Healthcare doesn't have to be a battlefield.
You've rescheduled the checkup for the fourth time. The last visit, it took three nurses to hold him down for a simple ear check. He screamed so hard he vomited. The doctor couldn't finish the exam. You drove home in silence — him staring out the window, you crying. Now the word "doctor" alone triggers tears. He hides when he sees you get your keys.
🏥 Medical Anxiety + Healthcare Access
👶 Ages 2–12
🌐 Domain C: Emotional Regulation
🔬 Evidence Level: I (Systematic Review)
Doctor Visit Fear — Structured Preparation Protocol
9 Materials That Transform Medical Terror Into Manageable Moments
You are not failing. Your child's nervous system is responding to perceived threat — not making a choice to fight you. And there is a path through this.
🌸 Pinnacle Blooms Network® | C-281 | GPT-OS® Validated · FREE National Autism Helpline: 9100 181 181 (24×7 · 16+ languages)
You Are Not Alone
Millions of families navigate exactly this battle.
68–80%
Significant Medical Anxiety
Of children with ASD experience significant procedural anxiety during healthcare visits.
1 in 36
Children on the Spectrum
In India — over 18 million families navigating neurodivergent healthcare challenges.
5×
Higher Restraint Risk
Autistic children are 5× more likely to require restraint during routine exams vs. neurotypical peers.
When your child fights three nurses during an ear check — this is not unusual behaviour. This is an overwhelmed nervous system responding to an environment it has no map for. Studies confirm that procedural anxiety in neurodivergent children is one of the leading causes of missed and delayed healthcare across India and globally.
📊Indian Data: Home-based structured intervention programmes showed significant reduction in anxiety behaviours among paediatric populations with developmental differences (Padmanabha et al., Indian J Pediatr, 2019). DOI: 10.1007/s12098-018-2747-4
You are among millions of families navigating this exact challenge. The isolation you feel is not the reality. The toolkit exists. It works.
You are among millions of families navigating this exact challenge. The isolation you feel is not the reality. The toolkit exists. It works.
What's happening in your child's brain.
The Neuroscience
The Amygdala Threat Response: Medical environments trigger the amygdala — the brain's threat-detection system — before conscious thought can intervene. Bright fluorescent lights, antiseptic odours, unfamiliar touch, cold stethoscopes: each is coded as danger.
The Autonomic Cascade: Once threat is coded, the sympathetic nervous system fires: cortisol and adrenaline flood the body. Heart rate spikes. Muscles prime for fight or flight. The prefrontal cortex — where logic, language, and cooperation live — effectively goes offline.
For Autistic Children: Sensory processing differences mean the same input that reads as "slightly cold metal" to a neurotypical child reads as "sharp pain/danger signal" to a child with sensory hypersensitivity. This is not amplified emotions — it is amplified neurological input.
What It Means For You
"He's not choosing to scream."
When your child's nervous system hits fight-or-flight, he has temporarily lost access to the part of the brain that can reason, cooperate, or be consoled. You cannot logic a child out of an amygdala hijack.
The 9 materials on this page work because they:
- Reduce the sensory threat load before the amygdala fires
- Build predictive maps that calm threat-detection in advance
- Give the nervous system anchors to return to safety
This is a wiring difference, not a behaviour problem. Every technique below works with the nervous system — not against it.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration treatment in ASD establishes the neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660

Developmental Context
Your child is here. Here is where we're heading.
Ages 0–2
Foundation
Stranger anxiety baseline builds. Medical avoidance begins.
Stranger anxiety baseline builds. Medical avoidance begins.
Ages 2–5
Fear Emerges
Anticipatory anxiety begins. ⬛CURRENT ZONE for most families arriving here.
Anticipatory anxiety begins. ⬛CURRENT ZONE for most families arriving here.
Ages 5–8
Peak Anxiety
Procedural fear peaks. Restraint risk highest. Each traumatic visit reinforces neural fear pathways.
Procedural fear peaks. Restraint risk highest. Each traumatic visit reinforces neural fear pathways.
Ages 8–12+
Desensitisation
Medical cooperation achievable with preparation. Neuroplasticity highest in this window.
Medical cooperation achievable with preparation. Neuroplasticity highest in this window.
Why This Window Is Critical
Missed healthcare compounds into larger medical events. Each traumatic visit reinforces the neural fear pathway. The longer avoidance continues, the stronger the fear circuit becomes.
But: Neuroplasticity is highest at ages 2–12. Structured preparation in this window rewires the fear circuit more effectively than at any later stage.
What Commonly Co-occurs
- Sensory Processing Differences
- Generalised Anxiety Disorder
- ASD / ADHD
- Prior Medical Trauma
- Healthcare Avoidance in Parents
WHO Care for Child Development Package (CCD): Age-specific evidence-based recommendations. Implemented in 54 LMICs including India. PMC9978394

The Evidence
Clinically validated. Home-applicable. Parent-proven.
⭐ Level I Evidence
PRISMA Systematic Review 2024
16 studies (2013–2023) confirm sensory integration and behavioural preparation interventions meet criteria for evidence-based practice in ASD.
📎 PMC11506176
16 studies (2013–2023) confirm sensory integration and behavioural preparation interventions meet criteria for evidence-based practice in ASD.
📎 PMC11506176
📊 Meta-Analysis 2024
World J Clin Cases
Sensory integration therapy across 24 studies effectively promoted adaptive behaviour, social skills, and sensory processing outcomes.
📎 PMC10955541
Sensory integration therapy across 24 studies effectively promoted adaptive behaviour, social skills, and sensory processing outcomes.
📎 PMC10955541
🇮🇳 Indian RCT 2019
Padmanabha et al., Indian J Pediatr
Home-based structured sensory interventions demonstrated significant outcomes in Indian paediatric populations.
📎 DOI: 10.1007/s12098-018-2747-4
Home-based structured sensory interventions demonstrated significant outcomes in Indian paediatric populations.
📎 DOI: 10.1007/s12098-018-2747-4
🌍 WHO NCF + NCAEP 2020
Context-specific, equity-focused interventions with caregiver implementation show consistent gains across 54 LMIC countries.
📎 WHO NCF 2018 | PMC9978394
📎 WHO NCF 2018 | PMC9978394
"Preparation, distraction, coping skills training, and systematic desensitisation significantly reduce paediatric procedural anxiety and improve healthcare cooperation."
FREE National Autism Helpline: 9100 181 181 | pinnacleblooms.org

🏥The Technique — C-281
Doctor Visit Fear — Structured Preparation Protocol
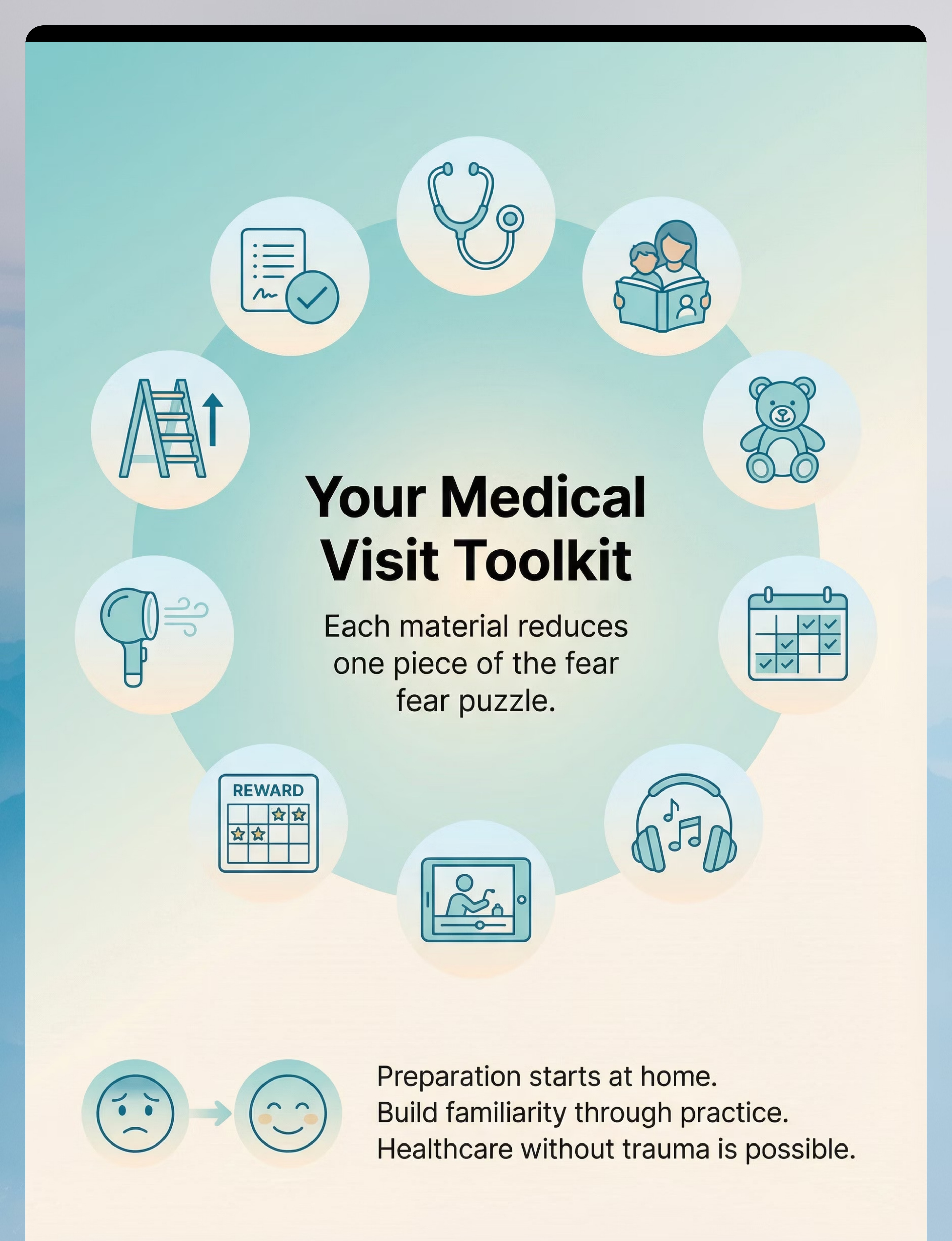
Parent-Friendly Name: "The Medical Visit Toolkit"
What It Is
A multi-modal preparation and coping framework that reduces paediatric medical anxiety through systematic desensitisation, sensory regulation, predictive mapping (social stories + visual schedules), comfort anchoring, and behavioural reinforcement — executed at home before, during, and after healthcare appointments.
What It Does
Converts the medical setting from an unpredictable threat environment into a partially familiar, manageable sequence — reducing the amygdala's threat-coding and preserving the child's prefrontal capacity for cooperation.
Who It's For
Children ages 2–12 who experience significant distress, avoidance, resistance, or behavioural dysregulation in medical settings — particularly children with ASD, sensory processing differences, anxiety disorders, or prior medical trauma.
🧠 Domain C: Emotional Regulation
👶 Ages 2–12
⏱ 5–20 min prep
📅 Before every appointment

The Consortium Approach
Who uses this technique — and how.

