
When holding a pencil is the hardest part of writing
It's 7 PM on a Tuesday. Your child has been sitting at the kitchen table for 40 minutes, trying to write five sentences for homework. Their hand is cramped around the pencil like a fist, the letters are shaky and barely legible, and the eraser has worn through to the page twice. The teacher sent home a note last week about "grip concerns." You've shown them the "right way" a dozen times — they try for three seconds and go right back. You don't know if this is normal, if you're missing something, or if you're already too late.
You are not failing. Your child's hand is still learning what it needs to know.
🌸 Pinnacle Blooms Consortium
OT Lead
Fine Motor Development Series
Episode F-593
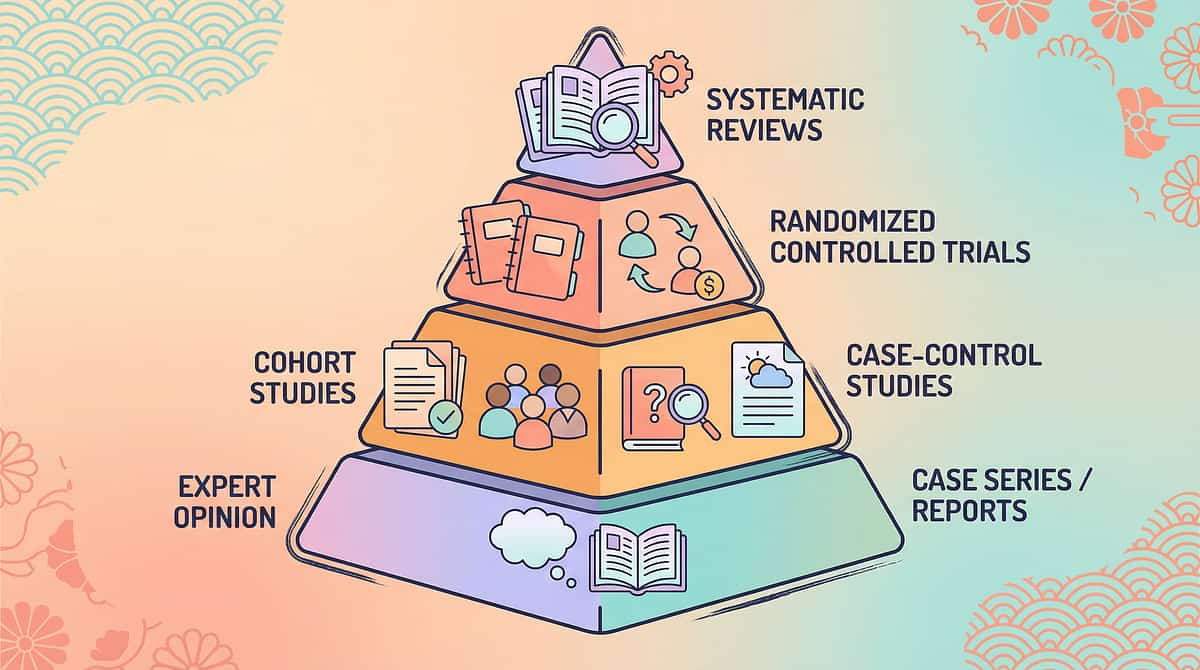
WHO Nurturing Care Framework (2018): Early caregiver awareness and action directly shapes the developmental trajectory. Recognition is the first therapeutic act. Reference: nurturing-care.org/ncf-for-ecd/
Millions of children worldwide struggle with pencil grasp. The science is clear — and so is the path forward.
1 in 3
Immature Grasp Patterns
Children entering primary school show immature pencil grasp patterns that affect their writing
80%+
ASD or DCD Impact
Children with ASD or DCD display fine motor challenges including grip difficulties that impact academic participation
6–8 wks
Typical Improvement Timeline
Typical timeline for measurable improvement when evidence-based materials and daily practice are combined
In India, studies across government and private schools show 28–40% of children in Class 1–3 have pencil grasp patterns that impair handwriting legibility and speed. With 250+ million school-enrolled children, this represents tens of millions of families navigating this challenge today.
"If your child struggles to hold a pencil, they are among the most commonly referred children in every occupational therapy clinic in India and worldwide. This is not rare. This is not permanent." — Pinnacle OT Consortium
PRISMA Systematic Review (2024): Sensory integration and fine motor interventions show consistent positive outcomes across pediatric populations. Meta-analysis: fine motor skill development directly predicts academic readiness. References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260

