
9 Materials That Help With End of Preferred Activity
"Five more minutes." You've said it. He heard nothing. The meltdown was already beginning.
Domain I: Transitions & Life Events | I-787
Pinnacle Blooms Network®
When your child cannot stop preferred activities — proven materials that make endings manageable. Scientific, home-applicable transition support by India's largest pediatric therapy consortium.
ACT I: THE EMOTIONAL ENTRY
The Recognition Moment
It's 6:47 PM. Your son has been playing with his trains for 40 minutes — peaceful, focused, genuinely happy. Dinner is ready. You walk over, crouch down, use your warmest voice: "Time to stop, sweetheart. Dinner's ready."
His face changes before the words finish leaving your mouth. The train gets thrown. The screaming starts. Twenty minutes later, dinner is cold, your daughter is crying at the table, and your son is still on the floor. All you asked was that he stop playing.
You weren't cruel. You gave a warning. You were patient. But ending a preferred activity — something he loves, something that was going well — is one of the most neurologically demanding transitions a child with autism faces. And for many families, it happens five, eight, twelve times a day.
"You are not failing. Your child's brain is locked onto what it loves — and being asked to leave that place genuinely hurts. This is neurology, not defiance. And it is solvable."
📞 FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | No Cost. No Registration.
WHO Nurturing Care Framework (2018): Responsive caregiving during emotionally challenging transitions is foundational to child development outcomes.
WHO Nurturing Care Framework (2018): Responsive caregiving during emotionally challenging transitions is foundational to child development outcomes.

ACT I — CARD 02
You Are Not Alone: The Numbers
This is one of the most common daily crises in autism parenting — and the data confirms you are far from alone in this struggle.
73%
Significant Difficulty
of children with ASD show significant difficulty ending preferred activities
4–8×
Daily Transitions
average preferred-activity transitions per child at home each day
38 min
Daily Meltdown Time
average cumulative meltdown time per day linked to activity endings in ASD families
You are among an estimated 8–10 million families in India alone navigating this exact challenge — the moment when a beloved activity must end and the child's nervous system revolts. Globally, difficulty ending preferred activities is among the top 3 daily behavioral challenges reported by parents of children with autism, ADHD, and related developmental profiles. It is not unique to your child. It is not caused by your parenting. And it is directly addressable with the right materials.
India has an estimated 18 million children with developmental disabilities (MoHFW, 2023). Among autism-diagnosed children attending structured therapy, transition-related behavioral challenges are reported by parents in >80% of intake assessments at Pinnacle centers.
📞9100 181 181 — Call any time. We understand.
PMC11506176 | PRISMA Systematic Review (2024): 80% of children with ASD display significant behavioral challenges during transitions. PMC10955541 | World J Clin Cases Meta-analysis (2024): Transition difficulties documented across 24 studies as primary family burden.
PMC11506176 | PRISMA Systematic Review (2024): 80% of children with ASD display significant behavioral challenges during transitions. PMC10955541 | World J Clin Cases Meta-analysis (2024): Transition difficulties documented across 24 studies as primary family burden.

ACT I — CARD 04
Where This Sits in Development
This Challenge Has a Developmental Context — and a Forward Path
Cognitive flexibility — the mental skill required to stop one activity and shift to another — develops significantly between ages 3 and 8, with continued maturation through early adolescence. For children with ASD, ADHD, or executive function differences, this developmental trajectory is delayed, not absent.
Ages 0–2
Regulation Basics & Object Permanence
Ages 2–4
Play Flexibility Seeds emerge
Ages 5–10 ★
TRANSITION SKILLS BUILD — You are here. Executive Function targeted window.
Ages 10–12
Executive Function Readiness expanding
Age 12+
Independence milestones possible
Per the WHO Care for Child Development Package (2023), executive function skills including task-switching are targeted developmental goals from ages 3–7. Children who receive structured support during this window show significantly better flexibility outcomes.
Common Co-occurring Profiles
Sensory Processing
70%+ of ASD children have sensory differences that amplify transition difficulty
ADHD Hyperfocus
Hyperfocus profiles intensify the neurological lock on preferred activities
Anticipatory Anxiety
Fear of what comes next compounds resistance to endings
Demand Avoidance (PDA)
Perceived loss of autonomy intensifies protest behaviors
"Your child is here. With the right materials and consistent practice, here is where we're heading: smooth endings, manageable transitions, and a child who can hear 'time to stop' without the world falling apart."

ACT II — CARD 07
Who Uses This Technique
Five Disciplines. One Converged Approach. Your Child at the Centre.
Occupational Therapy (Primary Lead)
OTs address the sensory regulation and executive function dimensions of activity endings. They design the sensory toolkit that keeps the child regulated during the transition and identify which sensory inputs in the preferred activity are driving the dysregulation.
Applied Behavior Analysis / BCBA
BCBAs engineer the antecedent strategies (timers, warnings, first-then) and consequence systems (token boards, reinforcement schedules) that make endings behaviorally manageable. They conduct functional analysis to understand what the behavior is communicating.
Speech-Language Pathology
SLPs address the comprehension gap — ensuring the child understands transition language, can communicate distress verbally rather than behaviorally, and can process social stories and transition narratives.
Special Education
Special educators implement transition systems in school and community settings, ensuring the home protocol generalizes beyond the family. They coordinate with classroom teachers for consistent messaging.
NeuroDevelopmental Pediatrics
NeuroDev doctors assess whether transition difficulty indicates underlying anxiety, sensory processing disorder, or executive function delay requiring medical support alongside behavioral intervention.
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type. A child stopping a preferred activity needs sensory support (OT), behavioral structure (ABA), language scaffolding (SLP), and environmental consistency (SpEd) — simultaneously."

ACT II — CARD 09 | MATERIAL 1
Material 1: Visual Transition Schedules
Canon Category: Visual Schedules / Communication Supports
"The foundation. Shows what's happening NOW and what comes NEXT."
Visual Transition Schedules are the cornerstone of end-of-preferred-activity support. They provide the child with concrete, visual information about the current activity and the one that follows — removing ambiguity that the brain interprets as threat. The schedule doesn't require the child to trust verbal language in a moment of emotional arousal; it anchors comprehension in pictures.
Why It Works
Same visual predictability principle whether laminated or hand-drawn. The brain processes sequence through imagery — lamination is not required for therapeutic effect.
Endorsed by: OT + ABA
Price Range: ₹300–₹1,500
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Paper + pen + stick figures on A4 sheet. Draw boxes for NOW and NEXT. Identical therapeutic mechanism.

ACT II — CARD 09 | MATERIAL 2
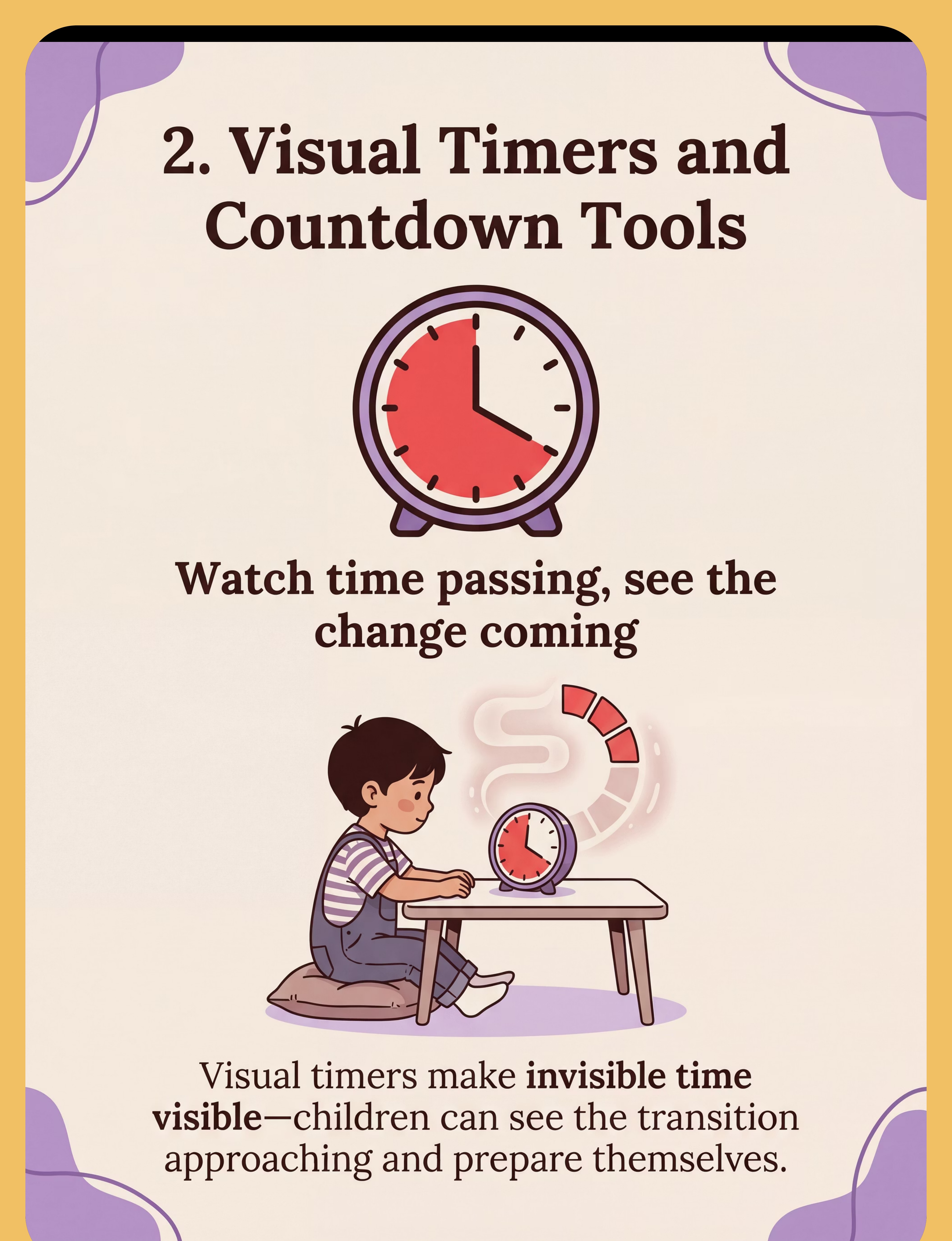
Material 2: Visual Timers & Countdown Tools
Canon Category: Transition Objects / Comfort Items
"Makes invisible time visible. The child sees the ending approaching."
The visual timer is arguably the single most important material in this protocol. Children with ASD struggle to comprehend abstract time — "5 more minutes" means nothing when time is invisible. A visual timer converts abstract time into a concrete, shrinking visual field. The child can see time passing and see the ending approaching — transforming a sudden surprise into a predictable event their nervous system can prepare for.
Clinical Notes
Must be placed before the preferred activity begins — never introduced at the moment of ending. The timer placed proactively is an antecedent intervention; reactive placement is merely a demand.
Endorsed by: Clinical-Grade | OT + ABA
Price Range: ₹400–₹2,000
Get It
✅Pinnacle Recommends | Clinical-Grade Visual Timer
DIY Version (₹0)
Mobile phone timer with screen facing child. Sand in a clear plastic bottle. Visual shrinkage communicates time passage identically.