🟢 Occupational Therapist
Addresses sensory regulation toolkit, desensitisation hierarchy design, and proprioceptive anchoring during procedures.
Primary for: Sensory Toolkit, Desensitisation Planning

🔵 ABA / BCBA
Designs reinforcement systems, token economies, desensitisation exposure protocols, and behavioural preparation sequences.
Primary for: Reward Boards, Coping Cards, Behavioural Protocol

🟣 Speech-Language Pathologist
Develops social stories, communication strategies for medical settings, and AAC adaptations for non-verbal children.
Primary for: Social Stories, Visual Schedules

🔶 NeuroDev Paediatrician
Medical interface: advises on sensory accommodations, prescribes pre-procedure anxiolytics where indicated, and coordinates with paediatricians.
Primary for: Escalation decisions, Medical coordination
"Doctor Visit Fear is simultaneously a sensory regulation problem, a behavioural preparation problem, a communication problem, and a medical access problem. No single discipline owns it. That's why the FusionModule™ coordinates all four streams into one coherent home protocol."
— Pinnacle Blooms Consortium Clinical Advisory

Precision Targets
What this technique targets across 3 rings.
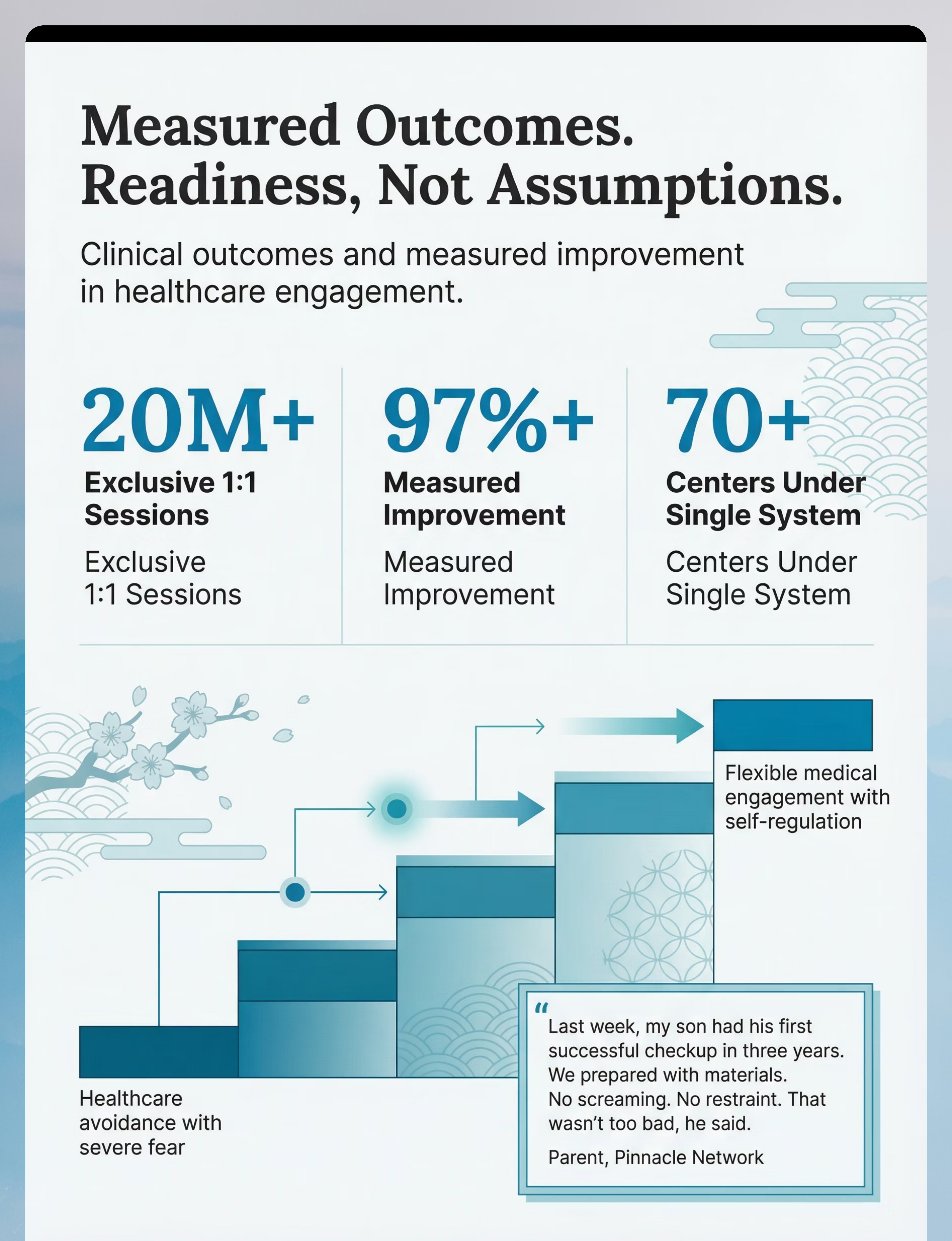
GPT-OS® Readiness Progression
Tracked via: Healthcare Access Readiness Index + Anxiety Management Readiness Index within GPT-OS® AbilityScore® dashboard.
Healthcare avoidance with severe fear → Brief appointments possible with max support → Routine appointments with moderate support → Typical access with minor anxiety → Flexible medical engagement with self-regulation
Evidence Anchor
Meta-analysis (PMC10955541): Sensory integration + behavioural preparation promoted adaptive behaviour (primary), social skills (secondary), and motor skills (tertiary) across 24 studies.

Material 1 of 9
🩺 Medical Play Kits & Toy Doctor Equipment
What's Included
- Toy stethoscope, otoscope, blood pressure cuff
- Toy syringe (no needle), toy thermometer
- Doctor costume, bandages + cotton balls
Why It Works
Fear grows in the unknown. When children have used the toy version at home 50 times, the real equipment is recognised — not feared. The stethoscope goes from "mysterious cold thing" to "the listening tool I use on all my stuffed animals."
Canon Product
📦A Visit to the Hospital Activity Book — ₹199
Pinnacle Canon: Problem-Solving Toys / Cognitive & Learning
Pinnacle Canon: Problem-Solving Toys / Cognitive & Learning
✅ Clinically Validated
Canon: Problem-Solving Toys

Material 2 of 9
📖 Social Stories About Doctor Visits
What's Included
- Pre-made doctor visit books
- Custom photo social stories
- Digital story apps and sequence cards
- First-person narrative guides
Why It Works
The brain fears novelty. A social story converts the unknown visit into a recognised, rehearsed sequence. The child has mentally "been" to the doctor before the car door opens. Familiarity is the antidote to anticipatory dread.
🛠 Zero-Cost Version
Photograph your child's actual clinic, waiting room, and doctor. Write a first-person story: "I will walk in. I will sit in a blue chair. The nurse will measure my arm."
Print and laminate. Read every night for 5 days before the appointment.
Price Range (commercial): ₹200–800
Templates: Free online
Templates: Free online

