
The Lights Flicker. Everyone Else Is Fine. Your Child Is in Pain.
Your daughter can't go anywhere with fluorescent lights. Grocery stores, shopping malls, her own classroom — the overhead lights flicker in a way that most people don't even notice, but she notices instantly. Within minutes, she's covering her eyes, complaining of headaches, becoming irritable and increasingly dysregulated.
Birthday parties are impossible. The moment someone turns on flashing decorations or a strobe effect, she's in tears — hands clamped over her eyes, begging to leave. Even certain screens trigger her. You've tried sunglasses. They just make everything darker — they don't stop the flashing sensation.
You are not failing. Your child's visual nervous system is perceiving light frequencies that most people unconsciously filter out. This is a neurological wiring difference — not a behaviour problem, not drama, not avoidance.
This intervention protocol — Environmental Modification for Flashing Light Sensitivity — gives you 9 evidence-based materials to protect your child, adapt their environments, and preserve their participation in life.
Sensory Solutions Series — Episode 66
Pinnacle Blooms Network® Consortium — Clinical Research Organisation • Speech-Language Pathology • Occupational Therapy • Applied Behaviour Analysis • Special Education • NeuroDevelopmental Paediatrics

ACT I — THE EMOTIONAL ENTRY
You Are Not Alone: The Numbers
These statistics represent millions of real families navigating the exact challenge you face. The flicker your child perceives is real. The pain is real. And evidence-based solutions exist.
80%
Visual Hypersensitivity in Autism
of children diagnosed with autism spectrum conditions experience sensory processing difficulties, with visual hypersensitivity among the most functionally limiting presentations.
Source: PRISMA Systematic Review (2024) — PMC11506176
5–20%
Photosensitive Migraine Rate
of migraine patients demonstrate photosensitive responses to fluorescent lighting at 50–60Hz — significantly higher in neurodivergent populations where sensory gating mechanisms differ.
Source: American Migraine Foundation; Epilepsy Foundation photosensitivity guidelines
18M+
Families in India Alone
families in India are navigating sensory processing challenges in their children — many without a name for what their child experiences, without tools, without support.
Source: WHO Global prevalence data + India Census extrapolation via Pinnacle GPT-OS® Diagnostic Intelligence
References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | WHO Nurturing Care Framework (2018)

What's Happening in Your Child's Brain
The Neuroscience: Critical Flicker Fusion Threshold (CFF)
Every human visual system has a threshold — the frequency at which flickering light appears continuous. For most people, fluorescent lights flickering at 50–60Hz appear as steady, constant illumination because their CFF smooths the oscillations into perceived continuity.
Your child's CFF threshold is different. Their visual processing pathway — running from the retinal ganglion cells through the lateral geniculate nucleus to the primary visual cortex — maintains temporal resolution at frequencies that should be filtered. Each flicker is individually perceived. The result is a conscious, aversive strobe experience in environments that appear perfectly normal to everyone else.
What This Means for Your Child
Fluorescent lights don't produce steady light. They turn on and off 50–60 times per second as the electrical current alternates. Most brains smooth this into continuous light. Your child's brain does not.
Every flicker reaches conscious perception. Every flicker is processed as a distinct light event. The visual cortex is being bombarded with temporal information it cannot suppress.
This is a wiring difference, not a behaviour choice. When your child covers their eyes, complains of headaches, or begs to leave — they are responding to genuine neurological input that you cannot see but they cannot ignore.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660

Where This Sits in Development
Understanding where your child sits on the developmental timeline helps you set realistic expectations and interpret what you're observing.
1
Birth–6 Months
Visual system undergoes rapid maturation. Pupillary light reflex establishes. Flicker sensitivity patterns may already be present but not yet observable as distress behaviours.
2
6–18 Months
Visual cortex begins integrating temporal light information. Early signs may include turning away from certain light sources or unusual visual fixation patterns.
3
⚡ 18–36 Months
Common Emergence Window. Flicker sensitivity becomes functionally apparent as the child enters diverse environments with fluorescent and variable lighting.
4
3–7 Years
Peak functional impact. School attendance, social participation, and community access directly affected. Comorbid headaches and nausea may emerge.
5
7–12 Years
Self-awareness develops. The child recognises and communicates their triggers. Self-advocacy skills become possible. Environmental management becomes more effective with child participation.
Co-occurring patterns commonly observed: Auditory hypersensitivity, tactile defensiveness, migraine-type headaches, vestibular sensitivity, anxiety in unpredictable environments.
References: WHO Care for Child Development (CCD) Package — PMC9978394 | UNICEF MICS indicators | WHO/UNICEF CCD Package (2023)
The Evidence Behind This Technique
Evidence Grade: Level II
Systematic Reviews + Clinical Consensus
Sensory integration intervention — including environmental modification and protective filtering strategies — meets criteria to be classified as an evidence-based practice for children with autism spectrum conditions and sensory processing differences.
Clinically validated. Home-applicable. Parent-proven. This technique has been reviewed and validated by the Pinnacle Blooms Consortium comprising CRO scientists, occupational therapists, speech-language pathologists, BCBAs, special educators, and neurodevelopmental paediatricians.

ACT II — THE KNOWLEDGE TRANSFER
The Technique: What It Is
Environmental Modification Protocol for Flashing Light Sensitivity
Parent-Friendly Name: "Light Protection Toolkit"
This is a multi-material environmental modification and personal protection protocol designed to reduce, filter, block, or eliminate flashing and flickering light stimuli that cause pain, distress, and functional impairment in children with photosensitivity and flicker sensitivity.
Unlike single-material interventions, this protocol deploys 9 complementary materials across 8 functional categories — from personal wearable protection (filtering glasses) through environmental modification (flicker-free lighting, window films) to recovery systems (dark space materials) and community navigation tools (advocacy cards, warning systems). One material category (gradual exposure) requires professional guidance.
The protocol follows a protection-first philosophy: protect the child from harmful stimuli, then adapt environments to reduce triggers, then — only when appropriate and under professional guidance — build tolerance gradually. The child's comfort and safety are paramount at every stage.
1
Domain
Sensory Processing / Visual System / Light Sensitivity
2
Age Range
3–12 years
3
Setting
Home + School + Community
4
Budget
₹100–₹15,000
Canon Material Link:Sunglasses / Light Filtering / Visual Sensory | Reel ID: A-066 — Sensory Solutions Series, Episode 66
Who Uses This Technique
This technique crosses therapy boundaries because the brain doesn't organise by therapy type.
Occupational Therapist (Primary Lead)
OTs lead sensory integration assessment and environmental modification planning. They evaluate the child's specific flicker sensitivity profile, recommend appropriate filtering tools, design recovery space protocols, and guide gradual exposure when clinically appropriate. The OT maps the child's sensory processing profile within the Pinnacle Sensory Integration Assessment framework.
NeuroDevelopmental Paediatrician / Neurologist
Medical evaluation is essential when flicker sensitivity presents with headache patterns suggesting migraine, or any indicators of photosensitive epilepsy. The neurologist determines seizure risk, guides medical management, and clears the child for exposure-based interventions. Medical coordination is mandatory for this technique.
Board Certified Behaviour Analyst (BCBA)
ABA principles guide the self-advocacy training, warning system implementation, and behavioural data collection. The BCBA designs reinforcement systems for the child's use of protective tools, develops self-monitoring protocols, and structures the functional behaviour assessment when avoidance behaviours become complex.
Special Educator
School-based environmental modification requires special education expertise. The SpEd coordinates classroom lighting accommodations, develops school-specific advocacy plans, and ensures the child's educational access is maintained through environmental adaptation rather than exclusion.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) — DOI: 10.1080/17549507.2022.2141327
What This Targets
🎯 Primary Target
Visual Sensory Tolerance — Increase the child's capacity to function in environments with variable lighting through protective tools and environmental modification.
Observable indicator: Duration of comfortable participation in fluorescent-lit environments increases week-over-week.
🎯 Secondary Targets
- Environmental navigation — the child learns to identify, prepare for, and manage triggering light environments
- Self-advocacy skills — the child communicates sensory needs to adults and peers confidently
- Recovery self-regulation — the child recognises early signs of visual overwhelm and independently accesses recovery strategies
- Anxiety reduction — anticipatory anxiety decreases as the child gains reliable protective tools
🎯 Tertiary Developmental Targets
- Social participation — parties, events, assemblies, community activities
- Academic performance — sustained attention in classroom environments
- Emotional regulation — overall regulatory capacity improves
- Family quality of life — fewer cancellations, expanded activity options
Reference: Meta-analysis (World J Clin Cases, 2024) — PMC10955541 | Sensory integration therapy across 24 studies

