

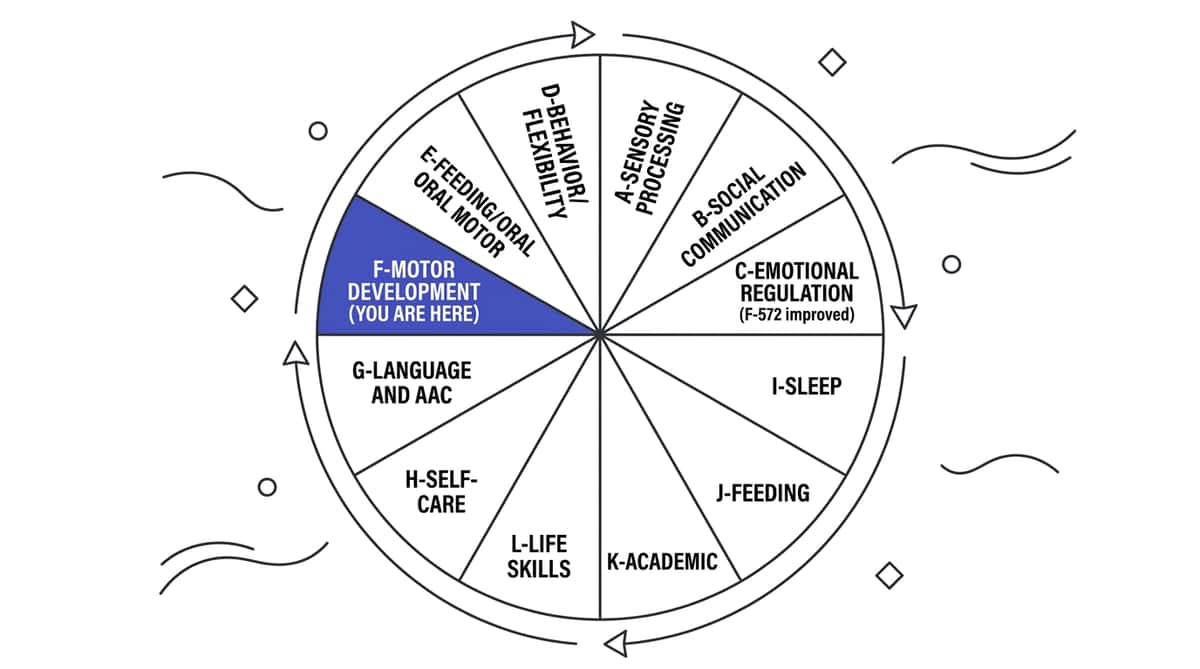
When Their Body Works Harder Than Everyone Else's
It is 9:15 AM. The school bell rang twelve minutes ago. While their classmates write in their notebooks without a second thought, your child is already slumped — shoulders rounded, spine curved into a question mark, head drifting toward the desk. The pencil feels like a ten-kilogram weight. By afternoon, they will be draped over the table, not because they are bored, but because their body has spent everything it has just staying upright. You have been told it is "just low muscle tone." You have been told they might grow out of it. They haven't. And you are watching them fight for every physical task that other children execute without a thought. Low muscle tone is not a life sentence. Strength can be built. Endurance can be developed. Your child can close the gap — and these 9 materials are where that journey begins. "You are not failing as a parent. Your child's nervous system is working at a different baseline — and that baseline can be trained upward. You are in the right place." — Pinnacle Blooms Consortium | OT • PT • ABA • SpEd • NeuroDev 📖 WHO Nurturing Care Framework (2018): Early caregiver awareness and targeted intervention directly shapes developmental trajectories.

