
9 Materials That Help With Fine Motor Play Ideas
Turning everyday play into hand skill development
🎯 Fine Motor Development — Episode 618
Ages 2–8
Pediatric OT

Fine Motor Play Ideas
ACT I — The Emotional Entry
It's 4:30 PM on a Tuesday. The occupational therapist's homework sheet sits on the dining table — trace these shapes, pick up these small objects with tweezers, cut along these lines. Your child takes one look, says "I don't want to," and disappears to the living room where they'll happily build with blocks for the next forty-five minutes.
You're not failing at this.
Your child's hands are speaking — you just need to understand their language. The resistance isn't defiance. It's communication.
"Therapy That Feels Like Playing"
"Your child doesn't resist fine motor development. They resist activities that feel like tests. The solution isn't better discipline. The solution is better play."
🏥Pinnacle Blooms Network® Multi-Disciplinary Consortium — OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO | 📞 FREE National Helpline: 9100 181 181 (16+ languages)
📊 You Are Not Alone — The Numbers
Millions of Children Are on This Same Journey
1 in 36
Children on the Spectrum
Children diagnosed with autism spectrum conditions globally — each family navigating a unique developmental path.
70–80%
Fine Motor Co-occurrence
Children with developmental conditions show fine motor delays as a significant co-occurring challenge requiring targeted support.
21M+
Therapy Sessions Delivered
Therapy sessions delivered by Pinnacle Blooms Network® — the world's largest integrated pediatric therapy system.
Fine motor difficulties don't signal a "broken" child. They signal a nervous system that processes sensory-motor information differently — a wiring variation that responds profoundly well to the right kind of structured, play-based practice. In India alone, conservative estimates place the number of children requiring fine motor therapeutic support at over 3 million. You are among millions of families navigating this exact challenge. The path forward is clearer than you think.
🧠 The Neuroscience — In Parent Language
Fine Motor Difficulty Is a Brain Wiring Variation — Not a Behavior Choice
Key Brain Regions Involved
Primary Motor Cortex — Plans and executes finger movements
Cerebellum — Coordinates timing and precision
Somatosensory Cortex — Processes touch feedback from hands
Basal Ganglia — Automates learned motor sequences
Premotor Cortex — Anticipates and prepares grip patterns
What This Means in Plain Language
When a child struggles with fine motor tasks, the communication pathways between brain regions are still consolidating. The motor cortex may plan a pinch grip, but the cerebellum hasn't yet calibrated the timing. The somatosensory cortex may over-amplify tactile feedback — making a pencil feel uncomfortable. This is not weakness. This is development in progress.
The extraordinary finding from neuroplasticity research: these pathways strengthen rapidly when the child is motivated. A child who resists worksheets but eagerly squeezes play dough is building the same neural networks. Motivated repetition grows myelin. Myelin speeds neural transmission. Speed equals skill.
Play isn't the easy route. Play is the optimal route.
📅 Developmental Context
Fine Motor Skills Build in Predictable Stages — Every Child Has a Starting Point
Fine motor play skill challenges most commonly become visible between ages 3–5, when pre-academic demands (coloring, cutting, fastening) begin. However, the roots of difficulty often trace back to early sensory processing and proprioceptive awareness in infancy. F-618 targets the entire continuum from ages 2–8.
Sensory Processing Differences
Tactile over- or under-sensitivity affecting material tolerance
Oral Motor Overlap
SLP connection — hand-mouth coordination patterns
Gross Motor Precedents
Gross motor delays that preceded fine motor emergence
Attention & Focus
ABA overlap — sustained engagement with fine motor tasks

🔬 Clinical Evidence — Research Grade
This Approach Is Evidence-Based. Not Opinion. Not Trend.
EVIDENCE GRADE: LEVEL I
PRISMA Systematic Review (2024) — 16 studies (2013–2023): Play-based sensory integration intervention confirmed as evidence-based practice for children with ASD. Fine motor outcomes among primary measured benefits. PMC11506176
Meta-Analysis (2024)
World J Clin Cases — 24 studies: Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and fine/gross motor skills across populations. PMC10955541
Indian RCT (2019)
Journal of Pediatrics (Padmanabha et al.) — Home-based sensory-motor interventions by trained parents demonstrated significant, measurable outcomes in Indian pediatric populations. DOI: 10.1007/s12098-018-2747-4
"Clinically validated. Home-applicable. Parent-proven." Play-based fine motor intervention IS the real therapy — backed by the strongest category of clinical evidence and aligned with WHO/UNICEF global frameworks for 197 countries.
📞 FREE consultation: 9100 181 181 | Speak with a Pinnacle OT specialist today

ACT II — Knowledge Transfer
🖐️ F-618 Technique Definition
Fine Motor Play Ideas — "The Hands That Play, Learn"
Fine Motor Play Ideas is a play-based occupational therapy approach that embeds targeted hand skill development within activities children intrinsically choose and enjoy. Rather than isolated finger exercises, this technique uses 9 categories of therapeutic play materials to simultaneously develop grip strength, pinch force, bilateral coordination, finger isolation, in-hand manipulation, and eye-hand coordination — while the child believes they're simply playing.
The core clinical insight: motivation-driven repetition builds motor pathways more efficiently than externally imposed drill. A child who spends 20 minutes squeezing play dough achieves more therapeutic dosage than a child who spends 5 minutes doing prescribed exercises before refusing to continue.
🏥 Domain
OT-FMP
⏱️ Session
5–20 min
👶 Age
2–8 years
📅 Frequency
Daily embedding
📋 Series
Fine Motor Play

🏥 Consortium Disciplines
This Technique Operates Across 5 Therapy Disciplines Simultaneously
Occupational Therapy (OT) — PRIMARY LEAD
OT drives F-618. Session structure, material grading, and sensory integration are OT-governed. Builds hand strength, coordination, tool use, and self-care independence.
Speech-Language Pathology (SLP)
SLPs incorporate fine motor play for oral motor preparation. Finger painting, play dough manipulation, and construction play support oral motor readiness and early literacy.
ABA/BCBA — Reinforcement Architecture
BCBAs design reinforcement systems. Motivation assessment, token economies, preference-based activity selection, and data collection protocols are ABA's contributions to F-618.
Special Education (SpEd)
SpEd connects fine motor play gains to pre-academic readiness — pencil grip for writing, scissors use for craft-based learning, puzzle completion for cognitive engagement.
NeuroDev Pediatrics — Clinical Oversight
NeuroDev pediatricians monitor the neurological basis of fine motor challenges, co-occurring conditions, and medical contraindications. They authorize home-based protocol implementation.
"The brain doesn't organize by therapy type. Fine motor development involves sensory processing (OT), communication (SLP), behavior (ABA), learning (SpEd), and neurology (NeuroDev) simultaneously. The Pinnacle consortium addresses all five — in every session."
🎯 Therapeutic Targets
F-618 Targets 7 Fine Motor Components — Precisely, Not Generally
Component | Observable Indicator | Materials That Target This | |
Grip Strength | Sustains squeeze for 5+ seconds | Play dough, tongs, spray bottles | |
Pinch Force | Holds thin object between thumb + finger | Sticker peeling, beads, puzzle knobs | |
In-Hand Manipulation | Adjusts object within hand without other hand | Puzzle rotation, coin manipulation | |
Bilateral Coordination | Two hands doing different roles simultaneously | Threading, scissors, building blocks | |
Eye-Hand Coordination | Places object precisely where intended | Puzzles, sticker targeting, threading | |
Finger Isolation | Moves one finger independently of others | Finger painting, poking activities | |
Graded Muscle Control | Adjusts force appropriately for task | Stamping, clay work, block stacking |
📖 Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy across 24 studies promoted adaptive behavior and motor skills. PMC10955541

🛒 Primary Materials — Your F-618 Toolkit
9 Material Categories. Start With What You Have. Add What You Need.

