
9 Materials That Help With Nonverbal Toilet Training
When words aren't available — but independence is still the goal.
You are not failing. Your child's communication system is built differently — and so must the training system. This is not a toilet training problem. It is a communication infrastructure problem — with precise, proven solutions.
Pinnacle Blooms Consortium®
OT • SLP • ABA • SpEd • NeuroDev
Evidence-Based • Home-Executable
Self-Care & Daily Living Skills — Episode 493 | Age Band: 3–15 years

ACT I — EMOTIONAL ENTRY
You Are Among Millions of Families Navigating This Exact Challenge
An estimated 18 million children in India live with developmental conditions affecting communication and self-care skills. Non-verbal or minimally verbal children face the sharpest gap between capability and independence — not because independence is impossible, but because standard training methods were never designed for them.
1 in 36
Children with ASD
Children globally diagnosed with autism spectrum disorder
80%
Toileting Challenges
Of autistic children experience significant toileting challenges, including delayed training
65–85%
Achieve Independence
Of nonverbal children achieve toileting independence with the right visual communication system
Sources: CDC Autism Prevalence Report, 2023 | Dalrymple & Ruble, Journal of Autism, 2012 | Pinnacle Clinical Outcomes, 20M+ sessions
"No words" does not mean "no way." It means the pathway must be built differently — visually, structurally, consistently. Across Pinnacle's 70+ centers and 70+ countries served, nonverbal toilet training is among the top 5 most-requested therapeutic guidance areas from families.

ACT I — THE NEUROSCIENCE
Why Standard Toilet Training Doesn't Work — and What Does
What Verbal Children Do Automatically
Their brain receives the signal "bladder is full," converts it into the word "potty," and produces speech. Adults respond. Training completes.
Three Neurological Differences
- Interoceptive processing difference: The internal signal from a full bladder may be perceived weakly, inconsistently, or not at all.
- Language production difference: Even if the sensation is perceived, the pathway from sensation → word → speech may be interrupted or absent.
- Sensory processing difference: Hard surfaces, cold temperatures, echoing flush sounds, and bright lights may trigger the nervous system's threat response.
The GPT-OS® Insight
These are not behavior problems. They are neurological infrastructure gaps. The solution is not repetition of the same verbal method — it is building visual communication infrastructure that bypasses the verbal pathway entirely.
THIS IS A WIRING DIFFERENCE. NOT A BEHAVIOR CHOICE. NOT A PARENTING FAILURE.
Research: Frontiers in Integrative Neuroscience (2020). DOI: 10.3389/fnint.2020.556660 | Mahler (2017), Interoception Curriculum

ACT I — DEVELOPMENTAL CONTEXT
Your Child Is Here. Here Is Where We Are Heading.
Age 18M
Bladder awareness begins
Age 2Y
Awareness of sensation begins
Age 3Y
Verbal daytime training begins (typical)
Age 4–5Y
Night dryness begins (typical)
Age 6Y+
Independence (typical) — Your child's journey starts here, regardless of chronological age
WHO and UNICEF developmental frameworks recognize that communication modality does not determine developmental ceiling. A nonverbal child aged 8 can achieve full toileting independence — the timeline is extended, not foreclosed.
What Commonly Co-Occurs
- Sensory processing differences (tactile, auditory, proprioceptive)
- Reduced interoceptive awareness
- AAC needs (alternative/augmentative communication)
- Executive function differences (sequencing, initiation, inhibition)
- Anxiety related to unfamiliar environments
GPT-OS® Readiness Progression
Complete Dependence
Emerging Awareness
Developing Visual Communication
Mastery Independence
ACT I — EVIDENCE GRADE
Clinically Validated. Home-Applicable. Consortium-Proven.
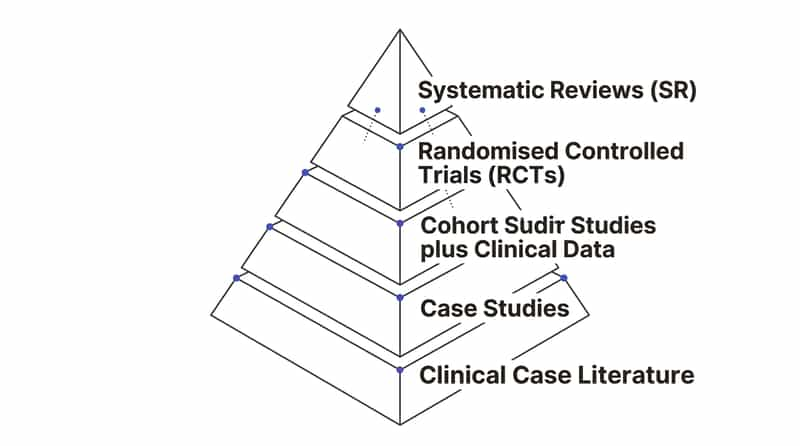
EVIDENCE GRADE: LEVEL I–II
Systematic Reviews + RCTs
20M+ Real-World Sessions
Study | Finding | Reference | |
NCAEP EBP Report (2020) | Visual supports classified as EBP for autism across self-care domains including toileting | NCAEP 2020 | |
Journal of Applied Behavior Analysis | Graduated training with visual communication achieves toileting independence in nonverbal children | JABA multiple studies | |
Dalrymple & Ruble (2012) | Structured visual protocols achieve independence in 65–85% of nonverbal/minimally verbal children | J Autism Dev Disord | |
Padmanabha et al. (2019) | Home-based structured visual interventions: significant outcomes in Indian pediatric population | Indian J Pediatr DOI: 10.1007/s12098-018-2747-4 | |
Pinnacle Clinical Outcomes | 97%+ measured improvement across self-care readiness indices via GPT-OS® protocol | 20M+ sessions, 70+ centers |
Visual communication systems and structured environmental supports eliminate the speech requirement from toilet training — enabling full independence across the same developmental trajectory as verbal training, with extended timelines and consistent implementation.
📞 For structured guidance tailored to your child: FREE Helpline 9100 181 181
ACT II — KNOWLEDGE TRANSFER
AAC-Supported Visual Communication Toilet Training System (E-493)
"Building the Bathroom Communication Bridge"
A structured, multi-material intervention system that replaces verbal communication requirements in toilet training with a purpose-built visual communication infrastructure. Rather than teaching the child to say "I need to go potty," this system teaches the child to use a visual toilet card, gesture, or AAC symbol to signal their need — while simultaneously building interoceptive body awareness, environmental sensory tolerance, and routine predictability through visual schedules.
Key Principle: Standard toilet training communicates through language. This system communicates through vision, structure, and consistent environmental cues. The learning target is identical — independence. The pathway is architecturally different.
Domain
Self-Care & Daily Living | AAC-Supported Communication | Sensory Processing
Age Range
3–15 years
Frequency
Every bathroom visit throughout the day
Lead Disciplines
OT • SLP • ABA/BCBA
ACT II — THE DISCIPLINES
How Each Discipline Contributes to This System
🟠 Occupational Therapy (Lead)
Primary Driver: Self-care skills, sensory environment adaptation, interoception development
The OT assesses the child's sensory profile, designs the sensory-adapted toilet setup, and develops the interoception building program. The OT ensures physical and sensory conditions are in place before any behavioral training begins.
🔵 Speech-Language Pathology (Co-Lead)
AAC system design, communication vocabulary programming, functional communication training
The SLP selects and programs the child's AAC system for toileting vocabulary — from a single toilet card to a robust multi-symbol system including: toilet, help, done, hurt, wet, dry, wash hands.
🟢 ABA / BCBA (Behavioral Architecture)
Protocol design, reinforcement schedules, data collection, generalization programming
The BCBA designs the graduated training protocol — schedule intervals, prompt hierarchy, reinforcement selection, and data collection. The BCBA ensures the communication card is treated as a functional communication response (FCR).
🟣 Special Education (Routine Integration)
Visual schedule design, school generalization, IEP toileting goals
The Special Educator ensures the visual system is replicated in the school environment with consistent materials, schedules, and caregiver training. Toileting goals are written into the IEP with measurable criteria.
"This technique crosses therapy boundaries because the child doesn't experience self-care as OT, communication as SLP, and behavior as ABA. They experience one bathroom routine. The Pinnacle FusionModule™ converges all four disciplines into a single coordinated protocol." — Pinnacle Consortium

