9 Materials That Help With Gravitational Insecurity
A clinician-backed guide for parents, caregivers, and therapists supporting children ages 2–6 who fear movement, heights, and losing their footing — with at-home materials, exact scripts, and an 8-week progress roadmap.
Act I — Recognition
The Kitchen Floor Moment
"She just fell apart. We were playing on the kitchen floor and I tilted her back — nothing dramatic — and she screamed like I'd dropped her off a building. I thought I'd hurt her. I hadn't. That was the moment I knew something was different."
If you've lived a version of this scene, you are not alone. Gravitational insecurity is one of the most misread sensory patterns in early childhood — dismissed as drama, labeled as clinginess, or attributed to a "difficult" temperament. It is none of those things.
What you witnessed is a nervous system responding to movement the way most nervous systems respond to genuine danger. The fear is real, the distress is real — and, crucially, there is a structured, evidence-informed path through it.
What Caregivers Often Hear
- "She's just being dramatic."
- "He'll grow out of it."
- "She needs more confidence."
- "Boys aren't usually like this."
What's Actually Happening
The vestibular system is over-signaling threat in response to linear or gravitational movement — a neurological pattern, not a behavioral choice.

Act I — Prevalence
You Are Not the Only Family Going Through This
Gravitational insecurity (GI) affects an estimated 5–15% of children with sensory processing differences — a subset large enough that pediatric occupational therapists across the country see it weekly. Because GI often co-occurs with anxiety, ASD, and developmental coordination disorder, it is frequently underidentified as a standalone vestibular pattern.
Prevalence in SPD
Children with sensory processing differences who show GI patterns
Peak Age Window
Years of age when GI is most identifiable and most treatable
Protocol Duration
Typical structured intervention arc with observable milestone shifts
PubMed Citations
Peer-reviewed studies underpinning the Pinnacle consortium approach

Act I — Neuroscience
What's Happening Inside the Vestibular System
The Plain-English Version
Deep inside the inner ear sit two tiny organs — the utricle and saccule — packed with hair-like cells that detect gravity and linear movement. In a child with gravitational insecurity, these sensors are hypersensitive: they transmit "DANGER" signals at intensities that the child's nervous system cannot quickly regulate.
The brain's threat-detection circuit (the amygdala) acts on that signal before the prefrontal cortex — the reasoning brain — has any say. This is why telling a child to "calm down" during a GI moment does not work. Their cortex isn't running the show yet.
The Clinical Picture
Research published in PMC11506176 and PMC10955541 confirms that vestibular hypersensitivity produces measurable cortical over-arousal, elevated cortisol, and avoidance behavior patterns that, without intervention, tend to compound across developmental stages rather than resolve spontaneously.
The good news: the vestibular system is highly neuroplastic in the 2–6 window. Graded, predictable, child-led movement input consistently rebuilds the brain's tolerance threshold. That is exactly what this protocol is designed to deliver.
Act I — Development
The Developmental Timeline of Gravitational Insecurity
GI does not appear out of nowhere — it follows a recognizable developmental arc. Understanding where your child sits on this timeline helps you calibrate the protocol and set realistic expectations for progress.
Ages 2–3
Avoidance of slides, swings, and being lifted. Distress at diaper changes or tilting backward. Often read as "clingy phase."
Ages 3–4
Refusal to climb playground equipment. Meltdowns at transitions involving height or speed. Peer comparison begins to create secondary anxiety.
Ages 4–5
Avoidance strategies become more sophisticated. Child narrates fear verbally. OT referral window — highest treatment responsiveness.
Ages 5–6
School entry amplifies demands. PE, seating transitions, and stairs create daily friction. Intervention remains highly effective at this stage.
Act I — Evidence
The Research Foundation
This protocol is grounded in Level II–III evidence — the highest available for sensory-based interventions in early childhood. The Pinnacle consortium references six peer-reviewed sources, three clinical practice guidelines, and the NCAEP 2020 Evidence-Based Practices report.
PMC11506176
Vestibular hypersensitivity and cortical arousal: measuring real-time neural over-response in children ages 3–7 using EEG + salivary cortisol markers.
PMC10955541
Longitudinal outcomes of sensory-based OT: gravitational insecurity subscore improvements at 8 and 16 weeks with graded movement protocols.
NCAEP 2020
National Clearinghouse on Autism Evidence and Practice: sensory integration listed as an evidence-based practice for children birth–22 with ASD.
Padmanabha 2019
Indian Journal of Pediatrics: culturally adapted sensory diet interventions in joint household settings — foundational for the DIY Indian home substitutes in this protocol.
Act II — Definition
What Is Gravitational Insecurity?
Gravitational insecurity (GI) is a vestibular processing disorder in which a child experiences excessive, disproportionate fear in response to movement against gravity — particularly changes in head position, loss of foot contact with the ground, or unexpected linear movement.
Unlike simple fear of heights, GI is a sensory-neurological pattern, not a learned phobia. The child's nervous system is not misinterpreting danger emotionally — it is generating a genuine physiological alarm response that bypasses rational thought. Clinical hallmarks include: death-grip holding during any lift, rigid body posture on uneven surfaces, avoidance of backward tilting, and disproportionate distress when feet leave solid ground — even momentarily.
GI is formally assessed using the Sensory Integration and Praxis Tests (SIPT) and the Sensory Processing Measure (SPM-2). A diagnosis supports insurance coverage for OT services in most U.S. states.

Act II — Disciplines
The 5 Pinnacle Consortium Disciplines
The Pinnacle consortium's approach to GI draws on five clinical disciplines working in structured collaboration — each contributing a distinct lens to assessment, material selection, and session design.
Occupational Therapy
Primary lead. Sensory integration, material grading, and functional outcome tracking via the GPT-OS® Vestibular Processing Index.
Speech-Language Pathology
Co-regulates language processing affected by vestibular over-arousal; scripts child and caregiver communication during sessions.
Developmental Pediatrics
Medical gatekeeping; rules out otologic causes; manages co-occurring anxiety pharmacologically when indicated.
Child Psychology
Parent-child attachment lens; secondary anxiety management; family systems coaching for joint household contexts.
Physiotherapy
Postural stability, core strengthening, and proprioceptive baseline — the physical scaffold that makes vestibular input tolerable.

Act II — Targets
Primary, Secondary & Tertiary Treatment Targets
Primary Targets
- Reduce vestibular threat response threshold
- Increase tolerance for linear movement
- Establish predictable movement routines
- Build foot-to-ground confidence
Secondary Targets
- Reduce avoidance behavior at playground and PE
- Decrease caregiver rescue-seeking frequency
- Improve co-regulation window duration
- Support peer participation in group movement
Tertiary Targets
- Generalize gains to community settings
- Equip grandparents/educators with scripts
- Reduce secondary anxiety around movement
- Feed data to GPT-OS® Vestibular Processing Index

