
It's not that he won't focus. His brain genuinely doesn't know how — yet.
Homework that should take 15 minutes stretches to two hours of redirecting, reminding, and frustration. He starts tasks and walks away mid-sentence. But put him in front of a video game and he's locked in for hours. You are not failing as a parent. Your child's attention system is developing differently — and differently does not mean permanently.
L-986 | Focus Building
Attention & Executive Function
Pinnacle Blooms Network®
You Are Not Alone — The Numbers
You are among millions of families navigating this exact challenge. In India alone, an estimated 3–5 million children between ages 4–12 experience significant attention difficulties that impact daily learning, social participation, and family wellbeing.
1
Clinical Criteria
Children meet clinical criteria for attention difficulties before age 10
2
ASD Co-occurrence
Of children with ASD display co-occurring attention and executive function challenges
3
Global Referrals
Of all pediatric therapy referrals globally cite attention as a primary concern
"The exhaustion you feel from being your child's external attention system is real, recognized, and shared by millions of families right now."
PRISMA Systematic Review (2024): 80% of children diagnosed with ASD display sensory processing difficulties with significant attention overlap. Global ADHD prevalence: 5.29% across 102 studies (Polanczyk et al.). References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
This Is a Wiring Pattern, Not a Willpower Problem.
The Prefrontal Cortex
The brain's "mission control" — decides what to pay attention to, filters distractions, and holds the plan in working memory. In children with attention difficulties, this region matures 3–5 years later than neurotypical peers and requires more environmental scaffolding to activate.
The Dopamine Pathway
Video games are engineered to trigger rapid dopamine release. Homework has no such mechanism. Your child isn't choosing video games — their dopamine system is responding to what it was wired to respond to.
The Sensory System
Many children cannot focus not because of cognitive deficits but because their nervous system is in a state of over- or under-arousal. Providing appropriate sensory input — movement, deep pressure, proprioception — reorganizes the nervous system toward the optimal arousal state for focus.
This is a wiring difference, not a behavior choice. And wiring can be shaped — especially in the pediatric window.
Frontiers in Integrative Neuroscience (2020): Neurological basis for sensory-based interventions in ASD established — somatosensory cortex over-amplification confirmed as mechanism. | PFC maturation timeline: Shaw et al., PNAS (2007).
Attention Is Not Fixed at Birth. It Develops.
Your child is on the journey — and understanding where they are in the developmental arc transforms how you respond to their attention challenges.
1
Age 2–3
2–5 min focus window. Simple cause-effect toys.
2
Age 3–5
5–15 min focus window. Beginning task completion with support.
3
Age 5–8
15–30 min focus window. Multi-step academic tasks.
4
Age 8–12
30–45 min focus window. Self-managed strategies.
5
Age 12+
45+ min focus window. Independent focus across contexts.
Current Challenge Zone: Most children struggling with focus sit in the Age 5–8 window — where expectations jump dramatically (homework, classroom listening, task completion) but the neurological infrastructure is still under construction.
A general guideline: children can sustain focused attention for approximately 2–5 minutes per year of age — on tasks that are appropriately challenging, interest-relevant, and sensory-supportive. Below this threshold with all conditions met is the clinical signal. Focus difficulties frequently co-occur with sensory processing differences, anxiety, sleep disruption, working memory challenges, ADHD, and learning differences.

Clinically Validated. Home-Applicable. Parent-Proven.
Every material and technique in this protocol rests on a foundation of peer-reviewed evidence — not trend, not anecdote. Here is the evidence base that governs this approach.
Level I Evidence — Sensory-Based Focus Interventions
A 2024 PRISMA systematic review analyzing 16 studies (2013–2023) confirmed that sensory integration-based interventions meet criteria for evidence-based practice in children with ASD and attention difficulties. Effect sizes were significant for: sustained attention duration, task completion rates, and reduction in caregiver-reported redirection frequency.
Level II Evidence — Environmental Modification for Attention
Studies consistently demonstrate that environmental modifications — noise reduction, workspace organization, visual scheduling — produce measurable improvements in on-task behavior without pharmacological intervention, particularly in children with sensory processing differences.
Level II Evidence — Material-Based Attention Scaffolding
Occupational therapy literature confirms weighted input, movement integration, and structured task supports improve attention regulation in pediatric populations across home and school settings.
Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions demonstrated statistically significant outcomes in attention-related behaviors when parent-administered with therapist guidance. Indian Journal of Pediatrics | DOI: 10.1007/s12098-018-2747-4
References: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4 | NCAEP Evidence-Based Practices Report (2020)

The Technique: What It Is
Domain: Attention & Executive Function — ATT-FOCUS
Age: 3–12 years
Duration: 10–20 min/session
Frequency: Daily integration
Focus Building Through Material-Based Attention Scaffolding
Parent-Friendly Alias: "Giving your child's brain the conditions it needs to focus — not demanding focus from a brain that hasn't been given what it needs."
Focus Building Through Material-Based Attention Scaffolding is an evidence-based approach that uses specific therapeutic materials and environmental tools to create the neurological conditions necessary for sustained attention in children. Rather than demanding focus through consequences and rewards alone, this approach provides the sensory regulation, time management scaffolding, environmental modification, and graduated challenge that the developing attention system requires.
The 9 materials in this protocol target different components of the attention system — sensory arousal regulation, selective attention, time perception, executive function support, and environmental distraction reduction — creating a multi-layered foundation for genuine, developing focus capacity.
Canon Categories
Sensory Tools | Visual Supports | Regulation Materials
Episode
L-986 | Attention & Executive Function Series
Reel Connection
Evidence-based companion to Reel L-986 from the 999 Reels Master library
Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type. Five disciplines converge around focus building at Pinnacle Blooms.
Occupational Therapy (Primary Lead)
OTs are the primary architects of material-based attention scaffolding. They assess the sensory processing profile, identify whether the child is a seeker or avoider, and guide weighted lap pad weight, wobble cushion inflation, and fidget tool selection.
Applied Behavior Analysis (ABA/BCBA)
ABA specialists design the reinforcement architecture, build data tracking systems, implement checklists, and systematically fade prompting as independent focus develops.
Special Education
SpEd specialists adapt focus-building materials for classroom and academic contexts, coordinating workspace organization and visual schedules aligned with IEP goals.
Speech-Language Pathology (SLP)
SLPs integrate focus-building materials into communication sessions. Attention is the prerequisite for all language learning — making these materials cross-disciplinary tools.
NeuroDevelopmental Pediatrics
NeuroDev physicians provide the diagnostic foundation: ADHD assessment, sensory processing evaluation, sleep analysis, and coordination of medication evaluation when clinical indicators warrant.

What This Targets
This is not a random activity. It is a precision tool with measurable targets — organized across three tiers from immediate behavioral goals to long-term developmental gains.
1
Primary Targets
- Sustained attention duration (time on task without redirection)
- Selective attention (filtering irrelevant stimuli)
- Attention initiation (starting tasks without extended warm-up)
- Task completion (seeing tasks through to their endpoint)
2
Secondary Targets
- Sensory regulation and arousal state management
- Working memory support
- Inhibitory control (resisting distraction)
- Time perception and self-monitoring
3
Tertiary Targets
- Academic readiness and classroom participation
- Independence in self-directed work
- Confidence through successful task completion
- Social attention in conversation and play
9 Materials That Help With Focus Building
Each material addresses a different component of the attention system. Together, they form a multi-layered scaffolding system for genuine, developing focus capacity.

1. Weighted Lap Pad or Blanket
Canon Category: Sensory Regulation
Deep pressure proprioceptive input activates the parasympathetic nervous system. Approximately 10% of child's body weight. Use during homework, reading, or circle time.
Price Range: ₹1,000–3,500
Deep pressure proprioceptive input activates the parasympathetic nervous system. Approximately 10% of child's body weight. Use during homework, reading, or circle time.
Price Range: ₹1,000–3,500

