
When Motion Feels Like Danger
Your child isn't being difficult. Their nervous system is treating movement as a genuine threat — and now you will learn to understand it.
"He froze at the top of the escalator. Completely frozen. The line of people behind us, my arms stretched toward him, him shaking — not a tantrum, pure terror. We had to take the stairs. Every time. For three years." — Parent of a 5-year-old, Pinnacle Network
🏥 Pinnacle Blooms Consortium Validated
Domain A • Sensory Processing • A-076
You are not failing your child. Their vestibular system is speaking a language only they can hear — and now you will learn to understand it.
📖WHO Nurturing Care Framework (2018): Early identification of sensory differences and responsive caregiving directly improves developmental outcomes. nurturing-care.org
🆓FREE National Autism & Developmental Helpline
9100 181 181
Available in 16+ languages across India
9100 181 181
Available in 16+ languages across India
1 in 6 Children Experiences Sensory Processing Challenges Severe Enough to Affect Daily Life
80%
Autism + Sensory
of children with autism display significant sensory processing difficulties
PMC11506176 (2024 PRISMA Review)
1 in 20
Vestibular Primary
children experience vestibular hypersensitivity as their primary sensory challenge
Sensory Processing Disorder Foundation
70%+
Daily Disability
of parents report movement sensitivity was the most disabling sensory issue in daily life
Pinnacle Network Clinical Data, N=12,000+
You are among an estimated 3.2 million families in India navigating this exact challenge right now.
With 18+ million children on the autism spectrum in India (WHO/UNICEF estimates), vestibular hypersensitivity is one of the most commonly reported — and least understood — sensory challenges facing Indian families today. The research is clear: this is real, it is widespread, and it is treatable.
📖PRISMA Systematic Review (2024): 80% of children diagnosed with autism display sensory processing difficulties. Meta-analysis confirms sensory integration therapy effectively promotes social skills, adaptive behavior, and motor skills. References: PMC11506176 | PMC10955541

It's Not Fear of Movement. It's a Nervous System That Can't Filter Movement Signals Properly.
The Science
The vestibular system lives in the inner ear. Its job: tell the brain where the body is in relation to gravity, and whether it's moving. In children with vestibular hypersensitivity, this system is set to "too loud."
Ordinary movement — a gentle swing, a car turning a corner, being lifted — sends a signal the brain interprets as: ⚠️ DANGER. FALLING. THREAT.
The child's freeze, panic, or terror response is real. The alarm is misfiring — but the fear is not manufactured.
The Technical Terms
Vestibular Hypersensitivity
Over-responsiveness to movement input
Gravitational Insecurity
Exaggerated fear when feet leave the ground or head position changes
Movement Intolerance
The practical daily-life limitation that results
This is not a behaviour problem. This is a neurology difference.

Movement Sensitivity Typically Emerges at 18 Months–3 Years. It Rarely Resolves Without Support.
Age 0–12 Months
Vestibular system develops. First movement experiences. Flag: Excessive distress when position changes.
Age 12–24 Months
Walking and climbing begin. ⚠️ Flag: Refuses to be lifted, walking avoidance, intense fear of movement.
Age 2–4 Years
🚨 The Critical Window. Active challenges: playground avoidance, car ride distress. You may be here.
Age 4–7 Years
School readiness impacted. PE and outdoor play affected. Intervention window: HIGH IMPACT.
Age 7–10 Years
With support: increasing tolerance and confidence. Without support: compensatory avoidance entrenches.
Age 10+
Habitual avoidance limits motor development and social participation. Harder — but not impossible — to shift.
🌍WHO Care for Child Development (CCD) Package — Age-specific evidence-based recommendations implemented across 54 countries. Movement sensitivity commonly co-occurs with: tactile sensitivity, anxiety, DCD, autism, and ADHD.
Your child is here. Here is where we're heading. The earlier intervention begins, the more neural plasticity works in your favour.
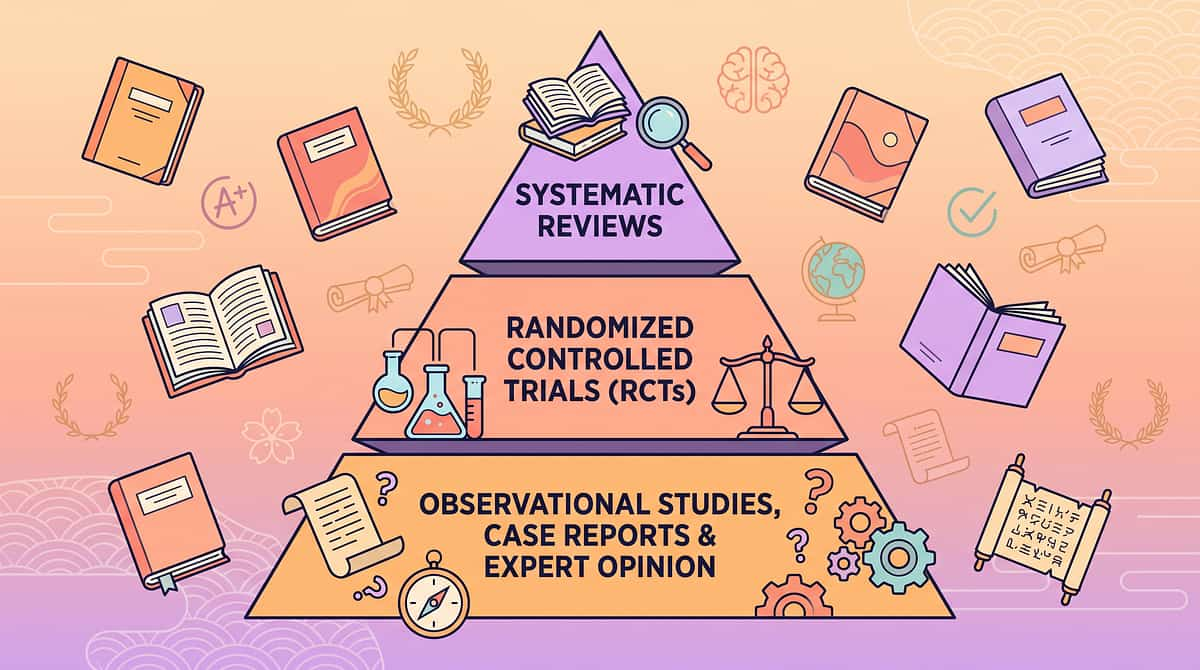
This Is Not Experimental. Vestibular Desensitisation Through Graded Movement Is an Evidence-Based Practice.
Evidence Grade: Level I
Systematic Review + RCT
85% Confidence Rating
📄 PRISMA Systematic Review 2024
16 studies (2013–2023) confirm sensory integration intervention is Evidence-Based Practice for ASD. Motor, social, and adaptive behaviour outcomes demonstrated.
📄 Meta-Analysis: World J Clin Cases 2024
24 studies confirm SI therapy effectively promotes sensory processing and gross/fine motor skills. 40-minute sessions showed maximum effectiveness. Home-based adaptations validated.
📄 Indian RCT: Padmanabha et al. 2019
Home-based sensory interventions in Indian pediatric population demonstrated significant outcomes. Parent-administered protocols proven effective.
20M+
Therapy Sessions
97%+
Measured Improvement
70+
Centers Across India
🇺🇸NCAEP 2020: Sensory Integration classified as Evidence-Based Practice for autism by the National Clearinghouse on Autism Evidence and Practice.
The Technique: Vestibular Desensitisation Through Graded Movement Exposure
Technique Identity
Parent-Friendly Name: Teaching the nervous system that movement is safe — one tiny step at a time
Code: A-076 | Domain: A — Sensory Processing / Vestibular System
Age: 2–10 Years
10–20 Min Sessions
3–5× Per Week
Home + Outdoors
What It Is & What It Does
A structured programme of graded movement experiences that gradually builds a child's nervous system tolerance for vestibular input — motion, height, acceleration, and positional change — using 9 specific material categories progressing from least threatening to more complex movement experiences.
It recalibrates the vestibular system's threat response through repeated, safe, child-controlled exposure. The nervous system learns — through hundreds of tolerated experiences — that movement is not danger.
The 9 Materials at a Glance
Grounded Movement Equipment
Slow Linear Swing Options
Proprioceptive Input Tools
Enclosed / Cocoon Swings
Child-Controlled Vehicles
Graduated Height Exposure
Rocking Furniture
Vehicle Travel Supports
Supported Social Movement Games

