9 Materials That Help With Hope Building
"She used to talk about what she'd be when she grew up. Now she says 'what's the point?'"
K-918 | Pinnacle Blooms Network®
Emotional Regulation Series
Act I — The Emotional Entry
The Recognition Moment
It starts quietly. The drawings that used to burst with colour go grey. The child who made plans for the future now shrugs when you mention next year. The one who used to try — even when things were hard — has stopped trying at all. Not because they're lazy. Not because they don't care. But because somewhere along the way, after enough disappointments, enough struggles, enough times of trying and falling short, they made a private, painful decision: it is safer to expect nothing.
Your child has lost hope. And you are watching it happen, helpless, heartbroken, searching for the words that will light the fire again.
You are not failing. Your child has not given up on life — they have given up on the possibility of change. That is a very different thing. And it can be rebuilt.
🏛️ Consortium Validated
Pinnacle Blooms Clinical Consortium
📋 K-918 | Episode 918
Emotional Regulation Series
👶 Ages 3–12
Home, school & clinic applicable

The Scale of This Challenge
You Are Not Alone — The Numbers
1 in 5
Children Affected
Children experiencing clinically significant hopelessness symptoms before age 12
60–80%
ASD & Motivation
Children with ASD who show reduced future orientation and motivation challenges
21M+
Sessions Recorded
Pinnacle Network sessions revealing hope and motivation as top family concerns
Childhood hopelessness is not rare. Learned helplessness — the belief that one's actions do not change outcomes — affects children across all neurodevelopmental profiles, and is particularly prevalent among children who have experienced repeated academic struggle, social rejection, or therapeutic setbacks. In India alone, an estimated 8–10 million children across developmental profiles show measurable deficits in hope orientation, goal-setting capacity, and future self-concept.
"You are not watching your child fail. You are watching their protective mind shield them from further pain. The intervention is not to demand hope — it is to create the conditions where hope naturally returns." — Pinnacle Blooms Clinical Consortium
📞Free Helpline: 9100 181 181 — Available 24×7 in 16 languages. All calls answered by trained clinical staff.
The Neuroscience
What's Happening in Your Child's Brain
The Science of Hope
Hope is not a feeling. It is a cognitive architecture.
According to Snyder's Hope Theory, hope consists of two neurological components:
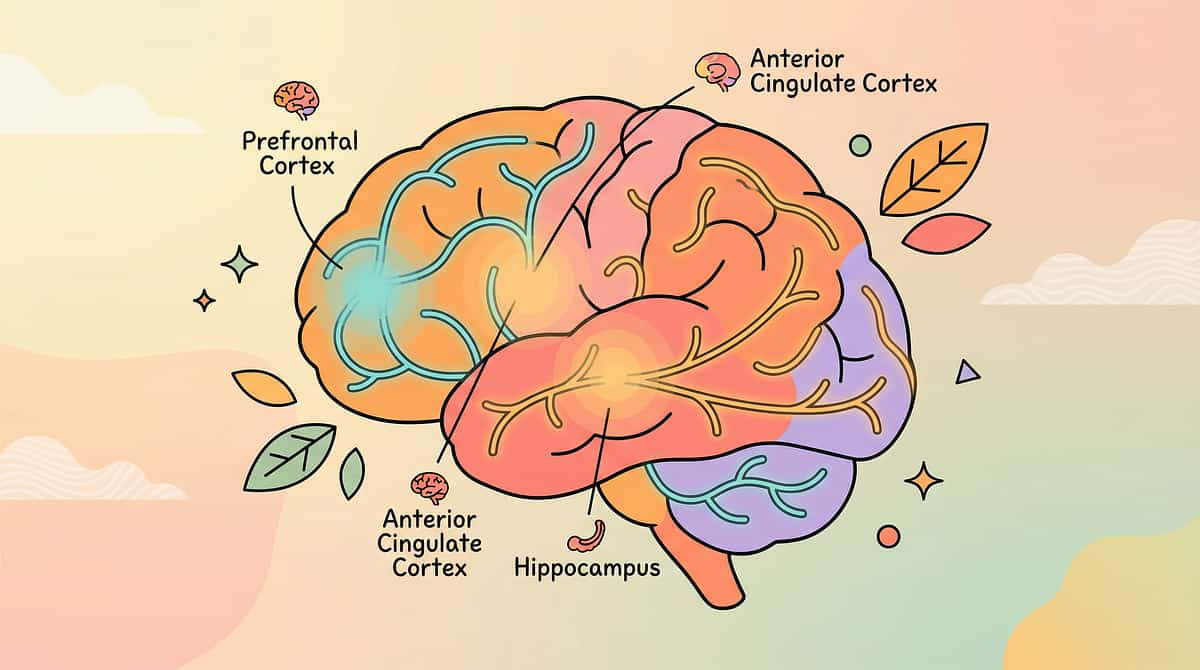
1. Pathways Thinking — The prefrontal cortex's ability to generate routes to desired goals. In hopeless children, this pathway-generation function is suppressed. The child literally cannot mentally navigate toward a goal.
2. Agency Thinking — The anterior cingulate cortex's role in generating the motivation to pursue those pathways. When a child has experienced repeated failure, the dopaminergic reward circuits that fuel "trying" become dysregulated.
This produces Learned Helplessness: a neurologically-reinforced belief that actions do not produce outcomes — not stubbornness or defiance, but an adaptive neurological response to an unresponsive environment.
In Plain English
Your child's brain has learned — from experience — that trying leads to pain. It is protecting them the only way it knows how: by shutting down the hope circuits before they can be disappointed again.
This is not a character flaw. It is an injury. And like all injuries, it heals — with the right intervention, consistently applied.
The 9 materials on this page are not "activities." They are neurological recalibration tools targeting a specific component of the hope architecture.
Brain Regions Involved
- Prefrontal Cortex — pathway generation, goal planning
- Anterior Cingulate Cortex — motivation, effort initiation
- Hippocampus — success memory encoding (suppressed in hopelessness)
- Amygdala — threat detection (hyperactivated, suppressing hope circuits)

Developmental Context
Hope Develops. And It Can Be Disrupted at Any Stage.
Ages 3–5 — "Present-Bound"
Hope = Now. Children live in the present. Hope is absorbed from caregiver optimism. Protective factors: positive immediate experiences, responsive caregiving. Risk: caregiver despair is contagious at this age.
Ages 6–8 — "Future Forming"
Hope = Goals. Future orientation begins. Goal-setting capacity emerges. Peer comparison starts. This is when the first school struggles can begin to erode hope. Critical window for intervention.
Ages 9–12 — "Identity Crystallising"
Hope = Self-Concept. Accumulated experiences become identity narratives: "I'm bad at this." Hopelessness here is the most treatment-resistant — but also the most transformative when properly addressed.
Commonly Co-Occurring Conditions
Depression
Hopelessness is a core diagnostic criterion in pediatric depression per DSM-5
Anxiety
Avoidance patterns overlap significantly with hopeless cognition
ADHD
Repeated failure experiences fuel hopelessness across settings
ASD
Social rejection and communication failures erode hope orientation
Learning Differences
Academic struggle is the most common precipitating factor

