
L-980 | INDEPENDENCE & ADAPTIVE SKILLS
9 Materials That Help With Daily Living Skills
"I still dress him every morning. He's seven." Every button. Every bite. Every bathroom trip. Ninety minutes of prompting before your day even begins. You are not failing. Your child's nervous system is navigating invisible mountains — and these 9 materials begin to change that, permanently.
OT Primary
ABA Validated
WHO Aligned
70+ Centers

YOU ARE NOT ALONE
Millions of families navigate this exact challenge every morning.
Face ADL Challenges
Of children with autism show significant difficulty in at least one daily living skill domain
Diagnosed in India
Children diagnosed with autism — the world's largest affected population
Sessions Delivered
1:1 therapy sessions delivered by Pinnacle across India
India is home to an estimated 18–20 million individuals on the autism spectrum. According to the National Trust for Welfare of Persons with Autism (2024), fewer than 15% receive structured occupational therapy for daily living skills — creating an enormous gap between need and access.
"You are among millions of families navigating this exact challenge. You are not alone. And there is a proven pathway forward."
PRISMA Systematic Review (2024): 80% of children with autism display sensory processing difficulties directly impacting self-care. PMC11506176.
THE SCIENCE BEHIND THE STRUGGLE
This isn't defiance. It's neurology.
"When your child can't button their shirt, their brain is genuinely struggling — not choosing to frustrate you. The motor planning circuits that make buttoning automatic for you require enormous conscious effort for them."
"When your child screams during tooth brushing, the sensation of bristles is neurologically amplified — it genuinely hurts more than it would for you."
This is a wiring difference, not a behavior problem. And wiring differences respond to specific, systematic teaching.

THE FOUR NEUROLOGICAL MECHANISMS
What's happening in your child's brain & body
Motor Planning (Praxis)
The cerebellum and premotor cortex must coordinate dozens of micro-movements to button a shirt. For children with developmental differences, these pathways are slower and require significantly more conscious effort.
Somatosensory Processing
The texture of a tag, water on skin, toothbrush bristles — when the somatosensory cortex over-amplifies tactile input, these experiences become genuinely aversive, not manipulative.
Executive Function & Sequencing
Getting dressed involves 10–15 discrete motor and cognitive steps. Working memory, task-switching, and inhibition must all coordinate — neurologically more demanding for children with autism.
Interoception — The Hidden Sense
Recognizing internal body signals (hunger, toileting need, temperature) requires a well-calibrated interoceptive system. Children who "don't notice" are experiencing interoceptive differences — not noncompliance.
These are the specific neurological reasons daily living skills must be taught differently — broken into smaller steps, supported by the right materials, approached with sensory awareness. Frontiers in Integrative Neuroscience (2020), DOI: 10.3389/fnint.2020.556660

THE DEVELOPMENTAL TRAJECTORY
Your child is not "behind." They are on a different timeline.
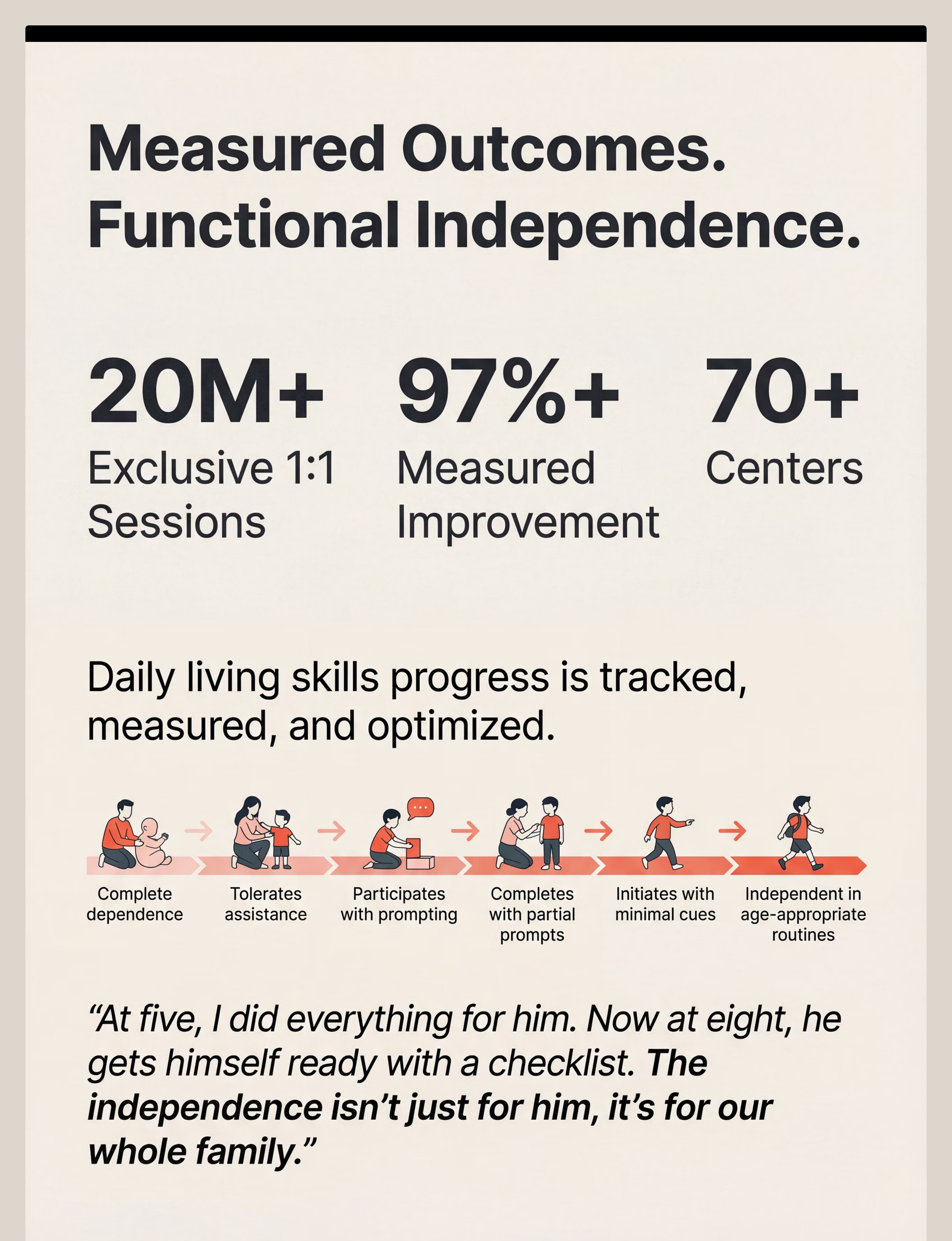
With the right support, moving forward — one skill at a time. The WHO milestone timeline shows typical acquisition, but your child's path is unique.
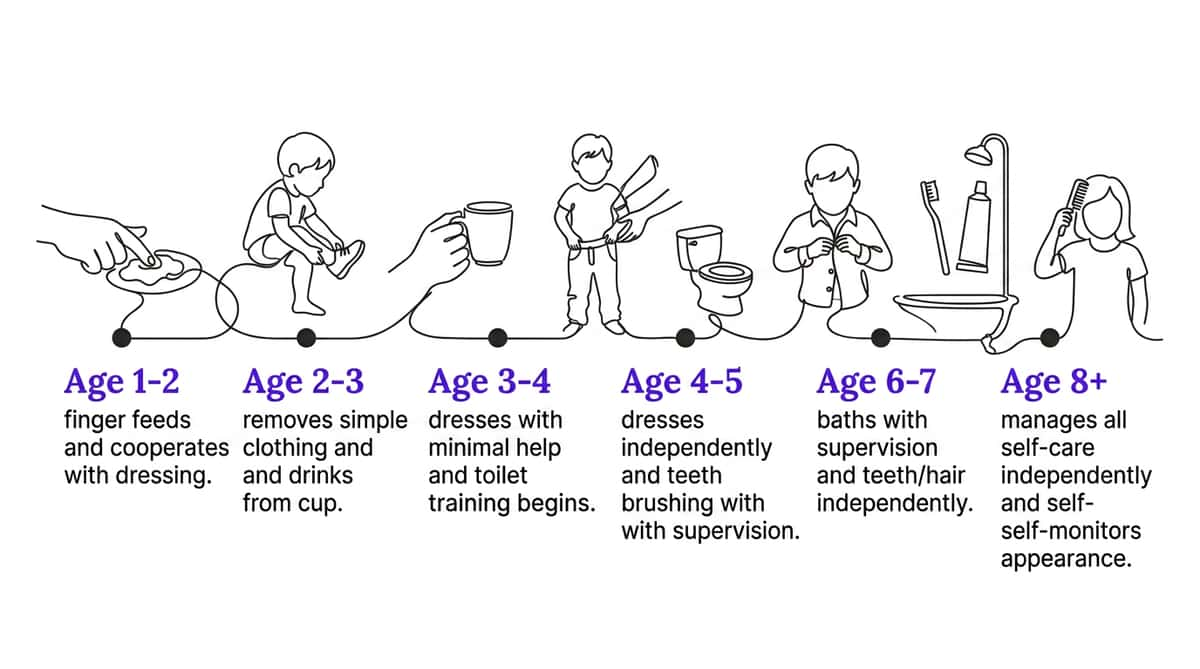
"Your child is here on this timeline. With consistent, materials-supported, task-analyzed teaching, the research shows significant ADL skill gains across 8–12 week intervention windows."