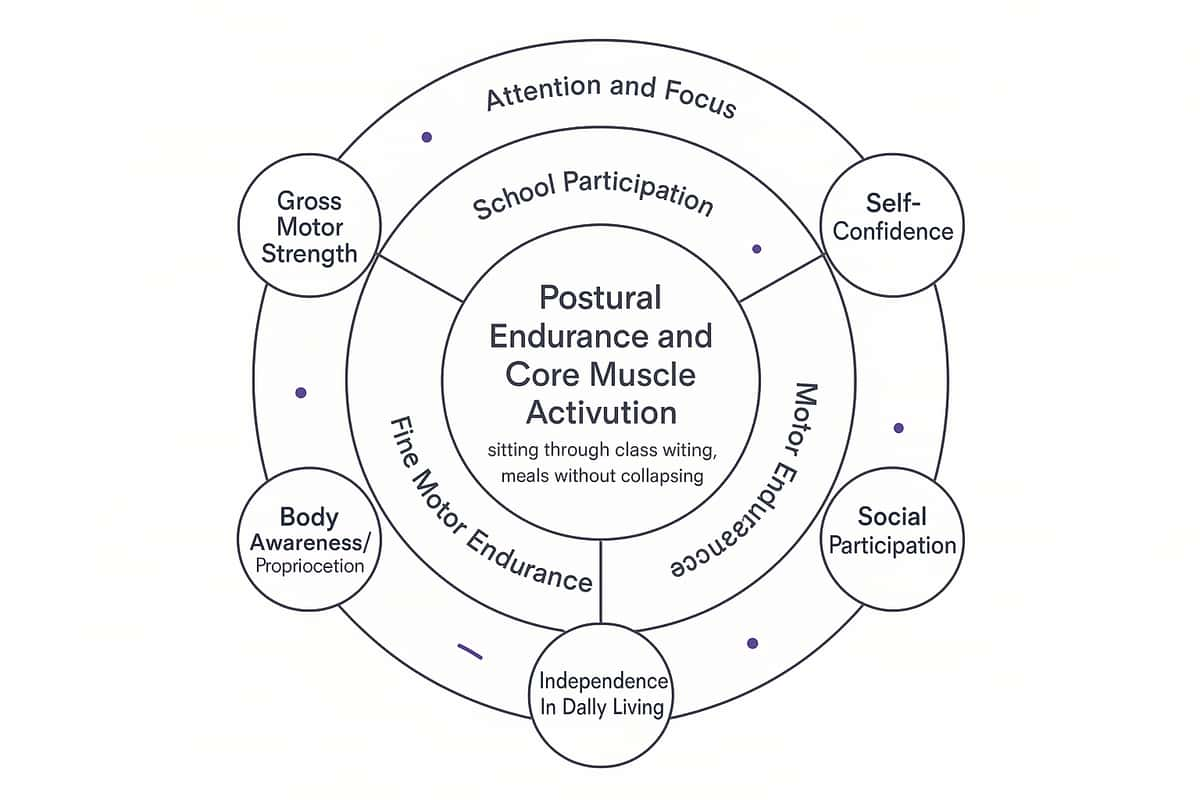
- Postural control: Holding the body upright against gravity
- Gross motor endurance: Running, climbing, playground activities
- Fine motor endurance: Writing, drawing, cutting, buttoning
- Oral motor function: Speech clarity, mealtimes




Clinical Material | ₹0 Household Alternative | Why It Works | |
Therapy Ball | Large, firm beach ball (₹80–150 at local markets) | Same unstable surface principle — use for short periods, monitor stability | |
Peanut Ball | Firm sofa cushion folded around child's waist for prone positioning | Supports the prone position while requiring some core engagement | |
Wedge Cushion | Firmly folded blanket/towel roll (2–3 inches high) placed under front edge of sitting surface | Creates the same anterior pelvic tilt — replace when it compresses flat | |
Resistance Bands | Old nylon stockings (tied in loop) or cut bicycle inner tube | Provides resistance for simple pulling exercises — functional for starting | |
Scooter Board | Smooth wooden board (30×45cm) with 4 furniture casters | Identical function if built correctly — requires adult construction and supervision | |
Compression Vest | Snug-fitting lycra/compression undershirt under clothes | Provides gentle trunk compression and body awareness | |
Foot Rest | Stack of firm textbooks or a shoebox filled with sand | Any stable surface at correct height — must not wobble | |
