
9 Materials That Help With Fecal Smearing
Fecal smearing (scatolia) has a function — sensory, communicative, or medical. Discover 9 evidence-based materials that address the cause. Practical home strategies from India's largest paediatric therapy consortium. 20M+ sessions. 97%+ improvement.
D-420
Behavioural Support
Ages 2–12
Fecal Smearing

ACT I — THE RECOGNITION MOMENT
"The smell hits me before I see it. My stomach drops every time."
You searched for help in the dark. You found it.
It's 3 AM. You find it — on the wall, on the bedding, hidden behind the headboard. You've cleaned this before. Many times. You do it in silence, crying quietly, wondering what you're doing wrong. At therapy reviews, you hesitate to even say the word. You've watched other parents recoil when you try to describe it. Even some professionals seem uncomfortable. So you manage it alone.
You are not failing. Your child is not broken. This behaviour has a function — and once that function is understood, it can be addressed. Systematically. Scientifically. At home.
🩺Fecal Smearing / Scatolia — Multi-Material Intervention System
"The behaviour no one talks about. The help you actually need."
"The behaviour no one talks about. The help you actually need."
"You are not failing. Your child's nervous system is speaking. We heard it."
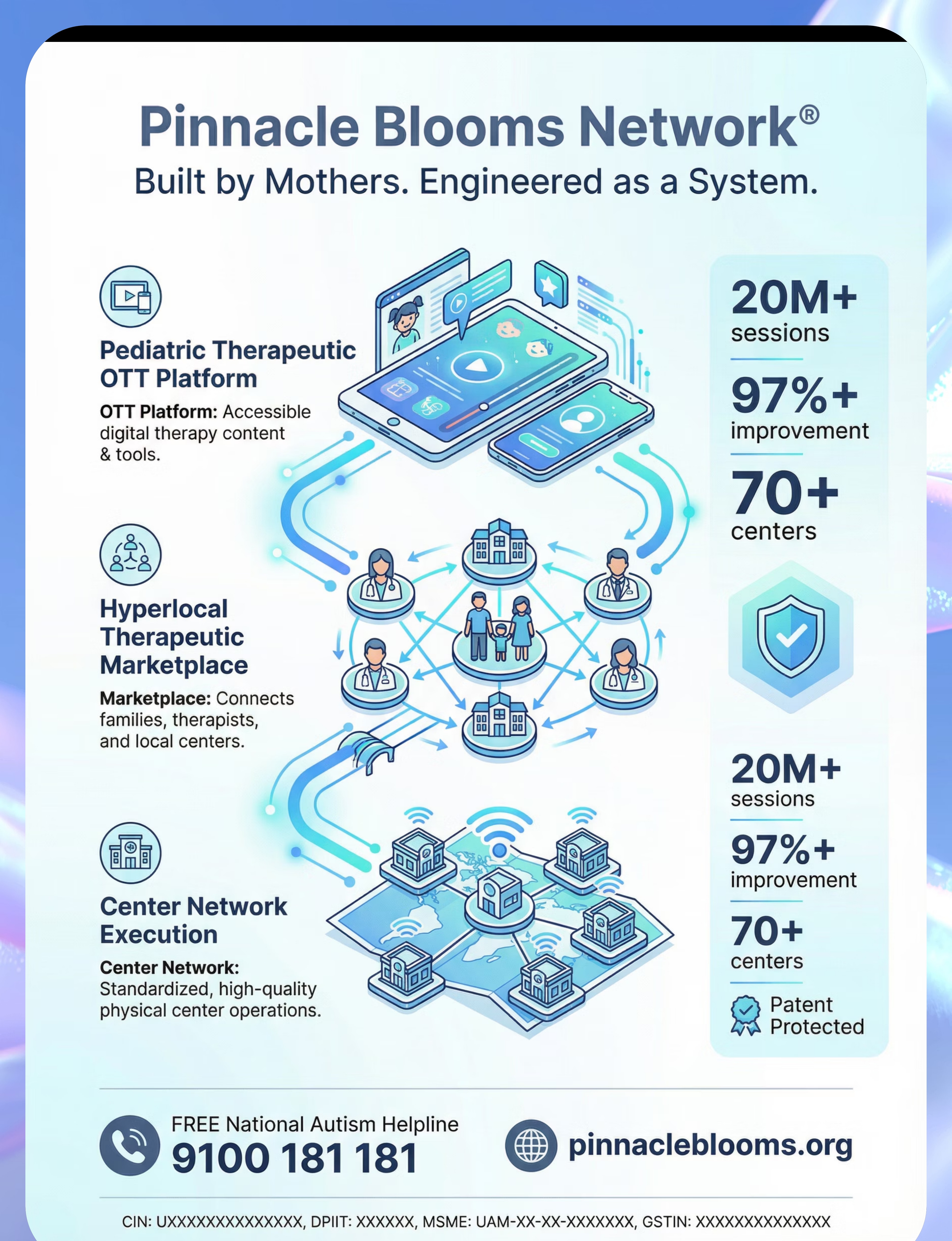
🏥 Pinnacle Blooms Consortium
70+ centres | 20M+ sessions | India's largest paediatric therapy network
📍 D-420 Series
Challenging Behaviours & Functional Alternatives — Episode 420
🔬 WHO NCF 2018
Early identification and parental awareness directly impacts outcomes

You Are Among Millions. This Is More Common Than Anyone Admits.
Fecal smearing — clinically termed scatolia — is one of the most underreported challenges in paediatric developmental care. Research documents it across autism spectrum disorder, intellectual disability, and sensory processing differences, yet families routinely manage it in isolation because stigma prevents open clinical conversation. The behaviour is not rare. The silence around it is.
80%
Sensory Differences
Children with ASD experiencing sensory processing differences (PMC11506176, PRISMA 2024)
65%
Manage Alone
Estimated families managing fecal smearing who never seek professional support due to shame
240M+
Global Children
Children worldwide with developmental disabilities (WHO 2023)
India's paediatric neurodevelopmental population exceeds 15 million children. Across Pinnacle Blooms Network's 70+ centres and 20M+ therapy sessions, fecal smearing presentations span all socioeconomic strata, geographies, and diagnostic profiles. No family should navigate this alone.
"You are among thousands of Indian families — and millions worldwide — navigating this exact challenge. The isolation you feel is manufactured by silence, not by reality."
The Neurological Mechanism
🔬Sensory Processing Pathway: The somatosensory cortex in many autistic children processes tactile input differently — particularly warm, soft, malleable textures. Feces provides a unique tactile-thermal-olfactory input profile that no other commonly available material replicates.
🔬Communicative Pathway: The behaviour may represent the only available signal when verbal or AAC communication is inaccessible. The child's anterior cingulate cortex registers unmet need — and the motor output is the behaviour itself. This is literally the child's voice.
🔬Medical/GI Pathway: Chronic constipation creates a neurological preoccupation with bowel movements. Pain, discomfort, and irregular gastrointestinal function alter interoceptive awareness, making feces psychologically prominent for the child.
This Is a Nervous System Event. Not a Character Flaw.
What this means for you:
- Your child is not "being disgusting on purpose."
- Your child is not "doing this to upset you."
- Your child's brain is meeting a need — or sending a signal — through the only means available.
- When we identify what that need or signal is, we can provide a better alternative.
This is sensory science. Behavioural science. Medical science. All pointing to the same conclusion: the behaviour has a function, and the function can be addressed.
Research: Frontiers in Integrative Neuroscience 2020 — Comprehensive framework for sensory integration/processing in ASD. DOI: 10.3389/fnint.2020.556660

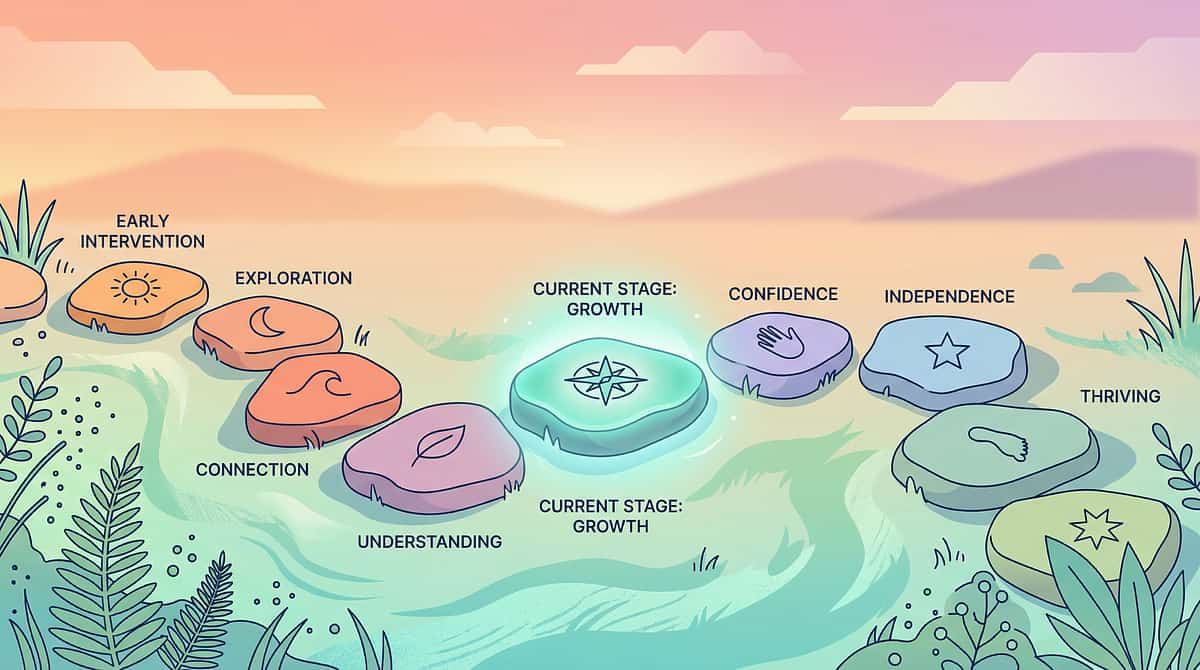
Your Child Is Here. Here Is Where We're Heading.
Understanding where your child sits on the developmental continuum — and what the intervention journey looks like ahead — transforms uncertainty into a clear, actionable path.
Age 18m–3yr
Exploratory phase typical. Brief body curiosity during toilet training is developmentally normal. Minimal reaction and redirection appropriate.
Age 3–5yr
Assessment warranted. Persistent smearing at this age warrants functional assessment. Sensory, communicative, and medical evaluation begins here.
Age 5–12yr
Comprehensive intervention. Significant unmet need requiring full ABA + OT + Medical + SLP multi-disciplinary assessment.
Beyond
Resolution zone. Behavioural Regulation Readiness Index: Green. Full functional independence achievable.
A key principle for children with autism: Developmental age, not chronological age, guides expectations. Many children with ASD function at 18m–3yr developmental levels in specific domains regardless of their chronological age. This is the working context for this intervention.
Research: WHO Care for Child Development (CCD) Package | UNICEF MICS developmental indicators | PMC9978394