CO-OCCURRING CONDITIONS
Typical challenges that compound ADL difficulties
Sensory Processing Disorder
80%+ comorbidity with autism — the foundational barrier to self-care tolerance
Developmental Coordination Disorder
DCD/Dyspraxia — motor planning basis of dressing and feeding challenges
ADHD
Attention required for multi-step self-care routines is significantly impacted
Anxiety
Transition resistance and rigidity in hygiene routines create daily friction

CLINICAL EVIDENCE GRADE
Clinically validated. Home-applicable. Parent-proven.
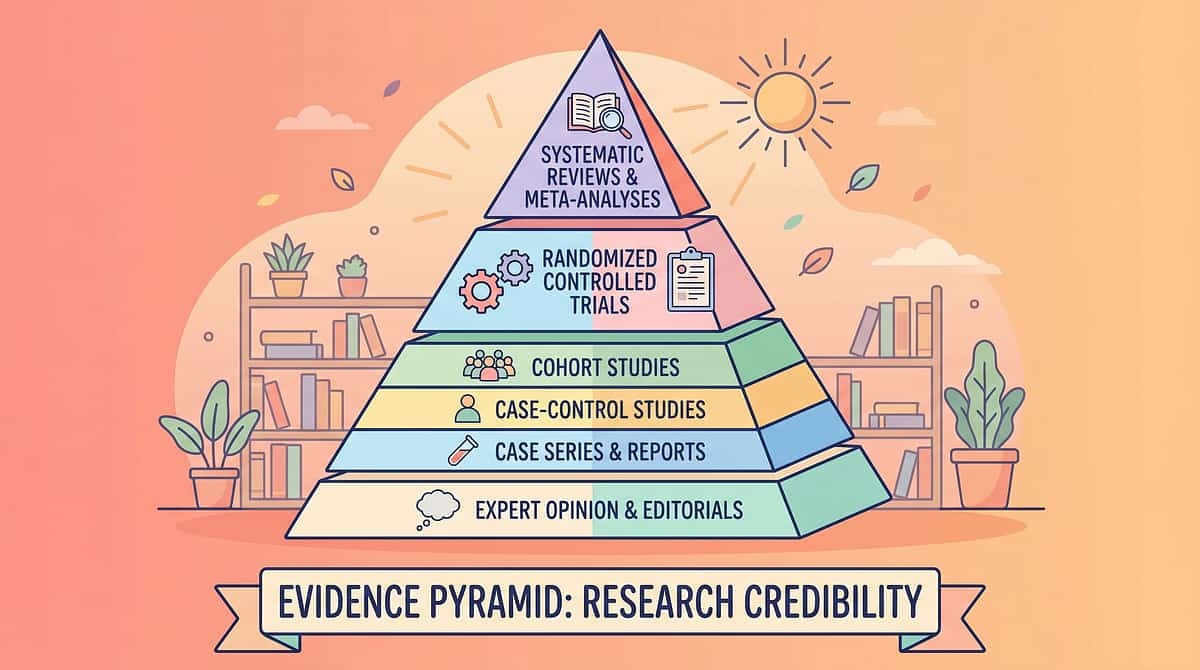
Evidence Grade: Level I–II
Systematic Reviews + Clinical RCTs — Supported by WHO, UNICEF & NCAEP
97%
Research Confidence
98%
Home Applicability
95%
Parent Deliverability

FIVE EVIDENCE PILLARS
The research foundation for these 9 materials
Task Analysis & Visual Supports — Level I
NCAEP (2020) classifies visual supports and task analysis as Established Evidence-Based Practices for autism.
Adaptive Equipment — Level II
AOTA Practice Guidelines confirm adaptive equipment's role in enabling independence while building underlying skills.
Sensory Modifications — Level I
PRISMA systematic review (2024): Sensory integration intervention meets evidence-based criteria for ASD. PMC11506176.
ABA-Based Motivation Systems — Level I
Token economy and First-Then contingencies: Level I evidence across 100+ studies. BACB-endorsed best practice.
Indian Context Validation
Padmanabha et al., Indian Journal of Pediatrics (2019): Home-based OT demonstrated significant outcomes in Indian pediatric population.
"These 9 materials are not accessories. They are clinical tools, validated by the same evidence base that governs therapy in 70+ Pinnacle centers across India."

WHAT THESE MATERIALS ARE
The Daily Independence Toolkit
Formal Name: Activities of Daily Living (ADL) Material Support System
Activities of Daily Living (ADLs) are the foundational self-care tasks required for personal maintenance and independent living: eating, dressing, toileting, bathing, and grooming. For children with developmental differences, these "simple" tasks involve complex intersections of motor planning, sensory processing, sequencing, interoception, and motivation. The 9 materials form a comprehensive support system — each targeting a different barrier domain — to systematically move children from dependence to functional independence.

THE CONSORTIUM BEHIND THESE MATERIALS
Who uses these materials
These materials are prescribed, monitored, and refined by an integrated consortium of pediatric specialists — because daily living skills cross every therapy boundary.
OT — Primary Lead
Occupational Therapists prescribe adaptive equipment, sensory modifications, task analysis, and establish ADL baselines using Vineland Adaptive Behavior Scales
SLP
Speech-Language Pathologists address oral motor components of feeding, communication during self-care routines, and social stories for toileting
ABA/BCBA
BCBAs design reinforcement systems, data collection protocols, prompt hierarchies, and First-Then motivation architectures
Special Education
Build self-monitoring systems, independence checklists, and generalize skills across school and home settings
NeuroDev Pediatrics
Provide the diagnostic foundation — motor planning assessments, sensory profiles, and medical clearance for interventions
"The brain doesn't organize by therapy type. A child learning to dress is simultaneously practicing motor planning (OT), following sequences (SpEd), managing sensory input (OT + NeuroDev), and responding to reinforcement (ABA)."
THERAPEUTIC TARGETS
Not random activities. Precision tools aimed at specific developmental domains.
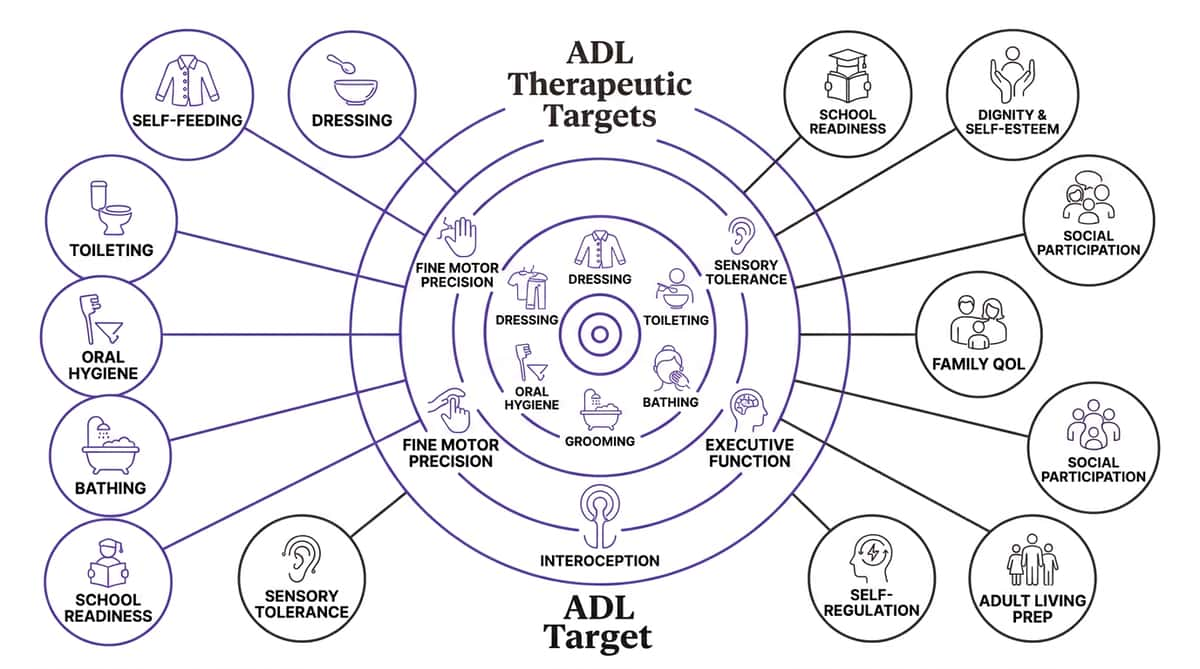
Each target is measured through GPT-OS® Self-Care Readiness Index and Adaptive Behavior Readiness Index, tracking progress from complete dependence to full functional independence.

