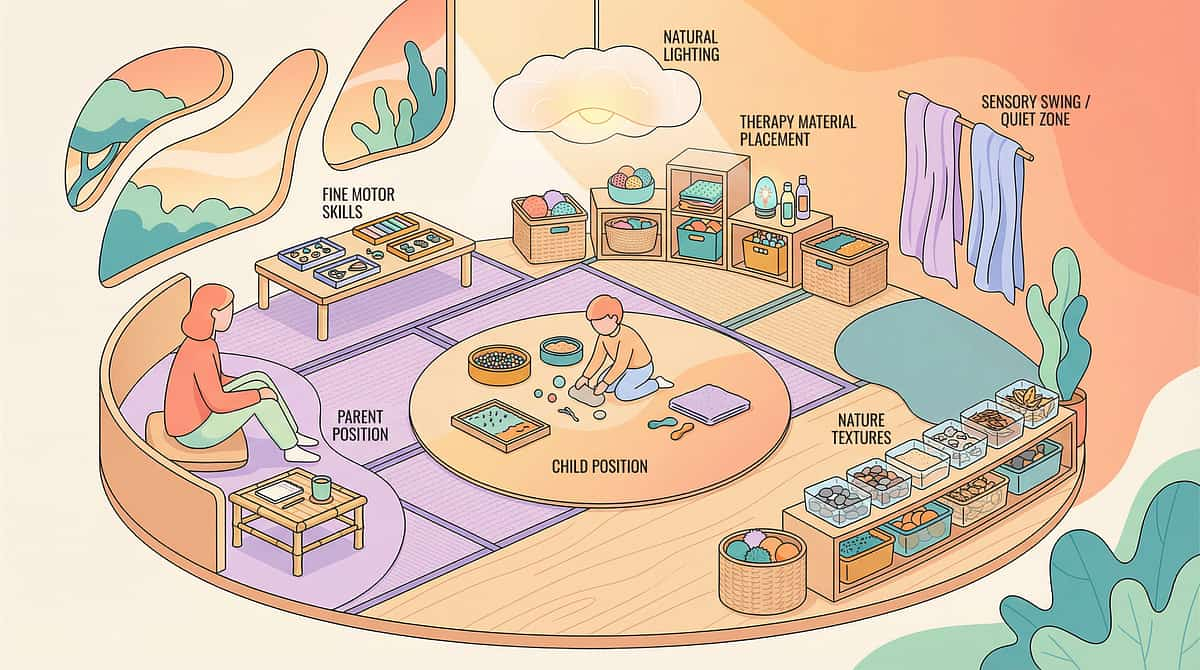
The Right Environment Makes Every Session Work Better
A well-prepared space removes the variables that can derail a session before it begins. Think of the setup as your first intervention — before you've even said a word to your child.
Room Setup Checklist
- All non-food pica targets removed or secured before session begins
- Chew necklace/tool already on child before session starts
- Visual cue card for replacement behaviour posted at child eye level
- Reinforcement items ready and accessible to parent
- Discrimination training materials laid out
- Monitoring camera active if used
- Phone off/silent — full attention to child during session
- Session duration timer set (10–20 minutes)
Sensory Environment
Lighting
Soft natural light preferred; avoid harsh fluorescent
Sound
Low background noise; no competing screens
Temperature
Comfortable; child not overheated (overheating increases seeking)
Space
Sufficient floor space for movement if needed
60-Second Readiness Assessment — Before Every Session
The best session is one that starts right. Run this quick check before every session — it takes under a minute and saves significant disruption.
Check | 🟢 GO | 🟡 MODIFY | 🔴 POSTPONE | |
Physical state | Fed, rested, no signs of illness | Mildly tired but calm | Fever, hunger, clearly unwell | |
Emotional regulation | Calm or mildly alert | Slightly elevated but redirectable | Active distress or meltdown | |
Recent pica incident | None in past 30 minutes | Minor incident, child re-regulated | Active or recent dangerous ingestion — medical check first | |
Oral seeking intensity | Baseline or low | Moderate seeking present | Intense, uncontrollable — provide chew tool first, session after | |
Environment | All targets removed | Minor oversight — fix before proceeding | Not safe — do not start | |
Caregiver state | Calm, focused | Somewhat stressed but manageable | Significant distress — get support first |
🟢 4+ Green → PROCEED
Full session as planned
🟡 2+ Yellow → MODIFY
Shorten duration, use easier version
🔴 Any Red → POSTPONE
Safety and regulation first, session after

Step 1: The Invitation — Begin Without Demand
Step 01 of 06
Duration: 30–60 seconds
Approach the child calmly in their current play space. Do not interrupt an ongoing activity. Position yourself at the child's level (floor if necessary). Make the chew necklace or safe alternative visually available — hold it, don't force it.