🟢 1. Play Dough & Modeling Clay
Builds grip strength, intrinsic hand muscles, and proprioceptive feedback. ₹100–400 | Homemade: ₹0
🧱 2. Building Blocks & Construction Sets
Precision placement, pinch strength, visual-motor integration. ₹200–2,000 | DIY: household containers

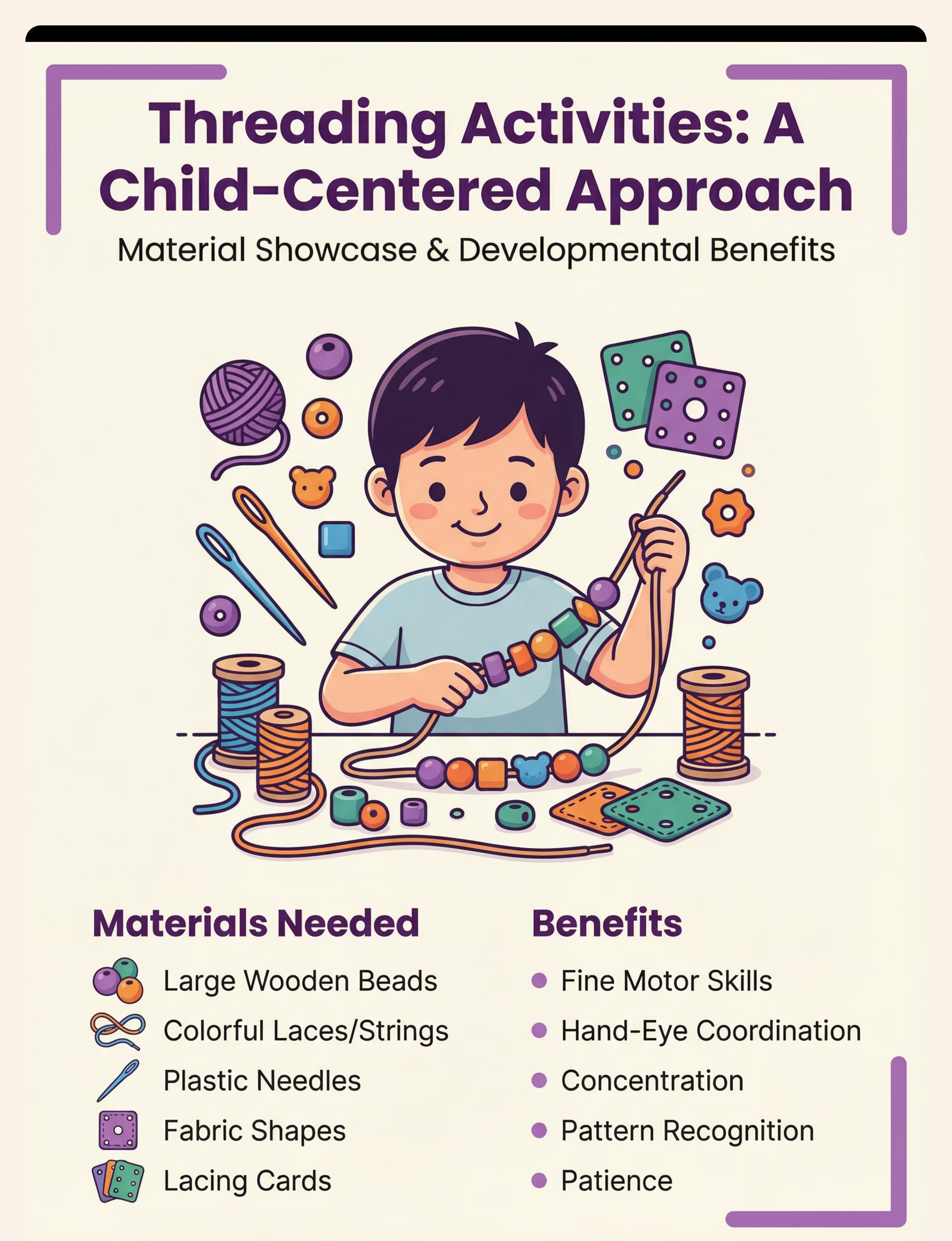
🔗 3. Threading & Lacing Activities
Bilateral coordination, eye-hand precision, sustained attention. ₹150–600 | DIY: pasta + string

⭐ 4. Stickers, Stamps & Peel-and-Stick
Pinch strength, finger isolation, eye-hand accuracy. ₹50–400 | ✅ Pinnacle Recommends: 1800+ Reward Sticker Book ₹364

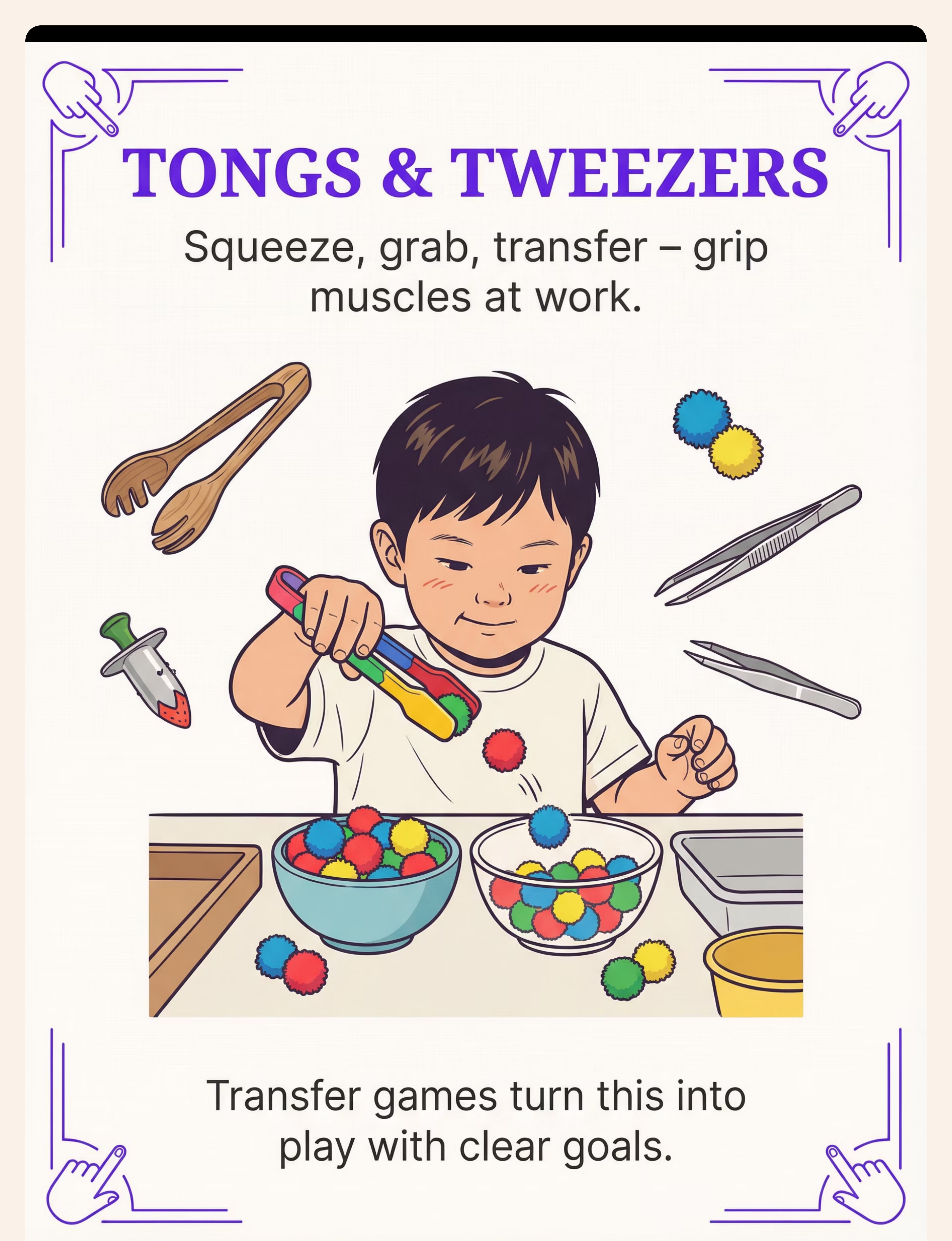
🥄 5. Tongs, Tweezers & Transfer Games
Tripod grip preparation, precision grasp, graded muscle control. ₹100–500 | DIY: clothespins + pom-poms

