
When They Run Out of Energy Before Other Kids
Building physical endurance through play and practice — a clinically validated guide for families and therapists.
F-580 · Gross Motor Domain
Ages 3–12
Pinnacle Blooms Consortium

The Stamina Gap Is More Common Than You Think
And it is not your child's fault. Across children with neurodevelopmental conditions, reduced physical endurance is one of the most frequently reported concerns — and one of the most responsive to the right intervention.
1 in 4
Endurance Deficit
Children with neurodevelopmental conditions show significantly reduced physical endurance compared to peers.
68%
Below-Average Fitness
Children with autism spectrum disorder demonstrate below-average cardiovascular fitness measures in systematic review data. PMC11506176, Children 2024
3–8×
Greater Fatigue
Greater fatigue per unit of activity in children with hypotonia vs. neurotypical peers — more effort, less output. Motor Physiology Research, Pediatric OT Literature
Across Pinnacle Blooms centers, physical endurance challenges are among the top 10 presenting concerns from parents of children with autism, ADHD, developmental coordination disorder, and low muscle tone. You are among millions of families navigating this exact challenge — and with the right materials and approach, the trajectory changes.
India Context: Physical inactivity in children has tripled since 2000 (WHO South-East Asia Report, 2022). Children with neurodevelopmental differences face compounded barriers — sensory, motor, and motivational. Structured, home-based endurance programming directly addresses these barriers.
Why Stamina Is Lower — And Why It Responds to Training
Cardiovascular, muscular, and motor coordination pathways all contribute to endurance in children.
Your child is not lazy.
Their cardiovascular and muscular systems have not yet received the sustained activity signal they need to develop efficiency. When a child is less active, the heart becomes less efficient at delivering oxygen during movement. Muscles — especially the slow-twitch endurance fibres — don't develop their fatigue-resistance capacity.
For children with low muscle tone (hypotonia), the baseline energy cost of simply standing or walking is higher — leaving less reserve for play. For children with autism or developmental coordination disorder, inefficient movement patterns mean their body burns more energy doing the same activity as a peer. More effort. Earlier exhaustion. Same playground.
The extraordinary news: Endurance responds to training at any level, at any age. The upward spiral starts with as little as 5 minutes of daily consistent activity.
"Physical activity interventions in children with ASD show measurable improvements in cardiovascular fitness, muscular endurance, and activity tolerance." — Frontiers in Integrative Neuroscience, 2020
Endurance Develops Progressively — and Intervention at Any Point Works
Children naturally build endurance through unstructured play — running, climbing, cycling. But when neurodevelopmental conditions create sensory overwhelm, motor inefficiency, or low tone, children withdraw from physical activity. The withdrawal triggers deconditioning. Deconditioning makes activity harder. Harder activity triggers more withdrawal. The cycle compounds.
Ages 1–2
Walking & First Steps
Ages 2–4
Running & First Climbing
Ages 4–6
Sustained Play 20–30 min
Ages 6–9
Organized Sports 45 min
Ages 9–12
Comparable Peer Activity
▲ F-580 Intervention Zone: Ages 3–12 — the most impactful window combining neuroplasticity and habit formation.
WHO recommends 60 minutes of moderate-to-vigorous physical activity daily for children ages 5–17. Children with autism and developmental delays typically achieve less than half this threshold — not because they won't, but because the activity isn't structured, engaging, or appropriately calibrated to their starting point.
Physical endurance challenges frequently co-occur with: Low Muscle Tone (Hypotonia) · Developmental Coordination Disorder · Autism Spectrum Disorder · ADHD · Sensory Processing Disorder · Poor Postural Control.

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level II
Systematic Review + RCTs · Multiple Populations · ✓ Validated in Indian RCT
Evidence Strength: 82%
Strong evidence base across 24+ qualifying studies and multiple systematic reviews.
PRISMA Systematic Review 2024
Structured physical intervention effectively promotes gross motor outcomes in children with ASD. PMC11506176
Meta-Analysis, World J Clin Cases 2024
24 studies confirm cardiovascular fitness, adaptive behavior, and social participation improve. PMC10955541
Indian RCT, Padmanabha et al. 2019
Home-based structured intervention significantly improved outcomes in Indian pediatric population. DOI: 10.1007/s12098-018-2747-4
Pinnacle Proof: 20M+ exclusive 1:1 therapy sessions · 97%+ measured improvement · 70+ centers across India · Children from 70+ countries served

ACT II: Knowledge Transfer
The Technique: What It Is
🏃 Progressive Physical Endurance Training Through Structured Play
Parent alias: "Building the battery"
Technique Code: F-580 · Domain: Gross Motor / Physical Development · Ages: 3–12 · OT + PT Primary · Home-Executable · Daily · 5–30 min · Progressive Protocol
Physical endurance intervention is a structured, progressive approach to building cardiovascular and muscular stamina in children whose activity tolerance falls below age-appropriate norms. Unlike formal exercise programs, it uses play-based, motivating activities — trampolines, bikes, obstacle courses, swimming, jump ropes — delivered in short, consistent daily sessions that gradually increase in duration and intensity as the child's body adapts.It is not a single activity. It is a framework: Start at the child's current level. Make it engaging. Increase gradually. Track progress. Celebrate every gain.
Who it's for: Children ages 3–12 who tire quickly during play, struggle to keep up with peers physically, avoid PE class, or have underlying low muscle tone, autism, ADHD, or developmental coordination disorder.

