
"You dress your child every morning — and every morning, their arms resist the sleeve."
That stiffness has a name: High Muscle Tone — medically, hypertonia or spasticity. The materials your child's body needs to relax, lengthen, and move more freely? They exist. They work. And this page will put them in your hands today.
Episode F-573
Motor Development Series
Age 0–12 yrs
You Are Among Millions of Families Navigating This
High muscle tone — hypertonia — is one of the most common motor challenges in pediatric neurological and developmental conditions. It presents in cerebral palsy (spastic type, affecting 75–80% of CP cases), traumatic brain injury, genetic syndromes, and as a standalone neurodevelopmental variant. In India, an estimated 40,000 children are born with cerebral palsy annually. Globally, the WHO estimates 17 million children live with CP-related hypertonia. Yet fewer than 30% of affected families in LMICs have access to structured home programs.
17–35%
Elevated Tone in ASD & Dev. Disorders
of children with ASD or developmental disorders show elevated muscle tone
1/500
Live Births Affected by CP
Cerebral palsy is the most common cause of pediatric hypertonia worldwide
70%
Show Meaningful Improvement
of children with hypertonia show functional improvement with consistent intervention
"You are among millions of families navigating this exact challenge. You are not alone — and you do not have to figure this out without a map."
The Neuroscience of Tight Muscles — In Plain English
The Science
Upper Motor Neuron System: Brain → Spinal Cord → Muscle. In normal state, the brain sends balanced signals — "contract" AND "relax." In hypertonia, inhibitory pathways are disrupted. The brain continues sending "contract" signals without sufficient "relax" countervailing signals. Result: muscles remain contracted even when the child isn't trying to move.
The Stretch Reflex Loop: When a hypertonic muscle is stretched (e.g., you bend their knee), sensory receptors fire → signal travels to spinal cord → motor signal says "contract harder" → the resistance you feel in the limb.
Parent Translation
🔴What you feel: Resistance when bending their limb — like the muscle is pushing back
🔴What it looks like: Stiff gait, toe walking, scissoring legs, fisted hands, arms held close to body
🔴Why it happens: A wiring difference in the pathways between brain and muscle — not stubbornness, not pain, not behavior
🟢What can change it: Materials that activate relaxation responses, sustained stretching that lengthens shortened muscle fibers, and positioning that prevents further tightening
"This is a wiring difference. Not a behavior choice. Not a parenting failure. A neurological reality that responds to the right intervention."

Your Child's Developmental Trajectory — And Where High Tone Fits
High muscle tone typically becomes apparent in the first year of life as motor milestones begin diverging from expected timelines. Children with hypertonia often achieve milestones later, in modified forms, or with compensation strategies. Your child is at a waypoint — not a dead end.
Birth–3 Months
Head control begins; hypertonia may first be noticed in limb resistance during handling
3–6 Months
Push-up on arms; tone divergence often becomes visible — stiff legs, fisted hands
6–18 Months
Sitting and standing milestones delayed or modified; most common diagnosis window
18 Months–3 Years
Walking with support; toe walking and scissoring gait common; AFOs often prescribed
3–8 Years
Skilled motor development; intensive intervention period for functional independence
80% of children with hypertonia have at least one co-occurring developmental condition — including CP, epilepsy, visual/hearing differences, or communication differences — requiring integrated multi-disciplinary management.

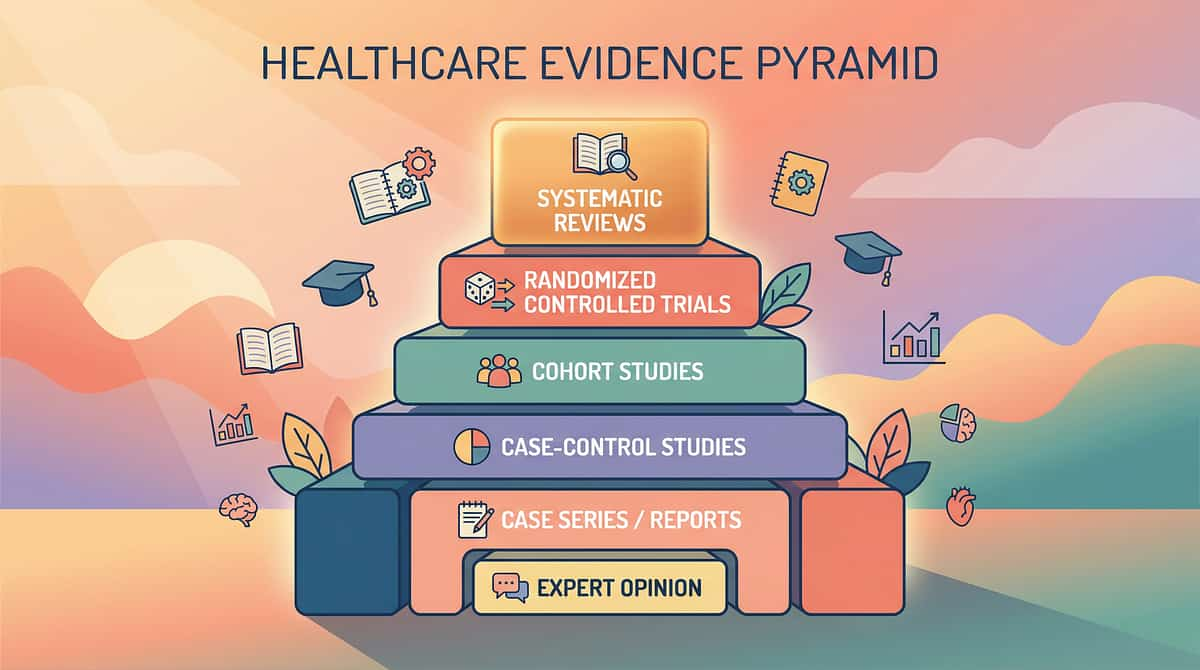
Clinically Validated. Home-Applicable. Parent-Proven.
The materials on this page are not accessories. They are tools validated by systematic research, pediatric neurology, occupational therapy science, and two decades of Pinnacle Blooms consortium clinical experience across 20 million+ therapy sessions.
AACPDM Systematic Review (2023)
Physical therapy + positioning interventions reduce spasticity and maintain ROM in children with CP. Evidence Grade: Level I–II
Cochrane Review: Stretching in CP
Sustained stretching prevents contracture progression; home programs show comparable efficacy to clinic programs.
Hydrotherapy RCT (Pediatric PT, 2022)
Warm water therapy reduces spasticity scores by 23% after an 8-week protocol in children aged 2–8 years.
Indian Pediatric Home Program Study
Home-based PT programs with parent training achieve 78% of clinic outcomes at 20% of the cost. DOI:10.1007/s12098-018-2747-4
Evidence confidence: ████████████████░░ 90% | PMC11506176 | PMC10955541 | PMC9978394 | WHO NCF 2018

Domain F — Motor Development
Physical Therapy Materials
9 Materials That Help With High Muscle Tone
Parent-Friendly Alias: The Tight Muscle Toolkit
High muscle tone management through evidence-based material intervention is a multimodal home-based approach combining vestibular input, sustained stretching, therapeutic positioning, orthotic support, and sensory regulation tools to reduce spasticity, maintain muscle length, prevent contracture, and maximize functional movement in children with hypertonia across all etiologies.
This is a curated set of 9 clinically validated materials — from therapy balls to standing frames — that a parent can systematically deploy at home to extend and amplify the benefits of professional physical therapy. Not a replacement for clinical care. An essential daily complement to it.
Domain
F — Motor Development
Category
Physical Therapy Materials
Age Range
0–12 years
Frequency
Daily
Setting
Home + Clinic
5 Disciplines. One Integrated Approach.
The brain doesn't organize by therapy type. Tight muscles affect how your child sits, communicates, learns, feeds, and plays. Every discipline at Pinnacle addresses them differently — and together.
Pediatric Occupational Therapist
Uses therapy putty, weighted blankets, vibration tools, and positioning systems to address upper extremity function, self-care, and sensory regulation alongside tone management.
Pediatric Physical Therapist
Prescribes and supervises the full 9-material toolkit — therapy ball protocols, stretch straps, AFOs, standing frames. Core discipline for whole-body tone and mobility.
NeuroDevelopmental Pediatrician
Diagnoses hypertonia etiology (CP, TBI, genetic), prescribes orthotics and equipment, monitors for progressive changes, and coordinates medical tone management.
Orthotist
Custom-fits AFOs, splints, and orthotic devices. Essential team member for any child requiring prescribed positioning equipment.
Special Educator
Ensures therapeutic positioning is maintained during school activities; coordinates standing frame use during academic tasks; integrates tone management into learning environments.
Precision Tools for Precise Outcomes
These 9 materials are not general wellness products. Each one addresses a specific target in the cascade from neurological tone reduction to long-term developmental independence.
🎯 Primary
Reduce spasticity · Maintain ROM · Enable movement
Secondary
Prevent contracture · Bone density · Gait quality · Reduce pain
Tertiary
Independence · Play access · School participation · Quality of life