ACT II — PRECISION TARGETS
Precision Targets: What This System Actually Builds
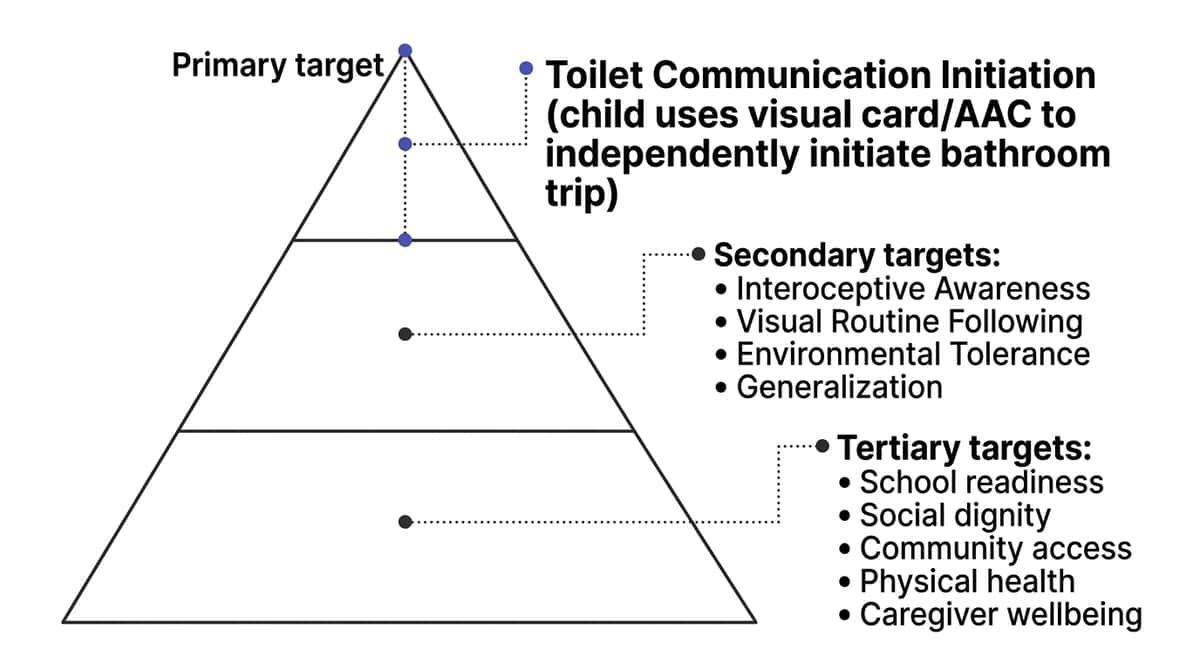
Primary Target
Functional Communication for Toileting Needs: Child uses a visual card, AAC symbol, or gesture to independently initiate a bathroom trip — not just comply when taken.
Observable indicator: Child reaches for toilet card / activates AAC symbol / leads adult to bathroom without being prompted.
Secondary Targets
- Interoceptive Awareness: perceive full-bladder signals
- Visual Routine Following: decreasing prompts over time
- Environmental Tolerance: bathroom without distress
- Generalization: home → school → community
Tertiary Targets (Long-term)
- School placement in general education programs
- Social participation in community settings
- Physical health (UTI prevention, constipation management)
- Caregiver wellbeing and reduced burden
ACT II — THE 9 MATERIALS
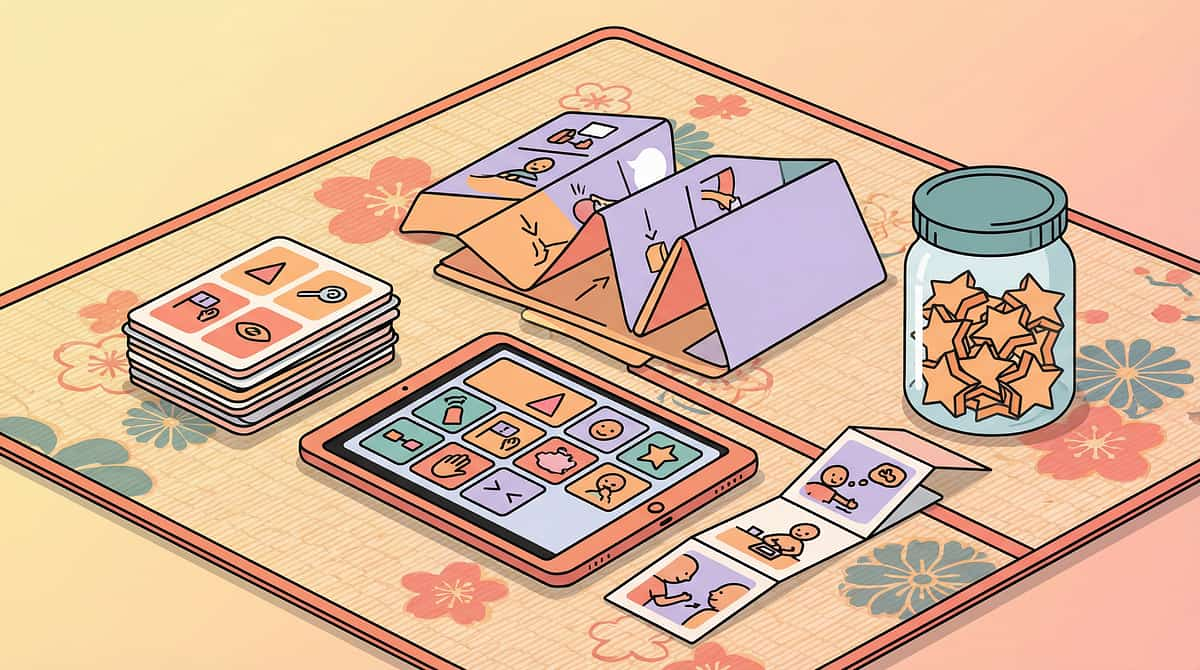
9 Materials. One System. All Available Today.
These 9 materials form an integrated system. Each addresses a different gap in the nonverbal toilet training infrastructure. Together, they create a complete visual-communication-based toilet training environment.