ACT II — CARD 09 | MATERIAL 3
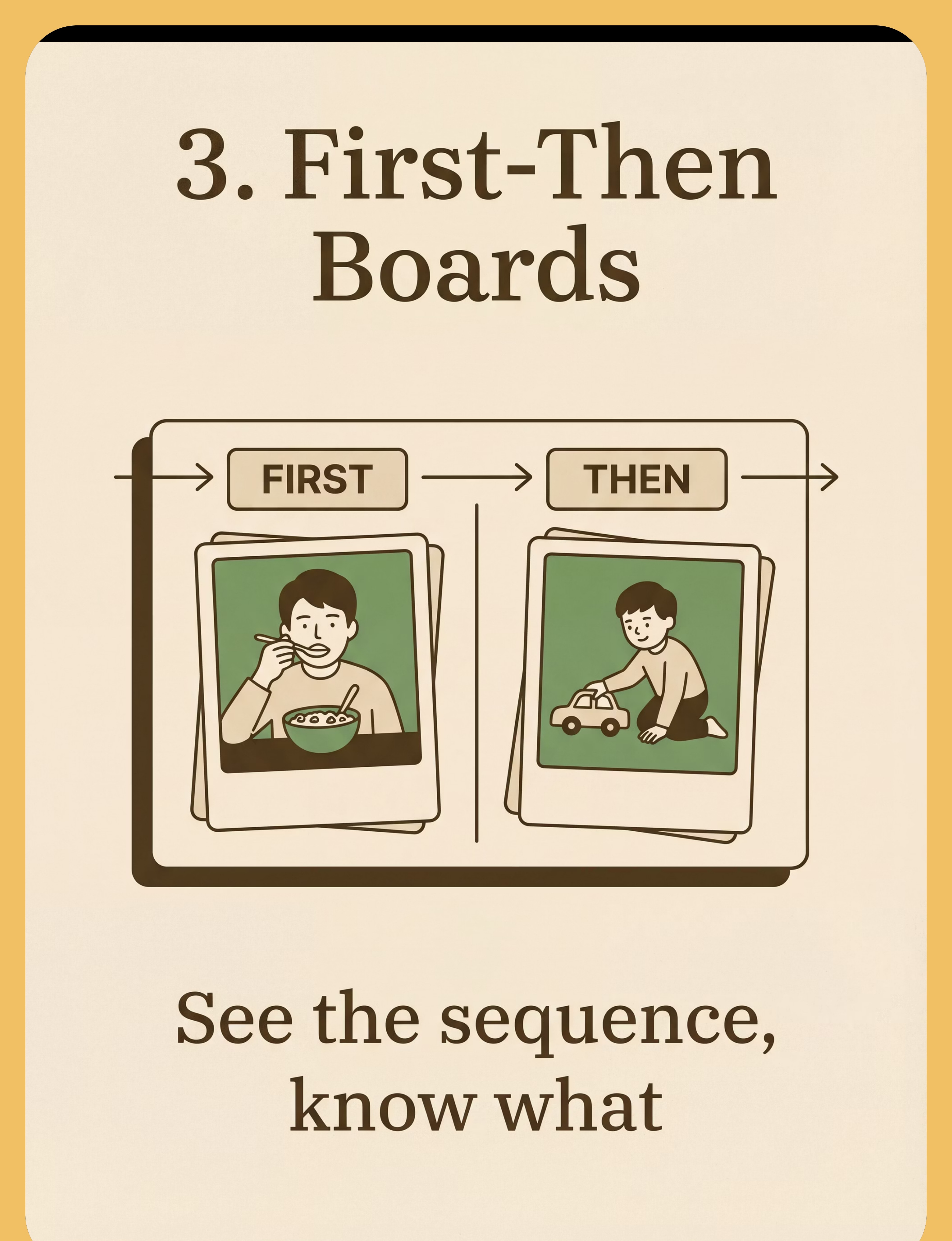
Material 3: First-Then Boards
Canon Category: Visual Schedules / Communication Supports
"Shows the sequence: first this ends, then something good follows."
The First-Then Board communicates the most powerful message in transition support: something good comes after the ending. Rather than experiencing the ending as a loss with nothing replacing it, the child can see that compliance leads to the next positive event. This shifts the neurological framing from "losing something I love" to "the path to something else I want."
Clinical Notes
The contingency structure is what matters — not the board material. Load pictures before the preferred activity begins. Position at child's eye level near the preferred activity zone.
Endorsed by: ABA + SLP
Price Range: ₹200–₹800
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Two sticky notes on the wall or fridge. Draw or write FIRST and THEN. The contingency structure is what matters — not the board material.

ACT II — CARD 09 | MATERIAL 4
Material 4: Transition Objects & Comfort Items
Canon Category: Transition Objects / Comfort Items
"Something constant when everything else changes."
When a preferred activity ends, the child's sensory regulation state is disrupted. A transition object provides a physical, sensory constant that the child can hold, feel, and rely on as the emotional landscape shifts. The familiar texture, weight, and smell of a preferred comfort item communicate regulation when words cannot. It is the child's portable safe base — carried through the transition moment.
Clinical Notes
Introduce the transition object during the preferred activity — not at the ending. It should be a familiar, present item, not one that appears only during distress. Pre-placement in the activity zone is essential.
Endorsed by: OT Sensory
Price Range: ₹100–₹1,000
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Child's existing stuffed animal or favorite toy. Any familiar object. Familiarity IS the therapeutic mechanism — no purchase required.

ACT II — CARD 09 | MATERIAL 5
Material 5: Transition Songs & Audio Cues
Canon Category: Music & Rhythm / Auditory Tools
"Consistent sound signals that a change is coming."
The nervous system responds powerfully to consistent auditory patterns. A dedicated transition song — used exclusively when a preferred activity is about to end — becomes a conditioned stimulus that begins preparing the brain for the shift before any verbal instruction is delivered. Over weeks of consistent use, the melody itself triggers the set-shifting signal, reducing the abruptness of endings. The key is absolute consistency: same song, same context, every ending.
Clinical Notes
Preview and adjust volume — some children have auditory sensitivities that cause timer sounds to escalate distress rather than reduce it. If this material worsens behavior, switch to visual-only alternatives.
Endorsed by: SLP + OT
Price Range: ₹100–₹500
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Parent hums or sings any consistent tune before every ending. The consistency of the audio cue is what trains the nervous system — no purchase required.
ACT II — CARD 09 | MATERIAL 6
Material 6: Transition Countdown Strips & Chains
Canon Category: Visual Schedules / Countdown Materials
"Touch the time. See it disappear. Make the abstract tangible."
Countdown strips and paper chains add a crucial physical, tactile dimension to time awareness that purely visual timers cannot provide. The child touches each link or strip, physically removes it, and watches the count shrink. This multi-sensory engagement — visual + proprioceptive + kinesthetic — deeply reinforces the concept of "fewer left, ending is near." For children who learn through movement and touch, countdown strips may be more effective than any clock-based timer.
Clinical Notes
Small chain links are a choking hazard for children under 3. Use large-format paper strips with young children. Supervise all sessions involving small manipulatives.
Endorsed by: ABA + OT
Price Range: ₹100–₹400
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Tear paper into 5 strips. Count them down together. Physical manipulation of countdown is achievable with any paper scraps.

