
When little hands can't hold on.
The spoon twists at breakfast. The crayon is fisted like they're two, not five. Toys tumble from fingers that never quite close in time. You are not failing. Your child's hand system is still learning — and it can be taught.
Technique F-591
Episode 591 of 600
Gross Motor & Physical Development

9 Materials That Help With Object Grasping
Pinnacle Blooms Network® | GPT-OS® Technique Page | F-591
🦾 Discipline
Occupational Therapy — Primary Lead. ABA, SLP, NeuroDev as secondary supports.
🎯 Domain
Fine Motor Skills / Hand Function / Grasp Development. Ages 0–8 years.
📋 Format
Home protocol. 10–20 min sessions. 3–5× per week. Parent-delivered.
✅ Evidence
Grade I–II. Systematic Review + RCT level. 20M+ sessions. 97%+ improvement rate.
"Every dropped object feels like a reminder of difference. But grasp is a skill. Skills develop with the right practice, at the right level, with the right materials. You're in the right place." — Pinnacle Blooms Consortium | OT + ABA + NeuroDev + SLP + SpEd
📞Helpline: 9100 181 181 — FREE | 16+ Languages | 24×7
You Are Not Alone: The Numbers
Grasp difficulties are not rare. They are a documented developmental pattern affecting children across every country, every background, every diagnosis profile. The gap isn't awareness — it's access to the right materials and the right protocol. This page closes that gap.
1 in 6
Motor Delays
Children experience developmental motor delays affecting hand function — WHO Global Data
80%
ASD Fine Motor
Children with autism spectrum condition show fine motor or grasp-related difficulties — PRISMA Systematic Review, 2024
97%+
Improvement Rate
Children at Pinnacle centers show measurable grasp improvement with structured intervention — Pinnacle Network RWE
8–10M
In India Alone
Children under age 8 navigating fine motor or grasp development delay — majority without structured therapeutic support at home
"When our therapist explained that 80% of autistic children have fine motor challenges, I stopped blaming myself. I started focusing on what we could actually do." — Mother of a 4-year-old, Pinnacle Hyderabad Center
References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | WHO Global Data on Developmental Disabilities

What's Happening in Your Child's Brain
🧠 The Science
This is a wiring difference — not a behavior problem. Understanding the neuroscience helps you understand why the right materials create real, lasting change.
Brain Regions Involved
- Somatosensory Cortex — touch processing
- Motor Cortex — movement execution
- Cerebellum — coordination and timing
- Proprioceptive Pathways — body-in-space awareness
- Corticospinal Tract — brain-to-hand signal highway
Why the Hand Doesn't Know How Hard to Grip
The somatosensory cortex processes touch signals from the fingers. In children with grasp difficulties, this system may under-report (leading to dropping) or over-report (leading to excessive squeezing and fatigue). The brain never gets calibrated feedback.
Why Fingers Don't Isolate Properly
Mature grasp requires independent finger movement — thumb and index act while the other three stabilize. This requires sophisticated corticospinal organization that develops through structured, repetitive practice.
Why Proprioception Matters
Children who don't "feel" where their hands are in space can't execute precise grasp patterns. Resistance-based materials (putty, clothespins) feed proprioceptive information directly into the sensory system — teaching the brain what "holding on" actually feels like.
Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660

Where This Sits in Development
Understanding your child's current developmental position is the first step to knowing where you're headed. Grasp development follows a predictable sequence — and structured intervention helps children progress through each stage with greater confidence and speed.
0–3 mo
Reflexive Grasp — automatic, not voluntary
3–4 mo
Ulnar Palmar — first voluntary grasp attempt
5–6 mo
Palmar Grasp — whole hand involved
6–9 mo
Radial Digital Grasp — fingers emerge
9–12 mo
Pincer Grasp — thumb + index finger
2–4 yrs
Tripod Grasp — pencil and spoon mastery
4–8 yrs
Tool Mastery — scissors, buttons, writing
Common co-occurring conditions: Autism spectrum condition, developmental coordination disorder (DCD/dyspraxia), hypotonia (low muscle tone), cerebral palsy, and sensory processing differences frequently co-occur with grasp difficulties.
Forward path: With consistent use of the 9 materials in this guide, progress typically follows: Tolerance → Pattern formation → Strength building → Functional use → Generalization.
References: PMC9978394 | WHO/UNICEF CCD Package (2023)

The Evidence Behind This Technique
Evidence Grade: I–II
Systematic Review + RCT
Clinically Validated. Home-Applicable. Parent-Proven. This is not anecdote — it is the convergence of systematic research, 20 million therapy sessions, and 70 centers of clinical observation, all pointing to the same conclusion: the right materials, used consistently, build functional grasp.
📚 PRISMA Systematic Review — Children, 2024
16 articles (2013–2023) confirm sensory integration and materials-based intervention meets criteria for evidence-based practice in children with ASD. PMC11506176
📚 Meta-Analysis — World J Clin Cases, 2024
24 studies demonstrate sensory integration therapy effectively promotes fine motor skills, adaptive behavior, and sensory processing. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
📚 Indian RCT — Padmanabha, 2019
Home-based sensory and motor interventions demonstrate significant outcomes in the Indian pediatric population — validating parent-administered protocols. Indian Journal of Pediatrics | DOI: 10.1007/s12098-018-2747-4
📚 WHO/UNICEF CCD Package, 2023
Care for Child Development implemented across 54 LMICs using household materials. Fine motor stimulation is a core component of caregiver-administered early intervention. PMC9978394
"This is not anecdote. This is the convergence of systematic research, 20 million therapy sessions, and 70 centers of clinical observation — all pointing to the same conclusion: the right materials, used consistently, build functional grasp." — Pinnacle Blooms Clinical Research Office

F-591: What Is This Technique?
The Grip-Building Home Kit
Technique Definition
Object Grasping Material Intervention is a structured, evidence-based occupational therapy approach using 9 specific therapeutic materials to develop the strength, pattern, and sensory awareness needed for functional hand grasping in children aged 0–8.
Each material targets a distinct component of the grasp system — from intrinsic muscle strength (therapy putty) to pincer pattern formation (tongs and tweezers) to sensory feedback calibration (textured objects).
This is not a craft activity. This is precision-targeted hand rehabilitation disguised as play.
Technique Identifiers
- Code: F-591 | Domain Code: FIN-GRASP
- Domain: Fine Motor / Grasp Development
- Sub-Domain: Prehension Patterns
- Age Range: 0–8 years
- Session Duration: 10–20 minutes
- Frequency: 3–5× per week
- Series: Episode 591 of 600
Canon Materials
Therapy Putty | Tongs & Tweezers | Sensory Balls | Pegboards | Finger Isolators | Clothespins | Lacing Cards | Squeeze Tools | Adapted Grips

Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type. Four disciplines contribute to making this protocol work at maximum effectiveness for your child.
Occupational Therapy — Primary Lead
OTs design the full grasp protocol: assess current grasp pattern, select appropriate materials and resistance levels, sequence activities by difficulty, and track progression from palmar to tripod grasp. The OT trains parents in correct material use and adjusts the home program based on data.
Speech-Language Pathology — Oral Motor
SLPs adapt squeeze and resistance tools for oral motor development. Children working on feeding skills benefit from the same graded-force training used in hand grasping — squeeze bottles translate directly to oral motor force control.
ABA / BCBA — Reinforcement & Data
BCBAs design the reinforcement schedule around grasp activities, ensuring motivation is maintained through correct behavioral principles. ABA data collection protocols track frequency, duration, and quality of grasp attempts across sessions.
Neurodevelopmental Pediatrics — Medical Context
NeuroDev pediatricians identify underlying conditions affecting grasp (hypotonia, coordination disorder, neurological differences) and ensure the material protocol is medically appropriate. They integrate grasp goals into the child's overall developmental plan.
"In our FusionModule™ approach, the OT designs the grasp protocol, the BCBA ensures it stays motivating and measurable, and the parent delivers it 5× per week at home. That convergence is why outcomes are different." — Pinnacle FusionModule™ Clinical Team
The Complete Object Grasping Material Kit
9 Evidence-Based Materials
Pinnacle Recommends
Each material targets a specific component of the grasp system. Used together, they address the full spectrum of grasp development. Total starter kit estimate: ₹2,200–9,600. Minimum viable kit: ₹700–2,000.
🟣 Material 1 — Therapy Putty
Resistive hand strengthening
Builds intrinsic hand muscles. Color-coded resistances: Extra-Soft → Extra-Firm.
₹300–1,200
Builds intrinsic hand muscles. Color-coded resistances: Extra-Soft → Extra-Firm.
₹300–1,200
🟣 Material 2 — Tongs & Tweezers
Pincer pattern training
Trains exact muscles and patterns for mature pincer grasp. Large tongs → craft tweezers progression.
₹150–800
Trains exact muscles and patterns for mature pincer grasp. Large tongs → craft tweezers progression.
₹150–800
🟣 Material 3 — Textured Sensory Balls
Sensory feedback enhancement
Stimulates tactile receptors, helping the brain calibrate grip force. Spiky, bumpy, ridged variations.
₹200–1,000
Stimulates tactile receptors, helping the brain calibrate grip force. Spiky, bumpy, ridged variations.
₹200–1,000
🟣 Material 4 — Pegboards & Pegs
Precise grasp practice
Require pincer or tripod grasp for each peg. High-repetition format builds both pattern and strength.
₹400–1,500
Require pincer or tripod grasp for each peg. High-repetition format builds both pattern and strength.
₹400–1,500
🟣 Material 5 — Finger Isolators
Independent finger control
Develops the ability to move individual fingers separately — prerequisite for mature tripod grasp.
₹300–1,500
Develops the ability to move individual fingers separately — prerequisite for mature tripod grasp.
₹300–1,500
🟣 Material 6 — Clothespins / Pinch Clips
Pinch strength builder
Spring resistance builds lateral pinch and 3-jaw chuck grasp. Zero-cost entry point for most families.
₹50–300
Spring resistance builds lateral pinch and 3-jaw chuck grasp. Zero-cost entry point for most families.
₹50–300
🟣 Material 7 — Lacing Cards & Threading
Sustained pincer endurance
Builds grasp endurance — maintaining pincer during extended activity — essential for writing and ADL tasks.
₹200–800
Builds grasp endurance — maintaining pincer during extended activity — essential for writing and ADL tasks.
₹200–800
🟣 Material 8 — Squeeze Bottles / Droppers
Graded pressure control
Develops tripod grip position and "just-right" force calibration. Immediate feedback: squeeze too hard = overflow.
₹100–500
Develops tripod grip position and "just-right" force calibration. Immediate feedback: squeeze too hard = overflow.
₹100–500
🟣 Material 9 — Weighted Utensils / Adapted Grips
Functional scaffold support
Allows participation in daily activities NOW while underlying skills develop. Includes pencil grips and built-up handles.
₹400–2,000
Allows participation in daily activities NOW while underlying skills develop. Includes pencil grips and built-up handles.
₹400–2,000
📞Clinical-grade products available through your Pinnacle center. Helpline: 9100 181 181

Material 1: Therapy Putty
Resistive Hand Strengthening
What It Does
Builds all 15 intrinsic hand muscles that power fine motor control. Color-coded resistances allow precise progression: Extra-Soft (for hypotonic hands) through Extra-Firm (for mastery-level challenge).
Core Exercises
- Full-hand squeeze → all fingers closing
- Pinch and pull → thumb + index, pull apart
- Finger pokes → each finger individually
- Roll into snake → cylindrical palm motion
- Find hidden objects → by feel
Correct Execution
Wrist neutral (not bent). Fingers actively pressing — not just palm contact. Both hands alternate if bilateral practice is intended.
Common Errors
- Using only palm with no finger involvement
- Bending wrist downward during use
- Holding with full fist without finger isolation
Progression Timeline
- Weeks 1–2: 3 min continuous squeeze
- Weeks 3–4: 5 min with 2 exercises
- Weeks 5–8: 8 min with 4 exercises
Safety
NOT edible — supervise children who mouth objects. Store in airtight container. Check for wheat/gluten allergy if using homemade version.
₹300–1,200 | DIY: Flour + salt + water + oil
Material 2: Tongs & Tweezers
Pincer Pattern Training
What It Does
Trains the exact muscles and movement patterns needed for mature pincer grasp. The tong mechanism forces the thumb and finger opposition pattern that is the foundation of all tool use.
Correct Grip Position
Thumb and fingers open the tong handles — NOT a full-fist squeeze. Index and middle finger on one handle, thumb on the other.
Progression
- Large kitchen tongs + pompoms/cotton balls
- Medium craft tongs + small erasers
- Tweezers + beads, dried pasta
Session Targets
- Weeks 1–2: 5 successful transfers
- Weeks 3–4: 10 transfers
- Weeks 5–8: 15–20 transfers, non-dominant hand added
Troubleshooting
If tong activities end in throwing objects: move to larger, softer targets (cotton balls). If still too challenging, return to clothespins to build pinch pattern first, then return to tongs.
Safety
Blunt-tip only. Supervise to prevent poking. Failed transfers are learning data — not failure.
₹150–800 | DIY: Kitchen tongs, salad servers, clothespins in pinch mode
Material 3: Textured Sensory Balls
Sensory Feedback Enhancement
What It Does
Stimulates tactile receptors in the fingertips, helping the brain calibrate grip force accurately. Spiky, bumpy, and ridged textures provide rich proprioceptive input that teaches the nervous system what "holding on" actually feels like.
Why Texture Matters
Children with poor sensory calibration can't regulate grip force because their brain doesn't receive adequate feedback. Textured surfaces amplify that feedback — essentially turning up the volume on the body's proprioceptive signals.
Types to Use
- Spiky massage balls — maximum tactile input
- Ridged rubber balls — moderate texture
- Bumpy foam balls — gentle introduction
- Smooth squeeze balls — least sensory input
For Sensory Avoiders
Start with smooth → bumpy → ridged → spiky over 2–4 weeks. Never force texture contact. Let the child lead initial exploration.
For Sensory Seekers
Use spikiest available. Deep-squeeze before precision activities.
₹200–1,000 | DIY: Pinecones, rough stones, balloon filled with rice