M1 — Visual Toilet Communication Cards
A laminated card with a clear toilet image — the child's voice for bathroom needs. Presented to any adult = immediate bathroom trip.
Price: ₹100–500 | DIY: ₹0 (photograph + laminate)

M2 — Visual Sequence Strip
A strip showing each bathroom step in order — pants down → sit → try → wipe → flush → wash → done. Posted at child's eye level.
Price: ₹150–600 | DIY: ₹0 (print + laminate)

M3 — Visual Timer
Shows time passing concretely — the child sees bathroom time approaching. Eliminates verbal warnings. Time Timer or sand timer.
Price: ₹300–1,500

M4 — Interoception Body Awareness Kit
Body maps, empty/full scales, belly-check activities. Teaches children to notice their own internal signals — the foundational layer for self-initiated toileting.
Price: ₹200–800 | DIY: ₹0 (body outline + scale printout)

M5 — Portable Visual Supports Kit
A travel pouch with mini duplicates of all communication and routine materials — for school, grandparents, community, and public bathrooms.
Price: ₹300–1,000

M6 — Sensory-Adapted Toilet Equipment
Padded toilet seat, step stool for foot grounding, quiet-close seat, dimmer switch. Makes the bathroom neurologically tolerable.
Price: ₹500–3,000

M7 — Visual Reinforcement System (Token Board)
Token board + tokens + progress chart. Concrete, immediate, visual reinforcement that works when verbal praise doesn't land. Pinnacle Recommends: The Rosette Imprint Reward Jar — ₹589 | 1800+ Reward Stickers — ₹364

M8 — Toilet Training Social Story
A personalized picture book about YOUR child's bathroom routine. Reviewed before bathroom trips to build familiarity and reduce anxiety.
Price: ₹200–800 | DIY: ₹0 (phone photos + print)

M9 — AAC Device / App with Toileting Vocabulary
The full communication system — toilet, now, later, done, help, hurt, wet, dry, wash hands. From low-tech picture board to high-tech device.
Price: ₹500–50,000
Starter Kit Minimum (₹0 budget possible): Visual toilet card + Sequence strip + Timer app (free) + Token board (handmade) | Comprehensive System: ₹2,450–58,600 | 📞 Ask our therapists: 9100 181 181

ACT II — DIY OPTIONS
Every Family Can Start Today — Regardless of Budget
WHO/UNICEF Equity Principle: Zero-Cost Options for Every Material
Material | Buy | Make (₹0) | |
Toilet Card | Printed symbol card, ₹100–300 | Photograph your actual toilet → print → laminate with tape | |
Sequence Strip | Pre-made bathroom strip, ₹200–500 | Photograph each step in YOUR bathroom → print → tape to wall | |
Visual Timer | Time Timer, ₹800–1,500 | Download "Time Timer" free app on any phone | |
Body Map | Printed body outline kit, ₹200 | Draw a simple body outline on A4 paper → mark belly area | |
Token Board | Printed token system, ₹200 | Draw 5 boxes on card → use any small stickers as tokens | |
Social Story | Printed story book, ₹300–600 | Phone photos → WhatsApp print service → bind with clips | |
Portable Kit | Dedicated therapy pouch, ₹300–500 | Any zip-lock bag or small zippered pencil case | |
Sensory Seat | Padded seat, ₹500–1,500 | Fold a soft towel over existing seat; non-slip bath mat for feet | |
AAC Vocabulary | Printed PECS board, ₹500–1,000 | Print toilet + done + help symbols from Boardmaker free symbols online |
Why Substitutes Work
The therapeutic principle is visual communication and environmental consistency — not the brand of the material. A toilet card made from a phone photograph of your own toilet is MORE concrete and recognizable than a commercial symbol. A sand timer from any stationery shop fulfills the same neurological function as a branded Time Timer.
When Clinical-Grade Is Non-Negotiable
If the child has significant sensory sensitivities, a professional-grade padded seat and quiet-close hardware may be essential — not optional. Consult the Pinnacle OT team: 9100 181 181

ACT II — SAFETY GATE
Read This Before You Start — Clinical Safety Gate
🔴 RED: DO NOT PROCEED IF:
- Child shows signs of illness, fever, GI distress, or urinary discomfort — rule out UTI or constipation first
- Child is in active emotional dysregulation or post-meltdown state
- Bathroom environment has not been assessed for sensory barriers
- No consistent communication system has been established yet
🟡 AMBER: MODIFY IF:
- Child shows mild resistance to bathroom (start with 30-second exposure, no demands)
- New bathroom environment (carry portable kit; first visit is orientation only)
- High-stress day for the family (shortened session; skip data tracking)
- Child recently had an accident (neutral response only — no verbal correction)
🟢 GREEN: PROCEED WHEN:
- Child is calm, fed, and in a regulated state
- Communication card/AAC is accessible and with the child
- Visual sequence strip is mounted and visible in bathroom
- Timer is set for scheduled bathroom interval
- Reinforcement materials are ready and immediately accessible
🔴 RED LINE — STOP IMMEDIATELY IF: Child shows severe distress (screaming, self-injury, extreme avoidance) | Signs of physical discomfort: holding genitals, crying while urinating, blood in urine/stool | Sudden regression after previous progress (rule out medical cause first) 📞 If you see these signs, call: 9100 181 181 (FREE, 24×7)

ACT II — ENVIRONMENT SETUP
The Bathroom as a Therapeutic Environment — Setup Protocol
Sequence Strip
Mounted at child's eye level, vertically, from toilet to sink. This is the child's script for the entire routine.
Toilet Setup
Seat reducer or padded seat fitted. Step stool positioned so feet rest completely flat — critical for stability and sensory grounding.
Timer Position
Visible from toilet position at child's seated eye line. Child should see time passing without turning their head.
Reinforcement Board
Placed on nearby surface, tokens ready, visible but not distracting. The promise of reward should be visible from the toilet.
Toilet Card Location
On child's person (lanyard, belt clip, or pocket) AND one duplicate near bathroom door at all times.
Sensory Adjustments
Lighting dimmed to child's preference. Quiet-close seat if possible. White noise app if echoing is an issue. Bathroom pre-warmed in cold months.
Remove from space: Excessive visual clutter, strong-smelling cleaning products during sessions, other children or pets during initial training phase. Parent position: Beside, not in front. Never looming.

