"Family Gatherings Become Torture for Your Child."
The moment you walk into a room with multiple conversations happening, you watch the color drain from their face. Their eyes dart around frantically. Their hands go to their ears. They start humming or making noises — anything to block out what's coming in. Or they shut down completely, retreating somewhere inside themselves where it's quieter.
It's not that they don't want to be there. It's not social anxiety. It's not rudeness. Their brain literally cannot separate the voices. Everything hits them at the same volume, with the same intensity, all at once.
You are not failing. Your child's nervous system is speaking. And there are 9 materials that can help.
Pinnacle Blooms Consortium® — Validated by SLP • OT • BCBA • SpEd • NeuroDev
Sensory Processing & Auditory Challenges — Episode 53
Age Band: 3–15 years
Auditory Processing | Sensory Filtering

You Are Among Millions.
Millions of families worldwide navigate this exact challenge. In India alone, with an estimated 2+ million children with ASD, auditory overwhelm in multi-speaker environments is one of the most reported functional barriers to family life, education, and community participation. You are not alone — and this is not your child's fault.
80%
Sensory Difficulties
Children diagnosed with autism display sensory processing difficulties, including auditory filtering challenges. Source: PRISMA Systematic Review, 2024 (PMC11506176)
1 in 36
U.S. Children with ASD
Children in the U.S. are identified with autism spectrum disorder — auditory processing challenges are among the most functionally limiting. Source: CDC MMWR, 2023
5–7%
APD in Schools
School-age children have clinically significant auditory processing disorder affecting classroom learning. Source: American Academy of Audiology

The Cocktail Party Effect — And Why Your Child Doesn't Have It
Your Child's Auditory Processing
ALL voices arrive at equal intensity. No filtering. A wall of undifferentiated sound — every voice, every scraping chair, every humming fan demanding attention simultaneously.
There is no "background." Everything is foreground.
Typical Auditory Processing
Most people have an automatic auditory filter called the "cocktail party effect." Your brain naturally suppresses irrelevant sounds while amplifying the voice you're attending to. You don't even know it's happening — it's effortless.
Your child's brain doesn't do this automatically. The auditory cortex and its connections to attention networks process every incoming sound with equal weight.
"This is a wiring difference, not a behavior choice. Your child cannot 'try harder to focus.' There is no internal volume dial for background noise."
Frontiers in Integrative Neuroscience (2020): Comprehensive framework establishing neurological basis for sensory processing differences in ASD. DOI: 10.3389/fnint.2020.556660
A Developmental Waypoint — Not a Permanent Destination
The ability to filter and prioritize auditory information develops throughout childhood — but for children with autism, ADHD, sensory processing disorder, or specific auditory processing disorders, this development is significantly different. Research demonstrates this doesn't resolve with maturation alone. The WHO Care for Child Development (CCD) Package, implemented across 54 countries, emphasizes that targeted intervention — not waiting — is the evidence-based approach.
0–12 Months
Basic sound localization and voice recognition emerging.
1–3 Years
Auditory discrimination developing; early filtering begins.
3–5 Years ⚠️ CHALLENGE ZONE
Auditory filtering demands increase as child enters group settings. Children with processing differences show clear difficulty here.
5–8 Years
Classroom demands expose filtering deficits. FM systems and accommodations become critical.
8–12 Years
Self-advocacy skills can develop. Technology and strategies become internalized.
12+ Years
With appropriate support, functional participation in multi-speaker environments is achievable.
"Your child is here. Here is where we're heading. The path forward is specific, measurable, and proven."
References: PMC9978394 | WHO/UNICEF CCD Package (2023) | WHO Nurturing Care Framework
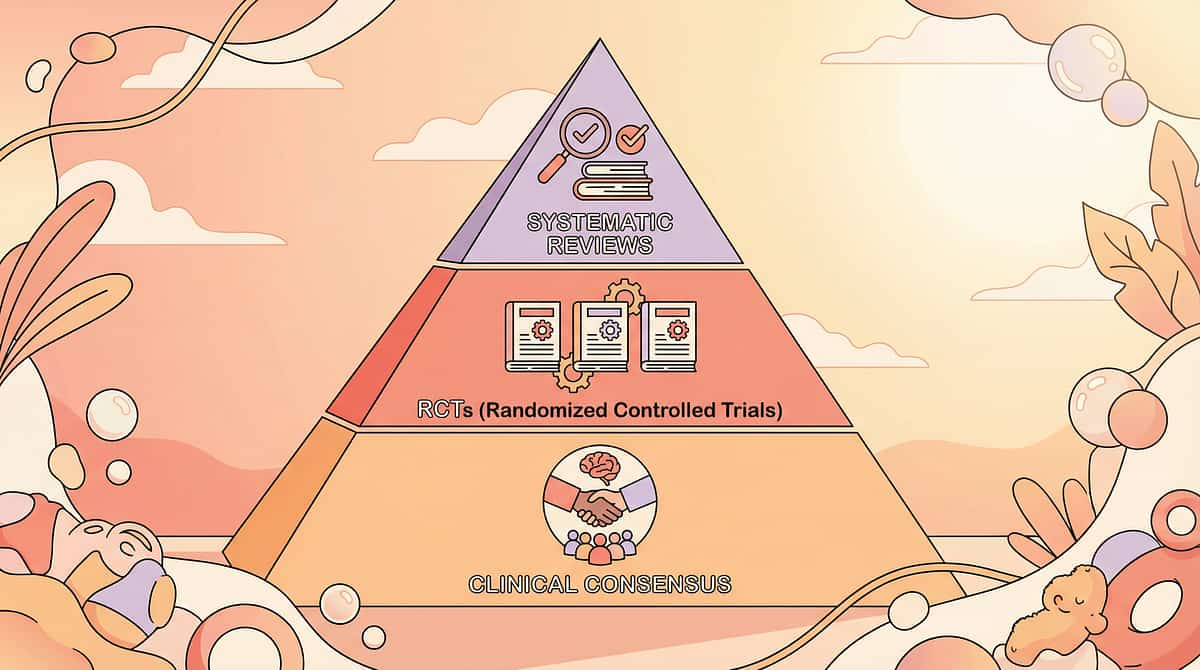
Clinically Validated. Home-Applicable. Parent-Proven.
⬛ Level II Evidence — Systematic Reviews + RCTs + Clinical Consensus
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria for evidence-based practice in ASD. → PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
Sensory integration therapy across 24 studies effectively promotes social skills, adaptive behavior, sensory processing, and motor skills. → PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT (Padmanabha et al., 2019)
Home-based sensory interventions demonstrated significant outcomes in Indian pediatric populations with established safety protocols. → DOI: 10.1007/s12098-018-2747-4
Cuvo & Riva (1980)
Generalization and transfer between comprehension and production is achievable with targeted intervention, suggesting auditory processing abilities can be developed, not just accommodated. → PMC1308134
This technique draws from established auditory processing intervention literature, WHO/UNICEF frameworks, and 20M+ therapy sessions in the Pinnacle Blooms Network. The 9 materials combine environmental modification, assistive technology, compensatory strategies, self-regulation training, and direct auditory skill building — all individually evidence-supported approaches.

