It's 7 AM. Breakfast is already on his shirt. The straw lies untouched.
His words blur together. And the paediatrician said: "He'll grow out of it."
You are not failing. Your child's oral muscles are speaking — and they need specific support, not time.
ORAL MOTOR DEVELOPMENT
L-983 | Domain L: Feeding & Oral Motor
Ages 0–8 Years
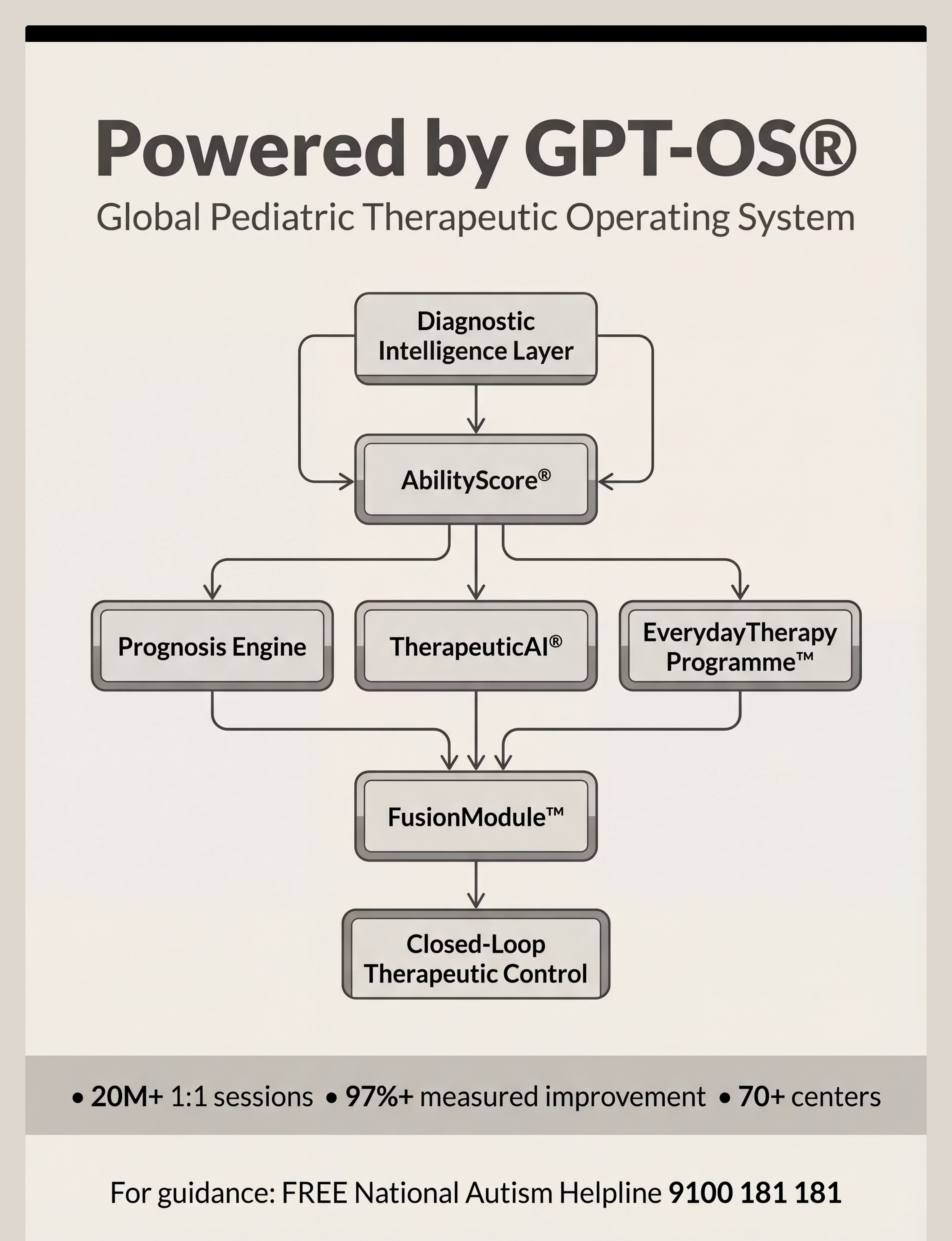
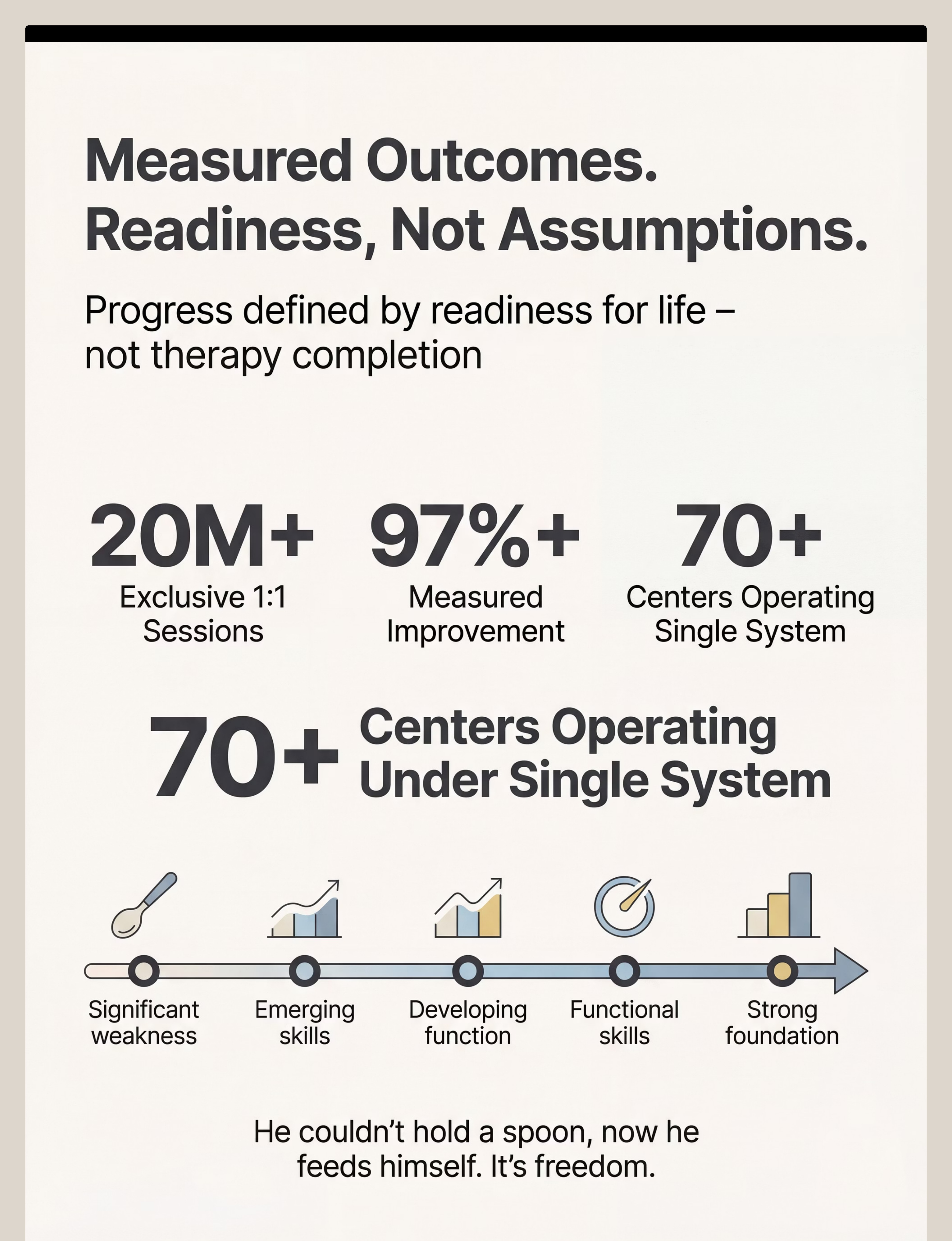
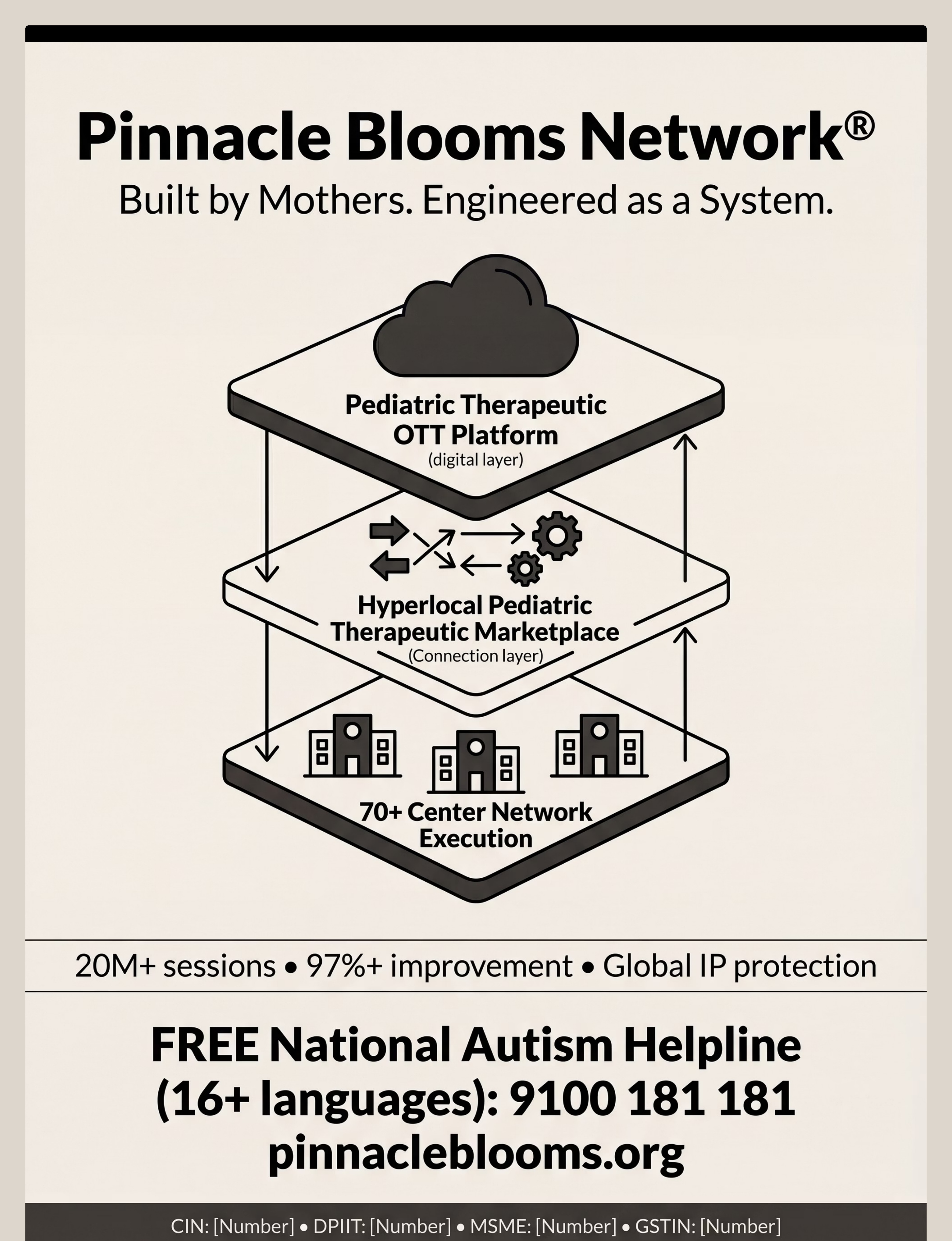
Validated by Pinnacle Blooms Network® — India's largest multi-disciplinary pediatric therapy consortium. 70+ centers. 20M+ sessions. 97%+ improvement.
ACT I — THE STORY
You Are Among Millions of Families Navigating This Exact Challenge
Oral motor weakness is not rare. It is not a parenting failure. It is a measurable, treatable neuromotor difference that responds to structured, consistent intervention. The jaw, lips, tongue, and cheeks are muscles — and muscles can be trained.
1
ASD & Oral Motor
Children with ASD experience significant oral motor difficulties affecting feeding and/or speech
2
Feeding + Speech Link
Children with feeding difficulties in early childhood also show speech intelligibility concerns
3
Pinnacle Sessions
Therapy sessions delivered where oral motor challenges were a primary or secondary target
India-specific data: Padmanabha et al. (Indian J Pediatr, 2019) documented significant oral motor skill deficits in Indian children referred for speech delay — confirming this is not a Western-centric phenomenon. DOI: 10.1007/s12098-018-2747-4
What's Happening in Your Child's Brain & Body
The Oral Motor Hierarchy
Your child's oral structures — jaw, lips, tongue, and cheeks — form a coordinated system that must work together for eating, drinking, and speaking. When any component is weak, uncoordinated, or under-regulated for sensory input, the whole system is affected.
The jaw is the foundation. If the jaw is unstable (wobbling instead of holding steady), the tongue and lips cannot do their fine motor work. A weak jaw forces compensation — the tongue and whole head move instead of precise muscle groups.
This is a wiring AND a strength issue. Some children have low muscle tone (hypotonia). Others have motor planning difficulties (oral dyspraxia). Others have sensory processing differences. The approach differs for each.
The Hierarchy
01
JAW
Stability base — the foundation
02
LIPS
Closure & suction
03
TONGUE
Lateralization & placement
04
CHEEKS
Tension & suction
05
SOFT PALATE
Breath & swallow
"This is a wiring difference, not a behavior choice."