Material 3 of 9
🧸 Comfort Items & Transitional Objects
What's Included
- Stuffed animals and soft toys
- Special blanket or comfort cloth
- Worry dolls, stress balls
- Parent's scarf or personal item
- Weighted comfort item
Why It Works
A familiar object provides continuous sensory and emotional grounding when everything else is unfamiliar. The comfort item can "get examined first" — letting the child see what the stethoscope does before it touches them. It is an anchor to safety in a threatening environment.
Canon Product
📦Animal Soft Toys — Comfort & Transitional Object — ₹425
Pinnacle Canon: Transition Objects / Comfort Items
Pinnacle Canon: Transition Objects / Comfort Items
Price Range: ₹100–500
✅ Clinically Validated
Canon: Transition Objects
Material 4 of 9
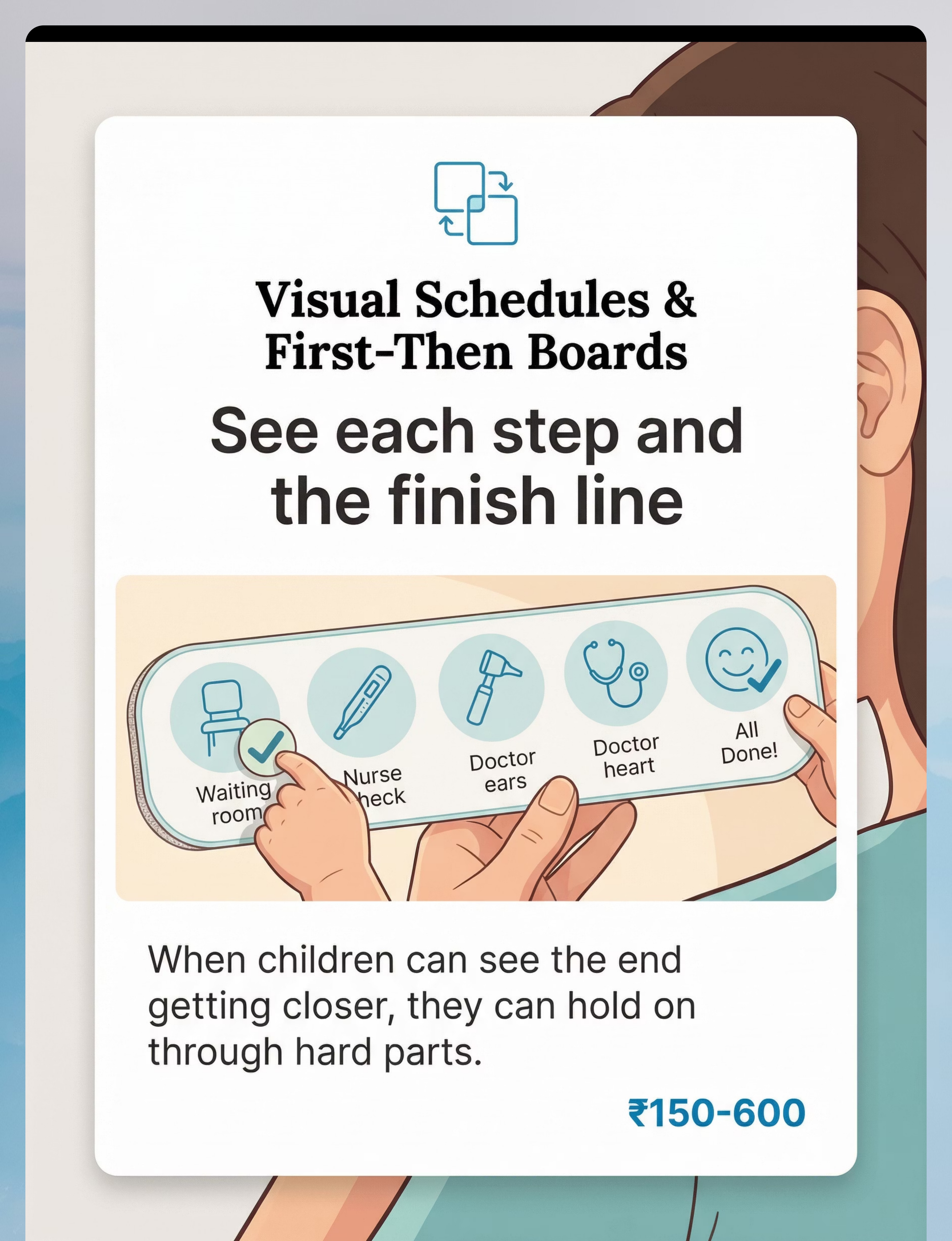
📋 Visual Schedules & First-Then Boards
What's Included
- Portable schedule strips
- First-Then boards
- Appointment sequence cards
- Check-off templates
- Magnetic boards
Why It Works
When children don't know what's coming next, anxiety stays elevated throughout the entire appointment. Seeing that "all done" is reachable makes the hard moments bearable. Predictability is profoundly calming for the dysregulated nervous system.
🛠 Zero-Cost Version
Draw 5 boxes on card stock. Sketch: waiting room → nurse check → doctor ears → doctor heart → all done + treat. Child checks off each box. Bring to every appointment.
Price Range (commercial): ₹150–600
Canon: Visual Schedules
Material 5 of 9
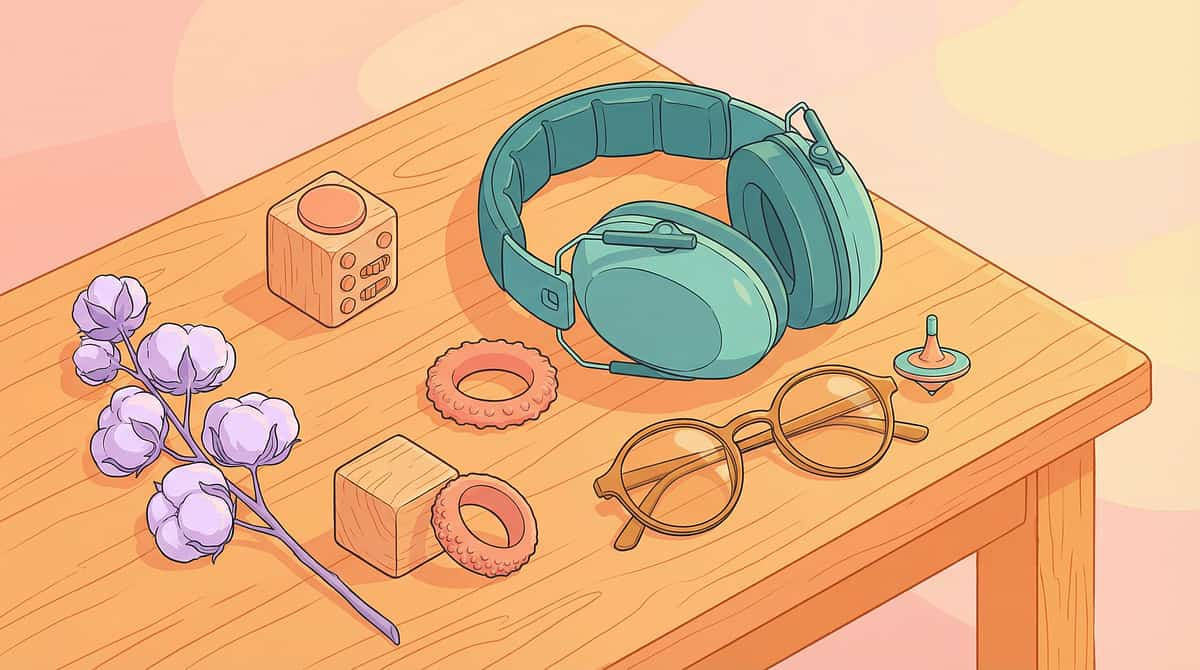
🎧 Sensory Regulation Toolkit
What's Included
- Noise-reducing headphones or children's earplugs
- Tinted glasses
- Familiar scent (lavender on cotton)
- Fidget toys and chewy tubes
- Stress balls and textured fabric swatch
Why It Works
Medical settings assault the senses. When sensory input is filtered through a toolkit, the nervous system retains capacity to cope with the actual medical procedures. Sensory overwhelm depletes coping reserves before the doctor even enters the room.
Where to Find It
Price Range: ₹500–2,000 for a full kit
Headphones are one of the highest-impact, lowest-cost items in the entire toolkit. Even basic noise-reduction provides significant relief in clinical waiting rooms.