ACT III — EXECUTION
Pre-Session Readiness: 60-Second Assessment Before Every Bathroom Trip
The best session is one that starts right. A bathroom trip that ends well with no elimination is worth more than a forced trip that ends in distress.
✅ GREEN: All 5 Needed → PROCEED
- Child is in a calm, regulated state
- Child has had sufficient fluid intake in past 60–90 minutes
- Communication card/AAC is accessible and with the child
- Timer has reached interval OR child has shown a physical signal
- Space is set up per the environment protocol
🟡 3–4 Green → MODIFY
Still take child to bathroom but only ask them to sit for 30 seconds with no elimination demand. Maintain routine. Reinforce participation regardless of outcome.
🔴 Less than 3 → POSTPONE
Do a preferred calming activity — vestibular input, proprioceptive input, preferred toy — for 5–10 minutes, then attempt again when child is regulated.
"THE BEST SESSION IS ONE THAT STARTS RIGHT. A BATHROOM TRIP THAT ENDS WELL WITH NO ELIMINATION IS WORTH MORE THAN A FORCED TRIP THAT ENDS IN DISTRESS." — Pinnacle OT Consortium
STEP 1 OF 6 ●○○○○○
Step 1: The Invitation — Bring the Child Into the Routine
The Exact Script
"Bathroom time." Hold up the toilet card or activate AAC toilet symbol simultaneously. Show, don't ask.
❌ NOT: "Do you need to go potty?" (question the child cannot answer)
❌ NOT: "Do you want to go?" (choice framing before routine is established)
✅ YES: "Bathroom time." + visual card + immediate movement toward bathroom
Body Language
- Stand beside, not in front of the child
- Move toward the bathroom naturally after showing the card — lead, don't push
- Keep your own affect calm and neutral (not overly animated, not tense)
What Acceptance Looks Like
- Child moves toward bathroom with or after you
- Child reaches for the toilet card themselves
- Child activates AAC symbol independently
- Child makes any orienting movement toward the bathroom
What Resistance Looks Like
Child moves away, sits down, or ignores. Response: Neutral. "Bathroom time." + visual once more. If continued resistance → postpone. Timing: 15–30 seconds only. This is a transition cue, not a negotiation.

STEP 2 OF 6 ●●○○○○
Step 2: Engagement — Child Is in the Bathroom, Building the Routine
Direct Attention to Sequence Strip
Point to step 1 (pants down). No verbal instruction needed — point only. The strip is the instruction.
Prompt Pants Management
Full physical prompt (hand-over-hand): Child has no pants skill. Partial prompt (touch at waistband): Child is emerging. Gestural prompt (point to waistband): Child is developing independence.
Toilet Seating
Guide child to sit. Ensure feet are flat on step stool. If resistant to sitting → start with 5-second sits and build gradually. Do not rush this phase.
Present Reinforcement Context
Ensure timer is visible. Show token board — child sees what's coming after success. The promise of reinforcement must be visible during the sitting phase.
What to Watch For: Child looks at sequence strip independently (positive — they're using it) | Child relaxes after initial resistance (sensory tolerance building) | Child points to or reaches for toilet card (communication initiation — celebrate this immediately) Timing: 1–3 minutes of sitting. No pressure for elimination in early weeks. Any seated time without distress earns the next step.

STEP 3 OF 6 ●●●○○○
Step 3: The Core Action — Seated Routine + Communication Practice
Part A: Scheduled Sitting with Body Awareness Prompt
While child is seated, parent places one hand lightly on the child's belly (or models touching own belly) and says: "Body check. Is there a feeling here?" — then waits 15–20 seconds in silence. Do not expect a response. Repeat this same action every session. Over weeks, this builds interoceptive attentional focus.
Part B: Communication Card Practice
Whether or not elimination occurs: hand the toilet card to the child. Guide them to "present" it back to you (hand-over-hand if needed). This conditions the card-presentation → bathroom-access sequence at a neurological level. Eventually the child initiates this without prompting.
Part C: Sequence Strip Following
After seated time: point to each step on the strip — wipe (guide hand), pants up (prompt), flush (if tolerated), wash hands (guide to sink). Follow the strip. Every step. Every time. Only neutral "Next." with a point. No verbal narration required.
Response Spectrum
✅ Ideal
Child sits, performs elimination, follows strip, presents card
🟡 Acceptable
Child sits without elimination, follows strip partially, tolerates routine
🔴 Concerning
Child becomes significantly distressed → end session neutrally, do not force → revisit troubleshooting
Duration: 3–8 minutes total for seated phase.

STEP 4 OF 6 ●●●●○○
Step 4: Dosage — How Many Times, How Often, How to Vary
Phase | Interval | Daily Trips | |
Phase 1 (Weeks 1–4) | Every 30–45 minutes | 10–15 trips/day | |
Phase 2 (Weeks 5–12) | Every 45–60 minutes | 8–12 trips/day | |
Phase 3 (Weeks 13+) | Every 60–90 min → self-initiation | Decreasing as self-initiation increases |
3 GOOD TRIPS > 10 FORCED TRIPS. Each bathroom trip that ends neutrally or positively — regardless of elimination — is a learning event. Repetition without distress is the training.
Variation Options (to Maintain Engagement)
- Rotate which token/sticker the child places on board
- Vary the preferred post-bathroom activity offered
- On Variation Day: play quiet music in bathroom (novelty without disruption)
- Practice different sequence strip card-pointing or matching
Satiation Indicators — When to End
- Child has been seated 5+ minutes without elimination and shows early distress signs
- Child has completed the strip sequence and is gesturing "done"
- Child activates "done" or "all done" on AAC device
"THREE GOOD REPETITIONS BUILD MORE NEURAL PATHWAY THAN TEN DISTRESSED ONES. READ YOUR CHILD'S STATE, NOT YOUR SCHEDULE."

STEP 5 OF 6 ●●●●●○
Step 5: Reinforcement — Concrete, Immediate, Meaningful
📞 Call 9100 181 181 to build your child's personalized reinforcement menu with a BCBA
Level 1: Any Sit Without Distress
One token on board + brief physical affirmation (high five, gentle squeeze). Deliver within 3 seconds of child leaving toilet area.
Level 2: Following Sequence Strip
Two tokens + preferred sensory input (proprioceptive squeeze, spinning, brief preferred activity).
Level 3: Elimination in Toilet
Token board completion + IMMEDIATE preferred activity/item (15–30 seconds). THIS IS THE JACKPOT. Make it obvious. Light up. Spin the reward jar.
Level 4: Independent Card Presentation / AAC Initiation
THIS IS THE GOAL. Even if they don't eliminate — this is the most important behavior in the entire system. Treat independently-initiated communication as the highest-value event.
Pinnacle Canon Reinforcement Products
- Visual Reward Jar: Rosette Imprint Reward Jar — ₹589
- Sticker rewards: 1800+ Reward Stickers — ₹364
- Sensory transition toy: Animal soft toys — ₹425
Never:
- Withhold scheduled bathroom trips as punishment
- Use food rewards in the bathroom (hygiene)
- Delay reinforcement by more than 5 seconds

STEP 6 OF 6 ●●●●●●
Step 6: The Clean Close — Transition Out Without Disruption
"All Done" Signal
Show or activate "all done" on AAC. Point to last step on sequence strip (washing hands + exit image). Signal must be consistent every session.
Hands Washing
Guide through hand washing as the final sequence step. This is non-negotiable — it teaches the complete routine, not just the toileting portion.
Material Put-Away
If using portable kit — guide child to put toilet card back in pouch. Builds ownership of the communication system.
Transition to Next Activity
Show a "first-then" visual: "First bathroom → Then [preferred activity image]." Make the next activity immediately and visibly appealing — bring it to the bathroom door if needed.
Data Entry (30 seconds)
While child is settled in next activity. Three tick boxes. 60 seconds. See Card 20 for the full tracking protocol.
Cool-Down for the Parent: Every bathroom trip completed without distress — even with no elimination — is a training success. You built routine. You built trust. You built communication. Note it.

