"He's 4 and still on baby food. Every meal, he gags on anything that isn't perfectly smooth."
You've tried everything. You've blended, you've mashed, you've hidden tiny pieces in puree — and still, the gagging comes. The retching. The fear in his eyes when he sees a lump on the spoon.
You are not failing. Your child's nervous system is speaking.
Food texture gagging is an involuntary neurological response — not pickiness, not manipulation, not a phase he'll "grow out of" on his own. The mouth is one of the most sensory-dense regions of the human body, and for your child, a tiny lump triggers the same protective reflex that prevents choking. His brain is trying to keep him safe.
There is a proven, systematic path from purees to family meals. You're about to learn the 9 materials that make it possible.
Pinnacle Blooms Network®
Sensory Solutions Series — Episode 14
Age Band: 18 months – 10 years

You Are Not Alone — The Numbers
Millions of families across the globe are navigating this exact challenge. The data tells a clear, reassuring story: food texture gagging is one of the most common sensory issues in pediatric development — and one of the most treatable.
80%
Sensory Processing Difficulties
of children with ASD experience sensory processing difficulties (PRISMA Systematic Review, 2024)
1 in 2
Feeding Challenges
children with autism have significant feeding challenges, with texture as the #1 trigger
70–90%
Texture-Based Refusal
of children referred for feeding therapy present with texture-based food refusal
Across 70+ countries, parents report the same pattern: a child who will only eat smooth foods, who gags or vomits when texture appears, who has a menu of 3–5 "safe" foods. This is not rare. This is not unusual. This is one of the most common sensory challenges in pediatric development — and it is one of the most treatable.
Source: PRISMA Systematic Review, Children (2024) | PMC11506176 | Meta-analysis: World J Clin Cases (2024) | PMC10955541

What's Happening in Your Child's Brain
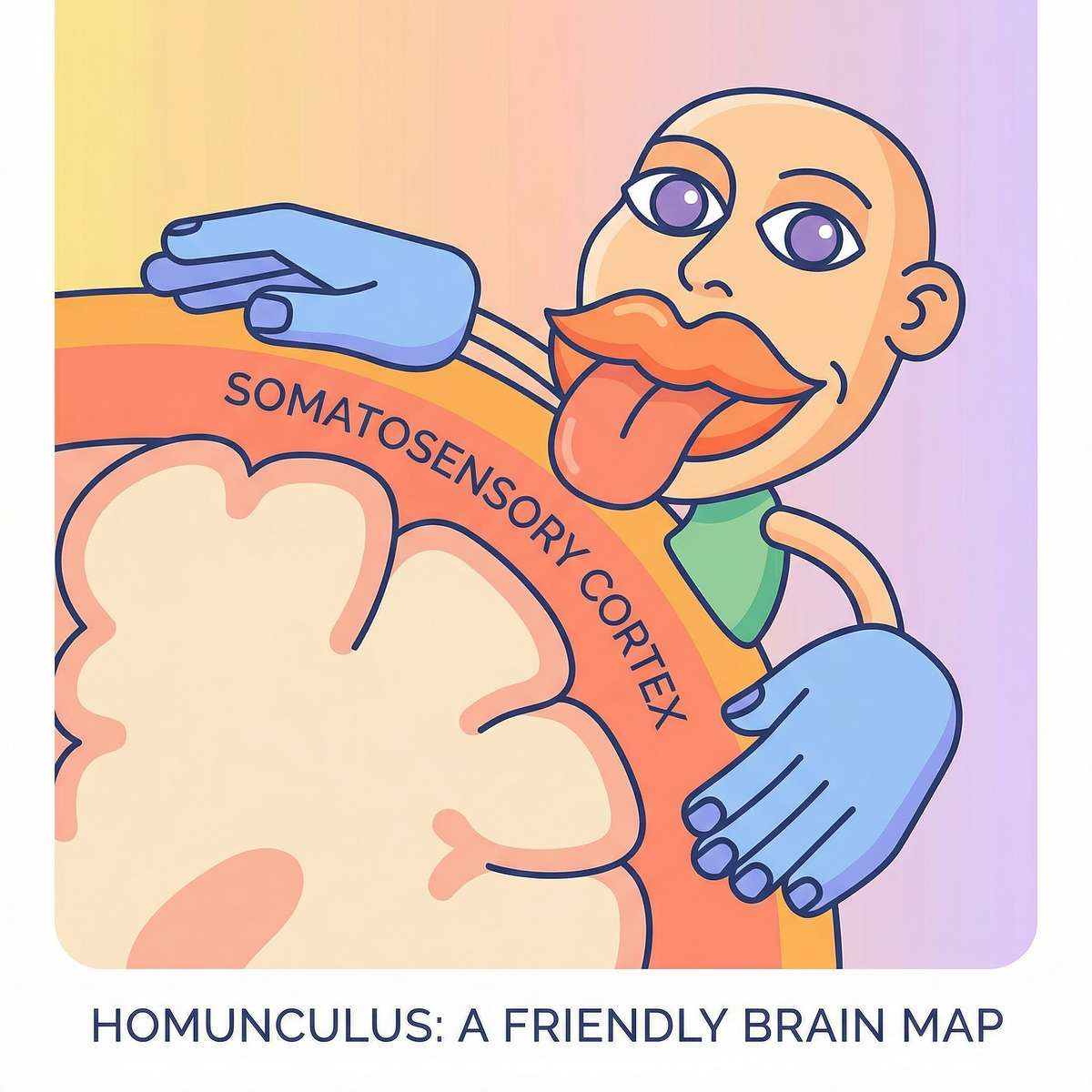
The mouth takes up more brain space than the entire torso.
The Oral Sensory System — Explained for Parents
Your child's mouth contains thousands of mechanoreceptors — tiny sensors that detect pressure, texture, temperature, and movement. These sensors send signals to a part of the brain called the somatosensory cortex.
In the famous brain "homunculus" diagram, the mouth and tongue are represented as enormous — because the brain dedicates a disproportionately large area to processing oral sensation. More brain space than the entire torso.
In children with oral tactile hypersensitivity, these receptors have a lower activation threshold. A texture that feels neutral to you — a small lump in dal, a piece of vegetable in khichdi — registers in your child's brain as intense, unexpected, and threatening.
The gag reflex activates. Not by choice. Not to manipulate. The brain fires a protective response: "This is dangerous. Eject it."
This is a wiring difference, not a behavior choice.
Source: Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660 | SPD Foundation: spdfoundation.net

Where This Sits in Development
Understanding the typical developmental timeline for food texture acceptance helps you see exactly where your child is — and where you're heading together. The window between 18 months and 6 years is the most critical period for building texture tolerance.
6 Months
Purees introduced
8 Months
Mashed textures
12 Months
Soft lumps tolerated
18 Months
Mixed textures expected
2–3 Years
Table food variety
4–6 Years
Full family meals
7–10 Years
Independent eating
Critical Window: 18 months – 6 years — When a child remains on purees beyond 18–24 months, the window for natural texture acceptance begins to narrow. Oral motor patterns (chewing, lateralizing food, managing a bolus) depend on practice with texture. Without that practice, the muscles and neural pathways don't develop on schedule.
Your child is here. Here is where we're heading. The 9 materials in this technique are designed to systematically move your child along this timeline — at their pace, led by their nervous system, supported by your consistency.
Co-occurring challenges to be aware of: Oral tactile hypersensitivity commonly co-occurs with broader sensory processing differences, limited diet variety (ARFID), oral motor weakness, and anxiety around mealtimes.
Source: WHO Care for Child Development (CCD) Package (2023) | PMC9978394 | UNICEF Developmental Monitoring Indicators
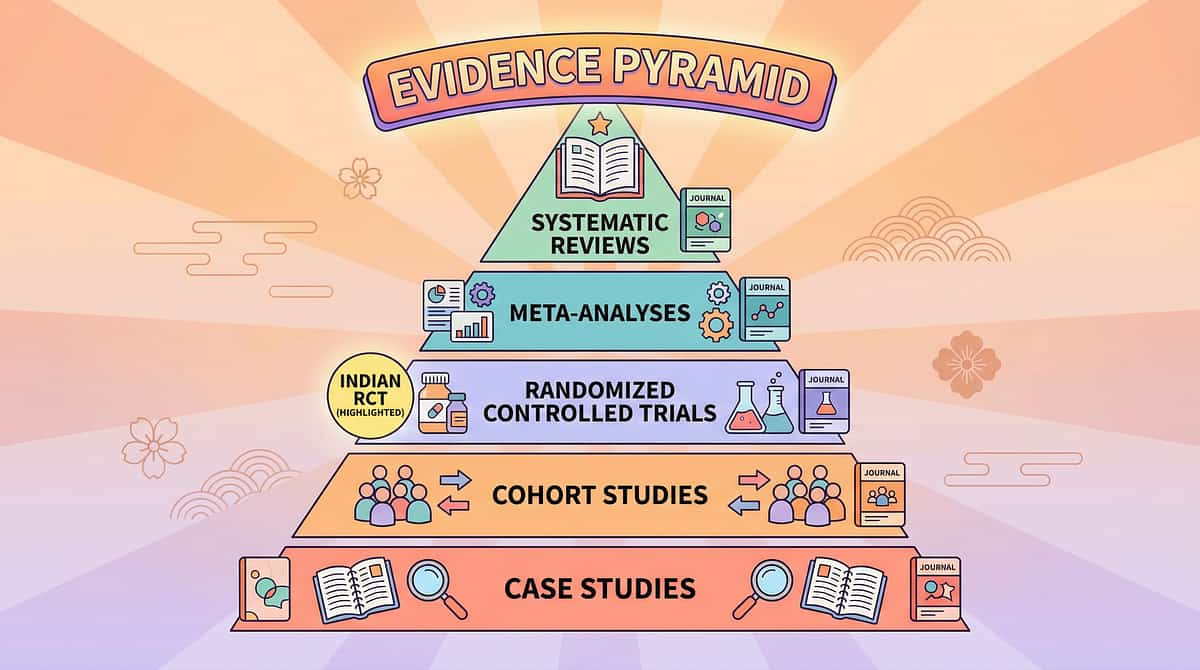
The Evidence Behind This Technique
Evidence Grade: STRONG (Level I–II)
Systematic Reviews with Meta-Analysis
The highest tier of clinical evidence supports this approach.
Randomized Controlled Trials
Including India-specific data from Padmanabha et al. (2019).
Cross-Discipline Clinical Consensus
SLP, OT, and ABA disciplines all converge on this intervention.
Key Findings
- 16 studies (2013–2023) confirm sensory integration intervention meets criteria as evidence-based practice for children with ASD — PRISMA Model Systematic Review, Children (2024)
- Home-based sensory interventions demonstrated statistically significant outcomes in a randomized controlled trial conducted in India — Padmanabha et al., Indian Journal of Pediatrics (2019)
- Sensory integration therapy effectively promotes adaptive behavior, sensory processing, social skills, and motor skills across 24 studies — Meta-analysis, World Journal of Clinical Cases (2024)
- SOS Approach to Feeding (Dr. Kay Toomey) provides the systematic desensitization framework underlying the texture progression protocol
Clinically validated. Home-applicable. Parent-proven.
Sources: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4 | ASHA Guidelines | Morris & Klein — Pre-Feeding Skills (2nd Ed.)

