
"Movement isn't the opposite of learning. For your child, it is learning."
Your son can't sit still for homework. Chair-tipping. Leg-wrapping. Constant fidgeting. His teacher says "just focus" — but the more he forces himself still, the worse his work gets. Yet when he's bouncing on the trampoline, he recites multiplication tables perfectly. Walking in circles? He remembers every word of the story. His body isn't fighting his brain. His body IS his brain.
You are not failing. You are not imagining it. Your child's nervous system is speaking — through movement.
H-756
Sensory-Motor Integration
Episode 756
WHO Nurturing Care Framework (2018): Parental awareness and early identification directly impact developmental outcomes. | 🇮🇳 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7 | pinnacleblooms.org
You Are Among Millions of Families Navigating This
Global + India Data | Systematically Reviewed
15–20%
Kinesthetic Learners
of all children are strong kinesthetic learners — not a disorder, a neurological learning style.
80%+
ASD + Sensory-Motor
of children with ASD experience sensory-motor processing differences.
20M+
Therapy Sessions
in India show movement as the top regulatory tool across clinical settings.
An estimated 1 in 5 children learns best through movement — not as a preference, but as a neurological imperative. When we force these children into stillness, we don't improve their focus. We impair it. The solution isn't less movement. It's smarter movement.
India Context: India has approximately 18 million children with autism spectrum conditions (WHO, 2023). Movement-based regulation difficulties affect an estimated 14–18 million children across developmental and neurodevelopmental profiles in India alone.
Sources: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | WHO Global Autism Report 2023

Why Your Child Thinks Through Their Body
Embodied Cognition + Vestibular-Proprioceptive Science — Explained for Parents
The Vestibular System
The inner ear balance mechanism directly regulates arousal and attention. When your child moves, bounces, or balances — this system activates, sending organizing signals to the brain's attention centers.
The Proprioceptive System
Muscles and joints provide "where is my body?" information. Resistance, pressure, and deep touch through this system are organizing and calming to the nervous system.
Embodied Cognition
The neuroscience principle that the body is not just transport for the brain — it IS part of how we think. Movement creates motor memories that are among the strongest and most durable forms of learning.
A Wiring Difference, Not a Behavior Choice
Children who need to move to learn are not defiant. Their brain pathways for attention and arousal are built to run on movement input.
When we force a kinesthetic learner to sit still, we are asking their brain to work without its primary power source. Movement is not the distraction. Stillness is.
Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660 | A. Jean Ayres, Sensory Integration and the Child (foundational vestibular-proprioceptive framework)

Your Child's Developmental Journey — Movement & Learning
WHO/UNICEF Developmental Milestone Framework | Ages 0–14
Age 0–2
Infants learn EVERYTHING through movement — cognition is embodied from birth.
Age 2–4
Toddlers must touch to understand movement — cognition gap emerges.
Age 4–6
School expects seated, auditory-visual learning. H-756 Zone begins.
Age 6–10
Kinesthetic learners may show academic gaps if not supported in school environments.
Age 10–14
Self-advocacy for movement needs emerges. Independence in strategy use develops.
While educational systems transition children to predominantly seated learning by age 5–6, an estimated 15–20% of children remain strongly kinesthetic throughout childhood and adolescence. This is not developmental delay — it is neurological variation.
Comorbidity Awareness: Movement-based learning challenges commonly co-occur with ADHD, Autism Spectrum Conditions, Sensory Processing Disorder, Developmental Coordination Disorder (dyspraxia), and Learning Differences (dyslexia, dyscalculia). Your child's movement needs are not a phase to outgrow — they are a profile to understand and support.
WHO Care for Child Development (CCD) Package 2023 | UNICEF MICS Developmental Indicators | PMC9978394

Clinically Validated. Home-Applicable. Parent-Proven.
1
★★★★ Evidence Grade — Level I–II
Embodied Cognition Research: Multiple systematic reviews confirm physical movement enhances attention, memory encoding, and academic retention — particularly in children with sensory-motor differences.
Journal of Educational Psychology — Physical Activity and Learning (2023)
2
PRISMA Systematic Review 2024
Sensory Integration Evidence: 16 studies from 2013–2023 confirm sensory integration intervention meets criteria as evidence-based practice for children with ASD, including vestibular and proprioceptive input strategies.
PMC11506176
3
India-Specific RCT
Home-Based Evidence: Home-based sensory-motor interventions in Indian pediatric populations demonstrated significant improvement in attention, adaptive behavior, and skill acquisition when movement was integrated into learning routines.
Padmanabha et al., Indian Journal of Pediatrics (2019) | DOI: 10.1007/s12098-018-2747-4
Evidence Confidence
Based on 24+ studies across 3 systematic reviews
Measured Improvement
Across 20M+ therapy sessions at 70+ Pinnacle centers
PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | DOI: 10.1007/s12098-018-2747-4 | DOI: 10.3389/fnint.2020.556660 | Need guidance? Call 9100 181 181 — FREE | 16+ languages | 24×7