Clinically Validated. Home-Applicable. Parent-Proven.
🛡️ Level I — Systematic Review + Multi-Disciplinary Consensus
Function-based behavioural intervention for fecal smearing is supported by: ABA functional analysis literature (BACB-level evidence), OT sensory processing research (systematic review level), Paediatric GI literature (medical consensus), and Communication-based replacement behaviour evidence (SLP RCTs).
Study | Key Finding | Ref | |
PRISMA Systematic Review 2024 | 80% ASD children have sensory processing differences requiring sensory-based intervention | PMC11506176 | |
Meta-analysis, World J Clin Cases 2024 | Sensory integration therapy effectively promotes adaptive behaviour across 24 studies | PMC10955541 | |
ABA Literature Consensus | Functional assessment + replacement behaviour = gold standard for automatic-reinforcement behaviours | NCAEP 2020 | |
Paediatric GI Research | Significant correlation: chronic constipation drives fecal smearing; medical treatment resolves behaviour | PMC1308134 | |
Padmanabha et al., Indian J Pediatr 2019 | Home-based sensory interventions show significant outcomes in Indian paediatric populations | DOI:10.1007/s12098-018-2747-4 |
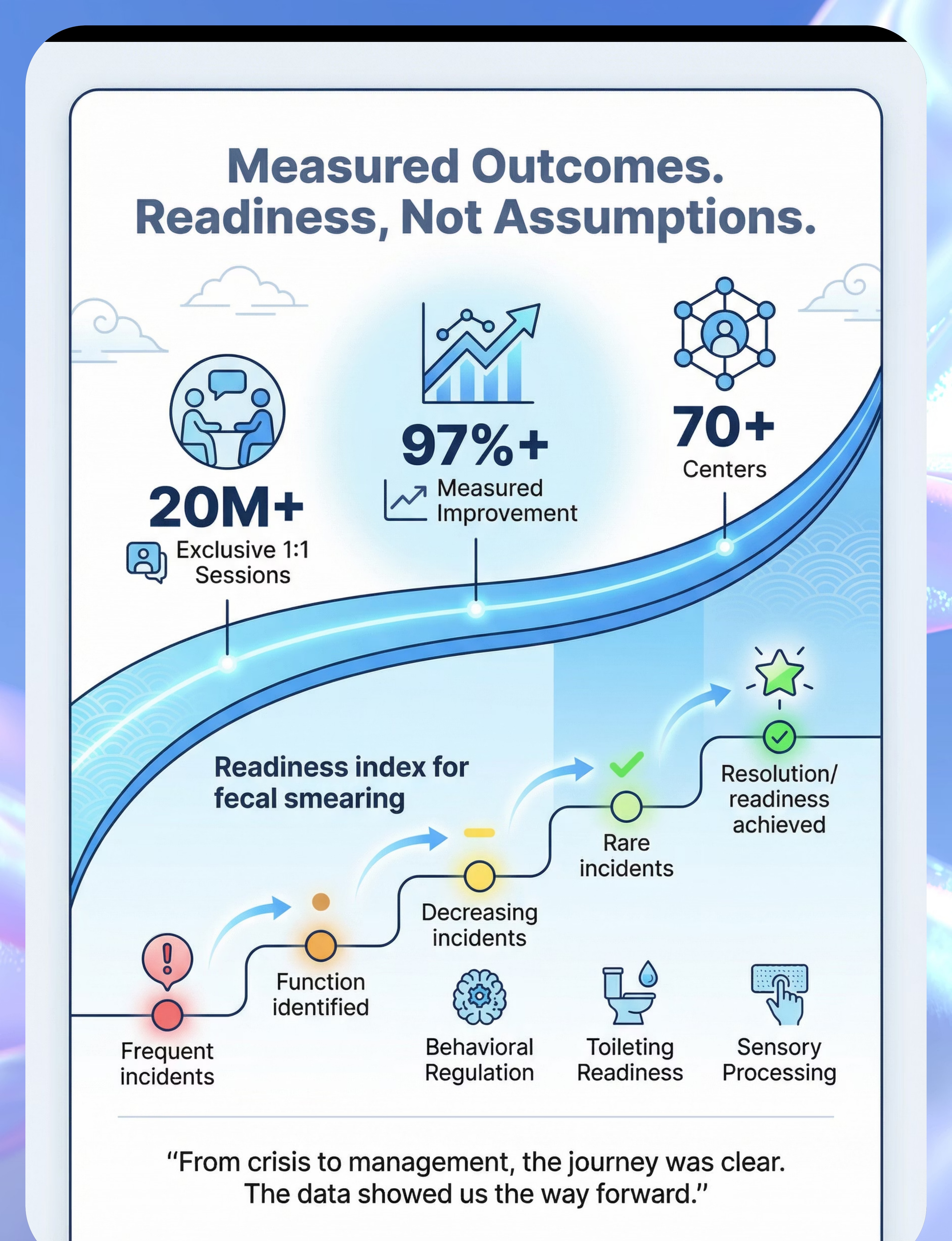
From 20M+ exclusive 1:1 therapy sessions across 70+ centres: children with fecal smearing who received function-based multi-component intervention showed measurable improvement in Behavioural Regulation Readiness Index within 8–12 weeks of consistent implementation.

ACT II — THE KNOWLEDGE TRANSFER
🎯 Multi-Material Function-Based Intervention for Fecal Smearing (Scatolia)
Parent-Friendly Alias: "The 9-Material Fecal Smearing Response System"
Fecal smearing (scatolia) is not a single behaviour — it is a behavioural class that serves one or more functions: sensory stimulation (seeking the specific tactile-thermal profile that feces provides), functional communication (signalling unmet needs when verbal/AAC communication is unavailable), medical response (behavioural preoccupation driven by constipation or GI discomfort), or attention-seeking (the behaviour produces immediate, intense caregiver response).
🧠 Behavioural Support
👐 Sensory Processing
🚽 Toileting / ADL
💬 Functional Communication
🏠 Environmental Modification
🩺 Medical / GI
Parameter | Specification | Parameter | Specification | Who Delivers | |
Age Range | 2–12 years | Frequency | Daily implementation | Parents + Caregivers + ABA + OT + Paediatrician + SLP | |
Setting | Home + School + All environments | Duration | 8–12 weeks minimum | Full multi-disciplinary team |

This Technique Crosses All Therapy Boundaries. The Behaviour Doesn't Organise by Therapy Type.

🏥 Paediatric ABA / BCBA (Primary Lead)
Conducts Functional Behaviour Assessment (FBA). Identifies whether function is sensory, communicative, attention-based, or automatic reinforcement. Designs the behaviour support plan and trains caregivers in function-based response protocols.
🖐️ Occupational Therapy — OT (Co-Primary)
Evaluates sensory processing profile. Identifies specific sensory properties the child seeks (texture, temperature, malleability). Designs individualised sensory diet and prescribes appropriate sensory alternative materials.

💬 Speech-Language Pathology (SLP)
Evaluates communication capacity. If behaviour serves a communicative function, designs AAC strategy, choice board system, or PECS protocol. Ensures child has functional means to express sensory needs and discomfort.
👩⚕️ NeuroDevelopmental Paediatrics
Rules out and treats GI causes — particularly chronic constipation. Provides bowel management programme. Evaluates for pain-related behavioural drivers and coordinates with ABA and OT on medical findings.

📚 Special Education / Parent Coaching
Generalises home-based protocols across all environments. Trains all caregivers, teachers, and support staff for consistency. Monitors implementation fidelity and provides family psychological support resources.
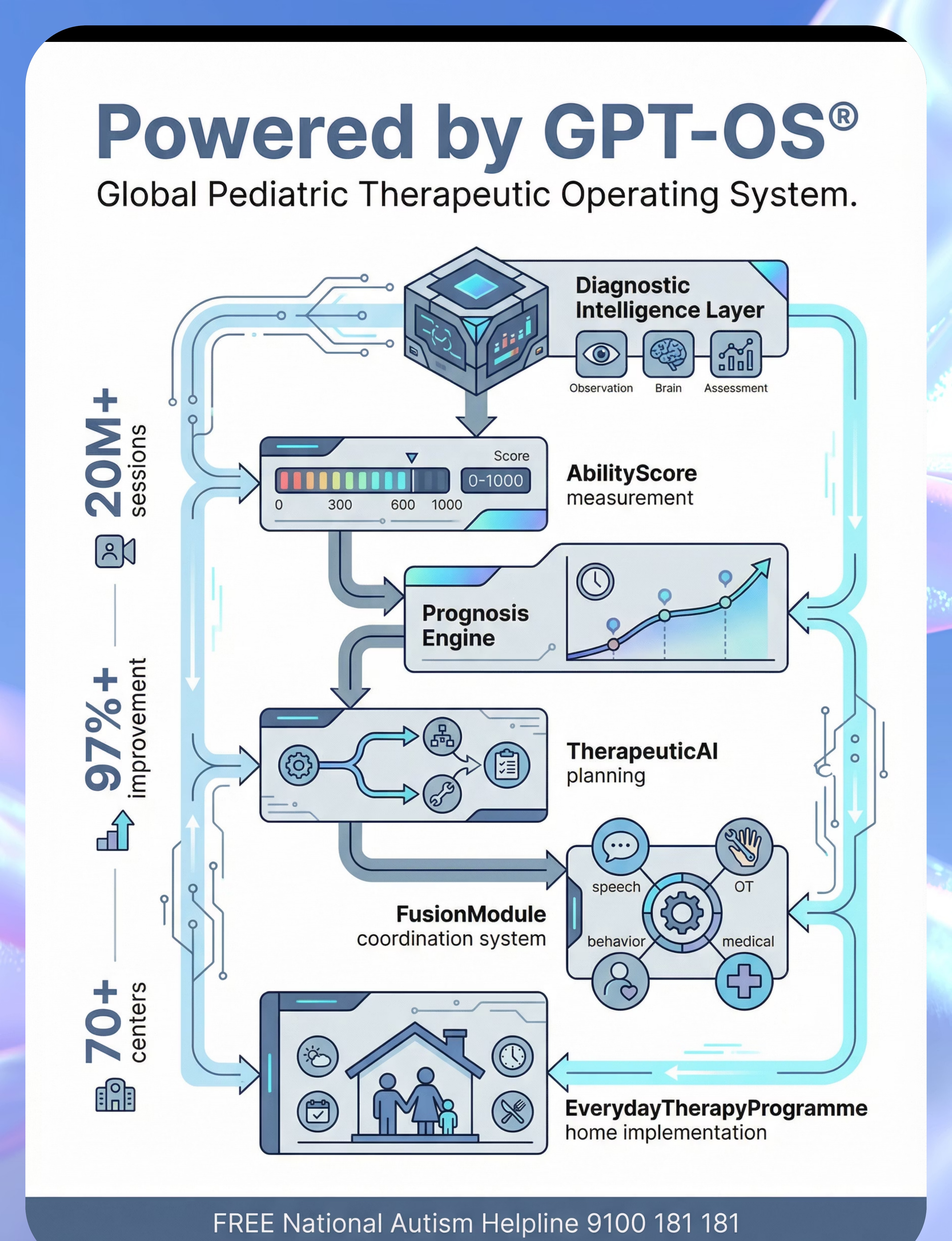
"Pinnacle Blooms Network's FusionModule™ coordinates all five disciplines into a single converged therapeutic pathway — eliminating the fragmented, siloed care that leaves this behaviour unresolved for years."
This Is a Precision System. 9 Materials. 4 Functions. One Resolution Protocol.
The intervention targets three concentric levels simultaneously. At the core: precise function identification and appropriate replacement behaviour. The secondary ring addresses the immediate functional needs — sensory regulation, communication, GI health, caregiver capacity, and environmental safety. The outer ring captures the broader developmental gains that emerge when the behaviour's function is consistently met through appropriate means across 8–12 weeks.
Research: PMC10955541 — Meta-analysis: sensory integration therapy promotes adaptive behaviour (primary), social skills (secondary), sensory processing + motor skills (tertiary) across 24 studies.