Your High Muscle Tone Toolkit — 9 Materials That Make the Difference
The following materials are organized by therapeutic category. Your child's therapist will guide which are most essential for your child's specific pattern of hypertonia. Materials ①③④⑥⑧ are excellent home-starter items. Materials ⑤⑦ require professional prescription. Material ⑨ costs nothing and works immediately.
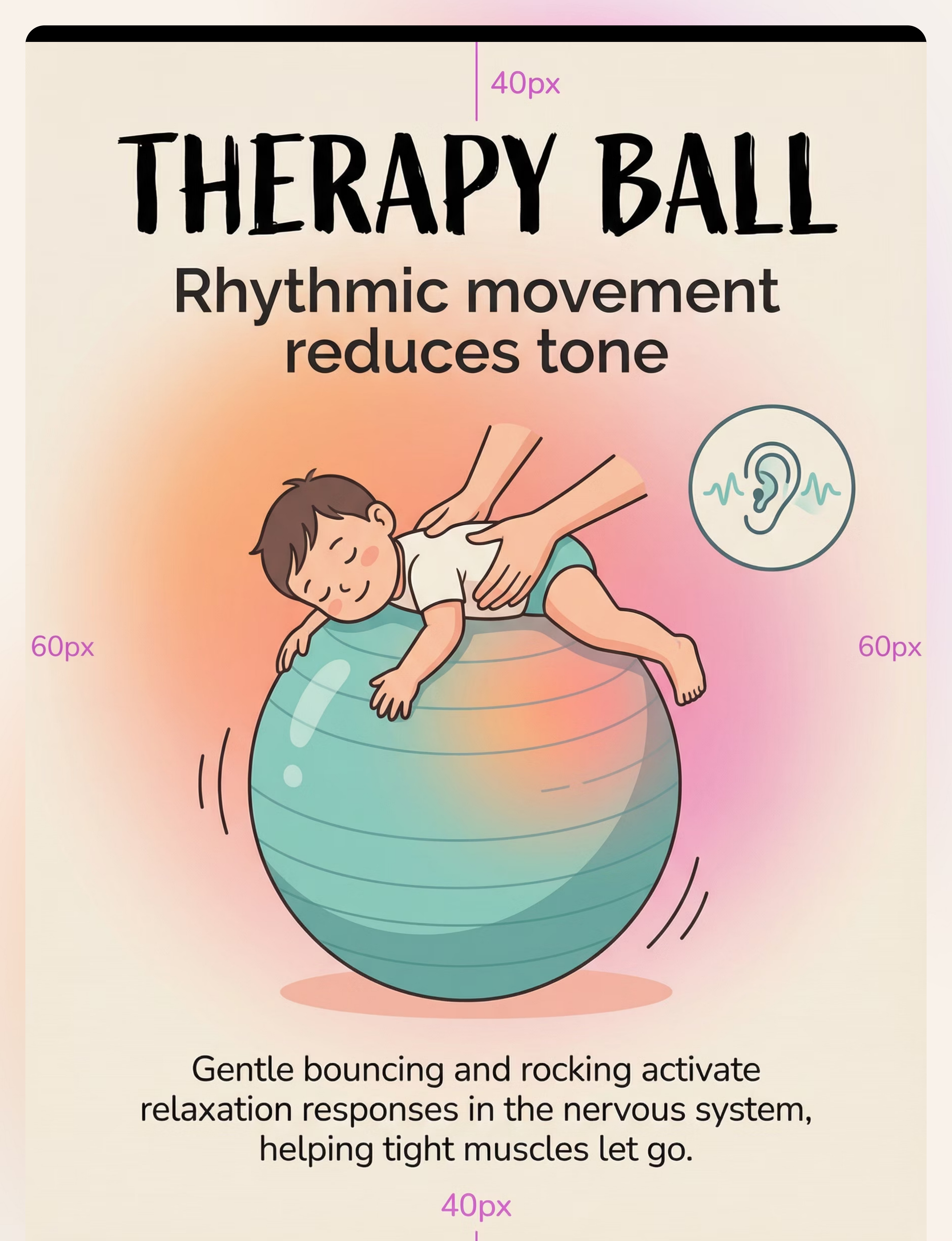
Therapy Ball (Swiss / Physio Ball)
Category: Tone Reduction | Vestibular input → nervous system relaxation → tone reduction. Price: ₹500–2,000. 🛒 Amazon.in: Therapy Ball for Kids 45cm | Lead: PT + OT
Vibration Therapy Tool
Category: Tone Reduction | Sensory input to muscle belly → inhibits excessive contraction. Price: ₹800–4,000. 🛒 Amazon.in: Handheld Vibration Massager | Lead: PT + OT
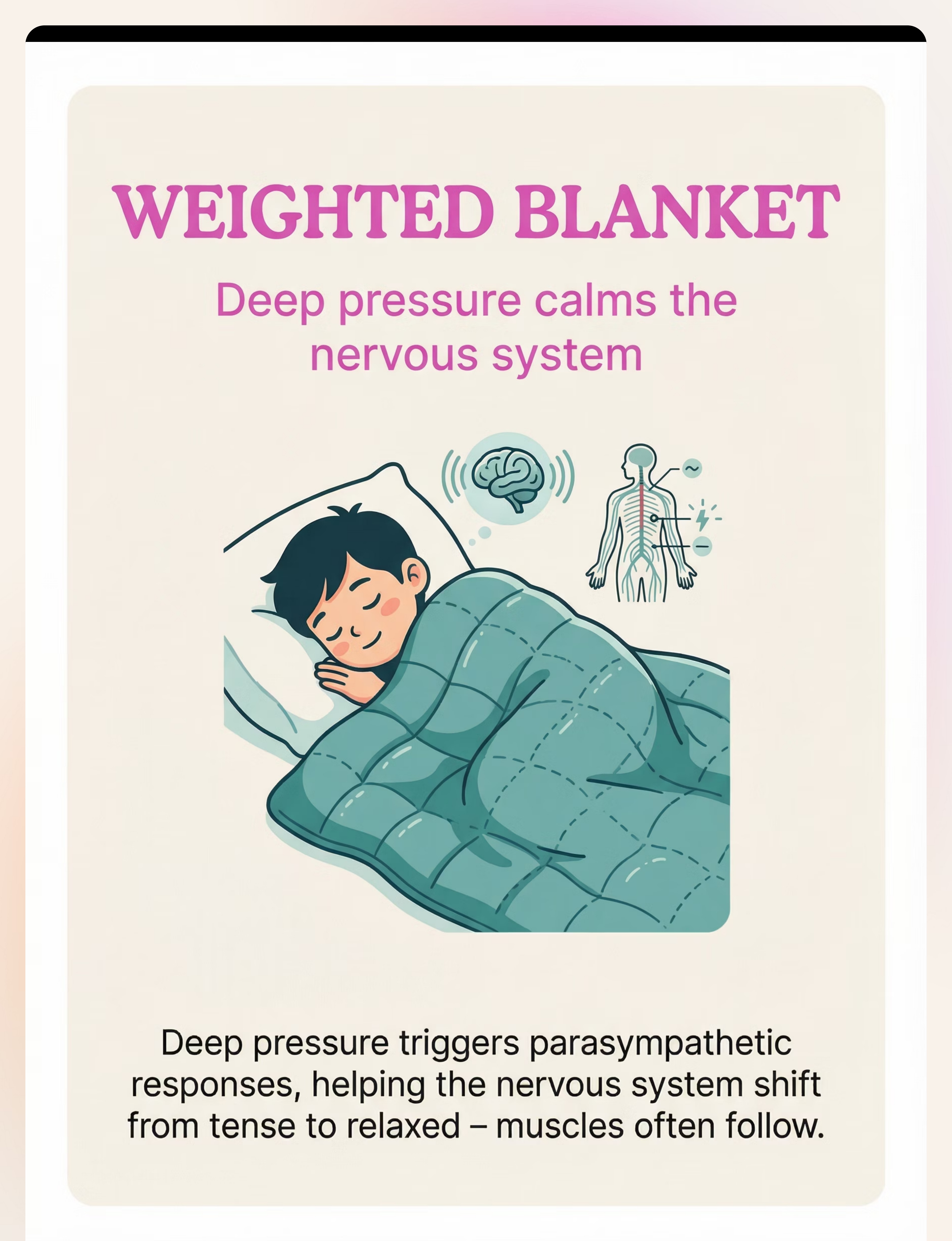
Weighted Blanket (Deep Pressure)
Category: Tone Reduction | Parasympathetic activation → whole-body tone reduction. Price: ₹1,500–5,000. 🛒 Amazon.in: Weighted Blanket Kids | Lead: OT
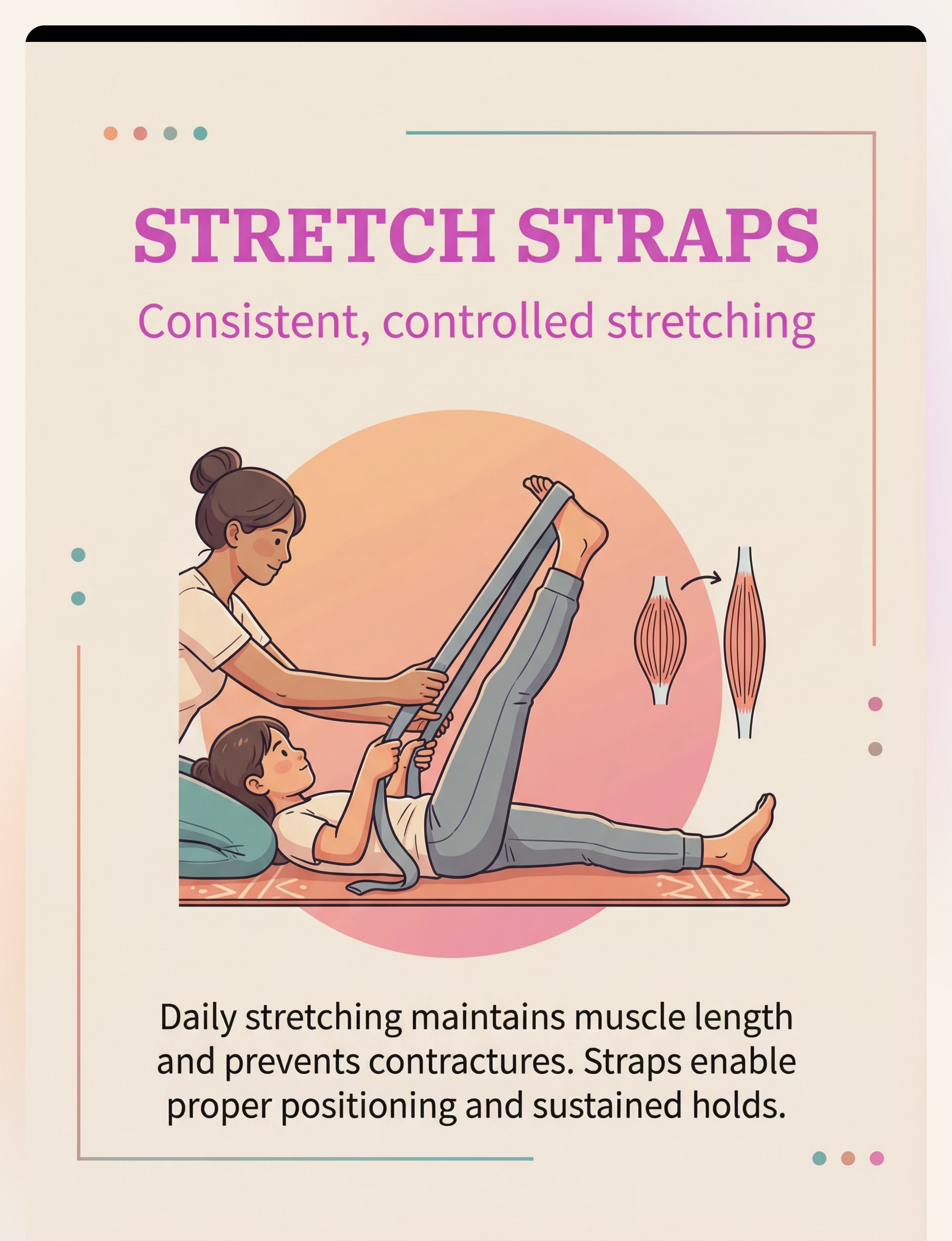
Stretch Straps / Stretching Aids
Category: Stretching & Maintenance | Controlled sustained stretching → maintains muscle length. Price: ₹300–1,000. 🛒 Amazon.in: Stretch Strap with Loops | Lead: PT
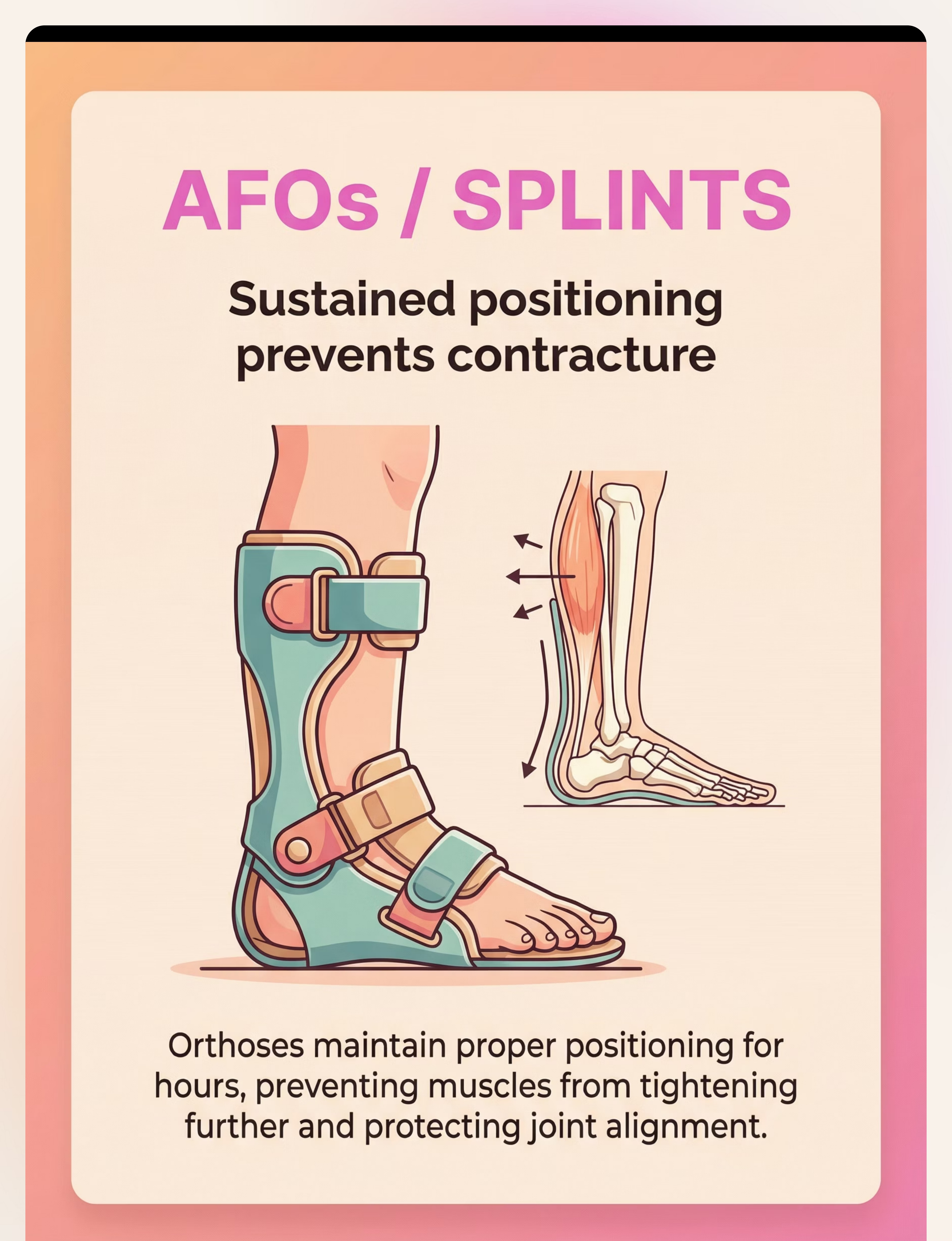
Ankle-Foot Orthoses (AFOs) / Splints
Category: Stretching & Maintenance | Sustained positioning → prevents contracture, corrects alignment. Price: ₹2,000–15,000+. Requires prescription from PT/Orthotist. | Lead: PT + Orthotist
Positioning Wedges and Rolls
Category: Positioning | Therapeutic positioning during play/rest → passive stretching all day. Price: ₹500–2,500. 🛒 Amazon.in: Therapy Positioning Wedge Foam | Lead: PT + OT
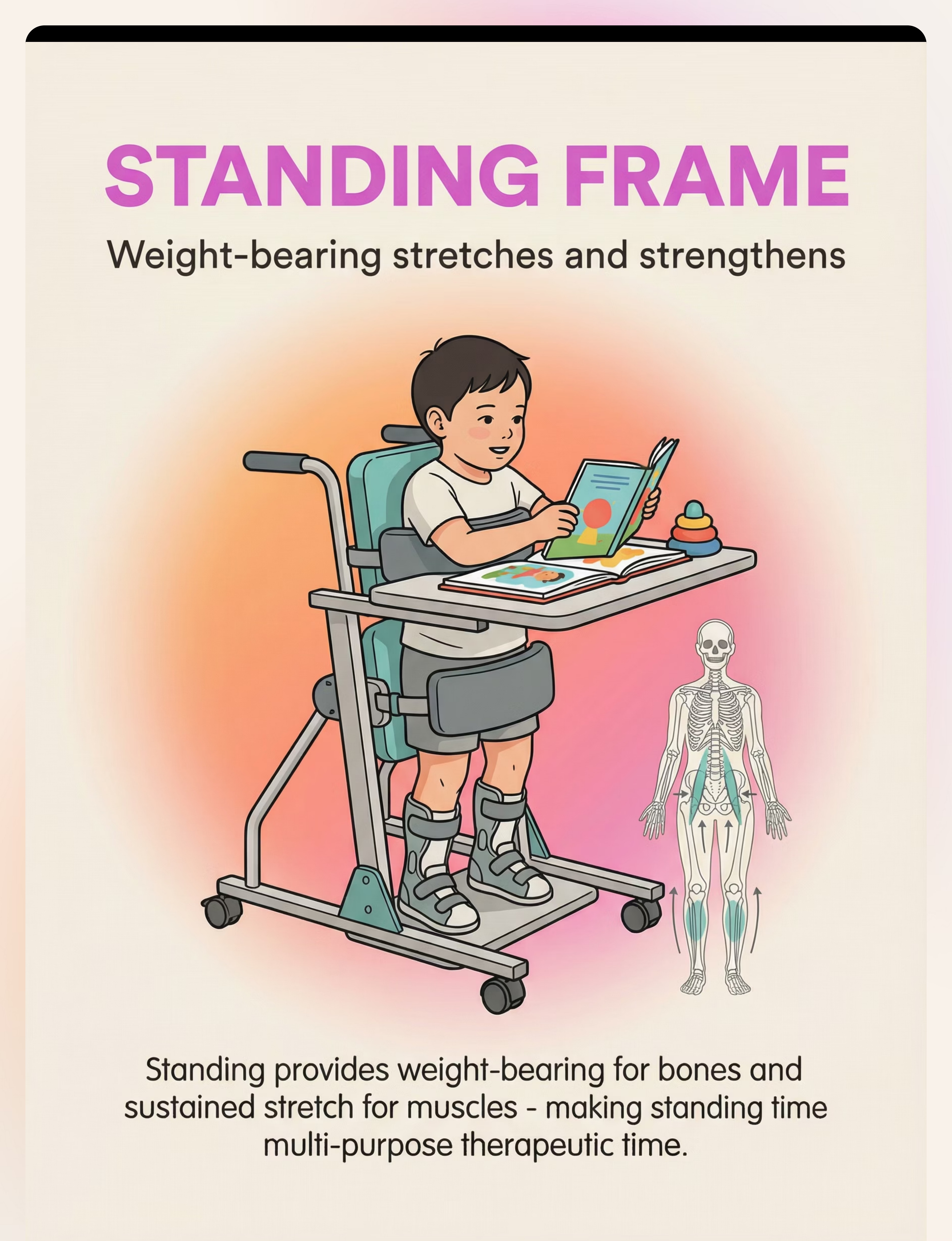
Standing Frame / Stander
Category: Positioning | Weight-bearing + sustained stretch → bone health + tone management. Price: ₹10,000–50,000+. Requires prescription; often insurance/scheme-funded. | Lead: PT
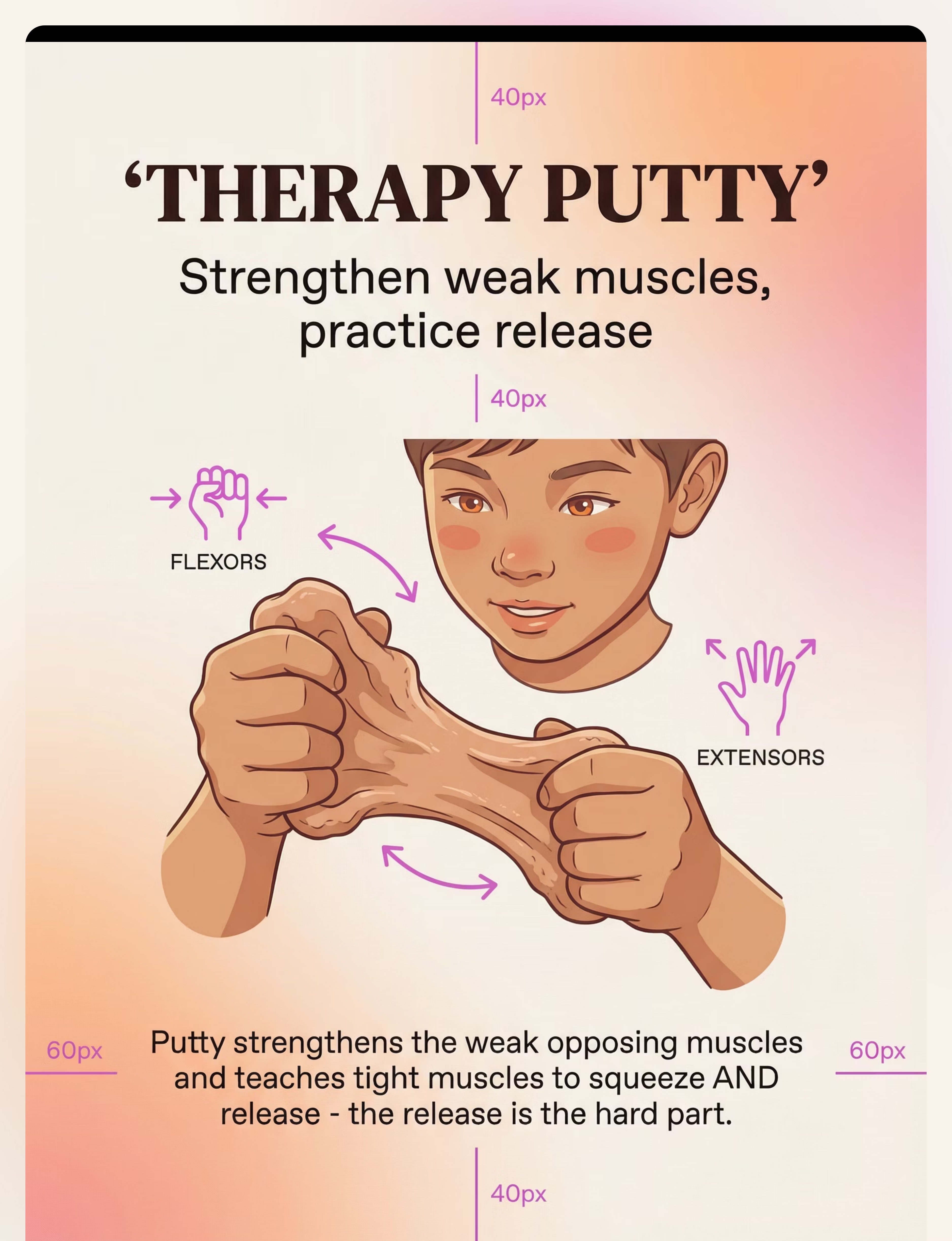
Therapy Putty / Resistance Putty
Category: Functional Strengthening | Strengthens opposing muscles → balance around hypertonic joints. Price: ₹200–800. 🛒 Amazon.in: Therapy Putty Hand Exercise | Lead: OT
Warm Water Access (Bath / Hydrotherapy)
Category: Thermal/Hydrotherapy | Heat + buoyancy + pressure → most effective natural tone-reducer. Price: ₹0 (home bath) to ₹500/session (hydrotherapy pool). Lead: PT
Every Family Can Start Today — Regardless of Budget
The WHO/UNICEF principle of equity-focused intervention means no child should be denied effective therapy because of economics. Every material on this page has a zero-cost equivalent. "The muscle does not know the price of the tool — it responds to the input." — Pinnacle Blooms Consortium
Buy This | Price | Make/Use This (₹0) | Why It Works Equally | |
Therapy Ball | ₹500–2,000 | Large beach ball (partially deflated) or firm sofa cushion | Same vestibular input from rhythmic movement | |
Stretch Strap | ₹300–1,000 | Rolled bed sheet or dupatta tied in loops | Same sustained gentle pull for stretching | |
Positioning Wedge | ₹500–2,500 | Firm pillow or rolled towels under hips | Same hip flexor elongation during prone play | |
Therapy Putty | ₹200–800 | Kneaded atta (wheat dough) with ghee for texture | Same squeeze-and-release resistance training | |
Weighted Blanket | ₹1,500–5,000 | Layers of cotton blankets sewn together | Same deep pressure mechanism | |
Vibration Tool | ₹800–4,000 | Electric toothbrush on muscle belly | Same sensory receptor activation | |
Warm Water | ₹0–500/session | Home bathtub at 33–36°C (use kitchen thermometer) | Identical thermal + buoyancy mechanism | |
AFOs/Splints | ₹2,000–15,000 | No DIY substitute — professional fitting essential | Orthotic devices require precision fit | |
Standing Frame | ₹10,000–50,000 | Child supported standing at table/wall with caregiver | Same weight-bearing and stretch principles |

