
Your Child Learns Best When Their Hands Are Doing the Thinking
It's a Tuesday afternoon and the worksheet is untouched. Your child has pushed away the pencil three times, turned the chair sideways, and is now stacking the eraser on top of the pencil box — quietly absorbed, completely focused. The irony hits you: this is concentration. Just not the kind the school asked for.
Hands-On Learning is not a workaround. It is the primary language of the kinesthetic nervous system. And there are 9 materials that speak it fluently.
You are not fighting a distracted child. You are watching a different kind of brilliant mind demand the right input.
🏛️Pinnacle Blooms Network® Consortium | OT • SLP • ABA • SpEd • NeuroDev
Evidence-Linked | Clinically Validated | Parent-Executed
📞 FREE National Helpline: 9100 181 181 | Available in 16 languages
Evidence-Linked | Clinically Validated | Parent-Executed
📞 FREE National Helpline: 9100 181 181 | Available in 16 languages

ACT I | THE EMOTIONAL ENTRY
The Data Behind What You're Seeing
68%
Kinesthetic Learners
Of children with neurodevelopmental differences show kinesthetic learning as their dominant processing style
1 in 36
Children with Autism
In India are identified with autism — the majority showing sensory-motor learning preferences
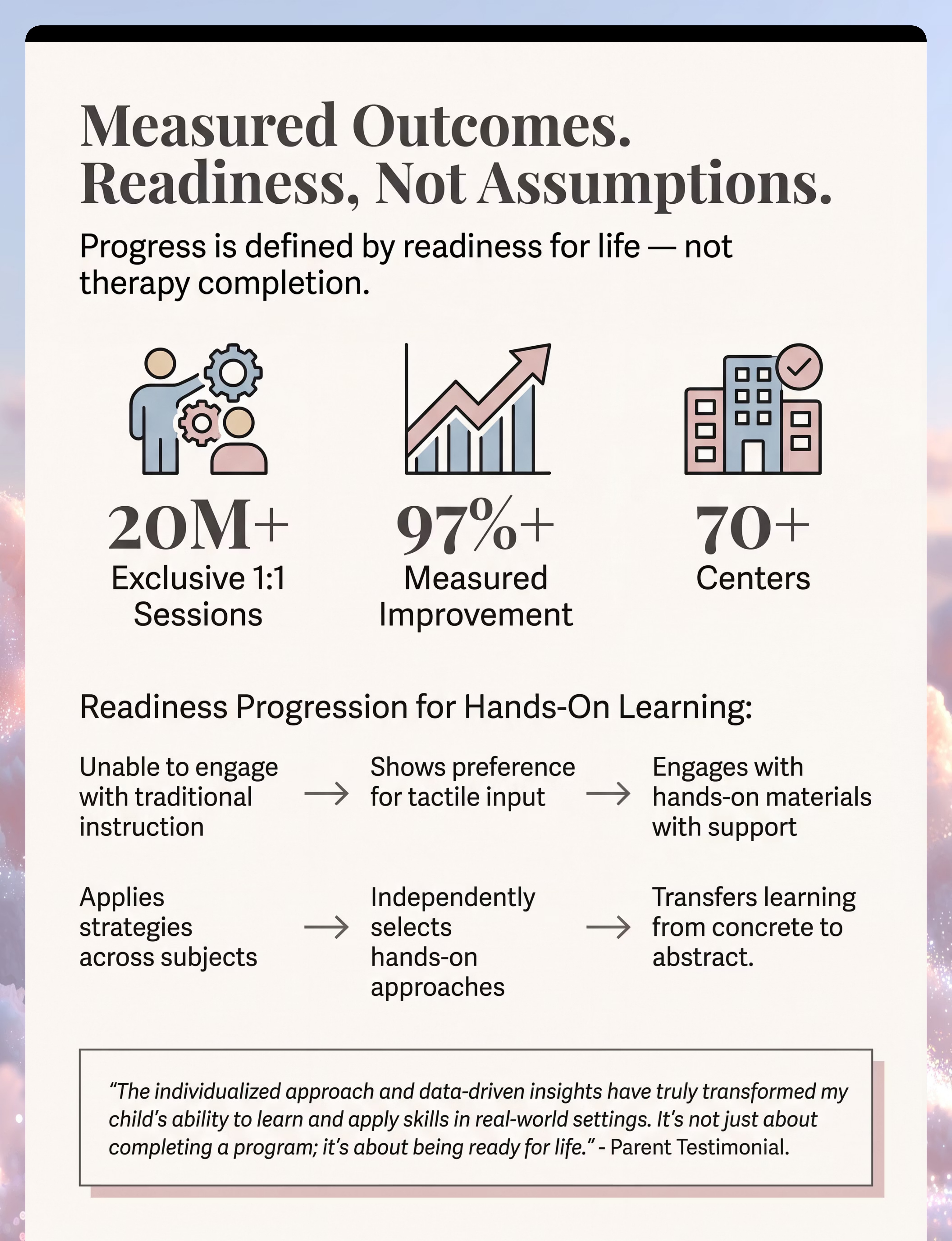
21M+
Therapy Sessions
Delivered by Pinnacle across 70+ centres, validating hands-on approaches daily
When your child must touch, build, move, or manipulate to understand — that is not defiance. That is the somatosensory cortex doing exactly what evolution designed it to do. Across 70+ countries, millions of families are raising children whose nervous systems demand learning through the body first.
India alone has an estimated 8–10 million children with autism spectrum conditions. The majority benefit significantly from tactile and kinesthetic intervention approaches validated across our network. You are among an estimated 2.3 million families in India navigating hands-on learning challenges right now. This page was built for you.

When Hands Learn, the Whole Brain Fires
The Kinesthetic-Tactile Learning Circuit
Key areas activated during hands-on learning:
- Somatosensory Cortex — primary touch processing
- Cerebellum — movement sequencing and motor learning
- Prefrontal Cortex — executive planning, engaged by doing
- Hippocampus — memory consolidation, strongest when paired with physical action
The Science, Simply Put
Your child's brain has a somatosensory cortex that processes every touch signal — texture, weight, temperature, shape. In many children with autism and sensory processing differences, this pathway is either hyper-sensitive (overwhelmed by touch) or hypo-sensitive (under-responding, seeking more).
Why hands-on learning works: When a child physically manipulates an object, the brain simultaneously activates motor planning, tactile discrimination, working memory, and long-term encoding. This is called embodied cognition — the scientific name for what you already instinctively know: your child remembers what they touched, built, and moved far longer than what they were told.
"This is a wiring difference, not a behaviour choice. The kinesthetic nervous system is not broken — it is demanding its native language." — Pinnacle NeuroDev Consortium

Your Child's Journey, Mapped
0–12 Months
Oral-tactile exploration — mouthing, grasping, feeling
12–24 Months
Object manipulation — banging, stacking, pouring
2–4 Years
HANDS-ON LEARNING ◄ YOU ARE HERE — Builds blocks, pours, stacks, sorts by feel
4–7 Years
Symbolic-representational learning — understands categories by doing
7–12 Years
Abstract reasoning layer — applies concepts without objects
Hands-on learning needs typically emerge as the dominant learning style between ages 2–7, often persisting as the preferred modality well into adolescence for children with autism and sensory processing differences. Children with hands-on learning profiles commonly co-present with Sensory Processing Disorder (SPD), Dyspraxia, ADHD, or Intellectual Disability (mild–moderate range).
📍 Your child is here — in the hands-on learning zone. 🎯 The research is unambiguous: tactile-kinesthetic foundation at ages 2–7 dramatically increases the probability of academic readiness at age 7+.