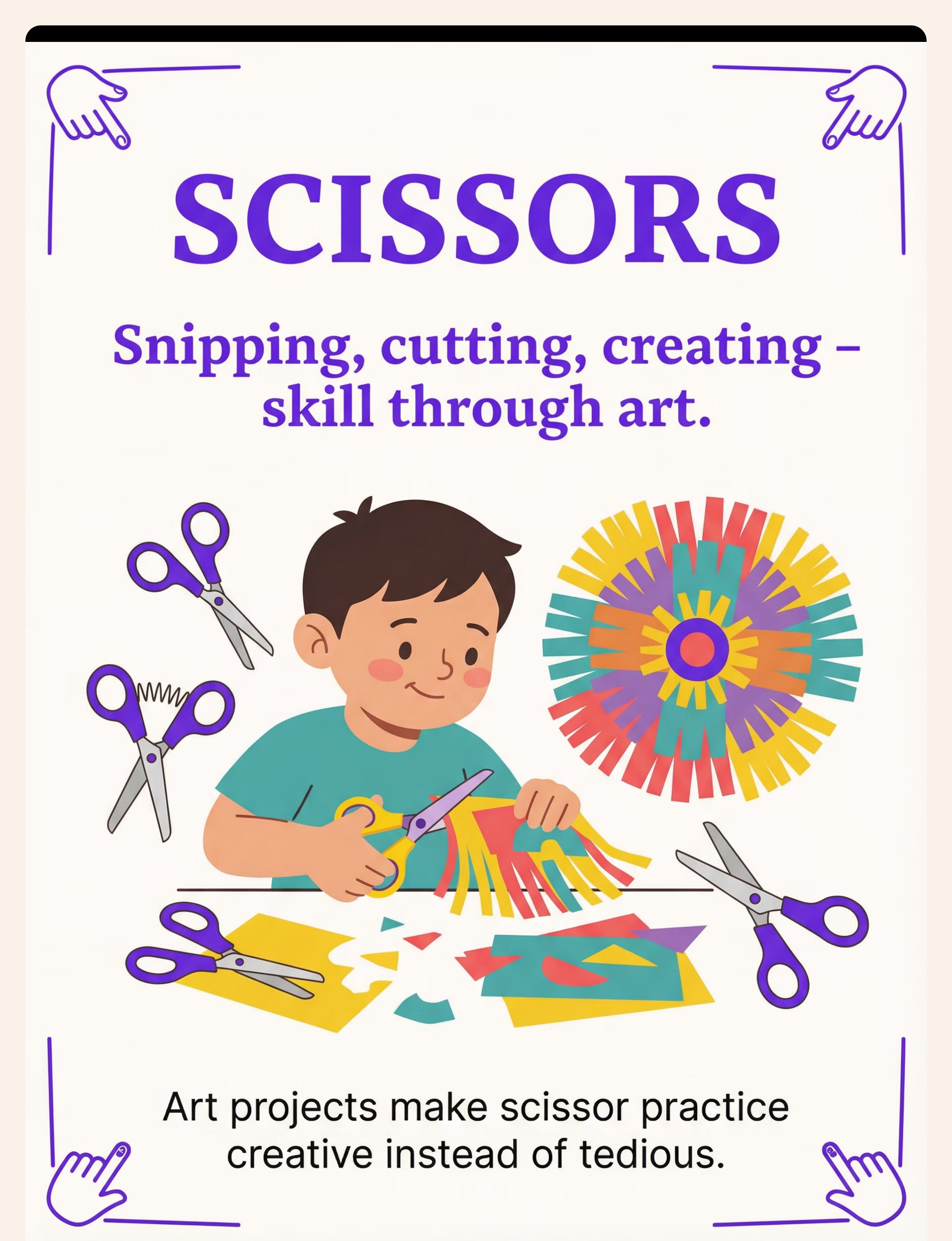
✂️ 6. Scissors & Cutting Activities
Bilateral coordination, in-hand manipulation, hand strength. ₹100–400 | Loop scissors recommended for beginners

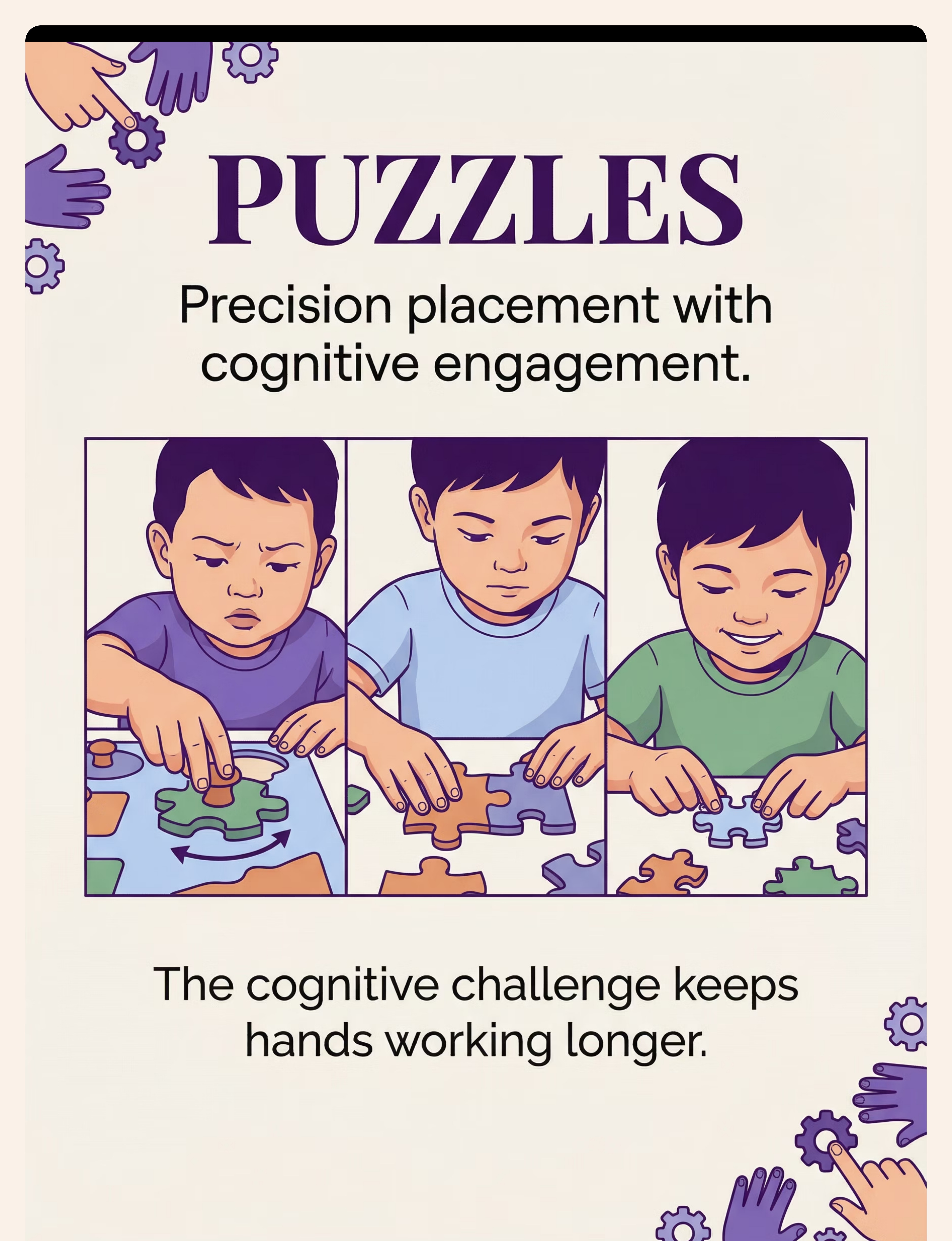
🧩 7. Puzzles & Shape Sorters
Pinch grip, in-hand manipulation, graded release, cognitive engagement. ₹200–1,000
🎨 8. Finger Painting & Sensory Art
Finger isolation, proprioceptive awareness, hand strength. ₹100–400 | DIY: cornstarch + food color

🏠 9. Everyday Life Activities
All fine motor components in authentic context, life skills. ₹0 — uses household items already in your home.