Who Uses This Technique
This technique lives across five therapy disciplines — because the body doesn't organize by specialty. A child who builds endurance in OT runs better in PE, participates more in ABA sessions, and engages more fully in Special Education activities.
🦺 Pediatric OT — Primary Lead
Sensory-motor integration, postural endurance, motor planning, adaptive equipment selection.
🏋️ Physical Therapy — Core Partner
Cardiovascular programming, muscular endurance protocol, low tone management, gait efficiency.
🧠 ABA / BCBA — Reinforcement
Motivation systems, habit formation, data tracking, reward scheduling, session design.
🩺 NeuroDev Pediatrics
Metabolic baseline assessment, cardiac clearance, hypotonia diagnosis, medication interaction review for fatigue.
🎓 Special Education
Integrates endurance support into PE accommodations, classroom movement breaks, school activity planning.
The Pinnacle FusionModule™ coordinates all five disciplines into a single, non-redundant therapeutic pathway. Multi-disciplinary coordination produces outcomes no single discipline achieves alone. DOI: 10.1080/17549507.2022.2141327
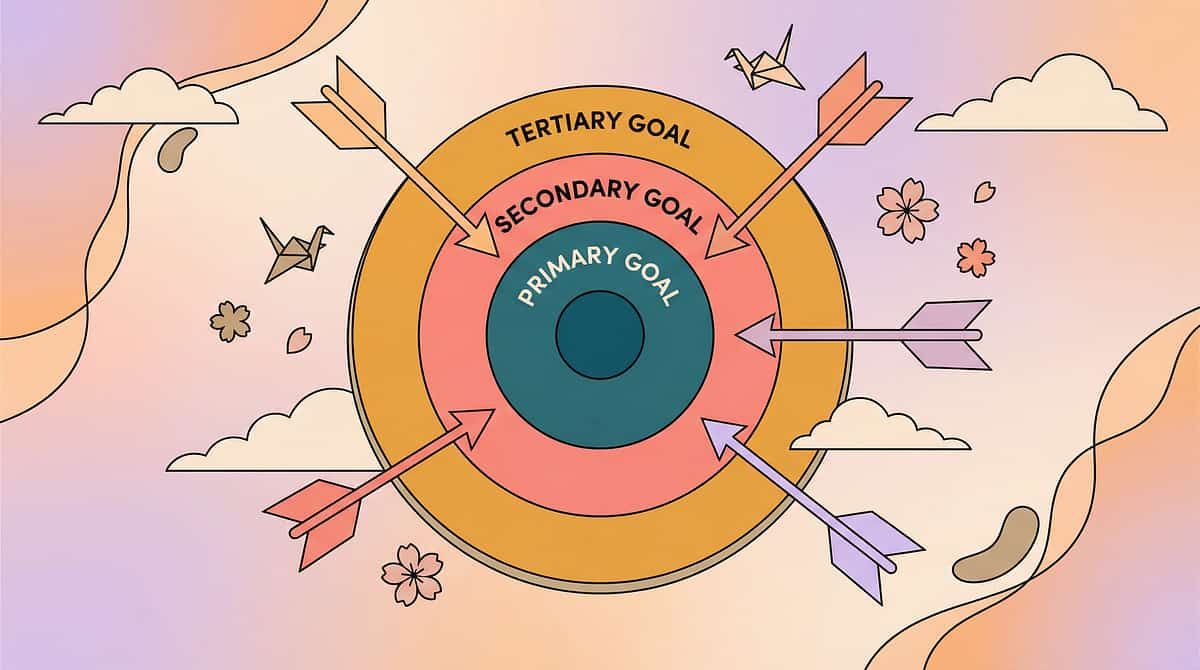
What This Targets
This is not a random activity. It is a precision tool with measurable targets across three concentric layers — each building on the one before.
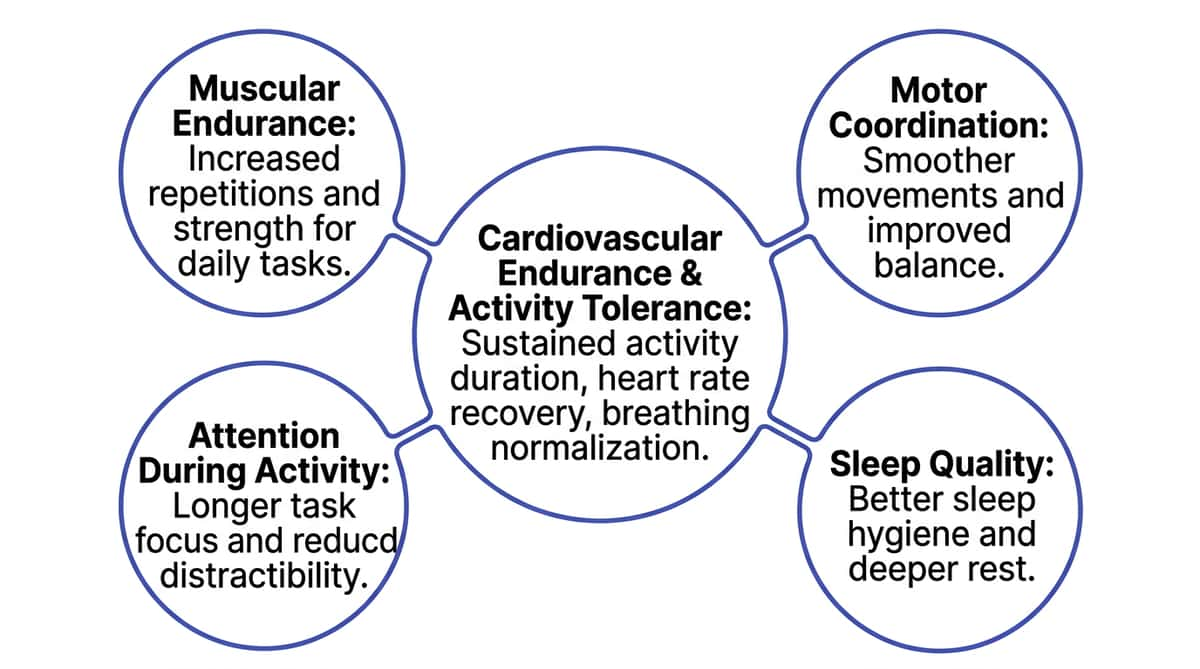
🎯 Primary: Cardiovascular Endurance + Activity Tolerance
Child sustains physical activity for progressively longer durations. Heart rate recovery time improves. Heavy breathing resolves faster after exertion.
⭕ Secondary: Muscular Endurance + Coordination + Sleep
Legs don't "give out" as quickly. Movement patterns become more efficient. Sleep onset improves as physical fatigue normalizes.
◎ Tertiary: Social + Academic + Confidence
Child stays in playground games longer. Participates in PE without sitting out. Willingly joins family outings. Self-identifies as "I can do this."

9 Materials That Help Build Physical Endurance
Each material below is backed by a clinical rationale — not selected at random. Together, they form a complete endurance-building toolkit for children ages 3–12.

1. Mini Trampoline / Rebounder
Clinical Rationale: Low-impact cardiovascular exercise children self-motivate to sustain longer than running. Builds CV endurance, leg strength, and core simultaneously. Rhythmic bouncing regulates sensory systems. Price: ₹2,000–8,000 | DIY: Mattress on floor (supervised) — ₹0

2. Balance Bike / Pedal Bike
Clinical Rationale: Cycling extends activity duration because seated movement requires less endurance than walking/running. Builds leg strength and CV fitness progressively. Functional transportation = daily endurance dose. Price: ₹3,000–15,000 | DIY: Community park cycle — ₹0

3. Obstacle Course Kit
Clinical Rationale: Transforms endurance training into engaging play. Interval-style activity builds both cardiovascular and muscular endurance while variety maintains engagement and disguises effort. Price: ₹1,000–5,000 | DIY: Chalk lines, rolled towels, plastic bottles as cones — ₹0

9 Materials — Continued

4. Resistance Bands (Child-Friendly, Light)
Clinical Rationale: Builds muscular endurance — the muscle's capacity to sustain effort without fatigue. High reps, light resistance = endurance training. Complements cardiovascular activities. Price: ₹300–1,000 | DIY: Old rubber tubing from hardware store — ₹50

5. Scooter Board
Clinical Rationale: Prone or seated propulsion using arms and legs builds significant upper body, core, and postural endurance — often undertrained in low-endurance children. Engaging enough that children sustain effort longer than during conventional exercises. Price: ₹500–2,000 | DIY: Smooth cutting board + socks on floor — ₹0

6. Jump Rope
Clinical Rationale: Most efficient cardiovascular endurance builder per minute. Quantifiable progress (count jumps). Even 2–3 minutes daily builds CV capacity. Progress tracking motivates sustained practice. Price: ₹100–500 | DIY: Soft rope or dupatta — ₹0
9 Materials — Continued

