
"He grabbed the teacher's face to smell her hair. She froze. He had no idea he'd done anything wrong."
Your child reaches out and touches — hair, skin, another child's hand — with genuine curiosity, zero malice, and zero awareness of what that means to the person receiving it. You've redirected. You've explained. You've felt that hot rush of shame when a stranger goes rigid.
You are not failing as a parent. Your child's nervous system and social cognition are processing the world differently. This is teachable. This is fixable. This is what evidence-based pediatric therapy exists for.
Technique C-315
Social Communication
Body Safety
Validated by India's largest pediatric therapy consortium — SLP • OT • ABA/BCBA • SpEd • NeuroDev | FREE Helpline: 9100 181 181 (24×7, 18+ languages)

The Scale of This Challenge — You Are Among Millions
Children with autism spectrum disorder frequently experience difficulty with tactile-social integration — understanding not just the physical sensation of touch, but the complex social rules governing when, where, with whom, and how touch is appropriate. This is not wilful misbehaviour. This is a genuine processing difference rooted in neurological architecture.
80%
Touch Boundary Challenges
of children with ASD show social-touch boundary difficulties
1 in 36
CDC Prevalence (2023)
children born today will be diagnosed with autism spectrum disorder
68%
Top Parental Concern
of parents report inappropriate touching as a top-5 behavioural concern in ASD
India is home to an estimated 18+ million children with neurodevelopmental conditions. Across Pinnacle Blooms Network's 70+ centres, inappropriate touching and boundary confusion ranks among the most frequently cited parental concerns during intake — and among the most successfully addressed with structured intervention.
"You are among thousands of families in India navigating this exact challenge this week. You found this page. That is the first step."
Why Touch Rules Don't "Stick" — The Neuroscience
What neurotypical children do automatically
When a neurotypical child reaches for a stranger's hair, three systems fire in ~200 milliseconds:
- Sensory cortex registers the action
- Social cognition network cross-references: "Is this appropriate?"
- Prefrontal cortex applies the brake: "Don't touch"
What may differ in ASD
In autism, connectivity between the sensory-motor system and social cognition network can be less integrated and slower to activate. The sensory curiosity fires immediately. The social brake takes longer — sometimes not activating at all in novel situations.
This is not a moral failure. It is a neural timing difference. What doesn't develop automatically can be explicitly taught. The brain's neuroplasticity means that with consistent, structured input, the "social brake" pathway can be strengthened — through conscious, verbal, visual rule learning.
"This is a wiring difference, not a behaviour choice. And wiring can be rewired."
The Developmental Timeline — Where Your Child Is Right Now
For children with ASD, development in this domain may be delayed by 2–4 years or more, and critically — the gap between understanding rules and applying them in real-time can remain wide even when the child can verbally recite the rules. This is why explicit, multi-modal, practice-based teaching is essential.
Age 2–3
Basic body awareness begins. Children start to understand "my body" as distinct from others.
Age 4–5
"Private parts" concept emerges — areas covered by a bathing suit are private. Challenge Zone 1.
Age 6–8
Touch rules differentiate by relationship: family hug vs. stranger handshake. Challenge Zone 2.
Age 9–12
Consent basics develop — asking before touching. Challenge Zone 3.
Age 13+
Complex social norms, intimacy boundaries, and online safety emerge as ongoing focus areas.
Inappropriate touching may co-occur with sensory seeking (OT domain), impulse control challenges (ABA domain), theory of mind delays (SLP domain), and anxiety-based approach behaviours. Pinnacle's FusionModule™ addresses all simultaneously.

This Technique Is Evidence-Based. Here's the Proof.
🛡️ Evidence Grade: Level II
NCAEP EBP: Confirmed
Supported by systematic reviews and multi-site RCTs, Technique C-315 draws on the most rigorously validated approaches in ASD intervention research. Every material category in the C-315 toolkit carries independent evidence-based practice status.
Source | Finding | Relevance to C-315 | |
NCAEP EBP Report (2020) | Social narratives, video modelling, BST classified as EBP for ASD | Core techniques used in body safety teaching | |
PMC11506176 (Children, 2024) | PRISMA review: 16 studies confirm sensory-social integration efficacy | Addresses sensory-driven touching behaviour | |
PMC10955541 (World J Clin Cases, 2024) | Meta-analysis, 24 studies: promotes social skills and adaptive behaviour | Body safety is a core adaptive behaviour domain | |
Padmanabha et al. (Indian J Pediatr, 2019) | Home-based structured intervention: significant outcomes in Indian paediatric population | Directly validates home-based protocol use |
"Children with ASD who receive explicit, structured, visual-supported body safety teaching demonstrate significantly improved compliance with touch boundaries compared to verbal instruction alone."
For personalised guidance: 9100 181 181 (FREE, 24×7) | Clinically validated. Home-applicable. Parent-proven.

Technique C-315 | Teaching Appropriate Touch & Body Safety
Technique Identity
- Formal Name: Behavioural-Social Skills Training for Appropriate Touch Boundaries and Body Safety Awareness
- Parent-Friendly Alias: "The Body Safety Teaching System"
- Age Range: 4–14 years
- Session Duration: 10–15 minutes
- Frequency: Daily during learning phase; 3×/week maintenance
One-Paragraph Definition
Teaching Appropriate Touch & Body Safety is a multi-modal, explicitly-structured intervention that teaches children with autism the rules governing touch: what is appropriate, with whom, in what context, and how to ask permission. Unlike expecting social rules to be absorbed naturally, this technique makes the invisible rules of touch visible through body safety materials, visual charts, social stories, sensory alternatives, and impulse control practice — delivered by parents at home as a structured daily protocol.
Social Communication
Behavioural Regulation
Body Safety
Sensory Processing

The Consortium Behind Technique C-315
This technique crosses therapy boundaries because the brain doesn't organise by therapy type. Body safety is simultaneously a behavioural target, a communication skill, a sensory regulation challenge, and an educational objective.
ABA/BCBA — Primary Lead
Behavioural Skills Training (BST) framework: instruction → modelling → rehearsal → feedback. Designs reinforcement schedules and manages antecedent control during learning phase.
Speech-Language Pathologist — Co-Lead
Social narratives and social stories (Gray's Social Story™). Pragmatic language and teaching scripts for asking permission. Vocabulary: "private," "permission," "safe touch," "unsafe touch."
Occupational Therapist — Sensory Layer
Identifies whether touching is sensory-seeking. Provides appropriate sensory alternatives (fidget tools, textured items). Addresses tactile processing differences underlying the behaviour.
Special Education Specialist — Generalisation Layer
Ensures body safety rules transfer across settings: home → school → community. Creates visual supports and adapted materials for classroom application.
NeuroDevelopmental Paediatrician — Clinical Oversight
Rules out medication-related disinhibition. Assesses impulse control baseline. Coordinates with psychology for anxiety-driven approach behaviours.
Reach the full consortium team: 9100 181 181 (FREE, 18+ languages)
Precision Targets — What C-315 Is Actually Building
Technique C-315 is a precision tool, not a random activity. It works across three concentric layers of developmental goals — each building on the last.
Observable Behaviour: Before C-315
- Touches others without asking
- Doesn't understand "no" to touch
- Touches private areas of others
- Meltdown when touch is redirected
Observable Behaviour: After C-315
- Pauses, looks at face, asks first
- Accepts "no" gracefully
- Stops, redirects to appropriate greeting
- Tolerates correction, substitutes behaviour
Material 1 — Body Safety Education Books & Materials
Canon Category: Social Stories / Visual Narratives
DIY Available
Body safety education books introduce the concept of private versus public body parts in a matter-of-fact, age-appropriate, and completely non-shaming way. They normalise the conversation for both child and parent, providing a shared language and a visual reference point that children with ASD can return to again and again.
DIY Version (₹0)
Draw 5 stick figures in bathing suits. Label covered areas "private." Read together daily. Simple, effective, and completely free.
Why it works: Understanding private vs. public is foundational to all subsequent body safety learning. Without this concept, no other rule in C-315 can be properly anchored.

