
Every morning, before you even open the door, you already know.
The sheets are wet. Again. They slept through it completely — didn't feel it, didn't wake up, don't understand why. And the shame in their eyes when they realize it has started breaking your heart.
E-502 | Ages 5–15
Gastrointestinal & Toileting Challenges
"You are not failing. Your child's brain is not yet waking to bladder signals during deep sleep. This is neurological — and it is treatable."
The brain that doesn't wake. Here is exactly why.
Nocturnal enuresis is not a behavioral problem. It is a wiring difference between the sleeping brain and the bladder — and understanding the three neurological factors changes everything about how you approach treatment.
🧠 High Arousal Threshold
Most children with bedwetting are extremely deep sleepers. When the bladder sends "full" signals upward through the spinal cord, the sleeping brain doesn't wake — the signal doesn't cross the arousal threshold.
🫘 Nocturnal Polyuria
Many children produce more urine at night than their bladder can hold. Insufficient vasopressin (antidiuretic hormone) tells the kidneys not to concentrate urine — more urine means a fuller bladder, earlier wetting.
🫧 Reduced Functional Bladder Capacity
Some children's bladders contract before they are completely full, creating urgency that arrives too quickly for the arousal pathway to activate — even when the bladder isn't truly full.
For children with autism: Interoceptive awareness — the brain's ability to perceive internal body signals including bladder fullness — is frequently atypical. Combined with deeper sleep patterns, this creates a compounding challenge requiring multi-modal support aligned with the child's sensory profile.

Developmental Timeline
Your child is here. Here is where this journey leads.
Nocturnal enuresis persisting beyond age 5 warrants assessment. Beyond age 7, active intervention is recommended. Without intervention, approximately 15% of children become dry each year naturally — with bedwetting alarm therapy, this timeline can be accelerated significantly.
Age 2–3
Daytime control begins
Age 4–5
Daytime dryness established
Age 5–7
Nighttime dryness typically begins for most children
Age 7–10
Nighttime independence achieved — your child may be here
Age 10–15
Full nighttime dryness with or without intervention
Common Co-occurring Conditions
- Autism Spectrum Disorder (ASD)
- Attention Deficit Hyperactivity Disorder (ADHD)
- Constipation / bowel dysfunction
- Sleep disorders
- Anxiety / psychological stress (secondary enuresis)
Natural Resolution Without Intervention
At age 7: ~10% still wet. At age 10: ~5%. At age 15: ~1–2%. With bedwetting alarm therapy, this timeline accelerates significantly.
"Waiting is a valid choice. But evidence-based intervention can give your child dry nights — and restored confidence — years earlier."
Level I Evidence
Clinically validated. Home-applicable. Parent-proven.
🔬 Primary Evidence
Cochrane Systematic Reviews on bedwetting alarm therapy: 65–75% success rate with consistent use. Lower relapse rates than pharmacological intervention. Bedwetting alarms meet Level I evidence criteria as the gold-standard first-line treatment for monosymptomatic nocturnal enuresis.
📊 Supporting Research
Cuvo & Riva (1980), JABA 13(2): Demonstrated that learned physiological responses — including arousal conditioning — can be systematically modified through behavioral approaches. Foundational evidence for alarm conditioning therapy. PMC1308134.
🏥 Clinical Consensus
International Children's Continence Society (ICCS): Bedwetting alarms recommended as first-line treatment. Desmopressin for nocturnal polyuria. Bladder training as adjunct.
Evidence Strength Ratings
75%
Evidence Strength
100%
Home Executability
100%
Safety Profile
60%
Speed of Results
12–16 weeks (alarm)
PMC1308134 | PMC11506176 | PMC10955541 | PMC9978394 | WHO NCF 2018 | ICCS Guidelines | Padmanabha Indian J Pediatr 2019

ACT II — THE SCIENCE
🌙 Nocturnal Enuresis Materials & Intervention System
Parent-Friendly Alias: "The Dry Nights Protocol" — A multi-modal, home-executable intervention framework combining behavioral conditioning (bedwetting alarms), environmental management (waterproof protection), physiological training (bladder capacity and arousal), and behavioral support (reward systems) to address nocturnal enuresis in children ages 5–15.
🏷️ Domain
Toileting / Urological Health / Occupational Therapy / Behavioral Support / Sleep Physiology
👶 Age Range
5–15 years | Nightly protocol | 12–16 weeks expected timeline
📍 Setting
Home — sleep environment | Daytime bladder training 2–3× daily
🧩 Canon
Toileting Support + Sensory Processing + Behavioral Reinforcement
E-502 sits within the Gastrointestinal & Toileting Challenges cluster (GI-05). Previous: E-501 Encopresis & Soiling. Next: E-503 Daytime Wetting. Full cluster: E-500 to E-504.

This technique crosses every therapy boundary — because the bladder doesn't organize by discipline.
Occupational Therapy (Lead)
Sensory processing assessment, interoception training, adaptive equipment selection, daily living skill development for toileting independence.
ABA / BCBA
Behavioral conditioning protocol design, reinforcement schedules, data-driven alarm training compliance, token economy implementation.
NeuroDev Pediatrics
Medical evaluation, vasopressin assessment, constipation management, desmopressin coordination, developmental trajectory monitoring.
Speech-Language Pathology
Interoception vocabulary building, communication scripts for children who struggle to express body signals, social impact of bedwetting.
Special Education
Visual schedule design, home routine structuring, school accommodation planning for children managing social anxiety around bedwetting.
FusionModule™ at Pinnacle converges all five disciplines into a single coordinated plan — so the alarm your child uses at night connects to the interoception work in OT, the reinforcement system in ABA, and the communication support in SLP. 📞9100 181 181 — FREE. Speak to a consortium coordinator.

