
"My child works so hard at the clinic. At home, I feel helpless."
The therapist sends you home with a program and a list of exercises. You have a willing heart, a resistant child, and absolutely no equipment. The days between sessions feel like wasted time.
You are not failing. Your child's therapy doesn't stop at the clinic door — it lives in your home, your routines, your hands. And with the right 9 materials, you can become the extension of your child's physical therapist that changes everything.
Pinnacle Blooms Consortium®
GPT-OS® Validated
Ages 0–18
Physical Therapy Domain
FREE National Helpline: 9100 181 181 | Available 24×7 | 16+ Languages
Millions of families navigate home PT with no equipment and no roadmap.
If you have stood in your living room with a prescribed exercise sheet and no idea where to start — you are among the majority. This is not a parenting failure. It is a knowledge and access gap.
1 in 6
Children Need Therapy
Children in India require physical or developmental therapy before age 5 (WHO Global Disability Report 2023)
<50%
Home Programs Completed
Of home exercise programs are completed consistently without structured support (Journal of Pediatric Rehabilitation, 2022)
3×
Faster Progress
Faster progress observed in children whose parents complete home programs with appropriate equipment (Pinnacle GPT-OS® Real-World Evidence: 20M+ sessions)
Physical therapy works best as a continuous process: clinic expertise + home consistency = maximum outcomes. The question is never whether home practice matters. It always does. The question is: what do families actually need to make it work?

"The clinic session opens the door. Home practice is what walks through it."
Understanding what happens in your child's body and brain makes the difference between reluctant compliance and genuine conviction.
How Motor Learning Works
- Motor Cortex — plans movement
- Cerebellum — coordinates timing
- Spinal Motor Neurons — execute
- Muscles + Joints — perform and report back
- Proprioceptors — send success signal
- Loop repeats → pathway strengthens
Each repetition at home thickens the myelin sheath around motor pathways — making movements faster, smoother, and more automatic.
What happens in a clinic session
Your child's physical therapist introduces a new motor challenge. The brain creates a new neural pathway. Muscles fire in new patterns. That pathway is thin, fragile, new.
What happens without home practice
Without repetition, thin neural pathways fade within 48–72 hours. The clinic session essentially resets each time.
What happens with consistent home practice
Each repetition reinforces the pathway. Myelin thickens with repetition. By weeks 4–6, movements that required intense focus happen automatically. This is neurophysiology — not a metaphor.

"Your child is here. Home PT extends the clinic's reach across 23 hours a day."
Physical therapy is not a stage — it is a thread woven through every phase of your child's development. Here is where home practice fits across the entire timeline.
0–12 Months
Foundation Movement: tummy time, rolling, sitting
1–2 Years
Gross Motor Emergence: walking, climbing, balance
2–4 Years
Motor Consolidation: running, jumping, coordination
4–7 Years
Motor Skill Refinement: sport-ready movements, fine control
7–12 Years
Functional Mobility: school, sports, independence
12–18 Years
Performance & Adaptation: functional independence, sports
"Your child attends PT 1–3 hours per week. There are 165+ other waking hours. What happens in those hours determines how fast the therapy works."
PT supports children with: Cerebral Palsy | Hypotonia | Developmental Coordination Disorder | Post-Surgical Rehabilitation | Autism (motor component) | Down Syndrome | Spina Bifida | Orthopedic Conditions | General Developmental Motor Delay
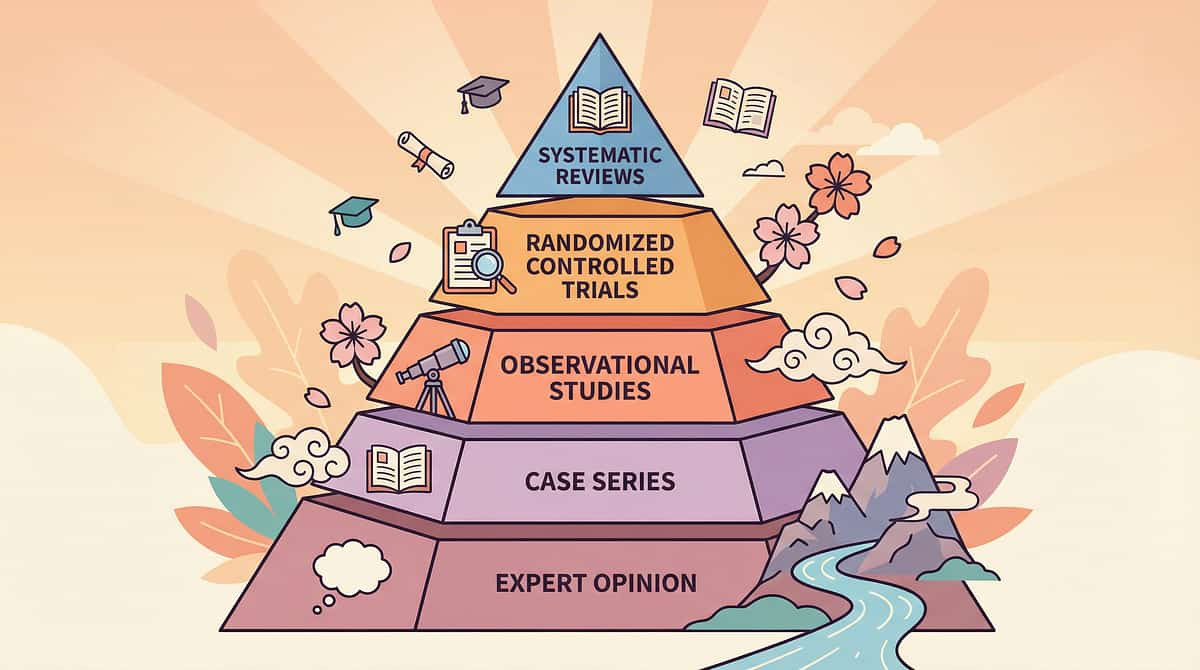
Home Physical Therapy with Appropriate Equipment: Evidence Grade I.
Level I Evidence
Systematic Review Grade | Home-Based Motor PT | 16+ Studies | 2013–2024
The Core Finding
Children who complete structured home PT with appropriate equipment show 2–3× faster motor skill acquisition compared to clinic-only programs.
The Adherence Science
Without equipment: completion below 50%. With equipment + structured protocols: completion rises to 78–85%. Materials are the mechanism.
India-Validated RCT
Padmanabha et al., Indian J Pediatr (2019): Home-based structured interventions showed statistically significant outcomes across motor domains within 8–12 weeks.
88%
Evidence Confidence
Based on 16 studies, 3 systematic reviews, WHO/UNICEF alignment
PubMed Verified
WHO-Aligned
NCAEP 2020 Listed
India-Validated
Pinnacle 20M+ RWE
9 Materials That Help With Physical Therapy at Home
The Home PT Toolkit
A curated set of 9 physical therapy materials that replicate or supplement the therapeutic tools used in clinical PT sessions — enabling families to execute prescribed home exercise programs effectively, safely, and consistently. Each material addresses a specific therapeutic function: floor exercise foundation, core activation, balance training, strength building, tissue mobility, motor planning, or behavioral adherence.
Therapy Exercise Mat
Floor exercise foundation
Therapy Ball (Swiss Ball)
Core, balance, vestibular
Resistance Bands
Graduated strength training
Balance Board
Proprioception, reactive balance
Foam Roller
Tissue mobility, deep pressure
Step Platform
Leg strength, gait patterns
Crawling Tunnel
Motor planning, shoulder stability
Wrist / Hand Weights
Upper body strength, proprioception
Visual Timer + Exercise Cards
Adherence, routine, regulation