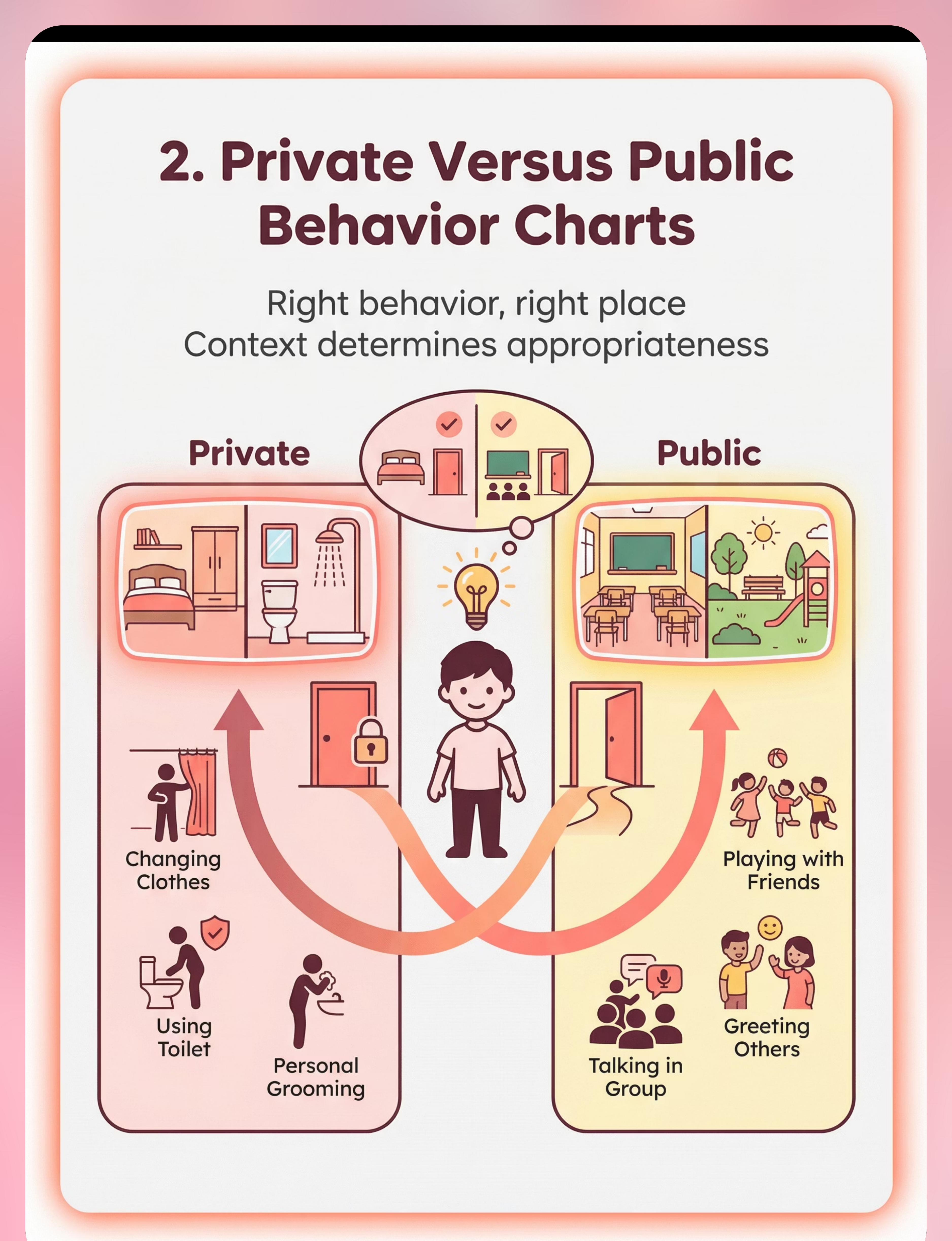
Material 2 — Private vs. Public Behaviour Charts
Canon Category: Visual Behaviour Charts
DIY Available
Private/public behaviour charts teach children that context determines appropriateness — the same behaviour that is perfectly fine at home may be completely inappropriate in a shop, classroom, or park. This spatial and contextual rule is one of the most powerful concepts in body safety teaching.
DIY Version (₹0)
Fold A4 paper in half. Left side: 🏠 "Private" (bedroom, bathroom). Right side: 🌍 "Public." Cut magazine pictures, sort and paste together with your child.
Display tip: Post the chart at the child's eye level near the front door — a visual reminder every time they leave the house.

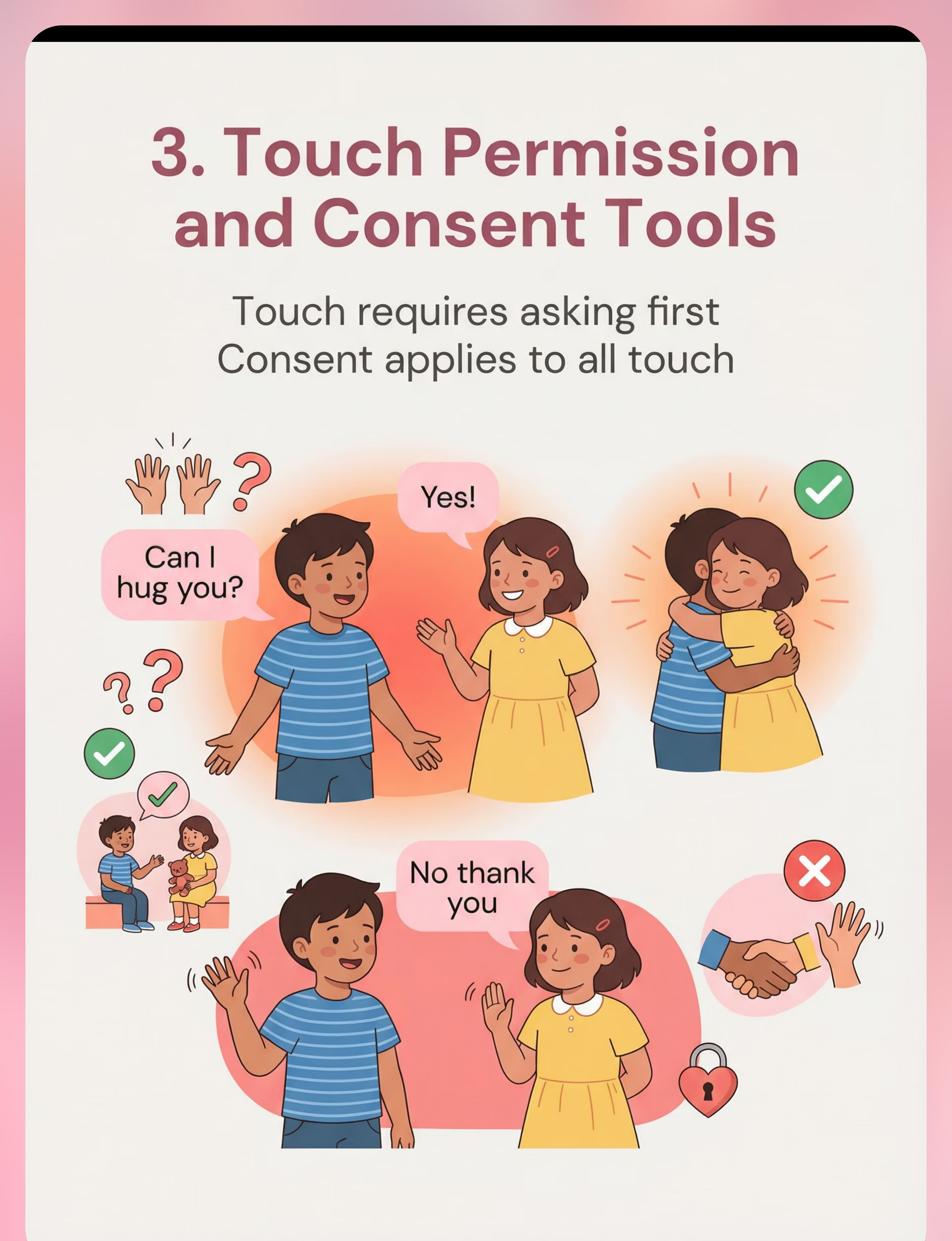
Material 3 — Touch Permission & Consent Tools
Canon Category: Social Stories / Permission Teaching
DIY Available
Consent tools make the abstract concept of asking permission concrete and visual. They teach children that touch requires an active, verbal request — and that waiting for an answer is part of the social script, not an optional step. This is among the most directly protective skills the C-315 protocol develops.
DIY Version (₹0)
Two index cards: ✅ "Yes I can touch" (happy face) and ❌ "No, I need to ask" (waiting face). Role-play with these cards daily until the permission sequence is automatic.
Key script: "When I want to touch someone, I ask: 'Can I hug you?' I wait for YES or NO. I respect their answer."
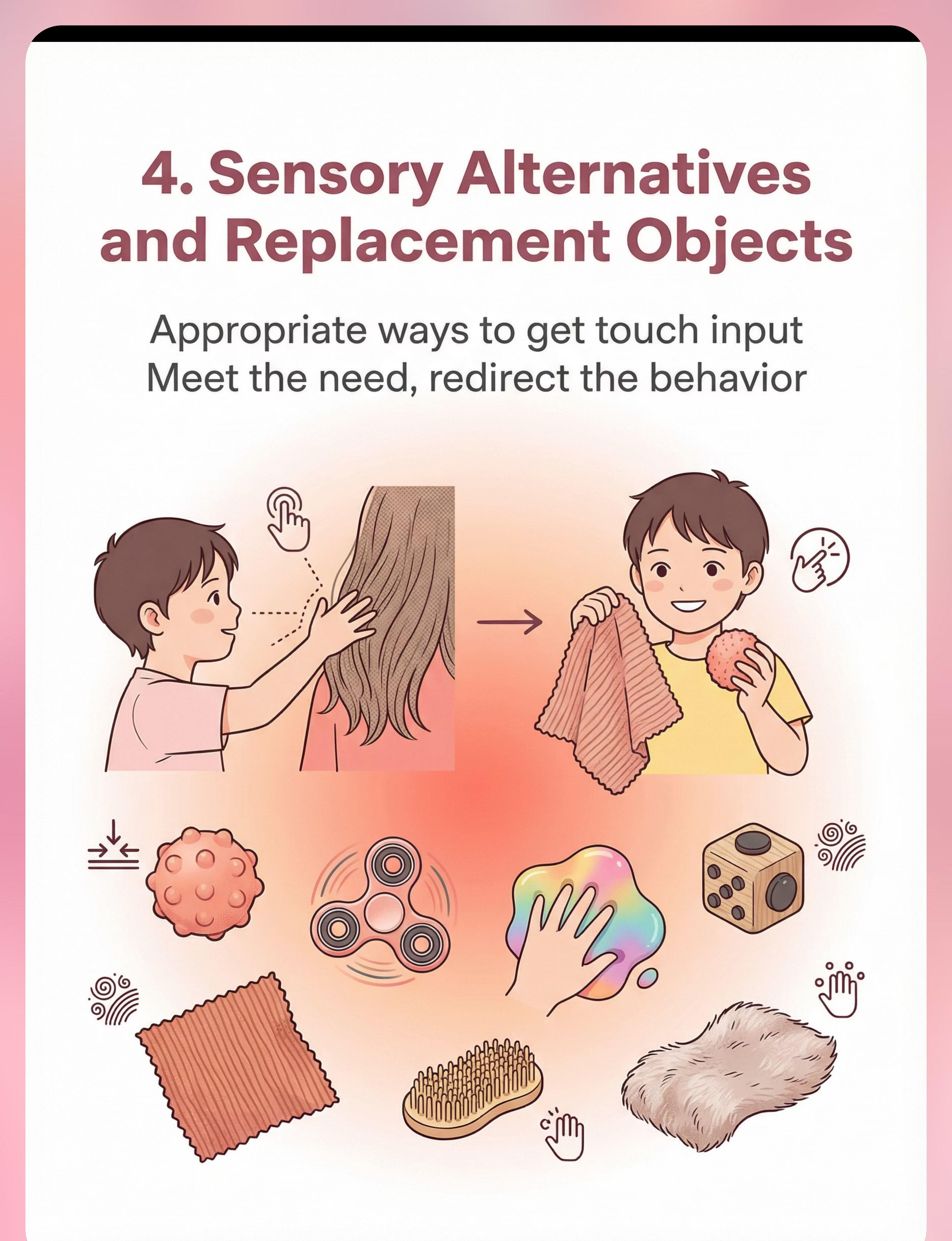
Material 4 — Sensory Alternatives & Replacement Objects
Canon Category: Sensory Tools / Tactile Alternatives
DIY Available
Many children with ASD touch others primarily to meet a sensory need — the texture of hair, the warmth of skin, the pressure of a hand. Sensory alternatives address the root need while removing the socially problematic behaviour. The OT principle is simple: meet the need, then teach the rule.
DIY Version (₹0)
Fill a small cloth bag with rice — a squeeze toy. Roll a clean pencil between palms. Carry a small smooth stone for tactile input. Offer these before entering sensory-triggering environments.
⚠️ Check for choking hazard if child mouths objects (under age 6 or significant oral sensory seeking). Choose objects size-appropriate to your child.