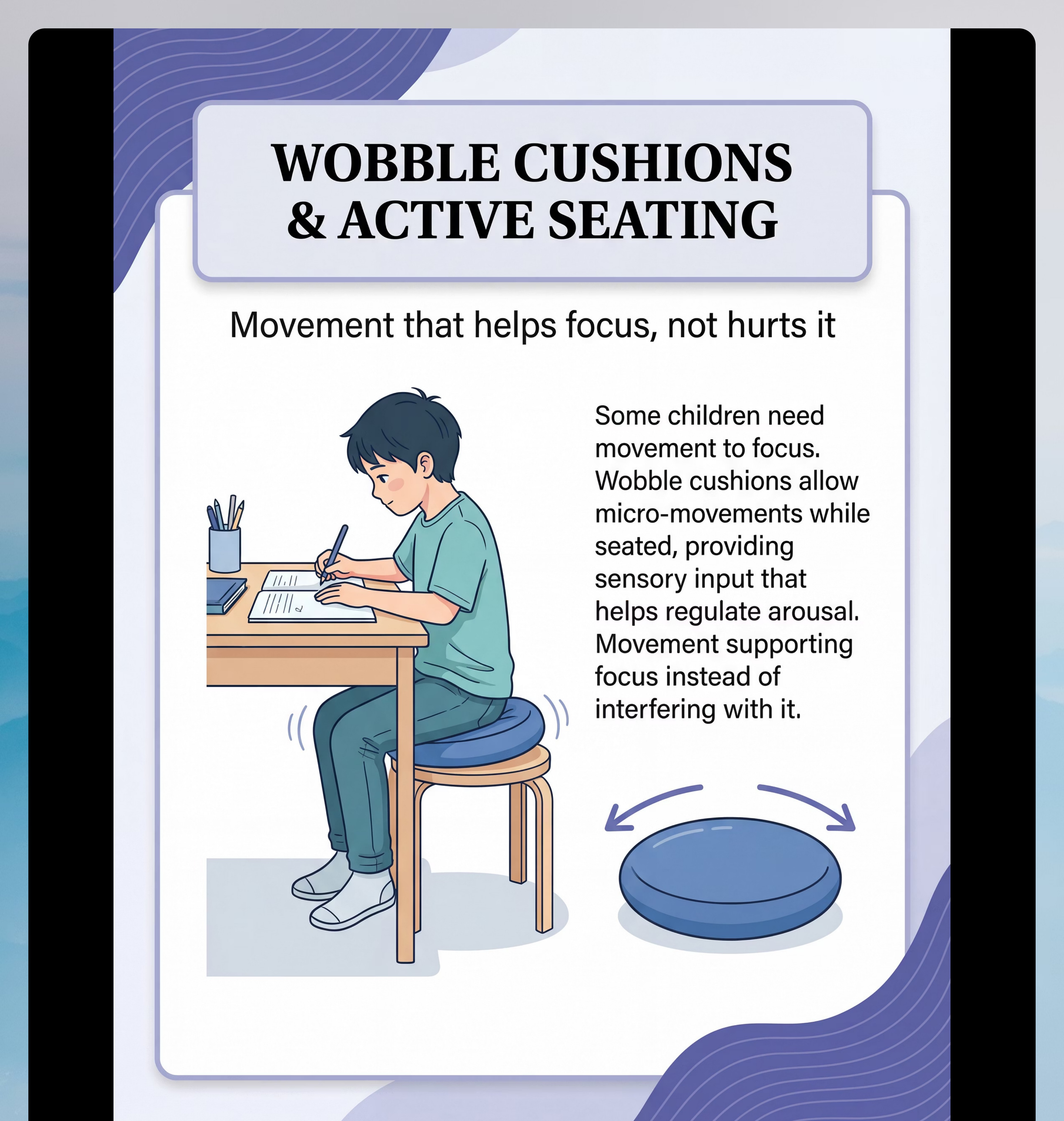
2. Wobble Cushion / Active Seating Disc
Canon Category: Sensory Regulation / Vestibular
Provides controlled micro-movement that channels sensation-seeking into non-disruptive motion, allowing the child to move AND attend simultaneously.
Price Range: ₹800–2,500
Provides controlled micro-movement that channels sensation-seeking into non-disruptive motion, allowing the child to move AND attend simultaneously.
Price Range: ₹800–2,500

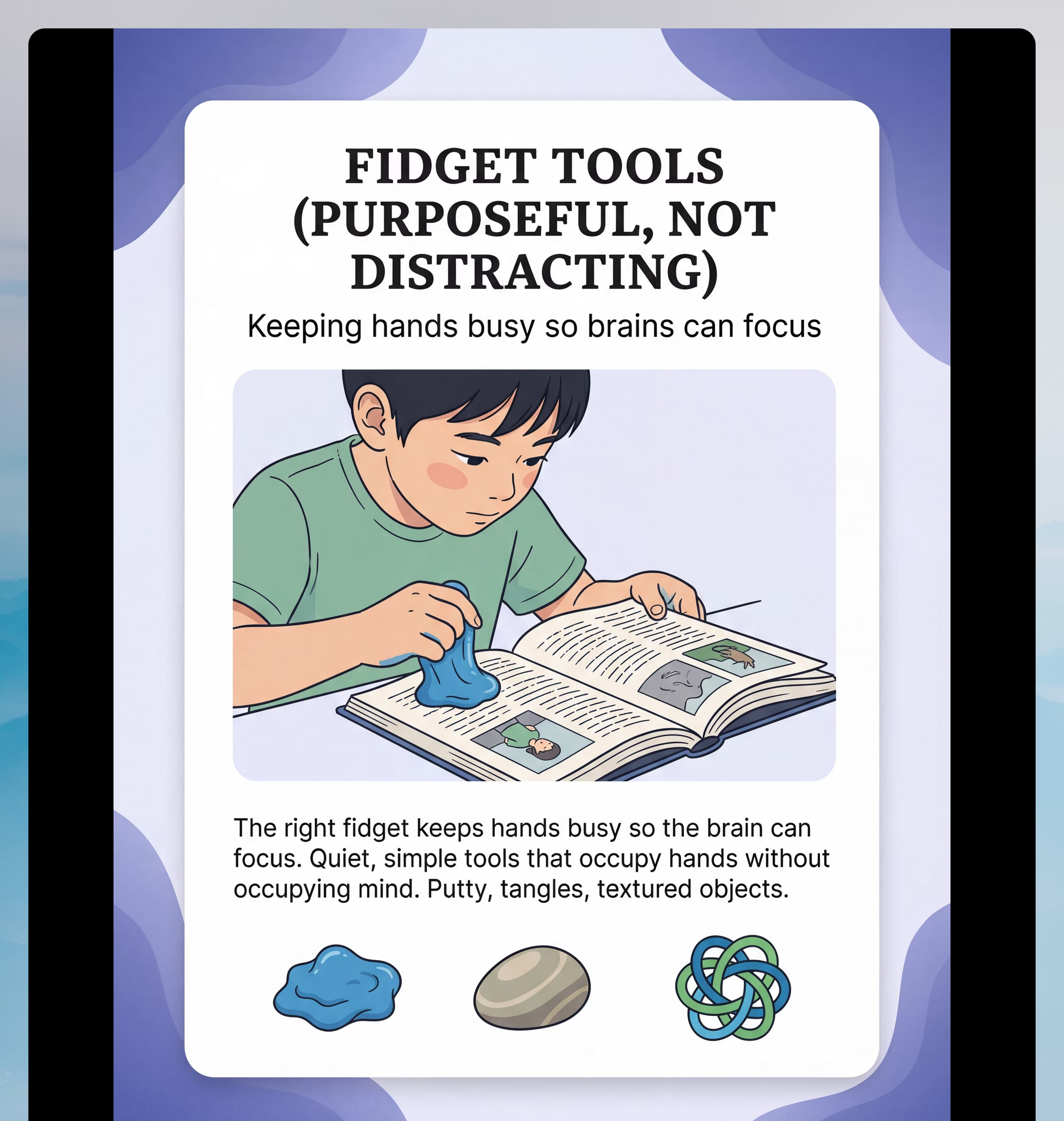
3. Fidget Tools (Purposeful)
Canon Category: Sensory Regulation / Tactile
Quiet, simple tools — therapy putty, tangle toys, textured stones — that can be used automatically without visual attention. The hands are busy; the mind is free.
Price Range: ₹100–800
Quiet, simple tools — therapy putty, tangle toys, textured stones — that can be used automatically without visual attention. The hands are busy; the mind is free.
Price Range: ₹100–800
Materials 4–6

