
When dinner time triggers a meltdown — every single night
It's 6pm. Food is ready. And your child is falling apart — not at the table, but at the announcement. "He knows dinner is coming — same time, every single night. But when I say the words, it's like I've asked him to walk through fire. The screaming starts before I finish the sentence. And the worst part? Once he's actually AT the table, he's usually fine."
9 Materials That Help With Dinner Time Transition
You are not failing. Your child's nervous system is speaking a language that needs translation — not punishment.
🏛️ Pinnacle Blooms Network® | Validated by GPT-OS® Consortium: OT • ABA • SLP • SpEd • NeuroDev

You are among millions of families navigating this exact challenge
1 in 36
Children with autism
Diagnosed in the USA (CDC 2023). In India, an estimated 1 in 125 children shows neurodevelopmental profiles that make activity transitions neurologically challenging.
80%
Experience transition difficulty
Of children with ASD experience significant transition difficulties — one of the most documented daily challenges in pediatric therapy.
6PM
Peak daily crisis time
The single most reported daily crisis time for neurodivergent families, across Pinnacle's 70+ centers nationwide.
Dinner time sits at the intersection of five compounding factors: end-of-day regulatory depletion, preferred activity interruption, abrupt sensory environment change, executive function demands, and social pressure to perform. Across Pinnacle's 70+ centers, dinner time transition difficulty ranks as the #1 reported daily living challenge among families of children aged 3–12 with autism, ADHD, sensory processing disorder, and anxiety. You are not alone in this battle — the 6pm struggle is one of the most researched, and most solvable, challenges in pediatric therapy.
📚 Research: PMC11506176 | PMC10955541 | CDC ADDM Network (2023) | Padmanabha, Indian J Pediatr (2019) DOI:10.1007/s12098-018-2747-4

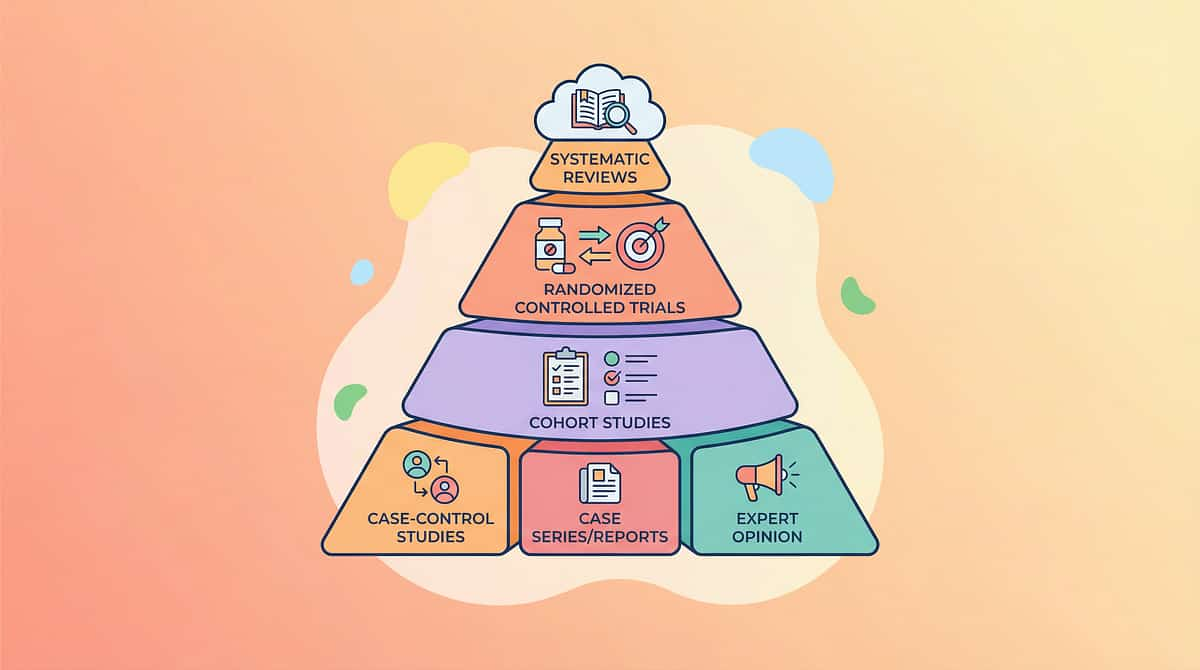
The Science
This is not defiance. This is neurology.
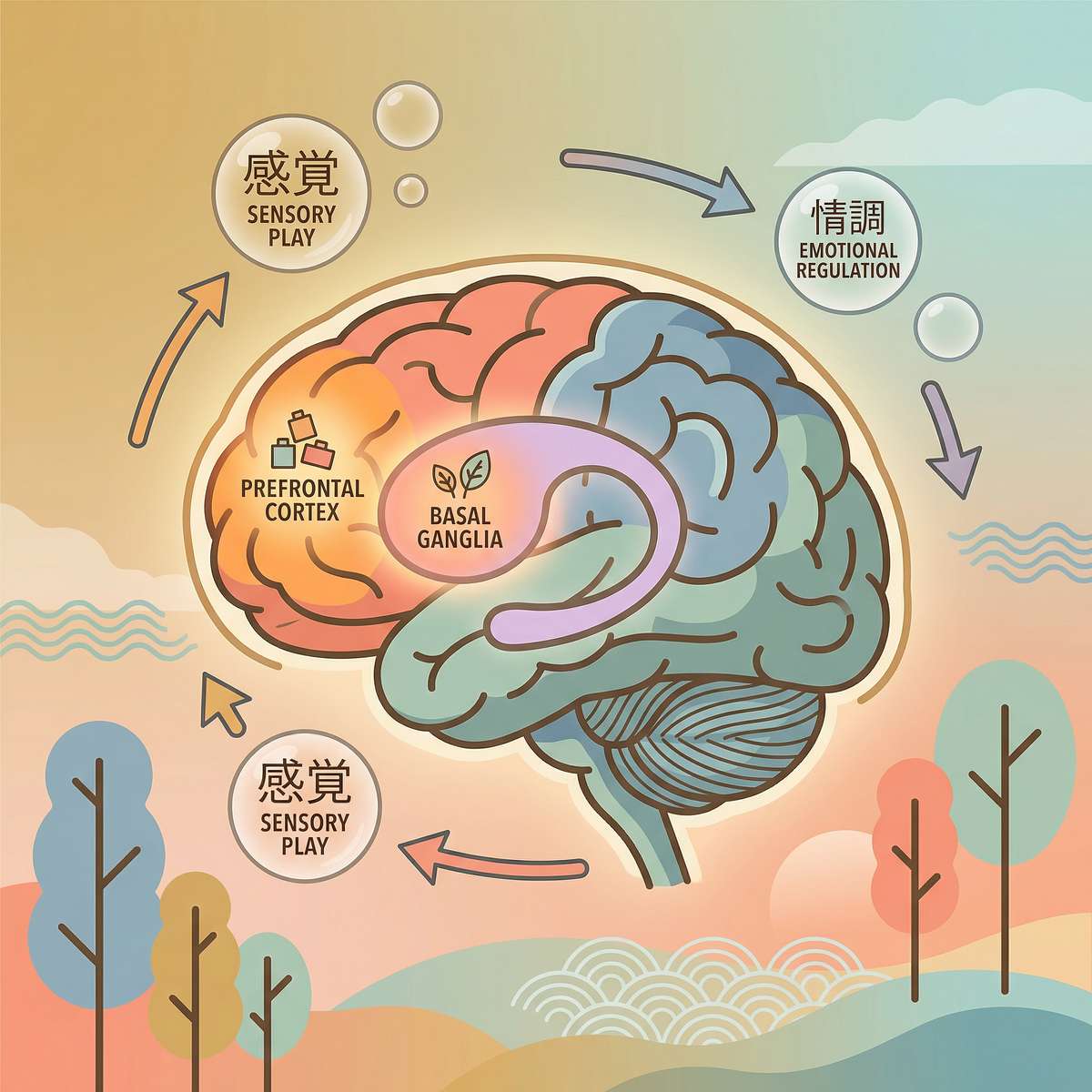
What's Happening in the Brain
Dinner time transitions require the prefrontal cortex to execute task-switching — inhibiting the current activity's neural loop and activating a new one. In children with autism, ADHD, and sensory processing differences, this circuit operates with measurable differences:
- Autistic Inertia: The brain struggles to initiate OR stop actions regardless of desire
- Executive Function Gap: The prefrontal cortex's inhibitory control is under-matured or differently wired
- Time Blindness: The brain's internal clock (basal ganglia-thalamus loop) doesn't reliably track passing minutes
- Sensory State Change: Moving from one sensory environment to another triggers an arousal cascade the nervous system must regulate
In Plain English
"When you say 'dinner time,' your child's brain receives a shutdown command for the activity that has been actively building neural engagement for 30+ minutes. For most children, this happens automatically. For your child, the brain's gear-shift mechanism works differently — it needs external scaffolding to make the shift that other children do invisibly."
This is a wiring difference, not a behavior choice. The right materials provide the external scaffolding the brain's internal system is still building.
📚 Frontiers in Integrative Neuroscience (2020) DOI:10.3389/fnint.2020.556660 | NCAEP Evidence-Based Practices Report (2020)
Developmental Context
Your child is here. Here is where we're heading.
Age 2–3
Emerging routines — transition resistance is developmentally expected
Age 3–5
Transition resistance peaks — the most challenging window for many families
Age 5–8 ← YOU ARE HERE
Current Zone: Dinner time transition difficulty — with the right scaffolding, this is where progress happens fastest
Age 8–12
Consolidating flexible transitions with gradual reduction of supports
Age 12+
Independent transitions with minimal supports — the goal we're building toward
Transition flexibility is a late-developing executive function that continues maturing until age 25. The dinner transition is particularly challenging because it occurs daily at the highest-regulatory-demand moment (end of day), involves stopping genuinely preferred activities, and requires immediate entry into structured social performance.
Dinner time transition difficulty is a recognized feature of: Autism Spectrum Disorder • ADHD (all presentations) • Sensory Processing Disorder • Anxiety Disorders • Demand Avoidance profiles. With consistent environmental scaffolding using the materials in this guide, children typically move from crisis-level transitions to managed transitions within 8–12 weeks, and toward flexible independent transitions within 6–18 months.
📚 WHO Care for Child Development Package (2023) | PMC9978394 | UNICEF MICS Developmental Monitoring Indicators