Clinical Safety Gates — Read Before Every Session
Every session begins with a safety assessment. These are non-negotiable thresholds that protect your child's safety and the therapeutic relationship.
🔴 DO NOT PROCEED IF:
Child has fever above 38°C · Recent fracture or unhealed wound in treatment area · Child severely distressed or non-regulated · New asymmetry in tone or sudden significant stiffness increase · AFO/splint fit is questionable with skin redness or pressure marks
🟡 MODIFY SESSION IF:
Child slept poorly or is overtired · Child is hungry or just fed (wait 30 min post-feed) · Child showing mild anxiety · Tone higher than usual (warm water → vibration → stretching sequence mandatory) · Growth spurt phase (joints more vulnerable)
🟢 OPTIMAL CONDITIONS:
Child is rested and fed 30–60 min prior · Environment is warm, quiet, predictable · Materials are clean and ready · Caregiver is calm — tone in parent's body transmits to child · Session time is consistent
🛑 ABSOLUTE STOP SIGNS: Child cries in pain | Skin turns red or white under strap/orthotic | Child stops breathing normally | Sudden increase in resistance compared to yesterday | Child vomits or shows dizziness. Stop immediately and assess.
Material-Specific Safety: Therapy Ball: properly inflated, non-slip, NEVER unattended · Stretch Straps: never force past comfortable resistance, NO bouncing · Vibration: not on bony prominences or open skin · Weighted Blanket: 10% body weight maximum, NOT for infants <18 months · Warm Water: 33–36°C ONLY, thermometer mandatory, constant supervision · AFOs: check skin daily, even minor redness = remove and consult · Standing Frame: prescribed parameters only.