Material 4: Pegboards & Pegs
Precise Grasp Practice
What It Does
Every single peg requires a pincer or tripod grasp to pick up, transport, and place. The high-repetition, structured format builds both pattern and strength simultaneously — each peg is one therapeutic rep.
Correct Grasp
Pincer or 3-jaw chuck (thumb + index + middle). Peg held near the tip, not at the base. Insert with wrist neutral, arm extending forward — not sideways. Controlled placement, not throwing.
Progression
- Weeks 1–2: 5–10 pegs per session, large holes, thick pegs
- Weeks 3–4: Increase by 5 each week
- Weeks 5–8: Full board (20–25 pegs), smaller peg sizes, pattern-copying from cards
Advanced Variations
Add cognitive load: copy a color pattern from a card while placing pegs. Switch to non-dominant hand. Use small pegs and small holes. Time the completion for motivation.
Safety
Choking hazard. Use large-peg version for children under 3 or any child who mouths objects.
₹400–1,500 | DIY: Cardboard + golf tees, colander + straws, foam block + sticks

Material 5: Finger Isolators / Puppet Tools
Independent Finger Control
What It Does
Develops the ability to move individual fingers independently — a prerequisite for mature tripod grasp. Children who use "mass movement" (all fingers move together) cannot form the isolated thumb-index opposition required for precise tool use.
Why It's a Prerequisite
Mature grasp requires the thumb and index finger to act precisely while the ring and little fingers stabilize. Finger isolators teach this differentiation — making all other grasp work more effective.
How to Use
- Finger puppets: animate one finger at a time in storytelling play
- "Two-finger games": only thumb and index finger allowed to tap/play
- Piano keys: individual finger pressing in sequence
- Sticker placement: peel and place with single finger only
Troubleshooting
If child uses full-fist grip on everything, start here. Don't move to tongs or pegboard until some finger isolation is emerging.
₹300–1,500 | DIY: Toilet paper roll with holes, finger puppets from cloth scraps

Material 6: Clothespins / Pinch Clips
Pinch Strength Builder
What It Does
Spring resistance builds lateral pinch and 3-jaw chuck grasp simultaneously. The clothespin is one of the most efficient — and lowest-cost — fine motor therapy tools available. Most families already own them.
Correct Execution
Pinch at the spring end with the thumb pad opposing index finger pad. Use the pads, not the fingertips. Open and close 10× before attempting to clip to an object — this "pre-fatigue" approach builds endurance systematically.
Progression Targets
- Week 1–2: 10 clips per session
- Week 3–4: 20 clips per session
- Week 5–8: 30 clips + reverse unclipping for bilateral variation
Creative Variations
Clip to round containers, fabric, paper edges, card stock strips. Clip-chain building as art activity. Color-sorting clip games.
Why It's the Best Starter Material
Zero-cost entry point. Immediate visual feedback. Transferable to many contexts. Children often find clipping intrinsically satisfying.
₹50–300 — Standard wooden clothespins already in most homes

Material 7: Lacing Cards & Threading
Sustained Pincer Endurance
What It Does
Builds grasp endurance — the ability to maintain a functional pincer grasp during an extended activity. This is distinct from strength. A child may have emerging pincer pattern but fatigue after 30 seconds. Lacing builds the stamina needed for writing and self-care tasks that require sustained grip.
Progression
- Week 1–2: 3 holes per session
- Week 3–4: 5 holes per session
- Week 5–8: Full card, progress to shoe-lacing pattern
Advanced Variations
- Small beads on string — increases precision demand
- Button threading — prepares for dressing independence
- Full shoe-lacing — ADL integration at mastery level
Safety
Laces longer than 30cm are a strangulation risk. Always supervise. Store out of reach between sessions.
DIY Version
Cardboard + punched holes + shoelace. Pasta on string. Button threading with household buttons. These are clinically equivalent to purchased lacing cards.
₹200–800 | DIY: Cardboard + holes + shoelace

Material 8: Squeeze Bottles / Droppers
Graded Pressure Control
What It Does
Develops tripod grip position AND "just-right" force calibration simultaneously. The immediate feedback mechanism is uniquely powerful: squeeze too hard = overflow, squeeze too softly = nothing comes out. The child's hand learns calibration in real time.
Correct Position
Thumb, index, and middle finger grip the bottle body — forming a natural tripod. This position mirrors pencil grip directly, making squeeze bottles an excellent pre-writing preparation tool.
Progression
- Start: Large squeeze bottle with wide opening
- Progress: Eye dropper / turkey baster
- Advanced: Pipette-sized droppers for precise art activities
Motivating Activities
Dropper art (drop colors onto paper towel). Watering small plants. "Fill the ice cube tray" with dropper. These embed therapeutic practice in meaningful, motivating contexts.
Safety
Teach safe direction — spray away from eyes. Clean bottles between uses to prevent mold.
₹100–500 | DIY: Kitchen ketchup bottle, turkey baster, any squeeze bottle