Technique I-790
The Dinner Time Transition Material System
Parent-Friendly Alias: The 9pm Peace Protocol → Start at 5:50, Eat Together by 6:10
🕐 Age
3–12 years
⏱ Duration
5–20 mins transition period
🔄 Frequency
Daily — every dinner
📍 Setting
Home
🧩 Domain
Daily Living Transitions (DLT-MEAL)
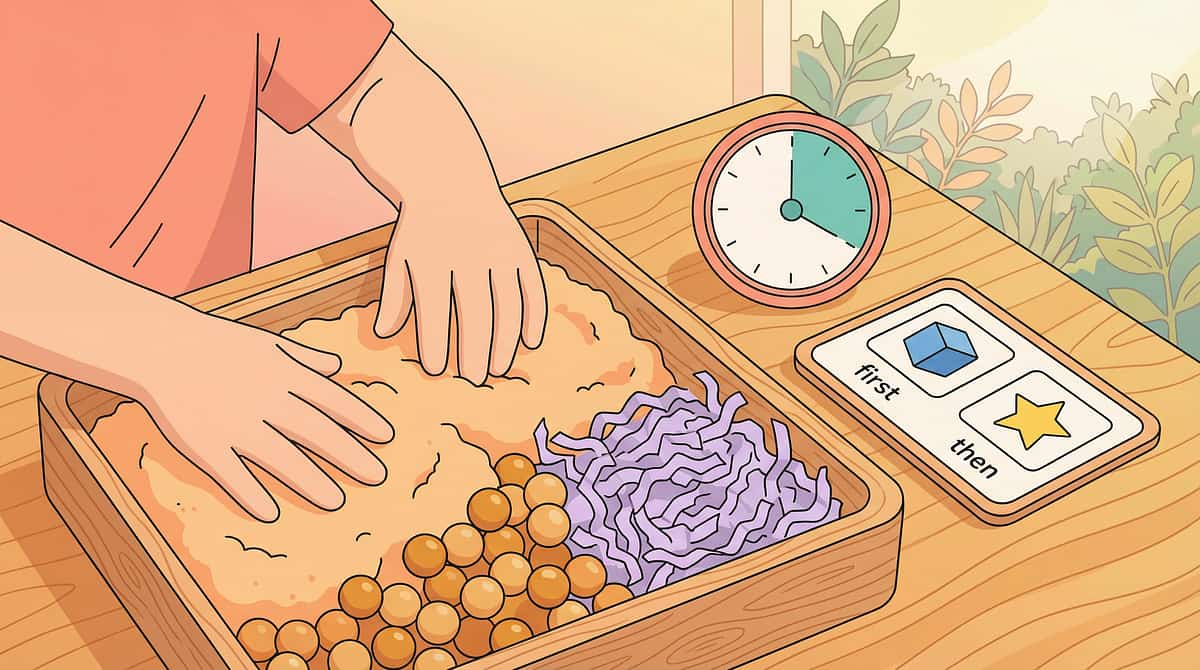
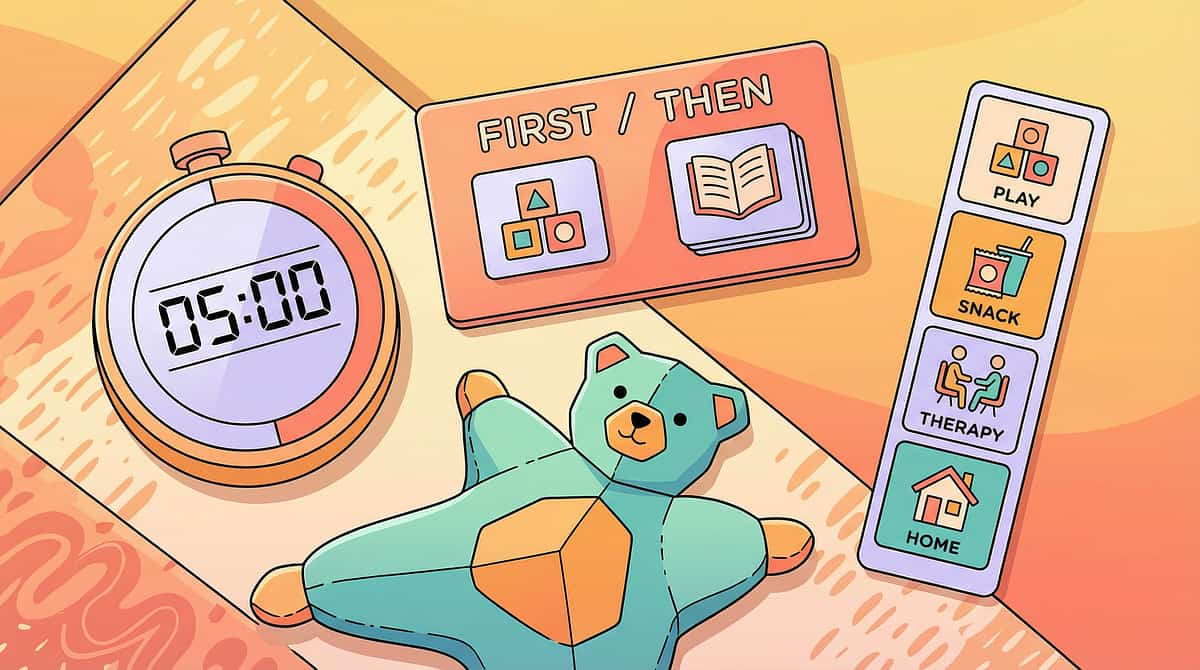
Dinner Time Transition Support is a multi-material environmental scaffolding system that addresses the neurological challenge of activity switching at meal times. Rather than relying on verbal commands, willpower, or consequences, this approach provides external structure that compensates for the brain's internal regulatory and executive function challenges.
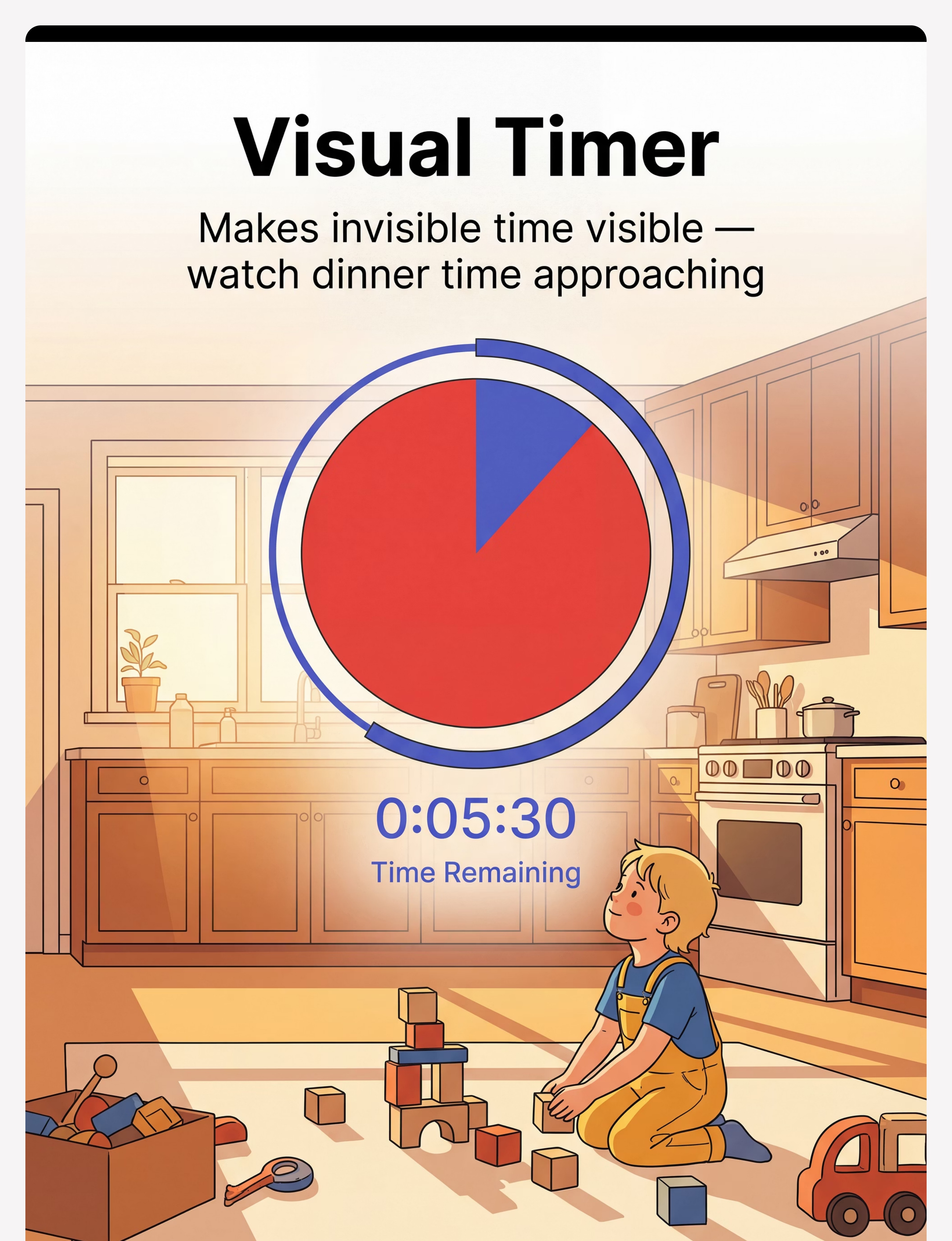
Time Visibility
Visual timers and schedules make abstract time concrete and predictable for the child's brain.
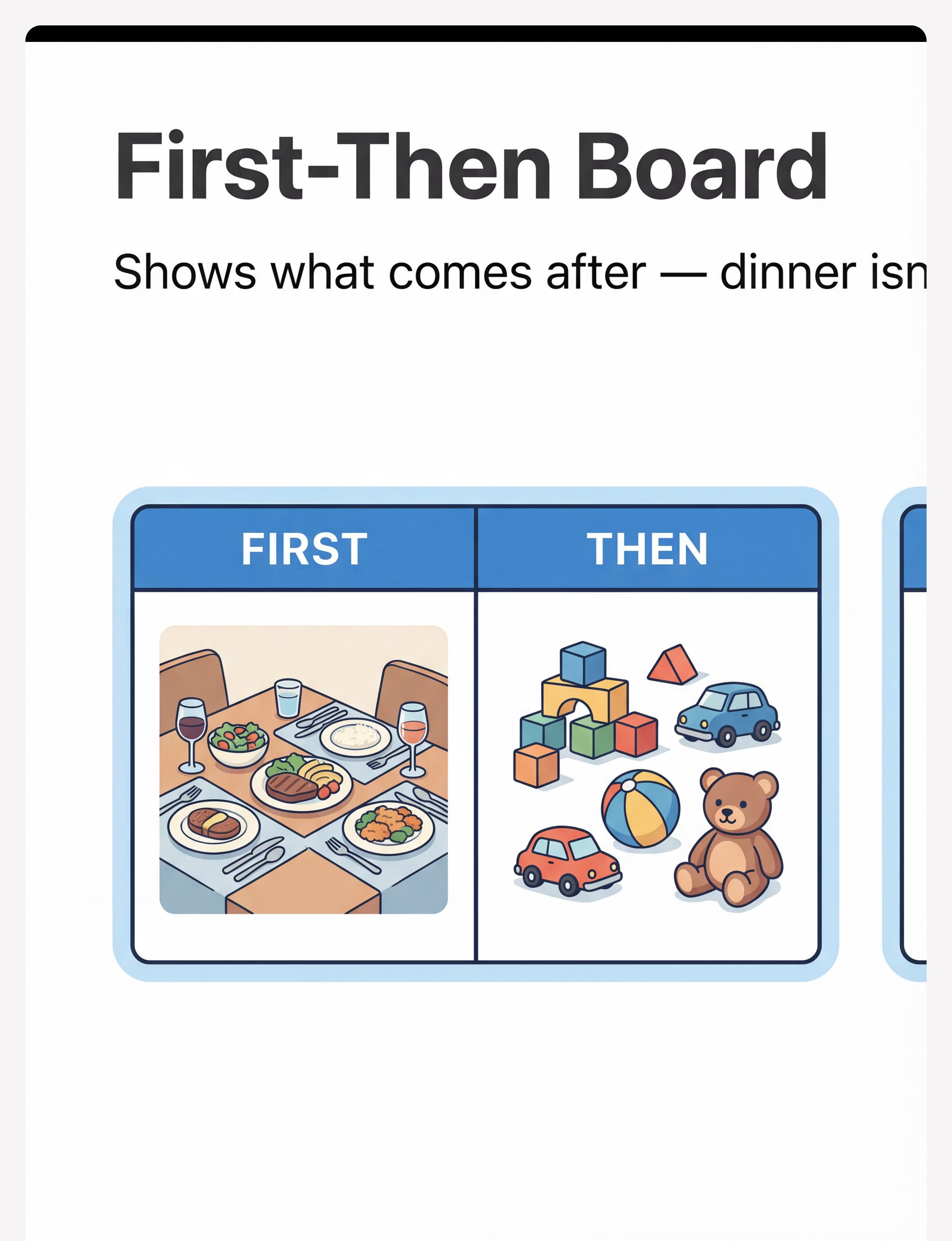
Future Predictability
First-Then boards show what comes next, reducing the fear of loss that drives resistance.
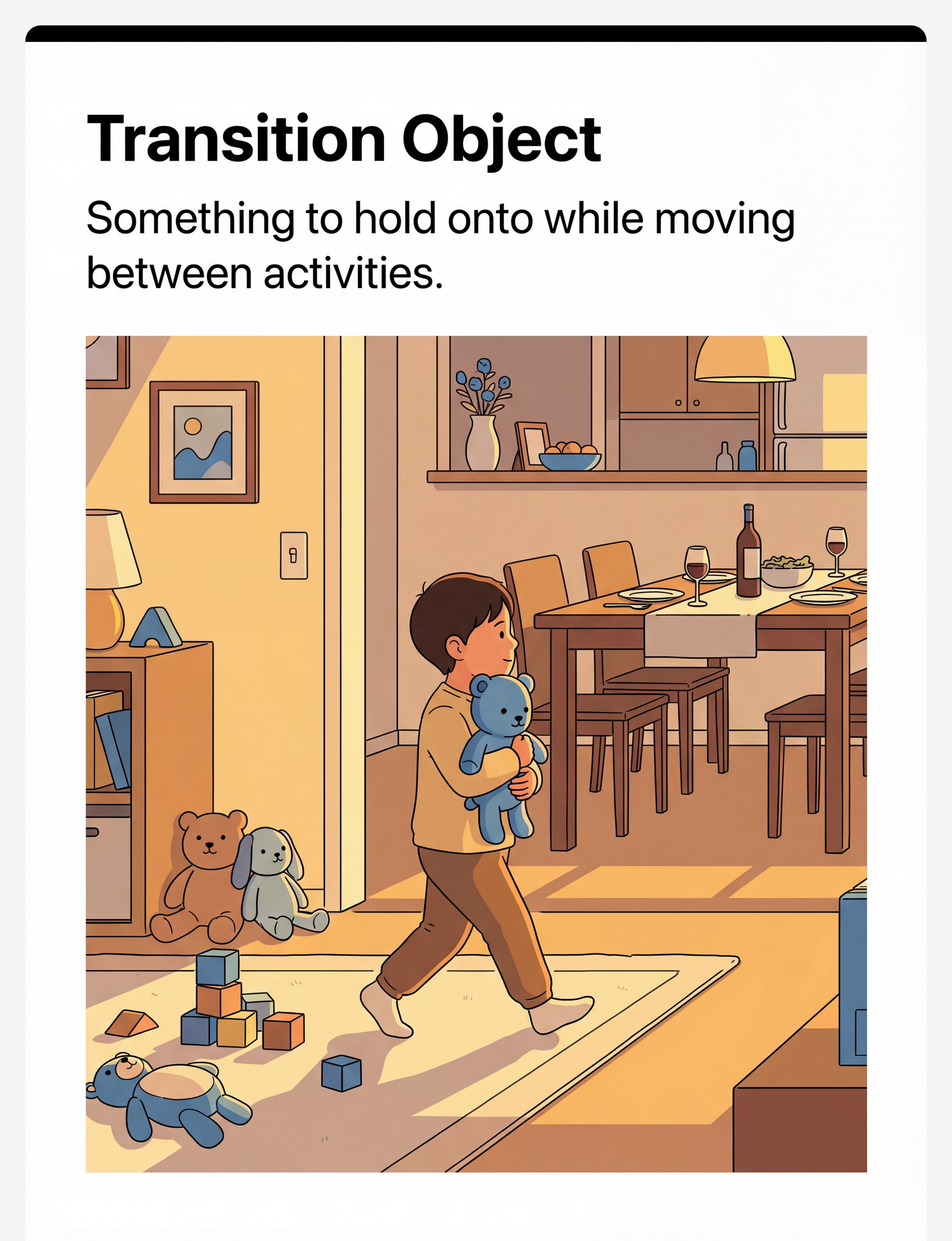
Activity Continuity
Closure rituals and transition objects honor the child's engagement rather than erasing it.
Sensory Regulation
Sensory bridge tools help the nervous system shift states without triggering an arousal cascade.
Motivational Scaffolding
Dinner jobs and reward systems make arrival at the table purposeful and rewarding.
💡 No single material works for every child. The 9 materials address different failure points in the transition chain. Identifying where YOUR child's transition breaks down determines which 2–3 materials to prioritize.
Multi-Disciplinary Team
Five therapy disciplines. One dinner table. Integrated through GPT-OS®.
🔵 Occupational Therapy
OTs design sensory bridge protocols, evaluate sensory profiles, and prescribe weighted tools, fidgets, and environmental modifications. OT addresses why the nervous system resists the sensory shift between activities.

