
Balance & Stability Building for Frequent Falling
You are not failing. Your child's balance system is speaking — and it can be strengthened. This consortium-validated intervention protocol addresses the vestibular, proprioceptive, core stability, and motor planning systems that underlie frequent falling — with 9 clinically validated materials you can use at home, starting today.

The Recognition Moment
She's five years old. She falls walking across the living room — no toy on the floor, no rug edge, nothing visible. She just goes down. Running in the backyard, she falls hard while her brother stays upright. Playground equipment that other children her age handle easily sends her tumbling. Her knees are permanently bruised — one set fading while new ones form on top. She's started calling herself "the falling girl."
This page exists for that moment. For you, standing in the kitchen wondering what you're missing. For the parent who has Googled every variation of "why does my child fall so much" at midnight. For the caregiver who has watched their child avoid the playground because they know what comes next.
🏛️Pinnacle Blooms Consortium — Clinical Research Organization • Occupational Therapy • Physical Therapy • ABA • Special Education • NeuroDevelopmental Pediatrics. Explore all Motor Development techniques →
You Are Among Millions
Frequent falling is not rare. It is not your fault. And it is addressable — with precision, with evidence, and with your hands. Millions of families across the world navigate this exact challenge every single day.
80%
Sensory Processing Difficulties
of children with ASD display sensory processing difficulties including balance and postural control challenges (PRISMA Systematic Review, 2024)
1 in 6
Global Coordination Difficulties
children globally experience developmental coordination difficulties that impact balance and motor function
28M+
Families in India
families in India alone navigate gross motor and balance challenges in their children
You are among millions of families navigating this exact challenge. Research confirms: PMC11506176 (PRISMA 2024), PMC10955541 (Meta-analysis, World J Clin Cases 2024), DOI: 10.12998/wjcc.v12.i7.1260. What is sensory processing? →

Balance Development: The Typical Trajectory
Frequent falling beyond age 3 that significantly exceeds typical clumsiness — especially with fear, avoidance, or impact on daily activities — signals that the balance, vestibular, or proprioceptive systems need targeted support. Here is where your child is, and where we are heading together.
6–12 Months
Sits independently; pulls to stand. If delayed: Falls backward/sideways from sitting; difficulty maintaining standing posture.
12–24 Months
Walks independently; runs with help on stairs. If delayed: Wide-based, stiff walking; unsteady running; avoids stairs.
2–3 Years
Walks up/down stairs; stands on one foot briefly. If delayed: Falls on stairs; cannot balance on one foot.
3–5 Years ⭐ KEY ZONE
Hops; balances 5+ seconds; navigates playground. If delayed: Falls multiple times daily, avoids climbing, fears movement.
5–7 Years
Rides bicycle; skips; complex playground navigation. If delayed: Persistent falling, bruising, activity avoidance.
Co-occurring challenges commonly seen: Low muscle tone (A-090) • Toe walking (A-092) • Clumsy/uncoordinated movement (A-093) • Delayed gross motor milestones (A-089) • Avoidance of physical activities (A-094). Related: Delayed Gross Motor Milestones →
What's Happening in Your Child's Brain
Balance isn't one thing — it's an orchestra. Three sensory systems send information to the brain simultaneously, which then coordinates hundreds of muscles to keep the body upright. When any system sends unclear or delayed signals, the orchestra falls out of sync — and so does your child.
The Three Systems That Keep Us Upright
- Vestibular System (inner ear) — detects head position and movement relative to gravity
- Proprioceptive System (muscles, tendons, joints) — senses body position without looking
- Visual System (eyes) — tracks the body's position relative to the environment
These three streams converge in the cerebellum and brainstem, which coordinate the motor response — activating the correct muscles at the correct time.
Plain English for Parents
This is a wiring difference, not a behavior choice. Your child isn't careless. Their brain is working with imprecise information from the balance system, the body position system, or both.
The critical insight: each of these systems can be strengthened. The vestibular system responds to movement input. Proprioception responds to deep pressure and heavy work. Core muscles respond to progressive strengthening. The brain rewires with structured, repeated practice.
Research: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660

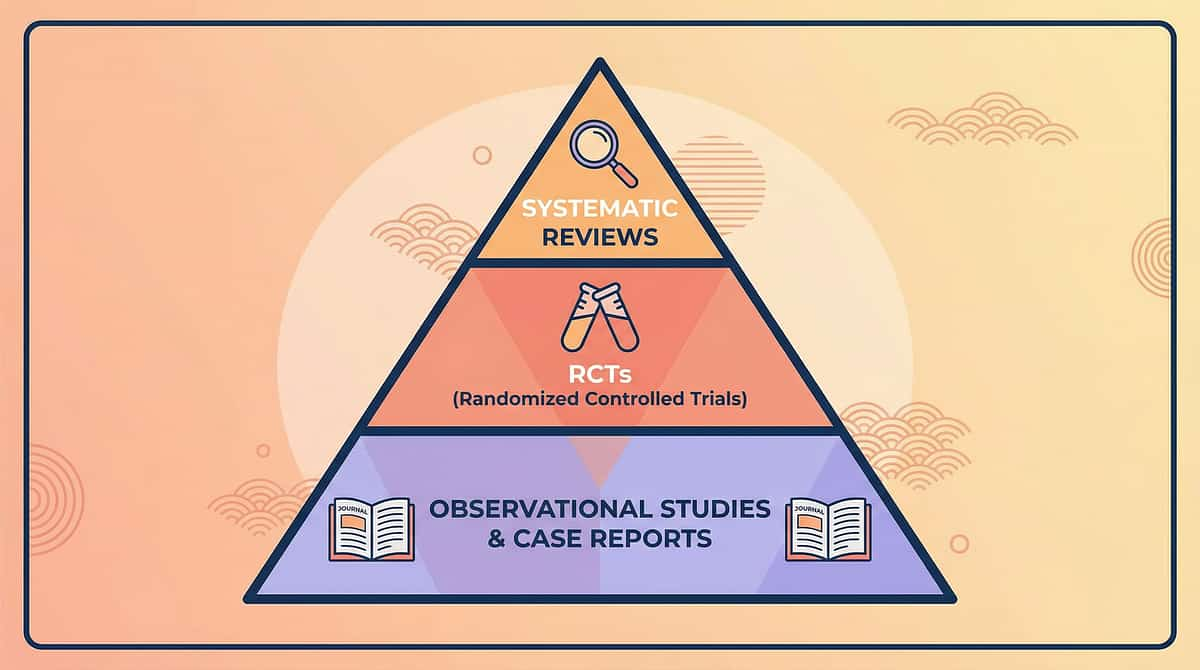
Evidence Grade: LEVEL I–II — Strong Evidence Base
16 Studies Confirmed
PRISMA Systematic Review (2024): Sensory integration intervention meets criteria for evidence-based practice for children with ASD. PMC11506176
24 Studies Analyzed
Meta-analysis demonstrates sensory integration therapy effectively promotes gross motor skills, fine motor skills, adaptive behavior, and sensory processing. PMC10955541
Indian RCT Confirmed
Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population (Indian J Pediatr, 2019). DOI: 10.1007/s12098-018-2747-4
Key finding in one sentence: Balance and motor interventions using structured materials produce measurable improvement in postural control, dynamic balance, and functional mobility in children with neurodevelopmental conditions. Clinically validated. Home-applicable. Parent-proven.

The Technique: What It Is
Gross Motor
Balance & Postural Control
Vestibular Processing
Sensory Integration
A progressive, multi-material intervention protocol that targets the underlying systems responsible for maintaining upright posture and dynamic balance in children who fall excessively. This is NOT teaching the child to "be more careful" — it is systematically strengthening the vestibular processing, proprioceptive awareness, core stability, and motor planning systems so that balance becomes automatic rather than effortful.
Age Range
2–10 years
Session Duration
10–20 minutes per session
Frequency
3–5 times per week
Total Protocol
8–12 weeks (progressive)
Canon Materials Mapped: Balance Boards • Stepping Stones • Therapy Balls • Vestibular Swings • Proprioceptive Tools • Core Equipment • Obstacle Courses • Sensory Mats • Balance Games. Canon Materials: Balance & Vestibular Equipment →
Who Uses This Technique
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type." Balance requires sensory processing (OT), physical capacity (PT), behavioral engagement (ABA), and environmental accommodation (SpEd) — all working together.
Occupational Therapist (PRIMARY LEAD)
Addresses sensory integration, vestibular processing, proprioceptive awareness, and functional balance for daily activities. OTs design the sensory-motor foundation that supports balance.
Physical Therapist (CO-LEAD)
Targets muscle strength, postural control, gait patterns, and progressive balance training. PTs address the biomechanical foundations of staying upright.
Board Certified Behavior Analyst
Designs reinforcement schedules for balance activities, addresses avoidance behaviors, builds confidence through systematic exposure and success.
Special Educator (SUPPORTING)
Ensures classroom and school adaptations for the child's balance needs. Modifies physical education participation and communicates with school staff about safety and accommodations.