ACT III — DATA CAPTURE
60-Second Data Entry: What to Record After Every Trip
Track These 3 Data Points
Field | What to Record | How | |
Trip initiated by | Schedule / Card (child) / Physical signal (child) / Adult-directed | Tick box | |
Elimination | Yes — Urine / Yes — BM / No elimination | Tick box | |
Child state | Calm throughout / Mild resistance / Significant distress | Tick box |
Bonus (When Time Allows)
- Did child follow sequence strip? (Fully / Partially / Not at all)
- Did child respond to reinforcement? (Yes / Delayed / No response)
Why This Matters
"60 seconds of data now saves hours of guessing later. When you bring your tracking data to your Pinnacle therapist, they can see patterns you cannot — the time of day when success is highest, the environmental variables that predict distress, the reinforcement responses that signal which rewards are working. Data is your child's progress made visible." — Pinnacle BCBA Team
Tracking Options
📋 Pinnacle E-493 Toilet Training Daily Tracker (Google Form) 📥 E-493 Paper Tracking Sheet (PDF) — for families without phone access during bathroom trips
ACT III — TROUBLESHOOTING
Most Sessions Won't Be Perfect. Here's What Each Problem Actually Means.
Session abandonment is not failure — it is data.
Problem 1: Child Refuses to Enter Bathroom
Why: Bathroom environment is still aversive to the nervous system. Fix: Return to sensory adaptation protocol. Spend one week on "bathroom desensitization only" — child enters, receives preferred activity inside, exits. Build tolerance before building behavior.
Problem 2: Child Enters but Screams When Seated
Why: Tactile aversion to seat OR insecure positioning (feet dangling). Fix: Check step stool (feet must be flat). Add padded seat cover. Start with 3 seconds of sitting + immediate reinforcement. Build gradually from there.
Problem 3: Child Uses Card Only When Prompted
Why: Child has learned the compliant behavior — not the communicative function of the card. Fix: Create "communication opportunities" — adult waits 10–15 seconds at scheduled time, creating a gap for child to initiate. Respond dramatically to any independent card use.
Problem 4: Success at Home, Not at School
Why: Visual systems are not consistent across environments. Fix: Identical materials at school. Portable kit carried daily. Train school staff using this page. Same timer intervals, same strip, same reinforcement system.
Problem 5: Success for 2 Weeks Then Regression
Why: (a) Medical — rule out UTI, constipation first; (b) Schedule change; (c) Reinforcement satiation; (d) Too-rapid interval increase. Fix: Medical check first. Then return to Phase 1 interval, refresh reinforcement menu.
Problem 6: Child Never Self-Initiates Despite Routine
Why: Interoceptive awareness insufficient; card is associated with schedule, not body sensation. Fix: Intensify interoception work daily. Create deliberate body-signal-to-card-use pairing after large fluid intake.
Problem 7: Caregiver Inconsistency
Why: Without consistent response, child learns the card "sometimes works" — and stops using it. Fix: Share the Family Caregiver Guide with ALL adults. Consistency is non-negotiable. One adult who doesn't respond breaks the system.

ACT III — PERSONALIZATION
This System Adjusts to Your Child — Not the Other Way Around
Sensory Avoider (Hypersensitive)
- Sensory adaptations are critical FIRST — full environment protocol
- Longer bathroom desensitization phase (1–2 weeks before any demands)
- Seated time starts at 3 seconds → builds very gradually
- Low stimulation bathroom: quiet, dim, minimal objects
- Preferred sensory comfort item allowed in bathroom
Sensory Seeker (Hyposensitive)
- Proprioceptive input (body squeezes) as transition INTO bathroom
- Fidget item permitted while seated (occupies seeking need)
- More animated reinforcement response (jumping, spinning is appropriate)
- Heavier tactile reinforcement (bear hug after success)
Ages 3–5
Focus on routine following and environmental tolerance first. Communication card is primary goal. Self-initiation is secondary.
Ages 6–10
Communication initiation is the primary goal. Begin school generalization early in this phase.
Ages 11–15
Privacy and dignity are paramount. Child-led pacing. Peer-level social story framing. Begin generalization to community settings.
ACT IV — THE PROGRESS ARC
Week 1–2: Foundation Phase — Tolerance, Not Mastery
Progress: 15%
Foundation Phase
✅ What You MAY See in Week 1–2
- Child enters bathroom with reduced resistance compared to Day 1
- Child will sit for 5–10 seconds (up from 0)
- First isolated instance of elimination in toilet — celebrate enormously, do not expect consistency
- Child begins to orient toward toilet card when held up
❌ What You Will NOT See Yet
- Self-initiated communication (this is weeks or months away)
- Consistent elimination on schedule
- Routine following without prompting
- Generalization to other environments
The Most Important Week 1–2 Achievement
Zero distress bathroom trips. If your child can enter the bathroom, sit briefly, and exit calmly — you have achieved the foundational goal. Everything else builds on this.
Parent Emotional Preparation
Week 1–2 is when most families want to quit. Progress feels invisible. Diapers are still full. But the neural pathways for the visual routine are forming right now, invisibly. Every consistent trip is a deposit in an account you cannot yet see.
Data to Watch
Track seated duration. Even 1 second longer per trip is measurable, real progress.
ACT IV — PROGRESS ARC
Week 3–4: The Neural Pathways Are Forming — Watch for These Signs
Progress: 40%
Consolidation Phase
Anticipation Emerging
Child begins moving toward bathroom when timer sounds — before adult prompts. This shows the schedule is becoming internalized.
Communication Emergence!
Child reaches for toilet card WITHOUT adult holding it out first. This is the earliest form of independent communication initiation. Celebrate immediately and dramatically.
Independent Strip Use
Child looks at sequence strip independently — not just when parent points. Child follows 2–3 steps with reduced prompting. Neural pathways are consolidating.
Interoceptive Awareness Beginning
Child touches belly area after fluid intake. Seated time increases to 30–60 seconds without distress. Pattern of successful elimination becoming visible in data.
"You may notice in Week 3–4 that you feel more confident. You're reading your child's signals better. The bathroom routine feels familiar. That parent confidence is real — and it accelerates outcomes because your child reads your regulated state." — Pinnacle Consortium OT