🟣 Applied Behavior Analysis
BCBAs design antecedent intervention systems — the timer, First-Then board, and dinner job are all ABA antecedent strategies. ABA structures the reinforcement schedule that makes transitions rewarding rather than punitive.

🟢 Speech-Language Pathology
SLPs design the visual communication supports (First-Then boards, visual schedules, picture-based closure rituals) that compensate for verbal processing difficulties. Language-based transition warnings often fail — visual supports succeed.

🟡 Special Education
Special educators generalize transition skills from home to school environments. Dinner time transition success builds the foundational flexibility skills required for all classroom and community transitions.
"The brain doesn't organize itself by therapy type. That's why we don't either." — GPT-OS® FusionModule™ principle

Material 1 of 9
📦 Visual Countdown Timer
What It Does
Makes abstract, invisible time concrete and visible for the child's brain. The timer becomes the authority — not the parent's voice. When the red is gone, dinner begins. This removes the adversarial dynamic from the transition announcement entirely.
Canon Category
Visual Schedule Materials
How to Use It
- Set at child's eye level where they are playing
- Set 10 minutes before dinner — let the child see you set it
- Point to it, say "when the red is gone, it's dinner time," then walk away
- Let the timer end the transition — never announce dinner before it rings
Product Options
Price Range: ₹400–1,500
🏅Pinnacle Recommends
DIY Alternative: Phone timer app + draw a clock face on paper with moving hand
Best For: All profiles — this is the single most universal starting material

Material 2 of 9
📦 First-Then Board
What It Does
Shows the child the promise that the preferred activity returns. The resistance to dinner is rarely about dinner — it's about fear of permanent loss. The First-Then board makes the promise visible, reducing anxiety about what happens after the transition.
Canon Category
Visual Schedule Materials
How to Use It
- Place "DINNER" in the FIRST slot, child's current activity in the THEN slot
- Introduce it alongside the timer at the 10-minute warning
- At timer end, bring the board WITH you to the child — don't point to it across the room
- Honor the "THEN" promise every single time. One broken promise sets back weeks.
Product Options
Price Range: ₹200–600
🏅Pinnacle Recommends
DIY Alternative: Two sticky notes on fridge: "FIRST: Dinner" + "THEN: [activity]"
Best For: Anxiety profiles, children who've experienced broken promises
Material 3 of 9
📦 Transition Object / Comfort Item
What It Does
A familiar, beloved object carried through the transition provides emotional anchoring during the state change. It reduces the sense of abandonment the nervous system experiences when a preferred activity is paused. The object is a portable piece of safety.
Canon Category
Transition Objects / Comfort Items
How to Use It
- Identify the child's existing preferred comfort object — no need to buy if one exists
- Hand the object to the child at the moment the timer ends
- The object sits on the table during dinner — it travels back after dinner
- Consistent location for the object matters — it lives in one spot
Product Options
Recommended:Animal Soft Toys — ₹425
🏅Pinnacle Recommends
DIY Alternative: Any small comfort item the child already has — never force a new one
Best For: Sensory avoiders, anxious profiles, ages 3–7
Safety Note: Check for choking hazard size for children under 3

