"You are among millions of families navigating this exact challenge. The isolation you feel is not because this is rare — it is because it is under-named."
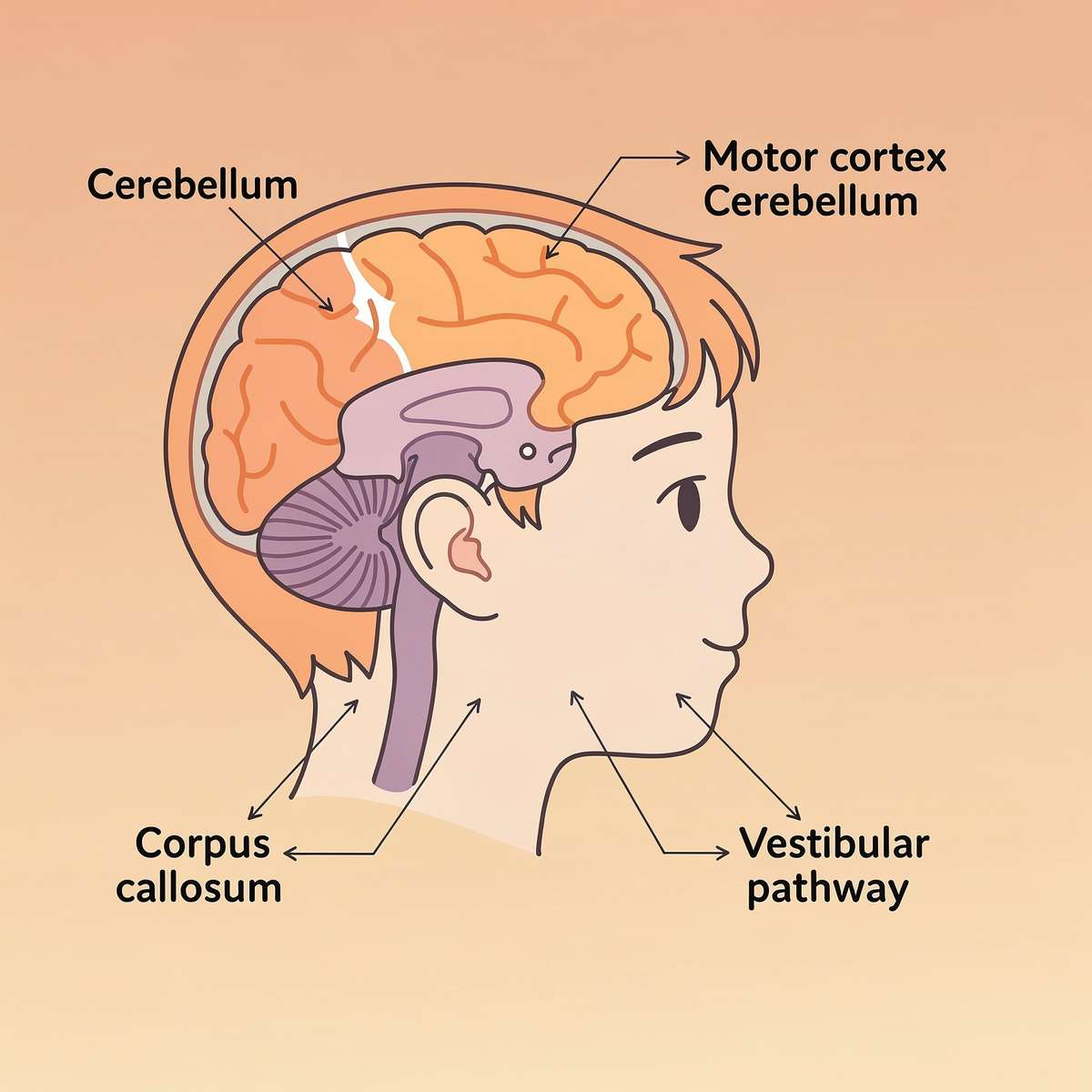