7. Swimming Pool Access / Swim Equipment
Clinical Rationale: Water buoyancy reduces fatigue perception, allowing longer exercise sessions. Builds cardiovascular, muscular, and respiratory endurance simultaneously. Ideal for children with hypotonia — buoyancy reduces joint load. Price: ₹500–3,000/month pool access | DIY: Large tub or bucket water play — ₹0

8. Child-Friendly Fitness Tracker / Activity Watch
Clinical Rationale: Makes activity visible and measurable. Gamified step-counting and active-minute tracking motivates sustained movement. What gets measured gets done. Converts abstract endurance goals into concrete daily achievements. Price: ₹1,500–5,000 | DIY: Paper tally chart with stickers — ₹10

9. Interactive Movement Video Games
Clinical Rationale: Children sustain physical activity far longer when engaged in a game than during formal exercise. Motion-based games provide sustained cardiovascular activity while the game's progression provides intrinsic motivation. Indoor, weather-independent. Price: ₹2,000–15,000 | DIY: YouTube GoNoodle / Just Dance (free) — ₹0

Every Family Can Start Today. Zero Cost. Maximum Impact.
The WHO Nurturing Care Framework principle: interventions must be accessible across all economic contexts. The DIY options below deliver the same clinical principle as commercial materials — the neuroscience doesn't change based on price.
Commercial Material | DIY / Household Alternative | Same Principle | |
Mini Trampoline ₹2,000–8,000 | Old mattress on floor / Sofa cushions to jump between | Cardiovascular demand + bilateral coordination | |
Balance Bike ₹3,000–15,000 | Community park cycles / Push-along scooter / Tricycle | Extended activity duration + leg endurance | |
Obstacle Course Kit ₹1,000–5,000 | Chalk lines + rolled towels + plastic bottles as cones | Sustained interval-style movement | |
Resistance Bands ₹300–1,000 | Old bicycle inner tube cut into strips | Muscular endurance loading at home | |
Scooter Board ₹500–2,000 | Smooth cutting board + socks on tiled floor | Upper body + core endurance | |
Jump Rope ₹100–500 | Old dupatta / soft rope | Most efficient CV endurance builder | |
Swimming Access | Garden sprinkler / shallow baby pool / water games | Whole-body low-impact endurance | |
Fitness Tracker ₹1,500–5,000 | Paper chart + sticker system + count jumps/laps | Gamified progress tracking | |
Movement Video Games ₹2,000+ | YouTube GoNoodle / Just Dance (free) / Action songs | Sustained movement through entertainment |
Zero-Cost Starter Protocol: Day 1: Chalk obstacle course + old rope jump → 5 min · Day 2: Mattress bouncing + counting game → 5 min · Day 3: Paper tally chart started · Week 2: Add 1 minute each day → Same clinical outcome. Zero rupees.
Safety First: Read This Before the First Session
Safety is the foundation of progress. Take 2 minutes with this traffic-light guide before beginning any session.
🔴 RED: Do Not Proceed
- Child has been diagnosed with a cardiac condition
- Child reports chest pain, dizziness, or breathlessness at rest
- Child has uncontrolled asthma or active respiratory illness
- Pediatrician has advised against physical exercise
- Child shows signs of acute illness (fever, infection, pain)
- Child has had a recent orthopedic injury or fracture
🟡 AMBER: Modify — Proceed With Caution
- Child has hypotonia — use low-impact activities first
- Child has hypermobile joints — avoid high-impact
- Child has sensory defensiveness — introduce equipment slowly
- Child has had a meltdown in the last 2 hours — postpone
- Child is very hungry or very tired — brief snack + 20-min rest first
🟢 GREEN: Clear to Proceed
- Medical clearance obtained if any amber flags apply
- Child is calm, alert, and has eaten within the last 2 hours
- Space is clear and safe for the planned activity
- Parent is prepared to supervise throughout
⛔ Stop immediately if: Lips turning blue or purple · Skin turning pale or grey · Child cannot catch breath after 3 minutes of rest · Child becomes unresponsive or extremely lethargic · Child reports chest pain or severe leg pain. 📞FREE Helpline: 9100 181 181 — If you are unsure whether to proceed, call us.

Set Up Your Space
The right environment prevents 80% of session failures before they happen. A well-configured space is as important as the materials themselves.
Space Preparation Checklist
- Furniture pushed to walls — full movement zone clear
- Slip hazard eliminated — yoga mat or carpet section for indoor activities
- Distractions removed — TV off, tablets away, screens out of sight
- Noise level reduced — no loud music; fan/AC at comfortable level
- Lighting — bright natural light preferred; avoid harsh fluorescent
- Temperature — comfortable 22–26°C; avoid midday heat for outdoor sessions
- Parent phone — silent mode (except for timing purposes)
- Water bottle filled and visible to child
- Timer ready (phone timer or visual timer)
Optimal Session Times
Best: Morning 8–10 AM — alertness peak, regulated state post-breakfast
Good: Late afternoon 4–6 PM — post-nap energy window
Avoid: Within 30 minutes of a meal · During TV time · After meltdowns · After 7 PM
Space Layout
① Parent position: side + slightly behind child ② Child start position: centre floor, facing equipment ③ Primary material: trampoline / obstacle course / jump rope ④ Secondary material: backup activity nearby ⑤ Water bottle + towel: always visible to child ⑥ Tracking chart: visible, easy to reach post-session Clear zone: 2 ft around all equipment
ACT III: Execution
Is Your Child Ready? The Readiness Check
The best session starts right. 60 seconds of assessment saves 20 minutes of struggle. Run this quick check before every session.
Check | ✅ Go | ⚠️ Modify | ❌ Postpone | |
Eating: Child has eaten in last 2 hours | Proceed | Quick snack first (10 min) | Nausea / stomachache | |
Rest: Child is not overtired | Proceed | 10-min quiet time first | Child is falling asleep | |
State: Child is calm, not mid-meltdown | Proceed | Regulation activity first | Active meltdown / distress | |
Interest: Any interest in materials | Proceed | Motivate with preferred item | Extreme avoidance | |
Health: No fever, illness, or pain | Proceed | Reduced intensity | Any illness symptom | |
Time: 15–30 uninterrupted minutes | Proceed | Shorten to 8–10 min | Less than 5 min available | |
Space: Setup complete | Proceed | Quick clear | Unsafe space |
5–7 Green
Start full protocol
3–4 Green, Some Amber
Start modified (shorter, simpler)
Any Red / Fewer than 3 Green
Postpone today — don't force it