Pencil grasp isn't stubbornness. It's neuromuscular architecture — and it can be built.
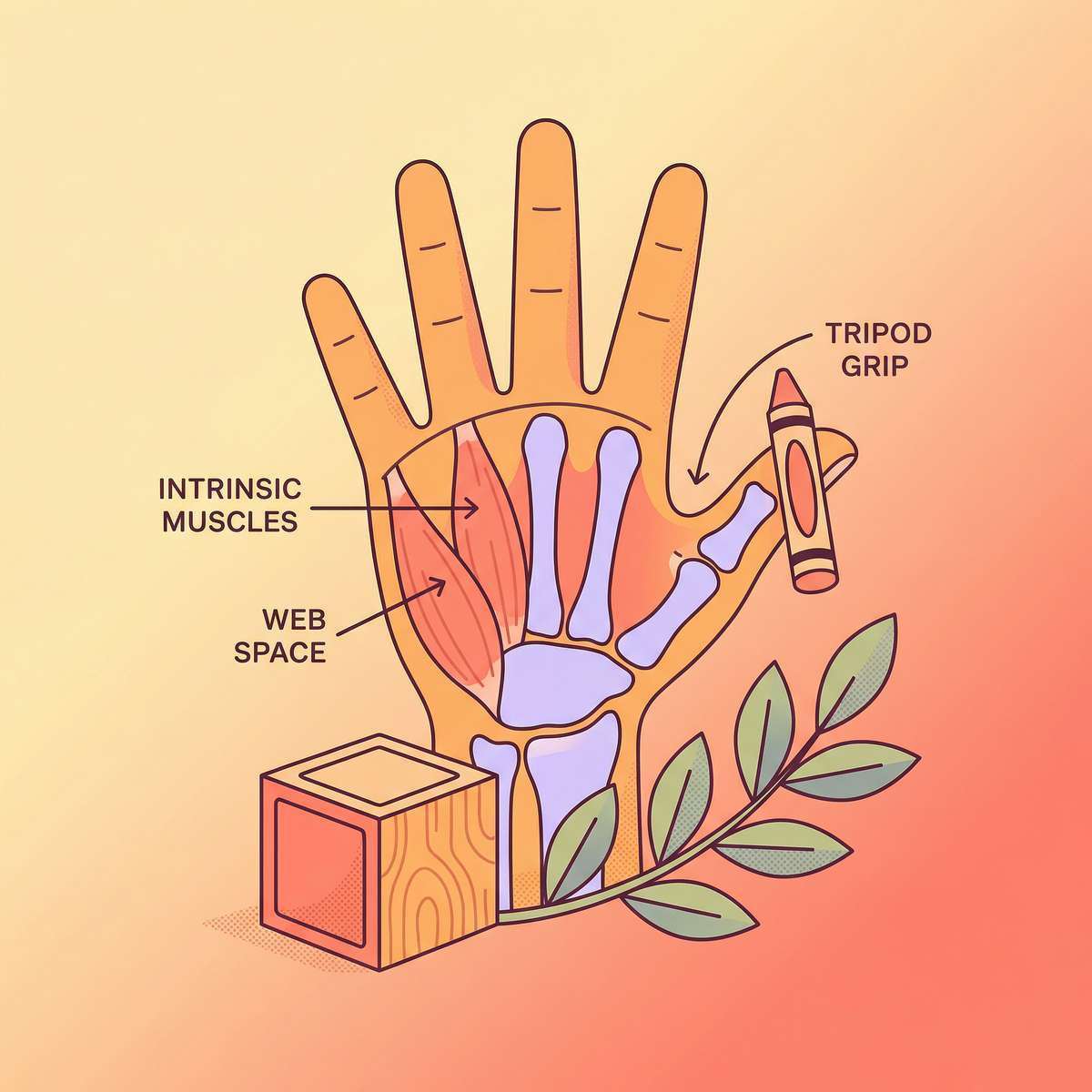
Intrinsic muscles
The engine of dynamic finger movement
Web space
Must be open and round for mature grasp
Tripod trio
Thumb + index + middle = the writing team
Stability base
Ring + pinky curled into palm
Wrist position
Slight extension = optimal control
Your child's pencil grasp is controlled by a network of tiny hand muscles called intrinsic muscles — not the big muscles of the forearm. These muscles require months of play, squeezing, pinching, and fine manipulation to develop strength and coordination.
When these muscles are still developing, the brain compensates by recruiting bigger muscles — and the child wraps their entire hand around the pencil (fist grip), or uses their whole wrist or arm to move it instead of just their fingers.
This isn't laziness or defiance. The neural pathways for dynamic finger movement are still forming. The right materials accelerate this process — they train the hand at the neurological level, not just the mechanical one.
🧠The Dynamic Tripod Principle: A mature pencil grasp uses the thumb, index, and middle finger as the movement team while the ring and pinky fingers tuck into the palm as the stability base. "Dynamic" means the fingers move the pencil — not the wrist. This transition takes time, the right inputs, and zero shame.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework confirming neurological basis for sensory-motor based interventions in childhood development — wiring differences respond to structured environmental input. Reference: DOI: 10.3389/fnint.2020.556660
Grasp patterns follow a predictable developmental sequence. Here is where your child is — and where they're heading.
1–1.5 yrs
Palmar Supinate
Whole fist, shoulder movement
Whole fist, shoulder movement
2–3 yrs
Digital Pronate
All fingers pointing down, shoulder/elbow movement
All fingers pointing down, shoulder/elbow movement
3.5–4 yrs
Static Tripod
3-finger hold but wrist moves the tool
3-finger hold but wrist moves the tool
4.5–6 yrs
Dynamic Tripod
Fingers move the pencil — not wrist
Fingers move the pencil — not wrist
6–7 yrs
Mastery
Automatic, efficient, sustainable
Automatic, efficient, sustainable
📍Common Intervention Zone: Most children referred for pencil grasp concerns are progressing through the static-to-dynamic transition. This is the highest-leverage intervention window. Materials and structured play accelerate what would take years to develop by chance.
Common co-occurring factors that can delay grasp progression:
Hypotonia
Low muscle tone affects intrinsic hand muscle strength
Autism Spectrum
Sensory sensitivities to tool textures, proprioceptive differences
DCD
Developmental Coordination Disorder affects motor learning speed
ADHD
Affects sustained attention during practice
Each of these has specific material adaptations. This page addresses all of them.
WHO Care for Child Development (CCD) Package: Evidence-based age-specific guidance implemented in 54 low- and middle-income countries. UNICEF MICS developmental monitoring across 197 countries establishes fine motor milestones as key school-readiness indicators. References: PMC9978394 | WHO/UNICEF CCD Package (2023)
These 9 materials are not guesswork. They are clinically validated, occupational-therapy-prescribed, and proven across 20M+ sessions.
PRISMA Systematic Review (2024) — Level I
Sensory integration and fine motor interventions meet evidence-based practice criteria for children with developmental challenges. 16 studies, 2013–2023, consistent positive outcomes.
Indian RCT — Padmanabha et al. (2019) — Level II
Home-based interventions using modified tools and structured activities demonstrated significant fine motor and handwriting outcomes in the Indian pediatric population.
Meta-Analysis, World J Clin Cases (2024) — Level I
Sensory-motor interventions effectively promoted fine motor skills, adaptive behavior, and school readiness across 24 studies.
"Clinically validated. Home-applicable. Parent-proven. Every material on this page has been deployed in Pinnacle Blooms centers across India's 70+ locations and refined through 20M+ exclusive 1:1 therapy sessions."
📞 FREE National Autism & Child Development Helpline: 9100 181 181 | 16+ languages | 24×7
References: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4 | NCAEP 2020 | WHO NCF 2018

ACT II: THE KNOWLEDGE TRANSFER
Cards 06–12
The Technique: What It Is
Pencil Grasp Development Through Adaptive Materials
Parent-friendly alias: "Building the Hand That Writes"
Pencil grasp development refers to the progressive maturation of how a child holds writing tools — from immature whole-hand fist grips through transitional patterns toward the mature dynamic tripod grasp (or functional quadrupod alternative). This process depends on multiple underlying skills: intrinsic hand muscle strength, finger isolation and independent movement, thumb opposition stability, open web space, and wrist positioning. This technique introduces 9 clinically selected materials that address these underlying components — not by correcting the child's grip directly, but by building the neurological and muscular foundation that makes a mature, functional grasp possible and sustainable.
Domain
Fine Motor Skills / Handwriting Readiness · Tool Modifications · Strengthening Materials · Positioning Supports · Precursor Skill Training
Age Range
3–10 years
Session Duration
10–20 minutes daily · Minimum 4×/week for accelerated progress
Episode
F-593 | Fine Motor Development Series