What You Need: Primary Materials (1–5)
Complete Materials List — Part 1 of 2
1
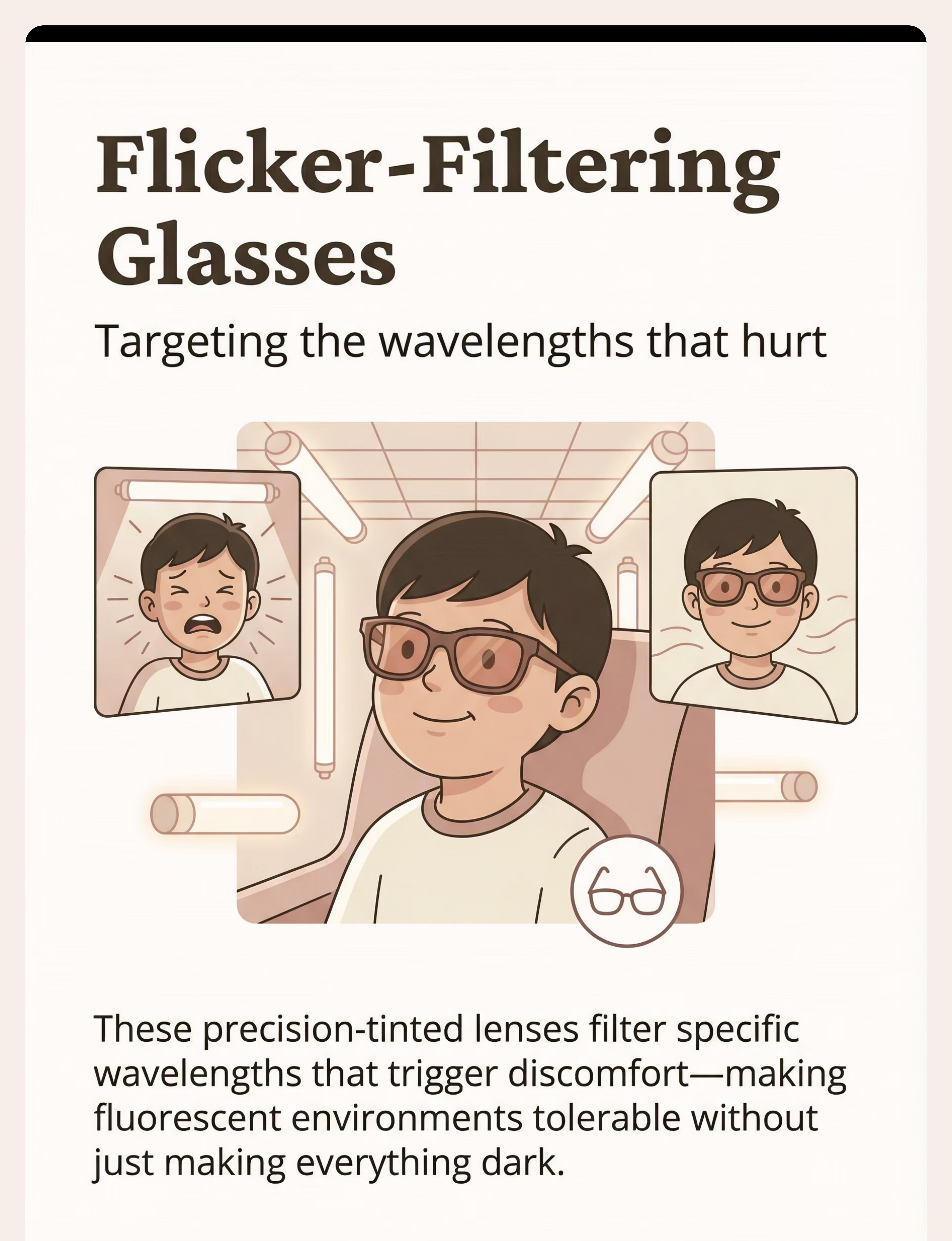
Flicker-Filtering Glasses (FL-41 Tinted Lenses)
Category: Sunglasses / Light Filtering / Visual Sensory | Price: ₹2,000–₹15,000
Includes: FL-41 or TheraSpecs-style precision-tinted lenses, amber/rose-tinted options, blue-light filtering glasses, clip-on tinted lenses, child-friendly frames.
2
Flicker-Free LED / Incandescent Lighting
Category: Environmental Modification / Lighting | Price: ₹300–₹2,000 per bulb
Includes: Incandescent bulbs, high-frequency flicker-free LEDs, DC-powered LEDs, warm-temperature (2700K–3000K) options, dimmable options.
3
Light-Filtering Window Films
Category: Environmental Modification / Visual | Price: ₹500–₹3,000 per window
Includes: Light-reducing films, UV/blue-light blocking films, anti-glare diffusing films, removable static-cling options.
4
Portable Light Shields and Screens
Category: Portable Sensory Tools | Price: ₹500–₹3,000
Includes: Desk-mounted overhead shields, portable folding screens, wide-brimmed hats, hood attachments, adjustable shielded desk lamps, DIY cardboard/foam-board shields.
5
Screen Modification Tools
Category: Digital Access / Sensory Adaptation | Price: Free–₹3,000
Includes: Blue-light filtering screen protectors, matte anti-glare films, f.lux/Iris software, built-in Night Shift/Night Light, high-refresh-rate monitors (120Hz+).

What You Need: Primary Materials (6–9)
Complete Materials List — Part 2 of 2
1
Recovery Space Materials
Category: Sensory Regulation Tools / Calming | Price: ₹300–₹2,000
Includes: Blackout curtains or pop-up dark tent, child-sized eye masks, cooling eye compresses, battery-operated candles/fairy lights, noise-cancelling headphones.
2
Advocacy Cards and Communication Tools
Category: Communication / Self-Advocacy | Price: ₹100–₹500
Includes: Laminated advocacy cards, medical alert-style bracelets, self-advocacy scripts, QR code links, teacher communication templates.
3
Predictability and Warning Systems
Category: Transition / Preparation Tools | Price: Free–₹500
Includes: Venue preview protocols, photosensitivity content databases, family code words, exit strategy planning.
4
⚠️ Gradual Exposure Tools — PROFESSIONAL GUIDANCE REQUIRED
Category: Therapeutic Equipment — Clinical Grade | Price: ₹1,000–₹5,000
Includes: Adjustable/controllable light sources, dimmer switches, colour-changing LEDs, timer systems, child-controlled stop mechanism.
This material REQUIRES occupational therapy supervision. Not for DIY use.
Total Investment Range: ₹100–₹15,000 | Essential Starters: Items 1 (glasses) + 2 (home lighting) — highest immediate impact

