
"He does it perfectly for his therapist. With me? Nothing."
It's 7:30 in the morning. You're getting your son ready for school. His therapist showed you a video yesterday — him labeling ten animals perfectly, following three-step instructions, counting to twenty without a single error. You were so proud. Now he's standing in front of you and he can't tell you what animal is on his shirt.
Reel L-956
Learning & Skill Transfer
ABA-GEN
You Are Not Alone: The Numbers
ACT I: Why
Generalization failure is the single most documented gap between therapy-room performance and real-world function in autism and developmental delay. It is not your child being "stubborn." It is not the therapist's work being wasted. It is a predictable, addressable, programmable neurological feature.
80%
Limited Generalization
of children with autism show limited spontaneous generalization of learned skills
5
Types of Failure
stimulus, setting, person, response, temporal — each requires explicit programming
100%
Skills Without Planning
of skills taught without planned generalization training fail to transfer
📊India data: Approximately 1 in 68 children in India is diagnosed with autism spectrum disorder. With an estimated 18 million affected individuals, the gap between clinical skill and functional skill represents one of the largest unaddressed therapy delivery failures in pediatric care.
Research from the Journal of Applied Behavior Analysis — and foundational work by Stokes & Baer as far back as 1977 — established that generalization does not happen automatically. It must be planned, taught, and measured. You are among millions of families who have been told "the skills are there" while watching them disappear the moment the clinic door closes. This page is for you.

What's Happening in Your Child's Brain
ACT I: The Science
The Context Trap
When your child learns a skill — say, "touch nose when asked" — their brain doesn't just encode the skill. It encodes the skill plus every surrounding feature: the therapist's voice, the specific chair, the particular flashcard, the clinic's lighting, the time of day.
This is called context-bound memory — and it is stronger, not weaker, in many neurodevelopmental profiles including autism. When the context changes (you, home, dinner table, evening), the retrieval cue is missing. The skill is there. The brain just can't find the door.
This is a wiring difference — not a behavior choice. Not stubbornness. Not a failure of love or learning.
Key Brain Regions
- Prefrontal Cortex — executive function & rule transfer
- Hippocampus — context-bound memory encoding
- Basal Ganglia — habit-locked responding
- Amygdala — threat-tagged environments
Key pathway: Hippocampal context-binding locks the skill to the environmental context where it was encoded.
"The hippocampus tags experiences with environmental context during encoding. In autism, this context-tagging can be exceptionally precise — meaning context changes disrupt retrieval more significantly than in neurotypical development." — Frontiers in Integrative Neuroscience (2020)

Where Generalization Sits in Your Child's Developmental Journey
ACT I: Timeline
Ages 0–18m
Skill Imitation
Ages 18m–3y
Single-Context Learning
Ages 3–6y ▶
GENERALIZATION ZONE — Critical Programming Window
Ages 6–12y
Flexible Application
Ages 12y+
Autonomous Self-Regulation
▶You are here. This is the generalization window — the most critical and most commonly under-programmed phase in structured therapy.
What Requires Explicit Programming
- Stimulus generalization (same skill, new materials)
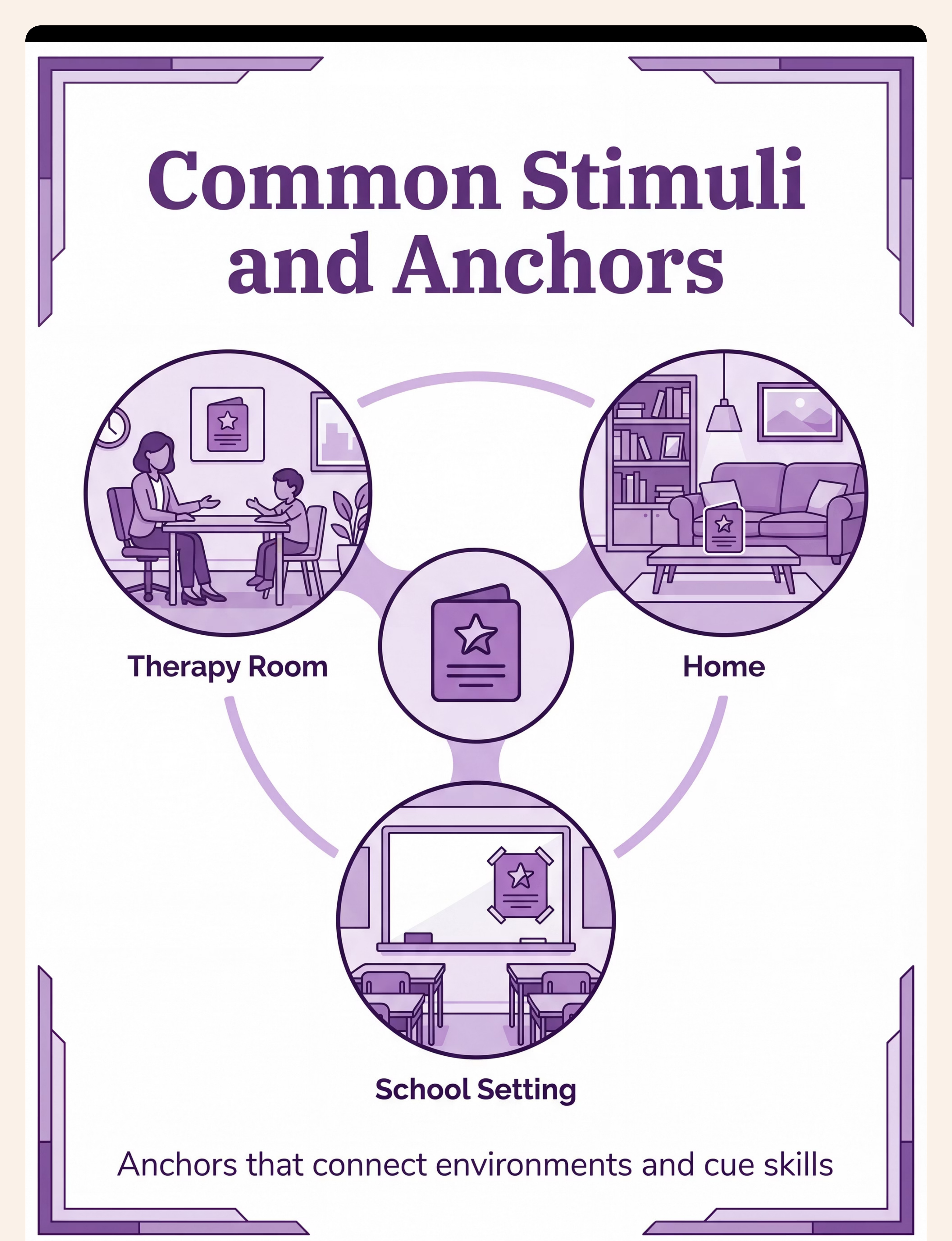
- Setting generalization (clinic → home → school)
- Person generalization (therapist → parent → teacher)
- Temporal generalization (maintenance over time)
Generalization Difficulties Co-occur With
- Sensory processing differences (context feels "wrong")
- Anxiety (new settings are threat-tagged)
- Executive function challenges (rules don't auto-transfer)
- Language processing differences (instructions sound different)
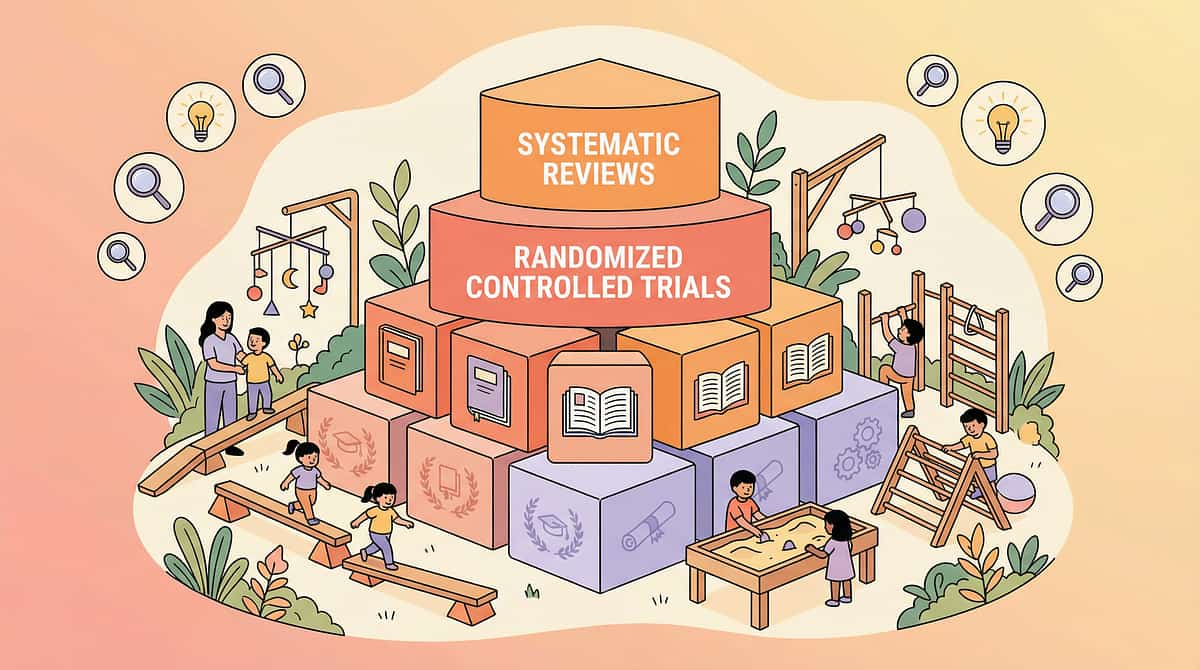
The Evidence Behind Generalization Programming
ACT I: Evidence
Level I Evidence
Stokes & Baer (1977)
Foundational framework: generalization must be systematically programmed, never assumed. The most-cited paper in generalization research. JABA, 10(2), 349–367
NCAEP (2020)
Multiple exemplar training, video modeling, and natural environment teaching classified as Evidence-Based Practices for autism — directly targeting generalization.
JABA (Multiple RCTs)
Structured generalization programs produce significantly superior skill retention vs. single-context teaching. Validated across hundreds of peer-reviewed studies.
"Programmed generalization produces 3–4x greater functional skill retention than acquisition-only training." — Journal of Applied Behavior Analysis, systematic literature review
Tag: Clinically validated. Home-applicable. Parent-proven. Evidence sources: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4