Pencil grasp sits at the intersection of five clinical disciplines. Here is how each one uses these materials.
🖐 Occupational Therapy (OT) — PRIMARY LEAD
OT is the primary discipline for pencil grasp development. OTs assess intrinsic hand muscle strength, finger isolation, wrist position, and sensory processing to identify the specific underlying deficit. They prescribe the exact combination of materials, grade the resistance, and progress the protocol. All 9 materials on this page are standard OT clinical tools.
🗣 Speech-Language Pathology (SLP) — SECONDARY
SLPs use fine motor materials during tabletop activities that also target communication. A child using therapy putty while naming objects, or using tweezers to build a scene for storytelling, integrates fine motor and language targets simultaneously — doubling therapeutic efficiency.
📊 ABA/BCBA — BEHAVIORAL INTEGRATION
ABA therapists use reinforcement principles to build the repetition needed for grasp pattern change. Correct finger placement → immediate specific praise → token economy progression. ABA also addresses avoidance behavior through systematic desensitization using modified tools.
🎓 Special Education (SpEd) — CLASSROOM EXTENSION
Special educators implement pencil grasp strategies in the classroom context, ensuring modified tools are available during academic work and that school tasks are graded to match the child's current grasp development level.
🧠 NeuroDev Pediatrics — MEDICAL OVERSIGHT
Neurodevelopmental pediatricians rule out underlying medical conditions (hypotonia, cerebral palsy, neurological conditions) that affect grasp and coordinate with OT on material selection and therapeutic intensity.
"The brain doesn't organize by therapy type. Pencil grasp requires the strength from OT, the repetition from ABA, the language integration from SLP, and the daily practice from SpEd — all working from the same clinical plan. This is why GPT-OS® FusionModule™ converges all five disciplines into one coordinated protocol."
WHO/UNICEF Adapted Nurturing Care Framework for SLPs (2022): Multi-disciplinary convergence produces superior outcomes to single-discipline delivery. Reference: DOI: 10.1080/17549507.2022.2141327

Material 1: Broken Crayons / Short Pencils
Tool Modifications
OT-Prescribed
₹0
How It Works
Eliminates fist grip by physical impossibility. A 2–3 cm crayon stub simply cannot fit inside a closed fist. The small size forces tripod positioning automatically — without any instruction, correction, or demand placed on the child.
What You Need
Cost: ₹0 — Break any existing crayons to 2–3 cm. Peel the wrapper for better grip feedback and sensory input.
Buy it: Search "golf pencils" or "short crayons" on Amazon.in
Why It's First on This List
This is the most immediately impactful modification in pediatric OT. It requires no purchase, no instruction, and no cooperation from the child — just a shorter crayon. Start tonight.
Material 2: Pencil Grips (Various Types)
Tool Modifications
OT-Prescribed
₹100–500
How It Works
Physical barriers and tactile cues guide finger position. The grip creates three resting points — one per tripod finger — so the brain receives proprioceptive feedback about where each finger belongs. Different designs (triangular, grotto, crossover) solve different grip problems.
Choosing the Right Grip
- Triangular grip: General guidance, low sensory demand
- Grotto grip: For children who wrap thumb over index finger
- Crossover grip: For thumb-crossing patterns
Cost: ₹100–500 (variety pack recommended — try multiple types)

Material 3: Therapy Putty / Hand Strengthening Putty
Strengthening Materials
OT-Prescribed
₹300–800
How It Works
Graded resistance builds intrinsic hand muscles — specifically the thumb opposition muscles, interosseous muscles, and lumbricals. These are the exact muscles that power dynamic grasp. Color-coded resistance levels (soft → extra firm) allow progressive loading as strength develops.
Therapeutic Exercises
- Pinch with tripod fingers (mirrors pencil grasp exactly)
- Hide small objects inside — find with fingertips only
- Roll into a snake using fingertip pressure
- Flatten with thumb and forefinger only
Cost: ₹300–800 (multi-resistance set)
Buy it:Amazon.in: Therapy Putty Set

Material 4: Vertical Surfaces (Easel / Chalkboard / Wall)
Positioning Supports
OT-Prescribed
₹0 → ₹3,000
How It Works
Vertical work automatically extends the wrist into optimal writing position and loads the shoulder — providing the proximal stability that enables distal precision. The physics of drawing on a wall does the therapeutic work without any instruction. Gravity becomes the therapist.
Zero-Cost Setup
Tape paper to the wall at shoulder height — this is therapeutically identical to a ₹3,000 easel. The mechanism is wrist extension, not the surface material.
- Paper taped to wall: ₹0
- Window + washable markers: ₹0
- Bathroom mirror + bath crayons: ₹0
- Children's easel: ₹2,000–3,000

Material 5: Tweezers & Small Tongs
Precursor Skill Training
OT-Prescribed
₹150–500
How It Works
Tweezers require the identical finger positioning as a tripod pencil grasp — but with dramatically clearer sensory feedback and immediately measurable results. Each successful pick-up reinforces the tripod pattern. A single sorting activity can produce hundreds of tripod-position repetitions.
Activity Ideas
- Transfer pom poms between bowls (easy)
- Sort objects by color with tweezers (standard)
- Timed challenge: how many in 60 seconds? (advanced)
- Place small objects on a picture to "decorate" it
Cost: ₹150–500 (variety set — different sizes = different difficulty)
Material 6: Clothespins
Strengthening Materials
OT-Prescribed
₹50–200
How It Works
Spring resistance directly targets thumb opposition and pinch endurance — the specific stamina that prevents grasp collapse during extended writing tasks. When a child's writing deteriorates after 5 minutes, clothespin training is often the direct solution. It builds the muscles that hold the grasp up for a full homework session.
Progressive Challenge
- Clip around a paper plate edge (visual guide, easy)
- Clip onto a string held between two points
- Build a caterpillar — clip each to the previous one
- Mini clothespins for advanced challenge
Cost: ₹50–200 (pack of 20 wooden clothespins)
Material 7: Cotton Ball / Pom Pom in Palm
Positioning Supports
OT-Prescribed
₹50–100
How It Works
Forces the ring and pinky fingers into the tucked position — creating the stable palm base that frees the tripod fingers for precision movement. The pom pom provides proprioceptive feedback about where the stability fingers are. "Keep the pom pom sleeping in your hand while you draw" is one of the most effective single instructions in pediatric OT.
How to Use It
- Place a small pom pom or cotton ball in the child's palm
- Have ring and pinky fingers close around it
- Then hand the pencil or crayon to the tripod fingers
- Begin drawing or writing activity
Cost: ₹50–100 · Any small cotton ball works identically