ACT II — CARD 09 | MATERIAL 7
Material 7: Social Stories & Transition Narratives
Canon Category: Social Stories / Books
"Know what happens before it happens. The power of rehearsal."
Social stories prepare the child's brain for transition events before they occur — during calm, regulated moments, not in the heat of a meltdown. By reading a short, predictable narrative about ending a preferred activity ("Sometimes iPad time has to stop. I feel sad. That's okay. Then I eat lunch. iPad will come back tomorrow."), the child rehearses the emotional and behavioral sequence in a low-stakes context. Over repetitions, the narrative becomes internalized as a script the brain reaches for when the real transition arrives.
Clinical Notes
For non-verbal or language-low children: use photos of your actual home and your actual activities — not generic illustrations. Personalization dramatically increases comprehension and emotional resonance.
Endorsed by: SLP + SpEd
Price Range: ₹200–₹800
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Parent writes 5 sentences: "Sometimes [activity] has to stop. I feel sad. That's okay. I will [next activity]. [Activity] will come back tomorrow." The narrative structure is what prepares the brain — not professional printing.

ACT II — CARD 09 | MATERIAL 8
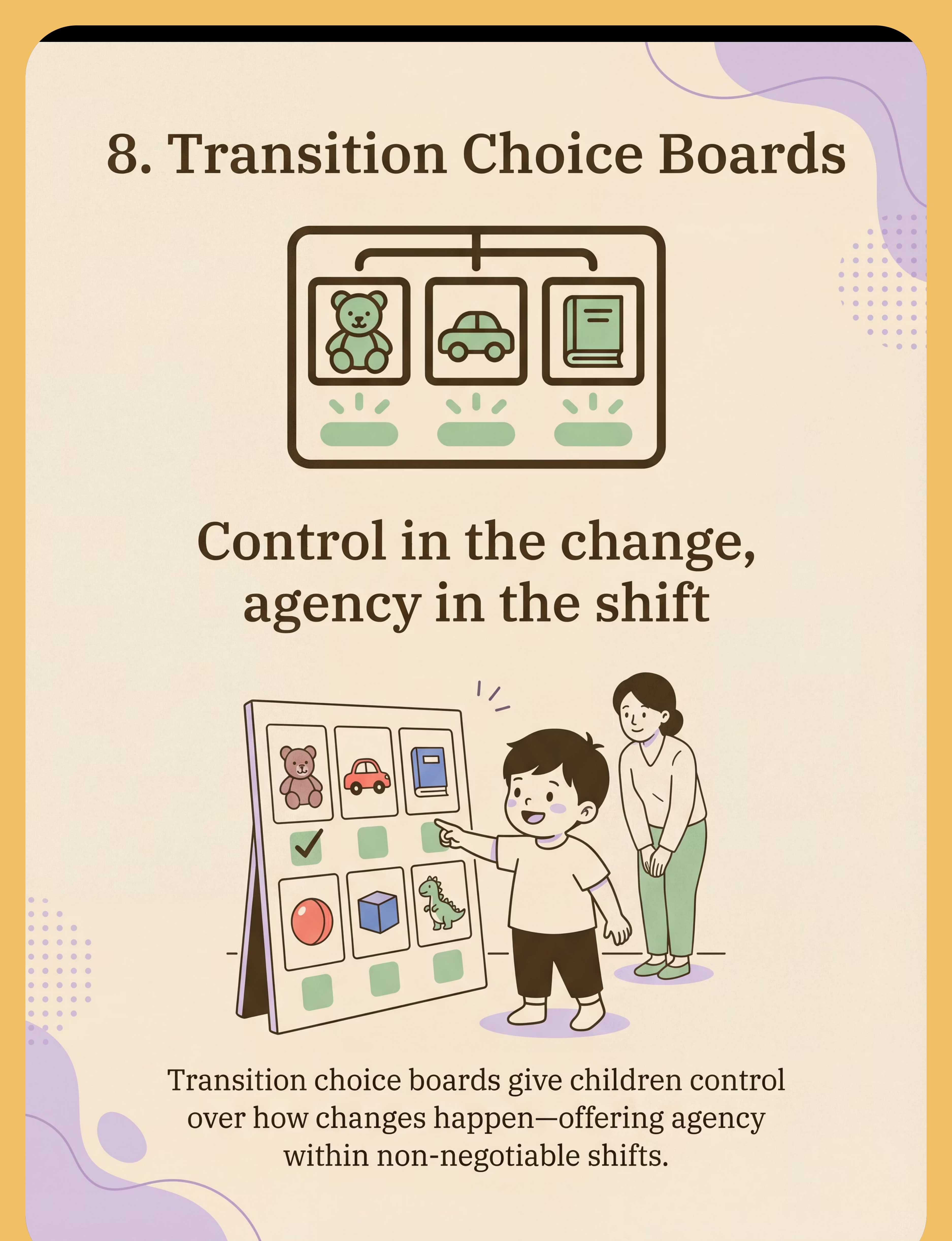
Material 8: Transition Choice Boards
Canon Category: Choice Boards / Visual Decision Tools
"Control in the change. Agency within the necessary shift."
One of the deepest drivers of transition resistance is loss of control. The choice board addresses this directly: instead of a unilateral directive ("stop now, go there"), the child is offered genuine agency within the non-negotiable ending. "Do you want to walk to dinner or skip? Carry your car or leave it?" Both options lead to the same destination — but the child has chosen the path. This neurological shift from "forced" to "chosen" can dramatically reduce protest intensity, because the ending is now, in a meaningful sense, the child's own decision.
Clinical Notes
Limit to 2 genuine options only. More choices overwhelm a dysregulating nervous system. Introduce the choice board in calm, low-stakes moments first — not during a meltdown.
Endorsed by: ABA + SLP
Price Range: ₹200–₹600
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Draw 2 pictures on paper. "Walk to dinner or skip to dinner?" Two genuine choices offered is the therapeutic mechanism — any visual works.

ACT II — CARD 09 | MATERIAL 9
Material 9: Token Boards & Reward Systems
Canon Category: Reinforcement Menus
"See progress. Earn rewards. Build positive associations with endings."
Token boards transform the ending moment from something that is purely aversive into something that earns a visible, tangible reward. Each cooperative transition earns a token; a completed board unlocks a meaningful reinforcer. Over time, the child begins to associate activity endings with earning — a profound neurological reframing. The visual progress bar of the filling token board also provides the child with a concrete, motivating goal that bridges multiple transition moments.
Clinical Notes
Deliver tokens within 3 seconds of cooperative behavior. Reinforce the attempt — not just the perfect ending. Celebrate protest that doesn't escalate to physical aggression. Gradually increase the number of tokens required as mastery builds.
Endorsed by: ABA Validated | BACB Aligned
Price Range: ₹150–₹600
Get It
✅Pinnacle Recommends
DIY Version (₹0)
Draw 5 circles on paper. Color them in with a marker after each good ending. Visual progress tracking is the mechanism — a paper board works identically.
Starter Kit Recommendation: Begin with Materials 2 + 3 + 9 (Visual Timer + First-Then Board + Token Board). This trio addresses the three core needs: time awareness, sequence clarity, and motivation. Total investment: ₹900–₹2,500.

ACT II — CARD 10
DIY & Substitute Options
Every Material Has a ₹0 Version. Start Today.
"No parent should be unable to support their child because of resource barriers. Every technique in the Pinnacle system has a household-material equivalent." — WHO/UNICEF Equity Principle
Material | ₹0 DIY Version | Why It Works | |
Visual Transition Schedule | Paper + pen + stick figures on A4 sheet. Draw boxes for NOW and NEXT. | Same visual predictability principle — the brain doesn't require lamination to process sequence. | |
Visual Timer | Mobile phone timer with screen facing child. Sand in a clear plastic bottle. | Visual shrinkage/flow communicates time passage identically. | |
First-Then Board | Two sticky notes on the wall or fridge. Draw or write FIRST and THEN. | The contingency structure is what matters — not the board material. | |
Transition Object | Child's existing stuffed animal or favorite toy. Any familiar object. | Familiarity IS the therapeutic mechanism — no purchase required. | |
Transition Song | Parent hums or sings any consistent tune before EVERY ending. | The consistency of the audio cue is what trains the nervous system. | |
Countdown Strip | Tear paper into 5 strips. Count them down together. | Physical manipulation of countdown is achievable with paper scraps. | |
Social Story | Parent writes 5 sentences about the sequence: stop → feel → okay → next → return. | The narrative structure is what prepares the brain — not professional printing. | |
Choice Board | Draw 2 pictures on paper. "Walk to dinner or skip to dinner?" | 2 genuine choices offered is the therapeutic mechanism — any visual works. | |
Token Board | Draw 5 circles on paper. Color them in with a marker after each good ending. | Visual progress tracking is the mechanism — a paper board works identically. |
Clinical Precision Note: When a child has significant sensory processing needs, clinical-grade materials (weighted items, specific textures, calibrated timers) may provide measurably better outcomes. DIY versions are excellent starting points — discuss clinical-grade options with your OT.