Material 4 of 9
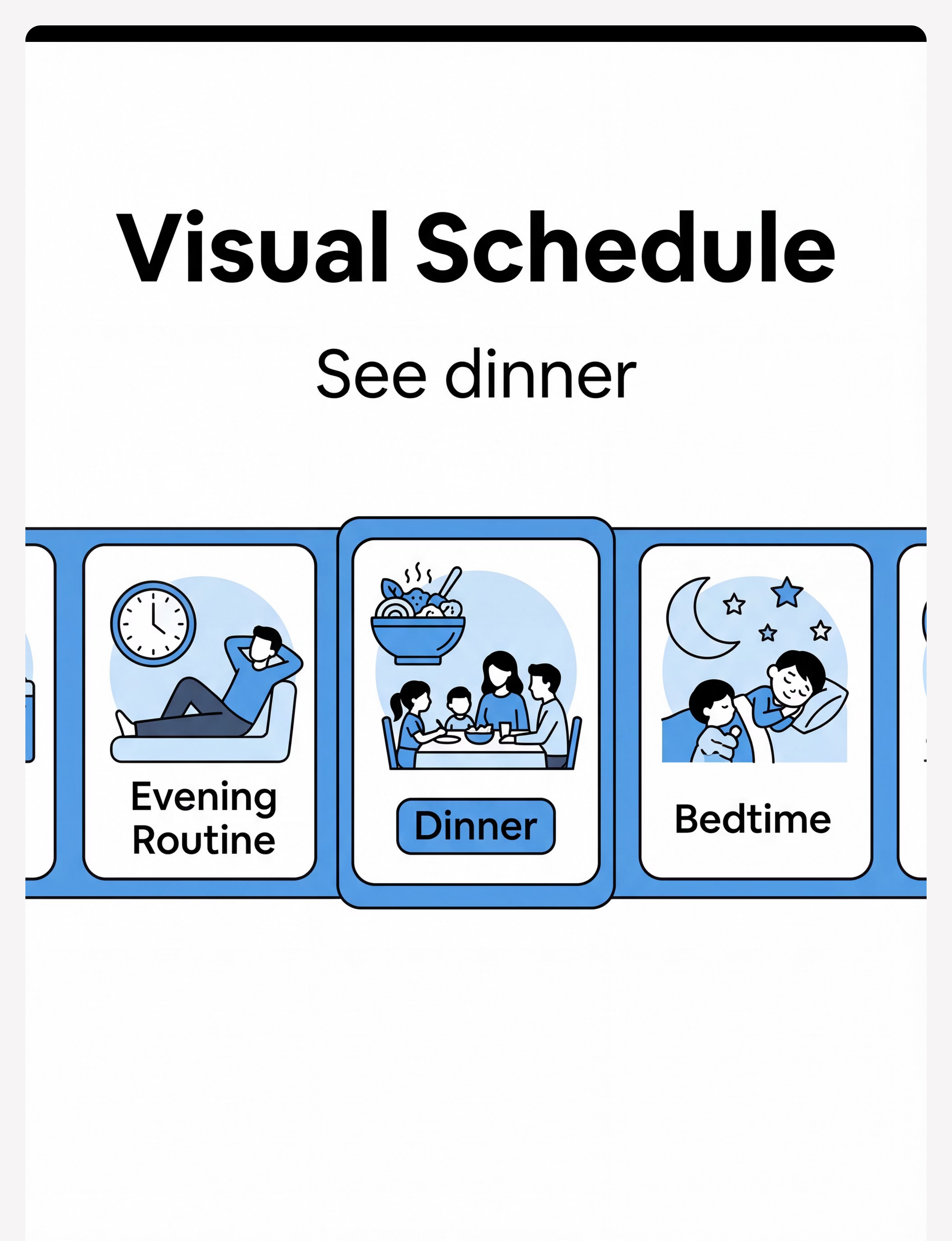
📦 Visual Schedule Strip (Evening)
What It Does
A visual sequence of the entire evening routine gives the child a map of what happens next. Unlike verbal warnings (which are processed and forgotten), the schedule strip remains physically present in the environment. The child can reference it independently, building executive function and reducing surprise at each transition.
Canon Category
Visual Schedule Materials
How to Use It
- Mount at the child's eye level in a hallway or kitchen
- Include 5–7 steps: snack → play → timer → dinner → bath → story → sleep
- At the 5-minute warning, reference it: "Look — dinner is the next picture"
- Let the child move a marker or flip the card when each step is done
Product Options
Price Range: ₹200–800
🏅Pinnacle Recommends
DIY Alternative: 5 index cards with drawings, taped to wall in sequence
Best For: Children who respond to "big picture" predictability; all profiles
Material 5 of 9
📦 Auditory Warning Device (Chime / Timer with Sound)
What It Does
A consistent, non-verbal auditory cue that signals the approach of dinner penetrates hyperfocus better than a parent's voice. The brain encodes the sound as a predictor — over 7–14 repetitions, the chime alone begins to trigger transition-readiness before any other signal. For ADHD profiles especially, layered auditory cues break through where visual tools alone do not.
Canon Category
Sensory Regulation Tools
How to Use It
- Use at the 5-minute warning, distinct from the timer alarm
- The same sound every day — consistency is the mechanism
- Can be a dedicated chime, specific song, or timer mid-point alert
- For ADHD profiles: multiple auditory layers (chime + song + timer) maximize penetration
Product Options
Price Range: ₹200–800
DIY Alternative: Same song played every day as dinner signal (free, Spotify) — the song becomes the cue
Best For: ADHD/hyperfocus profiles; children who don't register visual cues alone
Material 6 of 9
📦 Sensory Bridge Tools (Fidgets / Resistance Bands)
What It Does
A sensory bridge activity helps the nervous system shift from one sensory state (focused play) to another (social mealtime) without triggering an arousal cascade. Physical movement — jumping, carrying, bear walking — provides proprioceptive input that regulates the nervous system during the transition corridor. This is the most OT-specific material in the system.
Canon Category
Sensory Regulation Tools
How to Use It
- Introduce at the 5-minute warning: "In 5 minutes we'll do our jumping to the table"
- Execute immediately after the timer ends, before expecting table arrival
- Sensory seekers: increase intensity (harder activity = more regulating)
- Sensory avoiders: lighter input — carrying objects, slow walking with the fidget
Product Options
Price Range: ₹200–1,000
DIY Alternative: Jumping jacks, bear walk to table, carry water bottles — zero cost
Best For: Sensory seekers, physical resisters, children who meltdown at the boundary
Safety Note: Weighted items: maximum 10% of child's body weight. Consult OT for specific prescriptions.

Material 7 of 9
📦 Activity Closure / Parking System
What It Does
The closure ritual addresses the core emotional fear driving transition resistance: "If I stop now, my work will be destroyed or forgotten." A designated parking spot — a shelf, a tray, a special corner — communicates: your activity is safe; it will be here when you return. This single insight transformed dinner for Ayaan (Card 31) — the Lego parking spot was his turning point.
Canon Category
Visual Schedule Materials
How to Use It
- Identify or create a consistent, visible parking spot before starting the protocol
- At the 5-minute warning: "Start thinking about where to park your [activity]"
- At timer end: child physically places the activity in its spot before moving
- Take a photo if needed — some children need visual proof the activity is preserved
Product Options
Price Range: ₹100–500 (DIY-friendly)
DIY Alternative: Dedicated shelf space + verbal ritual "parked until later"
Best For: Children in mid-project hyperfocus; Lego, drawing, and building enthusiasts
DIY Cost: ₹0 — any existing shelf or tray works

Material 8 of 9
📦 Dinner Helper Apron + Role Badge
What It Does
A purposeful role at dinner transforms the child from a passive recipient of a demand ("come to dinner") to an active, necessary contributor ("dinner can't happen without you"). Purposeful movement — carrying napkins, filling cups, choosing music — fills sensory needs while accomplishing the transition. The dinner job is particularly powerful for ADHD and sensory-seeking profiles.
Canon Category
Reinforcement Menus
How to Use It
- Assign a real, meaningful task — not a pretend one. Children know the difference.
- The job begins the moment the timer ends — it pulls the child toward the table
- Rotate jobs weekly to maintain motivation
- Celebrate the role: "Dinner can't start without our napkin helper"
Product Options
🏅Pinnacle Recommends
DIY Alternative: Any real task: carry napkins, choose music, fill cups — apron optional
Best For: ADHD/hyperfocus profiles, sensory seekers, children who respond to purpose and ownership

Material 9 of 9
📦 Calm-Down Corner Kit
What It Does
A designated regulation space near the dining area gives the child a predictable recovery zone when the transition demand exceeds current regulatory capacity. Its presence alone reduces anticipatory anxiety — knowing there is a safe landing space makes the transition feel less like a cliff edge. It is used proactively, not as punishment.
Canon Category
Sensory Regulation Tools
How to Use It
- Located near the dining area — not far away, not in a bedroom
- Contains 1–3 regulatory tools the child knows and uses
- Introduced proactively: "If you need a minute before dinner, the corner is there"
- Maximum 5-minute use during dinner transition — then gentle invitation to table
Product Options
Price Range: ₹500–2,000
DIY Alternative: Corner with one pillow + one familiar comfort object — ₹0
Best For: Anxiety profiles, sensory avoiders, children with severe dysregulation responses
💡Starter Kit Recommendation: Start with just 3: Visual Timer + First-Then Board + Consistent Auditory Cue. Total starter investment: ₹800–2,900 | Zero-cost DIY version available in the next section.