This Technique Crosses Every Therapy Boundary — Because the Vestibular System Connects to Everything.

🦾 Occupational Therapist (Primary Lead)
Designs the graded exposure hierarchy, selects materials by sensory profile, and guides the vestibular desensitisation protocol. Trains parents for home execution.

🧠 ABA / BCBA
Creates systematic desensitisation programmes using graduated exposure with reinforcement. Measures tolerance duration and integrates movement challenges into daily routines.

🗣️ Speech-Language Pathologist
Uses movement as an arousal regulator before communication sessions. A regulated, non-anxious child engages better in language activities.

📚 Special Education Teacher
Addresses movement sensitivity as a barrier to PE and school transitions. Develops accommodation plans for escalators, stairs, and school travel.
"The vestibular system doesn't know which therapy modality trained it. A child who learns movement is safe through an OT's swing is also a child who can sit still for SLP, engage in ABA, and participate in SpEd. Movement tolerance is foundational to everything." — Pinnacle Blooms Consortium, Clinical Coordination Board
Parents and caregivers execute 70–80% of all intervention contact hours at home through GPT-OS® protocols. You are the most important therapist your child has.
6 Measurable Targets. All Trackable at Home. All Achievable.
Approach Behaviour
Before: Child refuses to enter playground area with swings.
After: Child approaches swing area without distress.
Measure: Distance child will voluntarily approach (metres)
After: Child approaches swing area without distress.
Measure: Distance child will voluntarily approach (metres)
Tolerance Duration
Before: Zero seconds tolerated on any moving surface.
After: 30+ seconds on grounded equipment without distress.
Measure: Stopwatch or phone timer
After: 30+ seconds on grounded equipment without distress.
Measure: Stopwatch or phone timer
Movement Acceptance
Before: Panics when picked up or position suddenly changes.
After: Tolerates being lifted with predictable verbal warning.
Measure: Caregiver rating scale 1–5
After: Tolerates being lifted with predictable verbal warning.
Measure: Caregiver rating scale 1–5
Vehicle Tolerance
Before: Severe distress on all car journeys.
After: 15-minute journey with regulated behaviour.
Measure: Journey duration and distress rating
After: 15-minute journey with regulated behaviour.
Measure: Journey duration and distress rating
Height Exposure
Before: Will not climb any structure, even 1–2cm elevations.
After: Climbs low climbing frame (30cm) with support.
Measure: Maximum height accessed without distress
After: Climbs low climbing frame (30cm) with support.
Measure: Maximum height accessed without distress
Peer Movement Play
Before: Watches all playground activity from sidelines.
After: Participates in one supported movement game with peers.
Measure: Observation count per week
After: Participates in one supported movement game with peers.
Measure: Observation count per week
📊AbilityScore® Integration: These targets feed directly into your child's GPT-OS® AbilityScore® — tracking vestibular domain progress from 0–1000 across 591+ developmental observations. pinnacleblooms.org/ability-score

Materials 1–3: Your First Three Movement Sensitivity Tools
9 Clinically-Mapped Materials
Start Here — Least Threatening

Material 1: Grounded Movement Equipment
Why: Provides vestibular input while keeping child connected to a stable surface — the gentlest entry point into the programme.
Price Range: ₹500–2,500

Material 2: Slow Linear Swing Options
Why: Linear, slow, predictable movement — the least threatening form of vestibular challenge. Predictability is the key ingredient that reduces fear.
Price Range: ₹2,000–8,000

Material 3: Proprioceptive Input Tools
Why: Deep pressure and heavy work ground the body before and during movement challenges. Proprioception is the nervous system's "anchor."
Price Range: ₹800–3,500
✅ All 9 materials are validated through Pinnacle's 128-Canon Material taxonomy and clinically trialled across 70+ centers with 20M+ therapy sessions.