MATERIAL 1 OF 9
Sensory Play Alternatives
Canon Category: Sensory / Tactile Materials
Function: Sensory-Seeking
The most important material category in this system. The goal is to match the specific sensory profile that feces provides — warmth, malleability, spreadability, tactile depth — through a safe, socially appropriate alternative. Warming the material before use is non-negotiable: tepid is not equivalent to the sensory profile the child's nervous system is seeking.
Product | Price Range | Best For | Search | |
Therapy Putty (various resistances) | ₹300–800 | Primary alternative — closest match | ||
Kinetic Sand | ₹500–1,200 | Children seeking spreadable texture | ||
Slime / Stretchy Tactile Materials | ₹200–600 | Oozing-through-fingers sensory input | ||
Warm Playdough | ₹150–400 | Budget-accessible; easy to warm |
📌Pinnacle Recommends: Warm before use. Test temperature on your own wrist. Match to the specific texture and temperature your child seeks — cold is not the same as warm for this nervous system.

MATERIAL 2 OF 9
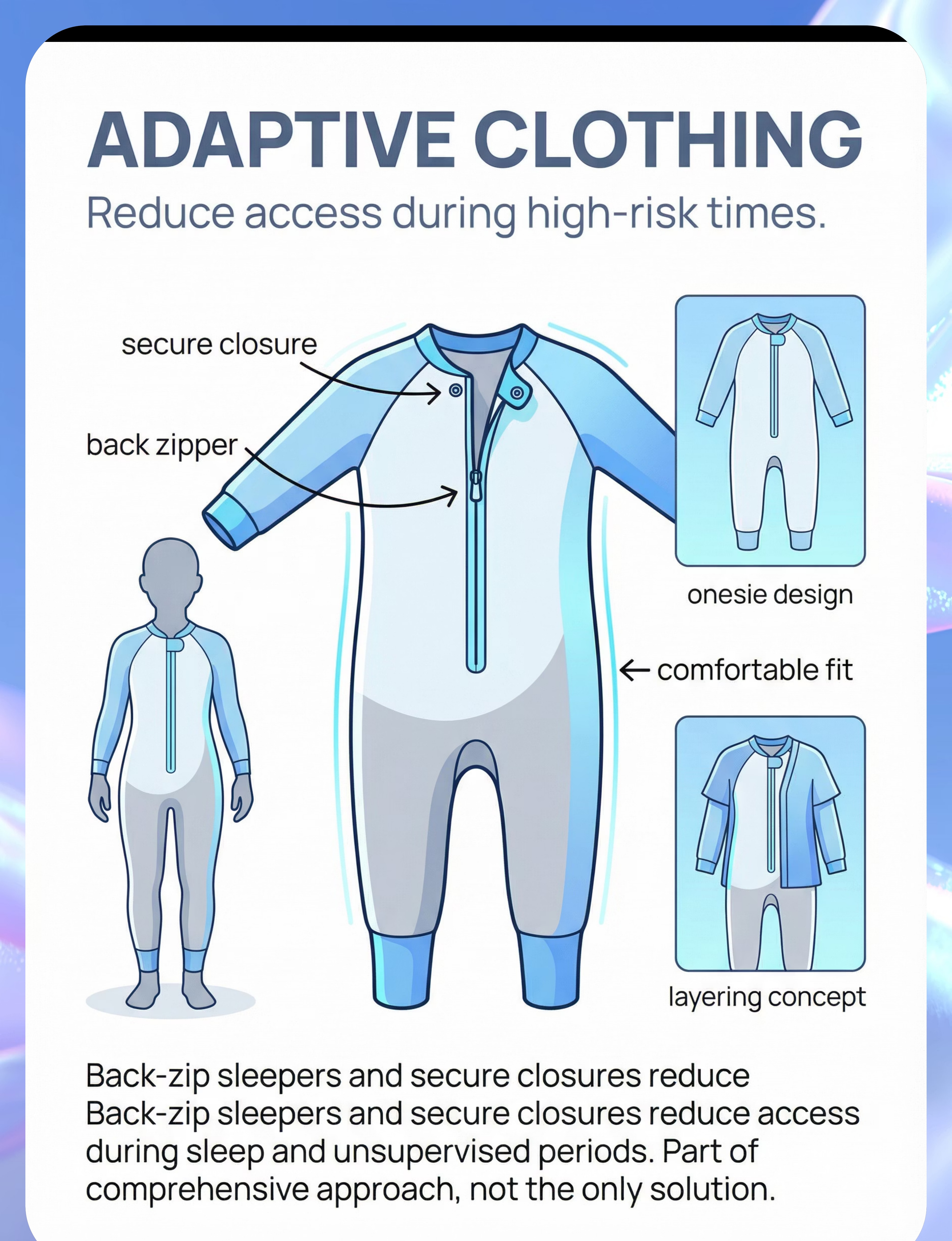
Adaptive Clothing
Canon Category: Adaptive Equipment / Access Prevention
Function: Environmental Barrier
Purpose
Reduce access during high-risk times — sleep, unsupervised periods, transition times. Adaptive clothing is a critical environmental management tool that reduces incident frequency while other intervention components are being established.
⚠️ Important Caveat
Adaptive clothing is part of a comprehensive approach only — not a sole intervention. It does not address the underlying function. Use alongside sensory alternatives, communication systems, and medical evaluation.
Recommended Products
DIY Alternative
Zip-up sleeper worn backwards; safety pin through zipper pull. Reduces access without specialised purchase. Always ensure no restriction to breathing or circulation.
Material Safety
✅ Must not restrict breathing or circulation
✅ Must not be used as physical restraint
✅ Must be easily removable by an adult
✅ Must not be used as physical restraint
✅ Must be easily removable by an adult