Multi-Material Auditory Overwhelm Management Protocol
Parent-Friendly Alias: "The 9-Tool Kit for Surviving Multiple Voices"
A comprehensive, multi-layered intervention approach that combines 9 categories of materials and strategies to help children with auditory processing differences manage environments where multiple people are speaking simultaneously. Rather than a single technique, this is a toolkit approach — reducing auditory input, improving signal-to-noise ratio, providing compensatory channels, teaching self-regulation, preparing for challenging environments, and building underlying skills.
The protocol is designed for home execution by parents and caregivers, with professional guidance for specific components (FM fitting, auditory therapy).
Domain
Auditory Processing | Sensory Filtering | Environmental Adaptation | Self-Regulation
Age Range
3–15 years across all severity levels
Setting
Home + School + Community + Social Events
Frequency
Daily integration — tools available in every environment
This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type
Speech-Language Pathologist (SLP) — Primary Lead
SLPs lead auditory processing assessment and intervention. They evaluate auditory figure-ground ability, recommend FM systems, design auditory training programs, and work on speech-in-noise comprehension. The SLP typically identifies the cocktail party effect deficit and coordinates the multi-material approach.
Occupational Therapist (OT)
OTs address the sensory processing component — evaluating auditory over-responsivity within the broader sensory profile, recommending environmental modifications, and designing self-regulation strategies. The quiet break space, coping cards, and preparation tools often come from the OT's sensory integration framework.
Board Certified Behavior Analyst (BCBA)
BCBAs design the self-advocacy and coping strategy training using ABA principles — teaching the child to recognize early overwhelm signs, request breaks, and use tools proactively. The behavioral approach ensures strategies are reinforced and generalized across environments.
Special Educator (SpEd)
Special educators implement classroom accommodations — FM system use, preferential seating, written backup for verbal instructions, and break access. They coordinate with teachers and develop IEP/504 accommodations ensuring the child's auditory needs are met in educational settings.
Audiologist
Audiologists conduct hearing and central auditory processing evaluations, fit FM systems, recommend appropriate noise-reduction technology, and may deliver auditory training therapy.
NeuroDevelopmental Pediatrician
NeuroDev pediatricians diagnose underlying conditions (ASD, ADHD, SPD) contributing to auditory processing differences, coordinate multidisciplinary care, and monitor developmental progress.
Reference: UNICEF/WHO Nurturing Care Framework adapted for SLPs (2022): DOI: 10.1080/17549507.2022.2141327
Precision Targets — This Isn't a Random Activity
🎯 Primary Target
Auditory Filtering & Figure-Ground Processing — The ability to attend to one auditory stream while suppressing competing background sounds. Observable: Child can follow one conversation while others occur; child remains regulated in multi-speaker environments for increasing durations.
🔵 Secondary Targets
- Self-Regulation in Noisy Environments — Recognize early overwhelm and deploy coping strategies before dysregulation
- Communication in Group Settings — Family conversations, classroom discussions, social interactions
- Auditory Memory and Processing Speed — Retain verbal information when competing signals are present
🟢 Tertiary Targets
- Social Participation and Inclusion — Attending family events, parties, restaurants without avoidance
- Academic Performance — Following classroom instruction and group activities
- Self-Advocacy and Independence — Requesting accommodations, using tools proactively
Reference: PMC10955541 — Meta-analysis: Sensory integration therapy promotes social skills (primary), adaptive behavior (secondary), sensory processing, and motor skills (tertiary) across 24 studies.
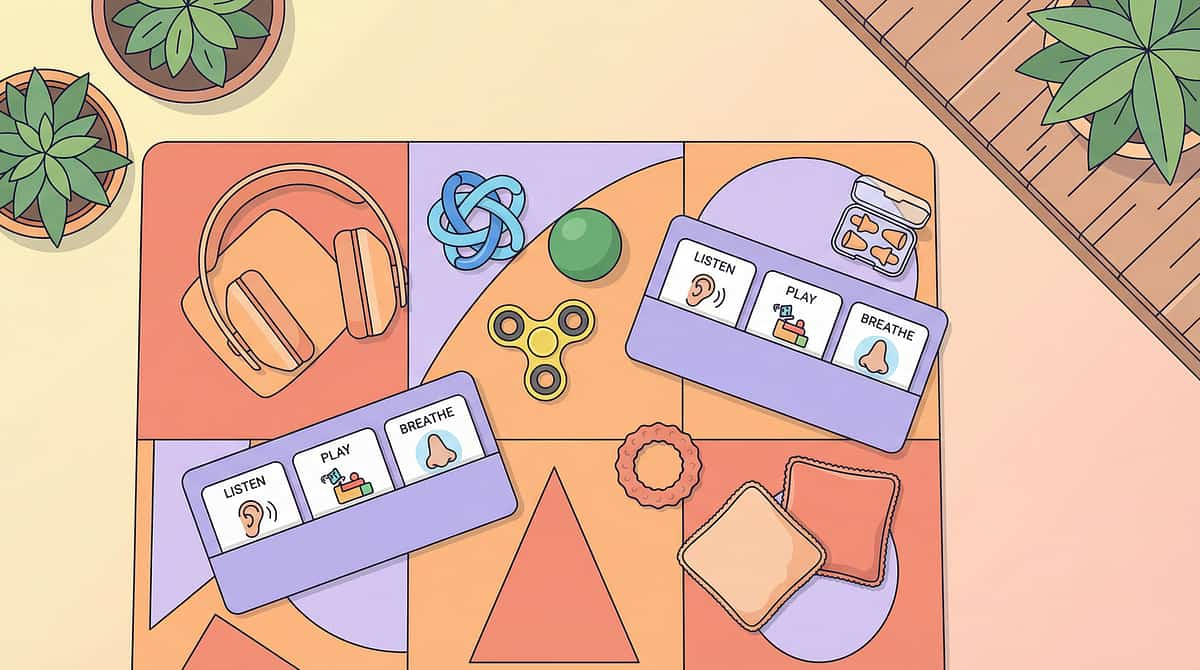
Your 9-Material Toolkit — Everything You Need