DIY and Substitute Options
Every parent can start today — regardless of budget. This is the WHO/UNICEF inclusion principle in action.
Buy This → DIY First Step
Flicker-Filtering Glasses: Before investing in prescription FL-41 lenses, try commercially available amber or rose-tinted glasses. Blue-light blocking glasses (₹200–₹800) may reduce screen-triggered symptoms. Try before committing to ₹10,000+ specialty lenses.
Window Films: Temporarily hang a thin white cotton sheet or muslin cloth over windows that receive harsh direct light. This diffuses and softens incoming light. Upgrade to proper films when ready.
Recovery Space: A blanket draped over two chairs creates a dark recovery tent. A folded damp cloth from the refrigerator serves as a cooling eye compress. A soft cotton scarf tied gently makes an eye mask.
Advocacy Cards: Write on a card: "I have photosensitivity. Flickering lights cause pain and headaches. I may need to wear tinted glasses or move away from certain lighting. Thank you for understanding." Laminate with clear tape.
Make This → Household DIY
Flicker-Free Lighting: Switch the child's bedroom and study desk to incandescent bulbs (₹30–₹80). Incandescent light has zero flicker. Use as reading/study lamps while transitioning to quality flicker-free LEDs.
Portable Shields: Cut an L-shaped barrier from cardboard or thermocol/foam board — position on the desk between the child and overhead fluorescent lights. A wide-brimmed hat or baseball cap blocks overhead light immediately.
Screen Tools — Completely Free: Enable built-in Night Shift (iOS), Night Light (Windows), or Night Mode (Android) immediately. Install f.lux (free software) on computers. Reduce screen brightness to minimum comfortable level.
Warning Systems — Completely Free: Call venues before visiting and ask about lighting type. Use "Does the Dog Die?" website for movie photosensitivity warnings. Create a family code word that means "I need to leave now."
⚠️NON-NEGOTIABLE — Gradual Exposure: No DIY substitute exists. This MUST be professionally supervised. Do not attempt exposure-based desensitisation at home without occupational therapy guidance.
Reference: WHO Nurturing Care Framework (2018) — equity-focused interventions | PMC9978394 | CCD Package across 54 LMICs

Safety First: Before You Begin
1
🔴 RED LINE — Stop and Seek Medical Evaluation If:
- Your child has ANY history of seizures or suspected seizure activity
- The child experiences loss of consciousness or unusual eye/body movements during light exposure
- Headaches are severe, persistent, or accompanied by visual aura, vomiting, or confusion
- The child reports visual phenomena (flashing shapes, zigzag lines) that persist after the light source is removed
- There is any family history of photosensitive epilepsy
These signs may indicate photosensitive epilepsy or migraine disorder requiring neurological evaluation. Call Pinnacle's FREE National Autism Helpline: 9100 181 181.
2
🟡 Caution — Modify Your Approach If:
- The child is currently experiencing a headache or migraine episode (wait for recovery)
- The child is in a state of high dysregulation from other triggers
- The child is ill, fatigued, or sleep-deprived (sensitivity is amplified when depleted)
- You are in an environment you cannot control (deploy portable protection only)
3
🟢 Proceed When:
- Medical clearance obtained (for children with any seizure or migraine history)
- Child is in a regulated baseline state
- Materials have been tested in a low-stakes environment first
- Recovery space is accessible
Contraindications — Never Do These:
- Never force a child to remain in triggering light environments to "toughen them up" — this causes genuine harm, pain escalation, and in susceptible individuals, seizures
- Never attempt gradual exposure without professional occupational therapy guidance
- Never tell the child the lights are fine or they are overreacting — this invalidates their genuine neurological experience and damages trust
- Never remove the child's protective tools as punishment or to "make them normal"
Reference: Indian Journal of Paediatrics RCT (2019) — DOI: 10.1007/s12098-018-2747-4 | Home-based sensory intervention safety protocols

Set Up Your Space
1
Zone 1 — The Child's Room / Study Area (Primary Safe Zone)
Replace ALL fluorescent lighting with flicker-free LED or incandescent bulbs. Apply window films to reduce glare. Position the desk lamp to the side (never overhead). Keep FL-41 glasses on a dedicated hook near the door — the child grabs them before leaving the safe zone.
2
Zone 2 — The Recovery Corner
Designate a specific corner with blackout curtains or a pop-up dark tent. Stock: eye mask, cooling compress (keep one in the refrigerator), battery-operated dim light, comfortable cushion or beanbag. The child must know this space exists and that using it is encouraged, never shameful.
3
Zone 3 — The "Go Bag" (Portable Protection Kit)
Prepare a small pouch for the school bag and a family outing bag containing: FL-41 glasses, portable desk shield (folding cardboard), wide-brimmed hat, advocacy cards, the family code word card, cooling eye compress in a ziplock.
4
Zone 4 — Digital Stations
On every screen the child uses: activate Night Shift/Night Light mode, install f.lux, apply matte anti-glare protector, set brightness to 40–60%, increase refresh rate to maximum available.
Environmental Checklist:✅ Home lighting converted ✅ Recovery space set up ✅ Go Bag packed ✅ Screens modified ✅ Family code word established ✅ School communication sent
Reference: Sensory Integration Theory (Ayres) — Environmental setup as core principle | PMC10955541

ACT III — THE EXECUTION
Is Your Child Ready? Readiness Check
This protocol is not a single therapy session — it's an environmental and protective system you are deploying across your child's life. However, each new material introduction should follow this readiness check.
Is the child in a regulated state?
Not mid-meltdown, not headache, not fatigued
Has the child eaten recently?
Sensory sensitivity amplifies on an empty stomach
Is the child in a familiar, comfortable environment?
Introduce new tools at home first
Is the child willing?
Invite, never force — "I have something that might help with the lights"
Do you have the recovery space ready?
In case the child needs to decompress after introduction
Is this a low-stakes time?
Not before school, not before an event — give time to adjust
🟢 All Yes → Proceed
Move to material introduction (Step 1)
🟡 Some No → Modify
Introduce as passive observation — no pressure
🔴 Child Distressed → Postpone
Provide comfort, access recovery space, try another day
The best intervention is one that starts with a willing child.

Step 1: The Invitation
Step 1 of 6
Introduce the material through invitation, not instruction. Every protection tool begins with the child's buy-in. For photosensitive children, trust is especially important — they've been told "the lights are fine" so many times that they may not believe you're offering real help.
Script for Flicker-Filtering Glasses (highest-impact material):"I learned something about those lights that bother you. You know how you can see them flickering and nobody else seems to notice? That's because your eyes are really good at seeing things other people miss. These special glasses were made to stop the flickering part of the light from reaching your eyes. They don't make everything dark — they just filter out the part that hurts. Want to try them on, just here at home first?"
What Acceptance Looks Like
- Child reaches for the glasses
- Child asks questions about how they work
- Child puts them on even briefly
- Child looks around the room with curiosity
What Resistance Looks Like — and How to Respond
- "Those look weird" → "That's okay. They come in different styles. Want to pick your own frame?"
- "They won't work" → "You might be right. But can we test them for 30 seconds? You decide if they help."
- Complete refusal → "No problem. They'll be here when you're ready." Place on the hook. Do not push.
Timing: 30–60 seconds. Brief. Low pressure. Child in control.
Reference: ABA Pairing Procedures — establishing motivating operations before demand | OT "Just-Right Challenge" principle

Step 2: The Engagement
Step 2 of 6
First Controlled Exposure Test. Once the child has voluntarily tried the protective tool (glasses, hat, shield), create a brief, controlled test environment.
For FL-41 Glasses Test:"Let's go into the kitchen [or any room with fluorescent/problematic lighting] for just 30 seconds with your new glasses on. I'm going to time it on my phone. If it feels bad at any point, we stop immediately. You're in charge."
How to Present the Test
- Keep it brief: 30 seconds to start
- Stay with the child — do not leave them alone in the test environment
- Hold the timer visibly — the child sees the countdown
- Have recovery space accessible within 10 seconds' walk
1
✅ Engagement
"This is actually okay!" / Looks around without squinting / Asks to stay longer → Extend to 60 seconds
2
⚡ Tolerance
"It's a little better" / Still squinting but not distressed → Note partial response, keep at 30 seconds
3
🛑 Avoidance
Eyes close, covers face, moves toward exit → Stop immediately. Validate: "Thank you for trying. We'll find something that works better."
Reinforcement cue — Praise the attempt, not the duration:"You just spent 30 seconds in that room with those lights and you did great. That took courage."
Timing: 1–3 minutes total including preparation and debrief.
Reference: PMC11506176 — Sensory integration intervention with structured material introduction