Step 1 of 6
The Invitation — Open With Curiosity, Not Commands
The child chooses to begin. This distinction — invitation vs. command — is the difference between a session that succeeds and one that creates lasting avoidance.
Parent Script
"Hey [name], I've got something fun. Want to see?"
[Show the material — hold it, demonstrate briefly, make it interesting]
"Look what I can do. Want to try?"
If the Child Resists
Don't push. Try: "Okay, just watch me." Demonstrate yourself for 30 seconds. Children often join once they see the activity is safe and enjoyable.
Body Language Guide
- Crouch to child's eye level — do not loom above
- Open, relaxed posture — shoulders down, no tension
- Warm, quiet energy — not over-excited (which can overwhelm)
- Material visible and accessible but not thrust toward child
Acceptance Cues to Look For
- Child approaches material voluntarily
- Child makes eye contact with material or parent
- Child reaches for material
- Child mirrors your demonstration
ABA Principle: This is the "pairing" phase — building positive association with the material before any therapeutic demand is placed. A child who wants to be there learns faster and sustains effort longer.
Step 2 of 6
The Engagement — Follow Their Lead
The child is now engaged. Your role is to introduce the material therapeutically — one instruction at a time, demonstrated first, with the first demand set at near-certain success.
Mini Trampoline
"Let's bounce together! One… two… three…" Count out loud. Keep energy warm but not loud. Vary: Jump on 2 feet → hop on one foot → jump and clap.
Obstacle Course
"See that tunnel? Can you get through it and touch the cone? Go!" Demonstrate first. Keep the first route simple — 2–3 obstacles only.
Jump Rope
"I'll count. Every jump you do is a point. Ready? Go!" Even 3 jumps is a win. Celebrate immediately.
Bike
"Can you ride to that tree and back? I'll wait right here." Clear, achievable, visible endpoint. Cheer on return.
Within 3 seconds of any engagement:"Yes! You're doing it!" — Specific praise. Enthusiastic but regulated. Reinforcement timing is everything.
Step 3 of 6
The Therapeutic Action — Sustained, Progressive Physical Effort Disguised as Fun
This is the active ingredient. Every minute of sustained activity is a dose of cardiovascular and muscular adaptation. The child does not need to know they are exercising. They need to stay engaged.
Weeks 1–2
Child's current maximum. Establish baseline. No pushing beyond tolerance.
Weeks 3–4
Current max + 20%. First progressive overload. Celebrate every extra minute.
Weeks 5–6
Current max + 40%. Consolidation phase. Consistency over intensity.
Weeks 7–8
Double week 1 duration. Mastery milestone. Real-world participation emerging.
Execution by Material
Trampoline: Start 3 min continuous bouncing → add music + counting → Vary: one foot hop, jump and clap. Progress: 3→5→8→12 min over 4 weeks.
Obstacle Course: 4–6 obstacles, time the run, repeat 3–5 times per session. Build to 6–8 rounds.
Jump Rope: Count consecutive jumps. Record. Beat last count. Start at 5 jumps → build to 20, 50, 100.
Swimming: Width of pool → 2 widths → full length. 2–3 sessions per week = significant improvement by week 6.
Execution Quality Indicators
✅ Ideal
Child is working (breathing faster), happy, sustaining effort.
⚠️ Acceptable
Child needs brief rest breaks but resumes activity voluntarily.
❌ Concerning
Child is distressed, refuses to continue, or shows safety flag symptoms.

Step 4 of 6
Repeat and Vary — Three Great Reps Beat Ten Forced Ones
Variety beats monotony. Repetition targets give structure; the variation menu gives the child fresh engagement every session.
Repetition Targets by Material
- Trampoline: 3 × 2–3 minute bounce sets with 60-second rest between
- Obstacle Course: 3–5 full course completions per session
- Bike: 1 continuous ride at target duration
- Jump Rope: 3–5 jump sets (count each)
- Swimming: Laps/widths × target count
- Resistance Bands: 2–3 sets of 15–20 reps, light resistance
Satiation Indicators — When the Child Has Had Enough
- Activity slows significantly; no motivation to continue
- Child seeks to exit or move to a different activity
- Quality of movement decreases noticeably
- Child becomes irritable or emotional
When you see these signs: wrap up warmly. The body has received its dose.
Variation Menu by Material
Trampoline: Basic bounce → Jump and clap → Hop on one foot → Jump and turn → Name an animal each bounce → Bounce to music rhythm
Obstacle Course: Forward → Backward → Carrying object → Eyes closed for one section → Time attack vs. yesterday → Team with parent
Bike: Flat route → Slight incline → Stop at landmarks → Speed intervals → Navigation game
Jump Rope: Two-foot jump → Alternating feet → Slow → Fast → Count to music beat → Eyes closed for 3 jumps
"3 good reps > 10 forced reps. The therapeutic dose is absorbed during willing, engaged activity. Forcing beyond satiation creates negative associations that reduce tomorrow's participation." — Pinnacle Blooms Consortium

Step 5 of 6
Reinforce and Celebrate — Timing Matters More Than Magnitude
Immediate, specific, enthusiastic reinforcement within 3 seconds of the desired behavior is the clinical standard. The chart below gives you a full reinforcement menu matched to your child's profile.
Reinforcement Type | Examples | Best For | |
Verbal Praise | "You jumped for 5 minutes — that's your record!" "Your legs are getting so strong!" | All children | |
Physical | High five, hug (if sought), fist bump, spin around together | Sensory seekers | |
Token Economy | Sticker on chart, star added, "energy point" earned | ABA-enrolled children | |
Activity Reinforcer | Choose next 2 minutes of bouncing style, choose tomorrow's activity | Autonomous children | |
Visual Progress | Mark jump count on wall chart, see fitness tracker number go up | Data-motivated children | |
Natural Consequence | "Because you rode your bike, now we can go to the park." | Higher-functioning profiles |
Critical ABA Principle: Celebrate the attempt, not just the success. If the child tried and didn't reach the target — that is progress. "You tried the full course — I'm so proud of that. Tomorrow we'll try again."
Step 6 of 6
The Cool-Down — No Session Ends Abruptly
Transition prevents the post-session crash. A well-managed cool-down creates positive anticipation for tomorrow's session.
Transition Warning Script
"Two more bounces, then we're all done!"
"One more time around the course — last one!"
"Finish at that tree, and we're done for today!"
Give 30-second advance warning. Then 15-second. Then done.
If Child Resists Ending
Give control: "Okay, two more — you choose: bouncing or the course?" Honor the choice. End after those two. Never remove the material without warning.
Cool-Down Sequence
- Complete final repetition with advance warning
- Slow down: gentle walk / quiet bounce / easy pedal
- "We're done! Let's catch our breath." — 3 deep slow breaths together
- Child helps put away one piece of equipment
- Water bottle — child drinks
- Tracking chart marked immediately (memory is fresh)
- Transition cue to next activity: "Now we [snack / play / rest]"
Visual Timer Note: For children who struggle with transitions, a visual timer showing "2 minutes left" removes the surprise of stopping. What children can see, they can prepare for. Visual supports are classified as evidence-based practice for autism — NCAEP 2020.
Capture the Data: Right Now
60 seconds of data now saves hours of guessing later. Track immediately after the session while the memory is fresh — this single habit is what separates families who see consistent progress from those who wonder why things stalled.
What to Track (3 Core Fields)
Duration
How many minutes did the child sustain activity? This number will trend upward over weeks — even when it doesn't feel like it.
Engagement Level
1 (refused/distressed) to 5 (fully engaged, self-motivated). Engagement level is often a leading indicator of endurance gains.
Material Used
Which of the 9 materials was used? This helps identify which materials work best for your child's profile.
Why This Matters
When you track duration over weeks, you will see the upward trend. On difficult days when progress seems invisible, the data shows you that week 1 was 5 minutes and week 6 is 12 minutes. That data is your anchor when doubt creeps in.
GPT-OS® Integration: Session data feeds the Physical Endurance Readiness Index in your child's GPT-OS® profile, automatically recalibrating recommendations and alerting your Pinnacle therapist to trends — before your next appointment.
ABA Data Collection Standards: Continuous measurement (duration, frequency) is standard practice for tracking behavior-analytic intervention. BACB Guidelines + Cooper, Heron & Heward, Applied Behavior Analysis 8th ed.