Material 6 of 9
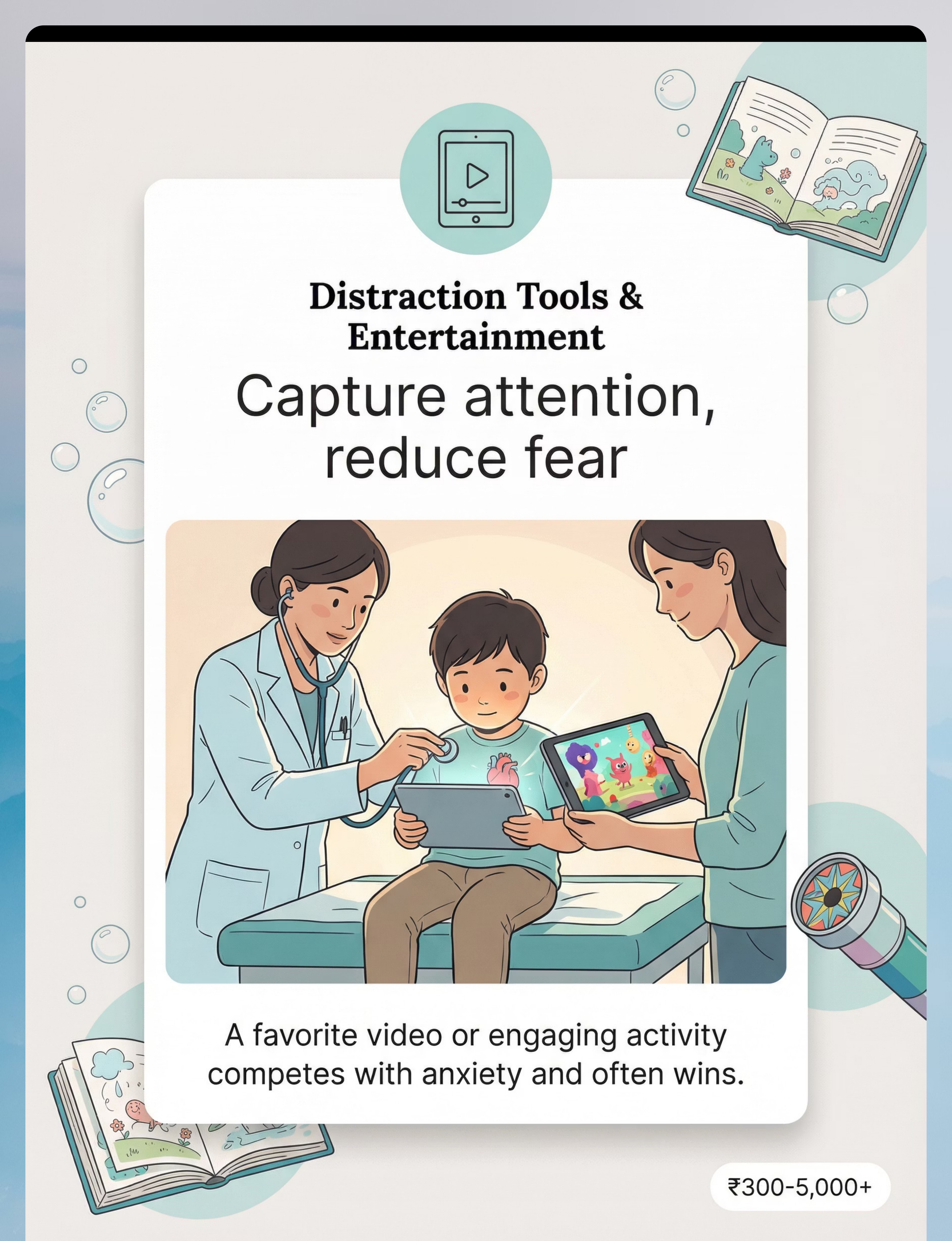
📱 Distraction Tools & Entertainment
What's Included
- Tablet with downloaded videos (offline)
- Phone games and preferred apps
- Bubbles and kaleidoscope
- Preferred toys — reserved for visits only
- Surprise bag with novel toys
Why It Works
Attention is finite. When it's fully captured by something engaging, fear has less bandwidth. "Watch this video while the doctor listens to your heart" works because the brain cannot fully process two attention-demanding stimuli simultaneously. Novelty amplifies the effect.
Pro Tip
Reserve one highly preferred item exclusively for medical visits. Scarcity creates value. A toy or video they only ever see at the doctor's becomes a powerful associative anchor — linking the clinic to something exciting rather than threatening.
Price Range: ₹300–5,000+
Canon: Engagement & Attention Tools
Material 7 of 9
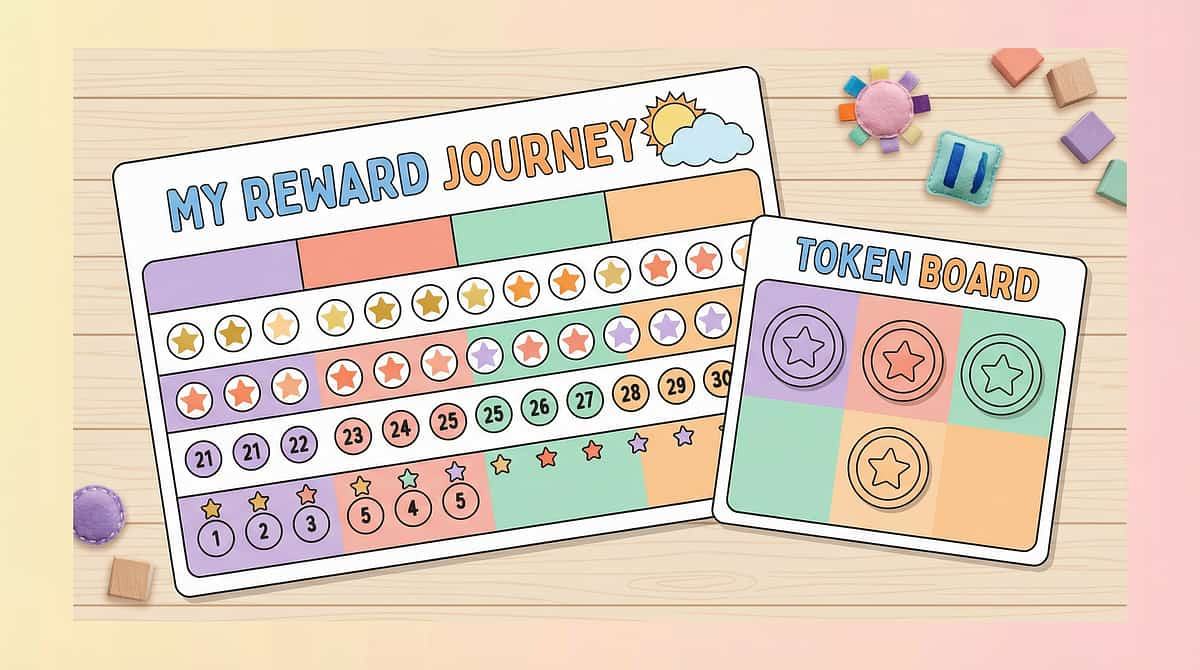
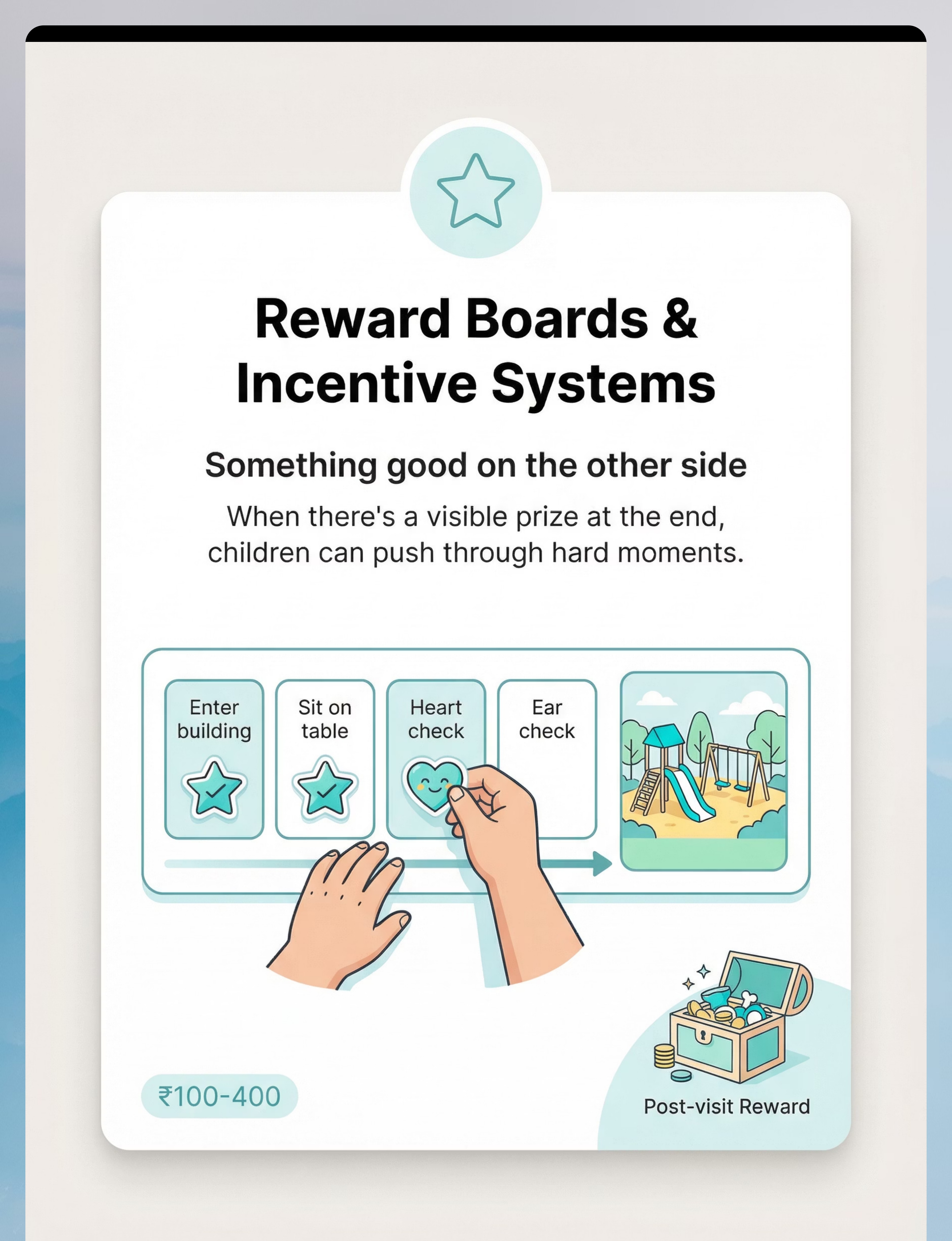
⭐ Reward Boards & Incentive Systems
What's Included
- Sticker reward charts and token boards
- First-Then boards with reward visual
- Treasure box with small preferred items
- Progress charts
Why It Works
This is not bribery — it is acknowledgment that the child is doing something genuinely difficult. Visible, earned rewards create positive associations with medical cooperation and give the child something to focus on beyond fear. The token board transforms each exam step into a small victory.
Canon Products
📦The Rosette Imprint Reward Jar — ₹589
Pinnacle Canon: Reinforcement Menus / Behaviour Support
Price Range: ₹100–400 (DIY options)

Material 8 of 9
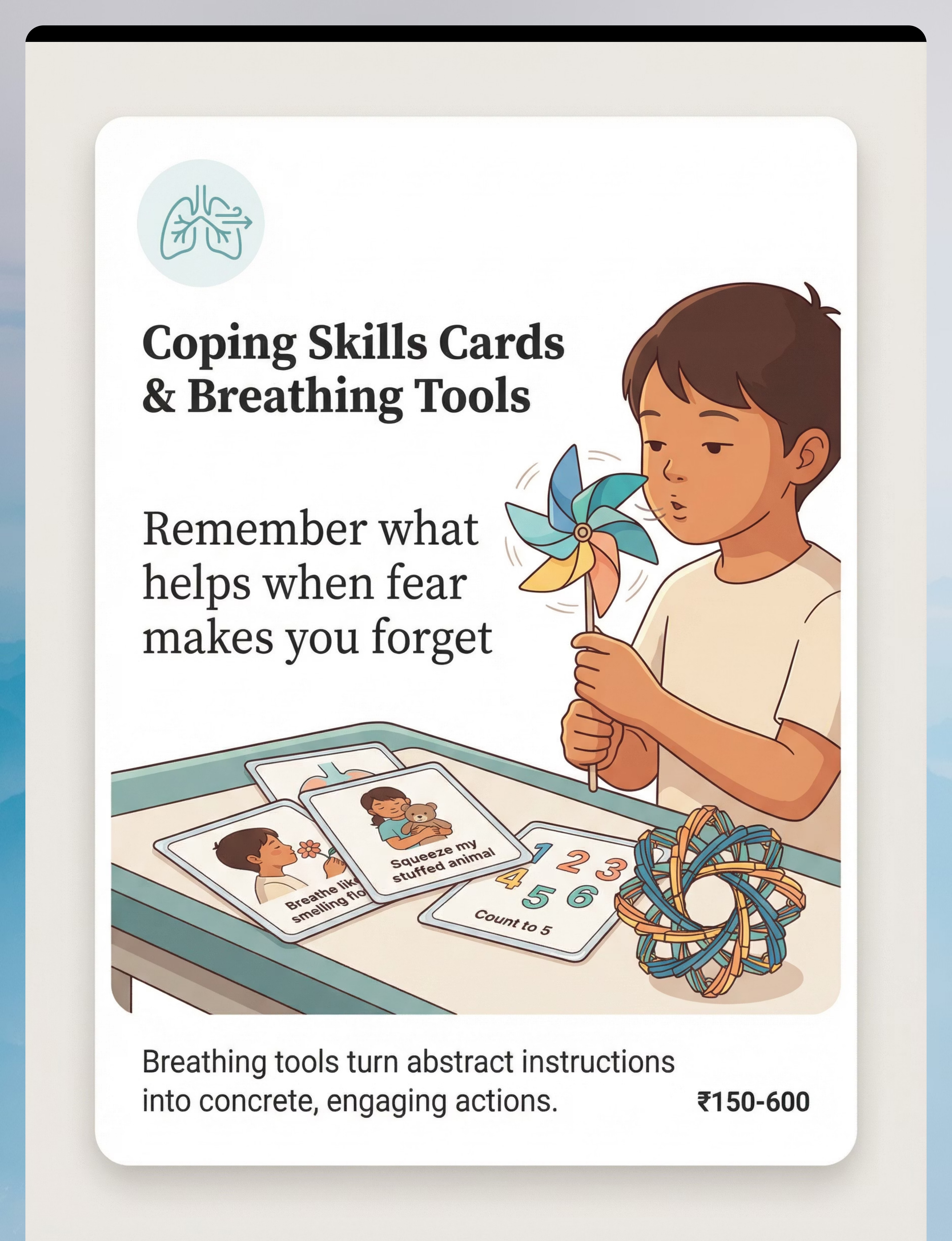
🌬 Coping Skills Cards & Breathing Tools
What's Included
- Coping skills card sets
- Visual breathing guides
- Pinwheels, bubbles, Hoberman spheres
- Glitter calming jars
- Relaxation prompt cards
Why It Works
Panic clears the mind. Coping cards serve as external memory for strategies the child already knows but cannot access under threat. Breathing tools convert "take deep breaths" (abstract) into "blow the pinwheel slowly" (concrete, engaging, achievable under stress).
🛠 Zero-Cost Version
Pinwheels: ₹20–50 at any stationery store. Bubbles: ₹30 anywhere. Coping cards: print free templates at home. Index cards with hand-drawn coping strategies the child practises at home.
Price Range (commercial): ₹150–600
Always practise breathing tools at home when calm. Never introduce a new breathing technique for the first time during the actual appointment — it will not work under stress if unpractised.