🏠 WHO/UNICEF Equity Principle
Every F-618 Material Has a ₹0 Home Version That Works on the Same Therapeutic Principle
Material | Clinical Version | ₹0 Household Version | Why It Works | |
Play Dough | Therapy Putty (₹350) | Flour + salt + water + oil | Same proprioceptive resistance | |
Building Blocks | LEGO/DUPLO (₹500+) | Cardboard boxes + toilet rolls | Same precision placement demand | |
Threading | Craft bead set (₹300) | Rigatoni pasta + shoelace | Same bilateral threading action | |
Stickers | Sticker book (₹364) | Tape tabs on paper | Same peeling + placement | |
Tongs | Craft tweezers (₹200) | Kitchen tongs / clothespins | Same squeeze-release grip | |
Scissors | Loop scissors (₹150) | Standard child scissors | Same bilateral cutting action | |
Puzzles | Knob puzzle (₹400) | Cardboard cut shapes | Same pinch + rotate + place | |
Finger Paint | Commercial paint (₹200) | Cornstarch + food color | Same sensory-motor feedback | |
Life Activities | Child tools (₹300) | Any household task | Most authentic fine motor |
Homemade Play Dough Recipe (Consortium-Grade): 1 cup flour + ½ cup salt + 2 tbsp cream of tartar + 1 cup water + 1 tbsp oil + food coloring → Cook on medium heat, stirring until ball forms → Knead when cooled. Store airtight 4–6 weeks. Resistance Scale: Less flour = Soft → Standard → More flour = Therapy Putty grade
Zero-cost full session: Pasta threading → Clothespin transfer → Cardboard puzzle → Cornstarch finger paint → Squeeze-bottle plant watering. Total cost: ₹0. Therapeutic value: Identical to ₹2,000 toolkit.

🏠 Environment Engineering
The Right Setup Prevents 80% of Session Failures Before They Start
Environment Setup Checklist
Surface: Table at child's elbow height OR foam mat on floor
Lighting: Natural preferred; bright enough to see fine detail
Sound: Quiet or soft neutral music; no TV, no competing audio
Materials: Pre-arranged within child's reach; one category visible at a time
Distractors removed: Tablets, phones (yours too), other toys not in use
Visual timer: Sand timer or phone timer available
Parent position: 45° beside child — collaborative, not across
Exit clear: Child can see the door; no feeling of being trapped
Environment Tone
Relaxed, curious, unhurried. The setup signals to the child: this is a pleasant space for playing, not a workspace for performing.
The environment itself is a therapeutic tool — often called "the invisible therapist" in sensory integration practice. A well-prepared space reduces the child's need to regulate against competing stimuli and frees their attention for the materials in front of them.
"Parent position: 45° beside child, NOT behind, NOT across — collaborative positioning makes you a co-player, not an overseer."

ACT III — The Execution
✅ Pre-Flight Readiness Check
The Best Session Is One That Starts Right
A 60-second readiness check before every session determines whether to proceed, modify, or postpone. This check is not optional — it IS the therapy. Pushing a session when the child isn't ready doesn't build resilience. It builds avoidance.
Check | Green ✅ | Amber ⚠️ | Red ❌ | |
Fed? | Meal within 2 hours | Light snack recently | Hungry / just ate large meal | |
Rested? | Slept well | Slightly tired | Overtired / just woken | |
Regulated? | Calm, engaged | Mildly unsettled | Distressed, escalating | |
Last meltdown | >3 hours ago | 1–3 hours ago | <1 hour ago | |
Sensory state | Receptive | Mildly sensitive today | High sensory defensiveness | |
Engagement | Showing interest | Neutral | Actively resisting |
🟢 GO — Full Session
≥5 Green indicators. Proceed with full 15–20 minute session.
🟡 MODIFY — Short Session
Mix of Green + Amber. Soft, preferred materials only. 5–8 minutes.
❌ POSTPONE
Any Red, or ≥3 Amber. Offer a preferred calming activity instead. This is wisdom, not failure.
STEP 1
The Invitation
Step 1 — The Invitation
Timing: 30–60 seconds | Principle: Low-demand, high-interest entry
"Hey, I've got something fun here. Want to see what it is?"
Set one material visually accessible — don't hand it; let curiosity pull. The child's eye contact with the material is the first micro-engagement.
"I was thinking we could make some dinosaurs / necklaces / towers — do you want to try?"
Offer a choice framing, not a directive. The child retains perceived autonomy — a core ABA pairing principle.
"You don't have to if you don't want. But look at this..."
Reduce demand; increase curiosity. Most children approach the material independently within 1–2 minutes of low-pressure exposure.
Acceptance Cues ✅
- Reaches for material
- Leans forward with interest
- Makes a comment or question
- Begins playing independently
If Resistance Occurs
"Okay, I'll be here if you want to join." Set the material out accessibly and engage with it yourself. Most children will approach independently when demand pressure is removed completely.

STEP 2
The Engagement
Step 2 — The Engagement
Timing: 1–3 minutes | Principle: Child-led exploration, therapist follows
For Play Dough
"Look at this — it's so squishy. I'm going to squeeze it... wow, it does this shape. What should we make?" Begin narrating with genuine curiosity. The child's brain mirrors adult engagement.
For Building Blocks
"How tall do you think we can build? Let's find out." Open-ended challenge framing activates intrinsic motivation without performance demand.
For Tongs Transfer
"These pom-poms need to move over here. Can you use these special grabbers to do it? I wonder if it's harder than it looks..." Natural framing introduces the therapeutic constraint invisibly.
Full Engagement
Child initiates, requests, problem-solves — follow their lead entirely
Tolerance Engagement
Child participates when guided — more structure, more enthusiasm
Passive Tolerance
Child is present but not initiating — simplify the task, increase the reward value
First moment of positive engagement → warm, immediate, specific praise within 3 seconds: "Yes! Look at you squeezing that — that's amazing!"
STEP 3 — CORE ACTION
Step 3 — The Therapeutic Action
Timing: 5–12 minutes | This is the active ingredient — the session's therapeutic core
Play Dough
Roll snakes (palm strength) → Pinch small pieces (finger isolation) → Poke individual fingers (proprioception) → Hide objects and dig (grip + search) → Flatten with thumb only (thumb opposition) → Create meaningful shapes (sustained engagement)
Building Blocks
Stack with controlled placement → Connect interlocking blocks (precision pinch) → Build to model (visual-motor integration) → Build with non-dominant hand → Demolish and rebuild (graded force + control)
Threading
Thread large beads on shoelace → Reduce bead/string size progressively → Create color patterns → Lace through card holes → Make "necklace for family member" (purpose creates motivation)
Stickers & Stamps
Peel sticker from backing (finger isolation + pinch) → Place on specific target (eye-hand accuracy) → Stamp with controlled pressure (graded force) → Create sticker art (sustained engagement)
Tongs & Tweezers
Transfer pom-poms bowl to bowl → Sort by color into compartments → Race against timer → Feed "pretend animal" (theme adds motivation) → Progress from large tongs → tweezers → fine tweezers

STEP 3 — CONTINUED
Step 3 — Therapeutic Action (Materials 6–9)
Scissors
Snip play dough snakes (safest first step) → Snip straws → Cut paper strips → Cut along thick lines → Cut simple shapes → Create paper art (motivation through creativity). Always supervise.
Puzzles
Insert knob puzzle pieces (tripod grip on knob) → Rotate piece to fit (in-hand manipulation) → Complete without picture clue → Progress piece count as skill develops. Celebrate each placement.
Finger Painting
Paint with single finger (isolation) → Make circles with thumb (opposition) → Press firm-soft-firm (graded force) → Draw letters/shapes in paint (pre-writing readiness)
Everyday Life Activities
Stir ingredients → Spread butter on bread → Peel banana → Button shirt → Water plant with squeeze bottle → Sort laundry → Any real task with authentic purpose. The most transferable fine motor practice.
Returns After Distraction
Child returns to task after brief distraction = appropriate engagement level
Requests "More"
Child requests "again" or "more" = optimal engagement — you've found the sweet spot
Modifies Independently
Child changes the activity independently = skill generalization beginning

STEP 4
Repeat & Vary
Step 4 — Repeat & Vary
Timing: 3–5 minutes | Principle: Dosage without tedium
Optimal Daily Dose: Multiple 5–10 minute bursts throughout the day > one session of 30+ minutes that ends in resistance. 3–5 good repetitions of target action per material → vary the task → move to next material or end while engaged.
Weekly Variation Playbook
Day | Play Dough | Tongs | Threading | |
Mon | Make snakes | Pom-poms transfer | Large beads | |
Tue | Hide treasure | Sorted by color | Pattern sequence | |
Wed | Sparkle dough | Ice cube tray | Pasta + string | |
Thu | Tools + cutters | Timer race | Lacing card | |
Fri | Child's choice | New object type | Make gift necklace |
Satiation Indicators (child has had enough): Pushing material away • Looking for other activities • Dropping precision • Giving "all done" signal. Clinical Principle: "3 good repetitions are worth more than 10 forced ones."