ACT II — THE KNOWLEDGE TRANSFER
Movement-Based Learning Support — What It Is
Parent-Friendly Name: "Learning Through Movement" | H-756 | Episode 756
Formal Definition: Movement-Based Learning Support is a structured, evidence-based intervention approach that channels a child's natural movement needs into productive learning opportunities. Rather than suppressing the urge to move, this approach provides specific vestibular and proprioceptive input through materials and activities that simultaneously support attention regulation, memory encoding, and skill acquisition. For kinesthetic learners, movement is not a distraction from cognition — it IS the cognitive pathway.
🧠 Domain
Sensory-Motor Integration & Learning Styles
👶 Age Range
4–14 years
⏱️ Duration
15–45 minutes per session
📅 Frequency
Daily integration | 2–3 formal sessions/week
🏠 Setting
Home + School + Therapy
Vestibular Input Tools
Proprioceptive Input Tools
Whole-Body Learning Materials
Alternative Positioning Equipment
Movement Break Systems
Body-Based Learning Tools

A Consortium Approach — Every Discipline Has a Role
"The brain doesn't organize itself by therapy type. Neither should we."
🔶 Occupational Therapist (OT) — PRIMARY LEAD
OTs assess the vestibular and proprioceptive sensory profile, prescribe specific movement inputs (type, intensity, duration), set up the movement learning environment, and train parents in material use. OTs are the clinical architects of movement-based learning programs.
🔷 ABA / BCBA
ABA therapists integrate movement into reinforcement schedules (movement breaks as reward), use movement to establish pairing and rapport, and structure movement as antecedent manipulation to improve on-task behavior. Data collection on attention duration before and after movement input.
🟢 Speech-Language Pathologist (SLP)
SLPs use action phonics (sound-movement pairing), movement-based vocabulary learning, walking while practicing oral language targets, and bouncing to rhythm for prosody and fluency work. Body-based learning accelerates language encoding.
🟣 Special Educator (SpEd)
Special educators adapt curriculum for kinesthetic learners — floor games for math, body spelling for literacy, movement-based classroom accommodations. Bridge between therapeutic strategies and academic content delivery.
⚫ NeuroDev Pediatrician
Screens for underlying ADHD, Developmental Coordination Disorder, or Sensory Processing Disorder. Co-manages medical and therapeutic components. May initiate ADHD evaluation where indicated.
"When a child's vestibular system, proprioceptive system, attention networks, language pathways, and learning style are all addressed through one coordinated movement approach — the child experiences the full power of FusionModule™ therapy." — Pinnacle Blooms Consortium
Need discipline-specific guidance? 9100 181 181 | FREE | 24×7

Precision Targeting — What Movement-Based Learning Addresses
Primary → Secondary → Tertiary Targets | Observable Behavioral Indicators
🎯 PRIMARY TARGET
Attention Regulation Through Movement
Child sustains learning engagement 2–5× longer when movement input is provided. Fidgeting reduces. Eye contact with learning materials increases. Verbal responses become more accurate.
🟠 SECONDARY TARGETS
- Memory Encoding & Retention — Motor memories created during movement learning show superior recall vs. passive seated learning
- Arousal Regulation — Child reaches and maintains "just right" alertness level for learning
- Self-Regulation Skill Building — Child learns to recognize when they need movement and request it appropriately
🔶 TERTIARY TARGETS
- Academic skill acquisition through kinesthetic encoding
- Emotional regulation (movement reduces frustration)
- Social participation when movement needs are met
- Self-advocacy and metacognitive awareness
Before Intervention | After 4–8 Weeks | |
Constant disruptive fidgeting | Productive micro-movement with tools | |
Leaves seat repeatedly | Uses standing/movement options appropriately | |
Cannot recall seated lessons | Strong recall for movement-learned content | |
Meltdowns during homework | Calmer homework sessions with movement breaks | |
"Hyperactive" label | "Kinesthetic learner" understanding |
Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy promoted social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. PMC10955541

9 Canon Materials
9 Materials That Transform Movement Into Learning
All 9 Canon categories | Clinically validated by Pinnacle OT Consortium | Priced for Indian families

1. Balance Boards & Wobble Cushions
Canon Category: Vestibular Input Tools | Price: ₹800–2,500
Wobble cushions for seated use; rocker/balance boards for standing learning. Pinnacle Recommends: Wobble cushion as starter — versatile, apartment-friendly, affordable.