1. Noise-Reducing Headphones / Ear Defenders
Canon: Sensory Regulation Tools | ₹800–3,500
Essential Starter Kit

2. Personal FM System / Remote Microphone
Canon: Assistive Technology | ₹15,000–60,000 | Requires audiologist evaluation for fitting

3. Visual Supports & Speaker Identification Tools
Canon: Visual Communication Aids | ₹200–1,000 | DIY-friendly

4. Environmental Acoustic Modifications
Canon: Environmental Adaptation | ₹1000–10,000 | Rugs, acoustic panels, soft furnishings

5. Noise-Canceling Headphones with Selective Input
Canon: Assistive Technology | ₹5,000–25,000 | For older children/teens

6. Self-Regulation & Coping Strategy Cards
Canon: Behavioral Support Tools | ₹200–800 | DIY-friendly
Essential Starter Kit

7. Quiet Break Spaces & Escape Valves
Canon: Environmental Adaptation | ₹500–5,000
Essential Starter Kit

8. Social Scripts & Environment Preparation Tools
Canon: Social Communication | ₹200–600 | DIY-friendly

9. Auditory Processing Therapy & Training Programs
Canon: Professional Services | ₹2,000–10,000 per session | Requires audiologist/SLP
Essential Starter Kit — Start Today: Noise-reducing ear defenders + Quiet break space identified + Visual coping strategy cards + FM system evaluation request for school. Total starter cost: ₹1,500–9,300.

Every Family Can Start Today — Regardless of Budget
Equity Principle: Not every family can order online. Not every village has same-day delivery. The WHO/UNICEF Nurturing Care Framework demands context-specific, equity-focused solutions. Every parent should be able to support their child TODAY.
Buy This | Make This (Zero-Cost Alternative) | |
Ear Defenders (₹800+) | Cotton balls gently at ear openings (temporary). Hands-over-ears with practiced calmness. Move to quieter location. | |
FM System (₹15,000+) | Position child directly facing speaker. Reduce distance. Use quiet voice, face-to-face, one person at a time. | |
Visual Speaker Cards (₹200+) | Hand-drawn photos of family members. Use a "talking spoon" — whoever holds it speaks. Point to whoever is talking. | |
Acoustic Panels (₹1,000+) | Hang thick blankets on walls. Add rugs/mats to hard floors. Close doors. Use heavy drapes. | |
Coping Strategy Cards (₹200+) | Draw simple cards on paper: "I need a break," "Too loud," "One person please." Laminate with tape for durability. | |
Quiet Break Space (₹500+) | Designate any quiet corner with a pillow and blanket. A closet, bathroom, or bedroom. Even under a table with a blanket draped over it. | |
Social Stories (₹200+) | Draw or write: "Tomorrow we go to grandma's. Many people will talk. I can wear my ear covers. I can go to the quiet room. I can say 'I need a break.'" |
Important Caveat: FM systems and auditory processing therapy require professional involvement and cannot be fully replicated with household materials. Request evaluation through your child's school or Pinnacle center.
Reference: PMC9978394 | WHO NCF Handbook (2022) — Household-material-based interventions across 54 LMICs

Safety Gate — Read This Before Using Any Material
🔴 CONTRAINDICATIONS — Do NOT Use If:
- Child has ear infection, ear pain, or recent ear surgery → No ear defenders or FM receivers until cleared by physician
- Child has known hearing loss → Ear protection may dangerously reduce already limited hearing. Consult audiologist FIRST.
- Child is under 3 years with small ear canals → Ensure headphones are age-appropriate size
- Child has a history of inserting objects into ears → Over-ear protection only; no earplugs
🟡 MODIFY If:
- Child resists wearing anything on ears → Start with 10-second trials; use desensitization; never force
- Child becomes MORE distressed with ear protection → Remove immediately; try environmental modifications instead
- FM system produces feedback or static → Remove receiver and have system checked by audiologist
🟢 PROCEED When:
- Child is in a regulated baseline state (not already overwhelmed)
- Materials introduced at home in calm settings before challenging environments
- Child understands the tool's purpose (age-appropriate explanation provided)
- Escape/break plan is in place before entering challenging environment
🔴 RED LINE — STOP IMMEDIATELY IF: Child shows pain or panic that increases with the tool. Child's ears show redness or irritation. FM system volume causes wincing. Child uses tools to completely avoid ALL social interaction for extended periods — the goal is participation with support, not total avoidance.
Reference: Indian Journal of Pediatrics RCT (2019): DOI: 10.1007/s12098-018-2747-4 — Safety protocols for parent-administered sensory interventions