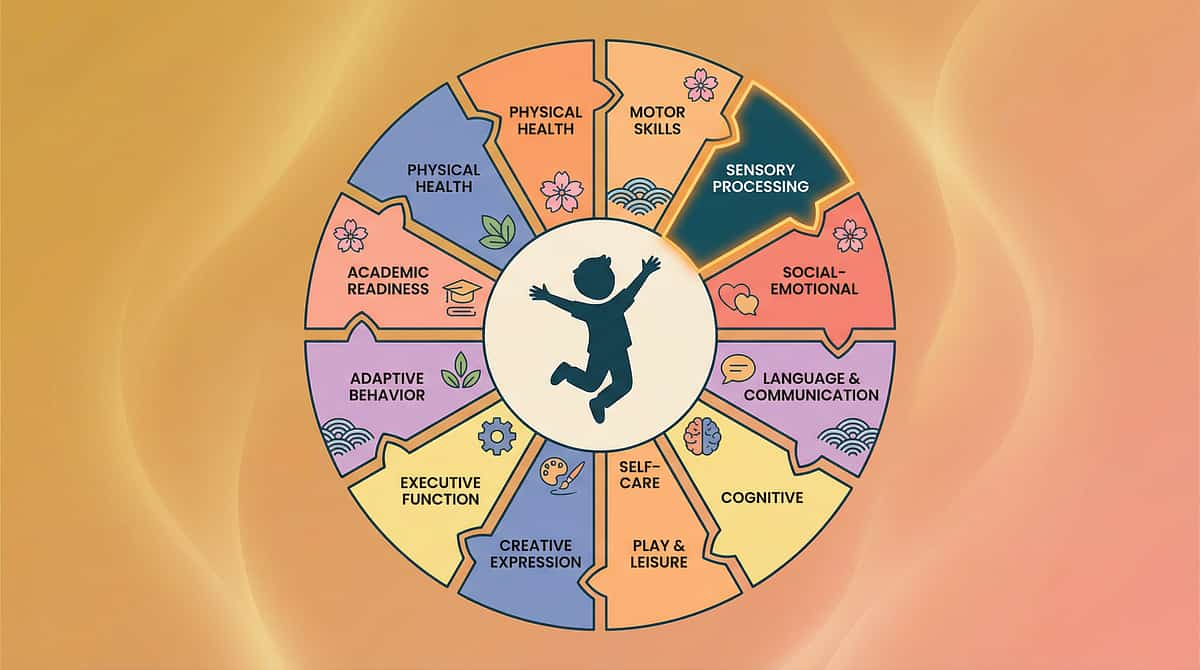
"This is a wiring difference in how motor signals are processed and coordinated. It is not laziness. It is not lack of trying. It is neurology."