Material 9: Weighted Utensils / Adapted Grips
Functional Scaffold Support
What It Does
This material is different from the previous eight: rather than building underlying skill in isolation, adapted grips and weighted utensils allow the child to participate in daily activities right now while the underlying strength and pattern develop. Function doesn't have to wait for mastery.
Types Available
- Pencil grips — triangular, oval, cushioned
- Built-up handle utensils — spoon, fork, toothbrush
- Weighted spoons and forks (OT-prescribed)
- Foam pipe insulation — DIY version for any handle
When to Use
Introduce adapted grips from Day 1 for mealtimes and pre-writing to reduce frustration and build participation. Do not wait until the child has "earned" them — they are therapeutic scaffolds, not rewards.
Important Note
Weighted utensils should be OT-prescribed for specific neurological reasons (tremor, proprioceptive seeking). Do not use weighted items without clinical guidance — incorrect weight can cause fatigue rather than benefit.
Phase Out Plan
As mastery develops (Week 6–8), begin gradually reducing adapted grip size toward standard. This is part of your OT's discharge plan.
₹400–2,000 | DIY: Foam pipe insulation wrapped around any handle

DIY & Zero-Cost Alternatives
WHO Equity Principle
₹0 Is a Valid Budget
Every family can start today. The therapeutic principle is in the activity, not the brand. A pinecone gripped correctly builds the same neural pathway as an ₹800 sensory ball. Every material in this kit has a household equivalent.
Material | Clinical-Grade (Buy) | Household Alternative (Make/Use) |
Therapy Putty | ₹300–1,200 | Homemade playdough (flour + salt + water + oil) or chapati dough during cooking |
Tongs & Tweezers | ₹150–800 | Kitchen tongs, salad servers, clothespins in pinching mode |
Sensory Balls | ₹200–1,000 | Pinecones, rough stones, textured sponge, balloon filled with rice |
Pegboards & Pegs | ₹400–1,500 | Cardboard + golf tees, colander + straws, foam block + sticks |
Finger Isolators | ₹300–1,500 | Toilet paper roll with holes, finger puppets from cloth scraps |
Clothespins | ₹50–300 | Standard wooden clothespins — this IS the DIY version |
Lacing Cards | ₹200–800 | Cardboard + punched holes + shoelace; pasta on string |
Squeeze Bottles | ₹100–500 | Kitchen ketchup/mustard bottle, turkey baster |
Adapted Grips | ₹400–2,000 | Foam pipe insulation wrapped around pencil/spoon handle |
WHO NCF Handbook (2022): Context-specific, equity-focused interventions. CCD Package in 54 LMICs confirms household-material intervention efficacy. PMC9978394

Safety First: Before You Begin
Read Before Every Session
Read this before every session. Without exception.
1
🔴 RED — DO NOT PROCEED
- Open wound, infection, or inflammation on hands/fingers
- Severe meltdown or extreme dysregulation episode currently occurring
- Physician-prescribed hand rest
- Unusual swelling, pain, or discoloration of hands
- Acute illness (fever, lethargy, unusual distress)
- Skin reaction, breathing difficulty, or allergic response to any material
2
🟡 AMBER — MODIFY AND PROCEED WITH CAUTION
- Child is tired or hungry → Shorten to 5 min, easiest materials only
- Difficult morning → Use preferred materials, skip resistance activities
- Sensory defensiveness today → Skip textured materials, use familiar putty only
- Previous session ended in frustration → Start with guaranteed success activity
3
🟢 GREEN — PROCEED NORMALLY
Child is: fed, rested, in a regulated state, no recent illness, no behavioral crisis in past 2 hours, hands are healthy and uninjured.

Set Up Your Space
Spatial precision prevents 80% of session failures. The environment is a therapeutic variable — treat it with the same care as the materials themselves.
Position Setup
- Child — 90°-90°-90° seated position (hips, knees, ankles all at right angles). Feet flat. Table at elbow height.
- Parent — Beside child (not across). Dominant hand side. Within arm's reach for physical guidance.
- Materials tray — To the side, not directly in front. Present one material at a time.
- Visual timer — Visible to child. Hourglass or digital, ≤15 min.
- Tracking sheet — Pre-filled with today's date and target behaviors.
Environment Settings
Factor | Recommendation |
Lighting | Bright, natural preferred. No flickering lights. |
Sound | Quiet. No TV/music during first 4 weeks. |
Temperature | 22–26°C. Warm hands before activities if cold. |
Surface | Non-slip table mat, wipeable surface. |
Distractions | Remove ALL screens from visual field. |
Duration | Set visual timer before starting. |
Pre-Session Heavy Work (2–3 min)
Wall push-ups, carrying books, pulling putty with both hands, or squeezing a stress ball. This proprioceptive "warm-up" primes the nervous system for fine motor work.
Is Your Child Ready? The Pre-Flight Checklist
📋 Protocol
60 Seconds. Every Time.
Run through this checklist before every session. The best session is the one that starts right. A 5-minute successful session is worth more than a 20-minute struggle.
# | Readiness Indicator | ✅ YES → Action | ❌ NO → Action |
1 | Child has eaten in past 2 hours | Proceed | Feed first (15-min wait) |
2 | Child slept reasonably | Proceed | Shorten to 5 min |
3 | No meltdown in past 90 minutes | Proceed | Wait for full regulation |
4 | Hands are healthy — no wounds, pain | Proceed | STOP — Do not proceed |
5 | Child shows awareness of environment | Proceed | Start with alerting activity |
6 | No escape behaviors pre-session | Proceed | Pre-session pairing first |
7 | No major schedule disruption today | Proceed | Use extra reinforcement |
✅ ALL YES
GREEN LIGHT. Proceed to Step 1: The Invitation.
⚠️ 1–2 NO
MODIFY. Shorten to 10 min, easiest materials, increase reinforcement density.
🛑 CRITICAL NO
POSTPONE. Today is not the day. Note: "Session postponed — [reason]."
Step 1: The Invitation
⏱️ 30–60 Seconds
Every Session Begins Here
Every session begins with an invitation, not a demand. This distinction is clinically significant — it determines whether the child's nervous system enters the session in an approach or avoidance state.
"Hey [child's name], look what I have! Want to see something cool? Come, let's play with the [material name] together."
Delivery Notes
- Voice: Warm, slightly excited — NOT pressured or urgent
- Body: Get to child's level (kneel or sit beside)
- Eye contact: Offer, don't demand
- Distance: Start 1–2 arm lengths away, material visible
✅ Acceptance Cues
- Looks at the material with curiosity
- Moves toward you or the material
- Points, reaches, or vocalizes interest
- Relaxed body posture
⚠️ Resistance Cues — Modify Now
- Turns body away
- Pushes material away
- Increases arousal (louder, faster movement)

Step 2: The Engagement
⏱️ 1–3 Minutes
The child is interested. Now deepen the connection — introduce the material. Model before you ask. One verbal instruction per action. Let curiosity lead.
For Therapy Putty
Place putty on table. Begin squeezing it yourself — exaggerate the action, be theatrical. "Look, I'm making it flat... and now I'm making a snake..." Let the child touch it first on their own terms.
For Tongs
Place objects (pompoms, cotton balls) in a bowl. Pick one up with tongs yourself. Say: "Can you pick up a blue one?" Only one demand — not five.
For Clothespins
Clip one to the edge of a container yourself. Hand child a clothespin. Don't instruct — let them discover the clip mechanism independently.
For All Materials
Present one material at a time. Model before asking. Use visual demonstration alongside verbal instruction. One verbal instruction per action.