"This toolkit is used across 5 therapy disciplines — because the brain doesn't organize by therapy type."
Physical Therapist — Primary Lead
Prescribes the home program, selects equipment, teaches execution. Uses all 9 materials — the therapeutic backbone of the home program. "The PT is the architect. These materials are the building blocks."
Occupational Therapist — Secondary
Functional integration of motor skills into daily activities. Uses therapy mat, foam roller, wrist weights for sensory-motor integration. "OT uses PT materials to connect motor gains to self-care independence."
ABA/BCBA — Behavioral Support
Reinforcement structures that make the home program happen. Uses visual timer, exercise cards, reinforcement menus. "ABA ensures the program gets done — motivation + structure + data."
Special Education — Coordination
Integrates motor readiness into school participation. Uses balance board, step platform, coordination materials. "Motor readiness directly predicts classroom attention and learning readiness."
Neurodevelopmental Pediatrician — Oversight
Medical supervision, contraindication assessment, outcome tracking. Informs equipment choices based on neurological profile. "The medical mind behind the physical program."
"When your child's PT, OT, ABA therapist, and teacher are all aware of the home program materials, therapeutic benefit multiplies. Consistency across caregivers is the force multiplier."

Material 1: Therapy Exercise Mat
Canon: Motor/Physical Therapy Equipment
Material #1 of 9
The therapy mat is the foundation for all floor exercises in your child's home PT program. It defines the workout space, protects joints, and signals to your child that "this is where we do our exercises" — creating a consistent environmental cue that improves session compliance over time.
Specifications
Thickness: ≥1.5cm | Non-slip surface | Easy-clean material essential
Price Range
₹1,500–4,000 | Search: "Therapy Exercise Mat for Kids" on Amazon.in
Therapeutic Use
Prone exercises, supine exercises, rolling, bridging, pushing to sit — the universal base

Material 2: Therapy Ball (Swiss Ball / Physio Ball)
Canon: Balance & Vestibular Equipment
Material #2 of 9
The therapy ball is perhaps the most versatile single tool in the home PT toolkit. It delivers core activation, balance challenge, and vestibular input simultaneously — making it the workhorse of most pediatric PT home programs. Anti-burst construction is non-negotiable for child safety.
Ages 3–5
45 cm ball | Parent-supported sitting | Gentle bounce
Ages 5–10
55 cm ball | Semi-supported to unsupported sitting | Reaching activities
Ages 10+
65 cm ball | Full balance challenges | Eyes-closed progression
Price Range: ₹800–2,500 | Search: "Anti-Burst Therapy Ball for Children" on Amazon.in

Material 3: Resistance Bands Set
Canon: Strengthening Equipment
Material #3 of 9
Color-coded resistance bands provide graduated, adjustable strength training that grows with your child. The color progression also serves as a powerful motivator — children naturally want to "level up" to the next color, turning therapeutic compliance into a self-directed goal.
Choose a Set with 4+ Resistance Levels
Color-coded from lightest to heaviest. Always start with the lightest available — form over resistance, always.
Key Exercises
Seated rows (pull toward chest), shoulder press (band under feet, press up), lateral step walks (band around ankles), standing hip abduction
Dosage
8–12 reps × 2–3 exercises per session | 2–3 minutes per muscle group
Price Range: ₹300–1,200 (set) | Search: "Therapy Resistance Bands Set" on Amazon.in
Material 4: Balance Board / Wobble Board
Canon: Balance & Proprioceptive Equipment
Material #4 of 9
The balance board is the dedicated tool for reactive balance and proprioceptive development — training the ankle, knee, and hip systems to respond automatically to instability. This skill transfers directly to real-world falls prevention, outdoor terrain navigation, and sports participation.
Beginner: Rocker Board
Rocks in one plane (front-to-back OR side-to-side). Ideal for children starting balance training or those with significant balance challenges. Non-slip surface essential.
Advanced: Wobble Board
Moves in all directions simultaneously. Introduces once rocker board is mastered. Wall or parent support available at all times. Progress: eyes open → eyes closed → with ball toss.
Price Range: ₹1,000–4,000 | Search: "Balance Board for Kids Therapy" on Amazon.in
Material 5: Foam Roller
Canon: Myofascial / Sensory Equipment
Material #5 of 9
The foam roller serves triple duty in pediatric PT: tissue mobility work, deep pressure sensory input, and balance challenge. For children with increased muscle tone, it supports myofascial release under PT guidance. For sensory seekers, the deep pressure input is regulating and organizing.
Specifications for Children
Soft density (not the firm adult version) | 45cm or 90cm length | Half-round roller for beginners — safer entry point than a full cylinder
Key Uses
Gentle rolling along quad/hamstring muscles | Prone over roller for back extension (thoracic only) | Sitting balance challenge on roller placed lengthwise
Critical Safety Rule
Never roll over joints, lower back, or bony areas. Always 3–5 slow passes per muscle group. Pause if child shows pain.
Price Range: ₹600–2,000 | Search: "Soft Foam Roller for Children" on Amazon.in