Material 8: Finger Isolation Games & Tools
Precursor Skill Training
OT-Prescribed
₹100–600
How It Works
Develops independent finger movement — the absolute prerequisite for any dynamic grasp pattern. Fingers that can only move as a unit cannot produce dynamic writing. Finger isolation training teaches the brain to recruit individual digits independently, which is the neurological foundation that makes tripod movement possible.
Activities That Work
- Finger puppets — one puppet per finger, name each
- Piano app or toy keyboard — press one key at a time
- "Itsy Bitsy Spider" with full individual finger isolation
- Draw a face on each fingertip with washable marker (free)
- "Now move just your pointer finger" naming exercises
Cost: ₹100–600

Material 9: Triangular Crayons / Flip Crayons
Tool Modifications
OT-Prescribed
₹200–500
How It Works
Three flat sides create three resting points for three fingers. The brain unconsciously positions one finger per side — producing a tripod grasp without instruction or correction. The geometry of the tool teaches the hand. This is passive, embedded therapeutic design at its most elegant.
Why Geometry Is the Therapist
Unlike round crayons or pencils — which allow any grip pattern — triangular tools make tripod the path of least resistance. The child isn't being corrected; the tool is providing the teaching through shape alone.
- Use for all coloring, drawing, and early writing tasks
- Ideal transition tool before introducing standard pencils
- Works for both left- and right-handed children
Cost: ₹200–500
📞 Need help selecting the right materials for your child's specific grasp challenge? Call 9100 181 181 — FREE | 16+ languages
Every material above has a ₹0 household version. Therapy begins today — with what you already have.
The WHO/UNICEF equity principle: Effective intervention cannot be conditional on purchasing power. Every technique in the Pinnacle system has a zero-cost alternative that delivers the same therapeutic mechanism.
Material | Commercial Version | ₹0 Household Version | Why It Works |
Short implements | Golf pencils / broken crayons | Break any existing crayon to 3 cm. Peel wrapper for better grip feedback | Same size constraint forces same tripod positioning |
Pencil grips | Adaptive grip devices | Wrap rubber band around pencil shaft; roll small piece of foam around shaft | Adds texture and bulk that guides finger placement |
Therapy putty | Color-coded resistance putty | Homemade playdough (flour + salt + water + oil); Blu-Tack/mounting putty | Provides resistance for pinching and strengthening |
Vertical surface | Commercial easel | Tape paper to wall at shoulder height; use window with washable markers | Same wrist-extension mechanics — gravity teaches regardless of surface cost |
Tweezers | Craft tweezers set | Kitchen tongs, ice tongs, chopsticks | Same tripod-analog finger position; feedback from picking up objects is identical |
Clothespins | Spring-loaded clothespins | Standard wooden clothespins; plastic bag clips | Same spring-resistance pinching mechanism |
Palm pom pom | Craft pom poms | Small cotton ball; crumpled tissue paper; small kneaded eraser | Same tucking mechanic for ring/pinky stabilization |
Finger isolation | Finger puppets | Draw face on each fingertip with washable marker; sticker on one finger | Same individual-finger movement and awareness training |
Triangular crayons | Triangular crayons/pencils | Wrap rubber band around regular pencil creating 3 tactile "sides" | Approximates the 3-point grip guidance of true triangular shape |
⚕️When commercial-grade materials are essential (not optional): Children with significant low muscle tone need higher-resistance therapy putty. Children with sensory hypersensitivities may require clinical-grade texture-specific grips. Children with cerebral palsy or neurological conditions should consult OT for specialized adaptive equipment. All other cases: household alternatives are therapeutically equivalent.
WHO Nurturing Care Framework (2018): Context-specific, equity-focused interventions. CCD Package implemented across 54 LMICs demonstrates household-material-based intervention efficacy. References: PMC9978394 | WHO NCF Handbook (2022)

Read this before you begin. Your child's safety is the foundation of every effective session.
🔴 RED — DO NOT PROCEED if:
- Child is currently having a meltdown or in a highly dysregulated state
- Child has open wounds, sores, or skin conditions on hands
- Child shows extreme tactile aversion to the specific material — do not force
- Child has a diagnosed condition where hand resistance exercises are contraindicated
- Child has a medical condition affecting hand/wrist bones or joints
🟡 AMBER — PROCEED WITH MODIFICATION if:
- Child is tired but not dysregulated — shorten to 5 minutes, preferred materials only
- Child has mild tactile sensitivity — introduce materials visually first
- Child shows resistance to specific tools — switch to household alternative
- Small object safety concern: ensure supervision, use larger alternatives for children who mouth objects
🟢 GREEN — PROCEED when:
- Child has eaten within the last hour
- Child has had rest and is not overtired
- Child is calm, alert, and available
- Environment is prepared and materials checked for safety
Material-Specific Safety Notes
1
🔴Choking hazards: Broken crayon pieces, small pom poms, putty — supervise ALL children under age 5 continuously. Use larger sizes for children who mouth objects regardless of age.
2
🔴Putty hygiene: Therapy putty is NOT edible. Wash hands before and after. Store in airtight container. Discard if contaminated.
3
🟡Clothespin pinch risk: Springs can pinch skin. Teach safe handling. Check for broken or sharp springs before use.
4
🟡Vertical surface stability: Ensure easel is stable and cannot tip. Use painter's tape (not permanent tape) on walls.
🔴STOP IMMEDIATELY if: Child cries or shows signs of pain during hand activities · Child's hand changes color (white, blue) during resistive activities · Child develops skin irritation or allergic reaction · Any session results in significant emotional distress for the child

The right environment is half the session. This setup prevents 80% of common session failures.
Follow these four positioning elements before every session. Unstable posture is the #1 hidden cause of poor pencil grasp — fix the seat before fixing the grip.
① Parent Position
Sit beside the child (shoulder-to-shoulder), not across. This allows natural hand modeling and support without confrontation.
② Child Seating
Feet flat on floor, hips at 90°, table at elbow height. This is non-negotiable for effective fine motor work.
③ Materials Tray
Place only 2–3 items for today's session within reach. Too many options cause distraction and reduce therapeutic focus.
④ Vertical Surface
Paper at shoulder height for warm-up. Begin every session vertically — horizontal writing surface comes only after.
⑤ Clear Exit
Ensure the child can see and access the exit. This prevents the trapped/confined feeling that increases resistance.
Remove From Space:
🚫 Screens · 🚫 Unrelated toys · 🚫 Food/snacks (save for prescribed reinforcement) · 🚫 Other children entering
Sensory environment: Natural or warm light preferred. Avoid harsh fluorescent overhead lighting. Quiet or soft instrumental music if beneficial. Room temperature comfortable — cold hands significantly affect fine motor performance.