9 materials. Each with a specific neurological job. All home-executable.
Every material in this list is clinically validated and aligned with ICCS treatment guidelines. Total estimated starter investment: ₹4,300–15,700. Essential starter kit (alarm + protection + diary + reward chart): ~₹3,500–12,000.
# | Material | Core Function | Price Range | |
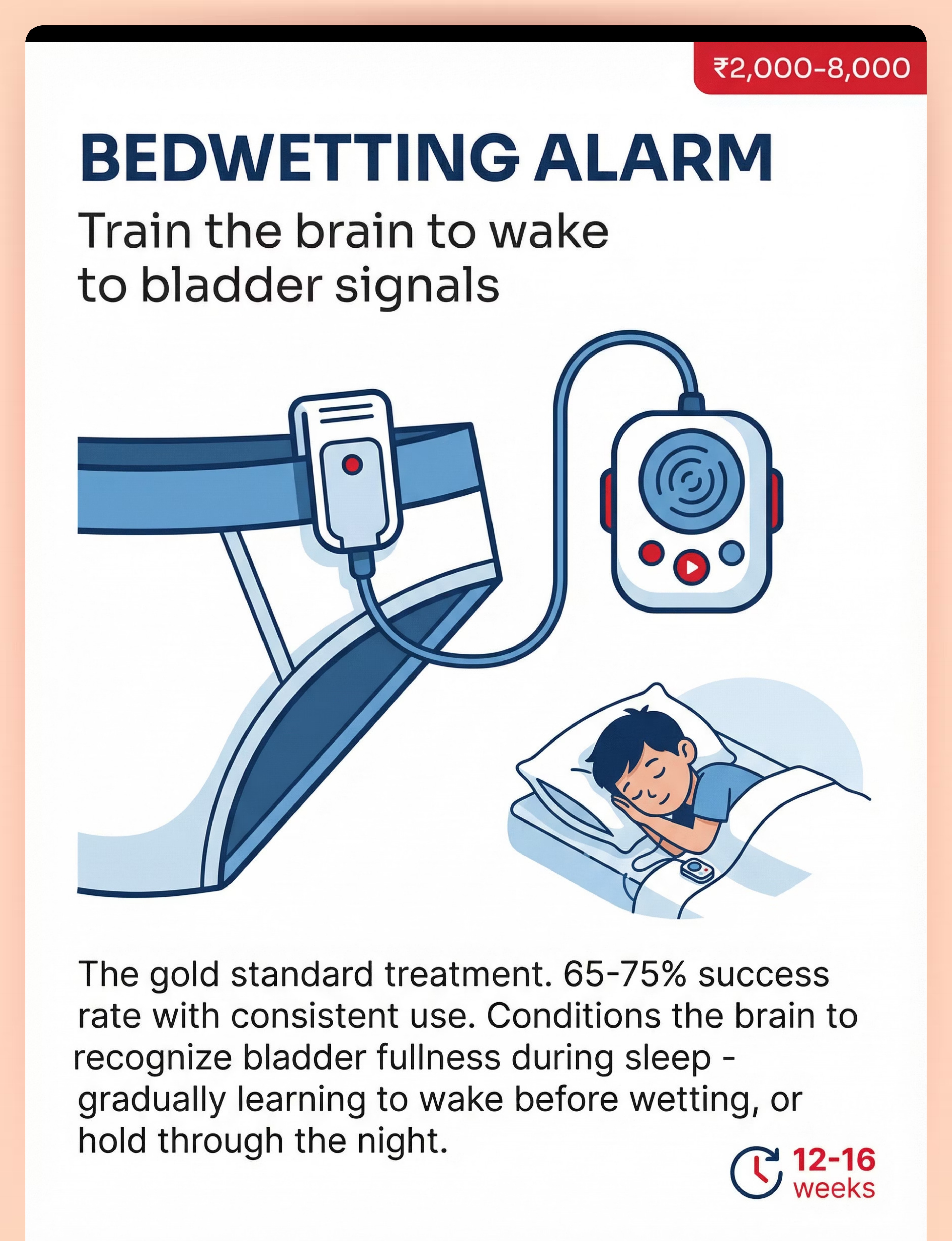
1 | 🔔 Bedwetting Alarm | Brain conditioning — arousal training | ₹2,000–8,000 | |
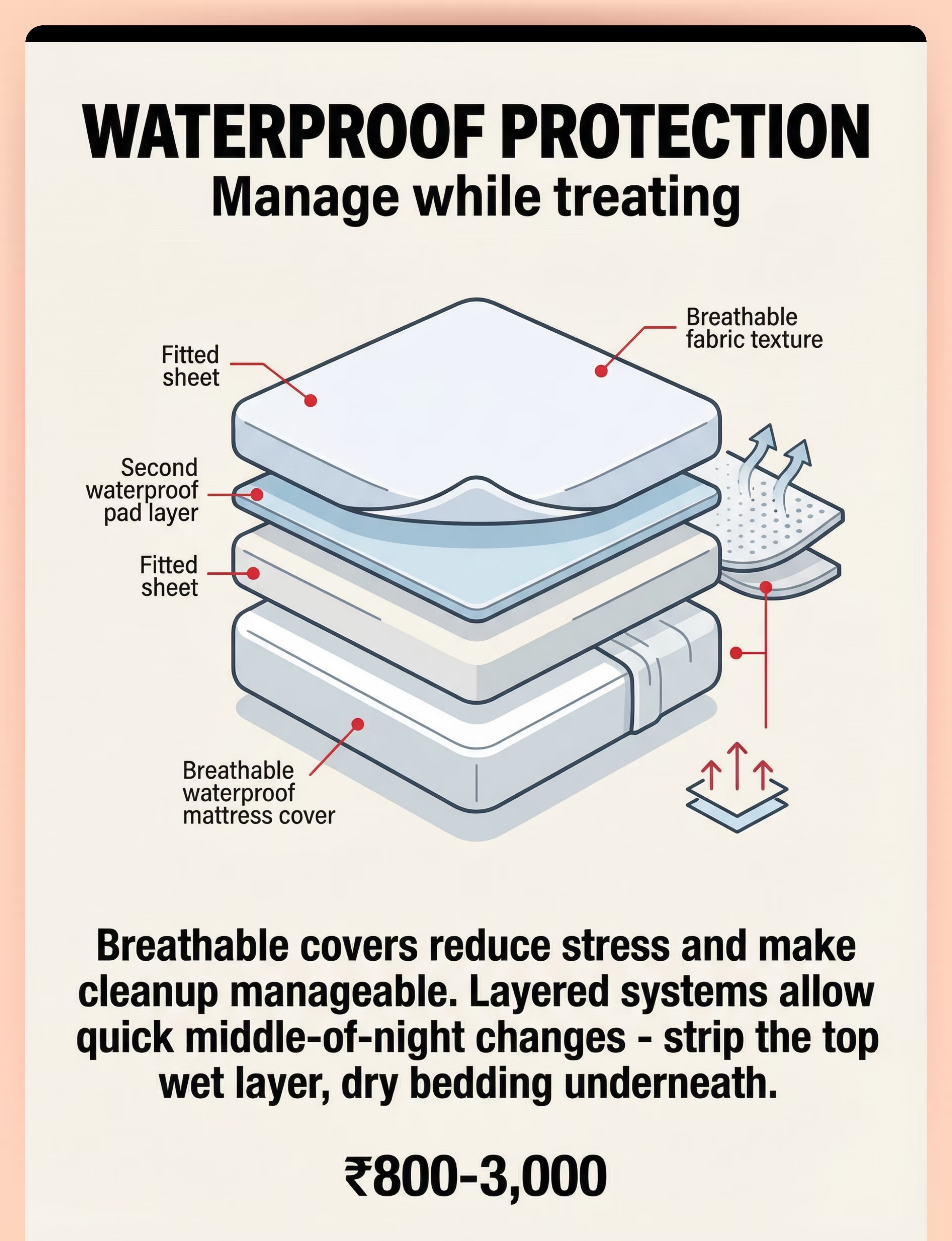
2 | 🛏️ Waterproof Protection | Manage while treating | ₹800–3,000 | |
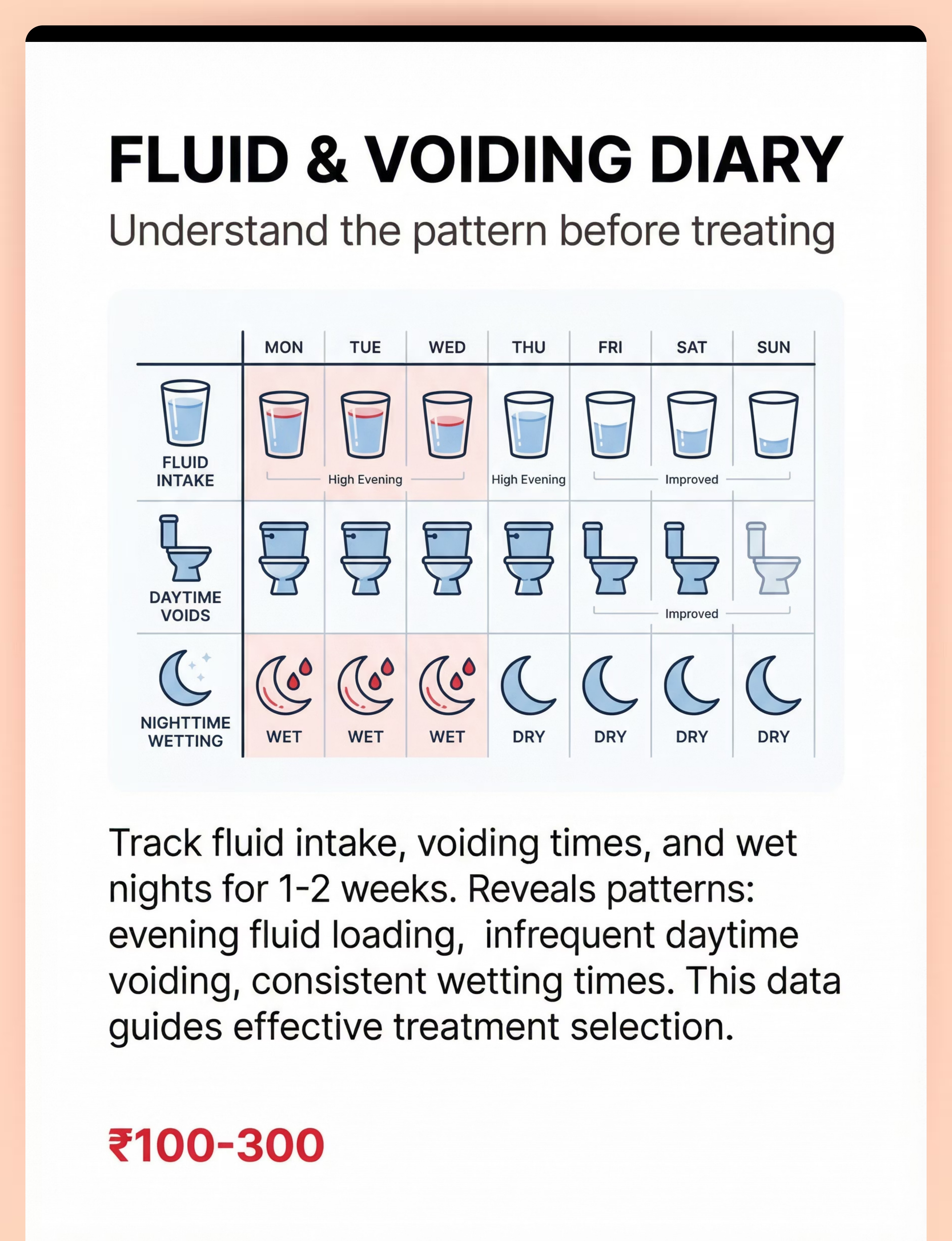
3 | 📓 Fluid & Voiding Diary | Understand the pattern first | ₹100–300 | |
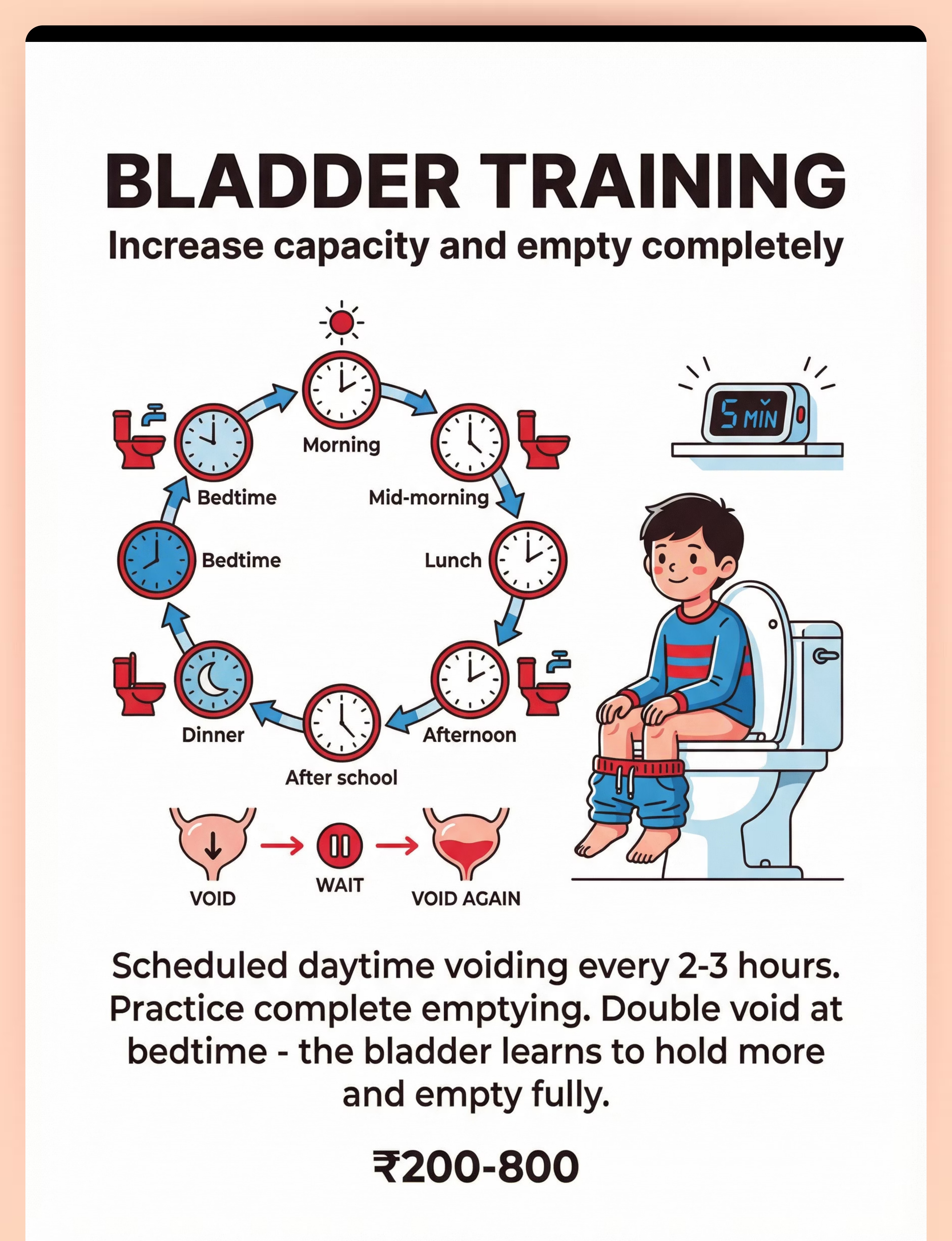
4 | ⏰ Bladder Training System | Expand capacity, empty completely | ₹200–800 | |
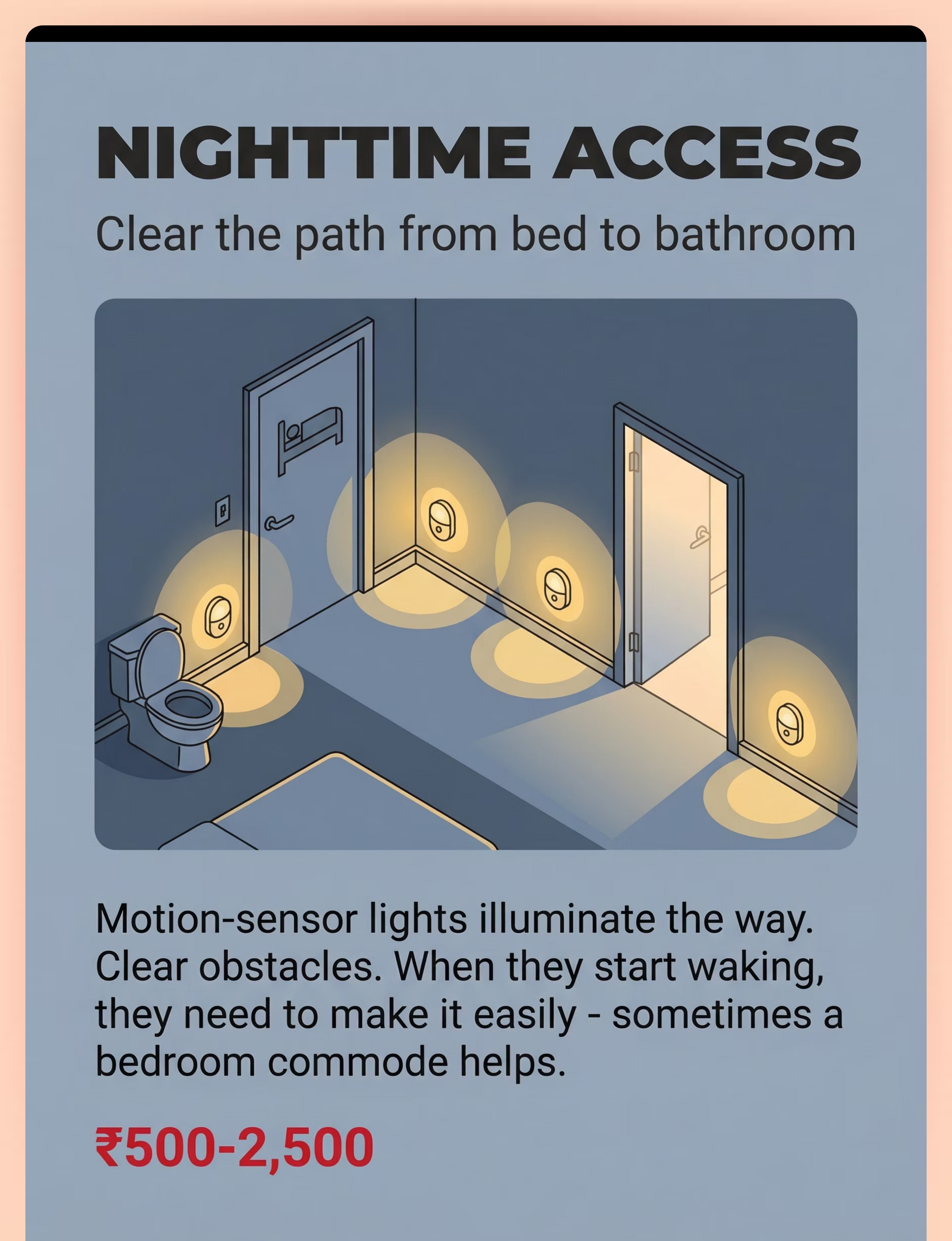
5 | 💡 Nighttime Lighting | Clear the path — bed to bathroom | ₹500–2,500 | |
6 | 👕 Absorbent Dignity Products | Protection without shame | ₹500–2,000/mo | |
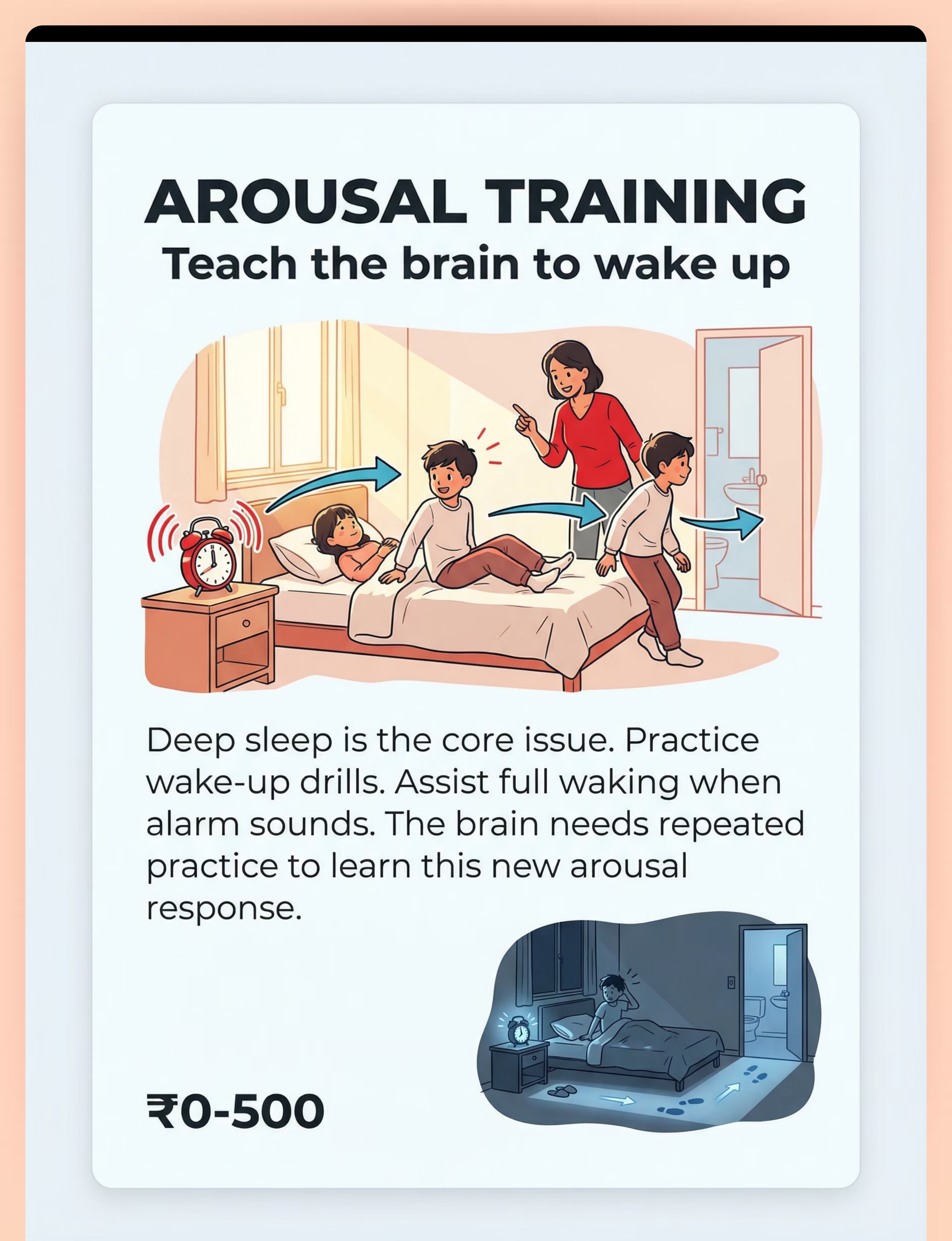
7 | 🌅 Arousal Training Kit | Teach the brain to wake | ₹0–500 | |
8 | ⭐ Reward System | Reinforce effort and progress | ₹200–600 | |
9 | 🏥 Professional Assessment | Match treatment to cause | ₹1,000–5,000 |