Precision Targeting — What This Protocol Addresses
This is not a random activity. Every session systematically challenges specific neurological and physical systems at multiple levels, from immediate balance mechanics to long-term life participation.
Observable Behavior Indicators: Falls per day decrease • Recovers balance without falling • Navigates stairs with reduced support • Plays on playground equipment • Participates in running and movement games • Self-confidence in physical activities increases. Research: PMC10955541 — Meta-analysis confirms sensory integration therapy promotes motor skills (primary), adaptive behavior (secondary), and social skills (tertiary) across 24 studies.

Your Balance-Building Toolkit — 9 Materials
These 9 clinically validated materials form the complete home intervention toolkit. Start with essentials under ₹3,000: Balance board (₹800–1,500) + Therapy ball (₹600–1,000) + Stepping stones or tape on floor (₹600–1,500 or free).
# | Material | Canon Category | Price Range | Buy | |
1 | Balance Board / Wobble Board | Balance Challenge Equipment | ₹800–4,000 | ||
2 | Stepping Stones / Balance Beam | Balance Challenge Equipment | ₹600–3,500 | ||
3 | Therapy Ball / Peanut Ball | Core & Postural Equipment | ₹600–2,500 | ||
4 | Vestibular Swing Equipment | Sensory Processing Equipment | ₹2,000–15,000 | ||
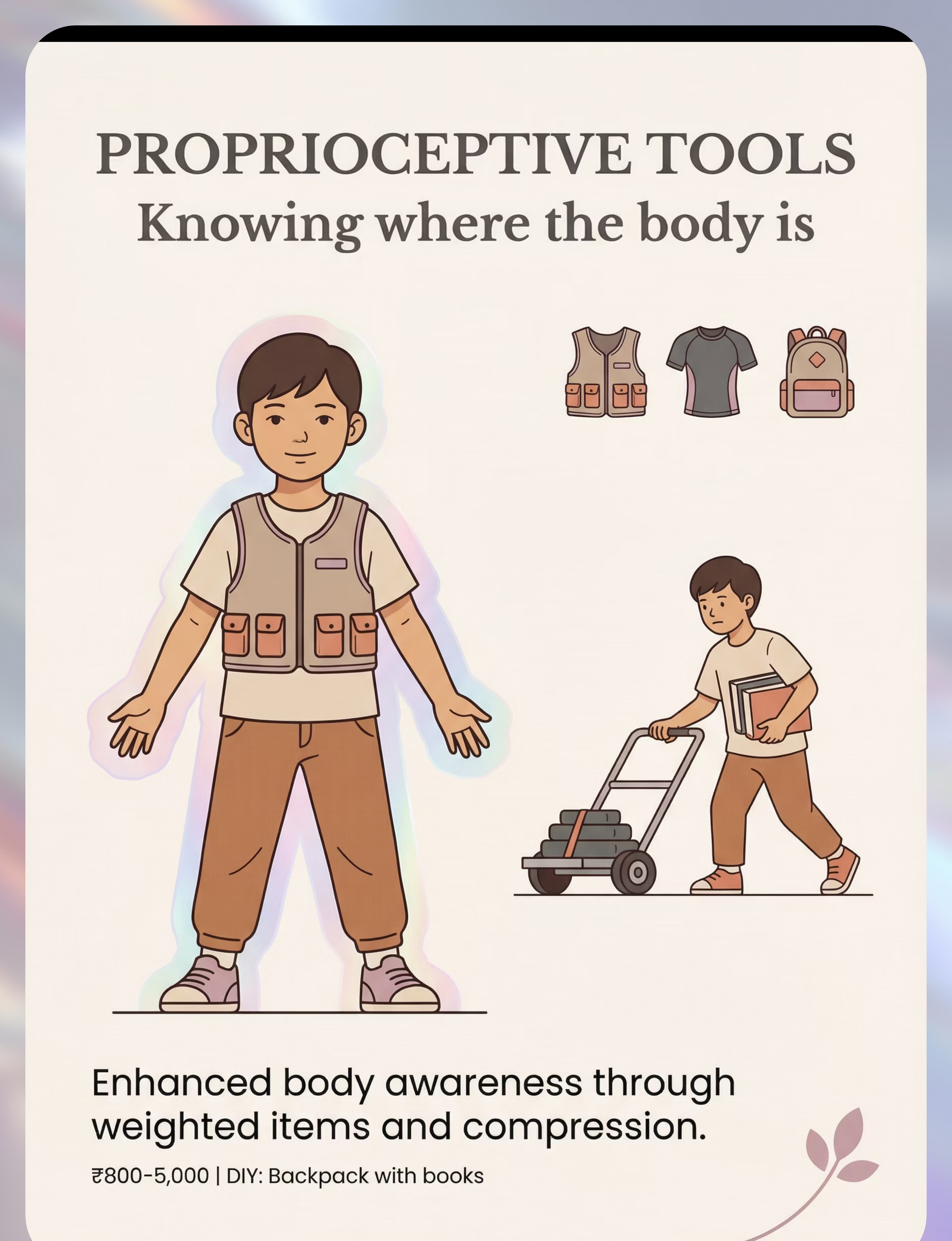
5 | Proprioceptive Tools (Weighted Vest, Compression) | Sensory Processing Equipment | ₹800–5,000 | ||
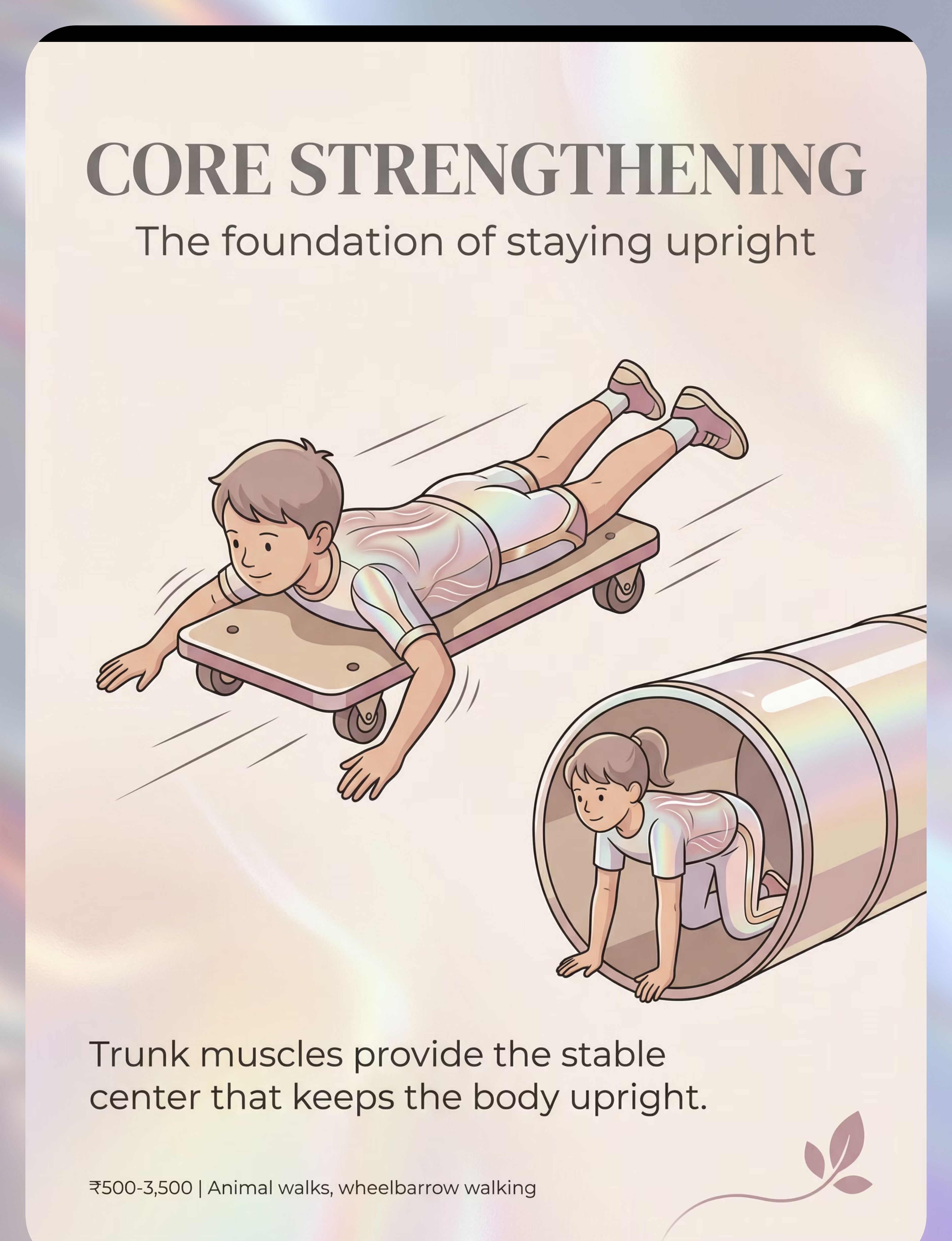
6 | Core Strengthening Equipment (Scooter Board, Tunnel) | Core & Postural Equipment | ₹500–3,500 | ||
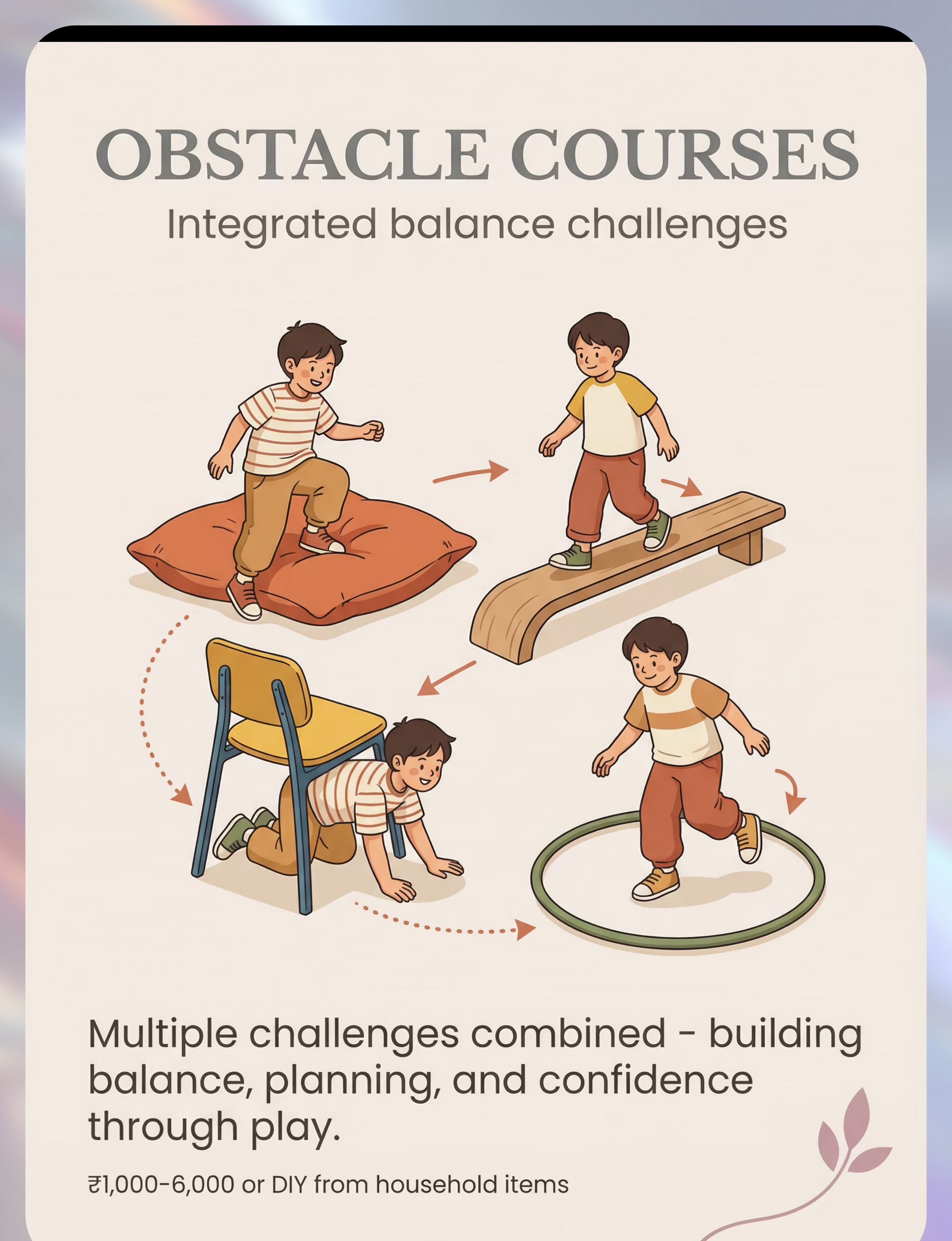
7 | Obstacle Course Materials | Integrated Practice | ₹1,000–6,000 or DIY | ||
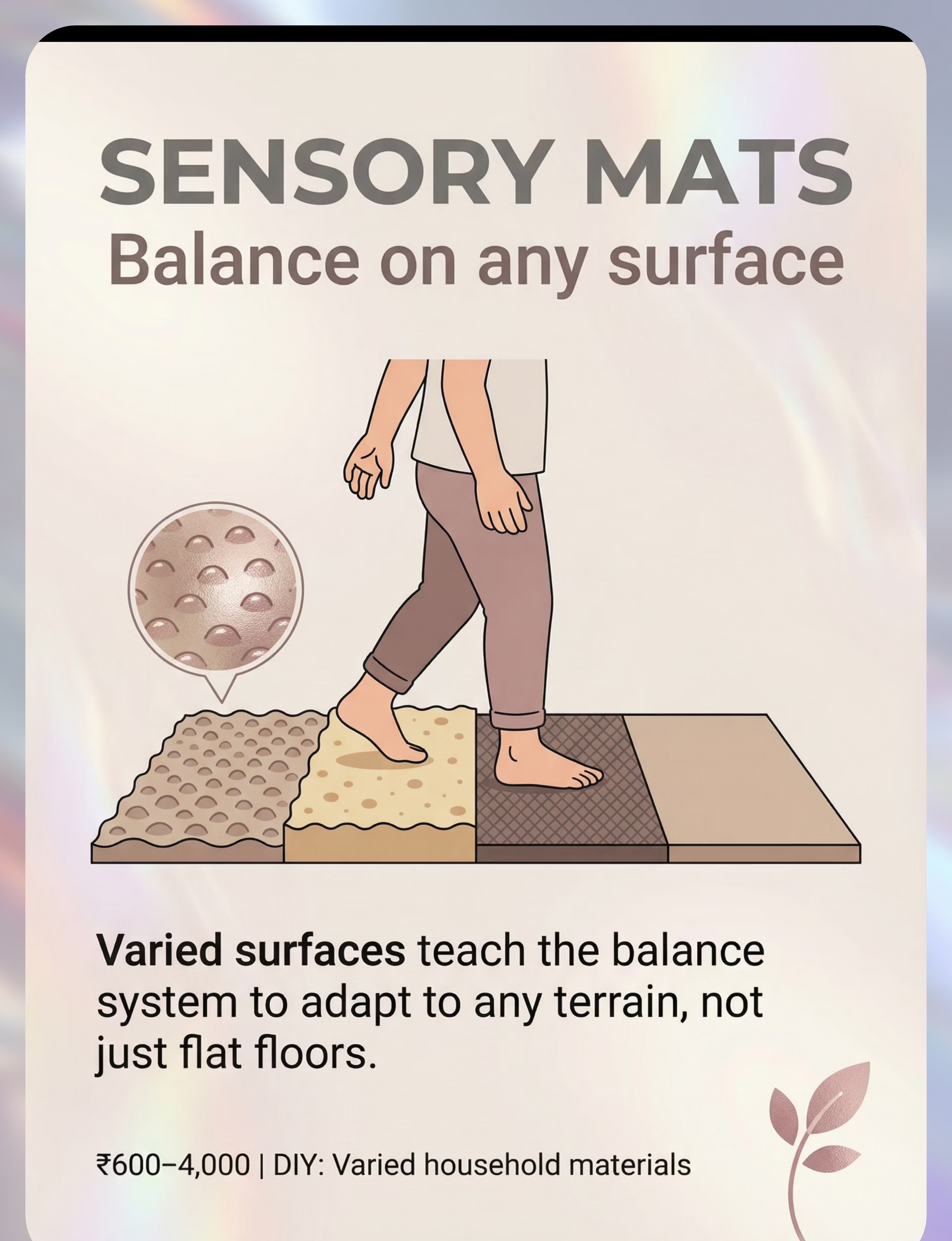
8 | Sensory Mats / Textured Surfaces | Surface & Environment | ₹600–4,000 | ||
9 | Balance Games (Hopscotch, Movement Cards) | Integrated Practice | ₹300–2,000 or free |