Step 3: The Therapeutic Action
⏱️ 5–12 Minutes
The Active Ingredient
This is where hand strength and pattern are built. The following execution details ensure you are practicing the right movements — not just going through the motions.
Therapy Putty — Core Actions in Order of Difficulty
Full-hand squeeze → Pinch and pull → Finger pokes (each finger individually) → Roll into snake → Find hidden objects. Correct: Wrist neutral, fingers actively pressing, not just palm contact.
Tongs — Grip and Transfer
Thumb and fingers open the handles — NOT full-fist squeeze. Large objects (pompoms) → medium (erasers) → small (beads). Target: 3–5 successful transfers per session in Week 1.
Pegboard — Controlled Placement
Pincer or 3-jaw chuck grasp (thumb + index + middle). Peg held near tip. Insert with wrist neutral, arm extending forward. Target: 5–10 pegs per session in Weeks 1–2. Increase by 5 each week.
Clothespins — Pinch with Pre-Fatigue
Pinch at spring end with thumb pad opposing index finger pad — use pads, not tips. Open and close 10× before attempting to clip to an object. Target: 20 clips per session by Week 4.

Step 4: Repeat & Vary
⏱️ 3–5 Minutes
Therapeutic Dosage
3 excellent repetitions are worth more than 10 forced ones. Repetition without variation creates rote performance, not generalized skill. The brain needs the same neural demand in different packaging.
Material | Weeks 1–2 | Weeks 3–4 | Weeks 5–8 |
Therapy Putty | 3 min continuous | 5 min, 2 exercises | 8 min, 4 exercises |
Tongs | 5 transfers | 10 transfers | 15–20 transfers |
Pegboard | 5 pegs | 10 pegs | Full board (20–25) |
Clothespins | 10 clips | 20 clips | 30 clips + unclip |
Lacing | 3 holes | 5 holes | Full card |
Variation Principles
- Putty: Change shape/exercise — same muscles, different forms
- Tongs: Change object size/texture — same pattern, different challenge
- Pegboard: Add pattern-copying — same grasp, added cognitive load
- Clothespins: Change what they clip to — same pinch, functional variety
⚠️ Satiation Indicators — Stop When You See These
- Full-fist replaces precision grasp (quality degrading)
- Activity pace slows significantly
- Child begins seeking escape
- Material use becomes aimless
Rule: Quality > Quantity. When satiation appears, move to cool-down.

Step 5: Reinforce & Celebrate
⏱️ 30–60 Sec Per Moment
Timing Matters More Than Magnitude
Immediate, specific, enthusiastic reinforcement is the fuel that keeps the engine running. Flat delivery doesn't work for many children — your energy matters clinically.
🌟 Social Reinforcers
Specific verbal praise ("Beautiful finger squeeze!"), high-five, hug, celebratory dance, funny face. Free and highly effective for most children.
🏆 Token Economy
Sticker for each peg completed → 5 stickers = preferred activity. Token systems show strong evidence across multiple systematic reviews.
🎁 Tangible Reinforcers
10–15 seconds with preferred toy. Small edible with dietary guidance. Used strategically for high-effort activities.
🎮 Activity Reinforcers
2 minutes preferred screen time. Playtime with preferred material. Free-choice activity following session completion.
✅ Critical Principles
- Reinforce the attempt, not just the success
- Specific > Generic: "Amazing pinching!" beats "Good job!"
- Immediate — within 3 seconds of behavior
- Enthusiastic — flat delivery doesn't work
❌ Never Do This
Never withhold earned reinforcement. Never add conditions after the behavior has occurred. Never use reinforcement as punishment leverage — it destroys trust and destroys the protocol.

Capture the Data: Right Now
📈 Progress Tracking
60 seconds of data now saves hours of guessing later. Data is what separates a structured therapeutic protocol from casual play. It shows you progress you can't see in the moment, flags when to adjust, and accelerates your therapist's clinical decision-making.
📊 Session Duration
Minutes completed per session. Record actual time — not intended time. Trends in duration reveal engagement trajectory.
✅ Materials Used
Check which materials were used each session. Which three are producing the most progress for your specific child?
⭐ Quality Rating
1–5 scale per session. "3 — moderate engagement, some avoidance of tongs." Pattern of consistent 1/5 on a material = adjustment needed.
Optional Precision Tracking
- Number of successful repetitions per material
- Grasp pattern observed (palmar / pincer attempt / pincer achieved / tripod)
- Behavior rating (1 = distressed, 5 = highly engaged)
How This Data Helps
- Week 4 vs. Week 1 shows measurable progress
- Consistent low ratings flag material adjustments
- Consistent 5/5 signals readiness to progress
- Shared with therapist → accelerates decisions
📞Need help setting up tracking? Call 9100 181 181