The Exact Words to Say
"Hey [name], I have your chewy necklace. Would you like to put it on? We're going to do something fun."
For non-verbal or minimally verbal children: Hand chew necklace to child. Point to neck. Use visual cue card showing child wearing necklace. Wait 5 seconds. If accepted — praise immediately. If not — place on tray within reach and proceed anyway.
Child Acceptance Cues
- Takes item willingly or tolerates placement
- Orients to the activity with neutral or positive affect
- Reduced seeking behaviour in the preceding 2 minutes
Child Resistance — What to Do
- Pushes away → Move item to reach-accessible spot; don't force; begin discrimination activity instead
- Avoidance → Increase pairing sessions (fun = chew necklace) before integration
- Distress → Postpone; provide safe sensory calming first
ABA Principle — Pairing: Establish the chew tool as a reinforcing object through association with positive interactions before using it as a replacement behaviour tool. The necklace must mean "fun" before it can mean "safe."

Step 2: The Engagement — Introduce Therapeutic Material in Play
Step 02 of 06
Duration: 1–3 minutes
Bring out the discrimination training cards or texture alternatives. Make it a game — not a lesson. "Let's sort these!" or "Which of these would taste good?" Place items on the mat. Let the child initiate exploration.
Material Introduction Sequence
01
Present discrimination cards face-up
02
Model the sort
"Apple → food!" [place in food box] "Crayon → not food!" [place in not-food box]
03
Offer cards to child to sort
04
Provide immediate feedback
Enthusiastic for correct sort; calm redirection for incorrect
Oral-Motor Integration (Parallel)
If the chew necklace is on: note whether child is spontaneously using it. If oral seeking behaviour arises during engagement, use this as a natural teaching moment:
"When you feel that feeling in your mouth — use your necklace."
Reinforcement Begins Now
Every correct discrimination sort → immediate verbal praise + token if using token economy. "Yes! Apple is food! High five!"

Step 3: The Core Intervention — Multi-Modal Simultaneously
Step 03 of 06
Duration: 5–12 minutes active therapeutic time
The pica intervention protocol runs THREE concurrent threads in every session. This is where the real work happens — all three must run together for maximum effect.
Thread A — Oral Sensory Provision
Chew necklace/tool remains accessible throughout. Parent monitors oral seeking signals and proactively offers the chew tool before the urge escalates. Script: "I can see you're feeling that way — here's your necklace."
Thread B — Discrimination Training
5–10 card sorts per session, progressing through levels: L1 (obvious food vs. non-food) → L2 (similar-looking items) → L3 (items child historically targets) → L4 (novel generalization items)
Thread C — Replacement Behaviour Practice
When oral seeking arises during the session, use it as a teaching moment. Show visual cue card: "Instead of [pointing to unsafe item] → [point to chew necklace]." Guide the redirect. Reinforce with highest available reinforcer.
Common Execution Errors to Avoid
❌ Rushing the card sort — slow down; comprehension is the goal
❌ Providing chew tool as reaction only — proactive provision is more effective
❌ High-stakes response to a pica attempt during session — calm redirect, no drama
❌ Running all three threads intensely simultaneously — prioritise by child's energy level
Step 4: Repeat & Vary — Where the Neural Pathway Forms
Step 04 of 06
Repetition is not redundancy — it is neuroscience. Studies on pica discrimination training show meaningful generalisation begins at 3–4 weeks of daily practice. The variation menu keeps sessions engaging while the repetition builds the pathway.