MATERIAL 3 OF 9
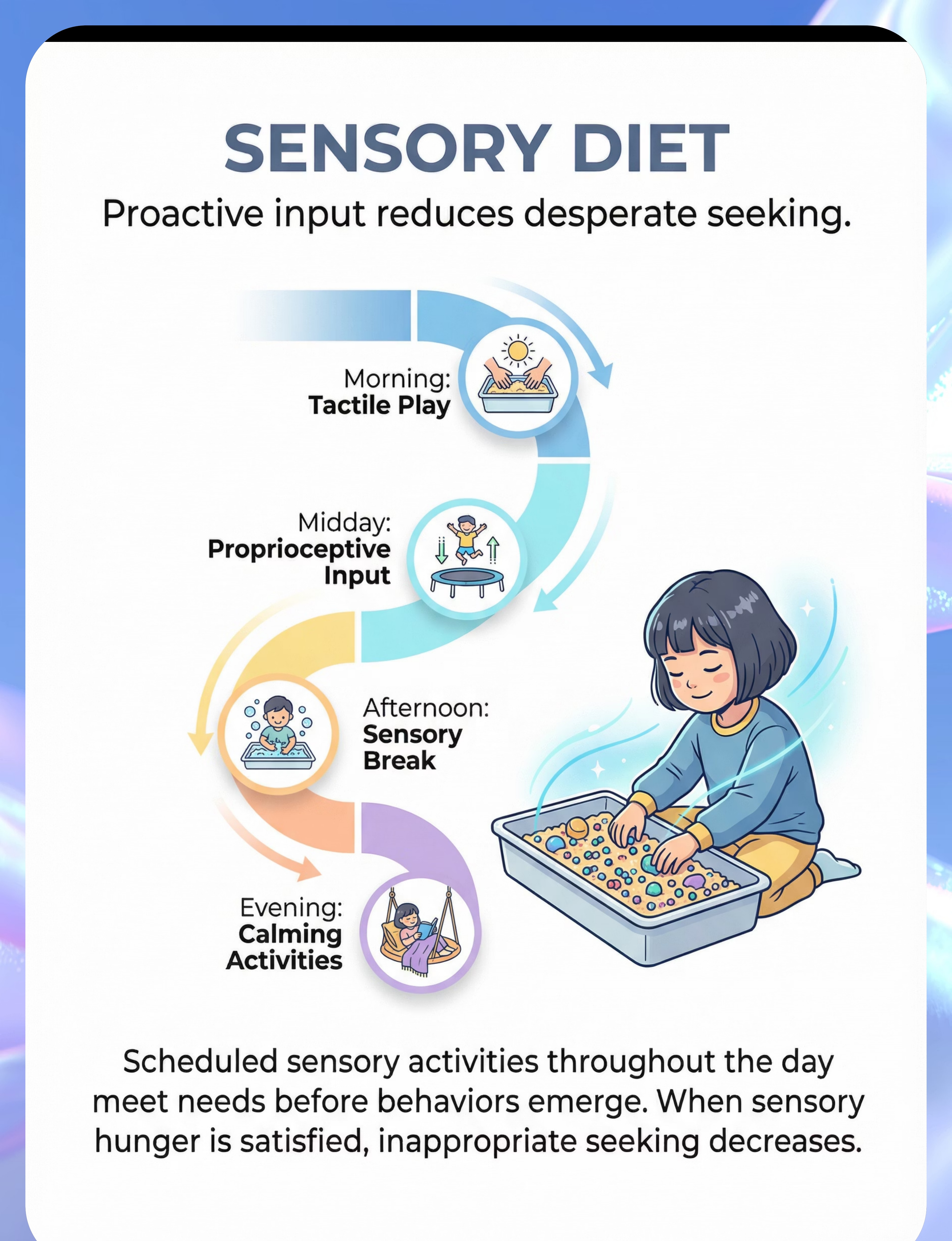
Sensory Diet Materials (Scheduled Input)
Canon Category: Sensory Diet Supplies
Function: Proactive Needs-Meeting
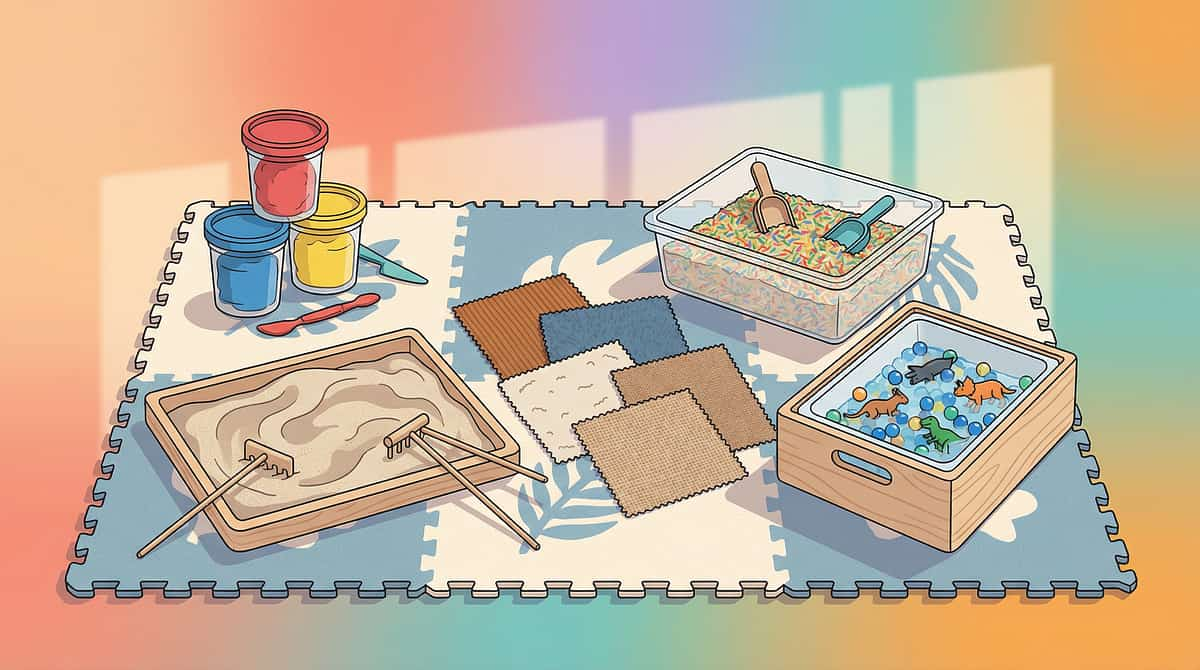
A sensory diet is a personalised, scheduled programme of sensory activities designed to proactively meet the child's sensory needs throughout the day. The critical insight: proactive sensory needs-meeting prevents the seeking behaviour from escalating to fecal smearing. By ensuring adequate tactile and proprioceptive input at regular intervals, the motivating operation that drives the behaviour is addressed before it peaks.
Sensory Bin + Fillers
Rice, beads, sand — contains and structures messy tactile exploration. ₹300–1,000
Tactile Boards / Texture Plates
Structured surface exploration for children who need variety. ₹400–1,200
Visual Schedule Strips
Predictability reduces anxiety and prepares the child for sensory sessions. ₹200–600
DIY Substitute: Large kitchen bowl + dried lentils/rice — same proprioceptive and tactile input profile as a commercial sensory bin. Zero cost.
MATERIAL 4 OF 9
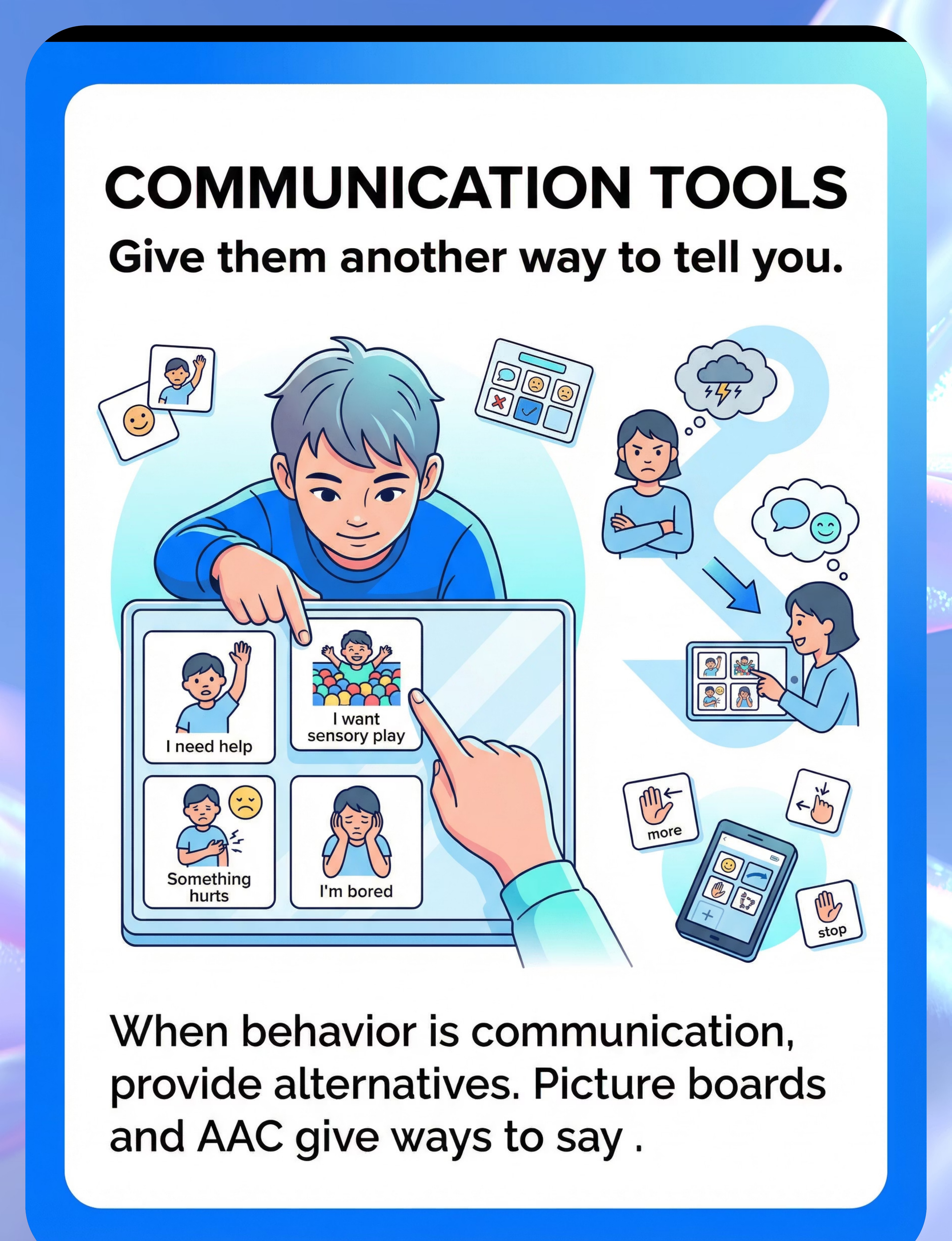
Communication Tools (AAC / Choice Boards)
Canon Category: Communication Supports
Function: Functional Communication Replacement
When fecal smearing serves a communicative function, the single most powerful intervention is giving the child a better, more efficient way to communicate the same message. Communication tools replace the behaviour as the child's voice — they do not suppress the underlying need; they give it a functional outlet.
PECS / Picture Exchange Cards
Visual communication cards that allow the child to exchange a picture to make a request. Begin with high-motivation sensory items. ₹300–800.
Choice Boards (Laminated, Velcro)
Two-picture boards are the simplest starting point. Child chooses between "this" and "this." Any choice = communicative success. ₹200–500.
AAC App Devices
For children with greater communicative potential, dedicated AAC devices open full expressive vocabulary. ₹1,000–10,000.
DIY Substitute: Photos cut from old magazines, arranged on cardboard. Visual choice = same communicative function as laminated commercial boards. The mechanism is the visual structure, not the material quality.
MATERIAL 5 OF 9
Toilet Timing Supports
Canon Category: Visual Schedules / Toileting Supports
Function: Predictable Bowel Management
Predictable, scheduled bowel movements — consistently occurring in the toilet — dramatically reduce both access to feces and the neurological preoccupation with bowel movements that drives smearing. The gastrocolic reflex creates a natural window 15–20 minutes after meals: this is the optimal timing for scheduled toilet sits.
Visual Toilet Schedule
Posted at child eye level. Step-by-step sequence with pictures: enter bathroom → pants down → sit → wait → wipe → flush → wash hands → leave. ₹150–400.
Bowel Tracking Chart
Records time, frequency, and consistency of bowel movements. Essential for identifying patterns and communicating with the paediatric team. ₹100–300 or free printable.
Toilet Timer / Sand Timer
Makes the waiting period concrete and manageable. Child can see "how much longer." Set for 5–10 minutes. ₹200–600.
DIY Substitute: Mobile phone timer with visual alarm. Identical function to a sand timer. Photographs of each toilet step printed and stuck with tape function identically to commercial laminated schedules.

MATERIAL 6 OF 9
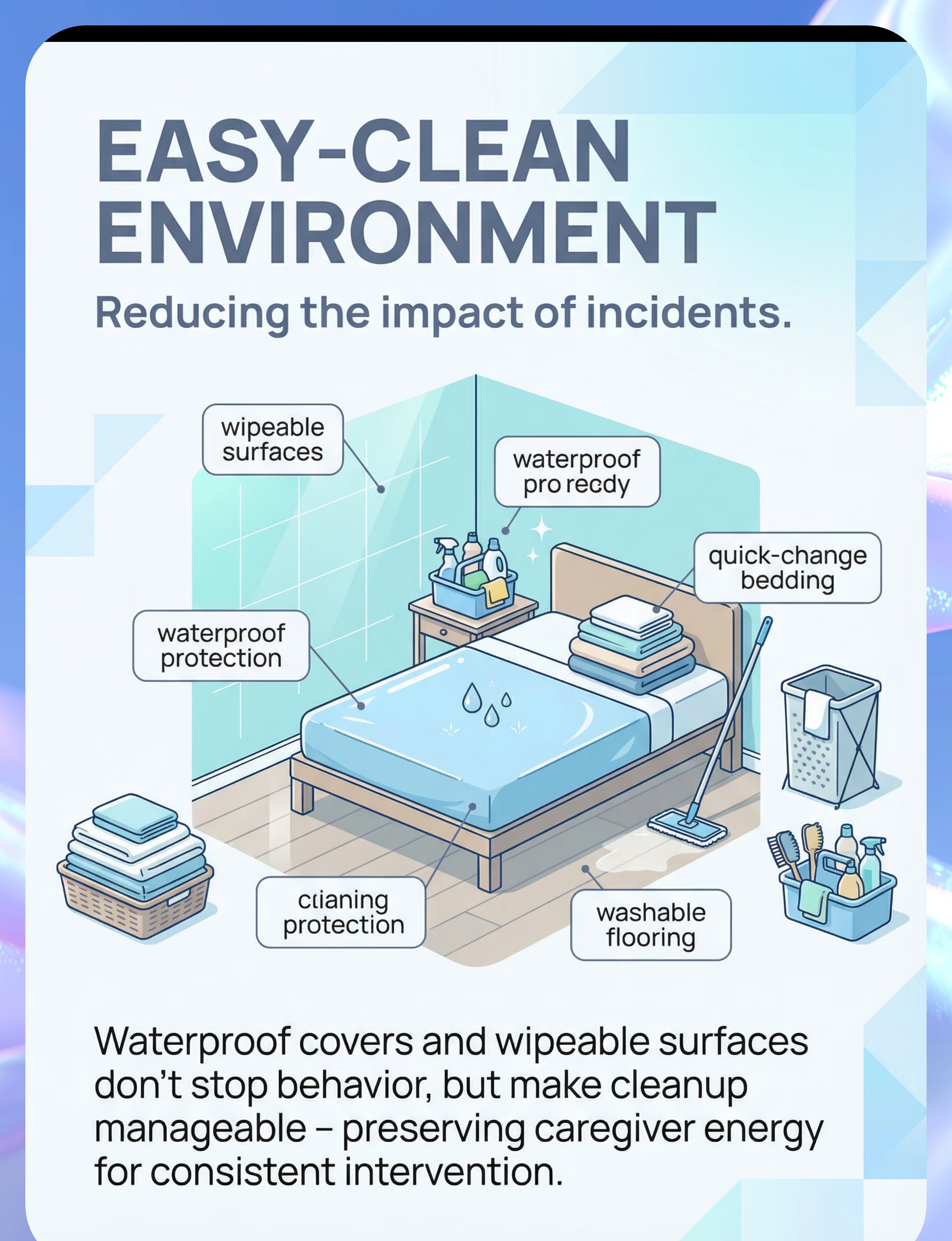
Easy-Clean Environment Supplies
Canon Category: Environmental Modification Supplies
Function: Caregiver Burden Reduction
Caregiver wellbeing is a clinical variable, not a luxury consideration. Reducing the physical and emotional burden of cleanup directly protects your capacity to implement intervention consistently — and removes the intense, emotionally charged caregiver response that may be inadvertently reinforcing the behaviour through attention.
Waterproof Mattress Protector
Essential for nighttime incidents. Reduces cleanup time from 30+ minutes to under 5 minutes. Protects the sleeping environment. ₹600–1,500.
Washable Wall Paint / Wipeable Surface Sheets
Convert affected wall surfaces to easily wipeable ones. Dramatically reduces cleanup time and eliminates residual odour. ₹500–2,000.
Enzymatic Cleaner
Breaks down biological matter at the molecular level. Eliminates odour completely — unlike bleach, which does not fully neutralise. ₹400–800.
⚠️Safety Note: Use enzymatic cleaners, not bleach, in the child's immediate environment. Bleach fumes are respiratory irritants, particularly for children with sensory sensitivities. Always use gloves during cleanup — feces contains E. coli, Salmonella, and other pathogens.