ACT III: THE EXECUTION — CARD 13
Is Your Child Ready? The Readiness Check
60 Seconds Before You Begin. The Best Session Starts Right.
Indicator | What to Look For | Check | |
Fed and hydrated? | Last meal within 90 minutes. Not asking for food. | ✅ / ❌ | |
Rested? | Not visibly fatigued. Eyes tracking normally. | ✅ / ❌ | |
Regulated? | No current signs of sensory overload or distress. | ✅ / ❌ | |
No recent crisis? | No meltdown in past 45 minutes. | ✅ / ❌ | |
Timer already visible? | Timer was set BEFORE preferred activity began. | ✅ / ❌ | |
Next activity ready? | What comes after is already prepared — no delay. | ✅ / ❌ | |
Parent calm? | You are regulated. You have your materials. You have a plan. | ✅ / ❌ |
6–7 Checks ✅ → GO
Proceed with full protocol as designed.
4–5 Checks ✅ → MODIFY
Shorten session, reduce demands, use simpler transition. Extend warning time to 10 minutes. Accept partial success as success.
Under 4 ✅ → POSTPONE
Offer calming activity. Try again in 30 minutes. Offer proprioceptive input or preferred calming sensory experience. Never force a session when conditions aren't right.
"The best session is one that starts right. A postponed session is not a failure — it is a data point and a professional choice."

STEP 1 OF 6
Step 1: The Advance Warning
Timing: 15–20 Minutes Before Ending
The Principle: Transition support begins before the preferred activity — not at the moment of ending. Setting the timer and showing the First-Then Board when the activity begins trains the child's nervous system to expect an endpoint, rather than experiencing it as a sudden interruption.
"[Child's name], we're going to play with [preferred activity]. Look — [point to timer] — when the red is all gone, it will be time to stop. And then [point to THEN picture on board] we'll have dinner/bath/[next activity]. Ready? Let's play!"
Body Language Guidance
- Crouch to child's level when delivering this message
- Point physically to the timer AND the First-Then Board
- Warm, matter-of-fact tone — not apologetic, not anxious, not negotiating
- Then step back and let the child engage freely with the preferred activity
Child Response Guide
Acceptance cues: Glances at timer and returns to play | Nods or repeats part of message | Ignores and continues playing (all acceptable)
Resistance signals: "No, NO stopping!" → Acknowledge: "You want to keep playing. The timer will tell us when." | Pulls timer away → Place out of reach but still visible
NCAEP (2020) classifies antecedent-based interventions as evidence-based practice for ASD.

STEP 2 OF 6
Step 2: The 5-Minute Warning
Timing: When Approximately 5 Minutes Remain on Timer
The Purpose: The 5-minute warning is the first explicit verbal cue that anchors to the already-visible timer. It is NOT introducing new information — it is narrating what the child can already see.
"[Child's name], look at the timer — 5 more minutes, then we stop [preferred activity]. See? [Point to timer.] 5 minutes. Then [point to THEN picture] dinner/bath/[next activity]."
If Using Countdown Strip — Add:
"Let's take off a link! [Remove one paper chain link or flip a countdown card.] 4 more links, then all done."
"Let's take off a link! [Remove one paper chain link or flip a countdown card.] 4 more links, then all done."
Child Engagement Notes
- If highly engaged: deliver warning and step back — do not interrupt the activity
- If child looks up: make eye contact, point to timer, say script, give thumbs up
- If child ignores: deliver anyway. The timer is doing the work — the verbal is reinforcing
Critical Principle
"The warning is not a negotiation opening. Deliver it warmly and confidently, then step back. You are providing information, not seeking permission."
Timing Discipline: Honor the timer. Do not extend. Extending once teaches the child that the timer is negotiable — and destroys its predictive power across all future transitions.

STEP 3 OF 6
Step 3: The Final Warning & Transition Object
Timing: 2 Minutes Before Ending
"[Child's name] — 2 more minutes. Last ones. When the timer beeps, [preferred activity] is all done for now. You'll have it again [tomorrow/after dinner/later]. 2 minutes."
The Transition Object Move
If the child has a designated transition object (stuffed animal, sensory fidget, comfort toy), bring it physically into the preferred activity zone now — place it beside the child. Do not comment on it. Simply have it available.
This pre-places the regulatory anchor before the ending, so the child can reach for it naturally rather than having it introduced as part of the demand.
Transition Song Cue
Begin humming or softly playing the designated transition song 1–2 minutes before ending. The melody itself signals "change is coming" and begins the neurological preparation.
What the Child's Nervous System Is Doing
The anterior cingulate cortex is beginning to fire its set-shifting signal — supported by the consistent environmental cues (shrinking timer, familiar melody, object nearby). The brain is being given lead time to prepare.
NCAEP (2020): Transition-based teaching + antecedent-based interventions evidence base. Sensory Integration: Proprioceptive/comfort input during transition preparation — OT clinical consensus.
STEP 4 OF 6
Step 4: The Ending Moment (Timer Beeps)
Timing: When Timer Signals
"Timer's done! [Activity] is all done. [Child's name], you did such good waiting. Now [point to THEN picture on board] — it's [next activity] time. Let's go! [Offer choice board if prepared: 'Do you want to walk or skip to dinner?']"
1. Narrate, Don't Negotiate
The timer ending is a fact, not a request. Deliver warmly but clearly. "Timer's done" — not "Sweetie, it's time to stop now if that's okay..."
2. Offer the Choice (Agency Within the Ending)
Present the choice board immediately: "Walk to the bathroom or hop?" This shifts focus from "NO, I won't stop" to "which way shall I go?"
3. Token Delivery Timing
If the child transitions cooperatively — or even with protest but without physical escalation — deliver a token IMMEDIATELY with specific praise: "You stopped so well! You earned your token!"
4. If Resistance Begins
Remain calm. Kneel. Warm eye contact. Repeat script once. Do not engage with protest beyond one repetition. Offer transition object. Offer choice board again. After 3–5 minutes, use gentle physical guidance with minimal language.
"The ending moment is the clinical moment. The goal is not a meltdown-free ending every time immediately — the goal is a progressively shorter, less intense ending over weeks."

STEP 5 OF 6
Step 5: Reinforce & Celebrate
Timing: Within 3 Seconds of Cooperative Transition
The Science of Reinforcement Timing: Reinforcement delivered within 3 seconds of the desired behavior is neurologically linked to that behavior. Beyond 10 seconds, the association weakens significantly. This is not a parenting philosophy — it is neurological fact.
"You STOPPED! I'm so proud of you! You waited for the timer and then you came! Token time — [child places or receives token]! That was amazing."
Verbal Praise
Enthusiastic, specific: "You stopped when the timer beeped!" Generic praise is less effective than naming the exact behavior.
Token / Sticker
Visual progress on the token board. Token Board ₹364 → | Reinforcement Set ₹589 →
Physical Affirmation
High-five, fist bump, brief hug if child accepts. Match the child's sensory comfort level.
Tangible Reward
Small preferred snack or 5 extra minutes of preferred activity later — when token board is complete.
Celebrate the Attempt: If the child transitioned with protest but without physical aggression — that IS progress. Token it. Name it. Celebrate it. Do NOT withhold reinforcement during protest that doesn't escalate. You are reinforcing the stopping behavior — not requiring a happy face.
STEP 6 OF 6
Step 6: The Cool-Down
Timing: Immediately Post-Transition | 1–3 Minutes
The Purpose: No session ends with the ending. The cool-down bridges the child from the emotional territory of transition into the next activity. Even a successful transition may leave mild residual dysregulation — the cool-down resolves it before the next activity begins.
"Great job finishing! Let's take a big breath. [Breathe together.] Now — [next activity] is ready for you. [Preferred activity] will be here again [tomorrow/after dinner]. It's waiting for you."
Cool-Down Activity Options (1–2 Minutes)
- 3 deep breaths together (co-regulation)
- Brief proprioceptive input: carry something heavy to the next location (books, a bag)
- Allow child to hold transition object for first minute of next activity
- Sing the last verse of the transition song together while walking to next activity
Bridging Move
Allow the child to bring ONE small item from the preferred activity to the next location briefly. "Bring your car to dinner — he can sit on the table." After child is settled, the item can be put away without resistance.
Material Put-Away Ritual
If age/ability appropriate, have child participate in putting preferred activity materials away. "Help me put the trains in the box — then we go eat." Participation in ending creates ownership of the closure.
If Child Resists Ending
Stay warm and calm. Wait. Do not escalate. The timer has done its work. Give the nervous system 3–5 minutes to self-regulate. Provide sensory input (deep pressure, proprioception). Then re-approach.