ACT III: THE EXECUTION
Cards 13–22
Before every session: this 60-second check determines whether today's session will succeed or fail.
Check | 🟢 Green — Go | 🟡 Amber — Modify | 🔴 Red — Postpone |
Fed? | Eaten within last hour | Light snack 2+ hrs ago | Hasn't eaten, actively hungry |
Rested? | Normal sleep, not fatigued | Slightly tired | Overtired, rubbing eyes |
State? | Calm, alert, making eye contact | Mildly dysregulated | Meltdown within last hour |
Pain? | No signs of discomfort | Mild general discomfort | Any hand/wrist pain signals |
Engagement? | Approached space willingly | Needed 1–2 redirects | Strong resistance to entering space |
Illness? | Well | Mild cold, no fever | Fever, active illness |
🟢 GO
4+ green checks: Proceed to full protocol
🟡 MODIFY
2–3 green, 1–2 amber: Shorten to 5–8 minutes, use highest-preference materials only, increase reinforcement density
🔴 POSTPONE
Any red check, or 3+ amber: Alternative calming activity today. Attempt tomorrow. Not a failure — it's clinical judgment.
If postponing today's session: Offer 5 minutes of preferred hand play (playdough, sensory bin, favorite toy) to maintain positive associations with hand activities without demand.
💙"The best session is one that starts right. A 5-minute session on a good day beats a 20-minute forced session on a difficult day every single time." — Pinnacle OT Consortium

Step 1 of 6: The Invitation
Duration: 30–60 seconds
What To Do
Bring the child into the activity through play — not instruction. The goal of Step 1 is to create willingness and curiosity, not to demonstrate the technique. The materials should look interesting before any demand is placed.
Body Language
- Stay at the child's eye level — sit down if needed
- Keep your tone light and genuinely playful
- No correcting, no directing, no "hold it like this" — yet
Exactly What to Say
"Hey, come see what I found."
[Place one material on the table and explore it yourself first]
"Look at this — watch what happens when I..."
[Demonstrate playing with material]
"Want to try?"
[Pause. Wait. Let curiosity win.]
Handling Resistance
✗ Child turns away → Explore it more dramatically for 30 more seconds, then re-offer
✗ Child says "no" → "That's okay. I'll just play with it." Continue exploring without demand for 60 seconds
✗ Child walks away → This is data. Consider postponing or switching to a different material

Step 2 of 6: The Engagement
Duration: 1–3 minutes
The child has accepted the invitation. Now introduce the therapeutic material purposefully while maintaining the play frame. This is when the material starts doing its neurological work — without the child knowing there's "work" happening.
For Broken Crayons
"Let's make something with these tiny crayons. Draw a rainbow — make it as big as the paper!"
For Therapy Putty
"This putty has a rubber duck hiding inside. Find it with your fingers!"
For Clothespins
"How many can you clip on the edge before they all fall? I'll count!"
For Tweezers
"Move all the pom poms from this bowl to that one. Only tweezers — your fingers can't touch!"
For Vertical Surface
"Draw the biggest circle you can on this paper — touch the edges with your chalk!"
What To Watch
- Child's hand position with the material (note without correcting yet)
- Engagement duration before attention shifts — this is today's baseline
- Facial expression: focused engagement vs. tolerance vs. distress
Reinforcement Cue: The moment the child picks up the material and uses it: "Yes! Look at that!" — specific, immediate, genuine praise. Reinforce the engagement, not the perfection.

Step 3 of 6: The Therapeutic Action
Duration: 5–10 minutes — the active ingredient
Strength-Building Materials (Putty + Clothespins)
Guide the child to pinch with thumb opposed to index AND middle finger together — this exact three-finger position mirrors the tripod grasp. 🖐"Put your pinching fingers like this — thumb here, these two fingers here." Target: 15–20 putty repetitions, 20+ clothespin clips per session. Track completion, not perfection.
Tool Modification Materials (Short crayons, Triangular crayons, Grips)
Simply provide the material and let it do the work. Short crayons cannot be fist-gripped. Triangular crayons guide finger placement automatically. Your role: keep the activity going so the correct hand position accumulates repetitions through drawing, coloring, or writing.
Precursor Skill Materials (Tweezers, Finger isolation)
Ensure tripod finger position on tweezers: thumb on one side, index and middle finger together on the other. For finger isolation: have child move only ONE finger at a time. Name it: "Now move just your pointer finger."
Positioning Supports (Vertical surface, Palm pom pom)
Vertical surface: ensure paper is at shoulder height. Do not correct the grasp — the position itself does the therapeutic work. Palm pom pom: place pom pom in palm, ring and pinky close around it, THEN hand the pencil. "Keep the pom pom sleeping in your hand while you draw."
🟢 Ideal
Child uses material correctly for 3+ minutes with engagement
🟡 Acceptable
Child uses material for 1–2 minutes, drifts, re-engages with prompt
🔴 Concerning
Child shows distress, pain, or complete disengagement — move to the Troubleshooting card

Step 4 of 6: Repeat & Vary
Duration: 3–5 minutes
Neural pathway formation requires repetition — but forced repetition destroys motivation. The target is 3 quality engagements within a session. Not 20 mechanical ones.
Material | Target Reps/Session | Satiation Signal |
Therapy putty exercises | 15–20 pinches | Hand shake, child puts putty down |
Clothespins | 20–30 clips | Fingers opening reluctantly |
Tweezers (transfer tasks) | 15–20 transfers | Drops increasing, disengages |
Short crayon coloring | Entire activity (sustained) | Asks to stop or switches hands |
Vertical surface drawing | 5–10 minutes sustained | Child moves away from surface |
Finger isolation games | 3–5 minutes | Stops differentiating fingers |
Variation Options to Maintain Engagement
Putty Variations
Easy: squeeze whole putty in palm · Standard: pinch with tripod fingers, flatten with fingertips · Advanced: hide 5 small objects — find each one using fingertip pinch only
Clothespin Variations
Easy: clip around paper plate edge · Standard: clip onto string held between two points · Advanced: build a "caterpillar" — clip each to the previous one using one hand
Tweezers Variations
Easy: transfer large pom poms between bowls · Standard: sort by color using tweezers · Advanced: timed challenge — how many in 60 seconds?
"3 quality repetitions outperform 10 forced ones every time. When you see the satiation signals — end the exercise naturally, not with correction."
Step 5 of 6: Reinforce & Celebrate
Timing: Within 3 seconds of desired behavior
What to Reinforce — Do NOT Wait for Perfect Grasp
The attempt — picking up the material with any 3-finger position
The persistence — continuing when it was hard
The improvement — 1 second longer than yesterday
The specific action — "I saw your three fingers holding the tweezers — that's exactly it!"
Verbal Praise
"I saw exactly what you did there — three fingers, holding it tight. That's the hand of a writer."
Token / Star Chart
One star per completed activity. Chart visible in workspace. Specific reward at 5 stars defined in advance with the child.
Natural Reinforcer
Complete the activity → 3 minutes of preferred interest. Must be earned AFTER the activity, not during.
Physical Celebration
High five, fist bump, or enthusiastic pat on back — immediate, specific, genuine.
"Celebrate the attempt, not just the success. The brain that tries hard needs more recognition than the brain that finds it easy."