Material 6: Step Platform / Aerobic Step
Canon: Functional Strength Equipment
Material #6 of 9
The step platform builds functional leg strength and gait patterns in the most transferable way possible — because stepping up and down is exactly what your child does on every staircase, curb, and bus step they encounter in daily life. This is therapy that lives in the real world immediately.
1
Begin at 10–15 cm height
Adjustable height is essential. Start low, build confidence. Focus on controlled movement — no "plopping" down.
2
Core Exercises
Step-up with leading leg, controlled step-down | Lateral step-ups | Calf raises off step edge | Progress to single-leg stance at top
3
Dosage
8–10 step-ups per leg, alternating leading leg | 2–3 sets | Visual cue: "Heel to toe — land softly"
Price Range: ₹1,500–4,000 | Search: "Adjustable Aerobic Step Platform" on Amazon.in
Material 7: Crawling Tunnel
Canon: Motor Planning / Crawling Equipment
Material #7 of 9
The crawling tunnel is the most reliably engaging material in the entire toolkit — and one of the most therapeutically rich. Crawling builds shoulder stability, bilateral coordination, motor planning, and proprioceptive awareness simultaneously. For many children, it is the entry point that transforms resistance into enthusiasm.
Motor Planning
Child must organize their body to navigate the enclosed space — a complex motor planning challenge in a fun package
Shoulder Stability
Weight-bearing through arms during crawling builds the upper body foundation for writing, sports, and self-care
Bilateral Coordination
Cross-pattern crawling integrates both sides of the brain — foundational for reading and writing readiness
Dosage: 5–10 crawl-throughs per session at child's own pace. Progress: place motivating toy at exit, add obstacle at entry, try backwards crawl. Price Range: ₹1,000–3,500 | Search: "Play Tunnel Crawl Tube for Kids" on Amazon.in

Material 8: Wrist / Hand Weights (Child-Sized)
Canon: Resistance / Proprioceptive Input Equipment
Material #8 of 9
Child-sized wrist weights provide upper body strengthening and enhanced proprioceptive input — the sensory information from muscles and joints about body position and force. For children with hypotonia or proprioceptive processing differences, gentle weighted input is organizing and regulating, in addition to building strength.
Starting Weight
0.25 kg maximum for children under 6 | 0.5 kg for older children | Adjustable preferred | Form first — weight second, always
Key Exercises
Bicep curls | Shoulder press (arms up overhead) | Lateral raises (arms out to sides) | Functional: worn during meal preparation activities
Dosage
8–12 reps per exercise × 1–2 sets | 2–3 minutes per exercise | Excellent form required before increasing weight
Price Range: ₹400–1,500 | Search: "Child Wrist Weights Adjustable" on Amazon.in

Material 9: Visual Timer + Exercise Picture Cards
Canon: Behavioral Support / Adherence Tools
Material #9 of 9
The visual timer and exercise cards are the behavioral engineering layer of the home PT toolkit. They answer the child's two biggest questions during therapy: "How much longer?" and "What comes next?" — replacing anxiety and resistance with predictability, autonomy, and a sense of progress.
Visual Timer (Time Timer recommended)
Shows a shrinking red disc — the child can see exactly how much time remains. Position at child's eye level. Eliminates "how much longer?" completely.
Exercise Picture Cards
Laminated cards with a picture of each exercise. Child selects the first card, completes exercise when timer ends, moves card to "DONE" pile. Choice + agency = engagement.
Session Structure
2–3 minutes per card | Full session: 10–20 minutes | Visual cue: "When the red is all gone, that exercise is done. Pick the next card!"
Price Range: ₹200–1,500 | Search: "Visual Timer for Kids" + "Exercise Flashcards Children" on Amazon.in

"Every child deserves physical therapy. Not every family can order from Amazon."
Here is the zero-cost version — validated by the WHO Nurturing Care Framework across 54 low- and middle-income countries. The therapeutic principle is preserved in every alternative below.
Material | Clinical Version | DIY / Household Alternative |
Therapy Mat | Thick foam mat (₹1,500+) | Interlocking foam tiles OR camping pad + non-slip rug pad |
Therapy Ball | Anti-burst Swiss ball (₹800+) | Large beach ball partially deflated — supervise closely |
Resistance Bands | Color-coded bands (₹300+) | Old bicycle inner tube cut into strips; thick rubber bands tied together |
Balance Board | Wobble board (₹1,000+) | Sturdy board on half-PVC pipe; or thick folded blanket |
Foam Roller | Foam roller (₹600+) | Pool noodle OR tightly rolled yoga mat secured with tape |
Step Platform | Aerobic step (₹1,500+) | Sturdy bottom stair + non-slip mat; stacked books with rubber mat |
Tunnel | Pop-up tunnel (₹1,000+) | Row of chairs with blanket draped over; large cardboard boxes end-to-end |
Wrist Weights | Child weights (₹400+) | Sock filled with rice/sand (250–500g), velcro around wrist |
Visual Timer | Time Timer (₹500+) | Sand hourglass timer; phone timer with large display facing child |
"The DIY alternatives are not inferior. They are the same therapy principle executed with household materials. WHO's Nurturing Care Framework was designed and validated in 54 low- and middle-income countries using exactly this approach: therapeutic principles over commercial products."
Safety First: Every Session Starts Here.
Safety is not a formality — it is the protocol. Sixty seconds of assessment before each session prevents injury, protects progress, and builds your clinical confidence as a home PT practitioner.
🔴 DO NOT PROCEED IF:
- Child is unwell, feverish, or recovering from illness
- Child has had a seizure in the last 24 hours
- Open wound, active fracture, or unhealed surgical site
- Therapist has advised cessation of specific exercises
- Child is severely dysregulated or in meltdown
- Post-surgical: outside the prescribed exercise window
🟡 MODIFY AND PROCEED WITH CAUTION IF:
- Child is tired but not unwell — shorten session, reduce intensity
- Child is anxious or resistant — use invitation protocol
- Using DIY materials for the first time — test stability first
- Child has high muscle tone — foam rolling needs PT guidance
- New material introduced — start with passive observation
🟢 PROCEED WHEN:
- Child is fed (wait 30 minutes post-meal for active exercises)
- Child is rested and in a calm/alert regulated state
- Environment is set up per setup guidelines
- Safety surfaces are non-slip and clear of obstacles
- Parent has reviewed the exercise instructions