Equity-First Approach
Every parent can start today. Zero-cost version included.
Following the WHO Nurturing Care Framework principle of equity-focused intervention, every material in this system has a zero-cost household alternative. Clinical-grade materials improve ease and consistency — they are never a prerequisite to starting.
Material | Clinical Version | DIY Household Alternative | |
Visual Countdown Timer | Time Timer® (₹1,500) | Phone timer app + draw a clock face on paper with moving hand | |
First-Then Board | Velcro board (₹400) | Two sticky notes on fridge: "FIRST: Dinner" + "THEN: [activity]" | |
Transition Object | Soft toy / fidget (₹400) | Any small comfort item the child already has | |
Visual Schedule | Printed strip (₹500) | 5 index cards with drawings, taped to wall | |
Auditory Warning | Chime / timer (₹500) | Same song played every day as dinner signal (free, Spotify) | |
Sensory Bridge | Resistance band / fidget (₹400) | Jumping jacks, bear walk to table, carry water bottles | |
Closure Ritual | Tray/parking system (₹300) | Dedicated shelf space + verbal ritual "parked until later" | |
Dinner Job | Helper apron (₹400) | Any real task: carry napkins, choose music, fill cups | |
Calm-Down Corner | Full kit (₹1,500) | Corner with one pillow + one familiar comfort object |
⚡Zero-Cost Complete System: Timer app + 2 sticky notes + child's existing toy + 5 drawn cards + one designated song + jumping jacks + verbal ritual + napkin job + one corner with a pillow = ₹0
⚠️ For children with severe sensory processing profiles, clinically graded weighted tools and specific fidget types make a meaningful difference. Consult your OT before substituting these specific materials. | PMC9978394 | WHO NCF Handbook (2022)
Safety Protocol
Read this before your first session.
🔴 STOP — Do Not Proceed If:
- Child is in active meltdown or severely dysregulated state before dinner
- Child is unwell, feverish, or in physical pain
- There has been a significantly traumatic event today
- You (the caregiver) are in crisis or highly dysregulated
- The dinner environment contains known overwhelming sensory triggers not yet addressed
🟡 MODIFY — Proceed with Adjustments If:
- Child is tired and showing early dysregulation signs (stimming increase, irritability)
- Routine has been disrupted today (school absence, medical appointment, guest visit)
- Child had a difficult transition earlier in the day — reduce expectations, simplify supports
- New food or new dinner setting is being introduced
🟢 GO — Optimal Conditions:
- Child has been home 30+ minutes and had a small snack
- Last transition (school to home) was manageable
- You have 5 minutes before dinner to set up visual supports
- The dinner environment is familiar and sensory demands are known
Material Safety Notes
- Timer devices: Not projectile-safe for children with throwing behaviors — mount on wall
- Fidgets/transition objects: Check for choking hazard size for children under 3
- Weighted items: Maximum 10% of child's body weight; never restrain with weighted blankets
- Sensory bridge foods (crunchy snacks): Mind dietary restrictions and appetite impact
🚨STOP IMMEDIATELY IF: Child shows self-injurious behavior, severe aggression, extreme physical distress, or if any transition support material becomes a projectile or weapon. Escalation: Self-resolve → Call 9100 181 181 → Teleconsultation → Clinic visit

Step 1 of 6
Step 1: The Invitation
Timing: 10 minutes before dinner | Duration: 1–2 minutes | ACT: Set the timer + bring the First-Then Board to the child
What To Do
- Set the visual timer for 10 minutes (or your child's optimal warning window)
- Place it at child's eye level where they are playing
- Bring the First-Then Board: "DINNER" in FIRST slot, child's current activity in THEN slot
- Crouch to child's level — do not stand over them
Therapist Script — Say This Exactly
"Hey [name]. Look — the timer is on. When all the red is gone, it's dinner time. First dinner. Then [activity]. The timer will tell us when."
Then: Point to timer, point to First-Then Board, and walk away. Do NOT wait for verbal acknowledgment. Do NOT negotiate or explain further.
What Resistance Looks Like — and What To Do
Child ignores or says "no." → Don't argue. Leave the timer in place. The visual works even without explicit acknowledgment. The information is received whether or not they show it.
🧠ABA Principle in Action: This is antecedent manipulation — changing the environment BEFORE the behavior to prevent the problem from occurring. | NCAEP EBP 2020 (Antecedent-based interventions)

Step 2 of 6
Step 2: The Engagement
Timing: 5 minutes before dinner | Duration: 1 minute | ACT: 5-minute warning + activity closure signal
What To Do
- Deliver the 5-minute auditory warning (chime, specific song, or timer mid-point sound)
- Reference the visual schedule: "Look — dinner is the next picture on the schedule"
- Begin the activity closure invitation: "Start thinking about a parking spot for your [toy/game]"
Therapist Script — Say This Exactly
"Five minutes, [name]. Look at the schedule — dinner's next. Start thinking where to park your [Lego/game/drawing] until after dinner."
Child Response Indicators
- Engagement: Child looks at schedule, may begin looking for stopping point ✅
- Tolerance: Child continues activity but glances at timer ✅
- Avoidance: Child ignores completely — increase visual salience, don't escalate verbally
Reinforcement cue: Any acknowledgment or schedule-glancing = quiet, specific praise: "Great — you looked at the timer. That's exactly right."
🌉The Sensory Shift Begins Here: If your child needs a sensory bridge, introduce it now: "In 5 minutes we'll do our [jumping/carry/bear walk] to the table." | Visual supports as EBP (NCAEP 2020)

Step 3 of 6
Step 3: The Therapeutic Action
Timing: At timer completion | Duration: 2–4 minutes | ACT: Timer ends → Activity closure ritual → Sensory bridge → Move to table
Execution Precision — What Matters Most
- Consistency: Same sequence, same words, same materials, every single day
- Momentum: Keep moving through steps — don't pause for negotiation mid-sequence
- Calm: Your nervous system regulates theirs. If you are stressed, they will escalate.
Common Execution Errors
- ❌ Announcing dinner verbally BEFORE the timer ends (defeats the timer's authority)
- ❌ Allowing one more minute after timer (destroys predictability)
- ❌ Carrying child physically without warning (activates fight-or-flight)
- ❌ Threatening consequences mid-sequence (triggers oppositional response)
Correct Responses to Resistance
- Child protests: "I know it's hard. The timer says dinner. You can do this."
- Child runs: Go WITH them, do not chase. "I'm walking with you."
- Child drops to floor: Wait 30 seconds calmly. Then: "Ready to walk? I'll walk with you."
📚 PMC10955541 | NCAEP 2020 | Antecedent-Based Intervention + Visual Supports as EBP

Step 4 of 6
Step 4: Repeat and Vary
ACT: Maintain consistent daily protocol with graduated variations
Phase | Approach | Goal | |
Week 1–2 | Use all supports consistently. Same sequence, same materials, every day. | Neural pathway formation — consistency IS the intervention | |
Week 3–4 | Identify which 2–3 materials your child responds to most strongly | Consolidate core supports | |
Week 5–8 | Consolidate around core supports; introduce single variations one at a time | Build independence and ownership |
Variation Toolkit (introduce one at a time after Week 2)
Shorter warning window
Builds independence — introduce at Week 4+ if consistent
Child sets the timer
Ownership + agency — introduce at Week 3+
Child places First-Then pictures
Buy-in and participation — introduce at Week 2+
Child chooses parking spot
Autonomy and self-direction — introduce at Week 2+
Different sensory bridge
Generalization across contexts — introduce at Week 3+
Pinnacle Principle: Consistency × Days = Neurological change. The 22nd repetition works differently than the 1st. Stay the course.
Step 5 of 6
Step 5: Reinforce and Celebrate
Timing: Within 3 seconds of the child being seated at the table | ACT: Deliver specific, immediate, authentic reinforcement
"You DID IT. You parked your game and walked to dinner. That took real courage. I'm proud of you."
🗣️ Verbal Praise (Always)
Specific, enthusiastic, immediate — every session, regardless of how hard it was. "You looked at the timer. You put your toy away. You came to dinner. That's amazing."
⭐ Token/Sticker System
One sticker per successful transition. Visible sticker chart at the table. Reward Stickers — ₹364 | Reward Jar — ₹589
🎯 Honor the First-Then Promise
The natural reinforcer: "Dinner first — and then straight to [activity], just like we agreed." This is non-negotiable and builds everything.
🍽️ Preferred Food at Dinner
Ensure one known-liked item is always on the plate during the transition training phase. Eating the preferred food reinforces arrival at the table.
⚠️ What NOT to do: ❌ Withhold reinforcement because the transition was hard (reinforce arrival, not ease of arrival) ❌ Use food as a bargaining tool mid-transition ❌ Over-praise in a way that feels performative. Celebrate the attempt, not just the success. A 15-minute transition that was 45 minutes last week is a win. Name it. | ABA Reinforcement Principles | BACB Ethical Guidelines
Step 6 of 6
Step 6: The Cool-Down
ACT: Signal transition end + honor the First-Then promise. This step is the payoff — and it is non-negotiable.
Close Dinner with Predictability
"Almost done — two more bites, then all done." Give the child a clear ending signal, just as you gave a clear beginning signal.
Transition Warning for Dinner Ending
"Dinner is finishing. In two minutes, you can go back to [activity]." Mirror the same warning structure used at dinner's beginning.
Release Cue
"Dinner is done. Great job. Time for [activity] — just like the First-Then board said." The promise is fulfilled. Trust is deposited.
Material Put-Away Ritual
Age-appropriate shared routine: child places plate in sink, parents clear table together. Shared closure signals the end of the transition demand.
Every kept First-Then promise builds a trust deposit. The child begins to believe that dinner ends and the preferred activity returns. Over weeks, the anxiety about the transition itself reduces — because the child has experienced that it is survivable and the good thing comes back.