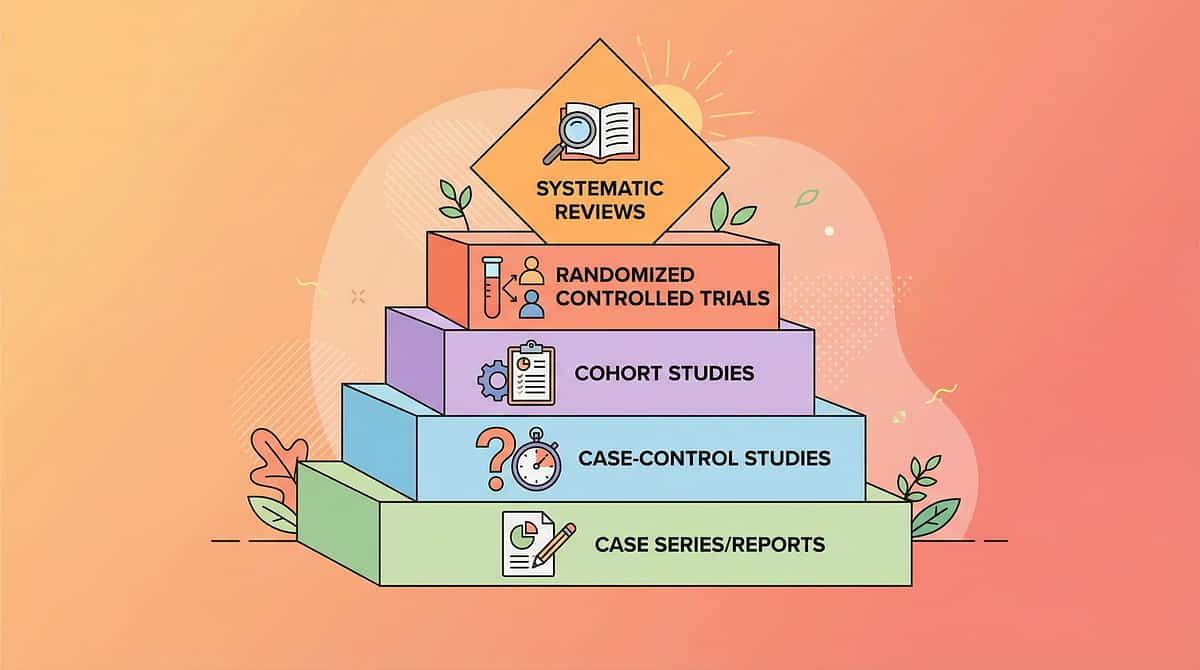
Study | Finding | Source | |
PRISMA Systematic Review (2024) | 16 studies confirm sensory-motor intervention meets evidence-based practice criteria for children with ASD | ||
World J Clin Cases Meta-Analysis (2024) | Sensory integration therapy significantly improved gross motor, fine motor, and coordination outcomes across 24 studies | ||
WHO Care for Child Development | Home-based motor interventions with structured caregiver guidance show significant outcomes across 54 LMICs | ||
Indian RCT — Indian J Pediatr (2019) | Home-based motor interventions demonstrated significant, measurable outcomes in Indian pediatric populations | ||
NCAEP Evidence-Based Practices (2020) | Motor-based and sensory-based interventions classified as evidence-based practice for ASD |
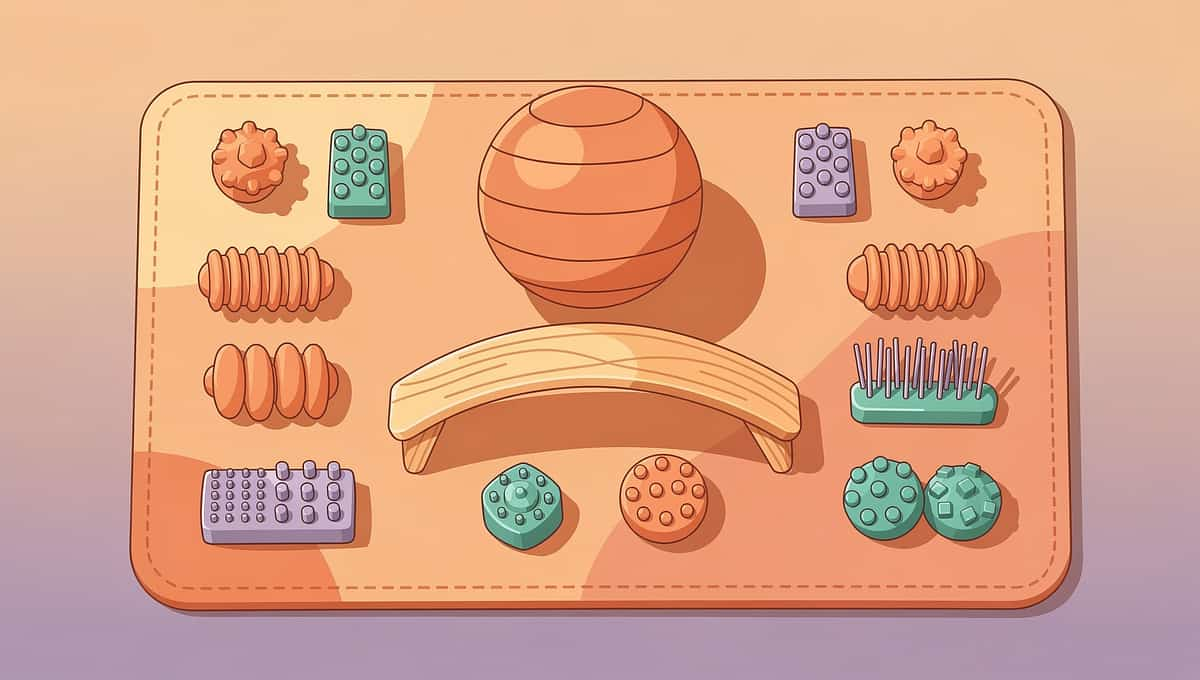
"The 9 materials on this page are drawn from occupational therapy evidence, motor learning research, and Pinnacle's 21 million therapy sessions. Every material has a mechanism. Every mechanism has a citation."