Materials 4–6: Building Containment, Agency & Height Tolerance

Material 4: Enclosed / Cocoon Swings
Why: Movement within a contained, protected space — sensory containment dramatically reduces fear response. The child feels held while experiencing vestibular input.
Price Range: ₹3,000–12,000

Material 5: Child-Controlled Vehicles
Why: The child controls speed, direction, and stopping — building agency over movement. Self-directed movement is fundamentally less threatening than externally imposed movement.
Price Range: ₹1,500–5,000

Material 6: Graduated Height Exposure Tools
Why: Systematic exposure to increasing heights in 1–2cm increments builds height tolerance through the graded exposure principle. Each tiny success rewires the threat response.
Price Range: ₹400–2,000
Materials 7–9: Rhythm, Travel Comfort & Social Movement Joy

Material 7: Rocking Furniture
Why: Rhythmic vestibular input in a safe, familiar home context — combining comfort with movement. The rocking chair is where many children first learn that motion can feel soothing rather than threatening.
Price Range: ₹1,200–6,000

Material 8: Vehicle Travel Support Tools
Why: Modifications that reduce vestibular distress during necessary car and auto journeys. Proprioceptive anchoring during travel transforms a daily stressor into a manageable experience.
Price Range: ₹300–1,500

Material 9: Supported Social Movement Games
Why: Social connection transforms movement from threat to shared joy. Partnership overrides fear — a trusted relationship is the most powerful de-sensitisation tool available. Cost: ₹0–500.
✅Pinnacle Recommends: All 9 materials validated through Pinnacle's 128-Canon Material taxonomy and clinically trialled across 70+ centers.
Every Family Can Begin Today. Zero Budget Required.
WHO/UNICEF equity principle: effective intervention must be accessible regardless of economic status.
Material | DIY Household Version | Why It Works | |
Balance Cushion | Firm sofa cushion on floor / folded blanket | Creates unstable surface; same vestibular input | |
Linear Swing | Blanket held at both ends by adults — gentle rocking | Linear movement principle identical | |
Proprioceptive Tools | Backpack with books; pushing against doorframe; bear hugs | Deep pressure mechanism is the same | |
Enclosed Swing | Large towel as hammock swing between two adults | Containment + linear movement | |
Child-Controlled Vehicle | Cardboard box as "boat" the child pushes | Agency over movement = same psychological effect | |
Height Exposure | Stack of books in 1cm increments | Graded exposure principle identical | |
Rocking Furniture | Adult rocking child on lap, slow rhythmic pace | Vestibular input delivered directly | |
Vehicle Supports | Rolled towel as neck support; close window | Same proprioceptive support mechanism | |
Social Movement Games | "Row Your Boat" — adult and child rocking together | Social containment of movement |
The most powerful movement tool in this programme costs ₹0 — it is a trusted adult's body. A child who will not sit on a swing will often lie across a parent's lap and allow gentle rocking. Start there. The nervous system doesn't care whether the vestibular input came from a ₹8,000 therapy swing or your arms.
Safety First: Read This Before Every Session
🔴ABSOLUTE STOP — Do NOT proceed if:
• Child is unwell, feverish, or has ear infection
• Child experienced meltdown or severe distress in past 30 minutes
• Child has known seizure condition without neurologist clearance
• Child has vestibular/cerebellar medical condition
• You are feeling impatient or under time pressure
• Child is expressing "no" through any communication modality
• Child is unwell, feverish, or has ear infection
• Child experienced meltdown or severe distress in past 30 minutes
• Child has known seizure condition without neurologist clearance
• Child has vestibular/cerebellar medical condition
• You are feeling impatient or under time pressure
• Child is expressing "no" through any communication modality
🟡AMBER — Modify before proceeding:
• Child had poor sleep → reduce intensity by 50%
• Child is hungry → feed first, wait 20 minutes
• Environment is busy/loud → find quieter space
• Child shows mild anxiety → use more proprioceptive input first
• Child had poor sleep → reduce intensity by 50%
• Child is hungry → feed first, wait 20 minutes
• Environment is busy/loud → find quieter space
• Child shows mild anxiety → use more proprioceptive input first
🟢GREEN — Proceed with confidence:
• Child is calm and regulated
• Time is unhurried
• Safe, clear physical space available
• Adult is calm and patient
• Child has had recent proprioceptive/heavy work input
• Child is calm and regulated
• Time is unhurried
• Safe, clear physical space available
• Adult is calm and patient
• Child has had recent proprioceptive/heavy work input
🛑STOP IMMEDIATELY IF: Child vomits, becomes very pale, complains of dizziness or headache, distress escalates rapidly, child goes limp or unresponsive, or shows self-injurious behaviour.
🆓9100 181 181 — Free clinical guidance available for all safety questions, 7 days/week.
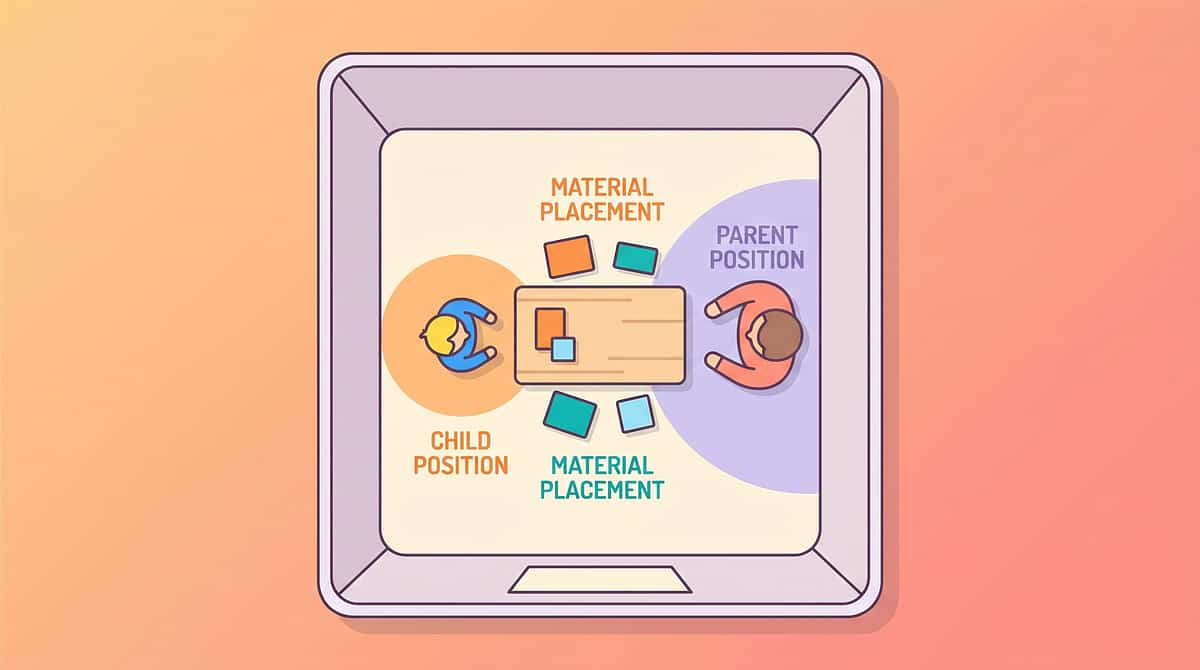
Set Up Your Space: Environment Determines 80% of Session Success
Prepare the environment first — not just the materials. A well-set space communicates safety before a single word is spoken.
Clear the Space
Remove all furniture/obstacles in 2m radius of movement equipment. Safety is non-negotiable.
Soft Surface Below
Yoga mat or carpet below and around all movement equipment. Adult hand within reach at all times.
Lighting & Sound
Soft lamps preferred over harsh fluorescent. No background TV or music. Conversation volume normal.
Parent Position
Always at child's eye level or below — never towering above. Place a visible timer where the child can see it. Predictability reduces fear.
Place a visual timer (sand timer or phone timer) where the child can see it. Children with movement sensitivity gain enormous confidence from knowing exactly "how long" any challenge will last.