Thread | Daily Repetitions | Weekly Sessions | Notes | |
Chew tool availability | Continuous / all waking hours | 7 days | Always on or within reach | |
Discrimination training | 10–20 card sorts | 5–7 days | Short bursts preferred | |
Replacement behaviour practice | At every pica attempt + 2 structured practices | Daily | Triggered + planned | |
Sensory diet activities | 3–5 heavy work/sensory input bursts | 7 days | Throughout the day |
Variation Menu (to maintain engagement)
- Change the card sets — use photos of items in your own home
- Change the "not food" objects being sorted (introduce new targets)
- Move the session to a different room (generalisation training)
- Include a sibling or caregiver variation (partner practice)
- Outdoor generalisation: practise discrimination in garden, playground
"3 correct, enthusiastic card sorts are worth more than 15 forced, resistant ones."
Step 5: Reinforce & Celebrate — Timing Is Everything
Step 05 of 06
The Rule: Within 3 seconds of any safe behaviour replacing pica → reinforce immediately, specifically, enthusiastically.
For correct discrimination sort:
"YES! That is NOT food! Amazing thinking! High five!"
"YES! That is NOT food! Amazing thinking! High five!"
For spontaneous chew necklace use:
"I saw you feel that feeling and you reached for your necklace! That is exactly right! You did it!"
"I saw you feel that feeling and you reached for your necklace! That is exactly right! You did it!"
For successful redirect from pica attempt:
"You stopped and chose your necklace instead. That was BRAVE. Token earned."
"You stopped and chose your necklace instead. That was BRAVE. Token earned."
Reinforcement Menu (find what works for your child)
Social
High fives, spinning, cheering, tickles, hugs
Token
Stickers, stamps, chips toward preferred activity
Access
2 min preferred screen, favourite toy, outdoor time
Sensory
Vibration toy, deep pressure, movement break
Food
Preferred snack — immediate, specific, small
Critical ABA Principle: Celebrate the ATTEMPT to use the safe alternative — not just the success. The attempt is the neural pathway being built.
Step 6: The Cool-Down — End Well, Every Time
Step 06 of 06
Duration: 2 minutes
Every ending shapes the next beginning. A consistent, predictable cool-down builds the routine that makes your child willing — and eventually eager — to return to the next session.
Transition Warning (30 seconds before ending)
"Two more cards, then all done. You're doing so well." Show visual timer counting down if available.
Wind-Down Activity (60 seconds)
Choose ONE: firm shoulder massage while child holds chew necklace — OR weighted blanket drape for 60 seconds — OR slow deep breathing together (3 counts in, 4 counts out) — OR quiet sit together, no demands, child-led.
Material Put-Away Ritual (30 seconds)
"Help me put the cards away. You did such good work today." Let child participate — motor closure creates a sense of completion.
Bridge to Next Session
"Tomorrow we'll practise again. Today you made two safe choices. That's two more than yesterday."
If child resists ending: Do not extend the session — use token: "One more card, then all done. Extra token." Follow through immediately. Predictable endings reduce resistance over time.

Capture the Data — Right Now
60 seconds of data now saves hours of guessing later. Record the following within 60 seconds of the session ending, while your observations are fresh.
Daily Pica Log — Pinnacle D-419
Date: _________________ Pica incidents today (count): ___
Items targeted: _________________
Safe chew tool uses observed: ___ Discrimination sort accuracy (%): ___
Replacement behaviour used (Y/N): ___ Session duration (minutes): ___
Child regulation at end (1–5): ___ Notes: _________________
Why This Data Matters
- Early detection of plateau or regression requiring protocol adjustment
- Evidence for medical providers and school teams
- Progress documentation for insurance and funding applications
- Contribution to India's largest paediatric behavioural safety dataset
"I did it. I recorded today's session. That data is going to help my child."

Nothing Went Right Today — And That's Data Too
"Session abandonment is not failure. It is a precise description of what needs to change." Use this troubleshooting guide whenever a session doesn't go as planned.
Child refused the chew necklace entirely
Why: Insufficient pairing; necklace not yet reinforcing.
Fix: Spend 5 days "pairing" — bring out necklace only during highly preferred activities. Never require it. Associate it with fun.
Fix: Spend 5 days "pairing" — bring out necklace only during highly preferred activities. Never require it. Associate it with fun.
Child sorted every card as "food"
Why: Concept of "not food" not yet established.
Fix: Return to concrete Level 1 pairs (apple vs. brick). Never advance until 80% accuracy at current level.
Fix: Return to concrete Level 1 pairs (apple vs. brick). Never advance until 80% accuracy at current level.
Pica incident during session
Why: Oral seeking exceeded safe outlet; unsafe item in environment.