Crawling Tunnel | Blanket over dining chairs in a row | Creates crawling motivation — modify height for different challenge levels | |
Pencil Grips | Rubber bands wrapped around pencil barrel (3–4 layers) OR triangular crayon pieces | Increases diameter, reduces grip force requirement |
- Child shows signs of illness, fever, or unusual fatigue today
- Child has had a significant fall or injury in the past 24 hours
- Undiagnosed or worsening motor condition with progressive symptoms
- Resistance bands are torn, frayed, or show wear marks
- Child is in acute emotional distress or meltdown state
- Joint hypermobility — reduce band intensity, ensure joint support
- High sensory sensitivity — introduce compression vest gradually
- Down syndrome — follow specific Down syndrome exercise guidelines
- Oral motor low tone — coordinate with SLP before oral motor exercises
- Floor cleared of tripping hazards within 2 metres
- Ball properly inflated (firm, not rock-hard)
- Resistance bands inspected — no tears, proper anchoring
- Child's shoes/socks: non-slip for ball activities
- Foot rest positioned and stable before child sits
- Unusual joint pain or clicking during exercises
- Sudden pallor, excessive sweating, or shortness of breath
- Falls from therapy ball (reassess sizing and stability)
- Skin irritation under compression vest

- Ball at homework desk — remove chair
- Wall within arm's reach for safety reference (not leaning, just reassurance)