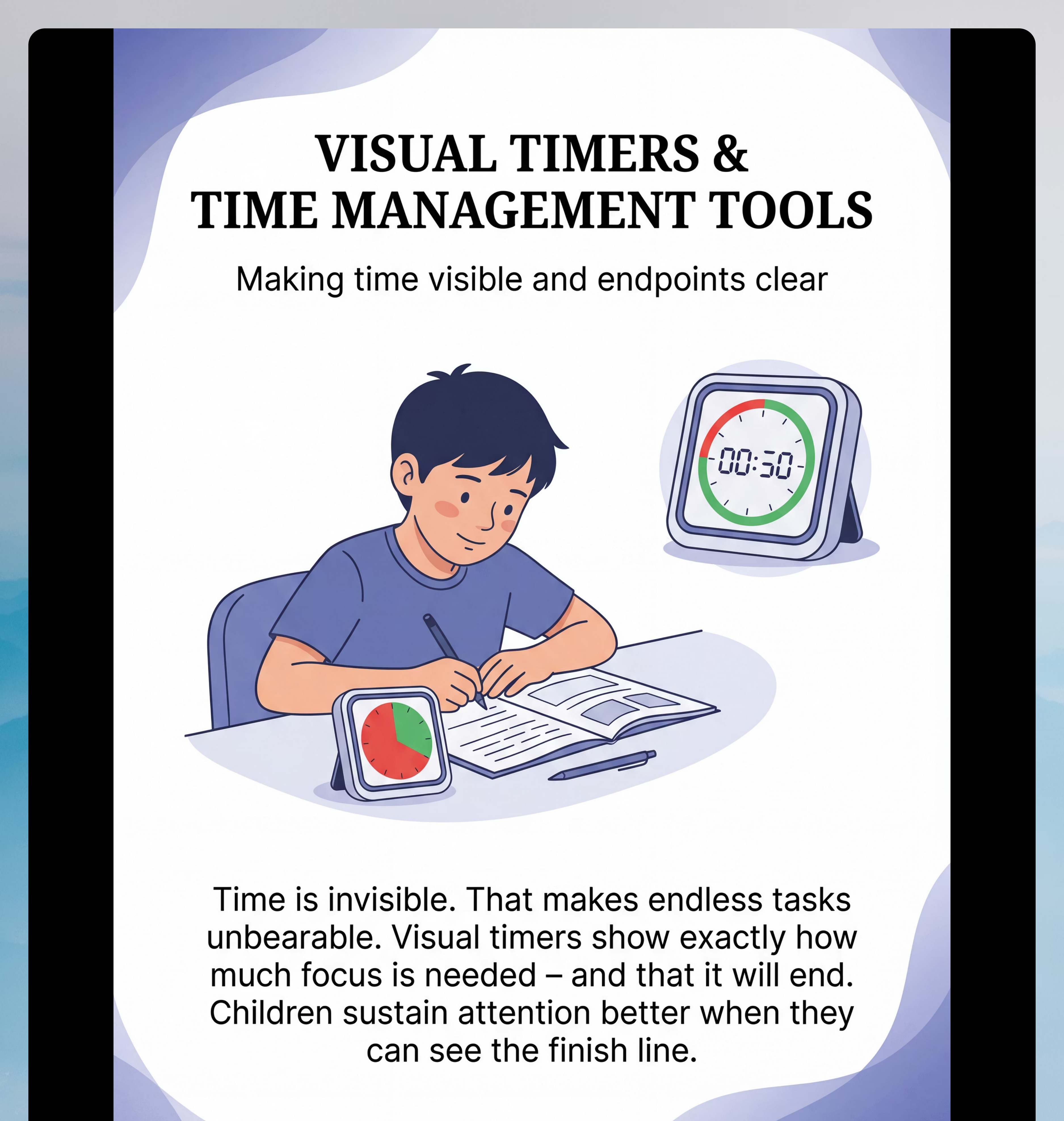
4. Visual Timer
Canon Category: Visual Supports / Time Management
Children with attention difficulties often have impaired time perception — tasks feel endless because the endpoint is invisible. Visual timers make time concrete and create the "just a little more" motivation as the end approaches.
Price Range: ₹500–2,000
Children with attention difficulties often have impaired time perception — tasks feel endless because the endpoint is invisible. Visual timers make time concrete and create the "just a little more" motivation as the end approaches.
Price Range: ₹500–2,000

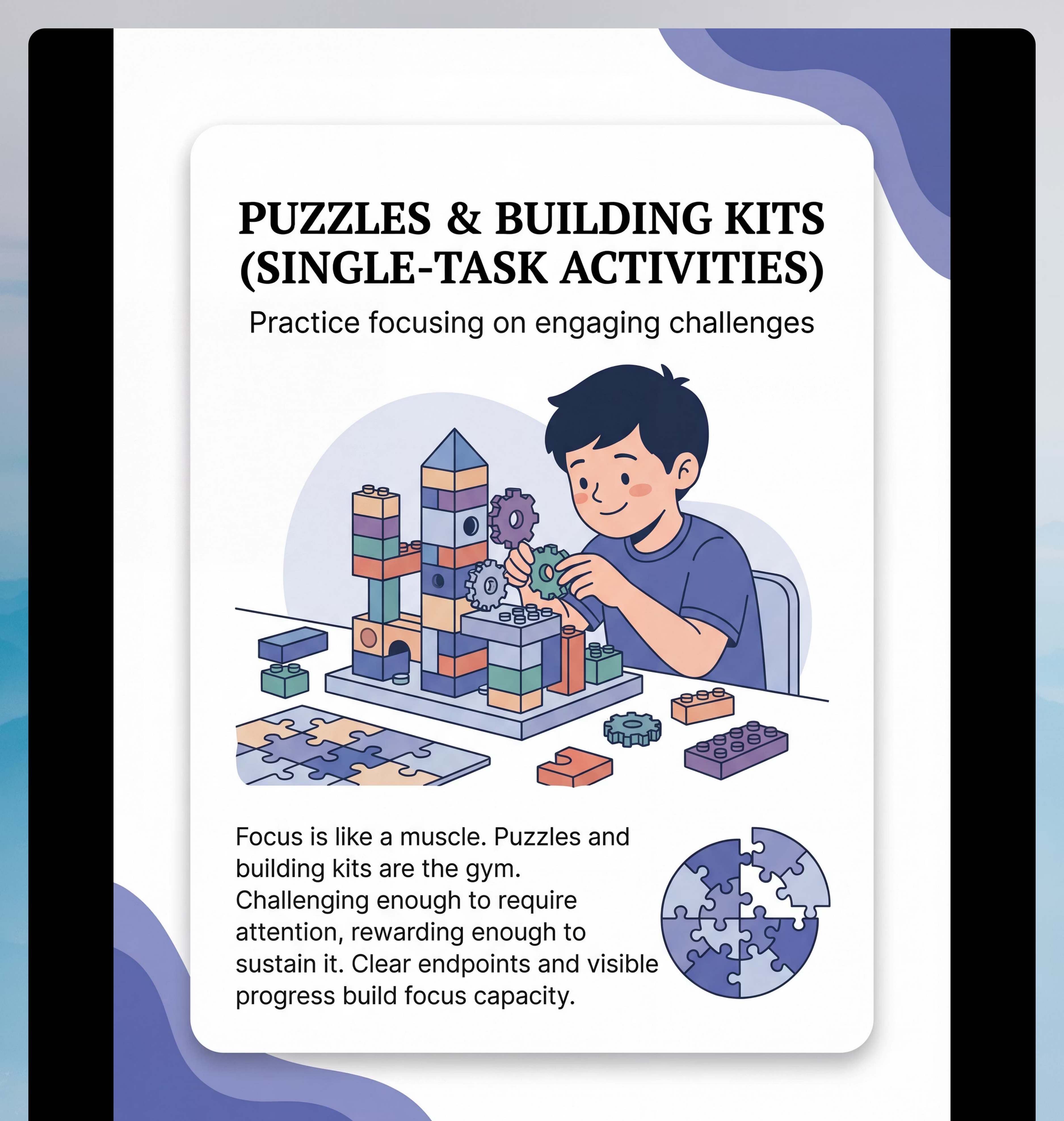
5. Puzzles & Building Kits (Single-Task)
Canon Category: Problem-Solving Toys
Focus is a muscle. Puzzles and building kits are the gym. Clear endpoint, visible progress, appropriate challenge — and that capacity transfers to less preferred tasks.
Price Range: ₹300–2,500
Recommended: SHINETOY Shut The Box Game — ₹428 | Smartivity DIY Clock Kit — ₹673
Focus is a muscle. Puzzles and building kits are the gym. Clear endpoint, visible progress, appropriate challenge — and that capacity transfers to less preferred tasks.
Price Range: ₹300–2,500
Recommended: SHINETOY Shut The Box Game — ₹428 | Smartivity DIY Clock Kit — ₹673

6. Noise-Reducing Headphones / Earmuffs
Canon Category: Sensory Regulation / Auditory
Many focus problems are actually filtering problems — the child hears everything and cannot prioritize. No music required — just silence that decreases the auditory sensory load.
Price Range: ₹500–3,000
Many focus problems are actually filtering problems — the child hears everything and cannot prioritize. No music required — just silence that decreases the auditory sensory load.
Price Range: ₹500–3,000
Materials 7–9

7. Checklist & Task Breakdown System
Canon Category: Visual Supports / Executive Function
Large tasks are overwhelming. Ten small steps are doable. Visual checklists externalize working memory and planning. Checking off each step releases a small dopamine reward, reinforcing continued engagement.
Price Range: ₹100–500
Large tasks are overwhelming. Ten small steps are doable. Visual checklists externalize working memory and planning. Checking off each step releases a small dopamine reward, reinforcing continued engagement.
Price Range: ₹100–500