Quick Navigation
Navigate This Page
This comprehensive guide is organized into six acts. Use these anchors to jump to the section most relevant to you right now.
Act I: Emotional Entry
Cards 1–5: Recognition, brain science, evidence
Act II: Knowledge Transfer
Cards 7–12: Technique, materials, safety, setup
Act III: Execution
Cards 13–22: Step-by-step protocol
Act IV: Progress Arc
Cards 23–30: Milestones, red flags, pathway
Act V: Community
Cards 31–37: Stories, support, research
Act VI: Close & Loop
Cards 38–40: FAQs, next steps, promise

Oral Desensitization & Texture Progression Protocol
Technique A-014
The 9-Material Feeding Toolkit
A structured, multi-material intervention that systematically reduces oral tactile hypersensitivity and builds food texture tolerance through two parallel tracks:
Track 1: Oral Desensitization
Outside mealtimes — using vibration, massage, and chew tools to calm the oral sensory system.
Track 2: Graduated Texture Exposure
Through meltable foods, textured utensils, food play, visual supports, and flavor bridging — all within a pressure-free, child-led framework.
Domain
Sensory → Oral-Tactile (SEN-ORL)
Age Range
18 months – 10 years
Session Duration
5–15 min (oral prep) + separate texture practice
Frequency
Daily oral prep; texture practice 3–5x/week
Setting
Home — kitchen, dining area, sensory play area
Who Uses This Technique — The Consortium
Food texture gagging crosses therapy boundaries because the brain doesn't organize by therapy type. An integrated team approach delivers the best outcomes for your child.
Speech-Language Pathologist (SLP) — Primary Lead
Designs the oral desensitization protocol, manages gag reflex modification, prescribes texture hierarchy, evaluates swallowing safety, and coordinates feeding therapy goals. The SLP's oral motor expertise drives the clinical framework.
Occupational Therapist (OT) — Sensory Architecture
Addresses the underlying sensory processing profile causing oral hypersensitivity. Designs the sensory diet that prepares the child's entire nervous system — not just the mouth — for texture challenges. Integrates proprioceptive, vestibular, and tactile inputs.
Board Certified Behavior Analyst (BCBA) — Behavioral Framework
Structures the reinforcement schedule, manages escape-maintained food refusal behaviors, designs systematic desensitization hierarchy, and ensures ABA principles of antecedent manipulation and consequence management. Tracks behavioral data.
Special Educator — Generalization & Daily Living
Bridges the feeding protocol to school lunch, social eating situations, and daily living independence. Develops visual supports, social stories for mealtimes, and peer modeling strategies.
Neurodevelopmental Pediatrician provides medical oversight, rules out GERD, dysphagia, and structural causes, and monitors nutritional adequacy throughout the intervention.
Source: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) | DOI: 10.1080/17549507.2022.2141327
What This Targets — Precision, Not Guesswork
This technique targets three interconnected layers of development. Each layer builds on the one before it, creating a comprehensive pathway from oral sensitivity to independent eating.
🎯 Primary
Child tolerates texture on spoon/in mouth without gagging for 5+ seconds
🎯 Secondary
Child willingly touches and smells 3+ previously refused food textures
🎯 Tertiary
Child participates in family meal with age-appropriate textures 3+ times/week
Source: Meta-analysis, World J Clin Cases (2024) | PMC10955541