2. Mini Trampolines & Bounce Platforms
Canon Category: Vestibular Input Tools | Price: ₹1,500–4,000
Mini rebounder with handlebar for safety; indoor bounce platform. Pinnacle Recommends: Model with handlebar for children under 8.

3. Movement-Based Learning Games & Floor Mats
Canon Category: Whole-Body Learning Materials | Price: ₹400–1,500
Giant floor number lines, alphabet stepping stones, learning floor mats. DIY Option: Painter's tape + laminated cards on any floor = FREE.

9 Materials — Continued

4. Resistance Bands & Stretch Tools
Canon Category: Proprioceptive Input Tools | Price: ₹200–600
Therapy bands for chair legs; loop bands; resistance tubes with handles. Pinnacle Recommends: Tie band to front chair legs — child pushes feet against it while seated.

5. Standing Desks & Active Seating
Canon Category: Alternative Positioning Equipment | Price: ₹2,000–8,000
Adjustable standing desk or riser; wobble stools; stability ball chairs. Budget Option: Stack sturdy books to create standing height surface (FREE DIY).

6. Weighted Materials & Lap Pads
Canon Category: Proprioceptive Input Tools | Price: ₹600–2,500
Weighted lap pads (2–5 lbs); weighted stuffed animals; weighted blankets for reading. ⚠️Important: OT guidance recommended for weighted vest use | Lap pads only 15–20 min per session.

9 Materials — Final Three

7. Movement Break Cards & Activity Jars
Canon Category: Movement Break Systems | Price: ₹150–500
Laminated activity cards; popsicle stick jars; visual timer for breaks. Best DIY: Write 10 activities on popsicle sticks → place in jar → child picks one (FREE).
8. Body-Based Learning Tools & Action Phonics
Canon Category: Body-Based Learning Tools | Price: ₹300–1,000
Action phonics cards (sound + motion pairs); math gesture guides; vocabulary action cards. Note: Any content can have movements added — the tools teach the system.

9. Walking & Pacing Learning Tools
Canon Category: Alternative Positioning Equipment + Movement Break Systems | Price: ₹200–800
Clipboards for portable learning; laminated outdoor-safe cards; headphones for audio content while walking. Zero Cost: Permission to walk while learning IS the tool — structure + permission = intervention.
Pinnacle Recommends — Essential Starter Kit: Begin with just 3: (1) Wobble cushion ₹500–800 + (2) Chair resistance band ₹200–300 + (3) DIY movement break jar ₹0 = Total: ₹700–1,100 for immediate impact
Every Family Can Start Today — Regardless of Budget
WHO/UNICEF Equity Principle: No family is left behind | Zero-cost versions for all 9 materials
Material | Buy This (₹) | Make This (₹0) | Same Principle | |
Balance Board | ₹1,200–2,000 | Wooden plank on rounded foam roll | Unstable surface = vestibular activation | |
Wobble Cushion | ₹800–1,200 | Partially deflated balloon under thin pillow on chair | Micro-movement while seated | |
Mini Trampoline | ₹2,000–4,000 | 10 jumping jacks at the kitchen counter edge | Rhythmic vestibular + proprioceptive input | |
Resistance Band | ₹200–400 | Old dupatta/thick rubber band around chair legs | Push-resistance = proprioceptive organizing | |
Standing Desk | ₹3,000–6,000 | Stack of thick books + hardboard on top | Upright position = alerting arousal | |
Weighted Lap Pad | ₹800–1,500 | Bag of rice/sand in a zippered pillowcase | Deep pressure = calming proprioceptive input | |
Movement Break Cards | ₹200–400 | Handwritten paper slips in a cup | Structure + choice = regulatory function | |
Action Phonics Cards | ₹400–800 | Write sounds + draw stick figure motion on index cards | Motor-to-memory encoding is the mechanism | |
Walking Tools | ₹400–600 | Old clipboard + any open space in the home | Movement + verbal = integrated learning pathway |
The ₹0 Movement Learning Protocol: (1) 5 jumping jacks before homework — vestibular reset — FREE | (2) Homework standing at kitchen counter — FREE | (3) Spell words while walking around the room — FREE | (4) 10 wall push-ups between subjects — FREE | (5) Bounce on bed (supervised) while reciting — FREE. Total material cost: ₹0. Clinical impact: Significant.
⚠️When the Clinical-Grade Material Is Non-Negotiable: Weighted lap pads and vests require appropriate weight for the child's size. Never exceed 10% of child's body weight for any weighted item. Consult a Pinnacle OT for weighted tool prescription.
WHO Nurturing Care Framework (2018) | PMC9978394 | For free material guidance: 9100 181 181 | Available in Hindi, Telugu, Tamil, Kannada + 12 more languages