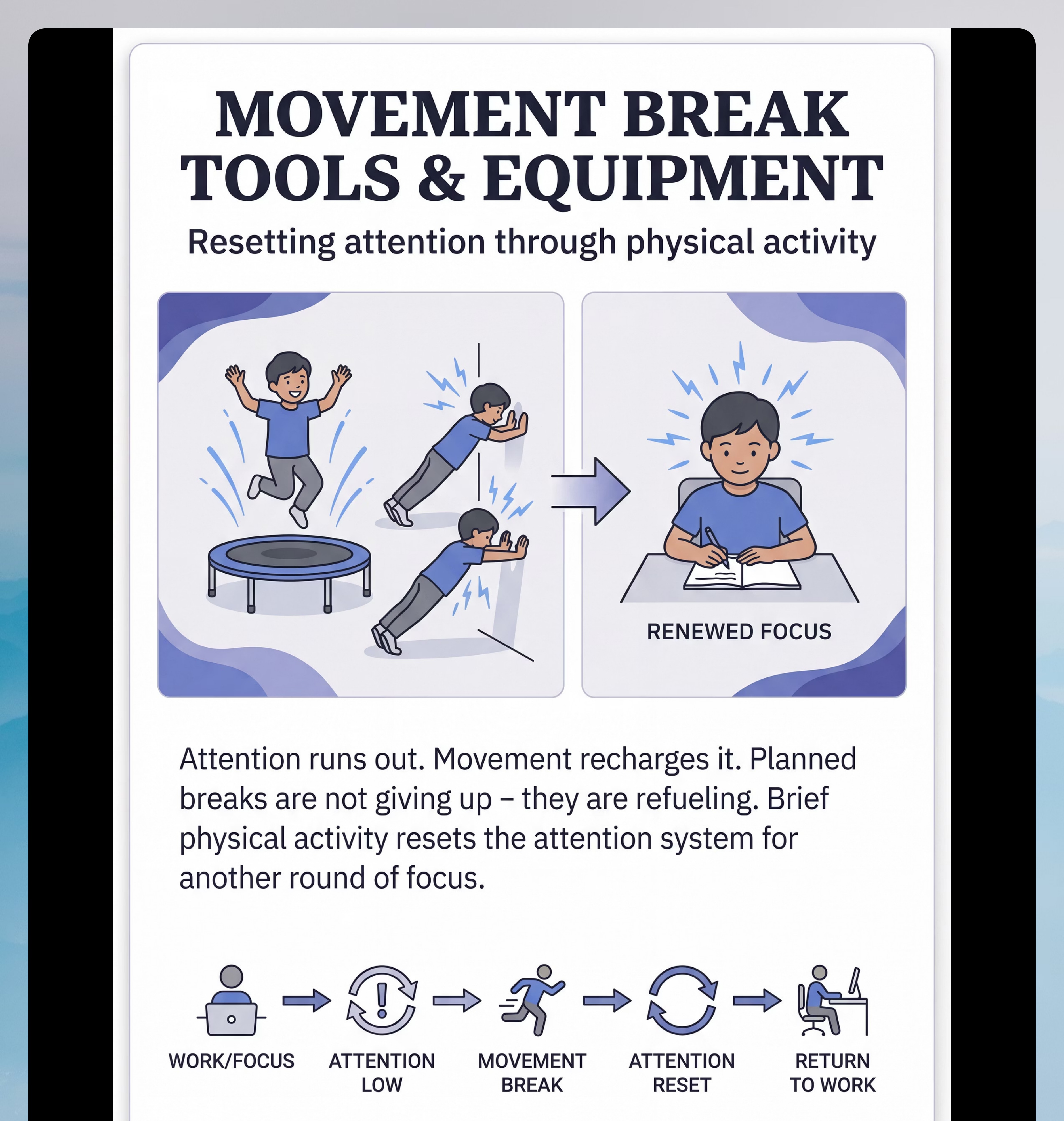
8. Movement Break Equipment
Canon Category: Sensory / Proprioceptive Reset
Attention runs out. Movement recharges it. Planned movement breaks — mini-trampoline, yoga cards, wall push-ups — allow the attention system to reset before fatigue causes complete focus collapse.
Price Range: ₹500–3,000
Attention runs out. Movement recharges it. Planned movement breaks — mini-trampoline, yoga cards, wall push-ups — allow the attention system to reset before fatigue causes complete focus collapse.
Price Range: ₹500–3,000

9. Focus-Friendly Workspace Organization Tools
Canon Category: Environmental Modification
Every visible object is something the brain must choose not to attend to. Organized, minimal workspaces reduce filtering demand, leaving more cognitive resources for the task.
Price Range: ₹300–1,500
Every visible object is something the brain must choose not to attend to. Organized, minimal workspaces reduce filtering demand, leaving more cognitive resources for the task.
Price Range: ₹300–1,500
Reinforcement Ecosystem: Pair all materials with proven reinforcement tools — Reward Jar (₹589) and 1800+ Reward Stickers (₹364) from the Pinnacle Canon database. Total Starter Kit Range: ₹3,800–16,800 for a comprehensive focus support system.
Every Family Can Start Today — ₹0 Versions of All 9 Materials
WHO/UNICEF Equity Principle: No child's development should be limited by household income. Every material in this protocol has a zero-cost household alternative based on the same sensory and cognitive principles.
Material | Commercial | ₹0 DIY Alternative | Why It Works | |
Weighted Lap Pad | ₹1,000–3,500 | Pillowcase filled with 1–2 kg dry rice, stitched closed | Weight is the therapeutic agent, not the product | |
Wobble Cushion | ₹800–2,500 | Partially deflated beach ball or folded firm cushion | Controlled instability provides the same vestibular micro-movement | |
Fidget Tool | ₹100–800 | Flour-filled balloon, smooth stone, rubber band around wrist | Tactile stimulation occupies hands — material is secondary to sensory principle | |
Visual Timer | ₹500–2,000 | Sand hourglass or phone timer turned face-up | Any visible time representation works | |
Puzzle / Building Kit | ₹300–2,500 | Drawing a specific picture, sorting household objects, stacking books by size | Clear goal + visible progress + appropriate challenge | |
Noise-Reducing Headphones | ₹500–3,000 | Quietest room, closed windows, white noise from fan, rolled cotton in ears | Any method that decreases unpredictable background sound | |
Checklist System | ₹100–500 | Paper + marker + stickers; whiteboard + dry erase marker | Externalized working memory — any visible step-tracking works | |
Movement Break Tools | ₹500–3,000 | Jumping jacks, wall push-ups, animal walks, dance to one song | The physical activity IS the therapeutic agent | |
Workspace Organization | ₹300–1,500 | Clear desk except current task; face wall; cardboard box as privacy screen | Visual competition reduction — minimize visible objects |
Safety First — Read This Before Your First Session. Every Time.
🔴 RED — DO NOT PROCEED if:
- Child is in active meltdown, severe distress, or emotional dysregulation
- Child shows signs of illness, fever, or physical pain
- Child is hungry or significantly tired (within 2 hours of sleep)
- Weighted materials: child cannot independently remove the lap pad
- Weighted materials: child is under 2 years old
- Noise headphones: child is near a road or at a playground requiring safety sound awareness
- Fidgets: child mouths objects AND materials have small parts
🟡 AMBER — MODIFY AND PROCEED CAREFULLY if:
- Child had a difficult day at school (use easier version — reduce session duration by 50%)
- Child is slightly elevated but not melting down
- First week of introducing any new material (introduce one at a time, 3-day trial minimum)
- Wobble cushion: child has balance challenges (ensure chair arms or desk edge for stability)
- Movement breaks: limited indoor space (modify to standing desk pushes, chair dips)
🟢 GREEN — PROCEED if:
- Child is fed, rested, and in a calm-to-regulated state
- Environment is prepared per Card 12
- You have 15–20 minutes of uninterrupted time
- You have reviewed the readiness checklist
RED LINE — Stop Immediately if: Child shows self-injurious behavior | severe distress escalation | strong physical refusal | signs of physical pain during weighted material use.
Helpline: 9100 181 181 — Free National Autism Helpline, 24×7, 16+ languages
Helpline: 9100 181 181 — Free National Autism Helpline, 24×7, 16+ languages