Is Your Child Ready? The 60-Second Readiness Check — Before Every Session
Step 0 of 6
Non-Negotiable
Check | ✅ GO | ❌ NOT TODAY | |
Child's last meal | 20+ minutes ago | Less than 20 minutes ago | |
Sleep last night | Adequate (6+ hours) | Poor or disrupted | |
Emotional state | Calm, regulated | Distressed, post-meltdown | |
Physical health | Healthy | Unwell, ear infection, fever | |
Your emotional state | Calm, patient | Stressed, hurried, frustrated | |
Time available | 20+ minutes, unhurried | Rushed or deadline approaching | |
Recent distress | None in past hour | Meltdown or high anxiety in past hour |
🟢 7/7 Checks
FULL SESSION: Proceed with planned protocol
🟡 5–6/7 Checks
MODIFIED SESSION: Reduce intensity 50%, shorter duration
🟠 3–4/7 Checks
MINIMAL SESSION: Proprioceptive input only, no movement challenge
🔴 0–2/7 Checks
POSTPONE: Calming activity today. A forced session increases sensitivity, not tolerance.
🆓9100 181 181 — If your child never reaches a GO state and you can't understand why, call our clinical team.

Step 1: The Invitation — Never a Command. Always an Invitation.
Step 1 of 6
Duration: 30–60 Seconds
This distinction — invitation versus command — is the entire technique. The child's nervous system cannot be forced into safety. It can only be invited.
"Hey, I've got something cool to show you. You don't have to do anything — just come and look with me."
Alternative Scripts
Non-verbal child: Hold material at child's level, wait. Make it interesting without pressure.
Highly verbal child: "I'm going to try the wobble board. Want to watch? You can try if you want."
Anxious child: "This is going to be super slow. You tell me when to stop and I'll stop immediately."
Reading the Response
✅ Child takes a step toward material
✅ Child makes eye contact with material
✅ Child's body softens slightly
✅ Child verbalises curiosity
✅ Child makes eye contact with material
✅ Child's body softens slightly
✅ Child verbalises curiosity
❌Backs away → Move material further away
❌Ignores → Play with it yourself; let curiosity work
❌Says "no" → "That's fine. We can just watch today." — honour it completely
❌Ignores → Play with it yourself; let curiosity work
❌Says "no" → "That's fine. We can just watch today." — honour it completely
Body Language: Crouch to child's height. Open posture. Slow, calm movements. Warm eye contact. Stay between child and exit — reassuring, not blocking.
Step 2: The Engagement — Introduce the Material on the Child's Terms
Step 2 of 6
Duration: 1–3 Minutes
Observe. Follow their lead. Never push. The therapeutic relationship is built in this phase — and it is the foundation everything else rests on.
Model First
Sit on the balance cushion yourself first. Model comfort and enjoyment. Place a favourite toy ON the material as a bridge to interest.
Wait
Let the child approach on their own timeline. Distance: start material 1–1.5 metres away. Let the child close the gap themselves.
Celebrate First Contact
One foot on the cushion, briefly — immediately praised with specificity. "I noticed you looked at it — that's brave."
Child's Response | What It Means | Your Action | |
Immediate approach | High trust, good day | Proceed; keep tempo gentle | |
Cautious circling | Processing; not refusal | Wait; narrate gently | |
Touch then withdraw | Exploring boundary | Praise the touch; no pressure | |
Avoidance | Heightened sensitivity today | Reduce to observation + proprioception |
Begin verbal praise at the earliest positive response — even a glance toward the material. Timing: within 3 seconds. Always name exactly what you're praising.

Step 3: The Therapeutic Action — The Active Ingredient
Step 3 of 6
Duration: 5–10 Minutes
Tolerated vestibular input, repeated, in a felt-safe context. This is the core therapeutic window — where neural recalibration actually happens.
Material 1: Grounded Equipment
Child stands or sits on wobble board. Adult provides one-finger support at first. Duration begins at 3 seconds. Child controls when they step off.
Material 2: Linear Swing
Child lies on platform swing (lying reduces height fear). Barely perceptible push — less than 5cm arc initially. Commentary: "I'm pushing just a tiny bit. Tell me to stop."
Material 3: Proprioceptive Prep
BEFORE movement: weighted vest or 5 minutes of heavy work (pushing wall, carrying books, bear hug). Then introduce movement challenge.
Intensity
Always one step BELOW child's visible tolerance threshold — never push to the edge
Duration
Stop BEFORE child wants to stop — leave them wanting more
Control
Child has stop/start agency at all times — establish a stop word or hand signal
Narration
Ongoing calm commentary: "You're doing it. Your feet are on the board. That's brave."
📖 Meta-analysis (World J Clin Cases 2024): 40-minute therapy sessions most effective. Home sessions 10–20 minutes; therapeutic action constitutes 40–60% of total session time. PMC10955541

Step 4: Repeat & Vary — 3 Good Repetitions Beat 10 Forced Ones
Step 4 of 6
Duration: 3–5 Minutes
Week 1
2–3 brief exposures per session (each 3–10 seconds). Building the foundation of trust.
Weeks 2–3
3–5 exposures per session (each 10–30 seconds). Neural pathways beginning to form.
Weeks 4–6
5–8 exposures (each 30–60 seconds). Consolidation and confidence building.
Weeks 7–8+
Extended exposures (60+ seconds) with variation in height, speed, and support level.
Variation Options
Variation A: Height
Balance cushion → thick foam pad → wobble board with slight tilt increase
Variation B: Speed
Linear swing arc increases by maximum 2cm per session
Variation C: Support
Two-hand hold → one hand → finger touch → verbal only → independent
Variation D: Duration
5 seconds → 10 seconds → 30 seconds → 1 minute
The Golden Rule: Always end on a success. Three seconds of genuine, unforced vestibular tolerance is therapeutic progress. End there. Come back tomorrow.