Step 3: The Therapeutic Action
Step 3 of 6
Systematic Deployment Across Environments. This is not a single activity — it's a systematic rollout of protection across your child's daily life. Implement in this order (easiest wins first).
Week 1: Home Base — You Control Everything
Replace lighting in child's room and study area with flicker-free alternatives. Apply window films. Set up recovery corner. Configure all screens with filtering software. Establish the "go bag" with portable tools.
Week 2: School — Requires Coordination
Send advocacy card/letter to class teacher. Request fluorescent modification above child's desk. Provide portable desk shield for classroom use. Ensure school has a designated recovery space. Brief the child on using the family code word with the teacher.
Week 3: Community Expansion
Begin using warning/preview systems for outings. Practice the code word system at a low-stakes outing (library, quiet store). Deploy full go bag for community activities. Test glasses in progressively more challenging lighting environments.
Week 4+: Full Integration
The protective system is in place. The child has tools for every context. Monitor, adjust, and celebrate participation wins. Begin professional consultation about gradual exposure (if appropriate).
Core Therapeutic Principle: Protection first, adaptation second, exposure only under guidance.
Reference: PMC10955541 — Meta-analysis confirming structured environmental modification efficacy

Step 4: Repeat and Vary
Step 4 of 6
Test Each Material in Multiple Contexts. Therapeutic generalisation requires each material to be tested across varied environments. A tool that works at home may need adjustment for school or community settings.
For Each of the 9 Materials, Test In:
1
Home
Controlled, lowest stress — always start here
2
Familiar Community
Grocery store, temple, relative's house
3
School / Classroom
With teacher coordination and desk modifications
4
Social Event
Birthday party, family gathering, celebration
5
Novel Environment
New restaurant, mall, cinema
Variation Protocol
- If glasses work in fluorescent lighting, test in dappled sunlight, against LED screens, at a celebration with decorative lights
- If the desk shield works in the classroom, test a portable version for the library, for tutoring sessions, for exam halls
- If the warning system works for planned outings, practise rapid deployment for unexpected encounters
Satiation indicator: If the child spontaneously reaches for their protective tool before you remind them — the material has been internalised. That's a win.
Key principle: 3 successful experiences in a new context > 10 forced exposures. Let the child accumulate positive experiences with their tools. Confidence builds protection capacity.
Key principle: 3 successful experiences in a new context > 10 forced exposures. Let the child accumulate positive experiences with their tools. Confidence builds protection capacity.

Step 5: Reinforce and Celebrate
Step 5 of 6
Use reinforcement within 3 seconds of the desired behaviour.
1
"You put on your glasses before we walked into the store — that was smart. You know what helps you and you used it. I'm proud of that."
2
"You used the code word at the party and we left calmly. That was excellent communication."
3
"You asked the teacher about the lights before the assembly. That's real self-advocacy."
What to Reinforce ✅
- Independently reaching for protective tools
- Communicating sensory needs to adults or peers
- Using the recovery space without shame
- Planning ahead (asking about lighting at a venue)
- Tolerating a brief exposure and then self-managing recovery
What NOT to Reinforce ❌
Enduring pain ("You're so brave for staying even though it hurt") — this teaches the child to ignore their own distress signals. Never reinforce suffering. Reinforce management.
Celebration Ideas
- A "lighting victories" chart — each successful outing gets a sticker
- The child names their glasses ("my magic glasses")
- Share the win with the family: "Priya went to Diya's birthday party today AND stayed for cake."
Celebrate the attempt, not just the success.
Reference: ABA Reinforcement Principles — immediate, specific reinforcement | BACB ethical guidelines

Step 6: The Cool-Down
Step 6 of 6
Post-Exposure Recovery Protocol. Even with protection, challenging environments deplete the photosensitive child's visual processing capacity. After any extended exposure to triggering environments, provide recovery time.
1
After School (Daily)
"You did a whole school day with those lights. Your eyes worked really hard. Let's do 15 minutes in the recovery corner with your mask on before homework."
2
After Social Events
"That party was loud and bright. Let's go to the quiet room for a bit. No rush."
3
After Unexpected Exposure
If the child encounters unexpected flashing (emergency vehicle, surprise strobe at an event):
- Remove from trigger immediately (use code word)
- Apply cooling compress over closed eyes
- Move to darkest available space
- Allow minimum 15–20 minutes before the next demand
- Do NOT debrief or discuss the trigger during recovery — just let the nervous system reset
Transition Cue: "When the timer goes to zero, recovery time is done and we can [next activity]. But if you need more time, just say so."
The recovery space is not punishment. It is medicine. The child who knows recovery is always available can tolerate more exposure — paradoxically increasing participation.
Reference: NCAEP Evidence-Based Practices Report (2020) — Visual supports and transition strategies

Capture the Data: Right Now
Capture 3 data points within 60 seconds of each exposure. This data drives your child's personalised progression within GPT-OS® and informs your occupational therapist's recommendations.
1
Data Point 1 — Environment Type
Fluorescent | LED | Outdoor/Sun | Screen | Decorative/Strobe | Mixed
2
Data Point 2 — Duration of Comfortable Participation
0 | 1–5 min | 5–15 min | 15–30 min | 30–60 min | 60+ min
3
Data Point 3 — Protection Level Used
Glasses | Hat/Shield | Modified Lighting | Screen Filter | Warning System | Recovery Space | No Protection Needed
Optional — Distress Level (0–5)
0 | No distress | |
1 | Mild awareness | |
2 | Mild discomfort, managed | |
3 | Moderate distress, needed break | |
4 | Significant distress, had to leave | |
5 | Severe distress, extended recovery |
60 seconds of data now saves hours of guessing later.
Tracking reveals patterns: Which environments are most challenging? Which tools are most effective? Is duration increasing over weeks? Is distress level decreasing?
Tracking reveals patterns: Which environments are most challenging? Which tools are most effective? Is duration increasing over weeks? Is distress level decreasing?
🔗Download the Pinnacle Flicker Sensitivity Tracker (PDF) at pinnacleblooms.org/trackers | 🔗Log directly into GPT-OS® in-app tracker
Reference: ABA Data Collection Standards — Cooper, Heron & Heward (Applied Behaviour Analysis)
What If It Didn't Go as Planned?
Common Challenges and Immediate Solutions. Session abandonment is not failure — it's data. Every difficult experience teaches you something specific about your child's sensitivity profile.
"The glasses don't seem to help."
Not all tints are equal. Amber/rose tints address fluorescent flicker specifically. Generic blue-light glasses may not filter the right wavelengths. Consider upgrading to clinical FL-41 lenses if commercial options fail. Some children need prescription-grade precision tinting — consult an optometrist experienced with photosensitivity.
"My child refuses to wear the glasses — they look 'different'."
Completely normal. Let the child choose their own frames. Some children respond to calling them "gaming glasses" or "special mission glasses." Introduce gradually — at home first, then in trusted environments. Peer explanation cards can help: "These glasses protect my eyes like yours protect you from the sun."
"The school won't change the lighting."
Provide formal medical/therapy documentation. Cite your child's right to reasonable accommodation. Offer DIY solutions that cost the school nothing — desk shield, hat permission, seat positioning. If resistance continues, escalate through Pinnacle's school accommodation consultation service.
"The child still gets headaches even with protection."
FL-41 glasses reduce but may not eliminate migraine-type headaches. If headaches persist with full environmental protection in place, medical evaluation is needed. This may indicate underlying migraine disorder requiring pharmacological management beyond environmental modification.
"We can't afford FL-41 glasses right now."
Start with zero-cost interventions: screen modifications (free software), desk positioning, DIY cardboard shields, hat use, recovery space from household materials. Even commercial amber glasses (₹200–₹800) provide partial relief while you save for clinical-grade options.
"Recovery space seems to make things worse — the child doesn't want to come out."
Distinguish between recovery (necessary nervous system reset) and avoidance (using recovery space to escape all demands). Set a timer for recovery. After the timer, transition to a low-demand activity — not directly into a triggering environment. If recovery space use is increasing rather than decreasing over weeks, consult your OT.