MATERIAL 7 OF 9
Reinforcement Menus (For Positive Attention System)
Canon Category: Reinforcement Menus
Function: Positive Attention + Motivation
Abundant, predictable, positive attention for appropriate behaviours is the counterweight to the attention that incidents have historically provided. The reinforcement system must make appropriate behaviour more rewarding than the target behaviour — for every function profile. Timing matters more than magnitude: reinforcement must occur within 3 seconds of the target behaviour.
🏆 The Rosette Imprint Reward Jar
Tokens for visual reinforcement system. Children can see their progress accumulating, making abstract reinforcement concrete and motivating.
₹589 | Buy on Amazon.in
✅ Pinnacle Canon
⭐ 1800+ Reward Sticker Book
Immediate tangible reinforcer for every successful alternative material use. Stickers are universally motivating across age groups and developmental levels.
₹364 | Buy on Amazon.in
✅ Pinnacle Canon
🧸 Transition Comfort Soft Toy
For transition period comfort reinforcement — particularly at high-risk times like bedtime and nap transitions when sensory seeking typically peaks.
₹425 | Buy on Amazon.in
✅ Pinnacle Canon
Token Economy Suggestion: Each time the child uses a sensory alternative, uses the communication board, or sits on the toilet: 1 token. At 5 tokens: access to preferred activity or item. Celebrate the attempt, not just the success — any engagement with the alternative material, even 2 seconds of touch, deserves genuine, warm reinforcement.

MATERIAL 8 OF 9
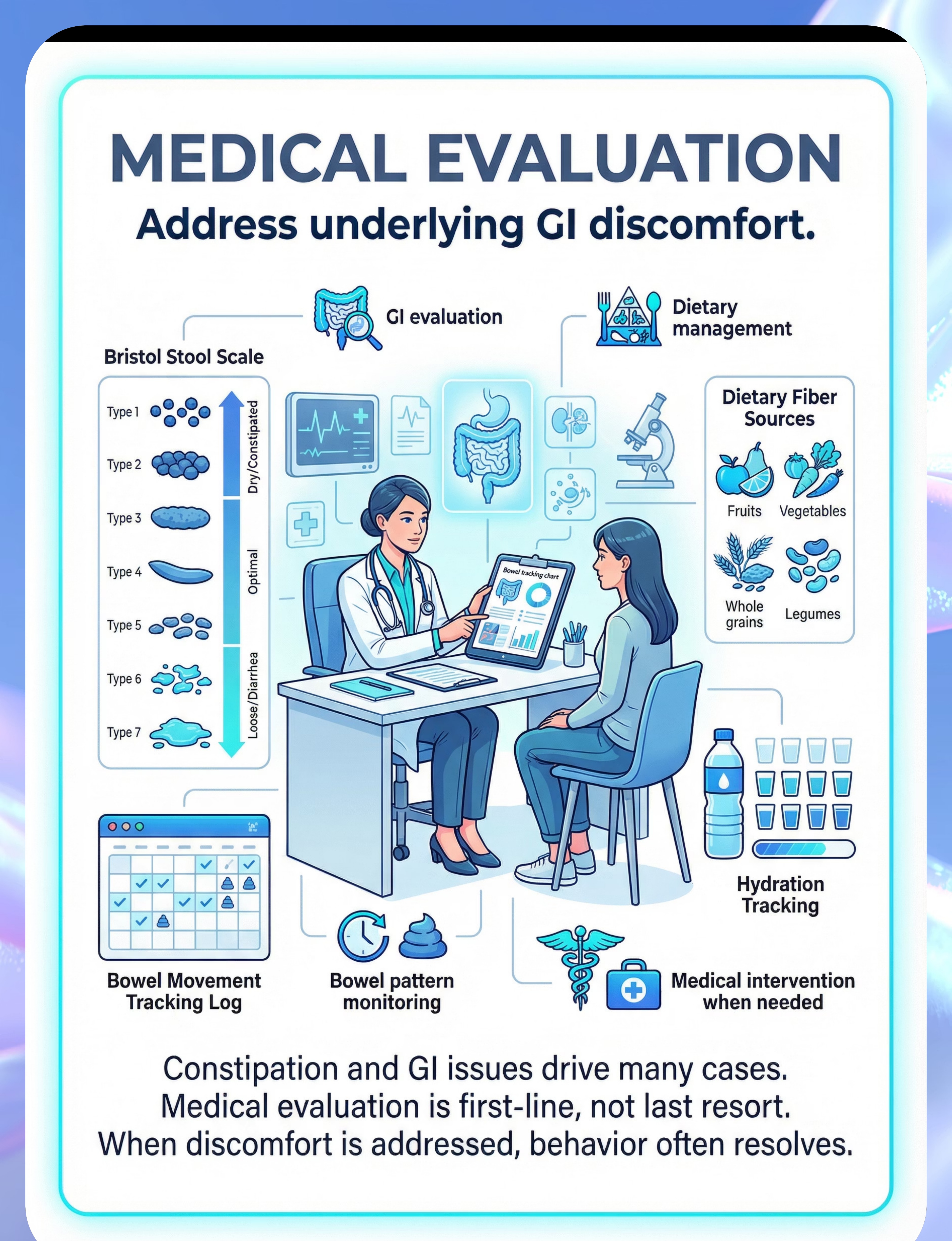
Medical Tracking Tools
Canon Category: Medical / GI Documentation
Function: Support Paediatric GI Evaluation
Medical evaluation is first-line, not last resort. Chronic constipation is one of the most powerful and treatable drivers of fecal smearing — and it is frequently overlooked because parents and even some clinicians default to behavioural explanations without ruling out physiological causes first. These tracking tools support the medical evaluation that must accompany any behavioural intervention.
Why Medical Documentation Matters
Without systematic bowel tracking, it is impossible to identify whether constipation, discomfort, or irregular bowel patterns are driving the behaviour. A paediatrician receiving detailed Bristol Stool Scale records and frequency logs can diagnose and treat GI causes in one or two appointments — potentially resolving the behaviour faster than any behavioural intervention alone.
Medical factors, when treated effectively, can produce the fastest resolution of fecal smearing of all intervention components.
Tracking Tools (All Available Free)
- Bowel Movement Log: Records date, time, frequency, and Bristol Stool Scale rating. Exercise book with structured columns = identical clinical value to commercial tracker. Free printable available via Google search.
- Bristol Stool Scale Chart: Visual reference for categorising stool consistency (Types 1–7). Essential communication tool with paediatric team. Search Amazon.in or free printable online.
- Abdominal Massage Guide: Available free at pinnacleblooms.org — supports bowel motility between medical appointments.

MATERIAL 9 OF 9
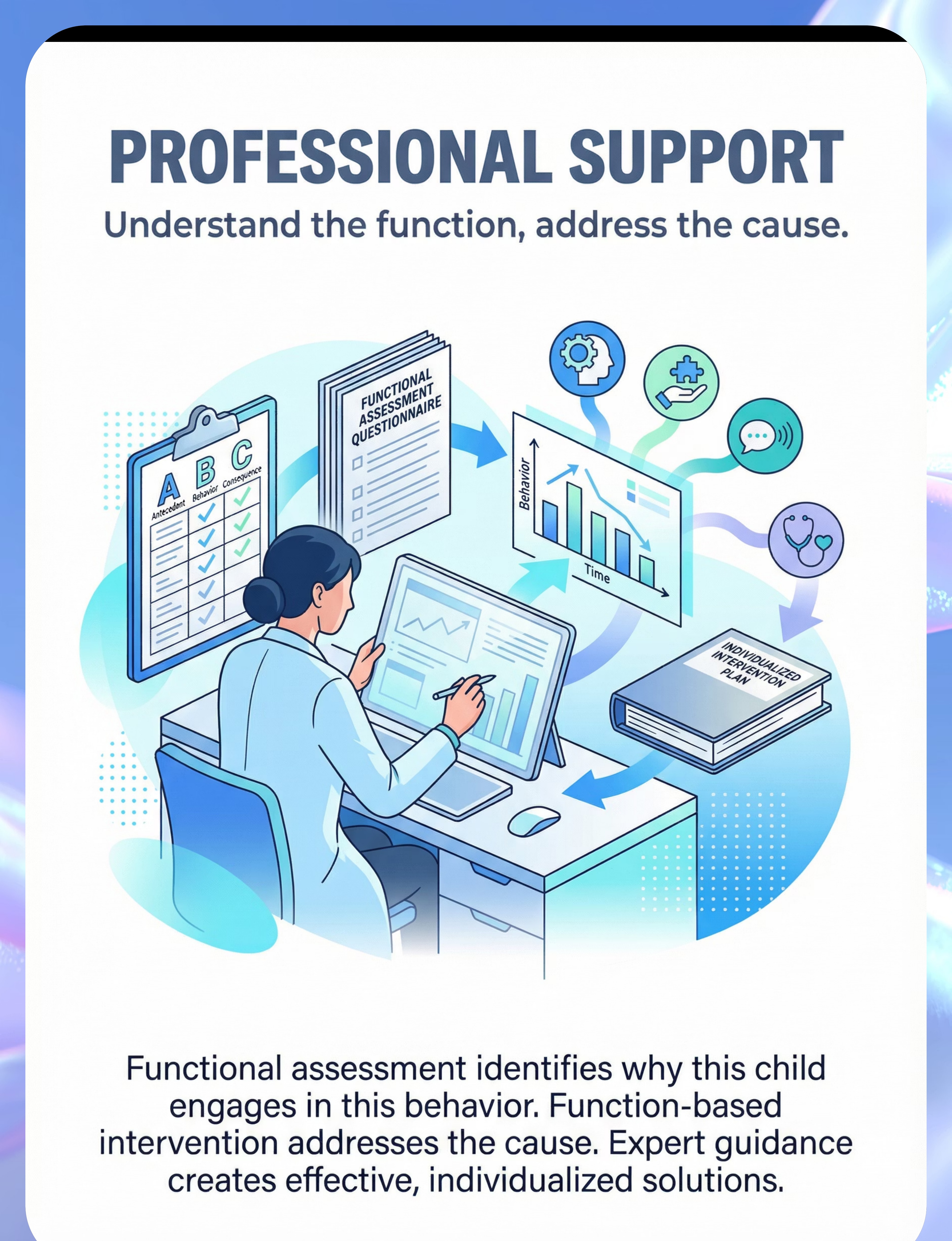
Professional Assessment Tools
Canon Category: Behavioural Assessment Documentation
Function: Support FBA and Behaviour Support Planning
The Functional Behaviour Assessment (FBA) is the diagnostic engine of this entire system. Without systematic antecedent-behaviour-consequence data, function identification is guesswork. These tools — all available at zero cost — transform daily observations into clinical intelligence that drives every material and protocol decision.
ABC Tracking Sheets (Antecedent-Behaviour-Consequence)
Record what happens immediately before the behaviour (antecedent), exactly what the behaviour looks like (behaviour), and what happens immediately after (consequence). 2 weeks of ABC data typically identifies function with high confidence. Free download or via Amazon.in.
Functional Assessment Questionnaire
Structured questionnaire covering sensory history, communication level, medical history, and behavioural patterns. Completed with caregiver and reviewed by BCBA. Available through all Pinnacle centres at no charge.
📞FREE National Autism Helpline: 9100 181 181 — For personalised material guidance in your language. Our trained counsellors will help you identify your child's primary function and recommend your first material. Available 24x7 in 16+ languages.
Every Indian Family Can Execute This Today. Zero-Cost Options Exist for All 9 Materials.
"Pinnacle's intervention architecture is designed on the WHO Nurturing Care Framework's equity principle: every strategy must be executable by a family with ₹0 in discretionary spending. Context-specific, resource-light intervention is not a compromise — it is a design requirement." — Pinnacle Consortium, GPT-OS® Equity Standards
Material | Clinical Grade | ₹0 Substitute | Why It Works | |
Sensory Alternatives | Therapy putty ₹400 | Warm homemade playdough (flour + salt + oil + warm water) | Same tactile-thermal profile: warm, soft, malleable | |
Tactile Exploration | Kinetic sand ₹600 | Damp garden soil in a tray | Same proprioceptive + tactile input profile | |
Messy Play | Slime ₹300 | Cooked oatmeal, cornstarch-water mixture | Spreadable texture, similar visual-tactile properties | |
Sensory Bin | Commercial bin ₹500 | Large kitchen bowl + dried lentils/rice | Contains and structures messy tactile exploration | |
Visual Schedule | Laminated schedule ₹400 | Photographs printed/cut, stuck with tape | Visual structure is the mechanism — not lamination | |
Choice Board | Printed AAC cards ₹300 | Photos cut from old magazines on cardboard | Visual choice = same communicative function | |
Toilet Timer | Sand timer ₹400 | Mobile phone timer with visual alarm | Identical function | |
Bowel Log | Commercial tracker ₹200 | Exercise book with date, frequency, consistency columns | Identical clinical value if consistently maintained | |
Adaptive Clothing | Specialist garment ₹1,500 | Zip-up sleeper worn backwards; safety pin through zipper pull | Reduces access without specialised purchase |
⚠️Important Caveat — When DIY will not work: If the child mouths or ingests materials, clinical-grade non-toxic alternatives are non-negotiable. Cooked oatmeal is safe. Cornstarch paste is safe. Garden soil is NOT appropriate for a child who mouths materials.
Read This Before Implementing Any Intervention. Non-Negotiable.
🔴 RED — STOP. Seek professional evaluation first if:
• Fecal smearing is new, sudden-onset, or intensifying rapidly
• GI distress signs: abdominal pain, bloating, blood in stool
• Child is ingesting feces (coprophagia) — immediate medical evaluation required
• Child has self-injured or become extremely distressed during cleanup
• Behaviour occurring at school/public settings creating safeguarding concerns
• Suspected physical pain not yet medically evaluated
• GI distress signs: abdominal pain, bloating, blood in stool
• Child is ingesting feces (coprophagia) — immediate medical evaluation required
• Child has self-injured or become extremely distressed during cleanup
• Behaviour occurring at school/public settings creating safeguarding concerns
• Suspected physical pain not yet medically evaluated
🟡 AMBER — Proceed with professional guidance:
• First time implementing sensory alternatives — OT guidance preferred
• Child has known sensory defensiveness to specific textures
• Multiple function hypothesis — FBA needed before choosing materials
• School-age child — coordinated home-school plan essential
• Child has known sensory defensiveness to specific textures
• Multiple function hypothesis — FBA needed before choosing materials
• School-age child — coordinated home-school plan essential
🟢 GREEN — Proceed with home implementation:
• Function reasonably identified (sensory-seeking, attention-based, predictable timing)
• Medical evaluation complete or no signs of GI distress
• Child is safe and not in distress
• At least one sensory alternative identified
• You can implement low-key, calm cleanup response
• Medical evaluation complete or no signs of GI distress
• Child is safe and not in distress
• At least one sensory alternative identified
• You can implement low-key, calm cleanup response
⚠️Medical Urgency: GI symptoms — severe constipation, abdominal pain, changes in stool — require MEDICAL attention, not behavioural intervention. Medical evaluation is first-line, not last resort.
📞9100 181 181 — If uncertain whether to proceed, call first.
📞9100 181 181 — If uncertain whether to proceed, call first.