Troubleshooting
Session abandonment is not failure. It's data.
"My child ignored the timer completely"
Why it happened: The timer hasn't yet become a reliable predictor — it takes 7–14 repetitions. What to do: Ensure the timer is at child's eye level and they see you SET it. Add pointing to the timer for the first 2 weeks every time.
"My child had a full meltdown when the timer ended"
Why it happened: The transition demand was too abrupt even with the timer. What to do: Add a sensory bridge immediately after timer end (jumping, carrying) before any expectation to move. Also check: was the "Then" sufficiently motivating?
"The First-Then board didn't help — they forgot it the second the timer rang"
Why it happened: In-the-moment dysregulation overrides cognitive reminders. What to do: Bring the board WITH you to the child at timer end. Point to it while saying the words. The visual needs to be physically present, not on the wall.
"My child sat at the table but was completely dysregulated and couldn't eat"
Why it happened: Residual transition distress at the table. What to do: Brief regulation break at the table (fidget, 3 deep breaths together, 60-second cool-down) before expecting eating engagement. Seated = success. Eating comes next.
"We tried this for 3 days and it's getting worse, not better"
Why it happened: First-day contrast effect — new structure increases resistance before it reduces it. What to do: Days 3–7 are often the hardest. If still escalating at Day 14, call 9100 181 181 for a teleconsultation.
"My child does this perfectly at school but fights it at home"
Why it happened: Masking and school fatigue mean home is where dysregulation releases. What to do: Increase supports at home (not reduce), acknowledge the extra effort school requires, consult with school to share what works there.
"I started the protocol but I couldn't stay consistent"
Why it happened: You are also tired at 6pm. Parent depletion is real. What to do: Simplify to one material only. One consistently-used material beats five inconsistently-used ones every time.

Personalization
No two children. No two protocols.
For the Sensory Seeker
Craves input, appears hyperactive
- Increase sensory bridge intensity — harder physical activity = more regulating
- Allow fidget/squeeze toy at table during dinner
- Shorter warning window may work better (10 min → 5 min)
- Dinner job involving heavy carrying is ideal — fills sensory need while completing transition
For the Sensory Avoider
Withdraws, overwhelmed by change
- Longer warning window (15–20 minutes preferred)
- Transition object is critical — keep it consistent
- Minimize new sensory demands at dinner table during transition period
- Calm-down corner should be very low-stimulus; regulation space quality matters
For ADHD / Hyperfocus Profile
Multiple auditory cues penetrate hyperfocus better than a single timer
- Physical involvement at timer end: child physically touches timer to turn it off
- Dinner job is the highest-impact material — purposeful movement beats passive "come to table"
- Very short warning windows may work better once trust is established
For Anxiety Profile
Maximum predictability is non-negotiable
- Never change the routine without warning
- First-Then MUST be honored every time — one broken promise sets back weeks
- Child choosing the "Then" activity increases perceived control
- Regulation corner presence reduces anticipatory anxiety even if rarely used
Age Adjustments
Ages 3–5
2 materials max. Keep it simple. Transition object is most important.
Ages 6–9
Standard 5-material protocol. Involve child in setting timer.
Ages 10–12
Transfer ownership progressively. Child sets timer, chooses job, runs closure ritual independently.
Week 1–2: Foundation Phase
In weeks 1–2, you are teaching a new language, not expecting fluency.
15%
Foundation Phase Progress
You are building neural pathways. They are not yet visible on the surface — but they are forming.
✅ What You Will Likely See
- Child begins to glance at the timer — even without acknowledging it
- Transition time reduces from baseline to slightly shorter
- One or two transitions happen with less intensity than before
- Child accepts the sensory bridge even if they still resist the table
⏳ What You Will NOT See Yet (and that's normal)
- Smooth, easy transitions — this comes at weeks 5–8
- Child referencing the visual schedule independently
- Voluntary movement toward the table before cueing
"If your child tolerated the timer for 3 seconds longer than last week — that is real, measurable progress. Neural pathway formation is not visible. It is cumulative. You are building something that does not yet show on the surface."
📊Data Checkpoint: Review your tracking data at Day 14. Are distress scores trending down, even slightly? Is transition duration shorter by even 2–3 minutes? Those are the signals. What matters most in Weeks 1–2 is consistency of the sequence, not smoothness of the transition. | PMC11506176 — Sensory integration intervention outcomes emerge across 8–12 week timelines.
Week 3–4: Consolidation Phase
The brain is forming new circuits. Watch for these early signals.
40%
Consolidation Phase Progress
Neural associations are strengthening. You may notice the first signs of anticipation.
✅ Child ANTICIPATES the timer
May look toward it before it ends — the neural association is forming. This is the first major signal.
✅ Faster table arrival
Child moves toward table within 2–3 minutes of timer ending (vs. 10+ minutes in Week 1).
✅ Reduced distress
Distress level during transition drops from 4–5 to 2–3 on your tracking scale.
✅ Closure ritual acceptance
Child completes the activity parking ritual with less resistance — the goodbye to the activity is becoming safer.
✅ Spontaneous schedule references
Child says "dinner's next" unprompted — executive function transferring beyond dinner.
"You may notice you are more confident too. Your calm at 5:55pm is different than it was 3 weeks ago. That is also real therapeutic progress."
⬆️When to Increase: If transitions are consistently taking under 10 minutes with distress levels of 2 or below, begin introducing child choice: child sets timer, child places First-Then pictures. | Neuroplasticity evidence — synaptic strengthening timelines in pediatric populations.
Week 5–8: Mastery Phase
Mastery indicators. The progress you've been building toward.
75%
Mastery Phase Progress
Three specific, observable, measurable criteria mark mastery for this protocol.
Mastery Criterion 1
Child moves to dinner table within 5 minutes of timer completion on 4 out of 5 days.
Mastery Criterion 2
Transition occurs with distress level 1–2 (calm acceptance or brief mild resistance) on 4 out of 5 days.
Mastery Criterion 3
Child independently executes 1+ transition support (sets timer, runs closure ritual, walks to dinner job) on 3 out of 5 days.
Maintenance Check — Week 6
Try removing ONE material for one week. Does performance hold? If yes, that material was scaffolding that is now internalized. If distress returns, reinstate immediately. Never remove more than one material at a time.
When to Progress
Child meets mastery criteria consistently → Explore: I-791 Bedtime Transitions | I-788 Morning Routines | Browse all Daily Living Transitions at techniques.pinnacleblooms.org
📚 PMC10955541 | BACB Mastery Criteria Standards

Clinical Awareness
Even in the celebration zone. Stay clinically aware.
🔴 Transition resistance INTENSIFYING despite consistent 4-week protocol
What it may indicate: Underlying anxiety disorder, unidentified sensory processing profile, or co-occurring condition requiring professional assessment.
🔴 Self-injurious behavior during transitions
What it indicates: Regulatory capacity is insufficient for the demand. Professional OT/ABA assessment required immediately.
🔴 Transitions have generalized to ALL daily activities
What it may indicate: Significant executive function impairment, autistic inertia, or anxiety disorder warranting comprehensive neurodevelopmental assessment.
🔴 Child eating significantly less or showing food refusal at the table
What it may indicate: Dinner context is associated with distress beyond the transition — a feeding therapy evaluation may be needed alongside transition support.
🔴 Child distressed or inconsolable for more than 30 minutes
What it indicates: The intervention intensity needs professional calibration. Call 9100 181 181 immediately.
🔴 You (the caregiver) are unable to maintain the protocol due to overwhelm
What it indicates: Parent support is needed. This is not weakness — it is a data point. Parent regulation is foundational to child regulation.