The Physical Stage — Environment Setup for Auditory Support
🏠 For Home / Family Gatherings
Child Position
Seated with back to wall or corner (reduces sound from behind). Facing the primary speaker.
Quiet Break Space
Identified room AWAY from gathering. Door that closes. Comfortable seating. Pre-stocked with comfort items.
Tool Station
Ear defenders, coping cards, and break request cards within child's reach — NOT hidden away.
Speaker Positioning
Primary conversation partner seated directly facing child, within 3 feet.
Remove Noise Sources
Background music/TV off. Close windows facing traffic. Turn off unnecessary appliances.
🏫 For Classroom
Preferential Seating
Front row, center or slightly off-center. Away from doorway, window, and HVAC.
FM System
Transmitter on teacher. Receiver on/near child. Backup batteries accessible.
Break Access
Identified quiet location (resource room, counselor's office). Break card on desk.
Visual Supports
Written instructions on board/paper. Turn-taking cue visible at all times.
Environmental Checklist
- Soft surfaces in child's primary area (rug under seating, curtains nearby)
- Ear defenders accessible — not in a bag across the room
- Break location identified and tested while quiet
- Family members/teachers briefed on the plan
- Lighting comfortable (fluorescent buzz is an additional auditory stressor)

60-Second Pre-Session Check — The Best Session Starts Right
1
Fed & Hydrated?
Hunger and thirst lower sensory tolerance. Ensure a snack and water before exposure.
2
Adequate Sleep?
Fatigue dramatically reduces auditory filtering capacity. A tired child needs a modified plan.
3
Regulated State?
Not recovering from a recent meltdown or upset. Check in with your child before entering the environment.
4
Tools Available?
Ear defenders, coping cards, and break plan are ready, accessible, and familiar to the child.
5
Preparation Done?
Social story reviewed, people previewed, plan discussed. No surprises.
6
Quiet Space Ready?
Identified, unlocked, comfortable, and the child has visited it while calm.
7
Exit Strategy Known?
"When I feel overwhelmed, I can ___." The child knows their own plan.
✅ GO (6–7 Yes)
Proceed with tools and plan in place.
🟡 MODIFY (4–5 Yes)
Proceed with shortened exposure time. Stay near exit. Keep ear defenders on from the start.
🔴 POSTPONE (0–3 Yes)
Today is not the day. Do a calming activity instead. There is no failure in postponing.
"The goal is functional participation with support. Not suffering. Not enduring. Participating — because the tools make it possible."

Step 1 — Introduce Tools Before the Challenge, Not During
Core Principle: Every material must be introduced when the child is calm, regulated, and at home — NEVER for the first time in the challenging environment. The tool becomes familiar and comforting before it's needed under stress.
Introducing Ear Defenders
Place ear defenders near the child during calm play. Let them touch, hold, examine. Put them on yourself first. Offer (don't force) to try for 10 seconds. Gradually increase duration over days. Practice at home with gradually increasing background noise — soft music, then TV, then conversation.
Introducing Coping Cards
Show each card: "I need a break," "Too loud," "One person please." Practice using them like a game. Child shows card → parent immediately responds by honoring the request. This builds trust that the cards WORK.
Introducing the Break Plan
Walk the child to the quiet space. Let them sit, experience the quiet. Practice going there and coming back. Make it positive — not a punishment space. "This is YOUR space for when sounds get too big."
Key Rule: If you introduce a coping tool and the child uses it, you MUST honor it immediately. If a child shows the "I need a break" card and it's ignored, they will NEVER use it again. Trust is built on consistent response.

Step 2 — Entering the Multi-Voice Environment
Before Entry — 5 Minutes Prior
Review the plan: "We're going in. Your ear defenders are here. Your quiet room is [location]. If it gets too loud, you can [show card / tell me / go to quiet room]." Check arousal level: "On a scale of 1–5, where are you?" If starting above 3, consider ear defenders ON from the start.
At Entry
Enter calmly. Position child in pre-planned spot — facing primary speaker, near exit, away from speakers/music. Tools within reach. Parent stays nearby for first 10–15 minutes to monitor and cue strategies.
First 5 Minutes
Watch for early overwhelm signs: eyes darting, hands near ears, increased fidgeting, face draining of expression, beginning to vocalize/hum. If signs appear → cue strategy: "Would you like your ear covers?" or "Show me your card if you need something." If no signs → allow natural engagement to continue.

Step 3 — Active Tool Use When Overwhelm Begins
🟡 Level 1 — Yellow Zone
Early Overwhelm: Child is uncomfortable but still functional.
- Offer ear defenders
- Move to quieter area within the environment
- Reduce conversations to one speaker at a time
- Remind of break option: "Remember, the quiet room is there if you need it"
🟠 Level 2 — Orange Zone
Moderate Overwhelm: Child is struggling. Fidgeting increases. May start covering ears.
- Put on ear defenders (or encourage child to)
- Reduce ALL simultaneous conversation near child
- Offer break: "Let's take a quiet break for a few minutes"
- If child uses coping card → honor IMMEDIATELY
🔴 Level 3 — Red Zone
Severe Overwhelm / Pre-Meltdown: Child showing distress. Covering ears. Beginning to vocalize. Trying to escape.
- Move to quiet break space IMMEDIATELY — no negotiation, no "just 5 more minutes"
- In quiet space: no talking, no demands, low light, comfort item available
- Allow FULL recovery before discussing return
- Returning is child's choice when regulated — NOT forced by time limit
Critical: Do not wait for a meltdown before acting. Every second of overwhelm beyond the child's capacity makes recovery longer and the next exposure harder. Early intervention is the entire strategy.