- Feet touch ground (correct ball size confirmed)
- Parent seated nearby for first 2 weeks
- 4m × 2m clear smooth floor area minimum
- All furniture edges padded or cleared from path
- Obstacles pre-arranged before child enters
- Parent at start/finish — let child work independently
- Chair secured (band looped under chair leg for seated exercises)
- Or parent holds band ends for facing exercises
- Standing space clear — 1m in all directions
- Applied during dressing routine or at desk
- Timer set for 20–30 minute wear windows
- Child has chosen preferred activity during wear
Lighting | Bright natural light — task clarity critical for motor feedback | |
Sound | Moderate — avoid sensory overload that drains cognitive resources | |
Duration | Start: 10–15 min. Build to 20–30 min over 4 weeks. | |
Distractions | TV off. Siblings in separate space for focused sessions. |

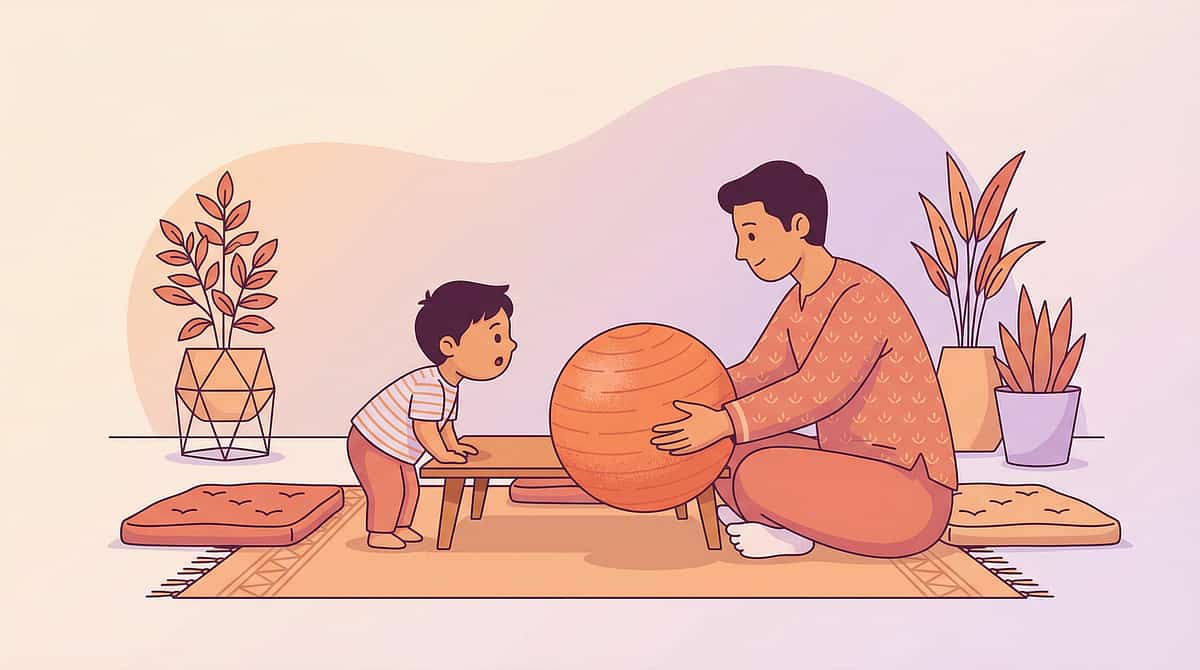
Parent Script:"Hey [name], I set up something fun for us! Want to see? It's your [therapy ball / scooter board / obstacle course]..." (Keep the language positive, inviting, never obligatory)
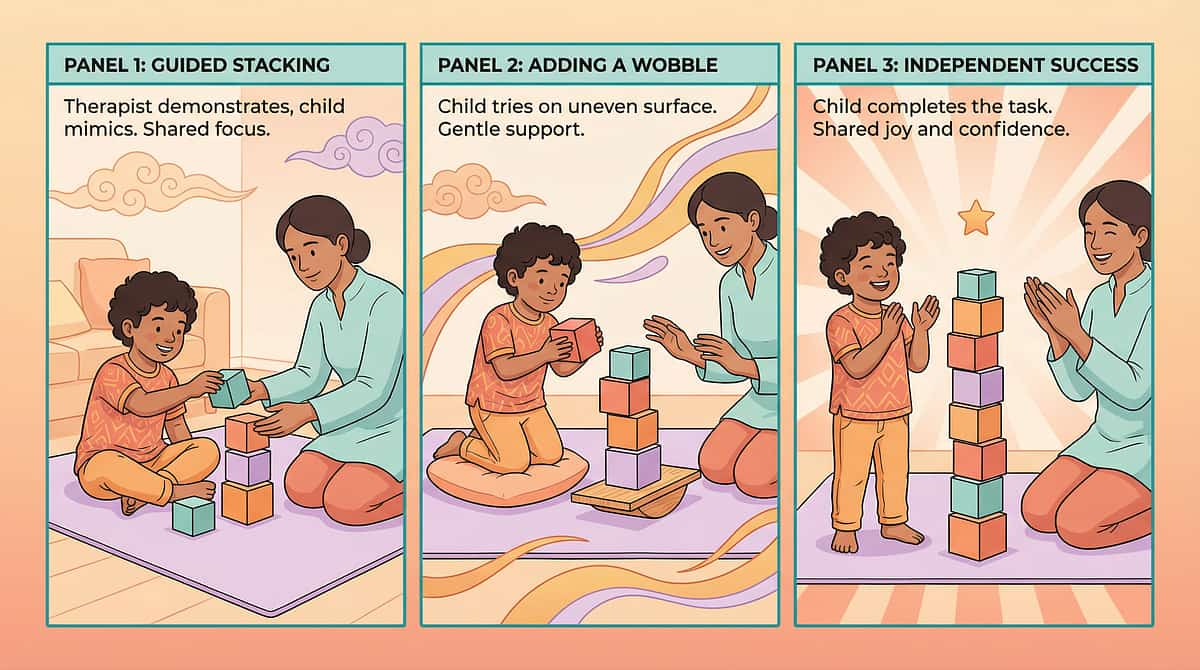
"I got the [therapy ball/scooter board] out! Want to try something? You don't have to — I just thought it looked fun."For more resistant children: "I'm going to do the obstacle course. Want to watch first? You can join any time."