Step 6 of 6: The Cool-Down
Duration: 1–2 minutes
Why the Cool-Down Is Non-Negotiable
Abrupt endings cause post-session dysregulation in many children — particularly those with ASD or sensory sensitivities. The cool-down transitions the nervous system from activated therapeutic engagement back to baseline. Sessions that end poorly are remembered as unpleasant — and avoided next time.
Transition Warning Script
"Two more [clips / pinches / transfers] — then we're all done for today."
(30 seconds later)
"One more — make it a good one."
(After final rep)
"Done! You finished the whole thing."
Cool-Down Activity (choose one)
🤲Hand massage: Gently press palms together and rub in circles. Calms the proprioceptive system.
🌬Hand shaking: "Shake out the tired fingers" — hands loose, shake gently. Releases tension from resistive work.
🎵Finger song: One familiar finger rhyme (Itsy Bitsy Spider, Where is Thumbkin) — light, familiar, positive ending.
Material Put-Away Ritual
Have the child help put materials away. This signals a clear "end," builds responsibility, and provides additional incidental fine motor practice. Then: "Great job today. Now you can [preferred next activity]."

You have 60 seconds after session ends before the details blur. Record these 3 things now.
1
Material Used Today
Broken crayons · Putty · Clothespins · Tweezers · Vertical surface · Pom pom palm · Triangular crayons · Grip · Finger isolation
2
Engagement Rating (1–5)
1 = refused · 3 = tolerated · 5 = requested more
Record today's rating honestly — patterns only emerge from consistent data.
Record today's rating honestly — patterns only emerge from consistent data.
3
Grasp Observation
Fist grip throughout · Mixed, some tripod attempts · Tripod most of the time · Consistent tripod, minimal prompting
📥 Download Tracking Sheet
Weekly paper tracker for families without smartphone access.
📱 GPT-OS® Integration
Already using GPT-OS®? Log this session in the Fine Motor → Pencil Grasp tracker. Your data shapes your child's personalized progression recommendations.
"60 seconds of data now saves hours of guessing later. Patterns only appear when data is captured."
Most sessions don't go perfectly. Here are the 7 most common challenges — and the immediate fix for each.
Problem 1: Child refuses to touch the material
Why: Tactile sensitivity, material unfamiliarity, bad timing
Fix: Don't introduce material to hands first. Place it on the table, explore it yourself for 2 minutes. Try a different material with lower tactile demand.
Fix: Don't introduce material to hands first. Place it on the table, explore it yourself for 2 minutes. Try a different material with lower tactile demand.
Problem 2: Child grips correctly for 5 seconds then reverts
Why: The new grasp requires active attention — not yet automatic. This is neurologically expected and normal.
Fix: This is progress, not failure. 5 seconds is the starting point. Celebrate it. Track it. Watch it extend.
Fix: This is progress, not failure. 5 seconds is the starting point. Celebrate it. Track it. Watch it extend.
Problem 3: Child refuses to use the pencil grip
Why: Grips feel different — different proprioceptive input. Resistance is sensory, not behavioral.
Fix: Switch to triangular crayons. Or try 3–4 different grip styles over consecutive days and let the child choose.
Fix: Switch to triangular crayons. Or try 3–4 different grip styles over consecutive days and let the child choose.
Problem 4: Hand fatigue within 2 minutes
Why: Intrinsic hand muscles are genuinely weak — this is data, not weakness of will.
Fix: Reduce resistance (softer putty, lighter clothespin spring), shorter duration, more frequent breaks. Report to OT — this is a strength issue requiring specific targeting.
Fix: Reduce resistance (softer putty, lighter clothespin spring), shorter duration, more frequent breaks. Report to OT — this is a strength issue requiring specific targeting.
Problem 5: Correct activity but no transfer to pencil
Why: Motor generalization from tweezers to pencil takes weeks — this is normal.
Fix: Bridge sessions: tweezers → immediately pick up pencil → draw 3 lines → back to tweezers. Keep the tripod muscle pattern warm.
Fix: Bridge sessions: tweezers → immediately pick up pencil → draw 3 lines → back to tweezers. Keep the tripod muscle pattern warm.
Problem 6: Session ended in meltdown
Why: Session too long, too demanding, too many corrections, or child wasn't truly ready.
Fix: Shorten tomorrow's session by 50%. Remove all correction language. Focus purely on positive engagement.
Fix: Shorten tomorrow's session by 50%. Remove all correction language. Focus purely on positive engagement.
Problem 7: Child gets bored within 1 minute
Why: Activity is below or above the "just-right challenge" zone, or reinforcement isn't motivating enough.
Fix: Increase challenge (harder variation) or increase reinforcement density. Consider whether this material matches this child's interests.
Fix: Increase challenge (harder variation) or increase reinforcement density. Consider whether this material matches this child's interests.
🔴Emergency Clause: If child became severely distressed, self-harmed, or showed acute distress — stop the session. Do not attempt the same material again this week. Contact your OT or call 9100 181 181 to review the protocol with a clinical team member.