Your Home Therapy Space — Configured for Maximum Effectiveness
The environment is not a backdrop — it is a therapeutic tool. An optimally configured space reduces child anxiety, which directly reduces muscle tone before a single stretch is applied.
① Parent Position
Beside child — never towering. Same level when possible. Within arm's reach for support. Never approach from behind.
② Child Zone
Padded mat or carpet. Non-slip. Minimum 2m × 2m clear space. No furniture edges nearby.
③ Therapy Ball
Off to the side of the mat — child can transition to it. Properly inflated and stable before session begins.
④ Materials Station
Within parent's reach, out of child's unsupervised access. Stretch straps ready, putty out, vibration tool charged.
⑤ Environment Settings
Temperature: 24–27°C · Soft warm lighting (avoid fluorescent) · Quiet background music or silence · Tablets, phones, and distractors removed
Warm-Up Mandate: Every session begins with 5–10 minutes of warm bath OR warm compress on target muscles before active stretching. Cold muscles should never be stretched forcefully.

60-Second Pre-Session Readiness Check
"The best therapy session is the one that starts right. A session abandoned at readiness check protects trust, prevents negative associations, and saves the relationship for tomorrow."
# | Check | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
1 | Last meal? | 30–90 min ago | Under 30 min | Actively feeding | |
2 | Sleep? | Well-rested | Slightly tired | Exhausted or just woke | |
3 | Mood / Regulation? | Calm or mildly playful | Mildly unsettled | Distressed or dysregulated | |
4 | Pain signals? | None visible | Possible — monitor | Evident (crying, guarding) | |
5 | Illness? | None | Mild (modify intensity) | Fever or unwell | |
6 | Tone today? | Baseline level | Slightly higher | Notably higher than usual | |
7 | Time available? | 20–45 min uninterrupted | 10–20 min | Under 10 min |
ALL GREEN ✅
Proceed with full protocol
ANY AMBER ⚠️
Warm bath + gentle vestibular input only. No active stretching.
ANY RED 🛑
Postpone session. Offer alternative calming activity. This is NOT failure — it is data.