Evidence Grade II
Clinically Validated. Home-Applicable. Parent-Proven.
📚 Positive Psychology / Hope Therapy (Snyder, 2000–2020)
Over 40 peer-reviewed studies demonstrate structured hope-building interventions produce measurable increases in academic achievement, psychological wellbeing, and goal-directed behaviour. Effect sizes: moderate to large (Cohen's d = 0.5–0.8).
📚 Growth Mindset Interventions (Dweck, 2006–2020)
Systematic review of 43 studies demonstrates mindset interventions improve motivation, persistence, and academic performance. NBER meta-analysis (2019): significant positive effects for lower-performing students.
📚 Gratitude Interventions (Emmons & McCullough, 2003)
RCTs demonstrate structured gratitude practices in children aged 8–11 produce measurable increases in wellbeing, optimism, and prosocial behaviour within 5–8 weeks.
📚 Goal Ladder / Self-Efficacy (Bandura, 1977–2001)
Self-efficacy theory is among the most replicated frameworks in psychology. Mastery experiences, vicarious learning, and verbal persuasion consistently improve hope orientation across populations.
📚 Indian Context (Padmanabha et al., Indian J Pediatr, 2019)
Home-based interventions for Indian pediatric populations demonstrate significant outcomes across emotional regulation and self-concept domains when parent-administered with structured protocols. DOI: 10.1007/s12098-018-2747-4
"The evidence for hope-building materials is not emerging — it is established. These are not experimental activities. They are tools drawn from some of the most replicated science in developmental psychology." — Pinnacle Blooms CRO Division

Act II — The Technique
🌱 What Is Hope Building?
Formal Name: Structured Hope-Building Material Protocol Parent-Friendly Alias:The Hope Toolkit — 9 Things That Rebuild Belief in Tomorrow
Hope-building material interventions are a structured set of 9 evidence-based therapeutic tools — spanning positive psychology, cognitive-behavioural, and strengths-based approaches — designed to rebuild the neurocognitive architecture of hope in children aged 3–12. Each material targets a specific component of Snyder's Hope Theory: pathways thinking (the ability to see routes to goals), agency thinking (the motivation to pursue them), and goal cognition (the ability to identify and hold meaningful objectives).
This is not "positive thinking." It is precision-engineered hope reconstruction — using the same mechanisms employed by clinical psychologists, pediatric behavioural therapists, and positive psychology practitioners — adapted for daily home execution by parents and caregivers.
What makes this different from "just being encouraging": Verbal encouragement ("You can do it!") does not rebuild hope because it bypasses the neurological components that are damaged. These materials work because they create actual experiences of success, tangible evidence of capability, concrete pathways to goals, and physical representations of positive future orientation. The brain changes through experience, not words.
🧠 Emotional Regulation
🌟 Positive Psychology
🎯 Self-Efficacy
💭 Cognitive Restructuring
🤝 Social-Emotional Development
Age Range: 3–12 years | Session Duration: 10–20 minutes per material, 3–5 times per week | Environment: Home, school, therapy clinic — all applicable
Multi-Disciplinary Consortium
Who Uses This Technique
🧠 Child Psychology (Primary Lead)
Clinical psychologists deploy hope-building materials as core components of CBT, ACT, and Positive Psychology Interventions. Hope assessment tools (Children's Hope Scale, Snyder 1997) establish baseline, and material-based interventions are titrated by clinical response.
🎨 Occupational Therapy
OTs use vision boards, hope kits, and sensory comfort items within sensory integration frameworks. The act of creating (collaging, crafting, organising a hope kit) engages sensorimotor systems that support emotional regulation while building hope-oriented cognition.
📊 ABA / BCBA
BCBA practitioners deploy success journals and goal ladders as data-collection tools that simultaneously function as reinforcement systems. Goal ladders use behavioural shaping — successive approximation — to build mastery experiences systematically.
📖 Special Education
SpEd professionals integrate growth mindset materials and goal ladders directly into academic intervention plans. Reading goal ladders, writing success journals, and classroom gratitude practices address the academic hopelessness most commonly precipitating factor.
👶 NeuroDevelopmental Pediatrics
NeuroDev pediatricians screen for clinical depression (PHQ-A), anxiety, and trauma that may underlie hopelessness. They determine whether hope-building materials are appropriate standalone or adjuncts to medication and specialist referral.
"The brain doesn't organise by therapy type. Hope is built simultaneously through emotional experience (Psychology), sensorimotor engagement (OT), behavioural reinforcement (ABA), learning success (SpEd), and physiological regulation (NeuroDev). All five disciplines contribute to hope reconstruction." — Pinnacle Blooms Consortium Clinical Statement
Material 1 of 9
📓 Success Journals & Accomplishment Books
Clinical Function
Evidence-building against hopeless cognition.
The physical act of writing in first person, past tense, activates hippocampal encoding of positive experiences. Over time, this counteracts the selective negative memory bias characteristic of hopelessness.
Therapeutic Dosage
1 entry per day minimum. 3 entries ideal. More than 5 per day creates diminishing returns.
How to Use It
Three daily entries: (1) Something I did today — any action, however small. (2) Something that went okay — however minor. (3) Something I'm proud of, even a little — can be as small as "I ate breakfast."
Purchase Options
Price: ₹100–400 | Canon Category: Reinforcement Menus / Writing Tools
✅ Zero-Cost DIY
Any dedicated notebook + coloured pens. Cost: ₹30–80. The clinical value is in recording, not the notebook's quality.

Material 2 of 9
🖼️ Vision Boards & Future Collages
Clinical Function
Future orientation — making the positive future tangible.
The future visualisation process reactivates dormant imagination circuits. For children in hopelessness, being asked "what do you want?" is neurocognitively difficult — the process itself is the intervention, not the product.
Therapeutic Dosage
Created once, revisited monthly. Keep it displayed where the child sees it daily — this is the visual anchor.
What the Child Searches For
- One thing they want to DO someday
- One place they want to GO
- One person they want to BE LIKE
- One thing that makes them smile to imagine
Purchase Options
Price: ₹100–300 | Canon Category: Visual Goal Systems / Art & Craft
✅ Zero-Cost DIY
Old magazines + cardboard + glue stick. Cost: ₹0–50. Images from any source activate future visualisation.

Material 3 of 9
💪 Strength Cards & Character Spotting Tools
Clinical Function
Self-perception repair — shifting focus from deficit to capability.
Fan out the cards. Sit silently while they look. Do not point to cards. Let them choose. The act of searching is therapeutic. You are externalising strengths the child cannot see yet.
Key Prompt
"Look through these and pull out any one that might — even a little bit — describe you. You don't have to be sure. Just maybe."
What to Do When Child Says "None of These Are Me"
Don't argue. Pick up one card (e.g., "Kind") and say: "I remember once when you [specific example]. That was this one." Offer it to them. Professional evaluation is indicated if this persists across 3 sessions.
Purchase Options
Price: ₹300–800 | Canon Category: Strengths-Based Assessment Tools
✅ Zero-Cost DIY
Handwritten cards with strength names + simple symbols. Cost: ₹0. Hand-writing strengthens the parent-child interaction.