Material 1 of 9
₹2,000–8,000
🔔 BEDWETTING ALARM | Train the brain to wake to bladder signals
A moisture sensor (worn in underwear or placed on a bed pad) connected to an alarm unit that activates immediately when wetness is detected. Available in wearable and wireless versions, with sound, vibration, and light alert modes for deep sleepers.
Why It Works — The Science
The alarm creates a conditioned arousal response. Each time wetting begins and the alarm fires, the sleeping brain is interrupted. Over 12–16 weeks, the brain learns to associate bladder fullness with waking arousal — shifting from waking after wetting, to waking during, to waking before, to sleeping through dry.
Success Rate
65–75% with consistent use | Lower relapse than medication (Cochrane Reviews | PMC1308134)
Expected Timeline
- Weeks 1–4: Waking after wetting (conditioning begins)
- Weeks 5–8: Waking faster, smaller wet spots, occasional dry nights
- Weeks 9–12: Waking before wetting, dry nights increasing
- Weeks 12–16: Target: 14 consecutive dry nights
- Post-14 dry: Overlearning phase (extra fluids before bed for 2 weeks)
Product Types
- Wearable clip-to-underwear sensor (most effective)
- Vibrating wrist alarm (for ASD/deep sleepers)
- Wireless pad sensor (mattress/sheet based)
- Multi-mode: sound + vibration + light combined
Key Caution: Child must FULLY wake — not turn alarm off while asleep. Parent presence is critical in the first 4 weeks. Search: "bedwetting alarm India" on Amazon.in