ACT IV — MASTERY
Week 5–8: From Routine Compliance to Self-Initiated Independence
🏅 Progress: 75%
Mastery Phase
Mastery Criterion | Observable Indicator | |
Communication Mastery | Child independently presents toilet card or activates AAC toilet symbol ≥ 3 times per day without prompt | |
Routine Mastery | Child follows complete sequence strip with gestural prompt only | |
Elimination Mastery | ≥ 80% of daytime eliminations occurring in toilet (not in diaper/underwear) | |
Environmental Mastery | System functioning at home AND one other environment (school or grandparents') |
Mastery Unlocked — What Comes Next
- Expand to underwear/pull-ups during waking hours
- Extend to second environment (school)
- Begin nighttime program if daytime mastery is established
- Progress to E-494 (Hygiene Routines for Nonverbal Children)
Stay vs. Move Forward
If environmental generalization is not yet achieved — stay and strengthen. Do not advance to the next technique until the current one is functional in at least two environments. The foundation must be solid.
Research: BACB mastery criteria standards + PMC10955541 (Meta-analysis on mastery outcomes)

ACT IV — MILESTONE
You Did This. Your Child Is Independent Because You Were Consistent.
🏆 MILESTONE REACHED
Your child now communicates their own bathroom needs. This is not a small thing. This is one of the most complex achievements in pediatric development — and it happened in YOUR home, through YOUR hands, with YOUR consistency.
School Access
Placement opportunities that were previously closed are now open to your child.
Social Participation
Settings that previously required diaper changes are now fully accessible.
Owned Communication
Your child has a communication system they own — not one borrowed from verbal templates.
A Lifelong Foundation
What you built together will persist for the rest of your child's life. Mark this date.
Journal Prompt:"What was the moment I realized something had changed? What did I see that told me the system was working?"
ACT IV — RED FLAGS
Even After Progress — These Signs Mean Pause and Seek Guidance
📞FREE 24×7 Helpline: 9100 181 181 | Teleconsult available within 24 hours
🔴 Physical Red Flags
- Blood in urine or stool at any point
- Child crying during urination (possible UTI or structural issue)
- Child holding urine for 6+ hours (possible retention)
- Sudden onset of constipation after training begins (withholding behavior)
- Significant weight loss, fatigue, or fever coinciding with training
🔴 Behavioral Red Flags
- Sudden complete regression after 2+ weeks of progress (rule out medical first)
- New self-injurious behavior appearing specifically in bathroom context
- Child developing extreme avoidance or phobia of bathroom
- Signs of significant anxiety (sleeplessness, food refusal, increased meltdowns)
🔴 Communication Red Flags
- Child stops using toilet card after previously using it consistently
- Child activates "hurt" or "help" on AAC during bathroom routine
Concern | Action | |
Physical red flag | Pediatrician or hospital FIRST — do not resume training until cleared | |
Behavioral regression | Pause training 5 days → teleconsult → modified restart | |
Anxiety escalation | OT sensory consultation → sensory environment reset → slower timeline |
ACT IV — PATHWAY MAP
Where This Leads: Your Child's Self-Care Development Roadmap
Lateral Alternatives
- E-492: Autism-specific toilet training (for children with emerging verbal skills)
- B-series: AAC system building (if communication system needs strengthening first)
Long-Term Developmental Goal
Full self-care independence across home, school, and community environments — enabling participation in mainstream education, vocational preparation, and community life. E-493 is the bridge that makes it possible.

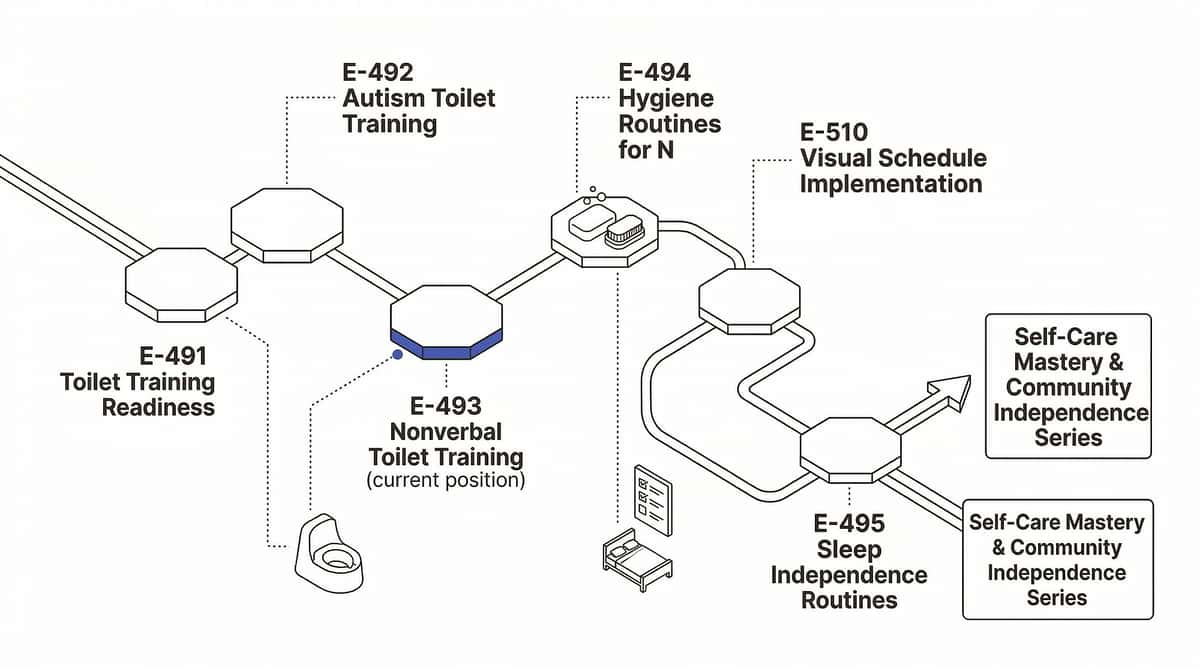
ACT IV — RELATED TECHNIQUES
Other Techniques in the Self-Care & Communication Domain
Your E-493 kit already covers the foundation for E-494, E-495, and E-510. The materials you own today carry forward.
Technique | Code | Difficulty | Materials You Already Own | |
Toilet Training Readiness | E-491 | 🟢 INTRO | Visual cards, timer | |
Autism Toilet Training | E-492 | 🟡 CORE | Sequence strips, rewards | |
Nonverbal Toilet Training | E-493 | 🟡CORE | Full kit from this page | |
Hygiene Routines (Nonverbal) | E-494 | 🟡 CORE | Sequence strips, AAC | |
Sleep Independence Routines | E-495 | 🟡 CORE | Visual timer, sequence strip | |
Older Child Toilet Training | E-513 | 🔴 ADVANCED | AAC, sensory equipment | |
Visual Schedule Implementation | E-510 | 🟢 INTRO | Timer, sequence strips |