Material 4 of 9
🪜 Goal Ladders & Step Charts
Clinical Function
Pathways thinking — breaking impossible goals into achievable steps.
Breaking the goal into steps activates pathways thinking. The first achievable step creates an immediate mastery experience — evidence that "I can do something." The first rung must be achievable within 24–48 hours.
How to Build It
- Write the child's chosen goal at the top
- Work backward: "What's the step just before reaching that goal?"
- Continue until you reach something achievable THIS WEEK
- First rung achievable within 24–48 hours
If Steps Feel Impossible
The steps are too large. Hopeless children need micro-steps — smaller than you think necessary. Ask: "What's something even easier than that?" Keep going until you reach something achievable within 24 hours. "Picked up a pencil" is a valid rung.
Purchase Options
Price: ₹50–200 | Canon Category: Visual Goal Systems / Progress Trackers
✅ Zero-Cost DIY
Paper + markers + stickers. Cost: ₹10–30. The visual metaphor of climbing is what matters.

Material 5 of 9
🫙 Gratitude Jars & Thankfulness Tools
Clinical Function
Attention retraining — building positive perception patterns.
1 note per day is sufficient. The ritual matters more than the volume. Consistency across 30+ days is when neurocognitive changes become measurable. Write the first note WITH the child — your note, about them: "I am grateful for [child's name] because..."
Critical Safety Note
Gratitude practice should never be used to dismiss or minimise the child's genuine pain. "At least you have..." is harmful. The goal is to expand awareness — not deny what's hard.
Opening the Conversation
"We're going to fill this jar. One good thing at a time. It can be tiny. 'My pillow is soft' counts. 'I didn't drop my lunch' counts. Want to do the first one together?"
Purchase Options
Price: ₹50–150 | Canon Category: Positive Psychology Tools
Pinnacle Recommended: Rosette Imprint Reward Jar → amzn.in/d/02C5R9Jn
✅ Zero-Cost DIY
Any washed food container + paper slips + pens. Cost: ₹0–20. The ritual of depositing notes is the intervention.
Material 6 of 9
📚 Growth Mindset Books & Stories
Clinical Function
Belief restructuring — "not yet" instead of "never."
Narrative content, not the physical book, is the mechanism. Stories from YouTube and parent-narrated family stories deliver the same clinical principle. Reading and watching activate different neurological processing pathways — both are valuable.
The "Not Yet" Reframe
Growth mindset books teach children that "I can't do this" becomes "I can't do this yet" — a single word shift that preserves future orientation even in limitation acknowledgment.
Key Recommended Titles
- The Most Magnificent Thing — Ashley Spires
- What Do You Do With a Problem? — Kobi Yamada
- Your Fantastic Elastic Brain — JoAnn Deak
Purchase Options
Price: ₹200–500 | Canon Category: Narrative Therapeutic Materials / Bibliotherapy
✅ Zero-Cost DIY
Stories from YouTube + parent-narrated family stories. Cost: ₹0. Narrative content, not the physical book, is the mechanism.

Material 7 of 9
🤲 Kindness & Contribution Projects
Clinical Function
Agency experience through helping — rebuilding sense of worth and purpose.
The act of giving, not the materials, is therapeutic. Kindness projects must be guaranteed-success. A rejected or unacknowledged kindness act will reinforce hopelessness. Start with family, then expand to friends, then community.
Advanced Version
For children at Stage 3–4: child designs and executes their own project with community connection. When a child notices someone else struggling and offers help, this is the most advanced hope indicator.
Why It Works
Children in hopelessness believe they have nothing to offer. A kindness project creates irrefutable evidence to the contrary — "someone's day is better because of you" is one of the most potent agency-building statements available.
Purchase Options
Price: ₹100–500 | Canon Category: Prosocial Development Materials
✅ Zero-Cost DIY
Card-making materials + a list of recipients. Cost: ₹0–50. The act of giving, not the materials, is therapeutic.

Material 8 of 9
📋 Worry-to-Action Planners
Clinical Function
Learned agency — transforming passive worry into active problem-solving.
Hopeless children are frequently trapped in worry loops — passive, circular, draining. The Worry-to-Action Planner breaks this loop by sorting worries into "Can Control" and "Can't Control" columns, then generating concrete actions for the controllable category.
The Cognitive Exercise
The cognitive exercise, not the paper format, is the tool. Any folded piece of A4 paper delivers the same clinical mechanism as a printed workbook.
Why This Rebuilds Hope
Every time a child identifies something they can do about a worry, their agency thinking receives direct activation. Over repeated sessions, the automatic question becomes "what can I do about this?" — a fundamental shift from passive to active orientation.
Purchase Options
Price: ₹50–200 | Canon Category: Cognitive-Behavioural Tools
✅ Zero-Cost DIY
Fold any paper into "Can Control / Can't Control" columns. Cost: ₹0. The cognitive exercise, not the paper format, is the tool.
Material 9 of 9
🧺 Hope Kits & Coping Collections
Clinical Function
Externalising hope when internal hope is depleted.
The Hope Kit is the safety net for bad days. When a child's internal hope circuits are temporarily overwhelmed, the Kit provides physical, tangible evidence that hope exists — outside of their current emotional state. The personalisation and curation process IS the therapy.
Closing Ritual
Close the box: "Everything in there is waiting for you when you need it." On bad days, open it together. Read the success journal entries from better days.
What Goes Inside
The child chooses everything. Suggested contents:
- A comfort object (soft toy, smooth stone)
- A favourite photograph
- A note from someone who loves them
- A reminder of a past success
- One strength card they believe in
Purchase Options
Price: ₹100–400 | Canon Category: Transition Objects / Coping Tool Sets
Pinnacle Recommended: Animal Soft Toys (comfort anchor) → amzn.in/d/022Lj6Fr
✅ Zero-Cost DIY
Any decorated box or biscuit tin + personally curated items. Cost: ₹0–100.
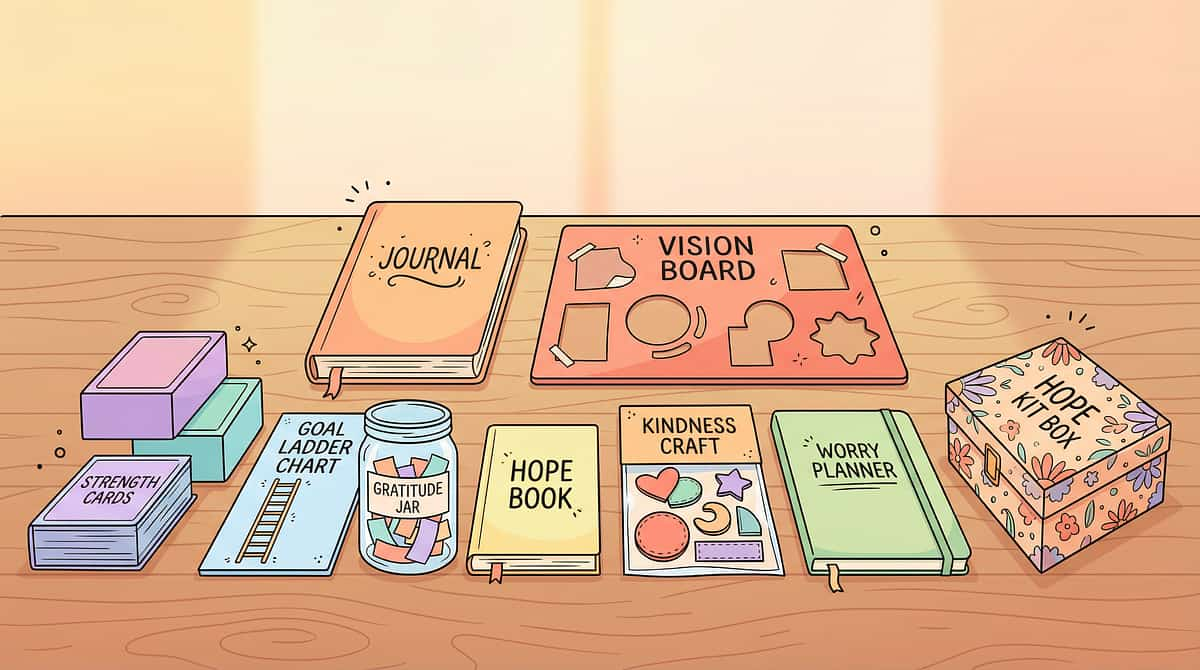
Complete Toolkit
9 Materials. One Hope Toolkit.
1
Success Journals
Evidence-building against hopeless cognition
2
Vision Boards
Future orientation — making the positive future tangible
3
Strength Cards
Self-perception repair — shifting from deficit to capability
4
Goal Ladders
Pathways thinking — breaking impossible goals into steps
5
Gratitude Jars
Attention retraining — building positive perception patterns
6
Growth Mindset Books
Belief restructuring — "not yet" instead of "never"
7
Kindness Projects
Agency experience through helping — rebuilding worth and purpose
8
Worry-to-Action Planners
Transforming passive worry into active problem-solving
9
Hope Kits
Externalising hope when internal hope is depleted
Budget (DIY)
₹50–200 total
Recommended
₹750–2,000 total
Full Clinical Kit
₹2,000–3,500 total