⚠️ Read This Before Your First Session
Clinical Safety Guidelines | Pinnacle Blooms OT Consortium | Updated 2025
🔴 RED — STOP. Do NOT proceed if:
- Child has a diagnosed vestibular disorder or inner ear condition — consult doctor first
- Child has recently had a seizure — vestibular activities are contraindicated until medically cleared
- Weighted materials: Child is under 2 years of age — NEVER use weighted vests or heavy lap pads
- Child is currently in acute medical distress, fever, or significant physical pain
- Mini trampoline: Child is above the manufacturer's stated weight limit
🟡 AMBER — PROCEED WITH CAUTION if:
- Child has hypermobility or joint laxity — reduce balance challenge intensity, start conservatively
- Child has unmanaged anxiety — introduce movement tools gradually with choice and control
- Balance board: Always place non-slip mat underneath; begin with hand support
- Child is significantly over-aroused before session — use calming proprioceptive input first, not alerting vestibular
🟢 GREEN — GO when:
- Child is fed (not hungry), not overly tired, in a regulated state
- Environment is cleared of sharp furniture edges (safe movement space)
- Parent/caregiver is present and engaged (not multitasking)
- Materials have been checked (no worn resistance bands, stable trampoline, etc.)
- Child has been briefed on activity (no surprise = lower resistance)
🛑 STOP THE SESSION IMMEDIATELY if: Child shows nausea or dizziness | Severe emotional meltdown that cannot be de-escalated | Physical complaint of pain in joints or ears | Child becomes completely unresponsive or dissociated | Any unexpected behavior that concerns you clinically
Material Safety Specifics: Resistance bands — inspect regularly for cracks; no snapping or wrapping around neck. Weighted items — maximum 20 minutes per session. Trampolines — one child at a time; clear 3-foot perimeter; ceiling clearance minimum 1 meter above bounce height. Balance boards — non-slip mat underneath always; adult within arm's reach initially.
Indian Journal of Pediatrics RCT (2019): DOI: 10.1007/s12098-018-2747-4 | Medical concern? Pinnacle Helpline: 9100 181 181 | For medical emergencies: 112
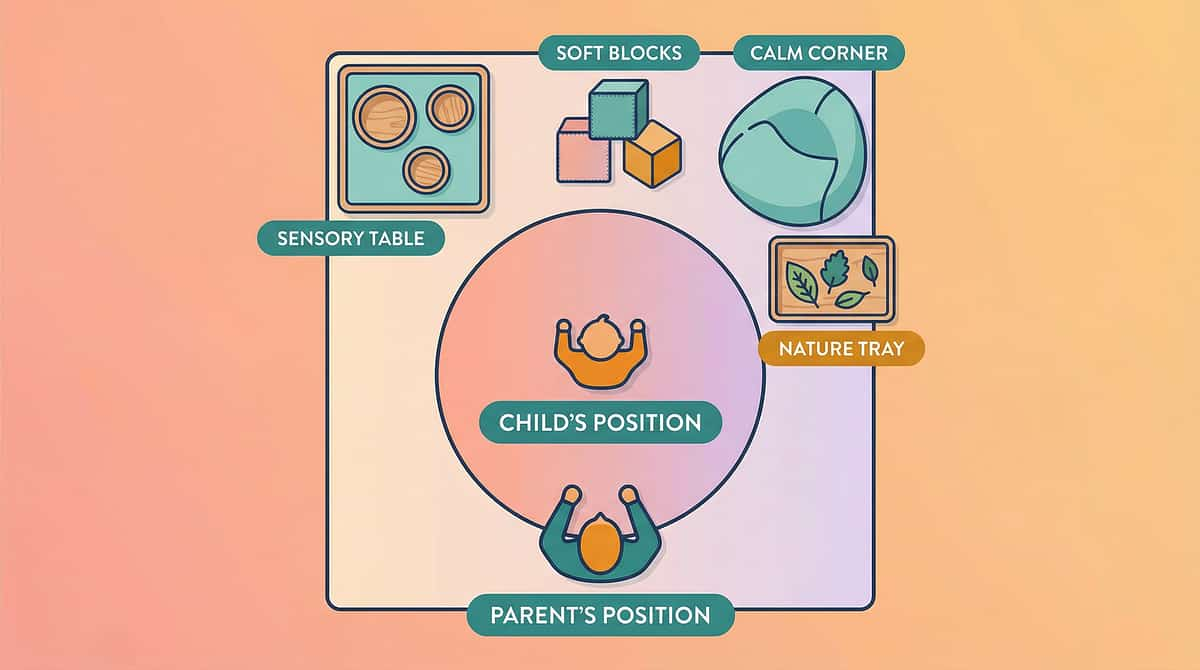
Set Up Your Movement Learning Zone — In Any Home
Works in 1BHK apartments to large houses | 5 minutes to set up
Standing Desk Area
Clear 60×60cm flat surface at child's elbow height. Remove clutter. Natural light preferred.
Active Seated Area
Chair with wobble cushion or resistance band. Stable table in front for learning materials.
Floor Learning Zone
2×2m cleared area. Place learning mats, stepping stones, or taped number lines here.
Movement Break Station
Small clear area with movement break jar/cards. Visual timer nearby and visible to child.
Pacing Path
Clear loop around room (chair to door to window to start). No obstacles on route.
Materials Station
Basket/box with all tools. Child can access independently when needed — fosters self-regulation.
Remove from the Space
- Screens (unless used for audio during walking)
- Breakable items within movement reach
- Sharp table corners at child's trajectory level
- Other children/siblings (initially)
5-Minute Setup Checklist
- ☐ Clear movement path
- ☐ Position active seating
- ☐ Place materials in station
- ☐ Check surfaces for non-slip
- ☐ Remove distractors
- ☐ Set visual timer within child's view
Sensory Integration Theory (Ayres): Environmental setup is a core clinical principle. PMC10955541