What If It Didn't Go As Planned?
Session abandonment is not failure — it is data. Every challenging session tells you something clinically important about your child's sensory profile, current capacity, and what to adjust next time. Here are the 7 most common problems and their evidence-based fixes.
Problem 1: Child refused to touch therapy putty
Why: Tactile defensiveness — texture may be aversive.
Fix: Start with visual engagement only (watch parent squeeze). Try cloth gloves for first touch. Progress bare hands over days/weeks. Never force contact.
Fix: Start with visual engagement only (watch parent squeeze). Try cloth gloves for first touch. Progress bare hands over days/weeks. Never force contact.
Problem 2: Full-fist grip on everything, won't isolate fingers
Why: Immature synkinesis (mass movement) — a developmental stage, not resistance.
Fix: Use "two-finger games" — activities where only thumb and index finger are allowed. Gradually transfer isolation to materials.
Fix: Use "two-finger games" — activities where only thumb and index finger are allowed. Gradually transfer isolation to materials.
Problem 3: Grips so tightly material breaks or objects are crushed
Why: Poor force grading + possibly under-responsive proprioception.
Fix: Switch to squeezable sensory balls with visible shape-change feedback. Use soft objects to establish "light grip" concept. Praise explicitly when grip is appropriate.
Fix: Switch to squeezable sensory balls with visible shape-change feedback. Use soft objects to establish "light grip" concept. Praise explicitly when grip is appropriate.
Problem 4: Child loses interest within 2 minutes
Why: Material not motivating enough, or short attention window.
Fix: Embed material use into preferred activity. Increase reinforcement rate — praise every 30 seconds.
Fix: Embed material use into preferred activity. Increase reinforcement rate — praise every 30 seconds.
Problem 5: Tong activities always end in throwing objects
Why: Frustration from difficulty, or sensory seeking.
Fix: Move to larger, softer objects (cotton balls). Return to clothespins (easier pinch pattern) and rebuild up to tongs.
Fix: Move to larger, softer objects (cotton balls). Return to clothespins (easier pinch pattern) and rebuild up to tongs.
Problem 6: Child does fine at home but refuses at therapy center
Why: Generalization hasn't occurred yet.
Fix: Bring home materials to the center session. Familiarity of the material bridges the setting gap.
Fix: Bring home materials to the center session. Familiarity of the material bridges the setting gap.
Problem 7: No visible progress after 3 weeks
Why: May need clinical re-assessment. Possible wrong resistance level or grasp demand level.
Fix: Contact your Pinnacle OT — 9100 181 181. Describe the data from your tracking sheet.
Fix: Contact your Pinnacle OT — 9100 181 181. Describe the data from your tracking sheet.

Adapt & Personalize
No Two Children Are Identical
The protocol described in this guide is a starting framework — not a rigid script. Every child's sensory profile, attention window, diagnosis, and motivational landscape is unique. Calibrate accordingly.
EASIER Modifications
- Extra-soft putty or homemade playdough
- Very large tongs with large pompoms
- Large holes and thick pegs on pegboard
- Reduce session to 5–7 minutes
- Increase reinforcement rate (every 30 seconds)
- 5-minute heavy work warm-up before fine motor
HARDER Variations (Mastery Level)
- Putty: medium-firm resistance, complex multi-step exercises
- Tongs: small objects (dried pasta, beads), non-dominant hand
- Pegboard: small pegs, pattern-copying from cards
- Lacing: full shoe-lacing pattern, small beads
- Squeeze bottles: pipette-sized, precise dropper art
Age | Priority Materials | Session Length | Grasp Target |
0–2 yrs | Textured balls, soft putty, large pegs | 5–8 min | Emerging palmar/pincer |
2–4 yrs | Clothespins, tongs, threading | 8–12 min | Pincer → tripod |
4–8 yrs | Full protocol, adapted grips for writing/feeding | 10–20 min | Functional tripod + tool use |
Week 1–2: What to Expect
📈 Tolerance Phase
Progress: 15%
Progress at Week 1–2 looks different from what you expect — and that's exactly right. This is the hardest phase. Sessions may feel chaotic. You may feel like nothing is working. Track the data. It will show progress you can't see in the moment.
✅ What You WILL See — These ARE Progress
- Child tolerates material being on the table without leaving
- Child touches material briefly (even just once per session)
- Slightly longer engagement duration than first session
- Less resistance to starting sessions (familiarity building)
- Any voluntary grasp attempt, even clumsy
❌ What You Will NOT See Yet — And That's Normal
- Strong, consistent pincer grasp
- Ability to use materials "correctly" by adult standards
- Carryover to daily activities (this comes later)
- Verbal requests to do the activity
"If your child tolerates the material for 3 seconds longer than last week — that is real, measurable progress." Neural pathway formation is invisible. The tolerance and approach behaviors you're measuring now are the precursors to strength and coordination you'll see in weeks 5–8.
Recommended frequency: 3–4 sessions per week in Weeks 1–2. Consistency > intensity. PMC11506176 — SI intervention outcomes emerge across 8–12 week timelines.
Week 3–4: Consolidation Signs
📈 Consolidation Phase
Progress: 40%
The neural pathways are forming. By Week 3–4, the brain has received enough structured repetition to begin automating grasp patterns. Look carefully for these signs — they are highly significant to therapists even when they seem small to parents.
1
Child anticipates the session
Looks for materials, brings them out independently. This is motivation emerging — a major behavioral milestone.
2
Engagement duration increases
Measure from your tracking sheet — even 2 minutes longer than Week 1 is clinically meaningful.
3
Reduced prompting needed
Child requires fewer verbal or physical cues to start or continue activities. Internal motivation is forming.
4
Attempts correct grasp pattern
Even imperfect pincer attempts — the pattern is emerging. The brain is reorganizing.
5
Reduced frustration
Emotional regulation during activities is improving. Fewer session-ending distress responses.
6
Spontaneous use outside sessions
Any voluntary use of a grasp material outside of structured time — powerful generalization signal.

Week 5–8: Mastery Indicators
📈 Mastery Phase
Progress: 75%+
Mastery is not perfection. It is functional independence. The goal was never a perfect laboratory grip — it was hands that work in the real world, at mealtimes, at school, during play.
Skill Component | Mastery Indicator |
Intrinsic strength | Squeezes medium-resistance putty for 3 minutes without fatigue |
Pincer pattern | Consistently uses thumb + index finger for objects ≥ 1cm |
Force grading | Holds soft object without crushing AND heavier object without dropping |
Endurance | Maintains functional grasp for full 15-minute functional task |
Generalization | Grasp pattern appears in at least 2 new contexts (mealtime, play, school) |
🎯 Generalization in Real Life
Uses spoon/fork with functional grip at mealtimes. Holds crayon/pencil in tripod or near-tripod position. Manages simple fasteners (buttons, zippers). Carries and transports objects without dropping.
🔄 Maintenance Check
Remove structured protocol for 1 week. Does the skill maintain? If yes: true mastery achieved. If regression occurs: continue structured sessions and add generalization practice.
➡️ Next Level
F-592 (Postural Control), F-597 (Hand-Eye Coordination), or F-600 (Block Stacking) depending on your child's profile. Your OT will guide sequencing.