THE 9 MATERIALS
9 materials. 9 barriers. 1 path to independence.
Nine evidence-based materials. Nine barriers addressed. One path to independence. Each one will get its own dedicated card — with the science, the setup, and the procurement path.
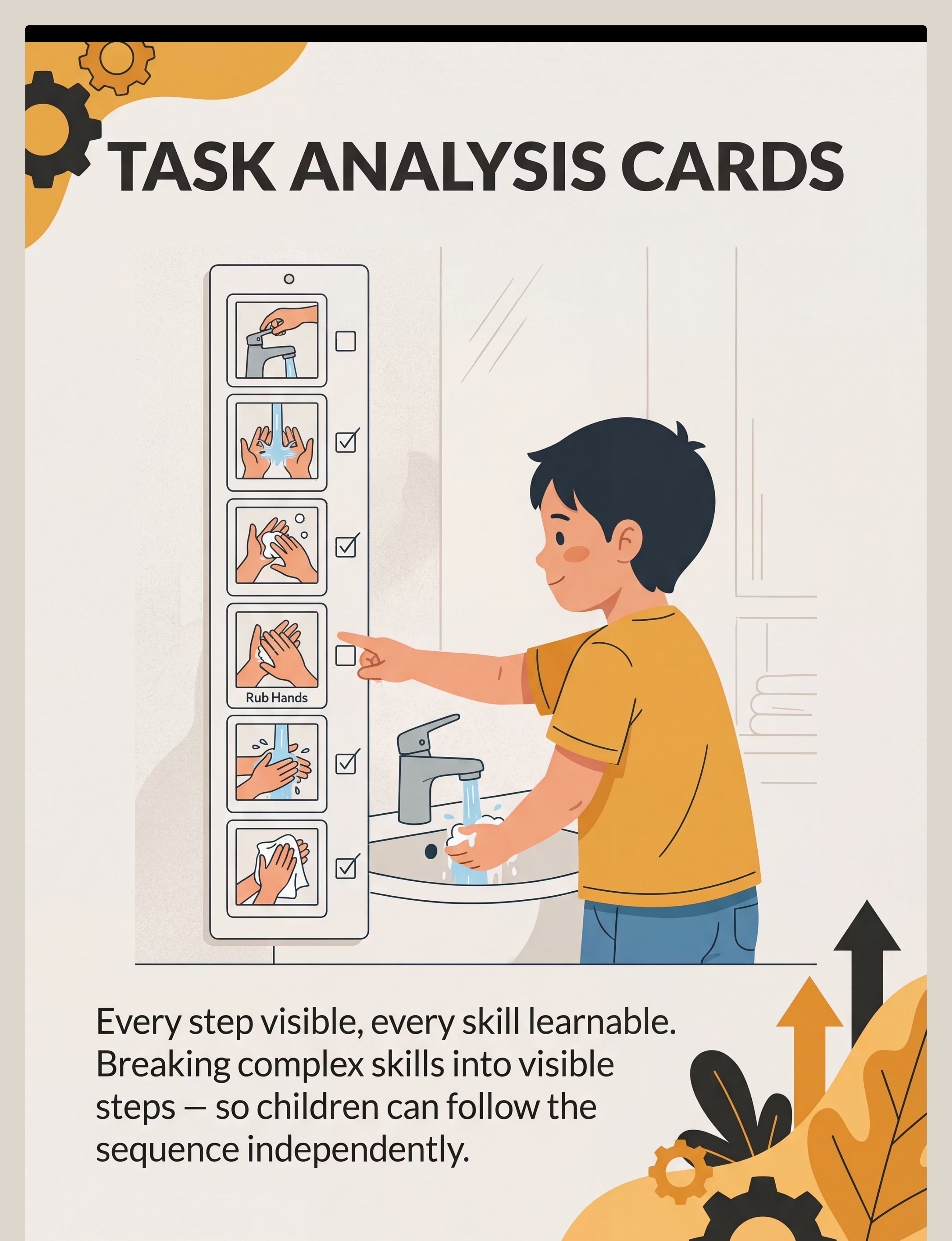
MATERIAL 1 OF 9
Visual Task Analysis Cards
The Science
Working memory and motor planning deficits mean the child cannot hold 10+ steps in mind while executing them. External visual sequences reduce cognitive load to zero — the card holds the memory, the child holds the brush.
What It Is
Laminated, pictorial step-by-step cards for each ADL skill — handwashing (10 steps), toothbrushing (12 steps), dressing (10+ steps), toileting (10 steps).
Every step visible, every skill learnable
Home Procurement: ₹200–800 | Search Amazon.in: "visual task analysis cards children autism"

MATERIAL 2 OF 9
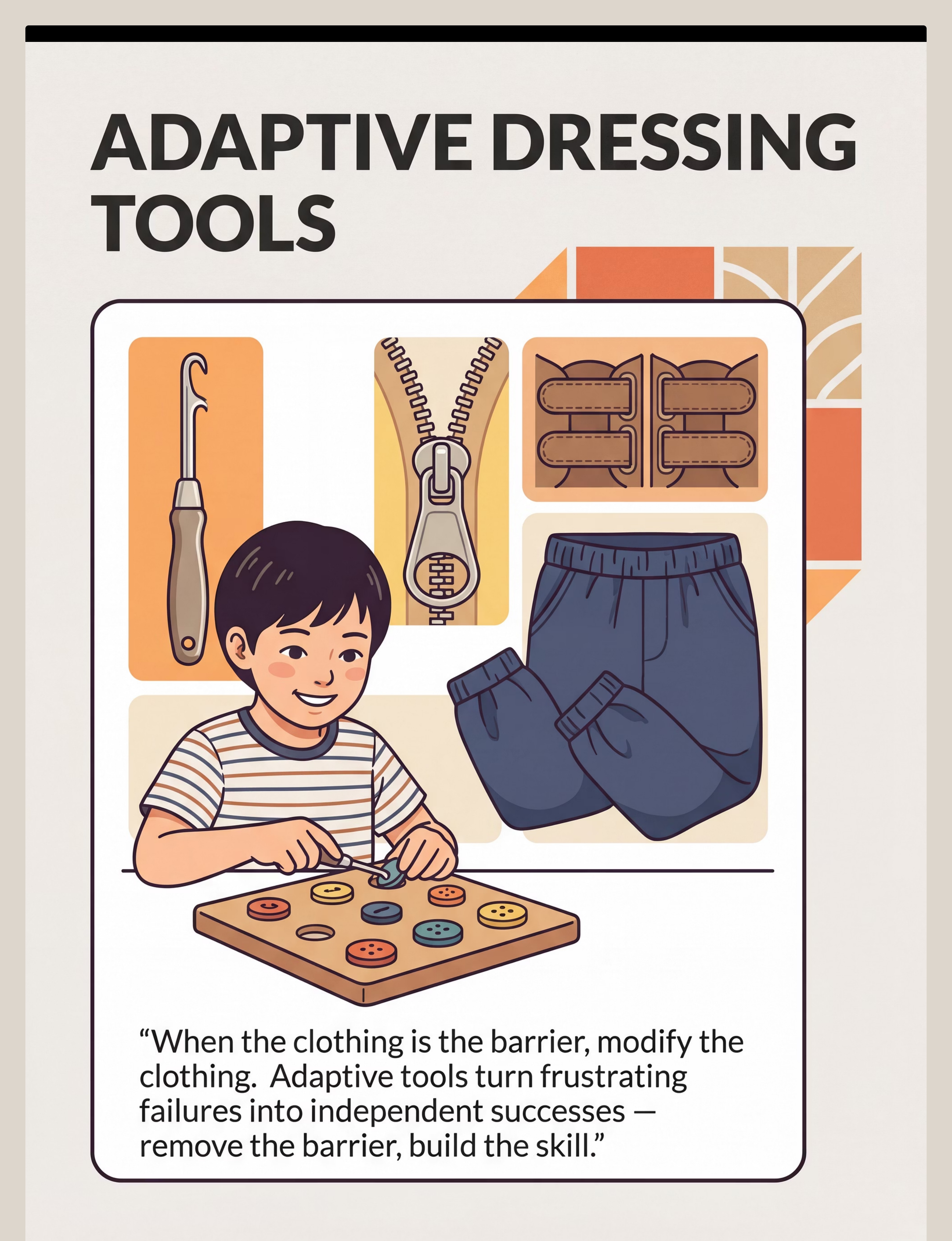
Adaptive Dressing Tools & Modified Clothing
The Science
Dressing failure is often not conceptual — it's physical. Buttons require bilateral coordination and fine motor precision. Tags create genuine sensory distress. Adaptive tools remove the barrier, enabling the skill to develop.
What It Is
- Button hooks and zipper pulls
- Elastic-waist pants and tagless seamless clothing
- Velcro shoe closures and sock aids
When clothing is the barrier, modify the clothing
Home Procurement: ₹300–1,500