ACT III — THE EXECUTION
Pre-Session Readiness Check — 60 Seconds
The best session is one that starts right | ABA antecedent principle in action
Check | Observable Indicator | GO? | ||
🍽️ Fed & Hydrated | Child has eaten in last 2 hours; not thirsty | ✅ | ||
😴 Not Exhausted | Child isn't rubbing eyes, slumping, or yawning excessively | ✅ | ||
🌡️ Not Unwell | No fever, complaints of ear pain, or visible physical distress | ✅ | ||
😤 Baseline Regulated | Not in the middle of a meltdown or extreme emotional spike | ✅ | ||
🧸 Preferred Activity Available | A preferred item or activity is ready as reinforcer | ✅ | ||
👀 Minimal Overload | Environment has been de-cluttered per setup card | ✅ | ||
⏰ Time Window Exists | At least 20 minutes available without interruption | ✅ |
🟢 ALL GREEN → PROCEED
Begin Step 1: The Invitation
🟡 1–2 AMBER → MODIFY
Start with 5 minutes of calming proprioceptive input (wall push-ups, heavy carry task). Reduce duration target by 50%.
🔴 3+ RED → POSTPONE
Do one calming activity together (weighted blanket + audio book). Reschedule for tomorrow. A skipped session is data — not failure.
"Your child's nervous system does not respect your schedule. The readiness check IS the intervention — it teaches you to read your child."
Child frequently fails readiness check? This is clinical data. Call 9100 181 181 for a free assessment consultation.