Before the Session Begins, the Environment Must Be Right.
Spatial precision prevents 80% of failures. The session environment communicates to your child's nervous system before any words are spoken. Calm space = lower arousal = greater therapeutic effect.
🏠 For Sensory Alternative Sessions
Room Selection: Child's room or play area — familiar, not clinical. Remove porous items from immediate reach during initial sessions. Washable floor surface preferred.
Material Placement:
1. Sensory alternative — at child's sitting level, within arm's reach, already out before child enters
2. Communication board — visible, accessible, within child's reach AT ALL TIMES
3. Reinforcement items — in your pocket, not visible yet
4. Cleaning supplies — accessible to you, out of child's sight
1. Sensory alternative — at child's sitting level, within arm's reach, already out before child enters
2. Communication board — visible, accessible, within child's reach AT ALL TIMES
3. Reinforcement items — in your pocket, not visible yet
4. Cleaning supplies — accessible to you, out of child's sight
Parent Positioning: Seated at child level. Side-by-side (not face-to-face). Warm, neutral expression. No tension in body posture.
💡Lighting: Soft, warm preferred. 🌡️Temperature: Warm playdough must be genuinely warm — test on your own wrist.
🚽 For Toilet Timing Sessions
Bathroom Setup:
- Child's toilet seat installed
- Step stool for foot support — critical. Feet dangling reduces ability to bear down effectively
- Visual toilet schedule posted at child eye level
- Preferred activity/book available for 5–10 minute waiting period
- Reinforcement system ready at door
🔇 Remove from ALL Sessions:
- TV/screen if it will compete with engagement
- Excessive distracting toys
- Other children if they create performance pressure
- Your phone — full presence is the active ingredient

ACT III — THE EXECUTION
60-Second Readiness Assessment. Never Push Through When the Child Isn't Ready.
Antecedent conditions determine intervention effectiveness. A session started in the wrong state will not only fail — it may create negative associations with the very materials you're trying to establish as preferred alternatives.
1
Biological Readiness
✅ Child has eaten (moderately satiated — not hungry, not just fed)
✅ Adequate sleep in last 24 hours
✅ No signs of illness, fever, or physical discomfort
✅ Bowel movement today (if constipated, toilet timing not ideal)
✅ Adequate sleep in last 24 hours
✅ No signs of illness, fever, or physical discomfort
✅ Bowel movement today (if constipated, toilet timing not ideal)
2
Neurological Readiness
✅ Child in a regulated state — not mid-meltdown or post-meltdown
✅ No sensory overload in last 30 minutes
✅ Child responds to your presence with neutral or positive affect
✅ No signs of pain or physical distress
✅ No sensory overload in last 30 minutes
✅ Child responds to your presence with neutral or positive affect
✅ No signs of pain or physical distress
3
Environmental Readiness
✅ Space set up as per Card 12 setup guide
✅ Materials ready and warm (if applicable)
✅You are regulated — your state directly affects session quality
✅ Adequate time available; no imminent interruptions
✅ Materials ready and warm (if applicable)
✅You are regulated — your state directly affects session quality
✅ Adequate time available; no imminent interruptions
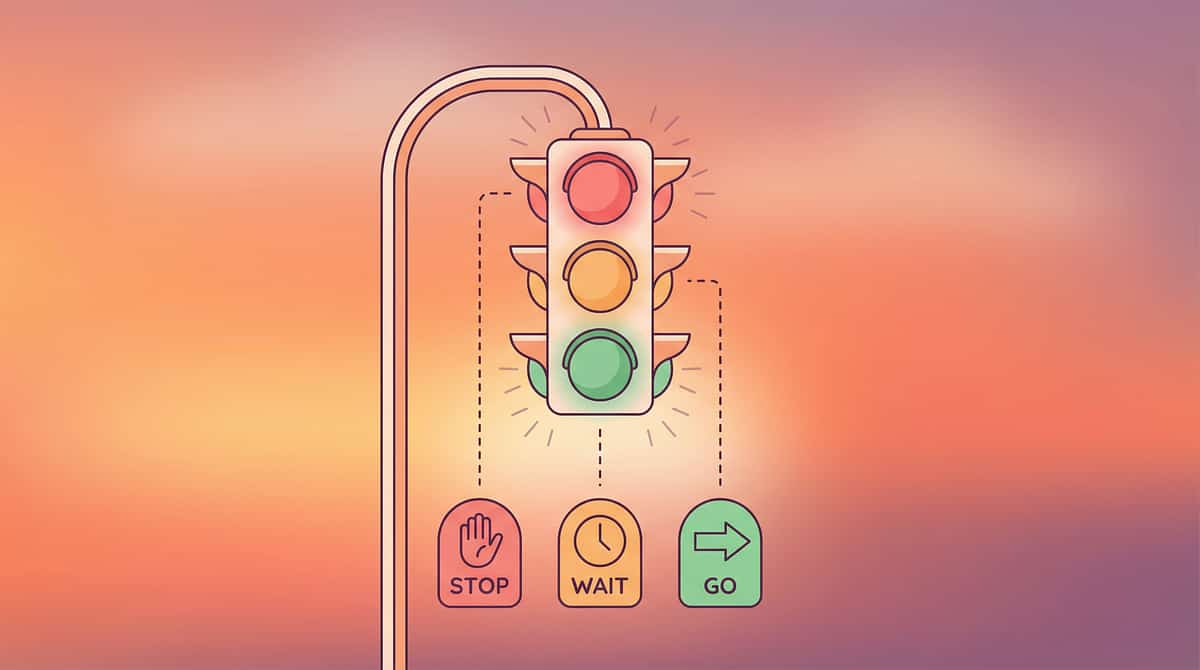
🟢 GO
All checks green → Proceed to Step 1
🟡 MODIFY
2–3 amber checks → Simplify to just presenting the sensory material without structured protocol
🔴 POSTPONE
Multiple red checks → Do a calming activity instead. Note what caused readiness failure

STEP 1 OF 6
The Invitation
Purpose: Low-Demand Entry
Timing: 30–60 seconds
Every protocol begins with an invitation, not a command. The child's nervous system enters the activity through low-demand, playful engagement — not therapeutic intent. The invitation must feel genuinely casual and appealing.
"Look what I have! [Produce the warm playdough/sensory material] It's so soft. I wonder what you'll do with this."
✅ DO
- Present material casually, without obvious therapeutic intent
- Touch the material yourself first — show it's safe and appealing
- Allow 10–15 seconds of just observing before any expectation
- If child reaches → reinforce immediately
- Maintain warm, curious expression throughout
❌ DON'T
- "Come here, we're doing sensory now" — demand framing
- Reference the target behaviour during the session
- Force hands toward material
- Show disappointment if child doesn't engage immediately
Resistance Cues → Modify Protocol
If child turns away, pushes material, or becomes distressed: do not escalate. Return to a calming activity and try again later. Never push through resistance.