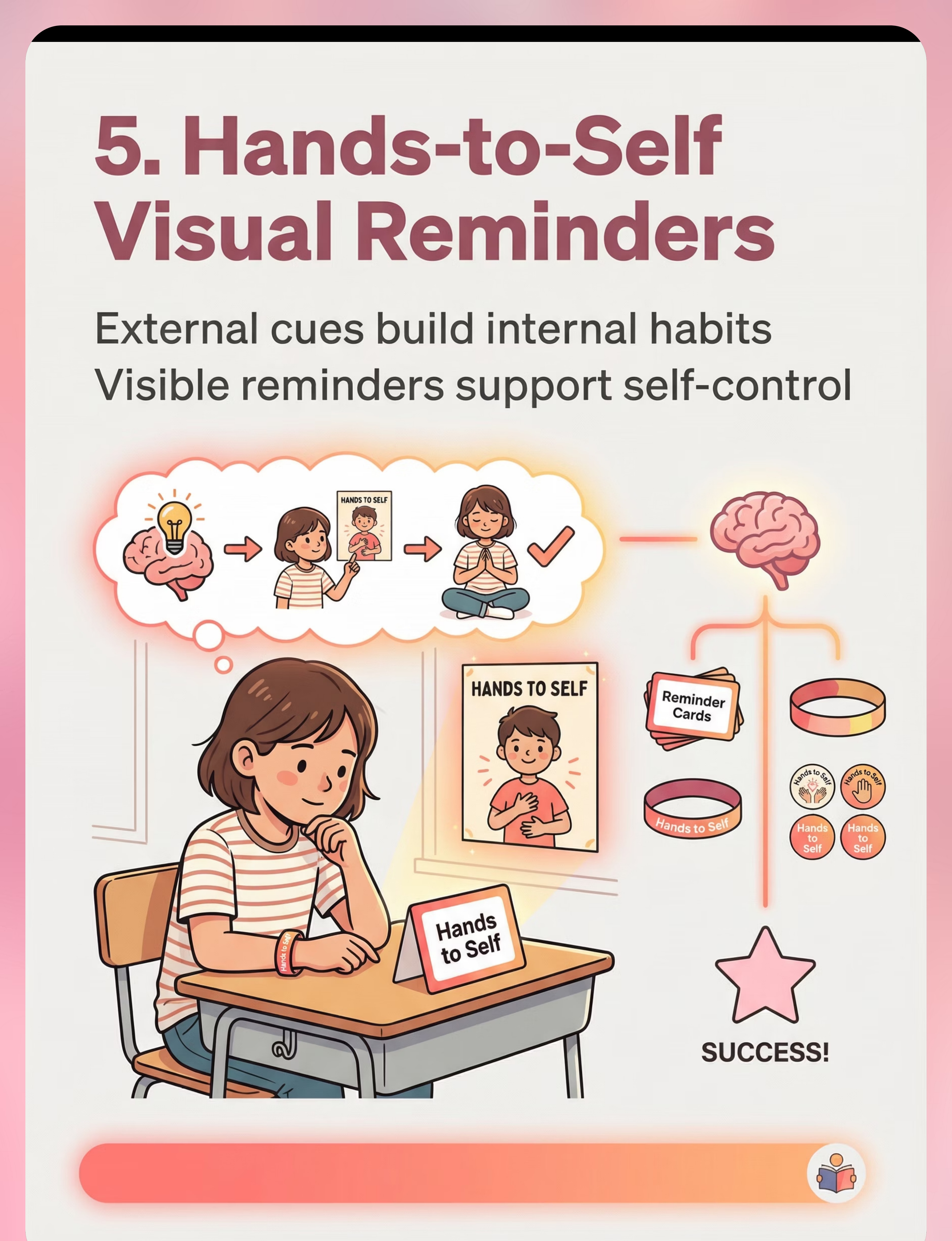
Material 5 — Hands-to-Self Visual Reminders
Canon Category: Visual Supports / Reminder Cues
DIY Available
External visual cues build internal habits. For children with ASD who struggle with real-time impulse inhibition, visible reminders in the environment serve as an external prefrontal cortex — providing the social brake that the neural pathway hasn't yet automated. These reminders are temporary scaffolding, not permanent tools.
DIY Version (₹0)
Write "HANDS TO SELF" on a rubber band. Child wears it on their wrist. Refresh the instruction every morning as a brief ritual. Post a matching sign at home, school bag, and classroom desk.
Fade out visual reminders gradually as the behaviour becomes self-directed — typically after Weeks 6–8 of consistent practice.