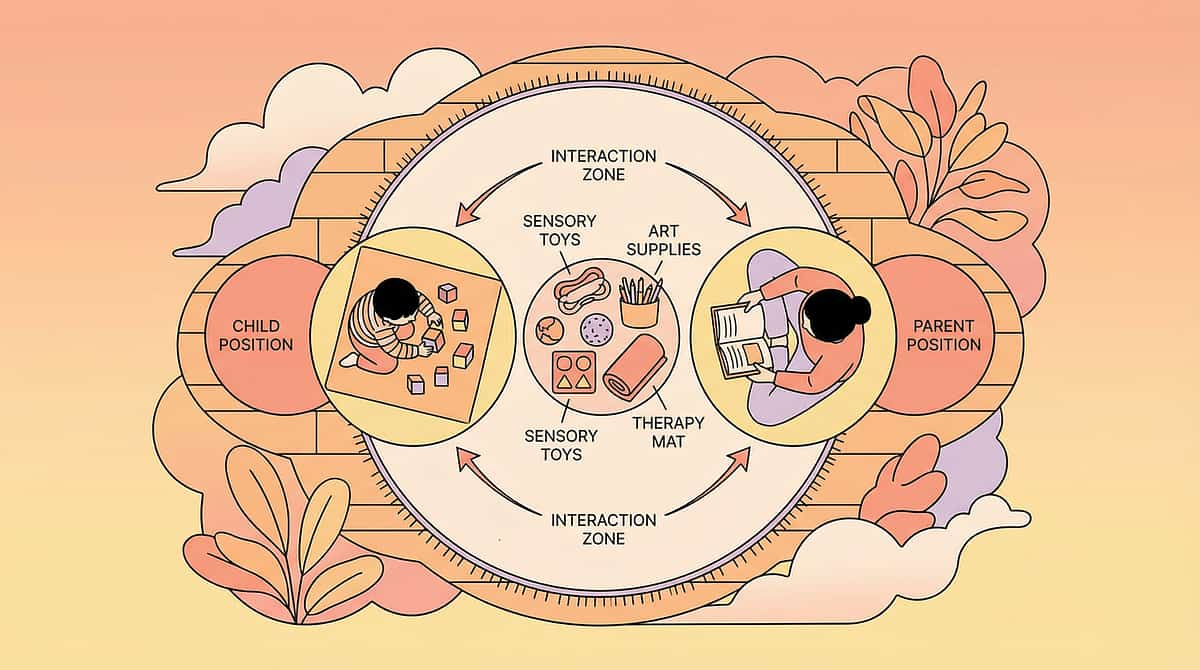
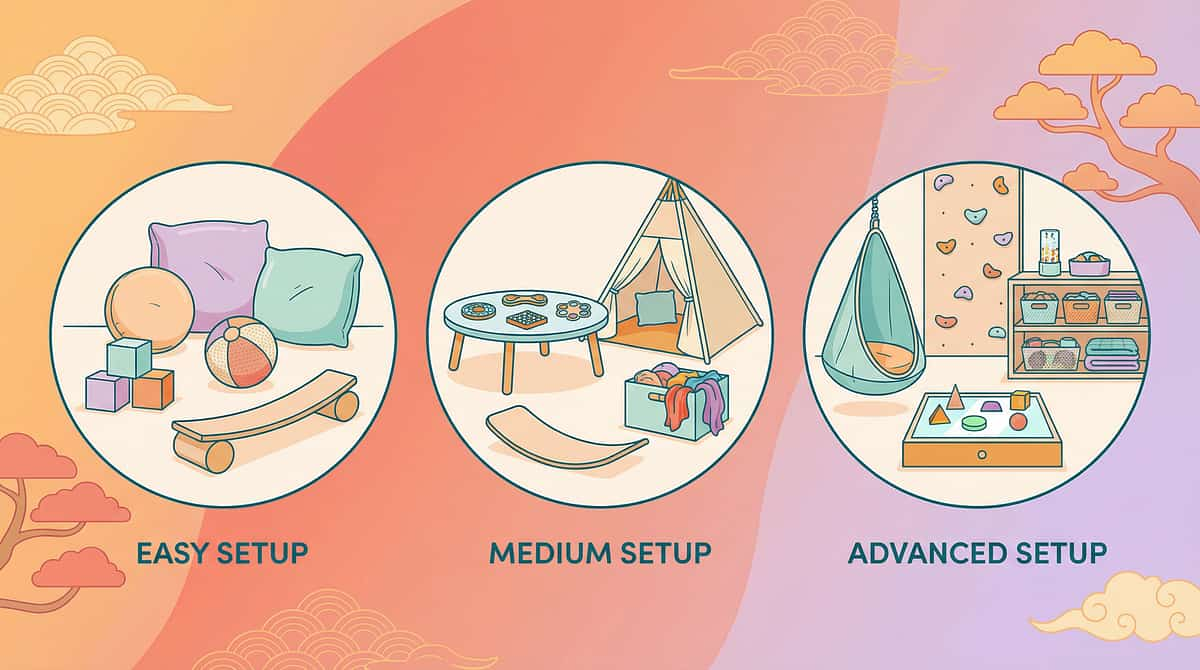
"The right environment makes the therapy happen. The wrong one makes it fail."
1
Clear a 3m × 3m Minimum Floor Space
Remove furniture edges, sliding rugs, and sharp objects from the exercise zone before bringing your child in.
2
Place Therapy Mat in Center
This is the child's primary exercise zone. Add non-slip rug pad underneath if the floor is slippery.
3
Position Support Within Reach
Wall, sturdy chair, or parent within arm's reach for all balance exercises. Never leave the child unsupported on a balance board.
4
Set Visual Timer at Child's Eye Level
Child must see the countdown during all exercises. This is non-negotiable for the timer to function therapeutically.
5
Remove Distractions
TV off, phone on silent, siblings in a separate space if possible. Competing attention fractures engagement.
6
Sensory Considerations
Natural light preferred over fluorescent flicker | Quiet or low-volume background music | Allow brief material exploration before exercise begins | Have a sensory break corner available if needed
"60 seconds now prevents 20 minutes of struggle later."
Step 0 — Pre-Session Readiness Check
Before every session, run this 7-point check. Your child's state in this moment is the single strongest predictor of session success. The best session starts from the right conditions — not forced compliance.
Check | 🟢 Go | 🟡 Modify | 🔴 Postpone |
Fed? | 30+ min post-meal | 20 min post-meal | Just eaten / hungry |
Slept? | Well-rested | Mild tiredness | Overtired / just woke |
Health? | Well | Minor sniffles | Unwell / feverish |
Mood? | Calm-alert | Slightly unsettled | Dysregulated |
Engagement? | Approaches materials | Needs invitation | Strong avoidance |
Injury/Pain? | None | None | Any pain complaint |
PT Alert? | No concerns | Note modification | Pause per PT guidance |
ALL GREEN → Proceed
Move to Step 1: The Invitation
MOSTLY AMBER → Modify
Shorter duration. Remove most challenging material. Simplified protocol.
ANY RED → Postpone
Offer calming alternative. Record the skip and reason. Try again later today or tomorrow.
"The session that starts right is the session that produces data. A forced session produces resistance. You are not behind if you postpone once — you are being clinically intelligent."