Generalization Programming: What It Is
ACT II: The Technique
Domain: ABA-GEN
Parent-Friendly Name: Making Skills Travel
Generalization is the process by which a skill learned in one context becomes available across all contexts where it is needed. It is not a bonus outcome — it is the goal of all structured therapy. A skill that exists only in the therapy room is not yet a functional skill. True learning means the child can use an ability with different people, in different places, with different materials, in varied situations — and can maintain that ability over time without continuous practice.
Technique Specifications
- Age Range: All ages — fundamental across the lifespan
- Session Duration: 10–20 min active protocol + ongoing natural environment practice
- Frequency: Daily integration; formal sessions 2–3x/week
- Reel: L-956 | Series Episode: 956
Five Types — All Must Be Programmed
- Stimulus Generalization
- Setting Generalization
- Person Generalization
- Response Generalization
- Temporal Generalization
Canon Material Links: Sorting Activities / Categorization | Problem-Solving Toys | Reinforcement Menus | Transition Objects

Which Therapy Disciplines Use Generalization Programming?
ACT II: Disciplines
ABA / BCBA — Primary Lead
Designs generalization programs; programs stimulus, setting, person, response, and temporal dimensions systematically.
SLP — Secondary
Extends communication skill generalization across conversational partners and natural language contexts.
OT — Secondary
Programs sensory and motor skill generalization to natural environments and functional daily living tasks.
SpEd — Secondary
Coordinates academic skill transfer from structured teaching to natural classroom and community contexts.
NeuroDev — Oversight
Monitors generalization readiness as part of overall developmental trajectory and neurodevelopmental profile.
"This technique crosses all therapy boundaries because the brain doesn't organize by therapy type — it organizes by context. When generalization is programmed across disciplines simultaneously, transfer happens 2–3x faster than single-discipline programming." — Pinnacle FusionModule™ Clinical Framework
What Generalization Programming Targets
ACT II: Targets
Generalization Type | What It Means | Observable Indicator | |
Stimulus Generalization | Same skill, different materials | Child labels "dog" with photo, toy, real dog, cartoon | |
Setting Generalization | Same skill, different environment | Child counts at home, school, supermarket | |
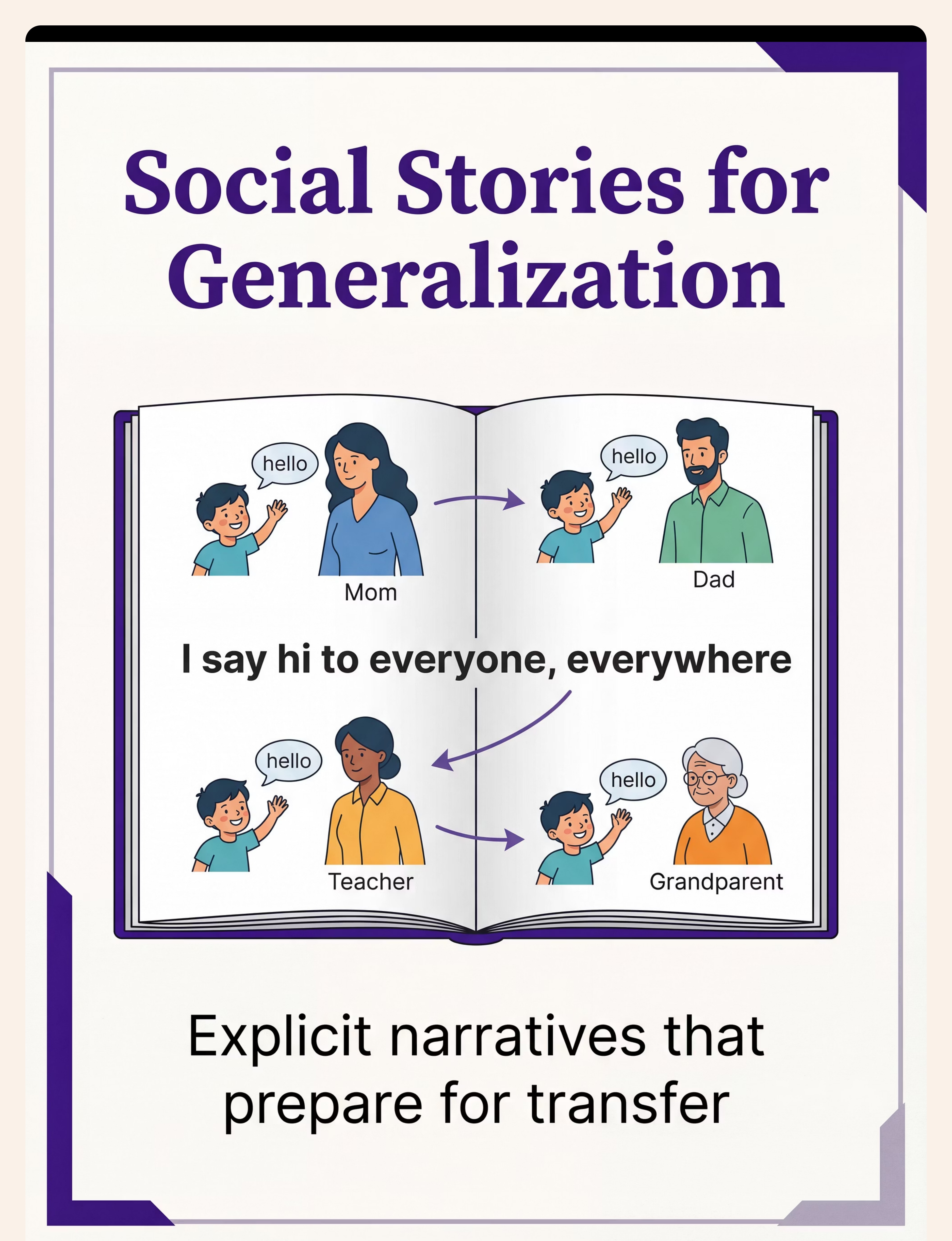
Person Generalization | Same skill, different instructor | Child follows instruction from parent, teacher, grandparent | |
Response Generalization | Same function, different form | Child says "help", "I need help", points, signs | |
Temporal Generalization | Skill maintained over time | Skill present 3 months after mastery without practice |
Secondary targets include: Reduced prompt dependency · Increased spontaneous skill use in natural environment · Family confidence and implementation consistency · Team coordination and unified teaching procedures
9 Materials That Help With Generalization
ACT II: Materials
Clinically Validated
Each of these 9 materials is a clinical tool — not a craft supply. The consortium has validated these against the Generalization Readiness Index in the GPT-OS® system.

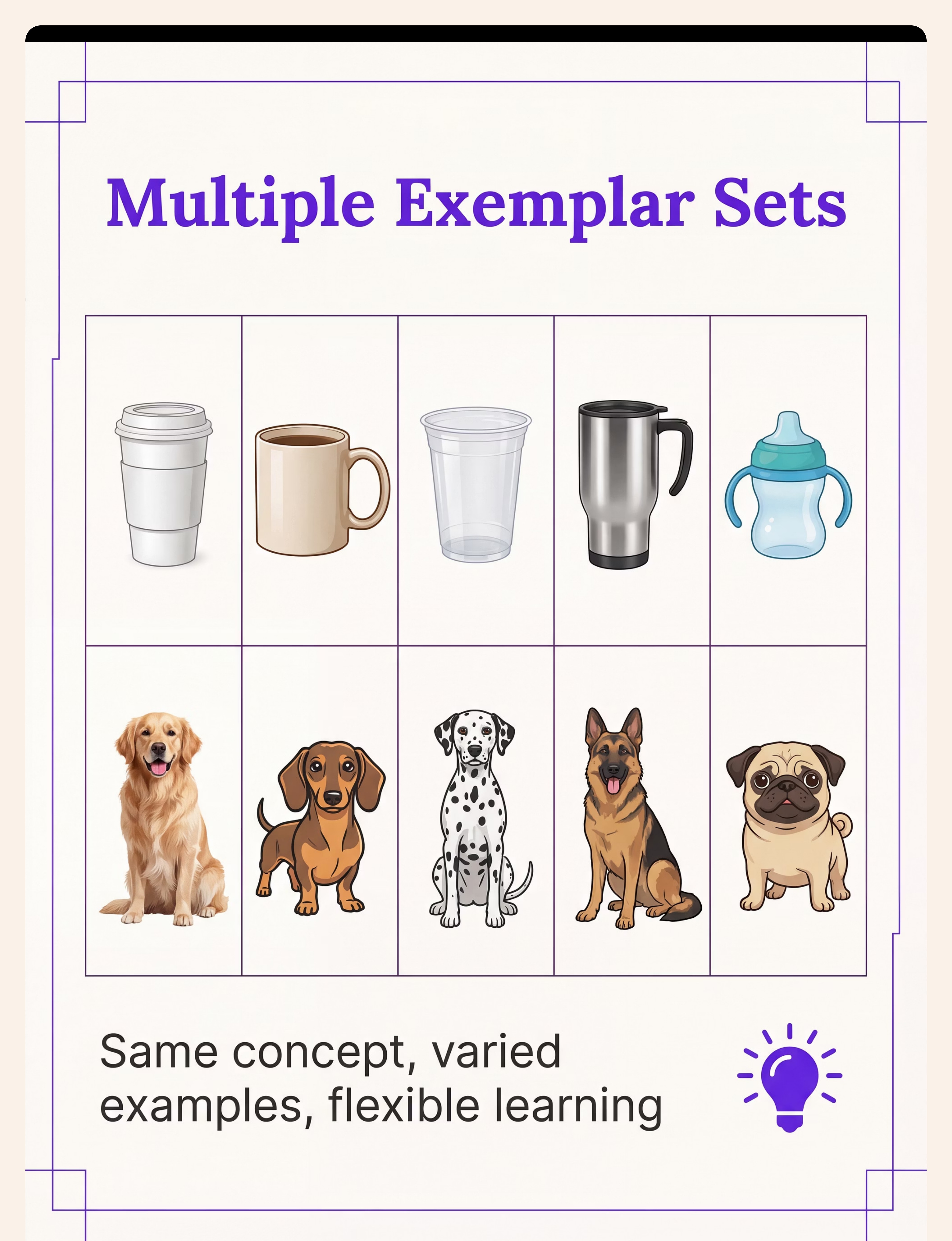
1. Multiple Exemplar Sets
Canon: Sorting Activities / Categorization | SKU #614 — ₹305 | Buy on Amazon.in →
The number of varied examples used during teaching is the single strongest predictor of generalization success. Gather 5–10 different representations of each target concept and rotate randomly. Never teach with a single example.
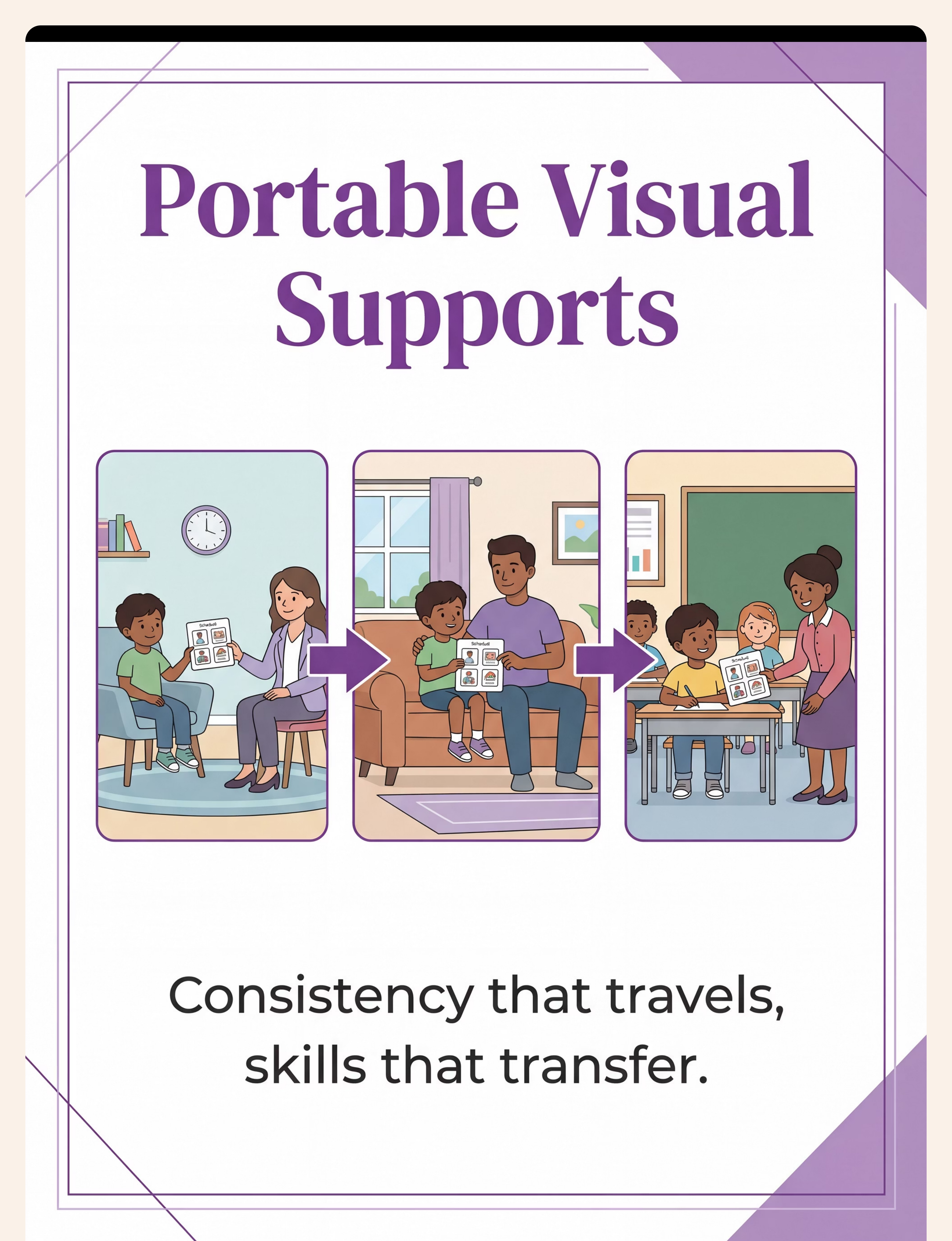
2. Portable Visual Supports
Canon: Transition Objects | SKU #118 — ₹425 | Buy on Amazon.in →
Same visuals in every setting. Send therapy visuals home. Use home photos in therapy. The visual thread connects learning across all contexts — the visual becomes a portable context.
3. Generalization Binders
Canon: Data Sheets / Tracking Materials | Find on Amazon.in →
The communication infrastructure ensuring therapy, home, and school all see the same targets, use the same procedures, and contribute to the same data. Everyone on the same page.