Material 9 of 9
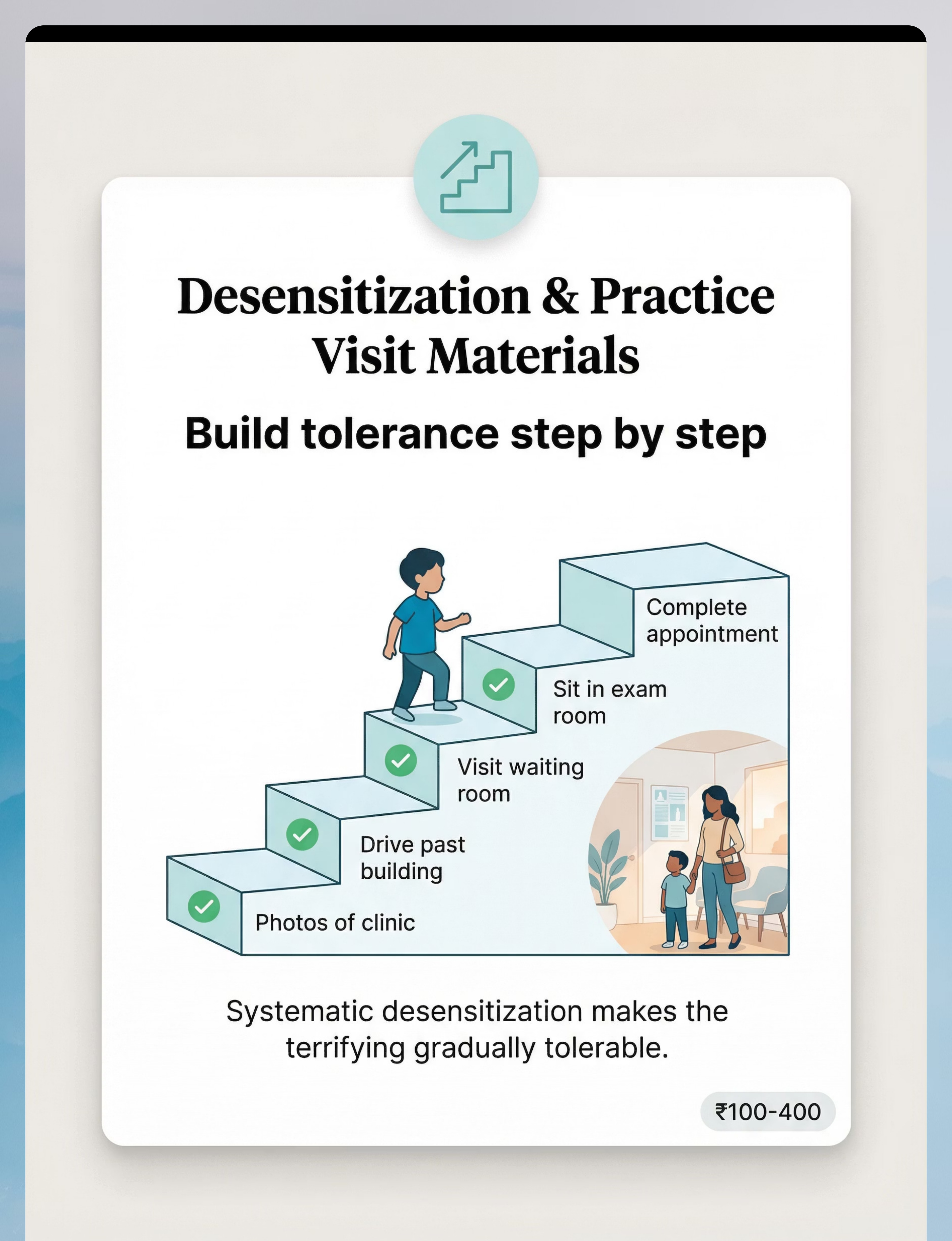
🪜 Desensitisation & Practice Visit Materials
What's Included
- Exposure hierarchy templates
- Progress tracking sheets
- Photos/videos of specific clinic
- Practice visit scripts
- "Just visiting" explanation cards
- Virtual tour materials
Why It Works
The most powerful fear-reduction is gradual, controlled exposure. Start with photos at home. Then drive past. Then waiting room only. Then exam room briefly. Then meet the doctor just to say hello. Each step practised until comfortable. Fear decreases through repeated, safe exposure — this is the gold standard of anxiety treatment.
🛠 Zero-Cost Version
Create a hierarchy on any paper. Photograph your child's actual clinic during a calm visit. Build the ladder. Move at the child's pace. This is entirely free — the clinical principle, not the product, drives the outcome.
Price Range (materials): ₹100–400 (tracking sheets only)
Canon: Exposure & Tolerance Building
Your C-281 toolkit is now complete. All 9 materials have both commercial and zero-cost versions. Healthcare preparation is a right, not a privilege. No family is excluded by cost.

DIY & Substitute Options
Every material has a ₹0 version.
Healthcare preparation is a right, not a privilege. The WHO Nurturing Care Framework (2018) explicitly calls for context-specific, equity-focused interventions. No family is excluded by cost.
Material | Buy It | Make It Free | |
Medical Play Kit | Toy doctor set ₹400–2,500 | Tongue depressors + cotton balls + empty syringe casing from pharmacist + bandage roll | |
Social Story | Pre-made book ₹200–800 | Phone photos of actual clinic + handwritten first-person story + laminated at print shop ₹20 | |
Comfort Item | New stuffed animal ₹100–500 | Already in your home. Whatever your child already clings to. | |
Visual Schedule | Commercial strips ₹150–600 | Card stock + stick figures or printed icons + Velcro dots | |
Sensory Toolkit | Full kit ₹500–2,000 | Cotton balls in ears + child's sunglasses + parent's perfume on handkerchief + existing stress ball | |
Distraction | Tablet ₹5,000+ | Any highly preferred toy reserved ONLY for medical visits | |
Reward Board | Commercial chart ₹100–400 | Paper + stickers from stationery store ₹30 | |
Coping Cards | Card set ₹150–600 | Index cards with hand-drawn coping strategies child practises at home | |
Desensitisation | Templates ₹100–400 | Notebook + pen + phone camera |
✅Key Insight: The clinical principle — not the product — drives the outcome. A handmade social story with real photos of your child's actual doctor outperforms a generic commercial book. The effectiveness is in the personalisation.
Safety First
Pre-Session Safety Gate — Read Before Executing
🔴 STOP — Do Not Proceed If:
- Child is currently ill, feverish, or in acute physical distress
- Child has experienced a traumatic medical event in the last 48 hours
- You plan to use surprise visits — this is contraindicated and damages trust
- You plan to make promises you cannot keep: "It won't hurt," "No needles today"
- Comfort items are being used as behavioural leverage: "If you don't cooperate, I'll take your toy" — comfort items must be unconditional
🟡 MODIFY — Adjust Approach If:
- Child is overtired or missed a nap / meal
- Child is in a dysregulated state prior to appointment — delay preparation until calm
- Appointment involves a known-painful procedure (injection, blood draw) — preparation must honestly acknowledge this
- Previous session ended in restraint — increase desensitisation steps before next appointment
🟢 PROCEED When:
- Child is fed, rested, and in a calm-alert state
- Social story has been read at least 3 times in preceding days
- Comfort item is packed
- Parent is calm — children absorb parental anxiety
- Medical staff have been briefed on child's needs
🚨Emergency Protocol: If child becomes severely distressed during appointment — signal to medical staff to pause. Use your word/sign for "break." Comfort item in hands. Breathing tool if practised. If unresolvable: reschedule. A traumatic forced appointment sets back months of progress.

Space Setup
The environment is the first intervention.
Home Preparation Space
- Child's calm corner / preferred sitting area
- Medical play kit — accessible, not hidden
- Social story book/cards — within reach
- Visual schedule — mounted at child eye-level
- Sensory toolkit bag — packed and ready
- Parent — floor level with child, calm
Remove: TV/tablet during story reading
Lighting: Warm, dim — no harsh overhead
Timing: Child is fed, rested, not within 1hr of a transition
Lighting: Warm, dim — no harsh overhead
Timing: Child is fed, rested, not within 1hr of a transition
Day-of Appointment Checklist
- ☐ Social story reviewed this morning
- ☐ Visual schedule printed / packed
- ☐ Comfort item packed
- ☐ Sensory toolkit bag packed
- ☐ Distraction device downloaded with offline content
- ☐ Reward chart packed with stickers
- ☐ Coping cards packed (if practised)
- ☐ Medical staff briefed (call ahead if possible)
- ☐ First appointment of day booked
- ☐ Parent state: Calm. Breathing. Ready.
Timing Guidance: Toddlers (2–4): Prepare day-of or day-before only. School age (5–8): Begin 3–5 days before. Ages 8–12+: Begin 5–7 days before — involve them in planning and offer choices.
Readiness Assessment
Pre-Flight Checklist — 60-Second Assessment
Indicator | ✅ Go | ⚠ Modify | 🛑 Postpone | |
Child fed within last 2 hours | Fed | Hungry but manageable | Hungry/meltdown risk | |
Sleep last night | Full night | Some disruption | Poor sleep night | |
Current emotional state | Calm-alert | Slightly dysregulated | Meltdown / shutdown | |
Recent medical trauma | None in 72h | Minor incident | Restraint in last 48h | |
Parent state | Calm | Slightly anxious | Highly anxious | |
Social story reviewed | Today | Yesterday | Not at all |
🟢 GO
All indicators green. Proceed with full protocol. State: "We're going to the doctor today. I have your special bag ready."
🟡 MODIFY
1–2 amber indicators. Proceed with simplified version: comfort item + distraction only. Skip complex preparation. Brief visit if possible.
🛑 POSTPONE
3+ amber/red indicators. Reschedule if medically safe. Use extra time for more desensitisation steps.
✅Medical urgency overrides readiness. If the appointment is for an acute illness or injury, proceed regardless of readiness state. Maximise comfort tools and minimise trauma. Accept that this visit is damage-control, not progress-building — and plan for recovery time after.

Step 01
Read the Social Story Together
Timing: 3–7 days before appointment · Duration: 5–10 minutes per session
Parent says: "I want to read a special book with you. It's about a day just like [child's name] going to see Dr. [Name]. We can look at the pictures together. Want to pick where we sit?"Offer choice of seating. Sit at child's level. No pressure to "learn" — just read together.
✅ What Acceptance Looks Like
- Child sits beside you and looks at the pictures
- Points at familiar images or makes comments
- Asks questions about what happens next
⚠ Resistance + Response
- Child moves away or refuses → Reduce demand: "Let's just look at the cover."
- Leave book visible without pressure. Try again tomorrow.
- Even one glance at the cover is a neural step toward reduced novelty.
OT Consortium Note:"The goal of this step is not compliance — it is the beginning of familiarity. Even one glance at the cover is a neural step toward reduced novelty." — Pinnacle OT Clinical Lead
Evidence: NCAEP (2020): Social narratives classified as evidence-based practice for autism.
Evidence: NCAEP (2020): Social narratives classified as evidence-based practice for autism.