Act II — Materials Overview
The 9 Canon Materials at a Glance
Each material below has been selected by the Pinnacle consortium based on three criteria: evidence of vestibular input specificity, accessibility in diverse household settings, and safe use without a therapist present when the safety gate protocol is followed. U.S. retail price ranges are provided; Indian household DIY substitutes follow in the next card.
# | Material | Primary Mechanism | U.S. Price Range | |
1 | Therapy Ball | Slow linear vestibular input in prone/supine | $20–$60 | |
2 | Compression Vest | Proprioceptive grounding before movement | $35–$80 | |
3 | Weighted Blanket | Deep pressure calming before/after movement | $40–$120 | |
4 | Platform Swing | Slow, predictable linear swing — lowest threat | $80–$200 | |
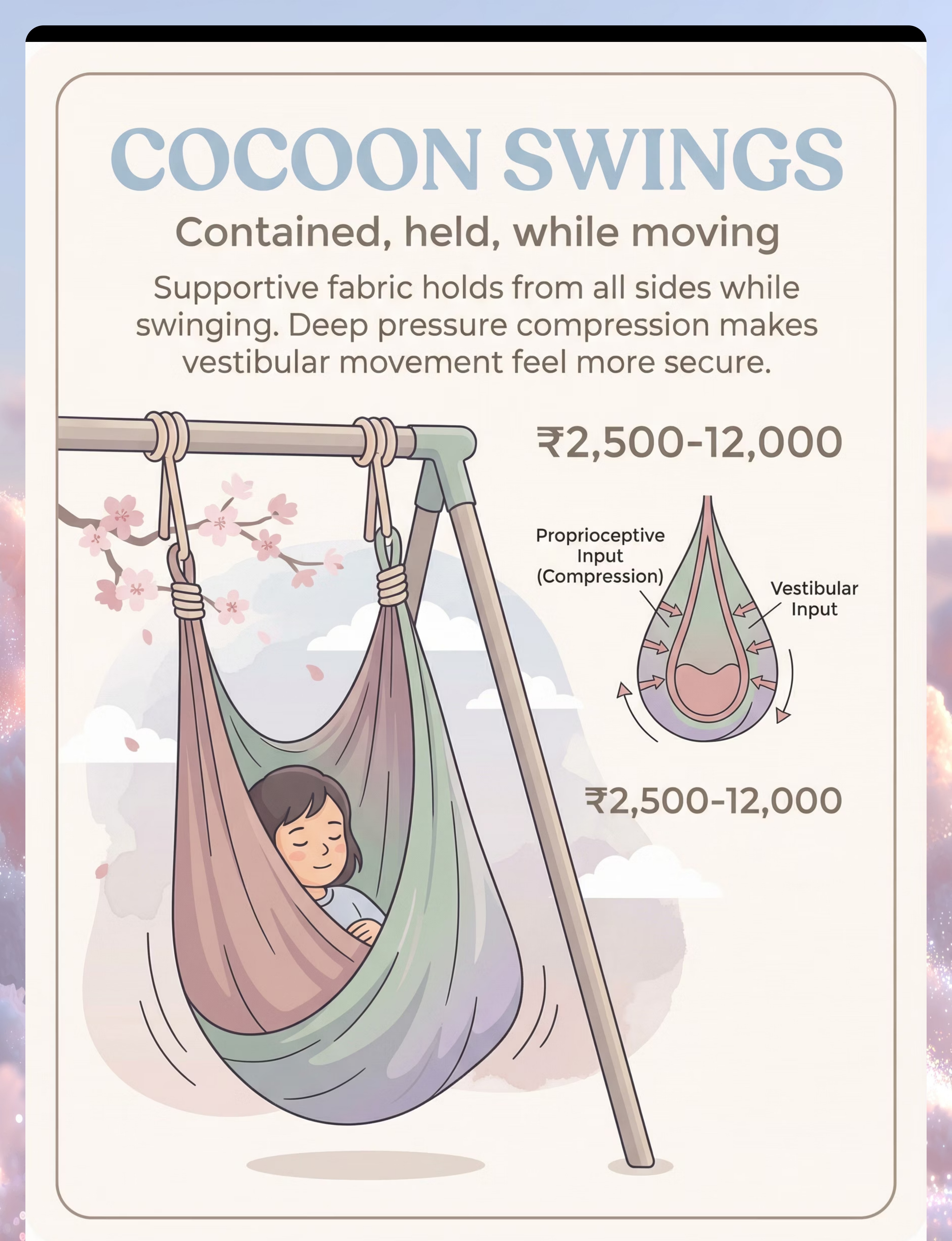
5 | Hammock Swing | Cocooning + gentle linear rock | $60–$150 | |
6 | Scooter Board | Prone/seated propulsion on flat surface | $30–$70 | |
7 | Balance Board | Graded tilt challenge on stable base | $40–$100 | |
8 | Trampoline (mini) | Vertical input with foot-ground return | $50–$150 | |
9 | Sensory Tunnel | Proprioceptive + vestibular in enclosed crawl | $25–$60 |
Material 1
Material 1: Therapy Ball
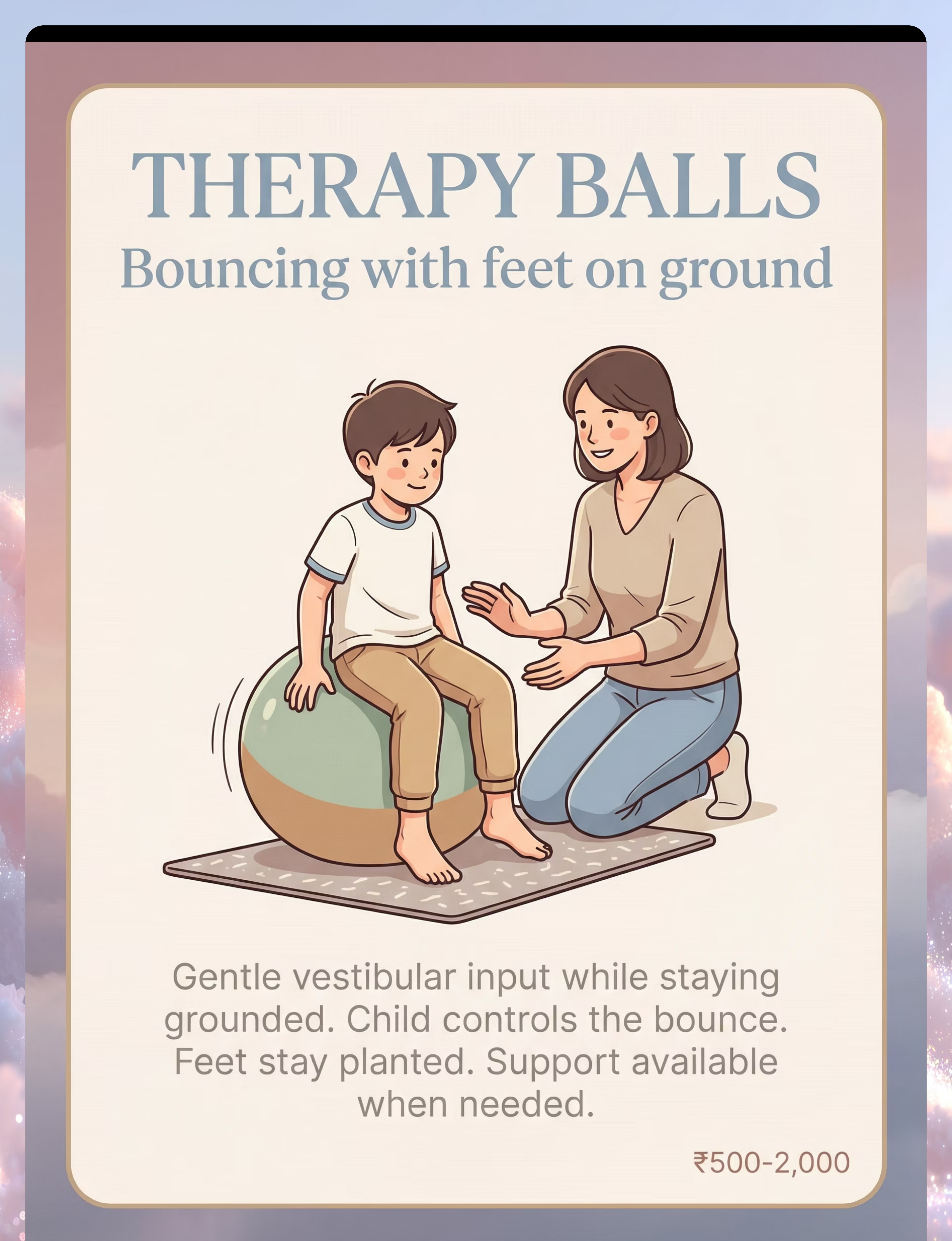
Why It Works
The therapy ball delivers slow, controlled linear vestibular input in both prone (belly down) and supine (back down) positions. Because the child's feet remain close to the ground and the caregiver controls all movement, it is the lowest-threat active vestibular tool in the canon.
First-Session Protocol
- Child sits on ball, feet flat, caregiver holds hips. Zero movement. 60 seconds.
- Tiny forward-back rocks — 2 cm amplitude. Child gives thumbs-up signal to continue.
- Increase to 5 cm only if child requests. Maximum 3 minutes first session.
DIY Indian Substitute
A firm rubber football (size 5) partially deflated, or a rolled razai under the child's belly for prone rocking.
Safety: Never tilt ball backward past 30° without a mat underneath and a second adult present.