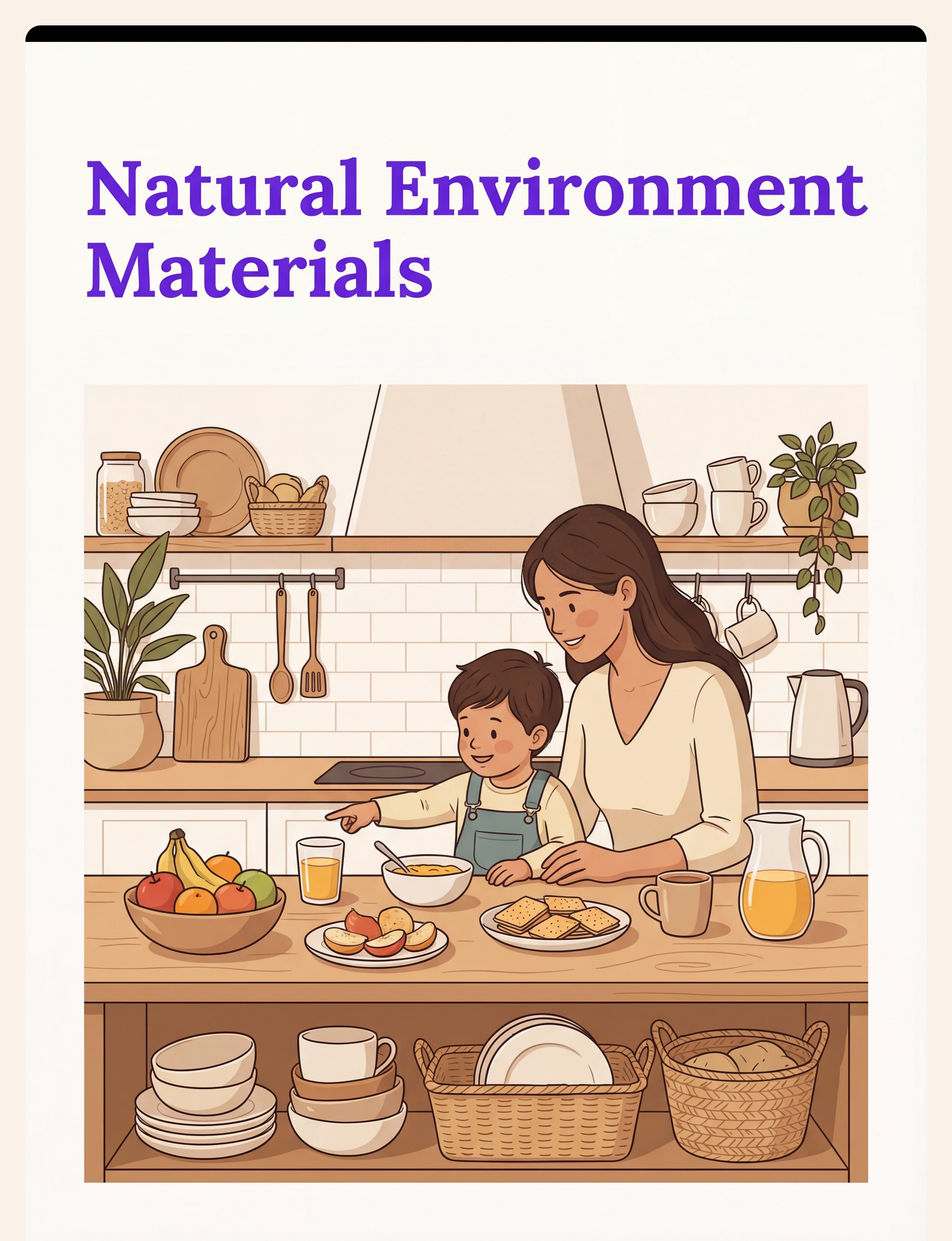
4. Real-World Object Collections
Canon: Sorting Activities / Categorization | SKU #577 — ₹628 | Buy on Amazon.in →
Therapy materials are artificial. Real life uses real objects. The more therapy materials resemble real life, the less translation is needed for generalization. Bring the world into the therapy room.
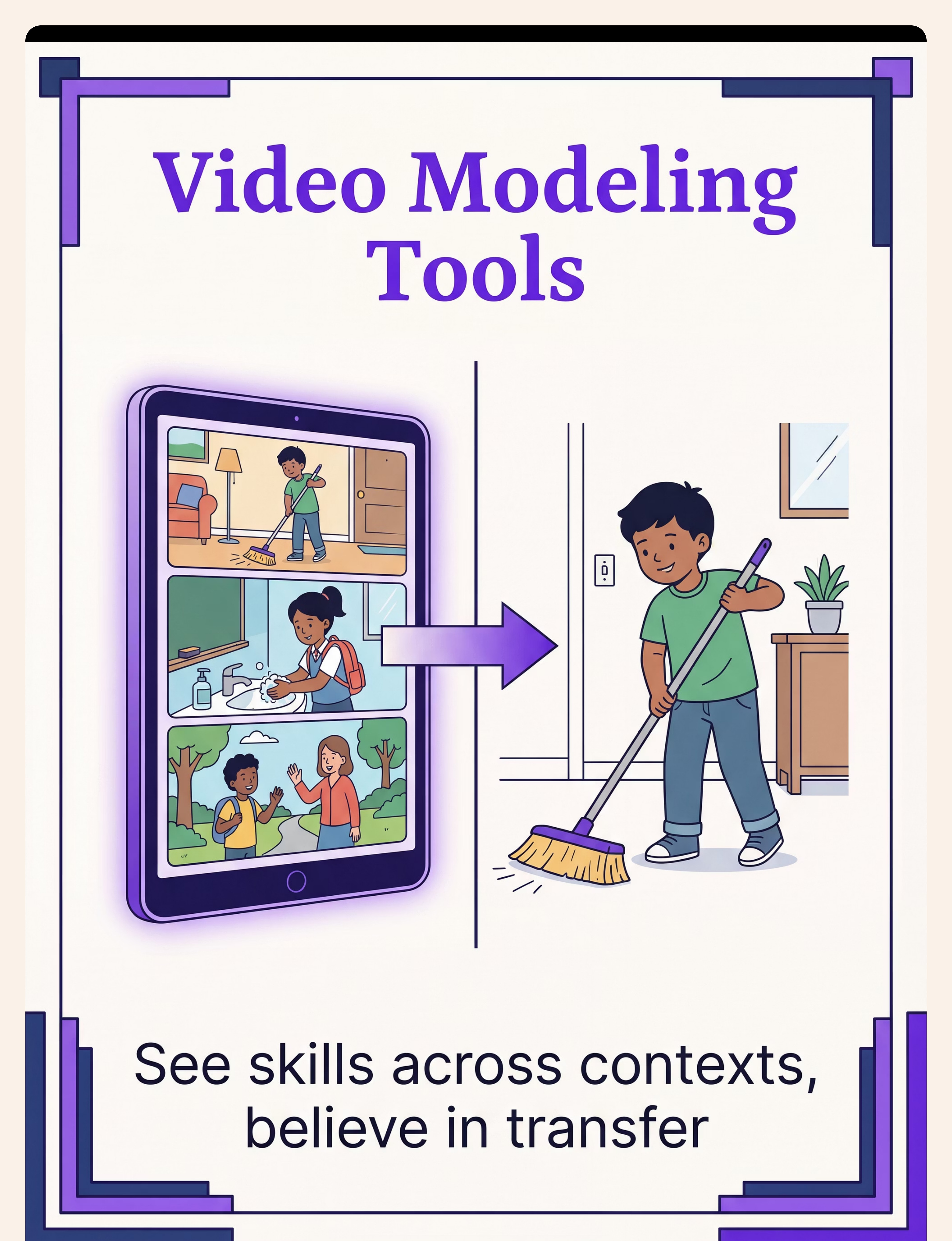
5. Video Modeling Libraries
Canon: Video Modeling Materials | Find on Amazon.in →
Video modeling shows the same skill performed by different people in different settings. Multiple models + multiple settings = built-in generalization training. The child watches the skill travel before making it travel.