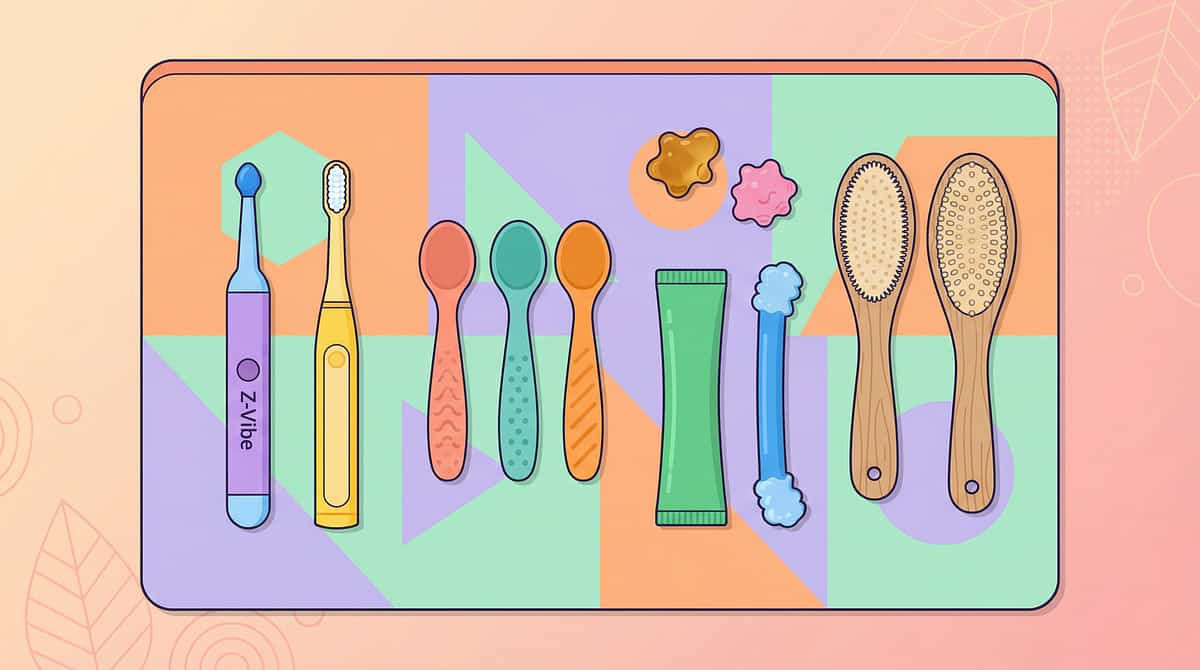
What You Need — The 9 Materials
Complete Toolkit: ₹3,000–₹8,000
Essential Starters: ₹2,000–₹4,500
Every material in this toolkit has a specific clinical purpose. Below is your complete shopping list with Canon categories and pricing for India.
# | Material | Canon Category | Price (INR) | Essential? | |
1 | Oral Vibration Tools (Z-Vibe / Vibrating Toothbrush) | Oral Motor Tools | ₹200–3,500 | ⭐ YES | |
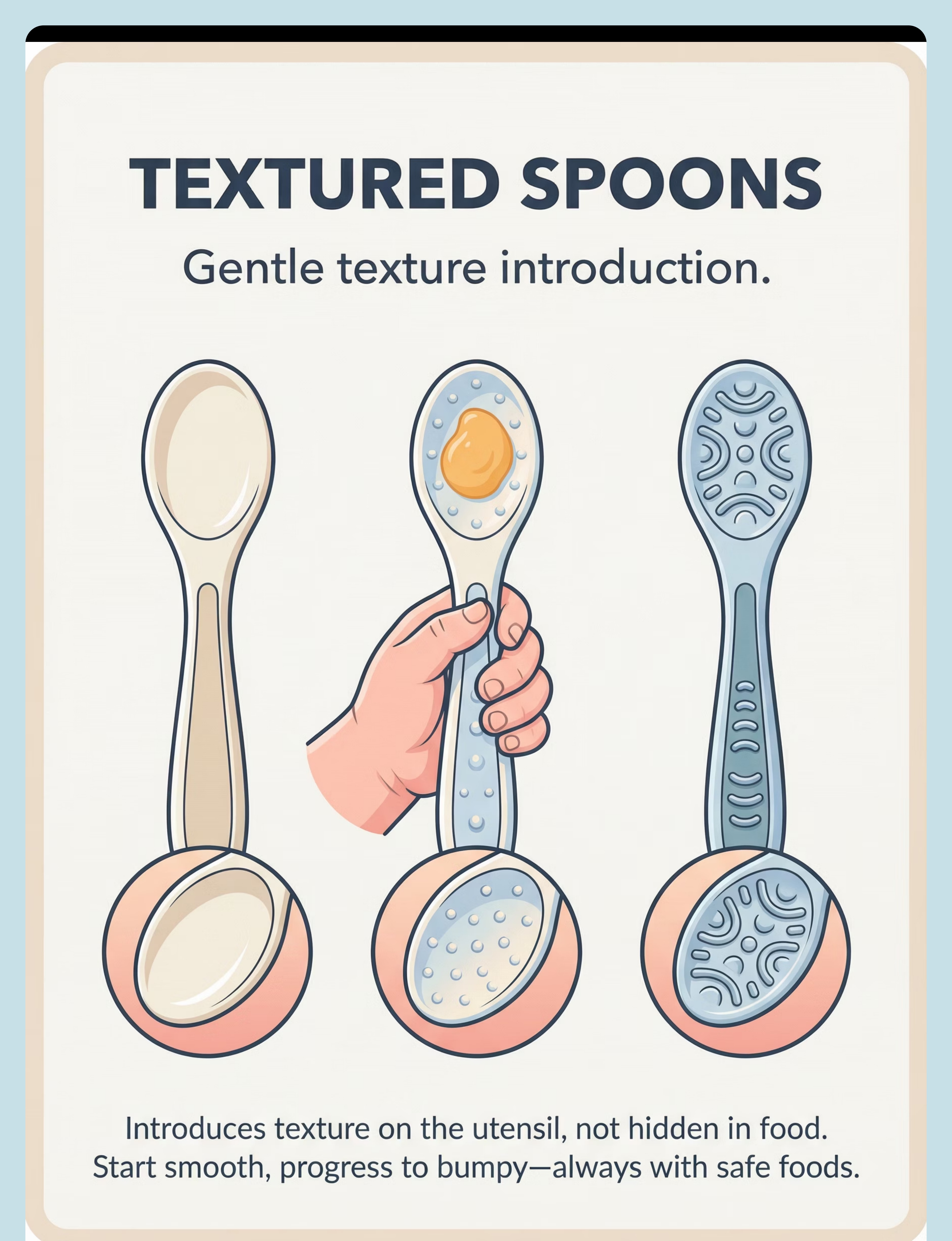
2 | Textured Spoons (Graduated Set) | Feeding Tools | ₹400–1,200 | ⭐ YES | |
3 | Oral Chew Tools (Chewy Tubes / ARK Grabbers) | Oral Motor Tools | ₹300–900 | ||
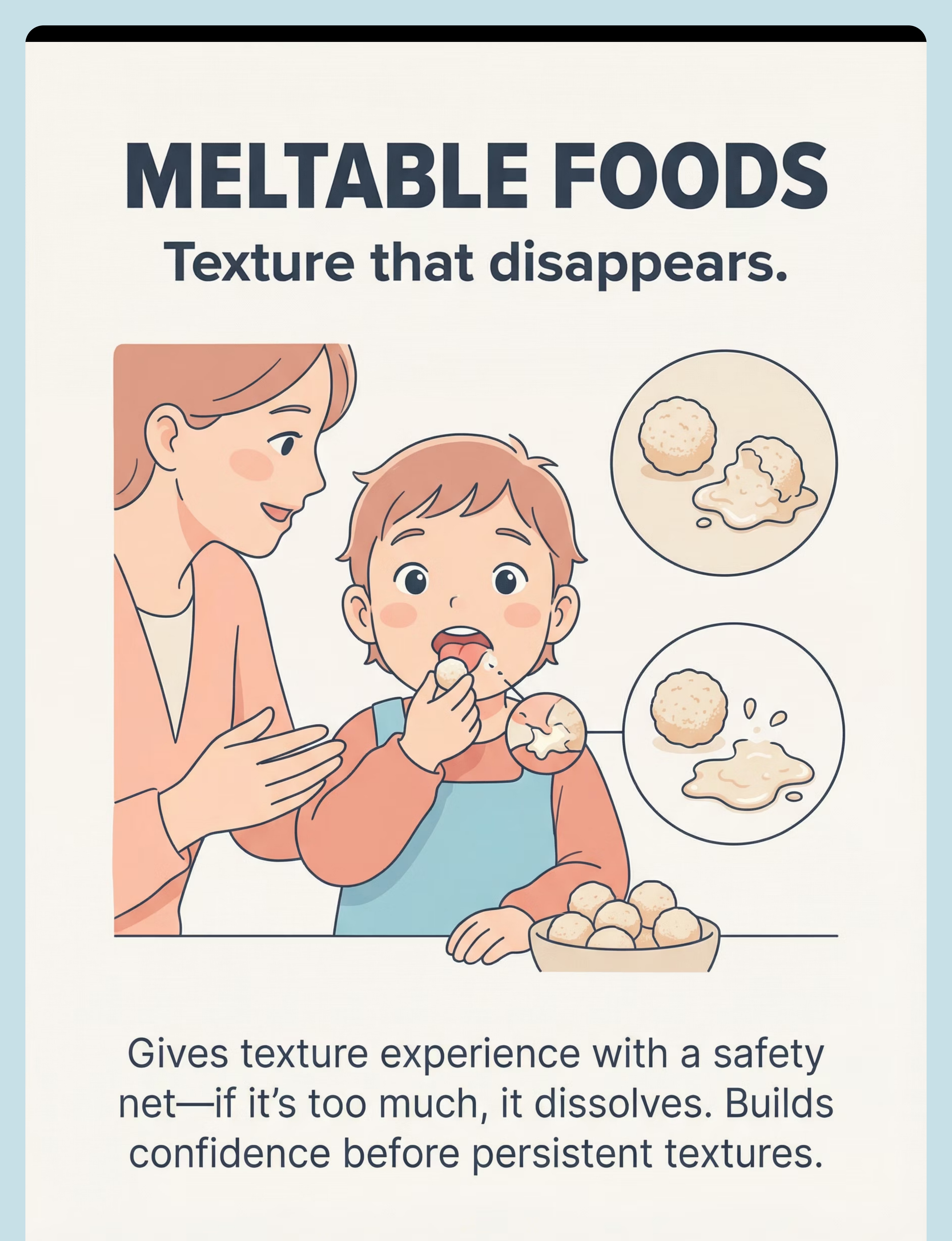
4 | Food Texture Bridges (Dissolving Puffs / Meltables) | Feeding Supplies | ₹150–400/pack | ⭐ YES | |
5 | Nuk Brush / Oral Massage Tools | Oral Motor Tools | ₹200–500 | ||
6 | Flavor Spray / Concentrated Taste Exposure | Feeding Tools | ₹200–600 | ||
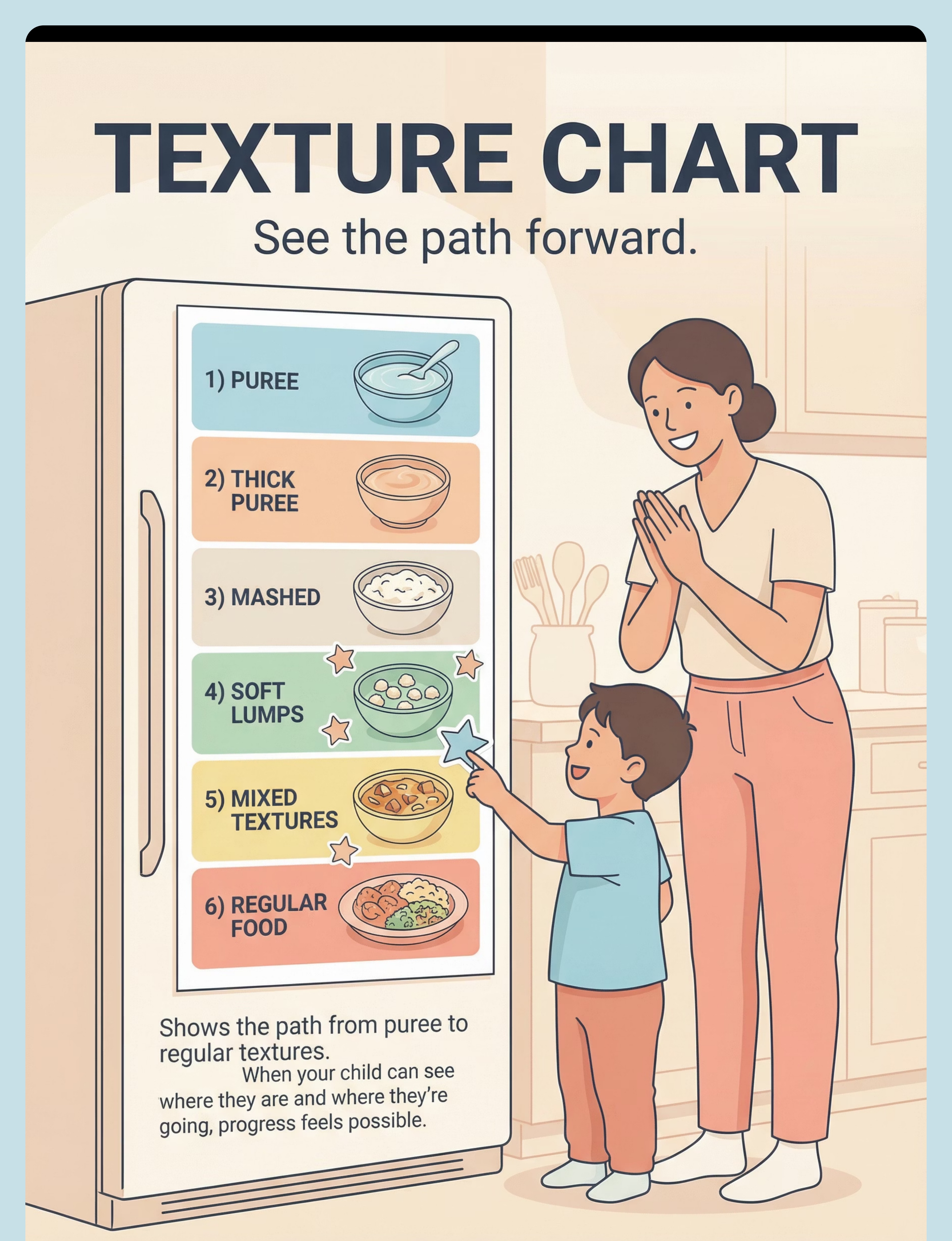
7 | Texture Gradient Food Chart | Visual Supports | ₹100–300 | ||
8 | Mirror for Mealtime / Oral Exploration | Sensory Tools | ₹300–800 | ||
9 | Food Play Kit (Non-Eating Exploration Tools) | Sensory Kits | ₹200–600 |
⭐ Essential Starters (begin here): Oral Vibration Tool (or vibrating toothbrush), Meltable Foods, Textured Spoons. You can start the protocol today with just these three.
DIY & Substitute Options — Start Today with What You Have
Not every family can order from Amazon. Not every village has same-day delivery. Every family deserves access to this intervention. This is the WHO/UNICEF inclusion principle in action.
Buy This | Make This (₹0 Alternative) | Notes | |
Z-Vibe (₹1,500–3,500) | Vibrating toothbrush (₹200) on gums, tongue, inner cheeks | Same deep proprioceptive input | |
Graduated Textured Spoons (₹400–1,200) | Food-safe silicone dots on regular spoons; mix spoon finishes | Smooth, soft, ridged variety | |
ARK Grabbers / Chewy Tubes (₹300–900) | Food-safe silicone teethers; frozen washcloths | Always supervise | |
Dissolving Puffs (₹150–400) | Freeze-dried yogurt bites, thin rice crackers, small papad pieces | Must dissolve quickly with saliva | |
Nuk Brush (₹200–500) | Soft silicone finger toothbrush, damp washcloth on finger | Gentle pressure only | |
Flavor Spray (₹200–600) | Diluted fruit juice in small spray bottle, thin dal/broth | Familiar flavors first | |
Texture Chart (₹100–300) | Hand-drawn 6-level chart with food photos, laminate with tape | Use star stickers for progress | |
Child-Safe Mirror (₹300–800) | Phone front camera or any unbreakable mirror at eating height | Builds oral awareness | |
Food Play Kit (₹200–600) | Kitchen spoons, small steel cups, empty containers | Separate "food play" time from meals |
⚠️ Non-negotiable: For children with severe oral aversion or swallowing concerns, clinical-grade oral motor tools (Z-Vibe) should be used under SLP guidance. DIY alternatives are for mild-moderate texture sensitivity.
Source: WHO Nurturing Care Framework (2018) | PMC9978394