Adapt and Personalise
No two children are identical — calibrate to your child.
1
Milder Profile
Notices fluorescent flicker but tolerates for 15–30 minutes with mild discomfort. Screen sensitivity managed with software adjustments alone. Can attend events with glasses + pre-warning.
Focus: Screen tools, warning systems, glasses for extended fluorescent exposure
2
Moderate Profile
Cannot tolerate unmodified fluorescent environments for more than 5–10 minutes. Headaches triggered by multiple light types. Social participation significantly limited.
Focus: Full environmental modification at home + school, glasses mandatory, recovery space essential, advocacy cards in active use
3
Severe Profile
Any flickering light triggers immediate distress or pain. History of migraine or seizure-like responses to light. Avoids most public environments.
Focus: ALL materials deployed simultaneously, medical coordination mandatory, gradual exposure ONLY under professional guidance
Age Adjustments
Ages 3–5
Parent manages all tools; child learns "eyes hurt" vocabulary and recovery space access
Ages 6–8
Child begins self-deploying glasses and hat; learns code word; participates in advocacy
Ages 9–12
Child independently manages toolkit; self-advocates with teachers; participates in tracking data; understands their own neurology
Sensory Seeker vs. Avoider: Most flicker-sensitive children are visual avoiders — but some may seek certain types of controlled light stimulation. For these children, provide safe visual stimulation channels (glitter jars, light projectors at safe settings) while protecting against harmful flicker.

ACT IV — THE PROGRESS ARC
Week 1–2: What to Expect
What "Progress" Looks Like at This Stage
- The child tries FL-41 glasses for 1–3 minutes indoors without complaint
- The child voluntarily enters their modified (flicker-free) room and comments that it "feels better"
- Screen time extends by 5–10 minutes with modifications active
- The child uses the recovery space once without prompting
- The child uses the code word correctly in practice (not yet in real situations)
What Is NOT Progress Yet (and That's Okay)
- The child will NOT tolerate an unmodified fluorescent classroom for a full school day
- The glasses will NOT eliminate all symptoms in all environments
- The child may still resist wearing glasses in public
- Headaches may still occur after challenging exposures
Parent emotional preparation: This stage feels slow. You are building an infrastructure, not performing a miracle. Trust the process.
If your child tolerates their modified bedroom for 5 minutes longer than last week without rubbing their eyes — that's real, measurable, neurological progress.
If your child tolerates their modified bedroom for 5 minutes longer than last week without rubbing their eyes — that's real, measurable, neurological progress.
Reference: PMC11506176 — Early-phase indicators focus on tolerance and participation

Week 3–4: Consolidation Signs
Progress: ~40%
Neural Pathways Forming. The protection system is taking hold. Here's what to look for.
Self-Initiation
The child reaches for glasses before leaving the house without prompting — one of the clearest early indicators that the protection system is being internalised.
School Reports Improving
Improved classroom attention since lighting accommodations. Teachers notice increased sustained work periods. Headache frequency decreasing week-over-week — track this as the most objective measure.
Shorter Recovery Times
Recovery time after exposure shortens (was 30 minutes, now 15). The child identifies "good lights" vs "bad lights" in new environments before experiencing distress.
Expanded Participation
The family attempts a previously avoided outing (mall, cinema) with full toolkit deployed. "Can we check the lights first?" replaces "I don't want to go" — anxiety shifting to anticipatory planning.
When to increase challenge level: If the child comfortably manages all current environments with protection, begin expanding to one new environment per week with the full toolkit. Never remove protection to "test" — add new venues with protection in place.
Parent milestone: "You may notice you're more confident too." When you stop cancelling plans and start planning with accommodations, the entire family dynamic shifts.
Parent milestone: "You may notice you're more confident too." When you stop cancelling plans and start planning with accommodations, the entire family dynamic shifts.

Week 5–8: Mastery Indicators
Progress: ~75%
🏆 Mastery Phase
Self-Directed Management Emerging. Here are the observable, measurable criteria for mastery.
1
Independent Tool Deployment
Child independently deploys appropriate protective tool before entering triggering environments — without parental prompting
2
External Communication
Child communicates sensory needs to at least 2 adults outside the family (teacher, coach, relative)
3
Proactive Recovery
Child uses recovery space proactively (before full distress) rather than reactively — a critical indicator of self-regulation development
4
Headache Reduction
Headache frequency reduced by ≥50% from baseline — the most objective, measurable outcome indicator
5
Participation Expansion
Child participates in at least 3 previously avoided activities with protection in place — functional access has measurably improved
6
School Improvement
School attendance or classroom participation has measurably improved — documented through teacher reports and academic records
🏆 Mastery Badge Criteria: The child's Sensory Processing Index within GPT-OS® shows sustained improvement across 4+ weeks. Functional Participation Index confirms expanded environmental tolerance. Environmental Tolerance Index shows ≥30% improvement from baseline.
Once mastery is maintained for 4 consistent weeks, consult your occupational therapist about whether gradual exposure (Material 9) is appropriate.
Once mastery is maintained for 4 consistent weeks, consult your occupational therapist about whether gradual exposure (Material 9) is appropriate.
Reference: PMC10955541 | BACB mastery criteria standards
Celebrate This Win
You Did This.
Remember Card 01? "The lights flicker. Everyone else is fine. Your child is in pain." That was 5–8 weeks ago.
Today, your child has glasses that filter the wavelengths that hurt. Their bedroom is a flicker-free refuge. Their school desk has a shield. Their screens are filtered. They have a code word, a recovery space, and the vocabulary to say: "I have photosensitivity. These are my glasses. Thank you for understanding."
Your child is not limited by lights anymore. They manage them.
You built this protection system. You converted your home lighting. You coordinated with the school. You packed the go bag every morning. You held your child's hand during the first test exposure and praised every brave attempt.
Your commitment changed your child's access to the world. That is measurable, evidence-based, neurologically real progress.
1
📸 Document This Milestone
Take a photo of your child at a place they couldn't go before. The birthday party. The classroom. The grocery store. Date it. This is evidence of change.
2
🎉 Celebrate as a Family
This is a win for everyone. The whole family's life just expanded. Share the moment — it belongs to all of you.
Red Flags: When to Pause
Safety Alert
🔴Pause and Consult If You Observe Any of the Following:
1
1. Increasing Headache Severity or Frequency
Despite full protection deployed → May indicate underlying migraine disorder progression requiring medical management
2
2. Any Episode Resembling a Seizure
Unusual eye movements, brief unresponsiveness, involuntary jerking during or after light exposure → URGENT: Neurological evaluation needed. Call emergency services if seizure occurs.
3
3. New Visual Symptoms
The child reports seeing shapes, patterns, or "snow" that persists after light exposure is removed → Neurological evaluation warranted
4
4. Protection Tools Causing Increased Anxiety
The child becomes more anxious about light environments despite having tools → May indicate anxiety disorder layered on top of sensory sensitivity, requiring psychological support
5
5. Complete Refusal of All Environments
Environmental avoidance expanding rather than contracting despite available protection → May indicate deeper functional avoidance requiring behavioural intervention
6
6. Physical Symptoms Beyond Headache
Persistent nausea, dizziness, or balance problems triggered by light → May indicate vestibular involvement requiring comprehensive sensory evaluation
Escalation Pathway
Level 1 — Self-Resolve
Adjust protection level, modify timing, use troubleshooting guide (Card 22)
Level 2 — Teleconsultation
Book a Pinnacle teleconsultation — 9100 181 181 (16+ languages, 24x7)
Level 3 — Clinic Visit
In-person evaluation at your nearest Pinnacle centre for comprehensive sensory profile reassessment
Trust your instincts. If something feels wrong, pause and ask.