Related Techniques
You already own materials for several of these.
Your visual timer, First-Then board, and visual schedule strip — purchased for dinner transition — apply directly to most related techniques in this domain. One investment, multiple techniques.
Technique | Code | Difficulty | Your Materials Apply? | |
Morning Routine Transition Support | I-788 | 🟡 Core | ✅ Same timer + schedule | |
Activity Stopping Strategies | I-789 | 🟢 Intro | ✅ Same closure rituals | |
Bedtime Transition Support | I-791 | 🟡 Core | ✅ Same visual system | |
Screen Time Ending Protocol | I-795 | 🟡 Core | ✅ Same First-Then board | |
Getting Dressed Transition | I-787 | 🟢 Intro | ✅ Same visual schedule | |
Leaving the Park / Outdoor Activity | I-801 | 🔴 Advanced | Partial — additional tools needed |
Developmental Map
This technique is one piece. Here is the full picture.
Dinner Time Transition is a Domain D (Behavior and Flexibility) technique with secondary impact on Domain C (Emotional Regulation) and Domain E (Feeding and Mealtime). Mastery of this technique feeds directly into the overall Adaptive Behavior Readiness Index within GPT-OS®.
Your Child's Next Domain Priorities
Domain A — Sensory Processing
Prioritize if sensory bridge was critical for this child's protocol
Domain C — Emotional Regulation
Prioritize if dysregulation was severe during transition attempts
Domain E — Feeding and Mealtime
Prioritize if dinner table participation remains challenging after transition is resolved
📚 WHO/UNICEF Nurturing Care Framework — Five components of nurturing care require holistic developmental monitoring.
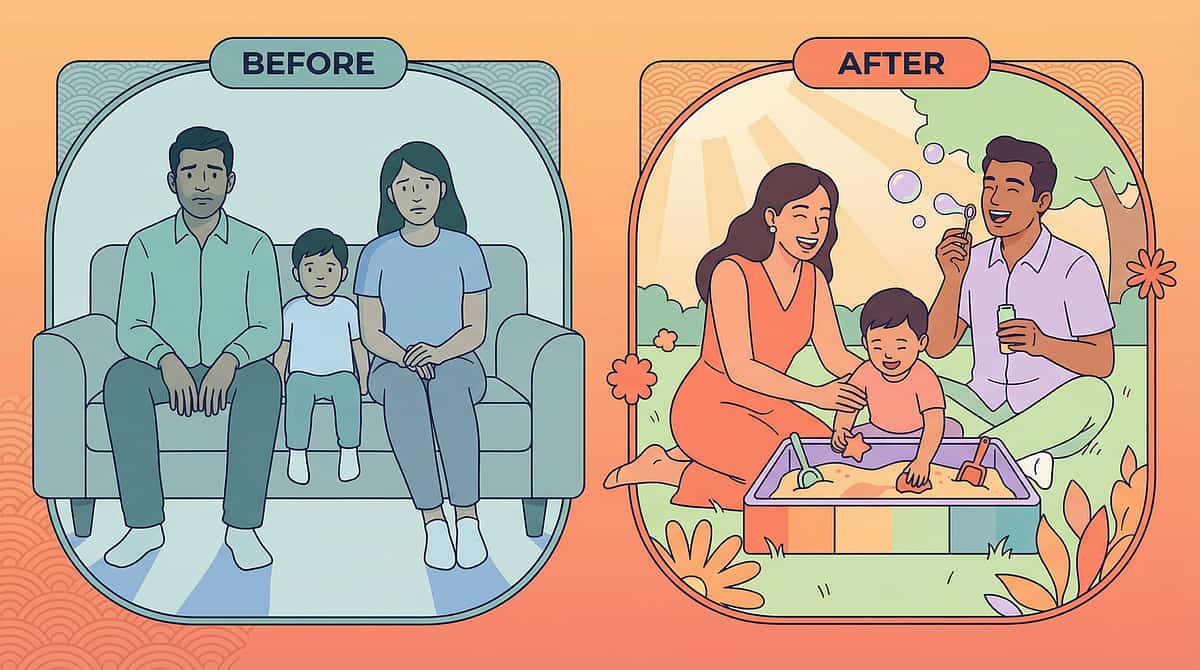
Real Families
Real families. Real dinners. Real change.
Ayaan, 6 — Mumbai
Before: "Every single evening ended with screaming. He'd been warned ten times. Transition took 45 minutes, dinner was cold, everyone was exhausted. We dreaded 5:30pm."
After — Week 9: "He now walks to the kitchen when the timer ends. Not always happily. But he comes. The parking system for his Lego was the turning point — he stopped feeling like we were destroying what he was building. Dinner is still noisy, but it's a family dinner now."
Timeline: 9 weeks. Primary materials: Visual timer + Lego parking spot + Dinner job (napkin setter).
Priya, 8 — Hyderabad
Before: "She didn't hear warnings. She didn't believe promises. 'You can play after dinner' meant nothing because she'd been disappointed before. The meltdown at dinner time was the worst part of our day."
After — Week 6: "The First-Then board changed something fundamental. She could SEE the promise. She started checking it mid-dinner — 'Is my game still there?' And when we honored it, every single night, she began to trust the system. Now she places her own 'Then' card before dinner."
Timeline: 6 weeks. Primary materials: First-Then board (visual contract) + parent commitment to honoring promises.
"What these families discovered is that dinner time transition difficulty is rarely about dinner. It's about trust, predictability, and neurological gear-shifting. When we reduce the cognitive and emotional demand of the transition itself, most children arrive at the table quite willingly. The meal was never the problem." — Pinnacle OT + ABA Team, GPT-OS® Protocol I-790
Professional Support
Home + clinic = maximum impact.
Your Specialist Team for I-790
🔵 Occupational Therapist
Full sensory profile assessment → specific sensory bridge prescription → weighted tool calibration. OT addresses why the nervous system resists the sensory shift.
🟣 BCBA / ABA Therapist
Functional assessment of transition resistance → individualized antecedent intervention design → data system setup and monitoring.
🟢 Speech-Language Pathologist
Visual communication support design → picture symbol selection → verbal script calibration for your child's language level.
🟡 Special Education Specialist
Generalization from home to school → teacher communication → IEP/ILP integration. What works at home can work everywhere.
70+ Centers Across India
Find your nearest Pinnacle center at pinnacleblooms.org/centers
📱 Teleconsultation Available
Can't travel to a center? Pinnacle offers teleconsultation for:
- Initial strategy review — which 3 materials to start with
- Data review at Week 2 and Week 4
- Escalation consultation if protocol is not showing progress
Insurance / Funding
OT and ABA services for autism are covered under select insurance plans and government disability support schemes in India. Our team can guide you through funding access.
Research Library
Deeper reading for the curious parent and the clinical professional.
[1] PRISMA Systematic Review (2024)
16 studies, 2013–2023. Sensory integration intervention meets criteria as evidence-based practice for ASD. Visual supports and antecedent strategies confirmed effective for transition management. PMC11506176 → PubMed
[2] Meta-Analysis: World Journal of Clinical Cases (2024)
24 studies. Sensory integration therapy effectively promotes adaptive behavior, self-regulation, and social skills. 40-minute structured sessions showed maximum effectiveness. PMC10955541 → PubMed
[3] Indian RCT: Padmanabha et al. (2019)
Home-based sensory interventions delivered by trained parents demonstrated significant outcomes across daily living domains in Indian pediatric population. DOI:10.1007/s12098-018-2747-4
[4] NCAEP Evidence-Based Practices Report (2020)
Visual supports, antecedent-based interventions, and parent-implemented interventions all classified as evidence-based for autism spectrum disorder. NCAEP 2020 Report
[5] WHO Care for Child Development Package (2023)
Implemented in 54 LMICs. Demonstrates household-material-based intervention efficacy. Equity principle: every parent can do this. PMC9978394 → PubMed

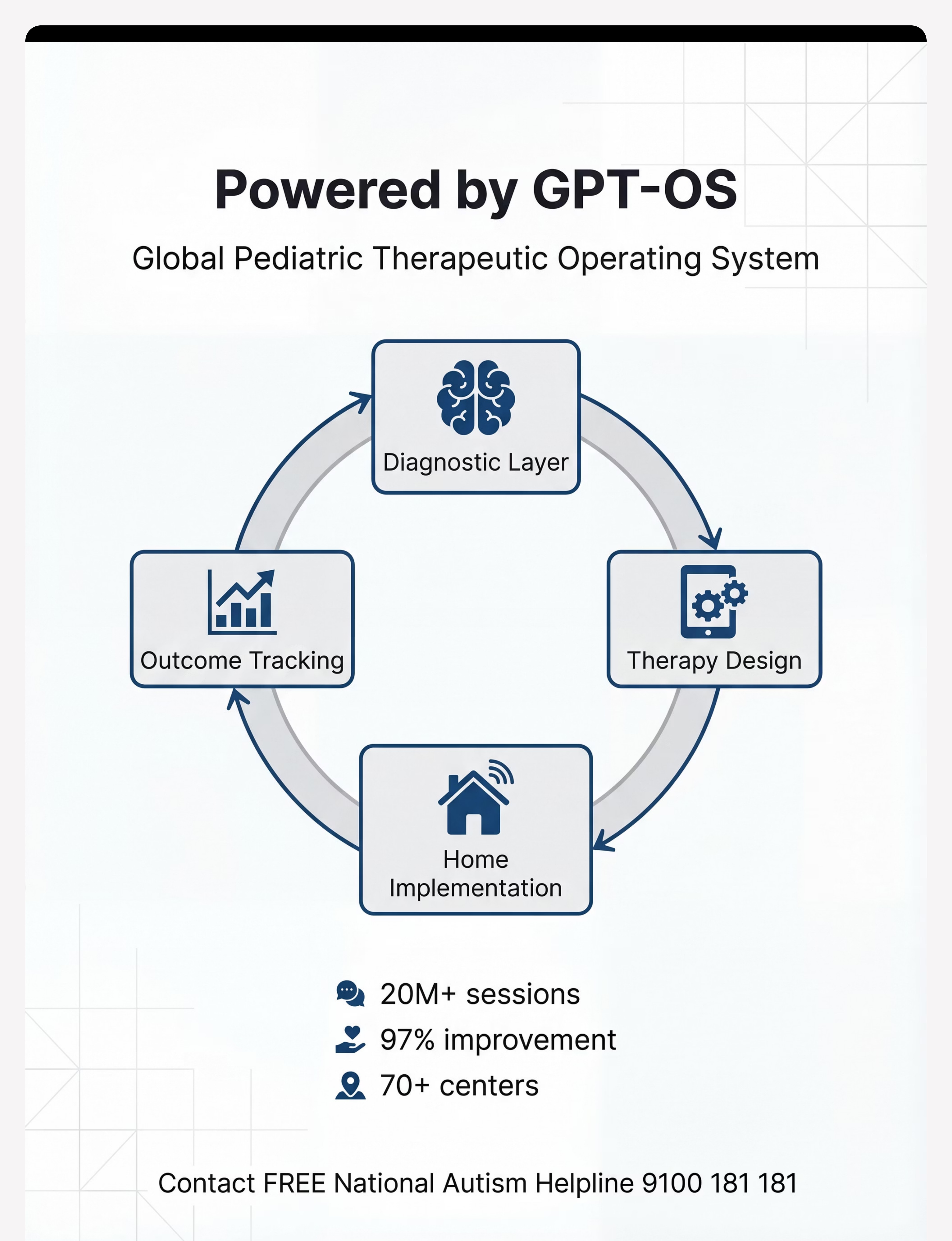
GPT-OS® Technology
This is not software. This is therapeutic infrastructure.
What GPT-OS® Learns from I-790 Data
- Which materials correlate with fastest transition time reduction for this profile
- What distress level patterns predict next-session success
- When to escalate to professional review vs. continue home implementation
Your Data Contributes to Population Knowledge
Population-level insights improve recommendations for every family navigating dinner time transitions globally. Your child's data — anonymized — helps the next child.
GPT-OS® Components Active for I-790
AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ | Independence Readiness Index
🔒Privacy Assurance: All data is anonymized for population-level analysis. Individual family data is visible only to your designated therapy team. | Digital health intervention evidence — 2024 meta-analysis, 21 RCTs, 1,050 participants.