What If It Didn't Go as Planned?
Session abandonment is not failure. It's data. Here's how to read it — and what to do differently next time.
Problem 1: Child refused to start
Why: Low motivation, activity not appealing, poor timing, sensory overwhelm. Next time: Choose a different material. Use a visual schedule showing the activity in advance. Start with a 1-minute version only. Pre-load motivation with a preferred reinforcer before the session begins.
Problem 2: Engaged for 1 minute then stopped
Why: Duration demand exceeded current tolerance — baseline is under 2 minutes. Next time: This IS the baseline. 1 minute is where you start. Next session: 1 minute + 15 seconds. Celebrate the 1 minute as a genuine win.
Problem 3: Child became emotional or cried during activity
Why: Physical exertion with low regulation capacity; or sensory overwhelm from the equipment. Next time: Immediate cool-down. Regulate first. Assess: was it the effort, the material, or the environment? Try a different material. Reduce duration significantly.
Problem 4: Child exhausted for 2 hours after
Why: Session duration or intensity exceeded recovery capacity. Common in first 2 weeks. Next time: Reduce duration by 30%. This is the body's first adaptation signal — next week will be better.
Problem 5: Child wants 30 minutes but you can't sustain supervision
Why: Child is highly motivated (excellent!) but needs varied programming. Next time: Use the variation menu from the Repeat & Vary card. Rotate between 2–3 materials per session to maintain engagement without exhausting supervision capacity.
Problem 6: Does well at home but refuses at school or playground
Why: Generalization hasn't occurred yet. Skills learned in one setting need deliberate practice in others. Next time: Share the protocol with teachers using the School Communication Template (Card 37). Gradually introduce materials in school context with the same invitation language.
Problem 7: No improvement after 3 weeks of daily sessions
Why: Possible underlying medical factor; or intensity not progressive enough; or baseline wasn't established correctly. Next time: Call 9100 181 181. Request PT assessment. Check whether medical factors were fully cleared. Review data — sometimes improvement is real but subtle.
Adapt and Personalize — No Two Children Are Identical
This card is yours to customize. Every child has a unique sensory profile, motor history, and motivation system. Use these adaptations to design the version of F-580 that fits your child precisely.
For Sensory Seekers (needs MORE input)
- Add weighted vest during activities (PT-approved)
- Use resistance bands with obstacle course
- Swimming with hand paddles for more resistance
- Add ball-carrying to obstacle course
- Bounce while holding a heavy therapy ball
For Sensory Avoiders (needs GENTLER approach)
- Start with quieter materials (bike > trampoline)
- Provide choice always — never surprise with new materials
- Short sessions (3–5 min) for longer duration weeks
- Swimming is often preferred (input is distributed)
- Use visuals to show what's coming and when it will end
For Low Muscle Tone / Hypotonia
- Swimming primary (buoyancy reduces load)
- Scooter board prone position (builds postural muscles)
- Resistance bands light (builds muscular endurance gently)
- Avoid high-impact jumping until PT clearance
- Focus on sustained movement over high-intensity bursts
For High Motor Drive / Very Active Profile
- Longer obstacle courses
- Bike with slight incline
- Add time challenge elements
- Multiple activities in one session
- Track records and celebrate improvements daily
Age | Preferred Materials | Duration Target | Key Principle | |
3–4 | Trampoline, balance bike, water play | 5–8 min | Fun first, zero pressure | |
5–6 | Obstacle course, jump rope basics, scooter | 8–12 min | Measurable challenge | |
7–9 | Bike, swim, jump rope, fitness tracker | 12–20 min | Progress tracking motivates | |
10–12 | Full kit, movement games, progressive targets | 20–30 min | Personal record focus |

ACT IV: The Progress Arc
Weeks 1–2: Establishing the Baseline
Progress is invisible — but it's happening. This is the phase where the foundation is poured. You just can't see it yet.
What You May See ✅
- Child is willing to try the material (even briefly)
- Child tolerates the activity for 1–5 minutes without distress
- Reduced resistance compared to first introduction
- Child asks "again?" at least once during the week
What Is Not Progress Yet (and that's normal) ❌
- Child's endurance hasn't noticeably increased — physiological adaptation takes 3–4 weeks
- Child still gets tired quickly — the pattern hasn't broken yet
- Child still prefers to sit — habit change is slow
What Is Actually Happening (invisible to the eye)
The cardiovascular system is beginning to adapt. Slow-twitch muscle fibres are receiving their first consistent training signal. Neural pathways linking "this activity = safe and enjoyable" are forming. The foundation is being poured.
"If your child tolerates the activity for 3 seconds longer than last week — that is real progress. Measure it. Celebrate it. 3 seconds this week, 30 seconds next week, 3 minutes next month."
Systematic review (Children, 2024): Early-phase indicators focus on tolerance and participation rather than skill mastery or endurance duration. PMC11506176

Weeks 3–4: Consolidation Signs
Neural pathways are forming. Watch for these specific behaviors — they are the clinical signal that the intervention is working beneath the surface.
Anticipates the Activity
Child goes to the equipment without being prompted — the habit is forming.
Duration Increased
Even 2–3 extra minutes is consolidation. Recovery time after activity is noticeably shorter than week 1.
Mentions Activity Outside Sessions
"Can we do the trampoline?" — The activity is entering the child's internal world.
Pride at Completion
Child shows satisfaction at finishing. Resistance at session start has reduced or disappeared.
When to Increase Intensity
If your child is completing sessions with clear energy remaining — increase by 10–15%. If sessions are still at capacity — maintain duration and focus on consistency. Never chase progress at the cost of willingness.
"You may notice you're more confident too. You know the routine. You know how your child responds. You know what works. That parental confidence is therapeutic in itself — children read it."

Weeks 5–8: Mastery Indicators
The upward spiral. Endurance unlocks participation — and participation builds more endurance. This is the phase where the work becomes visible to the world.
🏆 Physical Endurance Milestone — Unlock Criteria
- Child sustains activity for double the week 1 duration
- Child self-initiates activity at least once without prompting
- Child participates in one real-world activity (playground, PE, family walk) for longer than before
- Child reports feeling less tired or asks to continue when before they would have stopped
Generalization Indicators — The Gold Standard
The most important sign of mastery: skills appearing outside the structured session.
- Child runs longer at playground without stopping
- Child finishes PE class without sitting out
- Family walk extended compared to month 1
- Child joins physical play with peers spontaneously
Maintenance Check
Take one week at reduced intensity. If endurance holds — mastery is consolidated. If it drops quickly — continue sessions at current intensity for 2 more weeks before testing again.