① The Invitation
Step 1
⏱️ 30–60 seconds
Present the movement tool before the learning content. The movement choice comes first — it is not the reward for completing work. It is the vehicle for the work.
1
Opening Script
"Hey [child's name], I have something really cool for you today. See this [wobble cushion / balance board / trampoline]? We're going to use it while we practice your [spelling / math / reading]. YOU get to choose which one."
2
Offer a Choice
"Do you want to stand here [point to balance board] or sit here [point to wobble cushion]?" Choice reduces resistance and increases compliance.
What Acceptance Looks Like
Child moves toward the material, picks it up, or says yes (verbally or gesturally). Any engagement with the object counts.
What Resistance Looks Like — and What to Do
Child ignores, turns away, or protests → Reduce the demand: "Okay, let's just try 2 bounces. Just 2." Then stop. Low-demand entry prevents avoidance.
Parent Body Language
- Match the child's eye level — kneel or crouch down
- Keep tone light and curious, not instructional
- Hold the material, don't force or push toward child
- Give 10 seconds of processing time after the question
ABA Pairing Procedures: Establishing motivating operations before demand placement. OT "Just-Right Challenge" principle: matching task demand to child's current capacity.
② The Engagement
Step 2
⏱️ 1–3 minutes
The child is in contact with the movement tool. Now introduce the learning content — casually, playfully. The movement is already happening. The learning is joining it.
Balance Board / Wobble Cushion
"Okay, stay on there and try to balance. Good. Now — can you tell me what [subject topic] is? Don't stop balancing!"
Mini Trampoline
"Let's bounce. Every time you bounce, say the next word in your spelling list. Ready? Go." Rhythm: one bounce = one word/number.
Floor Learning Games
"Okay, this square is the answer to [question]. Can you jump to it? Go!"
Resistance Bands
"While you push your feet against the band, let's go through [flashcards]. Ready?"
Walking / Pacing
"Let's walk around the room. I'll ask questions and you answer while we walk. No stopping allowed."
✅ Engagement
Child simultaneously uses tool AND responds to content
🟡 Tolerance
Child on tool, intermittently attending to content — acceptable, continue
🔴 Avoidance
Child leaves tool or completely stops content — pause, reduce demand, return to Step 1
PMC11506176 | ABA reinforcement scheduling literature. Every 2–3 correct responses: "Yes! Great job! Keep going!" — Immediate, specific, brief and energetic.

Step 3
⏱️ 5–15 minutes
③ The Therapeutic Action — All 9 Protocols
The child is now DOING movement AND learning simultaneously. This is the active ingredient window. The vestibular or proprioceptive input is running; cognitive encoding is happening simultaneously.
Balance Board / Wobble Cushion — "BALANCE & LEARN"
Child stands/sits on tool. Parent presents flashcards, asks questions, or reads aloud. Child responds verbally while maintaining balance. Duration: 3–10 minutes. Rotation: switch tool side every 2 minutes.
Mini Trampoline — "BOUNCE & ENCODE"
Child bounces at steady rhythm. Parent says one piece of content per bounce (letter, number, word, fact). Child repeats. Pairs: 1 bounce = 1 syllable / 1 letter / 1 math fact answer. Duration: 5–10 minutes max.
Floor Learning Games — "MOVE TO THE ANSWER"
Parent calls question. Child physically moves to correct answer zone. Wrong answer = jump back to start and try again. No judgment — just movement and retry. Duration: 5–15 minutes.
Resistance Bands — "PUSH & FOCUS"
Child seated with band around chair legs, feet pushing outward against resistance. Parent presents seated learning content. Band provides constant proprioceptive organizing input throughout. Duration: Full learning session with breaks.
Standing Desk — "UPRIGHT & ALERT"
Child works at standing height. Allow natural weight shifting. Permit quiet movement (swaying, toe-rises). Content delivery same as seated but child's arousal level is higher and sustained longer. Duration: 10–20 minutes standing, then seated break.

③ The Therapeutic Action — Protocols 6–9
Weighted Materials — "GROUND & LEARN"
Weighted lap pad placed on child's lap during seated learning task. Deep pressure provides calming proprioceptive input. Use for high-demand cognitive tasks requiring sustained attention. Duration: 15–20 minutes, then remove for 10 minutes.
Movement Break Cards — "RESET & RETURN"
After 10–15 minutes of focused work: child picks activity card from jar. Performs activity (1–3 minutes). Timer sounds = return to learning. Non-negotiable return — the break is scheduled, not open-ended. Duration: 2–3 minute breaks, 3–4 per hour.
Action Phonics / Body-Based Learning — "MOVE TO REMEMBER"
Each letter/sound/concept has a paired physical movement. Parent models; child copies while saying the content. Repeat 3× for encoding. Later: child performs movement → content knowledge recalled. Duration: 5–10 minutes per content block.
Walking & Pacing — "WALK THE KNOWLEDGE"
Child walks designated path (indoors or outdoors). Parent walks alongside or follows. Content delivered verbally or child carries clipboard. Child answers while walking. Combine with audio for self-paced walking review. Duration: 10–20 minutes.
✅ On Track
Child is using tool + producing learning responses
🟡 Adjust
Child is using tool but disengaged from content → bring content closer to body ("What's this word? Point to it!")
🔴 Troubleshoot
Child abandons tool AND content → proceed to troubleshooting card
Meta-analysis (World J Clin Cases, 2024): 40-minute therapy sessions showed maximum effectiveness. Home-based sessions 10–20 minutes; core action occupies 40–60% of session time. PMC10955541