Step 4 — Reinforce Every Strategy Use
If Child Requested Ear Defenders
"Great job knowing what you needed. Your ear covers help, and you asked for them — that's really smart."
If Child Used Break Card
"I'm proud you showed me the card. That took courage. The quiet room is always here for you."
If Child Self-Initiated a Break
"You noticed your body was telling you something and you took care of it. That's a superpower."
If Child Managed the Whole Event
"You did it. The whole dinner. With your tools. That took real strength."
What NOT to Do
- ❌ "See, that wasn't so bad!" — Invalidates their effort
- ❌ "Next time try without the headphones" — Removes the support that made success possible
- ❌ "Your cousin didn't need a break" — Comparison is destructive
- ❌ Forcing the child to return before they're ready — Undermines the entire system
Principle: Every successful use of a coping strategy builds the neural pathway for future use. Reinforce the STRATEGY, not the absence of overwhelm. The goal is using tools well, not not needing them.

Step 5 — Recovery Is Not Optional
Immediately After
Move to quiet environment. No auditory demands. Offer preferred calming activity (not screen-based — screens add visual processing load). Don't immediately process the event — recovery first.
Within 30 Minutes
Check arousal level. If still elevated, continue quiet time. Offer a snack and water — sensory overwhelm depletes physical resources. If child initiates conversation, validate: "That was a lot of sound. You handled it with your tools."
Before Next Exposure
Allow adequate recovery time. Do NOT stack challenging auditory environments back-to-back. If this was a school day, reduce after-school demands. If this was a family event, the rest of the day should be quiet.
Exposure Duration | Minimum Recovery | |
30-minute exposure | Minimum 1 hour recovery | |
1–2 hour exposure | Remainder of day should be low-demand | |
Full school day | Quiet, unstructured evening |

Step 6 — What Gets Measured Gets Mastered
Tracking your child's progress is the difference between guessing and knowing. Five simple data points after each exposure will reveal trends that transform your approach over weeks — and give you concrete evidence to share with your child's clinical team.
Environment
Where? How many people? How noisy? Use a 1–5 scale for noise level and number of simultaneous speakers.
Duration Before Overwhelm
How long before first signs appeared? Track in minutes — this number should increase over weeks. It's your primary progress metric.
Tools Used
Which materials did the child use? Ear defenders / Break / Coping card / Visual supports / FM system / Preparation tools
Outcome
✅ Functional participation with tools (success) | 🟡 Participation but with significant difficulty | 🔴 Meltdown/shutdown requiring complete withdrawal
Recovery Time
How long before child returned to baseline regulation? This number should decrease over weeks — a key indicator of growing resilience.
Tracking Insight: Over 4–8 weeks, you should see: duration before overwhelm INCREASING, recovery time DECREASING, and the child self-initiating strategies MORE OFTEN. If you don't see these trends, consult your Pinnacle clinician or call the helpline.

Common Challenges and How to Solve Them
❓ "My child refuses to wear ear defenders"
Try different styles (headband, over-ear, in-ear for older children). Let the child choose the color/design. Start with 10-second trials during preferred activities. Never force. Some children prefer noise-canceling earbuds — they look like "normal" headphones.
❓ "The school says FM system isn't needed"
Request formal auditory processing evaluation by audiologist. With documented APD or ASD diagnosis, FM systems are a recognized accommodation. Request IEP/504 meeting. Contact Pinnacle's advocacy support: 9100 181 181.
❓ "My child uses breaks to avoid everything"
Distinguish between genuine overwhelm breaks and avoidance. Gradually shape return: "5 minutes in the quiet room, then let's try again for 2 minutes." Make participation rewarding. Consult BCBA for functional assessment.
❓ "Family members don't take it seriously"
Share this page. Explain: "This is a neurological difference documented in medical literature, not a behavior choice." If needed, have the child's therapist speak directly to family members.
❓ "It works at home but not at school"
Environment matters. Home may be quieter. School requires accommodations: FM system, preferential seating, break access, written backup. Request classroom observation by SLP or OT.
❓ "My child is getting worse, not better"
Stop. Consult professional. Increasing overwhelm may indicate: hearing loss, medication changes, increased anxiety, or a need for modified approach. Call Pinnacle Helpline: 9100 181 181.
Your Child Is Unique — Adapt the Protocol to Fit
By Age
Toddlers (3–4)
Environmental management is primary. Ear defenders normalized early. Parent manages all strategies.
Early Elementary (5–7)
Introduce coping cards. Begin teaching self-recognition of overwhelm. FM system in classroom.
Later Elementary (8–10)
Self-advocacy training. Socially normalized technology (earbuds). Written self-advocacy scripts.
Middle School+ (11–15)
Technology matches peer norms. Self-management becomes primary. Accommodation documentation for transitions.
By Severity
Severe
Maximum environmental protection. Short exposures. Always have exit plan. Professional involvement essential.
Moderate
Balance accommodation with gradual challenge. Teach strategies. Build duration incrementally.
Mild
Focus on self-advocacy and tool use. Minimal environmental modification needed. Build independence.
By Environment
Classroom
FM system + preferential seating + break access — the non-negotiable triad.
Family Gatherings
Ear defenders + quiet space + preparation + family education.
Public Spaces
Ear protection + exit plan + short duration + choice of quieter options.