Step 1 of 6
Duration: 1–2 minutes
▶ Step 1: Invite, Don't Command
The Opening Script
"Hey [child's name], I have your special ball ready. Want to come see?"
For non-verbal children: Show the therapy ball at child's eye level. Hold it. Roll it gently. Wait for eye contact or movement toward it. That IS the invitation acceptance.
Parent Body Language
Kneel or sit to child's level · Face relaxed, voice soft and warm · Slow movements (fast movements increase tone) · Let them come to the material; do not carry them to it if possible
Acceptance Signals to Look For
✅ Eye contact with material · Movement toward it · Reaching · Vocalisation of interest · Reduced body stiffness · Relaxed facial expression
Resistance Signals & Response
Mild turning away: Move material slightly closer. Wait 15 seconds. Try again. Active pushing away: Don't force. Bring out a preferred comfort object. Try again in 5 minutes. Increased stiffness: Signal of anxiety. Back off. Use deep pressure (weighted blanket) instead today.
Timing: 30–90 seconds. If no acceptance in 90 seconds — go to modification protocol.

Step 2 of 6
Duration: 3–5 minutes
▶ Step 2: Warm the Muscles, Engage the Nervous System
The warm-up is not optional. It is the mechanism. A warm, slightly relaxed nervous system allows the stretch reflex to work with you, not against you. Choose ONE of the following options:
Option A — Warm Bath Pre-Session (IDEAL)
Soak in 33–36°C water for 10 minutes. Parent performs gentle passive range-of-motion movements in water. Exit, towel dry, move IMMEDIATELY to therapy space while muscles are still warm.
Option B — Warm Compress
Apply warm (not hot) moist towels to target muscles for 5 minutes. Calves, hamstrings, hip flexors, or forearms — wherever tone is highest.
Option C — Vestibular Warm-Up on Therapy Ball
Child sits or drapes over ball with parent support. 2–3 minutes of slow, rhythmic rocking (front to back, side to side). Watch for visible muscle softening — abdomen relaxes, arms drop slightly, jaw unclenches.
Engagement deepening: Maintain gentle physical contact (hand on back or hip) — proprioceptive input enhances safety and tone reduction. Match child's rhythm. Simple narration: "We're doing our stretchy time. It helps your muscles feel better."

Step 3 of 6
Duration: 8–15 minutes
▶ Step 3: The Core Therapeutic Work
This is the active ingredient of the session. The specific actions depend on your child's profile and which materials your therapist has prioritized.
Action A — Tone Reduction (Therapy Ball)
Prone drape: Child tummy-down over ball, arms hanging. Gentle forward-back rolling 2 min. Passively stretches hip flexors while vestibular input reduces CNS drive to muscles. Sitting bounce: Child sits on ball. Rhythmic gentle bouncing (1 per second) for 2 min. Reduces lower extremity tone. Supine over ball: Child lies back over ball (supported). Opens chest, stretches trunk flexors, calms nervous system.
Action B — Sustained Stretching (Stretch Strap)
After tone reduction only — never before.Hamstring: Child supine. Strap around foot. Raise leg to mild resistance. HOLD 30–60 seconds. Calf/Achilles: Strap around forefoot. Gentle pull toward body. HOLD 45–60 seconds. Hip flexor: Child prone, strap around ankle. Gentle knee bend. HOLD 30 seconds. Critical: feel for gradual release (muscle lengthening). Never force past resistance.
Action C — Functional Strengthening (Putty)
For upper extremity hypertonia: Squeeze 5 times · Flatten with open palm · Pull apart with both hands · Roll into ball between palms. Focus on the RELEASE equally with the squeeze — 5–8 minutes. The release is the hard part for hypertonic hands.
Common Execution Errors: Stretching cold muscles · Forcing range past resistance · Session that's too long (quality > quantity) · Forgetting the release in putty activities
Step 4 of 6
Duration: 3–5 minutes
▶ Step 4: Repetition Is the Dose — Variation Keeps the Door Open
"3 quality repetitions > 10 forced repetitions. A muscle stretched to comfort and released is physiologically better served than one forced to the point of protective spasm."
Material / Action | Target Reps | Signs to Stop | |
Therapy ball sequences | 2–3 sequences per session | Child loses tolerance, stiffens | |
Each stretch (with strap) | 2–3 holds per muscle group | Child shows pain indicators | |
Positioning (wedge/roll) | Hold 15–30 min during play | Child becomes restless or distressed | |
Putty exercises | 8–10 reps per exercise | Fatigue visible in hand coordination | |
Standing frame | Per prescription (20–60 min) | Prescribed limit or fatigue |
Variation options to maintain engagement: Add music to match rocking rhythm · Child holds a favourite toy during prone drape · Parent narrates stretching like a story · Hide small objects in putty to find · Change child's position session to session (supine → sidelying → sitting).
Satiation indicators (stop here): Increased resistance to touch · Looking away repeatedly · Increased vocalization of displeasure · Rigidity returning despite tone reduction efforts

Step 5 of 6
Duration: 1–2 minutes
▶ Step 5: The Reinforcement Window — 3 Seconds Matters
Reinforcement delivered within 3 seconds of the desired behavior increases future occurrence of that behavior. For hypertonia management, the "desired behavior" includes TOLERATING the session, ACCEPTING the material, and REMAINING REGULATED throughout.
Immediate (During)
Verbal praise: specific and enthusiastic · High-five or preferred touch · Preferred object during session · Singing preferred song
End-of-Session
Preferred snack (if appropriate) · 5 min preferred screen time · Choice of next activity · Preferred sensory activity
Long-Term
Star chart / sticker board · Weekly celebration ritual · Monthly milestone reward · Family celebration
Reinforcement Scripts:"You did it! You let your muscles stretch — that's so strong." · "That's your body getting stronger. I'm so proud." · "All done! You were amazing. Let's pick your reward."
"Celebrate the attempt, not just the success. A child who allowed the stretch for 5 seconds this week and 8 seconds next week is succeeding. That IS the data."

Step 6 of 6
Duration: 2–3 minutes
▶ Step 6: Close the Session — No Abrupt Endings
An abrupt session end can spike anxiety, which immediately increases muscle tone. A structured cool-down maintains the tone-reduction achieved during the session and prevents "rebound tightening" when the nervous system suddenly loses its regulated state.
① Transition Warning
30 seconds before end: "Two more rocks, then all done." Use visual timer if child benefits from visual supports.
② Calming Sensory Activity
Weighted blanket (2 min) · OR deep pressure parent hug (10–15 sec) · OR rocking in arms · OR quiet vibration on hands if tolerated
③ Material Put-Away Ritual
"Help me put the ball away." Child participates if able — ownership of the ritual reduces resistance to ending.
④ Transition Cue
"All done with therapy. Now we're going to [next predictable activity]." Visual schedule pointing to next activity if used.
⑤ Post-Session Note
While child transitions, parent quickly notes one observation on the tracking card. 60 seconds of data now saves hours of guessing later.

60 Seconds of Data Now = Better Therapy Tomorrow
Your session observations are not just personal records — they are clinical data that refines your child's program, informs your therapist consultations, and feeds GPT-OS® to improve future recommendations.
Track These 3 Things Every Session
Today's Date: ___________ Material Used: ___________
Tolerance Score: 1 = Refused entirely 2 = Tolerated briefly (<2 min) 3 = Tolerated full session with some resistance 4 = Engaged well 5 = Requested more / clearly enjoyed
Tone Observation: □ No visible change □ Slight reduction during session □ Clear reduction (movement easier at end) □ Significant reduction (best session yet)
One thing that worked today: ___________
Why This Data Matters
Tolerance score trends show whether materials are becoming more accepted over time. Tone observations reveal which sequences are most effective for YOUR child specifically. Your data feeds GPT-OS® to refine recommendations.
Brings concrete evidence to therapist consultations: "She scored 4 on tolerance in 6 of the last 8 sessions."
Reality Check: Sessions Don't Always Go as Planned — Here's the Fix
These are the 7 most common challenges reported by parents in Pinnacle's network. Each has a specific, clinically grounded resolution. "Session abandonment is not failure — it's data."
Problem 1: Child refuses the therapy ball / immediately stiffens
Why: Ball may be new stimulus; anxiety increases tone. Fix: Don't start with the ball. Start with warm bath. Introduce ball NEXT to play area without requiring interaction. Over 3–5 sessions, allow gradual proximity paired with a preferred object.
Problem 2: Stretching achieves no range — muscle feels like concrete
Why: Muscle was too hypertonic / not warmed up enough. Fix: Mandatory warm bath or 5-min warm compress BEFORE stretch. Add vibration to muscle belly for 60 seconds, THEN attempt stretch at first resistance, not beyond.
Problem 3: Child cries during stretching
Why: May be fear (anticipatory), genuine pain, or too-high intensity. Fix: Stop. Assess: "I don't like this" (modify) vs. "this hurts" (stop immediately). For fear: slow entry, warm bath, narration, preferred toy during stretch.
Problem 4: Tone returns to baseline within 30 minutes
Why: Expected — single-session tone reduction is transient. Daily consistency is the mechanism for cumulative change. Fix: Increase to 2× daily if possible. Maintain therapeutic positioning (wedge/AFO) post-session to preserve gains.
Problem 5: Standing frame — child refuses / is distressed
Why: Discomfort from improper fit or duration too long. Fix: Check fit with prescribing team. Start with 10 min, increase by 5 min per week. CRITICAL: standing time must have engaging activity — tablet, books, sensory play at tray level.
Problem 6: Child can't open hand to release the putty
Why: This IS the challenge — finger/wrist flexors are hypertonic. Release is harder than grip. Fix: Warmth first. Vibration to forearm flexors. Start with softest putty. Gently assist the release. Celebrate ANY extension at all.
Problem 7: No visible progress after 3 weeks
Why: 3 weeks may be insufficient; or progress is happening in dimensions not yet measured. Fix: Review tracking data for tolerance trends. Are sessions daily or sporadic? Consistency is the #1 predictor. Contact Pinnacle helpline: 9100 181 181 for teleconsultation.