Material 3 of 9
₹100–300
📓 FLUID & VOIDING DIARY | You cannot fix what you don't understand.
Track for 1–2 weeks before starting treatment. The patterns your diary reveals will directly shape which treatment approach is right for your child's specific presentation — making it the single most valuable ₹100–300 you will spend.
Column | What to Record | |
Fluid intake | Time + approximate amount of each drink | |
Daytime voids | Time + volume if possible | |
Urgency/accidents | Any daytime symptoms | |
Nighttime wetting | Wet/dry + approximate size of wet spot | |
Wetting time | If known (alarm will reveal this) |
What Patterns Reveal
1
Evening fluid loading
→ Reduce evening drinks after 6 PM
2
Infrequent daytime voiding
→ Bladder training indicated (see Material 4)
3
Consistent wetting time
→ Targeted scheduled waking as bridge strategy
4
Large wet spots early night
→ Nocturnal polyuria / vasopressin issue — discuss desmopressin with pediatrician
Share your completed diary with your healthcare provider before choosing a treatment approach. DIY Version: School notebook with simple columns. Digital Version: Notes app or request GPT-OS® digital diary template.
Material 4 of 9
₹200–800
⏰ BLADDER TRAINING | Daytime habits build nighttime capacity.
A bladder exercised with regular, complete emptying develops greater functional capacity and stronger sphincter control — directly reducing nighttime overflow risk. Daytime training is not separate from the nighttime protocol; it is the foundation of it.
1
Scheduled voiding every 2–3 hours
Set a timer during the day. This establishes regular emptying habits and prevents the bladder from chronically overfilling.
2
Progressive delay
When urge is felt, wait 1–2 minutes before voiding. This gentle resistance builds functional bladder capacity over weeks.
3
Complete emptying — double void
Void, wait 2 minutes, void again. This ensures the bladder is fully emptied, reducing residual urine that triggers nighttime overflow.
4
Bedtime double void
Always void, wait 5 minutes, then void again before sleep. This is the single most important step of the entire bedtime routine.
Materials Needed: Visual voiding schedule poster | Timer (kitchen timer / watch alarm / phone) | Measuring container (optional, for tracking functional capacity) | Double voiding instruction card (laminated for bathroom wall)

Material 5 of 9
₹500–2,500
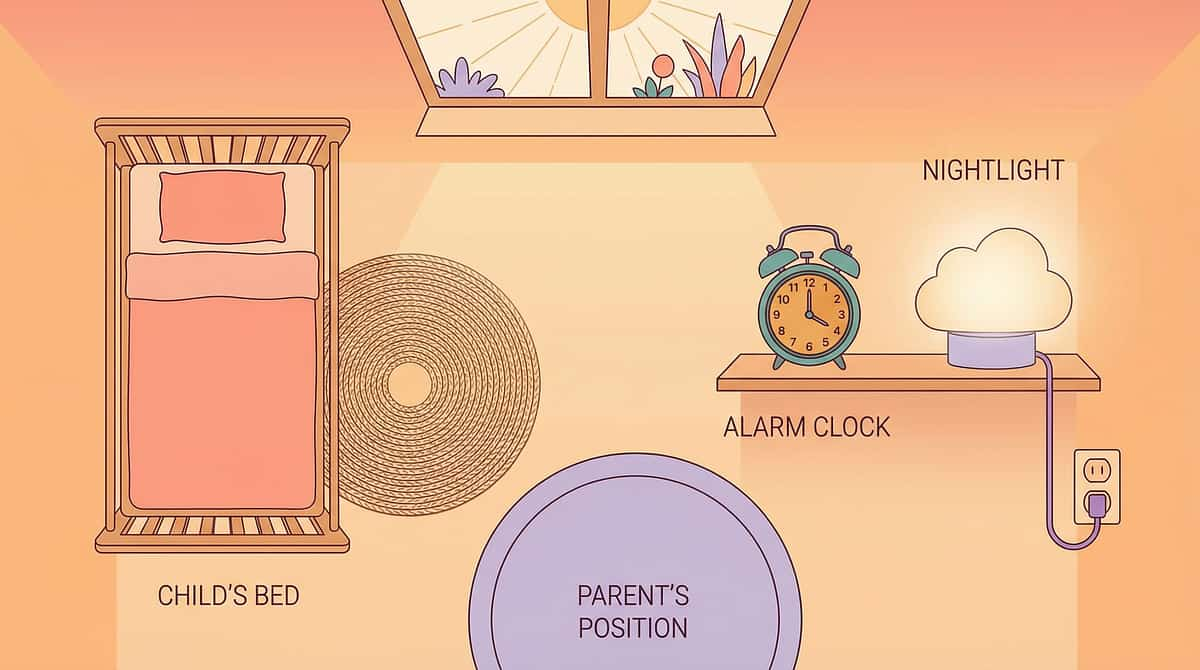
💡 NIGHTTIME ACCESS | Waking is only half the battle. They must also make it.
A child who begins waking to a full bladder — a positive sign that conditioning is working — will still wet if the path to the bathroom is too dark, too long, too scary, or too complex in a half-asleep state. The environment must meet the child halfway.
Environment Solutions
- Motion-sensor nightlights: bedroom → hallway → bathroom (auto-illuminate entire path)
- Bathroom door left open with soft light on
- Glow-in-the-dark path stickers on floor
- Clear all obstacles from the path
- Non-slip slippers beside bed for immediate use
- Bedroom commode for children whose bathroom is far or frightening at night
Practice Run
Walk the path during daytime with your child. Let them practice the route. Familiarity reduces decision-making friction at 2 AM — and friction at 2 AM means accidents.
For ASD / Sensory-Sensitive Children
Test light levels — some children need dimmer illumination, others need bright to orient. Find the balance. A scent-free environment from bedroom to bathroom reduces sensory overload that can interfere with waking and navigation.
Materials
Motion-sensor lights ×3–4 | Commode (if needed) | Bedside urinal (boys) | Non-slip slippers

Material 6 of 9
₹500–2,000/month
👕 ABSORBENT DIGNITY PRODUCTS | Protection cannot cost dignity.
The goal is not "diaper." The goal is underwear-style, age-appropriate protection that the child will actually wear without shame — because shame worsens bedwetting by increasing anxiety and stress hormones that physiologically interfere with arousal and bladder control.
Product Options by Age/Preference
- Youth pull-up style (looks/feels like underwear)
- Absorbent boxer briefs (older boys — age-appropriate design)
- Reusable absorbent underwear (normalizing, eco-friendly)
- Absorbent pads that insert into regular underwear (maximum dignity)
- Teen-sized options with minimal bulk
Family Protocol
- Involve child in choosing products — control reduces shame
- Frame as: "This is temporary. It keeps the bed dry while your brain learns."
- NEVER use as punishment or express disappointment when worn
- Store discreetly — child's dignity in changing process matters
- Change immediately upon waking — skin health is non-negotiable
Skin Safety
Change wet products immediately to prevent skin breakdown. Use gentle unscented wipes. Allow air exposure when possible. Reusable options significantly reduce ongoing monthly cost.