MATERIAL 3 OF 9
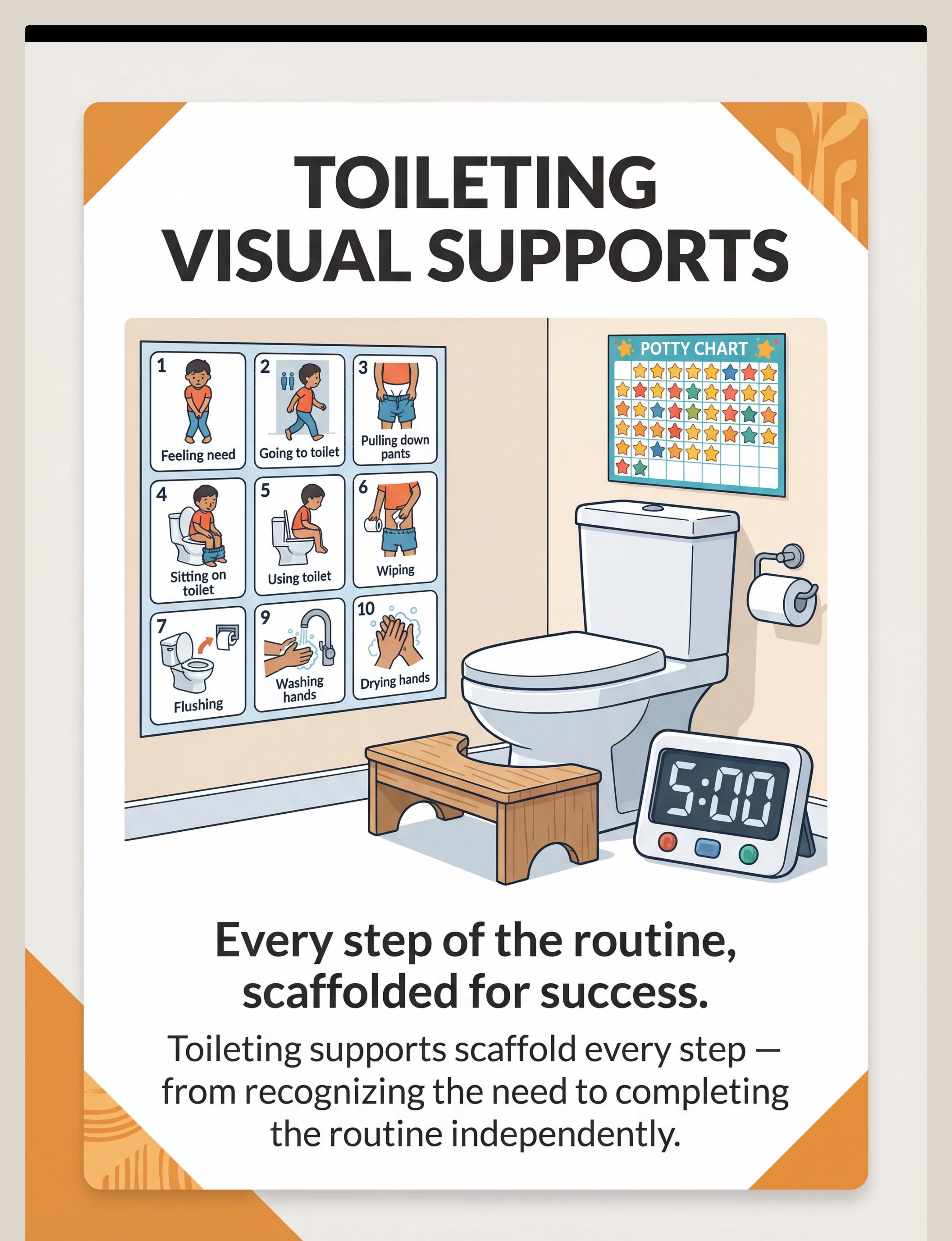
Toileting Visual Supports & Routine Aids
The Science
Toileting is a 10-component routine. Children who miss any component (interoception, clothing management, wiping, handwashing) remain toileting-dependent. Visual supports scaffold each component simultaneously.
What It Is
Toileting visual sequence (posted in bathroom), potty chart with stickers, digital/sand timer, footstool for positioning, wiping aids.
Every step of the routine, scaffolded for success
Home Procurement: ₹200–1,000
Pinnacle Recommends: Reinforcement Menus for toileting rewards — The Rosette Imprint Reward Jar ₹589

MATERIAL 4 OF 9
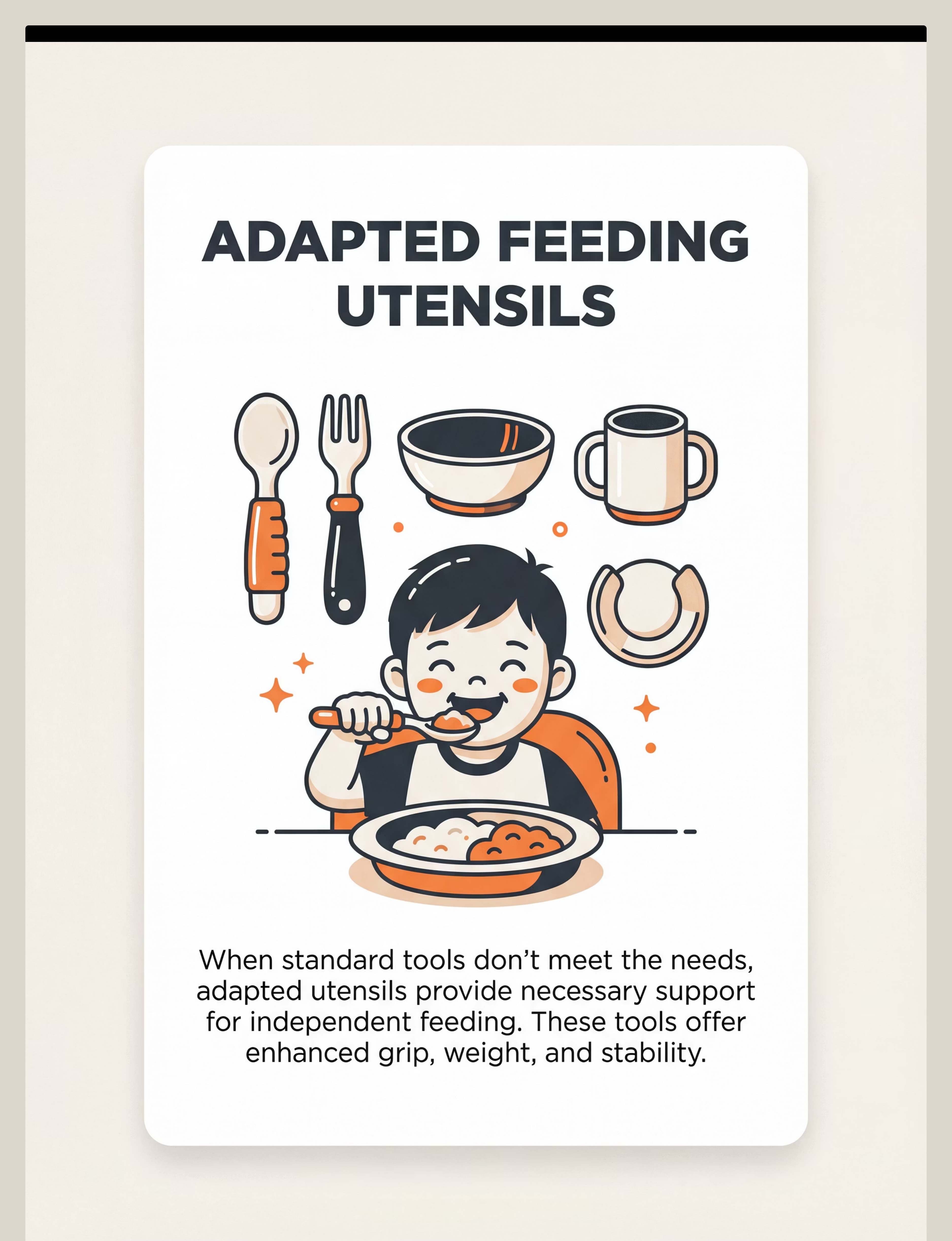
Adapted Feeding Utensils & Mealtime Tools
The Science
Self-feeding requires grip strength, bilateral coordination, oral-motor control, and sensory tolerance — all simultaneously. Adapted utensils remove the motor barrier, allowing the child to focus on oral-motor and sensory skill development.
What It Is
- Built-up grip spoons and forks
- Weighted utensils for proprioceptive feedback
- Non-slip bowls and plate guards
- Two-handled cups and angled utensils
Match the tool to the child, then progress
Home Procurement: ₹300–1,200
MATERIAL 5 OF 9
Oral Care Tools with Sensory Modifications
The Science
Oral hypersensitivity makes standard toothbrushing genuinely aversive — not dramatic. Sensory-modified tools provide the same dental hygiene function while reducing the sensory input intensity the child must tolerate.
What It Is
Ultra-soft/silicone bristle toothbrush, unflavored toothpaste, vibrating or non-vibrating options, visual 2-minute timer, step-by-step brushing sequence card, mouth mirror.
Making tooth brushing tolerable, then routine
Home Procurement: ₹200–800