Fix: Audit environment again. Increase chew tool availability. Do not dramatise the incident — calm redirect and record it.
Fix: Audit environment again. Increase chew tool availability. Do not dramatise the incident — calm redirect and record it.
Child became upset when chew tool was presented
Why: Negative association (previously forced); sensory texture mismatch.
Fix: Try different texture/resistance. Let child explore tool without using it. Never force oral contact.
Fix: Try different texture/resistance. Let child explore tool without using it. Never force oral contact.
No pica during session but incidents increased outside session
Why: Intervention containment — not yet generalising to other contexts.
Fix: Increase chew tool availability across all environments. Run brief (3-minute) discrimination practice in 3 different rooms this week.
Fix: Increase chew tool availability across all environments. Run brief (3-minute) discrimination practice in 3 different rooms this week.
Parent became frustrated and raised voice
Why: This is one of the most stressful behaviours a parent manages.
Fix: Stop the session. Breathe. Your frustration is data about YOUR support needs, not your child's failure. Call 9100 181 181 for parent coaching support.
Fix: Stop the session. Breathe. Your frustration is data about YOUR support needs, not your child's failure. Call 9100 181 181 for parent coaching support.

No Two Children Are Identical — Personalise Everything
The protocol described throughout this page is a framework, not a rigid script. Your child's unique sensory profile, age, verbal capacity, and specific pica targets should shape every element of how you implement it.
Oral SEEKER (craves intense input)
- Use firmest resistance chew tools available
- Prioritise heavy oral-motor exercise before discrimination training
- Increase frequency: discrimination training 4× daily in short bursts
- Introduce proprioceptive whole-body heavy work alongside oral intervention
Oral AVOIDER (defensive)
- Begin with visual-only discrimination training (no oral component initially)
- Pair chew tool with highest preferred reinforcer before expecting use
- Use vibrating tools at extremely low intensity to desensitise
- Consult SLP before proceeding
Limited Verbal / Non-Verbal
- Increase visual supports (picture exchange for "chew this instead")
- Add tactile cue: gentle tap on necklace = signal to use it
- Reduce language demands; increase modelling
Older Children (ages 9–12)
- Discreet chew options (pencil toppers, bracelets that look like jewellery)
- Self-monitoring checklists rather than parent-administered training
- School-integrated supports with privacy maintained
- Cognitive-behavioural discussion if understanding is present
Age Modifications: Ages 2–4: Environmental modification + chew tools ONLY; no formal discrimination training yet. Ages 5–8: Full protocol as described. Ages 9–12: Age-appropriate, dignity-preserving adaptations above.

Weeks 1–2: Safety First, Foundations Second
Progress: ~15%
Weeks 1–2
Week 1–2 is about establishing safety and beginning the foundations of change. Do not expect dramatic visible improvement yet — the groundwork being laid in these weeks is what makes everything else possible.
✅ You WILL See
- Gradual acceptance of chew tool during sessions (not necessarily outside yet)
- First correct discrimination sorts (food vs. obvious non-food)
- Environmental modification reducing access to key targets
- Your own increased confidence from having a plan
⏳ You WON'T See Yet
- Spontaneous chew tool use without prompting
- Reduction in overall pica attempts (may temporarily increase as items are removed)
- Generalised discrimination to novel environments
- Independent replacement behaviour
🔴 Common Week 1–2 Crisis: The week you remove environmental access to targets may show a spike in agitation and alternate seeking. This is expected. This is the sensory system protesting the removal of its outlet. It passes. Maintain chew tool availability intensively during this period.
0%
Baseline established
Pica incident count tracked from Day 1
30%
Chew tool acceptance
Target: 30% of offers accepted by end of Week 2
60%
Discrimination accuracy
Target: 60% at Level 1 by end of Week 2

Weeks 3–4: The Neural Pathway Is Forming
Progress: ~40%
Weeks 3–4
These are the signs most parents miss — because they're looking for the wrong things. Watch for the subtleties.
The Breakthrough Moment
Child reaches for chew necklace before a pica attempt — not just after. This proactive reach is the single most significant early indicator that the protocol is working at a neurological level.
The Hesitation
Child begins to hesitate before picking up a known pica target. Awareness is emerging — the prefrontal cortex is beginning to register the conflict between impulse and rule.