⚠️ Safety First — Before You Begin
Your child's safety is the absolute foundation of this protocol. Review these traffic-light guidelines before every session.
🔴 DO NOT PROCEED IF
- History of aspiration (food/liquid entering airway)
- Unexplained weight loss or failure to thrive — see pediatrician FIRST
- Known swallowing disorder (dysphagia) without medical clearance
- Currently ill, feverish, or has mouth sores
- Active gag-to-vomit cycle with ALL oral input
🟡 MODIFY & USE CAUTION IF
- Child has GERD (reflux) — oral tools may trigger episodes
- Child is under 18 months — simplify to vibrating toothbrush + meltables only
- Severe oral aversion (refuses toothbrush, medical exams) — begin with food play ONLY
- Known food allergies — check EVERY meltable food ingredient
🟢 PROCEED WHEN
- Child is calm, alert, and fed (never practice when hungry)
- At least 30 min after last meal for oral desensitization
- Separate from nutritional mealtimes
- Child seated upright with feet supported
- Parent is calm, patient, has 10–15 min uninterrupted
🛑 RED LINE — STOP IMMEDIATELY IF: Signs of choking (silent or audible), vomiting without recovery in 2–3 min, severe distress (inconsolable crying, self-injury), blue/grey coloring around lips or fingertips, aspiration signs (wet/gurgly voice, persistent coughing after swallowing).
Source: Padmanabha et al., Indian J Pediatr (2019) | DOI: 10.1007/s12098-018-2747-4

Set Up Your Space
Environment matters. The right setup reduces sensory distractions and creates a calm, predictable context that helps your child feel safe enough to explore.
Track 1: Oral Desensitization
(Before Meals — NOT at the dining table)
- Chair or couch — child seated comfortably, supported
- Oral tools tray — Z-Vibe/toothbrush, Nuk brush, chew tools arranged within reach
- Mirror (optional) — child can see their mouth
- Timer (visual) — 2-minute sand timer or phone timer visible
- Reinforcer — preferred toy/activity ready for after session
Track 2: Texture Practice
(Separate from meals — different table, different time)
- Small table or highchair tray — NOT the family dining table
- Textured spoons — smooth, bumpy, ridged available
- Meltable foods — 2–3 options in small portions
- Food play setup — tray with tongs, small containers, apron/bib
- Texture chart — visible on wall or fridge
- Napkin/spit cup — child always has an "out" option
Remove
Screens, siblings, dogs, loud music, strong cooking smells, previously aversive foods
Lighting
Natural, warm. Not fluorescent.
Sound
Quiet. No TV. Gentle background music OK.
Temperature
Comfortable. Not hot.
Source: Sensory Integration Theory (Ayres) | PMC10955541

Act III: The Execution
Is Your Child Ready? — 60-Second Readiness Check
Before every session, run through this quick checklist. It takes 60 seconds and ensures you're setting your child up for success, not frustration.
01
Child has eaten in the last 1–2 hours
NOT hungry — texture practice should never happen on an empty stomach
02
Child is calm and alert
Not tired, not post-meltdown, in a regulated sensory state
03
No illness, fever, or mouth pain
Physical health is a prerequisite for sensory challenge
04
30+ minutes since last meal
For oral desensitization activities specifically
05
Parent is calm and available
10–15 minutes of uninterrupted, patient presence
06
Space is set up per protocol
Tools ready, distractions removed, reinforcer prepared
All ✅ → GO
Begin full protocol
1–2 ✖ → MODIFY
Simplified version: food play only or chew tool exploration
3+ ✖ → POSTPONE
Alternative calming activity. Try tomorrow. No guilt.
"The best session is one that starts right."

Step 1: The Invitation (30–60 seconds)
Oral Desensitization Track
"Look what I have! It's your special mouth tickler. Want to try? You can hold it. You decide when it goes in your mouth."
Body language: Relaxed. Smile. Offer the oral tool in an open palm, not extended toward the child's face. Sit beside, not across from. Make yourself smaller — this reduces the sense of pressure.
What Acceptance Looks Like
- Child reaches for the tool
- Child watches with curiosity
- Child allows you to hold it near their face
- Child opens mouth slightly
What Resistance Looks Like
- Child turns head away
- Child pushes your hand
- Child becomes rigid or whiny
If resistance: Back off immediately. Place tool between you. Play with it yourself. Say: "That's okay. It's here when you want it." Wait. Many children approach within 2–3 minutes when pressure is removed.