Material-Specific Safety Notes
1
Weighted Materials
Maximum 10% of child's body weight. Never use for sleep in children under 7. Breathable, washable cover required. Check for filling allergies (latex, rice, poly pellets).
2
Wobble Cushion
Ensure correct inflation — too firm defeats the purpose; too soft creates instability risk. Supervise initially until the child demonstrates comfortable balance on the disc.
3
Fidget Tools
No small parts for children who mouth objects. Establish "fidget rules" explicitly before first use. Fidgets are therapeutic tools, not toys — communicate this distinction clearly to the child.
4
Movement Breaks
Clear safe space before beginning. Supervise trampoline at all times. Match movement intensity to the child's regulation need — energizing vs. organizing vs. calming all serve different purposes.
Indian Journal of Pediatrics RCT (2019): Home-based sensory intervention safety protocols established for parent-administered sessions with safety monitoring integrated. References: DOI: 10.1007/s12098-018-2747-4
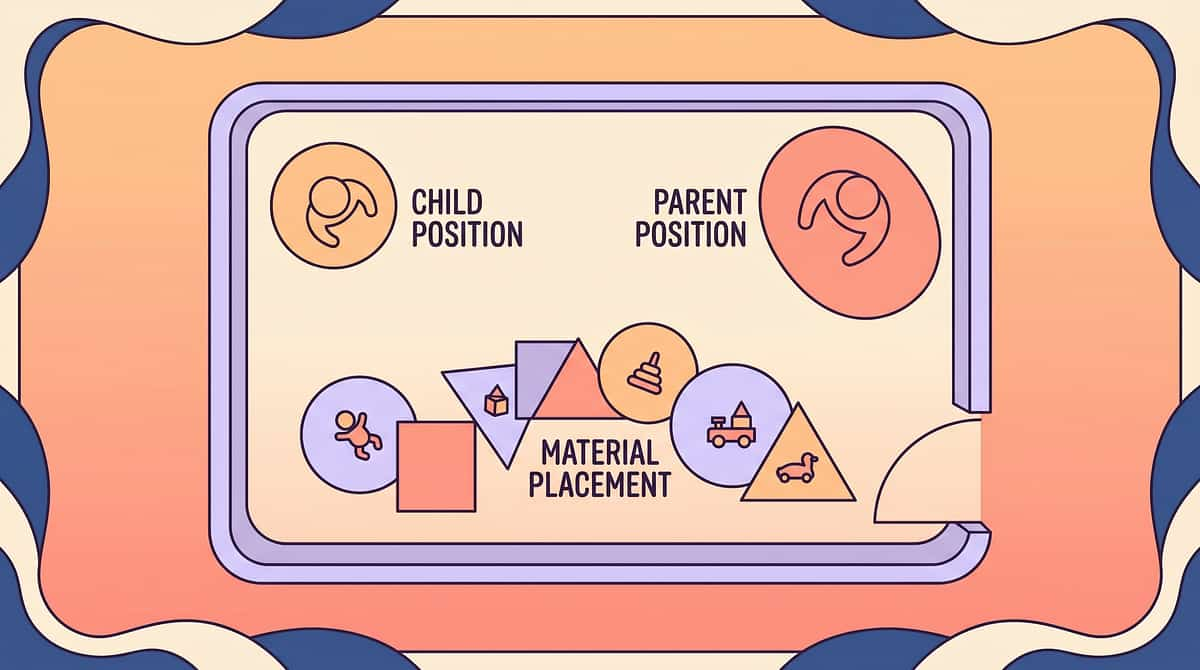
Set Up Your Space — The Environment Is as Important as the Technique
Get this right before you begin. Research confirms that 1:1 structured sessions in optimized environments show maximum effectiveness for attention interventions.
1
[1] Child's Position
Seated, feet flat on floor or supported, desk at elbow height. Lap pad in position if using. Wobble cushion on chair if using. Fidget in reach (but not visible if distracting).
2
[2] Parent's Position
45° to the side and slightly behind — visible but not dominant. Not hovering directly above. Creates monitoring without pressure — the child feels supported, not watched.
3
[3] Visual Timer Placement
In child's peripheral vision (not requiring a head turn), at eye level. Set to session target duration. The timer is the neutral authority — not the parent.
4
[4] Materials on Desk
Only what's needed for THIS session is on the desk. All other materials stored out of sight. Checklist visible if using. Visual clutter directly competes with attention.
5
[5] Movement Break Zone
2m × 2m clear floor space near the desk. Pre-identified — child knows this is the break zone before the session begins.
Environmental Optimization: Lighting: natural or warm white. Sound: below 50dB background. Temperature: 18–22°C if possible. Remove screens, unrelated toys, visual clutter, and noise sources from the child's line of sight.
Is Your Child Ready? — The 60-Second Readiness Check
The best session is one that starts right. Run through these 7 observable indicators before beginning — not as judgment, but as skilled therapeutic assessment.
# | Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
1 | Fed: Ate a full meal or adequate snack | Within last hour | 2–3 hours ago, energy stable | Hungry / skipped meal | |
2 | Rested: Slept adequately last night | 8–10 hrs, refreshed | Some tiredness but alert | Significantly sleep-deprived | |
3 | Regulated: Emotional state calm to engaged | Calm, even happy | Slightly elevated, not dysregulated | Active meltdown/distress | |
4 | Healthy: No signs of illness or discomfort | No signs | Mild cold, monitoring | Fever, pain, acute illness | |
5 | Recent History: No severe episode in last 2 hours | Clear window | Minor difficulty, recovered | Major incident, not recovered | |
6 | Environment: Space prepared per Card 12 | ✅ Done | Partially done | Not done — pause and set up | |
7 | Time: 15–20 minutes available | ✅ Full time | 10 minutes available | Less than 10 minutes |
7/7 ✅ FULL SESSION
Proceed to Step 1 with all materials
5–6/7 ⚠️ MODIFIED SESSION
Reduce duration by 50%, use simplified version, skip movement break
<5/7 🛑 POSTPONE
Try calming protocol, reassess in 30 minutes. Note in data tracker.
Parent Affirmation: Postponing a session when the child isn't ready is not failure — it's skilled therapeutic judgment. Every experienced therapist makes this call. You just made it too.
Step 1 of 6 — The Invitation
⏱ 30–60 seconds
STEP 1 of 6
The Principle: Every protocol begins with an invitation, not a command. The child enters willingly or not at all. Offer, don't place — let the child engage voluntarily.
"Hey — I have something interesting for you. Want to see?" (Show the wobble cushion OR the fidget tool — whichever is the child's current preference.) "You can sit on this while we do your task. Try it — see how it feels."
Parent Body Language Guidance
- Kneel or sit at the child's eye level — not standing over
- Relaxed posture — no urgency or tension visible
- Genuine curiosity in voice — you are discovering this together
- Offer, don't place — voluntary engagement is essential
If the Child Resists
- Refuses verbally → "No problem, it's just here if you want it." Leave it visible. Try again next session.
- Walks away → Follow, use transition object, offer activity in a different location
- Throws the material → Stop, calm, return to Red Light protocol. Session postponed.
Step 2 of 6 — The Engagement
⏱ 1–3 minutes
STEP 2 of 6
The Principle: The child is now physically in position. This step introduces the full material setup and anchors the task. Sensory foundation comes first — always.
1
A. Sensory Foundation First
Place the lap pad on the child's lap: "How does that feel? Good weight?" Confirm wobble cushion position: "You can move a little — that's okay. Moving helps your brain focus." Offer fidget: "This is for your hands. Hold it while we work."
2
B. Time Anchor — Together
Set the visual timer WITH the child: "How many minutes do you think you can focus today? Let's try [X] minutes." Let the child turn the timer dial if capable. Shared ownership of the endpoint transforms compliance into agency.
3
C. Task Introduction
Place only the task materials on the desk. "We're going to [describe task simply]. When the timer goes — we stop. Done. Break time." The endpoint must be clear, concrete, and honored without exception.
Reinforcement Cue: When child picks up fidget AND looks at task: "That's exactly right. Hands working, eyes on the task. Perfect." Immediate, specific, warm — within 3 seconds of the behavior.

Step 3 of 6 — The Therapeutic Action
⏱ 5–15 minutes (core session)
STEP 3 of 6
The therapeutic action is sustained, material-supported, structured focus on a single task for a predetermined time window. The child works — puzzle, building kit, worksheet, reading — with all supports active and the parent present but non-intrusive.
Minimum Intervention Protocol: Do not speak unless the child initiates, the timer reaches the midpoint, or a safety issue arises. Your presence is regulatory — you are the safe anchor, not the activity director. If the child begins to drift, use a quiet proximity cue (move 30cm closer) before verbal prompting.
Common Execution Errors and Corrections
Duration of Therapeutic Exposure
- Week 1: Start at 50% of child's observed comfortable focus window
- Weeks 2–3: Add 1–2 minutes per successful session
- Target: Age-appropriate sustained focus window per developmental chart