You Did This. Your Child Grew Because of Your Commitment.
Eight weeks ago, your child sat on the bench while others ran. You found 9 materials. You showed up daily. You counted the seconds. You celebrated the tiny wins nobody else noticed — 3 extra seconds on the trampoline, one more lap around the course, one morning they picked up the jump rope without being asked.
You didn't need perfect conditions. You needed consistency, warmth, and belief in what's possible. Your child's body responded. Because bodies always respond to the right conditions.
Week 1 Baseline
___ minutes of sustained activity · Starting material: ___
Week 8 Achievement
___ minutes of sustained activity · New materials mastered: ___
Real-World Evidence
Family walks / PE class / playground sessions now lasting longer than before week 1
Family Celebration Suggestion: Mark this milestone with a physical adventure — a longer family walk, a new bike route, a swim at a new pool. Let the celebration itself be an endurance activity. 📸 Take a photo of your child doing the activity that was hardest on day 1. That photo is evidence. Save it.
Red Flags: When to Pause Even in the Celebration Zone
Progress is real and meaningful — and these specific signs still require you to pause and seek guidance. They are not common, but they must not be ignored.
What You See | Why It Matters | What to Do | |
Child cannot recover breath within 5 minutes of stopping | May indicate cardiac or respiratory issue not previously identified | Stop activity. Rest. Two occurrences → pediatrician review before resuming. | |
Joints are swollen or child reports joint pain after activity | May indicate hypermobility-related injury or overuse | Reduce impact activities. PT assessment. | |
Progress has completely plateaued for 3+ weeks despite daily sessions | May indicate medical factor, motor planning issue, or programming mismatch | Call 9100 181 181. Request PT review. | |
Child becomes extremely fatigued for hours after a moderate session | May indicate metabolic, thyroid, or anemia-related factors | Pediatrician evaluation — rule out systemic causes. | |
Child's behavior significantly worsens during or after sessions | May indicate sensory overwhelm or autonomic regulation challenge | Reduce intensity. OT sensory profile assessment. | |
Child reports pain during activity (not tiredness — pain) | Must be investigated — do not push through pain | Stop. Rest. Medical evaluation before resuming. |
Escalation Pathway: 1st occurrence → Note in tracker, monitor. 2nd occurrence → Call 9100 181 181 for teleconsultation. 3rd occurrence → In-clinic evaluation. Urgent (breathlessness, unresponsiveness) → Emergency services first. 📞FREE Helpline: 9100 181 181 — Available 24×7
The Progression Pathway — Where F-580 Sits
You're not done. You're on a journey. Physical endurance is foundational to participation across all gross motor domains — and it opens the door to the next techniques in the sequence.
The most important sign of readiness to progress: skills are appearing outside the structured session. Use this guide to choose your next technique.
If endurance improved but... | Proceed to... | |
Core stability is weak (slumps while sitting) | F-581: Core Strength | |
Upper body tires quickly (arms weak) | F-582: Upper Body Strength | |
Leg strength is the primary limit | F-583: Lower Body Strength | |
All areas improved equally | F-581 → F-582 → F-583 in sequence |
Long-Term Developmental Goal: Full participation in organized sports, school physical education, family physical activities, and age-appropriate active play — with stamina comparable to peers.

Explore Adjacent Techniques in Gross Motor Domain F
Based on the 9 materials in F-580, you already own what you need for several adjacent techniques. Explore the full domain at your own pace.
F-578: Running Coordination
Obstacle Course · Lateral agility · Motor planning for running gait. CORE technique.
F-579: Jumping Skills
Trampoline · Jump Rope · Bilateral coordination. CORE technique.
F-580: Physical Endurance
★ YOU ARE HERE — All 9 materials active. Cardiovascular + muscular stamina.
F-581: Core Strength
Therapy Ball · Resistance Bands. ADVANCED — recommended next step.
F-582: Upper Body Strength
Resistance Bands · Scooter Board. ADVANCED.
F-584: Low Muscle Tone (Hypotonia)
Swimming · Scooter Board · Whole-body low-impact endurance.
Materials you already own for adjacent techniques: F-581 (resistance bands, therapy ball) · F-582 (resistance bands, scooter board) · F-579 (trampoline, jump rope) — no additional purchases required.
Your Child's Full Developmental Map
F-580 is one piece of a larger plan. The Pinnacle Blooms Network tracks 12 developmental domains — and your work in Gross Motor feeds directly into several others.
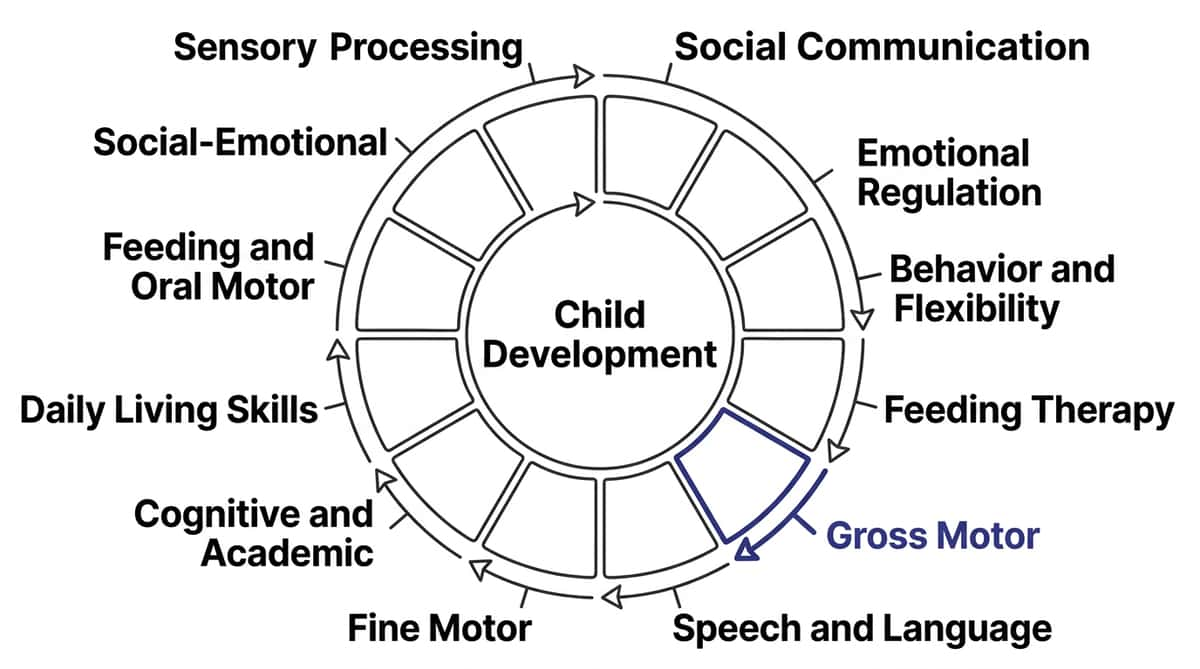
F-580 Feeds Directly Into:
- Domain F (Gross Motor): Primary domain — cardiovascular and muscular endurance
- Domain C (Emotional Regulation): Physical activity regulates the nervous system
- Domain J (Daily Living): Family participation restored — walks, outings, sports days
GPT-OS® Integration
Your child's GPT-OS® profile shows all 12 domains, tracks your AbilityScore® across each, and identifies which techniques to run in parallel for maximum convergent impact. Every data point from F-580 sessions improves recommendations for all children with similar profiles globally.