Step 2: The Engagement (1–3 minutes)
Z-Vibe / Vibrating Toothbrush
Material Introduction: Turn on the vibration. Let the child feel it on the back of their hand first (non-threatening location). Then offer cheek, then lips, then gums — always with the child's permission.
"Feel that buzz? Let's try it on your hand... your cheek... do you want to try inside? You hold it. You decide."
Child Response Spectrum
Engaged
Reaches for tool, explores independently, opens mouth voluntarily → Continue
Tolerating
Allows brief touch, neutral expression, doesn't pull away → Continue gently
Avoiding
Pulls back, closes mouth, turns head → Stay at last accepted location, or end and celebrate
Reinforcement cue: When the child allows ANY oral contact: "You did it! Your mouth is so brave!" — immediate, specific, enthusiastic.
Timing: 1–3 minutes of actual oral contact. The child controls the tool.
Step 3: The Therapeutic Action (3–5 minutes)
Core Oral Desensitization Protocol
This is the heart of Track 1. With the Z-Vibe or vibrating toothbrush — child holding it or parent (with permission) — follow this precise sequence:
1
Outer Gums
Vibration along the outside of both upper and lower gums. 10–15 seconds each side.
2
Inner Cheeks
Gentle vibration against the inside of each cheek. 10–15 seconds each side.
3
Tongue Tip
Brief contact with the front of the tongue. 5–10 seconds.
4
Tongue Middle
If tolerated, move vibration slightly further back. 5–10 seconds.
5
Palate
Gentle vibration on the hard palate (roof of mouth). 5–10 seconds.
⚠️ NEVER go past the point where gagging starts. The goal is to APPROACH the gag zone, not trigger it.
Common Execution Errors
- Moving too fast — spend MORE time on early, comfortable areas
- Holding the tool too firmly — light touch, let vibration do the work
- Continuing when child signals "done" — respect every "no"
- Doing this AT mealtime — oral prep must be SEPARATE

Step 4: Repeat & Vary (3–5 minutes)
Target repetitions: 2–3 complete passes through the oral desensitization sequence per session.
Variations to Maintain Engagement
Different Tools
Alternate between Z-Vibe and Nuk brush across sessions to keep novelty fresh.
Different Textures
Swap chew tool textures: smooth → bumpy → ridged across different days.
Flavor Addition
Dip oral tool in preferred flavor before use — motivates engagement.
Child-Led Order
Let the child choose which area of mouth to start with — builds autonomy.
Song/Rhythm
Pair oral stimulation with a favorite tune — creates positive association.
Satiation Indicators (Child Has Had Enough)
- Turns head away after previously accepting
- Pushes tool away
- Becomes restless or fidgety
- Yawns (overstimulation signal)
- Says or signs "all done"
"3 good repetitions are worth more than 10 forced ones."
Timing: Total oral desensitization session: 5–10 minutes including invitation and cool-down. Not longer.

Step 5: Reinforce & Celebrate
WHEN to reinforce: Within 3 seconds of any desired behavior. Timing matters more than magnitude.
"Your mouth was SO brave today! You let the buzz touch your tongue — that's amazing!"
Reinforcement Menu
Verbal Praise
Specific, enthusiastic, immediate: "You touched the bumpy spoon!"
Physical
High five, clap, hug — if child seeks physical affirmation
Token
Sticker on texture chart, star on reward board
Natural Consequence
Preferred activity immediately after session
Critical principle: "Celebrate the attempt, not just the success." Child touched the tool but didn't put it in their mouth? That's progress. Celebrate it. Child gagged but tried again? Extraordinary courage. Say so.

Step 6: The Cool-Down (1–2 minutes)
Transitions matter. A predictable ending builds trust and creates motivation for the next session.
Transition Warning (30 Seconds Before End)
"Two more touches, then all done with mouth practice!"
1
Last Repetition
The easiest, most comfortable one — end on success
2
Tool Put-Away Ritual
Child places tool in "mouth practice box" — builds ownership
3
Calming Input
Deep pressure hug, favorite sensory toy, or quiet activity
4
Transition Cue
"Mouth practice is all done! Now it's time for [preferred activity]."
If Child Wants to Continue
This is a positive sign. Still end on time. Wanting more creates motivation for the next session.
"I love that you want more! We'll do mouth practice again tomorrow. Your mouth is getting so strong."
If Child Is Upset/Dysregulated
Extend cool-down with calming sensory input. Do NOT restart the session. The child's nervous system needs transition support, not more stimulation.

Capture the Data — Right Now (60 Seconds)
Within 60 seconds of session end, record these data points. This habit transforms guessing into informed decision-making.
Oral Desensitization Tracker
Date | Duration of Oral Contact | Farthest Oral Area Reached | Child Mood | |
___ | ___ seconds | Lips / Gums / Cheeks / Tongue / Palate | 😊😐😟 |
Texture Practice Tracker
Texture Level Attempted | Accepted? | Foods Tried | Notes | |
___ | Y / N / Partial | ___ | ___ |
"60 seconds of data now saves hours of guessing later."

What If It Didn't Go as Planned?
Real sessions rarely look like textbook sessions. Here are the 7 most common challenges parents face — and exactly what to do about each one.
"My child refuses to open their mouth at all"
Don't start with oral tools. Start with food play (Material #9). Build comfort with touching, smelling, squishing textures with hands first. Oral work comes later. Also try: vibrating toothbrush on the OUTSIDE of cheeks/jaw — no mouth opening needed.
"My child gagged worse than before the session"
You went too deep or too fast. Return to the last comfortable area. If gums were fine but tongue triggered gagging — stay at gums for 1–2 more weeks. Gagging is information, not failure.
"My child liked the oral tools but still won't try food"
This is NORMAL and expected. Oral desensitization (Track 1) prepares the mouth. Texture progression (Track 2) introduces food. They are parallel but not simultaneous. Oral comfort comes first.
"My child was fine yesterday but rejected everything today"
Check: Is child tired? Ill? Stressful event? Sensory tolerance fluctuates. Skip a day. Return tomorrow. One bad session is not regression.
"Sessions turn into mealtime battles"
You are combining texture practice with nutritional meals. SEPARATE THEM. Texture practice = zero eating pressure. Nutritional meals = only accepted "safe" foods. Different table, different time, different expectation.
"My spouse/in-laws say I'm coddling him"
Share Card 3 (brain science) and Card 37 (family guide). Food texture gagging is neurological, not behavioral. The intervention is systematic desensitization, not giving in.
"We've been doing this for 3 weeks with no change"
Check: Is oral prep happening daily? Is it SEPARATE from mealtimes? Is the child controlling the tools? Are you at the right phase? If yes to all — consider SLP/feeding specialist evaluation. Some children need professional hands-on guidance to establish the foundation.
"Session abandonment is not failure — it's data."

Adapt & Personalize — No Two Children Are Identical
Every child has a unique sensory profile. Use these adaptation frameworks to tailor the protocol to your child's specific needs, energy level, and developmental stage.
Easier Version
For bad days, early weeks, or high anxiety. ONLY vibrating toothbrush on outer gums. Food play only — no eating expectation. Single meltable offered once. 3-minute sessions maximum.
Standard Version
As described in Steps 1–6. Full oral desensitization sequence, 2–3 repetitions, texture practice with meltables and textured spoons. 10–15 minute sessions.
Harder Version
For weeks 5+ when tolerance builds. Oral tools on tongue and palate. Soft persistent textures. Mixed textures on same plate. Child self-serving. 15–20 minute sessions.
Sensory Profile Variations
Sensory Avoider | Sensory Seeker | |
Slow, gentle approach | Can handle more intense oral input | |
Fewer stimuli at once | May need STRONGER vibration to register | |
Long pauses between touches | Faster pace, more variety | |
Quiet environment critical | Can handle some background stimulation |
Age Modifications
Under 2 Years
Vibrating toothbrush + meltables only. Short sessions (3–5 min).
2–4 Years
Full 9-material protocol. Food play is central.
5–7 Years
Add child participation in food preparation as exposure tool.
8–10 Years
Include child in goal-setting. Texture chart as a shared project.
Act IV: The Progress Arc
Week 1–2: What to Expect
15%
Progress Milestone
Foundation building — the hardest part is starting
Observable Indicators at This Stage
- Child tolerates oral tools for 5–10 seconds longer than baseline
- Reduced resistance to having tools NEAR the mouth
- Emerging curiosity: child may reach for tools independently
- During food play: child touches 1–2 new food textures (NOT eating them — touching is progress)
What "Progress" Looks Like Now
Your child allowing a vibrating toothbrush to touch their gums for 15 seconds instead of 10. That's 50% improvement. Your child picking up a dissolvable puff and sniffing it instead of pushing the bowl away. That's a step on the SOS hierarchy.
What Is NOT Progress Yet
Your child is NOT eating lumpy food yet — that's Phase 4–5. Your child may still gag during oral prep. The gag zone is shifting — slowly. Mealtime may look exactly the same. Texture practice is SEPARATE from meals.
"If your child tolerates the tool for 3 seconds longer than last week — that's real progress."