MATERIAL 6 OF 9
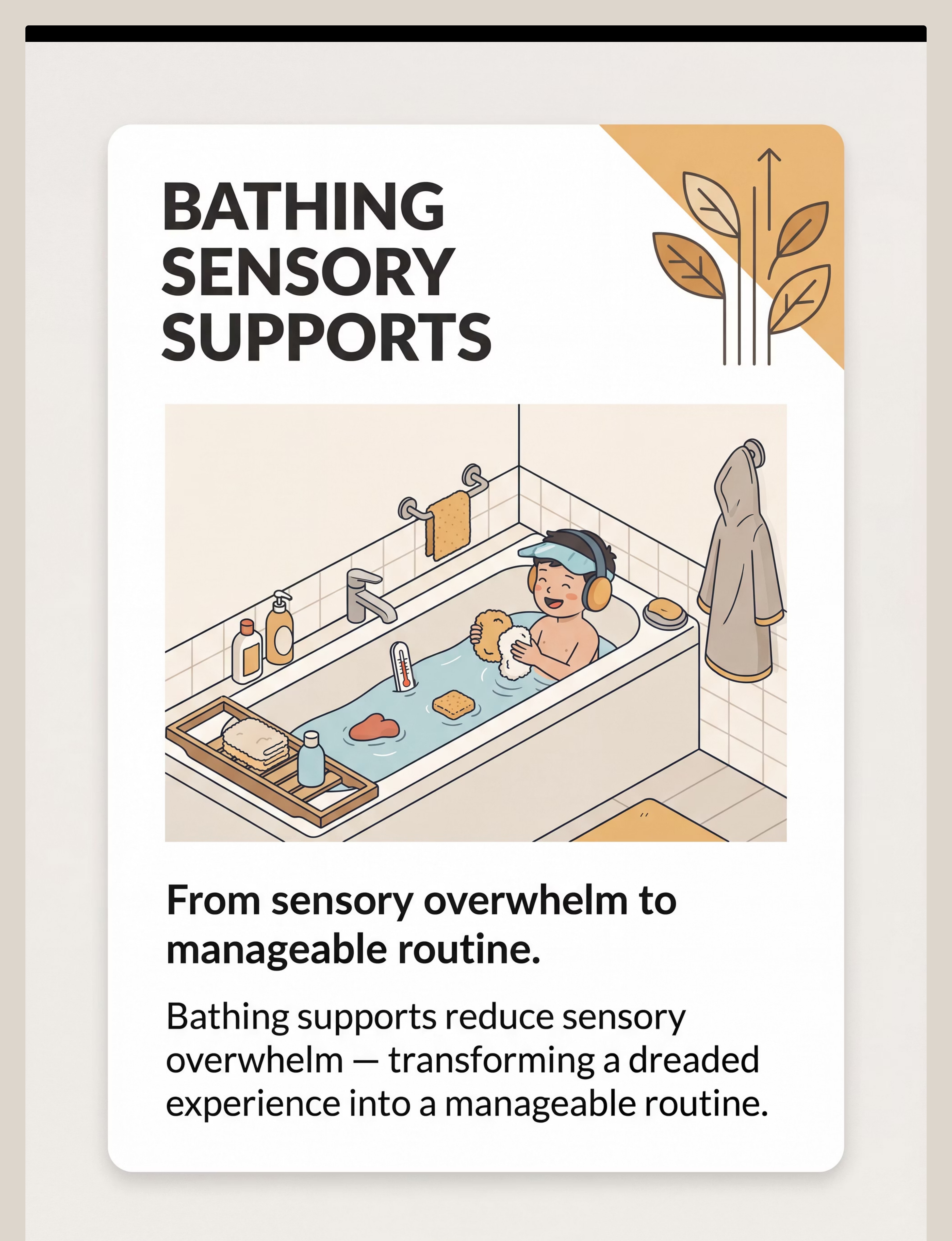
Bathing & Hygiene Sensory Supports
The Science
Bath time activates multiple sensory channels simultaneously — water temperature, wetness, soap texture, hair washing, sound. Sensory supports modulate each input channel independently, transforming sensory overwhelm into manageable routine.
What It Is
- Bath thermometer for consistent temperature
- Non-slip mat and bath visor/shield
- Fragrance-free gentle products
- Hooded towel, soft washcloth, rinse cup
From sensory overwhelm to manageable routine
Home Procurement: ₹300–1,000