Total Investment Range: ₹300–15,000. Canon Materials: Balance Board → | Canon Materials: Therapy Ball → | Canon Materials: Therapy Swing →
Every Family Can Start Today — Zero-Cost Alternatives
Not every family can order from Amazon. Not every village has same-day delivery. This card ensures every parent can begin TODAY with household items. The therapeutic principles are identical — the vestibular system responds to movement regardless of whether it comes from a ₹15,000 therapy swing or a playground swing.
Material | Buy This | Make This (Free) | |
Balance Board | Rocker/Wobble board (₹800+) | Thick plywood on half-round PVC pipe. Sand edges smooth. | |
Stepping Stones | Balance stone set (₹600+) | Foam pieces, carpet squares taped to floor, sturdy upturned containers | |
Balance Beam | Wood/foam beam (₹800+) | Tape line on floor → wooden board flat → board on bricks | |
Therapy Ball | Physio ball (₹600+) | Standard exercise ball, partially deflated for stability | |
Vestibular Input | Platform swing (₹2,000+) | Playground swings, blanket swing (two adults), spinning on swivel chair | |
Proprioceptive Input | Weighted vest (₹800+) | Backpack with books (5-10% body weight). Heavy work: carrying groceries, pushing laundry basket. | |
Core Strengthening | Scooter board (₹500+) | Bear walks, crab walks, army crawls, wheelbarrow walking, superman pose | |
Obstacle Course | Course set (₹1,000+) | Couch cushions, tape lines, pillows, blanket tunnels, hula hoops, chairs to crawl under | |
Balance Games | Game sets (₹300+) | Freeze dance (free), Simon Says with balance poses, flamingo contests, hopscotch (chalk = free) |
When clinical-grade is non-negotiable: If your child has severe vestibular dysfunction, significant hypotonia, or a medical condition contributing to falling, professional OT/PT assessment and clinical-grade equipment may be necessary. DIY versions are excellent for home practice but do not replace professional evaluation.