ACT IV — FULL DEVELOPMENTAL MAP
This Technique Is One Piece of a Larger Journey — Here Is the Full Map
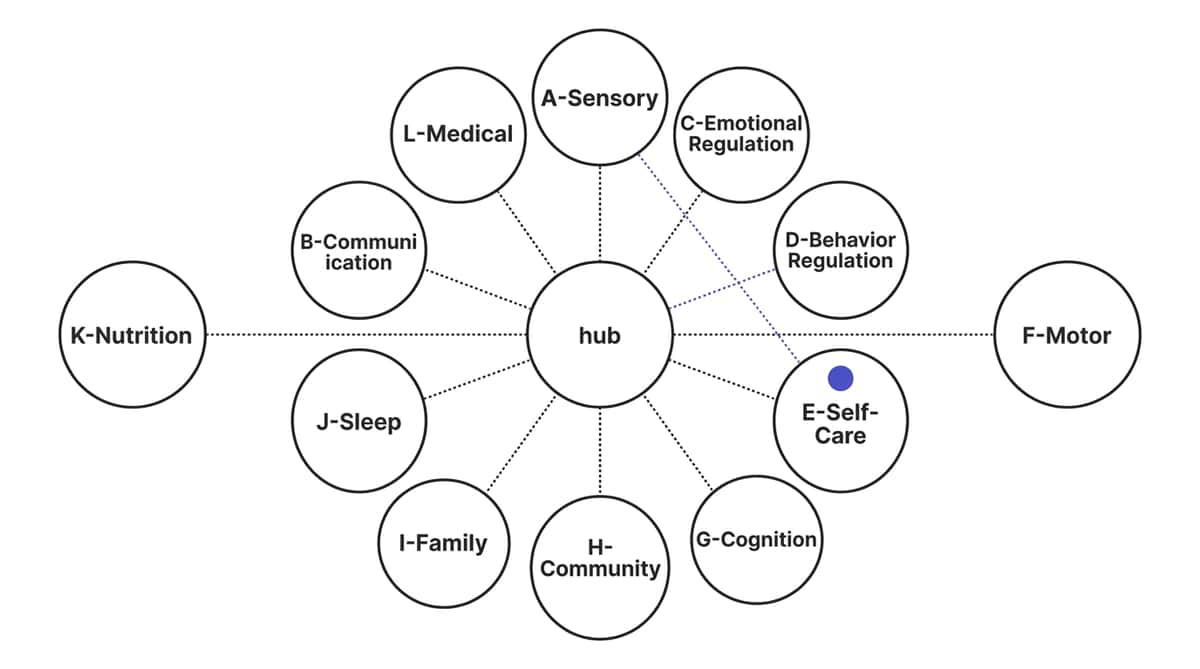
E-493 Within the Ecosystem
Nonverbal toilet training sits at the intersection of Domain E (Self-Care), Domain B (Communication), and Domain A (Sensory Processing). Progress here will directly accelerate outcomes in all three interconnected domains simultaneously.
What GPT-OS® Sees
When your child's E-493 data flows into GPT-OS®, the system cross-references it against the Communication for Needs Index, Self-Care Readiness Index, Sensory Processing Profile, and Interoception Development Index — making patterns visible across 20M+ sessions.
📞Request AbilityScore® Assessment: 9100 181 181

ACT V — THE COMMUNITY
From the Families Who Were Exactly Where You Are Now
"Eight Years. Then Three Months."
Before: "Our daughter was eight and completely nonverbal. Eight years of diapers. We had tried everything. Nothing worked because everything assumed she could tell us or answer us."
After: "Our Pinnacle OT introduced the toilet card as her literal voice. Three months of absolute consistency. She now presents her toilet card 8–10 times per day, independently, across home and school. She is 100% daytime independent."
— Parent, Pinnacle Center (anonymized) | Outcomes vary; illustrative case
"The Sequence Strip Changed Everything"
Before: "My son understood nothing verbal in the bathroom. Every step was a battle because he didn't know what came next. The unpredictability was the problem."
After: "The sequence strip at his eye level gave him the script he needed. Within six weeks, he was completing the routine with only a pointing gesture. He needed to SEE the steps — he just needed to know what was coming."
— Parent, 6-year-old, ASD Level 2 | Outcomes vary; illustrative case
"In our clinical experience across 20M+ sessions, the single biggest factor in nonverbal toilet training success is caregiver response consistency to the communication system. When every adult responds to the toilet card within 3 seconds — 100% of the time — the child's rate of independent communication increases dramatically." — Pinnacle OT/SLP/BCBA Consortium
ACT V — COMMUNITY CONNECTION
You Are Not Navigating This Alone — Join the Community
📱 WhatsApp Parent Group
Families across India and 70+ countries sharing daily progress, challenges, and wins. Moderated by Pinnacle therapists. Evidence-based only.
💬 Pinnacle Parent Forum
Searchable archive of 10,000+ parent questions answered by Pinnacle consortium therapists. Self-Care domain focus.
🤝 Peer Mentoring
A parent who has completed this journey with their nonverbal child — available for direct conversation with families just starting out.
📍 Local Parent Meetups
In-person parent groups at Pinnacle centers across India. Self-care skills focus monthly at each center location.
"Your experience — however hard — helps the parent who is 6 months behind you. Consider sharing your journey when you reach the other side."

ACT V — PROFESSIONAL SUPPORT
Home Practice + Professional Guidance = Maximum Outcomes
📞Book Assessment: 9100 181 181 (FREE, 16 languages, 24×7)
For E-493, Request a Therapist Specializing In:
- Pediatric OT — Self-care skills and sensory processing
- SLP — AAC systems and functional communication training
- BCBA — Toilet training behavioral protocols and data systems
Professional Assessment Path
- AbilityScore® Assessment (self-care domain)
- Sensory Processing Profile (OT)
- AAC Evaluation (SLP)
- Toileting Protocol Design (BCBA)
- School Integration Planning (SpEd)
70+ Centers Across India
Specialized in nonverbal toilet training | OT + SLP + ABA in one location
💻 Teleconsultation Available
Video consultation with Pinnacle specialists. Remote families welcome. Bring your tracking data, your questions, and your E-493 kit.
Funding / Insurance
Pinnacle can advise on government schemes, insurance claims, and disability support funding for therapy services in your state.
"HOME + CLINIC = MAXIMUM IMPACT. NEITHER ALONE IS ENOUGH."