ACT V: Community & Ecosystem
Three Families. Three Starting Points. One Direction: Forward.

Arjun, 5 years — Mumbai | Autism + Hypotonia
Before: Could not complete a 5-minute walk to school without asking to be carried. Playground visits ended within 10 minutes. Refused school sports day entirely.
Intervention: Mini trampoline daily (started at 3 minutes). Obstacle course twice weekly. Swimming Saturday mornings.
Week 8: Walks 15 minutes to school independently. Playground sessions now 35 minutes. Completed the school sports day — sitting out for only one event.
"He went from exhausted after five minutes to completing a family hike. His confidence changed too. He now asks to go to the park instead of asking to leave." — Mother, Pinnacle Network Mumbai

Priya, 8 years — Hyderabad | ADHD + DCD
Before: Always last in PE class. Sat out of relay races, refused swimming lessons, cried every sports day. Endurance test: 4 minutes of sustained aerobic activity.
Intervention: Jump rope with measurable progress. Bike rides with distance targets. Fitness tracker step challenge with father.
Week 10: Sustained 18 minutes of continuous activity. Joined the school swimming team. Sports day — participated in all events.
"The fitness tracker was everything for her. She became obsessed with beating her own step count. Exercise became something she was proud of, not something she was afraid of." — Father, Pinnacle Network Hyderabad

Rohan, 4 years — Bengaluru | Global Developmental Delay
Before: Tired after 3 minutes of active play. PT report noted "significant endurance deficit" and "very low baseline cardiovascular fitness."
Intervention: 5-minute daily bouncing (mattress — zero cost). Scooter board twice weekly. Parent-paced bike ride 3× per week.
Week 12: Sustained 14 minutes of continuous trampoline activity. First birthday party attended fully — played with other children for 40 minutes without asking to leave.
"We started with a mattress and a dream. Now he runs to the trampoline every morning before breakfast." — Mother, Pinnacle Network Bengaluru
Note: All case descriptions are illustrative and anonymized. Individual outcomes vary by child profile, underlying factors, and intervention consistency.
Connect With Other Parents — Isolation Is the Enemy of Adherence
You don't have to do this alone. Thousands of families across India and 70+ countries are navigating the same journey. Community connection is a clinical multiplier — parents who connect adhere longer and achieve better outcomes.
📱 Pinnacle Parents WhatsApp Community
Physical Endurance & Motor Development group. Daily tips, real-time support, session wins shared, questions answered by experienced parents and Pinnacle therapists.
💬 Online Discussion Forum
Topic threads: "Mini Trampoline Sessions" | "Building Bike Confidence" | "Swimming for Hypotonia" | "Jump Rope Progress Logs." pinnacleblooms.org/community
🤝 Peer Mentor Connection
Connect with a parent who has completed F-580 and F-581. Real-world guidance from someone who has been exactly where you are right now.
🏫 Local Parent Meetups
Pinnacle centers host monthly Parent Movement Sessions — parents bring children, therapists guide, families connect in person.
📞FREE National Autism Helpline: 9100 181 181 — If you need someone to talk to about your child's journey, call us. Free. 24×7. 16+ languages.

Your Professional Support Team — Home + Clinic = Maximum Impact
Research shows home-based intervention produces maximum impact when designed by a professional and executed by a trained parent. The clinic provides the prescription. The home provides the dose. Together — this is how 97%+ improvement happens.
Professional | Role in F-580 | Access | |
Pediatric Physical Therapist | Endurance baseline assessment, progressive programming, hypotonia management | Book Appointment | |
Pediatric OT | Sensory-motor integration, adaptive equipment selection, home program design | Book Appointment | |
BCBA / ABA Therapist | Reinforcement design, session motivation, habit formation architecture | Book Appointment | |
NeuroDev Pediatrician | Medical clearance, hypotonia diagnosis, co-occurring conditions | Book Appointment |
Teleconsultation — For Remote Families
Cannot travel to a center? Our therapists provide video-based assessment and home program design. Available in 16+ languages.
Find a Center
70+ Pinnacle Blooms centers across India. Filter by: Physical Therapy | Occupational Therapy | ABA | Integrated Assessment.
📞FREE National Autism Helpline: 9100 181 181

The Research Library — For the Parent Who Wants to Go Deeper
The evidence is all here. For the clinician presenting this to a skeptic, and for the parent who needs to know this is real.
PRISMA Systematic Review 2024
16 articles from 2013–2023 confirm structured physical intervention meets evidence-based practice criteria for children with ASD. Outcomes: improved cardiovascular fitness, activity tolerance, and social participation. PMC11506176
Meta-Analysis 2024 — World J Clin Cases
24 studies confirm structured physical activity promotes gross motor skills, cardiovascular fitness, adaptive behavior, and social participation in children with ASD. DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT 2019 — Padmanabha et al.
Home-based structured intervention demonstrated significant improvements in developmental outcomes in Indian pediatric population. Validates context-specific applicability of international evidence. DOI: 10.1007/s12098-018-2747-4
WHO Care for Child Development Package
Implemented across 54 low- and middle-income countries. Household-material-based interventions show efficacy across motor domains. Equity in access is a core principle. PMC9978394
NCAEP Evidence-Based Practices Report 2020
Movement-based interventions classified as evidence-based practice for autism. Video modeling, physical activity, and structured exercise are among the top-tier evidence categories. NCAEP 2020
Evidence Pyramid
Systematic Reviews
PMC11506176 · PMC10955541
RCTs
DOI:10.1007/s12098-018-2747-4
Cohort Studies
PMC9978394 (WHO CCD Package)
Clinical Consensus
NCAEP 2020 · BACB Guidelines · WHO GAPPA 2018
How GPT-OS® Uses Your Data
Your data helps your child — and every child like yours. Session data feeds a population intelligence layer that continuously improves recommendations for all families globally.
What GPT-OS® Learns From F-580 Data
- Which of the 9 materials produces best engagement for this child's profile
- Rate of endurance improvement (for prognosis calibration)
- Session timing that produces best outcomes
- Early warning patterns that predict sessions likely to fail
Data Protection
- ✓ PDPA compliant
- ✓ Individual data never sold
- ✓ Aggregated only for population AI improvement
- ✓ Parent controls all data sharing settings
- ✓ Right to delete at any time
21 RCTs, 1,050 participants confirm gamified digital health tracking produces measurable improvements in intervention engagement and outcomes. 2024 Meta-Analysis.

Watch the Reel — All 9 Materials in 60 Seconds
Watch a Pinnacle therapist demonstrate all 9 materials — with parent-child interaction shown for each, clinical rationale in on-screen text, and the full progress arc from bench-sitting to active participation.

▶ F-580: "9 Materials That Help With Physical Endurance" 60-second educational reel · Gross Motor Domain · Episode 580 of 999
When they run out of energy before other kids.
This Reel Shows:
- All 9 materials demonstrated briefly in sequence
- Parent-child interaction shown for each material
- Clinical rationale for each material in on-screen text
- Progress arc: from bench-sitting to active participation
- Pinnacle Consortium introduction and validation
Related Reels in Series:
← F-579
9 Materials That Help With Jumping Skills
→ F-581
9 Materials That Help With Core Strength
Video Modeling Evidence: Classified as evidence-based practice for autism (NCAEP, 2020). Multi-modal learning (visual + text + demonstration) improves parent skill acquisition compared to text-only resources.