⚠️ Safety Gate — Read Before Starting Any Balance Activity
Balance activities involve controlled instability. Read all safety guidelines before beginning. Frequent falling increases head injury risk — monitor for concussion signs after significant falls. Consider protective headgear for children with very frequent, uncontrolled falls, especially if protective responses are poor.
🔴 RED — Do NOT Proceed If:
- Child has had a recent head injury or concussion — seek medical clearance first
- Child is experiencing dizziness, nausea, or vertigo outside of activities
- Child has a seizure disorder and activities are not cleared by neurologist
- Child has an undiagnosed progressive condition (balance is getting worse)
- Child is ill, fatigued, or in a dysregulated state
🟡 AMBER — Proceed with Modification:
- Significant fear of movement — start with lowest-challenge activities only, with full physical support
- Very low muscle tone — ensure adequate physical support, reduce challenge level
- Recovering from a fall-related injury — modify to protect injured area
- Child becomes visibly anxious — reduce challenge, increase support, add preferred activities
🟢 GREEN — Go When:
- Child is rested, fed, and in a calm-alert state
- Environment is clear of hazards with safe landing surfaces
- Parent is ready to supervise actively throughout
- Materials are checked for stability and safety
- Child shows willingness (not coerced)
🚨STOP IMMEDIATELY IF: Child hits head during any activity | Child shows signs of concussion (confusion, vomiting, drowsiness) | Child becomes severely distressed and cannot be calmed | Child reports pain (not just challenge or effort)

Set Up Your Balance Therapy Space
Your physical environment is a therapeutic tool. The right setup reduces risk, increases challenge precision, and helps your child's brain receive cleaner sensory signals. Barefoot is often best for balance work — tactile feedback from feet supports proprioception.
1
Clear Floor Area
Minimum 2m × 2m clear space. Remove all tripping hazards, sharp-edged furniture, and small objects from the movement zone.
2
Soft Landing Surface
Mat, thick carpet, or foam padding beneath any elevated equipment — balance boards, stepping stones above floor level.
3
Wall or Stable Furniture
Within arm's reach for the child to grab if they lose balance. This is a safety and confidence tool.
4
Parent Position
Beside and slightly behind the child — close enough to catch, far enough to not restrict movement. This is your therapeutic zone.
5
Lighting & Sound
Well-lit. The visual system supports balance — dim lighting makes balance harder. Low background noise; soft rhythmic music works for some children.
Remove from the space: Screens/TV, noisy toys, unsupervised siblings, pets, breakable objects. Research: Sensory Integration Theory (Ayres) — Environmental setup is a core therapeutic principle. PMC10955541

Pre-Session Readiness Check (60 Seconds)
The best session is one that starts right. Pushing through when the child isn't ready creates negative associations with balance activities — the opposite of what we want. Run this check before every session.
✅ Child has eaten within the last 2 hours
Not hungry, not immediately after a large meal
✅ Child has slept adequately
Not overtired — fatigue impairs balance significantly
✅ Child is in a calm-alert state
Not mid-meltdown, not highly agitated, not drowsy
✅ No recent significant fall or injury
Not sore from a fall earlier today
✅ Child shows willingness to engage
May be neutral — doesn't need to be enthusiastic — but should not be actively resistant
✅ No signs of illness, environment is set up
No fever, no nausea, no dizziness. Card 13 completed.
Decision Gate:✅ All checked → GO. | ⚠️ 1–2 concerns → MODIFY: use simplest, floor-level activities with full hand support, shorter duration. | 🛑 3+ concerns → POSTPONE: do a calming activity instead (reading, gentle music, resting together). Try again tomorrow.

Step 1: The Invitation
30–60 Seconds
Do not command. Invite. Your body language matters as much as your words. Get down to the child's level. Smile genuinely. Touch the material yourself first — demonstrate it's safe. Step on the balance board yourself. Walk the stepping stones. Sit on the ball.
Say: "Hey [child's name], I have something really fun to try today! Look at this [balance board/stepping stones/ball]. Want to see what it does? I'll show you first!"
Acceptance Looks Like
Approaches the material • Watches with interest • Reaches to touch • Steps on with your support • Even just looks — that's a start
Resistance & What to Do
Turns away → "That's okay! It'll be here when you're ready. Want to watch me?" | Says "no" → Accept it. Curiosity often follows. | Shows fear → Demonstrate safety first.
Timing: 30–60 seconds. If no engagement after 60 seconds, move to a different, easier material or play a simple movement game instead. Research: ABA Pairing Procedures | OT "Just-Right Challenge" principle.
Step 2: The Engagement
1–3 Minutes
The child is curious. Now deepen the interaction by introducing the therapeutic material. The goal in this phase is simple: let them feel the wobble WITH your full support. They are learning that unstable surfaces are survivable.
"Okay, let's try it together! I'll hold both your hands. You step on, and I'll keep you safe."
Place board against wall
Limits tilt to one direction. Maximum safety for first exposure.
Hold both hands firmly
Guide the child to step onto the board with one foot, then the other. Full support.
Let them feel the wobble
WITH your full support. The sensation is the lesson. Don't prevent it — support through it.
Reinforce immediately
The MOMENT the child stands on the board, even for 1 second: "Look at YOU! You're balancing! Your body is doing amazing work right now!"
Child Response Guide: Engagement (smiling, adjusting) → Excellent, this is working. | Tolerance (neutral, allows it) → Good, continue gently. | Avoidance (trying to step off) → Reduce challenge. Hold firmly. "5 more seconds then we're done." Stop before the child wants to stop. Leave them wanting more.
Step 3: The Core Balance Challenge
3–8 Minutes
This is the active therapeutic ingredient. The child is engaged. Now systematically challenge their balance at the edge of their ability. Quality over quantity — 3–8 minutes of active balance challenge with real concentration is worth more than 20 minutes of passive tolerance.
❌ Common Execution Errors
- Holding the child too tightly — they need to feel the wobble to learn
- Progressing too fast — one level per session is often right
- Correcting verbally instead of physically — guide with hands, not words
✅ What Success Looks Like
The child should be working — mild effort, visible concentration — but not distressed. Ideal: concentrating, adjusting, recovering balance, showing growing steadiness. Concerning: crying, going rigid with fear → STOP. Return to Step 1.