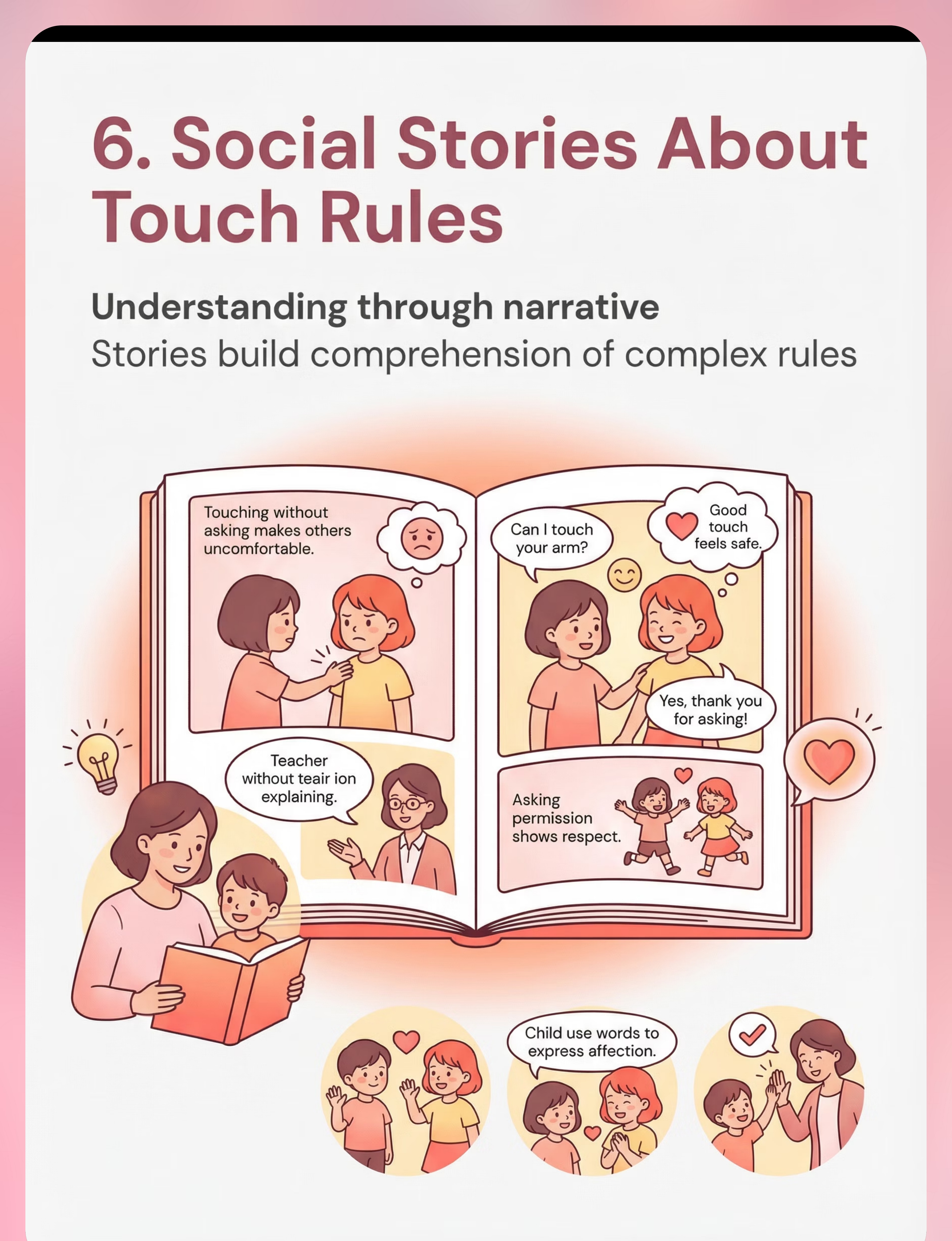
Material 6 — Social Stories About Touch Rules
Canon Category: Social Stories / Touch Rule Narratives
DIY Available
Social stories (Gray's Social Story™ framework) help children with ASD understand complex rules through narrative structure — a format their brains engage with more readily than direct instruction. Stories provide context, perspective-taking prompts, and a predictable script for what to do in specific situations.
DIY Version (₹0)
Write 5 sentences: "When I want to hug someone, I ask first. I say 'Can I hug you?' I wait for them to say yes. If they say no, I wave or high-five instead. Asking first shows I care." Illustrate with photos of your child.
Personalisation tip: Stories featuring the child's own name and photos are significantly more effective than generic printed stories. Your DIY version may outperform the purchased one.

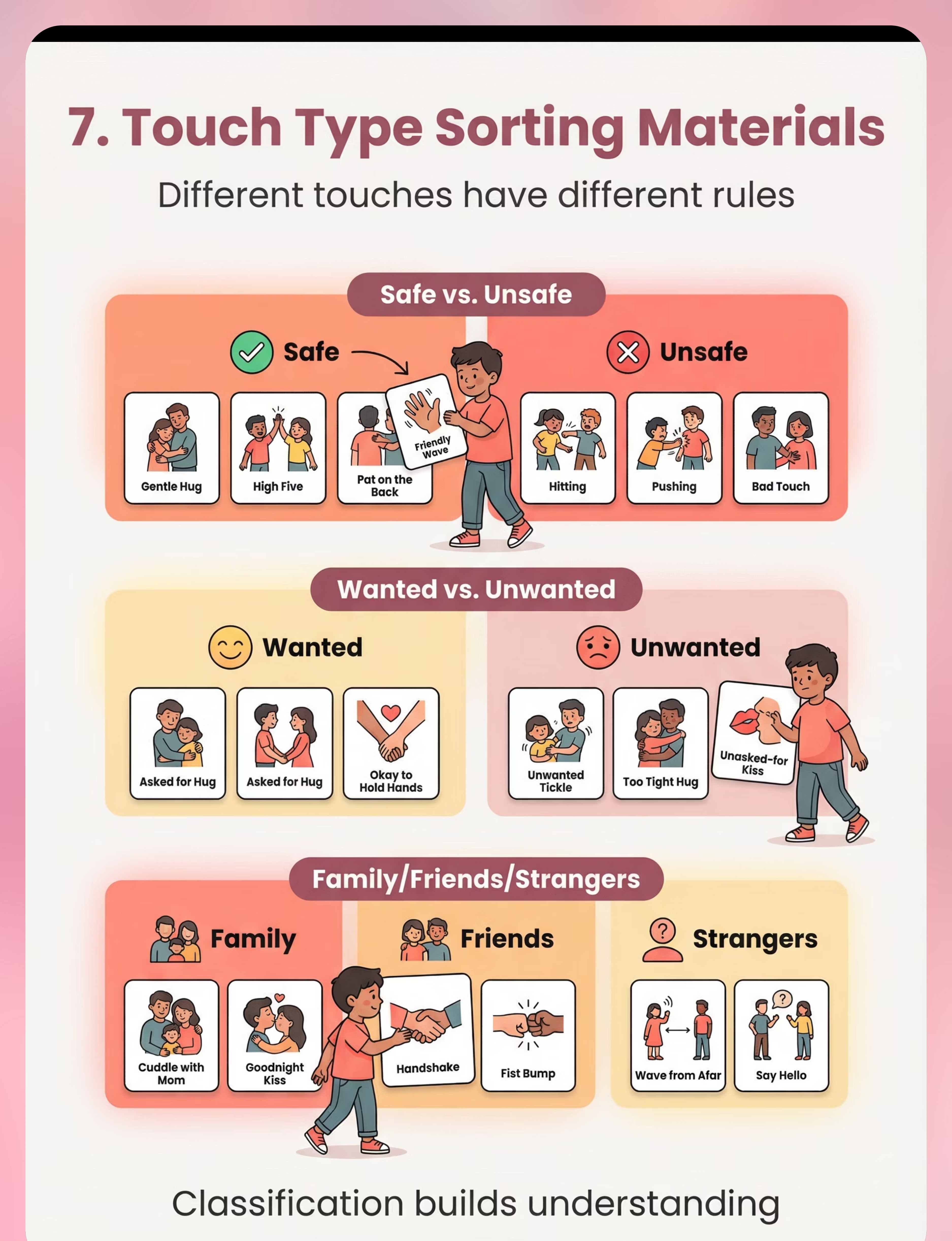
Material 7 — Touch Type Sorting Cards
Canon Category: Sorting Activities / Social Classification
DIY Available
Touch sorting cards teach the critical classification skill: not all touches are the same, and not all rules apply equally to all situations. Sorting activities are particularly effective for ASD learners because they provide a structured, concrete, hands-on task that naturally builds the categorical thinking underlying social rule application.
DIY Version (₹0)
12 index cards: draw or describe different touches. Sort into ✅ Safe (handshake, asked-for hug, high-five) and ❌ Unsafe (touching private parts, touching without asking, grabbing). Add cards as skills build.
Begin with obvious examples (high-five = safe; touching private parts = unsafe). Gradually introduce nuanced scenarios (hair touching, face patting) as skills consolidate.