MATERIAL 7 OF 9
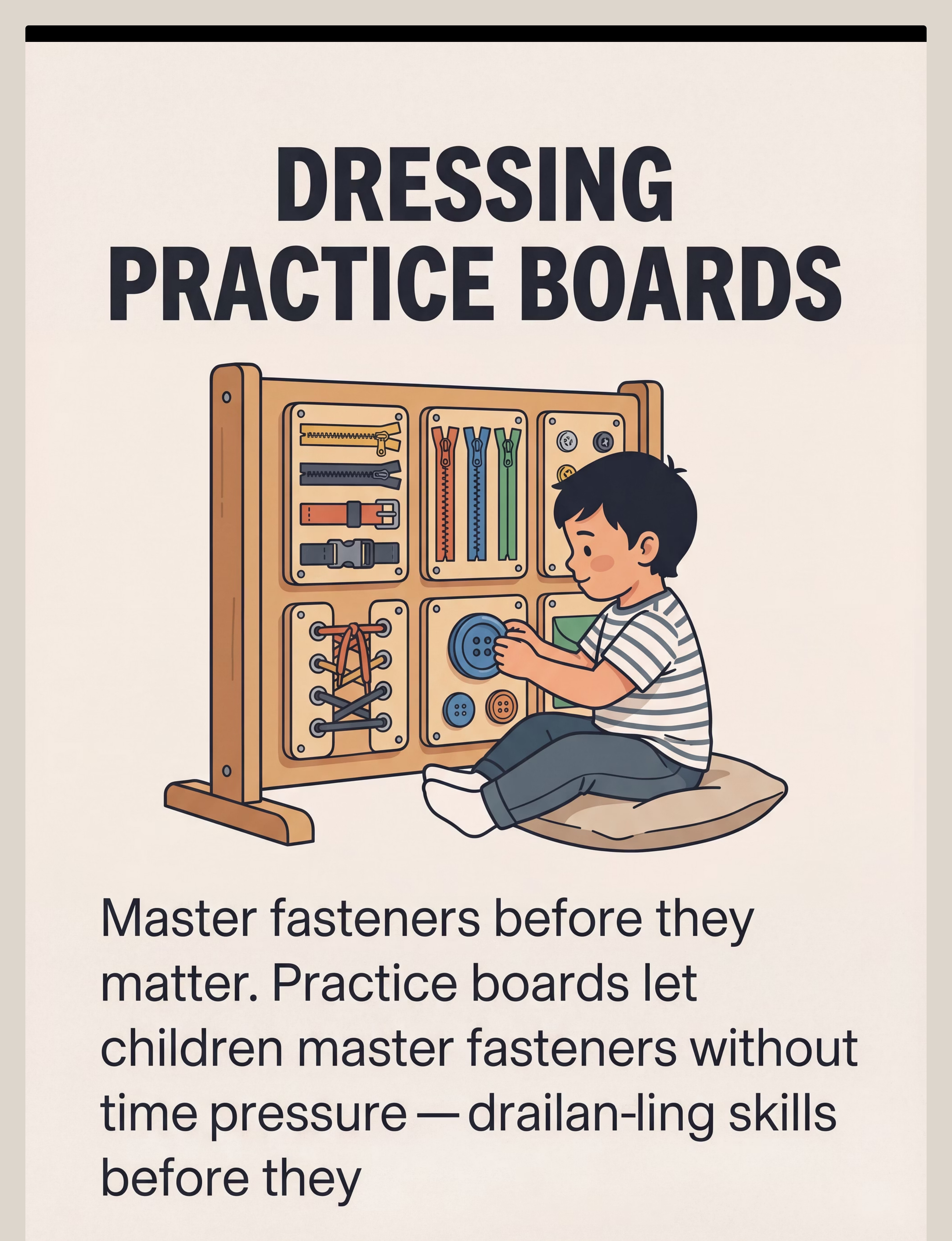
Dressing Practice Boards & Fastener Toys
The Science
Motor skill acquisition requires repetition in a low-stakes, low-pressure environment. Practicing fasteners on a board — where there is no mirror, no time pressure, no clothing resistance — builds the motor pattern that then transfers to actual clothing.
What It Is
Dressing frame/practice board with buttons, zippers, snaps, buckles, laces; dressing dolls or stuffed animals with real fasteners; busy boards; Montessori-style dressing frames.
Master fasteners before they matter
Home Procurement: ₹300–1,500
MATERIAL 8 OF 9
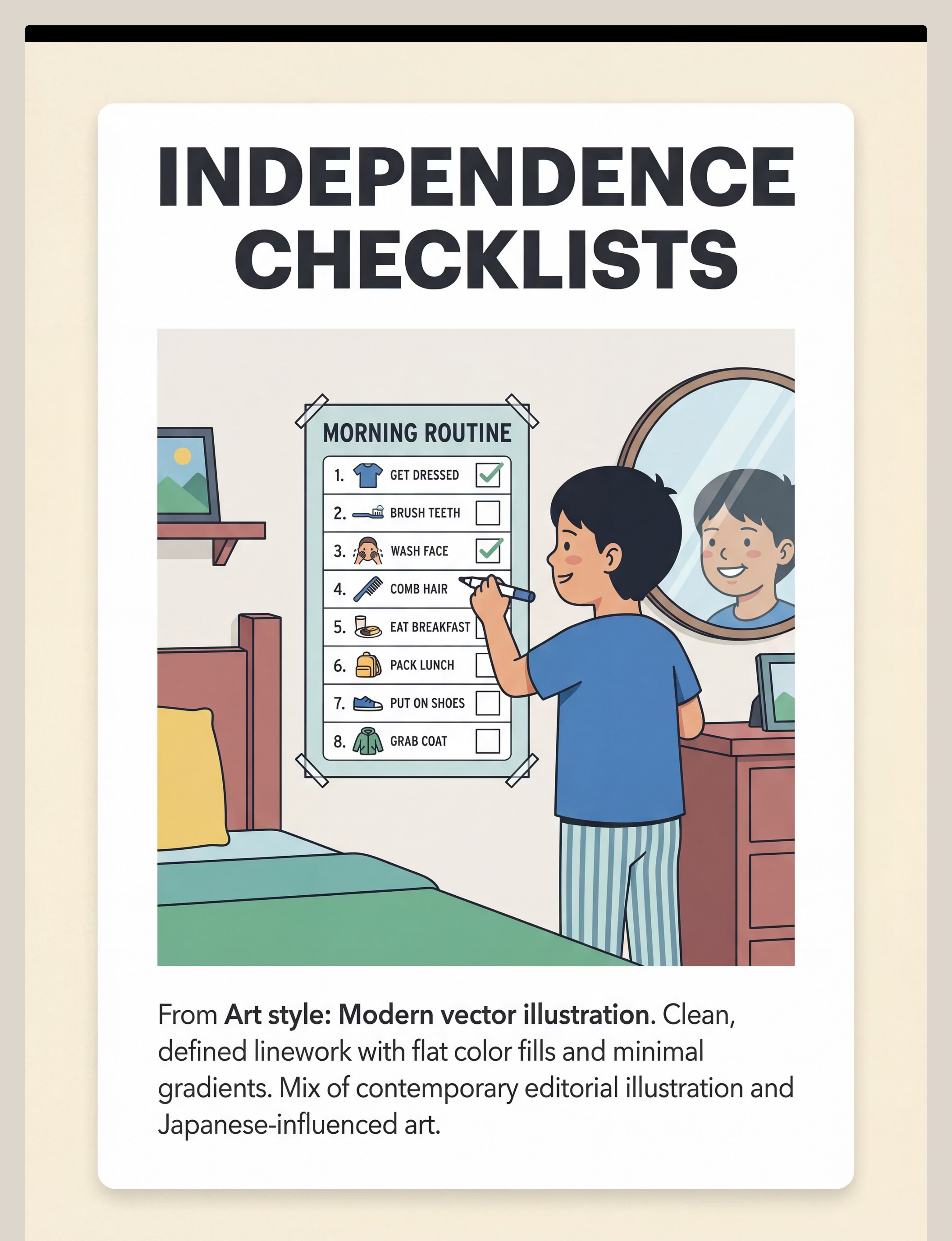
Independence Checklists & Self-Monitoring Systems
The Science
True independence requires internal guidance — metacognition. External checklists scaffold this internal monitoring, shifting locus of control from adult ("did you do it?") to child ("I checked it myself"). This is the difference between compliance and independence.
What It Is
Pictorial or written routine checklists for morning, evening, school; child-height mirror for appearance checking; 'done right' photo comparisons; self-check boxes; progress charts.
From "did you do it?" to "I checked it myself"
Home Procurement: ₹100–400 | DIY: printed checklists, laminated, dry-erase marker

MATERIAL 9 OF 9
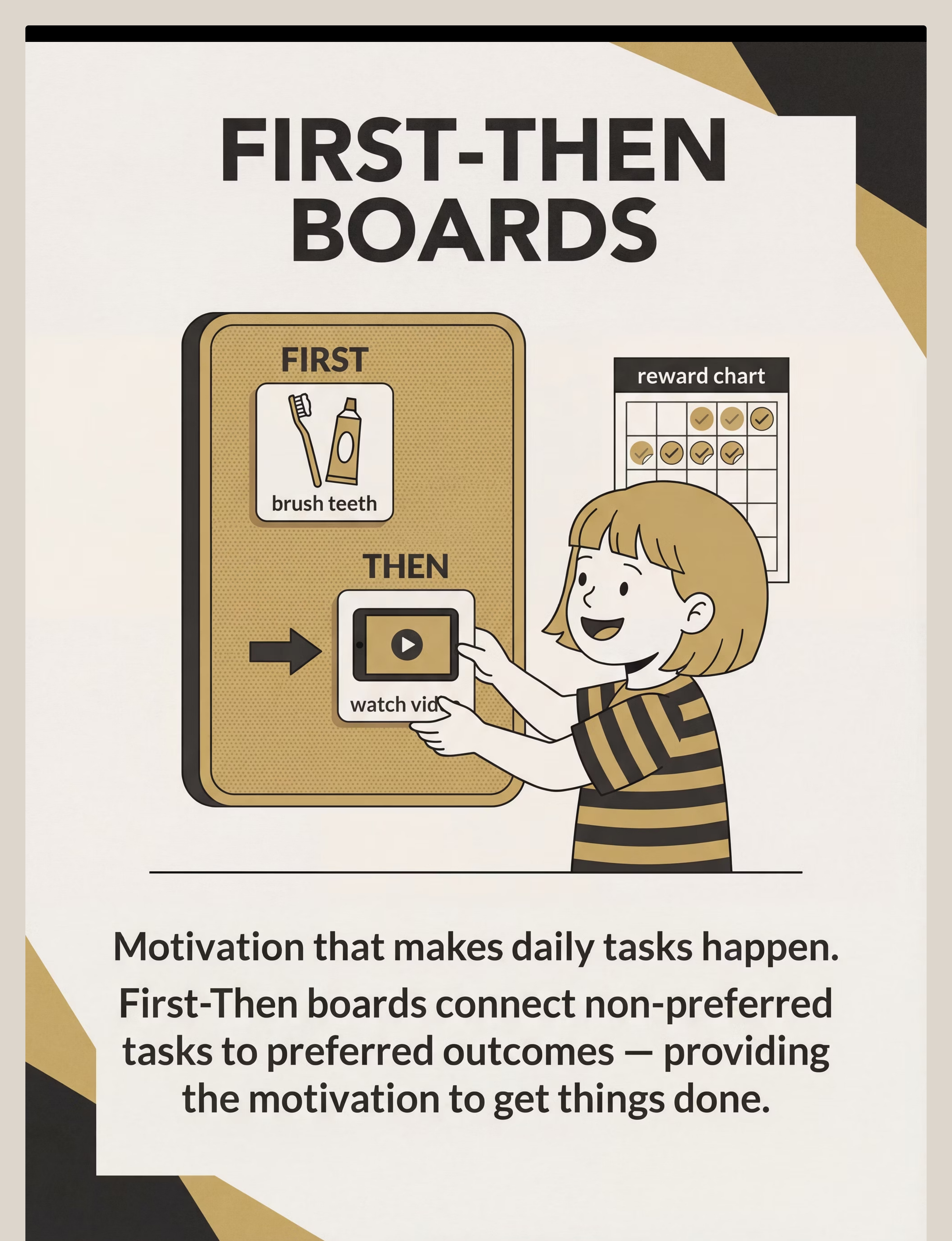
First-Then Boards & Motivational Systems
The Science
Operant conditioning principles (ABA): behavior precedes reinforcement. First-Then boards make the contingency visible, concrete, and motivating — reducing resistance to non-preferred tasks by making the preferred outcome immediately visible and predictable.
What It Is
First-Then visual board (velcro-backed picture icons), reward charts, token boards, sticker charts, identified preferred activities as 'Then' items.
Motivation that makes daily tasks happen
Home Procurement: ₹100–400
Pinnacle Recommends: Reinforcement Menu — The Rosette Imprint Reward Jar ₹589