- Handwriting quality and speed
- Ball skills (catching, throwing, kicking)
- Scissor use
- Bicycle riding
- Stair navigation
- Playground participation
- Physical activity participation and fitness
- Self-esteem and body confidence
- Peer social participation
- School-based academic performance
- Independence in daily living skills
- Longer sitting balance on unstable surface
- Successful catching at progressive distances
- Both hands working in complementary roles
- Rhythmic movement maintaining a beat










Material | Zero-Cost Version | Why It Works | |
Therapy Ball | Firm sofa cushion or folded blanket on the floor — child sits and maintains balance | Same principle: unstable surface requiring postural adjustment | |
Balance Board | A thick hardcover book under a wooden cutting board — stand and balance | Same vestibular and proprioceptive challenge at low intensity | |
Beanbags | Old socks filled with rice or beans, tied at the top | Identical slow flight, easy grip, doesn't roll away | |
Bilateral Toys | Old shoelace through cardboard with holes punched | Same bilateral hand-role differentiation (hold vs. thread) | |
Scooter Board | Folded blanket on smooth floor — child lies on stomach and pushes | Same prone proprioceptive input and arm-propulsion bilateral coordination | |
Jump Rope | A shoelace, long ribbon, or any rope-like household item | Identical timing and rhythm challenge | |
Target Games | Tape a circle on the wall; throw rolled socks at it | Same visual-motor calibration loop (aim → throw → feedback) | |
Obstacle Course | Pillows (step over), blanket fort (crawl through), taped line on floor (balance walk) | Same motor planning demands with novel sequences | |
Rhythm Tools | Two wooden spoons as drumsticks on any container | Same timing and bilateral rhythm coordination |
- Child is sick, running a fever, or has ear infection (vestibular activities contraindicated during ear infection)
- Child has had a meltdown or significant emotional dysregulation in the past 30 minutes
- Child has expressed pain in joints, back, or limbs — consult your PT before balance activities
- Latex allergy present — confirm therapy ball is latex-free
- Therapy ball is not properly inflated — risk of sudden deflation
- Child is in a state of severe sensory overload (e.g., covering ears, self-injurious behavior)
- Child has an unhealed injury affecting weight-bearing
- Child is tired but not ill — shorten session to 10 minutes, reduce challenge level
- Child is hungry — always conduct sessions 30–45 minutes after a meal
- Child skipped sleep — skip balance board, focus on beanbags (lower vestibular demand)
- Child is in a new environment — allow 5 minutes of free exploration before starting
- It's the first week — all activities at lowest difficulty, success guaranteed
- Child is fed, rested, regulated, and in their alert "learning window"
- Environment is set up (see Card 12) and hazards removed
- You have 15–30 minutes of uninterrupted time
- Non-slip surface is confirmed under balance activities
- An adult is present throughout (NEVER leave child unattended on balance equipment)

"The space IS the therapy. A chaotic environment produces a chaotic session. A calm, prepared space tells the child's nervous system: 'It is safe to learn here.'"