Level I Evidence
Systematic Review Grade
The Research Says: This Works
📚 Systematic Review (2024)
16 high-quality studies confirm hands-on sensory-motor intervention meets criteria as an evidence-based practice for children with ASD. Outcomes include improved academic engagement, skill retention, and adaptive behaviour. PMC11506176 — Children (MDPI), 2024
📚 Meta-Analysis (2024)
Across 24 studies, sensory integration and tactile-kinesthetic therapy effectively promoted social skills, adaptive behaviour, sensory processing, and gross/fine motor skills. PMC10955541 — World Journal of Clinical Cases, 2024
📚 Indian RCT (2019)
Home-based sensory and kinesthetic interventions delivered by trained caregivers demonstrated significant developmental outcomes in Indian pediatric populations — validating the home-execution model. Padmanabha et al., Indian Journal of Pediatrics
"Clinically validated. Home-applicable. Parent-proven." — Pinnacle Blooms Network® CRO Division
📞 Questions? Call 9100 181 181 — Free, 16 languages
📞 Questions? Call 9100 181 181 — Free, 16 languages

ACT II | KNOWLEDGE TRANSFER
H-754: Hands-On Learning Facilitation
🖐️ Technique Definition
What it is: A multi-material, kinesthetic-tactile intervention protocol that presents academic, cognitive, and adaptive skill content through direct physical manipulation of structured materials. It routes all learning through the child's tactile and proprioceptive systems — the sensory channels proven most accessible and retentive for children with autism, sensory processing differences, and neurodevelopmental profiles that favour embodied cognition.
What it does: Activates the somatosensory, motor planning, and hippocampal memory systems simultaneously — encoding information through physical experience rather than passive reception.
Who it's for: Children aged 2–12 with autism, sensory processing differences, ADHD, DCD, intellectual disability (mild–moderate), or any kinesthetic learning profile. Also effective for typically developing children who show a clear hands-on learning preference.
Session Badges
🎯 Domain
Domain H — Hands-On Learning
👶 Age Range
2–12 years
⏱️ Duration
15–30 min/session
📅 Frequency
3–5× per week
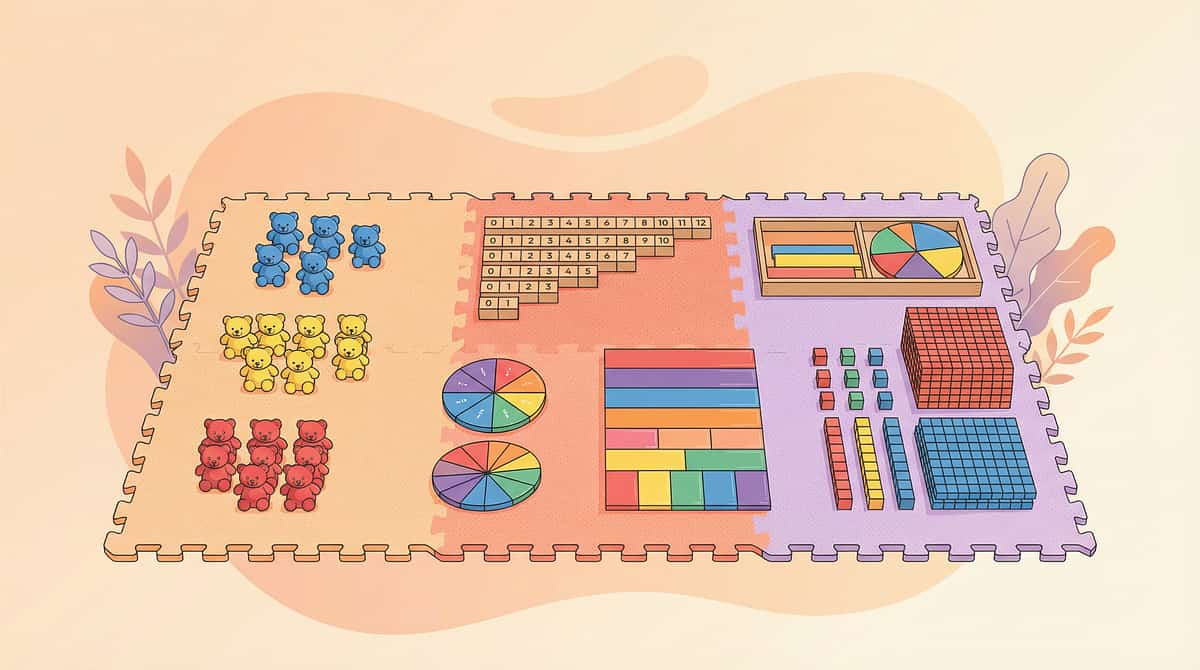
Canon Material Categories
- Math Manipulatives
- Building & Construction Sets
- Sensory Learning Materials
- Science Experiment Kits
- Letter & Word Building
- Art & Craft Materials
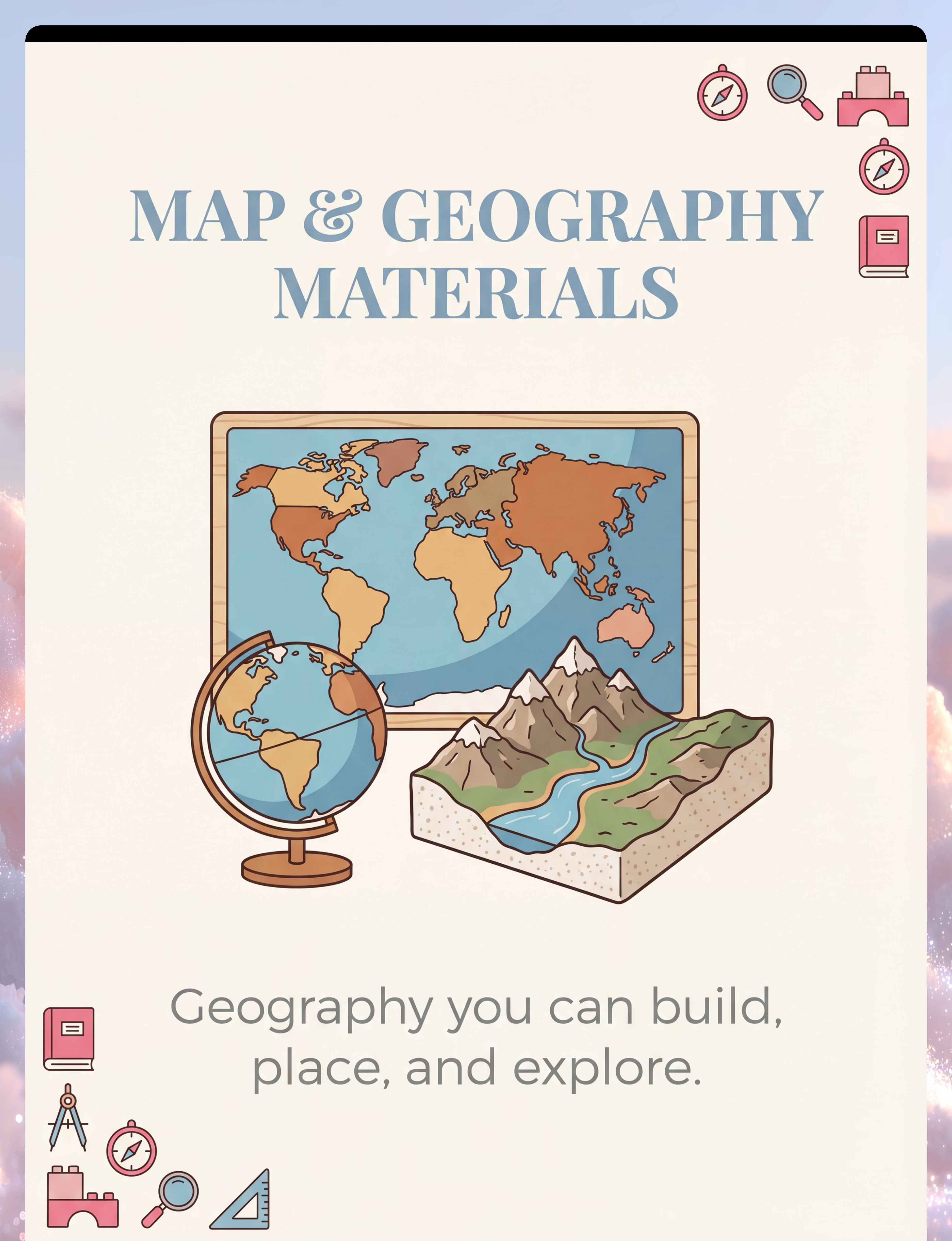
- Map & Geography Materials
- Movement-Based Materials
- Role-Play Materials