Step 5: Reinforce & Celebrate — Timing Beats Magnitude
Step 5 of 6
Within 3 Seconds of Desired Behaviour
"You did it! You stayed on that wobbly board! That was BRAVE. I'm so proud of you."
Specificity Rule: Always name exactly what you're reinforcing: "You kept your feet on the swing for 5 whole seconds" — not just "good boy/girl." The brain needs to know precisely which behaviour to repeat.
Type | Example | Best For | |
Social | Enthusiastic praise + hug/high five | Most children | |
Token | Star on chart; sticker; token | Children who like visual systems | |
Tangible | Preferred snack, favourite small toy | Highly food-motivated children | |
Activity | 2 minutes of chosen preferred activity | Activity-motivated children | |
Sensory | Access to preferred sensory input | Sensory-seeking children |
Celebrate the attempt, not just the success. A child who approached the swing and touched it — then walked away — has done something therapeutically significant. Reinforce that. The full swing ride comes later.
Step 6: The Cool-Down — The Transition Is Part of the Therapy
Step 6 of 6
Duration: 2–3 Minutes
Never end a session abruptly. How you close a session determines how the child's nervous system remembers it — and whether they'll say yes next time.
"Two more times, and then we're all done with the movement part. After that, we'll [favourite activity]. You've done amazingly today."
Verbal Warning
2 minutes before ending: "Almost done — two more." Never an abrupt stop.
Visual Timer
Set visible countdown timer so the child can see exactly how much time remains.
Proprioceptive Grounding
Deep pressure hug or weighted blanket for 60 seconds. This consolidates vestibular input.
Material Put-Away Ritual
If able, child helps put equipment away. Proprioceptive input + a sense of closure.
Verbal Close
"Movement time is done. You did something hard today. I'm proud of you."
If the child resists ending — this is progress. The child wanted MORE movement. Use the visual timer and say: "You can do it again TOMORROW. I'll write it down so we don't forget."
🆓9100 181 181 — If your child frequently cannot transition out of movement activities, our clinical team can help design a transition protocol.
Capture the Data: 60 Seconds Now Saves Months of Guessing Later
📊 Tolerance Duration
Timer in seconds. Example: "Stayed on wobble board: 8 seconds"
😌 Distress Level
Rating 1–5 (1=calm, 5=severe distress). Example: "Distress level: 2"
👋 Approach Behaviour
Spontaneous / Prompted / Refused. Example: "Approached: Prompted"
Simple Tracking Template
Date: ___________ Material Used: ___________
Tolerance Duration: ___ seconds
Distress Level: 1 2 3 4 5
Approach: Spontaneous / Prompted / Refused
Best Moment Today: ___________
Parent Note: ___________📱GPT-OS® Integration: Track directly in the GPT-OS® app → automatic AbilityScore® updates → weekly progress reports → therapist-visible data. pinnacleblooms.org/gpt-os-tracker
"Data is the language your child's development speaks. When you don't collect it, progress becomes invisible — and invisible progress is demoralising." — Pinnacle Blooms Consortium, Clinical Data Team

What If It Didn't Go as Planned? Most Sessions Aren't Perfect — That's Information.
Problem 1: Child Refused to Engage
Why: Dysregulation, tiredness, or sensory overload already present.
Fix: Run the readiness check (Card 15) more rigorously. Try again tomorrow. Start with the ₹0 version — your lap — before any equipment.
Fix: Run the readiness check (Card 15) more rigorously. Try again tomorrow. Start with the ₹0 version — your lap — before any equipment.
Problem 2: Fine for 2 Seconds Then Meltdown
Why: Material was one step too intense — beyond current tolerance threshold.
Fix: Drop intensity by 50%. Switch from wobble board to firm cushion. Sit on a stationary swing first — no movement at all.
Fix: Drop intensity by 50%. Switch from wobble board to firm cushion. Sit on a stationary swing first — no movement at all.
Problem 3: Child Loves It and Won't Stop
Why: Sensory-seeking behaviour alongside the sensitivity — common in mixed profiles.
Fix: A good sign neurologically. Use visual timers for session boundaries. Build in longer cool-down transitions.
Fix: A good sign neurologically. Use visual timers for session boundaries. Build in longer cool-down transitions.
Problem 4: Tolerates It in Session but Panics Elsewhere
Why: Generalisation hasn't occurred yet — skill is context-specific.
Fix: Explicitly practise in new environments, starting from observation. Generalisation requires its own deliberate programme.
Fix: Explicitly practise in new environments, starting from observation. Generalisation requires its own deliberate programme.
Problem 5: Progress Has Plateaued
Why: Adaptation curve; may need variation in approach or intensity.
Fix: Review progress data. Introduce a new material from the 9-material menu. Consider Pinnacle professional consultation.
Fix: Review progress data. Introduce a new material from the 9-material menu. Consider Pinnacle professional consultation.
Problem 6: Can't Tell If We're Making Progress
Why: Vestibular tolerance progress is often invisible until it suddenly isn't.
Fix: Review your Week 1 data. Tolerance from 0 to 15 seconds is massive progress. Document changes in daily life: car journeys, playground visits.
Fix: Review your Week 1 data. Tolerance from 0 to 15 seconds is massive progress. Document changes in daily life: car journeys, playground visits.
"Session abandonment is not failure. It is data that tells you the approach needs refinement. Our GPT-OS® algorithms have been refined by 21 million such data points."
Adapt & Personalise: No Two Children Are Identical
Your child's vestibular profile is unique. Adjust accordingly — the protocol is a framework, not a fixed script.
Progress along the difficulty continuum only when the child is comfortable and confident at their current level — never based on a calendar schedule.
Age | Priority Materials | Approach | Key Principle | |
2–3 years | Rocking furniture, body contact | Parent body as primary tool | Safety through relationship | |
3–5 years | Grounded equipment, linear swings | Low to ground, maximum control | Child always in control | |
5–7 years | Enclosed swings, height exposure | Social motivation; peer modelling | Make it a game | |
7–10 years | Child-controlled vehicles, social games | Autonomy; achievement framing | Celebrate mastery |
Children with co-occurring anxiety benefit from social story preparation before sessions, PECS visuals for the session sequence, and deep breathing strategies before beginning vestibular work.