Celebrate This Win
🏆 8 Weeks. You Did This.
You did this. Your child grew because of your commitment.
Your child arrived at this technique fumbling — objects slipping, fingers not listening, frustration building. You spent weeks setting up sessions, managing resistance, tracking data, adjusting approaches, celebrating small wins.
And now, those hands work differently. They grip with intention. They hold with strength. They pick up small objects with fingers, not fists. They can eat more independently. They can hold a crayon like they mean it.
📸 Document the Milestone
Take a photo of your child's hands holding something proudly. This moment deserves to be remembered.
📖 Journal It
Write in their development journal: "Week [X]: Mastered Object Grasping — F-591." These records matter.
🎉 Celebrate Together
Have the child's favorite meal. Mark the completion as a family event. The child earned this celebration.
🔔 Share Your Win
Share this milestone with your Pinnacle therapist. Your journey inspires families just starting theirs. Share with the Pinnacle Community →

Red Flags: When to Pause
⚠️ Trust Your Instincts
Even in the success zone — even after weeks of progress — some signals require you to stop and consult your Pinnacle therapist before continuing.
🔴 Red Flag 1 — Regression Without Explanation
After weeks of progress, sudden significant deterioration in grasp quality or session tolerance. Possible: underlying medical change, neurological event, significant environmental stressor. Action: Note date, circumstances, contact therapist.
🔴 Red Flag 2 — Consistent Hand Pain During Activities
Child pulling hand away, protecting hands, or showing pain behaviors specifically during grasp activities. Action: Stop all materials. Medical evaluation before resuming any protocol.
🔴 Red Flag 3 — Plateau for 4+ Consecutive Weeks
Implemented harder variations, increased frequency, and still zero measurable progress. Clinical re-evaluation needed. Possible: change in diagnosis, need for additional modality. Action: Call 9100 181 181.
🔴 Red Flag 4 — Sensory Response Worsening
Child becoming MORE distressed by materials over time, not less. Sensory integration may need a deeper clinical approach beyond home protocol. Action: Teleconsult with Pinnacle OT.
🔴 Red Flag 5 — Increasing Emotional Dysregulation
Sessions consistently ending in meltdowns despite adjustments. Possible anxiety around performance failure. ABA/behavioral intervention may be needed before resuming motor focus.
1
Self-Resolve
Try troubleshooting modifications from the previous section. Document what you tried.
2
Teleconsult
Call 9100 181 181 for phone or video guidance. Free for all Pinnacle families.
3
Center Visit
Book an OT evaluation at your nearest Pinnacle center. Find Your Nearest Center →

Related Techniques in This Domain
You already own materials for several of these techniques. Fine Motor & Hand Function is a complete domain — F-591 gives you strong foundations across the full series.

F-590 — Physical Therapy at Home

F-592 — Postural Control
Core stability for hand function. Core Level. Materials you own: ✅ Therapy putty used in warm-up
View Technique →
View Technique →
F-595 — Bilateral Coordination

F-597 — Hand-Eye Coordination

F-600 — Block Stacking
Controlled release and placement. Core Level. Materials you own: ✅ Blocks (household)
View Technique →
View Technique →

F-602 — Pre-Writing Development
Grasp → pencil skill translation. Advanced Level. Materials you own: ✅ Adapted grips, squeeze bottles
View Technique →
View Technique →
Families Who've Been Here
🤝 Community
From the Pinnacle Clinical Archive
Illustrative cases drawn from Pinnacle center clinical data. Names changed. Outcomes are individual and vary by child profile and intervention consistency.
Family A | Hyderabad Center
Before (Week 1): 4-year-old boy with ASD. Full-fist pencil grip, unable to pick up small objects with fingers, inconsistent spoon use. Refused touching putty due to tactile sensitivity. Sessions lasted under 3 minutes.
Protocol: Visual-only putty observation for 2 weeks. Clothespins Week 3. Large tongs Week 5.
After (Week 10): Consistent inferior pincer grasp. Able to thread 5 beads. Spoon use 80% accurate.
Protocol: Visual-only putty observation for 2 weeks. Clothespins Week 3. Large tongs Week 5.
After (Week 10): Consistent inferior pincer grasp. Able to thread 5 beads. Spoon use 80% accurate.
"My son picked up a grain of rice to show me he could. I cried." — Mother
Family B | Bengaluru Center (Remote Protocol)
Before (Week 1): 6-year-old girl with developmental coordination disorder. Good motivation but poor strength — therapy putty too hard. Tongs resulted in throwing. Writing avoidance.
Protocol: Homemade playdough for 3 weeks. Medium-resistance putty Week 4. Clothespins as chain-building game.
After (Week 8): Tripod grasp emerging. Writes name with decreasing prompting. Fork use correct 70% of meals.
Protocol: Homemade playdough for 3 weeks. Medium-resistance putty Week 4. Clothespins as chain-building game.
After (Week 8): Tripod grasp emerging. Writes name with decreasing prompting. Fork use correct 70% of meals.
"We started with playdough we made in the kitchen. I didn't believe these simple materials could change her handwriting. They did." — Father
Family C | Visakhapatnam Center
Before (Week 1): 3-year-old with hypotonia. Palmar grasp dominant where pincer should be established. Play limited to pushing large objects, no manipulation.
Protocol: Full protocol with extra-soft putty. Heavy work warm-up before every session. Sensory ball exploration daily.
After (Week 12): Emerging pincer on small food items. Self-feeding with spoon 60% of meals.
Protocol: Full protocol with extra-soft putty. Heavy work warm-up before every session. Sensory ball exploration daily.
After (Week 12): Emerging pincer on small food items. Self-feeding with spoon 60% of meals.
"He picked up a tiny bead with two fingers. In that moment, I saw his future differently." — Mother