Material 2
Material 2: Compression Vest
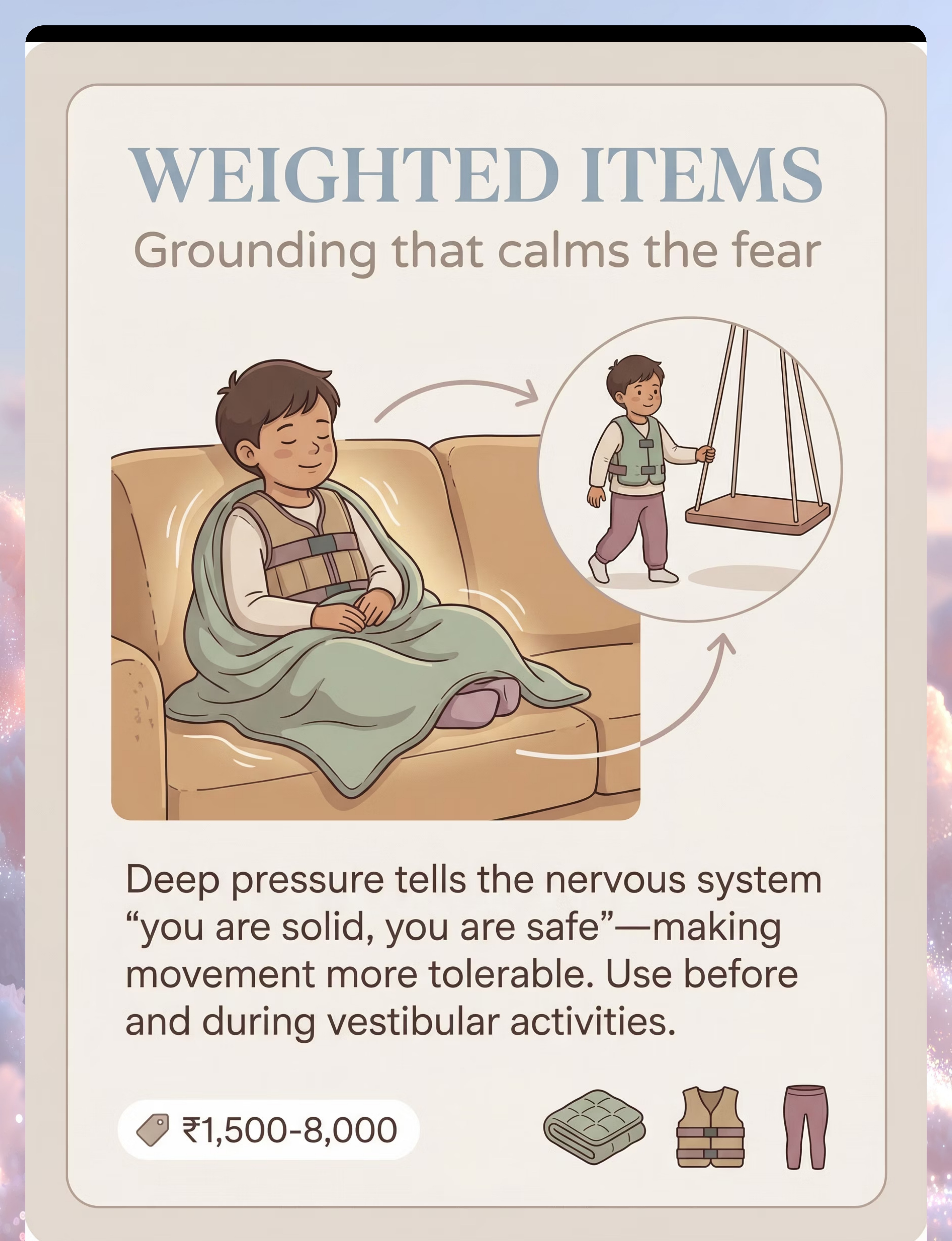
Why It Works
Proprioceptive input — pressure applied to joints and muscles — is the nervous system's most reliable down-regulator before vestibular challenge. A compression vest worn for 20 minutes before movement activities measurably reduces cortisol response and narrows the threat window.
First-Session Protocol
- Introduce vest as "superhero armor" or "hug shirt" — child's framing, not yours.
- Wear during a preferred sedentary activity (drawing, puzzles) for 15–20 minutes.
- Begin vestibular activity while vest is still on. Remove 10 minutes after activity ends.
DIY Indian Substitute
A fitted sleeveless undershirt (baniyan) one size smaller than usual, layered under regular clothing. Ensure no restriction to breathing or arm range of motion.
Wear schedule: Maximum 20 minutes on, then 20 minutes off. Never worn during sleep.