6. Generalization Probes & Data Sheets
Canon: Data Sheets / Tracking Materials | Find on Amazon.in →
Generalization must be measured, not assumed. Probe sheets test skill performance with untrained people, places, and materials. What isn't measured isn't managed. What gets measured gets programmed.

7. Community-Based Teaching Materials
Canon: Community Integration Materials | Find on Amazon.in →
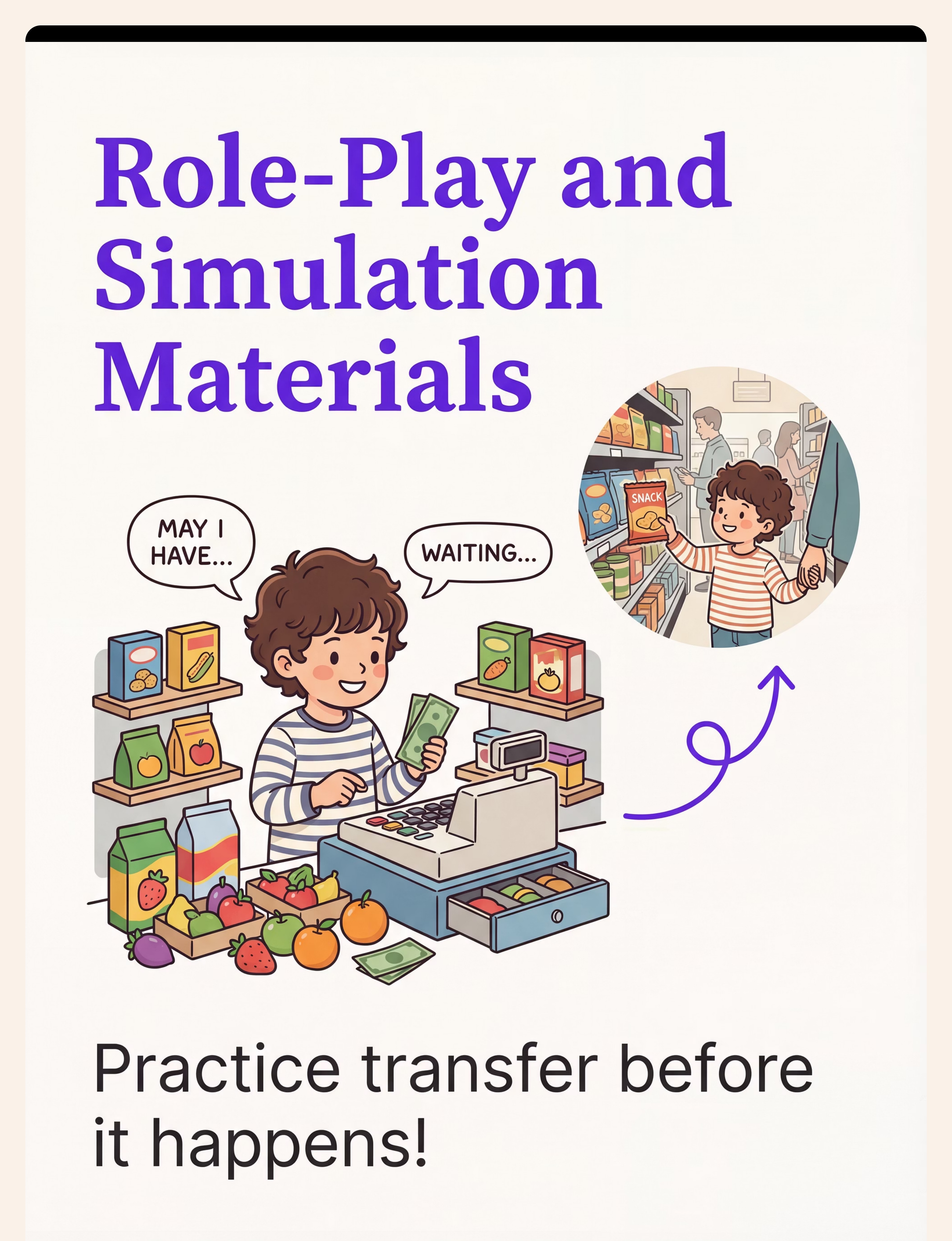
Community kits — photos of local settings, social stories, simulation materials, portable prompts — bridge therapy-room learning to real-world application before the child faces it cold.
8. Maintenance Schedules & Review Systems
Canon: Reinforcement Menus | SKU #803 ₹589 | #390 ₹364 | Buy on Amazon.in →
Maintenance schedules systematically revisit mastered skills on rotation — weekly to monthly to quarterly — ensuring the learning investment is preserved over time.

9. Multiple Instructor Training Materials
Canon: Parent Training Materials | Find on Amazon.in →
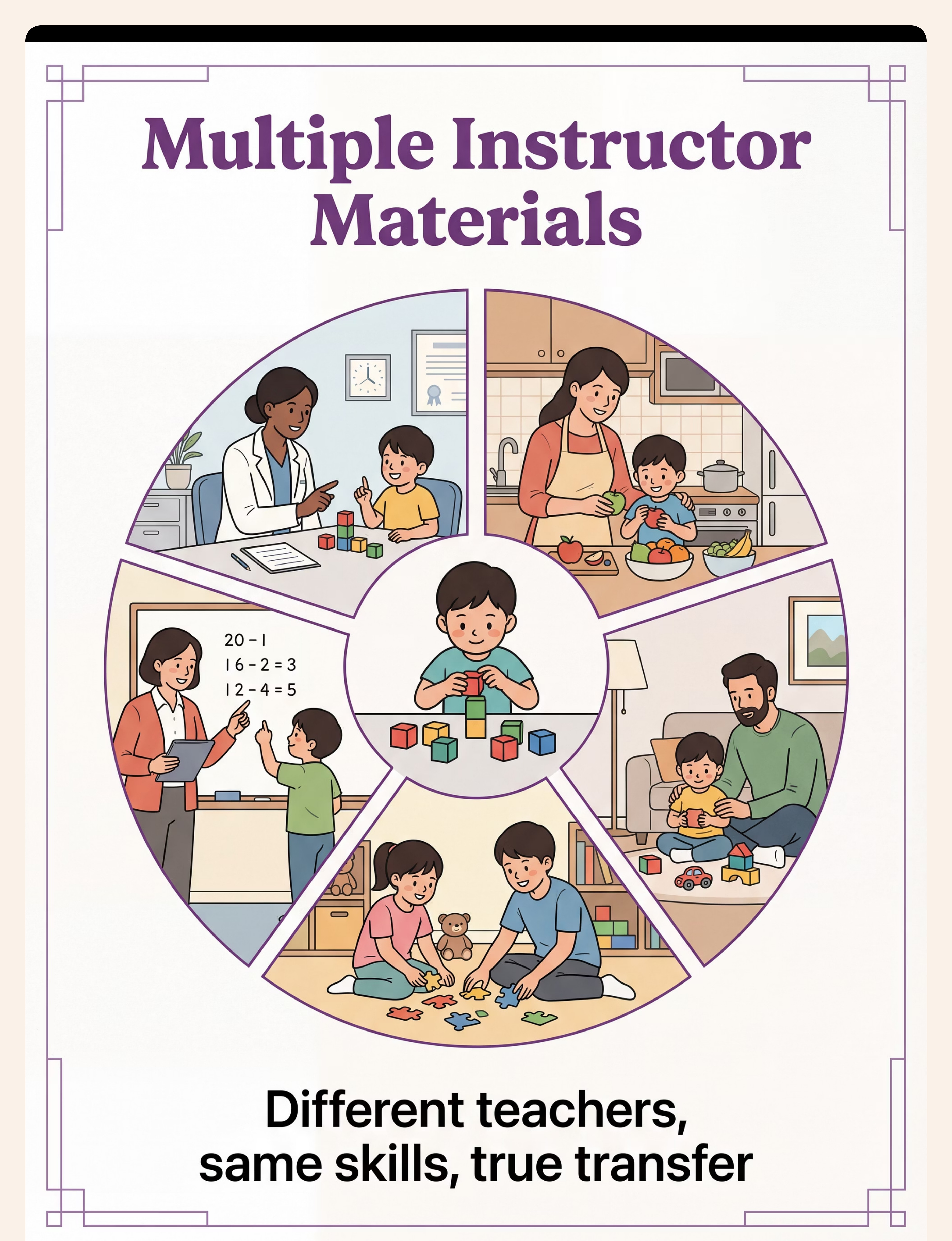
When only one person teaches a skill, the skill becomes bound to that person. Training guides, video demonstrations, and procedure checklists ensure everyone can teach consistently, building skill robustness.
💡Essential Generalization Starter Kit: Multiple exemplar set (₹305) + Portable visual supports (₹425) + Reinforcement menu for maintenance (₹364) + Generalization binder (DIY ₹0) = Under ₹1,100 to begin