Equity Principle
Every Family Can Start Today — Regardless of Budget
WHO/UNICEF equity principle: No child should be denied therapeutic intervention because of family income. Every one of these 9 materials has a zero-cost version that delivers the same clinical principle.
Material | Purchase Option | Zero-Cost DIY | Why DIY Works | |
Success Journal | Decorated notebook ₹150 | Old exercise book + coloured pens | The clinical value is in recording, not the notebook's quality | |
Vision Board | Poster board ₹200 | Old newspapers + cardboard packaging | Images from any source activate future visualisation | |
Strength Cards | Pre-printed set ₹500 | Paper cut into cards, written by hand | Hand-writing strengthens the parent-child interaction | |
Goal Ladder | Printed chart ₹100 | Paper + drawn ladder + stickers | The visual metaphor of climbing is what matters | |
Gratitude Jar | Decorative jar ₹120 | Washed food container + paper slips | The ritual of depositing notes is the intervention | |
Growth Mindset Books | Published books ₹300 | YouTube stories + parent-narrated family stories | Narrative content, not physical book, is the mechanism | |
Kindness Projects | Craft kit ₹300 | Paper + crayons already in the home | The act of giving, not the materials, is therapeutic | |
Worry Planner | Printed workbook ₹150 | Fold any paper into two columns | The cognitive exercise, not the paper format, is the tool | |
Hope Kit | Purchased box ₹200 | Decorated shoebox or biscuit tin | The personalisation and curation process IS the therapy |
The ₹0 version of hope-building: A notebook, a jar, a piece of paper, and a parent who consistently shows up — these are the essential ingredients. Everything else is enhancement, not requirement.

⚠️ Safety First
The Pre-Session Safety Gate
Hope-building is gentle but not risk-free. These safety guidelines protect your child and maximise intervention effectiveness. Read completely before beginning.
🟢 GREEN — Safe to Proceed
- Child is in a baseline-regulated emotional state
- Child has eaten, is not overtired, not ill
- You have 15–30 uninterrupted minutes
- Space is prepared as per setup guide
- No recent significant trauma in the past 24 hours
🟡 AMBER — Modify or Delay
- Child has had a particularly difficult day — reduce to 1 material
- Child shows low affect but is not in crisis — use gentlest materials
- You feel impatient or frustrated — postpone and self-regulate first
- Child recently experienced significant failure — address with empathy first
🔴 RED — Do Not Proceed
- Child has made statements about not wanting to live → Call 9100 181 181 IMMEDIATELY
- Child is in acute emotional crisis (panic, dissociation, severe distress)
- Child has experienced traumatic event within past 48 hours
- Persistent sadness, sleep disturbance, appetite changes for more than 2 weeks → Professional evaluation required
⚠️Hope-building materials are supplements to, NOT replacements for, professional mental health support in cases of clinical depression or suicidal ideation.⚠️ If a child cannot identify a single success, strength, or thing to be grateful for after gentle prompting — this indicates clinical depression requiring professional evaluation. Do not force entries. 📞Crisis Support: 9100 181 181 (24×7, 16 languages)
The Environment Is the First Intervention
Set Up Your Space
Environmental Conditions
- Lighting: Warm, soft — not overhead fluorescents. Afternoon or evening light ideal. Lamps over overhead lights.
- Sound: Quiet, or soft instrumental background music. No TV. No sibling noise if possible.
- Temperature: Comfortable, not cold.
- Remove: Screens, homework, anything associated with past failure. This space is success-only.
Room Choice
Choose the room where your child feels safest and most relaxed — not necessarily the bedroom. Many families use the kitchen table (associated with nurturing) or a cozy corner of the living room.
Parent Positioning
Sit beside your child, not across from them. Side-by-side positioning reduces the evaluative pressure of direct eye contact and creates a collaborative rather than instructional dynamic. This is the OT principle of "co-occupation" — doing together, not watching.
The Transition Ritual
Create a brief, consistent opening ritual — light a candle, play 30 seconds of a special song, or use a phrase: "This is our hope time." Ritual creates neurological distinction between ordinary time and therapeutic time.
Before You Begin
Place one material only in view. The others remain out of sight. Decision fatigue is real — too many materials creates overwhelm that mimics hopelessness.

Pre-Session Assessment
Is Your Child Ready? The 60-Second Check
Before beginning each hope-building session, check these 7 indicators:
Indicator | ✅ Green | ⚠️ Yellow | 🔴 Red | |
Physical state | Fed, rested, healthy | Tired but okay | Hungry, sick, overtired | |
Emotional state | Baseline calm or neutral | Low affect, quiet | Distressed, crying, shut down | |
Engagement signal | Makes eye contact, responds to name | Minimal response | No response, avoidant | |
Willingness signal | No active resistance | Some hesitation | Active refusal | |
Recent event | Normal day | Difficult but not crisis | Significant distress event | |
Caregiver state | Calm, present | Slightly stressed | Anxious, impatient, frustrated | |
Time available | Full 20 min available | 10 min available | Less than 10 min |
5–7 Greens
Full session — all materials available
3–4 Greens
Modified session — choose 1 material only; use the gentlest (Gratitude Jar or Hope Kit)
0–2 Greens
Postpone — do a co-regulation activity instead; try tomorrow
"A session that begins wrong rarely ends right. The best session is one that starts when both the child AND the parent are ready."