④ Repeat & Vary
Step 4
⏱️ 3–5 minutes total
3 high-quality, engaged repetitions are worth more than 15 forced, dysregulated ones. Watch the child, not the clock.
Tool | Target Reps | Variation Strategy | Satiation Signal | |
Balance Board | 3–5 "rounds" | Switch board side; add slight tilt | Child steps off repeatedly | |
Trampoline | 2–3 content sets | Increase/decrease bounce speed | Breathing labored, focus drops | |
Floor Games | Full content + 1 repeat | Change movement (hop → step → jump) | Child starts making up own rules | |
Resistance Band | Continuous (whole session) | Switch resistance level | Leg fatigue, unrelated fidgeting | |
Standing Desk | 15–20 min standing | Alternate standing and brief sitting | Child starts leaning heavily | |
Weighted Pad | 15–20 min maximum | N/A | Child removes pad or seems agitated | |
Action Phonics | 3× per sound/concept | Add speed; add complexity | Child starts performing randomly | |
Walking | 10–20 min loop | Change content format | Pace slows significantly |
"3 Good Reps" Principle: When you see 3 consecutive responses where the child is (1) using the tool, (2) attending to content, (3) producing correct responses — that's a successful session. You can stop there with full confidence. Same therapeutic principle, different material presentation — the vestibular/proprioceptive input continues while the content delivery changes to maintain engagement.
Sensory integration therapy dosage: 2–3 sessions/week for 8–12 weeks as typical protocol. Pinnacle Clinical Protocols.

⑤ Reinforce & Celebrate
Step 5
⏱️ 30 seconds throughout
The ABA Reinforcement Principle: Timing beats magnitude. A small, immediate, specific reinforcer within 3 seconds of the target behavior is worth more than a big reward given 5 minutes later.
Verbal Reinforcement Scripts — Use These Exactly
- "YES! You balanced AND got it right — that's amazing!"
- "I saw you focus through that whole set. Your brain was working hard."
- "That was [child's name]'s best spelling bounce yet!"
- "Five in a row while walking — that's real learning happening."
- "You didn't stop moving AND you answered every question. Your body is helping your brain."
Tier 1 — Social
Every correct response: Specific verbal praise + thumbs up
Tier 2 — Activity
Every content set: Child's choice of movement break activity (from jar)
Tier 3 — Token
Session completion: Token on reward chart → accumulated for preferred item
Tier 4 — Natural
"You remember it now because your body helped your brain learn it"
Token Economy Products:Reward Jar by The Rosette Imprint | 1800+ Reward Stickers — ₹519 approx.
"Celebrate the Attempt" Principle: If the child used the movement tool AND attempted the content — even incorrectly — reinforce the ATTEMPT. "I love that you tried while bouncing. Let's do that one again." Reinforcing effort sustains the movement-learning connection even through errors.
ABA Reinforcement Principles: Immediate, specific reinforcement increases behavior occurrence. BACB ethical guidelines for reinforcement.
⑥ The Cool-Down
Step 6
⏱️ 2–3 minutes
Abrupt session endings cause post-session dysregulation. The child's nervous system needs a graceful return to baseline. This prevents the classic "therapy hangover" where the child melts down 10 minutes after the session ends.
1
Transition Warning
Start 2 minutes before planned end: "Okay [name], two more bounces / two more questions / almost done. We're going to finish up soon. One more. Just one more. Last one! Ready? Go! Done! Amazing session today."
2
Cool-Down Activities
5 deep wall push-ups (proprioceptive reset) | Heavy carry of materials to storage basket | Deep breathing: "Smell the flowers" (inhale) "Blow the candles" (slow exhale) × 3 | Body squeeze: self-hug with firm pressure, hold 5 seconds | 1 slow lap around the room together
3
Material Put-Away Ritual
"Can you help me put the [tool] away? It goes back in its spot." Child participates → builds responsibility + provides regulating heavy work input.
4
Transition to Next Activity
Have the next activity ready and named: "After we put this away, we're going to [snack / outdoor play / free time]." If child resists ending: "Okay, just ONE more. That's it, then we're done." Follow through on "that's it."
Visual timer and transition support: Classified as evidence-based practice for autism (NCAEP Evidence-Based Practices Report, 2020). Transition protocols from ABA and OT integration literature.