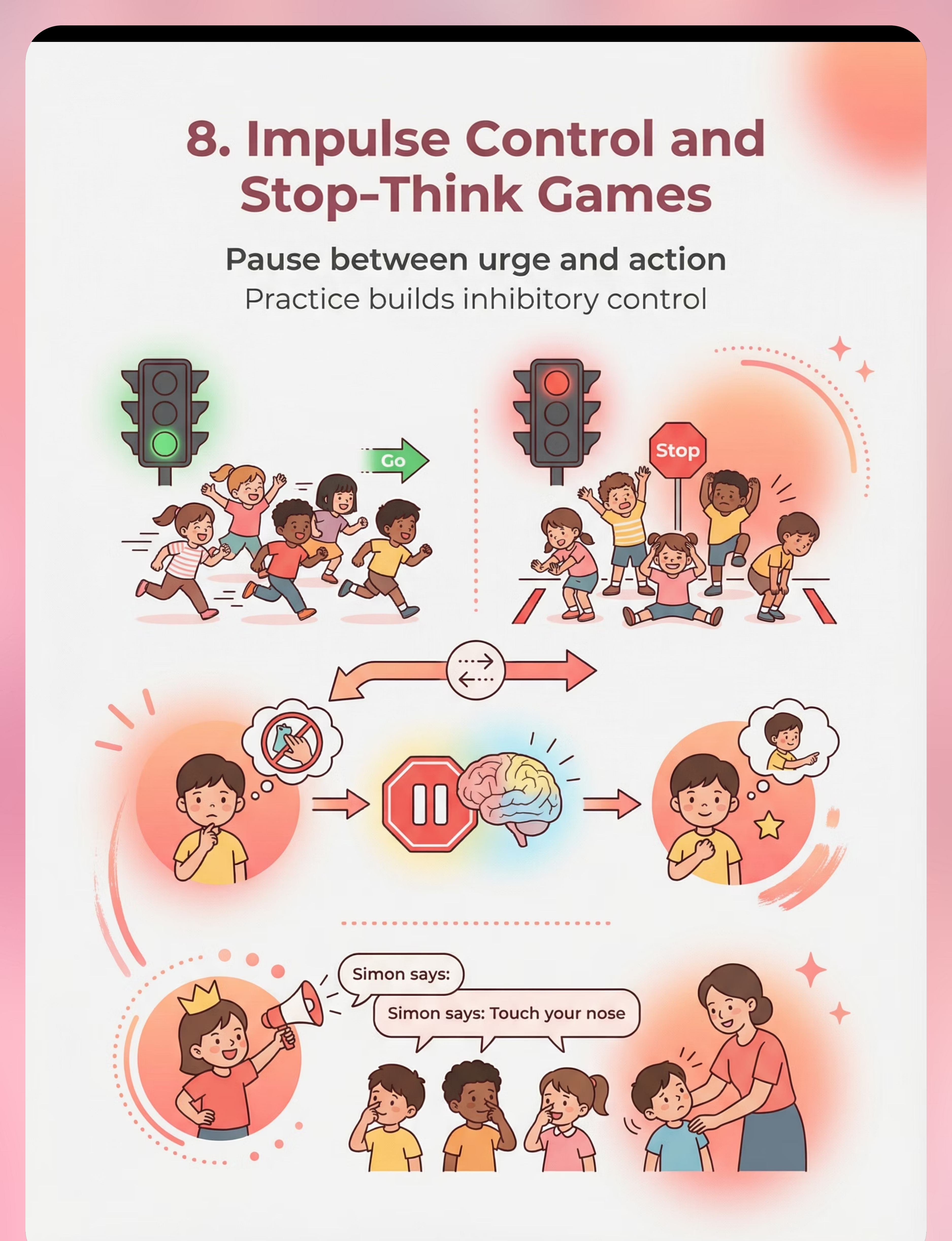
Material 8 — Impulse Control & Stop-Think Games
Canon Category: Impulse Control Games / Stop-Think Activities
DIY Available
Impulse control games build the pause-before-action neural pathway through repeated, enjoyable practice. For children whose touching behaviour is impulsive rather than sensory-driven, this is the most critical material category. Inhibitory control is a trainable skill — and games are the most effective training vehicle for young children.
DIY Version (₹0)
Play "Freeze" — put on music, freeze when it stops. Play "Simon Says" — only touch when Simon says. Both are free, immediately effective, and build exactly the neural pause needed for real-life touch inhibition.
Key insight: The child who can freeze in a game is building the same inhibitory mechanism they need to pause before reaching for a classmate's hair. Play IS therapy.
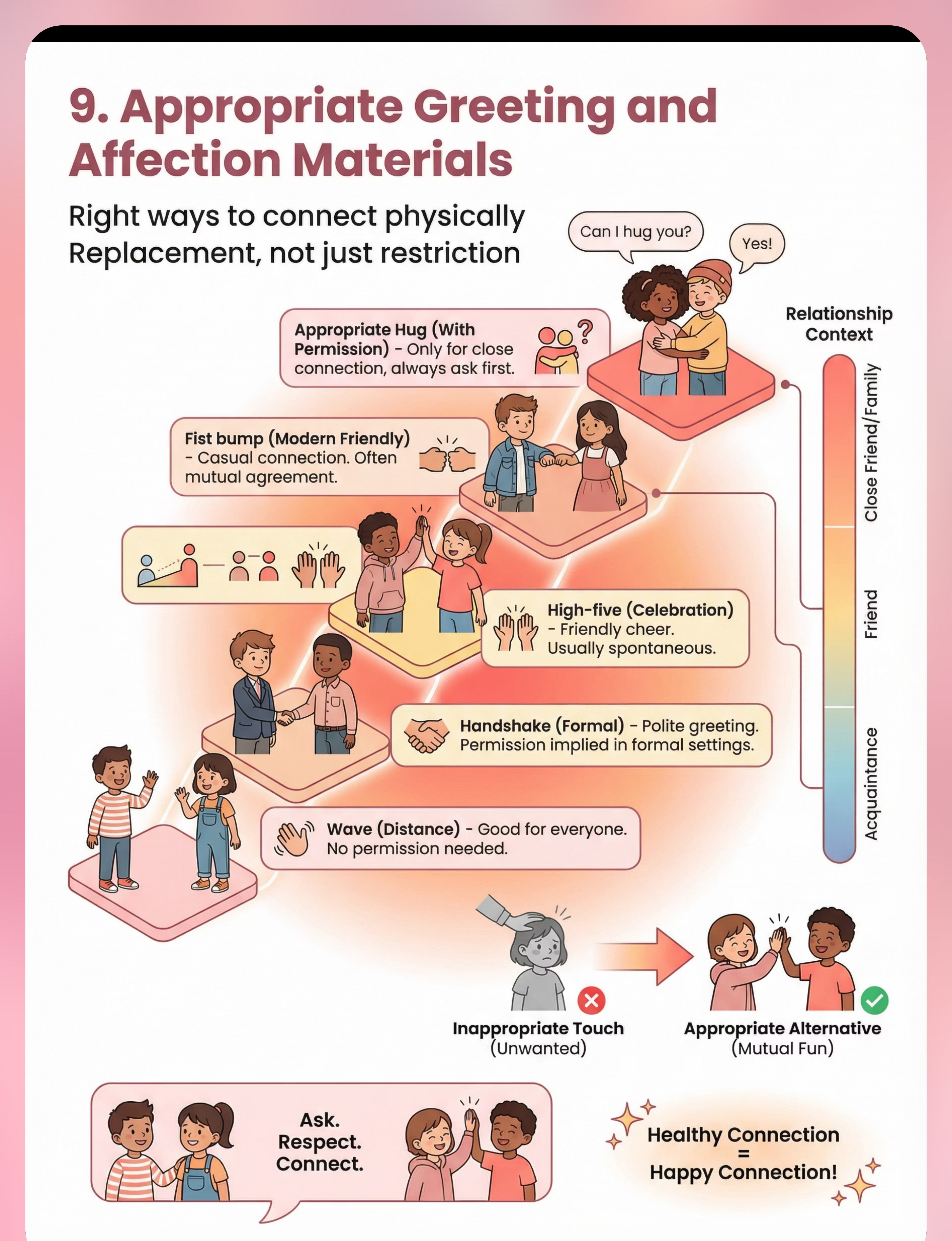
Material 9 — Appropriate Greeting & Affection Materials
Canon Category: Social Skills / Greeting Alternatives
DIY Available
The most sustainable body safety intervention is one that provides replacement behaviours, not just restrictions. The greeting ladder teaches children the full spectrum of appropriate physical connection — from wave to handshake to high-five to hug — matched to the relationship and context. This is the difference between teaching "don't touch" and teaching "here's how to connect."
DIY Version (₹0)
Draw the greeting ladder: Wave (anyone) → Handshake (acquaintance) → Fist bump (friend) → Side hug (close friend) → Full hug (family/with permission). Post on the fridge. Review before every social outing.
Total investment: ₹1,500–4,000 for all 9 materials commercially. Essential starters: Body Safety Books | Visual Charts | Sensory Alternatives

₹0 Versions — Every Material Has a Household Alternative
The WHO/UNICEF equity principle is clear: no family should be excluded from evidence-based intervention due to economic constraint. The brain learns the same rules whether the materials cost ₹500 or ₹0. Consistency of practice matters infinitely more than material quality.
When Commercial Materials ARE Needed
When sensory seeking is severe. When home-made materials are consistently destroyed. When professional-grade visual clarity is required for a specific child's processing profile.
The Zero-Cost Principle
Rice-filled cloth bag = sensory toy. A rubber band on the wrist = reminder cue. 5 sentences written by hand = social story. Index cards = sorting activity. Freeze game = impulse control training.
Starting Today
You can begin C-315 right now with a piece of paper, a pencil, and 10 minutes. The willingness to show up consistently is the only non-substitutable ingredient.
When clinical-grade material is needed, consult Pinnacle: 9100 181 181 — our team can advise on prioritisation for your child's specific sensory profile.