Weeks 1–2: Tolerance, Not Mastery. Approach, Not Engagement. Any Positive Is Significant.
📈 Progress Arc
Building the Foundation — ~15%
✅ Approach Closer
Child approaches movement material from 1 metre (previously 3 metres) without significant distress.
✅ First Tolerance
Child tolerates 3–5 seconds on grounded equipment (previously zero seconds).
✅ Observational Learning
Child watches parent on equipment without distress — observation stage is therapeutic.
✅ Daily Life Flickers
Slight reduction in distress during car journeys on familiar routes. One instance of spontaneous gentle self-movement.
"If your child tolerates 3 seconds on the wobble board this week versus zero last week — that is a measurable, clinically significant change in neural processing. It doesn't look like much. It is enormous."
Track this week: Tolerance duration (seconds) per session | Approach distance (metres) | Distress rating (1–5 scale)
Weeks 3–4: The Nervous System Is Rewriting Its Rules About Motion
📈 Progress Arc
Neural Pathways Forming — ~40%
Anticipation Shifts
Child anticipates the movement session with something other than fear — curiosity or even mild excitement appears.
Duration Grows
Child tolerates 15–30 seconds on grounded equipment independently, without requiring constant adult physical support.
Self-Initiation Emerges
Child begins to self-initiate gentle movement — rocking on a chair, choosing the wobble cushion without being prompted.
Daily Life Changes
Noticeable reduction in car journey distress on familiar routes. Approaches playground swing area without refusing to enter.
"You may notice YOU are more confident too. Your hesitation before offering movement has reduced. Your calm during the session has increased. This matters — the child's nervous system reads your nervous system."
When to Increase: Add 1 new material from the 9-material menu. Increase tolerance target by 15–20 seconds. Introduce first outdoor movement challenge in a controlled garden or balcony setting.

Weeks 5–8: Generalisation — The Real-World Test
📈 Progress Arc
Mastery Emerging — ~75%
Criterion | Mastery Benchmark | |
Grounded Equipment | 2+ minutes independent, no support | |
Linear Swing | 30+ seconds, 15–20cm arc, initiated voluntarily | |
Child-Controlled Vehicle | 5+ minutes in outdoor space independently | |
Car Journey | 20+ minute journey without significant distress | |
Heights | Climbs low play structure (30cm) with verbal reassurance only | |
Peer Play | Participates in one supported movement game with a peer |
Generalisation Indicators — Skill Appearing in OTHER Contexts
- Child voluntarily chooses rocking at home when self-regulating
- Child uses playground swing equipment with some adult support
- Car journeys have new routines emerging (music, counting, sensory supports)
- Child comments positively on movement: "that was fun" / "again"
🏅 Mastery Achieved — Movement Tolerance — Level: Core — Domain A • A-076
Celebrate This Win: You Did This
Remember that parent describing their child frozen at the top of an escalator? The absolute terror. The shrinking world. Now look at your data from Week 8.
That change is called neural recalibration. And you made it happen.
Visit the Park
Let them choose: stay on the edge or try the swing. No pressure. Just possibility. The offer itself is a victory.
Capture the Moment
Take a photo of them on any movement equipment they wouldn't have touched in Week 1. You will treasure it.
Journal Three Moments
Write down three specific moments of progress you witnessed. Progress in writing feels real and is sustaining.
"Parental self-efficacy is the strongest predictor of continued intervention. You have proven to yourself that you can do this. Keep going."

Red Flags: Even in the Progress Zone, These Signs Mean Pause and Seek Guidance
⚠️ Safety Alert
Flag | What It Looks Like | Why It Matters | Action | |
Regression Spike | Sudden major increase in movement fear after weeks of progress | May signal ear infection, illness, or acute anxiety | Medical check; pause advancement; teleconsult | |
New Sensory Signs | Sensitivity expanding to new sensory domains | Sensory profile may be shifting | Pinnacle full sensory assessment | |
Motor Regression | Loss of motor skills alongside avoidance | May signal neurological event — requires urgent evaluation | GP referral immediately | |
Night Terror Spike | Movement-related nightmares increasing | Technique intensity too high; nervous system overwhelmed | Reduce intensity 50%; consult OT | |
Food Refusal | New food refusal emerging alongside movement work | Sensory overload can manifest across systems | Check for oral sensory overload; review full sensory diet | |
Self-Regulation Collapse | Child can no longer self-regulate in previously managed situations | Intervention schedule may be too intensive | Review frequency; schedule Pinnacle assessment |
🆓9100 181 181 — Free clinical consultation for any red flag concern, 7 days/week.
The Progression Pathway: A-076 Is One Step in a Longer Journey
Every next technique builds on the vestibular tolerance A-076 created. You are not starting over — you are building up.
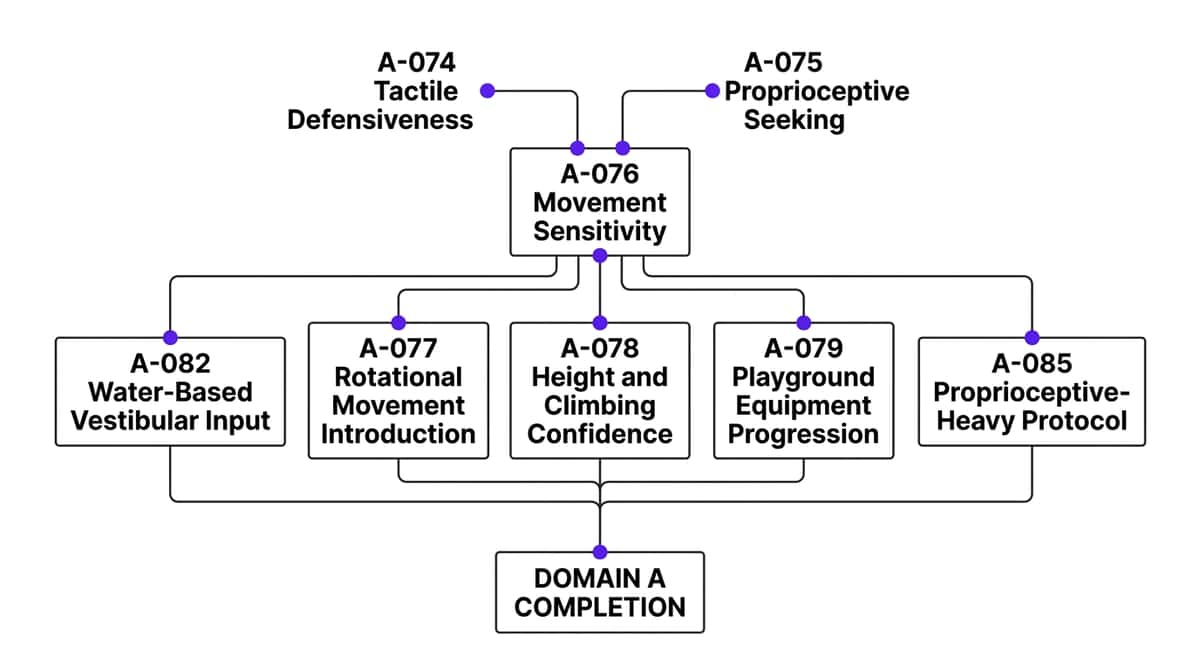
Choose Your Next Step Based on Response
- A-077 — Rotational Movement (if linear movement mastered)
- A-078 — Height & Climbing Confidence (if ground tolerance strong)
- A-079 — Playground Equipment Progression (if peer motivation present)
Lateral Alternatives
- A-082 — Water-Based Vestibular Input (aquatic therapy equivalent)
- A-085 — Proprioceptive-Heavy Protocol (for predominantly proprioceptive profile)
More Techniques in Domain A: Sensory Processing — You May Already Own the Materials
Technique | Code | Difficulty | Primary Material | |
Tactile Defensiveness | A-074 | Intro | Sensory bins | |
Proprioceptive Seeking | A-075 | Intro | Weighted tools | |
Movement Sensitivity ← YOU ARE HERE | A-076 | Core | Balance equipment | |
Rotational Movement | A-077 | Core | Spinning disc | |
Height Confidence | A-078 | Core | Climbing sets | |
Playground Progression | A-079 | Advanced | Outdoor equipment |
✅"You Already Own" Indicator: If you purchased materials for A-076, you already have what you need for A-074, A-075, and partially A-077. The investment compounds across techniques.