Your Child's Personal Auditory Support Plan
Use this template to document what works for your child. Share it with every caregiver, teacher, and family member who spends time with them. Consistency across environments multiplies impact.
Child Profile
My child's name: _______________
My child's age: _______________
Primary challenging environments: _______________
Tools That Work Best
- Ear defenders (brand/type: _______________)
- Noise-canceling headphones
- FM system (school-provided / personal)
- Visual supports
- Coping cards
- Quiet break space
- Social stories / preparation
Early Warning Signs & Recovery
My child's early warning signs of overwhelm: _______________
My child's preferred recovery strategy: _______________
Our family's plan for the next gathering: _______________
Share This Plan With
- Spouse / Co-parent
- Grandparents
- Teacher / School staff
- Therapist team
- Babysitter / Extended family

ACT IV: THE PROGRESS ARC
The First Two Weeks — Building the Foundation
✅ What You'll See
- Child is learning the tools exist and how they work (in calm settings)
- First real-world trials with ear defenders and coping cards
- Some resistance is normal — new tools require trust
- You will see what helps and what doesn't for YOUR child
- First data points being collected
⏳ What You Won't See Yet
- Independent strategy use (too early)
- Reduced overwhelm in challenging environments (tools are still being learned)
- Major behavioral change (foundation is being laid)
Parent Milestone: "By end of week 2, you should know which 2–3 tools your child responds to best. That's the foundation."

Weeks Three and Four — Neural Pathways Forming
Self-Initiated Tool Use Begins
Child begins reaching for ear defenders WITHOUT being prompted. This is a major milestone — trust in the tools is forming.
Break Requests Increase
This is GOOD — it means the child trusts the system. Duration in challenging environments begins to increase, even by 5 minutes.
Verbal Communication Emerges
Child may begin verbalizing overwhelm: "Too loud" or "I need quiet." This self-awareness is a critical developmental leap.
Less Pre-Event Anxiety
Willing to attend events previously refused. Calmer transitions in and out of noisy environments. The plan is reducing anticipatory dread.
Parent Milestone: "You may notice you're more confident too. The plan is working. You're not dreading every family event."

Weeks Five Through Eight — Mastery Emerging
Mastery Criteria
- ✅ Child self-initiates tool use in at least 2 different environments
- ✅ Duration in multi-speaker environments increased by at least 50% from baseline
- ✅ Recovery time decreased by at least 30% from baseline
- ✅ Meltdown/shutdown frequency reduced
- ✅ Child can verbalize or indicate their state: "I'm getting overwhelmed"
- ✅ Functional participation in at least one previously avoided environment (e.g., family dinner)
Generalization Indicators
- Strategies appearing in new, untrained environments
- Child advocating for needs with non-family adults (teacher, relative)
- Reduced dependence on parent cueing — self-monitoring emerging
🏆 Mastery Badge Criteria: Functional participation in a multi-speaker environment lasting 30+ minutes using self-initiated tools with self-directed recovery = MASTERY ACHIEVED
You Did This. Your Child Grew Because of Your Commitment.
For weeks, you introduced tools. You practiced when it was calm. You respected every break request. You prepared before every gathering. You tracked, you adapted, you persisted.And your child — who once couldn't survive 5 minutes in a noisy room — is now participating. Not perfectly. They still take breaks. They still wear ear defenders. They still need preparation. But they participate. They stay. They manage. They are not afraid.
That transformation — from avoidance to functional participation — happened because you showed up, every single day, with the right tools and unwavering commitment.
Family Celebration Suggestion: Mark this milestone. Take a photo at the next family dinner where your child stays through the meal. Write the date down. Tell your child: "Look what you can do now." This is their achievement and yours.

Clinical Guardrails — When to Pause and Seek Help
🔴 Red Flag 1
Child's overwhelm is INCREASING despite consistent tool use for 4+ weeks. May indicate hearing change, increased anxiety, inadequate tool fit, or underlying condition progression. Action: Audiological evaluation + Pinnacle consultation.
🔴 Red Flag 2
Child is using breaks to avoid ALL social interaction, not just noisy environments. May indicate anxiety disorder or social withdrawal beyond auditory issues. Action: Psychology/BCBA evaluation.
🔴 Red Flag 3
New symptoms: ear pain, headaches, dizziness, or ringing in ears. May indicate hearing issue, ear infection, or inappropriate noise exposure. Action: Immediate ENT/Audiology evaluation.
🔴 Red Flag 4
Child becomes aggressive or self-injurious during overwhelm episodes. May indicate overwhelm exceeding coping capacity, requiring a different approach. Action: BCBA consultation + possible environmental restructuring.
🔴 Red Flag 5
Complete regression — child returns to pre-intervention overwhelm levels. May indicate environmental change, medication change, or developmental shift. Action: Full reassessment. Call Pinnacle Helpline: 9100 181 181.
"Trust your instincts. If something feels wrong, pause and ask. You know your child best."
Your Developmental GPS — Where You Are and Where You're Going
Your child's progress doesn't end here. This technique is one node in a carefully sequenced pathway. Based on your child's response to the 9-material protocol, your next steps will branch into the most clinically relevant direction — always moving toward functional independence.
Long-Term Goal: Functional independence in multi-speaker environments with self-selected, self-managed accommodations.