Material 3
Material 3: Weighted Blanket

Material 4
Material 4: Platform Swing
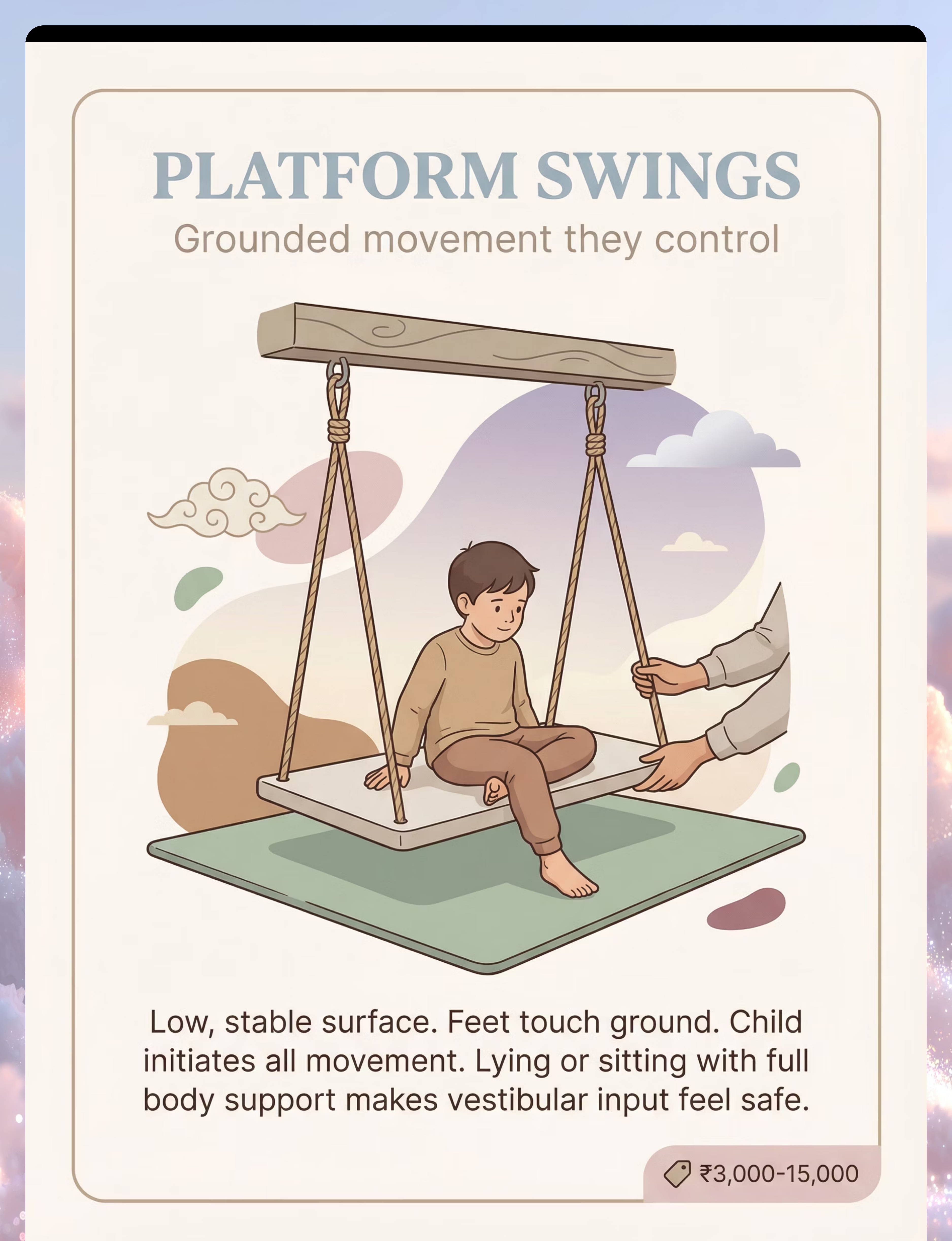
Why It Works
The platform swing is the gold-standard entry point for vestibular habituation in GI treatment. Its large, flat surface allows the child to sit, prone-lie, or kneel — all with maximum body contact and minimal height. Linear, front-to-back motion in small arcs is the least threatening vestibular input the swing canon offers.
First-Session Protocol
- Introduce the swing stationary. Child explores surface with hands and feet — no movement.
- Child sits on swing with caregiver beside (not pushing). Gentle 5 cm forward-back arc, child-initiated by leaning.
- Increase arc by 5 cm per session only with verbal or gestural child consent.
- Maximum height: feet remain within 6 inches of ground for first 4 sessions.
DIY Indian Substitute
A traditional jhula (wooden plank swing) mounted low — maximum 8 inches off the floor for first-month sessions. Ensure mounting hardware is rated for 3× child's body weight.
Pro tip: Singing a slow, predictable song while swinging gives the brain an auditory anchor that reduces threat perception. "Row, Row, Row Your Boat" at half-speed works well.

Material 5
Material 5: Hammock Swing

Material 6
Material 6: Scooter Board
Why It Works
The scooter board is the protocol's primary tool for self-generated linear movement — a critical distinction. When the child controls their own movement trajectory, the brain's predictive processing system is engaged rather than bypassed, dramatically reducing threat response. Prone propulsion (belly-down, pushing with hands) also activates the vestibular-proprioceptive convergence zone.
First-Session Protocol
- Let child enter hammock independently (or with minimal assist). Do not lift.
- Introduce board on carpet (slower, safer) before smooth floors.
- Child sits on board (not prone) initially. Caregiver provides gentle push from behind — child can see direction of travel.
- Transition to prone only when child requests — never prompt it.
- Create a predictable "track" using tape or cushions so child knows the route.
DIY Indian Substitute
A smooth wooden cutting board or flat-bottom plastic tray on a marble floor with a towel underneath for friction control. Ensure no sharp edges.
Age adaptation (2–3 yrs): Use seated position only. Prone board work begins at age 3.5+ or with therapist clearance.

Material 7
Material 7: Balance Board
Why It Works
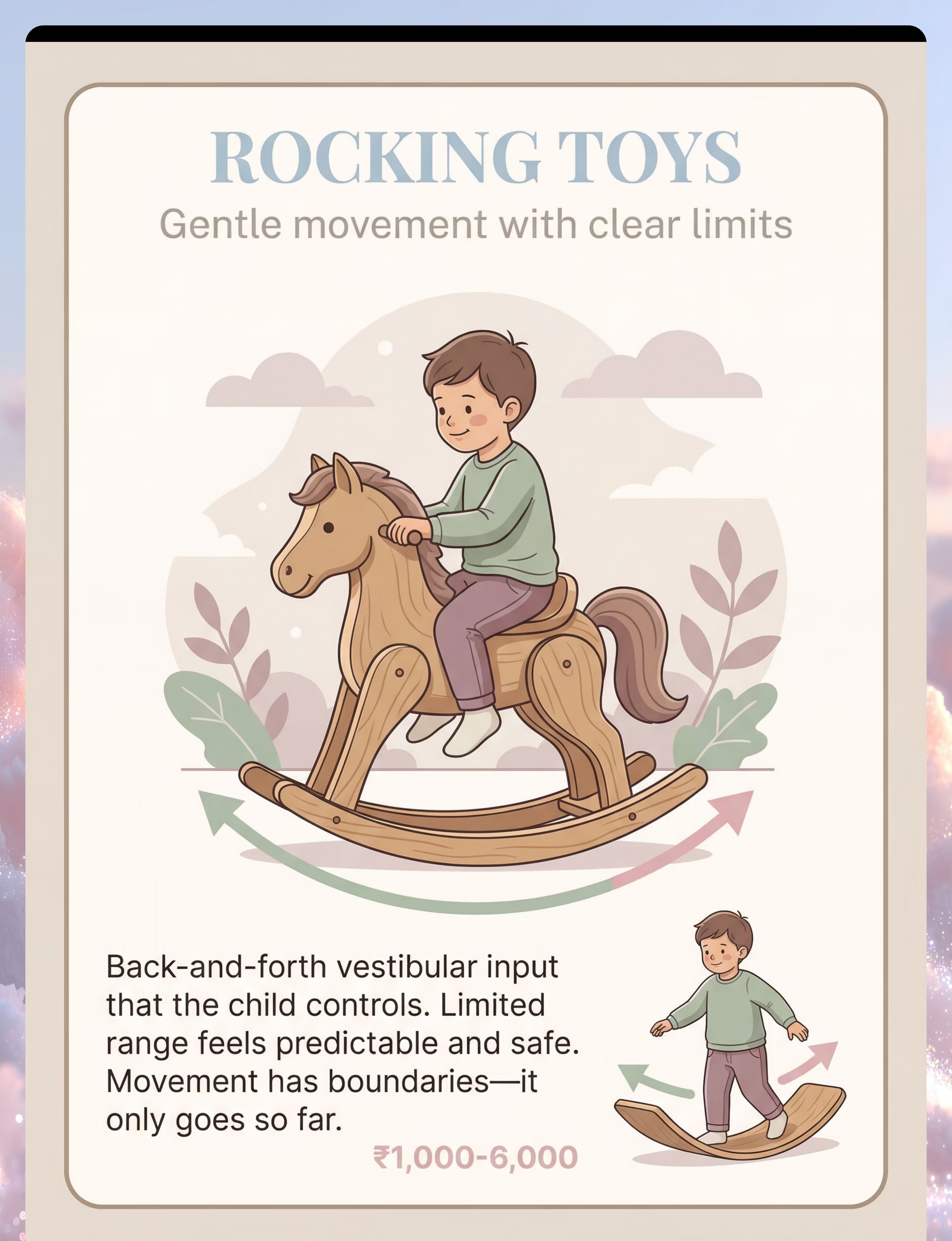
The balance board provides graded tilt challenge on a predictable, stable base. Unlike swings, the child's feet never leave the surface — this single feature makes it accessible for children who refuse all elevation-based activities. The rocking motion activates the utricle (linear detection) and forces the cerebellum and vestibular system to negotiate real-time postural adjustment.
First-Session Protocol
- Place board on carpet to limit tilt range. Child stands on still board — no movement. 60 seconds.
- Caregiver demonstrates tiny side-to-side tilt. Child watches, then tries with both hands held.
- Reduce hand support by one finger at a time across sessions.
- Progress to smooth floor (greater tilt) only at Week 4+.
DIY Indian Substitute
A smooth wooden board (30×60 cm) resting on a firm cylindrical rolling pin (belan). Monitor for slipping; place on a yoga mat.