STEP 2 OF 6
The Engagement
Purpose: Deepen Material Exploration
Timing: 1–3 minutes
The child is now engaged. Deepen the interaction by encouraging active material exploration. Demonstrate without directing — show what's possible, then follow the child's lead.
"You can squish it... pull it... make a ball... whatever you want. Watch — [demonstrate]."
🟫 For Warm Playdough
Present at body temperature or slightly warmer. Demonstrate squishing, rolling, pulling apart, pressing flat. Allow free exploration for 60–90 seconds. Gradually introduce tools (rolling pin, shape cutters, fork for texture) if child shows readiness.
🟡 For Kinetic Sand
Present in a contained tray. Demonstrate scooping, pouring, pressing, leaving impressions. The "moldable when squeezed, falls apart otherwise" property is the key sensory appeal for this specific material.
🟣 For Slime / Putty
Demonstrate stretching, pressing through fingers, folding. The sensory experience of material oozing through fingers is the therapeutic active ingredient — this is what makes slime uniquely effective for certain sensory profiles.
🟢 Engagement
Child touches, explores, vocalises positively — reinforce within 3 seconds: "You're touching it!"
🟡 Tolerance
Child allows contact but minimal active interest — acceptable, build slowly over sessions
🔴 Avoidance
Child pulls away or shows distress — scale back to observation only. Never push through

STEP 3 OF 6
The Therapeutic Action
Purpose: Sustained Sensory Engagement
Duration: 5–15 minutes
This is the active ingredient. The core action differs based on which function the behaviour is serving for your child — and matching the action precisely to the function is what makes this intervention effective rather than generic.
1
For Sensory Seeking / Automatic Reinforcement
Sustained tactile engagement with warm playdough, kinetic sand, or therapy putty for 5–10 minutes of uninterrupted exploration. The child's hands are engaged with a material that provides the specific sensory properties — warmth, malleability, spreadability, tactile depth — that feces provides, without health concerns. The goal is not to "teach" anything: it is to allow the sensory need to be fully met through appropriate means.
2
For Communication Function
Prompt the child to use the communication board to request the sensory activity: "Show me what you want." When child uses picture card or AAC → immediate access to preferred material. This builds the association: communication = sensory access. Over time, the child learns to request the experience through communication rather than behaviour.
3
For Attention-Seeking Function
The therapeutic action is your presence. Scheduled, predictable, warm 1:1 engagement. Child-led play for 10–15 minutes. Your full attention — undivided. No phone. Eye contact, responsive play, verbal commentary on child's actions. The child is learning: appropriate behaviour = abundant, predictable attention.
4
For Toilet Timing
Scheduled sit on toilet 15–20 minutes after meals (gastrocolic reflex window). Child on toilet with foot support. Preferred activity/book available. Timer set for 5–10 minutes. No pressure to produce. Reward for sitting (not for results initially). Prompt diaper change immediately after any bowel movement outside the toilet.
Research: PMC10955541 — Meta-analysis: 40-minute clinical sessions; home sessions 10–20 minutes with core action occupying 40–60% of session time.
STEP 4 OF 6
Repeat & Vary
Dosage Principle
3 good repetitions > 10 forced ones
Consistency is more important than intensity. A predictable daily sensory diet — delivered at regular intervals and at high-risk times — is the mechanism that gradually reduces the motivating operation driving the target behaviour.
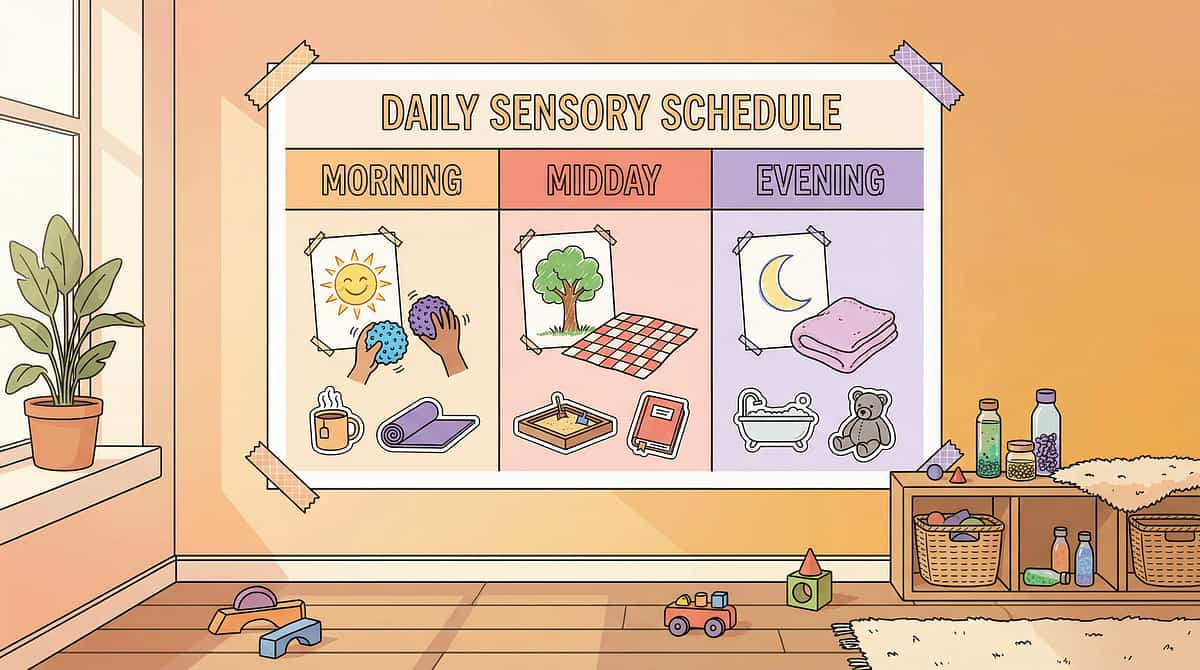
Morning
10–15 min tactile exploration (primary alternative material)
Midday
5–10 min proprioceptive input (heavy work, carrying, pushing)
Pre-High-Risk
10 min focused sensory engagement immediately before historically high-risk period (nap, bath, bedtime)
Evening
5–10 min calming tactile activity (warm bath, soft fabric exploration)
If child habituates to material | Try this variation | |
Bored with warm playdough | Add food colouring, change temperature, add texture tools | |
Kinetic sand loses appeal | Switch to wet sand, damp soil, or sensory rice bin | |
Slime no longer engaging | Change colour, add non-toxic glitter, change viscosity | |
Communication board not used | Simplify to 2-choice board; physically model pointing |
Frequency Guidance: Sensory diet sessions: 3–5x daily for first 4 weeks. Toilet timing: every day consistently, post-meals. Communication practice: every interaction where need can be expressed. Positive attention: minimum 3 scheduled 10-minute sessions daily.

STEP 5 OF 6
Reinforce & Celebrate
ABA Principle: Timing > Magnitude
Within 3 seconds. Specific. Genuine.
Reinforcement is the engine that builds new neural pathways. The timing must be immediate (within 3 seconds), the praise must be specific (name the exact behaviour), and the delivery must be genuine. Hollow praise is not reinforcing — children's nervous systems know the difference.
For sensory alternative engagement:
"You're using the playdough! That's exactly right!" [big smile, thumbs up, or preferred physical contact]
For communication board use:
"You showed me what you need!" [immediately provide the sensory material] "That's amazing communication!"
For toilet timing success:
"You sat on the toilet!" [deliver reinforcer immediately — sticker, token, or preferred item]
For high-risk period without incident:
"You played with your playdough AND you kept your clothes on. I am SO proud of you."
"Celebrate the attempt, not just the success." Any engagement with the alternative material — even 2 seconds of touch — deserves genuine, warm reinforcement. You are building a neural pathway, not evaluating performance.
📞9100 181 181 — For personalised reinforcement strategy guidance
📞9100 181 181 — For personalised reinforcement strategy guidance

STEP 6 OF 6
The Cool-Down
Purpose: Predictable Transition
Duration: 2 minutes
No session ends abruptly. The transition back to baseline is as important as the session itself. Abrupt endings create dysregulation and resistance to future sessions — gradually, the child begins to associate the sensory material with the aversive experience of having it removed, rather than with the positive experience of using it.
"Two more squishes, then we put it away." [Pause] "One more. Last one." [Pause] "All done! You did so well. Let's put it away together."
1
Transition Warning
"2 more, then all done." Give the child advance notice before ending.
2
Child-Participated Put-Away
Involve child in placing material in container (if able). Ownership of the ending reduces resistance.
3
Hand-Washing Ritual
Warm water + soap — provides additional tactile input AND hygiene closure. Builds a healthy post-session routine.
4
60-Second Calm Activity
Preferred soft toy, quiet book, or sitting in caregiver's lap. Allows the nervous system to return to baseline gently.
5
Transition Statement
"Now we're going to [next activity]." + visual schedule reference. Predictability is the antidote to transition resistance.
Research: NCAEP 2020 — Visual supports and transition procedures are classified evidence-based practice for autism.

60 Seconds After Session. Three Data Points. This Drives Every Recommendation.
"Without data, intervention is intuition. With data, intervention is science." The families at Pinnacle who track consistently see function identified within 2 weeks, incident frequency data enabling targeted antecedent manipulation within 4 weeks, and measurable progress within 8 weeks.
📊 Field 1: Incident Log
Did a fecal smearing incident occur today? YES / NO
If YES: When? (time) | Where? (room) | What preceded it? (antecedent)
📊 Field 2: Alternative Engagement
Did child engage with sensory alternative? YES / NO / PARTIAL
Duration (minutes): ___ Level: HIGH (child-initiated, sustained) / MEDIUM (prompted, brief) / LOW (refused)
📊 Field 3: Communication Use
Did child use communication board/AAC to request sensory activity? YES / NO / ATTEMPTED
Notes: _______________
GPT-OS® Integration: Your data feeds into GPT-OS®'s Behavioural Regulation Readiness Index for your child. As patterns emerge, TherapeuticAI® adjusts recommendations. This data belongs to your child's therapeutic journey — it is the most valuable 60 seconds of your day.
📞9100 181 181 | Free D-420 Tracking Sheet PDF available at pinnacleblooms.org/downloads/D-420-family-guide
📞9100 181 181 | Free D-420 Tracking Sheet PDF available at pinnacleblooms.org/downloads/D-420-family-guide

Not Working? Here's Why — And What To Do.
If an intervention isn't working after consistent implementation for 2 weeks, the hypothesis about function is likely incorrect — not the child's willingness to change. Return to assessment. The behaviour is always communicating something; the task is to find what.
Challenge | Likely Reason | Solution | |
Child ignores sensory alternative entirely | Material doesn't match specific sensory profile | Try different temperature, texture, viscosity. Conduct sensory profile assessment (OT referral) | |
Incidents continue despite alternative availability | Wrong function targeted — may be communicative or medical | Re-do function hypothesis. Track antecedents for 1 week. Rule out GI issues medically | |
Child uses alternative AND still smears | Behaviour partially maintained by attention function | Ensure cleanup is low-key, neutral, brief. Increase scheduled positive attention. Evaluate for mixed function | |
Adaptive clothing ineffective | Child has found workaround, or wrong garment type | Layer with second garment. Use different closure type. Consult OT on adaptive clothing options | |
Toilet timing not producing results | Gastrocolic reflex timing off, or constipation interfering | Medical evaluation for GI issues. Adjust post-meal timing — some children's reflex peaks at 30–45 min | |
Communication board ignored | System too complex, or reinforcement for use not strong enough | Simplify to 2-picture board. Increase reinforcement for any use immediately. SLP consultation | |
Parent too emotionally reactive during cleanup | Attention reinforcement of behaviour | Practise neutral, brief cleanup script. Two-person cleanup if possible. Seek caregiver support | |
All strategies tried, nothing working | Complex mixed function requiring professional FBA | Contact Pinnacle: 9100 181 181. Professional functional behaviour assessment is required |

This Is a System, Not a Script. Adapt to Your Child.
No two children present identically. The 9-material system is a framework — personalisation based on your child's specific function profile, age, and sensory intensity level determines what to prioritise, what to sequence, and how to pace implementation.
1
🔴 Sensory-Seeking Profile
Higher-intensity tactile materials (highest resistance therapy putty, mud play, finger paint). More frequent shorter sessions (every 2 hours). Materials available 24/7, not just scheduled.
2
🟡 Communicative Profile
AAC/PECS takes priority over sensory materials. Every sensory access mediated through communication system. Build communication fluency before relying on materials alone.
3
🟢 Medical/GI Profile
Medical intervention first. Bowel timing and management protocols are primary. Sensory alternatives are secondary until GI factors are addressed.
4
🔵 Attention-Seeking Profile
Positive attention system primary. Scheduled engagement 4–6x daily. Neutral cleanup essential. Materials used to prevent boredom during previously under-stimulated periods.
Young Child (2–4yr)
1 material only. 3–5 min sessions. Maximum sensory appeal. Minimal language demands.
School-Age (5–8yr)
Child chooses between 2–3 alternatives. More explicit communication training.
Older Child (9–12yr)
Can participate in function discussion. Self-monitoring systems. Explicit sensory communication.