Discrimination Progress
Sorting accuracy reaches 70–80% at Level 1; beginning Level 2. Pica incidents reduced by 20–30% from baseline. Child begins to anticipate discrimination card sessions.
The Parent Shift
By Week 3–4, most parents report reduced acute terror (replaced by informed vigilance), growing confidence that the intervention is working, and a first moment of thinking: "We might actually get through this."
If Not Progressing: No shame, no failure. Call Pinnacle: 9100 181 181. A BCBA or OT will review the data and adjust. Most plateaus at Week 3–4 are protocol fit issues, not child capacity issues.

Weeks 5–8: The Behaviour Is Changing at Its Root
Progress: ~75%
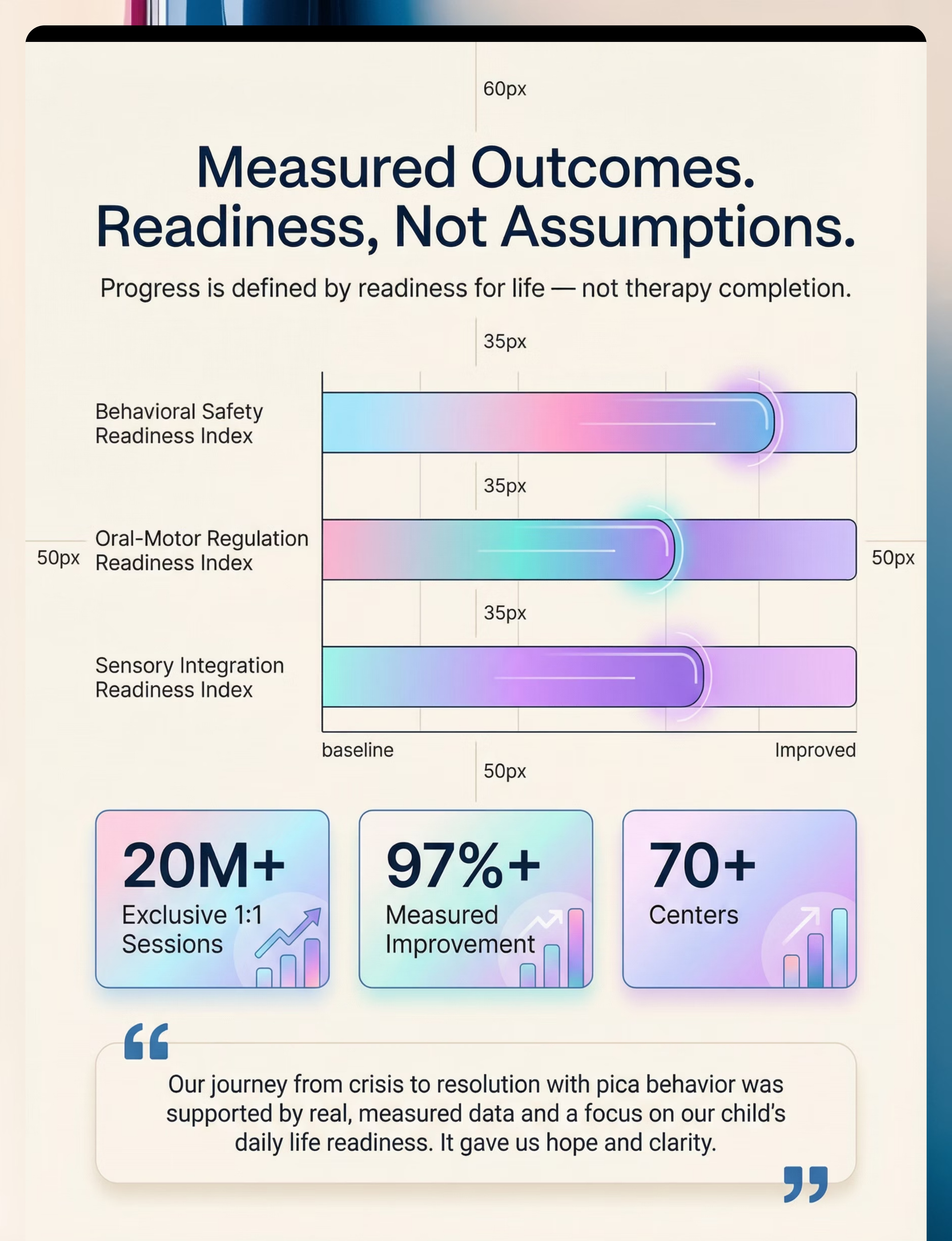
🏆 Behavioural Safety Readiness — Progressing
By weeks 5–8, you are no longer managing a crisis. You are watching a child build a new capability. The behaviour is changing not because you are blocking it — but because the neural alternatives are becoming stronger.