🛑 Read This Before You Begin Every Session
🟢 GREEN — Full Protocol
- Child is calm and regulated (not post-meltdown, not hungry)
- Parent is calm and emotionally available
- Session materials prepared and child-safe
- No distressing event in past 2 hours
- Child is rested
🟡 AMBER — Modified Protocol
- Child slightly elevated → shorter session (5 min)
- Parent has limited time → 1 material only
- Child recently redirected → extra patience, no shame framing
🔴 RED — Do Not Proceed
- Child in active meltdown or within 60 min post-meltdown
- Parent significantly dysregulated
- Child ill, in pain, or very hungry
- Recent traumatic event
🔴RED LINE: If child discloses any inappropriate touching they have received, STOP the session, reassure calmly, and call 9100 181 181 immediately. Never question the child yourself.
⚠️Language tone is critical: Body safety teaching must NEVER be shame-based. Use correct anatomical terms (WHO recommended). Age-calibrate all materials — a 4-year-old's teaching looks entirely different from a 12-year-old's.

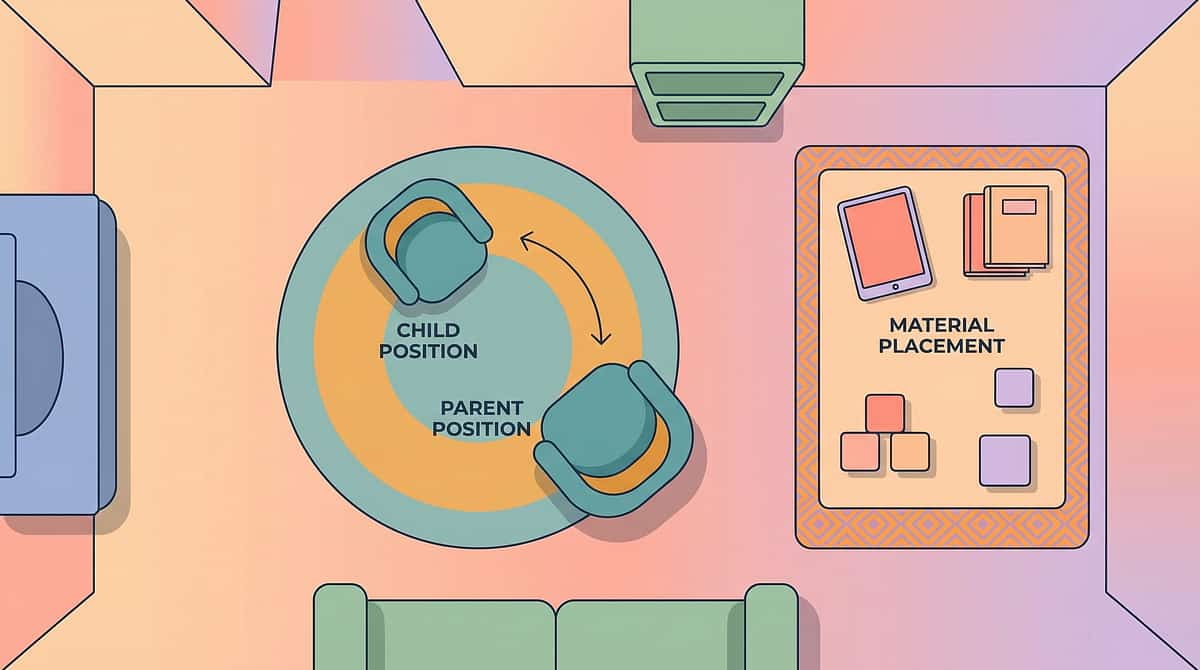
Your C-315 Session Space — Set Up in 3 Minutes
A calm, predictable environment is itself a therapeutic intervention. The setup is not housekeeping — it's clinical. Research confirms that 1:1 individual treatment sessions within structured environments produce the strongest outcomes.
Setup Checklist
- Visual chart at child's eye level on the wall
- Session materials in a basket/tray (not scattered)
- Parent seated beside child, not across (collaborative, not confrontational)
- TV off | Siblings out | Phone on silent
- Visual timer visible (hourglass or phone timer)
- "Well done" tokens/stickers ready
- Door closed for privacy and focus
Sensory Environment Notes
Lighting: Natural light preferred. Avoid harsh overhead fluorescents — sensory comfort aids regulation and learning readiness.
Sound: Quiet. Some children benefit from very soft background music at low volume. Never use TV or loud media.
Temperature: Comfortable. Child in comfortable, non-restrictive clothing. Tactile comfort supports emotional regulation throughout the session.
Position: Beside the child, at their level — never looming above. Collaborative posture signals safety, not authority.
60-Second Pre-Session Check — Go / Modify / Postpone?
Before every session, run this brief readiness assessment. "The best session is one that starts right. A 3-minute successful session beats a 15-minute battle."
Indicator | ✅ Go | ⚡ Modify | 🔴 Postpone | |
Hunger | Fed within 2 hrs | Slightly hungry → snack first | Very hungry → feed, wait 20 min | |
Sleep | Well-rested | Tired → shorten to 5 min | Very tired → skip today | |
Emotional state | Calm, neutral, curious | Elevated → start with sensory toy | Crying, agitated → not today | |
Recent incident | None | Minor redirect → acknowledge first | Meltdown within 60 min → not today | |
Interest level | Engaged or neutral | Resistant → offer choice of 2 activities | Refuses all engagement → try evening |
5–6 ✅ = GO
Full protocol
3–4 ✅ = MODIFY
Shorter, easier version
0–2 ✅ = POSTPONE
Try again in 2–4 hours
Step 1 — Open the Session (30–60 Seconds)
Step 1 of 6
Invitation Phase
💬 "Hey [child's name], let's do our special learning time! Today we're going to look at our body safety cards. Want to pick where we sit — here or here?"
Giving a choice of seating (not whether to do the activity) activates autonomy while maintaining the session structure. This small moment of control significantly reduces resistance.
Body Language Guidance
- Kneel or sit at child's level — never loom over
- Open body posture (no crossed arms)
- Soft, warm tone — not excited or urgent
- Follow their attention briefly before redirecting to materials
If Child Resists
- Runs away: "I'll have the cards here when you're ready"
- Says "no": "That's okay. I'm just going to look at them for a minute"
- Ignores: Start interacting with materials yourself — curiosity often follows
Timing: 30–60 seconds only. Don't extend the invitation phase unnecessarily — the session begins when they engage, not when they say yes enthusiastically.

Step 2 — Introduce the Body Safety Materials (1–3 Minutes)
Step 2 of 6
Engagement Phase
For Younger Children (4–7): Opening Script
Start with Body Safety Education Book or Private/Public Chart.
💬 "Look at this — see this picture? These are the parts of our body that are private. Private means they belong to YOU. No one can touch your private parts except your doctor when Mummy/Daddy is there, or when you need help to wash. That's the rule."
Point to the visual chart as you speak. Let the child touch the chart and point to pictures.
For Older Children (8–14): Opening Script
Start with Touch Type Sorting Cards or Private/Public Behaviour Charts.
💬 "Today we're going to sort these cards — some touches are okay, some are not. Let's figure them out together. You're the expert on your own body."
Engagement Indicators
- Engagement: Looking at, touching, or asking about materials
- Tolerance: Passively present — still counts
- Avoidance: Pushing materials away — modify approach
Reinforcement cue: The moment the child looks at or touches the material: "Good looking! Good noticing!" — reinforce approach behaviour immediately.

Step 3 — The Core Teaching Sequence (5–10 Minutes)
Step 3 of 6
Therapeutic Action — Main Event
This five-step sequence is the active ingredient of C-315. Quality matters more than quantity — a focused 5-minute sequence consistently applied outperforms a distracted 20-minute session.
Common Error | Correction | |
Shaming language ("That's wrong/bad") | Rephrase: "That's the learning part — here's the rule" | |
Teaching too many rules at once | One rule per session until mastered | |
No follow-through in real life | Real-life redirects must use exact session language | |
Child refuses role-play | Use puppets/stuffed animals instead of direct role-play |
Step 4 — Repetition That Sticks (3–5 Minutes)
Step 4 of 6
Repetition Phase
Target: 3–5 practice repetitions per rule per session. Three genuine, attended repetitions build a stronger neural pathway than 10 repeated with a child who has checked out. Read your child, not the clock.
Card Rotation
Each session, introduce 1 new touch type sorting card alongside 2 already mastered.
Story Variation
Read a different social story panel; ask prediction questions: "What does the child do next?"
Role-Play Rotation
Parent → child → stuffed animal → peer sibling (with supervision). Variety maintains engagement.
Game Version
Simon Says: touch your nose → DON'T touch my nose. Builds inhibitory control through play.
Stop repetition when: child begins scripting heavily, responses become rote/mechanical, child becomes irritable, or 3 strong engaged repetitions are complete. Satiation produces no learning.