ACT IV — THE PROGRESS ARC
Week 1–2 Progress
What Week 1–2 Actually Looks Like
Most parents expect dramatic change immediately. This is the recalibration card. Week 1–2 is the hardest — you are implementing strategies while incidents are still occurring. This is not failure. This is the lag period between establishing new neural pathways and seeing behavioural change.
✅ Progress Indicators for Week 1–2
- Child tolerates sensory alternative material (even without actively seeking it)
- Child resists ending session — good sign; material is preferred
- Communication board used at least 1–2 times per day
- Toilet timing sits completed consistently (even without on-toilet bowel movement)
- You have identified a pattern in antecedent data (when/where incidents occur)
- Incident frequency not expected to decrease yet — but antecedents becoming clearer
❌ What Is NOT Progress Yet
- Incidents stopping entirely (too early)
- Child independently seeking sensory alternatives without prompting
- Complete communication fluency (this takes months)
- GI issues resolving (medical process takes time)
Patience Metric
"If your child engaged with the playdough for 30 seconds longer today than last week — that is real, measurable, neurologically meaningful progress."
Every day of consistent implementation is building the foundation. Hold course.
Research: PMC11506176 — Sensory integration intervention outcomes emerge across 8–12 week timelines.

Week 3–4 Progress — Neural Pathways Forming
Consolidation Signs
By weeks 3–4, the neural pathways established through consistent daily practice begin to consolidate. The child's nervous system has received enough repeated, structured input to begin generating spontaneous approach behaviour — one of the clearest indicators that the alternative is becoming genuinely preferred.
Child begins to approach sensory materials without prompting
Spontaneous approach = neural pathway consolidating. This is the most reliable single indicator of genuine progress.
Incident frequency beginning to decrease
Even 20–30% reduction is meaningful. Track against your Week 1 baseline data.
Antecedent pattern now clear
You can predict high-risk times with accuracy. This allows proactive placement of alternatives before the motivating operation peaks.
Communication board use increasing
Child initiates at least some requests without prompting. The communication system is beginning to serve its intended function.
You feel more confident and less reactive
Your own regulation during incidents may be removing the attention reinforcement that was maintaining the behaviour. This matters clinically.
Week 5–8 Progress — The Behaviour Is Becoming Unnecessary
Integration
The sensory needs are now being met through appropriate means consistently enough that the behaviour is losing its function. The child's nervous system has learned: "This material gives me what I need. The other behaviour is no longer necessary."
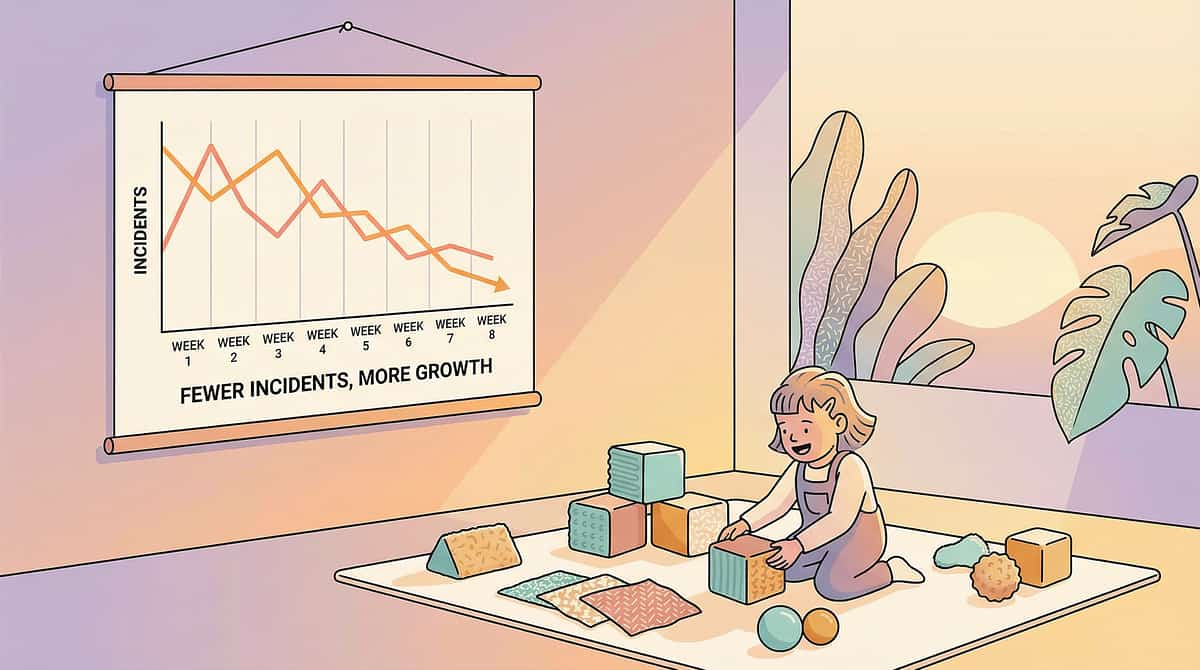
50%
Incident Reduction
Minimum reduction from baseline by week 8 of consistent implementation
70%
Target Reduction
Achievable reduction by week 8–12 with full multi-component implementation
8–12
Weeks to Results
Consistent implementation timeline for measurable behavioural change
Generalisation Targets — Begin extending the alternative to new settings:
- Is the sensory material available at school? Coordinate with the teacher
- Is there a sensory alternative in the car? (For travel high-risk periods)
- Do grandparents and other caregivers know the protocol?
If GI intervention was initiated: bowel patterns should be stabilising by this point. Consistent, comfortable, regular bowel movements reduce behavioural preoccupation with feces dramatically.
Neuroplasticity literature: synaptic strengthening through repeated structured input follows predictable timelines in paediatric populations. Week 5–8 represents consolidation of new pathways.

Every Win Deserves to Be Named. You Are Building a Different Future.
🌟 Milestone 1
First time child touched sensory alternative without prompting
🌟 Milestone 2
First incident-free day
🌟 Milestone 3
Child used communication board to request sensory activity
🌟 Milestone 4
First on-toilet bowel movement
🌟 Milestone 5
First incident-free week
🌟 Milestone 6
Child went through a high-risk period without incident
🌟 Milestone 7
Spontaneous use of alternative material at school
🌟 Milestone 8
Family member reports confidence in managing the situation
"You have done something that most families never manage: you asked for help, you understood the science, you implemented a system with consistency, and you held course through the hard weeks. Your child's behaviour changed because YOU changed. Because you offered something better. Because you met the need. That is clinical work. That is therapy. That is love expressed as a system."
📞9100 181 181 — Share your milestone with our team. They want to hear it.

Know When Home-Based Implementation Needs Professional Escalation.
🚨 Escalate Immediately
- Coprophagia (child ingesting feces) — medical emergency evaluation
- Behaviour spreading to school/public settings — safeguarding concern
- Child showing self-injury associated with the behaviour
- GI symptoms: blood, severe pain, inability to have bowel movements
- No reduction in incident frequency after 8 weeks of consistent implementation
- New-onset behaviour after period of absence — may indicate change in medical status
⚠️ Escalate Within 2 Weeks
- Function remains unclear after 4 weeks of data collection
- Communication board system not building despite consistent implementation
- Multiple failed attempts at toilet timing with no progress
- Caregiver burnout at crisis level — this is a clinical need, not a personal failure
1
Call Pinnacle Helpline: 9100 181 181
Free, 24x7, available in 16+ languages. A trained counsellor will triage your situation immediately.
2
Request AbilityScore® Comprehensive Assessment
Specify that you need: Functional Behaviour Assessment (BCBA) + Sensory Evaluation (OT) + Medical Evaluation (paediatrician) + Communication Assessment (SLP).
3
Access Nearest Pinnacle Centre
pinnacleblooms.org/centers — 70+ locations across India, plus teleconsultation for remote families.
This Is One Technique in a System. Here's the Larger Map.
D-420 is one node in a connected network of evidence-based technique pages. Depending on the function profile your data reveals, the next technique in your child's therapeutic journey may be one of the following pathways.
If Sensory Function Is Primary
→ D-419: Sensory-Seeking Behaviours and Appropriate Alternatives — The broader sensory-seeking framework of which fecal smearing is one expression.
If Communication Function Is Primary
→ B-Series: AAC and Functional Communication Techniques — Full AAC system design for children whose behaviour is serving a communicative function.
If Toileting Readiness Is the Target
→ D-425: Toileting Challenges in Special Needs Children — The comprehensive toileting readiness programme.
If GI / Medical Factors Are Primary
→ unknown link — Medical management of the physiological component.
For Broader Behavioural Framework
→ unknown link — Prerequisite reading for all challenging behaviour interventions.
Related Techniques & Resources
unknown link
Prerequisite reading for all challenging behaviour interventions. The foundational framework for function-based analysis.
Direct precursor to fecal smearing intervention. The complete sensory-seeking framework.
Related sensory-behavioural challenge that often co-occurs with sensory-seeking behaviours.
Core skill for eliminating smearing opportunity. The complete toileting readiness programme.
unknown link
Medical component of this intervention. Essential reading for any GI-function hypothesis.
Essential parallel resource. Caregiver wellbeing is a clinical variable, not a luxury.

ACT V — THE COMMUNITY & ECOSYSTEM
You Are Not The First. You Will Not Be The Last. Read What's Possible.
Parent, Pinnacle Network, Hyderabad
"Three years. Every morning I dreaded what I'd find. We discovered through a Pinnacle OT assessment that our son was seeking the exact texture and temperature of the playdough alternative we introduced. Within 6 weeks of having warm therapy putty available before bed, incidents reduced by 90%. Now it's rare — and when it happens, we have a system. We got our sanity back. More than that: we understood our son for the first time."
Outcomes represent this family's experience. Individual results vary.
Parent, Pinnacle Network, Bengaluru
"We thought it was deliberate. We thought he was angry at us. The functional assessment showed it was 100% communication — he couldn't tell us his stomach hurt. Once we got the GI issues treated and gave him a simple choice board with 'something hurts' on it, the behaviour stopped within 3 weeks. Three years of mystery resolved in three weeks when we had the right framework."
Parent, Pinnacle Network, Chennai
"I was ashamed to tell anyone — even my mother. When I called the Pinnacle helpline, the person on the other end said 'you're not the first parent to call about this today.' I cried for 10 minutes from relief alone. Just knowing I wasn't alone changed everything."
📞9100 181 181 — Someone who understands is waiting. Free, 24x7, 16+ languages.
Preview of 9 materials that help with fecal smearing Therapy Material
Below is a visual preview of 9 materials that help with fecal smearing therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

This Behaviour Thrives in Silence. Community Breaks That.
Isolation is not the reality — it is the product of stigma. Families managing fecal smearing are not rare. They are simply invisible to each other. Community changes that. Every caregiver who connects, shares, and supports another shortens the time between onset and resolution for every family that follows.
💬 Pinnacle Parents WhatsApp Community
For families managing fecal smearing, pica, and related behaviours. Non-judgmental, experienced-parent moderated, clinician-reviewed. Available in 16 languages. Join via pinnacleblooms.org/community
🧑🤝🧑 Peer Mentoring
Connect with a parent who has successfully implemented this protocol and is willing to walk alongside you. Request peer mentor: care@pinnacleblooms.org
📍 Local Pinnacle Parent Meetups
70+ centres across India — monthly parent groups address challenging behaviours in supportive, professional-facilitated settings. Find nearest centre: pinnacleblooms.org/centers
🌍 Global Network
Pinnacle families span 70+ countries — India, UAE, USA, UK, Singapore, Canada, Australia, and beyond. You are part of a worldwide community of families who understand.
"Over 1,000 individuals from 111 countries contributed to the WHO Nurturing Care Framework — community engagement is not supplementary to intervention. It IS intervention."