Step 4 of 6 — Repeat & Vary
⏱ 3–5 minutes
STEP 4 of 6
Dosage Principle: 3 quality, child-engaged focus intervals > 10 forced, struggled-through attempts. The measure of a successful session is not duration — it is quality of engagement during the focus window.
When the timer sounds for a movement break: child and parent move to the designated break zone together for 3–5 minutes of physical activity — jumping jacks, animal walks, wall push-ups. A timer is set for the break too, so the break has a known endpoint. When it sounds: "Break done. Back to work."
Satiation Indicators — When the Child Has Had Enough
Engagement quality declining each interval (not improving with movement breaks)
Increased emotional affect around task materials
Fidget becoming disruptive — visual attention on fidget, not task
Physical agitation increasing despite movement breaks → End the session. Do not push through satiation.
Step 5 of 6 — Reinforce & Celebrate
⏱ Within 3 seconds of completion
STEP 5 of 6
The Reinforcement Principle: Timing matters more than magnitude. Immediate, specific, enthusiastic reinforcement delivered within 3 seconds of the desired behavior is neurologically more powerful than a large reward given 10 minutes later.
"You did it. You focused for [X] minutes. That was real focus. I saw you use the cushion AND keep your eyes on the task. That's what focus building looks like."
"You stayed even when it got hard. That's the important part. Your brain just got stronger."
Verbal Praise
Within 3 seconds of timer completion. Specific behavioral labeling — name exactly what the child did.
Physical
High-five, fist bump, hug if appropriate — immediately after the verbal praise.
Token/Sticker
Add to reward chart immediately in child's presence. The visual record matters enormously.
Tangible Reinforcer
Delivered within 60 seconds. Reward Jar (₹589) | 1800+ Reward Stickers (₹364)
Celebrate the Attempt, Not Just the Success: If the child completed only 60% of the session with 2 redirects — still reinforce: "You came back after the movement break. That took focus. That counts."
Step 6 of 6 — The Cool-Down
⏱ 2–3 minutes
STEP 6 of 6
The Principle: No session ends abruptly. Abrupt endings cause post-session dysregulation. The cool-down transitions the child from therapeutic engagement to baseline with dignity and predictability.
1
A. Transition Warning (30–60 seconds before cool-down)
"Two more. Then we're all done for today." Show on timer: "See — 2 minutes left." Predictability is the therapeutic agent here.
2
B. Material Put-Away Ritual
"Let's put the cushion back. Put the fidget in its spot." Child participation in put-away ritual transfers ownership and signals closure — the child ends the session with agency.
3
C. Cool-Down Activity (1–2 minutes)
One calming, low-demand activity: slow breathing (3 counts in, 5 out) × 3 | gentle wall push-ups × 5 | quiet preferred sensory activity | quiet sitting in a comfortable position for 60 seconds. NOT a high-stimulation reward.
4
D. Transition to Next Activity
"Session done. You can [next activity — specific, known]." Clear, predictable next step. No ambiguity. The timer is the neutral authority — not the parent.
Capture the Data — Right Now
60 seconds of data now saves hours of guessing later. Three fields only — observable, not subjective. Each session's data feeds into the GPT-OS® Attention & Focus Index.
Field | Record | |
Date | ___/___/___ | |
1. Focus Duration (actual, not planned) | ___ minutes on task without redirect | |
2. Redirections Needed | ___ times | |
3. Regulation Quality (Rate 1–5) | 1 Dysregulated | 2 Struggled | 3 Adequate | 4 Good | 5 Excellent |
Download PDF Tracker: Printable 4-week tracking sheet for L-986.
What GPT-OS® Does With This Data
After 7 sessions, the system generates an updated recommendation — whether to increase timer duration, introduce the next material, or escalate to professional assessment. This is not passive record-keeping. This is the feedback loop that makes the intervention adaptive.
GPT-OS® learns which materials show highest effectiveness for your child's specific age band and sensory profile — and adjusts the recommended pathway automatically.
ABA Data Collection Standards: Continuous measurement (frequency, duration, latency) and discontinuous measurement as standard practice. Cooper, Heron & Heward, Applied Behavior Analysis, 8th ed.
What If It Didn't Go as Planned? — 7 Most Common Problems
Most sessions don't go perfectly. Session abandonment is not failure — it's data. Here are the seven most common problems, their root causes, and precise fixes.
Child refused to sit at the desk at all
Why: Invitation experienced as demand. Pre-session anxiety or setup wasn't child-driven.
Fix: Begin next session with a 2-minute preferred activity at the desk. The desk must first become a neutral or positive space. Reduce all visible work materials.
Fix: Begin next session with a 2-minute preferred activity at the desk. The desk must first become a neutral or positive space. Reduce all visible work materials.
Child kept taking off the lap pad
Why: Incorrect weight, wrong texture, or child isn't in a proprioceptive-seeking state today.
Fix: Reduce weight. Try a different textile. Some days the sensory need isn't for pressure — try movement instead. Don't force it.
Fix: Reduce weight. Try a different textile. Some days the sensory need isn't for pressure — try movement instead. Don't force it.
The fidget became a toy — child stared at it
Why: The fidget is too visually interesting. Effective fidgets are boring to look at.
Fix: Switch to a simpler tactile fidget — smooth stone, hairband to stretch, Velcro stuck under the desk edge. The correct fidget disappears into the background.
Fix: Switch to a simpler tactile fidget — smooth stone, hairband to stretch, Velcro stuck under the desk edge. The correct fidget disappears into the background.
Movement break didn't help — child came back MORE dysregulated
Why: Movement break was too high-stimulation (exciting, activating) rather than organizing (rhythmic, heavy-work).
Fix: Redesign the break. Avoid exciting activities. Use organizing heavy work: wall push-ups, carrying heavy books, slow rhythmic bouncing, animal walks.
Fix: Redesign the break. Avoid exciting activities. Use organizing heavy work: wall push-ups, carrying heavy books, slow rhythmic bouncing, animal walks.
Child cried when the session ended
Why: Child was in flow (a good problem!) or session ending felt abrupt despite cool-down.
Fix: Honor the flow state — extend 2–3 minutes. Then ensure cool-down is longer and more predictable. Increase the transition warning window.
Fix: Honor the flow state — extend 2–3 minutes. Then ensure cool-down is longer and more predictable. Increase the transition warning window.
Child finished the timer and immediately demanded a screen
Why: This is actually success — the child honored the timer contract.
Fix: This is not a problem. Add 30 seconds of verbal celebration before screen access to ensure the behavioral connection is clear.
Fix: This is not a problem. Add 30 seconds of verbal celebration before screen access to ensure the behavioral connection is clear.
Nothing worked — child refused everything
Why: Wrong day. Environmental stressor. Physical state off. It happens.
Fix: Log as "Postpone — child not ready." Try tomorrow. Consistency over time matters more than any single session. Call 9100 181 181 if this is the pattern over 5+ consecutive sessions.
Fix: Log as "Postpone — child not ready." Try tomorrow. Consistency over time matters more than any single session. Call 9100 181 181 if this is the pattern over 5+ consecutive sessions.
Adapt & Personalize — No Two Children Are Identical
This is how you personalize the protocol for your child's unique sensory profile, age, and current capacity.
Level 1 — Easiest Start
2–3 min focus | 1 material | No formal task — preferred play activity only
Level 2
5 min focus | 2 materials | Simple single-step task
Level 3 — Standard Protocol
10 min focus | 3 materials | Graded task with checklist
Level 4
15 min focus | Full material set | Academic work
Level 5 — Advanced
20+ min focus | Full set | Complex multi-step academic work with self-monitoring
For the Sensory Seeker (needs MORE input)
- Increase wobble cushion use during all tasks
- Movement break every 10 minutes (not every 15–20)
- Heavier lap pad (toward upper limit of 10% body weight)
- Crunchy snack before session (jaw proprioception is organizing)
- Allow fidget AND movement simultaneously — both is fine
For the Sensory Avoider (overwhelmed by input)
- Skip wobble cushion — standard flat seating
- Lap pad lighter or no weight at all
- Minimal or no fidget
- Noise-reducing headphones are critical
- Workspace maximally bare — even less than the standard setup
- Movement break should be calm, not exciting
Bad Day Protocol: Run a Mini Session — 1 material, 3 minutes, preferred activity, immediate reinforcement. Maintain the habit without pushing the system.
Age-Based Modifications
The full protocol adapts meaningfully across the 3–12 age range. Match the demands to the developmental window — not to expectations.