EQUITY INCLUSION — EVERY FAMILY CAN START TODAY
DIY & Substitute Options
The principle matters more than the product. Every material on this page has a ₹0 version. Per WHO Nurturing Care Framework (2018): Effective interventions must be context-specific and equity-focused.
🛒 BUY THIS | 🏠 MAKE THIS (₹0–100) | |
Visual Task Analysis Cards ₹200–800 | Photograph your child performing each step on your phone → print → laminate with tape → post at point of use | |
Adaptive Dressing Tools ₹300–500 | Velcro under decorative buttons. Elastic shoelaces. Remove ALL clothing tags with scissors | |
Toileting Supports ₹200–500 | Drawn sticker chart on A4 paper. Sturdy stool or thick book stack. Sand timer ₹50 | |
Adapted Feeding Utensils ₹300–800 | Wrap foam pipe insulation or thick rubber band around spoon handle. Damp kitchen towel as non-slip mat | |
Oral Care Tools ₹200–400 | Ultra-soft baby toothbrush. No toothpaste initially. 2-minute kitchen timer |
"The therapeutic mechanism — task analysis, visual clarity, sensory modification, systematic reinforcement — is delivered by the principle, not the price tag."

CLINICAL SAFETY GATE — READ BEFORE EXECUTING
Safety First: Before You Begin
These materials are safe. But every child and every situation has specific considerations. Please review before beginning.
🔴 RED — ABSOLUTE STOP CONDITIONS
Child in active meltdown or severe distress. Fever or illness within 24 hours. Medication change within 48 hours. Known dysphagia requires SLP clearance before self-feeding practice. Never use punitive consequences for toileting accidents. Never leave child unattended in bath. Water temperature ≤38°C/100°F.
Child in active meltdown or severe distress. Fever or illness within 24 hours. Medication change within 48 hours. Known dysphagia requires SLP clearance before self-feeding practice. Never use punitive consequences for toileting accidents. Never leave child unattended in bath. Water temperature ≤38°C/100°F.
🟡 AMBER — MODIFY APPROACH
Child resistant today → use simpler version, shorter duration. New environment (travel) → skip practice demands. Post-illness → restart with easiest version. Ensure no small parts for children who mouth objects.
Child resistant today → use simpler version, shorter duration. New environment (travel) → skip practice demands. Post-illness → restart with easiest version. Ensure no small parts for children who mouth objects.
🟢 GREEN — PROCEED WHEN
Child is fed, rested, and in calm-alert state. Parent is regulated. Environment is set up. Materials are ready and familiar. Routine time slot is consistent.
Child is fed, rested, and in calm-alert state. Parent is regulated. Environment is set up. Materials are ready and familiar. Routine time slot is consistent.

MATERIAL-SPECIFIC SAFETY & EMERGENCY PROTOCOL
Safety notes for every material
Visual Cards
Laminate safely, round corners, no staples within child's reach
Dressing Boards
Ensure buttons, snaps and small pieces are securely attached — no loose items for children who mouth
Feeding Utensils
Always supervise. Weighted utensils are NOT substitutes for professional swallowing assessment
Oral Care
Maintain regular pediatric dental checkups. Significant dental aversion requires specialist consultation
Bathing
Non-slip surfaces mandatory. Children must never be left unattended
EMERGENCY PROTOCOL: If the child becomes severely distressed (self-injury, severe aggression, acute panic): STOP the session immediately. Remove demands. Offer transition object. Contact Pinnacle helpline 9100 181 181 for guidance.

THE THERAPEUTIC ENVIRONMENT
Set up your space
The space is the first material. Get it right and 80% of resistance dissolves before the session begins.
🚿 Bathroom
For toileting, oral care, bathing, face/hand washing. All materials at child's eye/hand level — independence requires access. Visual sequences posted where the skill happens. One visual at a time. Pre-warm bathroom if child is cold-sensitive.
🚪 Bedroom / Dressing
Clothes laid out in dressing sequence — underwear first, then pants, then shirt. Remove excess options. Mirror at child height. Checklist visible. Screen off, door closed during dressing.
🍽️ Kitchen / Dining
Feet flat on floor, hips at 90°, table at elbow height. No screens during meals. Small portions. First-Then board visible. Adapted utensil in dominant hand.

PRE-SESSION CHECKLIST
60 seconds of readiness checking saves 30 minutes of failed session management.
Fed within last 2 hours — not hungry (hunger = dysregulation)
Rested — not showing signs of fatigue or over-tiredness
No fever, illness, or pain visible
No recent meltdown in last 60 minutes
In calm-alert state — not hyper-aroused or shut-down
In familiar environment with familiar adult
Transition to this activity has been signaled (not sudden)
ALL 7 ✅ GO
Begin the full protocol as planned. Your child is ready.
4–6 🟡 MODIFY
Use simplified version. Shorter duration, single-step focus.
≤3 🔴 POSTPONE
Offer calming alternative. Try at next scheduled slot. This is not failure — this is clinical wisdom.
STEP 1 OF 6
The Invitation
Timing: 30–60 seconds | Discipline Lead: ABA + OT (Pairing & Low-Demand Entry)
Core Principle: Every ADL session begins with an invitation, not a command. The child must be paired with the activity before any demand is placed.
Therapist Scripts
Dressing: "Hey, I saw your dressing board! Want to see if you can do the big zipper today? I bet it's easier than yesterday."
Toothbrushing: "Okay, teeth time! You pick — star toothbrush or striped one? You decide."
Toileting: "Bathroom time! Let's check the picture list — you're the expert now."
Feeding: "Lunch time! You get to use your special spoon. Should we put the mat down?"
Body Language: Eye level (crouch or sit). Calm warm energy. Open side-by-side posture. A smile is the first therapeutic tool.

STEP 2 OF 6
The Engagement
Timing: 1–3 minutes | Discipline Lead: OT + SLP (Material Introduction + Language Modeling)
The child is now oriented toward the activity. This step introduces the therapeutic material and the visual support system. Parent models FIRST — "watch me" — before expecting the child to try.
Visual Task Cards
"Look — our picture list! Step 1 says... turn on the water. Can you do Step 1?" Point to EACH step as you name it.
Dressing Board
"Look at all these! Big button, small button, zipper. Which one shall we start with?" Let child choose. Choice = investment.
First-Then Board
"FIRST [task] — THEN [reward]." Show the 'Then' picture BEFORE the task. The reinforcer must be seen before the demand.
Adapted Utensils
"This is your special spoon — see how it fits in your hand like this?" Physical demonstration precedes verbal instruction.
Reinforcement Cue: The moment the child touches the material: "Yes! Perfect! You picked it up!" — immediate, specific, enthusiastic praise.