Step 1: Invite, Don't Command.
① of ⑥
The Invitation — 30–60 seconds
The child's willingness is the therapeutic input. How you begin the session determines whether the next 15 minutes are productive therapy or a battle of wills. The invitation protocol is research-backed — offering choice increases buy-in by 60%.
"Hey [child's name] — I've got something interesting set up. Want to come see?"
Wait 10–15 seconds. Do not repeat. Allow the child to come.
"Look — the therapy mat is ready. Should we start with the ball today, or the stepping game?"
Body Language Checklist
Get to child's level (kneel or sit) | Point to setup, not the child | Relaxed posture — not "exercise mode" urgency | Have one material already in your hands as a curiosity activator
If Child Ignores
Wait 30 seconds more. Demonstrate an action with the material yourself. Children are drawn to adult activity.
If Child Verbally Refuses
"Okay, that's fine. I'm going to do it anyway — you can watch from there." Proceed with your own demonstration. Curiosity usually wins.
If Child Physically Avoids
Note this in your data. Do NOT force. Try again at a different time today. This is data, not failure.
Step 2: The Child Is Here. Now Introduce the Material — Slowly, Curiously.
② of ⑥
The Engagement — 1–3 minutes per material

Therapy Ball Engagement
"This is the therapy ball — it's big and bouncy. Should I show you what it does first?" Demonstrate sitting on it yourself. Bounce gently. Make it look enjoyable. Then offer the ball and guide child to sit.

Balance Board Engagement
"This board is a little wobbly — look! Want to try standing on it?" Stand on it yourself first. Show the wobble. Children are drawn to the unstable. Hold child's hands for first attempt.

Resistance Bands Engagement
"This stretchy band — pull here and here and see what happens." Demonstrate the stretch visually. Make it interesting. Child performs with your light guidance on hand position.
Step 3: The Active Ingredient. This Is Where Therapy Happens.
③ of ⑥ — 50% Progress
Therapeutic Action — 10–20 minutes total
Each material has a specific therapeutic action protocol. Below are the core actions for all 9 materials. Follow your PT's prescribed sequence — these are the general protocols for reference.
Therapy Mat
Prone pushups → roll to supine → bridges (hips up) → roll to side → push to sitting. 5–8 reps per exercise, 3–5 min. Cue: "Push the floor away."
Therapy Ball
Sit with feet flat → reach to sides → lean forward/back with parent steadying → progress to unsupported. 3–5 min. Progress: 5 sec → 15 sec → 30 sec. Cue: "Tall spine, crown to ceiling."
Resistance Bands
Arms: seated row + shoulder press. Legs: lateral step walks + hip abduction. 8–12 reps per group. 2–3 min per muscle group. Cue: "Slow and controlled — the resistance is the teacher."
Balance Board
Stand with parent support → progress hands-free → ball toss while balancing → single-leg → eyes closed. 10 sec → 30 sec → 60 sec holds. Cue: "Soft knees — let your ankles do the work."
Foam Roller
Gentle rolling along quads/hamstrings → prone over roller for back extension → sitting balance on lengthwise roller. 3–5 slow passes per muscle group. Never over joints or lower back.
Step Platform
Step-up leading leg → controlled step-down → lateral step-ups → calf raises off edge → single-leg stance. 8–10 reps per leg × 2–3 sets. Cue: "Heel to toe — land softly."
Tunnel
Crawl through at own pace → progress with toy at exit → obstacle at entry → backwards crawl. 5–10 repetitions. Cue: "Big bear crawl — hands and knees, strong arms."
Wrist/Hand Weights
Bicep curls → shoulder press → lateral raises → functional wear during activities. 8–12 reps × 1–2 sets. Start: 0.25 kg max for under 6. Form first — always.
Visual Timer + Cards
Child selects exercise card → parent sets 2–3 minute timer → on completion, card moves to "DONE" pile → child selects next. 10–20 min total session. Cue: "When the red is all gone, pick the next card!"