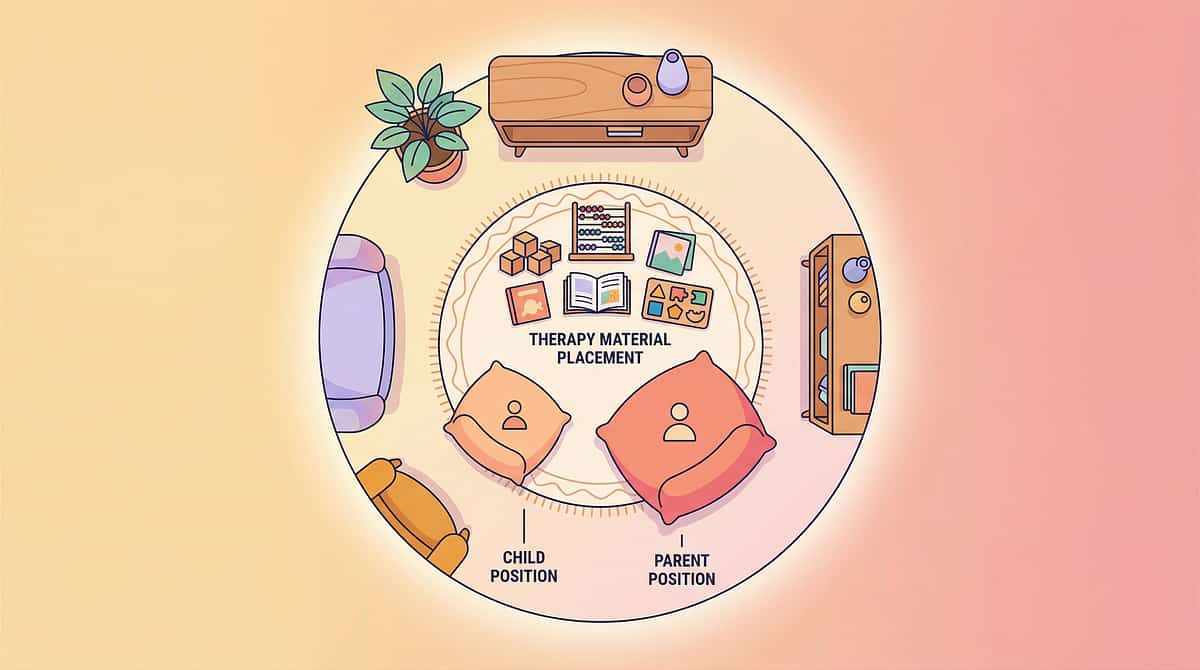
- Position: At child's level, not towering above
- Expression: Enthusiastic but relaxed — not anxious about whether they'll cooperate
- Distance: Within arm's reach but not blocking
- Body: Open posture, facing the equipment, not the child
- Child moves toward the equipment
- Child watches with interest
- Child asks a question about it
- Child picks up or touches the material
- Child turns away → Narrate what you're doing: "I'm bouncing on the ball. It's bumpy!"
- Child says "no" → "Okay! I'll just do it myself for a bit." (Continue without pressure)
- Child becomes distressed → Postpone. Come back tomorrow with lower demand presentation.

Response | What It Means | Action | |
Active engagement | Optimal — proceed | Reinforce, continue | |
Passive tolerance | Acceptable — build slowly | Maintain, don't push further yet | |
Mild avoidance | Needs adjustment | Simplify, reduce demand | |
Active refusal | Session not working | Modify or postpone |

Material | Target Reps | Rest Between | Sessions/Week | |
Therapy ball sitting | 1 session (duration) | N/A | Daily | |
Prone peanut ball reaches | 5–10 reps | 20s between | 5×/week | |
Resistance band rows | 8–12 reps × 2 sets | 30s between sets | 4–5×/week | |
Scooter board runs | 5–8 runs | 30s between | 4–5×/week | |
Obstacle course circuits | 2–3 circuits | 1 min between | Daily |
- Ball sitting → Ball sitting while catching/throwing
- Prone over ball → Prone reaching for named objects
- Prone over ball → "Row the boat" rocking
- Seated rows → Overhead press → Bicep curls
- Bilateral → Unilateral (more core demand)
- "Superhero training" narrative framing
- Straight runs → Cone slalom
- Prone → Supine (lying on back, legs push)
- Individual → Parent-child (parent gently pulls rope)
"YES! Did you feel your tummy muscles working? That's your body getting STRONGER!""You did 8 pulls! Last week was 5! You are BUILDING strength!""Your posture looked great on the ball today — your back was so straight!"
- High-five + specific verbal praise
- "Therapist's record book" — child writes/stamps their reps
- Parent physically demonstrating excitement
- Sticker chart: 1 sticker per session → 10 stickers = agreed reward
- "Strength points" visual tracker on wall
- Progress photo: same activity, weeks apart — visible growth
- "You did your circuits — now 15 minutes of your choice activity"
- Preferred snack immediately after session
- Sibling/parent competition element
"Two more scoots, then we're all done!""One more circuit — make it your best one — then rest time.""Last pull — strong finish!" (Always pre-warn transitions. Abrupt endings cause resistance to starting next time.)