DIY & Zero-Cost Substitutes: Because Therapy Can't Wait for Amazon
ACT II: Equity
WHO Inclusion Principle
This card embodies the WHO/UNICEF inclusion principle. Every intervention technique at Pinnacle Blooms is designed to be accessible at every economic level — from urban clinic to rural home.
Material | ₹0 DIY Alternative | Why It Still Works | |
Multiple Exemplar Sets | Cut images from old magazines/newspapers (5–10 per concept). Use real household objects. | Same neurological principle — varied stimuli enable concept extraction | |
Portable Visual Supports | Print photos from phone, laminate with sticky tape. Punch hole, attach to keyring. | Portability and consistency are the active ingredients, not the material quality | |
Generalization Binder | Repurpose any notebook. Section with paper dividers. Share photos via WhatsApp family group. | The function is coordination — a WhatsApp group coordinates as effectively as a physical binder | |
Real-World Objects | Every home already has real-world objects. Use actual plates, clothes, food items, toys. | The most powerful version IS the ₹0 version — real objects, not therapy toys | |
Video Modeling Library | Record 30-second phone videos. Multiple family members, multiple rooms, one skill. | Self-created videos with familiar faces accelerate generalization faster than professional content | |
Generalization Probe Sheets | Draw a simple grid on paper: rows = settings, columns = dates. Mark + / – per trial. | The data is the value, not the format of the sheet | |
Community Kit | Take 5 photos of the places your child visits. Print at any digital photo shop (₹5/print). | Authentic local photos are MORE effective than generic teaching images | |
Maintenance Schedule | Use any calendar. Circle dates for skill review. 1 = this week. 2 = next week. 3 = next month. | Consistency of review matters. The calendar is the tool. Paper works. | |
Instructor Training Materials | Write 3 sentences per skill: "What to do. What to say. What to reward." Share via WhatsApp. | Simplicity enables consistent implementation across more people |
"A skill is accessible to every child when the tools to teach it are accessible to every family. Zero-cost alternatives are not inferior — they are, in many cases, superior because they use real life." — WHO Nurturing Care Framework | Pinnacle Consortium Equity Principle
Safety Framework: Before You Begin Any Generalization Session
ACT II: Safety First
🔴 STOP — Do Not Proceed If:
- Child is in acute distress, illness, or post-meltdown within 30 minutes
- Environment is unsafe for the specific probe
- Probe materials have not been safety-checked (choking hazards, sharp edges, toxic residue)
- Child shows signs of extreme anxiety related to the new setting
🟡 MODIFY Before Proceeding If:
- Child is tired, hungry, or mildly dysregulated — use easiest version, highest reinforcement
- New setting carries moderate anxiety — use portable visual support
- Probe is with an unfamiliar person — pair initially with known instructor
🟢 PROCEED When:
- Child is fed, rested, in regulated state
- Environment has been previewed (photo or social story shown beforehand)
- At least one familiar person is present for first probe in new setting
Material Safety Specifics
- Laminator sheets: Non-toxic, child-safe only. Ensure no sharp laminated edges.
- Real-world objects: Remove residue from food containers before use. Check for small parts.
- Video devices: Screen time managed; device cords secured.
- Portable keyring cards: Breakaway lanyard only (never fixed-loop cord on neck).
🚨STOP IMMEDIATELY if: Child shows self-injurious behavior, severe meltdown, physical aggression, extreme dissociation, or signs of medical distress. Session abandonment is not failure — it is the correct clinical decision. Call 9100 181 181 for guidance.

Setting Up for Generalization Practice at Home
ACT II: Setup
Child Position
Familiar seat. Comfortable. Clear sightline to materials. Back to distractions.
Parent/Instructor
45° angle, within arm's reach — not directly in front. Reinforcement visible but not within grab reach.
Materials Table
All varied exemplar sets arranged in view and within reach. Start with 3–5 items maximum.
Data Sheet
Accessible to instructor, not intrusive to child's experience. Timer set (optional but helpful).
Remove Distractions
TV, tablet, unrelated toys removed. Exit clear — child can leave without obstacle.
Sensory Setup
Natural lighting preferred. Background noise: low and consistent. Temperature: comfortable, not stimulating.
For generalization across rooms, each room needs only: the same visual support cue, the target materials (real-world objects naturally present), and a brief transition script: "Now we're going to try this in the kitchen."
Pre-Session Readiness Check: 60 Seconds, Every Time
ACT III: Execution
Before You Begin
Check | ✅ GO | 🟡 MODIFY | 🔴 POSTPONE | |
Fed in last 2 hours? | Yes | Light snack available | Hungry — feed first | |
Rested (last night + today)? | Well-rested | Mild tiredness | Overtired | |
Regulated state? | Calm | Mild irritability | Post-meltdown < 30 min | |
No signs of illness? | Healthy | Mild cold, monitor | Fever or unwell | |
Receptive to familiar person? | Engaging | Intermittent | Rejecting all contact | |
Target skill present in teaching setting? | Reliable | Emerging | Not yet acquired | |
Environment set up and safe? | Yes | Minor adjustments needed | Not ready |
✅ ALL GREEN
PROCEED TO STEP 1 — The Invitation
🟡 SOME AMBER
SIMPLIFIED VERSION — shorter, higher reinforcement, familiar person only
🔴 ANY RED
POSTPONE — use calming activity (see Reel L-943 Emotional Regulation)
"The best generalization session is one that starts right. A child who is dysregulated, hungry, or anxious will not generalize — they will confirm that the new context is threatening. Starting right is not just kindness. It's clinical precision." — Pinnacle Clinical Protocol L-956

Step 1 of 6: The Invitation
ACT III: Step 01
0–60 seconds
What You Do
Begin with a natural, playful, low-demand opening that brings the child into the activity without triggering avoidance. No commands. An invitation.
Body Language
- Kneel or sit to child's eye level
- Open posture, relaxed shoulders
- Voice: warm, curious, slightly lower energy
- No sustained eye contact demand — let the child lead gaze
Script Box — Exact Words
"Hey — look at this! I found something interesting. Want to see?" [Show one familiar exemplar] "You're so good at this. Let's play."
What Acceptance Looks Like
- Child moves toward the material
- Child touches or picks up material
- Child makes eye contact or vocalizes positively
If Child Resists
- Walks away → Follow at distance, don't pursue forcefully
- Throws material → Calmly retrieve. "Let's try again." No frustration.
- Passive but present → That is acceptance. Proceed.

Step 2 of 6: The Engagement
ACT III: Step 02
1–3 minutes
Script Box
"And look — here's another one. Different, but the same idea." [Introduce novel exemplar] "Same thing, different look. What do you think?"
How to Present the Novel Material
- Don't hide or surprise — present openly and calmly
- Hold at a neutral distance (not pushed toward child)
- Keep previous familiar exemplar visible (security bridge)
- Smile. Your calm signals safety in novelty.
Child Response Spectrum
- Engagement: Child reaches, touches, labels, responds correctly → Reinforce immediately
- Tolerance: Child observes but doesn't engage → Acceptable. Verbally name the item. Move on.
- Avoidance: Child looks away or pushes away → Hold position 3 seconds. Offer verbal label only. Then put aside.
Reinforcement Cue: Any correct response to the novel material — even a glance — receives immediate, enthusiastic reinforcement. This is the generalization moment.
Step 3 of 6: The Core Generalization Trial
ACT III: Step 03
5–10 minutes
The Active Ingredient: The structured generalization trial — presenting the target skill opportunity with a material, person, or setting that was NOT used during original teaching.
Panel A — Stimulus Trial
Present 3–5 varied exemplars simultaneously. Ask the standard target question across all representations.
Script: "Show me [concept] — this one... and this one... and this one?"
Data: ✓ or ✗ for each novel exemplar
Panel B — Setting Trial
Take the familiar skill to a new room or location. Same materials. Same script. New setting.
Script: "Let's try this in the kitchen. Same game, different room."
Data: ✓ or ✗ in new setting
Panel C — Person Trial
Have a second family member (already briefed) conduct the same trial using the same materials and script.
Script: "[Child name], can you show me [concept]?"
Data: ✓ or ✗ with novel instructor
Quality Level | Description | Action | |
✅ Ideal | Correct response without prompt, within 3 seconds, with any novel stimulus | Reinforce & continue | |
🟡 Acceptable | Correct response with light gestural prompt to novel stimulus | Reinforce & fade prompt | |
🔴 Concerning | No response or incorrect with even familiar materials | Stop & return to acquisition |
Step 4 of 6: Repeat & Vary
ACT III: Step 04
5–10 minutes
The Principle: Generalization requires many different examples across many repetitions. The brain extracts the concept when it sees it enough times in enough variations.
Repetition Guide
- Target per session: 3–5 correct generalization trials per material type
- Total trials: 10–15 novel-exemplar presentations across session
- Ratio: ~70% known exemplars, ~30% novel — maintains engagement while introducing novelty
Variation Options
- Vary the material: photo → toy → real object → drawn image
- Vary the location: 2 different rooms within same session
- Vary the presenter: second family member conducts same trial
- Vary the phrasing: "Show me" → "Where's the?" → "Find [X]"
- Vary the context: morning routine, play, snack time
Satiation Indicators — When to Stop
- Increasing latency (taking longer to respond)
- Decreased accuracy on known exemplars (fatigue signal)
- Physical withdrawal from materials
- Increased self-stimulatory behavior
"3 good generalization trials are worth more than 15 forced ones. When the child is fresh and reinforced, every correct trial builds the neural pathway. When the child is done, forcing trials teaches avoidance."

Step 5 of 6: Reinforce the Transfer
ACT III: Step 05
Within 3 seconds. Specific. Enthusiastic. Every time.
Reinforcement Script
"YES! You showed me [concept] with a DIFFERENT one! That's incredible!" "You got it! Same thing, new picture — you knew it! AMAZING."
Specificity matters: Generic "good boy/girl" is less effective than specific "You identified the dog even in the cartoon — that's generalization!"
Natural Reinforcer Hierarchy
- Functional access — item/activity named transfers to real-world access
- Social praise from multiple people (person generalization reinforcer)
- Token economy progress (visual progress system)
- Preferred item/activity from reinforcement menu
Canon: Reinforcement Menus → Products #803 ₹589 | #390 ₹364 → Amazon.in
"Celebrate the attempt, not just the success. When a child reaches toward a novel exemplar — even incorrectly — they are showing you the behavior we want: engaging with novelty. That attempt is data and it deserves acknowledgment."
Step 6 of 6: The Cool-Down
ACT III: Step 06
1–2 minutes
The Principle: No generalization session ends abruptly. The child needs a predictable, gentle close that marks the transition back to unstructured time. This prevents post-session dysregulation — especially important after the cognitive demand of novel-stimulus processing.
Transition Script
"Two more... one more... and we're all done! Great work!" [Activate visual timer for final 60 seconds] "Now let's put these away together." "You were so amazing today. We practiced [concept] in so many different ways."
Cool-Down Activity — Choose ONE
- Child-directed free play (decompression)
- Sensory calming input preferred by child
- Simple, familiar, mastered skill (confidence restoration)
- Preferred music or quiet visual
Material Put-Away Ritual
When possible, have child participate in putting materials away. This signals clear session end, practices organization skills (secondary target), and creates a predictable transition marker the child can rely on.
If Child Resists Ending
"I know — it was fun! We'll do this again [tomorrow / after school]. Let's remember: [summary of achievement]."
Use visual timer and concrete transition object (Canon #118 — ₹425)

Capture the Data — Within 60 Seconds
ACT III: Data
60 seconds of data now saves hours of guessing later.
Quick Session Tracker
- Session Date: _______________
- Material Type Tested: Multiple Exemplars / New Setting / New Person / Community Kit / Video Model
- Novel Exemplar Trials: ___ correct out of ___ total
- New Setting Trials: ___ correct out of ___ total
- New Person Trials: ___ correct out of ___ total
- Child State Today (1–5): ___
- Notes: _______________________
Why Data Matters for Generalization
Unlike acquisition data (did the child learn the skill?), generalization data answers the harder question: did the skill travel?
Without systematic probe data:
- Teams assume generalization is occurring when it isn't
- Skills move off the active program list before truly generalized
- Parent observations go unvalidated
- Programming decisions are based on guesswork
🔗GPT-OS® Integration: Data entered feeds directly into the Generalization Readiness Index within AbilityScore® — tracking progress from "skill present in one context only" to "spontaneous generalization across settings."