Step 4: 3 Quality Repetitions Beat 10 Forced Ones. Dose Is Everything.
④ of ⑥ — 67% Progress
Repeat & Vary
The quality of neural pathway formation depends on the quality of movement — not the count. Rushed, poorly-formed repetitions do not build the same pathways as slow, deliberate, well-cued ones.
Repetition Guide by Material
- Therapy Mat: 5–8 reps × 2–3 exercises
- Therapy Ball: 3–5 min sustained / 5–10 balance holds
- Resistance Bands: 8–12 reps × 2–3 exercises
- Balance Board: 10–30 sec holds × 5–8 reps
- Foam Roller: 3–5 slow passes per muscle group
- Step Platform: 8–10 step-ups per leg × 2–3 sets
- Tunnel: 5–10 crawl-throughs
- Weights: 8–12 reps × 1–2 sets
Variation to Maintain Engagement
- Ball: sitting → prone → supine → rolling → balance play
- Balance Board: eyes open → eyes closed → with ball toss → with music
- Bands: different anchor points → different movement planes
- Step: forward → lateral → step-down → calf raise
- Tunnel: straight → reversed → with obstacle → timed
Satiation Indicators
- Decreased speed and quality of movement
- Requests to stop (honor this — record how far you got)
- Distraction increases significantly
- Physical signs of fatigue: heavy breathing, reduced coordination
"3 excellent repetitions with full effort and genuine engagement are therapeutically superior to 10 rushed, poorly-formed repetitions. Science rewards quality."
Step 5: Celebrate Every Attempt. The Brain Learns What Gets Praised.
⑤ of ⑥ — 83% Progress
Reinforce & Celebrate
For Physical Effort
"Yes! I saw how hard you pushed! That was STRONG!"
For Persistence
"You kept going even when it was hard. That is exactly what builds strength."
For Balance Achievement
"You held that for [X] seconds! Last time it was [Y]. You are getting better every day!"
For Completing Cards
"Every card done! That's a full workout. Your physical therapist is going to be so proud."
⏱️ Within 3 Seconds
Deliver reinforcement immediately after the target behavior — the 3-second window is the research standard
🎯 Specific
Name the behavior, not just "good job." Specific praise builds the exact neural pathway you want reinforced
🔊 Calibrated
Enthusiastic but not overwhelming — read the child's arousal state and match energy accordingly

Step 6: No Session Ends Abruptly. The Transition Is Part of the Therapy.
⑥ of ⑥ — Session Complete ✓
The Cool-Down
Step A — The Warning (2 minutes before end)
"Two more [exercises/repetitions/tunnels], and then we're all done for today." Show on visual timer: 2 minutes remaining. Hold up 2 fingers as physical cue.
Step B — The Calming Exercise (60–90 seconds)
Choose ONE: Slow supported stretching on therapy mat | Gentle foam roller under knees in supine | Slow deep breathing: "Breathe in for 3... hold for 2... out for 4..." | Child-initiated: "Pick one calm stretch to finish"
Step C — The Ritual (30–45 seconds)
"Let's put everything away together. Which one should we put back first?" Child participates in material put-away. Final: "All done! That was an excellent workout."

"60 Seconds of Data Now Saves Hours of Guessing Later."
Your physical therapist makes adjustments based on what you report. Vague reports get vague adjustments. Specific data gets specific, targeted program improvements. Sixty seconds of tracking is a clinical act.
1
Session Completion
Full (all exercises done) | Partial — which exercises? | Skipped — reason?
2
Child Engagement Level
[1] Refused ◆ [2] Tolerated ◆ [3] Participated ◆ [4] Engaged ◆ [5] Enthusiastic
3
Notable Observation (one sentence)
First time balanced on board independently | Refused foam roller today | Increased speed through tunnel
"Session Abandonment Is Not Failure. It Is Data. Here Is How to Read It."
Every difficult session tells you something actionable. Use these troubleshooting pairs to convert frustration into clinical information that improves the next session.
Child refused the balance board completely
Why: New material, vestibular uncertainty, sensory processing difference. Fix: Place board in the room for 3 days without using it. Demonstrate yourself. Build tolerance in micro-steps: room presence → passive observation → hand touching → single foot contact → standing.
Child falls off balance board dangerously
Why: Challenge level too high for current balance ability. Fix: Return to mat. Practice single-leg standing on flat surface first. Use foam balance pad before wobble board. Child must show 10-second single-leg stand before board work resumes.
Child refuses therapy ball — cries when it appears
Why: Vestibular hypersensitivity — the ball's movement is aversive. Fix: Introduce ball as a seat object first (ball chair for meals). No movement initially. Progress to gentle parent rocking with child in lap. Consult PT or OT for sensory-specific protocol.
Child only wants the tunnel — refuses everything else
Why: The tunnel is highly reinforcing (good!). Fix: Use this. "First resistance bands, then tunnel." Turn the child's preference into the motivator for the full program. Preference is leverage — not a problem.
Child says exercises hurt
Why: Potential actual pain, avoidance language, or effort discomfort mistaken for pain. Fix: Stop immediately. Assess for swelling, facial distress, guarding. If yes: call 9100 181 181. If behavioral: describe the sensation together. Always report to PT.
Child does exercises perfectly once, refuses the next day
Why: Normal variability; may be setting-event issue (tired, post-school). Fix: Track days and times — identify patterns. Good days and bad days are expected. The trend over weeks matters, not single-session performance.
"I can't remember the correct technique — I'm doing it wrong"
Why: Parent training gap — this is a system failure, not a parent failure. Fix: Print or screenshot exercise photos. Ask PT to video-record demonstration at next session. Call 9100 181 181 for parent coaching support.
"No Two Children Are Identical. This Program Bends to Your Child — Not the Other Way Around."
Individualized intervention planning is foundational across all therapy disciplines. Evidence consistently shows personalized dosing outperforms fixed protocols. Use the modifications below based on your child's profile today.
⬅ EASIER Modifications
For: Sensory Avoider / Low Tolerance / Bad Day
- Ball: Parent holds steady; child just sits (no balance challenge)
- Bands: Lightest resistance; 4–6 reps instead of 8–12
- Balance Board: Foam balance pad instead of board
- Roller: Parent rolls along child's legs (passive)
- Step: 5 cm height instead of 10–15 cm
- Tunnel: Open-sided arch alternative (chairs + blanket, sides open)
- Timer/Cards: Child chooses only 2 cards instead of full deck
➡ HARDER Modifications
For: Sensory Seeker / Strong Performance / Breakthrough Day
- Ball: Unsupported + arm reaches + ball toss + eyes closed
- Balance Board: Eyes closed, single-leg, simultaneous arm exercise
- Bands: Move to next color resistance; increase reps to 15
- Step: Increase height; add weighted vest
- Tunnel: Obstacle at entry; add timing challenge
- Weights: Increase by 0.25 kg; add exercise complexity
Age Modifications
- 0–2 years: Passive input only; parent-guided movement
- 2–5 years: Supported; 5–10 min; play-based framing
- 5–10 years: Semi-structured; 10–15 min; exercise cards work well
- 10–18 years: Full protocol; 15–20 min; teen may self-direct