Clinically Validated. Home-Applicable. Parent-Proven.
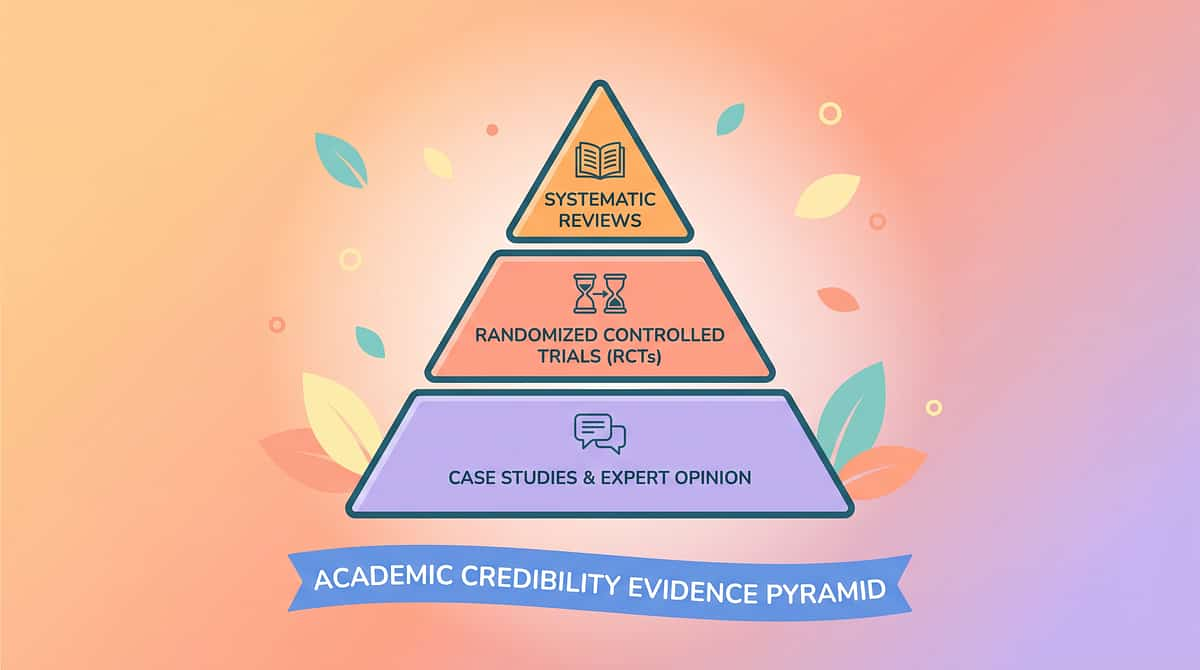
The evidence behind oral motor intervention is robust — built from multiple randomized controlled trials, systematic reviews, and an Indian RCT demonstrating real-world outcomes for Indian pediatric populations. This is not guesswork. This is science you can act on at home.
1
Level I — Systematic Review
PRISMA Review (2024)
16 studies (2013–2023) confirm oral motor and sensory integration intervention meets evidence-based practice criteria for children with ASD.
→ PMC11506176
2
Level I — Meta-Analysis
World J Clin Cases (2024)
24 studies confirm therapy effectively promotes adaptive behavior, motor skills, and sensory processing.
→ PMC10955541
3
Level II — Indian RCT
Padmanabha et al. (2019)
Home-based oral motor and sensory interventions demonstrated significant, measurable outcomes in Indian pediatric populations.
→ Indian J Pediatr, DOI: 10.1007/s12098-018-2747-4
4
Level III — NCAEP 2020
Evidence-Based Practice
Video modeling of oral motor techniques classified as EBP. Multi-modal delivery (video + hands-on) improves parent skill acquisition.
→ NCAEP EBP Report, 2020
82%
Evidence Strength
Strong — Multiple disciplines corroborate across RCTs, systematic reviews, and clinical guidelines

ACT II — WHAT YOU NEED
9 Materials That Help With Oral Motor Development
Parent-Friendly Alias: "The Mouth Training Toolkit"
Oral motor development refers to the progressive strengthening, coordination, and sensory integration of the jaw, lips, tongue, cheeks, and soft palate — the structures used for both feeding and speech. This technique introduces 9 clinically validated materials that target specific components of oral motor function — usable at home, during mealtimes, and during play.
📂 Domain
Feeding & Oral Motor (Domain L)
👦 Age Range
0–8 Years
⏱ Session Duration
10–20 minutes
📅 Frequency
Daily — integrated into meals & play
🔢 Episode
L-983 of 999

Who Uses This Technique: 5 Disciplines, One Goal
This technique lives at the intersection of 5 disciplines. Your child's team already uses it — now you can too. The brain doesn't organize itself by therapy type. Neither should your child's intervention.
Speech-Language Pathologist
PRIMARY LEAD. Assesses oral motor function, identifies the specific weakness profile (jaw vs. lip vs. tongue vs. sensory), designs the hierarchy of materials, and monitors speech intelligibility outcomes.
Occupational Therapist
CO-LEAD: Sensory + Feeding. Addresses oral defensiveness, texture aversion, hypo/hypersensitivity, and supports feeding skill development within sensory integration theory.
ABA / BCBA Therapist
Reinforcement + Data. Designs the reinforcement schedule, implements data collection, and integrates the protocol with the child's behavioral goals. Token economies make oral motor exercises rewarding.
Special Educator
Generalization. Extends oral motor practice into school settings — mealtimes, recess, structured activities — ensuring skills generalize beyond the home and therapy clinic.
NeuroDevelopmental Paediatrician
Medical Oversight. Rules out structural causes (tongue tie, palate issues, neurological conditions), coordinates with ENT/orthodontics, and monitors developmental trajectory.

Material 1 of 9
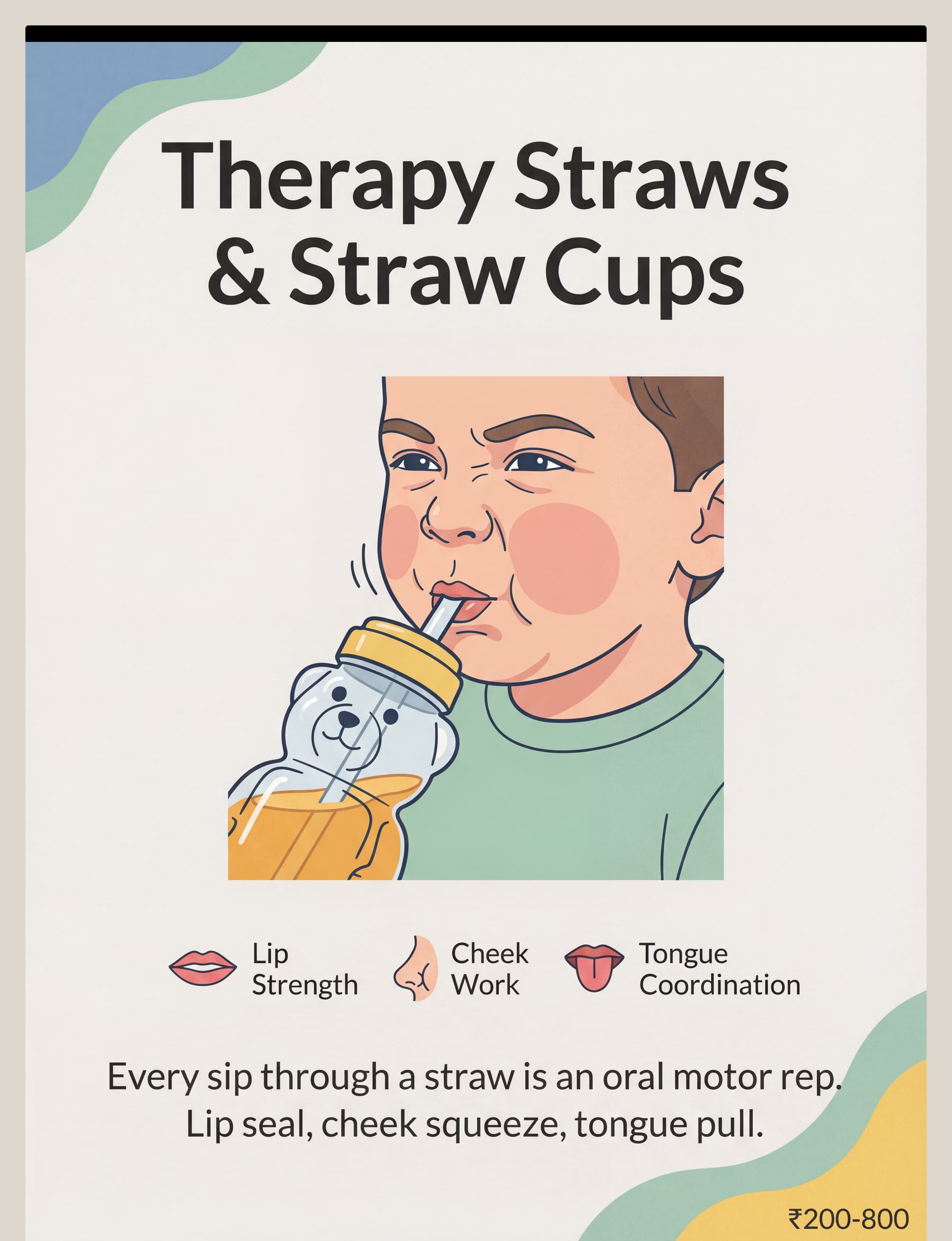
Material 1: Therapy Straws & Straw Cups
What It Targets
Lip strength, cheek tension, and tongue retraction. Every successful sip is a complete oral motor repetition: lip seal → cheek squeeze → tongue retraction → swallow sequence. Target 10–20 successful sips per session.
How to Use It
Position the straw at midline — not the corner of the mouth. Start with thicker liquids (smoothie, yogurt drink) for more resistance, then progress to thinner liquids as strength builds. Short straw → longer straw → thinner straw as skill increases.
Pinnacle Recommends: Honey bear straw bottle or recessed-lid straw cup without a valve — the valve allows gravity flow and removes the therapeutic demand.
At a Glance
💰Price Range: ₹200–800
🔗 Search Amazon.in → "Therapy Straw Cup Honey Bear"
🏠DIY Alternative: Regular straw cut to 10 cm. Use with a thick smoothie for resistance. Free from your kitchen.
⏱Session Target: 10–20 sips, cheeks visibly working (not gravity flow)
📈Progress: Thick liquid → thin liquid → shorter straw → longer straw