ACT III — CARD 21
What If It Didn't Go as Planned?
Most Sessions Don't Go Perfectly. Here's What to Do.
"Session abandonment is not failure — it's data. Every difficult session tells your therapist something valuable about your child's current profile."
❓ Child threw the timer
Why: Timer introduced reactively (at ending) rather than proactively (at beginning). Or timer associated with loss.
Fix: Next session: set the timer BEFORE the activity begins. Try a different timer format (sand timer vs. digital).
Fix: Next session: set the timer BEFORE the activity begins. Try a different timer format (sand timer vs. digital).
❓ Choice board was ignored
Why: Too many choices, or child couldn't process the visual in a moment of dysregulation.
Fix: Reduce to 2 options only. Introduce choice board in a calm moment first. Practice choice-making in low-stakes situations.
Fix: Reduce to 2 options only. Introduce choice board in a calm moment first. Practice choice-making in low-stakes situations.
❓ Token board working but transition still takes 20 minutes
Why: This timeline is appropriate — token systems take 2–4 weeks to show transition time reduction. You are in the building phase.
Fix: Continue consistently. Do not raise the bar yet. Consistency now = compression later.
Fix: Continue consistently. Do not raise the bar yet. Consistency now = compression later.
❓ Transition song makes it worse
Why: Some children are auditory-sensitive. The musical cue may increase anxiety rather than reduce it.
Fix: Switch to visual-only countdown. Remove auditory cue. Assess auditory sensitivity with OT.
Fix: Switch to visual-only countdown. Remove auditory cue. Assess auditory sensitivity with OT.
❓ First-Then Board is ripped off the wall
Why: In dysregulation, anything nearby becomes a target.
Fix: Move board to less physically accessible location. Use digital version on device. Maintain it anyway — consistency matters even when disrupted.
Fix: Move board to less physically accessible location. Use digital version on device. Maintain it anyway — consistency matters even when disrupted.
❓ Cooperative with one parent but not the other
Why: Inconsistency across adults destroys the system. Consistency between caregivers is the strongest variable in transition success.
Fix: Both caregivers must use identical scripts, same timer, same materials. Share this page with all caregivers. See Card 37.
Fix: Both caregivers must use identical scripts, same timer, same materials. Share this page with all caregivers. See Card 37.
❓ Child became severely distressed (self-harm or aggression)
Why: Session demand may have exceeded the child's current regulatory capacity.
Fix: Stop immediately. Provide safety. Call 📞9100 181 181 for immediate clinical guidance. Document and discuss with your OT/BCBA.
Fix: Stop immediately. Provide safety. Call 📞9100 181 181 for immediate clinical guidance. Document and discuss with your OT/BCBA.

ACT IV: THE PROGRESS ARC — CARD 23
Week 1–2: What to Expect
15%
Weeks 1–2: Baseline Setting
You are building the infrastructure. Visible outcomes emerge in weeks 3–8.
✅ Expect to See
- Child begins to look at timer (even without acting on it) — neural tracking is beginning
- Transition time still 10–20 minutes, but slightly decreasing
- One or two sessions with noticeably less intense protest — inconsistent but present
- Child occasionally repeats "then dinner" or refers to First-Then Board — comprehension forming
❌ Do NOT Expect Yet
- Meltdown elimination — this is baseline establishment
- Consistent compliance — variability is normal in weeks 1–2
- Generalization to other caregivers or settings — too early
- Child using materials independently
"If your child tolerates the material for 3 seconds longer than last week — that is real, measurable, neurological progress."
Data to Track: Duration from timer beep to movement. Record daily. Look for any directional trend — even 30 seconds shorter is data showing the system is having effect.
PMC11506176 | Systematic review: Transition intervention outcomes emerge across 8–12 week timelines. Early-phase indicators: tolerance and participation rather than skill mastery.

ACT IV — CARD 24
Week 3–4: Consolidation Signs
40%
Weeks 3–4: Consolidation Phase
The system is taking hold. Neural pathways are forming.
Consolidation Indicators — What the Child Shows
🧠 Anticipatory Behavior
Child looks at timer unprompted. May walk to it. May refer to First-Then Board without prompting — the external scaffold is becoming internal.
🗣️ Language Emergence
"Timer not done yet." "Then snack." "5 more minutes?" — spontaneous use of transition language signals deep comprehension forming.
📉 Reduced Intensity
Peak meltdown level decreasing from 5 → 3–4. Duration shortening from 20 minutes → 8–12 minutes. These are measurable neurological changes.
🤝 Cooperation with Materials
Child no longer throws or avoids timer. Begins to engage with countdown strip or token board. Materials are becoming familiar tools, not threats.
"You may notice that you are more confident. You know the script. You trust the timer. Your regulated affect is itself a therapeutic input — your child's nervous system reads yours."
When to Increase Frequency: If you have been using the protocol for the most difficult transitions only — in weeks 3–4, begin extending to all preferred-activity endings. Build the generalization.

ACT IV — CARD 25
Week 5–8: Mastery Indicators
75%
Weeks 5–8: Mastery Phase
The badge unlocks. Here's what mastery looks like — specific, observable, measurable.
Transition Within 5 Minutes
Child transitions within 5 minutes of timer beep, 4 out of 5 sessions, for two consecutive weeks.
Independent Board Reference
Child refers to First-Then Board independently before ending (unprompted) in at least 3 sessions.
Intensity Level 1–2
Meltdown intensity at endings is consistently Level 1–2 — brief verbal protest, no physical aggression, rapid recovery.
Generalization
Skill generalizes to at least one setting beyond home — school transition, grandparents' house, community outing.
Material Independence
Child can accept "timer broken today — let's use 5 fingers countdown" without severe dysregulation, demonstrating the skill lives in the child, not the material.
🏅PINNACLE MASTERY UNLOCKED: I-787 — End of Preferred Activity
TRANSITION FLEXIBILITY: LEVEL 1 | Ready to advance to: I-788
Maintenance Check: Does the skill persist through a 2-week holiday without consistent practice? If yes — the skill is internalized. If significant regression occurs — extend consolidation before advancing.
TRANSITION FLEXIBILITY: LEVEL 1 | Ready to advance to: I-788
Maintenance Check: Does the skill persist through a 2-week holiday without consistent practice? If yes — the skill is internalized. If significant regression occurs — extend consolidation before advancing.

ACT IV — CARD 27
Red Flags: When to Pause
Even in the Success Zone — Trust Your Instincts.
🚨 Regression After Mastery
Skills that were solid for 3+ weeks suddenly and severely regress without environmental explanation. This may indicate underlying medical, sensory, or psychological change requiring assessment.
🚨 Escalating Aggression
Physical aggression during transitions that is increasing rather than decreasing after 4+ weeks of consistent protocol use. This requires functional behavior assessment — not just more materials.
🚨 Extreme Anxiety About Endings
Child is showing significant anxiety about activity endings BEFORE they happen — checking for timers obsessively, refusing to begin preferred activities due to fear of ending. May indicate anxiety disorder requiring psychological support.
🚨 No Progress After 8 Weeks
If intensity and duration of transition difficulty shows no directional improvement after 8 consistent weeks, a formal functional assessment by OT + BCBA is warranted.
🚨 Self-Injurious Behavior
Any emergence or increase in self-injurious behavior during transitions requires immediate professional assessment. Do not attempt to continue protocol until evaluated.
📞FREE Pinnacle Helpline: 9100 181 181 — Available 24×7 | 16+ Languages
"Trust your instincts. You know your child. If something feels wrong, pause and ask. That is not overreaction — that is parent expertise."
"Trust your instincts. You know your child. If something feels wrong, pause and ask. That is not overreaction — that is parent expertise."