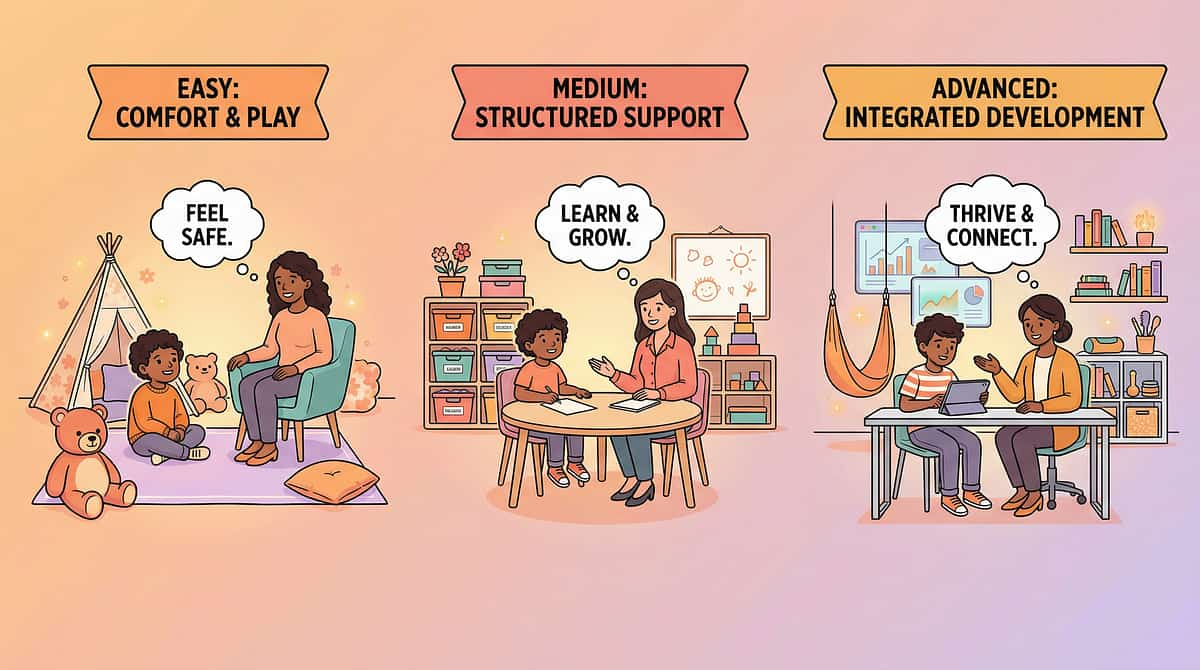
- Focus on peanut ball and floor activities
- Obstacle courses are the primary vehicle (not "exercises")
- 5–10 minute maximum per session
- Parent modelling is the primary teaching tool
- Introduce therapy ball sitting for homework
- Resistance bands in game format
- Scooter board racing with siblings/parent
- Pencil grips for all school writing
- Longer strengthening circuits (15–25 minutes)
- Resistance band "workout" framing (older children respond well)
- Self-monitoring with personal tracking chart
- School accommodation package as standard
- Increase intensity: heavier band, faster scooter board, more bouncing
- Add crash pad at end of obstacle course
- Weighted vest more beneficial
- More proprioceptive input in warm-up
- Introduce materials more slowly — days of exploration before use
- Less bouncing, more static ball sitting
- Compression vest over weighted vest
- Quieter environment, predictable routine

- Child tolerates ball sitting for 3–7 minutes (from less or zero)
- Slight reduction in slumping speed — slightly longer before posture collapses
- Child begins to anticipate and accept the session routine
- First resistance band repetitions possible (even if only 3–5 reps)
- Obstacle course completed once (even if slowly)
- Sustained independent postural control (comes at weeks 5–8)
- Obvious strength gains visually
- Spontaneous use of correct posture without cueing
"If your child tolerates the ball for 4 seconds longer than Day 1, that is measurable neurological progress. The muscle fiber recruitment patterns are changing. The proprioceptive map is being drawn. You may not see it yet — but it is happening."