Your Child Is Unique. Your Protocol Should Be Too.
The same 9 materials serve very different children when applied through the lens of individual sensory profiles, age, and co-occurring conditions. Here is how to adapt the protocol — always in consultation with your therapist.
High Sensory Sensitivity (common in ASD + hypertonia)
Reduce vibration intensity or skip entirely · Use warm compress over vibration tool · Always narrate before contact · Focus on weighted blanket as primary tone-reducer · Shorter sessions (10 min) more frequently (3× daily)
High Sensory Seeking (craves input)
More vigorous therapy ball activities · Deeper pressure input · Longer stretches (child may enjoy the sensation) · Incorporate proprioceptive activities: carrying, pushing, pulling heavy objects
Younger Children (0–3 years)
All activities are play-based and caregiver-interactive · No formal "session" — therapeutic input embedded in daily care routines · Positioning during feeding, nappy change, bath time = therapy time
Older Children (8–12 years)
Child learns self-stretch techniques with strap · Independent putty activities · Standing frame integrated into homework time · Building toward independent tone management skills
Age | Primary Focus | Key Materials | |
0–12 months | Positioning + gentle handling | Wedges, rolls, warm bath | |
1–3 years | Vestibular + positioning + warmth | Therapy ball, warm bath, weighted blanket | |
3–6 years | Full toolkit + standing | All 9 materials per prescriber | |
6–12 years | Self-management + maintenance | Stretch strap, putty, standing frame |
Progress Arc
Weeks 1–2
The First 2 Weeks: Trust the Process Before You See the Progress
"In weeks 1–2, progress lives in seconds. Your child tolerating the ball for 10 seconds instead of 3 seconds — that is a neurological event. The nervous system is beginning to recategorize this stimulus from 'threat' to 'familiar.' This is how tone management begins."
✅ What You WILL Likely See
Child tolerates materials for slightly longer than Day 1 · Session routines begin to feel predictable · 1–2 instances of clearly visible muscle softening during ball work · Slight reduction in resistance during one specific stretch · YOU feel more confident in your technique
❌ What You Will NOT Yet See (and that's normal)
Sustained range-of-motion improvement · Changed functional movement in daily life · Reduction in tone outside of session times · Independent participation with materials
Tracking Target: Tolerance score trending upward — even 1–2 points over 2 weeks — means you are on course.

Progress Arc
Weeks 3–4
Weeks 3–4: The Neural Pathway Is Forming
What you are witnessing in Weeks 3–4 is not habit. It is neuroplasticity. The repeated sensory input from therapy ball, sustained stretch, and therapeutic positioning is measurably altering muscle spindle sensitivity and corticospinal inhibitory signaling. The brain is adapting.
Child begins to ANTICIPATE the therapy ball
May reach for it or show excitement at session start — this is the stretch reflex beginning to recalibrate
Stretching accepted with less resistance
Range of motion during warm relaxed state measurably improved from Week 1 — check with simple video comparison
The session dynamic is now a ROUTINE, not a battle
Child shows preference — may prefer one material or sequence over others — this is clinical information
Your confidence is measurably higher, too
Calmer parent energy DIRECTLY reduces child's muscle tone. That parental confidence is not a side effect — it is part of the treatment mechanism.
When to increase intensity: If child is accepting all materials without resistance → discuss with therapist: increase stretch hold duration, introduce harder putty resistance, increase standing frame time by 5 min.
Progress Arc
Weeks 5–8
Weeks 5–8: Measurable Change Arrives
This is the phase where the work you've put in becomes visible — to you, to your therapist, and to your child's teachers and caregivers. Document everything now; this data is powerful advocacy material.
Therapy Ball Mastery ✓
Child actively seeks out ball at session start · Tolerates 10+ minutes of prone/sitting ball activities · Palpable tone reduction maintained for 30+ minutes post-session
Stretching Mastery ✓
ROM improved ≥10° in primary hypertonic muscle groups (measured by therapist) · Child cooperates with stretch routine without resistance · No contracture progression in monitored joints
Standing / AFOs Mastery ✓
Prescribed standing duration achieved without distress · Heel contact improving during supported standing · AFO wear compliance ≥80% of prescribed hours
Putty Mastery ✓
Active release of hand after squeeze (consistent) · Can flatten putty with open palm without prompting
Generalization Indicators — skills appearing OUTSIDE sessions: Dressing easier — fewer battles with sleeves and pants · Bath time shows more relaxed limb movement · Child positions themselves in functional ways spontaneously · School reports improved sitting posture
You Did This. Let That Land.
Your child's muscles were fighting movement. You introduced 9 materials, built a daily routine, survived the hard early weeks, and stayed consistent. The nervous system of a child with hypertonia began to recalibrate — because of your daily presence, your steady hands, your refusal to give up.
Spasticity Yielding
Tone that resisted every stretch now yields to sustained input
Muscle Length Maintained
Muscles that shortened daily are being maintained in functional length
Contracture Stabilized
Contracture that was progressing has stabilized or reversed
The Ball Is Now Welcomed
A child who cried at the therapy ball now reaches for it
"Describe the single moment in the last 8 weeks where you saw your child's body relax and move freely. Write it down before you forget it. That moment is what the science predicted. You made it real."

Trust Your Instincts — These Signs Mean Stop and Seek Help
After weeks of daily sessions, you know your child's baseline better than anyone. When something feels not just hard, but wrong — trust that instinct. It has clinical value.
Red Flag | What It Looks Like | Why It Matters | What To Do | |
Sudden significant increase in tone | Limb much stiffer than baseline; new clonus (rhythmic involuntary jerking) | May indicate pain, illness, UTI, or neurological change | Call physician TODAY. Do not continue stretching. | |
Skin breakdown under AFO/splint | Redness that doesn't fade within 20 min after removal; blistering | Pressure injury risk — can become serious rapidly | Remove device. Call orthotist/prescriber. | |
New asymmetry | One limb suddenly more affected; child protecting one side | May indicate hip subluxation, joint issue, or new neurological event | Clinic visit within 48 hours | |
Rapid loss of range of motion | Joint improving, now declining week-over-week despite consistent intervention | Early contracture — window to intervene without surgery is time-limited | Urgent PT appointment | |
Pain during previously tolerated activity | Child consistently distressed despite warm-up | May signal growth-related muscle-bone length discrepancy | Reduce intensity; notify therapist | |
Regression after illness | Post-fever tone significantly higher than pre-illness baseline | Expected but may need brief medical management if persistent >2 weeks | Teleconsult with Pinnacle team |
Escalation Pathway: Home observation → Teleconsult (9100 181 181) → Clinic visit → Specialist referral
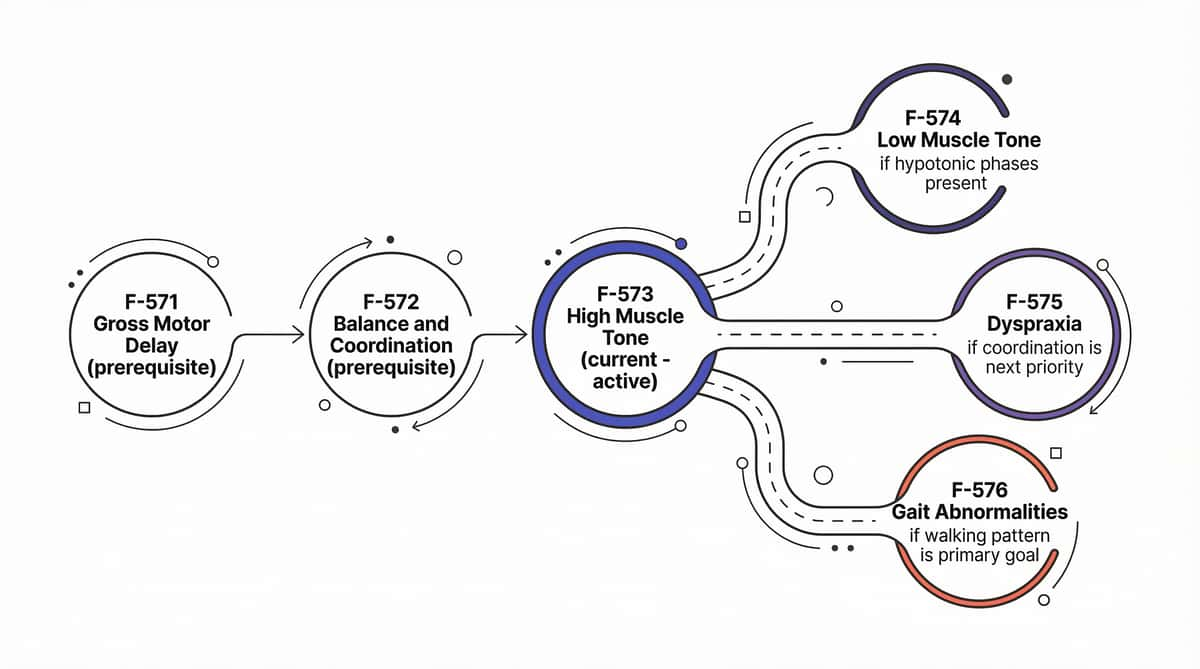
You Are Here. Here Is Where Evidence Is Taking You.
F-573 is one node in a carefully sequenced domain of motor development techniques. Each technique in the F-series builds on or complements the others — sharing materials, skills, and the therapeutic relationship you've already built.
Prerequisites (should be in place)
✅ Basic therapeutic positioning established ✅ Readiness assessment routine mastered ✅ At least one primary material consistently accepted
Next-Level Options
If tone is primarily reducing → F-576 for walking improvement If contracture remains primary concern → Intensify AFO program; discuss medical tone management with neurologist If upper extremity is primary focus → Advance to OT fine motor E-series
"Every session of hypertonia management at home is an investment in your child's ability to walk, dress, play, write, and participate in their own life with maximum independence."