Five Disciplines. One Protocol. Total Coverage.
Occupational Therapist (Primary Lead)
Selects, grades, and sequences hands-on materials based on the child's sensory profile. Calibrates tactile input intensity, proprioceptive demands, and fine motor complexity. Monitors sensory tolerance and adjusts material presentation in real-time.
Speech-Language Pathologist
Embeds language targets within hands-on activities. While the child builds, sorts, or manipulates, the SLP layers in vocabulary, sequencing language, descriptive narration, and communication demands that emerge naturally from the activity context.
ABA / BCBA Therapist
Structures the hands-on activity as the context for discrete trial training, task analysis, reinforcement scheduling, and behaviour shaping. Tracks engagement duration, on-task behaviour, and skill acquisition data across sessions.
Special Educator
Adapts academic curriculum content — numeracy, literacy, science, geography — into hands-on material formats. Ensures alignment with IEP goals and school curriculum while using manipulatives as the bridge to abstract academic concepts.
NeuroDev Paediatrician
Provides the diagnostic framework that identifies the hands-on learning profile, monitors developmental progression, and coordinates medical co-management where sensory differences are neurologically complex.
"This technique crosses therapy boundaries because the brain doesn't organise by therapy type. The kinesthetic system serves language, behaviour, cognition, and motor function simultaneously." — Pinnacle Blooms Consortium
📞FREE Helpline: 9100 181 181 | Connect with the right specialist today
Material 1 of 9
Math Manipulatives
What They Are
Counting bears, number rods, fraction tiles, base-10 blocks — tangible representations of abstract numerical concepts. These are the bridge between a child's hands and the abstract world of numbers.
Clinical Function
Converts abstract math concepts into tactile objects the child can sequence, count, and compare physically. The hand-to-object contact is the neurological anchor for the number concept — without it, numbers remain floating abstractions for kinesthetic learners.
🛒 Recommended Product
🔄 ₹0 DIY Version
Use dried beans, bottle caps, or pebbles as counting units. Place in a muffin tin, count into groups, sort by quantity. Identical proprioceptive input, zero cost.
📞 Need guidance on which materials to prioritise? FREE: Call 9100 181 181

Material 2 of 9
Building & Construction Sets
What They Are
LEGO, magnetic tiles, wooden unit blocks, interlocking cubes — physics and engineering through direct assembly. Every structure a child builds is a hypothesis tested by their hands.
Clinical Function
Activates spatial reasoning, motor planning, cause-effect understanding, and persistence. The child learns that effort + structure = result — a foundational concept for academic and life learning.
🛒 Recommended Products
Kidology Pull Out Spike Toy — ₹380
Buy on Amazon.in
Buy on Amazon.in
🔄 ₹0 DIY Version
Empty cardboard boxes, toilet rolls, and tape — build towers, bridges, and vehicles. Same spatial-motor planning demands, same cognitive activation. Zero cost.

Material 3 of 9
Sorting Activities & Categorisation
What They Are
Colour sorting sets, shape sorters, attribute blocks, classification trays. Every sorting activity is the brain learning to impose order on the world — a deeply satisfying kinesthetic act.
Clinical Function
Develops logical thinking, category formation, and visual-tactile discrimination through physical sorting. The child's hands enact the cognitive operation before their verbal language can name it.
🛒 Recommended Products
Brainy Bug Flashcards with Audio — ₹305
Buy on Amazon.in
Buy on Amazon.in
🔄 ₹0 DIY Version
Sort household items by colour, size, or shape into muffin tin sections. Buttons, pebbles, bottle caps — identical categorisation and discrimination demands. Zero cost.

Material 4 of 9
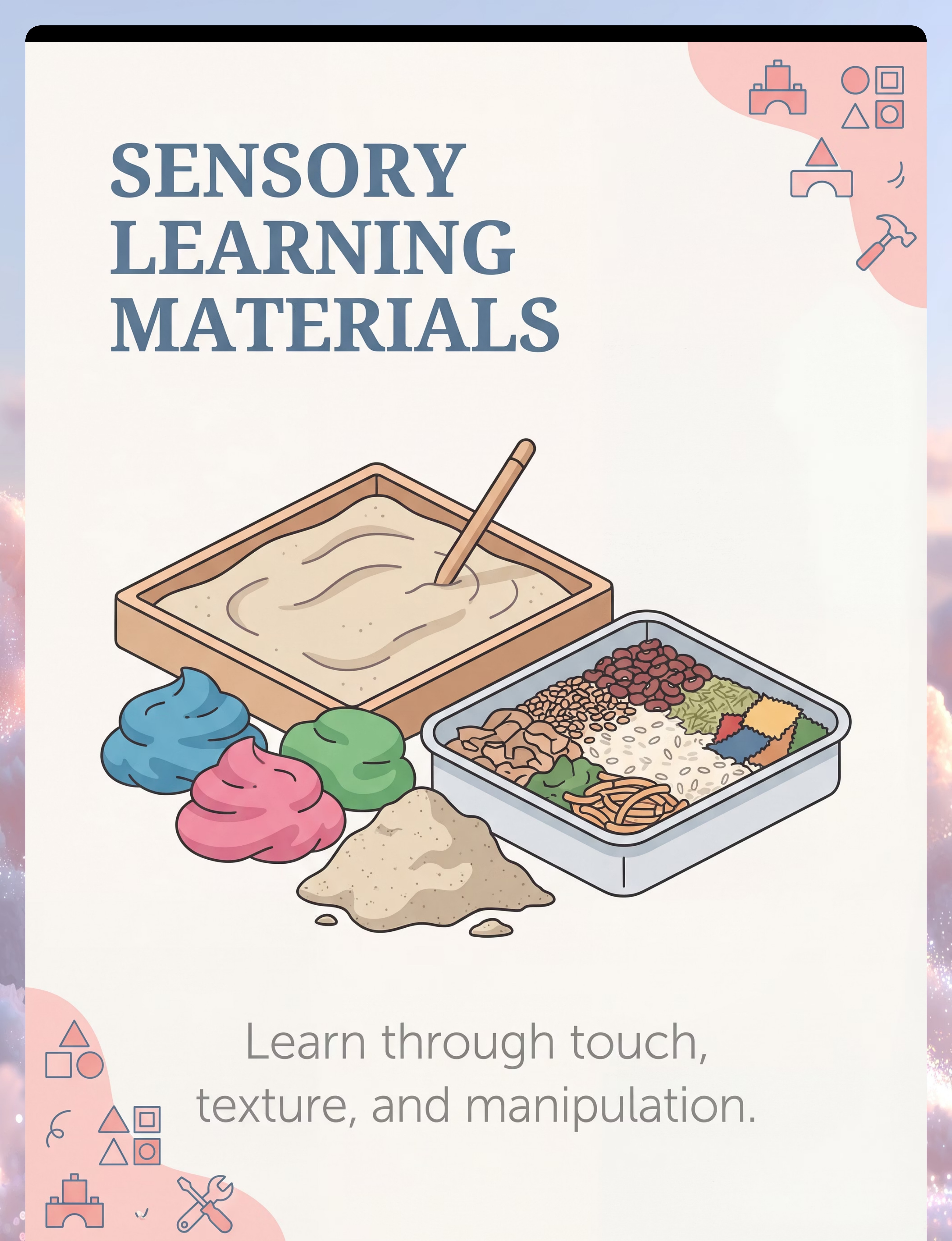
Sensory Learning Materials
What They Are
Sand trays, kinetic sand, sensory bins with rice or lentils, play dough, cloud dough. These materials provide the deep proprioceptive input that the kinesthetic nervous system is constantly seeking.
Clinical Function
Provides deep proprioceptive and tactile input that regulates the arousal system while simultaneously embedding academic content — letters in sand, counting objects in bins. Regulation and learning happen at the same moment.
🛒 Find on Amazon.in
🔄 ₹0 DIY Version
Fill a tray with uncooked rice or dal. Hide letters, numbers, or small objects inside. Child searches, finds, and sorts — deep tactile and proprioceptive regulation at ₹0–₹50 total.
For children with severe tactile defensiveness, OT-recommended materials with specific sensory properties may be clinically necessary. Contact 9100 181 181 for guidance.

Material 5 of 9
Letter & Word Building
What They Are
Foam letters, magnetic alphabet sets, sandpaper letters, moveable alphabet sets. These materials transform reading and spelling from an abstract visual task into a physical act of construction.
Clinical Function
Makes phonics and spelling a physical, hands-on act rather than an abstract visual task — dramatically improving retention for kinesthetic learners. The child builds the word with their hands before their voice can say it.
🛒 Find on Amazon.in
🔄 ₹0 DIY Version
Write letters on index cards, bottle caps, or clay slabs. Child physically arranges them to form their name, then simple CVC words. Trace each letter in a sand tray before placing — kinesthetic + visual + tactile = triple encoding.