"You will notice your child starting to use slightly better posture even outside the therapy time. This is generalization — the neural pathway activated during structured sessions starting to fire in other contexts. This is THE sign that intervention is working."
GPT-OS® Readiness Index | Before F-572 | At Mastery | |
Postural Control RI | Level 1–2 | Level 3–4 | |
Motor Strength RI | Level 1–2 | Level 3–4 | |
Physical Endurance RI | Level 1–2 | Level 3 |
"Eight weeks ago, your child was slumping through every seated activity, avoiding playgrounds, and coming home exhausted from simply existing in a school. You chose to understand rather than accept. You chose to act rather than wait. You set up the space, you did the sessions on the hard days, you captured the data, you adapted when things didn't work — and you kept going.Your child's muscles did not change. Their tone is the same. But their STRENGTH is different now. Their endurance is different. Their confidence in their own body is different. And that happened because of you." — Pinnacle Blooms Consortium







"He didn't change overnight. But every week there was one thing he could do that he couldn't the week before. That kept us going." — Arjun's mother
"The peanut ball was the breakthrough. She stopped fighting tummy time when it was 'playing in the valley'." — Priya's mother
You Don't Have to Do This Alone
Isolation is the enemy of adherence. Community multiplies outcomes. 📱 WhatsApp: Motor Development Parent Circle Parents navigating low muscle tone, hypotonia, and motor delays — sharing strategies, celebrating wins, asking questions. → Request to Join via 9100 181 181 🌐 Online Forum pinnacleblooms.org/community — Domain F (Motor Development) parent section. Moderated by Pinnacle therapists. Evidence-based discussions. 