STEP 5
Reinforce & Celebrate
Step 5 — Reinforce & Celebrate
Timing: Within 3 seconds of desired behavior | Principle: Immediate, specific, enthusiastic
Verbal Praise
"YES! You did it! Look at that grip — so strong!" / "That was perfect threading — I can't believe how focused you were!" / "Your hands are getting SO good at this!"
Behavior-Labeled Praise
"I noticed you used your pinching fingers on that one — that's exactly right!" / "You kept trying even when it was tricky. That's the brave way."
Natural Consequence
"Look at what you made! Let's show it to Dad/Grandma." / "That necklace is going on your shelf — you earned that."
Sticker Reward
Visual, tactile, motivating — and peeling the sticker IS a fine motor activity (Reward Sticker Book ₹364)
Activity Token
Choose next activity — reinforces autonomy alongside behavior
Parent Enthusiasm
Free and the most powerful reinforcer available. Never underestimate it.
📞9100 181 181 — Ask a BCBA about personalizing your reinforcement menu. Celebrate the attempt, not just the success. The attempt IS the therapeutic event.
STEP 6
The Cool-Down
Step 6 — The Cool-Down
Timing: 1–2 minutes | Principle: No session ends abruptly
Abrupt session endings cause dysregulation spikes, negative associations with the activity, and resistance at next session's start. The cool-down signals: "This was a complete, safe experience. You are safe. This was good."
Transition Warning
"Two more [snakes / transfers / pieces], then we're all done for now." Show visual timer actively counting down 2–3 minutes before ending.
Cool-Down Activity
Heavy proprioceptive input: press palms flat on table together, push for 10 seconds. Shake hands out: "Shake out all the hard work!" Or brief hand massage / pressing palms.
Material Put-Away Ritual
"Let's put the [dough/blocks/beads] to sleep. Can you help?" Child participation in cleanup IS fine motor practice — picking up, placing in container, closing lids.
Closing Ritual
Same ending sequence every session creates safety and predictability. "Great work today. I'm proud of you." + specific praise → transition to next preferred activity.
If child resists ending: "Two more [actions], then the [material] has a rest. It'll be here tomorrow." Never promise tomorrow unless you mean it — predictability builds trust.
📊 Data Capture
Within 60 Seconds of Session End
60 Seconds of Data Now Saves Hours of Guessing Later
3 Data Points — No More
Point 1: Engagement Level (1–5)
- 1 = Refused / avoided
- 2 = Tolerated
- 3 = Participated
- 4 = Initiated
- 5 = Requested more
Point 2: Duration of active engagement (minutes actually working, not just present)
Point 3: Material(s) used + child's response (e.g., "Play dough: high engagement | Scissors: some resistance")
Quick Tracking Format
DATE: _____ | MATERIAL: _____
ENGAGEMENT: /5 | DURATION: ___min
OBSERVATION: ________________
NEXT SESSION PLAN: __________Patterns emerge across 7–10 sessions. Single sessions don't tell the story. The data you collect today shapes your personalized F-619 and F-620 recommendations via GPT-OS®.

🔧 Troubleshooting
Session Abandonment Is Not Failure. It's Data. Here's What to Do With It.
Problem 1: Child refused to engage at all
Why: Poor timing (hungry, tired, overstimulated) or demand pressure too high. Solution: Switch to child's highest-preference activity. Reduce goal to "touch the material once." Try again tomorrow at a different time of day.
Problem 2: Engaged briefly then lost interest
Why: Task too easy (boring) or too hard (frustrating), or session ran past attention window. Solution: Note which materials held interest. Shorten to 3-minute bursts. Introduce novelty variation.
Problem 3: Became frustrated with the material
Why: Challenge level too high; task demand exceeded current skill. Solution: Move one step easier (larger objects, simpler action). Success must come before challenge.
Problem 4: Child kept putting material in mouth
Why: Oral sensory seeking, developmental mouthing, or tempting material. Solution: Switch to edible-safe materials (yogurt paint, cornstarch dough, Cheerio threading). Consult SLP for oral sensory input strategy.
Problem 5: Child upset when session ended
Why: Session was successful (positive sign!) but transition was abrupt. Solution: Implement transition warning system (Step 6). Use visual timer. Create consistent ending ritual.
Problem 6: Only wants one material and resists others
Why: Preferred material is highly motivating — useful data. Solution: Use preferred material as entry point every session. Gradually introduce new material alongside the preferred one.
Problem 7: No visible progress after 2–3 weeks
Why: Timeline expectations may need calibration; or technique needs professional input. Solution: Review engagement score data. If engagement improving but skill isn't, continue. If stagnant, call 9100 181 181.

⚙️ Personalization Engine
F-618 Is a Framework. Your Child Is the Blueprint.
Age-Based Adaptations
Ages 2–3
Large objects, whole-hand actions, 3–5 minute sessions, floor-based play. Focus on exploration and tolerance.
Ages 3–5
Medium objects, emerging precision, 5–10 minutes, table-based. Begin introducing therapeutic constraints naturally.
Ages 5–8
Smaller objects, precision focus, 10–15 minutes, instruction-following. Pre-academic skills become primary targets.
Bad Day Version
One material, 5 minutes, child's choice, no performance expectation. Any contact = success.
Breakthrough Day Version
Add complexity, introduce new material alongside familiar, extend session naturally.

ACT IV — The Progress Arc
📅 Week 1–2
Weeks 1–2: Tolerance Is the Win. Not Mastery.
15%
Progress at Week 2
Neural familiarity is building. The pathway is being formed — the skill follows the pathway.
What to Look For ✅
- Child stays near the material 30 seconds longer than Week 0
- Resistance begins later in the session than before
- Child accepts a specific material type without visible distress
- One spontaneous reach for any material
- Any voluntary engagement, however brief
What Is NOT Expected Yet ✗
- Significant improvement in grip or pinch strength (too early)
- Extended engagement periods (still building)
- Requesting the activity independently
- Generalization to other contexts
"You've run 10+ micro-sessions this week. Each one built neural familiarity. You're building the pathway — the skill will follow the pathway." If your child tolerates the material for 3 seconds longer than last week — that is measurable, real, neurological progress.
Data Checkpoint: Review your session notes. Is engagement score trending from 1–2 toward 2–3? That's the signal the approach is working.

📅 Week 3–4
Consolidation
Weeks 3–4: Neural Pathways Are Forming. Watch for These Signs.
40%
Progress at Week 4
Consolidation is underway. Anticipation, preference, and self-correction are the hallmarks of this phase.
Anticipation
Child reaches for materials before session begins — the activity has become a predictable, desired event in their routine.
Preference Emerging
Child asks for a specific material ("dough!") or leads toward the activity corner independently.
Extended Duration
Engagement now sustaining 5+ minutes without redirection — a significant neurological milestone.
Self-Correction
Child adjusts grip or technique when it doesn't work — without adult prompt. Motor learning is internalizing.
"You may notice you're more confident too. Your instincts about timing and adaptation are becoming informed by real data. You're becoming a precision home therapist."