Material 6 of 9
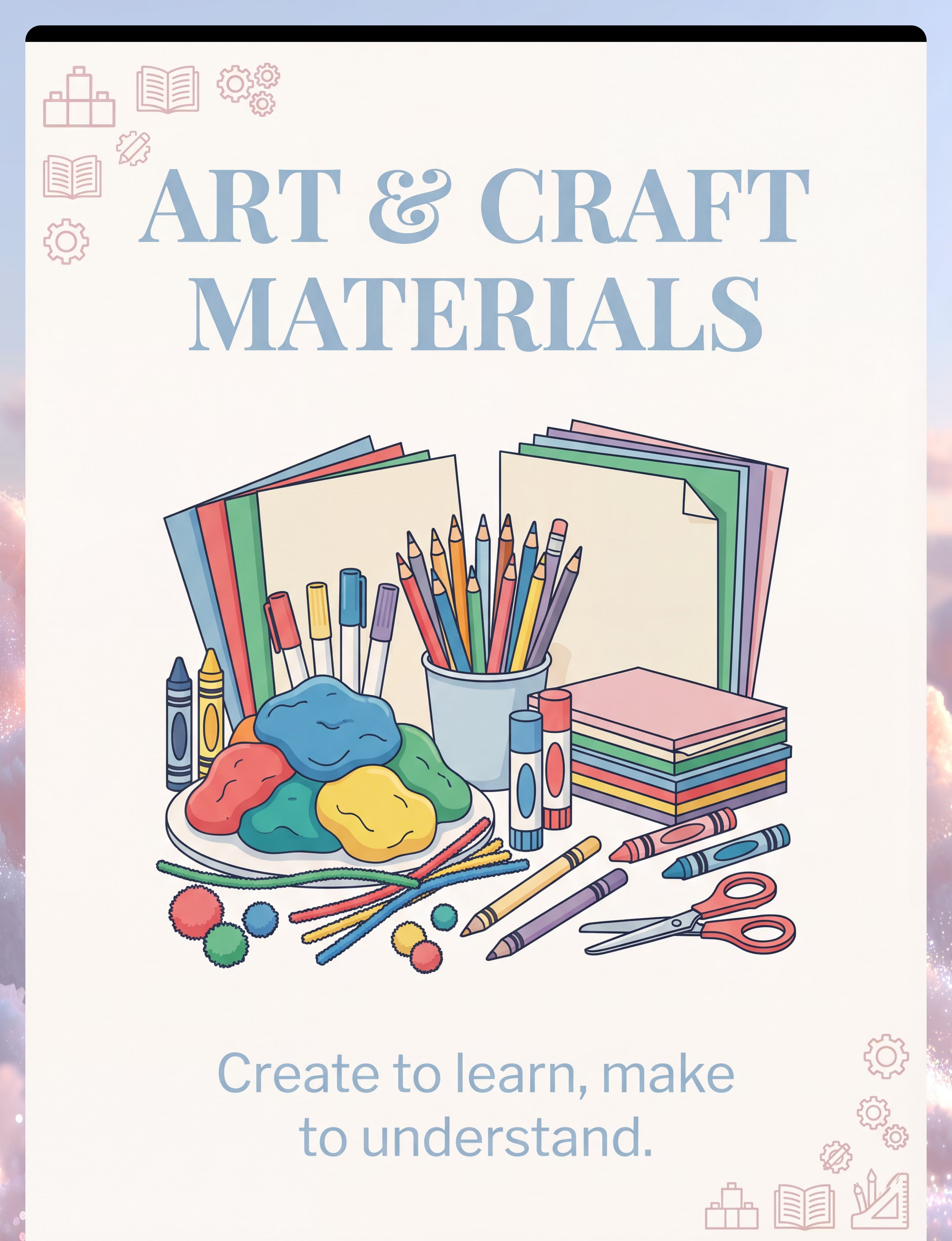
Art & Craft Materials
What They Are
Clay, playdough, finger paints, collage materials, threading beads, mosaic tiles. Art-making is not a break from learning — for kinesthetic learners, it is learning's most natural expression.
Clinical Function
Combines fine motor development with creative expression and cognitive planning — the hands-on learning trifecta. The child plans, executes, and evaluates — all through their hands.
🛒 Find on Amazon.in
🔄 ₹0 DIY Version
Homemade salt-dough (flour + salt + water) is clinically equivalent to commercial playdough. Natural paints from turmeric or beetroot add tactile variety at ₹0–₹20. The clinical function is identical.
Choking hazard note: Check for wheat/gluten sensitivity before using homemade dough. Art materials must be non-toxic — confirm before purchase.

Material 7 of 9
Science Experiment Kits
What They Are
Simple experiment kits, magnets, measurement tools, nature collections, magnifying lenses. Science, at its core, is hands-on inquiry — the natural domain of the kinesthetic learner.
Clinical Function
Converts inquiry learning into direct hands-on experimentation — the scientific method as a kinesthetic experience. The child does not read about cause and effect; they create it with their hands.
🛒 Find on Amazon.in
🔄 ₹0 DIY Version
Vinegar + baking soda eruptions, bean sprouting in cotton wool, shadow tracing with sunlight — identical inquiry-learning activation at ₹0–₹30. Nature itself is the best science kit.

Material 8 of 9
Movement-Based Learning Materials
What They Are
Hopscotch mats, yoga cards, body-movement learning games, floor number lines. The whole body is a learning instrument — these materials activate it fully.
Clinical Function
Encodes academic content through whole-body movement — the most powerful memory-consolidation pathway for children with proprioceptive-seeking profiles. Jump-counting and jump-spelling are among the most effective early literacy and numeracy approaches for kinesthetic learners.
🛒 Find on Amazon.in
🔄 ₹0 DIY Version
Draw number hopscotch on the floor with chalk or tape. Jump-count. Jump-spell. Draw a body outline on paper and label body parts. Identical proprioceptive encoding of academic content at zero cost.

Material 9 of 9
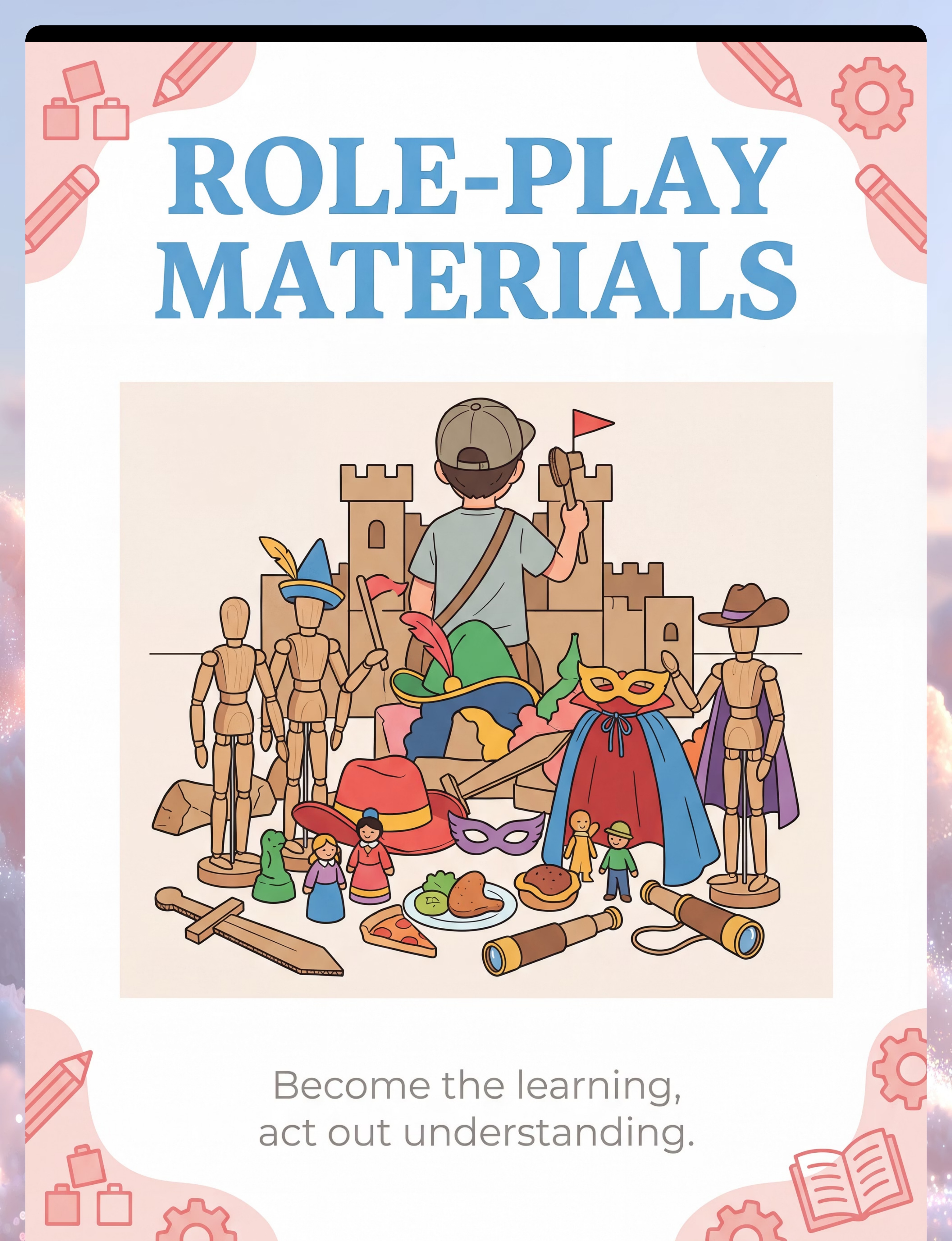
Role-Play & Dramatic Play Materials
What They Are
Doctor kits, kitchen sets, puppet theatres, costume props, social scenario figurines. Children learn social rules by physically living them — role-play is social cognition's native environment.
Clinical Function
Embeds social cognition, language, and emotional understanding into physical enactment — learning social rules by physically living them. The child does not merely hear about how to greet a doctor; they become the doctor.
🛒 Find on Amazon.in
🔄 ₹0 DIY Version
Old clothes as costumes, cardboard props, household items as play tools — the same social-cognitive enactment pathway is activated regardless of material cost. A cardboard box becomes a shop counter; a wooden spoon becomes a doctor's instrument.
📞 Need guidance on which materials to prioritise for your child? FREE: Call 9100 181 181 — Our therapists help you choose based on your child's profile.