No two children are the same. This is how you tune these 9 materials to your specific child.
1
EASIER — Difficult days, new starts, sensory-sensitive children
Use 1 material only (highest preference). Session: 5 minutes maximum. Broken crayons on vertical wall surface — lowest demand, highest natural positioning benefit. Putty in palm, just squeeze.
2
STANDARD — Typical session (3–4 times per week)
2–3 materials per session, 10–15 minutes total. Standard repetitions as prescribed. Introduce one variation per session.
3
ADVANCED — Progress plateau, or strong baseline
Increase putty resistance one level. Mini clothespins (smaller = harder). Fine-point tweezers with very small objects. Write letters with modified tools. Timed challenges for speed and accuracy.
By Child Profile
🔊 Sensory Seeker
Lead with therapy putty (high resistance), weighted pencil, clothespins × 30. More proprioceptive input = better. Vertical surface with full-body lean.
🛡 Sensory Avoider
Begin with visual exploration before hand contact. Start with smoothest materials (pom pom in palm, triangular crayons). Gradually introduce putty over multiple sessions.
💨 ADHD Profile
Short bursts: 2 minutes on, 1 minute break, 2 minutes on. Maximum novelty — rotate through 3 materials. Gamify: beat your own record.
⚡ Hypotonia Profile
Prioritize putty and clothespins (strength first). Vertical surface is essential. Accept slower progression — the foundation takes longer to build but is equally achievable.
ACT IV: THE PROGRESS ARC
Cards 23–30
Week 1–2 is about tolerance and first contact. Not mastery. Not habit. Contact.
15%
Early Tolerance Phase
Where you are in the progress arc during weeks 1–2
8–12 wks
Full Program Timeline
Evidence-based timeline for measurable fine motor and grasp outcomes
✅ You May See in Weeks 1–2
- Child tolerates the material for slightly longer each session
- Reduced initial resistance to starting the activity
- Some spontaneous tripod position with modified tools (broken crayons, triangular crayons)
- Emerging curiosity — asking to do "the putty game" again
⚠ You Will NOT Yet See
- Consistent tripod grasp with a regular pencil
- Transfer of grasp to homework or school writing
- Significant hand strength improvement (takes 3–4 weeks)
- Spontaneous correct grasp without materials
💙 The first two weeks are the hardest. Your child is building something that has never existed before in their nervous system. Progress is happening at the cellular level before it appears at the behavioral level. Your consistency in weeks 1–2 is the investment that weeks 3–8 will pay back.
Something is shifting. Week 3–4 is when the neural pathways begin to consolidate — and when most parents first see the moment of spontaneous change.
40%
Consolidation Phase
Progress arc position at weeks 3–4
Consolidation Indicators — Specific Behaviors to Watch For
✅ Child anticipates the activity — may ask for it, or find materials independently
✅ Grasp with modified tools is now consistent — less correction needed
✅ Some unprompted tripod grasp attempts with regular pencil (brief, inconsistent — this is right on schedule)
✅ Writing sessions with modified tools are now noticeably less effortful for the child
✅ Child talks about the materials positively or shows them to family members
Generalization Seeds: You may notice the child picks up a fork or spoon differently · Holds other small objects with fingers more than fist · General fine motor confidence increases (opening packages, using scissors more easily). These are early signs that the neural pathway is generalizing beyond the specific activity.
💙"By Week 3–4, you may notice you feel more confident too. The routine is established. The battles are reducing. You are becoming a skilled home therapist — not by training, but by consistent, loving practice."

The grasp is beginning to live in the body, not just the activity. This is mastery approaching.
75%
Mastery Phase
Progress arc position at weeks 5–8
🏆 Mastery Criteria — Observable, Specific, Measurable
Criterion 1
Child holds regular pencil with functional tripod or adapted tripod in 3 out of 4 writing/drawing tasks without physical prompt
Criterion 2
Child can write 3–5 sentences or draw for 5+ minutes without reporting hand pain or fatigue
Criterion 3
Grasp pattern maintained across at least 2 different settings (home + school, or home + grandparent's house)
Criterion 4
Child no longer needs modified tools as a prerequisite — uses them as preference, not necessity
🏆Mastery Unlocked: When Criteria 1–3 are met consistently for 1 week = mastery milestone. Proceed to F-594 (Scissor Skills) or reinforce with Handwriting Legibility techniques. If Criteria 1–2 are met but not 3–4: maintain current protocol for 2 more weeks to deepen automaticity.

You did this. Your child grew because you showed up — every day, when it was hard, when it wasn't working, and when it finally did.
In 5–8 weeks of consistent use of these 9 materials, your family has:
Built Strength
Intrinsic hand muscle strength that wasn't there before
Wired a Pathway
A neural pathway from finger movement to pencil control that will last a lifetime
Transformed Homework
Turned an exhausting writing battle into a structured, manageable activity
Built a Foundation
Created the foundation for every piece of written work your child will produce for the rest of their academic life
🎉"Take a photo today of your child writing their name with a normal pencil — without a prompt from you. Print it. Put it somewhere visible. This is the evidence of eight weeks of your love, translated into their capability."
"You are not a trained occupational therapist. You are something more powerful — you are the person this child trusts completely, showing up every day with a broken crayon and a pom pom and a fierce, consistent belief that their hand could learn. It did."
Even after progress, these specific signs mean: pause and seek professional input. Trust your instincts.
🔴 1. Persistent pain during writing tasks after 6–8 weeks
Possible underlying joint hypermobility, structural issue, or hypotonia that needs medical evaluation. Not safe to continue high-resistance activities without clearance.
🔴 2. No improvement despite consistent 6–8 week protocol
Underlying deficit may be more significant than materials alone can address. Formal OT evaluation for specific component skill assessment is indicated.
🔴 3. Child avoids ALL fine motor activities — not just writing
Possible broader sensory processing disorder, DCD, or motor learning difficulty requiring specialist assessment.
🔴 4. Grasp improvement in sessions but zero transfer to real writing
Generalization deficit — possibly ASD-related or DCD-related. Specialist-guided generalization protocol required.
🔴 5. New hand symptoms: color changes, numbness, swelling
Medical evaluation immediately. Stop all hand resistance activities. Contact pediatrician.
🔴 6. Significant emotional distress now associated with all hand activities
The protocol has created avoidance conditioning. Requires clinical reset — contact OT or Pinnacle helpline before continuing.

These techniques all live in the Fine Motor Development domain. You may already own the materials for some of them.

F-591 · Object Grasping
Level: Intro · Materials: Putty, varied objects · If you have therapy putty from F-593, you're already equipped for this technique.
F-592 · Pincer Grasp
Level: Intro-Core · Materials: Tweezers, small objects · The tweezers from F-593 are your primary tool here too.

F-594 · Scissor Skills
Level: Core · Materials: Age-appropriate scissors · The hand strength built in F-593 directly powers scissor control.

F-595 · Handwriting Legibility
Level: Core · Materials: Modified writing tools, pencil grips · All tools from F-593 carry forward into this domain.

F-596 · Letter Formation
Level: Core-Advanced · Materials: Lined paper, pencil grips · Builds on the stable grasp established in F-593.

F-597 · Writing Speed & Endurance
Level: Advanced · Materials: Timer tools · The endurance built by clothespins and putty in F-593 feeds directly into this outcome.
✅You have therapy putty and clothespins from F-593? You're already equipped for F-591 (Object Grasping) and F-592 (Pincer Grasp).