Mastery Criterion | Threshold | |
Pica incident frequency | Reduced ≥50% from baseline | |
Chew tool use | Spontaneous use observed in 3+ contexts without prompting | |
Discrimination accuracy | 80%+ at Level 2; beginning Level 3 | |
Replacement behaviour | Child initiates safe alternative in ≥50% of observed urge moments | |
Environmental independence | Functioning safely in 2+ environments without maximum supervision |
🏠 Home Badge
Safe in home without maximum supervision
🏫 School Badge
Teacher reports pica reduction with alternative use
🌳 Community Badge
Safe at playground with standard supervision
🛒 Independence Badge
Child uses chew tool independently without prompting
You Did This.
You spent weeks watching your child constantly. You removed every dangerous item from every room. You researched, implemented, adjusted, and tried again. You called the helpline when you needed help. You recorded data even on the days you were exhausted. You are not the same parent who read Card 01 in terror.
"You have reduced dangerous non-food ingestion. You have given your child a safe alternative. You have built a discrimination skill that did not exist before. These are real neurological changes in a real brain — changes you caused."
Your child is safer today than they were 8 weeks ago. That is your work.
🎉 Family Celebration
Do something your child loves today — purely celebratory, no therapy agenda. Let them feel your joy.
📝 Journal Prompt
"Write one sentence: What was different this week? What did I see my child do that I couldn't have imagined on Week 1?"
🤝 Share Progress
Join the Pinnacle community and share your milestone — your story will become someone else's hope.

🚨 Pause and Seek Professional Consultation If You See These
Red Flag | What It Looks Like | Action | |
Ingestion escalation | Pica incidents increasing despite 3+ weeks of consistent intervention | Immediate BCBA consultation — functional reassessment needed | |
New or more dangerous targets | Child shifts to targeting batteries, medications, sharp objects | Emergency medical evaluation + BCBA/medical co-consult | |
Severe distress around chew tools | Child becomes extremely agitated when chew tool is presented | SLP assessment for oral defensiveness; do not force | |
Complete absence of progress at week 6 | No measurable change in any tracking metric | Protocol review with Pinnacle therapist — not a failure, a signal | |
Caregiver breakdown | Caregiver not coping — sleep deprived, in crisis | STOP. Respite care immediately. Parent mental health is a clinical necessity. | |
Medical symptoms | Vomiting, abdominal pain, unusual stool, weight loss, extreme fatigue | Immediate paediatric evaluation — GI complications possible |
Escalation Pathway: Self-resolve (minor, seen before) → Adapt per Personalisation card → Teleconsultation within 48 hours → Clinic visit → Emergency: 1800-116-117
"Trust your instincts. If something feels wrong, it is worth a phone call. Every time."
Where You Are. Where You're Going. The Full Journey.
Cluster: Behavioural Safety — Oral Regulation Series
D-417
Understanding Oral Sensory Seeking
D-418
When Mouthing Continues Beyond Toddlerhood
D-419 — YOU ARE HERE
9 Materials That Help With Pica Behaviour
D-420
Medical Complications of Pica — what to monitor, when to act
D-421
Building Oral Regulation Skills — from crisis management to long-term independence
D-425
Sensory Diet Fundamentals — systemic sensory regulation
Branching Paths From D-419
Sensory driver primary
→ Proceed to D-421: Building Oral Regulation Skills
Medical complications concern
→ Proceed to D-420: Medical Complications of Pica
Broader sensory seeking
→ Branch to D-425: Sensory Diet Fundamentals
Behavioural function unclear
→ Teleconsult for Functional Behaviour Assessment
More Tools for Your Child's Oral Safety Journey
Technique | Code | Difficulty | Canon Material | Link | |
Understanding Oral Sensory Seeking | D-417 | 🟢 Intro | Chew Tools | ||
When Mouthing Continues Beyond Toddlerhood | D-418 | 🟢 Intro | Oral-Motor Tools | ||
Medical Complications of Pica | D-420 | 🟡 Core | Medical Monitoring | ||
Building Oral Regulation Skills | D-421 | 🟡 Core | Chew Tools + OT | ||
Sensory Diet Fundamentals | D-425 | 🟡 Core | Sensory Diet Tools | ||
ABA Functional Assessment for Challenging Behaviours | D-380 | 🔴 Advanced | Behavioural Tools |
"Materials You Already Own" Indicator: If you completed the materials cards in this page, you already own materials for D-417, D-418, and D-421. You can start any of these today.