Material 2 of 9
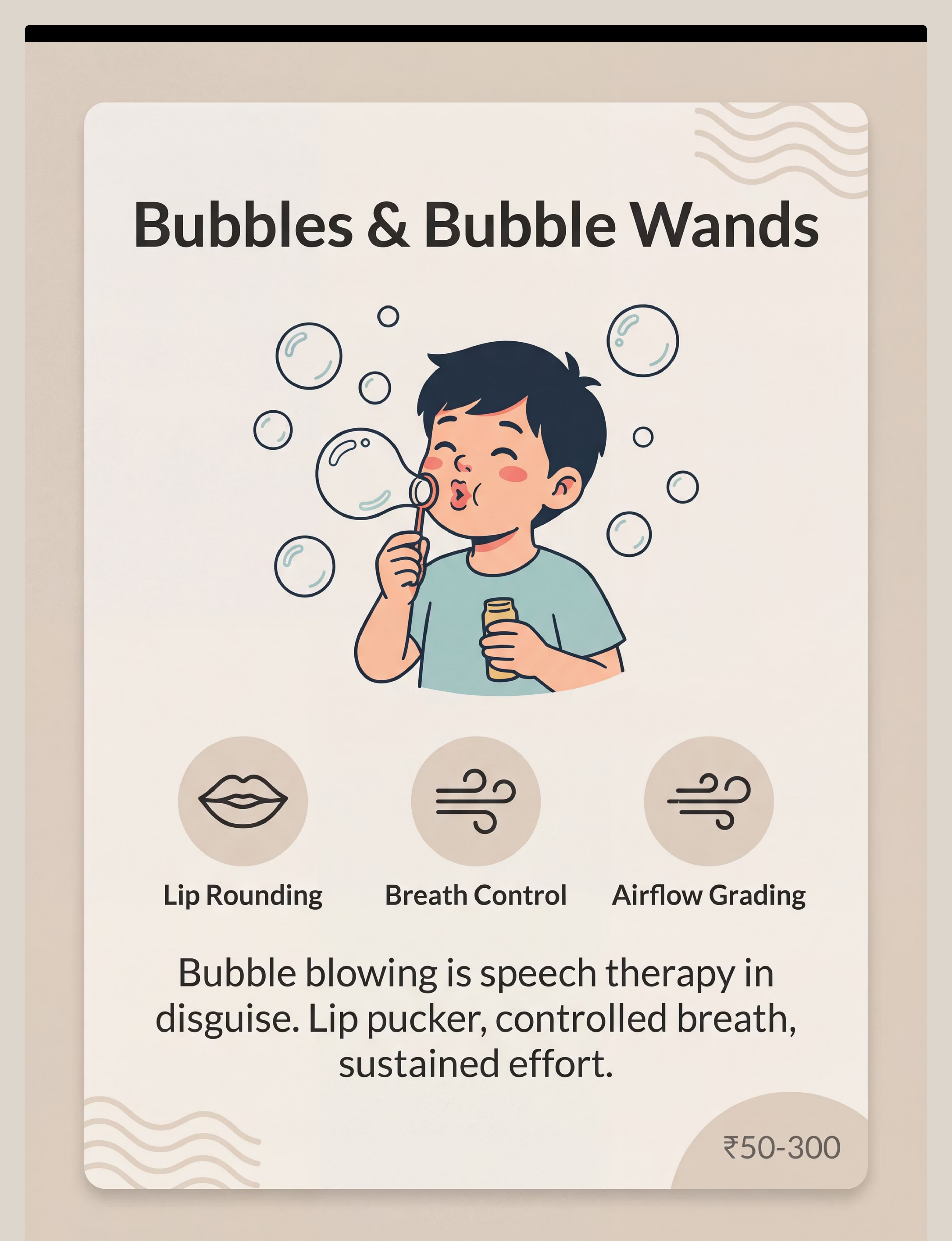
Material 2: Bubbles & Bubble Wands
What It Targets
Lip rounding, breath control, and airflow grading. Each bubble attempt is an oral motor rep: the child must sustain a lip pucker, control their breath speed, and grade the airflow. Bubbles are the easiest, most motivating starting point for most children.
How to Use It
Start with a small wand close to the child (model blowing yourself first). Gradually move to larger wands and farther distances. Progress: blow bubbles → blow bubbles in water through straw → blow cotton ball across table. Target 5–10 genuine bubble attempts per session.
This is the safest starting point. If your child does nothing else today, do bubbles. Near-zero cost, immediately motivating, and genuinely therapeutic.
At a Glance
💰Price Range: ₹50–300
🔗 Search Amazon.in → "Bubble Wands Therapy"
🏠DIY Alternative: 1 tsp dish soap + 1 cup water. Wand = pipe cleaner bent into a loop. Or blow through a straw into a cup of water.
⏱Session Target: 5–10 attempts; lip pucker visible before each blow
📈Progress: Small wand → large wand → water blowing → cotton ball blowing
Material 3 of 9
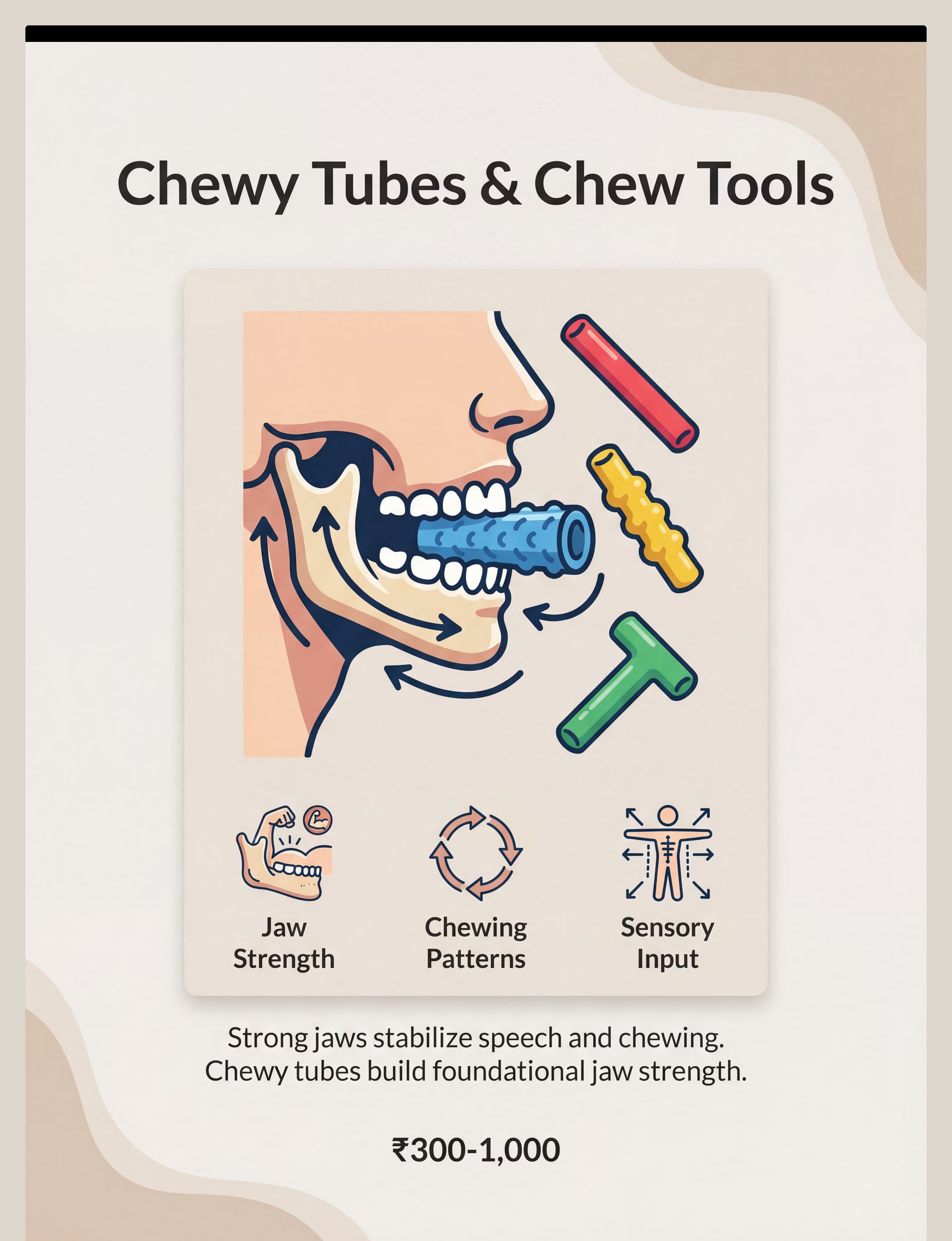
Material 3: Chewy Tubes & Chew Tools
What It Targets
Jaw strength, organized chewing patterns, and proprioceptive input to the jaw. Bilateral biting (alternating sides) builds the jaw stability that underlies all other oral motor work. The jaw is the foundation — chewy tools build it.
How to Use It
Child bites down on tube with molars, holds pressure, then bites on the opposite side. Target 10 bilateral reps (5 each side) per session. Start with soft resistance and upgrade only when the child demonstrates consistent, even pressure on both sides. Progress to a rotary chewing motion as jaw strength develops.
Start with SOFT resistance. Upgrade resistance only as jaw strength builds. Never use hard resistance before the child is ready — poor-quality reps reinforce compensatory patterns.
At a Glance
💰Price Range: ₹300–1,000
🔗 Search Amazon.in → "Chewy Tubes Oral Motor Autism"
🏠DIY Alternative: Firm silicone teether (already at home). Crunchy carrot sticks. Firm bread crust — all provide jaw proprioceptive input.
⏱Session Target: 10 bilateral bites (5 each side); even pressure both sides
📈Progress: Soft → medium → firm resistance; center → left molar → right molar