ACT IV — CARD 28
The Progression Pathway
You Are Not Done. You Are On a Journey.
Prerequisite Mastery Check
Before advancing to I-788 (Screen-to-Non-Screen), ensure:
- Visual timer is being used proactively (before activity begins)
- Transition occurs within 5 minutes consistently
- Child references First-Then Board independently
Your Next-Level Path
Path A — Screen activities hardest: → I-788: Screen to Non-Screen
Path B — Dinner/bath/bedtime remain hard: → I-790/I-791/I-792
Path C — Unexpected changes still severe: → I-801: Unexpected Transitions
This technique feeds directly into the Independence Readiness Index + Daily Living Readiness Index — GPT-OS® tracks this progression toward full transition flexibility across all life domains.
ACT IV — CARD 29
Related Techniques in This Domain
Domain I: Transitions & Life Events — You Are Part of a Complete System.
Technique | Code | Difficulty | Your Materials | |
9 Materials That Help With All Transitions | I-781 | 🟡 CORE | ✅ Timer + First-Then Board | |
9 Materials That Help With Morning Transitions | I-782 | 🟡 CORE | ✅ Schedule + Timer | |
9 Materials That Help With Activity Changes | I-786 | 🟢 INTRO | ✅ Full Kit | |
9 Materials That Help With End of Preferred Activity | I-787 | 🟡 CORE | ★ YOU ARE HERE | |
9 Materials That Help With Screen to Non-Screen | I-788 | 🟠 ADVANCED | ✅ Timer + Token Board | |
9 Materials That Help With Transition Warnings | I-793 | 🟡 CORE | ✅ Countdown Strip | |
9 Materials That Help With Transition Objects | I-795 | 🟢 INTRO | ✅ Comfort Items | |
9 Materials That Help With Bedtime Transition | I-792 | 🟠 ADVANCED | ✅ Social Stories |
Materials You Already Own: If you've completed I-787, you own: Visual Timer, First-Then Board, Token Board, Transition Object, Social Story, Countdown Strip, Choice Board. These 7 materials cover 80% of Domain I techniques. You are already equipped.
ACT IV — CARD 30
Your Child's Full Developmental Map
This Technique Is One Piece of Your Child's Entire Developmental Journey.
The Whole-Child Perspective
"This technique is one piece of a larger plan. A child who masters activity endings is also building emotional regulation, executive function, and family harmony — gains that ripple across all 12 domains. This is not isolated skill training. This is whole-child development."
GPT-OS® Integration
See your child's progress tracked across all 12 domains, 349 skills, and 79 developmental abilities.
Powered by AbilityScore® | WHO/UNICEF Nurturing Care Framework (2018)
ACT V: THE COMMUNITY & ECOSYSTEM — CARD 31
Families Who've Been Here
From the Same Crisis. To a Different Daily Life.
"We couldn't go to the park anymore. Every single time — guaranteed 45-minute meltdown in the parking lot. He would scream, hit me, lie on the ground. The neighbors saw. I stopped taking him anywhere. We were prisoners of his preferred activities."
After (14 weeks, Pinnacle Hyderabad Center):
"Last Saturday we went to the park. I set the visual timer when we arrived. When it beeped, I showed him the First-Then Board — 'First goodbye to park, then McDonald's.' He said 'bye park, bye slide.' And walked with me to the car. I cried in the car. He sang to himself."
— Parent, Pinnacle Network | Child age 6, ASD Level 2
"Screen time was our nightmare. We knew it would be a battle every single time. So we stopped giving screens entirely — which meant our son had nothing calming. Then we were told to use screens therapeutically but transition off them with structure. I didn't believe it would work."
After (8 weeks, Home Protocol):
"He now SETS the timer himself before he starts YouTube. He says 'five minutes timer, then eat.' Yesterday he told his father 'timer done, bye phone.' My husband thought I was exaggerating. He's not anymore."
— Parent, Pinnacle Online Community | Child age 8, ADHD + ASD
Clinical Note: Individual results may vary. Outcomes depend on child's specific profile, caregiver consistency, protocol adherence, and co-occurring conditions. These are representative outcomes from the Pinnacle clinical network.
"This child's transition duration reduced from 45+ minutes to under 8 minutes over 14 weeks. The key was parental consistency — same timer, same script, same materials, same caregiver across mother, father, and grandmother."
"This child's transition duration reduced from 45+ minutes to under 8 minutes over 14 weeks. The key was parental consistency — same timer, same script, same materials, same caregiver across mother, father, and grandmother."

ACT V — CARD 32
Connect With Other Parents
You Should Not Be Doing This Alone.
"Isolation is the enemy of adherence. Parents who implement home therapy alone are significantly more likely to abandon protocols in weeks 3–4. Parents who implement with community — even one other family navigating the same thing — are significantly more likely to see the 8-week outcomes."
WhatsApp Parent Group
Active parents using I-787 and related Domain I techniques. Share wins, ask questions, stay motivated.
Online Community
Moderated forum. Verified parents. Therapist-supported discussions.
Peer Mentoring
Connect with an experienced parent who has completed I-787 and can walk with you through the process.
Local Parent Meetups
Organized through your nearest Pinnacle center. Check for local schedule.
"Your experience — your wins, your hard weeks, your learned adjustments — is clinical data that helps another family. Consider sharing your journey. You are not just a parent. You are a node in a system that is changing outcomes for children across India and 70+ countries."