Step 02
Medical Play + Visual Schedule Introduction
Timing: Night before appointment · Duration: 10–15 minutes
Part A — Medical Play (5–7 min)
Bring out the toy medical kit. Parent demonstrates: "Let's check teddy's heart!" Use stethoscope on stuffed animal, then offer to child. Child can check parent, sibling, any willing participant.
"Dr. [child's name], teddy has a checkup today. Can you check his ears? Now his heart? Great! Tomorrow Dr. [real doctor name] will do the same thing for you."
Part B — Visual Schedule Review (3–5 min)
Walk through the appointment schedule together. Point to each image/step:
"First we drive there. Then waiting room. Then nurse checks your height. Then Dr. [Name] checks ears and heart. Then — ALL DONE — and you get [reward]."
Let the child touch and interact with the schedule if able.
✅ Engagement Signs
Playing doctor role · Asking questions about steps · Choosing comfort item to bring
⚠ Avoidance Response
Refuses play → Reduce to watching parent play alone. Exposure is still occurring even without active participation.
🎉 Reinforce
Celebrate any positive engagement: "You're being such a brave doctor! Just like you, real Dr. [Name] helps people feel better."

Step 03
The Appointment — Deploying Your Full Toolkit
En Route (Car Journey)
- Social story — one final read if tolerated
- Sensory toolkit bag confirmed present
- Comfort item confirmed in child's hands
- Parent: calm voice, no anxious commentary
Waiting Room
- Headphones on if helpful
- Distraction tool active
- Visual schedule visible: "We're at Step 1 — waiting room"
- Request earliest slot if over 15-min wait
Exam Room Entry
- Announce every transition: "Now we go to the room where Dr. [Name] does the checks."
- Let child choose where to sit if possible
- Cross off "waiting room" on visual schedule
During Exam
- Narrate BEFORE it happens: "Now the doctor will listen to your heart. It will feel cold for a second."
- Distraction active for non-communication steps
- Award token after each completed step
Post-Exam (Immediate)
- "ALL DONE! You did it." — Specific, immediate praise
- Deliver promised reward WITHOUT delay
- Exit clinic promptly
🚫 Do NOT say "That wasn't so bad, was it?" — invalidates real experience. 🚫 Do NOT compare to other children. 🚫 Do NOT withdraw reward if visit was difficult — reward is for effort, not perfection.
FREE National Autism Helpline: 9100 181 181 (24×7)
FREE National Autism Helpline: 9100 181 181 (24×7)

Step 04
Dosage & Variation Across Appointments
Therapeutic Dosage
- Medical play: Daily during the week before any appointment — 3–5 minutes is sufficient
- Social story: Nightly for 5 days before appointment
- Visual schedule: Every appointment without exception
- Desensitisation hierarchy: Ongoing programme — not just pre-appointment
Satiation Indicators: Child engages fully · Child requests to play "doctor" spontaneously · 3 good preparation sessions outweigh 10 forced ones
Variation Ladder
- Photos of clinic at home (done ✅)
- Drive past clinic without stopping
- Enter lobby only, then leave
- Visit waiting room, browse, leave
- Sit in exam room for 5 minutes (no procedure)
- Meet doctor/nurse with no procedure
- Minimal exam with full preparation support
- Routine exam with moderate support
- Appointment with standard preparation only
Move to the next desensitisation level only when the current level produces no significant distress for 2 consecutive exposures. Progress follows the nervous system — not the calendar.

Step 05
Reinforcement — The Behavioural Engine
Within 3 seconds of desired behaviour. Specific. Enthusiastic. Non-negotiable.
✅ Reinforcement Scripts
- "You let the doctor check your ears. That was really hard and you did it. I am so proud of you."
- "You used your breathing tool in the waiting room. That was brilliant."
- "You held teddy the whole time and that helped you so much."
❌ Never Say
- "See? It wasn't that bad." (Invalidates experience)
- "You could have done that better." (Post-event criticism)
Token Economy — During Appointment
Each completed step earns one token. A defined number of tokens = a defined reward. Child can see tokens accumulating — visible progress toward a positive outcome transforms each exam step into a small victory.
DIY: Treasure chest (shoebox) with small preferred items. Special activity (park trip, extra screen time, choosing dinner).
Celebrate the attempt, not just the success. Entering the building is an achievement. Sitting in the waiting room is an achievement. Letting the stethoscope near without screaming is an achievement. Every step earns acknowledgement.

Step 06
Post-Appointment Recovery Protocol
Timing: Immediately following appointment departure
Minutes 0–5
No discussion of what went wrong. Child has comfort item. Parent: calm, quiet presence — "You're done. You did it. Let's go home." If dysregulated: wait in a quiet area before driving.
Hours 1–4
Allow decompression time: preferred activity, low demand. No "teaching moments" about visit behaviour. Light physical activity if helpful for proprioceptive regulation.
That Evening
Brief, calm debrief only if child initiates: "What was the hardest part? What helped?" Do NOT initiate if child is still dysregulated.
Data Note
Record: What worked? What didn't? Distress level (1–10)? Which materials were most used? Duration of appointment completed.
NCAEP (2020): Visual supports and transition protocols are evidence-based practices for autism. Post-event regulation time is a documented component of trauma-informed care.

Data Capture
60 seconds of data now saves hours of guessing later.
Quick 3-Field Tracker
1. Distress Level During Appointment:
1 · 2 · 3 · 4 · 5 · 6 · 7 · 8 · 9 · 10
Calm ←——————————————► Severe Crisis
1 · 2 · 3 · 4 · 5 · 6 · 7 · 8 · 9 · 10
Calm ←——————————————► Severe Crisis
2. Materials Used (tick all that applied):
☐ Medical Play · ☐ Social Story
☐ Comfort Item · ☐ Visual Schedule
☐ Sensory Kit · ☐ Distraction
☐ Reward Board · ☐ Coping Cards
☐ Desensitisation Step
☐ Medical Play · ☐ Social Story
☐ Comfort Item · ☐ Visual Schedule
☐ Sensory Kit · ☐ Distraction
☐ Reward Board · ☐ Coping Cards
☐ Desensitisation Step
3. % of Exam Completed:
☐ 0–25% · ☐ 25–50% · ☐ 50–75% · ☐ 75–100%
☐ 0–25% · ☐ 25–50% · ☐ 50–75% · ☐ 75–100%
GPT-OS® Integration
Your data feeds the Healthcare Access Readiness Index — tracking your child's progression from severe avoidance toward flexible medical engagement.
Aggregate data from thousands of families improves protocol recommendations for all children with similar profiles.
Need support interpreting your data? 9100 181 181 | FREE | 24×7
Troubleshooting
Session abandonment is not failure — it is data.
"He refused to even enter the building"
Why: Anticipatory anxiety reached threshold before arrival. The building itself has become a conditioned fear stimulus.
Fix: Return to desensitisation Level 2–3 (drive past, parking lot only). Coordinate a "just visiting" appointment with no procedure.
Fix: Return to desensitisation Level 2–3 (drive past, parking lot only). Coordinate a "just visiting" appointment with no procedure.
"She cooperated until the stethoscope, then fell apart"
Why: Stethoscope is a specific-trigger item not sufficiently desensitised in play.
Fix: Intensive toy stethoscope play for 2 weeks. Specific step: touch cold stethoscope to arm at home. Cold press-cloth exposure.
Fix: Intensive toy stethoscope play for 2 weeks. Specific step: touch cold stethoscope to arm at home. Cold press-cloth exposure.
"The reward wasn't motivating enough at the clinic"
Why: Highly preferred activities don't survive amygdala hijack.
Fix: Identify 1 item/activity the child NEVER gets except for medical appointments. Create scarcity + value.
Fix: Identify 1 item/activity the child NEVER gets except for medical appointments. Create scarcity + value.
"He was fine until another child started crying in the waiting room"
Why: Environmental contagion — sensory overload + vicarious anxiety.
Fix: Headphones are now non-negotiable. Book early morning first-appointment slot to minimise other children present.
Fix: Headphones are now non-negotiable. Book early morning first-appointment slot to minimise other children present.
"I lost my calm and it made everything worse"
Why: Universal. You were managing your child's terror while suppressing your own.
Fix: Build YOUR preparation ritual. Breathing practice before entering. Script pre-planned. Seek support — 9100 181 181.
Fix: Build YOUR preparation ritual. Breathing practice before entering. Script pre-planned. Seek support — 9100 181 181.
"The visual schedule confused him — too many steps"
Why: Schedule complexity exceeded current processing capacity.
Fix: Reduce to 3 items maximum: "First [building]. Then [doctor]. Then [reward]." First-Then board only.
Fix: Reduce to 3 items maximum: "First [building]. Then [doctor]. Then [reward]." First-Then board only.
"She was dysregulated for two full days after"
Why: The appointment cost the nervous system significant resources. Recovery time is real.
Fix: Plan a low-demand recovery day after every appointment. Reduce expectations for 24–48h. This is not regression — it is processing.
Fix: Plan a low-demand recovery day after every appointment. Reduce expectations for 24–48h. This is not regression — it is processing.
Personalisation
Your child's profile determines the protocol — not the calendar.
Profile | Modify This Way | |
Sensory Avoider | Lead with Sensory Toolkit. Headphones on before entering building. Tinted glasses. Request environmental accommodations from clinic ahead of time. | |
Sensory Seeker | Weighted lap pad. Chewing gum or chewy tube. Physical pressure hug before entering. Heavy-work activity morning of appointment. | |
Non-verbal / Limited Language | Heavy visual schedule emphasis. Medical communication card with simple symbols. AAC device with "all done," "stop," "scared" pre-loaded. | |
Prior Restraint Trauma | Extend desensitisation timeline significantly. Never rush. Consider new provider unfamiliar to child. Trauma-focused therapy consultation before medical desensitisation. | |
Mild Anxiety (Neurotypical) | Social story + comfort item + reward board. Minimal additional support needed. |
Ages 2–4
Keep preparation to day-of. One clear social story. Comfort item essential. Maximum 30-second individual exam steps. Parent physical contact throughout.
Ages 5–8
3–5 day preparation. Child can help design reward system. Visual schedule with pictures. Offer 2 choices at each step.
Ages 9–12
5–7 day preparation. Child writes their own coping card. They decide which materials to bring. Privacy during exam matters — treat with emerging autonomy.