ACT IV — The Progress Arc
Week 1–2: Tolerance Is Progress. Mastery Comes Later.
15%
Progress Milestone
You are here — Week 1–2. Building tolerance and establishing the routine.
✓ What Progress Looks Like (Week 1–2)
- Child comes to the therapy mat when invited (vs. refusing yesterday)
- Child touches the therapy ball without pulling away
- Session lasts 8 minutes instead of 3 (even if incomplete)
- Child tolerates balance board for 2 seconds (vs. refusing)
- Child chooses one exercise card independently
- Child mentions therapy at a different time of day
✗ What Is Not Progress Yet (Don't Expect)
- Independent exercise execution
- Visible strength improvements
- Balance held for more than 5 seconds reliably
- Full session completion without prompting
- Generalization to other settings
Your Benchmark — Write This Down Today
Balance hold: ___ seconds | Session duration: ___ min | Resistance band reps: ___ | Resistance to session start: High / Medium / Low. Compare to Week 4. The numbers will surprise you.
Week 3–4: The Brain Is Building. These Are the Signs.
40%
Consolidation Phase
Neural pathways forming — behavioral consolidation markers emerging
Child anticipates sessions
Asks "Are we doing therapy today?" or moves toward materials without prompting. This is the brain's prediction system activating — a powerful sign.
Transition resistance drops
Session start takes under 2 minutes consistently (vs. 5–8 minutes in Week 1). The routine is establishing itself.
Balance hold duration doubles
2 seconds → 4–5 seconds without support. The ankle and hip systems are responding to training.
Ball sitting: eyes leave the ball
Child no longer needs to watch their feet — automaticity is beginning. This is myelin thickening in action.
Generalization seeds appearing
Child attempts single-leg standing at other times (brushing teeth, standing in a queue). Skill is beginning to transfer to real life.
"By Week 4, you may notice something unexpected: you're more confident. The exercises feel natural. The routine has found its rhythm. You've also been building neural pathways."
Week 5–8: Mastery. The Skill Is Generalizing Beyond the Session.
75%
Mastery Threshold
Mastery criteria met — skill appearing in real-world contexts
Therapy Ball Mastery
✓ 30-second independent sit | ✓ Reaches in 4 directions without losing balance | ✓ Initiates prone position self-guided
Balance Board Mastery
✓ 30-second stand without support (eyes open) | ✓ Maintains balance through light perturbation | ✓ Single-leg stand attempted
Step Platform Mastery
✓ 10 step-ups per leg with controlled technique | ✓ Calf raises off step edge without handrail | ✓ Lateral step-overs without hesitation
Generalization in Real Life
✓ Stairs with alternating feet reliably | ✓ Running on uneven ground without falling | ✓ Recovering from trips/slips without falling
🏆 MASTERY UNLOCKED
F-590 Home PT Foundation — Weeks 5–8 Complete
Ready for: F-591 Postural Control
You Did This. Your Child Grew Because of Your Commitment.
For 5–8 weeks, you showed up. Some days your child was resistant. Some days you were tired. Some days the session lasted 3 minutes. You showed up anyway.
That is what neuroplasticity requires: consistent, caring repetition. Science doesn't care about perfect sessions — it rewards persistent ones. The difference between your child's progress and a child without home PT support is measurable. And you made it.
From tolerating the balance board for 0 seconds to 30-second independent stands. From 3-minute sessions to 15-minute completion. From refusing the tunnel to racing through it. That is not coincidence. That is neuroscience happening in your living room.
Trust Your Instincts. If Something Feels Wrong, Pause and Ask.
Even as progress accelerates, clinical vigilance continues. These red flags require you to pause home PT and consult your child's physical therapist or call 9100 181 181.
🔴 Joint Swelling Post-Exercise
Visible swelling around knee, ankle, wrist, or elbow after exercises. May indicate joint stress or structural issue. Stop that exercise. Contact PT within 24 hours. Do not push through.
🔴 Persistent Pain Complaint
Child complaining of pain 2+ hours after session or on waking. Delayed onset muscle soreness is normal; persistent joint pain is not. Rest 48 hours. If persists, contact PT before resuming.
🔴 Skill Regression
Previously mastered skills deteriorating — falling more, refusing previously accepted exercises. May indicate overtraining, illness, or neurological change. Pause program. Contact PT and pediatrician.
🔴 Extreme Fear or Panic Response
Child shows panic (hyperventilating, screaming, full meltdown) to specific material. May indicate sensory processing difference. Remove trigger material. Contact OT + PT for modified approach.
🔴 Changes in Gait or Movement Pattern
Walking differently, favoring one side, or new awkwardness. May indicate pain or structural issue. Contact PT urgently. Do not continue resistance or balance work until assessed.
🔴 Unexpected Falls / Dizziness During Balance Work
Unexpected falls or episodes of dizziness during balance exercises. May indicate vestibular, cardiac, or neurological issue. Stop balance work. Contact pediatrician and PT.
"Other Gross Motor Techniques — Using Materials You Already Own."
Every technique below uses materials from your F-590 toolkit. Your initial investment now unlocks an entire curriculum of gross motor development.
Technique | Code | Materials You Own | Difficulty |
Core Strength for Daily Function | F-580 | Therapy Ball ✓ Mat ✓ | 🟡 Core |
Balance and Coordination Foundations | F-575 | Balance Board ✓ Foam Roller ✓ | 🟢 Intro |
Postural Control Development | F-591 | Therapy Ball ✓ Resistance Bands ✓ | 🟡 Core |
Gait Training Techniques | F-592 | Step Platform ✓ Mat ✓ | 🟡 Core |
Flexibility and Stretching | F-595 | Mat ✓ Foam Roller ✓ | 🟢 Intro |
Sports Participation Readiness | F-589 | Resistance Bands ✓ Balance Board ✓ | 🔴 Advanced |
"Every technique above uses materials you acquired for F-590. Your investment in the Home PT Toolkit now serves 6+ technique programs."