ACT V — CARD 33
Your Professional Support Team
Home Therapy Works Best When Backed by Professionals Who Know Your Child.
Discipline | What They Add to Your Home Protocol | |
Occupational Therapist | Sensory profile assessment. Identifies which sensory inputs in preferred activities are most dysregulating. Customizes transition object selection and environmental setup. | |
BCBA / ABA Therapist | Functional behavior assessment. Identifies the specific function of transition resistance (escape, sensory, attention). Optimizes reinforcement schedule and token system design. | |
Speech-Language Pathologist | Language comprehension assessment. Creates personalized social story. Ensures transition language matches child's receptive level and AAC vocabulary. | |
NeuroDev Pediatrician | Rules out medical factors (sleep deprivation, anxiety, sensory processing disorder). Advises on medication support where clinically relevant. |
"Home + clinic = maximum impact. A parent who practices 5 days at home and attends one clinic session per week generates 6× the intervention dosage of clinic-only therapy. You are not supplementing professional care — you ARE a core part of the therapeutic team."
Book Your Support
Available in 16+ languages | For families outside Pinnacle center network
📞FREE National Autism Helpline: 9100 181 181 — 24×7 | 16+ Languages
ACT V — CARD 34
The Research Library
For the Curious Parent. The Full Evidence Base.
📚 PMC11506176 — PRISMA Systematic Review (2024)
16 articles (2013–2023): Structured visual and behavioral supports for activity transitions meet evidence-based practice criteria for ASD. Children journal.
Read on PubMed →
Read on PubMed →
📚 PMC10955541 — Meta-Analysis (2024)
24 studies confirm visual, behavioral, and environmental transition supports effectively reduce meltdown frequency and improve family quality of life. World J Clin Cases.
Read on PubMed →
Read on PubMed →
📚 Indian RCT — Padmanabha et al. (2019)
Home-based structured behavioral intervention demonstrated significant improvement in transition compliance in Indian pediatric ASD population. Indian J Pediatr.
Read Full Study →
Read Full Study →
📚 NCAEP Evidence-Based Practices Report (2020)
Visual supports, antecedent-based interventions, and reinforcement systems classified as evidence-based practices for autism spectrum disorder.
Access NCAEP Report →
Access NCAEP Report →
📚 WHO Nurturing Care Framework (2018) + CCD Package (2023)
Responsive caregiving and structured home intervention cited as essential components of child development across 197 countries.
Access WHO NCF →
Access WHO NCF →
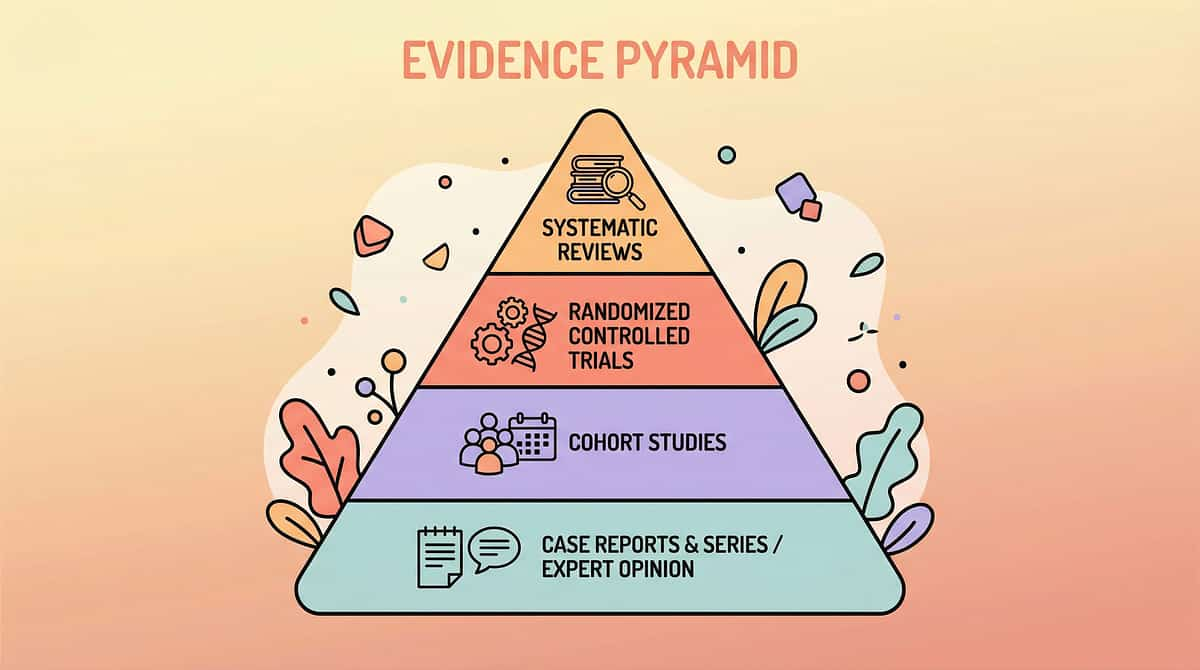
Citation Standard: Oxford Centre for Evidence-Based Medicine (OCEBM) levels of evidence.
ACT V — CARD 35
How GPT-OS® Uses Your Data
Your Sessions Power the World's Most Advanced Pediatric Therapy Intelligence.
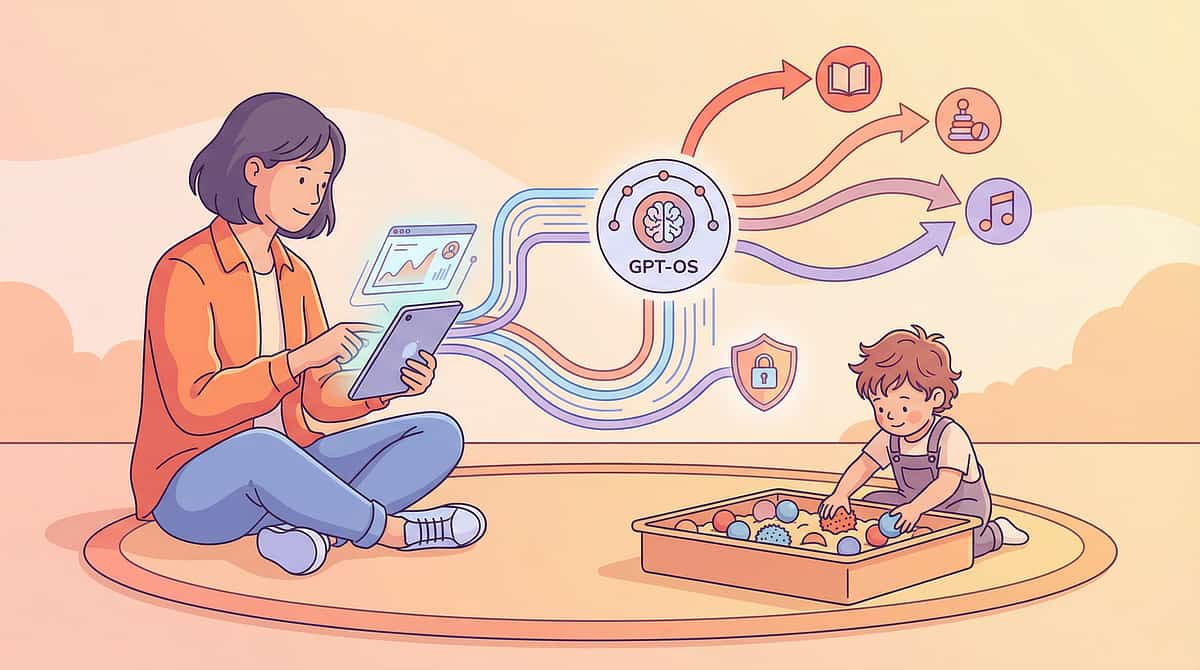
What GPT-OS® Learns From I-787 Data
- Optimal warning window for YOUR child (5 min vs. 10 min vs. 20 min)
- Which materials produce fastest transition for YOUR child's profile
- Trajectory prediction: when your child is likely to hit mastery criteria
- Comparison with 20M+ session database to identify what works for similar profiles
Privacy Assurance
"Your child's data is stored in a de-identified, encrypted system. Your data helps every child like yours — while your child's identity is protected. We do not sell, share, or use data outside of therapeutic improvement purposes."
Population-Level Impact
Every family that uses GPT-OS® contributes to a dataset that makes recommendations more precise for all families. Your data helps a parent in Chennai, in Kolkata, in Dubai, in London.
ACT V — CARD 36
Watch the Reel
Watch the 60-Second Reel That Surfaces This Challenge.
Reel Metadata
Reel ID: I-787
Title: 9 Materials That Help With End of Preferred Activity
Series: Domain I — Transitions & Life Events
Episode: 787 of 999
Duration: 60–75 seconds
Presented by: Pinnacle Blooms Consortium Therapist Team
Title: 9 Materials That Help With End of Preferred Activity
Series: Domain I — Transitions & Life Events
Episode: 787 of 999
Duration: 60–75 seconds
Presented by: Pinnacle Blooms Consortium Therapist Team
Therapist Introduction
"In this reel, our therapy team walks through the 9 materials that make ending preferred activities survivable — for your child and your family. The science is real. The materials are available in India. The protocol works. Here's what to use and how."
Related Reels in This Series
NCAEP (2020): Video modeling is an evidence-based practice for ASD. Multi-modal learning (visual + text + video demonstration) improves parent skill acquisition.

ACT V — CARD 37
Share This With Your Family
This Protocol Only Works If Everyone Uses It. Consistency Is the Mechanism.
"Consistency across caregivers multiplies impact. A child who experiences this protocol from one parent but not from the other, or at home but not at school, has fundamentally weaker consolidation than a child whose entire environment uses the same system."
Share & Download
"Explain to Grandparents" — Simplified Version
"When [child's name] is doing something he loves and we need to stop it, his brain genuinely finds it hard. We use a special timer and a picture board every time. The timer starts BEFORE the activity. When it beeps, we say [script]. Please do the same — every time. Consistency is what helps his brain learn."
WHO CCD Package: Multi-caregiver training critical for intervention generalization. PMC9978394

ACT VI: THE CLOSE & LOOP — CARD 38
Frequently Asked Questions
Questions Every Parent Asks. Answered by the Consortium.
❓ Q1: My child ignores the timer entirely. Should I drop it?
No. Ignoring the timer is normal in weeks 1–2. The timer's effect is cumulative. What builds the association is consistent use — not immediate response. Continue using it even when ignored. Within 3–4 weeks, most children begin to track it visually. → See Card 23
❓ Q2: How do I handle a meltdown that's already started?
Stop all demands. Do not repeat the transition instruction. Provide safety. Offer sensory regulation support (transition object, proprioceptive input). When the child is calm (Level 1–2), complete the transition — but with reduced demands. Never abandon the transition entirely (it teaches that meltdowns delay transitions indefinitely). → See Card 21
❓ Q3: Does this work for children with little or no language?
Yes — and the visual materials (timer, First-Then Board with photos, transition object) are MORE effective for non-verbal children than verbal warnings alone. Remove language demands from the protocol; increase visual supports. AAC device with "ALL DONE" → "EAT/BATH" sequence pre-loaded. → See Card 22
❓ Q4: Should I give extra time after the timer to avoid a meltdown?
No. This is the most common error families make, and it destroys the system. If you extend time after the timer, the child learns the timer is negotiable — and every future transition will be contested. Honor the timer every time. → See Card 15
❓ Q5: What if the preferred activity is a therapy-related activity?
Same protocol applies. Even therapeutic activities must end. The skill being built is generalized activity-ending, not category-specific. Your therapist will agree that ending therapeutic activities gracefully is itself a therapeutic goal.
❓ Q6: Is it okay to use iPad/screen as the "THEN" reward?
In the short term, yes — if screen is the most motivating reinforcer. In the long term, gradually diversify the reward menu so the child builds flexibility around rewards as well as activities. Your BCBA can guide the fading process. → See Card 18
❓ Q7: We've been consistent for 8 weeks and see no improvement. What now?
Request a formal functional behavior assessment from a BCBA. Lack of progress after consistent 8-week implementation indicates either: (a) an unidentified function driving the behavior, (b) a sensory/medical factor not yet addressed, or (c) a co-occurring anxiety profile requiring psychological support. This is not a failure — it's data that guides the next step. 📞 9100 181 181 → See Card 27
❓ Q8: At what age should we expect full independence without visual supports?
For neurotypical children, 8–10 years. For children with ASD, this varies widely — some will use visual supports into adolescence and that is clinically appropriate and successful. The goal is functional independence, not material-independence. A 12-year-old who manages activity endings smoothly using a timer is succeeding.