Techniques That Work Alongside This One
A-051: Understanding Auditory Processing Differences
Foundation knowledge for this entire toolkit. Start here if you haven't already. → techniques.pinnacleblooms.org/auditory-processing/understanding-auditory-processing
A-052: Sensory Overload in Noisy Environments
Broader sensory overwhelm beyond voices — addresses the full sensory landscape. → techniques.pinnacleblooms.org/sensory-processing/noisy-environments
A-054: Classroom Auditory Attention
School-specific auditory strategies for following instruction in a classroom of 30+ students. → techniques.pinnacleblooms.org/auditory-processing/classroom-auditory-attention
A-055: Sound Sensitivity and Hyperacusis
When ALL sounds are too much, not just voices. Addresses broader sound tolerance challenges. → techniques.pinnacleblooms.org/auditory-processing/sound-sensitivity
K-3300: Advocating for Classroom Accommodations
How to get FM systems, preferential seating, and breaks written into your child's school plan.
K-3310: Creating Sensory-Friendly Home Environments
Whole-home acoustic and sensory optimization — make your child's primary environment consistently supportive.
12 Developmental Domains — Your Child's Complete Journey
Auditory processing doesn't exist in isolation. It affects communication, social participation, academic performance, and emotional regulation. The GPT-OS® system maps these connections across all 12 domains, sequencing your child's intervention pathway toward integrated, whole-child development.
🔵 You Are Here
Domain A, Position 53 of 100+ techniques in the Sensory Processing & Auditory Challenges domain.
How Domains Connect
Auditory processing affects communication (Domain C), social participation (Domain D), classroom performance (Domain F), and emotional regulation (Domain H). Every technique in the Pinnacle system maps these interdependencies — so your child's plan is never isolated.

ACT V: THE COMMUNITY & ECOSYSTEM
From Families Who've Walked This Path
"Family dinners used to end in meltdowns every single time. My son couldn't process everyone talking at once. Now, with his ear defenders nearby, a quiet break space identified, and practiced coping phrases, he manages full family meals. Not perfectly — he still takes breaks — but he participates, he stays regulated, and he doesn't dread family time anymore. We went from complete avoidance to functional participation in about four months of consistent support."
— Parent, Pinnacle Network
"The FM system in the classroom changed everything. My daughter went from being called 'inattentive' and 'not trying' to being one of the most engaged students. She could finally HEAR the teacher without fighting through the noise of 30 other kids. Nobody even notices the technology anymore."
— Parent, Grade 3 student
"We started with just ear defenders and a quiet corner. That's it. Two things. Within three weeks, our son was voluntarily attending family events he'd refused for two years. Knowing the tools existed — knowing he had an escape valve — reduced his anxiety enough to try."
— Parent, 8-year-old with ASD
Individual results vary. These represent real family experiences within the Pinnacle network. Illustrative cases; outcomes vary by child profile and severity.

You're Part of a Community of Millions
You don't have to figure this out alone. Millions of families across India and the world are navigating the same challenges, sharing the same moments of frustration and breakthrough. Connect with them — and let your story be part of someone else's turning point.
Pinnacle Parent Community
Join thousands of parents sharing what works. → pinnacleblooms.org/community
WhatsApp Support Group
Auditory Processing Family Network — real-time peer support from parents who understand.
FREE National Autism Helpline
9100 181 181 — 16+ languages, 24x7. Always a human voice when you need one.
Email Support
care@pinnacleblooms.org — For questions, resources, and guidance from the Pinnacle team.
The Professionals Who Can Help
🏥 Pinnacle Center Locator
70+ centers across India. Find the center nearest you. → pinnacleblooms.org/centers
💻 Teleconsultation
Can't visit a center? Book a teleconsultation for auditory processing guidance from anywhere in India. → pinnacleblooms.org/teleconsult
📞 Helpline
FREE National Autism Helpline: 9100 181 181 — 16+ languages, 24x7 access to guidance.
The Evidence Behind Every Recommendation
Every recommendation on this page is grounded in peer-reviewed research from audiology, sensory integration science, behavioral therapy, and global child development frameworks. This is not a collection of tips — it is a clinically anchored protocol.
Cuvo & Riva (1980)
Generalization and transfer between comprehension and production. Journal of Applied Behavior Analysis, 13(2), 315–331. Key finding: Auditory processing abilities can be developed through targeted intervention. → PMC1308134
PRISMA Systematic Review (2024)
Sensory integration intervention as evidence-based practice for ASD — 16 articles, 2013–2023. → PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
Sensory integration therapy across 24 studies. Promotes social skills, adaptive behavior, sensory processing, motor skills. → PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Padmanabha et al. (Indian J Pediatr, 2019)
Home-based sensory interventions RCT — Indian pediatric population. → DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework (2018)
Early identification and caregiver support as foundations for child development. → nurturing-care.org
WHO/UNICEF CCD Package (2023)
Care for Child Development — evidence-based recommendations for caregivers across 54 countries. → PMC9978394
Frontiers in Integrative Neuroscience (2020)
Framework for evaluating sensory processing treatment in ASD. → DOI: 10.3389/fnint.2020.556660
NCAEP Evidence-Based Practices Report (2020)
Video modeling and visual supports classified as evidence-based practices for autism.
American Academy of Audiology
Clinical practice guidelines for auditory processing disorder diagnosis and management.

Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
This is not software. This is therapeutic infrastructure.
Diagnostic Intelligence Layer
Converts 591+ structured observations across 349 skills and 79 developmental abilities into standardized diagnostic clarity.
AbilityScore®
A patented universal developmental score (0–1000) establishing baseline, severity, and longitudinal change — comparable across time, therapists, and centers.
Prognosis Engine
Predicts developmental trajectories using historical patterns from 20M+ real therapy sessions.
TherapeuticAI®
Determines therapy focus, intensity, sequencing, and escalation thresholds — always under licensed human clinical authority.
EverydayTherapyProgramme™
Translates clinical plans into daily, home-executable micro-interventions. THIS PAGE is part of that system.
FusionModule™
Coordinates speech, OT, behavior, special education, and medical inputs into a single converged pathway.
Closed-Loop Therapeutic Control
Observation → Score → Plan → Execute → Re-measure → Adapt. Plans change only when the child's data changes.
20M+
1:1 Sessions
Real therapy sessions powering the intelligence engine
97%+
Measured Improvement
Across children in the Pinnacle network
70+
Centers
Across India delivering GPT-OS® guided care
160+
Countries
Where patents have been filed for this system
For structured guidance, contact the FREE National Autism Helpline: 9100 181 181