What If It Didn't Go As Planned?
ACT III: Troubleshoot
Session abandonment is not failure — it's data. The technique needs adjustment, not you.
Child refused all novel materials
Why: Novel stimuli can be aversive if introduced too quickly — child has learned "novel = demanding."
Fix: Return to 100% familiar exemplars for 2–3 sessions. Pair novel materials with high-value reinforcement before any demands. Make novelty safe before making it educational.
Performed at home but failed in new setting
Why: Setting generalization requires preparation. Cold exposure to new settings produces avoidance, not learning.
Fix: Preview the new setting via photos. Use social story. Bring same familiar materials to new setting first. Gradual exposure, not sudden immersion.
Only responded to me, not the second instructor
Why: Person generalization failure — skill is bound to you. The second instructor is a novel stimulus.
Fix: Begin pairing: both of you present simultaneously. You prompt, second instructor delivers reinforcement. Gradually fade your prompting while second instructor takes over.
Skills deteriorated after a break
Why: Maintenance failure — skill was not yet robustly generalized before practice stopped.
Fix: Return to acquisition if needed. Increase maintenance probe frequency. Skills that fade needed more overlearning before the maintenance phase.
Progress on probe data but skill doesn't appear spontaneously
Why: Probe performance and spontaneous use are distinct. Prompt-free probe trials ≠ natural environment use.
Fix: Add natural environment teaching (NET) component — create organic opportunities for the skill to occur and reinforce natural use specifically.
Child generalizes to inappropriate contexts
Why: Over-generalization requires discrimination training — teaching when the skill is and isn't appropriate.
Fix: Add discrimination training component. Consult ABA specialist. This reflects generalization ability working — just without boundary-setting.
Adapt & Personalize: No Two Children Generalize the Same Way
ACT III: Personalize
Sensory Seeker
- Use tactile, 3D, textured exemplars
- Integrate movement into setting changes
- Multiple instructors with high-energy delivery
Sensory Avoider
- Use visual/distant presentation first; build to tactile
- Preview all new settings with extensive social story
- One new instructor at a time; gradual desensitization
Language-First Learner
- Lead with visual supports; minimize verbal demand during novel-stimulus trials
- Use gesture/picture response options before verbal label
- Pair communication symbols with all generalization exemplars
Profile Type | Pattern | Primary Strategy | |
Setting-bound learner | Skill perfect in therapy, fails everywhere else | Setting generalization + portable visual supports | |
Person-bound learner | Only performs for primary therapist | Multiple instructor training, rapid person rotation | |
Material-bound learner | Only recognizes taught flashcard, not real objects | Real-world objects + multiple exemplar expansion | |
Time-bound learner | Learns quickly but loses skills rapidly | Overlearning + aggressive maintenance scheduling |
Age Adaptations: Under 3 — focus on person & stimulus generalization within natural play. Ages 3–7 — clinic ↔ home ↔ school is the priority trio. Ages 7+ — community generalization becomes the primary target.

Week 1–2: The Foundation Phase
ACT IV: Progress Arc
Foundation Phase — 15%
What You Will Likely See ✅
- Child shows increased tolerance of novel materials (not mastery — tolerance)
- Mild curiosity toward new settings rather than immediate refusal
- Reduction in resistance to second instructor (even if compliance is minimal)
- Parent confidence beginning to build
What Is NOT Yet Expected ❌
- Spontaneous generalization without prompting
- Consistent correct responses to all novel exemplars
- Skill transfer to community settings
- Maintenance without continued practice
Micro-Progress Markers
- Week 1, Day 3: Child doesn't turn away from the second family member attempting a trial
- Week 1, Day 5: Child touches a novel exemplar even without a correct label
- Week 2, Day 2: Child moves between rooms without behavioral escalation
- Week 2, Day 4: One correct unprompted response to novel stimulus — bank this data point
"If your child tolerates a novel exemplar for 3 seconds longer this week than last week — that is measurable, real neural pathway formation. Celebrate it."
Week 1–2 is the patience phase. The neurological rewiring is happening beneath what you can see. Trust the protocol. Trust your data. Trust the process.

Week 3–4: The Consolidation Phase
ACT IV: Progress Arc
Consolidation Phase — 40%
60%
Novel Exemplar Accuracy
Target accuracy without prompting — a consolidation milestone
40%
Progress Milestone
Overall progress through the generalization programming arc at Week 3–4
70%
Trigger Next Phase
70%+ accuracy across 2 novel stimulus types triggers expansion to a 3rd type
🌟"When your child labels something in the real world that you didn't specifically practice — a dog on the street, counting real objects, following an instruction you gave without any preparation — that is generalization becoming part of who they are, not just what they do in sessions."
Consolidation Indicators ✅
- Child begins to anticipate the session — approaches materials without invitation
- Second instructor receiving same-level response as primary instructor
- Child demonstrates skill in a second setting with only light support
- First instances of spontaneous generalization — skill appearing naturally, unprompted
Parent Milestone
"You may notice you're more confident too — you've been implementing a systematic generalization program for 3 weeks. You now know how to teach your child to transfer skills. That is irreversible expertise."

Week 5–8: The Mastery Phase
ACT IV: Mastery
75% Complete
Dimension | Mastery Criterion | |
Stimulus Generalization | 90%+ correct with novel exemplars never used in teaching, across 3 consecutive probe sessions | |
Setting Generalization | 80%+ correct in 3 distinct settings (clinic / home / school or community) | |
Person Generalization | 80%+ correct with 3 different instructors including at least 1 minimally trained person | |
Response Generalization | Demonstrates 2+ functional response forms for same target | |
Maintenance | 80%+ correct at 30-day probe with no active practice in interim |
✅ Fully Achieved When
Skill appears spontaneously in natural environment without any adult prompt, consistent across 4+ weeks, maintained at 30-day probe.
🏆 When to Move On
All mastery criteria met → Link to L-957 (Skill Maintenance Materials) or next technique in your GPT-OS® personalized plan.
🎉 Generalization Mastered. Skills Now Travel.
ACT IV: Celebrate
You did this. Your child grew because of your commitment.
Over the past 5–8 weeks, you programmed stimulus generalization using varied exemplar sets, extended skills to new settings through systematic exposure, trained multiple instructors so the skill doesn't live in one person, and built maintenance systems so this investment is protected over time.
The skill your child practiced in therapy now belongs to them everywhere. Not just in the clinic. Not just with one therapist. Everywhere.
Generalization Wall
Document all the places and people the skill has traveled to — a visual record of your child's growing world.
Family Victory Video
Record your child demonstrating the skill in 3 different settings — a keepsake and a clinical record.
Milestone Journal
"On [date], [child's name] used [skill] at [place] for the first time. We were proud."

Red Flags: When to Pause and Seek Professional Consultation
ACT IV: Safety
Not fear — awareness. These are specific thresholds, not vague concerns.
🚨 Skill regression across all settings simultaneously
May indicate neurological change, illness, medication effect, or significant trauma. Do: Pause new generalization programming. Consult neurologist or pediatrician. Contact Pinnacle helpline.
🚨 Extreme distress during generalization probes
Anxiety-driven avoidance can masquerade as generalization failure — requires clinical assessment. Do: Cease probing. Consult BCBA for anxiety-informed generalization protocol.
🚨 No progress on any dimension after 8 weeks of consistent implementation
May indicate the acquired skill is not yet truly mastered, or there's a prerequisite gap. Do: Request formal generalization assessment from BCBA. Review acquisition criteria.
🚨 Skills generalize to inappropriate contexts
Over-generalization requires discrimination training. Do: Add discrimination training component. Consult ABA specialist.
🚨 Family conflict around the generalization program
Inconsistency across instructors is the most common cause of generalization failure. Do: Family training session with BCBA or Pinnacle therapist. Generalization binder review.
🚨 School environment actively resistant to generalization procedures
Setting generalization to school requires school buy-in. Do: Request school-based consultation. Pinnacle's school liaison team can assist.

The Generalization Progression Pathway
ACT IV: Pathway
You Are Here: L-956
Skills fade quickly?
Generalizes slowly?
Not generalizing to people?
→ Focus: Multiple Instructor Training (Card 09, Material 9) + L-957
Excellent generalization?
→ Accelerate to L-958 Fluency Building — skill is portable, next goal is automatic and fast
Related Techniques in the Learning & Skill Transfer Domain
ACT IV: Related
✅ If you have the Canon Materials from this page, you're already equipped for L-957 and L-960 — you don't need new purchases to start the next technique.