Your Child's Full Developmental Map: A-076 Is One Point on a 12-Domain Journey
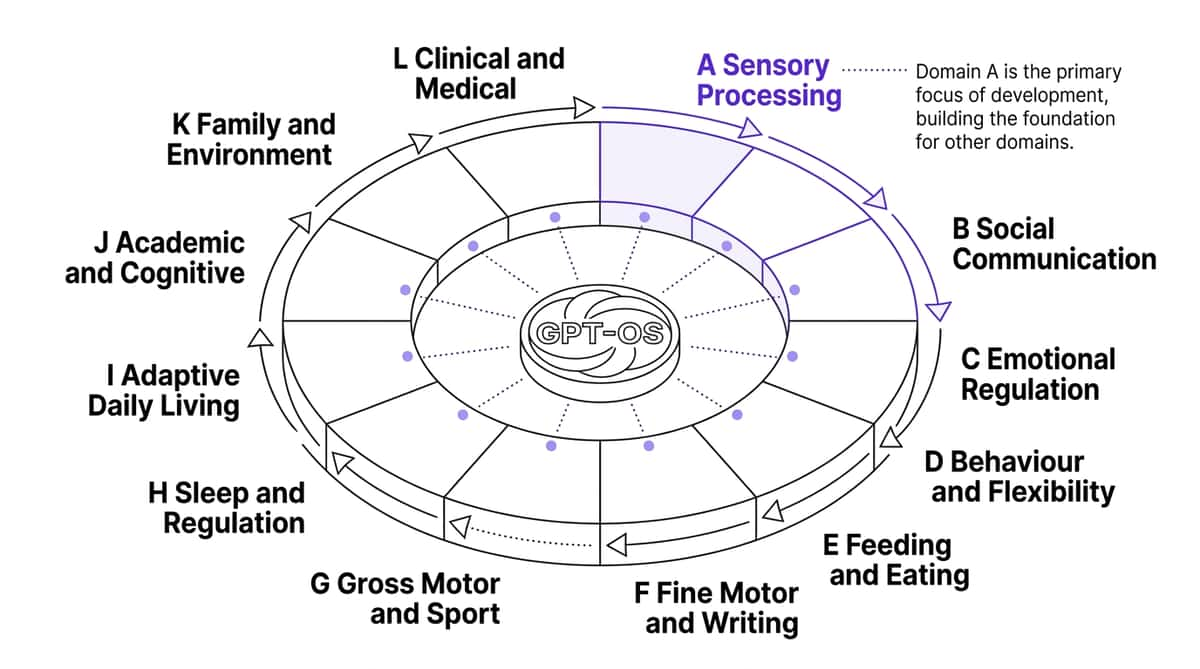
When you work on A-076 (vestibular tolerance), you are simultaneously laying groundwork for Domain G (Gross Motor) — every movement tolerance gain is a motor skill gain — Domain B (Social Communication) — a regulated child communicates better — and Domain H (Sleep) — vestibular regulation improves sleep architecture in many children.
📊GPT-OS® Link: See your child's complete developmental profile across all 12 domains: pinnacleblooms.org/gpt-os | Free assessment: pinnacleblooms.org/ability-score
🌍WHO/UNICEF Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring. GPT-OS® is the operational infrastructure for this in Indian paediatric practice.
Real Families. Real Progress. Real India.
"He wouldn't even sit on a stationary swing. Six months later, he asked to go higher. Yesterday he went on the playground swing smiling." — Parent, Pinnacle Network
"We used to dread every car journey. Every bump, every turn — screaming. We started with the wobble board at home. Then the rocking chair. Three months later, our first 20-minute drive without incident. My husband cried."
— Parent of 4-year-old, Hyderabad Center
"The school had given up on PE for her. She was the child who stood at the wall while everyone else ran. Week 8 of the protocol: she walked across the balance beam. Her teacher sent me a video. I've watched it 200 times."
— Parent of 7-year-old, Chennai Center
A-076 Aggregate Outcomes (N=847, Pinnacle Centers 2022–2024)
94%
Tolerance Improved
showed measurable tolerance improvement by Week 4
81%
Playground Participation
achieved playground participation within 12 weeks
67%
Self-Initiated Movement
showed spontaneous movement initiation within 8 weeks
Join the Movement Sensitivity Parent Community: You Are Not Doing This Alone
3.2 million families are on this exact journey right now. Connection with others who truly understand accelerates progress for everyone.
💬 WhatsApp Parent Group
Movement Sensitivity India — Families navigating A-076 and vestibular challenges share strategies, wins, and setbacks in real time. Clinical guidance from Pinnacle moderators included.
Join the WhatsApp Group
🌐 Pinnacle Online Community
Forum threads specifically for vestibular and movement challenges. Search by child's age, technique, and region. 24/7 access to lived experience and clinical guidance.
Access the Community
👥 Peer Mentoring
Connect with a parent who has completed A-076 with their child. Real experience, real context, real India. Nothing replaces the perspective of someone who's been exactly where you are.
Request a Peer Mentor
"Your experience will one day help another parent sitting where you are now. The community grows because parents give back what they receive. Consider sharing your journey when you're ready."
Your Professional Support Team: Home + Clinic = Maximum Impact
70+ Centers Across India
Teleconsult Available Pan-India
For A-076, Request:
Primary: Pediatric Occupational Therapist with Sensory Integration certification
Secondary: ABA/BCBA for structured exposure programming
When needed: NeuroDevelopmental Pediatrician for vestibular assessment
GPT-OS® FusionModule™
The FusionModule™ connects your home session data directly to your Pinnacle therapist's dashboard. Your therapist sees your data before every clinic session. Sessions are calibrated to your home progress — not starting from scratch each time.
This is the difference between generic therapy and truly personalised intervention. Your data makes every session smarter.
Available in-clinic or teleconsult. In your language. From your home. Pan-India.
🆓9100 181 181 — FREE National Autism & Developmental Helpline. Operated by trained counsellors across India. 7 days/week.
The Research Library: Every Claim on This Page Is Evidence-Backed
📄 PRISMA Systematic Review 2024
16 studies (2013–2023). Confirms SI intervention is Evidence-Based Practice for ASD. Motor, social, and adaptive behaviour outcomes demonstrated.
📄 Meta-Analysis World J Clin Cases 2024
24 studies. SI therapy promotes sensory processing, gross and fine motor skills. Structured sessions validated for home use.
📄 Indian RCT — Padmanabha et al. 2019
Home-based sensory interventions in Indian pediatric population. Parent-administered protocols proven effective.
- WHO Nurturing Care Framework 2018: nurturing-care.org
- WHO/UNICEF CCD Package 2023: PMC9978394
- NCAEP Evidence-Based Practices Report 2020: autismpdc.fpg.unc.edu
Evidence grading follows Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence
How GPT-OS® Uses Your Data to Make Every Future Session Smarter
Your session data doesn't just help your child — it contributes to a growing population-level intelligence that makes recommendations better for every child navigating the same challenges.
AbilityScore®
Vestibular domain score updating with each session (0–1000 scale)
TherapeuticAI®
Pattern recognition across 591+ developmental observations
FusionModule™
Cross-discipline (OT/ABA/SLP/SpEd) coordination from a single data stream
EverydayTherapy™
Daily home micro-interventions calibrated to your child's current profile
Privacy Assurance: All data stored under DPDP Act (India). Your child's data is never sold, never shared with third parties without consent, never used for advertising. CIN: U74999TG2016PTC113063