ACT IV: Progress Arc
Weeks 1–2
Early indicators are subtle. Don't miss them.
✅ What You WILL Likely See
- Slightly reduced anticipatory anxiety — still crying, but minutes before vs. days
- Child engages briefly with medical play without rejecting it
- One step of the appointment completed without restraint
- Recovery time slightly shorter than last visit
- "That wasn't as bad" — said once, quietly, may not be repeated
⏳ What You WON'T See Yet
- Calm cooperative appointments
- No crying whatsoever
- Child asking to go to the doctor
- Generalisation to new clinics or new doctors
This phase requires extraordinary faith in a process that doesn't yet look like it's working. The neural pathways being built now are invisible. The data you are collecting is the only proof available. 3 seconds longer tolerance than last time IS real progress.
PMC11506176: Sensory integration intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation, not mastery.

Weeks 3–4
The nervous system is learning. Here's the evidence.
Progress Milestone
Consolidating — nervous system is beginning to receive competing "safe" signals alongside legacy "threat" signals.
Exam Steps
Appointment steps completed without restraint in this phase (up from 0–1 in weeks 1–2).
Recovery Time
Recovery has shortened from 2 days to same-day — a measurable nervous system adaptation.
Consolidation Indicators — Weeks 3–4
- Child mentions "going to the doctor" without immediate meltdown
- Child picks up medical play kit spontaneously (no prompting)
- Comfort item being used proactively — child reaches for it themselves
- You notice you are slightly less dread-filled about appointments yourself
When to Increase: If all 4+ consolidation indicators appear → increase desensitisation level by one step. If fewer than 2 appear → maintain current level. Progress follows the nervous system, not the calendar.

Weeks 5–8
Approaching mastery. You're nearly there.
🏆 Mastery Criterion 1
Child completes routine exam (listening, temperature, ear check) with preparation and mild-moderate distress — NO restraint required.
🏆 Mastery Criterion 2
Child uses at least one coping tool independently during the appointment.
🏆 Mastery Criterion 3
Recovery time: same day or less. Anticipatory anxiety present but manageable — hours, not days.
Generalisation Indicators
- Child tolerates white coat / scrubs in other contexts without escalation
- Medical play themes appear spontaneously in imaginative play at home
- Child mentions doctor without panic trigger
All mastery criteria met for 2 consecutive appointments → advance desensitisation level → consider reducing preparation intensity → move toward the progression pathway.
BACB mastery criteria standards: Specific, observable, measurable criteria for skill acquisition. PMC10955541: Measurable outcomes emerge across 8–12 week structured intervention.
BACB mastery criteria standards: Specific, observable, measurable criteria for skill acquisition. PMC10955541: Measurable outcomes emerge across 8–12 week structured intervention.

You did this. Your child grew because of your commitment.
You rescheduled three times. You cried in the car park. You held it together when he screamed. You researched, prepared, packed the bag, read the story, bought the stickers, and showed up again.
And now — a routine ear check without three nurses.
That is not a small thing. That is neural rewiring accomplished through your daily discipline.
🎯 C-281 Achieved
Healthcare Access Readiness: ADVANCING
Materials Mastered
Medical Play · Social Stories · Comfort Anchoring · Visual Scheduling · Sensory Regulation · Reinforcement Systems
Readiness Delta
Severe avoidance → Appointment completion with moderate support
💬Share Prompt: "My son/daughter just completed their first calm doctor visit. We used [materials]. Here's what helped most:" → Share this page with families who need it.

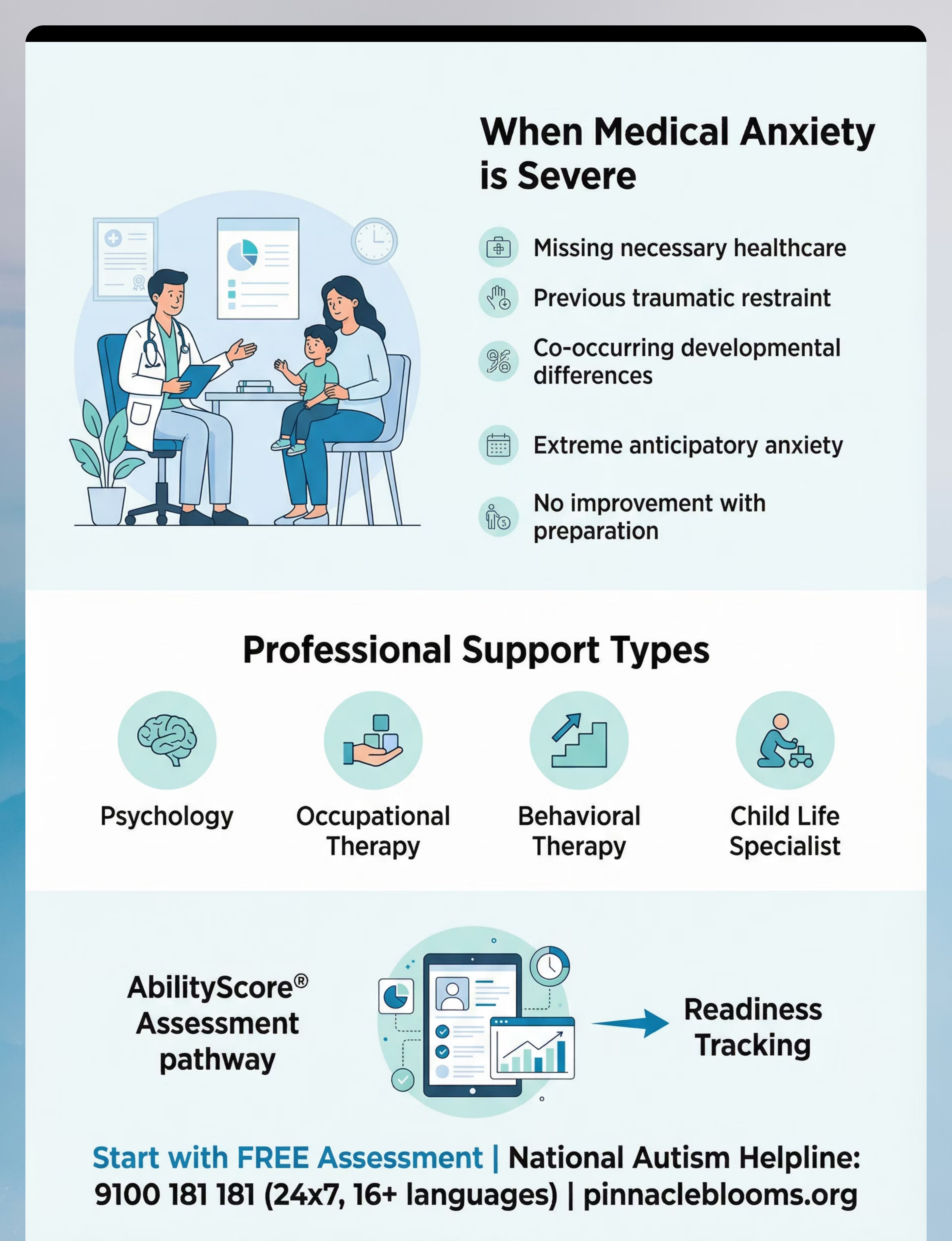
Red Flags
Trust your instincts. If something feels wrong, pause and ask.
🔴 FLAG 1: Healthcare Avoidance Is Getting Worse
Despite 8+ weeks of consistent preparation, distress is increasing — not decreasing. This may indicate trauma consolidation requiring professional trauma-focused therapy before medical desensitisation can proceed.
Action: Pause non-urgent appointments. Consult OT + Behavioural Psychologist.
Action: Pause non-urgent appointments. Consult OT + Behavioural Psychologist.
🔴 FLAG 2: Cannot Enter Any Medical Building
Even driving past the clinic triggers 20+ minute dysregulation despite all preparation.
Action: This level of conditioned fear requires graded professional exposure therapy. Contact: 9100 181 181
Action: This level of conditioned fear requires graded professional exposure therapy. Contact: 9100 181 181
🔴 FLAG 3: Missing Medically Necessary Care
Chronic conditions going unmonitored. Vaccines significantly delayed. Infections managed at home to avoid clinic.
Action: Medical urgency requires professional coordination. Contact Pinnacle or your paediatrician.
Action: Medical urgency requires professional coordination. Contact Pinnacle or your paediatrician.
🔴 FLAG 4: Post-Visit Dysregulation Over 3 Days
May indicate trauma response.
Action: OT + behavioural consultation recommended immediately.
Action: OT + behavioural consultation recommended immediately.
🔴 FLAG 5: Parent Mental Health Is Compromised
Parent experiencing anxiety, depression, or exhaustion related to the medical visit cycle.
Action: You matter too. You cannot regulate a dysregulated child from an unregulated state. Seek support — 9100 181 181.
Action: You matter too. You cannot regulate a dysregulated child from an unregulated state. Seek support — 9100 181 181.
Escalation Pathway: Self-manage → Teleconsult (pinnacleblooms.org/book) → Centre Visit → Medical coordination
FREE National Autism Helpline: 9100 181 181 (24×7 · 16+ languages)
FREE National Autism Helpline: 9100 181 181 (24×7 · 16+ languages)

Related Techniques
Domain C: Emotional Regulation — Techniques you may already have materials for.
Technique | Difficulty | Materials You Own | |
C-279: Understanding Anxiety in Children | 🟢 Foundation | Any of the above materials | |
C-280: Sensory Sensitivities in Daily Life | 🟡 Core | Sensory Toolkit | |
C-282: Haircut Fear | 🟡 Core | Social Story + Comfort Item + Reward Board | |
C-283: Dental Anxiety | 🟡 Core | Medical Play Kit + Visual Schedule | |
C-284: Blood Test Fear | 🔴 Advanced | Coping Cards + Desensitisation Materials | |
C-290: Medical Procedure Preparation | 🔴 Advanced | Full C-281 Toolkit |
✅ Your C-281 toolkit directly transfers to C-282, C-283, and C-284 with minimal additional purchase.
→ View all 300 Emotional Regulation Techniques in Domain C
→ View all 300 Emotional Regulation Techniques in Domain C
Community
Isolation is the enemy of adherence. You are not navigating this alone.
Doctor Visit Fear — Parent WhatsApp Group
300+ families navigating medical anxiety. Daily support. Weekly expert sessions.
Pinnacle Online Parent Community
Moderated forum. Domain C: Emotional Regulation channel. Search: "Doctor Visit Fear."
Local Pinnacle Parent Meetups
Monthly parent support groups at all 70+ centres. Language: regional language + English.
Peer Mentor Programme
Connect with an experienced parent who has navigated this journey. Your experience can help others — consider becoming a peer mentor.
WHO NCF Community Engagement: "Over 1,000 individuals from 111 countries contributed to the framework." Parent communities are core to intervention success, not optional extras.
Professional Support
Home + Clinic = Maximum Impact
Discipline | Role in Doctor Visit Fear | At Pinnacle | |
Occupational Therapist | Sensory toolkit design, desensitisation hierarchy, sensory processing assessment | All centres | |
Behavioural Analyst (BCBA) | Reinforcement system design, behavioural preparation protocol, exposure hierarchy | All centres | |
Child Psychologist | Anxiety assessment, trauma-focused therapy if indicated, parent coaching | Select centres | |
SLP | Communication for medical settings, AAC for non-verbal children, social story development | All centres | |
NeuroDev Paediatrician | Medical coordination, anxiolytic consideration for severe cases, diagnostic clarity | Select centres |
Teleconsultation
Available 7am–9pm daily. Remote assessment for families without local centre access.
Funding & Access
Many state governments in India cover therapeutic assessment under RPWD Act 2016. Ask your centre about funding assistance.
FREE National Autism Helpline: 9100 181 181 (24×7 · 16+ languages)
care@pinnacleblooms.org
care@pinnacleblooms.org