Step 4: Repetition & Variation
3–5 Minutes
"3 good reps > 10 forced reps."
Target repetitions: 3–5 rounds of the core challenge. Variation maintains engagement while deepening the neurological learning — the brain is strengthening the same pathways through different inputs.
Change the Game
"Can you balance while I count to 10? While we sing a song? While you hold a stuffed animal?"
Add Targets
Place toys at different heights and positions for the child to reach while balancing — adds vestibular and proprioceptive challenge.
Change Materials
Shift from balance board to stepping stones to therapy ball — keeps engagement high across a session.
Modulate Challenge
More support → less support → add head turns → add reaching. Progress within session or across sessions.
Satiation Indicators — Stop When You See: Looking away repeatedly • Trying to get off the activity • Quality of balance attempts declining • Increased irritability or frustration • Body going limp or very stiff. When you see these: "Great job today! You worked so hard. We're all done with balance. Let's [preferred activity]."

Step 5: Reinforcement — Immediate, Specific, Enthusiastic
Timing: Within 3 seconds of the desired behavior. Not at the end of the session — IN THE MOMENT. Celebrate the attempt, not just the success. A child who steps onto a balance board and wobbles for 2 seconds has made a brave choice. That matters.
✅ Say This
- "Your body just balanced for FIVE whole seconds! That's your BEST yet!" (Specific)
- "Did you feel that? Your body caught itself! Your balance system is getting stronger!" (Body-aware)
- "You wobbled AND you stayed up! That's what strong balance looks like!" (Process praise)
❌ Avoid This
- "Good girl." — Too vague, provides no information
- "Wow!" — No information about what was good
Reinforcement Menu
- Verbal praise (always — specific to what the child did)
- High-five, thumbs up, clapping
- Preferred activity after session
- Sticker chart / token system
- Video of the child balancing to watch together

Step 6: Cool-Down & Transition
1–2 Minutes
No session ends abruptly. The transition out of balance work is as important as the session itself. Abrupt endings increase refusal and negative associations with the activity — a smooth cool-down preserves the positive experience and prepares the nervous system to return to baseline.
1
Transition Warning (2 minutes before end)
"Two more balances, then we're all done!"
2
Countdown
"Last one! Make it your best one!"
3
Cool-Down Activity
Gentle rocking on therapy ball • Bear hug / deep pressure hug • Lying on cushion or beanbag • Slow, controlled stretching • Quiet reading or music for 1–2 minutes
4
Material Put-Away Ritual
"Can you roll the ball back to its spot? Can you put the stepping stones in the box?" Proprioceptive input (heavy work) AND builds routine.
5
Transition Cue
"Balance time is all done. You worked so hard today. Now it's [next activity] time."
Research: Visual supports and transition strategies classified as evidence-based practice for autism — NCAEP Evidence-Based Practices Report (2020).

Capture the Data: Right Now
"60 seconds of data now saves hours of guessing later." This data is what transforms hope into evidence. When your therapist asks "How's she doing at home?" — you'll have the answer, not just an impression. Record immediately after each session, while it's fresh.
Data Point | How to Record | Example | |
Falls during session | Tally count | ㅣㅣㅣ = 3 falls | |
Longest balance hold | Seconds (use phone timer) | 8 seconds on balance board | |
Engagement level | 1-5 rating (1=refused, 3=tolerated, 5=enthusiastic) | 4 — engaged, asked to continue |
Optional additional data: New skill observed | Challenge noted | Child's emotional state
1
📥 Download Tracking Sheet
Balance Tracking Sheet PDF — Print and post on your refrigerator for daily recording.
2
📱 GPT-OS® Digital Tracker
Log sessions digitally with automatic progress graphs and trend analysis. Log in →
Troubleshooting — Because Most Sessions Don't Go Perfectly
"Session abandonment is not failure — it's data." If the child couldn't engage today, that information helps you plan a better session tomorrow. Here are the most common problems and evidence-based responses.
1
Child refused to step on the balance board
Normal, especially early on. Place the board where the child can see it. Step on it yourself. Let the child come to it on their own timeline. Try a lower-challenge option first (balance disc on the floor).
2
Child became fearful and immediately got off
Too much challenge too fast. Place the board against a wall. Hold both hands firmly. Count to 3 and celebrate wildly. Build from there — one second at a time.
3
Child fell off and got hurt
Ensure soft landing surface. Reduce challenge level. Increase support. Falls during balance work are expected — minor bumps are part of learning. Significant falls mean the challenge is too high.
4
Child engaged for 2 minutes then lost interest completely
2 minutes of engaged balance work IS a full session for a young child or beginner. Celebrate it. Build duration gradually over weeks — not days.
5
Child cried and I forced the session to continue
Stop. A forced session teaches the child to fear balance activities. Reset tomorrow with a much easier version. Pair materials with preferred activities first. Trust rebuilds slowly.
6
No improvement after a week / Child falls MORE after sessions
Weeks 1-2 show tolerance, not mastery (see Card 23). Temporary fatigue can cause increased falling immediately post-session — ensure adequate rest. If falls increase persistently over days, reduce intensity and consult OT/PT.
Adapt & Personalize This Protocol
No two children are identical. This protocol is a framework, not a prescription. Use the difficulty slider and profile modifications below to find your child's precise starting point and progression path.
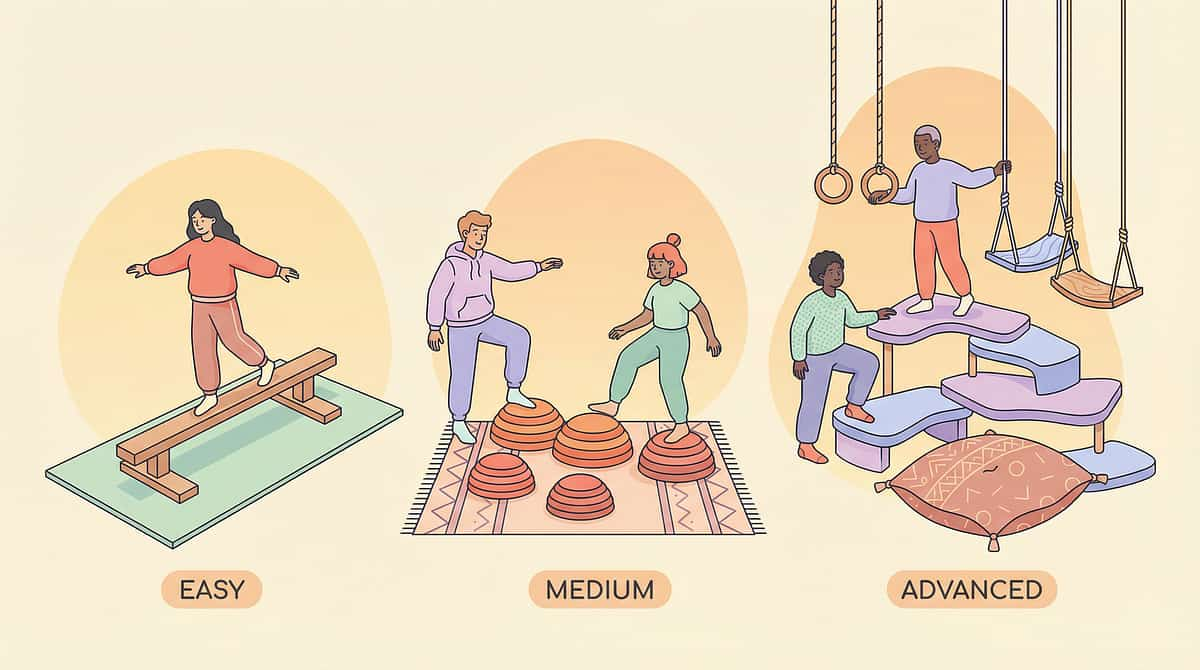
1
EASIEST — Floor-Level, Maximum Support
Tape line on floor, walk with hand held • Sit on therapy ball with adult holding at hips • Stand on partially deflated disc with wall support
2
MODERATE — Low-Level, Decreasing Support
Balance board against wall, one hand held • 3 stepping stones on floor with fingertip support • Simple 3-station obstacle course, level surfaces
3
ADVANCED — Elevated, Independent
Balance board free-standing, no support • Stepping stones at varied heights, independent • Complex 6+ station obstacle course, varied surfaces
By Sensory Profile
- Sensory Seeker: More vestibular input, faster pace, dynamic games, more challenge to engage
- Sensory Avoider: Very slow progression, maximum support, calming activities before/after, never force
- Low Muscle Tone: Core emphasis, shorter duration, peanut ball, rest breaks built in
By Day Type
- For Bad Days: Floor-level only. Full support. 2-3 minutes maximum. End with success, however small.
- For Breakthroughs: Add ONE new challenge. Record it. Celebrate it. Don't add five — consolidate first.