Week 3–4: Consolidation Signs
40%
Progress Milestone
Consolidation — neural pathways are forming
Consolidation Indicators You May Notice
- Child anticipates oral prep and may approach you or ask for the "mouth tools"
- Gag trigger point has shifted BACK (tongue was trigger → now only deep tongue/palate)
- Child VOLUNTARILY puts chew tool in mouth during free play
- Food play: child is now touching, smelling, AND bringing food to lips
- Meltable foods: child may accept 1–2 dissolvable puffs without gagging
Behavioral Changes Signaling Neural Pathway Formation
Less Mealtime Anxiety
Unfamiliar food is on the table and child isn't distressed — even if not eating it
Reduced Escape Behaviors
Less leaving the table, less crying before food arrives
Spontaneous Food Talk
Child names or points to foods without distress — a huge cognitive shift
"You may notice you're more confident too." By week 3–4, the parent's anxiety about mealtimes often begins to decrease. You're seeing the system work. Trust it.
Week 5–8: Mastery Indicators
75%
Progress Milestone
Mastery building — skills are generalizing
Mastery Criteria — Specific, Observable, Measurable
01
Full oral sequence without gagging
Child tolerates gums → cheeks → tongue → palate without gagging
02
3+ meltable foods accepted independently
Child self-feeds dissolvable puffs, crackers, or similar textures
03
Textured spoon tolerance
Child uses bumpy/ridged spoon with preferred food without distress
04
Food play with 5+ textures
Child willingly participates in exploration with different textures
05
2+ levels on texture gradient chart
Measurable movement up the texture hierarchy
Generalization Indicators
- Child tries a new texture at a restaurant or relative's house
- Child touches or smells a sibling's plate food without being asked
- Toothbrushing tolerance improves (oral desensitization generalizes)
🏆 Mastery Unlocked: Ready for Phase 5 — Persistent Soft Textures. If 3 out of 5 criteria met → stay 2 more weeks. If fewer than 3 → return to troubleshooting (Card 22), consider professional consultation.

🎉 Celebrate This Win
You did this. Your child grew because of your commitment.
5–8 weeks ago, your child gagged on anything that wasn't perfectly smooth. Today, they're reaching for oral tools, accepting meltable textures, playing with food they once refused to touch.
This is not a small thing.
Every 2-minute oral prep session you showed up for — even on tired days, even when it felt like nothing was changing — was reshaping your child's neural pathways. Every dissolvable puff your child accepted was a victory. Every food play session where they squished rice between their fingers was a step toward family dinners.
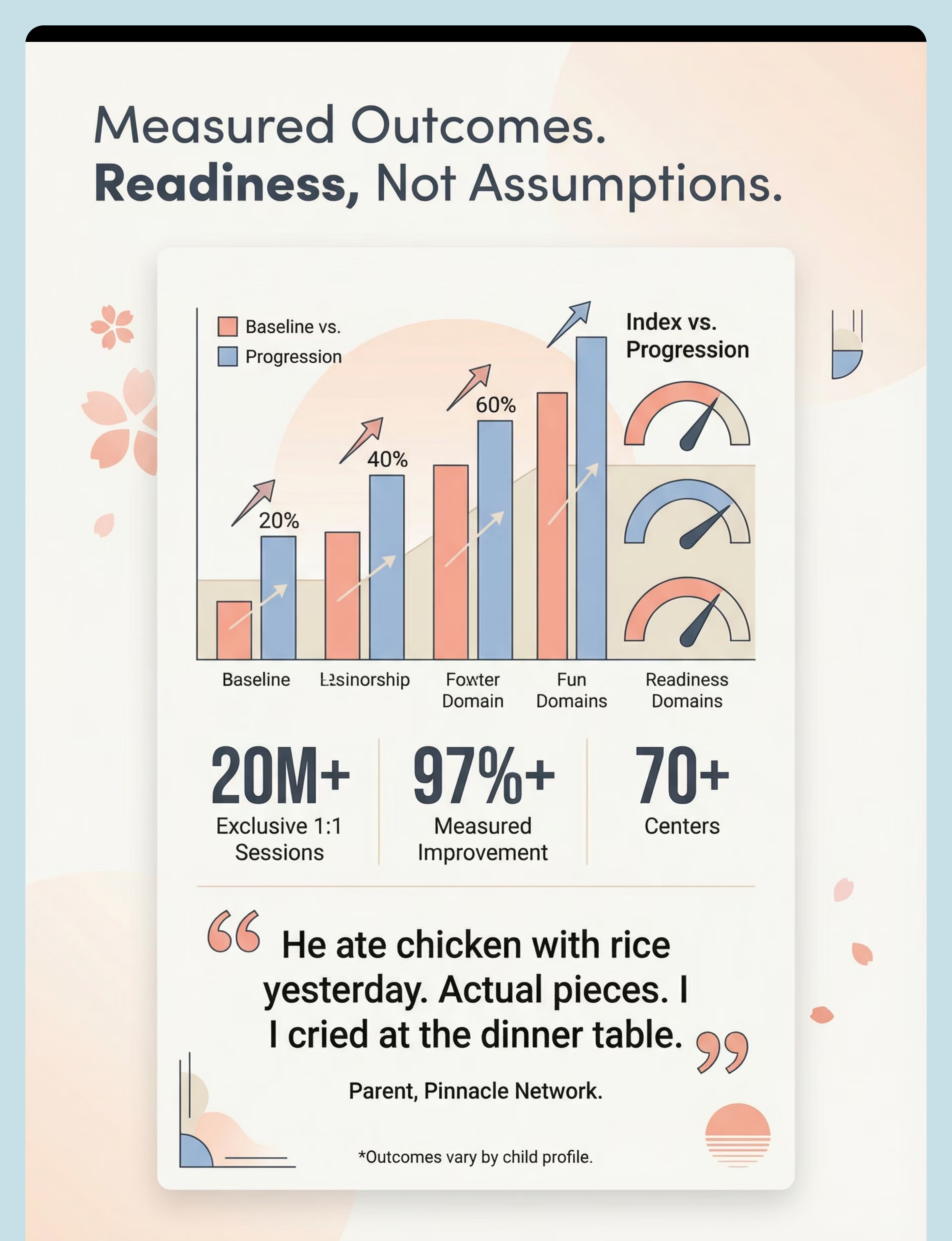
"He ate chicken with rice yesterday. Actual pieces. I cried at the dinner table." — Parent, Pinnacle Network
Outcomes vary by child profile.
Family Celebration Suggestion
Mark the texture chart together. Take a photo. Document this milestone. In 6 months, when your child is eating khichdi with soft vegetable pieces, you'll want to remember where you started.
🚩 Red Flags — When to Pause and Seek Help
Trust your instincts. This protocol is safe when implemented correctly, but there are clear signals that warrant professional support.
1
Weight loss or growth stalling
If your child is not maintaining their growth curve, nutritional intervention is needed alongside texture work.
2
Aspiration signs
Persistent coughing or wet/gurgly voice DURING or AFTER swallowing — may indicate food is entering the airway.
3
Gagging worsening
If gagging becomes MORE frequent or intense despite 4+ weeks of consistent, correct protocol.
4
Complete oral refusal
Child begins refusing ALL oral input including previously accepted tools, toothbrush, and safe foods.
5
Mealtime relationship severely strained
Both parent and child are in distress at every session — the intervention is causing more harm than benefit.
6
No progress after 8–10 weeks
Consistent daily oral prep + weekly texture practice with zero observable change.
If something feels wrong, pause and ask. Your instincts are valid clinical data.
FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
The Progression Pathway — Your Developmental GPS
This technique sits within a broader ecosystem of interconnected interventions. Understanding the pathway helps you see where you've been, where you are, and where you're heading.
The 6-Phase Texture Progression Within A-014
Phase | Name | Weeks | Key Materials | |
1 | Foundation — Regulate Oral System | 1–3 | Oral Vibration, Nuk Brush, Chew Tools | |
2 | Utensil Texture Introduction | 4–6 | Textured Spoons, Mirror | |
3 | Food Play & Exposure (No Eating Pressure) | 7–10 | Food Play Kit, Flavor Spray | |
4 | Meltable Bridge | 11–14 | Meltable Foods, Texture Chart | |
5 | Persistent Soft Textures | 15–20 | Textured Spoons, Texture Chart | |
6 | Mixed Textures & Generalization | 21+ | All materials as support |
Lateral alternatives: If child responds to CRUNCHY but not soft → A-017 may be a better entry point. If the challenge is VARIETY not texture → A-016 addresses neophobia specifically.
Related Techniques in Oral-Tactile Processing
Your investment in the 9-material feeding toolkit transfers across the entire Oral-Tactile domain. You already own materials for 4 of these 6 techniques.