Indicator | 🟢 GO | 🟡 MODIFY | 🔴 POSTPONE | |
Body state | Alert, moving around comfortably | Subdued but cooperative | Crying, rigid, or overwhelmed | |
Eye contact / Responsiveness | Responding to name, looking around with interest | Responding slowly | No response to name, glazed expression | |
Eating status | Had a meal 30–45 min ago | Ate lightly 1+ hour ago | Hungry OR just finished eating | |
Sleep | Slept well previous night | Mild tiredness | Overtired / didn't sleep | |
Recent events | Calm past 2 hours | Minor frustration earlier | Meltdown within last hour | |
Physical comfort | Moving without favoring any limb | Slightly stiff | Limping or guarding an area |

"Hey, I have something fun for you. Want to see if you can sit on this ball without falling off? I'll hold it for you at first."
- "Want to" — child-directed, no coercion
- "I'll hold it at first" — reduces fear of failure
- Framed as fun/game — not therapy, not work
- Short and specific — easy for child with language differences to process
- Get to child's level — kneel or sit, not standing over them
- Hold the material first — show it, explore it, let them touch before doing
- Relaxed posture — your anxiety becomes their anxiety
- Face toward the child — not toward the material
- Turns away → "It's okay, you can just watch me do it first."
- Verbal protest → "We'll only do it for 1 minute, then you choose what we do."
- Physical avoidance → Reduce demand: put the material on the floor and simply sit nearby


- Child sits on therapy ball, feet flat on floor, hips/knees at 90°
- Begin with hands on ball for support. Parent holds ball steady.
- Week 1: Hold for 10 seconds without hands on ball
- Week 2: Gentle bouncing with parent holding both hands
- Week 3: Reaching for objects while sitting (breaking up balance compensation)
- Week 4+: Throwing/catching beanbags WHILE sitting on ball
- Beginner: Stand on rocker board, hands touching wall. Goal: 30 seconds continuous
- Intermediate: No wall support. Eyes open. Rock side to side gently.
- Advanced: Stand while catching/throwing beanbag OR counting backward from 10
- Expert: Eyes closed for 10-second intervals (removes visual compensation)
- Drop beanbag from one hand, catch with both hands (30 cm height)
- Toss up 50cm, catch with both hands
- Toss right hand → catch both hands
- Toss left hand → catch both hands
- Toss right → catch left (crossing midline — KEY bilateral milestone)
- Partner toss at 1m distance, two-hand catch

- Lacing cards: one hand holds the card, other hand threads. Rotate which hand does which.
- Pop tubes: two hands push and pull simultaneously
- Beading: one hand holds the string, other hand threads the bead
- Child lies on stomach (prone) on scooter board
- Propel forward using hands only — arms alternate or push simultaneously
- Navigate straight line → gentle curve → obstacle course
- Advanced: Carry a ball or small stuffed animal while scooting (adds upper limb challenge)
- Jumping in place (no rope) with rhythm — 20 consecutive jumps
- Turn rope at sides while standing still — build the wrist turning motion
- Jump over rope lying on the ground
- Jump over rope swung slowly by two adults at ankle height
- Jump over rope swung at knee height
- Hold handles, step over rope one at a time
- One jump + one turn of the rope
- Ring toss: Begin 30cm from target. Success = move back 15cm. 3 misses = move forward.
- Velcro darts: Begin 50cm. Progress same way.
- Bowling: 1 meter distance. Progress by 0.5m for every 3 successful knocks.
- Course A (Beginner): Cone weave (3 cones) → step over pool noodle → walk balance beam
- Course B (Intermediate): Add tunnel crawl → jump into 3 hula hoops → carry a beanbag throughout
- Course C (Advanced): Timed course + carry an object + 5 exercises at end
- Drum: Play at 60 BPM (one beat per second). Child matches. Build to 80 BPM.
- Ribbon sticks: Move in circles, figure-eights, up-down to music with clear beat
- Parachute (group): Lift together on "1", lower on "2" — count aloud

Material | Target Reps/Session | Variation Strategy | |
Therapy Ball | 3–5 minutes continuous | Change arm positions, add reaching tasks, try eyes closed | |
Balance Board | 3 sets of 30–60 seconds | Change surface under board, add cognitive dual-task | |
Beanbags | 20–30 tosses per stage | Change size, color, toss height, distance | |
Bilateral Toys | 5–10 minutes continuous | Change material (lacing → pop tube → beading) | |
Scooter Board | 5–8 runs per course | Change course layout, add obstacles, change speed | |
Jump Rope | 10 attempts per stage | Change rope weight, change timing cues | |
Target Games | 20–30 throws | Change target size, target distance, throwing arm | |
Obstacle Course | 3–5 complete runs | New course layout each week | |
Rhythm Tools | 5–8 minutes | Change tempo, change instrument, add movement |
"The brain builds motor skills through variable practice — not just repetition of the exact same action. Vary the angle, the distance, the speed, the size. The brain learns the principle of the movement, not just one version of it."