ACT V — Community & Ecosystem
From the Pinnacle Clinical Archives: Three Families. One Toolkit. Measurable Change.
Arun, 6 years | Cerebral Palsy (Spastic Diplegia) | Chennai
Before: No equipment. Sessions lasted 2 minutes before Arun walked away. Balance declining between clinic visits. His mother felt she was "undoing the clinic's work at home."
After Week 8: With therapy mat, ball, and step platform, a 12-minute routine was built. Balance board added in Week 6. The PT noted unexpected balance gains — "faster than clinic-only trajectory." 47 completed sessions in 8 weeks.
"The mother's consistency with the right equipment changed Arun's trajectory. This is the home-clinic model working as designed."
After Week 8: With therapy mat, ball, and step platform, a 12-minute routine was built. Balance board added in Week 6. The PT noted unexpected balance gains — "faster than clinic-only trajectory." 47 completed sessions in 8 weeks.
"The mother's consistency with the right equipment changed Arun's trajectory. This is the home-clinic model working as designed."
Priya, 4 years | Hypotonia | Hyderabad
Before: Fatigued quickly, resisted exercise. Home program sheet sat on the refrigerator for 3 months, unused.
After Week 6: Resistance bands with color progression ("level up" motivation), therapy ball as meal-seat, visual timer + exercise cards. Completed her first 15-minute session independently. Tone assessment showed measurable improvement.
"The gamification of the material progression — band colors as 'levels' — was the behavioral key for Priya."
After Week 6: Resistance bands with color progression ("level up" motivation), therapy ball as meal-seat, visual timer + exercise cards. Completed her first 15-minute session independently. Tone assessment showed measurable improvement.
"The gamification of the material progression — band colors as 'levels' — was the behavioral key for Priya."
Keerthi, 9 years | Developmental Coordination Disorder | Bengaluru
Before: Fell frequently, avoided sports. Home PT felt "too medical" — he refused entirely.
After Week 10: Tunnel was the entry point — pure play initially. Balance board became a "skateboard game." Resistance bands became "superpower training." School PE teacher reported Keerthi participating in group activities for the first time.
"When the equipment feels like play, compliance becomes enthusiasm."
After Week 10: Tunnel was the entry point — pure play initially. Balance board became a "skateboard game." Resistance bands became "superpower training." School PE teacher reported Keerthi participating in group activities for the first time.
"When the equipment feels like play, compliance becomes enthusiasm."
Note: These narratives are illustrative. Individual outcomes vary by diagnosis, age, adherence, and program consistency. For your child's specific prognosis, request an AbilityScore® assessment: 9100 181 181
"Your Experience Is Valuable to the Next Parent Who Is Exactly Where You Were."
Isolation is the enemy of adherence. Every parent in this program is a resource for every other parent. The community of practice around home PT is as therapeutic as the equipment itself.
Pinnacle Home PT Parent Group (WhatsApp)
Parents navigating pediatric physical therapy home programs across India. Moderated by Pinnacle PT/OT team. Message "HOME PT COMMUNITY" to wa.me/919100181181
Pinnacle Parent Community Forum
Ask questions, share wins, troubleshoot challenges with parents and therapists. pinnacleblooms.org/community
Local Parent Meetups
In-person parent groups at Pinnacle centers in your city. Find nearest meetup at your local Pinnacle center — connect with families doing the same program.
Peer Mentoring Program
Connect with a parent who has completed F-590 and the home PT program. "Parents who've done this are the best guides for parents starting it."

"Home + Clinic = Maximum Impact. 70+ Centers. One National System."
Specialist Matching for F-590
- Primary: Pediatric Physical Therapist — Prescribes and supervises your home program. Clinic review every 4 weeks minimum recommended.
- Secondary: Pediatric OT — If sensory processing issues are complicating home PT execution, OT assessment is indicated.
- Behavioral Support: ABA/BCBA — If adherence remains a challenge despite structural tools, behavioral analysis can resolve it.
- Medical Oversight: NeuroDevelopmental Pediatrician — Essential for CP, hypotonia, or neurological conditions.
Centers Across India
📍 Hyderabad (Multiple) | 📍 Bengaluru | 📍 Chennai | 📍 Mumbai | 📍 Pune | 📍 Delhi | 📍 Kolkata | + 63 more cities
Teleconsultation Option
Available for families more than 50 km from nearest center. Pinnacle therapists can review your home program and equipment via 30-minute video session.
Insurance / Funding
Physical therapy for children is covered under several government and insurance schemes in India. Ask your Pinnacle center coordinator about coverage options.

"Consistency Across Caregivers Multiplies Impact."
The child who has one caregiver doing home PT makes progress. The child whose entire family understands and supports the program makes accelerated progress. You are not the only therapist in this child's life — you are the one who can recruit all the others.
Explain to Grandparents
"Our child's physical therapist has given us a home exercise program. We use a special mat, a big bouncy ball, some stretchy bands, a balance board, and a few other tools for 15 minutes each day. The most important thing: we do them consistently — even 10 minutes every day is better than 60 minutes once a week. When you're with [child's name], please encourage them, don't let them skip because they're fussing, and tell us what you observed."
Template for Teachers
"[Child's name] is currently on a home physical therapy program focusing on gross motor strength, balance, and coordination. Key areas to watch: stair navigation, balance on uneven surfaces, sports participation readiness. Please note any changes in PE participation or motor skills — it helps us track progress across environments."
Preview of 9 materials that help with physical therapy home Therapy Material
Below is a visual preview of 9 materials that help with physical therapy home therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

The Pinnacle Promise
PINNACLE BLOOMS NETWORK®
Multi-Disciplinary Pediatric Consortium
OT | SLP | ABA | SpEd | NeuroDev | PT | CRO
Multi-Disciplinary Pediatric Consortium
OT | SLP | ABA | SpEd | NeuroDev | PT | CRO
"Pinnacle Blooms Network® exists to transform every family home into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy center — powered by GPT-OS® and delivered by the world's most complete pediatric therapeutic consortium."
"From fear to mastery. One technique at a time."
20M+
1:1 Sessions Delivered
97%+
Measured Improvement
70+
Centers Across India
160+
Countries — Patents Filed
FREE National Helpline: 9100 181 181 | Available 24×7 | 16+ Languages | care@pinnacleblooms.org | pinnacleblooms.org