Connect With Other Parents
Isolation is the enemy of adherence. When you're the only one in your household running these sessions, the weight is real. Joining a community of parents doing the same work multiplies your motivation, your problem-solving, and your confidence.
WhatsApp Community
Parents working on F-591 and related fine motor techniques share daily wins, ask questions, and support each other. 10,000+ active Pinnacle families.
Join the Fine Motor Parent Community →
Join the Fine Motor Parent Community →
Pinnacle Parent Forums
Moderated online discussion boards organized by technique domain. Search "Fine Motor / F-591" for this technique's dedicated thread.
Access Forums →
Access Forums →
Local Parent Meetups
70+ Pinnacle centers host monthly parent meetups. Connect with families in your city working on similar goals.
Find a Meetup Near You →
Find a Meetup Near You →
Peer Mentor Programme
Connect with a parent who has already completed F-591 and the full fine motor sequence. Real-world guidance from someone who has walked this exact path.
Request a Peer Mentor →
Request a Peer Mentor →
"I found another mother in the WhatsApp group whose son had the same tong-throwing problem. She figured out that cotton balls instead of beads made all the difference. That one tip saved us two weeks of frustration." — Parent, Pinnacle Network
Your experience helps others. Consider sharing your F-591 journey once you complete the 8-week protocol. Share My Story →
Your Professional Support Team
Home + Clinic = Maximum Impact. The most effective intervention combines consistent parent-delivered home sessions with periodic clinical oversight and adjustment. You don't have to navigate this alone.
🏥 In-Clinic OT Sessions
70+ Pinnacle centers with certified Occupational Therapists specializing in fine motor and hand function. For F-591: OT evaluates current grasp pattern, prescribes precise putty resistance, designs your personalized home program.
Book OT Session →
Book OT Session →
📱 Teleconsultation
For families outside major cities or with scheduling constraints — video consultation with a Pinnacle OT for home program design and review. Available 9AM–6PM Mon–Sat. Response within 24 hours for urgent cases.
Book Teleconsult →
Book Teleconsult →
📞 FREE Helpline — 9100 181 181
16+ languages. 24×7. No appointment needed. For any question about F-591 or any other technique — call and speak with a trained advisor immediately. Free for all families across India.
WHO NCF Progress Report (2023): 48% increase in countries adopting ECD policies. Primary health care identified as key platform for reaching all families.
The Research Library
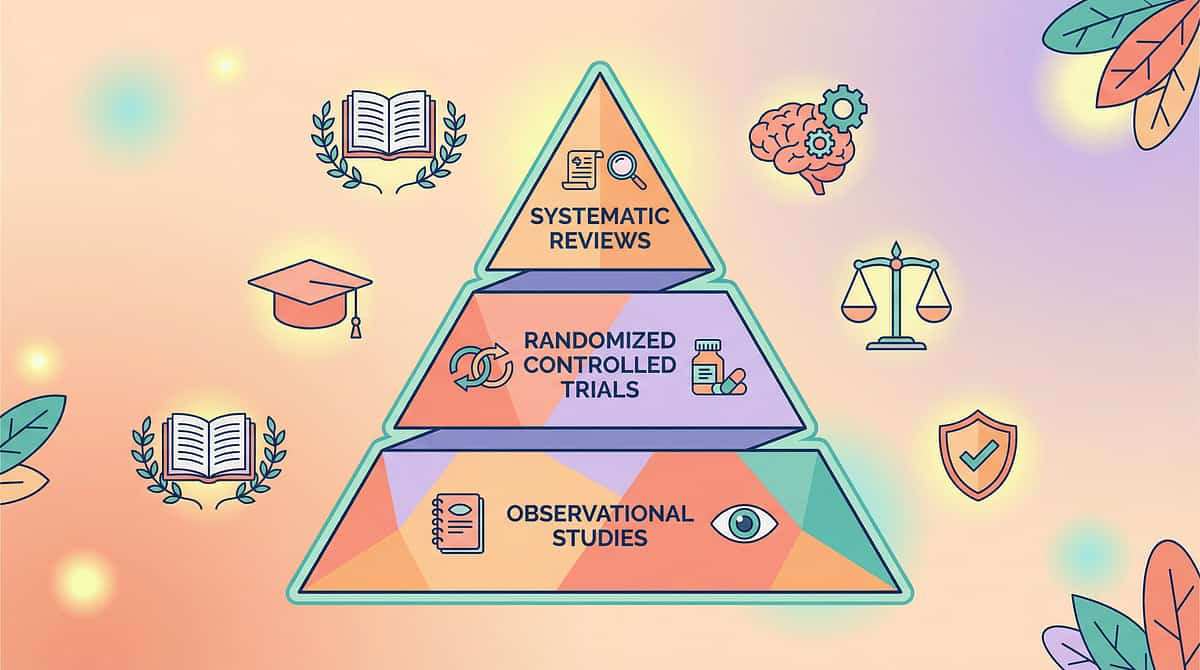
Evidence Grade I–II
Deeper Reading for the Curious
Deeper reading for the curious parent and the thorough clinician. Every claim in this guide is anchored in peer-reviewed research. Evidence grading follows Oxford Centre for Evidence-Based Medicine (OCEBM) levels.
📚 [1] PRISMA Systematic Review — Children, 2024
16 articles (2013–2023) confirm sensory integration intervention is evidence-based practice for children with ASD. Includes fine motor and hand function outcomes. Strongest level of evidence available.
PMC11506176 →
PMC11506176 →
📚 [2] Meta-Analysis — World J Clin Cases, 2024
24 studies. Sensory integration therapy effectively promotes fine motor skills, adaptive behavior, sensory processing. Effect sizes reported.
PMC10955541 → | DOI: 10.12998/wjcc.v12.i7.1260
PMC10955541 → | DOI: 10.12998/wjcc.v12.i7.1260
📚 [3] Indian RCT — Indian Journal of Pediatrics, 2019
Padmanabha et al. Home-based sensory and motor interventions: significant outcomes in Indian pediatric population. First major Indian-context validation of parent-administered protocols.
DOI: 10.1007/s12098-018-2747-4 →
DOI: 10.1007/s12098-018-2747-4 →
📚 [4] WHO Care for Child Development Package, 2023
Household-material early intervention across 54 LMICs. Fine motor stimulation as core component. Population-level evidence confirming parent-delivered efficacy.
PMC9978394 →
PMC9978394 →
📚 [5] NCAEP Evidence-Based Practices Report, 2020
National Clearinghouse on Autism Evidence and Practice. Classifies fine motor intervention, video modeling, and structured material-based practice as evidence-based for autism and developmental delays.
NCAEP 2020 Report →
NCAEP 2020 Report →
Additional References: WHO Nurturing Care Framework (2018): nurturing-care.org | Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660 | BACB Guidelines for Reinforcement in Behavioral Intervention
Preview of 9 materials that help with object grasping Therapy Material
Below is a visual preview of 9 materials that help with object grasping therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Pinnacle Promise
From Fear to Mastery
One Technique at a Time
Pinnacle Blooms Network® is India's largest multi-disciplinary pediatric therapy consortium — operating 70+ centers, delivering 20M+ exclusive 1:1 therapy sessions, achieving 97%+ measured improvement across Fine Motor Readiness, Hand Function Readiness, Self-Care Readiness, Pre-Academic Skills, and Daily Living Readiness indexes.
Powered by GPT-OS® (Global Pediatric Therapeutic Operating System) — the world's only end-to-end operating system governing pediatric therapy diagnosis, prognosis, design, execution, measurement, and readiness outcomes at population scale.
Contact
Statutory Identifiers
- CIN: U74999TG2016PTC113063
- DPIIT: DIPP8651 (Govt. of India)
- MSME: Udyog Aadhaar TS20F0009606
- GSTIN: 36AAGCB9722P1Z2
Proprietary Systems
GPT-OS® | AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ are proprietary systems of Pinnacle Blooms Network®.
© 2025–2026 Pinnacle Blooms Network® — Unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.