Material 4 of 9
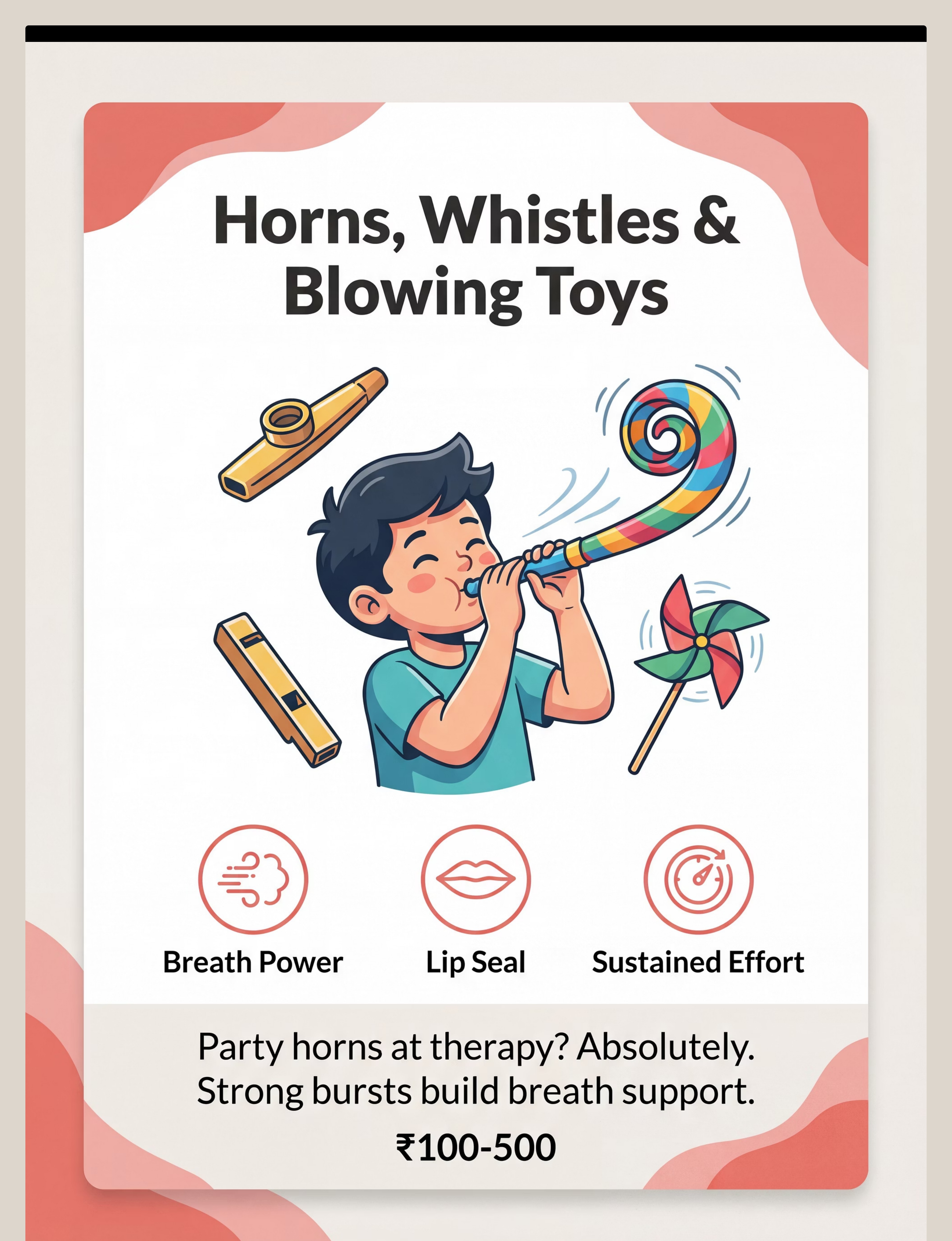
Material 4: Horns, Whistles & Blowing Toys
What It Targets
Breath power, sustained lip seal, and respiratory effort. To produce sound from a horn or whistle, the child must maintain complete lip contact around the instrument and sustain diaphragmatic breath support — both critical oral motor skills. The goal is not volume; it is duration and consistency of airflow.
How to Use It
Start with the easiest instrument (kazoo, party horn). Have the child attempt 3–5 sustained blowing efforts of 2–3 seconds each per session. Rotate instruments for variety and to maintain engagement. Celebrate the sound — the child immediately hears and feels success.
Best value: Kazoo + party horns (₹20–50). Rotate for variety. Each new instrument slightly changes the lip and breath demand, providing progressive challenge automatically.
At a Glance
💰Price Range: ₹100–500
🔗 Search Amazon.in → "Blowing Toys Horns Whistles Speech Therapy Kids"
🏠DIY Alternative: Paper towel roll + humming = DIY kazoo. Cotton balls blown across a table. Pinwheel from kitchen foil.
⏱Session Target: 3–5 sustained blows lasting 2–3 seconds each
📈Progress: Easy kazoo → party horn → recorder → sustained blowing games

Material 5 of 9
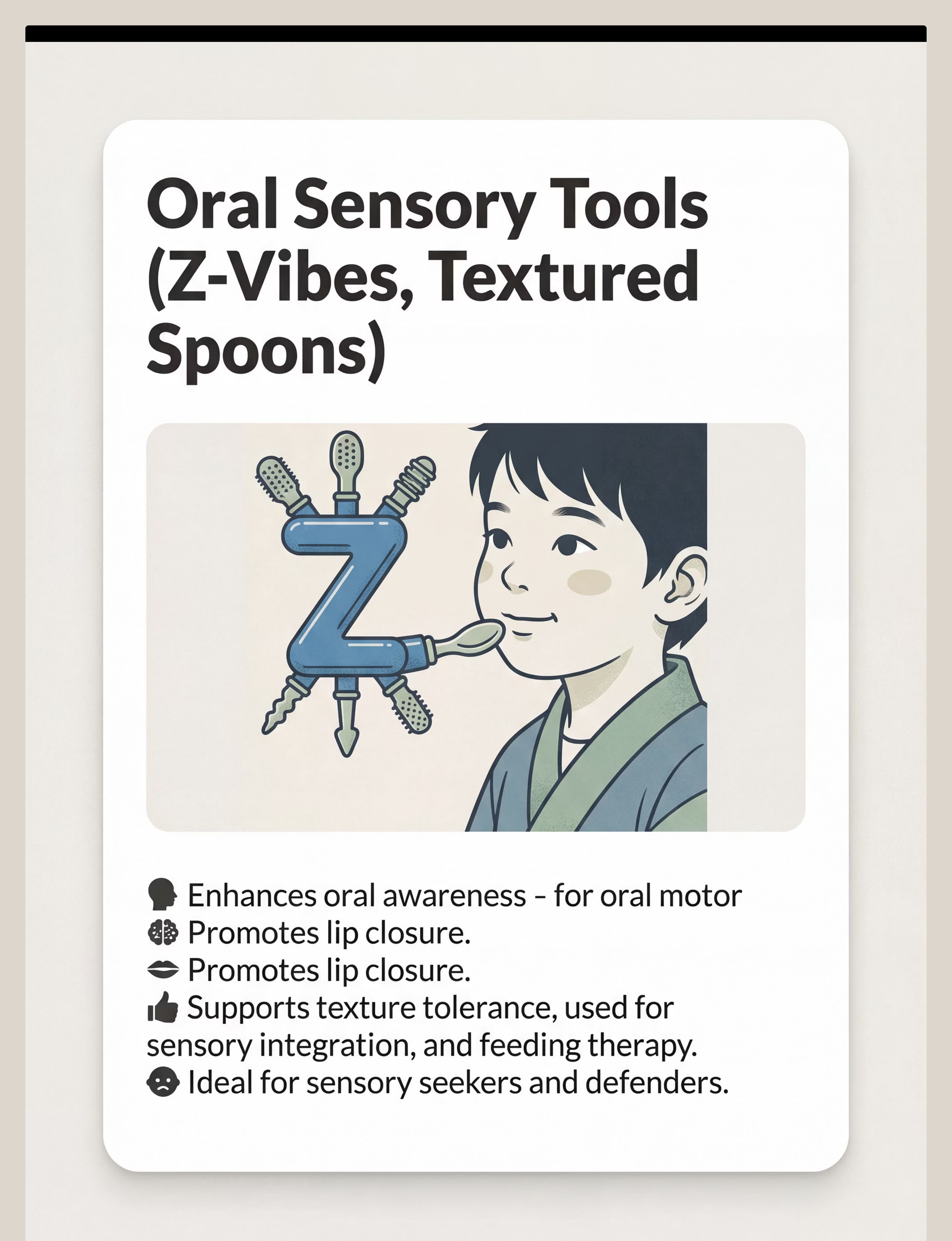
Material 5: Oral Sensory Tools (Z-Vibes, Textured Spoons)
What It Targets
Oral awareness, sensory normalization, and lip/tongue sensory feedback. Many children with oral motor difficulties have reduced awareness of where their tongue and lips are — they can't feel the oral posture that is expected of them. Vibration and texture provide powerful sensory alerting input that wakes up oral awareness.
How to Use It
Apply the vibrating tip to outer gums, cheeks, and tongue following your SLP's prescribed protocol. Duration: 2–3 minutes of targeted oral input per session. Introduce gradually — start with brief, peripheral exposure (outer cheeks) before moving to intraoral use. Always follow therapist guidance on placement sequence.
Introduce GRADUALLY. Vibration is powerful sensory input — for a hypersensitive child, too much too fast causes avoidance. Start at the periphery (outer cheeks) and work inward over days or weeks.
At a Glance
💰Price Range: ₹800–2,500
🔗 Search Amazon.in → "Z-Vibe Oral Motor Vibrating Speech Tool"
🏠DIY Alternative: Electric toothbrush (supervised). Damp textured washcloth for oral massage. Temperature variation — cold vs. room-temperature spoon provides sensory contrast.
⏱Session Target: 2–3 minutes of targeted sensory input per session
📈Progress: Outer cheeks → outer gums → tongue tip → full intraoral protocol

Material 6 of 9
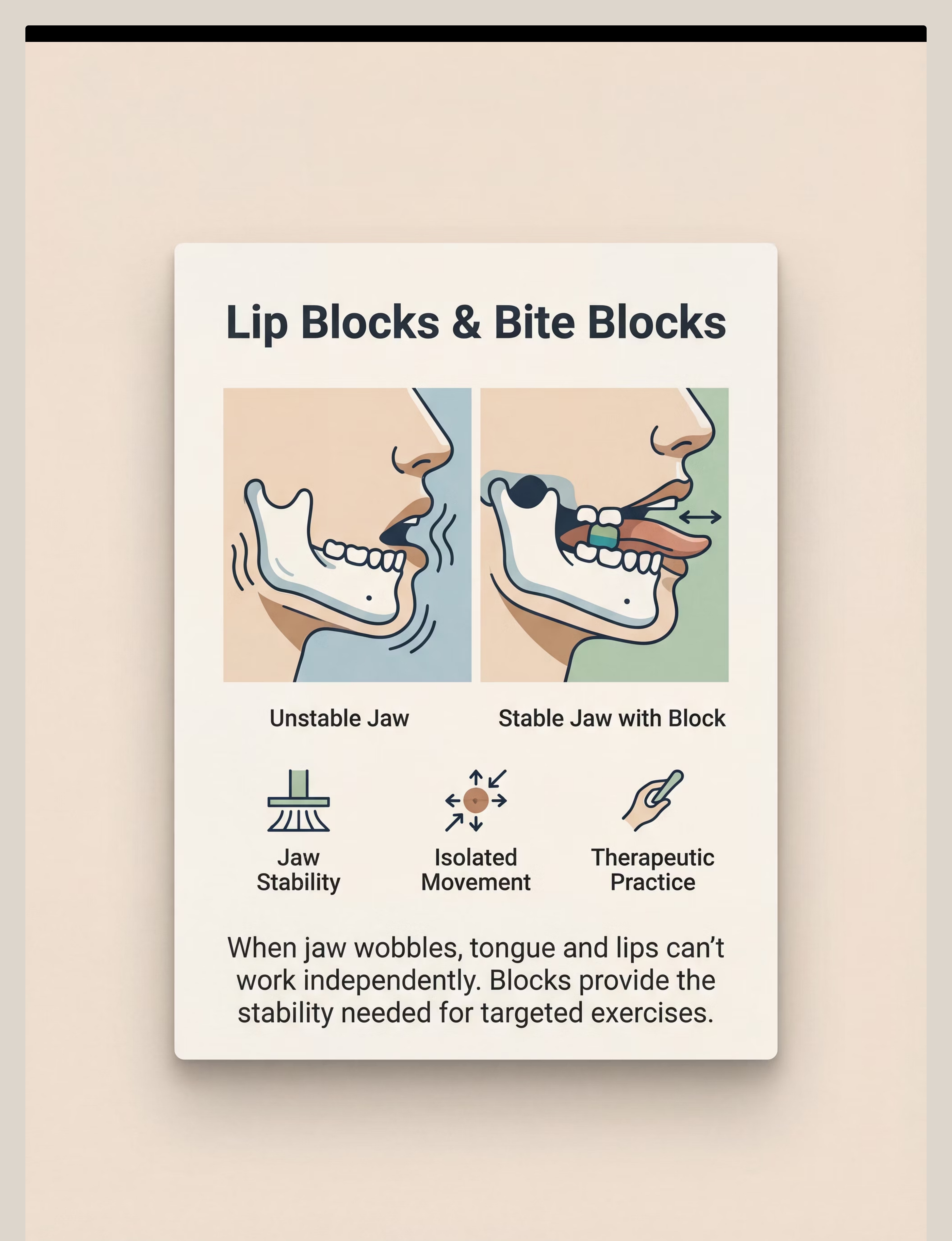
Material 6: Lip Blocks & Bite Blocks
What It Targets
Jaw stability as a stable base, and isolated lip/tongue movement. The bite block holds the jaw at a fixed position, freeing the tongue and lips to practice fine motor movements independently — without the jaw compensating. This is the most precise oral motor intervention on this list.
How to Use It
The bite block is placed between the molars at a specific jaw opening height (determined by the SLP). With the jaw stabilized, the child then performs isolated tongue and lip exercises. This isolates the target structure — the tongue or lips — without jaw compensation masking the deficit.
⚠️ SLP GUIDANCE REQUIRED. Do not use bite blocks without professional instruction, proper sizing, and trained supervision. Incorrect use can reinforce compensation patterns. This is the one material on this list that requires clinic guidance before home use.
At a Glance
💰Price Range: ₹500–1,500
🔗 Search Amazon.in → "Bite Block Oral Motor Therapy"
🏠DIY Alternative:⚠️ NO SAFE DIY — consult your SLP for guidance. Tongue depressors from pharmacy (₹30 for a pack) under professional guidance only.
⏱Session Target: As prescribed by SLP — not self-directed
📈Progress: Determined by SLP based on jaw stability measurements
👶Age Consideration: Typically introduced at 5–8 years with SLP