A-015: Toothbrushing Meltdowns
Difficulty: Intro | Materials overlap:✅ Z-Vibe, Nuk Brush
A-016: Won't Try New Foods
Difficulty: Core | Materials overlap:✅ Food Play Kit, Flavor Spray

A-017: Only Eats Crunchy Foods
Difficulty: Core | Materials overlap: Partial — Texture Chart, Mirror

A-018: Drools Excessively
Difficulty: Core | Materials overlap:✅ Oral tools, Chew tools

A-022: Overstuffs Mouth
Difficulty: Advanced | Materials overlap: Partial — Mirror, Chew tools

A-012: Barefoot Refusal
Difficulty: Intro | Materials overlap:❌ Different materials needed
Domain: Sensory → Oral-Tactile Processing (SEN-ORL) | Part of the 20-Category Pinnacle Taxonomy

Your Child's Full Developmental Map
This technique — A-014: Food Texture Gagging — sits within Domain A: Sensory Processing, specifically the Oral-Tactile subdomain. But your child's development isn't siloed.
Oral sensory work connects to multiple developmental domains:
Speech & Language
Oral motor development enables articulation and phonological skills
Behavior
Mealtime behavior is directly linked to sensory tolerance
Daily Living
Eating independence is a core life skill
Social Participation
Family meals, birthday parties, school lunch
Nutrition & Health
Adequate nutrition supports cognitive and physical development
"This technique is one piece of a larger plan."
Source: WHO/UNICEF Nurturing Care Framework (2018) — Five components of nurturing care.

Act V: Community & Ecosystem
Families Who've Been Here — Aarav's Story
Before
Aarav, age 3.5, ate only smooth yogurt, applesauce, and one brand of baby cereal. He gagged on rice. He vomited from dal with even tiny lentil pieces. His mother was blending all family food separately. Weight was dropping.
After (14 Weeks)
Aarav eats soft idli, mashed rice with dal, dissolvable puffs, banana pieces, and is attempting curd rice with small vegetable pieces. Gagging reduced from every meal to rare incidents with new textures. Weight stable.
"He ate chicken with rice yesterday. Actual pieces. I cried at the dinner table." — Aarav's mother
From the Therapist's Notes: Aarav's gag trigger point shifted from the front of the tongue to the back of the palate over 8 weeks of daily oral desensitization. Food play was the turning point — once he was comfortable touching dal, the transition to tasting happened naturally.
Anonymized. Illustrative outcomes; individual results vary by child profile.
Families Who've Been Here — Meera's Story
Before
Meera, age 5, had been on pureed food for 3+ years. Parents had tried hiding lumps in puree — which triggered worse gagging and food refusal. The family was eating dinner in shifts — Meera's blended food first, then the family meal.
After (20 Weeks)
Meera eats at the family table. Her plate includes soft roti pieces with ghee, mashed potato, soft paneer, and she's exploring soft fruit pieces. Meltable foods are now "boring" — she wants "real food."
"For the first time in three years, we all sit and eat together." — Meera's father
Meera's journey illustrates a powerful truth: the protocol works even when previous approaches have failed. The key difference was separating texture practice from nutritional mealtimes and following the child-led, systematic desensitization framework rather than the hiding-lumps approach.
Anonymized. Illustrative outcomes; individual results vary by child profile.
Connect With Other Parents
Isolation is the enemy of adherence. You're not the only parent blending food at midnight. You're not the only one who cried when everyone said "he'll eat when he's hungry." Connection with families on the same journey is therapeutic — for you.
Feeding Challenges Parent Group
WhatsApp community for parents navigating texture sensitivity. Verified by Pinnacle clinical team. Share wins, ask questions, find support.
Pinnacle Parent Forum
Online discussion threads organized by challenge type. Browse stories from families at every stage of the journey.
Local Parent Meetup
Monthly meetups at Pinnacle centers across 70+ locations in India. Face-to-face connection with families who understand.
Peer Mentor Match
Connect 1:1 with a parent who has completed this journey. Their experience becomes your roadmap.
"Your experience helps others — consider sharing your journey."
Your Professional Support Team
Home + Clinic = Maximum Impact. Home-based intervention works best when supported by professional guidance. Pinnacle's 70+ center network provides the clinical infrastructure behind your home sessions.
Services for Food Texture Gagging
Speech-Language Therapy
Feeding-focused SLP-led oral desensitization and texture progression
Occupational Therapy
Comprehensive sensory profile assessment and sensory diet design
Parent Training
Hands-on coaching in oral prep techniques and texture hierarchy
EverydayTherapyProgramme™
Daily home protocols designed and monitored by your clinical team
FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7

The Research Library — For the Curious Parent
Key Studies Supporting This Technique
- PRISMA Systematic Review (2024) — 16 articles from 2013–2023 confirm sensory integration as evidence-based practice for ASD → PubMed: PMC11506176
- Meta-analysis: Sensory Integration in ASD (2024) — 24 studies confirm effectiveness across adaptive behavior, sensory processing, social skills → PubMed: PMC10955541
- Indian RCT: Home-Based Sensory Interventions (2019) — Padmanabha et al. demonstrated significant outcomes for parent-administered interventions → DOI: 10.1007/s12098-018-2747-4
- WHO Nurturing Care Framework (2018) — Foundational framework for ECD across 197 countries → nurturing-care.org
- NCAEP Evidence-Based Practices Report (2020) — Identifies sensory integration and visual supports as evidence-based
- SOS Approach to Feeding — Dr. Kay Toomey's Sequential Oral Sensory framework
- Pre-Feeding Skills — Morris, S.E. & Klein, M.D. (2nd Edition)
- ASHA Guidelines — Pediatric feeding disorders guidelines
- SPD Foundation — spdfoundation.net — Oral cavity receptor density research
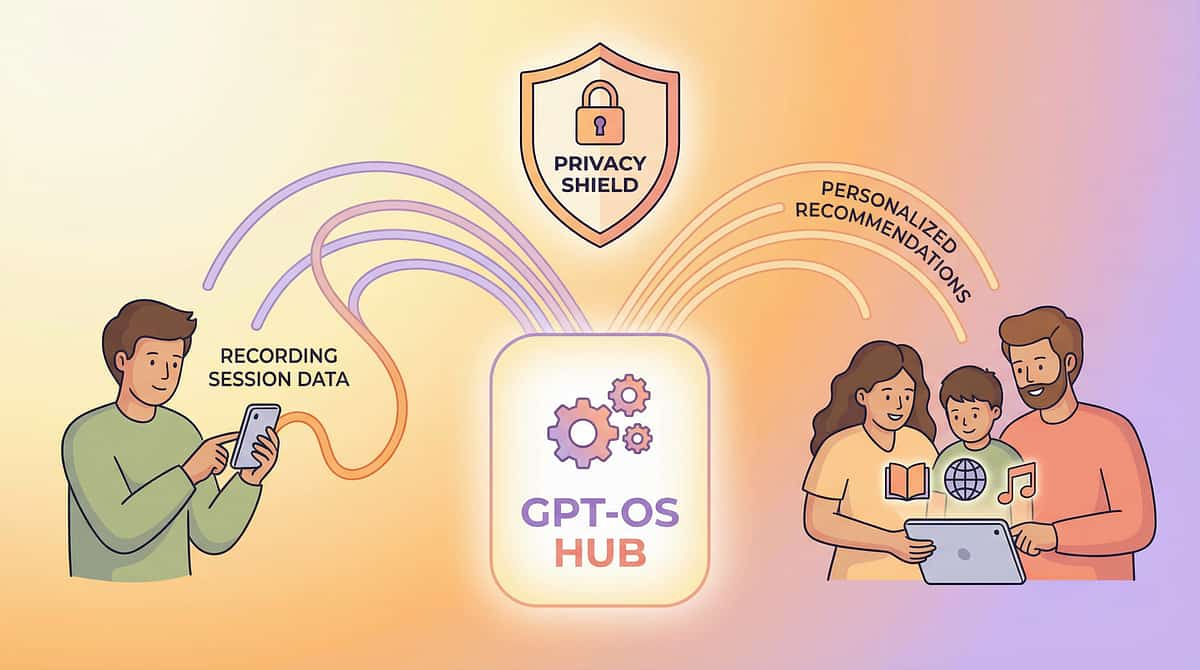
How GPT-OS® Uses Your Data
What GPT-OS® Learns From Your Food Texture Gagging Data
Desensitization Rate
Session-over-session trend of gag reflex tolerance
Optimal Session Length
When diminishing returns begin for YOUR child
Material Effectiveness
Which of the 9 tools works best for YOUR child
Readiness Signals
Data-driven progression to next phase
Risk Signals
Patterns that warrant professional consultation
Privacy & Data Protection
- Your child's data is encrypted and stored under medical-grade security protocols
- Data is NEVER shared with third parties
- Population-level insights (anonymized, aggregated) improve recommendations for all families
- You retain full ownership and can request deletion at any time
"Your data helps every child like yours." 20M+ sessions of data power GPT-OS®'s recommendation engine — making every family's journey smarter.