📅 Week 5–8
🏆 Mastery Zone
Weeks 5–8: Mastery Unlocked — Look for These Badge Criteria
75%
Week 5–8 Progress
Mastery zone. Skills are becoming automatic and beginning to generalize to daily life contexts.
1
Multi-Material Engagement
Child engages with 3+ different F-618 materials without prompting across a single week.
2
Sustained Focus
Session duration reaches 10–15 minutes with maintained focus and minimal adult redirection.
3
Grip Strength Observable
Can hold pencil/crayon for 2+ minutes without fatigue — a direct pre-academic readiness indicator.
4
Fingertip Pinch
Pinch is fingertip-based (not whole-hand) for small objects 80%+ of the time, without reminders.
5
Bilateral Coordination
One hand stabilizes while the other works — without being reminded. Both hands collaborating spontaneously.
🏅F-618 FINE MOTOR PLAY — CORE MASTERY UNLOCKED — Child demonstrates play-based fine motor engagement with 3+ material categories → Ready for F-619: Bilateral Coordination Activities
🎉 Celebrate This Win
You Did This. Your Child Grew Because of Your Commitment.
Over the last 5–8 weeks, you showed up consistently — on tired evenings, on difficult days, through the sessions that felt pointless and the breakthroughs that took your breath away. You converted resistance into tolerance, tolerance into engagement, and engagement into skill.
"Your child's hands are stronger. Their confidence is higher. Their world is larger. That happened because a parent — you — chose to act."
✅ Avoidance → Participation
Fine motor engagement transformed from active resistance to voluntary, joyful play
✅ Hand Strength Built
Measurably increased through play-based dosage over consistent daily micro-sessions
✅ Bilateral Coordination
Emerging in daily activities — both hands working together spontaneously
✅ Therapy = Play
The conflict has been resolved — they are the same thing now, in your home
Family Celebration Suggestion: Display your child's best play creation — a sculpture, bead necklace, or building — somewhere visible. Every time they see it, the accomplishment is reinforced. Journal Prompt: "Week 1: My child [describe early behavior]. Week 8: My child [describe current behavior]. The difference is: ___"
🚨 Clinical Guardrails
Trust Your Instincts — If Something Feels Wrong, Pause and Ask
🔴 1. Consistent Regression Despite Consistent Practice
After 6+ weeks, engagement has not improved at all AND fine motor function appears to be declining. Action: Teleconsult with Pinnacle OT — may indicate an underlying condition not addressed by F-618 alone.
🔴 2. Hand or Wrist Pain During Activities
Child verbally reports or behaviorally shows pain during fine motor activities. Action: Stop all fine motor practice immediately. See NeuroDev pediatrician to rule out hypermobility, joint issues, or injury.
🔴 3. Unusual Hand Dominance Patterns
Strong hand dominance before age 12 months OR no dominance by age 5 can indicate neurological asymmetries. Action: Developmental assessment at nearest Pinnacle center.
🔴 4. Significant Impact on Daily Self-Care or School
Child cannot independently eat, dress, or participate in classroom activities despite 8 weeks of consistent practice. Action: Formal OT evaluation and individualized intervention plan.
🔴 5. Self-Injurious Behavior During Sessions
Any self-directed harm in context of fine motor frustration. Action: ABA consultation immediately. Call 9100 181 181 now.
📞9100 181 181 — FREE | 16+ languages | 24×7
🗺️ Developmental GPS
Every Technique Is a Waypoint. Here Is Where F-618 Sits in the Journey.
If Sensory Seeker
→ F-619 Bilateral Coordination is primary next step. Ready to add complexity and dual-hand demands.
If Sensory Avoider
→ Return to F-617 Sensory Integration for supplementary consolidation before advancing.
If Self-Care Is Priority
→ Jump to F-625 Self-Care Fine Motor as parallel track alongside continued F-618.
🔗 Fine Motor Domain
Related Techniques — You Already Have Materials for Some of These
Technique | Code | Level | Materials You Already Own | |
In-Hand Manipulation Skills | F-616 | 🔵 Core | Coins, puzzle pieces from F-618 toolkit | |
Fine Motor + Sensory Integration | F-617 | 🔵 Core | Play dough, sand (same as F-618) | |
Fine Motor Play Ideas (You Are Here) | F-618 | 🔵 Core | All 9 materials | |
Bilateral Coordination Activities | F-619 | 🔵 Core | Threading, scissors from F-618 | |
Visual-Motor Integration Games | F-620 | 🟡 Intermediate | Puzzles, building blocks from F-618 | |
Self-Care Fine Motor Skills | F-625 | 🟡 Intermediate | Everyday items, sticker book from F-618 |
Your F-618 sticker book → works for F-625 (buttoning practice reward) | Your play dough → works for F-617 (tactile desensitization) | Your tongs → works for F-619 (bilateral tool coordination). Your toolkit stretches far.
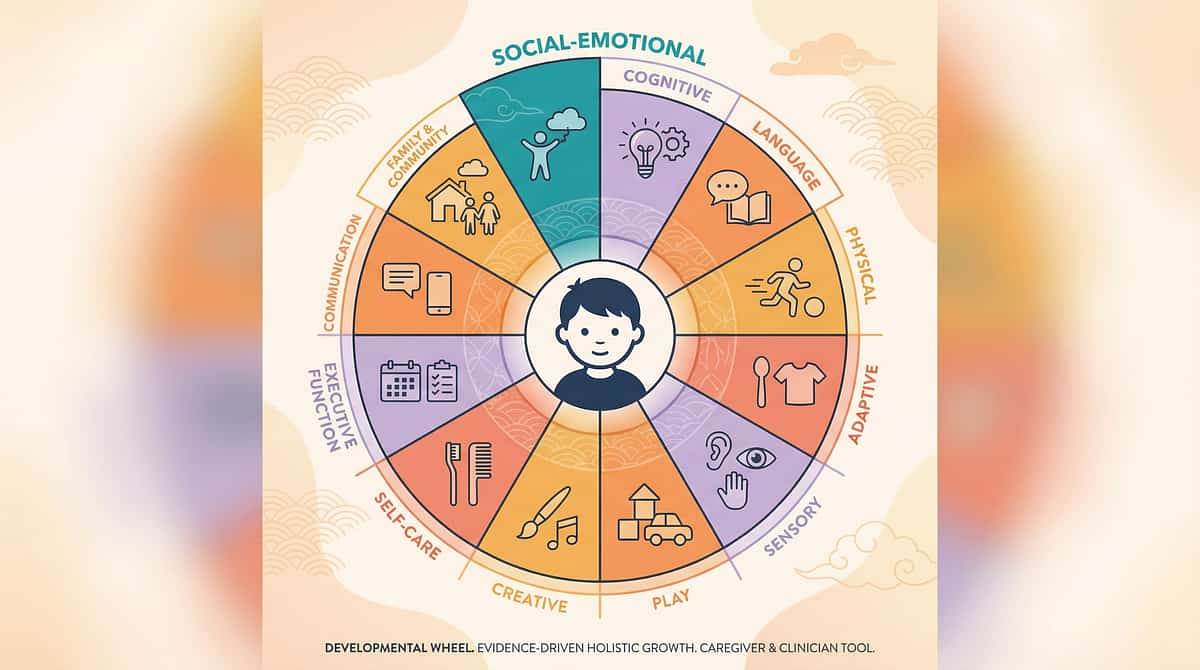
🌐 Whole-Child View
This Technique Is One Piece of a Larger Plan
Fine motor development doesn't exist in isolation. A child who struggles with hand skills may also have sensory processing differences (Domain A), self-care challenges (Domain I), cognitive engagement variations (Domain H), and play skill development differences (Domain G). GPT-OS® tracks all 12 domains simultaneously — because your child develops as a whole person.
ACT V — Community & Ecosystem
💚 Real Families. Real Outcomes.
Three Families Who Started Where You Are Now