Watch: 9 Materials That Help With Multiple Voices Overwhelm
Reel ID: A-053
Series: Auditory Challenges — Episode 53
Duration: 75–85 seconds
This 60-second reel introduces the 9 materials in visual format — a compassionate, clear walkthrough designed for parents, caregivers, and educators. Presented by a Pinnacle Blooms Consortium Speech-Language Pathologist with auditory processing specialization.
Reel Details: Reel ID: A-053 | Series: Sensory Processing & Auditory Challenges — Episode 53 | Domain: Auditory Processing | Sensory Filtering | Environmental Adaptation | Duration: 75–85 seconds. For the complete clinical protocol, step-by-step execution guide, and evidence base — you're on the right page. Keep scrolling.
Consistency Across Caregivers Multiplies Impact
If only one parent knows the tools, the child has support in only half their environments. When grandparents, teachers, babysitters, and extended family understand the why and the how — the child's world becomes consistently manageable across every setting they inhabit.
WhatsApp
Share this page directly with family members who care for your child.
Email to School
Send to teachers and school staff. Copy the URL: techniques.pinnacleblooms.org/auditory-processing/multiple-voices-overwhelm
1-Page Family Guide (PDF)
Simplified version for grandparents — the essential points in plain language, one page.
Teacher Communication Template
"What my child needs in the classroom" — a ready-to-send letter template.
"Explain to Grandparents" Simplified Version: "[Child's name] has a brain that processes sound differently. When many people talk at once, they can't separate the voices — everything arrives at the same volume. It's not behavior. It's neurology. They have tools that help: ear covers, a quiet room, and cards that ask for help. When they use these tools, please support them immediately. Breaks aren't rudeness — they're survival."

ACT VI: THE CLOSE & LOOP
Your Questions, Answered
Will my child ever handle noisy environments without tools?
Many children develop improved auditory filtering over time, especially with auditory processing therapy. However, some will always benefit from tools in challenging environments — and that's okay. The goal is functional participation, not elimination of all support. Many adults with auditory processing differences successfully use noise-canceling technology and environmental strategies throughout their lives.
How do I get an FM system for my child's classroom?
Request an auditory processing evaluation from an audiologist. With documented APD or ASD, FM systems are a recognized educational accommodation. Request an IEP or 504 meeting with your school. Pinnacle's advocacy team can support this process: call 9100 181 181.
My child won't wear ear defenders — they hate things on their head.
Try headband-style ear protection, which applies less pressure. In-ear noise-reducing earplugs may work for older children. Desensitize gradually: let them hold, then touch to head for 2 seconds, then wear for 10 seconds during a preferred activity. Never force — find the format they'll accept.
Is this auditory processing disorder? Should we get tested?
If your child consistently struggles in multi-speaker environments despite normal hearing, an auditory processing evaluation is recommended. Full CAPD testing is reliable after age 7. Younger children can be assessed through behavioral observation. Start with an audiological hearing test to rule out hearing loss.
How is this different from just being shy or introverted?
Introversion is a personality preference for quieter settings. Auditory processing overwhelm is a neurological experience where the brain physically cannot filter competing sounds. The child isn't choosing to avoid noise — their auditory system is being overloaded. The distinction changes the intervention from "push through" to "provide support."
Can these materials help at school AND at home?
Yes — most materials work across environments. Ear defenders and coping cards are portable. Environmental modifications need to be made at each location. Consistency across all environments builds the fastest progress.
How much does all this cost?
The Essential Starter Kit (ear defenders + quiet space + coping cards + social stories) costs ₹1,500–9,300. Many items are DIY-friendly at zero cost. FM systems (₹15,000–60,000) may be provided by schools. Auditory therapy (₹2,000–10,000/session) is a professional service.
Should I avoid taking my child to noisy places entirely?
No — complete avoidance prevents the child from developing any coping capacity. The approach is graded, supported exposure: short durations, with tools, with exit plans. Avoidance should be strategic (skip the incredibly loud reception) not total (avoid all family events forever).
Didn't find your answer?

From Knowledge to Action — Start Today
You have the knowledge. You have the tools. You have the protocol. Everything this page contains — the science, the steps, the materials, the community — exists for one reason: so that your child can participate in the full life they deserve. The next step is yours.
🟢 Start This Technique Today
Launch GPT-OS® guided session for Multi-Material Auditory Overwhelm Protocol.
📞 Book a Consultation
FREE National Autism Helpline: 9100 181 181 (16+ languages, 24x7)
📖 Explore Next Technique
A-054: Classroom Auditory Attention — expand your child's success into their school environment.
Validated by the Pinnacle Blooms Consortium® — SLP • OT • BCBA • SpEd • NeuroDev • Audiology
Preview of 9 materials that help with multiple voices overwhelm Therapy Material
Below is a visual preview of 9 materials that help with multiple voices overwhelm therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Pinnacle Promise
"From fear to mastery. One technique at a time."
A parent arrives on this page scared, confused, and exhausted — watching their child suffer in every noisy room. By the end, they have 9 proven tools, a step-by-step protocol, tracking systems, and a community. Their home becomes a therapeutic center. Their child begins to participate in life.
This is the Pinnacle Promise. 70,000+ techniques. One child at a time. Powered by GPT-OS®.
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
SLP • OT • BCBA • SpEd • NeuroDev
Certifications
ISO 13485: Medical Device QMS
ISO/IEC 27001: Information Security
DPIIT: DIPP8651 | MSME: TS20F0009606
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention planning with licensed audiologists, speech-language pathologists, and occupational therapists. Persistent auditory processing difficulties warrant professional evaluation to rule out hearing loss and identify specific processing challenges.
Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2