The Progression Pathway
Your Child's Pathway — From Here
1
← Prerequisite
Visual processing foundations. General sensory processing assessment and AbilityScore® baseline.
2
⭐ Current Position
A-066: Environmental Modification for Flashing Light Sensitivity
← YOU ARE HERE
3
Path A — Flicker Sensitivity Improves
Expands from flicker-specific to broader photosensitivity management
4
Path B — Screen Sensitivity Primary
Deep-dive into digital access optimisation
5
Path C — Headaches Persistent
Migraine and headache management protocol integration
↔ Lateral Alternatives
- A-075: Sensory Overwhelm in Stores — Multi-sensory environmental approach
- A-080: Migraine-Like Symptoms — Medical-first approach
Long-term developmental goal: Self-directed sensory management across all contexts → Full community participation → Independence in environmental advocacy
Related Techniques in This Domain
Visual Sensory Processing — You already have materials that support these techniques:
1
🔹 A-064: Child Avoids Eye Contact
Uses light filtering + environmental control foundations you've already built
View Technique | Difficulty: Core
2
🔹 A-067: Difficulty With Bright Environments
Direct extension of your flicker protection to general photosensitivity
View Technique | Difficulty: Core
3
🔹 A-068: Screen Sensitivity
Builds on your screen modification tools with deeper digital access strategies
View Technique | Difficulty: Core
4
🔹 A-075: Sensory Overwhelm in Stores
Multi-sensory protection for community navigation — you already have the visual component
View Technique | Difficulty: Core
5
🔹 K-990: Understanding Visual Sensory Processing
Parent education deep-dive into the neuroscience and intervention options
View Knowledge Base | Type: Education
6
🔹 K-995: Advocating for Sensory Accommodations at School
Amplifies your advocacy card deployment with structured negotiation frameworks
View Knowledge Base | Type: Advocacy
Browse full Visual Sensory Processing domain →techniques.pinnacleblooms.org/domains/sensory-visual
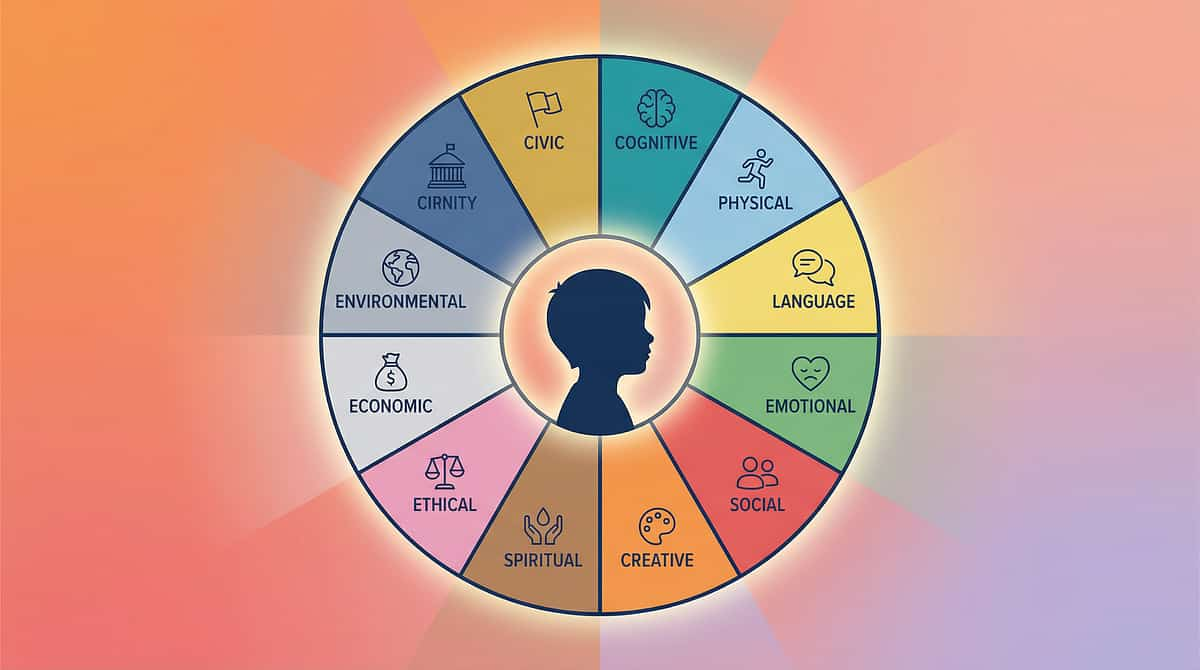
Your Child's Full Developmental Map
This technique is one piece of a larger plan. Flashing light sensitivity lives within Domain A: Sensory Processing — one of 12 developmental domains tracked and optimised by GPT-OS®.
1
A ⭐ Sensory Processing
Currently Active
2
B — Communication & Language
3
C — Social Interaction & Play
4
D — Emotional Regulation & Behaviour
5
E — Motor Development
6
F — Daily Living & Self-Care
7
G — Academic & Cognitive
8
H — Feeding & Nutrition
9
I — Sleep & Circadian
10
J — Community Participation & Safety
11
K — Family Systems & Support
12
L — Transition & Independence
Every technique page you visit is a precision intervention within one domain. GPT-OS® coordinates across all 12 simultaneously. Environmental modification for flicker sensitivity (this technique) improves Sensory Processing (A), which cascades into improved Academic (G), Community Participation (J), and Emotional Regulation (D).
🔗See your child's full profile → Request AbilityScore® Assessment | 📞 FREE National Autism Helpline: 9100 181 181
Reference: WHO/UNICEF Nurturing Care Framework (2018) — holistic developmental monitoring across five nurturing care components

ACT V — THE COMMUNITY AND ECOSYSTEM
Families Who've Been Here
Real Families. Real Outcomes. Names changed. Outcomes represent individual experiences; results vary by child profile. Statistics represent aggregate Pinnacle Network outcomes.
1
Family 1 — The "Magic Glasses" Story
Before: Avya (age 6) could not enter her classroom without tears. The fluorescent lights triggered headaches within 10 minutes. She was moved to a separate room — which solved the light problem but created social isolation.
After (8 weeks): FL-41 glasses prescribed through Pinnacle OT. Classroom returned with glasses + desk shield + teacher education. Avya calls them her "magic glasses." She attended her first full school assembly in 14 months.
Parent: "We went from avoiding every store, every party, every trip — to planning outings with her glasses, her go bag, and her confidence. She's not limited by lights anymore. She manages them."
Therapist Note: "Avya's Sensory Processing Index improved 40% in 8 weeks. Her Functional Participation Index doubled. The key was protection first — not exposure."
2
Family 2 — The School Advocacy Win
Before: Rahul (age 9) was labelled as "disruptive" because he would leave his desk, pace the room, and eventually refuse to work under fluorescent lights. Multiple behavioural interventions failed.
After (6 weeks): Comprehensive sensory profile identified visual flicker sensitivity as the primary trigger. Classroom lighting modified above his workstation. Portable shield provided. Screen modifications applied to his tablet. Advocacy card created by Rahul himself.
Parent: "Once the school understood it was the lights, not his attitude, everything changed. His teacher became his biggest advocate."