Week 1–2: Tolerance & Willingness
Progress: 15%
This is the hardest phase — effort without visible results. Trust the process. Neural pathways are forming beneath the surface. Your consistency is the active ingredient at this stage.
1
✅ What Progress Looks Like NOW
- Tolerates balance board for 5 → 10 seconds
- Steps onto stepping stones with help (previously refused)
- Sits on therapy ball without crying
- Engages in 2–3 minutes of balance activities
- Resistance decreasing — less "no," more "okay"
2
❌ Not Progress Yet (Manage Expectations)
- Falling frequency has NOT decreased yet — this takes weeks
- Independent balance has NOT appeared yet
- Child is NOT excited about activities (neutral tolerance IS progress)
"If your child tolerates the balance board for 3 seconds longer than last week — that's real progress."
Research: PMC11506176 — Sensory integration intervention outcomes emerge across 8-12 week timelines. Early-phase indicators focus on tolerance and participation rather than skill mastery.

Week 3–4: Neural Pathways Forming
Progress: 40%
Something shifts in weeks 3-4. The daily sessions have begun to build the neural infrastructure that supports automatic balance. You may notice you're more confident too — your hands are supporting less, your worry is decreasing. You're seeing what's possible.
Child anticipates balance time
May approach materials or ask for them — a complete reversal from week 1 refusal.
Balance hold times increasing measurably
Your tracking data (Card 21) now shows a clear upward trend — this is the neural pathway forming.
Self-correction appearing
You see the wobble-catch-recover pattern. The child's brain is beginning to correct automatically.
Generalization seeds sprouting
Walking along curbs outside of session. Standing on one foot briefly during play. Attempting stairs with less grip on the railing.
When to increase intensity: If the child consistently succeeds at the current level across 3+ sessions, increase ONE variable: duration OR support reduction OR surface challenge. Not all three at once.

Week 5–8: Functional Balance Emerging
Progress: 75%
By weeks 5-8, balance is no longer purely effortful — it is beginning to become automatic. Generalization is the key indicator here: skill appearing outside of structured sessions, in the real world, without prompting.
✅ Mastery Criteria
- Falls per day decreased by 50%+ from baseline
- Stands on balance board independently for 15+ seconds
- Crosses stepping stones with minimal or no support
- Navigates stairs with reduced railing dependence
- Walks on grass, slopes, uneven surfaces with fewer falls
🌍 Generalization Indicators
- Balance improvements visible at school and playground
- Teacher reports increased physical activity participation
- Child runs, plays, climbs with more confidence
- Spontaneous physical play returning: "Watch me, Mom!"
🏅 "Mastery unlocked" when: Child's falls are within typical range for age AND child participates in age-appropriate physical activities without excessive fear or avoidance. Maintenance check: If you skip 3-4 days and the child maintains gains — the skill is consolidating. If balance regresses immediately — more practice is needed.

🎉 You Did This.
Your child arrived at this page falling multiple times a day. Knees permanently bruised. Calling themselves "the falling girl." Refusing to try. You — parent, caregiver, champion — spent weeks kneeling on the floor next to a balance board. Holding hands on stepping stones. Counting seconds on a therapy ball. Building obstacle courses from couch cushions.
"From fear to mastery. One technique at a time."
She doesn't call herself "the falling girl" anymore. She says "watch me, Mom" — and then runs.
📸 Milestone Photo
Take a photo of your child on their balance board today. Compare it to week 1. Show it to them. This is a milestone photo.
📖 Mark This Day
Write today's date in your journal: the day balance changed. This moment matters — it is evidence of what love and consistency build.
🤝 Tell Someone
Tell your partner, your parent, your friend what you built together. Your child grew because of your commitment.
🚩 Pause & Seek Professional Guidance If You See:
"Trust your instincts — if something feels wrong, pause and ask." Most balance improvement is gradual and steady. These specific signs warrant professional evaluation rather than continued home practice alone.
Balance Getting WORSE After 4+ Weeks
Especially after consistent practice. May indicate an underlying medical condition requiring evaluation — do not continue without professional guidance.
Falls Resulting in Head Injuries
Frequent head-first falls, especially if the child does not put hands out to catch themselves (poor protective responses). Seek OT/PT assessment.
New Neurological Signs
Sudden onset of balance loss, one-sided weakness, vision changes, severe headaches, or coordination changes that weren't there before.
Severe Gravitational Insecurity Worsening
Clinging, panic, refusing to be tilted or moved in any direction — gravitational insecurity worsening rather than improving.
One-Sided Balance Difficulty
Consistently falls to one side, or one leg appears weaker than the other — requires medical evaluation.
Balance Loss with Seizure-Like Episodes
Staring spells, stiffening, unresponsive moments accompanying balance difficulties — seek immediate medical consultation.
Escalation pathway: Minor regressions after illness → resume protocol. | Plateau after 6+ weeks → teleconsultation. | Any red flag → clinic visit. Find your nearest Pinnacle center → | 📞FREE National Autism Helpline: 9100 181 181 (24x7, 16+ languages)
Your Child's Balance Journey — The Progression Pathway
Understanding where your child is on the progression map helps you plan intentionally, celebrate appropriate milestones, and choose the right next technique when this protocol completes.

More Techniques in Motor Development & Balance
Your balance-building toolkit serves multiple techniques across the motor development domain. You already own materials for these.

Intro difficulty.✅ Therapy ball, stepping stones

Intro difficulty.✅ Core equipment, therapy ball

Core difficulty.✅ Sensory mats, balance board

Core difficulty.✅ Obstacle courses, stepping stones

Core difficulty.✅ Balance games, obstacle courses

Intro difficulty.✅ All 9 materials
This Technique Is One Piece of a Larger Plan
Balance difficulty rarely exists in isolation. Your child's balance challenges may connect to sensory processing, low muscle tone, coordination, confidence and emotional regulation, and playground social participation. GPT-OS® maps the complete picture across all 12 developmental domains.
Request AbilityScore® Assessment
When you work with a Pinnacle therapist, AbilityScore® assesses all 12 domains and creates a prioritized intervention plan — so you're not guessing which domain needs attention most.
Explore All 12 Domains
700,000+ techniques across 12 developmental domains — all evidence-based, home-executable, and clinically validated by the Pinnacle Blooms Consortium.