STEP 3 OF 6
The Therapeutic Action
Timing: 5–15 minutes | Discipline Lead: OT + ABA (Skill Building + Prompt Hierarchy)
This is the active therapeutic window. Use the least intrusive prompt that produces success — working from full physical guidance down toward independence.
Prompt Hierarchy (most → least support)
Full Physical (hand-over-hand)
Partial Physical (light touch)
Model (show the action)
Gesture (point to card)
Verbal ("what does step 3 say?")
Visual (card only)
Independent
STEP 3 CONTINUED — MATERIAL-SPECIFIC ACTION
Action protocols per material
Task Analysis Cards
Stand beside child at point of use. Child looks at Step 1 → executes → marks off. Prompt only if hesitation >5 seconds. Common Error: Parent tells child instead of letting child read the card. Point to the card, not to the action.
Dressing Practice
Child selects fastener. Parent models once normal speed, once slow motion. Child attempts. Common Error: Rushing through all fasteners. Master ONE fastener type per session.
Feeding Utensil
Correct positioning first. Scoop → raise → bring to mouth as three coached phases. Common Error: Praising only successful bites. Praise correct grip, correct scoop, correct raise independently.
Toileting Routine
Child enters at timer-cued time. Follows visual sequence. Parent positioned to the side, not facing — for privacy dignity. Common Error: Reminding verbally. Point to the visual card. Let the card do the prompting.
Duration Guidance
- Toothbrushing: 2 full minutes (timer essential)
- Handwashing: 30–45 seconds (visual timer or song)
- Dressing practice board: 5–10 minutes
- Feeding: entire meal, 15–25 minutes, with support as needed
- Toileting routine: full completion, no rushing
STEP 4 OF 6
Repeat & Vary
Principle: 3 good repetitions > 10 forced ones.
Therapeutic Dosage
Skill | Daily Frequency | Weekly Target | |
Handwashing | Every toileting + meals | 8–12x/day | |
Toothbrushing | Morning + evening | 14x/week | |
Dressing | Daily morning | 7x/week | |
Fastener practice | 5–10 min/day | 5x/week | |
Feeding (self) | Every meal | 21x/week | |
Toileting routine | Every trip | 4–8x/day |
Satiation Indicators: Increasing errors, slowing down, looking away repeatedly, attempting to leave. Respond: "Two more, then all done!"

STEP 5 OF 6
Reinforce & Celebrate
Timing: Within 3 seconds. Principle: Immediate. Specific. Enthusiastic.
Reinforcement delivered within 3 seconds of the target behavior is 4x more effective than delayed reinforcement. The child's brain is wiring connections — the praise must arrive while the wire is live.
Tier 3 — Tangible/Preferred
Sticker on potty chart, reward jar item, token board exchange. For children who need concrete motivation.
Tier 2 — Specific Verbal Praise
"You did Step 7 yourself — I didn't help at all!" Avoid generic "good job." Name what they did right.
Tier 1 — Natural Consequences
"You got dressed yourself — we can go outside RIGHT NOW!" Most powerful for generalization.
What to Celebrate (not just completion)
- Attempting a step for the first time
- Doing one step without a prompt
- Tolerating a previously aversive material for one additional second
- Staying at the task despite frustration
- Using the visual card independently
STEP 6 OF 6
The Cool-Down
Timing: 1–2 minutes | Principle: No session ends abruptly.
Abrupt endings cause post-session dysregulation. A predictable cool-down sequence prevents the "session hangover" — the meltdown that follows when a structured activity stops without warning.
Transition Warning Language
"Two more steps, then we're all done!" · "One more, then we put the materials away." · "Last one — then [preferred activity]!"
Sensory Cool-Down Options: Proprioceptive input (joint compression, heavy lifting). Vestibular (brief swing or rocking). Tactile comfort (preferred texture, weighted blanket for 2 minutes).
60-SECOND DATA CAPTURE
Capture the data: right now
60 seconds of data now = weeks of clarity later. Don't wait until tonight.
Record 3 Fields Only
- Completion level (independent → refused)
- Key observation (1 sentence)
- Caregiver rating (😰😐😊🌟)
Patterns That Emerge in 4 Weeks
- Which steps are consistently stuck
- Which skills are plateauing
- Which environments produce better performance
- How prompt levels change over time
CLINICAL TROUBLESHOOTING
What if it didn't go as planned?
Session abandonment is not failure. It's data. Here's what it means and what to do next.
Q1: "My child refused to touch the material at all today."
Today's sensory/regulatory state is incompatible with this demand level. Not a regression. Next time: Pre-session sensory diet (5 min heavy work). Highest-value 'Then' item. Single easiest step only.
Today's sensory/regulatory state is incompatible with this demand level. Not a regression. Next time: Pre-session sensory diet (5 min heavy work). Highest-value 'Then' item. Single easiest step only.
Q2: "We got through 3 steps, then complete meltdown."
Fatigue or satiation hit mid-sequence. The session was one step too long. Next time: End at Step 2. Build back up one step at a time over the week.
Fatigue or satiation hit mid-sequence. The session was one step too long. Next time: End at Step 2. Build back up one step at a time over the week.
Q3: "My child does it perfectly with me but refuses with grandparents/teachers."
The skill is learned in one context but not generalized. This is common and expected. Next time: Deliberately practice with different caregivers using the SAME materials and language.
The skill is learned in one context but not generalized. This is common and expected. Next time: Deliberately practice with different caregivers using the SAME materials and language.
CLINICAL TROUBLESHOOTING — CONTINUED
More common failure modes
Q4: "The visual task analysis cards aren't working — child ignores them."
The child hasn't been taught to USE the cards. Posting them is not enough. Next time: Explicitly teach card use — "Before each step, touch the picture, then do it." Start with just 2 pictures. Reward card-referencing behavior specifically.
The child hasn't been taught to USE the cards. Posting them is not enough. Next time: Explicitly teach card use — "Before each step, touch the picture, then do it." Start with just 2 pictures. Reward card-referencing behavior specifically.
Q5: "My child won't do it independently — always waits for me to start."
Prompt dependency. The adult has been initiating every step. Next time: Time-delay strategy — stand near the material, say nothing for 5 seconds. If no initiation, point to Step 1 but say nothing. Gradually increase delay. Reinforce heavily for any self-initiation.
Prompt dependency. The adult has been initiating every step. Next time: Time-delay strategy — stand near the material, say nothing for 5 seconds. If no initiation, point to Step 1 but say nothing. Gradually increase delay. Reinforce heavily for any self-initiation.
Q6: "6 weeks of tooth brushing and no progress."
Likely: wrong starting point (sensitivity needs more desensitization first), wrong toothbrush type, or inconsistent practice. Next time: Return to oral desensitization — finger in mouth → finger with cloth → soft finger brush → standard brush. Longer runway than expected. Consult Pinnacle OT at 9100 181 181.
Likely: wrong starting point (sensitivity needs more desensitization first), wrong toothbrush type, or inconsistent practice. Next time: Return to oral desensitization — finger in mouth → finger with cloth → soft finger brush → standard brush. Longer runway than expected. Consult Pinnacle OT at 9100 181 181.
YOUR CHILD'S PROFILE → YOUR PERSONALIZED VERSION
Adapt & Personalize
No two children are identical. No two ADL programs should be.
⬇️ Easier Modifications
- Single step only, not full sequence
- Hand-over-hand throughout
- Extra-long 'First' preview, extra-large 'Then' reward
- Verbal + physical prompts at every step
- Maximum 3 minutes duration
- Most preferred environment
⬆️ Harder Modifications
- 2 full routines in a row
- Remove one visual card — child must remember
- Timer challenge: "Beat your record!"
- New environment (grandmother's, school)
- New adult (generalization)
- Child teaches YOU (metacognition)
SENSORY & AGE-BASED VARIATIONS
Individualization Matrix
Sensory Avoider (Hypersensitive) | Sensory Seeker (Hyposensitive) | |
Softer fabrics, tagless always | Can tolerate more texture variation | |
Ultra-soft toothbrush, unflavored paste | May respond to vibrating toothbrush | |
Fragrance-free everything | Light scents can be motivating | |
More time between steps | Can move faster through sequences | |
Fewer steps per session | Can practice longer sequences |
PROGRESS ARC — PHASE 1
Week 1–2: What to Expect
Look for tolerance — not mastery.
These are the signals that tell you the neurological change is beginning. Progress: 15%
✓ Observable Indicators
- Reduced protest — less screaming at the start of routine
- Increased duration — tolerates toothbrushing 20s vs. 5s
- Material acceptance — allows adapted spoon without throwing
- Visual card glancing — begins to look at cards
- Reduced physical resistance — dressing takes 10 min not 20
⏸ Not Yet Expected
- Independent completion without prompts
- Skill performance in new setting
- Requesting to do the routine themselves
- Completing more than 3 steps independently
"Your child's resistance is not about the task — it's about unfamiliarity. By week 2, the routine itself becomes a form of familiarity. Resistance reduction IS progress."
Preview of 9 materials that help with daily living skills Therapy Material
Below is a visual preview of 9 materials that help with daily living skills therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

PROGRESS ARC — PHASE 2
Week 3–4: Consolidation Signs
The child begins to anticipate.
The neural pathways are forming. Watch for these signals. Progress: 40%
Anticipation Behavior
Child moves toward the bathroom/dressing area without being prompted at the usual time
Reduced Prompt Level
What needed physical guidance now responds to gesture; what needed gesture now responds to verbal
Self-Correction
Child notices they skipped a step and goes back to it
Ownership Language
"My toothbrush," "my steps," "my chart" — possessive language signals investment
Spontaneous Reference
Child points to visual card without being directed to
First-Then Internalization
Child begins saying "first teeth, THEN tablet" on their own