Watch the Reel — A-014
Sensory Solutions Series — Episode 14
Oral-Tactile Processing
"9 Materials That Help With Food Texture Gagging"
Watch a Pinnacle therapist demonstrate each of the 9 materials, show correct oral desensitization technique, and walk through the texture progression in 75 seconds.
Video content reinforces what you've read here — seeing the Z-Vibe in action, watching a child accept a meltable puff for the first time, and understanding the precise angle and pressure for oral massage.
Therapist
Pinnacle Blooms Feeding Specialist (SLP)
Duration
~75 seconds
Tone
Warm, validating, non-judgmental
Share This With Your Family
If only one parent knows the technique, impact is limited. Consistency across caregivers multiplies impact exponentially.
💬 WhatsApp
Pre-formatted message with technique summary and page link
📧 Email
Shareable link with technique overview
🔗 Copy Link
techniques.pinnacleblooms.org/sensory/food-texture-gagging-materials
Downloadable Resources
- 📄Family Guide (1-page PDF) — Simplified overview for spouse, grandparents, household helpers
- 👴"Explain to Grandparents" Version — Large font, simplified language, key do's and don'ts
- 🏫Teacher Communication Template — Letter explaining your child's texture sensitivity and needed accommodations
Key message for family members: "Your grandchild/student isn't being difficult or picky. Their brain processes food texture differently — a tiny lump triggers the same reflex that protects against choking. We're using a proven, systematic approach to build tolerance. Here's how you can help: never force food, celebrate any interaction with new textures, and follow the approach on this page."
Act VI: Close & Loop
Frequently Asked Questions
How long until my child eats normal food?
Typical timeline is 12–24+ weeks from purees to mixed textures, but this varies significantly. Some children progress faster on oral desensitization but slower on actual food texture. The key is consistency, not speed.
Should I stop blending his food while doing this?
NO. Never remove safe foods. Nutritional meals stay safe (blended/pureed if that works). Texture practice is SEPARATE. When your child is ready, they will naturally start rejecting purees in favor of the textures they've learned to tolerate.
My child only gags on certain textures — does this still apply?
Yes. Many children have a specific texture profile — they may tolerate crunchy but not soft, or smooth but not lumpy. The 9 materials work across all texture profiles. Start with the specific texture type your child avoids.
Can I use this for a child under 18 months?
Modified version only. Use vibrating toothbrush (gentle, external) and age-appropriate meltable foods. No chew tools with small parts. Consult your pediatrician.
Is this the same as the SOS Approach to Feeding?
This protocol incorporates SOS principles alongside oral motor therapy (SLP), sensory integration (OT), and applied behavior analysis. It's an integrated, multi-disciplinary protocol — not a single framework.
What if my child has ARFID?
Texture sensitivity is often a component of ARFID. This technique addresses the sensory component. ARFID may also involve anxiety, low appetite, or fear of choking, which require additional clinical support.
Do I need to buy all 9 materials?
No. Start with the 3 Essential Starters (vibrating toothbrush, meltable foods, textured spoons). Add others as needed. Many have DIY alternatives (Card 11).
My child eats biscuits at school but nothing at home
This is common. School foods are often dry/crunchy (easier textures). Home foods tend to be wetter, mixed, and more complex. Work on home textures using this protocol. Share the teacher template so school understands.
Preview of 9 materials that help with food texture gagging Therapy Material
Below is a visual preview of 9 materials that help with food texture gagging therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.












Link copied!

Your Next Step — Start Now
You've read the science. You understand the brain. You have the materials list, the protocol, the troubleshooting guide, and the progression pathway. Now: act.
🟢 Start This Technique Today
Download the tracking sheet, set up your space, run the readiness check, and begin Step 1. Your child's journey starts with one 2-minute session.
📞 Book a Consultation
Connect with a Pinnacle feeding specialist for personalized guidance. 9100 181 181 | pinnacleblooms.org/consult
➡️ Explore Next Technique
A-015: Toothbrushing Meltdowns | A-016: Won't Try New Foods
The Pinnacle Promise
"From fear to mastery. One technique at a time."
You arrived on this page scared, confused, and exhausted. Your child's gagging felt like a wall with no door. Now you have 9 keys — each one evidence-based, home-executable, and validated by a consortium of experts who have guided 20M+ therapy sessions across 70+ centers.
Your child's nervous system is remarkable. It can learn. It can adapt. It can grow. And you — the parent who showed up, who read every card, who is ready to begin — you are the catalyst.
🗣️ SLP
🧠 OT
📊 BCBA
📚 SpEd
👨⚕️ NeuroDev
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System.
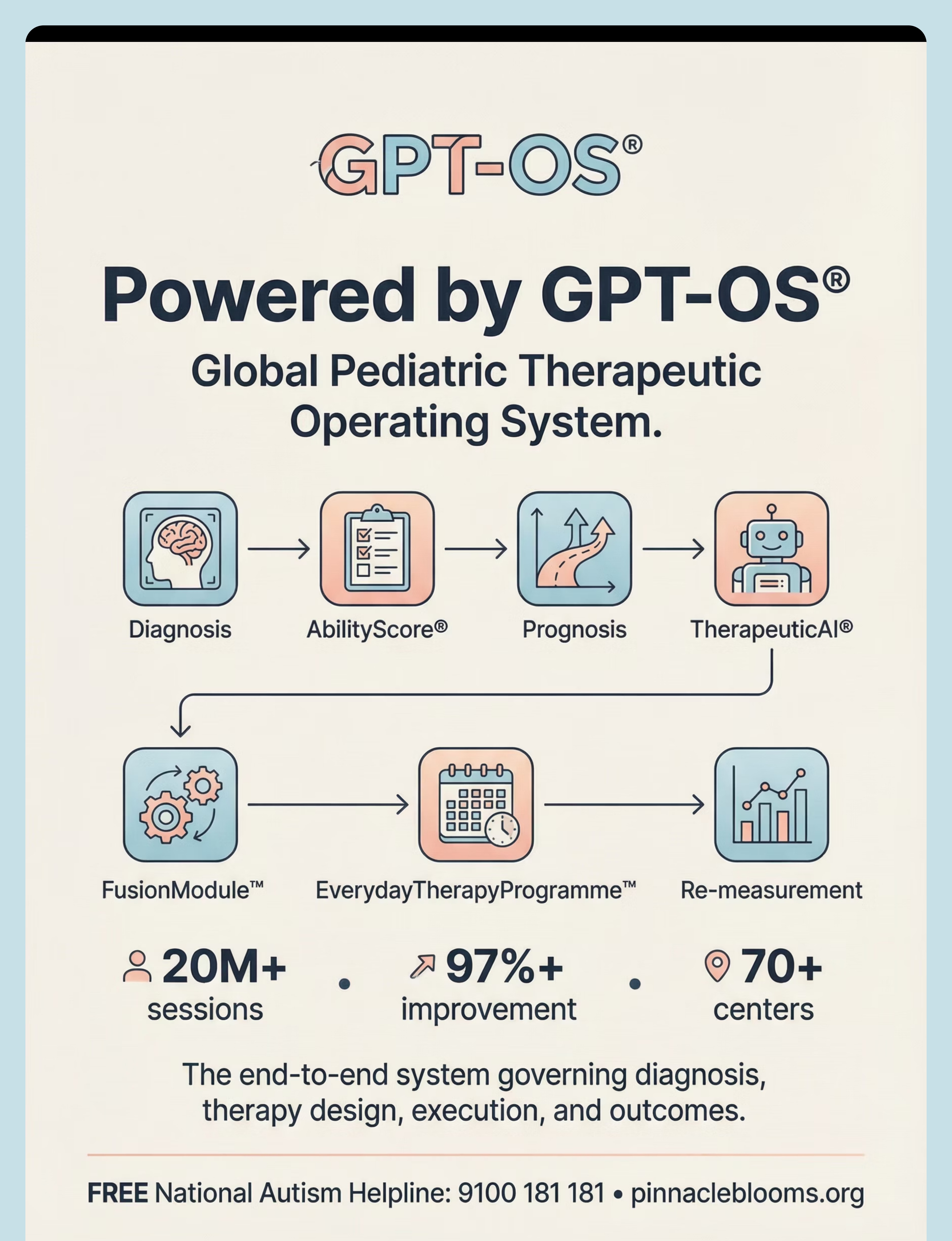
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
20M+ sessions • 97%+ measured improvement • 70+ centers • Patents filed across 160+ countries
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed speech-language pathologist or occupational therapist. If food texture gagging is affecting nutrition or growth, please consult a qualified feeding specialist. Individual results may vary. Texture progression should be child-led and never forced.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Contact: FREE National Autism Helpline: 9100 181 181 | pinnacleblooms.org | care@pinnacleblooms.org