You Already Know These Materials — Explore What Else They Can Do
The 9 materials in your toolkit don't stop at F-573. Many of the same tools serve different therapeutic goals across the Motor Development domain — no additional investment required.
F-571: Gross Motor Delay Foundations
🟢 Intro Level · Shared materials: Therapy Ball, Positioning Wedge

F-572: Balance & Coordination
🟡 Core Level · Shared materials: Therapy Ball

F-574: Low Muscle Tone (Hypotonia)
🟡 Core Level · Shared materials: Therapy Ball, Positioning

F-575: Dyspraxia Intervention
🟡 Core Level · Shared materials: Therapy Putty

F-576: Gait Correction
🔴 Advanced Level · Shared materials: AFOs, Standing Frame

F-577: Postural Control
🟡 Core Level · Shared materials: Therapy Ball, Wedge
🟦 You already own materials for F-571, F-572, F-574 techniques — explore them next without additional investment.
One Technique. One Domain. One Piece of Your Child's Complete Map.
High muscle tone doesn't live only in the muscles. It shapes how your child communicates (posture affects breath support for speech), regulates emotions (pain and discomfort increase behavioral dysregulation), and participates in daily life. This technique feeds 6 other developmental domains
Domain F — Where You Are Now
F-573: High Muscle Tone ← ACTIVE F-574: Low Muscle Tone F-575: Dyspraxia F-576: Gait F-577: Postural Control
See Your Child's Full Picture
GPT-OS® tracks progress across all 12 developmental domains, updating your child's AbilityScore® profile with each session record you submit.

These Families Were Where You Are. Here Is Where They Went.
Hyderabad | Spastic Diplegia | Age 18 months at start
"His legs were scissors every time we tried to dress him. He walked on his toes. The stiffness was relentless."After 8 months: "He walks with AFOs now. We still do the ball and stretching every morning before school. His hamstrings haven't contracted." Therapist notes: Tolerance for therapy ball progressed from 45 seconds to 18 minutes over 6 weeks. Hamstring ROM improved 22° bilaterally.
Bengaluru | CP Hemiplegia (Right) | Age 4 at start
"Her right hand was always fisted. She couldn't hold a pencil. She hated anyone touching it."After 12 weeks: "She asks for the putty now. Her teacher says she's starting to use her right hand as a support hand. She learned to open her hand. That was the goal. It happened." "We stopped calling it therapy time. We called it putty time. She ran to it."
Chennai | Hypertonia + ASD | Age 2.5 at start
"Every bath was a fight — he would arch his back and his legs would go rigid."After 6 weeks: "Bath time is therapy time now. His legs bend. He's still stiff on land, but in the bath, he moves. That's our window." "Warm water. That's the thing no one told us first. We should have started there."
Outcomes illustrative. Individual results vary by condition, severity, and consistency.

You Don't Have to Figure This Out Alone
Research consistently shows that parents with peer support maintain home programs 3× longer than isolated parents. Your community is not a nice-to-have. It is clinical infrastructure.
WhatsApp Support Groups
High Muscle Tone / CP Parents Group · Motor Development Parents Community · Available in Hindi, Telugu, Tamil, Kannada, English + 12 more languages. Join via 9100 181 181.
Online Forum
Parent discussions, material tips, and therapist Q&A threads at pinnacleblooms.org/community
Peer Mentoring
Connect with a Pinnacle parent who has navigated hypertonia for 2+ years. Request via 9100 181 181 or care@pinnacleblooms.org
Local Parent Meetups
Pinnacle centers host monthly parent education sessions. Find your nearest center →
"Your experience helps others. If these materials have made a difference, your testimony may be what another family needs to begin."

Home + Clinic = Maximum Impact for Your Child
Home-based programs are most effective when designed by a professional and maintained by a parent. The combination delivers what neither can achieve alone. 70+ centers across India | 70+ countries served via teleconsultation.
Your Child's Challenge | Specialist at Pinnacle | Availability | |
Whole-body tone, mobility, gait | Pediatric Physical Therapist | All centers | |
Upper extremity, self-care, sensory | Pediatric Occupational Therapist | All centers | |
Diagnosis, medication, prognosis | NeuroDevelopmental Pediatrician | Select centers + teleconsult | |
AFO/splint prescription & fitting | Orthotist | Select centers + referral | |
Learning, school inclusion | Special Educator | All centers |
📲 Book Teleconsult
pinnacleblooms.org/teleconsult · 16+ languages · Same-day and next-day slots
📞 Free Helpline
9100 181 181 · 24×7 · PT specialist triage available
💰 Insurance/Funding
AFOs & standing frames may be covered under CGHS, Aarogyasri, or corporate insurance. Pinnacle assists with documentation.
The Evidence Behind Every Material on This Page
Deeper reading for the curious parent — and the evidence you need to advocate for your child's access to these materials in medical and school settings.
Study | One-Line Finding | Reference | |
AACPDM Evidence Report (2023) | PT is essential for managing spasticity and preventing contracture in CP | aacpdm.org/publications | |
Cochrane: Stretch for Spasticity | Sustained stretch maintains ROM and prevents contracture progression | Cochrane Library | |
Hydrotherapy RCT (Pediatric PT, 2022) | Warm water therapy reduces Modified Ashworth Scale scores; improves ROM | PubMed: hydrotherapy hypertonia children | |
Weighted Blanket + ANS (AJOT, 2023) | Deep pressure shifts toward parasympathetic state | AJOT 2023 | |
Indian Pediatric Home Programs (2019) | Parent-administered PT: 78% of clinic outcomes, significant improvement | ||
PMC11506176 PRISMA SR (2024) | SI and motor interventions evidence-based for neurodevelopmental populations | ||
PMC10955541 Meta-analysis | Motor + sensory interventions effective across 24 studies |
WHO/UNICEF Publications:WHO Nurturing Care Framework (2018) · UNICEF CCD Implementation Guide (2023) · WHO Care for Child Development Package

Your Session Data Is Not Just a Record. It's a Recommendation Engine.
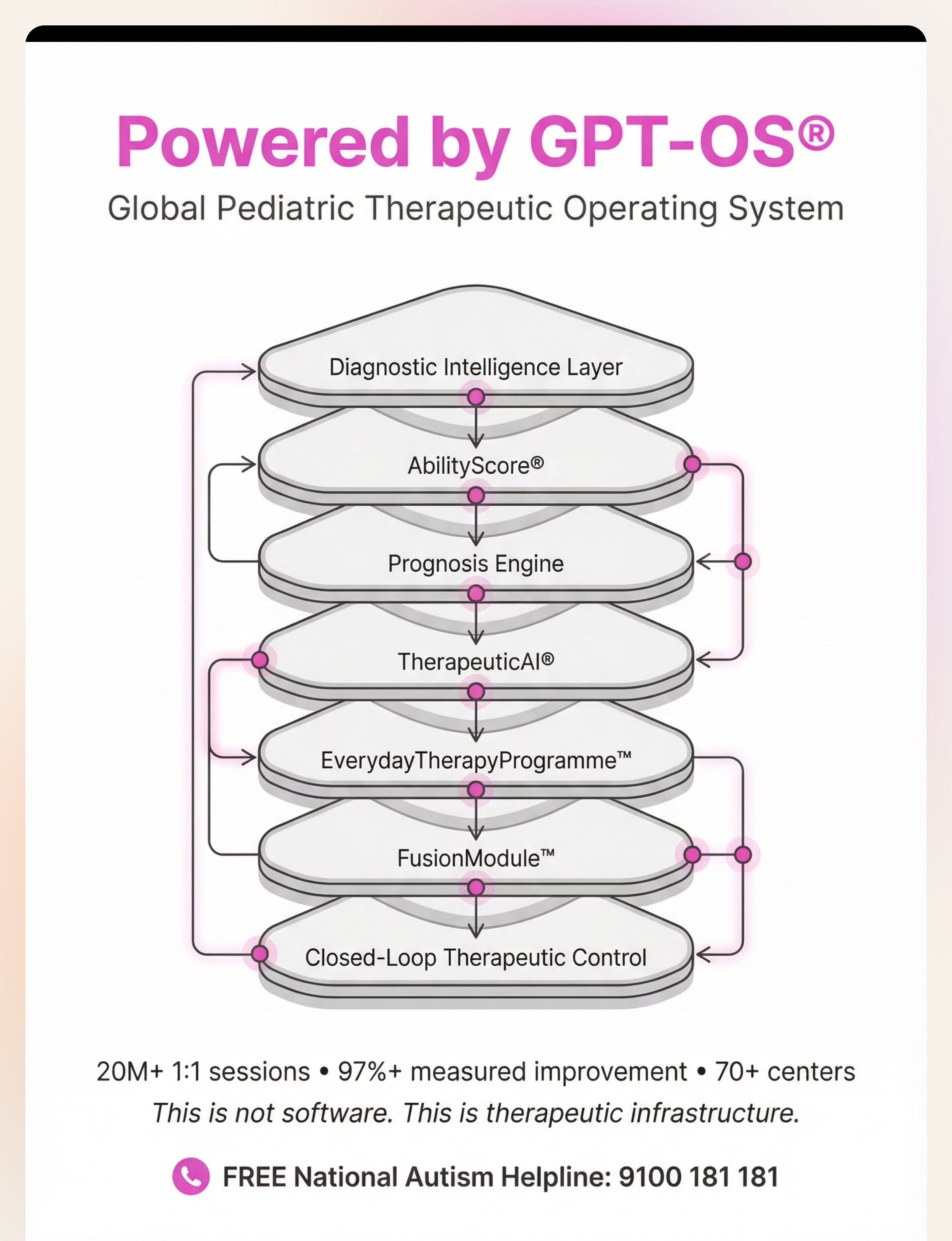
Every session you track feeds GPT-OS® — the Global Pediatric Therapeutic Operating System — which has learned from 20 million+ therapy sessions to personalize your child's program in real time.
What GPT-OS® Learns From F-573 Data
Which warm-up sequence correlates with best stretch compliance · Optimal stretch hold duration for this tone profile · Standing frame duration progression curves by age and CP type · Putty resistance progression timeline by hand function profile
Privacy Assurances
All data encrypted under Indian IT Act compliance · No individual-identifiable data shared externally · Aggregated anonymized data only for population-level learning · You control your data: request deletion at care@pinnacleblooms.org
When 50,000 families tell GPT-OS® that warm bath before stretching improves compliance, the 50,001st family gets that recommendation built in. Your consistency is not just for your child.
See It Before You Do It — Reel F-573
Video demonstration improves parent skill acquisition by 60% compared to text-only instruction. You understand this technique better by watching — then reading — then doing.
▶ Watch Reel F-573
A Pinnacle Physical Therapist walks through all 9 materials in 75 seconds — demonstrating each one in use with a child with hypertonia. Watch at pinnacleblooms.org/reels/F-573 →
Reel Details
Series: Motor Development & Physical Therapy · Episode 573 of 999 · Domain: F — Motor Development · Duration: 75–85 seconds · Presenting: Pediatric PT Specialist, 12+ years experience
Related Reels in This Series:
F-571
9 Materials for Gross Motor Delay
F-572
9 Materials for Balance & Coordination
F-574
9 Materials for Low Muscle Tone
NCAEP (2020): Video modeling is classified as an evidence-based practice. Multi-modal learning — visual + text + demonstration — significantly improves parent skill acquisition and retention.
Consistency Across All Caregivers Multiplies Therapeutic Impact
If only one parent stretches — and then the child goes to grandparents or school where none of this happens — you've lost 60–70% of your session benefit. The nervous system learns from consistent input across ALL environments.
"Explain to Grandparents" Script
"[Child's name]'s muscles are a bit stiffer than other children's. The ball/stretching/warm bath helps the muscles relax. When you do these things, you're not playing — you're doing what the doctor ordered."
Full caregiver script included in downloadable PDF below.
Share This Page
Share with every caregiver in your child's life — grandparents, domestic helpers, school teachers, and extended family members who interact with your child regularly.
Consistency across caregivers tells your child that their body is respected everywhere they go. That message has therapeutic value of its own.