Every Material Has a ₹0 Version
WHO/UNICEF equity principle: No family is excluded by economic status. Every technique in the Pinnacle system has a zero-cost implementation pathway.
Clinical Material | Household Substitute | Why It Works | ₹0 | |
Math manipulatives | Dried lentils, buttons, pebbles | Same tactile-count function, identical proprioceptive input | ✅ | |
Building sets | Cardboard boxes, tape, toilet rolls | Same spatial-motor planning demands | ✅ | |
Kinetic sand / sensory bin | Rice, flour, or clean soil in a tray | Same deep tactile and proprioceptive regulation | ✅ | |
Letter tiles | Letters written on bottle caps or stone | Same tactile-phonics connection | ✅ | |
Clay / playdough | Homemade dough (flour + salt + water) | Identical fine motor and sensory demands | ✅ | |
Science kits | Baking soda + vinegar, sprout jars | Same inquiry-learning activation | ✅ | |
Hopscotch mat | Tape on floor or chalk outdoors | Identical proprioceptive encoding of academic content | ✅ | |
Role-play kits | Old clothes, cardboard, household items | Same social-cognitive enactment pathway | ✅ | |
Sorting sets | Muffin tin + mixed household objects | Identical categorisation and discrimination demands | ✅ |
When clinical-grade is non-negotiable: For children with severe tactile defensiveness or significant sensory modulation disorders, material texture, weight, and resistance do matter. In these cases, OT-recommended materials with specific sensory properties may be clinically necessary. Contact our free helpline: 📞9100 181 181

Read This Before You Begin Every Session
🔴 STOP: Contraindications
Do NOT proceed if your child:
- Is in active meltdown or post-meltdown recovery
- Is showing signs of illness — fever, pain, nausea, or fatigue
- Has open wounds, skin infections, or active dermatitis on hands or feet
- Has a known allergy to any material components
- Has been prescribed "sensory rest" by their OT
🟡 CAUTION: Modify with Care
Proceed with modifications if:
- Child is in a hyperactive or highly stimulated state — simplify material
- Child showed avoidance last session — reduce sensory intensity
- Child is hungry or hasn't toileted recently — basic needs first
- Child shows mild resistance to a specific material — offer alternative
🟢 GO: Pre-Session Checklist
Proceed normally when:
- Child is calm, fed, rested, and in a receptive baseline state
- Child has had no major distress in the last 30 minutes
- All materials are at room temperature
- Parent/caregiver is calm with 20–30 minutes of uninterrupted time
🚨STOP IMMEDIATELY IF: Child vomits, loses consciousness, develops hives or breathing difficulty, or is in extreme distress that cannot be de-escalated within 3 minutes. Discontinue immediately. Seek medical attention. Call 9100 181 181 for clinical guidance.

The Environment Is the First Intervention
Space Setup Checklist
1
Surface
Floor mat or low table — child's feet flat on ground for proprioceptive grounding
2
Lighting
Natural or warm light — avoid fluorescent overhead lighting which can increase sensory load
3
Sound
Quiet environment — or soft, familiar background music at low volume
4
Materials
2–3 items only for first sessions. TV off, phones on silent, distracting objects removed
5
Temperature
Room 22–26°C | Materials at room temperature — cold materials can trigger defensiveness
Parent Positioning Note
Sit beside your child, slightly behind their shoulder — not opposite. This removes the performance pressure of face-to-face engagement and allows you to model from behind, which is the OT-recommended position for hands-on learning facilitation.
Being beside means beside — not across the table, not standing over. Your physical position communicates: We are doing this together.
Exit Route
Always ensure the child can leave the space without climbing or obstruction. The freedom to leave is what makes it safe to stay.
Reinforcer Placement
Pre-selected reward kept within reach, not in view. Available immediately on task completion.

ACT III | THE EXECUTION
60-Second Pre-Session Readiness Assessment
Do not skip this step. The best session is one that starts right.
# | Check | YES ✅ | NO ❌ | |
1 | Child has eaten in the last 90 minutes | Continue | Feed first, wait 20 min | |
2 | Child has toileted in the last 30 minutes | Continue | Toileting break first | |
3 | Child is not showing signs of illness | Continue | Postpone session | |
4 | Child is in an alert (not overexcited or drowsy) state | Continue | Regulatory activity first | |
5 | Child has not had a major meltdown in the last 45 minutes | Continue | Wait for full regulation | |
6 | Child's hands and skin are clean and intact | Continue | Address skin issues first | |
7 | Parent/caregiver is calm and has uninterrupted time | Continue | Reschedule for better moment |
🟢 ALL 7 = GO
Proceed to Step 1: The Invitation
🟡 5–6 = MODIFY
Shorten session to 10 minutes, use the child's highest-preference material only
🔴 4 or Below = POSTPONE
This is not failure. This is excellent clinical judgement. Do a calming activity and try again tomorrow.

Step 1
The Invitation
⏱️30–60 seconds
🗣️ Say This (or adapt to your child's language level)
"Hey! Come look at what I've got for you today."
[Place ONE material on the table — do not speak yet. Let the child's curiosity do the work.]
"Want to see what this does?"
Body Language Guidance
- Sit down before inviting the child — already at their level
- Use a calm, curious tone — not excited performance, not a directive command
- Make eye contact optional — do not require it to begin
- Offer material with an open, flat hand — not thrust forward
✅ Acceptance Cues — What YES Looks Like
- Child moves toward the material
- Child looks at the material for 2+ seconds
- Child reaches out or points
- Child stays in the space without moving away
❌ Resistance Cues — What NO Looks Like
- Child moves away immediately → Move material slightly further. Wait 10 seconds. Try another item.
- Child ignores completely → Comment on the material yourself without requiring response.
- Child vocalises distress → Do not push. Transition to a regulatory activity.
ABA Pairing Note: Pair yourself with reinforcement before placing any demand. Sit near the child's preferred item for 2 minutes first. Become the person who brings fun — not demands.

Step 2
The Engagement
⏱️1–3 minutes
The child has moved toward the material. Now deepen the interaction by introducing the material actively — through demonstration, not instruction.
🗣️ Script — What to Say
"Look — I'm going to smoosh this." [Smoosh the clay yourself]
Wait. See if the child reaches.
If yes: "Your turn." [Slide material toward child]
If no: "It feels funny!" [Continue engaging yourself without looking at child for approval]
Material Introduction Technique
- Present material at mid-line — directly in front of child, at hand height
- Start with the material the child is most likely to tolerate
- Keep your hands visible — model with your own hands
- Do not narrate excessively — too many words compete with tactile processing
Response Spectrum
🟢 Engagement
Child manipulates spontaneously → Follow the child's lead entirely
🟡 Tolerance
Child watches but doesn't touch → Narrate your own actions, wait, reduce expectation
🔴 Avoidance
Child pushes material away → Acknowledge, offer alternative material from the 9
✅When to praise: The moment the child touches the material — "Yes! You got it!" Immediate, specific, enthusiastic.
Step 3
The Therapeutic Action
⏱️5–15 minutes — the main event
This is the active ingredient of the session. The child is now physically manipulating the learning material in a way that encodes the target skill.
Math Manipulatives
Child physically counts, arranges, compares, and groups objects. Do not count for them — guide their hands to touch each object as they count. The hand-to-object contact is the neurological anchor for the number concept.
Building Sets
Present a simple structure to copy (3–4 pieces). Child assembles. Narrate the spatial language: "on top," "next to," "under." Complexity increases only when child completes current challenge with ease.
Sensory Bins
Hide 5–10 objects of different categories in the bin. Child finds, names (verbally or by gesture), and sorts. The searching and finding provides deep proprioceptive and tactile input that regulates while teaching.
Letter Building
Child physically arranges letter tiles to form their name, then simple CVC words. Trace each letter in the sand tray before placing the tile. Kinesthetic + visual + tactile = triple encoding.
Role-Play
Assign a social scenario. Child physically enacts with props. Parent plays supporting character. Language, social rules, and emotional regulation are embedded in the play — not taught didactically.
Duration Guidance: First sessions — 5–8 minutes is excellent. Target by week 4: 15–20 minutes. Never extend beyond the child's interest window — ending on a high beats extending to burnout every time.