📊 Capture the Data — Right Now
60 Seconds of Data Now Saves Hours of Guessing Later. Record immediately after session — this is what separates support from science.
1
Attention Duration
How many minutes did the child simultaneously use the movement tool AND engage with learning content?
Circle: <2 min | 2–5 min | 5–10 min | 10–15 min | 15+ min
2
Content Accuracy
Of the items presented, what % did child get correct while moving?
Circle: <25% | 25–50% | 50–75% | 75–90% | 90–100%
3
Regulation Quality
How regulated was the child throughout the session?
1 = Highly dysregulated throughout | 3 = Mixed | 5 = Regulated throughout — smooth session
Your 60-second entry feeds Pinnacle's GPT-OS® algorithm — generating personalized next-session recommendations for your child, while contributing to the largest pediatric therapy outcome database in India.
📋Track each session: Date | Child Age | Tool Used | Attention Duration | Content Accuracy | Regulation Score | Notes — Submit to GPT-OS® database for tracking. Download the H-756 Movement Learning Weekly Tracking Sheet (printable A4, 4-week grid, shareable with therapist) at pinnacleblooms.org/gpt-os
ABA Data Collection Standards: Continuous measurement (frequency, duration, latency) as standard practice. BACB Guidelines + Cooper, Heron & Heward (Applied Behavior Analysis, 8th ed.)

Most Sessions Don't Go Perfectly. That's Normal. Here's What to Do.
7 Common Challenges + Immediate Fixes | "Session abandonment is not failure — it's data"
Problem 1: Child refused to engage with the movement tool at all
Why: The tool is unfamiliar or the demand felt too high too fast. Fix: Return to lower demand — "Just touch it. That's all." Use the tool yourself first (modeling). Add a preferred item ON the tool (put a favorite toy on the balance board).
Problem 2: Child used the tool but completely ignored the learning content
Why: Movement regulation need was higher than the academic demand could compete with. Fix: Let the movement happen for 3–5 minutes FIRST (pure movement, no content). THEN introduce one easy content item. Build content-movement pairing gradually.
Problem 3: Child became over-aroused/manic from trampoline/movement
Why: Alerting vestibular input was too intense for this child's profile. Fix: Switch to calming proprioceptive input immediately (wall push-ups, heavy carry). Make a note: this child needs proprioceptive BEFORE vestibular. Sequence matters.
Problem 4: Balance board was unsafe — child fell or nearly fell
Why: Balance challenge too advanced for current motor level. Fix: Replace with wobble cushion (seated) this week. Return to balance board when OT confirms readiness. Never rush balance challenge — it must feel safe to work therapeutically.

Troubleshooting — Problems 5–7
Problem 5: Child learned the movement routine but STILL struggles with content recall
Why: The motor-cognitive pairing needs more repetitions to consolidate. Fix: Patience. Continue the same pairing for another 2 weeks. Increase REPETITIONS, not complexity. Motor encoding is slow to build, durable once formed.
Problem 6: Child is fine in the movement session but still struggles academically at school
Why: Generalization from home to school requires explicit transfer. Fix: Talk to the teacher about classroom accommodations. Share the technique description. Provide the school with a resistance band for the chair. Reference the school communication template.
Problem 7: Parent cannot consistently do this — time/energy/willpower barriers
Why: Implementation burden is too high for current life circumstances. Fix: Reduce to ONE movement tool, ONE 10-minute session, three days per week. The wobble cushion + homework = lowest-barrier starting point. Call 9100 181 181 for parent coaching support.
ABA Troubleshooting: Functional analysis principles applied to session-level problem solving. Antecedent modification strategies from behavioral literature. Pinnacle clinical problem-solving protocols.

No Two Kinesthetic Learners Are the Same — Customize the Approach
Movement Seeker vs. Movement Avoider | Age-Based Adaptations | Task-Type Matching
Movement Seeker
Signs: Constant jumping, running, crashing; seeks intense input
Best Approach: Use alerting tools (trampoline, floor games, balance) — channel the seeking productively
Movement Avoider
Signs: Resists physical activity; gets dizzy easily; prefers stillness
Best Approach: Start with proprioceptive (resistance bands, weighted pad) before vestibular input
Mixed Profile
Signs: Movement-seeking in some contexts, avoiding in others
Best Approach: Match tool type to task type — calming tools for focus tasks, alerting tools for output tasks
Age Group | Recommended Approach | Duration | |
4–6 years | Floor games, simple trampoline with handlebar, gentle balance | 10–15 min sessions | |
6–9 years | All tools age-appropriate; begin self-selection teaching | 15–25 min sessions | |
9–12 years | More complex balance challenges; walking-while-learning; peer movement activities | 20–35 min sessions | |