From the Pinnacle Network: Real Journeys, Measured Outcomes
Anonymised. Outcomes vary by child profile. Illustrative of clinical patterns seen across the Pinnacle Network.
Asha, Hyderabad — Boy, 7 years, ASD + pica targeting batteries and grout
Before (Week 0):"Three ER visits in one month. I stopped leaving any room. I followed him everywhere. I was terrified every single day. I didn't know there was a word for what he was doing."
After (Week 10):"He wears his chew necklace now. He reaches for it himself. The last ER visit was 9 weeks ago. I still watch him — I always will — but I'm watching with a plan now, not with terror."
Therapist's Notes: Functional assessment identified strong oral sensory drive. Chew tools providing equivalent input reduced pica incidents by 67% within 8 weeks. Discrimination training at Level 3 by week 10.
Priya, Bengaluru — Girl, 5 years, pica targeting fabric and thread
Before (Week 0):"She had eaten the stuffing from two pillows. Her teachers didn't know what to do. I was ashamed to explain it to anyone."
After (Week 12):"The school has a protocol now. She has a chew bracelet that looks like jewellery. No incidents in 6 weeks. She's in a regular classroom."
Therapist's Notes: Texture matching — nori and textured crackers matched the fibrous quality she sought in fabric. Combined with discrimination training and OT sensory diet, the behaviour resolved in this specific functional category.
Rahul, Delhi — Father, child 9 years, pica targeting soil and plaster
Before:"I thought my son was doing it to provoke me. I was angry for two years. Then a BCBA at Pinnacle explained the function. The anger left immediately."
After:"Understanding why changed everything. Once we addressed the sensory need and the iron deficiency — his ferritin was critically low — the behaviour resolved within 6 weeks of supplementation plus the protocol."

Watch: 9 Materials That Help With Pica Behaviour
The Reel that surfaced this challenge — now with the full protocol behind it.
D-419 Reel
Series: Safety & Challenging Behaviours — Episode 419
Domain: Behavioural Safety / Oral-Motor / Sensory Processing
Duration: 75–85 seconds
Domain: Behavioural Safety / Oral-Motor / Sensory Processing
Duration: 75–85 seconds
The Reel gives you the 9 materials in 75 seconds. This page gives you the science, the protocol, the troubleshooting, and the community behind every one of those materials. Both are necessary. The Reel surfaces the knowledge. The page delivers the mastery.
Related Reels in This Series
About This Content
"This content is produced by India's largest consortium of paediatric therapists — OT, SLP, BCBA, Special Educators, and NeuroDev Paediatricians — unified under GPT-OS®. Every recommendation on this page has been reviewed, validated, and aligned with WHO/UNICEF evidence standards. This is not social media content. This is clinical knowledge designed to be used."
Pinnacle Blooms Consortium | OT • SLP • ABA • SpEd • NeuroDev
Preview of 9 materials that help with pica behavior Therapy Material
Below is a visual preview of 9 materials that help with pica behavior therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!
The Pinnacle Promise
"From fear to mastery. One technique at a time."