Your Child's Full Developmental Landscape
ACT IV: Whole Child
Domain L: Learning & Skill Transfer — Your Current Domain
This is the domain that activates all other domains. Every skill developed in Domains A through K needs generalization to become functional. Generalization is the infrastructure layer of all developmental work.
If Your Child Is Also Receiving
- OT (Domains A/I): Generalization programs for sensory and motor skills run in parallel
- SLP (Domain B): Communication generalization across conversation partners is a specific sub-program
- ABA (Domains C/D/K): All behavior and academic programs should include generalization from session one
📞 Or call FREE: 9100 181 181 (16 languages, 24×7)
Families Who Have Navigated This Exact Challenge
ACT V: Community
Ritu & Aanya — SLP-Led Generalization
Before: Aanya, aged 6, had been in speech therapy for 18 months. 100% accuracy requesting snacks in the clinic. At home: still grabbing, not asking. At school: not answering teachers. Two different children in two different worlds.
After: The team introduced multiple exemplar training across 40 object categories. They trained Ritu, the grandmother, and the school teacher using procedure guides. Portable visual cards traveled between settings. At 14 weeks, Aanya spontaneously asked for water in the school cafeteria with a teacher she had only met twice.
"We were told her skills 'were there' for over a year. What we needed was for them to travel. Once we understood that, everything changed." — Ritu, Pinnacle Network parent
Dev's Father — ABA-Led Generalization
Before: Dev, aged 8, mastered 23 academic skills in ABA over 6 months. His BCBA was proud. But at school, his teacher reported no progress. Dev only performed for his primary therapist, in the clinic, using specific teaching materials.
After: Generalization binder created. All 23 skills mapped with probe data targets. Parents trained, school visits arranged, multiple exemplar sets built. At 10 weeks: 18 of 23 skills had generalized to school. Parent-administered probe accuracy: 79%.
"For 6 months we thought the therapy wasn't working. It was working — it just wasn't designed to travel yet." — Dev's father, Pinnacle Bengaluru
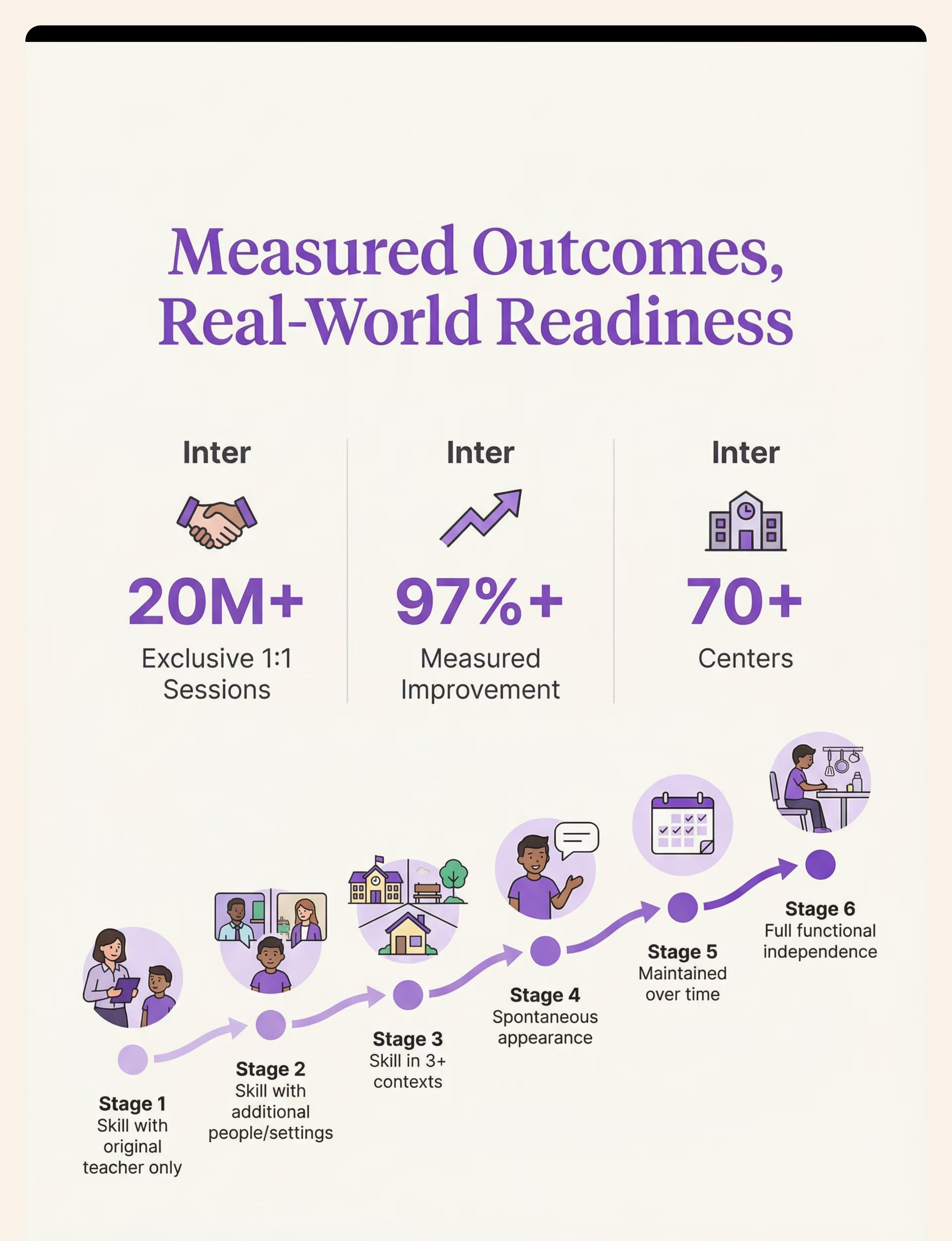
Outcomes are illustrative case composites. Individual results vary. Pinnacle center outcome data: 20M+ sessions, 97%+ measured improvement.

Connect With Other Parents Working on Generalization
ACT V: Community
Isolation is the enemy of adherence. You are not alone in this.
Join the Generalization Parent Group
Challenge-specific parent WhatsApp community for families working on skill transfer → pinnacleblooms.org/parent-groups
Pinnacle Parent Community Forum
Share data, ask questions, post wins, get support from parents 6 months ahead of you → pinnacleblooms.org/community
Local Parent Meetup
Pinnacle centers organize monthly parent support meetings. → Find my center
Connect With an Experienced Parent
A parent who has successfully programmed generalization and wants to mentor others → Request peer mentor
"Your experience — the weeks of patient implementation, the data collection, the moments your child's skill traveled for the first time — that knowledge can shorten the journey for the next family. Consider sharing your story."

Your Professional Support Team: 70+ Centers Nationwide
ACT V: Professional Support
Generalization Specialist (BCBA)
- Design formal generalization programs
- Conduct formal generalization probes
- Train all instructors consistently
SLP for Communication Transfer
- Program communication skill transfer across all conversational contexts
- Multiple exemplar training for language
- Parent-professional collaboration model
OT for Sensory Generalization
- Extend sensory and motor skills to natural environments
- Community-based functional skill training
- ADL generalization programming
📞Book a Teleconsultation — Available in 16 languages → pinnacleblooms.org/teleconsult | Or call: 9100 181 181 (FREE, 24×7)
"Home-based generalization works best when supported by professional guidance. The clinic gives you the protocol. The home gives you the repetition. Together, they create the functional skill."
The Research Library: For the Curious Parent
ACT V: Research
Deeper reading for families who want to understand the science behind every session.
📚 Stokes & Baer (1977)
Foundational paper establishing that generalization must be systematically programmed. The most-cited paper in generalization research. JABA, 10(2), 349–367 | Search PubMed →
📚 NCAEP Evidence-Based Practices Report (2020)
Classifies multiple exemplar training, video modeling, and natural environment teaching as EBPs targeting generalization in autism. | Access →
📚 PRISMA Systematic Review (2024) — PMC11506176
16 articles confirming generalization-linked sensory integration interventions as evidence-based for ASD. DOI: 10.12998/wjcc.v12.i7.1260 | PubMed →
📚 Meta-Analysis — PMC10955541 (2024)
24 studies confirming therapy promotes generalization of social skills, adaptive behavior, and motor skills with measurable effect sizes. | PubMed →
📚 WHO Nurturing Care Framework (2018)
Global framework emphasizing caregiver-mediated interventions across all settings for sustainable developmental outcomes. | WHO NCF →
📚 Padmanabha et al. (2019) — India
Indian RCT of home-based interventions demonstrating significant outcomes in Indian pediatric population. Indian J Pediatr, DOI: 10.1007/s12098-018-2747-4

How GPT-OS® Uses Your Generalization Data
ACT V: Technology
What GPT-OS® Learns From L-956 Data
- Which generalization dimension is your child's current strength vs. barrier
- Optimal exemplar quantity for this learner
- Setting generalization velocity (how quickly settings transfer)
- Maintenance interval requirements
- Person generalization pattern (how many exposures before new instructor is accepted)
🔒 Privacy Assurance
All session data is encrypted, stored under DPDP Act 2023 compliance, and never sold or shared with third parties. Your data is used only to personalize your child's therapeutic plan and contribute to population-level insights.
"Your data helps every child like yours. When you record generalization probe results, you're contributing to the largest real-world evidence base for pediatric skill transfer in the world — 20M+ sessions."

Watch the Reel: 9 Materials That Help With Generalization
ACT V: Video
Reel L-956
Presented by the Pinnacle Blooms Clinical Consortium — BCBA Division with ABA, SLP, OT, SpEd, and NeuroDev perspectives integrated. Duration: 75–85 seconds.
Multiple Exemplar Sets
Same concept, many examples — the strongest predictor of generalization success
Portable Visual Supports
Same cue, every setting — the visual thread that connects contexts
Generalization Binders
Everyone on the same page — team coordination infrastructure
Real-World Objects
Therapy with actual life items — the most powerful exemplar type
Video Modeling Libraries
See it everywhere, do it everywhere — built-in generalization training
Generalization Probes
Measure transfer, don't assume it — what gets measured gets programmed
Community Teaching Kits
Bridge to real-world application before the child faces it cold
Maintenance Schedules
Keep skills alive over time — the investment protection system
Multi-Instructor Materials
Same skill, anyone can teach — robustness through distributed instruction
Share This With Your Entire Support Network
ACT V: Share
Consistency across caregivers multiplies impact. One parent implementing generalization creates limited results. An entire family network implementing generalization creates functional skills.
Share Buttons
Downloadable Family Guide
📄 The complete generalization protocol in 1 page — for spouses, grandparents, and teachers
For Grandparents & Extended Family
"[Child's name] is working on using skills they've learned in therapy in all settings, not just with their therapist. Here's what helps: 1. Use these same words when you ask them to do something. 2. When they get it right, say the reinforcement script. 3. Try the same task in different rooms and at different times. 4. You're teaching the skill to travel — and that's the most important job."
Teacher Communication Template
Dear [Teacher name], We are working on generalization programming for [child's name] at home and through [therapy center]. Our current target skills are [list]. We use [procedure] consistently. Would you be willing to review our generalization binder and support the same prompting procedures at school? Our therapist is happy to connect.