From Falling to Flying — Real Family Journeys
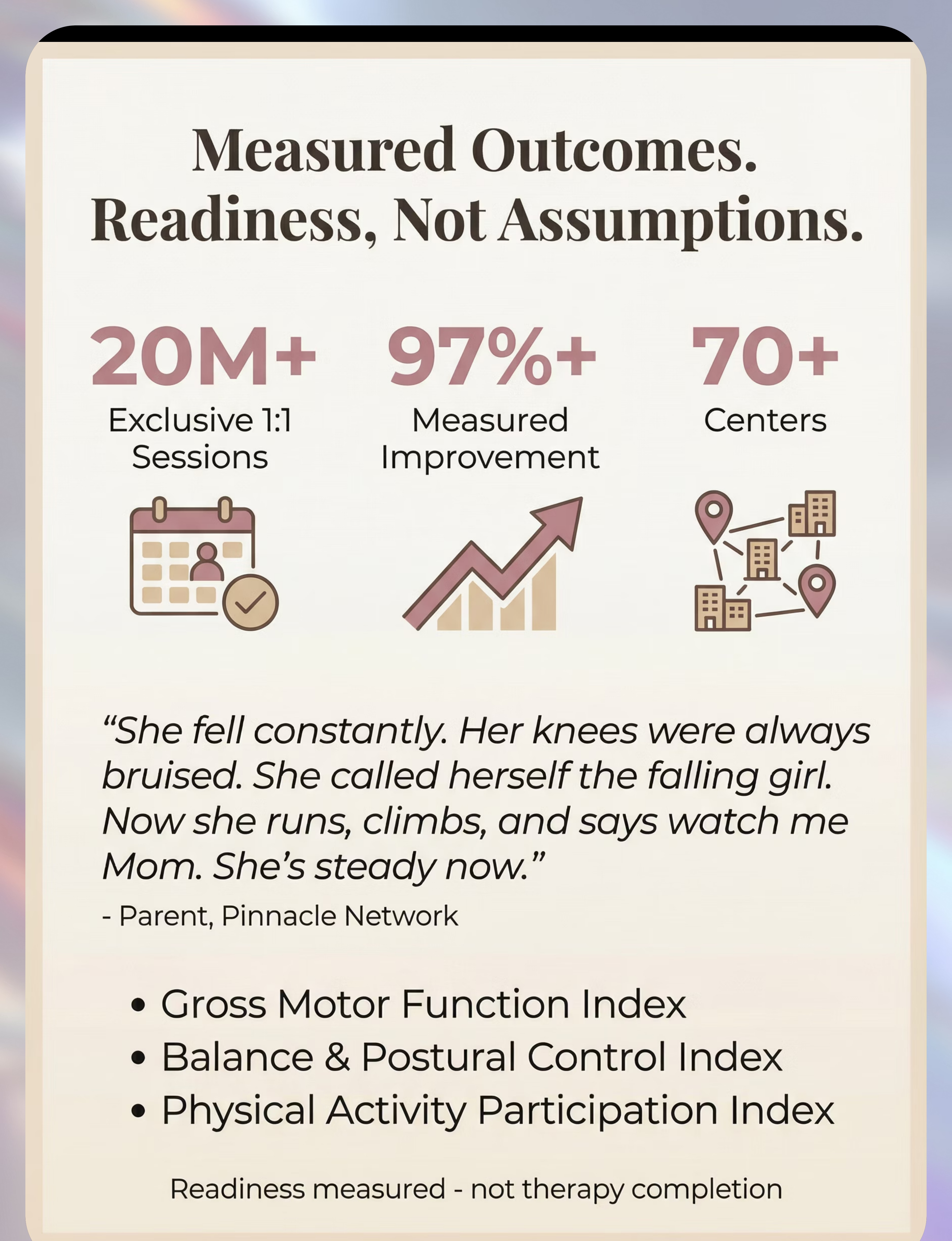
"My daughter fell multiple times every day. Her knees were always bruised. She'd started refusing to try physical activities because she knew she would fall. She called herself 'the falling girl.' We started OT focused on her balance — therapy balls for core strength, balance boards, vestibular swings, and lots of obstacle courses that made it fun. At home, we did exercises that felt like games. It was slow at first — the falling didn't stop right away. But after a few months, I noticed the falls were less frequent. She was catching herself more. Her confidence started coming back. Now, eight months later, she runs in the backyard with her brother and keeps up. She climbs the playground equipment. She goes down stairs without a death grip on the railing. She doesn't call herself 'the falling girl' anymore. She says 'watch me, Mom' and then runs. She's steady now."
— Parent, Pinnacle Network. Illustrative case. Outcomes vary by child profile, severity, consistency of intervention, and underlying contributing factors.
From the Therapist's Notes: "This child's falling was driven by a combination of vestibular processing inefficiency and core weakness. Addressing both simultaneously — vestibular input through swings and movement plus core strengthening through therapy ball and scooter board work — produced faster progress than either alone."
You're Not Doing This Alone
Consistency multiplies when you're connected to a community of families navigating the same challenge. Share tips, ask questions, celebrate milestones — with people who understand what it means to count balance-seconds on a living room floor.
Balance & Motor Development Parent WhatsApp Group
Share tips, ask questions, celebrate milestones with other parents whose children face balance challenges. Join the community →
Pinnacle Online Parent Forum
Searchable archive of parent questions, therapist answers, and family experiences across all developmental domains. Visit the forum →
Local Pinnacle Parent Meetups
Monthly in-person gatherings at your nearest Pinnacle center. Meet other families. Share strategies. Build your support network. Find meetups near you →
Peer Mentoring
Connect with an experienced parent who has navigated frequent falling and balance challenges. Real advice from someone who has been exactly where you are.

Home + Clinic = Maximum Impact
Home-based balance work is powerful. Combined with professional OT/PT guidance, it becomes transformational. Every home session you run is amplified by what your therapist observes, adjusts, and progresses in clinic.
📍 Find Your Nearest Pinnacle Center
70+ centers across India. Occupational therapy, physical therapy, sensory integration therapy, and motor skills programs — all under GPT-OS® clinical governance. Center Locator Map →
🩺 Therapist Matching
Get matched with an OT or PT who specializes in balance, vestibular processing, and motor coordination for children. Request Therapist Match →
📱 Teleconsultation
Can't visit a center? Book a video consultation with a pediatric OT/PT who can review your child's balance profile, assess your home setup, and guide your protocol. Book Teleconsultation →
💰 Insurance & Funding
Many health insurance plans cover OT/PT services for developmental conditions. Pinnacle can help navigate your coverage options and identify available funding pathways.
📞FREE National Autism Helpline: 9100 181 181 (24x7 • 16+ languages)
The Evidence Base — For the Curious Parent
Every recommendation on this page is traceable to peer-reviewed evidence. Deeper reading for the curious parent who wants to understand the science behind the protocol.
PRISMA Systematic Review (2024)
16 articles (2013–2023) confirm sensory integration intervention meets evidence-based practice criteria for children with ASD. PMC11506176
Meta-Analysis, World J Clin Cases (2024)
24 studies demonstrate sensory integration therapy effectively promotes gross motor skills, fine motor skills, adaptive behavior, and sensory processing. PMC10955541
Indian RCT (Indian J Pediatr, 2019)
Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population. Padmanabha et al. DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework (2018)
Global framework for early childhood development interventions. nurturing-care.org
WHO CCD Package (2023)
Caregiver-delivered developmental interventions across 54 LMICs demonstrating efficacy of home-material-based approaches. PMC9978394
Frontiers in Integrative Neuroscience (2020)
Framework for evaluating sensory processing treatment in ASD, establishing neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660
Your Data Powers Better Outcomes
Every session you record contributes to the largest pediatric developmental dataset on Earth. The 21 million sessions in GPT-OS® weren't collected at once — they were contributed one session at a time, by parents like you.
What GPT-OS® Learns from Your Data
- Your child's rate of improvement vs. population average
- Which materials produce the most engagement and progress
- Optimal session frequency and duration for your child's profile
- When to progress to next difficulty level — data-driven, not guesswork
🔒 Privacy & Data Protection
- Your child's data is encrypted and anonymized for population-level analysis
- Never shared with third parties
- You own your data — request deletion at any time
- Population-level patterns help every child like yours
📹 Watch: 9 Materials That Help With Frequent Falling
Video content reinforces everything on this page through a different learning modality — watching a therapist demonstrate is often the missing piece between reading a protocol and executing it confidently.
Reel A-091 — Main Reel
~75 seconds. Demonstrates all 9 materials in action with real children. ▶️ WATCH REEL A-091 →
A-091-DD-01 — Deep Dive
Balance Board Progressions — step-by-step demonstration of all 6 progression levels with a Pinnacle OT. ▶️ Watch →
A-091-DD-02 — Deep Dive
Understanding Vestibular Input for Balance — clinical explanation of how the inner ear drives balance and how therapy targets it. ▶️ Watch →
See the materials. See the techniques. See the transformation. Research: Video modeling classified as evidence-based practice for autism (NCAEP, 2020). Multi-modal learning improves parent skill acquisition and confidence. Browse all Motor Development Reels →