Share This With Your Family — If Only One Caregiver Uses This, the Impact Is Halved
Consistency across caregivers multiplies impact. A technique executed 5× per week across multiple caregivers produces outcomes no single caregiver can achieve alone. Share this page today.
WhatsApp Template (Pre-Filled)
"[Name], I found this technique page for building physical endurance in children — it's from Pinnacle Blooms and has 9 materials + a full step-by-step protocol. Really helpful for [child's name]. Here's the link: techniques.pinnacleblooms.org/gross-motor/physical-endurance-F-580"
"Explain to Grandparents" Version
"[Child's name] is doing an endurance-building program with 9 activities — trampoline, bike, obstacle course, jump rope, swimming, and others. They need to do one activity for [X] minutes every day. When you're with them: encourage them to keep going, count out loud with them, celebrate when they finish. Don't carry them or let them stop too early — but also never force if they're distressed. Call [parent] if unsure."
Also Available to Download
- F-580 in 1 Page — Simplified version for grandparents, aunts/uncles, babysitters, school teachers
- School Communication Letter Template — Explains the program, requests PE accommodation, provides movement break suggestions

ACT VI: Close
Frequently Asked Questions — Answered by the Pinnacle Consortium
Q1: My child has hypotonia (low muscle tone). Is it safe to do jumping activities?
Begin with low-impact activities: swimming, scooter board, and bike riding. These build endurance without the joint loading that jumping creates. Once a physical therapist has confirmed readiness, trampoline and jump rope can be progressively introduced. Call 9100 181 181 for a free consultation on your child's specific profile.
Q2: How many of the 9 materials should I buy to start?
Start with one or two that are accessible and appealing to your child. A jump rope (₹100) + DIY obstacle course (₹0) is a complete starting kit. Add materials as the routine establishes and your child responds well. The mini trampoline is the highest-return single purchase if your budget allows one item.
Q3: My child has autism and doesn't like being sweaty or physically uncomfortable.
Strategies: (1) Start with shorter sessions before discomfort sets in. (2) Use swimming — water regulates temperature naturally. (3) Provide sensory comfort items nearby. (4) Build in sensory breaks with preferred calm activities. An OT assessment adds enormous value here — they can select the most tolerable activities for your child's specific sensory profile. Call 9100 181 181.
Q4: We've been doing this for 2 weeks and I see no improvement. Should I continue?
Yes — expect improvement from weeks 3–4, not weeks 1–2. If you're at 2 weeks and see engagement (child is willing to participate even briefly), you are succeeding. Endurance improvement becomes observable in weeks 3–5. If there is no engagement or willingness after 3 weeks, call us — there may be a technique adjustment needed.
Q5: Can my child do two or three of these activities in one session?
Absolutely — rotating between 2 materials is often more effective than one material for 20 minutes. The variety maintains engagement and works different muscle groups. A session might be: 5 min trampoline → obstacle course 2 rounds → jump rope 30 jumps. This is a complete endurance session.
Q6: My child is 3 years old. Which materials are appropriate?
For ages 3–4: Trampoline with handle (supervised), balance bike, water play, and a simple 2–3 obstacle course are ideal. Jump rope is usually appropriate by age 4–5. Swimming is appropriate from infancy with a parent in the water. Resistance bands typically from age 5 with adult supervision. Fitness tracker at 4+.
Q7: How does this connect to my child's therapy at the Pinnacle center?
F-580 is designed as the home extension of the clinical gross motor program. Your Pinnacle OT/PT designs the clinical program; F-580 gives you the daily home dose that compounds the clinic's work. When you log data in GPT-OS®, your therapist sees your child's home response and calibrates clinic sessions accordingly. Home + clinic = maximum impact.
Q8: When will my child be able to participate in PE class like their peers?
For most children who begin F-580 with daily practice, meaningful PE participation improvement is visible by week 6–8. Full peer-comparable participation typically requires 3–6 months of consistent practice, depending on starting point and underlying factors. Children with hypotonia may require 6–12 months. Progress is real — it's a matter of timeline, not direction.
Didn't find your answer? 📞9100 181 181 — FREE. 24×7. 16+ Languages.

Your Next Step: Start Now
Your child's endurance will not build from reading about it. It builds from 5 minutes of consistent, daily, joyful movement. The best time to start was a month ago. The second best time is today.
✦ Validated by the Pinnacle Blooms Consortium ✦
OT • PT • ABA • SpEd • NeuroDev • CRO • WHO-Aligned • UNICEF-Aligned
20M+ Sessions · 97%+ Improvement
70+ Centers · Children from 70+ Countries · 16+ Languages
📞 FREE National Autism Helpline: 9100 181 181 · 24×7 · 16+ Languages
Preview of 9 materials that help with physical endurance Therapy Material
Below is a visual preview of 9 materials that help with physical endurance therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Pinnacle Promise
"From fear to mastery. One technique at a time." — The Pinnacle Blooms Consortium
NeuroDev Pediatrics
Medical clearance, hypotonia diagnosis, metabolic assessment, medication review.
Occupational Therapy
Sensory-motor integration, adaptive equipment, home program design.
Speech-Language Pathology
Communication during activity, social participation, instruction comprehension.
ABA / BCBA
Reinforcement architecture, habit formation, data-driven session design.
Special Education
PE accommodations, classroom movement breaks, school activity planning.
WHO / UNICEF Aligned
Nurturing Care Framework · Care for Child Development Package · Global Action Plan on Physical Activity.
21M+
Therapy Sessions
Exclusive 1:1 sessions delivered across the Pinnacle network.
97%+
Measured Improvement
Across enrolled children with consistent home + clinic protocol.
70+
Centers in India
Children from 70+ countries served. 16+ languages supported.
← F-579: Jumping Skills
🏠 Return to Top
F-581: Core Strength →
Medical Disclaimer: This content is educational and informational. It does not constitute individualized medical advice and does not replace assessment and intervention by licensed physical therapists, pediatricians, occupational therapists, or other healthcare professionals. Physical endurance challenges in children can have various underlying causes. Medical evaluation is recommended to rule out cardiac, respiratory, metabolic, or other medical conditions before beginning any exercise program. Children with known health conditions should not begin new physical programs without explicit medical clearance. Always consult qualified healthcare providers. Individual results vary by child profile, underlying factors, and intervention consistency.
Legal: Company: Bharath Healthcare Laboratories Pvt. Ltd. · CIN: U74999TG2016PTC113063 · DPIIT Recognition: DIPP8651 · MSME: Udyog Aadhaar TS20F0009606 · GSTIN: 36AAGCB9722P1Z2 · © 2026 Pinnacle Blooms Network®. All rights reserved. GPT-OS® · TherapeuticAI® · AbilityScore® · FusionModule™ · EverydayTherapyProgramme™ are trademarks of Bharath Healthcare Laboratories Pvt. Ltd. Patents filed in 160+ countries.
📞 9100 181 181 (FREE National Autism Helpline) · 🌐pinnacleblooms.org · care@pinnacleblooms.org · 📍 70+ Centers across India