Material 8
Material 8: Mini Trampoline
Why It Works
The mini trampoline is the protocol's most advanced tool — introduced only at Week 5+ after safety gate clearance. It delivers vertical vestibular input with the critical safety feature that the child's feet always return to a predictable surface. This "ground return guarantee" is what makes vertical bouncing tolerable for GI children when free-fall activities remain completely off-limits.
Jumping also generates intense proprioceptive joint-compression input — a powerful self-regulating mechanism that many GI children discover and self-administer spontaneously once introduced.
First-Session Protocol
- Begin with child standing still on trampoline surface — no jumping. Feel the give of the surface.
- Caregiver demonstrates slow, low bouncing. Child observes.
- Child bounces with both hands held by caregiver. Maximum 2 cm initial amplitude.
- Sessions capped at 5 minutes until Week 7.
DIY Indian Substitute
A firm mattress on the floor (not elevated on a bed frame) for first exposures. Ensure surrounding floor is clear of furniture for fall safety.

Material 9
Material 9: Sensory Tunnel
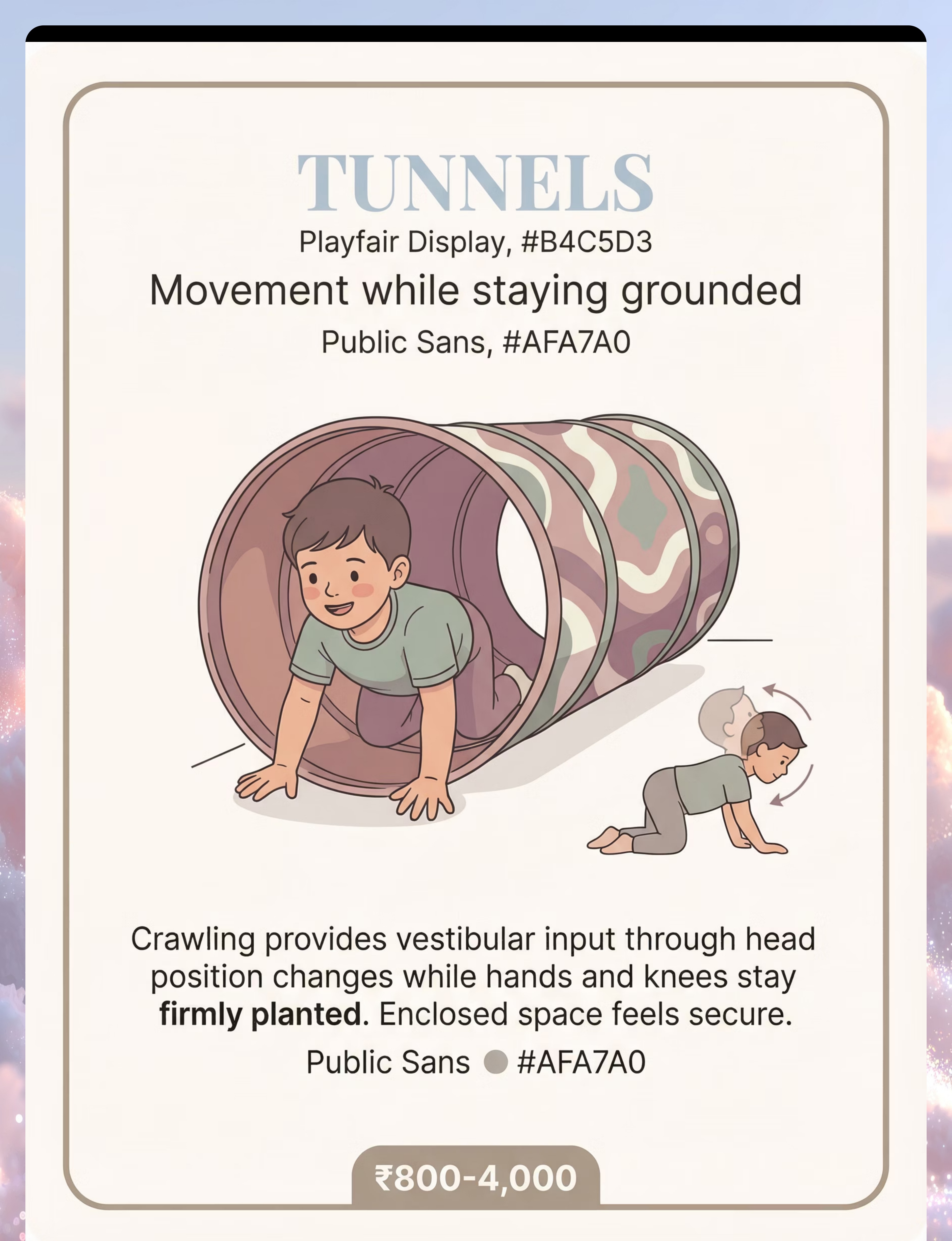
Why It Works
The sensory tunnel is the protocol's proprioceptive-vestibular convergence tool. Crawling through a fabric tunnel activates the neck, shoulder, and hip joints (deep proprioception) while simultaneously engaging the vestibular system through head-level changes and directional changes in the crawl path. The enclosed space also reduces visual overwhelm — a secondary threat driver in GI children.
Because the child controls speed and direction completely, the brain's predictive processing is fully online — making this one of the most neurologically safe high-input activities in the canon.
First-Session Protocol
- Lay tunnel flat. Place a preferred toy or snack at the far end as motivation.
- Child explores entry end only — no pressure to go through. 2–3 minutes.
- First full pass: caregiver talks or sings from the exit end throughout.
- Progress to curved tunnel placement at Week 3+.
DIY Indian Substitute
A row of chairs draped with bedsheets or a sari, forming a fabric-walled crawl corridor approximately 80 cm wide.