Step 4
Repeat & Vary
⏱️3–5 minutes
Core Principle: 3 good, willing repetitions of a skill embed it. 10 forced repetitions generate aversion. Choose quality and willing participation over quantity every time.
Session Stage | Target Repetitions | Notes | |
Week 1–2 | 2–3 reps per material | Build willingness and positive association first | |
Week 3–4 | 4–6 reps with variation | Introduce slight variation to each rep | |
Week 5–8 | 6–10 reps with complexity increase | Skill is consolidating; increase challenge |
Variation Strategies — Keep the Skill, Change the Context
Change the colour of the material — same task, different visual input
Change the container — sorting into a bowl vs. a box vs. a line
Change the position — table → floor → standing
Change the social partner — parent → sibling → grandparent
Satiation Indicators — When Enough Is Enough: Child pushes material away · Child looks away persistently for 10+ seconds · Child vocalises boredom · Child leaves the space. When any of these appear → proceed immediately to Step 5. Do not add "one more."

Step 5
Reinforce & Celebrate
⏱️30–60 seconds — immediate, every time
ABA Reinforcement Principles
Timing: Within 3 seconds of the desired behaviour. Not at the end of the session — at the moment of the target response.
Specificity: Not "good boy/girl" — "You counted all 5! You did it!" Name exactly what the child did.
Magnitude: Matched to the child's reinforcer hierarchy. What works for one child fails for another.
Recommended Products
Reward Stickers (1800+ pack) — ₹364 Amazon.in | 🏅 Pinnacle Recommends
Reward Jar — ₹589 Amazon.in | 🏅 Pinnacle Recommends
Reinforcement Menu
🗣️ Social
Cheering, clapping, high five, hug — for socially motivated children
🍓 Edible
Small preferred food piece — strong motivator; use sparingly
🎮 Activity
30 seconds of preferred activity — sustainable long-term reinforcer
🏅 Token
Sticker, star, stamp — builds toward larger reward; scaffolds executive function
🎯 Intrinsic
Child sees their own completed structure — builds internal motivation over time
"Celebrate the attempt, not just the success. A child who tried and didn't finish deserves reinforcement for trying. That's how you get them back tomorrow." — Pinnacle ABA Division

Step 6
The Cool-Down
⏱️2–3 minutes — mandatory
No hands-on session ends abruptly. The transition from active sensory engagement back to baseline requires a structured de-escalation ritual. Without it, the child may seek more input — leading to escalating behaviour post-session.
Transition Warning — 2 Minutes Before Ending
🗣️"Two more goes, then we're all done for today." Hold up 2 fingers. If child uses PECS or AAC — show the "finished" symbol.
Final Repetition — Signal Completion
🗣️"Last one! You did it. All done." Use the child's established "finished" signal — spoken, signed, or visual.
Material Put-Away Ritual (30 seconds)
Child participates in returning materials to their box. This proprioceptive input — picking up, placing, pressing lid on — continues calming input while building routine ownership.
Transition Activity (1 Minute)
Move immediately to a known, preferred, low-demand activity — deep pressure hug, preferred object, or brief outdoor time.
If dysregulation post-session is a recurring pattern: 📞9100 181 181 — our OT team can advise on cool-down protocol design.

60-Second Data Entry — Do This Now, Before You Forget
Data recorded within 60 seconds of session end is clinical-grade data. Data recorded an hour later is a guess.
H-754 Session Log
Date: ____________ Material(s) Used: ____________
1. Engagement Duration
[ ] <5 min [ ] 5–10 min [ ] 10–20 min [ ] 20+ min
[ ] <5 min [ ] 5–10 min [ ] 10–20 min [ ] 20+ min
2. Participation Quality
[ ] Refused [ ] Tolerated [ ] Engaged [ ] Initiated
[ ] Refused [ ] Tolerated [ ] Engaged [ ] Initiated
3. Outcome Note (one sentence only)
"Today, child _________________________________"
"Today, child _________________________________"
Overall session rating: ☆☆☆☆☆
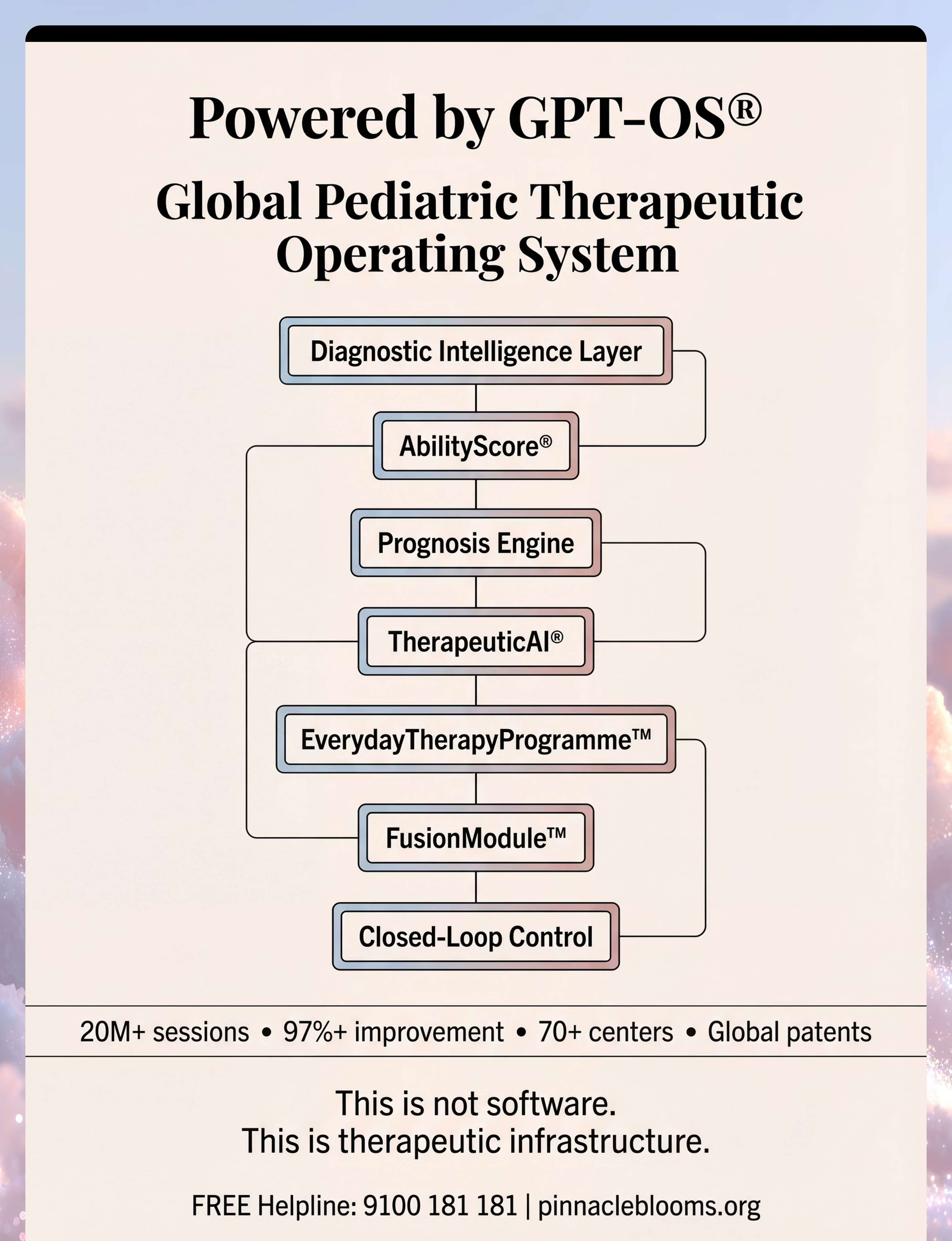
GPT-OS® Integration
If you are a Pinnacle GPT-OS® user, log this session in the TherapeuticAI® dashboard. Your data shapes your child's personalised intervention trajectory and feeds the FusionModule™ cross-discipline coordination layer.
Downloads
Track Online
"60 seconds of data now saves hours of guessing later."