ACT V — RESEARCH LIBRARY
The Evidence Foundation: For the Parent Who Wants to Go Deeper
Study | Finding | Reference | |
NCAEP EBP Report (2020) | Visual supports classified as evidence-based practice for autism across self-care | ncaep.fpg.unc.edu | |
PMC11506176 (PRISMA, 2024) | Sensory integration intervention meets EBP criteria for children with ASD | pubmed.ncbi.nlm.nih.gov | |
PMC10955541 (Meta-analysis, 2024) | SI therapy promotes adaptive behavior, social skills, sensory processing | pubmed.ncbi.nlm.nih.gov | |
PMC9978394 (WHO CCD) | Home-based caregiver-implemented intervention efficacy across 54 LMICs | pubmed.ncbi.nlm.nih.gov | |
Padmanabha et al. (2019) | Indian RCT: home-based visual interventions — significant outcomes in Indian pediatric population | Indian J Pediatr DOI: 10.1007/s12098-018-2747-4 | |
AOTA Practice Guidelines | Self-care skill development and adaptive toileting guidelines | aota.org |
ACT V — GPT-OS® DATA
Your 60 Seconds of Data. Powering Personalized Recommendations.
What GPT-OS® Learns from E-493 Data
- Time-of-day patterns for elimination success (optimizes schedule)
- Correlation between child state and elimination rate
- Communication initiation frequency over time (measures independence progress)
- Environmental variables associated with success vs. distress
Your Data Helps Every Child Like Yours
Anonymized, aggregated data from families implementing E-493 improves the recommendation engine for all families navigating nonverbal toilet training — across India and 70+ countries.
Privacy Assurance
All data is encrypted, anonymized at processing, and stored under Indian data protection standards. Individual child data is never shared without explicit consent.
To Enroll
📞 Call 9100 181 181 to connect your family to the GPT-OS® dashboard and start receiving personalized recommendations.

ACT V — WATCH THE REEL
Watch the Original Reel That Surfaces This Challenge
"Nonverbal toilet training is one of the most challenging and most misunderstood areas in pediatric therapy. Every method online assumes speech. When speech isn't there, those methods simply don't apply. But here is what I want every family to know: nonverbal does not mean incapable. Visual communication systems build exactly the bridge that verbal children get automatically through language. I've seen children at age 12 achieve full independence after years in diapers — because someone finally gave them the right visual tools. That's what these 9 materials do." — Pinnacle Consortium OT
▶ Reel E-493
9 Materials demonstrated visually in real home settings. A Pinnacle OT walks through each material in 60 seconds.
Series
Self-Care & Daily Living Skills | Episode 493 | Pinnacle Blooms Network® Content Library
Related Reels
E-491: Toilet Training Readiness | E-492: Autism Toilet Training | E-494: Hygiene Routines for Nonverbal Children
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning improves parent skill acquisition.

ACT V — SHARE THIS PAGE
One Parent Implementing This System Is Good. Every Caregiver Implementing It Is Transformative.
The visual communication system only works when EVERY adult who cares for your child uses it identically. If the toilet card gets a bathroom response at home but not at school, the child learns the card "sometimes works" — and stops using it.
"Explain to Grandparents" Version
"When [child's name] gives you this card / points to this symbol on their device, it means they need the bathroom RIGHT NOW. Take them immediately. Don't ask questions. Don't wait. The card is their way of saying the words they can't speak. Respond exactly the same way you would if they said 'I need to go.'"
Teacher / School Communication Template
"[Child's name] is using a visual toilet communication system developed by Pinnacle Blooms Network®. The system requires:
- Identical toilet communication card available at school
- Immediate response to card presentation — within 3 seconds
- Visual sequence strip posted in school bathroom
- Same reinforcement system as used at home
Please contact [parent name] or call Pinnacle 9100 181 181 for training."

ACT VI — THE CLOSE
Questions We Hear From Families Every Day — Answered
Q1: How long will nonverbal toilet training take?
Timeline varies significantly. Most children show first signs of the system working within 2–4 weeks. Daytime independence typically emerges between 3–12 months of consistent implementation. Some children require 18–24 months. Do not compare to verbal toilet training timelines — this is a different developmental pathway.
Q2: My child is 10 years old. Is it too late?
No. We have supported children achieving full independence at age 14 and beyond. Neuroplasticity does not end at age 5. Older children often have clearer communication preferences and stronger visual processing skills — which can actually accelerate progress once the right system is in place.
Q3: Do I need an expensive AAC device, or will a homemade card work?
Start with a homemade toilet card — it works. A photograph of your actual toilet is MORE concrete than a commercial symbol for most children. An AAC device is the eventual goal, but a single toilet card is a complete starting system. Don't wait for equipment to start.
Q4: My child uses the toilet when taken but never initiates. What do I do?
This is the most common pattern — compliance without initiation. Focus exclusively on teaching the card as an initiation behavior: create "communication opportunities" where you wait for the child to present the card before taking them. Make independent card use the most highly reinforced event in the system.
Q5: School says they can't implement the visual system. What do I do?
This is an IEP right. Toileting independence is a functional life skill, and the accommodations required are legally mandated supports for eligible children. Request an IEP meeting. Bring this page. Call 9100 181 181 — our Special Education advocates can advise.
Q6: My child is afraid of the flush. We can't get past it.
Flush aversion is extremely common and very addressable. Begin by having the child exit the bathroom before flushing. Then: listen from outside → listen from inside with door open → watch from inside → eventually participate. This desensitization takes 2–6 weeks. Never force proximity to the flush sound.
Q7: Can this work if my child also has intellectual disability?
Yes. The visual communication system is designed precisely for children whose learning pathway is visual and behavioral rather than verbal. Children with intellectual disability may require more repetitions and longer timelines — but the same system applies. IQ is not predictive of toileting independence achievement.
Q8: Is there a night-time training component?
Nighttime training is addressed only after daytime mastery is established for 4+ consecutive weeks. Nighttime bladder control is physiologically different and typically comes later. Focus completely on daytime independence first, then consult your Pinnacle team about a nighttime protocol.

ACT VI — START NOW
Your Child Can Have This Independence. The System Is Here. Begin Today.
Right now, somewhere in India, a child who has been in diapers for 6 years is presenting a toilet card for the first time — because their parent implemented this system this week. That parent started exactly where you are. They read this page. They made a laminated card with a phone photograph. They mounted a printed sequence strip. They responded immediately, every time. Three months later, their child speaks with a card held in their hand.
🏛️ Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev • CRO
20M+ Sessions | 97%+ Improvement | 70+ Centers | 70+ Countries
Preview of 9 materials that help with nonverbal toilet training Therapy Material
Below is a visual preview of 9 materials that help with nonverbal toilet training therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

ACT VI — THE PINNACLE PROMISE
From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Network® exists for the parent who was told "nothing can be done" — and refused to believe it. We exist for the child whose nervous system was called a problem, when it was always a pathway. We exist to transform every home into a 24×7 personalized therapeutic environment — not because we think parents should do the work of therapists, but because we know that the 23 hours between therapy sessions are where children actually grow.E-493 is one technique in a library of 70,000+. Each one is the same promise: science, made practical. Evidence, made human. Independence, made possible.
Consortium Disciplines
Pediatric OT • SLP • ABA/BCBA • Special Education • Neuro-Developmental Pediatrics • Clinical Research Operations • WHO/UNICEF Aligned Frameworks
Loop Navigation
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention from licensed occupational therapists, speech-language pathologists, or behavior analysts. Delayed toileting may indicate underlying medical, developmental, or sensory conditions requiring professional evaluation. Always consult your child's healthcare team before beginning or modifying any toileting program. Individual results vary based on child profile, underlying condition, caregiver consistency, and implementation fidelity.
CIN: U74999TG2016PTC113063 | DIPP8651 (Govt. of India) | Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are registered marks/trademarks of Bharath Healthcare Laboratories Pvt. Ltd.
📞 FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | pinnacleblooms.org