Material 7 of 9
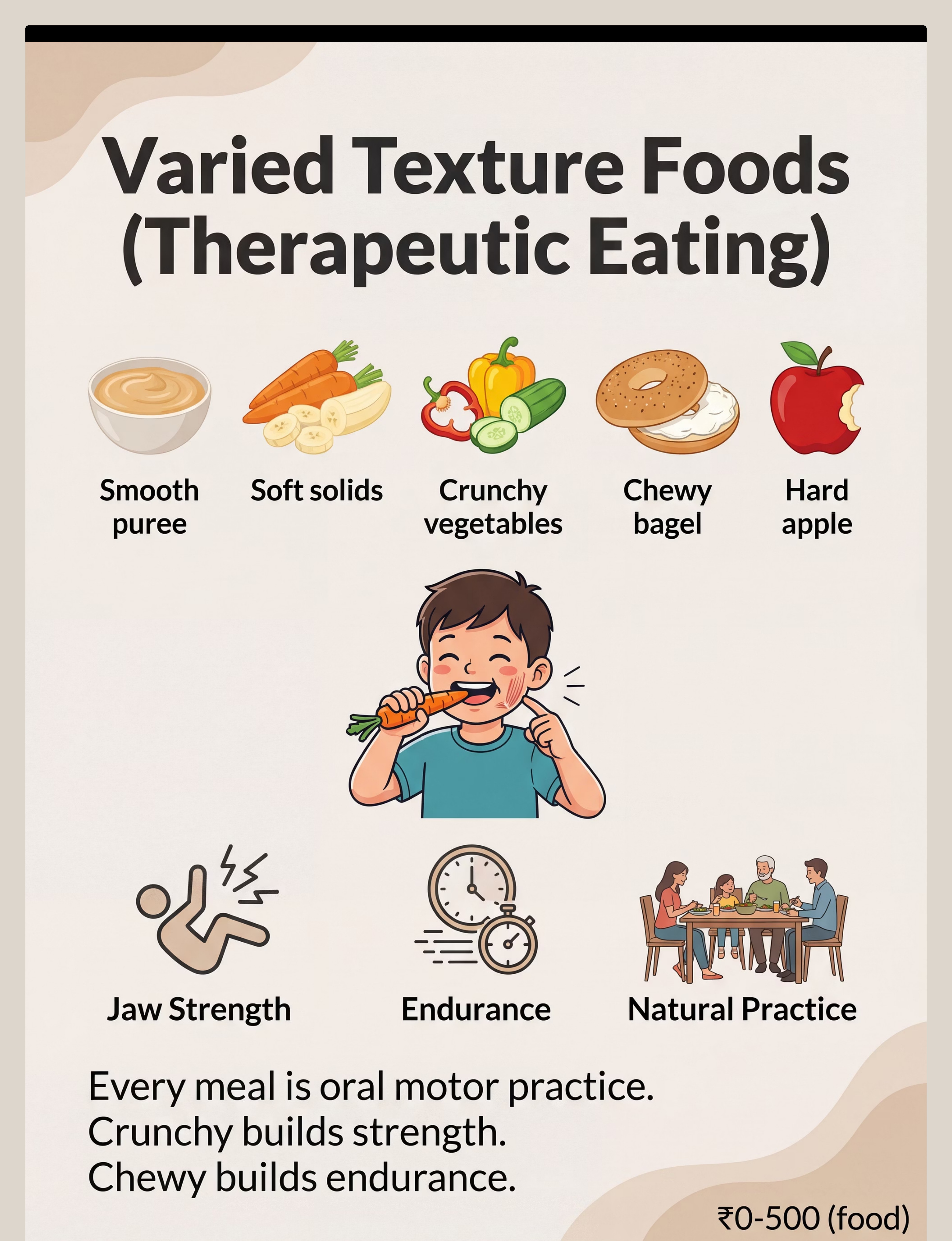
Material 7: Varied Texture Foods (Therapeutic Eating)
What It Targets
Jaw strength, chewing endurance, and texture tolerance. Every meal is an oral motor session. Therapeutic eating means deliberately choosing food textures that build the jaw, tongue, and cheek muscles — not just the textures your child currently accepts.
How to Use It
Child chews crunchy or chewy food on molars (not incisors). Target 15–20 chewing cycles per bite before swallowing. Progress through a texture hierarchy: dissolvable/melt-in-mouth (puffs, freeze-dried fruit) → soft chewable (banana, soft bread) → crunchy (crackers, carrots) → chewy (bagel, dried fruit, meat).
This is your kitchen. No purchase needed. Every meal is oral motor practice. Crunchy (carrots, crackers) → Chewy (bagel, meat) → Mixed texture. The principle costs nothing — just intentionality.
At a Glance
💰Price Range: ₹0–500 (normal food costs)
🏠Always available: Raw carrots, celery, apple slices, rice crackers, dried fruit, cheese cubes — zero additional cost
⏱Session Target: 15–20 chewing cycles per bite; jaw moving, not just swallowing whole
📈Texture Progression:
- Dissolvable/melt-in-mouth
- Soft chewable
- Crunchy
- Chewy
- Mixed texture
⚠️ Never push past the gag reflex. Back up one level if gagging occurs.
Material 8 of 9
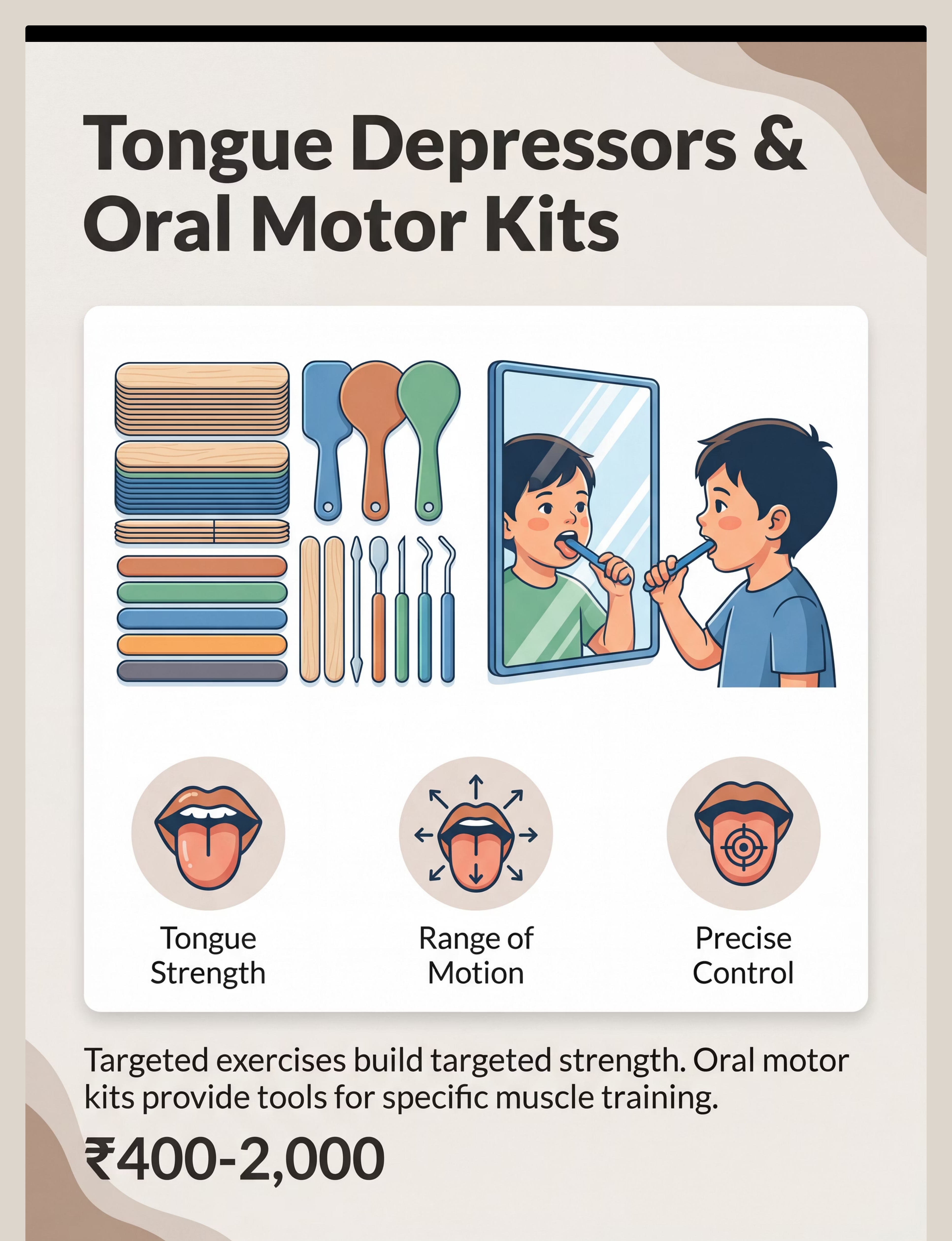
Material 8: Tongue Depressors & Oral Motor Kits
What It Targets
Tongue strength, range of motion, and precise tongue placement. The tongue must be able to move independently, elevate, lateralize (move food to molars), and retract — all while the jaw stays stable. Oral motor kits provide structured, progressive tongue exercises that build this fine motor control.
How to Use It
Follow SLP-prescribed tongue exercises: tongue up-down-left-right (5 reps each), tongue tip elevation (5 reps), tongue lateralization (5 reps each side). Use peanut butter or jam placed at target locations as a natural motivator for tongue movement. Always pair with a mirror for visual feedback.
Ask your SLP for specific exercises before beginning. Random tongue exercises can reinforce incorrect movement patterns. Precision matters more than effort here — a few correct reps are worth more than many compensatory ones.
At a Glance
💰Price Range: ₹400–2,000
🔗 Search Amazon.in → "Oral Motor Kit Tongue Exercises Therapy"
🏠DIY Alternative: Tongue depressors from pharmacy (₹30/pack) + peanut butter on lips for licking practice + mirror for visual feedback
⏱Session Target: 5 reps per movement, as prescribed by SLP
📈Progress: Tongue up/down → lateralization → retraction → precise placement