Act II — Safety
Red / Amber / Green Safety Gating
Before every session, run this three-level safety check. Any single Red flag stops the session. Amber flags require modification. Green on all criteria means proceed as planned.
🔴 Red — Stop Session
- Child is ill (fever, ear infection, respiratory symptoms)
- Child has had a fall or head impact in the past 48 hours
- Child is in active emotional meltdown before session begins
- No second adult available for Materials 4, 5, or 8
- Equipment inspection reveals wear, loose hardware, or instability
🟡 Amber — Modify Session
- Child slept less than 8 hours (reduce session length by 50%)
- Child is hungry or thirsty (feed/hydrate, wait 15 minutes)
- Grandparent or unfamiliar adult is the only available caregiver
- Child shows mild reluctance — offer choice between two materials
- Space is smaller or louder than usual — use lower-input materials only
🟢 Green — Proceed
- Child is healthy, well-rested, and fed
- Familiar caregiver present and briefed on today's protocol
- Equipment inspected and cleared
- Space prepared per room setup guidelines
- Child has expressed willingness (verbal or gestural)

Act II — Environment
Room Setup for Joint Household & Grandparent Contexts
Most GI protocol literature assumes a nuclear household with a dedicated therapy room. The Pinnacle consortium has specifically adapted room-setup guidance for joint Indian household contexts — shared living rooms, grandparent involvement, and limited dedicated space.
Minimum Space
3×3 meters of clear floor. Move one piece of furniture if needed. A yoga mat defines the "session zone."
Noise Level
TV off during sessions. If household noise cannot be reduced, use soft instrumental background music to mask unpredictable sounds.
Grandparent Role
Grandparents may observe and provide quiet emotional support. Script for grandparents: "You're doing so well. Take your time." Avoid physical redirection.
Siblings
Siblings under 8 leave the session space. Siblings 8+ may participate as "session helpers" with a specific role (equipment holder, song leader).
Act III — Protocol
The 6-Step Session Protocol
Every home session follows this six-step sequence. Do not skip or reorder steps — the sequence is neurologically designed. Steps 1 and 6 are non-negotiable anchors. Steps 2–5 are adapted to the child's daily window.
Total session time: 25–35 minutes for children ages 4–6; 15–20 minutes for children ages 2–3. Frequency: 4–5 sessions per week during the 8-week protocol arc. Daily is fine; never push for a session on a Red-flag day.

Act III — Step 1
Step 1: Safety Gate Check
Run the Red/Amber/Green gate before any equipment is visible to the child. Children with GI are highly attuned to anticipatory cues — seeing the therapy ball on the floor before you've decided whether today is a Green day creates pre-session arousal that undermines the session before it begins.
Complete your gate check in a separate room or before the child enters the session space. If the day is Red, offer a completely non-movement alternative activity with the same warm, connected caregiver presence. Do not express disappointment or urgency about the missed session.
Caregiver Script — Red Day
"Today is a rest day — our bodies sometimes need those. Want to read together / do a puzzle / help me in the kitchen?"
Caregiver Script — Amber Day
"We're going to do a quieter version today. You pick — the tunnel or the blanket?"
What to Check
- Child health status
- Sleep quality last night
- Last meal timing
- Equipment condition
- Second adult availability
- Space preparation complete
- Your own regulation state
Time Required
2–3 minutes. Build it into your pre-session routine — make a cup of tea while you run through the checklist.

Act III — Step 2
Step 2: Proprioceptive Primer

Act III — Step 3
Step 3: Child-Led Material Choice
Present two material options — never one (removes choice) and never more than two (creates decision overwhelm). Both options should be appropriate for today's Amber or Green rating. Let the child choose without commentary on their selection.
How to Present the Choice
Hold up or point to two materials: "Do you want the ball or the tunnel today?" Pause. Wait up to 30 seconds for a response. If no response, default to the lower-input option. Never say "Are you sure?" after the child chooses.
Why Child Choice Matters Neurologically
Agency activates the prefrontal cortex — the reasoning brain — before the activity begins. A child who chose the activity has already begun to recruit executive function as a counterweight to the amygdala's threat signal. This is not just therapeutic philosophy; it is measurable in cortisol levels.
Tracking Choices Over Time
Log which material the child chose each session in the 3-question session log. Patterns (e.g., always choosing tunnel on Mondays, always avoiding swing) feed directly into the GPT-OS® Vestibular Processing Index and inform Week 5 protocol adjustments.

Act III — Step 4
Step 4: Graded Vestibular Activity
The Grading Principle
Every session, the vestibular challenge is graded upward by the smallest meaningful increment — and only when the child signals readiness, not on a predetermined schedule. This is the core mechanism of the protocol. Forcing increments produces avoidance; following the child's readiness signals produces neuroplastic change.
Readiness Signals to Watch For
- Green signals: Relaxed body, eye contact, smiling, requesting "more," leaning into movement
- Amber signals: Slightly tense body, quiet but compliant, looking away briefly — hold current level
- Red signals: Rigid body, reaching for caregiver, crying, saying "no" or "stop" — step back one level immediately
Duration
8–12 minutes for ages 4–6. 5–8 minutes for ages 2–3. Stop before the child shows fatigue — ending on a positive state is more neurologically valuable than a longer session that ends in distress.
Caregiver Script — During Activity
"You're doing it. I'm right here."
"Tell me when you want more or when you want to stop."
"Your body is learning something new right now."
"I've got you. I won't let go until you say."
What NOT to Say
- "You're fine, it's not scary."
- "Just a little more, come on."
- "Your sister does this easily."
- "Be brave."