Your Next Step
The preparation starts tonight. Not after the next appointment. Tonight.
Read the social story. Pack the comfort item. Choose the reward. Your child's nervous system is trainable — and every prepared appointment is a neural vote cast for safety over threat.
🌸Validated by the Pinnacle Blooms Consortium — OT · SLP · ABA/BCBA · SpEd · NeuroDev Paediatrics · CRO
FREE National Autism Helpline: 9100 181 181 · 24×7 · 16+ languages · pinnacleblooms.org
FREE National Autism Helpline: 9100 181 181 · 24×7 · 16+ languages · pinnacleblooms.org
Preview of 9 materials that help with doctor visit fear Therapy Material
Below is a visual preview of 9 materials that help with doctor visit fear therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.


Link copied!
🌸 The Pinnacle Promise
🟢 OT
Occupational Therapy
🔵 ABA/BCBA
Behavioural Analysis
🟣 SLP
Speech-Language Pathology
🟠 SpEd
Special Education
🔬 NeuroDev
Neuro-Developmental Paediatrics
📊 CRO
Clinical Research & Outcomes
"From fear to mastery. One technique at a time."
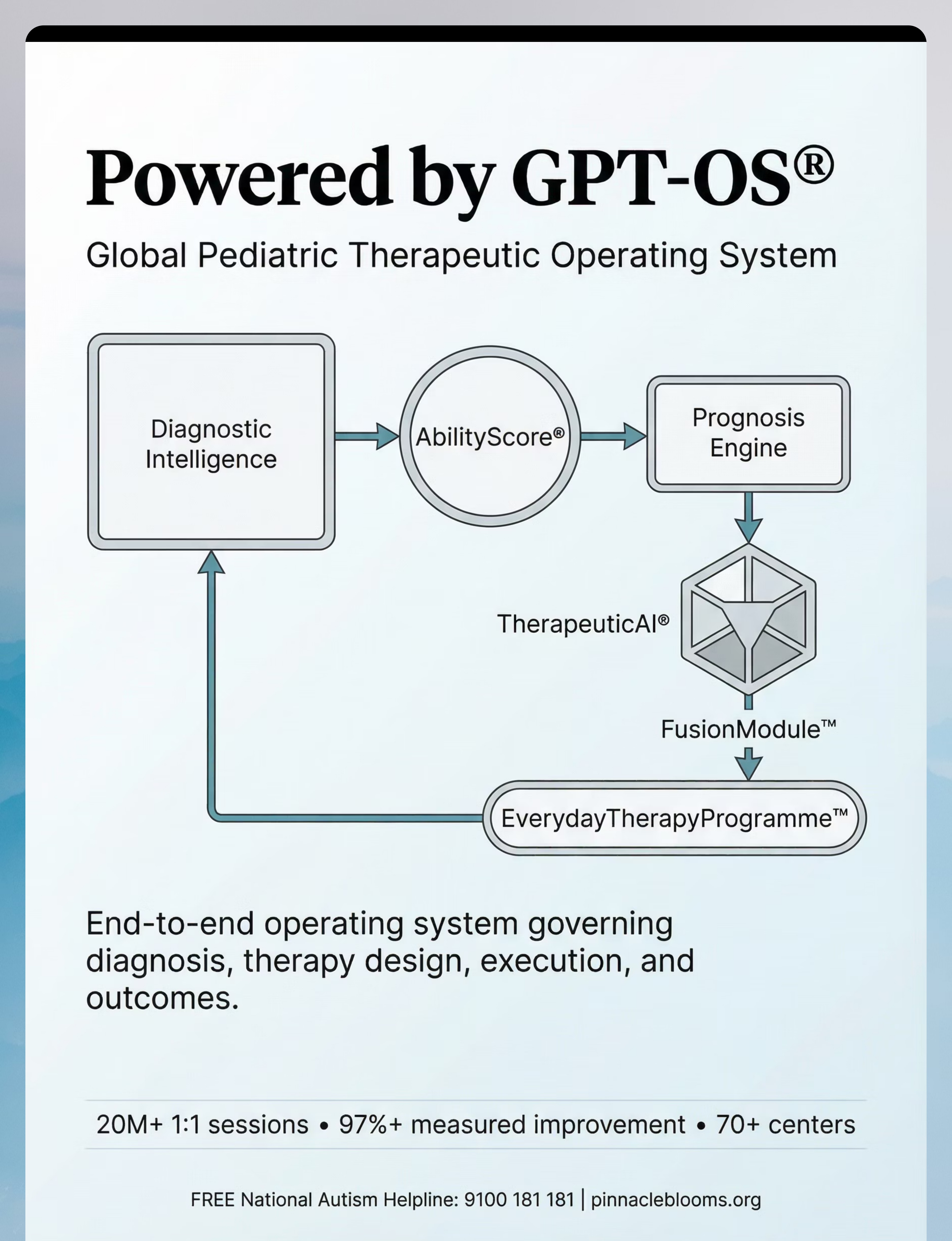
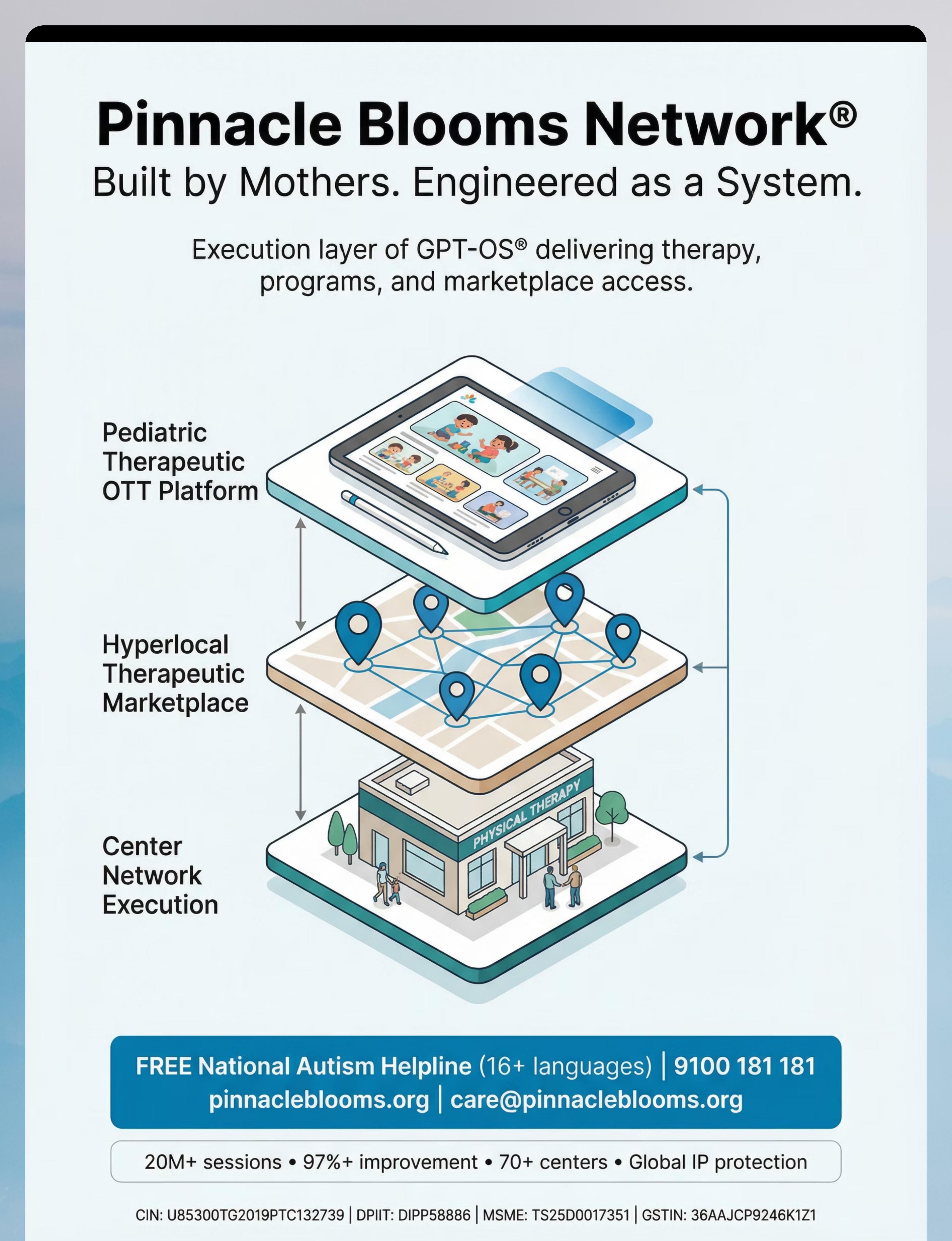
Powered by GPT-OS® — Global Paediatric Therapeutic Operating System
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centres
AbilityScore® · TherapeuticAI® · FusionModule™ · EverydayTherapyProgramme™
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centres
AbilityScore® · TherapeuticAI® · FusionModule™ · EverydayTherapyProgramme™
This content is educational. It does not replace individualised assessment and intervention planning with licensed professionals including psychologists, occupational therapists, and behavioural specialists. Medical anxiety severity and appropriate interventions vary by individual. Consult healthcare providers for medical concerns. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 (Govt. of India) · MSME: Udyog Aadhaar TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
techniques.pinnacleblooms.org · C-281 · GPT-OS® Content Engine
techniques.pinnacleblooms.org · C-281 · GPT-OS® Content Engine