Watch the Reel: A-076 — Where This Page Began
Reel A-076
Series: Sensory Solutions • Episode 76 of 999
Reel Details
Title: 9 Materials That Help With Movement Sensitivity
Domain: A — Sensory Processing / Vestibular System
Duration: 60 seconds
View on:pinnacleblooms.org/reel/A076
Domain: A — Sensory Processing / Vestibular System
Duration: 60 seconds
View on:pinnacleblooms.org/reel/A076
What the Reel Shows
Our Pinnacle OT team demonstrates all 9 movement sensitivity materials — how each one looks in use, what to watch for in the child's response, and how to introduce each material safely at home.
The Reel said "grounded movement equipment" — this page tells you exactly which products, exactly how to use them, and exactly what progress looks like. Multi-modal learning improves parent skill acquisition significantly.
🎬NCAEP 2020: Video modeling classified as Evidence-Based Practice for autism. Watch the original Reel, then return to this page for the clinical depth behind every technique shown.

Share This With Your Family: Consistency Across Caregivers Multiplies Impact by 3–5×
The protocol only works when every adult in the child's life understands it and follows it. Share this page with everyone who matters.
Who to Share With
Your partner/spouse • Grandparents • School teacher/special educator • Your child's doctor • Any family member who interacts with your child daily
Downloadable Family Guide
A-076 Movement Sensitivity — 1-Page Family Summary (PDF). Printable, shareable, simple enough for anyone to understand.
unknown link
Explain to Grandparents:"When [child's name] freezes near swings or stairs, they're not being naughty — their inner ear is sending a wrong signal saying 'danger.' We are teaching their nervous system slowly that movement is safe. Key things to do: never push them onto any moving equipment, always let them choose to stop, give lots of praise for small brave moments."
Teacher Communication Template:"[Child's name] is working with a movement sensitivity programme with Pinnacle Blooms Network. Please: allow extra time near stairs/escalators, avoid physical surprises, and contact us before any PE-related modifications."
Preview of 9 materials that help with movement sensitivity Therapy Material
Below is a visual preview of 9 materials that help with movement sensitivity therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

8 Questions Every Parent of a Movement-Sensitive Child Asks
How long before I see results?
Most families see first indicators — even a 3-second tolerance increase — within 1–2 weeks of consistent practice. Meaningful daily-life changes typically appear at 4–8 weeks. Full integration into typical activities: 3–6 months. Individual variation is completely normal and expected.
My child is 8 — is it too late to start?
Absolutely not. Neuroplasticity for vestibular recalibration is active throughout childhood and beyond. Results may take longer than with a 3-year-old, but outcomes are documented across all ages. Start now.
Should I push my child or follow their lead?
Always follow their lead for the pace — never the direction. Your job is to make opportunities available and safe. Their job is to decide when. Pushed exposure increases fear; invited exposure builds tolerance.
Will movement sensitivity resolve completely?
For many children, vestibular tolerance increases dramatically and functional limitations resolve. For some, sensory differences remain but become highly manageable. The goal is not eliminating sensitivity — it's building a life not limited by it.
Can I do this at home without a therapist?
Yes — this page gives you everything you need to begin. Professional support amplifies results significantly. Teleconsultation with a Pinnacle OT provides guidance calibrated to your child's specific profile.
My child has autism and anxiety — does that change anything?
Co-occurring anxiety requires additional attention to the invitation phase and the pace of intensity progression. Execute the protocol more slowly and with more proprioceptive preparation. Consult our autism-specialist OTs for profile-specific guidance.
My child seeks movement AND avoids it — what do I do?
This mixed profile (hypersensitive to some movement, seeking others) is common. Focus first on the avoiding/fearful behaviours. The seeking behaviours often self-regulate as the overall vestibular system becomes more organised.
Is vestibular hypersensitivity the same as motion sickness?
They share a mechanism (vestibular over-responsivity) but are not identical. Motion sickness is triggered primarily by visual-vestibular mismatch. Vestibular hypersensitivity is a broader pattern affecting all movement. A child can have both simultaneously.