Connect With Other Parents
Isolation is the enemy of progress.
You are not the only parent who has left a birthday party early, cancelled a movie outing, or explained for the hundredth time that "the lights hurt her." Connect with families navigating the same challenge.
Pinnacle Parent Community — Visual Sensory Processing Support
Join families managing light sensitivity, photosensitivity, and visual overwhelm. Share resources, strategies, and hard-won experience with parents who truly understand.
Local Pinnacle Centre Parent Meetups
Monthly in-person gatherings at your nearest Pinnacle centre. Find your local community at pinnacleblooms.org/centres
Peer Mentoring
Request to be matched with an experienced parent who has walked this exact path — through your Pinnacle centre coordinator. A shortcut through weeks of trial and error.
"Your experience helps others. Consider sharing your family's journey."
When you share your child's lighting modifications, your school advocacy approach, or your go bag contents — you hand another parent a shortcut through weeks of trial and error.
Reference: WHO NCF Community Engagement Principles — parent support networks improve intervention outcomes
Your Professional Support Team
Home + Clinic = Maximum Impact. Home-based environmental modification is powerful — but professional guidance amplifies every outcome.
1
🔍 Comprehensive Sensory Integration Assessment
Full visual sensitivity profile mapping — identifies specific wavelengths, frequencies, and environmental triggers unique to your child. Conducted by certified occupational therapists within the GPT-OS® Diagnostic Intelligence Layer.
2
📊 AbilityScore® Assessment
Your child's universal developmental score (0–1000) establishing baseline severity across all sensory and functional domains. Comparable across time, therapists, and centres.
3
📋 Personalised EverydayTherapyProgramme™
Daily, home-executable micro-interventions specific to your child's flicker sensitivity profile — generated by TherapeuticAI® and monitored through GPT-OS®.
4
🏥 70+ Centres Across India
Every centre operates under GPT-OS® clinical standards with measurable accountability. Find your nearest Pinnacle centre →
5
📱 Teleconsultation Available
For families beyond centre access — remote evaluation, guidance, and monitoring. Full clinical quality, wherever you are.
📞FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24x7 | No cost
Reference: WHO NCF Progress Report (2023) — primary health care as platform for essential ECD interventions

The Research Library
The Evidence Base — For Parents Who Want to Go Deeper
1
Level I — Systematic Reviews & Meta-Analyses
📄PRISMA Systematic Review (2024): "Sensory Integration Intervention for Children with ASD" — 16 articles from 2013–2023 confirm evidence-based practice classification
PubMed: PMC11506176 | Children (Basel), 2024
PubMed: PMC11506176 | Children (Basel), 2024
📄Meta-Analysis (2024): "Sensory Integration Therapy for ASD" — 24 studies demonstrating effective promotion of social skills, adaptive behaviour, sensory processing, and motor skills
PubMed: PMC10955541 | World J Clin Cases, DOI: 10.12998/wjcc.v12.i7.1260
PubMed: PMC10955541 | World J Clin Cases, DOI: 10.12998/wjcc.v12.i7.1260
2
Level II — Clinical Trials
📄Indian RCT (2019): Home-based sensory interventions for children with ASD — demonstrated significant outcomes with parent-administered protocols
DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Paediatrics
DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Paediatrics
3
Level III — Clinical Guidelines & Frameworks
📄WHO Nurturing Care Framework (2018):nurturing-care.org
📄WHO/UNICEF CCD Package (2023):PubMed: PMC9978394
📄NCAEP Evidence-Based Practices Report (2020):NCAEP EBP Report
📄WHO/UNICEF CCD Package (2023):PubMed: PMC9978394
📄NCAEP Evidence-Based Practices Report (2020):NCAEP EBP Report
4
Condition-Specific Resources
📄Epilepsy Foundation: Photosensitivity and Seizures Guidelines epilepsy.com
📄American Migraine Foundation: Light Sensitivity and Migraine Research americanmigrainefoundation.org
📄Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory processing treatment in ASD DOI: 10.3389/fnint.2020.556660
📄American Migraine Foundation: Light Sensitivity and Migraine Research americanmigrainefoundation.org
📄Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory processing treatment in ASD DOI: 10.3389/fnint.2020.556660

How GPT-OS® Uses Your Data
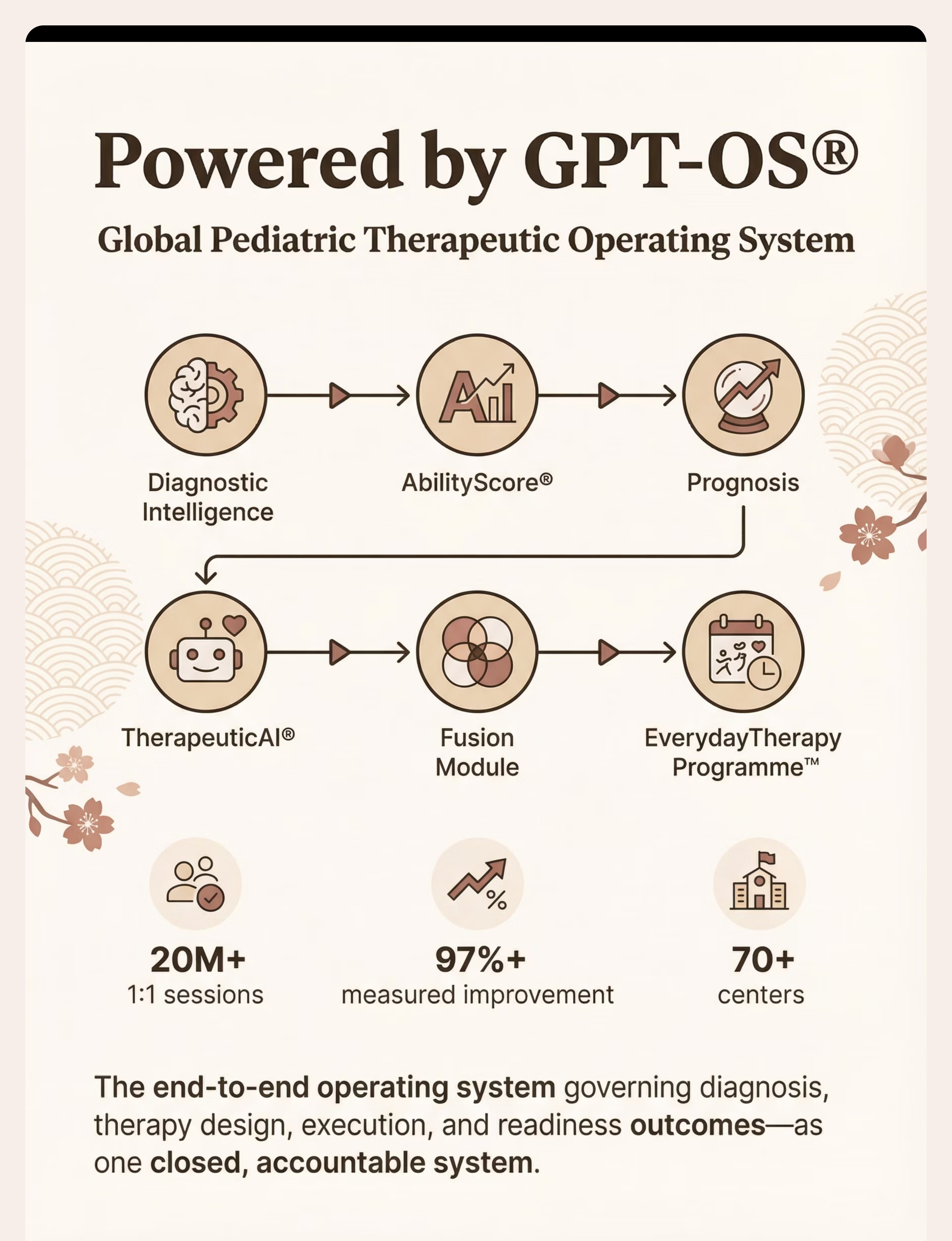
Powered by GPT-OS® — Global Paediatric Therapeutic Operating System. GPT-OS® is the end-to-end operating system governing diagnosis, prognosis, therapy design, execution, monitoring, and readiness outcomes — as one closed, accountable system.
What GPT-OS® Learns From This Technique
- Which material combinations produce fastest improvement for your child's flicker sensitivity profile
- Optimal deployment sequence for your child's age, severity, and co-occurring conditions
- Environmental trigger patterns unique to your child that inform proactive preparation
- Progress trajectory prediction — when to expect mastery milestones
Privacy Protection
- All data encrypted in transit and at rest
- HIPAA-equivalent privacy standards
- Your child's data is never sold or shared
- Population-level insights (de-identified) improve recommendations for all families
Your data helps every child like yours.
20M+ 1:1 sessions • 97%+ measured improvement • 70+ centres • Patents filed across 160+ countries
20M+ 1:1 sessions • 97%+ measured improvement • 70+ centres • Patents filed across 160+ countries
Watch the Reel
1
📹 Reel ID
A-066
2
📺 Series
Sensory Solutions — Episode 66
3
🎯 Domain
Sensory Processing / Visual System / Light Sensitivity
4
⏱️ Duration
75–85 seconds
This Reel shows a Pinnacle therapist demonstrating each of the 9 materials in this protocol — from FL-41 glasses fitting to recovery space setup to advocacy card creation. Seeing the materials in action reinforces what you've read and adds a vital visual learning layer.
📹Watch: "9 Materials That Help With Flashing Light Sensitivity"
🔗 Watch on Instagram: @pinnacleblooms | 🔗 Watch on YouTube: Pinnacle Blooms Network
🔗 Watch on Instagram: @pinnacleblooms | 🔗 Watch on YouTube: Pinnacle Blooms Network
About the Presenter: A Pinnacle Blooms occupational therapist specialising in sensory integration and visual sensory processing intervention, speaking from 20M+ collective therapy sessions across the Pinnacle Network.
Reference: NCAEP (2020) — Video modelling is classified as evidence-based practice for autism | Multi-modal learning improves parent skill acquisition