Act III — The Protocol
Step 1 of 6
Step 1 — The Invitation
⏱ Timing: 1–2 minutes | The ABA Pairing Principle meets OT Just-Right Challenge.
1
Ages 3–6
"I found something really cool. Can I show you?" [Reveal one material — e.g., the Success Journal — decorated with their name]
2
Ages 7–10
"I want to do something with you. It's not homework. It's kind of like... discovering things. Want to try for just 5 minutes?"
3
Ages 10–12
"I've been reading about some things that actually help when everything feels pointless. Not fake-cheerful stuff — real things. Can I show you one?"
When Resistance Appears
Child shrugs / "I don't want to"
"Okay. It's here if you change your mind." Do NOT withdraw the material — leave it visible. Wait 2 minutes. Try once more.
Child says "it's stupid"
"I thought that too at first. Want to see what it is before deciding?"
Child leaves the space
Pause for today. Do not pursue. Note the response for tomorrow's session start.

Step 2 of 6
Step 2 — The Engagement
⏱ Timing: 2–5 minutes | The child is engaged. Now deepen the interaction.
For Success Journals
"This is your book. Only good things go in here. Every time you write something in it, it becomes proof. Proof that you did something. Proof that something went right. Want to write the first thing?"
Start with: "What's one thing that happened today that wasn't terrible?"
For Gratitude Jars
"We're going to fill this jar. One good thing at a time. It can be tiny. 'My pillow is soft' counts." Write the first note WITH the child — your note, about them: "I am grateful for [child's name] because..."
For Strength Cards
"Look through them and pull out any one that might — even a little bit — describe you." Fan out the cards. Sit silently while they look. Do not point to cards. Let them choose. The act of searching is therapeutic.
Engagement Indicators
Child begins the activity without you leading
Child asks a question about the material
Child adds something you didn't suggest
Child shows the material to a sibling or pet (generalisation signal!)
Reinforcement cue (within 3 seconds of any engagement):"I noticed that." / "That's a real one." / "Yes — that counts."Do NOT: Evaluate, correct, or redirect at this stage. Whatever the child offers is correct.

Step 3 of 6
Step 3 — The Therapeutic Action
⏱ Timing: 5–10 minutes (core therapeutic window) — This is the active ingredient. The neurological work happens here.
For Success Journals
Child writes, draws, or dictates 3 entries: (1) Something I did today, (2) Something that went okay, (3) Something I'm proud of, even a little. Writing in first person activates hippocampal encoding of positive experiences.
For Goal Ladders
Build a ladder for ONE child-chosen goal. Write the goal at the top, work backward to steps, continue until something is achievable THIS WEEK. First rung must be achievable within 24–48 hours. Creates immediate mastery experience.
For Vision Boards
Child searches for: one thing to DO someday, one place to GO, one person to BE LIKE, one thing that makes them smile to imagine. The search process itself reactivates dormant imagination circuits.
Response Spectrum
Ideal ✅ | Acceptable ⚠️ | Concerning 🔴 | |
Engaged, adds beyond prompts | Complies with minimal participation | Cannot generate any content, freezes | |
Shows micro-expressions of positive affect | Maintains neutral affect throughout | Shows distress, crying, refusal | |
Generalises beyond the session | Completes activity and disengages | Says "there's nothing good" / "I can't think of anything" |
If Concerning responses occur: Do not push. Close the session warmly. Note the response — this is clinical data. Consider professional consultation. 📞 9100 181 181

Step 4 of 6
Step 4 — Repeat & Vary
⏱ Timing: Across sessions — daily or 3–5× per week
Hope is not rebuilt in a single session. The clinical evidence points to 5–8 weeks of consistent practice for measurable changes in hope orientation.
1
Success Journal
1 entry per day minimum. 3 entries ideal. More than 5 per day creates diminishing returns.
2
Goal Ladder
Review the current rung DAILY. Celebrate completed rungs IMMEDIATELY. Do not add new rungs until the previous one is fully climbed.
3
Gratitude Jar
1 note per day is sufficient. The ritual matters more than the volume. Consistency across 30+ days is when neurocognitive changes become measurable.
4
Vision Board
Created once, revisited monthly. Keep it displayed where the child sees it daily — this is the visual anchor.
Satiation Indicators — When to Vary, Not Stop
Child completes the activity mechanically, without engagement → Switch materials, not frequency
Child asks "do we have to?" but still participates → Introduce a new material from the 9
Child begins substituting non-meaningful content → Read together or do a kindness project to break the pattern
3 genuine reps > 10 mechanical ones — Pinnacle Clinical Axiom

Step 5 of 6
Step 5 — Reinforce & Celebrate
⏱ Timing: Within 3 seconds of any hope-aligned behaviour
Reinforcement Scripts
Natural, not performative:
- "I noticed that."
- "That's real. That happened."
- "You found that yourself."
- "One rung climbed."
- "You just added to your proof."
- "That's yours. It's in the jar now."
- "Someone's day is better because of you."
- "You found something you could do."
What NOT to Say
- ❌"I'm so proud of you!" — Places focus on caregiver approval, not child achievement
- ❌"See? Things aren't so bad!" — Dismisses genuine difficulty
- ❌"I knew you could do it!" — Implies the child doubted unnecessarily
✅ Instead
Specific, child-focused, achievement-referenced language. Reference the exact action, the exact material, the exact moment.
Tangible Reinforcement
For children who benefit: Reward Stickers — 1 sticker per journal entry, per goal rung climbed, per gratitude note. Reward Jar — tokens accumulate, exchanged for child-chosen reward.
Celebrate the attempt, not just the achievement. The child who tried to think of a success and couldn't — but stayed in the chair — is doing the hardest work. That too is celebrated.