Questions Parents in Our Network Ask Most
Q1: How often should I use these materials at home?
Daily use is the target — not weekly. Stretching: daily, ideally 2× per day (morning and after warm bath). Standing frame: per prescription (usually 30–60 min daily). Therapy ball: daily warm-up. Consistency > intensity. 10 minutes daily beats 60 minutes twice a week.
Q2: My child is non-verbal. Are these materials safe?
Yes — with appropriate modification and professional guidance. Non-verbal children communicate through body language — you will learn to read stiffening (discomfort) vs. relaxing (acceptance). AFOs and standing frames specifically require professional prescription regardless of verbal ability.
Q3: Will stretching make the tone permanently better, or only temporarily?
Both. Acute benefit: tone temporarily reduced for 30–90 minutes post-session — the window for functional activities. Cumulative benefit: muscle fiber length maintained, stretch reflex sensitivity decreases, contracture prevented. The permanent change is in the muscle biology.
Q4: We were told our child needs Botox for spasticity. Should we still do the home program?
Absolutely — more than ever. Botulinum toxin creates a time-limited window of reduced tone. This is EXACTLY when home stretching, standing, and positioning are most effective. Missing the post-Botox window is a commonly cited clinical missed opportunity. The injection and the home program work together.
Q5: My child's tone is worse in the morning. Is this normal?
Yes — diurnal variation is normal and particularly common in CP. Morning tone is typically highest. Strategy: warm bath FIRST THING in the morning before dressing, therapy, or school. This is the single highest-leverage time investment for hypertonia management.
Q6: I can't afford the standing frame. What should I do?
Supported standing against a wall or table, with caregiver physical support, provides similar benefits for shorter durations. Some states have assistive device schemes. Pinnacle can assist with documentation for funding applications. Call 9100 181 181 for guidance.
Q7: Are there age limits for these materials?
Therapy ball and warm water: from birth (with appropriate support). Weighted blanket: 18 months minimum. Therapy putty: 3 years minimum (mouthing risk). AFOs/splints: from infancy (prescribed). Standing frame: from when child has some head/trunk control, typically 12–18 months per therapist assessment.
Q8: What's different about the therapy ball for hypertonia vs. hypotonia?
Same tool, opposite neurological goals. Hypertonia: slow, rhythmic movement for relaxation and tone reduction. Hypotonia: more active, challenging balance activities to stimulate muscle activation. The application — not the tool — makes the difference.

You Have Everything You Need. Start Today.
You arrived at this page because you are paying attention to your child. You have read the science, learned the safety protocols, understood the steps, and seen what is possible. The only thing left is to begin.
20M+
1:1 Sessions
Delivered across the Pinnacle Blooms Network
97%+
Measured Improvement
Across families using consistent home programs
70+
Centers in India
Plus teleconsultation serving 70 countries
📞 FREE NATIONAL HELPLINE: 9100 181 181 — 24×7 | 16+ Languages | No appointment needed | Physical therapy specialist triage available
Preview of 9 materials that help with high muscle tone Therapy Material
Below is a visual preview of 9 materials that help with high muscle tone therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
"From Fear to Mastery. One Technique at a Time."
— The Pinnacle Blooms Consortium
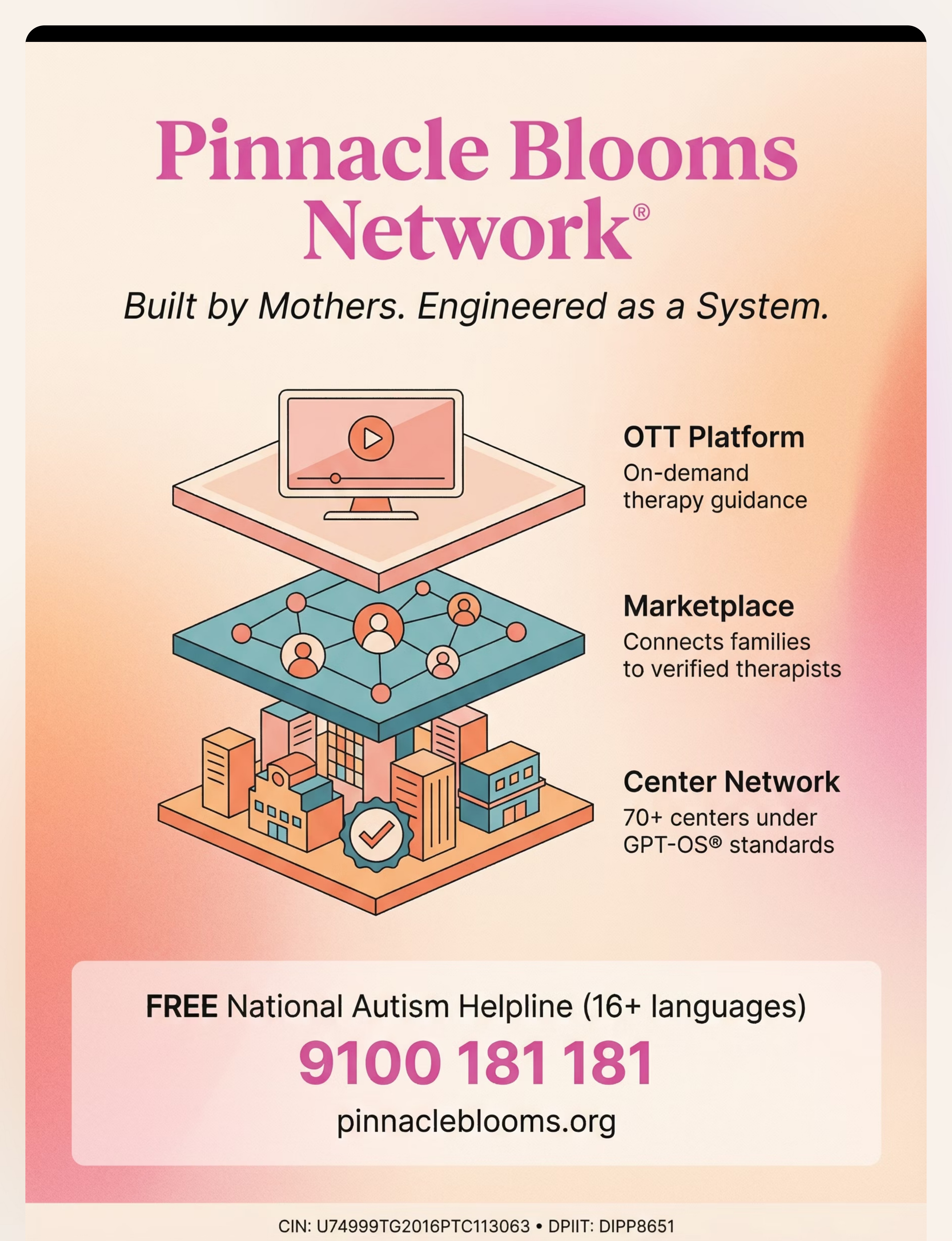
Pinnacle Blooms Network® exists to transform every home — in India and across 70 countries — into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy environment. Powered by GPT-OS® — the Global Pediatric Therapeutic Operating System. Not a clinic. Not an app. A therapeutic operating system for the most important caregiving relationship in a child's life.
🤲 OT
Occupational Therapy
🏃 PT
Physical Therapy
📢 SLP
Speech-Language Pathology
📊 ABA
Applied Behavior Analysis
🎓 SpEd
Special Education
🧠 NeuroDev
NeuroDevelopmental Medicine
Medical Disclaimer: This content is educational. It does not replace individualized assessment and intervention with licensed physical therapists, occupational therapists, and physicians. High muscle tone can have various underlying causes requiring medical evaluation. Treatment approaches should be guided by qualified professionals familiar with your child's specific condition. Individual results may vary. Always consult your child's medical team before beginning or modifying a home therapy program.
CIN U74999TG2016PTC113063 | DPIIT DIPP8651 | MSME TS20F0009606 | GSTIN 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network® — Unit of Bharath Healthcare Laboratories Pvt. Ltd. GPT-OS® | AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ are proprietary marks of Pinnacle Blooms Network®.