Material 7 of 9
₹0–500
🌅 AROUSAL TRAINING | The brain can learn to wake. But it needs practice.
Most children with bedwetting are profoundly deep sleepers. The arousal response — waking in response to an internal signal — is a learned and conditionable response. Practice during waking hours trains the brain for nighttime. And the best part: the drills cost nothing.
1
Daytime Wake-Up Drills (3× per week — make it a game)
Child lies in bed. Parent sounds alarm. Child practices: alert → sit up → stand → walk to bathroom → touch toilet. Reinforce immediately: "You did it! That's exactly what your brain is learning to do at night."
2
Night Protocol — When Alarm Sounds
Parent responds immediately. Full waking confirmation: eyes open, oriented, standing. Walk to toilet together. Void completely. Return to bed, reset alarm, brief reinforcement. Record in diary.
3
For Deep Sleepers / ASD
Place alarm unit across the room (child must get up to silence it). Use multi-mode alarm (sound + vibration simultaneously). Vibrating alarm watch on wrist — direct physical sensation bypasses auditory deep sleep.
Materials: Alarm clock for daytime drills | Practice log | Vibrating alarm watch (optional, if needed for deep sleepers or sensory-sensitive children) | Cost: ₹0–500

Material 8 of 9
₹200–600
⭐ REWARD SYSTEMS | Reward what they CAN control. Dry nights will follow.
The ABA Principle: Bedwetting is NOT under voluntary control. Punishing wet nights increases shame, anxiety, and stress — all of which worsen bedwetting. What the child CAN control is cooperation with treatment. Reward that, and dry nights become the natural outcome.
Behavior | Reward Type | |
Wore alarm to bed | ⭐ sticker | |
Woke up when alarm sounded | ⭐⭐ sticker | |
Got up and went to toilet | ⭐⭐⭐ sticker | |
Followed full bedtime routine | ⭐ sticker | |
Dry night | 🌟 Special star + verbal celebration |
Parent Script for Wet Morning:"No problem. The alarm is working. Your brain is learning. Let's set up for tonight." — NEVER penalize wet nights. Simply note them without comment. This single script change transforms the morning experience for both parent and child.
NEVER: Express disappointment about wet nights | Withdraw rewards for wet nights | Compare to siblings or other children | Use bedwetting as leverage for other behaviors.
Material 9 of 9
₹1,000–5,000 per consultation
🏥 PROFESSIONAL SUPPORT | Right diagnosis. Right treatment. Right timeline.
Nocturnal enuresis has three distinct physiological mechanisms — arousal deficit, nocturnal polyuria, and reduced bladder capacity. Each requires a different primary treatment. Without assessment, families often spend weeks on the wrong approach for their child's specific presentation.
🔴 Seek IMMEDIATE Evaluation
Pain with urination | Blood in urine | Fever + urinary symptoms | Sudden excessive thirst | Swelling in face/legs
🟡 Seek PROMPT Evaluation
Secondary enuresis (new wetting after 6+ dry months) | Daytime symptoms + nighttime wetting | Age 7+ with nightly wetting | Not improving after 3 months | Significant emotional distress
🟢 ROUTINE Assessment
Age 5+ with regular bedwetting | For assessment before choosing treatment approach — bring completed 2-week diary, wet/dry calendar, and questions list
Professional Team
- Pediatrician: First evaluation, rule out medical causes, prescribe desmopressin if needed
- Pediatric Urologist: Complex or non-responding presentations
- Child Psychologist: Secondary enuresis, anxiety assessment
- Occupational Therapist: Interoception, sensory processing, ASD-related factors
- BCBA/ABA Therapist: Behavioral protocol design, alarm compliance
Pinnacle Blooms Network®
Our NeuroDev Pediatrics team, OT specialists, and BCBA network are trained in the intersection of bedwetting and developmental differences.
📞9100 181 181 — FREE | 24×7 | 16+ languages

Every family — regardless of income — can begin tonight. Here is how.
This page follows the WHO Nurturing Care Framework's mandate for context-specific, equity-focused interventions applicable across all economic levels. Every material has a zero-cost alternative — because a child's dry nights should not depend on household income.
Material | Purchased Version | DIY / Zero-Cost Version | |
Bedwetting Alarm | ₹2,000–8,000 wearable sensor | Loud alarm clock across room at predicted wetting time; parent does scheduled lifting as bridge | |
Waterproof Protection | Breathable mattress encasement | Plastic tablecloth + cotton sheet layered; hospital disposable pads | |
Voiding Diary | Printed tracker | School notebook with simple columns; hand-drawn grid | |
Bladder Training | Visual schedule poster | Handwritten schedule on paper; kitchen timer for intervals | |
Nighttime Lighting | Motion-sensor lights | Torch/phone left on low near path; glow stickers on floor | |
Absorbent Products | Youth pull-ups | Folded cloth with waterproof outer layer; repurposed cloth nappy | |
Arousal Training | Vibrating watch | Loud clock across room; parent-check at predicted wetting time | |
Reward Chart | Printed sticker chart | Hand-drawn calendar; dried lentils as tokens in a jar |
Non-Negotiable: Bedwetting alarm conditioning cannot be fully replicated without some form of moisture-detection device. For families unable to purchase, ask your pediatrician about loan programs or NGO support schemes in your area. Research: PMC9978394 | WHO NCF Handbook (2022)

Read before starting. These are the lines you do not cross.
🔴 STOP — Do Not Proceed
- Blood in urine
- Pain with urination at any time
- Signs of urinary tract infection (fever, burning, frequency with small amounts)
- Child is in active emotional crisis or extreme distress about bedwetting
- Secondary enuresis with suspected medical cause — seek evaluation first
- Alarm causing severe anxiety rather than gradual conditioning
🟡 MODIFY — Proceed with Adjustment
- Child with autism who is noise-sensitive: trial vibration-only mode first
- Child with trauma history: involve therapist before starting alarm
- Child refusing to participate: do not force — establish buy-in first
- Constipation present: address bowel function before bladder training
- Child very distressed about wearing alarm: start with pad sensor, not wearable
🟢 PROCEED
- Child is generally willing (even if reluctant)
- No active medical symptoms
- Parent has realistic 12–16 week commitment
- Bedtime routine established and consistent
- Daytime behavior baseline stable
Child State Requirements Before Each Night: Not ill (fever, infection active) | Adequate fluid intake throughout day (restriction worsens, not helps) | Bowels moved today or recently (constipation directly worsens bedwetting) | Emotionally regulated — not in active meltdown or acute distress
ACT III — THE PROTOCOL
Prepare the environment. Session failures are almost always environmental.
Before the first night of protocol, walk through this checklist completely. Environmental preparation is not optional — it is the first therapeutic act. A prepared room reduces nighttime friction, protects dignity, and makes every alarm response faster and more effective.
1
Alarm Setup
Sensor attached to underwear / pad in correct position. Alarm unit placed at distance that requires waking to silence it.
2
Path Clear
Path to bathroom clear of all obstacles. Motion-sensor lights tested and working. Bathroom door open, nightlight on.
3
Protection Ready
Waterproof protection system in place (layered). Spare pajamas and sheet set within reach. Diary/tracker on bedside table.
4
Reinforcement Visible
Reward chart on wall, visible from bed. Parent alert system in place — parent's door open or shared alarm monitor for first 4 weeks.
Environmental Recommendations: Temperature comfortable (not too hot — sweating disrupts sleep and increases discomfort) | Sound quiet enough that alarm will be audible | No TV or gaming devices on in bedroom

60-second pre-session check. The best night starts right.
Indicator | GO ✅ | MODIFY ⚠️ | POSTPONE ❌ | |
Child is generally calm and regulated | ✅ | — | ❌ If active meltdown | |
No fever or active illness | ✅ | — | ❌ If unwell | |
Had adequate fluids today | ✅ | — | ❌ If heavily restricted | |
Bowels moved today/recently | ✅ | ⚠️ Monitor | ❌ If severely constipated | |
Child has been explained the process | ✅ | ⚠️ Brief reminder | ❌ If completely refusing | |
Alarm battery checked | ✅ | — | ❌ If not working | |
Evening routine completed | ✅ | — | — |
5–7 YES
Full protocol — proceed with confidence
3–4 YES
Modified protocol — skip alarm, do double-void routine only
Fewer than 3 YES
Postpone tonight — maintain protection system and diary only
"The best session is one that starts right. A missed night is not failure — it is clinical wisdom."