Ages 3–5
- Sessions maximum 5 minutes
- Use only 1–2 materials
- Focus building activity = preferred play task (puzzle, building kit)
- Timer is a sand hourglass
- Checklist is 2–3 picture steps maximum
Ages 5–8
- Standard protocol — 10–15 minute sessions
- Full material toolkit
- Academic tasks are now appropriate
- Parent proximity active throughout
- Reinforcement delivered every interval
Ages 8–12
- Child can self-select materials and set the timer themselves
- Introduce self-monitoring: "How focused were you? Rate yourself 1–5."
- Fade parental presence gradually (30cm per session)
- Move toward independent protocol execution over 4–6 weeks
Week 1–2: What to Expect
Progress: ~15%
Tolerance & Introduction Phase
Week 1–2 is about tolerance and introduction — not mastery. The materials are new, the child is still calibrating, and the results aren't obvious yet. Your job this week is to show up consistently, not to achieve perfect sessions.
Child tolerates the weighted lap pad for 2+ minutes without actively removing it
Child sits on wobble cushion for at least one focus interval without complaint
Child accepts the visual timer as the session endpoint without arguing when it sounds
First successful focus interval completed — even if just 3 minutes
Parent completes 5+ sessions (consistency in this window is the only metric that matters)
What is NOT Progress Yet: Significant improvement in homework completion speed (weeks away) | Independent focus without parent proximity (not this phase) | Generalization to school (not this phase). You may also see increased limit-testing as the novel materials create novelty-seeking behavior temporarily.
Week 3–4: Consolidation Signs
Progress: ~40%
Neural Pathways Forming
The neural pathways are forming. Watch for these specific signs — most parents miss them because they're looking for dramatic change rather than subtle behavioral shifts.
Child Anticipates the Session
Gets the cushion out without being asked. This spontaneous material retrieval is evidence of internalized routine — a fundamental executive function milestone.
Timer Sounds and Child Asks for More Time
"Can I have 2 more minutes?" — they want to finish. This is the first emergence of intrinsic focus motivation. It is a major clinical indicator.
Child Protests the Movement Break Ending
They want to return to the task. This is the most significant early consolidation indicator of the entire 8-week protocol. Honor it.
Homework Time Reduces 10–20%
Fewer redirections needed. Teacher sends ONE fewer "distracted" note home. These are the real-world transfer indicators — the protocol is generalizing.
Parent Milestone: You may notice you're more confident in your decisions during sessions. That's real skill development — yours. You are becoming a clinical operator of this protocol.
Week 5–8: Mastery Indicators
Progress: ~75%
🏅 Mastery Badge Unlocking
Mastery isn't perfection. It's consistent, self-directed focus emerging in real-world conditions. These five criteria define mastery for the L-986 protocol.
1
Age-Appropriate Duration — 3 of 5 Sessions
Child sustains focus for age-appropriate duration in at least 3 out of 5 consecutive sessions without verbal redirection.
2
Self-Selects Materials
Child independently chooses at least 2 of the 9 materials before sessions begin — demonstrating internalized self-regulation awareness.
3
Self-Monitoring Language
"I need a break,""Can I use the wobble cushion?""How much time left?" — the child is now monitoring their own attention state.
4
Teacher Reports Improvement
Noted in at least one of: task completion, classroom attention, homework quality. The skills are generalizing beyond the home protocol.
5
30%+ Reduction in Parental Redirections
Parent-required redirections during homework have reduced by 30%+ from the Week 1 baseline — the most concrete measure of genuine progress.
When 4 of 5 mastery criteria are met consistently → Move to the next technique in the progression pathway or intensify with therapist guidance. If 2–3 criteria met → Extend to Week 9–12. Some children need a longer consolidation window — this is clinical wisdom, not failure.
You Did This. Your Child Grew Because of Your Commitment.
Over the past 5–8 weeks, you have shown up consistently when it was hard. You held the session structure even on difficult days. You gave your child's brain the sensory conditions it needed to access focus.
1
What You Built
- Learned to read your child's arousal state and respond rather than react
- Built a home environment that supports, rather than competes with, attention
- Created neural pathways that will compound for years
2
What Your Child Built
- The prefrontal cortex received structured input it will retain
- Internal regulation skills now emerging will develop further
- A history of successful task completion — the foundation of confidence
3
Family Celebration Prompt
Plan a celebration your child helped choose — their agency in celebrating their own growth is itself a focus and executive function exercise.
"Write or photograph: What is the ONE moment from these 8 weeks that showed me my child can focus? Keep this. Return to it on hard days."
Red Flags — When to Pause and Consult
Even in the success zone, these signs mean pause and consult. Trust your instincts. Early escalation is always better than delayed intervention.
Escalation Pathway: Self-resolve → Teleconsult (9100 181 181) → Nearest Pinnacle center visit → Formal multi-disciplinary assessment
1
🔴 No improvement after 12+ sessions
Data consistently shows regulation quality 1–2 for 12+ sessions with no upward trend. May indicate sensory processing disorder, ADHD, or anxiety requiring formal OT assessment. Call: 9100 181 181
2
🔴 Sessions consistently triggering meltdowns
More than 3 sessions in a row ending in severe emotional dysregulation. Technique or materials may be mismatched to the child's sensory profile. Stop and consult OT. Call: 9100 181 181
3
🔴 Self-injurious behavior appearing
Head-banging, biting, scratching during or following sessions. This is a clinical emergency requiring immediate professional review. Stop all home sessions immediately. Urgent: 9100 181 181
4
🔴 Sleep disruption worsening significantly
Child sleeping 2+ hours less than baseline since protocol began. Review session timing (avoid within 2 hours of bedtime). Consult developmental pediatrician.
5
🔴 School escalating to "cannot function in classroom"
School requesting formal assessment, IEP referral, or medication conversation. Request AbilityScore® assessment at nearest Pinnacle center. This is the appropriate next step.
6
🔴 Parent's own capacity is severely impaired
Parent experiencing burnout, depression, or relationship strain from the therapy burden. A burned-out parent cannot deliver an effective protocol. Pause home sessions and call. 9100 181 181
The Progression Pathway
Every technique is a waypoint, not a destination. Here is where you go from here — and how your child's response profile determines which path is right.
Path A — Strong Responder (4–5 criteria met)
Proceed to L-987: Self-Regulation — building the internal emotional regulation that makes focus sustainable. Simultaneously add L-988: Task Initiation — getting started independently.
Path B — Moderate Responder (2–3 criteria met)
Extend L-986 for 4 additional weeks with increased intensity. Add therapist-guided sessions at Pinnacle center. Consider formal ADHD evaluation via the red flag escalation pathway.
Path C — Sensory Seeker Profile
Before progressing, deepen sensory regulation foundation. Consider Domain A sensory techniques as parallel protocol running alongside L-986 extension.
Long-Term Developmental Goal: The attention system built through L-986 is the prerequisite foundation for academic reading comprehension, mathematical reasoning, peer conversation, classroom participation, and independent daily living skills. This is not a homework technique. This is brain infrastructure.
Related Techniques in This Domain
You already understand this domain. The materials you've gathered are the foundation for four related techniques — you've already built the library.
Technique | Domain | Difficulty | Canon Materials | |
L-985: Working Memory Building | Attention & Exec Function | ⭐⭐ | Problem-Solving Toys, Visual Supports | |
L-984: Impulse Control Techniques | Attention & Exec Function | ⭐⭐ | Reinforcement Menus, Timers | |
L-987: Self-Regulation Materials | Attention & Exec Function | ⭐⭐⭐ | Full sensory toolkit | |
L-988: Task Initiation Strategies | Attention & Exec Function | ⭐⭐ | Checklists, Visual Supports | |
G-661: Attention Skills | Domain G | ⭐ | Basic engagement materials | |
G-662: Focus & Concentration | Domain G | ⭐⭐ | Focus materials set |
✅ You Already Own Materials For These: The weighted lap pad, visual timer, fidget tools, and checklist system from this protocol are the primary materials for L-985, L-987, and L-988. You have already built the material library for 4 related techniques.
All above techniques fall within: Attention, Self-Regulation & Executive Function — the highest-leverage developmental domain for school readiness and daily living skills.