Step 5 — Reinforcement That Works (Within 3 Seconds)
Step 5 of 6
Reinforcement Phase
The reinforcement window: deliver within 3 seconds of desired behaviour. Not 30 seconds. Not "good job, and later I'll give you...". Immediate → specific → enthusiastic.
💬 Script 1
"YES! You asked first! That is EXACTLY the rule! I'm so proud of you!"
💬 Script 2
"You stopped yourself and asked — that took real bravery! High-five!"
💬 Script 3
"You remembered the body safety rule all by yourself!"
Tier | Type | Example | |
Immediate (always) | Verbal praise | "YES! That's exactly right!" | |
Session-level | Token/sticker | Add star to behaviour chart | |
Daily | Small tangible | Extra 5 min preferred activity | |
Weekly | Bigger reward | Child chooses weekend activity |
Celebrate the attempt, not just the success: "You tried to remember the rule — that counts! Tomorrow we practise again." Token economy: 5 tokens = agreed reward. Start easy, increase difficulty as skills build.

Step 6 — Close the Session with a Ritual (1–2 Minutes)
Step 6 of 6
Cool-Down Phase
No session ends abruptly. A structured close prevents post-session dysregulation and teaches the child that ending is safe and predictable — not a loss.
1
Advance Warning (30 sec before end)
💬 "Two more cards, then we're all done for today!" Use a visual timer — watch it count down together.
2
The Put-Away Ritual
Child helps put materials back in the basket. Participation in closure = ownership. 💬 "Let's put the cards to sleep. They'll be ready for us tomorrow."
3
The Summary Sentence
💬 "Today we practised: ask before touching. You remembered! See you tomorrow for more."
4
Transition Cue + Final Reinforcement
Point to the next activity. Deliver one last piece of praise or token, warmly. The session ending is not a punishment.
If child resists ending: "All done — we can do more tomorrow" said once, calmly, then transition. A 2-minute sand hourglass at the start of cool-down lets the timer end the session, not the parent — reducing resistance significantly.
60-Second Data Capture — Do This Before You Forget
Within 60 seconds of session end, record 3 data points. 60 seconds of data now saves hours of guessing later. Your data drives your child's personalised plan.
📋 C-315 Session Log
Rule Practised Today:
- □ Asking permission
- □ Private parts
- □ Safe/unsafe touch
- □ Touch type sorting
- □ Appropriate greeting
Child Compliance Rating:
- □ Full (did it independently)
- □ Prompted (needed 1–2 reminders)
- □ Partial (attempted but struggled)
- □ Refused (session modified)
Real-Life Touch Behaviour Log
When the behaviour occurs outside sessions, note:
- Where it happened (home/school/public)
- Who was targeted
- Whether child self-corrected or needed redirect
This real-world data is the most important data of all — it shows whether in-session learning is generalising to natural environments.
Log directly in the Pinnacle app: pinnacleblooms.org or call 9100 181 181
It Didn't Go Perfectly. Here's What to Do.
Most sessions don't go perfectly. Session abandonment is not failure — it's data. It tells you what to adjust. Below are the seven most common session problems and their evidence-based solutions.
Child refused to engage with materials at all
Why: Session timing, hunger, recent overstimulation, or materials not yet motivating. Next time: Offer materials choice, start with sensory toy, try different time of day.
Child recited rules verbally but still touched inappropriately
Why: Knowing a rule ≠ applying it in real-time. This is normal. Next time: Increase in-the-moment redirects. Reduce time between session teaching and real-life practice.
Child became distressed when body safety was mentioned
Why: Previous shame responses OR a possible disclosure signal. Next time: Use completely neutral language. If distress is unusual, consult Pinnacle: 9100 181 181
Child asks permission compulsively/anxiously for every touch
Why: Overcorrection — rule learned too rigidly. Next time: Introduce nuance: "With Mummy/Daddy — hugs without asking. With friends and strangers — always ask first."
Parent lost patience and raised voice during session
Why: This is human. Body safety topics can feel urgent and stressful. Next time: End session, re-regulate yourself first, resume tomorrow. A calm parent is the most powerful therapeutic tool.

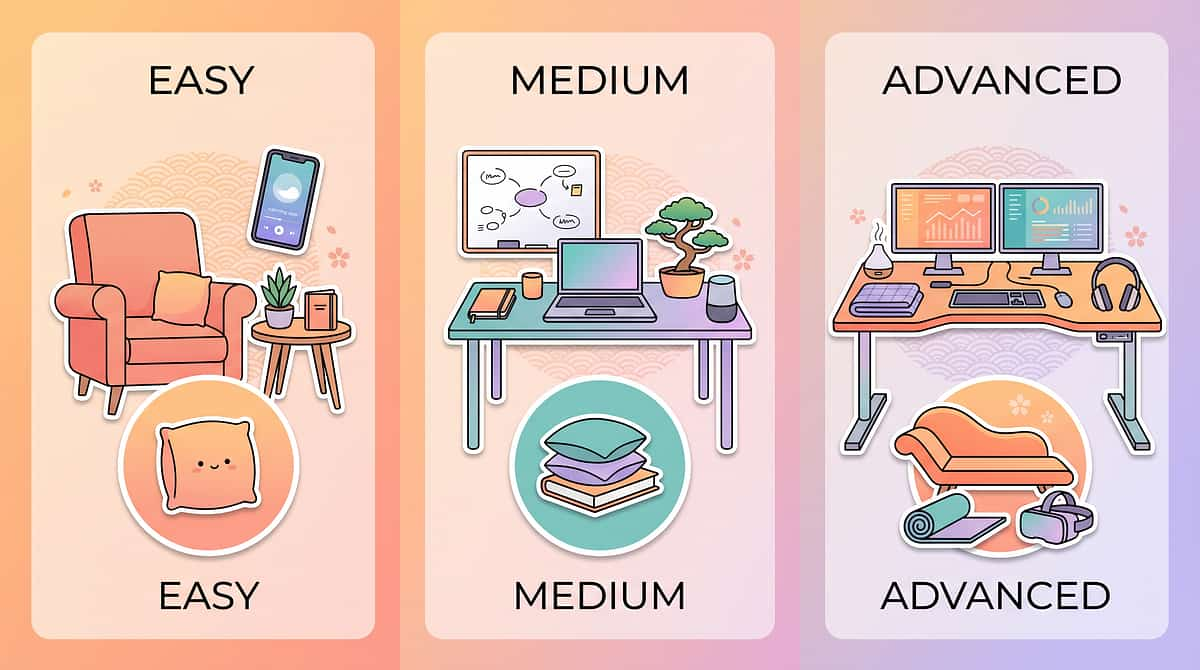
Calibrate C-315 to YOUR Child
No two children are identical. Use this difficulty progression to match the protocol exactly to your child's current developmental level, sensory profile, and communication capacity.
1
Level 1 — Intro
One rule only: "Private parts are private." Picture books only, no role-play. 5-min sessions. Parent leads; child points.
2
Level 2 — Building
Two rules + sorting cards. Simple puppet role-play begins. 10-min sessions. Child completes sentences.
3
Level 3 — Consolidating
All 9 material types over 3-week rotation. Direct role-play with parent. 15-min sessions. Child states rule independently.
4
Level 4 — Mastery
Real-life coaching in community settings. Child explains rules to a younger sibling. Weekly maintenance sessions. Self-monitoring and self-correction.
Sensory Profile | Adaptation | |
Sensory seeker (touches for tactile input) | Provide rich tactile alternatives before teaching sequence. Meet the need, then teach the rule. | |
Impulsive (acts before thinking) | Emphasise Stop-Think games heavily. Insert pause training before rule teaching. | |
Anxious (people-pleasing) | Teach that saying NO to unwanted touch is okay. Balance with safe greeting options. | |
Low verbal | Visual-only protocol: charts, sorting cards, picture pointing. No scripted verbal responses required. |
Weeks 1–2 — The Foundation Phase
Progress: 15%
Foundation Phase
✅ What You WILL See
- Child can point to private parts on the chart when asked
- Child can recite 1–2 rules when prompted
- Child is tolerating session materials without avoidance
- Child is beginning to recognise the session routine ("body safety time")
❌ What You Will NOT See Yet (And That's Okay)
- Spontaneous rule application in real life (this is Weeks 4–6)
- Asking permission before touching (this is Weeks 3–5)
- Stopping behaviour independently without a parent redirect
Weeks 1–2 are about foundations, not outcomes. You are laying the neural groundwork. The behaviour in real life may not change yet — and that is completely normal. The research says it takes 6–8 weeks minimum for behavioural generalisation. If your child tolerates the chart for 30 seconds longer than Week 1 Day 1 — that is measurable, real progress.
Frequency target: 4–5 sessions in Weeks 1–2. Daily where possible. Never force two consecutive days if child is resistant.