Frequently Asked Questions
ACT VI: FAQ
My child knows the skill in therapy but not at home. Is this common?
This is the most common pattern in structured pediatric therapy, and it is fully expected and fully addressable. Skills become bound to teaching contexts. With deliberate generalization programming — varied materials, multiple instructors, setting exposure — skills travel. You are not experiencing failure; you are experiencing the most common gap between therapy-room acquisition and functional use.
How long does generalization programming take?
Most families see early stimulus generalization within 2–4 weeks of consistent multiple-exemplar training. Setting generalization typically requires 4–8 weeks. Person generalization often follows within the same window. Community generalization is an 8–16 week target. Maintenance is ongoing.
Do I need a BCBA to program generalization?
A BCBA is ideal for designing formal programs and troubleshooting complex profiles. However, the principles on this page can be implemented at home by informed parents. For children with complex behavioral profiles or no generalization across multiple weeks, a BCBA consultation is recommended. Call 9100 181 181 for guidance.
Are these materials suitable for non-verbal children?
Yes. Generalization programming is especially important for AAC users and non-verbal children. Multiple exemplar training works across response modalities (pointing, eye gaze, device activation). Portable visual supports are directly applicable. Video modeling is highly effective for children who learn visually.
Can we work on generalization at the same time as new skill acquisition?
Yes — and ideally, you should. Begin multiple exemplar training from session one of acquisition, not after mastery. Don't wait for a skill to be "mastered" before beginning generalization — by then, the stimulus binding is very strong. Build generalization into acquisition from day one.
We tried generalization before and it didn't work. What was missing?
The most common reasons: (a) only one person was teaching, (b) only one type of material was used, (c) probe data was never collected so "working" was assumed not measured, (d) maintenance wasn't programmed. Review which materials in Card 09 were not part of the previous program.

Your Next Step. Start Today.
ACT VI: Act Now
A skill isn't truly learned until it travels.
You now know how to make it travel. You have the science, the materials, the step-by-step protocol, the troubleshooting framework, and the full support of the Pinnacle Blooms Network behind you. The only remaining step is to begin.
🏛️ OT • SLP • ABA/BCBA
Validated by Pinnacle Blooms Consortium®
SpEd • NeuroDev • CRO
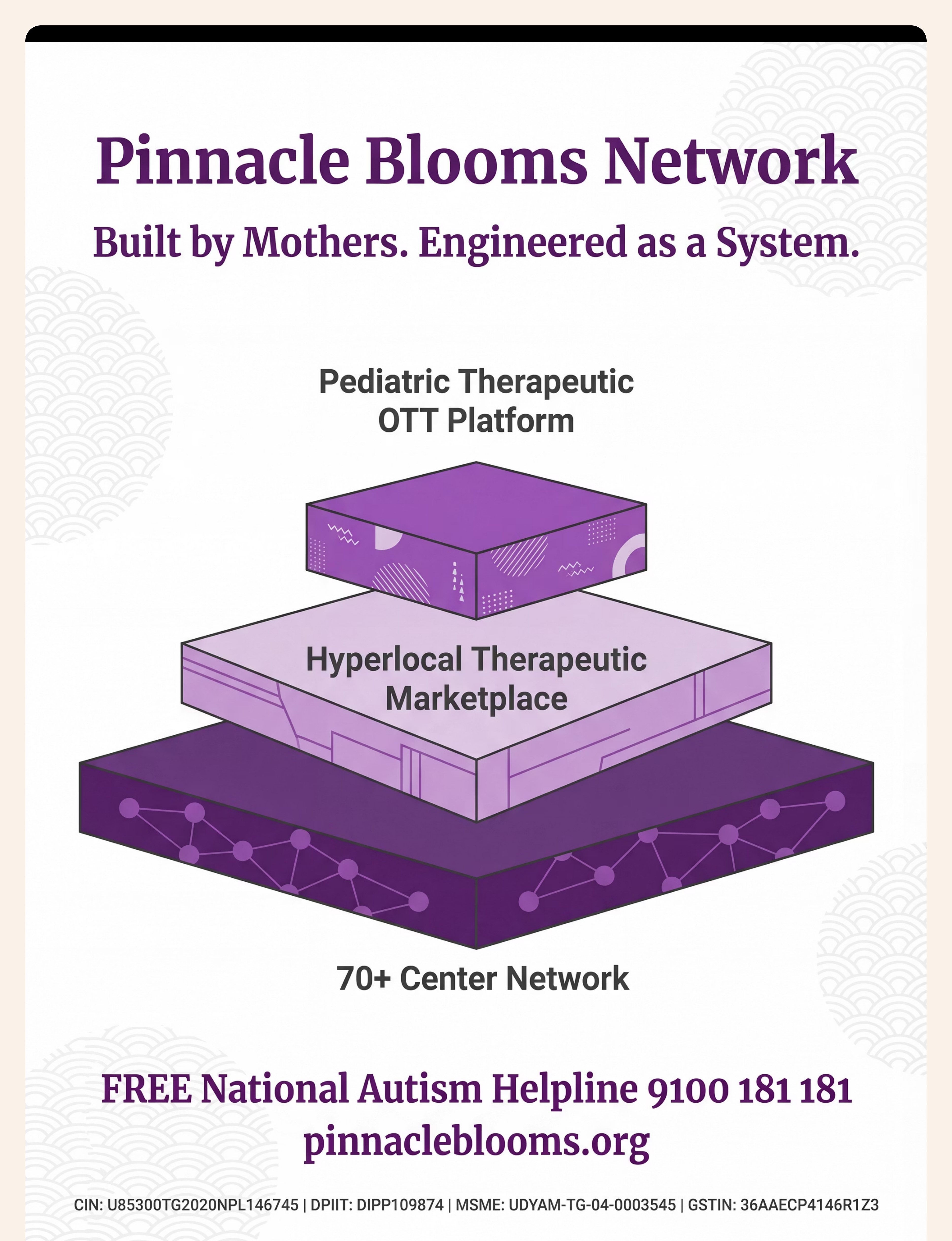
Built by Mothers. Engineered as a System.
FREE Helpline: 9100 181 181
16 languages | 24×7 | pinnacleblooms.org
Preview of 9 materials that help with generalization Therapy Material
Below is a visual preview of 9 materials that help with generalization therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

The Pinnacle Promise
ACT VI: Close
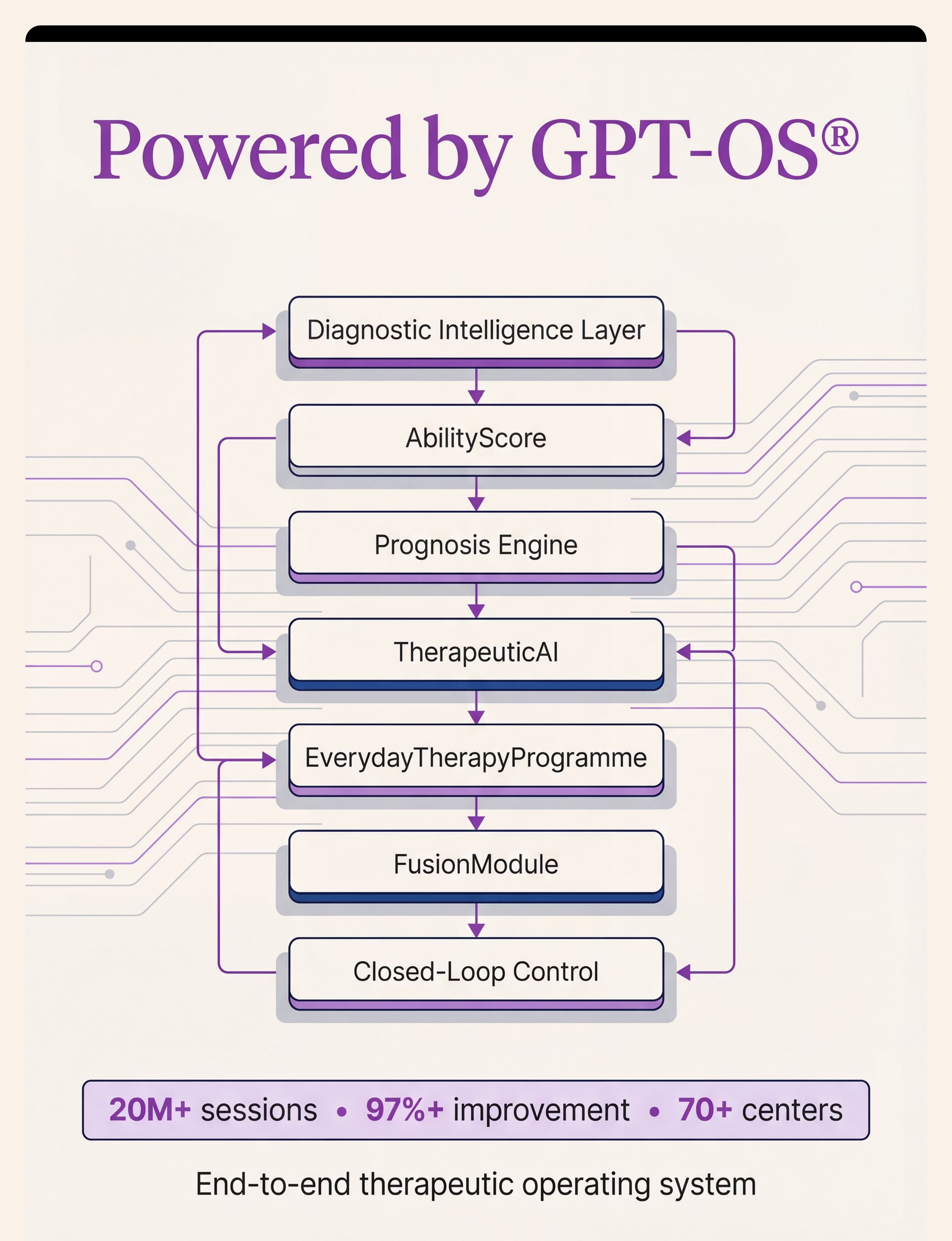
🏛️ Pinnacle Blooms Network®
Global Pediatric Therapeutic Operating System
GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™
20M+ Sessions | 97%+ Improvement
70+ Centers | 70+ Countries | Patents Filed: 160+ Nations
CRO • Pediatric OT • Pediatric SLP • ABA/BCBA • SpEd • NeuroDev • WHO/UNICEF Aligned
"From fear to mastery."
One technique at a time. Built by Mothers. Engineered as a System.
Medical Disclaimer & Legal
This content is educational and informational only. It does not constitute medical advice, clinical diagnosis, or individualized treatment programming. Generalization protocols should be designed and supervised by qualified BCBAs, SLPs, OTs, or licensed special educators based on individual learner assessment. Individual results vary.
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DIPP8651 | care@pinnacleblooms.org
FREE National Autism Helpline: 9100 181 181 | 16 languages | 24×7