Arjun, 4 years — Hyderabad
Before: Would run from any table activity. OT worksheets went untouched. "Fine motor exercises" meant meltdowns within 2 minutes.
Intervention: OT introduced play dough as "dinosaur creation time." No mention of therapy. 7-minute sessions, child's lead.
After Week 6: Arjun spent 20 minutes daily creating dinosaur scenes. Grip strength measurably improved. Began requesting "dough time" independently.
Intervention: OT introduced play dough as "dinosaur creation time." No mention of therapy. 7-minute sessions, child's lead.
After Week 6: Arjun spent 20 minutes daily creating dinosaur scenes. Grip strength measurably improved. Began requesting "dough time" independently.
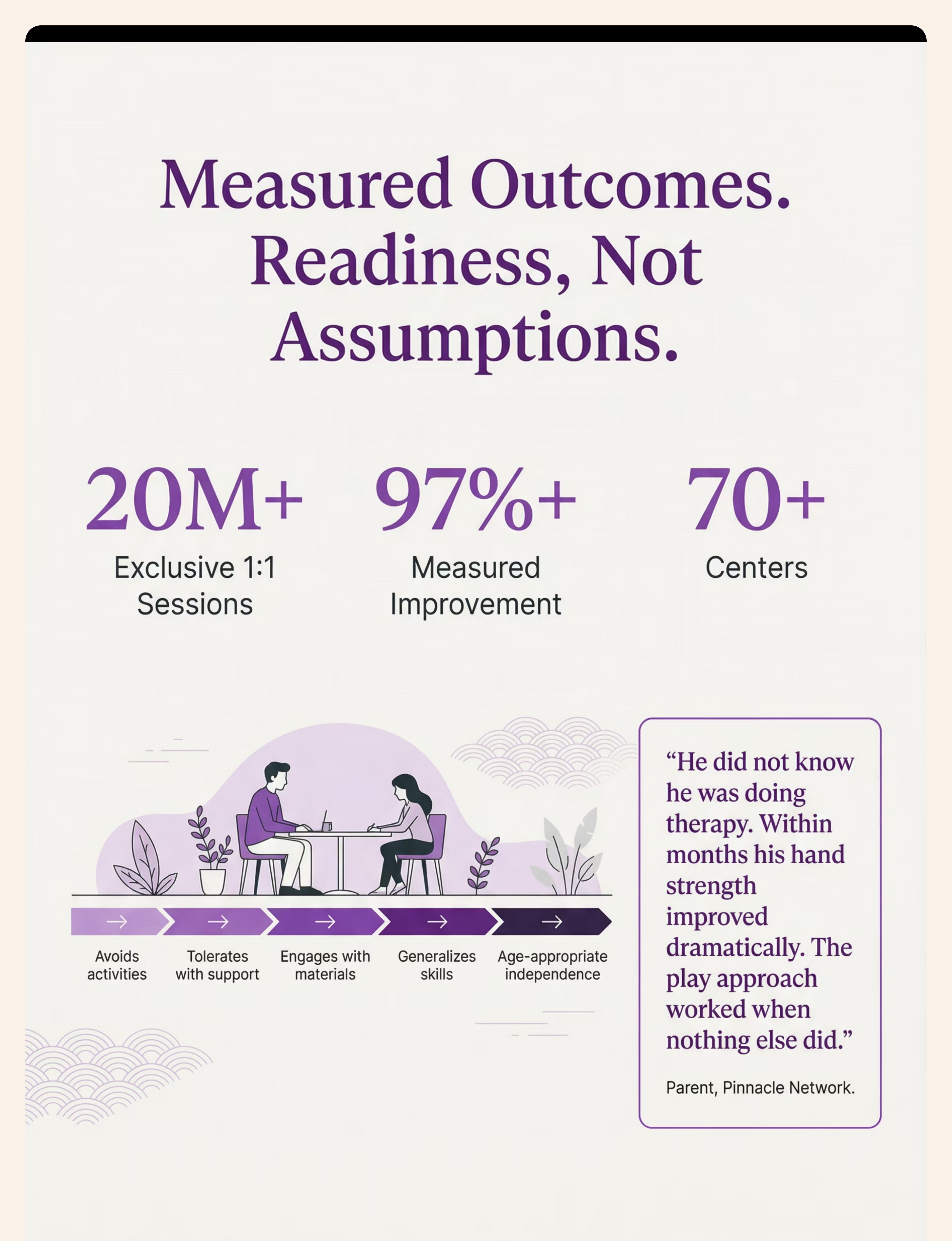
"He didn't know he was doing therapy. Within months, his hand strength improved dramatically. The play approach worked when nothing else did."

Priya, 3.5 years — Bengaluru
Before: Strong tactile avoidance — refused wet, sticky, or resistive materials. Avoided all craft activities at playschool.
Intervention: Started dry: blocks, puzzles, sticker books. Gradual tactile introduction over 4 weeks before first play dough contact.
After Week 8: Tolerates finger painting with one finger. Voluntarily peels stickers. Attempts to button shirt independently.
Intervention: Started dry: blocks, puzzles, sticker books. Gradual tactile introduction over 4 weeks before first play dough contact.
After Week 8: Tolerates finger painting with one finger. Voluntarily peels stickers. Attempts to button shirt independently.
"Desensitization through preferred materials is the fastest path. We never pushed. We invited." — Therapist's Notes

Kiran, 6 years — Chennai
Before: Scissors use was completely avoidant. Pencil grip caused fatigue in under 2 minutes. Academic performance impacted.
Intervention: Play-based cutting: snipping play dough snakes, cutting straws, creating paper art.
After Week 7: Cuts along straight lines with standard child scissors. Colors for 8-minute periods. Teacher reports improved writing endurance.
Intervention: Play-based cutting: snipping play dough snakes, cutting straws, creating paper art.
After Week 7: Cuts along straight lines with standard child scissors. Colors for 8-minute periods. Teacher reports improved writing endurance.
"I stopped trying to make him do 'therapy' and started making him want to play. That was the entire shift."
Illustrative cases based on composite clinical patterns from Pinnacle Network. Individual outcomes vary.

🏥 Professional Support
70+ Pinnacle Centers. One National Helpline. Zero Barriers to Getting Help.
🖐️ Primary Specialist
Pediatric Occupational Therapist — Fine Motor, Sensory Integration. Your first and most important clinical partner for F-618.
📊 ABA/BCBA
Reinforcement systems, data collection, motivation-based session design. Essential for adherence.
🧠 NeuroDev Pediatrician
Medical oversight, red flag monitoring, co-occurring condition assessment. Consulted when red flags arise.
Service Option | Best For | How to Access | |
In-Center OT | Full assessment + supervised sessions | Book at nearest Pinnacle center | |
Teleconsultation | Guidance + troubleshooting | pinnacleblooms.org/consult | |
Home Program Review | Check current approach | Via helpline | |
AbilityScore® Assessment | Baseline + personalized plan | Any Pinnacle center |
📞9100 181 181 | FREE | 16+ languages | Available NOW
📚 Research Library
The Science Behind Fine Motor Play Intervention — Direct Sources
PMC11506176 — PRISMA Systematic Review (2024)
16 studies (2013–2023): Sensory integration + play-based fine motor intervention confirmed as evidence-based practice for ASD. Fine motor outcomes among primary measured benefits. View on PubMed →
PMC10955541 — Meta-Analysis, World J Clin Cases (2024)
24 studies: SI therapy effectively promotes social skills, adaptive behavior, sensory processing, fine and gross motor skills. Strongest category evidence base. View on PubMed →
PMC9978394 — WHO/UNICEF CCD Package
Evidence-based caregiver interventions implemented in 54 LMICs. Household-material-based approach validated across diverse populations. View on PubMed →
Padmanabha et al., Indian J Pediatr (2019)
Indian RCT: Home-based sensory-motor interventions by trained parents showed significant outcomes in Indian pediatric populations. DOI: 10.1007/s12098-018-2747-4. View at DOI →
NCAEP (2020) — National Clearinghouse
Video modeling and play-based approaches classified as evidence-based practices for autism. Multi-modal parent learning improves skill acquisition. NCAEP Report →
Evidence Grade Summary: Level I (Systematic Review) evidence base for play-based fine motor intervention. Home-applicable. Parent-administrable. WHO/UNICEF aligned for 197 countries.