STEP 1 of 7
Every protocol begins with invitation, not command.
"Hey [name], time for our bedtime routine. Tonight we're going to set up your alarm. Remember — every time that alarm goes off and you wake up, your brain is getting stronger. You're training it. Want to set it up together?"
Body Language Guidance
- Calm, matter-of-fact tone (not tense or anxious)
- Sit at child's level
- Express confidence, not worry
- If child hesitates: "That's okay. We'll just set it up and see how tonight goes."
What Acceptance Looks Like
- Child moves toward bed
- Child allows sensor to be attached
- Any level of participation — even passive tolerance is acceptable
What Resistance Looks Like & How to Modify
- "I don't want the alarm" → "Okay, we'll use the pad version tonight. Same process."
- "I'm tired" → "That's perfect — you're going to sleep really well. Let's just get the alarm on."
- Refusal → Do not force. Use protection system only. Record in diary. Discuss tomorrow.
Timing: 5–10 minutes as part of regular bedtime routine

STEP 2 of 7
The alarm is on. The brain is ready. Sleep begins.
"The alarm is set. If it goes off tonight, I'll come in and we'll do our routine together. Remember — the alarm going off is GOOD. It means it's working. Just wake up fully when you hear it."
1
Double void
Toilet → wait 5 minutes → toilet again. This is the most important step of the entire pre-sleep protocol.
2
Sensor check
Confirm sensor position and alarm activation. Test briefly if uncertain.
3
Review plan
"When the alarm sounds — you wake up, you get up, you go to toilet."
4
Positive close
Brief reinforcement of effort (not outcome): "You set up the alarm. That takes courage."
Child Response Monitoring: Engagement (child participates actively) → excellent, reinforce enthusiastically. Tolerance (child allows process passively) → acceptable, maintain calm positive tone. Avoidance (child withdraws) → reduce demands, protect dignity, try tomorrow.

STEP 3 of 7
When the alarm sounds — this is the moment that matters.
The alarm activation is the core therapeutic event. Every response — however imperfect — is a conditioning trial. Seven clean responses are worth more than twenty half-awake ones. Be present. Be consistent. Be calm.
Hear alarm → Move immediately
Within 30 seconds. Do not wait.
Ensure full waking
Child must be standing, oriented, not just turning off alarm. Eyes open.
Walk together to bathroom
"Up you go. Bathroom. Let's go." Calm, not frantic.
Child voids completely
Or tries — sometimes alarm fires early, little to void. Complete the protocol regardless.
Return, reset, reinforce
Help change if needed. Reset alarm. "You did it. That's your brain learning."
❌ Child turns off alarm while asleep
→ Arm unit on wrist, not beside head; parent responds faster
❌ Child refuses to get up fully
→ Do not carry — insist on walking; this is the therapeutic act
❌ Parent frustrated/angry
→ Remove emotion from protocol; this is physiological training, not a behavior choice

STEP 4 of 7
Consistency over 12–16 weeks is the treatment. Not one night.
Week 1–4
Parent assists every alarm response. Child participates as able. Conditioning begins invisibly.
Week 5–8
Child leads, parent supports from doorway. First dry nights may appear.
Week 9+
Child independent, parent monitors from own room. Dry nights increasing.
Post-14 Dry Nights
Overlearning phase begins. Extra fluids before bed for 2 more weeks — consolidates learning.
Week 16–24
Total typical program for durable response. Gradual alarm reduction over 2–3 weeks.
Satiation/Burnout Signs
- Child becoming increasingly resistant to alarm
- Parent exhaustion threatening consistency
- No progress indicators after 12 weeks of consistent use
If Burnout Is Emerging
Brief 1-week pause (maintain protection only), reassess, restart. Note: pause extends the overall timeline.
"3 good alarm responses > 10 half-awake ones."

STEP 5 of 7
Timing matters more than magnitude. Immediate. Specific. Genuine.
For Wet Nights (alarm activated — this is progress)
"You heard the alarm. You woke up. You walked to the bathroom. That is exactly what we're training. Put your star on the chart for waking up."
→ Sticker for: alarm worn, waking response, bathroom visit
For Dry Nights (target outcome)
"You stayed dry all night! Your brain did it. That is a big deal."
→ Special star + small token reward + enthusiastic celebration
Reinforcement Menu (ABA Canon)
Verbal
Specific and immediate: "You woke up to the alarm — that's amazing"
Physical
High five, hug — child's preference always
Token
Sticker, stamp, coin toward prize jar
Activity
Extra 10 minutes of preferred activity next day

STEP 6 of 7
The bedtime routine IS the therapy. Consistency of environment = consistency of neural conditioning.
6:30 PM onwards
Reduce fluid intake (normal reduction, not severe restriction). Calm activities only — no screens, vigorous play.
30 min before sleep
Bath/shower (body awareness, sensory regulation). First void (scheduled). Put on absorbent underwear/alarm sensor.
5–10 min before sleep
Double void (most important step). Alarm sensor check. Light reading or quiet activity.
Lights out
Positive bedtime conversation (30 seconds): "Tomorrow, tell me how it went. I'm proud of you for doing the routine."
If Child Resists the Routine
- Visual schedule on wall (reduces negotiation)
- First-Then: "First routine, then [preferred activity/story]"
- Consistent time every night (circadian rhythm supports bladder hormones — vasopressin secretion is time-sensitive)
Why Consistency Matters at the Neural Level
Vasopressin (antidiuretic hormone) secretion is regulated by circadian rhythm. A consistent sleep schedule trains the body clock to produce more vasopressin at the right time — reducing nighttime urine volume physiologically, alongside behavioral conditioning.

STEP 7 of 7
60 seconds in the morning. Data that transforms outcomes.
Pattern recognition is powerful. After 2 weeks, the diary reveals whether the alarm is firing earlier (brain learning), wet spots are smaller (capacity increasing), and dry nights are clustering (conditioning solidifying). These micro-signals are invisible without data.
Field | What to Record | |
Date | Today | |
Night result | Wet / Dry / Alarm activated | |
Response quality | Woke immediately / Needed assistance / Slept through |
📥 PDF Download
E-502 Printable 12-Week Tracking Calendar — print and use immediately tonight
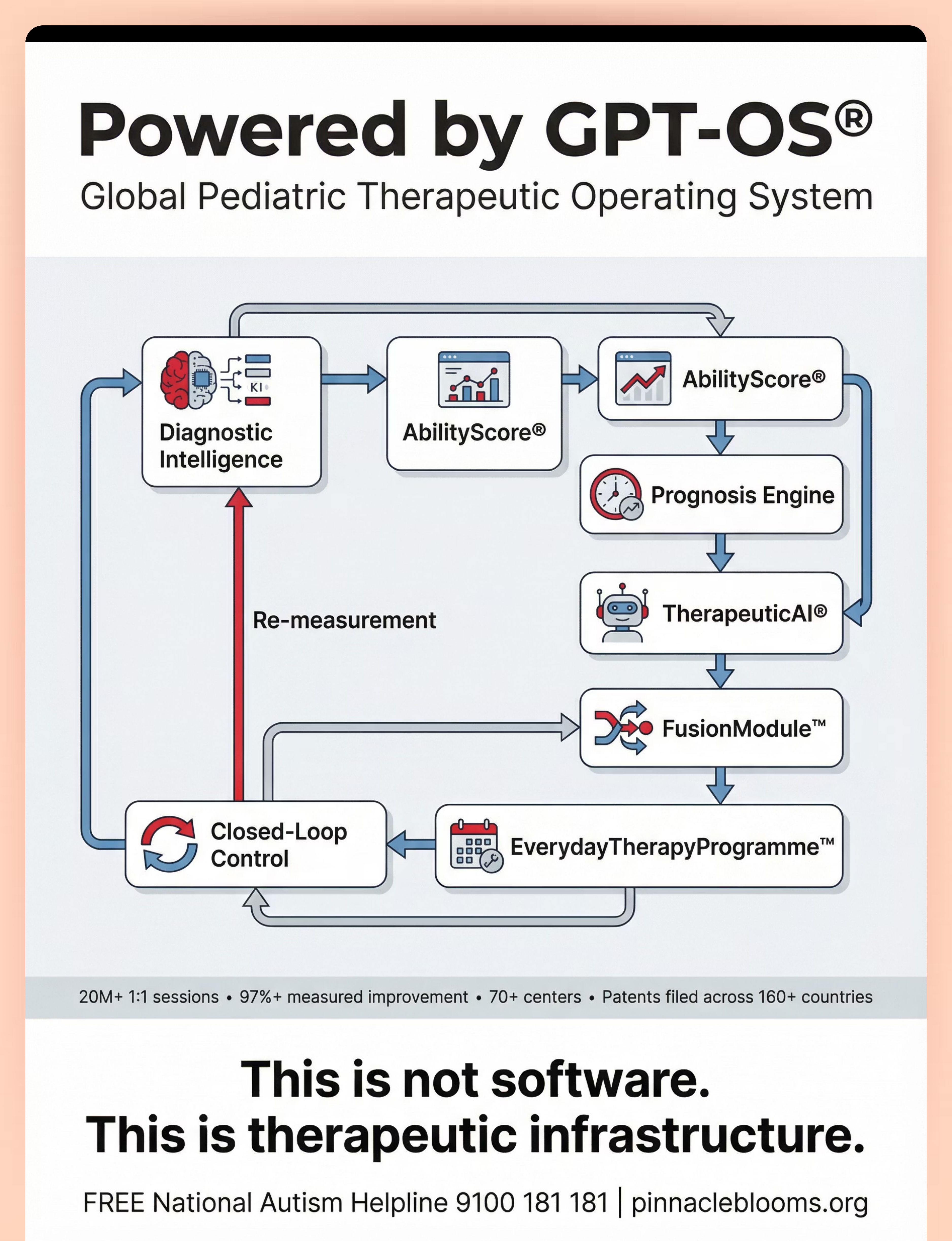
📱 GPT-OS® Integration
Log directly in GPT-OS® app → data feeds TherapeuticAI® → personalized protocol adjustments → Prognosis Engine updates
📊 Weekly Summary
Every Sunday: count wet nights this week + note any changes in wetting time or wet spot size