ACT V: THE COMMUNITY & ECOSYSTEM
Cards 31–37
Three families. Three different challenges. Three paths through these 9 materials.
Family 1 — The Fist Grip
Before: 6-year-old boy, Class 1, fist-gripping every pencil. Writing homework requiring 45 minutes for one page, daily tears, teacher note: "Unable to keep up with class copying tasks."
Materials Used: Broken crayons daily, therapy putty before school, vertical surface drawing evenings.
Week 4:"He picked up a regular pencil and I heard him say 'I'm holding it right' — he knew. He knew before I said anything."
Week 8: Static tripod grasp consistent, homework time reduced to 20 minutes, teacher removed pencil grip accommodation.
Materials Used: Broken crayons daily, therapy putty before school, vertical surface drawing evenings.
Week 4:"He picked up a regular pencil and I heard him say 'I'm holding it right' — he knew. He knew before I said anything."
Week 8: Static tripod grasp consistent, homework time reduced to 20 minutes, teacher removed pencil grip accommodation.
Family 2 — The Sensory Avoider
Before: 5-year-old girl, ASD diagnosis, refused to hold any writing implement, extreme distress at pencil contact, school refusing to write.
Materials Used: Triangular crayons (week 2), pom pom in palm, finger isolation games before any writing task.
Week 3:"She held the triangular crayon herself for the first time. Not because we asked — because she picked it up. That was the whole week right there."
Week 7: Functional adapted grasp established, writing accepted in structured OT sessions, transitioning to classroom.
Materials Used: Triangular crayons (week 2), pom pom in palm, finger isolation games before any writing task.
Week 3:"She held the triangular crayon herself for the first time. Not because we asked — because she picked it up. That was the whole week right there."
Week 7: Functional adapted grasp established, writing accepted in structured OT sessions, transitioning to classroom.
Family 3 — The Tired Hand
Before: 8-year-old boy, no diagnosis, but hand cramping after 5 minutes of writing, illegible second half of every written task, avoiding all written work.
Materials Used: Clothespins (20 daily), therapy putty (medium resistance), pencil grip for pressure reduction.
Week 5:"His teacher texted me. She said his last two pages of a writing assessment were as legible as his first page. She'd never seen that before."
Materials Used: Clothespins (20 daily), therapy putty (medium resistance), pencil grip for pressure reduction.
Week 5:"His teacher texted me. She said his last two pages of a writing assessment were as legible as his first page. She'd never seen that before."
Illustrative cases representing outcome patterns across Pinnacle Network families. Individual outcomes vary based on child profile, underlying condition, and intervention consistency.
You are not doing this alone. There are thousands of families doing this exact protocol tonight.
Pinnacle Fine Motor Parent WhatsApp Group
Join 2,000+ parents navigating fine motor and handwriting challenges. Share session wins, ask questions, and get peer support from families who've been exactly where you are.
Join WhatsApp Group →
Join WhatsApp Group →
Pinnacle Parent Online Community
Forum organized by technique, challenge type, and age group. Search "F-593 Pencil Grasp" to see all discussions about this specific technique.
Join Online Community →
Join Online Community →
Local Parent Meetups
Pinnacle centers organize monthly parent skill-share sessions — see how other families implement home protocols and ask your questions in person.
Find Nearest Center Meetup →
Find Nearest Center Meetup →
Peer Mentoring
Connect with an experienced parent who has already completed this protocol and can guide you through the first four weeks.
Request a Peer Mentor →
Request a Peer Mentor →
"Your experience helps others. The parent behind you is exactly where you were eight weeks ago. When you're ready — share your journey."
Home practice is powerful. Professional guidance makes it precise. Both together produce extraordinary outcomes.
Services at Your Nearest Center
🖐Occupational Therapy: Pencil grasp evaluation, AbilityScore® fine motor assessment, individualized material prescription
📊ABA Therapy: Behavioral reinforcement programming for writing avoidance and task approach behavior
🎓Special Education: School liaison, classroom accommodation planning, teacher training on modified tools
🧠NeuroDev Pediatrics: Ruling out underlying medical conditions; coordination with OT protocol
Can't Get to a Center?
Get specialist consultation from home via teleconsultation. Our OT team can review your child's current grasp, recommend the exact material combination for their profile, and guide your home sessions — all without leaving your house.
📞9100 181 181 — FREE National Autism & Child Development Helpline
16+ languages | 24×7 | No appointment needed | Call right now
16+ languages | 24×7 | No appointment needed | Call right now
Research consistently shows that home-based intervention + clinical guidance produces 2–3× better outcomes than either alone.

Consistency across all caregivers multiplies impact. This page is for everyone who works with your child.
Share This Page
📱 WhatsApp
Pre-formatted: "This page helped us with [child's name]'s pencil grip. 9 materials, simple steps. techniques.pinnacleblooms.org/fine-motor/pencil-grasp-materials-F-593"
📧 Email
Subject: "Pencil Grasp Materials That Are Working For Us"
📥 Download
Pencil Grasp Home Guide — One Page PDF. Includes all 9 materials, daily session structure, what to watch for, helpline number.
💙 Explain to Grandparents — Simplified Version
"Your grandchild holds the pencil in a tight fist because the small muscles in their hand are still developing. These activities help those muscles grow:
1. Use broken crayons — short ones make them hold it with three fingers naturally.
2. Squeeze playdough or putty for 5 minutes every day.
3. Draw on the wall with paper taped up — wrist goes straight, which is better for the hand.
You don't need to correct their grip. Just do these activities. The grip changes by itself."
📝 Teacher Communication Template
Dear [Teacher name], [Child name] is currently working on pencil grasp development with our OT team. We are using a home protocol (F-593). At school, would it be possible to provide: (1) triangular crayons or pencils for written work, (2) a pencil grip on [child's] writing implement, (3) brief breaks during extended writing tasks? We are happy to share our OT's protocol summary. Thank you.
Preview of 9 materials that help with pencil grasp Therapy Material
Below is a visual preview of 9 materials that help with pencil grasp therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

🌸 The Pinnacle Promise
Our Mission
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® exists to transform every home into a 24×7, personalized, multi-disciplinary, evidence-based therapeutic environment — so that no child waits for a clinic appointment to receive what their brain needs today.
GPT-OS® · AbilityScore® · TherapeuticAI® · EverydayTherapyProgramme™ · FusionModule™
Patents Filed in 160+ Countries
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
OT · SLP · ABA · SpEd · NeuroDev · CRO
WHO/UNICEF Aligned
OT · SLP · ABA · SpEd · NeuroDev · CRO
WHO/UNICEF Aligned
Medical Disclaimer
This content is educational and informational. It does not replace individualized assessment and intervention from licensed occupational therapists or other qualified healthcare professionals. Pencil grasp development varies by child — not all children will develop a traditional tripod grasp, and functional alternatives exist. Persistent grasp difficulties may indicate underlying conditions requiring professional evaluation. Always consult your child's therapy team before implementing interventions. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network® | Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2