Material 9 of 9
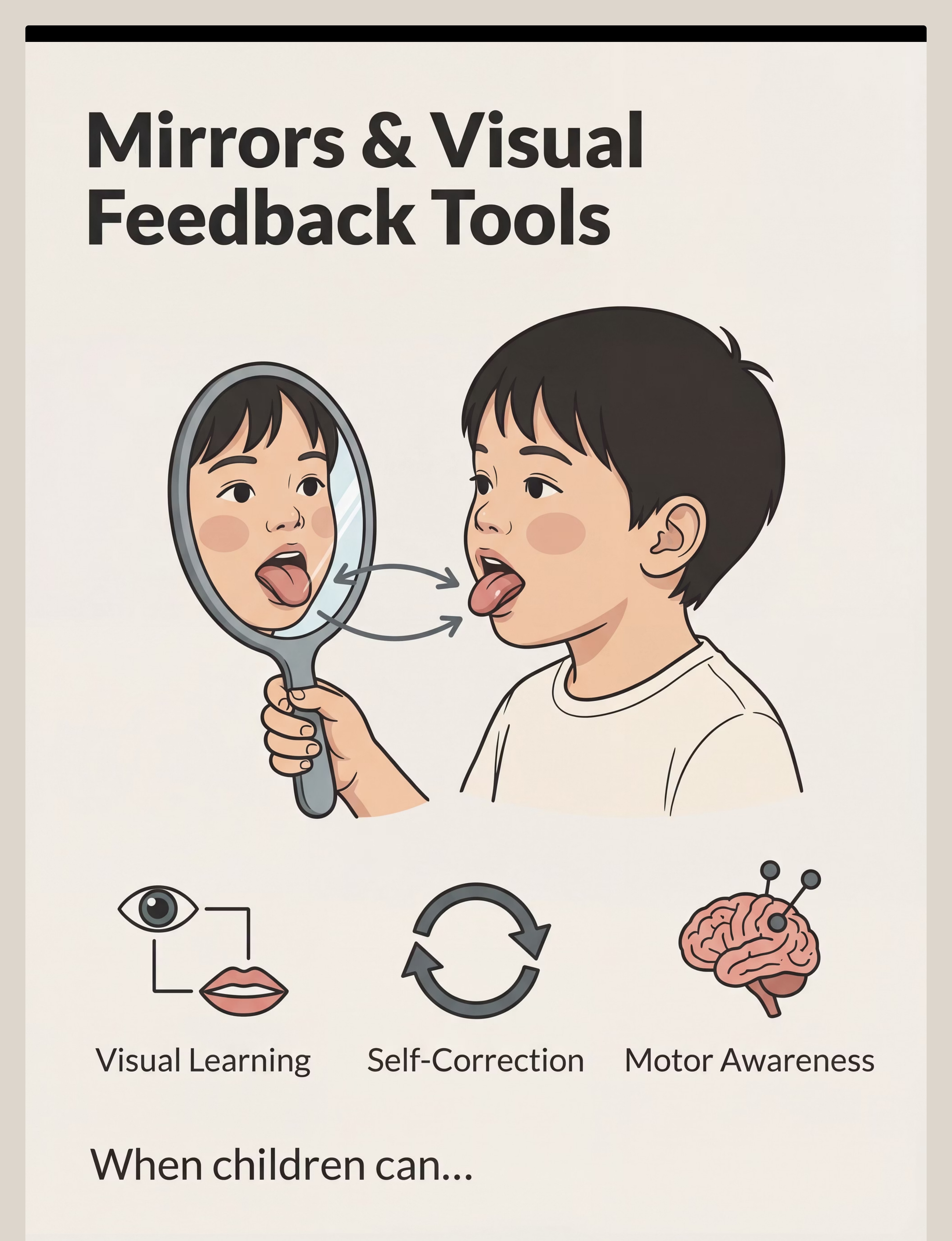
Material 9: Mirrors & Visual Feedback Tools
What It Targets
Motor learning through visual feedback, self-correction, and body awareness. Children with oral motor difficulties often cannot feel what their mouth is doing. A mirror gives them the visual information to see — and correct — their oral posture and movements in real time. Visual feedback is how motor learning accelerates.
How to Use It
Position mirror at child's eye level. Begin with "Copycat" games — parent demonstrates a movement (tongue out, lip pucker, big smile), child watches in mirror and imitates. Target: tongue up-down-left-right × 5; big smile → round lips × 5; lip pop × 10. The child should be watching themselves, not you, during practice.
Phone camera in selfie mode works perfectly — free and always available. The bathroom mirror works too. Parent's face as live model: "Watch my mouth. Now you try."
At a Glance
💰Price Range: ₹100–500
🔗 Search Amazon.in → "Unbreakable Therapy Mirror Children"
🏠DIY Alternative: Phone camera in selfie mode. Bathroom mirror. Parent's face as live model.
⏱Session Target: 5 reps per movement; child watching self-correction in mirror
📈Progress: Simple imitation → tongue exercises → lip exercises → full movement sequences
⭐Pro Tip: This is the turning point for many children. Seeing their own mouth movements is uniquely motivating.
All 9 Materials at a Glance
Each material targets a specific component of the oral motor hierarchy. Together, they build a complete foundation — from jaw to lips to tongue to sensory awareness.
Material | Primary Target | Price Range | SLP Required? | |
1. Therapy Straws | Lip strength, cheek tension | ₹200–800 | Recommended | |
2. Bubbles | Lip rounding, breath control | ₹50–300 | No — start today | |
3. Chewy Tubes | Jaw strength, chewing patterns | ₹300–1,000 | Recommended | |
4. Horns & Whistles | Breath power, lip seal | ₹100–500 | No — start today | |
5. Oral Sensory Tools | Oral awareness, sensory input | ₹800–2,500 | Yes — guidance needed | |
6. Bite Blocks | Jaw stability, isolated movement | ₹500–1,500 | YES — required | |
7. Therapeutic Foods | Jaw strength, texture tolerance | ₹0 (your kitchen) | No — start today | |
8. Oral Motor Kits | Tongue strength, range of motion | ₹400–2,000 | Yes — exercises prescribed | |
9. Mirrors | Visual feedback, motor learning | ₹100–500 | No — start today |
✅Starter Kit (Budget under ₹800): Bubbles (₹50) + short straw from kitchen + kitchen mirror + crunchy snack foods + party horn (₹20) = Complete starter kit at near-zero cost. You can begin today.
Every Family Can Start Oral Motor Therapy Today. No Purchase Required.
🌍 WHO Nurturing Care Framework: Context-specific, equity-focused, accessible-to-all
The principle is the same whether you spend ₹0 or ₹5,000. Lip muscles need suction practice. Jaw muscles need resistive input. Sensory awareness needs targeted input. The material is the vehicle — the principle is the engine.
Material | Buy This | Make This (₹0) | |
Therapy Straw | Honey Bear Straw Cup ₹300 | Regular straw cut to 10 cm. Use with thick smoothie for resistance. | |
Bubbles | Commercial bubble kit ₹100 | 1 tsp dish soap + 1 cup water. Wand = pipe cleaner loop. Or blow through straw into cup of water. | |
Chewy Tool | Chewy tube ₹400 | Firm silicone teether. Crunchy carrot sticks. Firm bread crust. | |
Blowing Toy | Party horn ₹20 | Paper towel roll + humming = DIY kazoo. Cotton balls blown across table. | |
Oral Sensory Tool | Z-Vibe ₹1,200 | Electric toothbrush (supervised). Damp textured washcloth. Temperature variation with spoon. | |
Bite Block | Commercial grade ₹700 | ⚠️ NO safe DIY. Tongue depressors from pharmacy under SLP guidance only. | |
Therapeutic Food | N/A — it's your kitchen | Raw carrots, celery, apple slices, rice crackers, dried fruit, cheese cubes. | |
Oral Motor Kit | Commercial kit ₹1,000 | Tongue depressors + peanut butter on lips for licking + mirror for visual feedback. | |
Mirror | Safety mirror ₹200 | Phone camera in selfie mode. Bathroom mirror. Parent's face as live model. |

Safety First: Before You Begin
Safe oral motor practice depends on knowing when to proceed, when to modify, and when to stop. Read this card carefully — and save 9100 181 181 in your phone before you begin any session.
🔴 STOP — Do Not Proceed
- Child is unwell, feverish, or has active respiratory infection
- Any history of aspiration confirmed by medical team
- Child is in sensory meltdown or behavioral dysregulation right now
- Bite blocks being used without SLP training and supervision
- Choking-risk materials with children under 18 months without direct supervision
- Severe oral aversion — forced entry causes trauma. Consult first.
🟡 AMBER — Modify & Proceed With Caution
- Tongue tie (ankyloglossia) — confirm with paediatrician before resistive tools
- Medications that affect muscle tone — check with neurologist first
- Sensory hypersensitivity — start with bubbles or mirror only. Never force.
- Dental issues — avoid hard resistive foods; use softer therapeutic options
- Oral sensory seeker — ensure all chew tools are BPA-free, food-grade, sized appropriately
🟢 GREEN — You Are Ready When:
- Child is calm, alert, rested, and had a recent small meal
- Medical clearance for oral motor intervention confirmed
- Materials are clean, age-appropriate, BPA-free
- You have read through all technique cards
- Emergency helpline 9100 181 181 saved in your phone ✅
🚨 STOP IMMEDIATELY if you observe: Coughing or choking during material use • Blue tinge around lips (cyanosis) • Extreme distress, severe gagging • Any material disappears (choking risk)

ACT II — SETUP
Set Up Your Space: The Right Environment Prevents 80% of Session Failures
A well-prepared space reduces child anxiety, minimizes distractions, and maximizes the quality of oral motor engagement. Set this up once — then it becomes your dedicated practice zone.
1
① Child Position
Seated with feet flat on floor or footrest (not dangling — affects jaw and core stability). Upright, 90° hip angle. Head neutral, not tilted back. For floor: cross-legged with back support.
2
② Parent Position
Beside child at eye level (not hovering above — reduces anxiety). Demonstrating, not directing. Calm, unhurried body language. Your energy sets the tone for the session.
3
③ Materials Tray
Placed within easy reach but out of immediate view (prevents fixation before ready). Organized in order of use. All materials pre-cleaned and checked for damage before each session.
4
④ Environment
Remove distracting screens and noisy toys. Reduce competing smells (perfume, food cooking). Natural lighting is best — avoid harsh fluorescent. Soft background music optional; observe child's response.

Step 1: The Invitation
Step 1 of 6
Duration: 30–60 seconds
Bring your child into the activity without a command. Present one material (start with bubbles or a mirror) as play, not therapy. Match your energy to your child's current state — calm or gently playful. You are not starting a session. You are starting a conversation.
"Hey, want to see something cool?" (Place bubbles or mirror nearby — don't hand it yet.) "Look at this..." (Blow a bubble yourself or make a funny face in the mirror.) "Your turn?"
For non-verbal / limited verbal children: Use a visual choice board — show 2 materials, let child point or reach. Their choice = their invitation.
✅ Acceptance Cues (Ready)
- Reaches toward material
- Eye contact or orientation toward material
- Body leaning in
- Vocalizes or uses AAC to indicate interest
✗ Resistance Cues (Modify or Wait)
- Turns away, pushes material back
- Increases stereotyped behavior
- Crying or distress vocalizations

Step 2: The Engagement
Step 2 of 6
Duration: 1–3 minutes
Deepen the interaction by introducing the therapeutic aspect of the material — naturally, not clinically. The child is engaged with play; you are engineering the oral motor demand embedded in that play. The therapeutic work should feel invisible to the child and meaningful to you.
1
🫧 Bubbles
"Let's see how big we can make it... pucker your lips... like this... now blow slowly..." Model lip rounding — child imitates.
2
🥤 Therapy Straw
"Silly straw race! Let's see who can finish their smoothie first!" Position straw at midline — not corner of mouth.
3
🦷 Chewy Tube
"This is your chewy. Bite here... and here... and here." Demonstrate bilateral biting pattern — child follows.
4
🪞 Mirror
"Let's play Copycat! Can you stick out your tongue like me? Now curl it up..." Exaggerate movements. Make it a game.
Praise immediately when the child produces oral motor engagement — even partial, even approximate. "Yes! Great blowing! Did you feel your lips work?!" Reinforcement within 3 seconds of the behavior is the most powerful learning signal.
Step 4: Repeat & Vary
Step 4 of 6
Duration: 3–5 minutes
Oral motor skills require repetition to build strength and neural automaticity — but too many repetitions causes fatigue and loss of quality. Find the sweet spot: quality over quantity, always.
"3 good reps > 10 forced reps." Quality of movement matters more than quantity. When the jaw drops and compensates, or lips open during suction — that is a signal to rest, not push.
Variation keeps engagement high and provides progressive challenge:
For Bubbles
Small wand → big wand → blow bubbles in water through straw → blow a cotton ball across the table
For Straw
Thin straw → thick straw → shorter → longer → thicker liquid → thinner liquid
For Chewy Tube
Soft resistance → medium → firm | Position: center → left molar → right molar
For Mirror
Tongue lateralization → tip elevation → lip rounding → lip retraction → lip pop
Satiation Indicators — session has had enough: Child pushes material away repeatedly • Jaw dropping, movement quality decreasing • Distraction increasing sharply • 15+ minutes have passed

Step 5: Reinforce & Celebrate
Step 5 of 6
Duration: woven throughout session
Immediate, specific, enthusiastic reinforcement delivered within 3 seconds of the desired behavior is the most powerful driver of skill learning. Magnitude matters less than timing and specificity. "Good job!" is too vague — name exactly what you saw.
1
"Amazing! Your lips stayed together the whole time you blew — I saw them work so hard!"
2
"Did you hear that bubble? That was YOUR breath that made it!"
3
"Your jaw bit down strong on both sides — I can see those muscles getting stronger!"
4
"You watched yourself in the mirror AND fixed your tongue — that is a superpower!"
Reinforcement Menu Options
🏷️ Social
Thumbs up, high five, hug, dance celebration together
⭐ Token
Star sticker on chart, point toward preferred activity
📲 Activity
3 min preferred screen time, choose next activity, favorite toy access
🎮 Natural
The bubbles themselves, funny mirror faces, chewy sensation as the reward
"Celebrate the attempt, not just the success." A child who tried to blow and produced no bubble still moved their lips. That is a rep. That is progress.