Step 6 of 6
Step 6 — The Cool-Down
⏱ Timing: 2–3 minutes — No session ends abruptly. Especially not a hope-building session.
The transition out of a therapeutic activity — back to ordinary life — must be handled with care. Abrupt endings can undo the emotional work of the session, especially for children who have experienced therapy as something done to them rather than with them.
Success Journal
Close it with both your hands around it: "All of that is yours. It doesn't go anywhere."
Goal Ladder
Point to the rung completed today: "One rung. It's marked. It happened."
Gratitude Jar
Place the final note together: "Okay. It's in there. Good."
Hope Kit
Close the box: "Everything in there is waiting for you when you need it."
If child resists ending — this is a positive clinical sign. Do not extend. Instead: "I know. Let's do it again tomorrow. Same time?" Tomorrow commitment is a hope-building act in itself: there will be a tomorrow, and it will include this.Post-session: Immediately record one observation — what did the child do that they didn't do last session? This is your clinical data.
Track Every Session
Capture the Data — Right Now
"60 seconds of data now. Months of clarity later." — Pinnacle Blooms Clinical Axiom
Data Point 1 — Material Used
Which of the 9 materials were used today? Circle or tick each material used in the session.
Data Point 2 — Engagement Level (1–5)
1: No engagement, session abandoned | 2: Minimal participation | 3: Passive compliance | 4: Active participation | 5: Full engagement — child initiated and generalised
Data Point 3 — Hope Marker
One specific thing the child said or did indicating hope orientation. Any "I can..." statement, goal-related comment, positive self-reference, or expression of future anticipation.
Weekly review: At the end of each week, look at the 5–7 data points together. Are engagement levels trending up? Are hope markers appearing more frequently? Are hopeless statements decreasing?
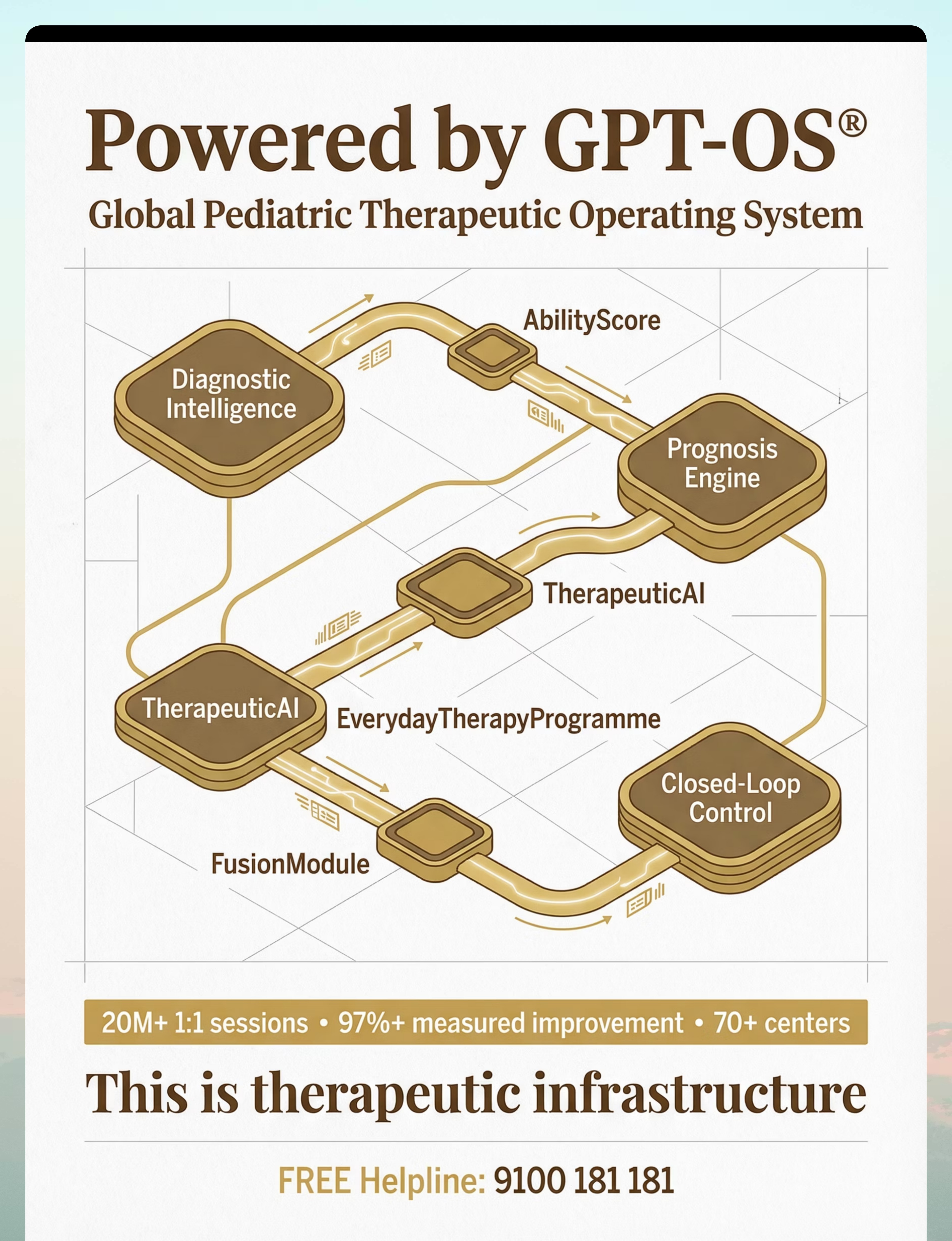
GPT-OS® Integration: This data feeds your child's Hope & Optimism Index — one of the 12 readiness indexes that GPT-OS® tracks across the developmental profile. 📞 9100 181 181

Troubleshooting
Most Sessions Don't Go Perfectly. Here's What to Do.
Session abandonment is not failure. It is data. Every difficult session tells you something about where the hope deficit lives.
Problem 1: "I can't think of anything good"
Why: The child's negative memory bias is currently stronger than their ability to access positive memories. What to do: Don't push. Instead, you write an entry about THEM: "Let me think of something good about you." Read it aloud. One entry by end — yours about them is sufficient.
Problem 2: Rejects all strength cards ("none of these are me")
Why: Self-perception is severely distorted toward deficit. What to do: Pick up one card (e.g., "Kind") and say: "I remember once when you [specific example]. That was this one." Offer it to them. Professional evaluation indicated if this persists across 3 sessions.
Problem 3: Child destroys the journal or vision board
Why: Hope materials can trigger anger in deeply hopeless children — hope feels forced or cruel. What to do: Do NOT react with disappointment. Calmly say: "That's okay. We can make another one when you're ready." Do not restart that material for at least 1 week.
Problem 4: Gratitude practice produces toxic positivity
Why: You may have used gratitude to dismiss the child's pain with "But at least..." What to do: Stop immediately. Validate first: "I hear you. That was really hard. And also — not instead, also — this small thing is here too."
Problem 5: Goal ladder steps feel impossible
Why: The steps are too large. What to do: Rebuild with smaller rungs. Ask: "What's something even easier than that?" Keep going until you reach something achievable within 24 hours. "Picked up a pencil" is a valid rung.
Problem 6: Engaged in sessions but no generalisation
Why: Normal in early phases — hope materials are working within the session but haven't transferred to independent cognition. What to do: Create environmental anchors — display the vision board, keep the gratitude jar on the kitchen table, leave the success journal open.
Problem 7: Caregiver feels the activities are not "working"
Why: Hope rebuilding is slow and not linear. Absence of dramatic change in weeks 1–3 is expected. What to do: Review the data from the session tracker. Look at engagement trends, not statements. Trust the process.