Reality Check: Most Sessions Don't Go Perfectly — That's Normal
Session abandonment is not failure. It is data. Here is what the data means.
Problem 1: Child Refused All Materials Immediately
Why it happened: The child may be under-regulated (tired, hungry, overstimulated) or the material wasn't within their sensory tolerance.
Next time: Run the readiness check more rigorously. Offer the highest-preference material first — the one the child has previously shown interest in.
Next time: Run the readiness check more rigorously. Offer the highest-preference material first — the one the child has previously shown interest in.
Problem 2: Child Threw or Destroyed Materials
Why it happened: Likely seeking stronger proprioceptive input than the material provides — or expressing frustration at an expectation they didn't understand.
Next time: Offer heavier, more resistive materials (clay, wooden blocks, resistive putty). Reduce complexity. No demand for first 3 minutes.
Next time: Offer heavier, more resistive materials (clay, wooden blocks, resistive putty). Reduce complexity. No demand for first 3 minutes.
Problem 3: Child Engaged for 2 Minutes Then Shut Down
Why it happened: Sensory saturation — the nervous system hit its capacity. This is useful data about the child's current tolerance window.
Next time: Shorten session to 3–5 minutes maximum, then extend by 1 minute per week.
Next time: Shorten session to 3–5 minutes maximum, then extend by 1 minute per week.
Problem 4: Child Engaged with Materials but Ignored the Learning Objective
Why it happened: Normal and correct early-stage behaviour. The nervous system is prioritising regulation and enjoyment before academics.
What to do: Let it. Regulation through enjoyable play IS the intervention in weeks 1–3.
What to do: Let it. Regulation through enjoyable play IS the intervention in weeks 1–3.

Troubleshooting Continued: Three More Common Challenges
Problem 5: Child Only Engaged if a Parent Was Doing It Too
Why it happened: Social motivation or attachment-based safety. This is excellent data.
Next time: Joint engagement IS the therapeutic model. Parent participating beside the child is clinically ideal, not a compromise.
Next time: Joint engagement IS the therapeutic model. Parent participating beside the child is clinically ideal, not a compromise.
Problem 6: Child Became Upset at Clean-Up / End of Session
Why it happened: Transition difficulty — extremely common in autism. The cool-down ritual may need strengthening.
Next time: Introduce visual timer 3 minutes before ending. Rehearse the "finished" signal during non-session times. Make clean-up its own hands-on game.
Next time: Introduce visual timer 3 minutes before ending. Rehearse the "finished" signal during non-session times. Make clean-up its own hands-on game.
Problem 7: Child Was Perfect at Home but Showed None of the Skills at School
Why it happened: Generalisation is a separate clinical target. Mastering a skill in one environment does not automatically transfer.
Next time: Begin variation practice — different people, different rooms, different times of day. Share the protocol with the school via the family guide.
Next time: Begin variation practice — different people, different rooms, different times of day. Share the protocol with the school via the family guide.
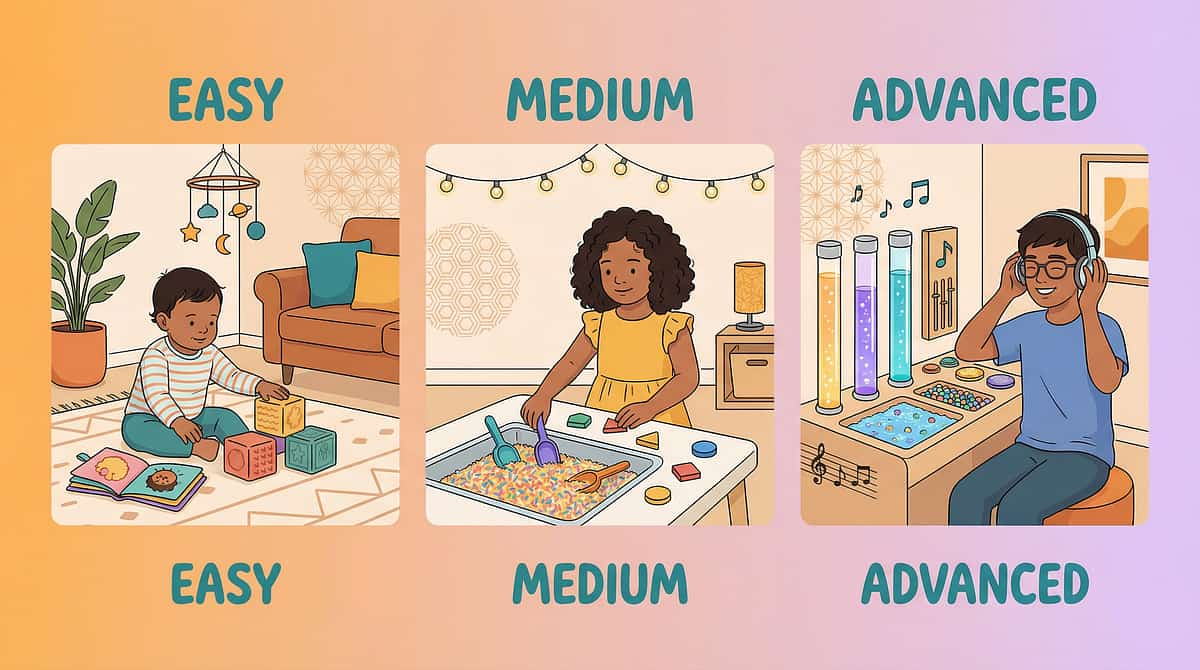
No Two Children Are Identical. Here's How to Adjust.
For Tactile SEEKERS (Hypo-Sensitive)
Use heavy, resistive, deeply textured materials — clay, resistive putty, weighted objects
Add proprioceptive pre-loading: 2 minutes of wall push-ups before the session
Embed more academic content — seekers can handle complexity layered onto rich sensory input
For Tactile AVOIDERS (Hyper-Sensitive)
Begin with tools (spoons, sticks, gloves) — indirect contact first
Progress to tolerated textures only (smooth, dry, at room temperature)
Never force hand contact — allow the approach to be child-initiated
Age-Based Adaptations
2–3 Years
Sensory exploration only — no academic embedding; pure regulation and play
3–5 Years
Simple sorting, stacking, pouring — basic concepts embedded lightly
5–8 Years
Full curriculum embedding — maths, literacy, science via materials
8–12 Years
Complexity, sequencing, project-based learning — multi-step construction
Bad Day Version: One material. No academic expectation. Child's lead only. 5 minutes maximum. Celebrate participation.
ACT IV | THE PROGRESS ARC
Week 1–2: The Tolerance Phase
15%
Phase Progress
Foundation being poured
Most parents expect transformation in week 1. What's actually happening in weeks 1–2 is the nervous system learning that this material is safe. That is the entire clinical goal of weeks 1–2.
✅ Reduced Refusal Latency
Child takes 30 seconds instead of 5 seconds to refuse. That's progress.
✅ Increased Proximity
Child sits near the materials even if not touching — that's approach behaviour.
✅ Duration Increase
Engagement goes from 1 minute to 2 minutes. That's 100% improvement.
✅ Reduced Distress
Child's protests are shorter or less intense. The nervous system is de-escalating its threat response.
"If your child tolerates the clay for 3 seconds longer this week than last week — that is measurable neurological progress. Write it in your log. It counts."
You may feel this is not working. You are wrong. You are in the foundation-pouring phase. The building cannot begin until the foundation is set.
Week 3–4: Neural Pathway Forming
40%
Phase Progress
Neural consolidation underway
🧠 Anticipatory Behaviour
Child moves toward the material space before the session is formally announced. The nervous system is now predicting — and predicting positively.
🧠 Preference Signals
Child begins reaching for one specific material from the set. The nervous system has identified its optimal sensory entry point.
🧠 Reduced Coaching Needed
Fewer prompts required to maintain engagement. Internal motivation is emerging from the consistent positive experience.
🧠 Spontaneous Communication
Child begins labelling, commenting on, or requesting during hands-on activity. Language emerges from regulated engagement.
By week 4, if the child is engaging for 10+ minutes with low resistance, it is clinically appropriate to add a second material, increase academic embedding, and increase session frequency from 3× to 5× per week. By this stage, most parents report feeling significantly more confident — you now know this child's sensory preferences, resistance signals, and reinforcer hierarchy.