Every roadblock has a clinical response. Here are the most common ones.
🔍 "My child sleeps through the alarm completely"
Move alarm unit to across-room position. Switch to vibration + sound combined mode. Increase alarm volume. Parent assists waking in first 4 weeks (expected). Consider vibrating wrist alarm. This is normal in weeks 1–4.
🔍 "We're 6 weeks in and nothing is changing"
Review protocol fidelity: Is child fully waking each time? Is alarm activating consistently? Check sensor placement. Review voiding diary for daytime patterns. Check for constipation. If all correct — normal timeline: 65–75% succeed by week 16.
🔍 "My child refuses to wear the alarm anymore"
Involve child in choosing alarm type. Switch to pad sensor. Take 3-night break. Revisit rewards for compliance. If sustained refusal — consult OT for sensory sensitivity component. 📞 9100 181 181
🔍 "We achieved 14 dry nights and then regression occurred"
Normal without overlearning phase. Implement overlearning: extra fluids before bed, continue until 14 more consecutive dry nights. Relapse rate reduced significantly with this step — do not skip it.
🔍 "My child with autism won't tolerate the alarm sensation"
Desensitize to alarm sound/vibration during daytime (play it briefly, reward tolerance, increase exposure). Vibration-only mode during desensitization. OT support for sensory tolerance building via Pinnacle FusionModule™.
🔍 "Doctor says just wait — they'll grow out of it"
Valid approach. Also valid: bedwetting alarm at age 7+ accelerates resolution significantly. Share ICCS guidelines with your pediatrician. Request urology referral if no progress by age 8–9. The choice is yours — informed.
No two children wet the same way. No two protocols are identical.
For Younger Children (5–7 years)
- Parent fully manages alarm response — child participates as able
- Reward system more frequent and tangible
- Shorter evening routine — simpler double void steps
- More emphasis on mattress protection, less pressure on alarm compliance
For Older Children/Teens (10–15 years)
- Maximum privacy in protocol execution
- Child manages own alarm, tracks own data
- Frame as "brain training" not "bedwetting treatment"
- Social motivation: sleepovers, camps as explicit goals
- Silent vibration mode only — no audible alarm preferred
For Children with Autism
- Visual schedule for every step of bedtime routine (laminated card)
- Social story about "brain learning" for arousal training
- Interoception sessions with OT alongside alarm training
- Sensory-modified alarm (vibration preferred over sound)
- Longer timeline expectation: 16–24+ weeks is normal
- FusionModule™ ASD-specific protocol via Pinnacle
For Children with ADHD
- Highly structured external routine management (parent-led)
- More frequent reward delivery
- Data tracking made visual and interactive
- Alarm compliance tracked as separate behavioral goal
ACT IV — PROGRESS
Progress in weeks 1–2 looks nothing like you expect. Here is what it actually looks like.
✅ What You WILL See
- Alarm activating (this means it's working)
- Wetting continuing (expected — conditioning takes time)
- Child possibly sleeping through alarm (normal)
- Parent fatigue increasing (expected — this is real commitment)
📈 What Counts as Progress
- Child wears alarm without major resistance
- Child walks to toilet when assisted (even groggily)
- Alarm is activating consistently (sensor working)
- No regression in daytime behavior or emotional state
"Weeks 1–2 are the hardest. Nothing seems to be working. The nights are disrupted. You may wonder if it's worth it. It is. The conditioning is happening at the neural level — invisible to you, but measurable later. Most families who quit do so in week 3. Don't."
If your child tolerates the alarm for one more second than last week — that is real, measurable neurological progress. The brain is building the pathway. Trust the timeline.

The neural pathway is forming. Here are the signs most parents miss.
Week 3–4 brings consolidation signs that are easy to overlook if you're only watching for dry nights. Shift your attention to these subtler, deeply meaningful indicators — they are the true evidence that conditioning is working.
Child waking faster after alarm sounds
vs. sleeping through in weeks 1–2. The arousal threshold is lowering.
Wet spots beginning to appear smaller
The alarm is activating earlier in the void — the brain is responding sooner.
First dry night(s) appearing
Celebrate — but do not create pressure around them. One dry night is not the target; 14 consecutive is.
Child begins reporting "I felt like I needed to go last night"
This is the arousal threshold lowering. The signal is getting through. This is the moment everything changes.
Parent Milestone
You may notice YOUR confidence increasing. The routine feels more automatic. The morning conversation shifts from shame to data. This is the family system adapting alongside the child — both growing.
When to Increase Intensity
If child is consistently waking to alarm: increase daytime arousal drills to 3× per week. If voiding diary shows consistent late-night wetting: explore desmopressin with your pediatrician for those specific nights.

14 consecutive dry nights. This is a neurological achievement. Celebrate it properly.
"Your brain learned. You did that."
1
Family Acknowledgment
Make it real and meaningful. Child's choice of celebration (within reason). Verbal articulation: "Your brain learned. You did that."
2
Document the Moment
Photo with reward chart. Note the date. Share with grandparents if child wishes — builds the community of celebration.
3
The Overlearning Phase (critical — do not skip)
After 14 consecutive dry nights: have child drink extra fluids before bed for 2 weeks, continuing alarm protocol. This consolidates learning under higher bladder load — significantly reducing relapse rates.
4
What Comes Next
Gradual alarm reduction over 2–3 weeks (not sudden removal). Transition from absorbent products (child decides timeline for dignity). First sleepover planning. Maintenance monitoring for 3 months.
These signals override the protocol. They are not setbacks. They are information.
1
🔴 Stop Protocol Immediately
- Any urinary symptoms: pain, burning, blood, frequency with small volumes (UTI possible)
- Sudden excessive thirst + urination (new-onset diabetes)
- Child in acute psychological crisis related to bedwetting
- Any physical harm from alarm or protocol (skin breakdown, fear response)
2
🟡 Pause and Evaluate
- Secondary enuresis onset (was dry, now wetting again after 6+ months) — medical cause must be ruled out first
- No progress after 16 weeks of fully consistent use — specialist referral
- Emotional distress escalating despite consistent positive approach — psychology referral
- Constipation severely worsening — bowel treatment before bladder
3
🟢 Continue With Adjustment
- Occasional regression during illness or high stress — temporary, resume when stable
- Child losing motivation — refresh reward system, involve child in redesign
- Parent fatigue threatening consistency — enlist second caregiver, maintain nightly protection at minimum

You already know the materials. Here are techniques that use them.
The voiding diary, reward chart, and alarm from E-502 form the foundation for multiple related techniques. You already own the essentials.

E-503: Daytime Wetting Materials
Shared materials: Diary, bladder training, reward chart. Core difficulty level.
E-504: Toilet Training Resistance
Shared materials: Visual schedules, reward systems. Core difficulty level.

E-505: Toileting Anxiety
Shared materials: Reward systems, OT sensory support. Intermediate difficulty.

E-500: Chronic Constipation
Shared materials: Diary, medical coordination. Foundation level.
Dry nights are one milestone on a much larger developmental journey.
This Technique's Domain Contribution
E-502 contributes to Domain E (GI/Toileting), Domain L (Daily Living Skills), and feeds Domain B (Social Communication — sleepover participation) and Domain C (Emotional Regulation — shame reduction, confidence building).
GPT-OS® Full Profile
To see your child's complete developmental profile across all 12 domains — including their AbilityScore® baseline, active technique recommendations, and progress across Readiness Indexes — connect via GPT-OS®.
📞9100 181 181 | pinnacleblooms.org | Request AbilityScore® Assessment