ACT VI — CARD 39
Your Child's Next Transition Can Be Different.
Start Today.
You have the science, the materials, the protocol, the progress map, and the community. This knowledge is yours. Your child's transitions can change. The brain that struggles to stop today is the brain that will manage change independently tomorrow — because of you, and the consistent, scientific, loving work you are willing to do.
📞FREE National Autism Helpline: 9100 181 181
Available 24×7 | 16+ Languages | No Cost. No Registration.
Available 24×7 | 16+ Languages | No Cost. No Registration.
🏛️ Validated By
Pinnacle Blooms Consortium | OT • SLP • ABA/BCBA • SpEd • NeuroDev • CRO
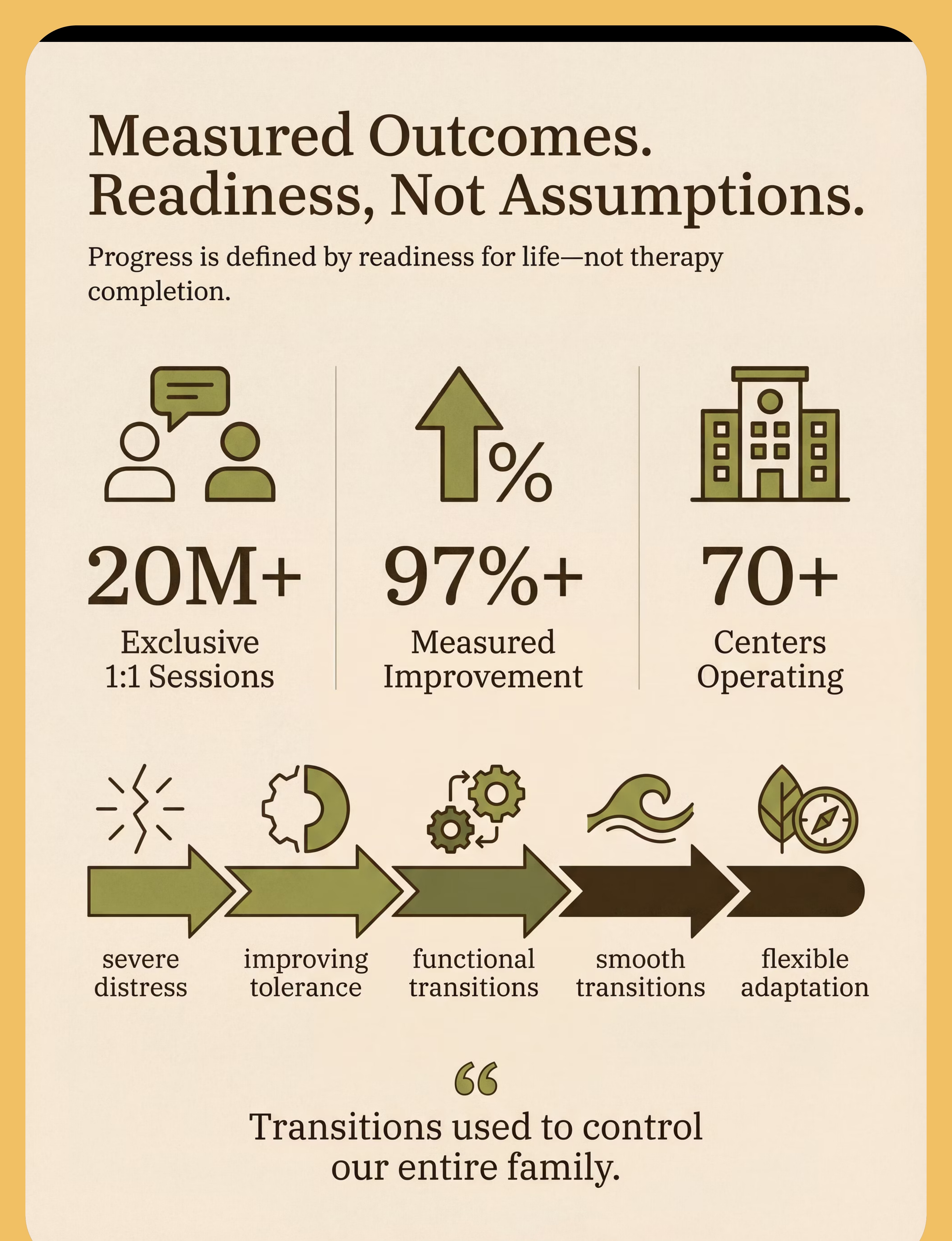
20M+ Sessions
1:1 clinical sessions across 70+ centers | 97%+ Measured Improvement
160+ Countries
Patents filed | GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™
Preview of 9 materials that help with end of preferred activity Therapy Material
Below is a visual preview of 9 materials that help with end of preferred activity therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

ACT VI — CARD 40 | THE PINNACLE PROMISE
The Pinnacle Promise
"From fear to mastery. One technique at a time."
You arrived on this page scared, exhausted, and searching for something real. You now have the science, the materials, the protocol, the progress map, and the community. This knowledge is yours. Your child's transitions can change. The brain that struggles to stop today is the brain that will manage change independently tomorrow — because of you, and the consistent, scientific, loving work you are willing to do.
🏛️ Pinnacle Blooms Network®
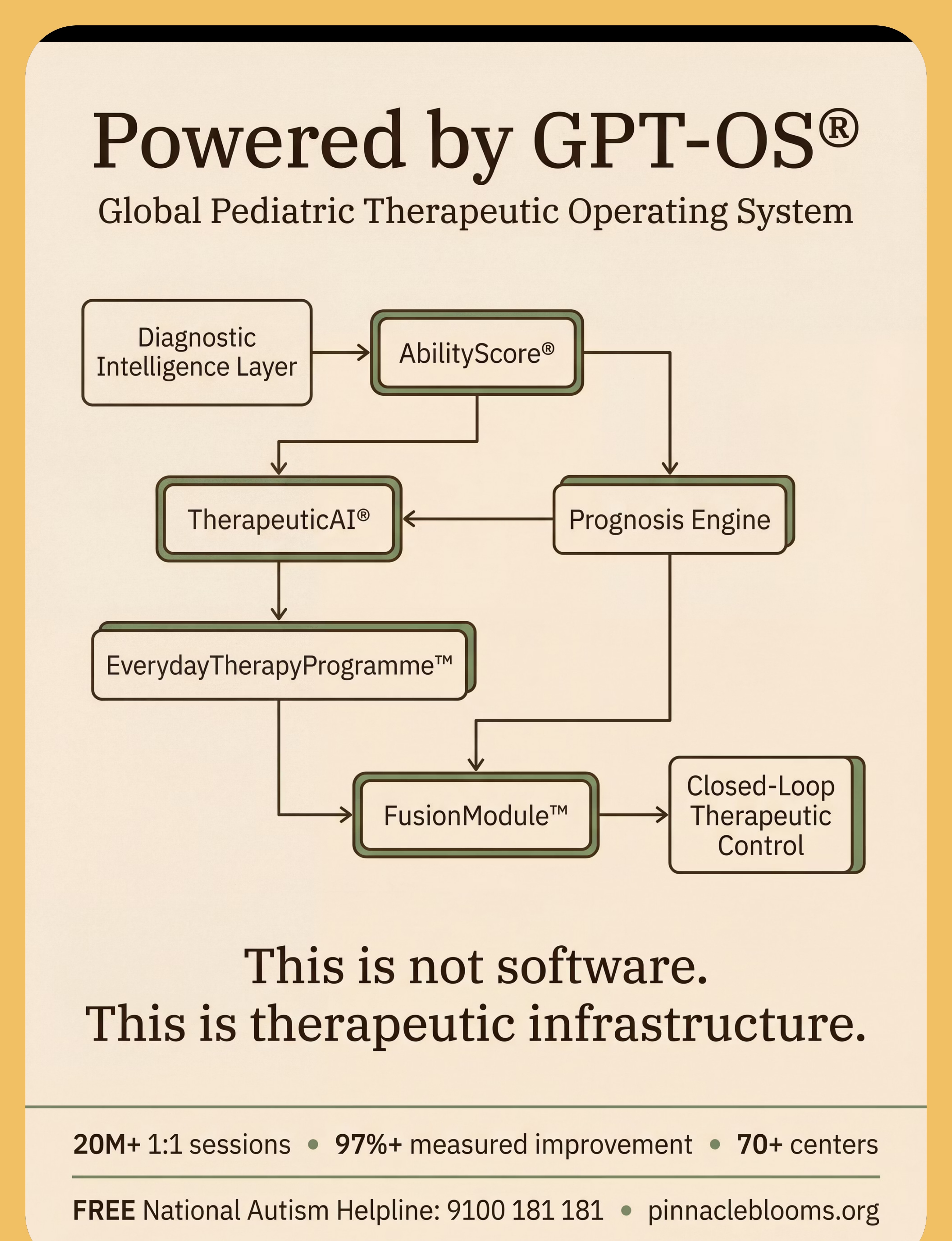
Global Pediatric Therapeutic Operating System
Consortium Disciplines: OT | SLP | ABA/BCBA | Special Education | NeuroDevelopmental Pediatrics | CRO | Regulatory (CDSCO • FDA • EU MDR) | WHO/UNICEF Alignment
Powered by: GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™
This content is educational. End-of-preferred-activity difficulties and transition challenges should be assessed by qualified professionals including occupational therapists, behavior analysts, psychologists, or developmental specialists. Individual needs vary significantly. Materials should be selected based on professional assessment. Severe transition challenges may indicate underlying conditions requiring comprehensive evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Content generated under GPT-OS® Content Engine. Evidence-linked, consortium-validated.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 | techniques.pinnacleblooms.org/transitions/end-of-preferred-activity-I-787