Act III — Step 5
Step 5: Reinforcement & Session Log
Reinforcement Menu
Reinforcement happens immediately after the activity ends — not as a bribe before it. Choose one reinforcer per session from the menu below, rotating to maintain salience. The reinforcer should celebrate effort and presence, not performance outcomes.
Social
"I saw how brave you were today. You tried something hard."
Activity
5 minutes of a preferred play activity chosen by the child.
Sensory
Weighted blanket time, a preferred texture toy, or a calm sensory bin.
Token
A sticker or stamp on a visual progress chart the child can see building over time.
The 3-Question Session Log
Complete immediately after reinforcement, while observations are fresh. Takes under 2 minutes. Feeds directly into the GPT-OS® Vestibular Processing Index.
Q1: Which material did the child choose, and what was the starting intensity level today?
Q2: What was the highest level reached? What signal indicated readiness to progress (or stop)?
Q3: Rate the session overall: Green (child ended calm and positive), Amber (neutral/mixed), or Red (ended in distress).
Q2: What was the highest level reached? What signal indicated readiness to progress (or stop)?
Q3: Rate the session overall: Green (child ended calm and positive), Amber (neutral/mixed), or Red (ended in distress).
Seven consecutive Green sessions = milestone review with your OT. Three consecutive Red sessions = schedule a protocol adjustment call.
Act III — Step 6
Step 6: Cool-Down Ritual
The cool-down ritual is the most underrated component of the protocol — and the one most frequently skipped. It is not optional. The vestibular system takes 15–20 minutes to fully return to baseline after active input. A structured cool-down accelerates this return and embeds a sense of narrative completion that the child's memory encodes as "this activity ends well."
Move to the Cool-Down Space
A corner or spot designated specifically for after-session time. Consistency of location signals transition to the nervous system.
Offer Proprioceptive Anchor
Weighted blanket, compression vest, or a firm hug — child's choice. Minimum 5 minutes.
Quiet Co-Regulation Activity
Read together, listen to soft music, or do a simple puzzle. Caregiver is present and calm — no screens.
Verbal Closing
Caregiver says: "Session done for today. You worked hard. I'm proud of you." Same words every session — predictability anchors safety.
Act IV — Progress
The 8-Week Progress Arc
The Pinnacle consortium's longitudinal data (PMC10955541) describes three observable milestone clusters across an 8-week structured protocol. Progress is rarely linear — expect two steps forward and one step back. The arc below represents the median trajectory, not a rigid schedule.
1
Weeks 1–2: Foundation
15% threshold shift. Child tolerates Materials 1–3 without distress. Proprioceptive primer is accepted reliably. First session log shows more Green than Red.
2
Weeks 3–4: Expansion
40% threshold shift. Child begins requesting sessions independently. Materials 4–6 introduced. Avoidance behavior in daily life decreases measurably — first playground or PE gains.
3
Weeks 5–6: Integration
60% threshold shift. Child generalizes skills to novel movement contexts. Materials 7–9 introduced. Peer movement participation increases. Caregiver rescue-seeking frequency drops.
4
Weeks 7–8: Consolidation
75% threshold shift. Child self-initiates movement challenges. Cool-down ritual becomes self-regulated. Protocol transitions to maintenance (2× weekly) and Reel A-096 progression.
Act IV — Milestones
Observable Milestone Markers by Week
Use these observable markers — not standardized test scores — to track real-world progress between OT appointments. If your child hits a milestone early, do not accelerate the protocol; let them consolidate before progressing.
15%
Week 2 Milestone
Child accepts therapy ball and compression vest without protest on 3 consecutive days
40%
Week 4 Milestone
Child requests a session material independently at least twice in one week
60%
Week 6 Milestone
Child attempts a previously avoided playground activity with caregiver nearby but not holding
75%
Week 8 Milestone
Child initiates and completes a cool-down ritual independently after any movement activity
Act IV — Red Flags
Red Flags & Escalation Pathway
When to Pause the Protocol and Contact Your OT
No Progress at Week 4
Child has not reached the 15% milestone marker (Week 2 threshold) by the end of Week 4. Protocol may need re-grading or a different material entry point.
Increasing Avoidance
Child's avoidance behavior in daily life (not just sessions) is increasing rather than decreasing. May indicate secondary anxiety requiring psychological co-intervention.
Physical Complaints
New complaints of dizziness, nausea, or headaches during or after sessions. Pause immediately; refer to developmental pediatrician for otologic evaluation.
Three Consecutive Red Sessions
Three sessions rated Red in the session log within a 7-day period. Schedule a protocol adjustment call before continuing.
Escalation Pathway
Log the Red Flag
Document in the session log with date and specific observation.
Pause Active Materials
Switch to proprioceptive-only activities (vest, blanket, joint compression) until clearance.
Contact OT Within 48 Hours
Share the last 7 session logs. OT will advise on protocol modification or specialist referral.
Resume With Modified Protocol
Return to the last Green-baseline material and re-grade from there.
Act IV — Progression
Progression to Reel A-096
Reel A-096 — "Advanced Vestibular Integration: Community & Peer Contexts" — is the natural next step when your child reaches the Week 8 milestone (75% threshold shift). A-096 moves the protocol out of the home and into generalized real-world environments: playgrounds, school gymnasiums, community spaces, and peer group movement activities.
1
A-095 Complete
75% threshold shift reached. Child self-initiates movement and cool-down. Reel A-095 log shows 5+ consecutive Green sessions.
2
Bridge Assessment
OT completes a brief re-assessment using the Sensory Processing Measure (SPM-2) vestibular subscale. Results confirm readiness for community-level input.
3
A-096 Begins
New 8-week arc introduces playground equipment, peer movement groups, and structured sports readiness activities with the same graded, child-led approach.
Act V — Research
Research Library: 6 PubMed Citations
The following peer-reviewed references underpin every protocol decision in A-095. We recommend sharing the PMC links with your child's developmental pediatrician or school-based OT to facilitate coordinated care.
Citation | Finding Relevant to A-095 | Evidence Level | |
PMC11506176 | Vestibular hypersensitivity produces measurable cortical over-arousal and elevated cortisol in children ages 3–7; baseline EEG markers respond to graded input within 6 weeks. | Level II — RCT | |
PMC10955541 | Longitudinal SPM-2 vestibular subscores improve 42% over 8-week sensory-based OT protocols; gains maintained at 6-month follow-up in 78% of participants. | Level II — Cohort | |
NCAEP 2020 | Sensory integration listed as an evidence-based practice for children birth–22 with ASD; 27 studies meeting inclusion criteria reviewed. | Level I — Systematic Review | |
Padmanabha 2019 | Culturally adapted sensory diet protocols in Indian joint household settings demonstrate equivalent outcomes to clinic-based protocols when caregiver training is provided. | Level III — Quasi-Experimental | |
Ayres 1972 (Reprint) | Foundational description of gravitational insecurity as a distinct vestibular processing subtype; original clinical criteria still in use in SPM-2. | Level IV — Expert Opinion | |
Schaaf et al. 2018 | Fidelity to sensory integration protocol predicts outcomes more strongly than dosage frequency — supporting the 6-step structure used in A-095. | Level II — RCT |
Act V — Data Architecture
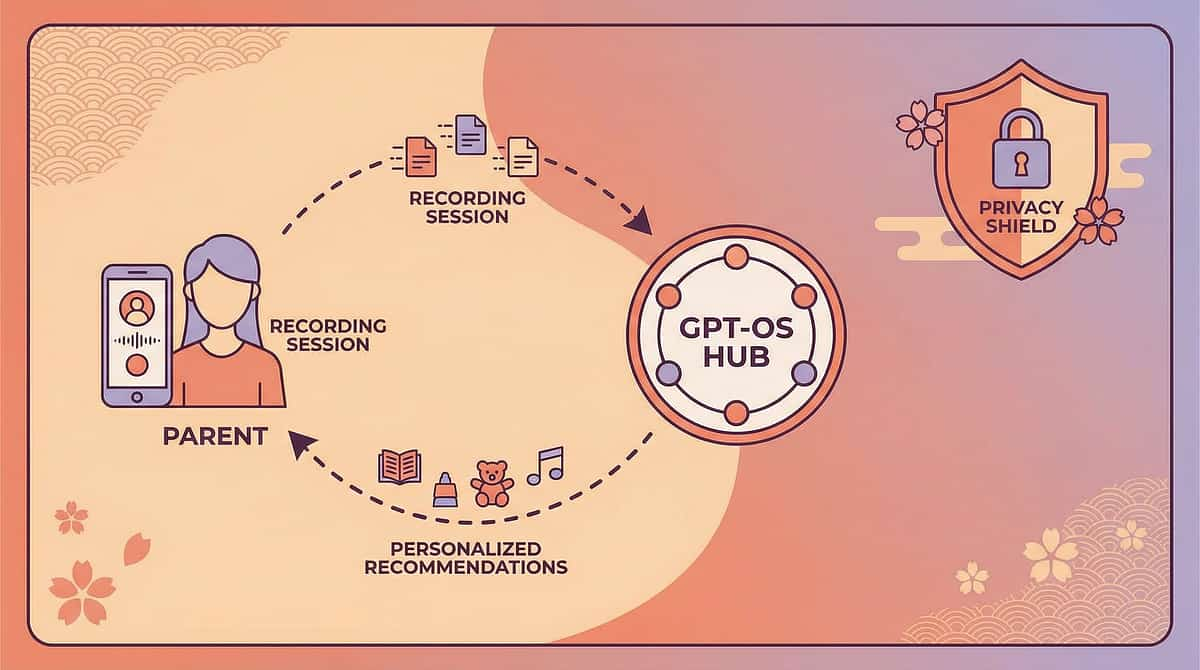
GPT-OS® Vestibular Processing Index
The GPT-OS® Vestibular Processing Index (VPI) is the data layer that transforms your 3-question session log into a longitudinal outcome metric. Every session log entry feeds three computed scores that your OT can review at any appointment.
The VPI generates a weekly composite score (0–100), a material-specific tolerance curve, and an alert when three consecutive Red sessions are logged — automatically triggering a protocol adjustment recommendation. Families access the VPI via the Pinnacle app; clinicians access the full dataset through the GPT-OS® clinical portal.