🤝 Peer Mentoring Connect with a parent who has completed F-572–F-580 with their child. Real experience, practical guidance. → Request a Peer Mentor via 9100 181 181 📍 Local Parent Meetups Monthly in-person gatherings at 70+ Pinnacle centers across India. → Find Your Nearest Center: pinnacleblooms.org/centers "Your 8 weeks of experience is priceless to the parent starting Week 1 today. Consider sharing your journey — your child's progress story becomes someone else's hope." 📖 WHO NCF: Parent support networks improve adherence and outcomes across pediatric intervention programs. 📞 9100 181 181 | 16+ languages | 24×7


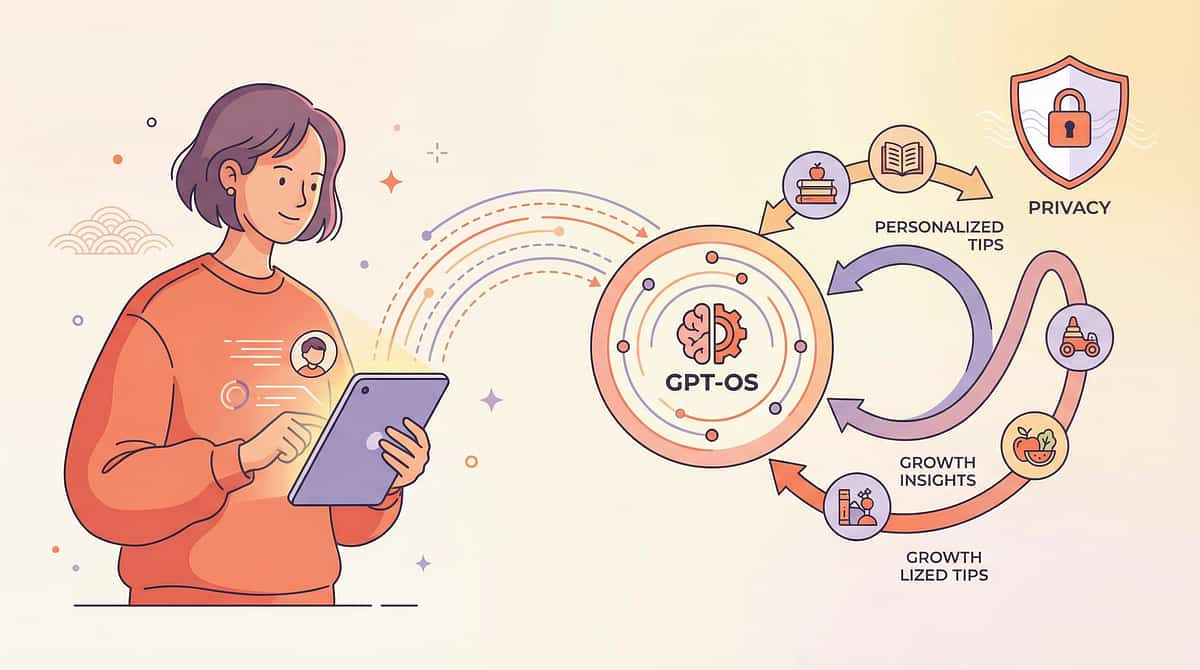
- Your child's motor strengthening response rate vs. age-matched norms
- Which materials yield the best engagement/outcomes ratio
- Optimal session timing and duration for this child's profile
- Readiness triggers for F-573 progression
- All data de-identified at source
- Stored under ISO 27001-equivalent standards
- Never sold to third parties
- Parent controls data access and deletion
- Governed under India IT Act compliance framework
"When your child's data enters GPT-OS®, it joins 20 million+ session records. The patterns from those 20 million sessions make the recommendation for your child more precise. Your data helps every child like yours."

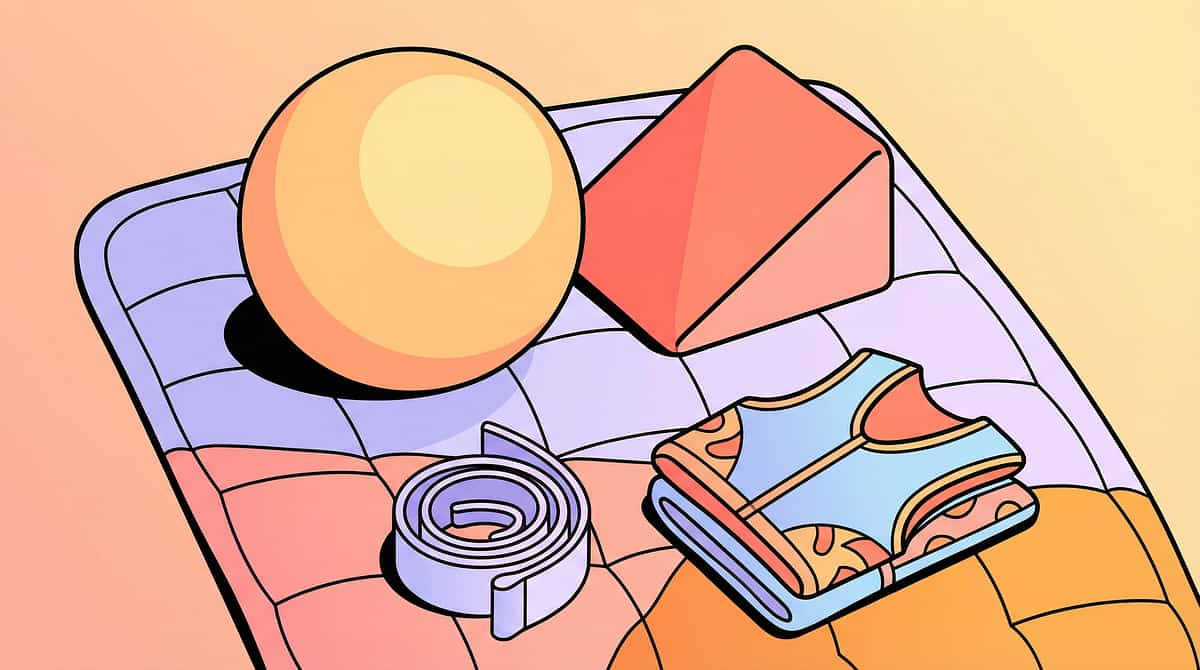
Preview of 9 materials that help with low muscle tone Therapy Material
Below is a visual preview of 9 materials that help with low muscle tone therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