Week 5–8: The Mastery Phase
75%
Phase Progress
Mastery criteria within reach
Mastery Criterion | Observable Indicator | |
Engagement Duration | 20+ minutes sustained hands-on engagement with minimal redirection | |
Independence | Child selects and initiates use of a preferred material without adult prompting | |
Academic Embedding | Child demonstrates the embedded concept with 80%+ accuracy | |
Generalisation | Skill demonstrated in at least 2 different settings (home + school OR home + clinic) | |
Maintenance | Skill persists across a 2-week period without daily structured practice |
🏆H-754 Mastery Unlocked when ALL 5 criteria are met on 3 consecutive measurement days. When achieved, advance to the next technique in the Domain H progression pathway.

You Did This.
Eight weeks ago, your child couldn't tolerate clay on their fingers. Today, they built a village with it.
You did not just teach your child to use materials. You rewired their nervous system's relationship with the sensory world. You proved that their home is a therapy centre. You proved that you are a clinical force in their development.
By completing H-754: Hands-On Learning, your child has now established a reliable sensory entry point for new learning, an expanded tolerance for tactile input, at least one embedded academic skill through kinesthetic encoding, and a home-based protocol they will carry forward into every domain.
🎉 Tonight
Let your child choose dinner
📸 Photo Prompt
Take a photo of your child with the material they mastered — add it to your progress journal
📤 Share
Post in your Pinnacle parent community with #H754Mastery
You arrived at Card 01 watching a child push away a worksheet. You leave here watching a child reach for clay. That is the journey.

Even in Progress: Know These Warning Signs
🚨 Flag 1: Self-Injurious Behaviour During or After Sessions
Head-banging, biting self, hitting self — particularly if this increases during hands-on sessions. The sensory input may be exceeding the nervous system's regulatory capacity.
Action: Pause immediately. Consult OT before resuming.
Action: Pause immediately. Consult OT before resuming.
🚨 Flag 2: Significant Regression in Other Skills
If a previously mastered skill (toileting, sleep, feeding) deteriorates during H-754 implementation, the cumulative sensory load may need assessment.
Action: Log and call 9100 181 181.
Action: Log and call 9100 181 181.
🚨 Flag 3: Persistent Skin Reactions to Materials
Redness, rash, or persistent avoidance of a specific material — possible allergic or sensory sensitisation response.
Action: Discontinue that specific material. Report to your OT.
Action: Discontinue that specific material. Report to your OT.
🚨 Flag 4: Seizure Activity
Any episode of loss of consciousness, uncontrolled body movement, or absence episode during or after high-sensory sessions.
Action: Emergency medical attention immediately. Inform NeuroDev physician.
Action: Emergency medical attention immediately. Inform NeuroDev physician.
🚨 Flag 5: Distress Worsening Week Over Week
If by week 4 the child shows more resistance, more distress, and less engagement than week 1 despite protocol adherence, the technique may need modification or temporary discontinuation.
Action: Do not push through. Book a teleconsultation.
Action: Do not push through. Book a teleconsultation.
"You see this child every day. If something feels wrong, pause and ask. Your clinical instinct as a parent is data."
Escalation Pathway: Self-resolve (1 session) → Teleconsult (9100 181 181) → Clinic Visit → NeuroDev Assessment
More Techniques in Domain H: Hands-On Learning
Browse techniques that use materials you may already own from H-754.
Code | Technique Name | Difficulty | Materials You Own | |
H-750 | Sensory Bin Learning Foundations | 🟡 Intro | ✅ Sensory bins | |
H-751 | Math Manipulatives for Number Sense | 🟡 Intro | ✅ Counting objects | |
H-752 | Letter Building with Tactile Materials | 🟡 Intro | ✅ Letter tiles, sand | |
H-755 | Project-Based Learning for STEM Concepts | 🟠 Core | ✅ Building sets | |
H-758 | Dramatic Play for Social Cognition | 🟠 Core | ✅ Role-play kits | |
H-760 | Abstract Concept Embodiment | 🔴 Advanced | ✅ Manipulatives |
🏠"You already own materials for 6 of these techniques."
→ Browse all Domain H Techniques → Browse all 70,000+ Techniques by Domain
→ Browse all Domain H Techniques → Browse all 70,000+ Techniques by Domain

ACT V | COMMUNITY & ECOSYSTEM
Families Who Started Where You Are
Priya, Mother of Arjun, 5 years — Hyderabad
Before H-754: Arjun would not sit at the table during homework. Any worksheet attempt ended in meltdown within 90 seconds. He was labelled "non-compliant" at school. 6 weeks later: Introduced counting bears for maths and letter tiles in a rice bin for reading. By week 3, Arjun was requesting "rice letters" before dinner. By week 6, he was counting to 20 using objects he'd gathered himself. He was reintegrated into mainstream class with a hands-on learning accommodation plan.
"I was told he couldn't learn. But he was learning all along — just not in their language. H-754 gave us his language."
Rajesh & Sunita, Parents of Meera, 7 years — Bangalore
Before H-754: Meera had mastered all skills individually at the clinic but showed none at home or school. The disconnect was causing significant family stress. H-754 Protocol: Replicated the clinic's manipulative-based maths approach at home using dried lentils, buttons, and a muffin tin (₹0 total cost). Meera's home data matched clinic data within 3 weeks. Generalisation gap closed. School teacher trained via the family guide.
"We had the therapy and no idea how to bring it home. This page told us exactly what to do — with things from our own kitchen."
From the OT's Notes on Arjun: "Arjun's profile showed strong proprioceptive seeking with moderate tactile defensiveness to wet textures. The rice bin was ideal — deep proprioceptive input without wet contact. We scaffolded from bin to table over 4 weeks. The compliance wasn't the breakthrough. The motivation was."
You Don't Have to Do This Alone
📱 Hands-On Learning Parent WhatsApp Group
Join 3,400+ parents across India navigating Domain H together. Share wins, ask questions, and find people who understand exactly what you are living.
→ Join H-754 Parent Community
→ Join H-754 Parent Community
💬 Pinnacle Parent Forum — Domain H
Ask questions, share wins, troubleshoot sessions with parents who have been exactly where you are.
→ Visit the Forum
→ Visit the Forum
📍 Local Pinnacle Parent Meetups
Monthly meetups at your nearest Pinnacle centre — meet therapists, other families, and see hands-on learning demonstrations live.
→ Find Your Nearest Centre
→ Find Your Nearest Centre
🤝 Peer Mentoring
Request a connection with an experienced parent (3+ months ahead of you in the H-754 journey) for one-on-one support.
→ Request a Mentor
→ Request a Mentor
"Your 6-week journey will become another family's breakthrough story. Consider sharing your experience — it matters more than you know."
📞FREE National Helpline: 9100 181 181 | 16 languages | Every day
Home + Clinic = Maximum Impact
Your home protocol and your clinic sessions are not competing — they are complementary. The home provides frequency and generalisation; the clinic provides clinical precision and progression. Together, they create the most powerful intervention environment possible.
Occupational Therapist
Material selection for your child's sensory profile
Speech-Language Pathologist
Language embedding in hands-on activities
ABA / BCBA Therapist
Behaviour and reinforcement design
Special Educator
Curriculum alignment and IEP goals
NeuroDev Paediatrician
Medical co-management of sensory profile
Find a Centre
→ Find Your Nearest Pinnacle Centre (70+ centres across India)
🖥️ Teleconsultation
Our specialists cover H-754 protocol guidance via video call. Families from 70+ countries have been served through Pinnacle Teleconsult.
📞FREE: 9100 181 181 — 16 languages. Immediate triage.
Insurance and funding pathways available in select states. Ask our helpline for guidance on government therapy scheme coverage.
Preview of 9 materials that help with hands on learning Therapy Material
Below is a visual preview of 9 materials that help with hands on learning therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Watch: 9 Materials That Help With Hands-On Learning
🎬 Reel Title
9 Materials That Help With Hands-On Learning
📋 Reel ID
H-754 | Row 910 | Domain H
👩⚕️ Presenting Therapist
Pinnacle Occupational Therapist, Sensory Integration Specialist
This page was built from and for the H-754 Reel. Everything you have read here is the clinical depth behind the 9 materials shown in the video. Watch the Reel to see the materials in action, then use this page to execute the full protocol at home.
You've read the science. Now watch the hands. Then do the session. Text + Video + Practice = the deepest learning pathway for parents, just as it is for children.
Video modelling is an evidence-based practice for autism (NCAEP, 2020). Watching a therapist demonstrate activates the same mirror neuron networks that hands-on execution does — priming your motor memory for the session.
📞 Questions about what you saw? Call 9100 181 181 — FREE
📞 Questions about what you saw? Call 9100 181 181 — FREE