Personalisation
No Two Children Build Hope the Same Way
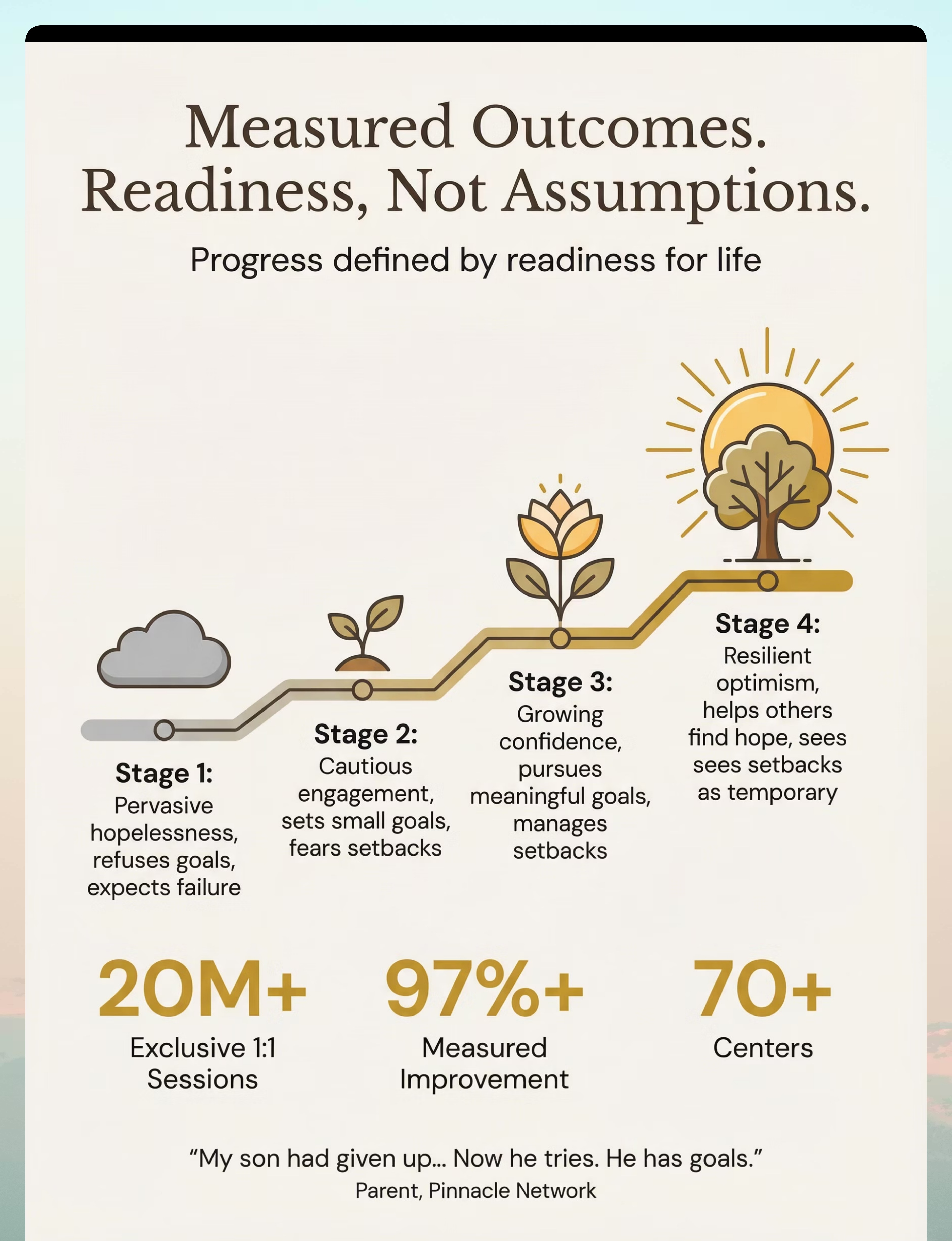
⬇ Easier Version (Stage 1–2)
- Success Journal: caregiver writes, child dictates or draws. 1 entry only.
- Goal Ladder: only 3 rungs, first achievable today.
- Gratitude Jar: caregiver and child contribute equally (1 each per session)
- Strength Cards: begin with 5 cards only — obvious strengths pre-selected by caregiver
- Hope Kit: build together; caregiver adds first item
⬆ Harder Version (Stage 3–4)
- Success Journal: 5 entries per day, child adds photo evidence
- Goal Ladder: 10 rungs, child writes all steps independently
- Strength Cards: child interviews family members about observed strengths
- Kindness Projects: child designs and executes their own project
Personality-Based Variations
Verbal / Language-Oriented
Success journals flourish. Growth mindset books and discussions. Word-based gratitude notes.
Visual / Artistic
Vision boards first. Draw the goal ladder instead of writing. Illustrate strength cards with self-portraits.
Action / Kinesthetic
Kindness projects first (doing > reflecting). Physical goal ladders. Worry-to-action planners with physical actions.
Social Children
Involve a sibling or friend in the vision board. Gratitude notes for others. Contribution projects with community connection.
Introverted / Private
Keep materials private — no sharing required. The journal is theirs alone. The hope kit is personal, never shown without permission.
Age Modifications at a Glance
Tool | Ages 3–5 | Ages 6–9 | Ages 10–12 | |
Journal | Picture-only | Written + drawn | Written, reflective format | |
Goal Ladder | 3-rung picture ladder | 5-rung word + picture | 10-rung detailed | |
Gratitude Jar | Jar with stickers instead of notes | Short phrase notes | Full sentence notes | |
Strength Cards | Caregiver-made | Child selects from pre-made | Child writes own |
Weeks 3–4
Week 3–4: Consolidation Signs
Something Is Shifting. Watch for These Signs.
Anticipatory Behaviour
Child asks "are we doing our hope time today?" without being prompted. This is the most significant early consolidation marker — the activity has become expected and wanted.
Spontaneous Generalisation
Child mentions the vision board during an unrelated conversation. Child points to their goal ladder without prompting. Hope has moved outside the session.
Reduced Resistance
Initial session resistance decreases. The child begins the activity more quickly with less prompting. The approach to the materials becomes easier.
Expanded Content
Journal entries become more detailed, less minimal. Strength card selections expand beyond the obvious first choices. Gratitude notes show more nuance.
Behaviour Changes
Subtle shifts in response to setbacks. Child still experiences disappointment but the duration of the hopeless response decreases measurably.
The neural pathway principle: Repeated structured positive experience literally changes the brain. The hippocampus begins encoding positive memories more readily. The prefrontal cortex's pathways thinking circuits receive consistent activation.
"You may notice that you feel more confident too." Parents who execute hope-building protocols consistently report a parallel shift in their own hopefulness about their child's trajectory. The caregiver-child hope system is bidirectional.
Weeks 5–8
Week 5–8: Mastery Indicators
The Hope Architecture Is Forming. These Are the Signs.🏅
🌟 Goal Setting Independence
Child sets a goal without being asked. Any goal — even "I want to finish this drawing." The spontaneous activation of goals thinking indicates pathways restoration.
🌟 Success Attribution Shift
Child attributes a success to their effort rather than luck: "I studied for that" instead of "I just got lucky." This is the core indicator of learned helplessness reversal.
🌟 Hope Language
Regular use of "not yet" framing. "I can't do that yet" — future orientation is present even in limitation acknowledgment.
🌟 Setback Recovery Speed
After a disappointment, the child returns to baseline faster. Same pain — shorter duration. Hopelessness responses are shorter and less intense.
🌟 Contribution Orientation
Child asks about doing a kindness project. Child notices someone else struggling and offers help. This is the most advanced indicator — hope has expanded to include others.
"Mastery Unlocked" criteria (K-918): The child has demonstrated, across 3+ consecutive sessions: independent goal-setting, spontaneous positive self-reference, use of hope tools without prompting, and reduced frequency/duration of hopeless statements. After 2 weeks of stable mastery, GPT-OS® recommends moving to K-919 (Self-Esteem) while maintaining K-918 materials as ongoing practice.