Your Child's Full Developmental Map
Focus building is one piece of a larger developmental picture. GPT-OS® tracks your child's profile across all 12 domains simultaneously — ensuring no developmental need goes unnoticed.
Domain A — Sensory Processing
Sensory regulation is the precondition for attention — often co-active with L-986
Domain B/C — Communication / Emotional Regulation
Regulated attention enables both language and emotional control — bidirectional relationship
Domain D — Behavior & Flexibility
Attention difficulties frequently co-occur with behavioral rigidity — parallel intervention often indicated
→ See Your Child's Full AbilityScore® Profile: Request assessment at 9100 181 181 or pinnacleblooms.org/abilityscore
Families Who've Been Here
These families started exactly where you are right now. All outcomes are illustrative; individual results vary based on child profile, protocol consistency, and co-occurring conditions.
Arjun, 7 — Hyderabad
Before (Week 0): Homework took 2–3 hours daily with constant parental redirection. Teacher sent weekly notes: "not attending." School was recommending ADHD assessment and potentially medication.
After (Week 8): Three 15-minute focused intervals with 5-minute movement breaks. Same total homework time — completely different experience. Arjun rates his own focus 4/5 most days. Teacher sent a note this week — to say she noticed improvement. No medication initiated.
"The weighted cushion and the timer changed everything. He needed to know when it would end. Once he could see that, he could start."
Priya, 5 — Bengaluru
Before: Couldn't complete a 5-piece puzzle without walking away. Play dates frequently ended with her lying on the floor, refusing to participate. Parents felt helpless — not understanding the sensory need beneath the behavior.
After: Completes 24-piece puzzles independently. Play date duration extended by 12 minutes on average. Used the fidget tool spontaneously during a school class photo — seated waiting — and her teacher was impressed.
"I thought she was just a 'fidgety child.' Now I understand she was seeking input her nervous system needed. Giving it to her — not fighting it — made all the difference."
From the Therapist's Notes: This is the most common focus intervention success pattern — time perception support + sensory regulation + movement breaks = sustainable homework engagement.
Connect With Other Parents
Isolation is the enemy of adherence. You don't have to navigate this alone — and the parent two months ahead of you has the exact practical wisdom you need right now.
🟢 Focus Building Parent WhatsApp Group
Challenge-specific peer group for families implementing L-986 and related attention techniques. Share data, ask questions, celebrate wins.
Join the group →
Join the group →
💬 Online Forum — Attention & Executive Function
Moderated by Pinnacle clinicians. Parent-sourced questions, therapist responses, weekly focus-building challenges.
Access forum →
Access forum →
📍 Local Parent Meetups
Pinnacle centers host monthly parent peer sessions. Find your nearest: 9100 181 181 or Center Locator →
🤝 Peer Mentoring
Connect with an experienced parent — 3+ months into the attention program — who can share what worked. Request a mentor: care@pinnacleblooms.org
Community Invitation: Your experience helps others. If you're 8 weeks in and seeing results — consider sharing your journey. The parent you help by sharing might be exactly where you were on Week 1.
Your Professional Support Team
Home + clinic = maximum impact. Professional guidance multiplies home-based gains. If you're in a Pinnacle city, center-based assessment accelerates home protocol outcomes by an average of 40%.
What a Pinnacle OT Does for Focus Building
- Conducts formal sensory processing assessment (determines seeker vs. avoider profile)
- Calibrates weighted material to precise body weight and sensory need
- Designs individualized protocol within GPT-OS® framework
- Coordinates with school — teacher training and classroom accommodation letters
- Monitors AbilityScore® Attention Index and adjusts intervention intensity
70+ Center Network
Pinnacle centers operating across India. Outside India: Teleconsultation is the pathway. Insurance/funding: sensory integration OT services may be covered. Call 9100 181 181 for eligibility check.
Book a Consultation
Primary Discipline for L-986: Occupational Therapy — sensory profile assessment, weighted material calibration, workspace setup consultation, and attention protocol design.
📞 9100 181 181
Available 24×7 | 16+ languages | FREE initial consultation
The Research Library
Deeper reading for the curious parent and the clinical professional. Every recommendation on this page has a source — graded by the Oxford Centre for Evidence-Based Medicine levels.
Level I — PRISMA Systematic Review (2024) | PMC11506176
"16 studies (2013–2023) confirm sensory integration intervention is evidence-based practice for children with ASD and attention difficulties." Significant effect sizes for sustained attention duration, task completion rates, and caregiver-reported redirection frequency. PubMed →
Level I — Meta-Analysis, World J Clinical Cases (2024) | PMC10955541
"Sensory integration therapy across 24 studies effectively promotes social skills, adaptive behavior, sensory processing, and motor development."PubMed → | DOI: 10.12998/wjcc.v12.i7.1260
Level II — WHO Care for Child Development Package (2023) | PMC9978394
"Household-based, caregiver-administered interventions demonstrate efficacy in 54 LMICs. Parent training is the highest-leverage pediatric development investment."WHO Publication →
Level II RCT — Padmanabha et al. (2019) | Indian J Pediatr
"Home-based sensory intervention programs with parent administration showed statistically significant improvement in attention-related behaviors." DOI: 10.1007/s12098-018-2747-4
Clinical Consensus — NCAEP Evidence-Based Practices Report (2020)
"Visual supports, video modeling, and structured environmental arrangements are classified as evidence-based practices for autism and attention difficulties."NCAEP Report →
Additional resources: CHADD (chadd.org) | AOTA Sensory Integration Practice Guidelines | Harvard Center on the Developing Child — executive function research | ADDitude Magazine
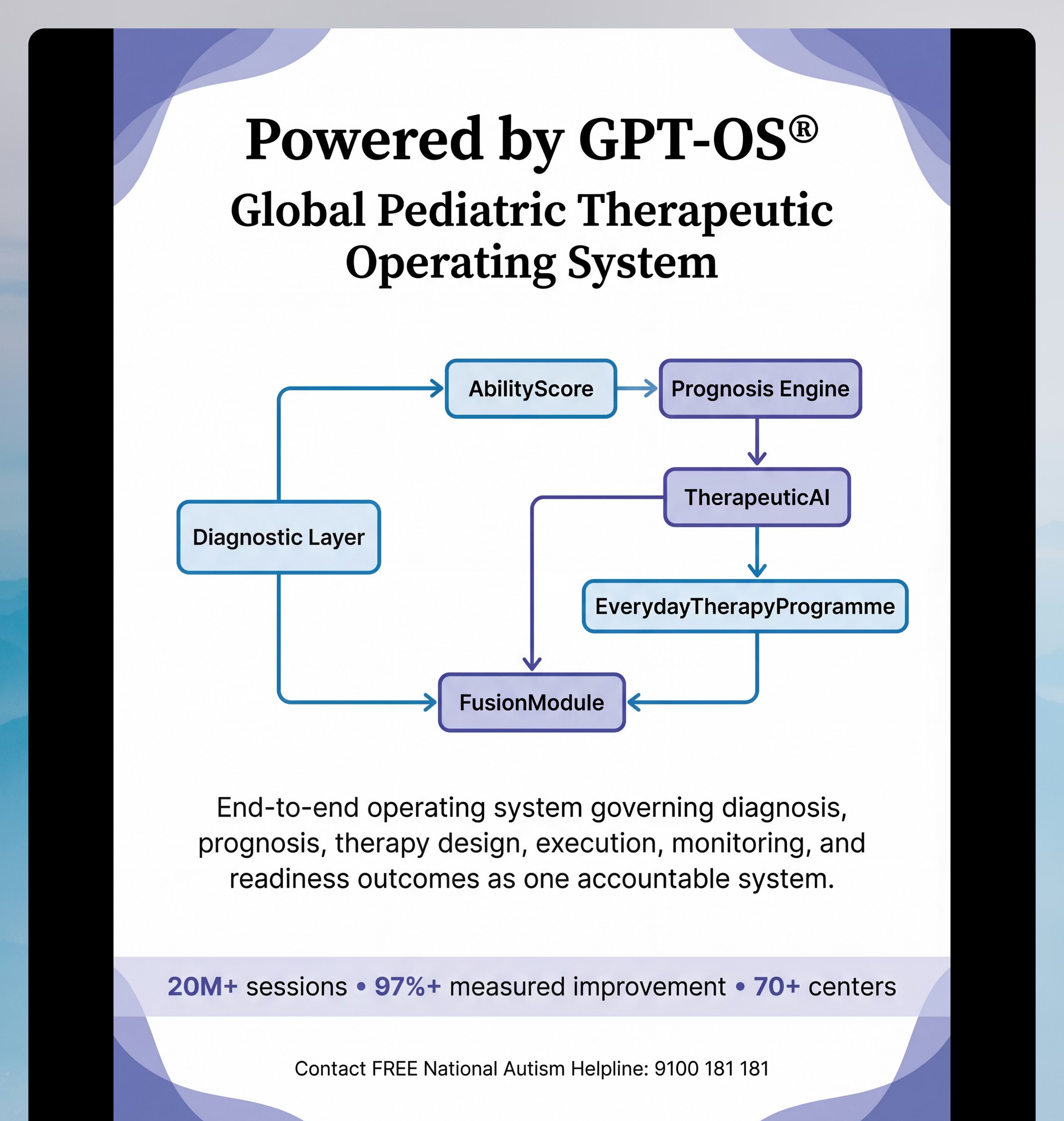
How GPT-OS® Uses Your Data
Your data doesn't disappear. It drives personalized recommendations for your child — and improves the system for every child in the 20M+ session network.
What GPT-OS® Learns From L-986 Data
- Which focus duration thresholds are achievable by age band and sensory profile
- Which of the 9 materials show highest effectiveness correlation with focus outcomes
- Optimal movement break timing for different regulation profiles
- Which material combinations produce fastest progression (e.g., weighted pad + timer is more effective than timer alone)
- When the protocol should escalate to clinical assessment vs. continue home protocol
Privacy and Data Protection
- All data anonymized at individual level before population analysis
- Individual family data accessible only to family and assigned Pinnacle therapist
- No data shared with third parties
- Data protection under Indian IT Act and Pinnacle's privacy framework
"Your data helps every child like yours." The 20M+ sessions that power GPT-OS® came from families who chose to contribute. Every session logged makes the system better for the next family who arrives where you are today.
Preview of 9 materials that help with focus building Therapy Material
Below is a visual preview of 9 materials that help with focus building therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
Frequently Asked Questions
Questions parents ask at Pinnacle centers and in our community — answered with clinical clarity and parental empathy.
Q: My child focuses on video games for hours. Does he really have an attention problem?
Yes, and this is the most common question we receive. The ability to hyperfocus on high-stimulation, high-interest activities is characteristic of ADHD and attention differences — not evidence against them. The brain's dopamine system activates powerfully for video games and cannot replicate that for homework. This is not a choice — it is a wiring difference. The intervention is to build the scaffolding that makes focus accessible in lower-stimulation contexts.
Q: How long before I see results?
Most families notice the first signs of change (tolerance of materials, reduced session resistance, 1–2 fewer redirections) by Week 2–3. Meaningful focus improvement in homework time typically emerges by Week 4–6. Generalization to school settings: Week 6–10. These are averages — individual profiles vary significantly.
Q: Do I need all 9 materials or can I start with fewer?
Start with 3: weighted lap pad (or DIY equivalent), visual timer, and one fidget tool. These three address the most common underlying mechanisms. Add materials as you observe what your child responds to. The full toolkit is an ecosystem, not a prescription.
Q: My child's school says he needs medication. Should I try this protocol first?
This is a clinical decision requiring formal ADHD evaluation by a developmental pediatrician — not one that should be made by the school, by you, or by this web page. For many children, appropriate sensory support and structured attention training significantly reduces functional difficulties. For others, medication is clinically appropriate and works best when combined with non-pharmacological interventions. Get the formal evaluation: 9100 181 181