Consistency Across Caregivers Multiplies Impact
If only one parent executes the protocol, the child gets 10–20 minutes of balance work a day. If both parents, grandparents, and school staff are aligned, balance building becomes woven into the entire day — every surface, every transition, every opportunity.
Share This Page
📥 Download 1-Page Family Guide PDF
Simplified protocol for grandparents, teachers, and other caregivers. Large font. Key steps only. Print and share.
"Explain to Grandparents" Version
"[Child's name] falls frequently because the balance system in their brain needs extra practice to strengthen — just like muscles get stronger with exercise. You can help by: (1) letting them walk on varied surfaces, (2) playing balance games with them, (3) not catching them before they wobble — they need to feel the wobble to learn from it, (4) celebrating every attempt at a physical challenge."
Teacher Communication Template: "Dear [Teacher], [Child's name] is working on balance and stability. Please note: (1) they may need extra time on stairs, (2) a seat near the wall provides security, (3) please encourage playground participation with available adult support, (4) falls are expected and part of their development — please respond calmly." Research: WHO CCD Package — multi-caregiver training critical for intervention generalization. PMC9978394

Your Questions, Answered
Why does my child fall so much? Is something wrong?
Frequent falling indicates the vestibular system (inner ear balance), proprioceptive system (body position sense), core muscles, or motor planning are developing differently. It's a neurological wiring difference — not carelessness, laziness, or bad parenting. And it's addressable with targeted intervention.
Will my child ever have normal balance?
With consistent, appropriate intervention, most children show significant improvement. Many achieve age-appropriate balance within 6-12 months of structured practice. The systems that support balance respond to targeted input — they can be strengthened.
How long before I see results?
Tolerance and willingness improve in weeks 1-2. Measurable balance changes typically emerge around weeks 3-4. Functional improvements (fewer falls in daily life) usually appear by weeks 5-8. Full protocol is 8-12 weeks, though some children need longer.
Can I do this at home or do I need a therapist?
Both. The home protocol on this page is designed for parent execution. However, professional OT/PT assessment identifies the specific underlying causes and tailors the intervention. Home practice between professional sessions produces the fastest progress.
Is frequent falling a sign of autism?
Frequent falling can occur in typically developing children, children with autism, children with developmental coordination disorder, and children with other neurological conditions. It warrants professional evaluation regardless of other diagnoses.
My child is afraid to move now. How do I help them try again?
Start with the absolute easiest version — floor-level, full support, 30 seconds. Make it fun, not therapeutic. Pair with preferred activities. Celebrate every attempt. Rebuild trust gradually. Never force physical activity on a fearful child.
Are the DIY materials as good as commercial ones?
The therapeutic principles are the same. A tape line on the floor activates the same balance systems as a ₹3,000 balance beam. Commercial equipment offers more precise challenge grading and durability, but household alternatives are effective for home practice.
When should I be worried versus patient?
Be patient if: progress is slow but present, the child is engaging, the pattern is improving. Be concerned if: balance is worsening, falls involve head injuries, new neurological signs appear, or the child has stopped attempting movement. See Card 28 for full red flag guidance.
Preview of 9 materials that help with frequent falling Therapy Material
Below is a visual preview of 9 materials that help with frequent falling therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

You've Read the Evidence. You've Seen the Path. Now Choose Your Next Step.
🟢 Start This Technique Today
Download the protocol, gather your starter materials (balance board + therapy ball + tape on floor), and run your first 10-minute session tonight.
🔵 Book a Professional Assessment
Have your child's balance formally assessed by a Pinnacle OT/PT. Identify the specific underlying causes. Get a personalized treatment plan.
Book Assessment → | 📞 9100 181 181
🟣 Explore the Next Technique
Continue your motor development journey with the next recommended technique in the progression pathway.
🏛️Validated by the Pinnacle Blooms Consortium — OT • PT • SLP • ABA • SpEd • NeuroDev Pediatrics • CRO
Medical Disclaimer: This content is educational and does not replace assessment by a licensed occupational therapist, physical therapist, or healthcare provider. Frequent falling should be evaluated to understand underlying causes, rule out medical conditions, and guide appropriate intervention. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 • DPIIT: DIPP8651 • GSTIN: 36AAGCB9722P1Z2
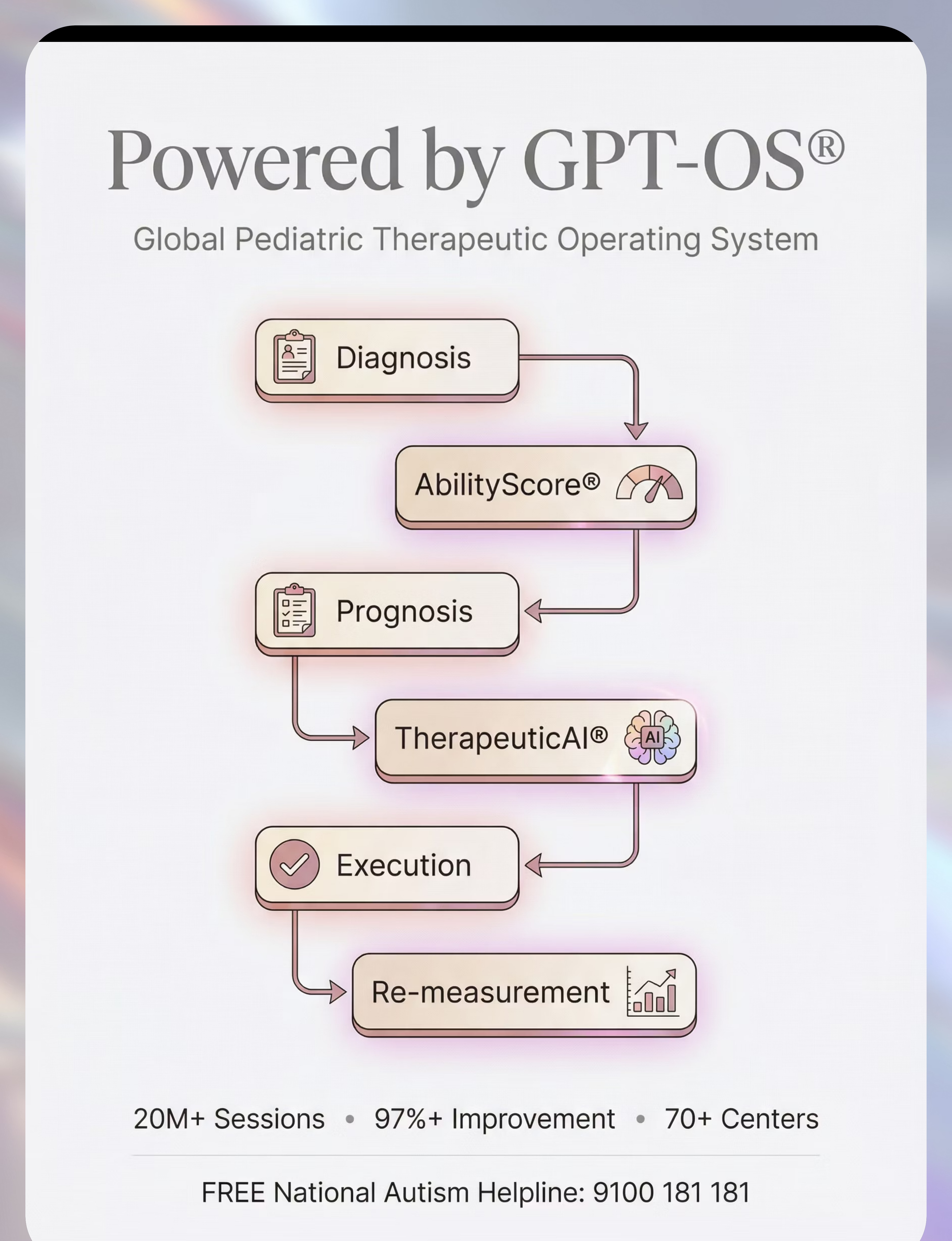
Powered by GPT-OS® | Global Pediatric Therapeutic Operating System — 21M+ sessions • 97%+ measured improvement • 70+ centers • Patents filed across 160+ countries