Capture the Data: Right Now — Within 60 Seconds
"60 seconds of data now saves hours of guessing later." Before the moment is gone, record three simple fields. This data becomes your child's oral motor progress story — and your SLP's most valuable tool.
1
Field 1 — Date & Material Used
Date: ___ | Materials used today: Straw / Bubbles / Chewy / Horn / Sensory / Block / Food / Kit / Mirror
2
Field 2 — Participation Rating (1–5)
1 = Refused | 2 = Minimal tolerance | 3 = Participated with support | 4 = Participated independently | 5 = Sought it out!
3
Field 3 — One Observation
"Today I noticed: ___" (e.g., "She kept lip seal for 2 seconds on the straw" / "He bit the chewy tube on both sides for the first time")
BACB data collection standards — ABA continuous measurement protocols (Cooper, Heron & Heward, Applied Behavior Analysis, 8th Ed.)
What If It Didn't Go As Planned?
Reality Check: Most sessions aren't perfect. That's not failure — that's data. Here are the most common session challenges and exactly what to do next time. Every problem has a clinical reason and a practical solution.
My child refused to put anything near their mouth
Why: Oral defensiveness / sensory hypersensitivity. The mouth is highly protected neurologically.
Next time: Start from maximum distance — hold bubble wand 30 cm from child, blow yourself. Bring closer only when child shows interest. Never force proximity.
Next time: Start from maximum distance — hold bubble wand 30 cm from child, blow yourself. Bring closer only when child shows interest. Never force proximity.
My child chewed the straw instead of using it
Why: Jaw sensory-seeking behavior — the straw provides proprioceptive input they're craving.
Next time: This is useful data. Introduce chewy tube for jaw input BEFORE straw work. Meet the sensory need first.
Next time: This is useful data. Introduce chewy tube for jaw input BEFORE straw work. Meet the sensory need first.
My child gagged when I introduced the textured food
Why: Gag reflex may be hypersensitive (anteriorly positioned). Normal in oral motor difficulties.
Next time: Back up one texture level. Stay at that level for 1–2 weeks. Never force textured food past the gag reflex.
Next time: Back up one texture level. Stay at that level for 1–2 weeks. Never force textured food past the gag reflex.
My child could only blow bubbles for 3 seconds
Why: This IS the weakness. Low respiratory support + low lip endurance. 3 seconds is their current baseline.
Next time: 3 seconds is your starting point. Track duration each session. Aim for 4 seconds next week.
Next time: 3 seconds is your starting point. Track duration each session. Aim for 4 seconds next week.
My child moved their whole jaw instead of just tongue in mirror exercises
Why: Jaw instability causing compensatory movement. Tongue can't work independently yet.
Next time: Introduce chewy tube work to build jaw stability FIRST. Then return to tongue exercises.
Next time: Introduce chewy tube work to build jaw stability FIRST. Then return to tongue exercises.
My child lost interest after 3 minutes
Why: Attention, motivation, or fatigue. 3 minutes of genuine engagement > 15 minutes of forced compliance.
Next time: 3 minutes IS your session length for now. Keep it short, end on success. Gradually extend.
Next time: 3 minutes IS your session length for now. Keep it short, end on success. Gradually extend.
I feel like I'm doing it wrong
Why: You probably aren't — but precision matters in oral motor therapy.
Next time: Take a video and share with your SLP at the next appointment. Book a teleconsult at 9100 181 181.
Next time: Take a video and share with your SLP at the next appointment. Book a teleconsult at 9100 181 181.

ACT IV — PROGRESS
Weeks 1–2: Tolerance, Not Mastery
This is the foundation-pouring phase.
15%
Foundation Phase
Progress in Weeks 1–2 is about building tolerance and establishing routine — not achieving mastery
🟢 This IS Progress | 🔴 This is Not Yet Progress | 🟡 This is Normal | |
Child tolerates bubble wand near face without crying | Child can't yet blow a bubble | Refusing mirror work | |
Accepts straw in mouth for 5 seconds | Not yet creating suction | Gagging on textured food (decreasing) | |
Sits for 5-min session (even with fidgeting) | Can't yet sustain chewy tube | Varying participation day to day | |
1–2 sessions with Rating 3+ out of 5 | Still drooling consistently | Needing high reinforcement ratio |
"If your child tolerates the bubble wand for 3 seconds longer this week than last — that is real, measurable, meaningful progress. Oral motor work is counted in millimeters, not miles."
Data to Watch: Participation rating trending up (even by 0.5 points) • Refusal rate decreasing • First successful straw sip — mark the date!

Weeks 3–4: Consolidation Signs
Neural pathways for oral motor movement are forming through repeated, structured input. The brain is learning what the mouth should feel like.
40%
Consolidation Phase
Skill consolidation begins to emerge — watch for these specific observable indicators
Child anticipates the activity
Brings the bubble wand to you. Moves toward the materials tray. Asks for "the chewy." This is intrinsic motivation — the strongest sign of consolidation.
First sustained straw use
3–5 consecutive sips without prompting. Mark this date. This is a measurable motor milestone.
Drooling visibly reduced
Reduced in focused/alert moments — even if still present during fatigue or distraction. The lip closure muscles are strengthening.
Chewy tube accepted bilaterally
First time child bites on both sides without resistance. Jaw stability baseline is rising.
Child watches self in mirror with interest
Not avoidance — curiosity. This signals growing oral body awareness and readiness for motor learning.
When to increase frequency or intensity: Participation rating consistently 4–5 out of 5 • Child seeking materials between sessions • SLP says "Ready to progress"
Weeks 5–8: Mastery Indicators
75%
Mastery Phase
Observable, measurable mastery criteria emerging across oral motor skill domains
Skill | 🏆 Mastery Indicator | |
Straw drinking | Uses straw for all beverages without prompting | |
Lip closure | No drooling during play/focus activities | |
Jaw stability | Chews on both sides; food doesn't fall from mouth | |
Blowing | Blows out birthday candles; sustained bubbles >5 seconds | |
Tongue control | Can lick lips fully; moves food laterally to molars | |
Texture acceptance | Eating 3+ texture groups independently at mealtimes | |
Speech clarity | Primary caregiver reports improvement; SLP confirms |
Generalization Indicators — The Real Test
Skill appearing in new contexts is the gold standard of mastery. Watch for: using a straw at restaurants without prompting • reduced drooling at school (teacher reports) • eating a variety of textures at a friend's house • speech more intelligible to strangers.