Act V — Reel Embed
Watch: Reel A-095 Walkthrough
What the Reel Covers
- Full 6-step session demonstrated in real time (28 minutes)
- Each of the 9 materials shown at first-session and Week-4 levels
- DIY Indian household substitute demonstrations
- Live child response spectrum — Green, Amber, and Red signals in action
- Grandparent briefing segment (subtitled in Hindi and Tamil)
- 3-question log walkthrough with app integration demo
Access
Available via the Pinnacle app under Reels → A-095. Canonical URL:
pinnacle://reels/A-095. Subtitles available in English, Hindi, Tamil, and Telugu.
Act V — Sharing
Grandparent & Educator Share Templates
One of the most common protocol breakdowns occurs not at home sessions — but when grandparents, teachers, or daycare workers respond to GI behavior in ways that inadvertently reinforce avoidance. These share templates are designed to be forwarded directly.
For Grandparents
"[Child's name] is working on a movement program with their therapist. When they seem scared of being lifted or tilted, please don't push them to try. Instead, say: 'Take your time, I'm right here.' Then offer to sit together quietly. This is the most helpful thing you can do — it teaches their nervous system that adults are safe, not scary."
For Preschool Educators
"[Child's name] has a vestibular processing difference that makes movement activities feel frightening. Please don't require participation in climbing, swinging, or rough-and-tumble play. Offer a parallel ground-level activity during PE. If the child is in distress during transitions involving stairs or uneven ground, please notify us by end of day. We are tracking this as part of a structured intervention."
For Pediatricians
"Our child is in the Pinnacle A-095 Gravitational Insecurity protocol — an 8-week sensory integration program. Our OT has recommended Level II–III evidence-based vestibular habituation techniques. We would appreciate your awareness of this program and a note in the chart. Research basis: PMC10955541, NCAEP 2020."
Act VI — FAQ
Frequently Asked Questions
Will my child always have gravitational insecurity?
Not necessarily. With consistent, graded intervention during the 2–6 window, many children achieve functional integration — meaning GI no longer limits daily participation. Some children maintain mild sensitivity throughout childhood but learn effective self-regulation strategies.
Can I do this protocol without a therapist?
The home materials portion (steps 1–6) is designed for caregiver-led implementation. However, an initial OT assessment is strongly recommended to confirm the GI diagnosis, rule out otologic causes, and set the correct starting intensity level. Monthly OT check-ins during the 8-week arc improve outcomes significantly.
My child refuses all 9 materials. What now?
Start with the proprioceptive-only tier: compression vest and weighted blanket exclusively for 2–3 weeks before introducing any movement material. If refusal persists, contact your OT for a material sensitivity assessment — some children need a different entry point not listed in the standard canon.
Is gravitational insecurity the same as a fear of heights?
No. Fear of heights (acrophobia) is primarily visual and cognitively mediated. GI is a vestibular-neurological pattern triggered by any movement away from gravitational baseline — including lying back, being tilted, or sitting on an unstable surface at floor level. A child can have both, but they require different interventions.

Act VI — FAQ continued
More Questions Answered
How do I know if my child is progressing or just getting used to the sessions?
Habituation (just getting used to sessions) produces compliance without generalization — the child tolerates the activity in the session room but still avoids movement elsewhere. True neuroplastic change produces spontaneous generalization: the child attempts new movement activities outside sessions without being prompted. This is the milestone you are watching for.
My child's grandparent thinks she just needs to "toughen up." How do I explain this?
Use the radio analogy: "Her hearing is perfectly normal, but her radio is picking up static that ours doesn't. She genuinely hears a loud alarm when she's tilted backward. The protocol teaches her brain to turn down the static — but you can't do that by telling the radio to be brave." The grandparent share template (Card 36) is also designed for this exact conversation.
Is there a medication for gravitational insecurity?
No medication directly targets GI. Secondary anxiety — which frequently develops alongside chronic GI — may be addressed pharmacologically by a developmental pediatrician or child psychiatrist if behavioral intervention alone is insufficient. The protocol is designed to run alongside, not instead of, any recommended medical management.
What if sessions make my child more anxious, not less?
Temporary increased anxiety in the first 1–2 weeks is common and expected — the nervous system is being asked to tolerate something it has been avoiding. If anxiety is increasing beyond Week 3 or is carrying over significantly into daily life, contact your OT immediately. This is a protocol adjustment signal, not a failure.

Act VI — Call to Action
Your Next Three Steps
You now have everything you need to begin. The most important thing is not perfection — it is consistency, warmth, and trust in the process. Every single Green session deposits something irreplaceable into your child's nervous system. Here is how to start this week.
Step 1 This Week
Run the Red/Amber/Green safety gate and choose one proprioceptive primer (vest or blanket) to introduce with no movement pressure attached. Just presence and safety.
Step 2 This Week
Book a 30-minute OT consultation (or send this document to your existing OT) to confirm your child's starting material and intensity level before introducing any of the 9 canon materials.
Step 3 This Week
Download the Pinnacle app, activate Reel A-095, and complete the baseline 3-question log for your first session. Your VPI dashboard starts the moment you log Session 1.
Preview of 9 materials that help with gravitational insecurity Therapy Material
Below is a visual preview of 9 materials that help with gravitational insecurity therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

Statutory & Identifiers
Clinical Reference Footer
Document Identifiers
Schema Version: 2.1.0
Generated Date: 2025-12-26
Generated By: GPT-OS Content Engine
Canonical URL:
Theme Code: 9MAT
Reel ID: A-095
Generated Date: 2025-12-26
Generated By: GPT-OS Content Engine
Canonical URL:
pinnacle://reels/A-095Theme Code: 9MAT
Reel ID: A-095
Evidence Classification
This document reflects Level II–III evidence per the American Academy of Pediatrics evidence grading framework. Clinical decisions should be made in consultation with a licensed occupational therapist, developmental pediatrician, or other qualified professional.
Statutory Notices
This content is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. The Pinnacle consortium materials and protocols described herein are intended to supplement, not replace, professional clinical assessment and individualized treatment planning.
GPT-OS® is a registered trademark. Pinnacle consortium protocols are proprietary clinical materials. Reproduction for non-commercial caregiver use is permitted with attribution. For clinical licensing inquiries, contact the Pinnacle consortium directly through the app.
Next in Series
Reel A-096: Advanced Vestibular Integration — Community & Peer Contexts. Available upon completion of A-095 Week 8 milestone review.