Watch the Reel
Watch the therapist demonstrate these 9 materials in 60 seconds.
🎬 Reel ID
I-790
🏷️ Series
Daily Living Transitions — Episode 790
⏱ Duration
75–85 seconds
👶 Age Band
3–12 years
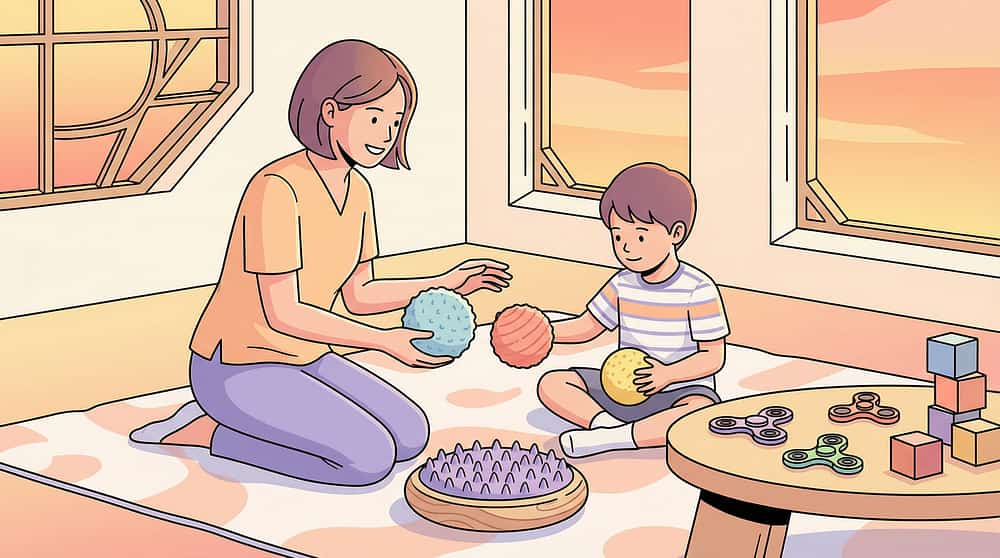
What You'll See in the Reel
01
Visual timer showing countdown during play time
02
First-Then board presentation and reference
03
Child carrying transition object toward table
04
Sensory bridge activity (jumping, carrying)
05
Activity closure ritual (parking spot)
06
Child performing dinner helper job
07
Successful arrival at dinner table — family together
"Dinner time transition difficulty is one of the most documented — and most misunderstood — daily challenges in neurodivergent families. It looks like defiance. It is neurology. These 9 materials provide the external scaffolding the brain needs." — Pinnacle Blooms Consortium OT + ABA + Child Development Team
📚 Video modeling is an Evidence-Based Practice for autism (NCAEP 2020). Watching a demonstration before executing the protocol increases parent confidence and accuracy by up to 40%.
Share This Page
Consistency across caregivers multiplies impact. Share this page.
When every adult in a child's life uses the same sequence, the same materials, and the same language, the neurological effect compounds. Share this page with everyone who feeds your child.
For Spouses / Partners
"This is the protocol we're following for dinner time. Please watch the reel (Section 44) and use the same sequence I do. If we both do the same thing, it works twice as fast." Share: techniques.pinnacleblooms.org/daily-living-transitions/dinner-time-transition-I-790
For Grandparents — The 3 Things to Always Do
- Set the timer 10 minutes before dinner and show it to the child
- Show the First-Then board: "First dinner, then [activity]"
- Let the timer end the transition — do NOT say "dinner time" before it rings
For Teachers / School — Template
"[Child's name] is working on activity transitions using visual supports at home. The most effective tools are: visual timer, First-Then board, and auditory warning sequence. If possible, using similar systems at school for activity transitions would accelerate generalization. Our therapy team is happy to connect."
FAQ
Your most common questions, answered.
How long before I see results?
Most families see measurable reduction in transition duration and distress level within 2 weeks. The first week often shows no improvement — or slight worsening. This is normal (extinction burst or novelty resistance). Week 2–3 is when the trend turns. Full, consistent transitions typically emerge at weeks 5–8.
My child is 3 years old. Is this too young?
No. Ages 3–5 benefit most from the visual timer + transition object + one consistent auditory cue. Keep it to 2 materials maximum. The visual supports work because they bypass verbal processing — age-appropriate regardless of language level.
What if my child destroys the visual schedule?
This is important information: the visual is creating anxiety, not reducing it. Switch to a different format — verbal + single First-Then rather than full schedule. Some children do better with less predictability visible at once. Consult your OT.
We tried visual timers before. They didn't work.
Two common failure reasons: (1) The timer wasn't at the child's eye level where they were playing — visibility is critical. (2) The timer was used without the First-Then board — the timer alone shows the loss; the First-Then board shows the gain. The combination is significantly more effective than either alone.
My partner doesn't believe in "all this visual stuff."
The research in Section 42 is the answer. Visual supports are classified as Level 1 Evidence-Based Practice for autism and ADHD by the National Clearinghouse on Autism Evidence and Practice (2020). This isn't parenting philosophy — it's applied neuroscience.
Do I have to do this every day? We have bad days.
Yes, daily consistency is the intervention. On bad days, simplify (one material only) rather than skipping. A 5-minute simplified version on a hard day maintains the neural association better than skipping entirely. The sequence matters more than the smoothness.
My child has no diagnosis. Can we still use these materials?
Absolutely. These materials work for any child who struggles with activity transitions, regardless of diagnosis. Transition difficulty exists on a spectrum. If significant impairment persists despite consistent 4-week protocol, it is worth seeking a developmental assessment.
What's the difference between this and just being consistent with discipline?
Discipline addresses motivation and compliance. These materials address capacity — they compensate for genuine neurological difficulty in task-switching. A child who cannot shift gears due to executive function challenges will not respond to discipline for the inability. They need scaffolding. When capacity is supported, behavior naturally improves.
Your child is ready for dinner to be easier.
Start today.
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
🏛️ Validated by the Pinnacle Blooms Network® Consortium | OT • SLP • ABA/BCBA • SpEd • NeuroDev • Pediatrics
Preview of 9 materials that help with dinner time transition Therapy Material
Below is a visual preview of 9 materials that help with dinner time transition therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

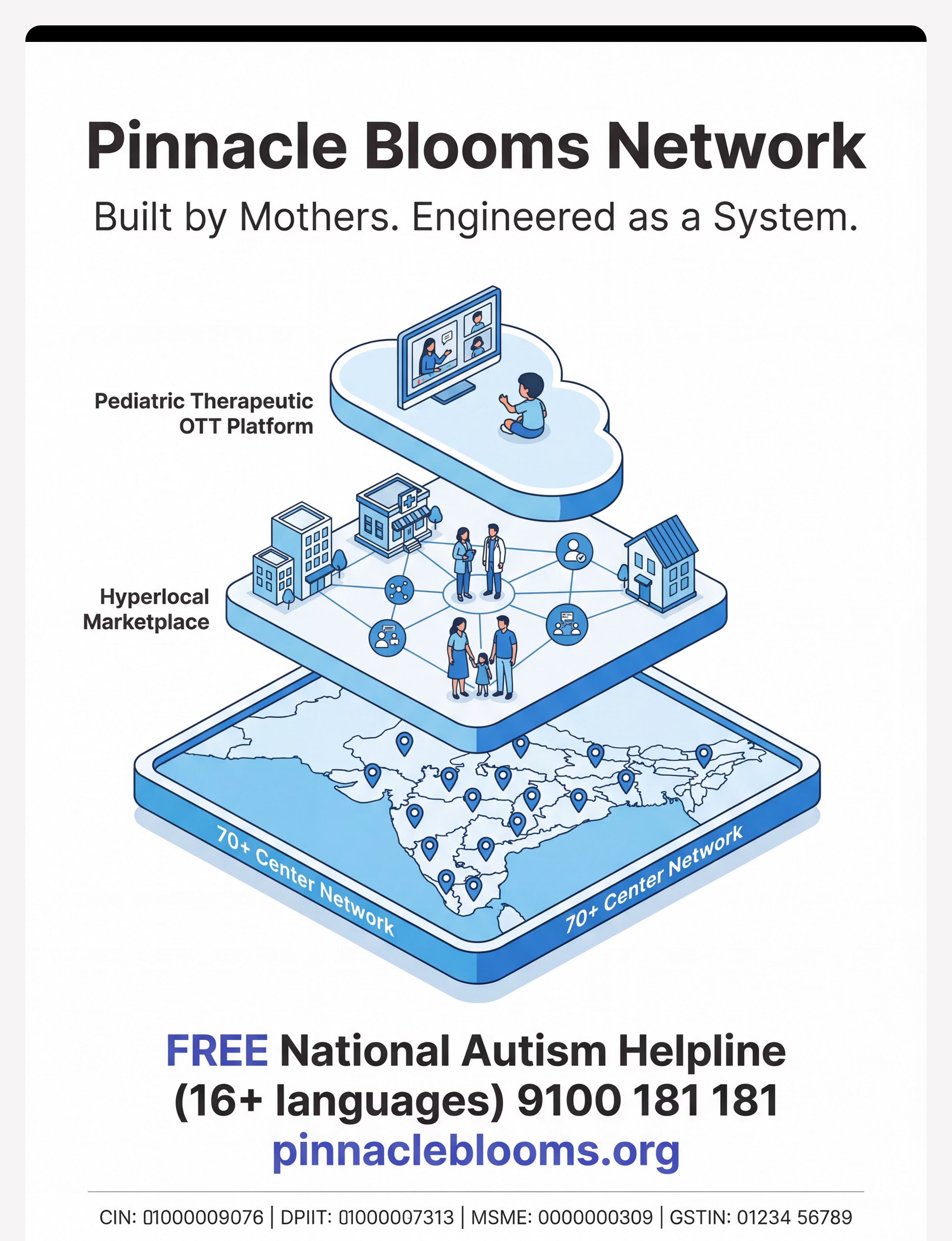
Pinnacle Blooms Network®
🏛️ The Pinnacle Promise
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24×7 personalized pediatric therapy center — serving children from 70+ countries through the GPT-OS® platform. 21 million therapy services. 97%+ proven improvement.
Next Techniques in Your Journey
I-791: Bedtime Transition Support
I-788: Morning Routine Transitions
Browse All Daily Living Techniques
Medical Disclaimer
This content is educational. Transition difficulties can indicate underlying conditions requiring professional assessment. Individual children require individualized approaches developed with qualified therapists. Severe transition difficulties, self-injurious behavior, or prolonged daily dysfunction warrant professional evaluation. Strategies should be adapted to each child's specific needs with qualified professional guidance. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Identifier | Number | |
CIN | U74999TG2016PTC113063 | |
DPIIT Recognition | DIPP8651 (Govt. of India) | |
MSME Udyog Aadhaar | TS20F0009606 | |
GSTIN | 36AAGCB9722P1Z2 |
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Content protected under Indian Copyright Act.
GPT-OS® | AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ are registered trademarks and proprietary systems of Pinnacle Blooms Network®. Patents filed across 160+ countries. All clinical data governed by GPT-OS® data standards.
techniques.pinnacleblooms.org | I-790 | DLT-MEAL | WHO/UNICEF-Aligned