Share This With Your Family
Consistency across caregivers multiplies impact. If only one parent deploys the protection system, it's limited. When grandparents, school teachers, nannies, and other caregivers understand the protocol — your child is protected everywhere.
1
🟢 WhatsApp
Send this technique page to your family group
2
📧 Email
Forward to school, spouse, grandparents, caregivers
3
🔗 Copy Link
techniques.pinnacleblooms.org/sensory-processing/flashing-light-sensitivity-materials-A066
📋 Explain to Grandparents (Simplified Version):
"Your grandchild has sensitive eyes that can see lights flickering in a way most people can't. It causes real pain — like a constant strobe. We've set up special glasses, changed our lights at home, and have a recovery corner. If the child covers their eyes or says the code word, please take them to a quiet dark space immediately. It's not drama — it's their nervous system asking for help."
📝 Teacher Communication Template:
"Dear [Teacher], [Child] has been diagnosed with photosensitivity / flicker sensitivity. Flickering fluorescent lights cause [headaches/distress/difficulty concentrating]. We have provided [FL-41 glasses / desk shield / hat]. Please allow their use in class. A designated recovery space would be beneficial. I've attached an information card. The child's occupational therapist at Pinnacle Blooms ([contact]) is available for consultation."
Reference: WHO CCD Package — PMC9978394 | Multi-caregiver training as critical for intervention generalisation

ACT VI — THE CLOSE AND LOOP
Frequently Asked Questions
Will my child always need these glasses/tools?
Many children develop increased tolerance over time, especially with professional guidance. Some continue to use filtering glasses as a preference even as sensitivity decreases — similar to anyone wearing sunglasses on a bright day. The goal is not eliminating the tools but giving the child choice and agency.
Could this be photosensitive epilepsy? Should I be worried?
Photosensitive epilepsy affects approximately 3% of people with epilepsy. If your child has never had a seizure and has no family history, epilepsy risk is low — but not zero. If your child has ever had a seizure, unusual eye movements during light exposure, or brief episodes of unresponsiveness near lights, seek neurological evaluation immediately.
Can my child use regular sunglasses instead of FL-41 glasses?
Regular sunglasses reduce ALL light equally — they make everything darker but don't address flicker specifically. FL-41 glasses selectively filter the wavelengths (blue-green, 480–520nm) most associated with fluorescent triggers. Many children report sunglasses "don't help" but FL-41 glasses "fix the flashing." Start with amber-tinted commercial glasses as a low-cost test.
Is the school legally required to modify lighting?
Under India's Rights of Persons with Disabilities Act (2016) and most international disability frameworks, schools are required to provide "reasonable accommodations" for students with documented sensory disabilities. A formal letter from your child's treating therapist or neurologist creates the basis for accommodation requests. Pinnacle's school accommodation consultation can help navigate this process.
How do I know if a LED bulb is truly "flicker-free"?
Use the smartphone camera test: point your phone's camera at the LED while set to slow-motion video. Flickering bulbs will show visible dark bands scrolling across the image. True flicker-free bulbs appear steady. Also look for specs mentioning "high-frequency driver," "DC power," or "flicker-free" certification.
My child's sensitivity seems to get worse during exams/stress. Is that normal?
Absolutely. Sensory processing is mediated by the autonomic nervous system, which is directly affected by stress, fatigue, illness, and emotional state. Sensitivity amplifies under stress. During high-demand periods, deploy maximum protection and increase recovery space access. This is not regression — it's predictable physiology.
At what age can my child start managing this independently?
Most children begin self-deploying tools (glasses, hat) by age 6–7 with prompting, and independently by age 8–10. Self-advocacy (explaining needs to adults) typically emerges at age 8–9 with practised scripts. Full independence is typically achievable by age 10–12.
Does screen time make flicker sensitivity worse?
Unmodified screen time can exacerbate sensitivity through blue light emission, low refresh rates, and flickering content. Modified screens (Night Shift, high refresh rate, reduced brightness, content filtering) can actually be well-tolerated. The key is modification, not avoidance. Digital access is essential for learning — modify the tool, don't remove it.
Didn't find your answer? 🔗 Ask GPT-OS® | 📞 Book a teleconsultation: 9100 181 181

Your Next Step: Start Now
You've read the science. You have the tools. Your child is waiting.
1
🟢 Primary Action: Start This Technique Today
Deploy Material 1 (flicker-filtering glasses) and Material 2 (flicker-free home lighting) — the highest-impact combination. Follow the Week 1 protocol from Card 17 (Step 3: The Therapeutic Action).
2
🔵 Secondary Action: Book a Professional Consultation
Comprehensive Sensory Integration Assessment + AbilityScore® + Personalised EverydayTherapyProgramme™
📞9100 181 181 (FREE | 16+ languages | 24x7)
3
⚪ Tertiary Action: Explore the Next Technique
Validated by the Pinnacle Blooms Consortium
Preview of 9 materials that help with flashing light sensitivity Therapy Material
Below is a visual preview of 9 materials that help with flashing light sensitivity therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
The Pinnacle Promise
From fear to mastery. One technique at a time.
Pinnacle Blooms Network® — Built by Mothers. Engineered as a System.
This intervention technique page was developed by the Pinnacle Blooms Consortium — a multidisciplinary body of Clinical Research Scientists, Speech-Language Pathologists, Occupational Therapists, Board Certified Behaviour Analysts, Special Educators, and NeuroDevelopmental Paediatricians — powered by GPT-OS® and validated against 20M+ exclusive 1:1 therapy sessions with 97%+ measured improvement across 70+ centres.
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed healthcare provider, neurologist, or occupational therapist. Significant photosensitivity, especially with any history of seizures or symptoms suggesting photosensitive epilepsy, requires medical evaluation. Some interventions in this content require professional supervision. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Statutory Identifiers: CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME Udyog Aadhaar: TS20F0009606
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24x7