You Did This.
Your child's mouth is stronger because you showed up — consistently — for weeks.
Over the past 5–8 weeks, while juggling everything else in your life, you set up a dedicated practice space, learned 9 therapeutic materials, tracked progress when it would have been easier to guess, pushed through the days when your child refused, and celebrated the 3-second improvements that no one else could see.
A Stronger Jaw
More active lips, a more coordinated tongue — built rep by rep, session by session
Straw Milestone
May be using a straw for the first time — a measurable oral motor victory
Less Drool Today
May have less drool on their shirt today than 8 weeks ago — lip muscles are working
Clearer Speech Ahead
On a trajectory toward clearer speech and more confident eating in every setting
🎉 Family Celebration: Cook a meal together that uses a new texture your child now accepts. Let them see — and feel — the difference they've made.
📸 Photo/Journal Prompt: "Before (Week 1): ___ | After (Week 8): ___" Document in your phone or print for your home therapy folder. This is evidence of transformation.
Red Flags: When to Pause and Consult
Even after progress, stay alert. These signs mean pause and consult — not panic, but prompt action. Trust your instincts. If something feels wrong, it deserves investigation. Call 9100 181 181 for guidance.
🚨 STOP AND CONSULT IMMEDIATELY: Any coughing, choking, or wet/gurgly voice quality during or after eating/drinking (may indicate aspiration risk) • Sudden regression after achieving progress • New or worsening drooling with facial asymmetry or weakness • Child reports pain in jaw, mouth, or throat during exercises • Extreme oral aversion worsening despite gradual exposure
⚠️ PAUSE AND TELECONSULT WITHIN 1 WEEK: Participation rating dropping to 1–2 consistently after previously higher engagement • No change across all 9 materials after 8 weeks of consistent daily practice • Child developing new avoidance behaviors • Feeding affecting weight gain or nutrition
Domain L: Feeding & Oral Motor — Explore Your Full Toolkit
The materials you already own from L-983 connect directly to these related techniques. You are not starting over — you are expanding. Therapy Straws, Mirrors, and Chewy Tubes appear across multiple Domain L techniques.
🟢 INTRO
L-981: 9 Materials for Transitioning to Solid Foods
The entry point. Therapeutic foods (from your kitchen) and texture introduction strategies for children moving from purees to table foods.
🟡 CORE
L-982: 9 Materials for Self-Feeding Independence
Adaptive utensils, feeding skill development, and supported independence at mealtimes. Core prerequisite to L-983.
🔴 ADVANCED
L-984: 9 Materials for Articulation Practice
The next step after L-983. Mirror, oral motor kit, and precision exercises for speech sound accuracy and intelligibility.
🟡 CORE
L-950: 9 Materials for Oral Motor Input
Chewy tools, straw activities, and proprioceptive oral input for children who are sensory-seeking or need foundational jaw work before L-983.
ACT V — COMMUNITY
Real Families. Real Progress. Specific Timelines.
Not promises — documented outcomes. These composite vignettes represent the kinds of outcomes families achieve with consistent, structured oral motor practice and professional support.
Riya's Story — Bangalore
Age 3.5 years
Before: Drooled constantly — multiple shirt changes daily. Could not use any straw. Diet: smooth purees and thin liquids only. Speech 30% intelligible even to parents. Mealtimes: 45–60 minutes, exhausting.
Intervention: 8 weeks of daily home oral motor practice. Therapy straws (honey bear) + daily bubbles + SLP sessions 2×/week.
After (Week 8): Straw drinking functional for all beverages. Drooling reduced to occasional. Soft chewable foods tolerated. Parents report 30% improvement in speech clarity.
"I spent three years thinking this was just who she was. Eight weeks of consistency showed me — and her — that her mouth could learn." — Riya's mother
Arjun's Story — Hyderabad
Age 5 years
Before: Open mouth posture. Could not blow out birthday candles at ages 3 or 4. Jaw slid side to side during chewing. Food pocketed in cheeks. Speech 60% intelligible; /p/, /b/, /m/ sounds weak.
Intervention: Mirror work + bilateral chewy tube + therapeutic eating + SLP sessions.
After (Week 10): Closed mouth posture at rest 80% of the time. Blew out all 5 candles at his 5th birthday party. Jaw stable during chewing. Speech intelligibility improved to 80%.
"The mirror work was the turning point. He could finally see what his tongue was doing." — Arjun's father
Connect With Other Parents: Isolation is the Enemy of Adherence
Your people are here. Families navigating oral motor development are a vibrant, generous community — sharing wins, troubleshooting setbacks, and holding each other through the hard days. The WHO NCF engaged over 1,000 individuals from 111 countries in building its framework: community engagement is a core therapeutic principle, not an optional extra.
📱 WhatsApp Parent Group
Pinnacle Oral Motor Parent WhatsApp Group — families navigating oral motor development challenges, sharing wins, questions, and honest struggles in real time.
💬 Online Parent Forum
Moderated discussion forum for parents of children with feeding difficulties and oral motor challenges. At pinnacleblooms.org/community
🤝 Peer Mentoring
Connect with a family who has navigated oral motor intervention and is willing to share their journey and answer your real-world questions.
📍 Local Pinnacle Meetups
Monthly in-person parent meetups at Pinnacle centers — Hyderabad, Bangalore, Chennai, Mumbai, Delhi, and 60+ more cities across India.
Your Professional Support Team: 70+ Centers Across India
Home practice and professional support work together to produce maximum impact. Your nearest Pinnacle center is closer than you think — and teleconsultation means expert guidance is available regardless of where you live.
🏥 Pinnacle Center Visit (In-Person)
70+ centers across India. Comprehensive oral motor assessment + feeding evaluation + SLP + OT + multi-disciplinary team. Same-day assessment available at most centers.
→ Find My Nearest Center | → Book an Appointment
pinnacleblooms.org/centers
pinnacleblooms.org/centers
📱 Teleconsultation (Remote)
Expert SLP + OT oral motor consultation from anywhere in India or internationally. Same GPT-OS® clinical standards as in-person visits.
→ Book Teleconsult
pinnacleblooms.org/teleconsult
pinnacleblooms.org/teleconsult
📞 FREE National Helpline
Expert guidance. 16+ languages. Available 24×7. For questions, concerns, referrals, and immediate support.
9100 181 181
Specialty Matching for Oral Motor
Primary: Speech-Language Pathologist (Oral Motor + Feeding specialist) | Secondary: Occupational Therapist (Sensory + Feeding) | As indicated: Orofacial Myologist • ENT • Paediatric Dentist • Feeding Therapy team
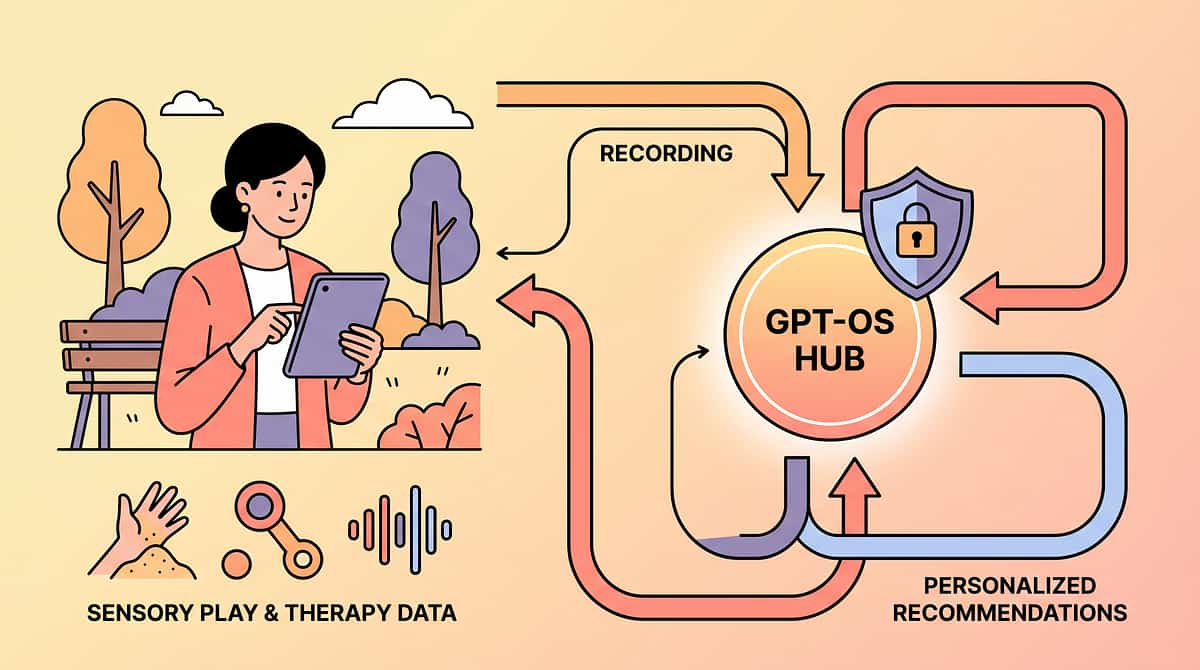
How GPT-OS® Uses Your Session Data to Make Your Child's Plan Smarter
Every session you log makes your child's plan smarter — and contributes to better outcomes for every child like yours. Population-level data from 20M+ sessions powers the recommendations that make GPT-OS® more accurate for every new family.
What GPT-OS® Learns From Your Data
- Your child's oral motor response curve (rate of improvement)
- Which materials your child responds best to (personalized material ranking)
- Optimal session timing and duration for your child
- Predictive indicators for when to escalate to professional evaluation
🔒 Privacy Assurance
All data is encrypted, de-identified for population analysis, and governed by India's DPDP Act. Your child's individual data is never sold or shared without explicit consent.
→ Privacy Policy: pinnacleblooms.org/privacy

Watch the Reel: L-983 in 75 Seconds
Video modeling is classified as evidence-based practice for autism (NCAEP, 2020). Watching + reading + doing = maximum parent skill acquisition. This reel shows all 9 oral motor materials demonstrated by a Pinnacle SLP — see exactly what each material looks like in use.
"In this reel, our SLP demonstrates the jaw-to-lip-to-tongue hierarchy in action. Watch for the cheek engagement during straw use, the lip rounding during bubbles, and the bilateral bite pattern with the chewy tube. These are the movements your child's mouth is learning." — Pinnacle SLP Consortium
Reel L-983 | Feeding & Oral Motor Series | Episode 983 of 999
Watch on the Pinnacle Blooms Instagram, YouTube, or the techniques.pinnacleblooms.org platform. Demonstrates: therapy straws • bubbles • chewy tubes • blowing toys • sensory tools • bite blocks • therapeutic eating • oral motor kits • mirrors
Watch on the Pinnacle Blooms Instagram, YouTube, or the techniques.pinnacleblooms.org platform. Demonstrates: therapy straws • bubbles • chewy tubes • blowing toys • sensory tools • bite blocks • therapeutic eating • oral motor kits • mirrors
📱 Instagram
@pinnacleblooms — Reel L-983 in Feeding & Oral Motor highlights
▶️ YouTube
Pinnacle Blooms Network® — Domain L playlist, Episode 983
🌐 Website
techniques.pinnacleblooms.org/feeding-oral-motor/L-983
Share This With Your Family: Consistency Across ALL Caregivers Multiplies Impact
The grandparent, the teacher, the nanny — they all need this too. A child who practices with one caregiver and has no support from others progresses at a fraction of the rate of a child whose entire environment supports oral motor development. Share now.
Share This Page
For Grandparents — The Short Version
"The therapist has given us 9 tools to help [child's name]'s mouth get stronger. Blowing bubbles, drinking from straws, and chewing special foods are all part of it. Let me show you. It takes 10 minutes and fits into snack time."
📄 Download Resources
L-983 One-Page Family Guide (PDF)
Simplified A4 print-ready guide: 9 materials, quick-start instructions, safety notes, and the Pinnacle helpline. For grandparents, teachers, nannies.
Simplified A4 print-ready guide: 9 materials, quick-start instructions, safety notes, and the Pinnacle helpline. For grandparents, teachers, nannies.
School Communication Template
Formally communicate with school staff about oral motor accommodations: straw access, texture-appropriate snacks, mirror practice during morning routine.
Formally communicate with school staff about oral motor accommodations: straw access, texture-appropriate snacks, mirror practice during morning routine.

ACT VI — FAQ
Frequently Asked Questions
Answers to the questions every parent asks. Grounded in clinical evidence, written in plain language, and specific enough to actually help you make decisions today.
How long before I see results?
Most parents observe first changes (reduced drooling in focused moments, first successful straw sip) within 2–4 weeks of consistent daily practice. Measurable functional improvement typically emerges at 6–10 weeks. Full oral motor skill development is a 6–18 month journey depending on severity.
Can I do this without a speech therapist?
Home materials and play-based activities (bubbles, straws, mirror work, therapeutic eating) are safe to begin immediately. However, bite blocks, Z-Vibes, and structured tongue exercises require SLP guidance. For any child with significant oral motor difficulties, professional evaluation is essential. Call 9100 181 181 for guidance.
My child has autism. Are these techniques autism-specific?
These materials are used across oral motor difficulties regardless of diagnosis. Autism frequently co-occurs with oral motor challenges, but the materials target the underlying jaw-lip-tongue weakness directly. The approach is adapted (higher reinforcement, sensory considerations, visual supports) for autism — but the therapeutic principles are universal.
Is a sippy cup okay?
Sippy cups do not build oral motor skills — they function similarly to bottles, with gravity doing the work rather than the child's lip and cheek muscles. Transition to open cups and straws as soon as your child has sufficient jaw stability. Your SLP can advise on timing.
More Frequently Asked Questions
How many materials do I need to start?
One is enough. Start with bubbles or a straw — both cost under ₹100. Once you've established a routine with one material, add a second. You do not need all 9 materials simultaneously. The starter kit (bubbles + short straw + kitchen mirror + crunchy snack + party horn) costs under ₹800 and covers the full therapeutic spectrum.
My child only ate purees and is now 5 years old. Is it too late?
No. Oral motor skills can be developed at any age — the brain retains significant plasticity throughout childhood and into adolescence. Earlier is better, but 5 years is not too late. Professional assessment will identify the current baseline and design an appropriate progression.
How is oral motor development related to autism?
Children with ASD frequently present with oral motor difficulties due to sensory processing differences, motor planning challenges, and low muscle tone. These are not caused by autism but co-occur with high frequency. Oral motor intervention is standard practice in comprehensive ABA + SLP treatment for autism.
What if my child bites me or the materials aggressively?
Oral biting may indicate: (1) proprioceptive seeking — introduce chewy tube with appropriate resistance; (2) communication of refusal — review ABA communication support; (3) sensory hypersensitivity causing dysregulation. Consult your BCBA and SLP together. 9100 181 181.
Preview of 9 materials that help with oral motor development Therapy Material
Below is a visual preview of 9 materials that help with oral motor development therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
ACT VI — START NOW
Reading About Oral Motor Development is Step One. Step Two Starts Now.
You have the knowledge. You have the materials (or the DIY alternatives). You have the protocol, the progress map, the community, and the full backing of India's largest multi-disciplinary pediatric therapy consortium. The only thing left is to begin.
1
Start This Technique Today
Launch GPT-OS® guided oral motor session. Start with bubbles — today, at home, right now.
2
Book a Professional Consultation
SLP + OT oral motor assessment at a Pinnacle center. Or call 9100 181 181 for teleconsult.
3
Track Your First Session
Record your 3 fields within 60 seconds: date/material, participation rating 1–5, one observation.
4
Explore the Next Technique
When ready: L-984 — 9 Materials That Help With Articulation Practice is waiting.
📞 FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7
1
🗣️ SLP
Primary Lead
2
🖐️ OT
Sensory + Feeding
3
🧠 ABA/BCBA
Reinforcement
4
📚 SpEd
Generalization
5
🧬 NeuroDev
Medical Oversight