🎉 Milestone Reached
Celebrate This Win
"You started this journey when your child had stopped believing. When 'what's the point?' was the most common phrase in your home. When the drawings went grey and the plans stopped being made."
You showed up, session after session, often without visible results. You held hope for your child when they couldn't hold it themselves. You were the external hope system — the living evidence that tomorrow was worth showing up for.
📓 The Journal
Created evidence against hopelessness
🖼️ The Vision Board
Built a map to the future
💪 Strength Cards
Revealed invisible capabilities
🪜 Goal Ladder
Broke the impossible into possible
🫙 Gratitude Jar
Trained eyes to see good
📚 The Books
Showed "can't" has a prefix: "not yet"
🤲 Kindness Projects
Proved your child matters
📋 Worry Planner
Built agency from passivity
🧺 Hope Kit
Gave hope a home
Family celebration suggestion: Take a photo of the full hope kit, the completed goal ladder, the vision board. Date it. Title it: "[Child's name] — [Date] — The day hope came back."Journal prompt: Write one thing your child said or did in the past 8 weeks that they would NOT have said or done when you started. That is the measure of what happened here.

Progression Pathway
K-918 in Context — Your Child's Journey
K-916: Disappointment Management
Prerequisite — building tolerance for setbacks
K-917: Self-Compassion
Prerequisite — reducing self-critical responses
★ K-918: Hope Building ★
YOU ARE HERE — rebuilding belief in tomorrow
K-919: Self-Esteem
Recommended next — foundation reinforced with purpose and identity
K-920 → K-930s: Resilience Advanced Series
Identity development and advanced resilience skills
Branching Options Based on Your Child's Response
Responded via Goal Ladder
→ K-919 Self-Esteem — pathways thinking reinforced with purpose and identity work
Responded via Kindness Projects
→ K-820 Community Connection — social purpose as ongoing hope engine
Challenging due to Anxiety
→ Address Anxiety Management (Domain C) before continuing K-919
Limited Progress + Depression Signs
→ Professional evaluation required before progression. Call 9100 181 181.
Related Techniques
More Techniques in the Emotional Regulation Domain
All 6 related techniques use materials from the K-918 Hope Toolkit. Your investment in these 9 materials supports the entire Emotional Regulation domain.
Technique | Code | Level | Materials You Already Have | |
Self-Compassion Practice | K-917 | Core | Journal ✓ Strength Cards ✓ | |
Disappointment Management | K-916 | Core | Worry Planner ✓ | |
Self-Esteem Building | K-919 | Core | Strength Cards ✓ Journal ✓ | |
Identity Development | K-920 | Advanced | Vision Board ✓ Strength Cards ✓ | |
Motivation Restoration | K-915 | Core | Goal Ladder ✓ Reward System ✓ | |
Resilience Fundamentals | K-930 | Advanced | Hope Kit ✓ All materials ✓ |
Domain K — Emotional Regulation & Positive Psychology Cluster EMO-09 | Techniques K-900 through K-950
The Developmental Map
Hope Is One Piece of a Larger Plan
GPT-OS® monitors 12 developmental domains across your child's profile. K-918 is in Domain K: Emotional Regulation — and its effects ripple outward.
Domain B — Communication
A hopeful child communicates more. Hope building directly improves social language and expressive communication.
Domain E — Attention
Hopeless children show reduced attention and engagement. Hope restoration improves attentional capacity concurrently.
Domain C — Behaviour
Many behavioural challenges are driven by hopeless cognition ("it doesn't matter anyway"). Hope building reduces avoidance motivation.
"This technique is one piece of a larger plan. But it is a crucial piece — hope is the oxygen that makes all other developmental work possible."
Act V — Community & Ecosystem
From "What's the Point?" to "Not Yet."
Family A | Delhi | Child: 10 years, ASD + Academic Struggles
"My son had completely given up. After years of struggling in school and being teased, he stopped trying, stopped dreaming, stopped believing anything could change. He wouldn't set goals because he said he'd never reach them."
8 weeks later: "He still struggles. But he tries now. He has goals. When he fails, he says 'not yet' instead of 'never.' He has a hope kit in his room. When things are hard, he opens it and remembers why to keep going."
Family B | Hyderabad | Child: 7 years, Developmental Delays
"She used to make plans and get excited about things. After two years of therapy with slow progress, she stopped believing it was working. She'd sit in sessions with her arms crossed. 'Waste of time,' she'd say — a 7-year-old."
6 weeks later: "She points to the vision board and says 'I'm going to do that one next.' She made a card for her therapist saying 'thank you for helping me.' She contributes now. She believes in tomorrow."
"The most consistent finding across our 20M+ sessions is that hope restoration precedes all other developmental gains. A hopeless child cannot effectively participate in any therapy. Hope is not a soft metric — it is the foundational enabling condition for every other intervention to work." — Pinnacle Blooms Consortium, Child Psychology Division
📞9100 181 181 — Share your family's journey and inspire others
Community
You Are Not Doing This Alone
The isolation of parenting a child with developmental challenges is itself a clinical risk factor. Parents who are connected to other families implementing the same interventions show significantly higher adherence and better child outcomes than isolated parents.
📱 WhatsApp Parent Circle
Active families sharing session notes, wins, and troubleshooting support. Join the Hope Building Parents group at wa.pinnacleblooms.org/hope-building
💬 Online Parent Forum
Discussion threads organised by child age, challenge level, and material type. Moderated by Pinnacle clinical team. pinnacleblooms.org/community/hope-building
🤝 Peer Mentoring
Talk to a parent who has completed K-918 and is willing to share their journey. Available through your nearest Pinnacle centre or by calling 9100 181 181.
📍 Local Parent Meetup
Monthly parent meetups at Pinnacle centres — domain-specific, facilitated by therapists. Find nearest group at pinnacleblooms.org/centers
"Your experience helps others. Consider sharing your K-918 journey — the parent who struggled for 6 weeks and then watched their child say 'not yet' for the first time is exactly the story another parent needs to hear."
Preview of 9 materials that help with hope building Therapy Material
Below is a visual preview of 9 materials that help with hope building therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
Professional Support
Home + Clinic = Maximum Impact
🧠 Child Psychology
Formal hope assessment (Children's Hope Scale), depression screening, CBT/ACT with hope-focus, caregiver coaching for hope-building implementation at home.
📊 Behavioural Therapy (ABA/BCBA)
Goal ladder construction based on behavioural baseline, reinforcement schedule optimisation, data analysis from session tracking sheets.
🎨 Occupational Therapy
Sensory integration support for hope kit contents, vision board construction support, environmental setup consultation.
📖 Special Education
Integration of hope materials into school IEP, teacher training for hope-supportive language, academic goal ladders aligned with curriculum.
👶 NeuroDev Pediatrics
Depression screening, anxiety assessment, medical rule-out, medication evaluation if clinically indicated.
The combination principle: A parent implementing K-918 at home daily, supported by a Pinnacle therapist reviewing data weekly, produces outcomes that neither home-only nor clinic-only approaches can match.
📞FREE National Helpline: 9100 181 181 — Available 24×7 in 16 languages. All calls answered by trained clinical staff.