ACT V — COMMUNITY
From the families who came before you.
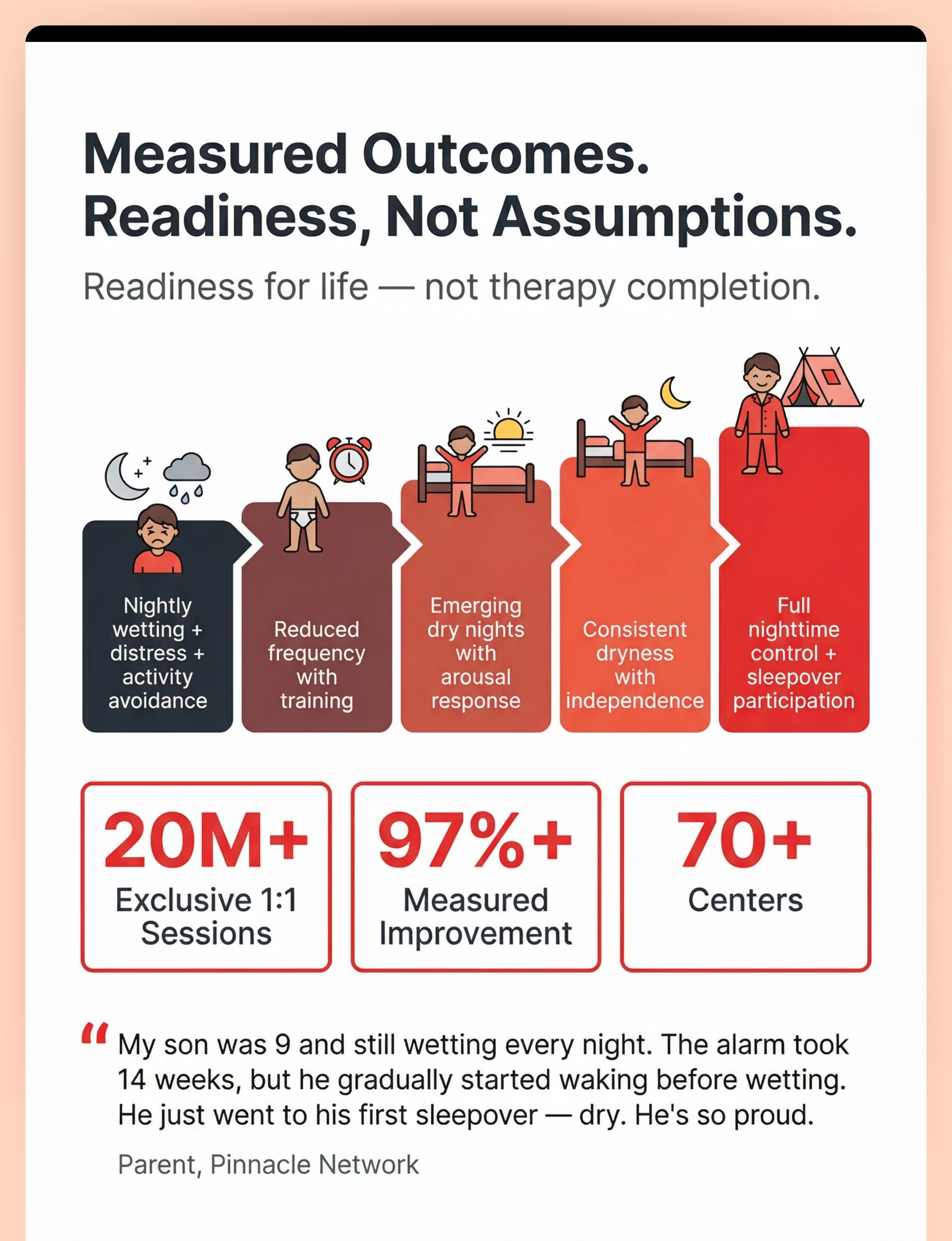
"My son was 9 and still wetting every night. We'd tried limiting fluids, waking him up at 11 PM — nothing worked consistently. Our Pinnacle OT recommended the bedwetting alarm and showed us exactly how to use it. It took 14 weeks of consistent use, but he gradually started waking before the alarm sounded. Then he started sleeping through dry. He just went to his first sleepover — dry. He came home and said, 'Mum, I did it.' I cried for an hour."
— Parent, Pinnacle Hyderabad Center(Illustrative case; outcomes vary by child profile, enuresis type, and treatment compliance.)
"We had tried everything the internet suggested. Then our Pinnacle therapist identified that our daughter's autism and deep sleep patterns were creating a compound challenge that needed both OT interoception work and the alarm. Three months later — dry nights are the norm. The alarm just confirmed what her body was already learning."
— Parent, Pinnacle Bengaluru Center(Illustrative case.)
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
You are not navigating this alone.
Connect with thousands of Indian families navigating nocturnal enuresis across the Pinnacle network — sharing what worked, what didn't, and how they kept going through the 14-week journey. Community accountability is one of the strongest predictors of protocol completion.
WhatsApp Community
Pinnacle Parents | GI & Toileting Support Group — active daily discussion, peer tips, milestone celebrations
Pinnacle App
Family Connect module — track sessions, connect with your therapy team, access E-502 digital resources
Online Community
pinnacleblooms.org/community — forums, guides, and peer support moderated by consortium coordinators
"Put the alarm unit on the other side of the room from week 1 — game changer."
"The overlearning phase is the secret most families skip. Don't skip it."
"We involved our son in choosing the alarm. That 30 minutes of autonomy transformed his buy-in."
📞9100 181 181 — FREE | 24×7 | 16+ languages. For families who need direct professional guidance right now.
70+ centers across India. Specialist support within reach.
Whether you are in a major metro or a smaller city, Pinnacle Blooms Network® has specialist pediatric therapy support within reach — and teleconsultation available for families outside major centers.
Service | Discipline | Details | |
Nocturnal Enuresis Assessment | NeuroDev Pediatrics | Medical evaluation, mechanism diagnosis — arousal deficit vs. nocturnal polyuria vs. reduced bladder capacity | |
Alarm Training Guidance | OT + ABA | Protocol setup, sensor fitting, compliance support, troubleshooting | |
Interoception Training | OT | Body signal awareness specifically for ASD/ADHD presentations | |
Behavioral Protocol Design | BCBA | Structured alarm compliance program with reinforcement schedule | |
Parent Coaching | Multi-disciplinary | Home implementation support, script coaching, data interpretation | |
AbilityScore® Assessment | GPT-OS® | Full 12-domain developmental baseline for your child |
📞 Call
9100 181 181 — FREE, 16+ languages, 24×7
🌐 Book Online
pinnacleblooms.org/book
📧 Email
care@pinnacleblooms.org
💻 Teleconsult
Full online consultation available for families outside major centers
Consistency across caregivers multiplies impact by 3–5×.
When grandparents, school teachers, and second caregivers understand the protocol and respond consistently, the conditioning is reinforced across every environment — not just at home with one parent at night. Share this page widely.
📥 Family Guide PDF
E-502 Nighttime Wetting: What Every Caregiver Needs to Know — 1-page, print-ready
📥 12-Week Tracking Calendar
Print and use immediately tonight — structured grid for every night of the protocol
📥 Grandparent Simplified Version
Non-clinical, warm, practical one-pager — explains the protocol without medical terminology
📥 School Communication Template
For teachers and school counselors managing social anxiety around bedwetting at school
"Explain to Grandparents" Key Messages:
1. Bedwetting is not laziness — the brain is a deep sleeper that doesn't wake to signals.
2. No punishment, ever — shame makes bedwetting worse physiologically.
3. The alarm is the treatment — it is training the brain, not just catching accidents.
4. Celebrate effort (waking up, routine compliance) — not just dry nights.
School Communication Template: "[Child] is currently completing a 12-16 week bedwetting alarm training program. Please note: [Child] may be managing temporary fatigue from disrupted nights. Please avoid any reference to this condition in class. If [Child] needs bathroom access without delay, please accommodate. Thank you for your support."

ACT VI — FAQ & CLOSE
Questions every family asks. Answered by the Pinnacle consortium.
My child is 8 years old and still wetting every night. Is this normal?
Yes — at age 8, approximately 8–10% of children still experience regular bedwetting. It is more common in boys and has a strong genetic component. It does NOT indicate a character flaw, laziness, or emotional problem. Active intervention with a bedwetting alarm is recommended from age 7 onwards for persistent bedwetting.
How long does the bedwetting alarm really take to work?
Realistically: 12–16 weeks of nightly consistent use for most children. Some show improvement by week 6–8; others need the full 16 weeks. The first 4 weeks often show no visible change — this is the neural conditioning phase. Do not stop before week 12. Success rate: 65–75% with full protocol compliance.
My pediatrician says to just wait. Why should I try the alarm?
Waiting is valid — most children do outgrow bedwetting. However, bedwetting at age 8–9 carries real psychological cost: missed sleepovers, social anxiety, shame. The alarm accelerates the natural process with a 65–75% success rate and no medication side effects. ICCS guidelines recommend alarm therapy as first-line treatment from age 7.
My child with autism refuses to wear the alarm. What do I do?
Start with desensitization: play the alarm briefly during the day, reward tolerance, gradually increase exposure. Use vibration-only mode initially. Try pad sensor instead of wearable. Involve an OT trained in sensory desensitization. FusionModule™ at Pinnacle integrates OT sensory work with alarm compliance. 📞 9100 181 181
Preview of 9 materials that help with nighttime wetting Therapy Material
Below is a visual preview of 9 materials that help with nighttime wetting therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

More questions answered.
Does restricting fluids at night help?
Moderate reduction after 6 PM is appropriate. Severe restriction is counterproductive — it concentrates urine, may cause constipation, and doesn't address the arousal mechanism. Adequate daytime hydration (8 glasses) is essential for bladder health and effective training.
My child was dry for 6 months and now wets again. Is this different?
Yes — this is secondary enuresis and requires medical evaluation to rule out: UTI, new-onset diabetes, constipation, or significant psychological stress/trauma. Do not start alarm training until medical causes are excluded. 📞 9100 181 181 for immediate guidance.
Can I use desmopressin medication instead of the alarm?
Desmopressin works well for children with nocturnal polyuria and is very useful for special occasions (sleepovers, camps) while alarm training is in progress. However, relapse rates when medication stops are higher than alarm therapy. Most urologists recommend alarm training as the primary treatment with desmopressin as adjunct.
My child is having great success — when can we stop the alarm?
After 14 consecutive dry nights, complete the overlearning phase (extra fluids before bed for 2 weeks, continue until 14 more dry nights). Then gradually reduce alarm use over 2–3 weeks — do not stop abruptly. Monitor for 3 months with a brief diary if any regression appears.
Didn't find your answer? 💬 Ask GPT-OS® | 📞9100 181 181 FREE | 📧 care@pinnacleblooms.org