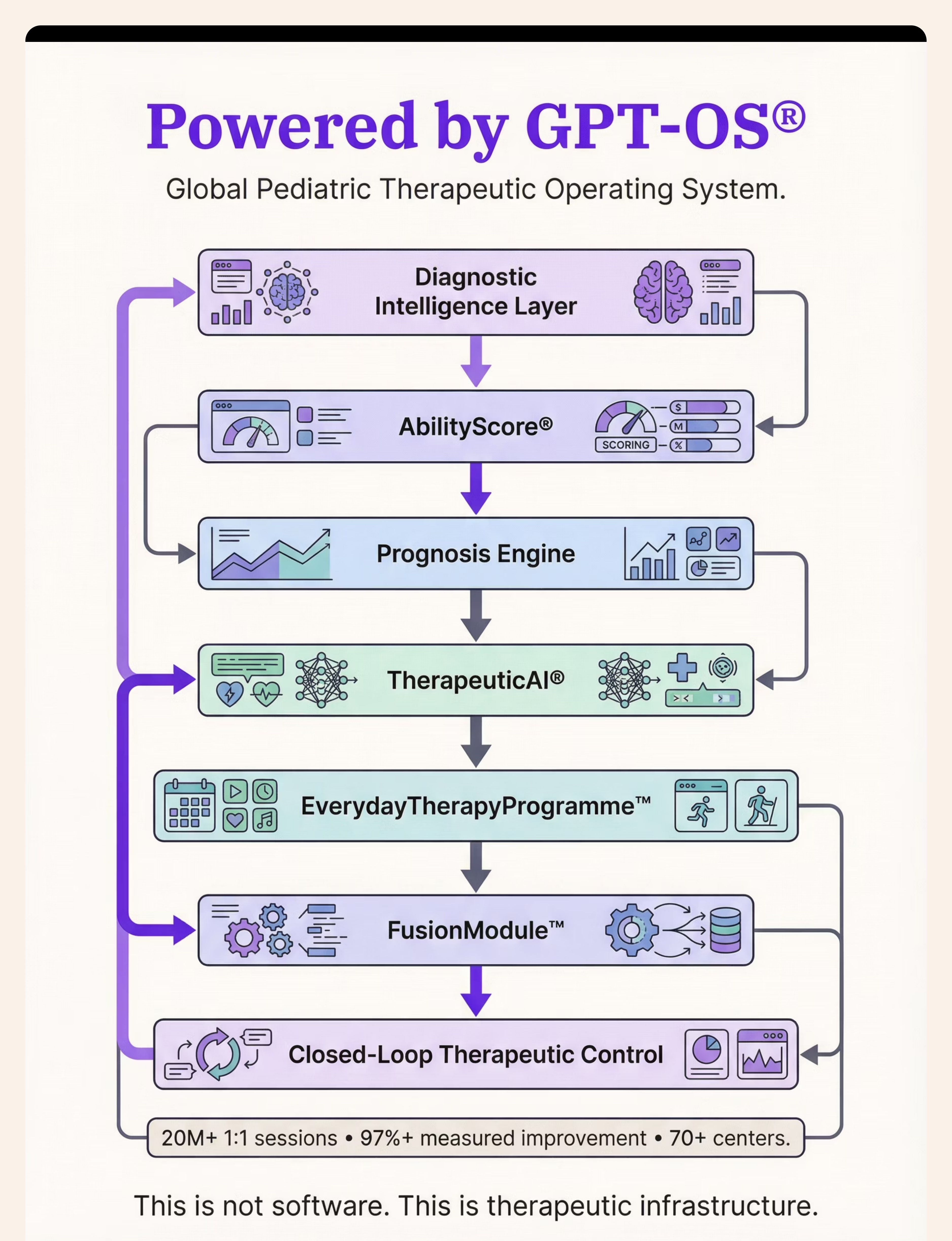
⚙️ GPT-OS® Intelligence Layer
Your Data Helps Every Child Like Yours

🎬 From the 999 Reels Content Ecosystem
Watch the Reel That Brought This Page to Life
Reel Identity
Reel ID: F-618
Domain: F — Fine Motor Development
Series: Fine Motor Development in Children
Episode: 618 of 999
Duration: 60–75 seconds
Domain: F — Fine Motor Development
Series: Fine Motor Development in Children
Episode: 618 of 999
Duration: 60–75 seconds
Reel Content Map
- 0:00–0:06 Hook: "When therapy feels like work, play becomes the therapist"
- 0:06–0:51 All 9 materials — 4–5 seconds each with voiceover
- 0:51–0:55 CTA: Save, Share, Follow
- 0:55–1:15 GPT-OS® and Pinnacle closure
About This Reel
A Pinnacle occupational therapist demonstrates the actual therapeutic actions described on this page — play dough manipulation, tong transfer games, threading, sticker placement, and more — in a real home setting with a real child. The theory on this page becomes visible practice.
Multi-Modal Learning
This evidence page (reading) + the reel (visual + audio) + your implementation (kinesthetic) = three-modality parent learning that produces the fastest skill acquisition. NCAEP (2020) classifies video modeling as evidence-based practice for autism.

📤 Share With Your Family
The More Caregivers Who Know This, the Faster Your Child Progresses
Consistency across caregivers multiplies impact. When everyone who spends time with your child understands the approach, therapeutic dosage multiplies naturally throughout the day — without adding sessions.
"Explain to Grandparents" Version
"[Child name] is working on building hand strength through play. These 9 activities look like regular playing — but they're actually helping [his/her/their] hands get stronger. When [child name] plays with play dough, blocks, stickers, or tongs, that's exactly what the therapist wants. Let [child name] play and say: 'I love watching your hands work!'"
Teacher Communication Template
"[Child name] has an OT-guided fine motor development program at home. In class, any opportunity for manipulative play (play dough, threading, building, cutting) supports [his/her/their] development. Please encourage fingertip grip rather than whole-hand grip when using tools. Thank you for your collaboration."

ACT VI — The Close
❓ Frequently Asked Questions
Your Questions Answered — Before You Have to Ask
Q1: How long before I see results?
Most parents notice tolerance improvements within 2 weeks. Skill improvements become visible around weeks 4–6. Full motor integration typically occurs at 8–12 weeks of consistent practice. Timeline varies by child's starting point and consistency of home practice.
Q2: My child only engages for 3 minutes. Is that enough?
Yes. Three focused, engaged minutes of play-based fine motor work is clinically meaningful. Motivated repetition — even brief — builds myelin faster than extended reluctant practice. Build duration gradually. Do not force extensions that produce resistance.
Q3: Should I tell my child we're doing "therapy"?
This is a clinical judgment, not a rule. If your child responds well to "this helps your hands get strong," use it. If it creates performance anxiety, describe it as "play time" and let the development happen invisibly.
Q4: Which material should I start with?
Start with your child's highest-interest category. Sensory seekers: play dough or finger painting. Sensory avoiders: blocks or puzzles. Highly motivated children: stickers. The first material establishes the pattern — make it one they'll say yes to.
Q5: Can both parents run sessions?
Both parents can and should run sessions — this is ideal for consistency. Use the Card 37 Family Guide to ensure both use the same approach. Consistency of technique matters more than consistency of person.
Q6: My child does great at home but not in therapy. Normal?
Completely normal, and clinically positive. Skills generalize from easiest context (home) to harder contexts (clinic) over time. Inform your OT of the home performance — they can bridge the gap in clinic sessions.
Q7: Does this work for non-autistic children with fine motor delays?
Yes. F-618 is designed for autism and neurodevelopmental conditions but is equally applicable to any child with fine motor challenges. The play-based approach is the WHO/UNICEF recommended approach for all pediatric populations.
Q8: When should I seek professional evaluation?
See Card 29 (Red Flags) for specific thresholds. Generally: seek evaluation if fine motor difficulties impact daily self-care, pre-academic readiness, or quality of life after 8 weeks of consistent home practice. Call 9100 181 181 for free consultation.

✅ Your Next Step
Your Child's Development Doesn't Wait. Neither Should You.
The window of maximum neuroplasticity for fine motor development is now. Every day of engaged, play-based practice compounds toward the milestone your child deserves. You have the knowledge. You have the materials. You have the evidence. The next step is simply to begin.
🏥 Validated by the Pinnacle Blooms Consortium
🖐️ OT • 🗣️ SLP • 📊 ABA • 📚 SpEd • 🧠 NeuroDev
20M+ Sessions • 97%+ Improvement • 70+ Centers • GPT-OS® Powered
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
Preview of 9 materials that help with fine motor play ideas Therapy Material
Below is a visual preview of 9 materials that help with fine motor play ideas therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

🌸 The Pinnacle Promise
From Fear to Mastery. One Technique at a Time.
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
✅ WHO/UNICEF Aligned
Evidence-Based • Clinically Validated • Parent-Proven
🖐️ OT | 🗣️ SLP | 📊 ABA | 📚 SpEd | 🧠 NeuroDev | 🔬 CRO
Multi-Disciplinary Consortium. All Five Disciplines. Every Child.
This content is educational and informational in nature. It does not replace evaluation, diagnosis, or treatment by licensed healthcare providers. Fine motor difficulties may indicate underlying neurodevelopmental conditions requiring professional assessment. If your child has significant difficulty with hand skills affecting daily activities, school performance, or quality of life, please consult qualified occupational therapists or developmental specialists. Individual outcomes vary. Statistics represent aggregate outcomes across 70+ Pinnacle centers and 21 million therapy services.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, and FusionModule™ are proprietary systems of Pinnacle Blooms Network®.
care@pinnacleblooms.org | 📞 9100 181 181 | techniques.pinnacleblooms.org