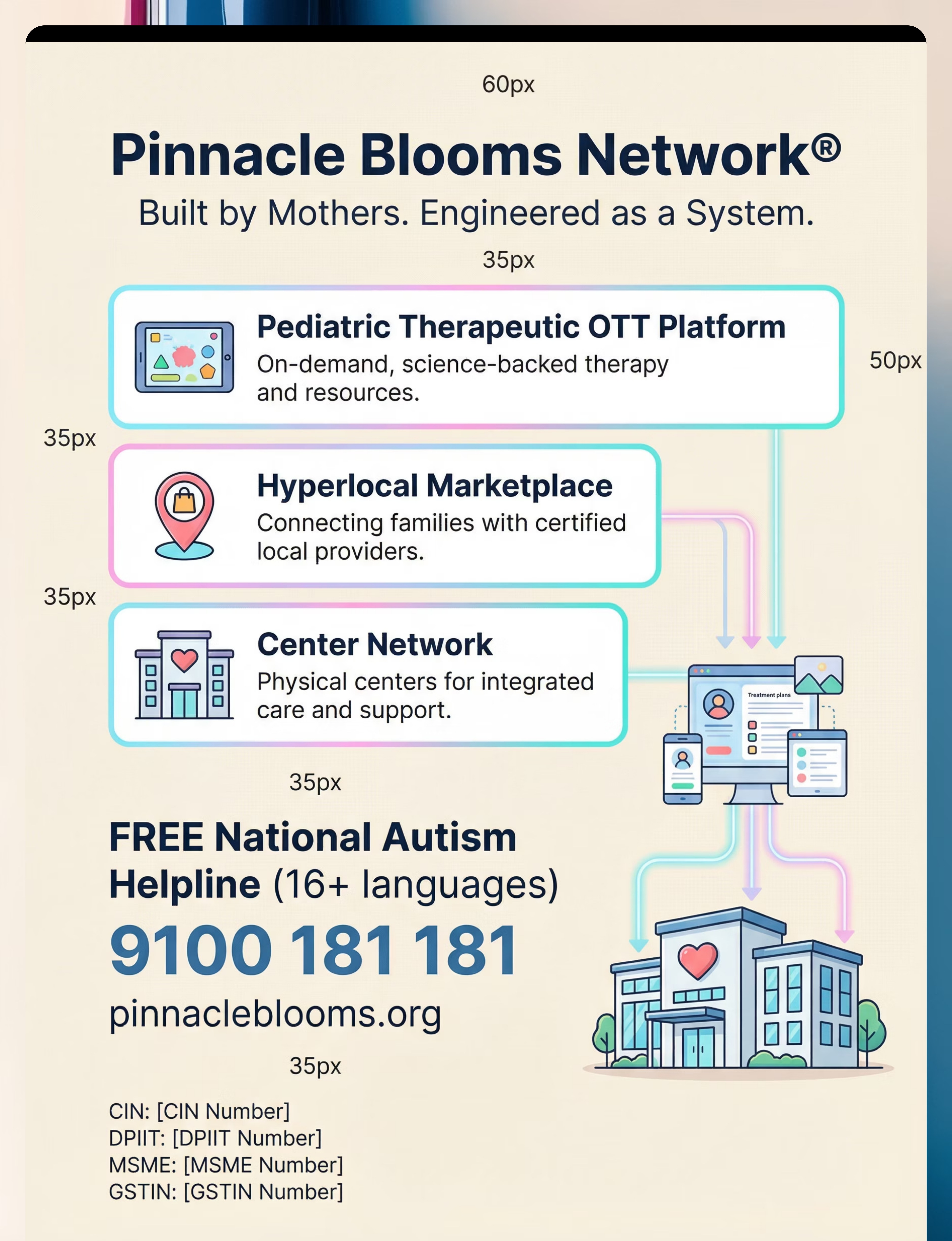
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System.
OT • SLP • ABA/BCBA • Special Education • NeuroDev Paediatrics • CRO
WHO/UNICEF-grade evidence | 20M+ Sessions | 97%+ Measured Improvement | 70+ Centres
OT • SLP • ABA/BCBA • Special Education • NeuroDev Paediatrics • CRO
WHO/UNICEF-grade evidence | 20M+ Sessions | 97%+ Measured Improvement | 70+ Centres
Disclaimer: This content is educational. It does not replace individualised assessment and intervention planning with licensed behavioural specialists, occupational therapists, speech-language pathologists, and medical providers. Pica requires comprehensive evaluation to identify underlying causes and medical monitoring for complications. Seek immediate medical attention for ingestion of toxic, sharp, or obstructive materials. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
1
Statutory Identifiers
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
2
Next Recommended Technique
D-420: Medical Complications of Pica — What to Monitor and When to Act
→ techniques.pinnacleblooms.org/behavioral-safety/pica-medical-complications-D-420
→ techniques.pinnacleblooms.org/behavioral-safety/pica-medical-complications-D-420
3
Copyright
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™ are registered trademarks.