Weeks 3–4 — Neural Pathways Are Forming
Progress: 40%
Consolidation Phase
The consolidation phase contains the behavioural changes most parents miss — small, easy to overlook, but they are the real indicators of neural pathway formation.
Anticipates the Session
"Are we doing body safety time today?" — the routine is internalised.
Begins to Pause
A slightly longer pause before reaching for something or someone. The social brake is activating.
Checks Before Touching
Child glances at parent before touching — the permission-seeking reflex is emerging.
First Self-Correction
"Oh — I should ask first." Celebrate this moment enormously. It is the technique working.
This week: increase practice complexity with realistic scenarios, introduce the topic before social situations arise ("We're going to Grandma's — what's the touching rule?"), and consider moving from Level 1 to Level 2 on the difficulty slider.
Weeks 5–8 — Mastery Is Unlocking
Progress: 75%
Mastery Phase
Your child has mastered C-315 when they demonstrate ALL of the following criteria consistently and independently:
🏆 Mastery Badge Criteria
- Consistently asks permission before non-family touch in familiar settings (>80% of opportunities)
- Correctly identifies private vs. public body parts without chart
- Sorts all 9 touch type cards independently and accurately
- Stops behaviour within 1–2 seconds when verbal reminder given
- States body safety rule spontaneously in ≥2 novel situations
- Accepts "no" to a touch request without distress
🌍 Generalisation Indicators
- Skill appearing at school (teacher feedback confirms)
- Skill appearing with unfamiliar adults in the community
- Child teaches the rule to a sibling or younger child — the deepest generalisation marker
Maintenance Check
Run one session per week without the structured sequence — just review the chart together. Does the behaviour maintain? Yes = mastery. No = needs more consolidation weeks.
"When your child pauses, looks at another child, and asks 'Can I touch my toy?' — completely unprompted, in the middle of play — that is the technique working. That moment is the 5 weeks of daily practice paying off."

🎉 You Did This. Your Child Grew Because of You.
Five to eight weeks ago, you started this page scared and exhausted. You showed up — sometimes imperfectly, sometimes for just 5 minutes, sometimes with a shaky voice because this topic is hard. You showed up.
Your child now has something they didn't have before: an explicitly learned map of a social world that doesn't come naturally to them. They know what "private" means. They're beginning to understand that touch requires permission. They're learning that their body has rules — and so does everyone else's.
🎂 Make a Certificate
Create a "Body Safety Certificate" together — child's name, the date, "I know my body safety rules!" A tangible marker of real achievement.
📸 Capture the Moment
Take a photo with the visual chart they've been working with. Write down: "On [date], [child's name] first spontaneously asked permission before touching."
🎁 Choose a Reward
Child chooses a small reward from the reinforcement menu. This milestone deserves celebrating with the same intentionality as any other major developmental achievement.
Share your story with our team: 9100 181 181 | care@pinnacleblooms.org

🔴 These Signs Mean: Pause and Consult Now
This card contains critical safety information. Read fully before continuing the programme.
🔴 Child Discloses Inappropriate Touch by Another Person
Action: STOP all sessions immediately. Reassure calmly. Do NOT question the child. Consult a professional same day. Call 9100 181 181 immediately.
🔴 No Behavioural Change After 8+ Weeks of Consistent Daily Sessions
Action: Schedule an AbilityScore® assessment to recalibrate. The intervention may need professional optimisation. Call 9100 181 181.
🔴 Behaviour Has Escalated in Frequency, Intensity, or New Targets
Action: Do not continue solo. A Functional Behaviour Assessment (FBA) is needed. The behaviour function may differ from what was assumed.
🔴 Child Becomes Extremely Distressed or Dissociates During Teaching
Action: STOP immediately. Consult a clinical psychologist. This level of distress requires professional support. Call 9100 181 181.
🔴 Parent Cannot Remain Calm/Shame-Free Consistently
Action: Request a parent coaching session via Pinnacle before continuing solo. This is not failure — it is wisdom. Call 9100 181 181.

What Comes Next — Your C-315 Progression Map
C-315 is one carefully positioned step in a larger developmental journey. Understanding where you are — and where you're heading — makes every session feel purposeful rather than isolated.
If C-315 Is Mastered
- → C-316: Understanding Consent and Personal Boundaries (deepens the consent framework)
- → C-313: Reading Social Cues (complements with nonverbal awareness)
- → D-Domain: Behavioural Flexibility Techniques
If C-315 Is Partially Mastered
- → C-315-DD-01: How to Use Body Safety Books Systematically
- → Return to C-314: Personal Space Awareness (prerequisite foundation)
This technique feeds into: peer social safety, abuse prevention literacy, and ultimately — independent adult social navigation. This is not just therapy. It is foundational life protection.
Related Techniques — Continue the Journey
If you have Body Safety materials from C-315, you already have the foundation for C-316 and C-314 — no new purchases required. Your existing materials stretch further than you think.
Code | Technique | Difficulty | Material Match | |
C-312 | Child Prefers Adults Over Peers | 🟡 Core | Social Stories | |
C-313 | Reading Social Cues | 🟡 Core | Expression Cards | |
C-315 | Appropriate Touch & Body Safety — YOU ARE HERE | 🟡Core | Body Safety Materials | |
C-314 | Understanding Personal Space | 🟢 Intro | Space Maps | |
C-316 | Consent & Personal Boundaries | 🔴 Advanced | Consent Tools | |
C-317 | Emotion Recognition in Social Context | 🟡 Core | Emotion Cards |
One Technique. One Domain. One Piece of a Bigger Picture.
C-315 addresses one critical node in the Social Communication domain. Your child may also benefit from techniques addressing sensory processing, emotional regulation, and behavioural flexibility — all of which interact directly with body safety behaviour.
GPT-OS® AbilityScore® System
Tracks your child across all 12 domains simultaneously, generating personalised intervention sequencing so you're always working on the highest-impact technique for your child's current developmental stage.
"This technique is one piece of a larger plan — and every piece matters."
See the Bigger Picture
C-315 directly connects to:
- Sensory Processing techniques — why they seek touch
- Emotional Regulation — what happens when told no
- Behavioural Flexibility — adapting rules to different settings

From the Pinnacle Network — Families Like Yours
Rohan, Age 7 — Hyderabad (ASD Level 1)
Before: Rohan would hug strangers at the supermarket and touch his teacher's hair for the texture. School complaints were weekly. His mother was in constant anticipatory anxiety in public. After 8 weeks: Rohan waves first. He asks "can I?" 70% of the time before touching. School complaints have stopped.
💬 "I can go to the supermarket without rehearsing disaster scenarios." — Rohan's mother
Priya, Age 10 — Pune (ASD + ADHD)
Before: Priya would grab peers by the arm, kiss adults without warning, and became distressed when told not to. After 6 weeks: She wears a wristband reading "ASK FIRST." Her Stop-Think impulse control has generalised. Peer relationships have improved noticeably.
💬 "She told me: 'Mummy, I asked Ananya before I hugged her and she said yes and we both smiled.' That single sentence was worth everything." — Priya's mother
Arjun, Age 5 — Delhi (ASD Level 2)
Before: Arjun grabbed food off strangers' plates and pulled at hair. Family had stopped going out. After 10 weeks: He says "high-five?" instead of grabbing. Family is visiting restaurants again.
💬 "At week 7 I almost gave up. Week 8 — he asked permission for the first time in real life. I cried." — Arjun's father
Illustrative cases based on Pinnacle clinical experience. Individual outcomes vary by child profile, consistency of implementation, and co-occurring conditions.
Preview of 9 materials that help with inappropriate touching Therapy Material
Below is a visual preview of 9 materials that help with inappropriate touching therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

Frequently Asked Questions About C-315
My child knows the rules but still touches inappropriately. Why?
Verbal rule knowledge (language centre) and real-time inhibition (prefrontal cortex) are different neural processes. Bridging them takes 4–8 weeks of consistent practice in real contexts. Keep going — generalisation follows consolidation. → See Card 32.
My child is 12. Is it too late?
Absolutely not. Adolescence is a critical window — social expectations increase dramatically. The protocol modifies for older children (Level 3–4, Card 30). Body safety education at 12 is protective for life.
Should I use anatomical terms for body parts?
Yes. WHO, AAP, and major paediatric bodies globally recommend correct anatomical terminology. Children who know correct words can communicate more clearly if they experience inappropriate touch — euphemisms reduce safeguarding effectiveness.
The behaviour improved at home but not at school. How do I address this?
Generalisation requires parallel implementation. Use the Teacher Template (share: "When [name] touches without asking, please say 'Ask first' — wait for the ask — then respond"). Consistent language across home and school is essential.
My child now asks permission for EVERYTHING — even family hugs. Is this overcorrection?
Yes — a common early-phase overcorrection. Introduce nuance: "With Mummy, Daddy, Grandma — hugs without asking. With friends and strangers — always ask first." The Greeting Ladder (Material 9) addresses this directly.
Didn't find your answer? Ask GPT-OS® → | Book Teleconsultation → | 9100 181 181 (FREE, 24×7, 18+ languages)
The Pinnacle Blooms Network® Promise
"From fear to mastery. One technique at a time." Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24×7, personalised, multi-disciplinary paediatric therapy environment — accessible to every family, everywhere.
OT
SLP
ABA/BCBA
SpEd
NeuroDev
CRO
This content is educational and does not replace assessment by a licensed speech-language pathologist, occupational therapist, behaviour analyst (BCBA), psychologist, or developmental specialist. Individual results vary. © 2025 Pinnacle Blooms Network® | Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | GSTIN: 36AAGCB9722P1Z2