Type | Examples | |
Social | High-five, thumbs up, hug, "WOW" face | |
Verbal | Specific praise ("You balanced for 30 seconds!"), not generic ("Good job") | |
Token | Sticker chart: 5 stickers = small preferred activity. Sticker Reward Charts ₹364 | Reward Token Set ₹589 | |
Activity | 5 minutes of preferred play after 15 minutes of coordination practice | |
Natural | "You caught it! Now try to throw it back to me." (activity continues as reward) |

- Wall push-ups (5–10 reps) — deep proprioceptive input, organizing
- Log roll on carpet (child rolls slowly from one side of mat to other)
- Bear hug from parent — deep pressure, co-regulation
- Heavy work — carry the therapy ball back to its spot, stack the materials
- Therapy ball: encourage bouncing and larger movements
- Balance board: move to more challenging surfaces faster
- Scooter board: increase speed, add gentle bumps to floor
- Rhythm tools: louder music, faster tempo, more vigorous movement
- These children will love coordination activities — channel the energy
- Begin ALL balance activities with two-point support (both hands touching a surface)
- Build tolerance gradually — 5 seconds before 30 seconds
- Warm up with firm proprioceptive input BEFORE vestibular activities
- Use calming rather than energizing music for rhythm activities
- Never force or rush — trust-building precedes challenge
3–5 years | Shorter sessions (10–15 min), more parent play partner, simpler obstacle courses | |
6–8 years | Standard protocol as written, peer partner activities where possible | |
9–12 years | Can understand "why" — explain the brain science (Card 03), goal-setting, self-monitoring |

"If your child tolerates the therapy ball for 8 seconds this week vs. 5 seconds last week — that IS real, measurable progress. The brain is forming new motor pathways. They are invisible on the outside. They are happening on the inside."

- Child is completing sessions without fatigue and asking for more → add 5 minutes
- Child is succeeding 9/10 times on current challenge → increase difficulty
- Child is generalizing skills to daily life → introduce next material category

Material | Mastery Indicator | |
Therapy Ball | 60 seconds sitting balance without hands, while catching beanbags | |
Balance Board | 60 seconds no support, eyes closed for 10-second intervals | |
Beanbags | Catches 8/10 at 2-meter partner toss with one hand | |
Bilateral Toys | Completes lacing independently, uses scissors correctly for cutting straight lines | |
Scooter Board | Navigates 5-obstacle course in under 60 seconds | |
Jump Rope | 10 consecutive jumps with self-turned rope | |
Target Games | Hits target at 2 meters, 7/10 attempts | |
Obstacle Course | Completes 8-obstacle course from memory (without being shown each time) | |
Rhythm Tools | Maintains beat at 80 BPM for 2 minutes continuously |
You committed to 5–8 weeks of consistent motor coordination practice with your child. You showed up on the days they refused. You modified when things didn't work. You celebrated 3-second improvements when the world tells parents to expect dramatic transformations. Your child's brain has built new neural pathways because of your consistency.
"I kept trying. And something got easier." — Every child who completes 8 weeks of coordination therapy


"This technique is one piece of a larger plan. GPT-OS® sees the whole child — and this is one precise intervention in a personalized developmental architecture."
"He crossed the finish line and looked at me like he had just climbed Everest. And for him — he had."
"We were told for years that she was being careless. She was 8 years old and crying that her hands didn't work right. That's not careless. That's a child with DCD who needed someone to see the wiring, not judge the output."

"You have data, observations, and lived experience that no clinical study can replicate. Consider sharing your child's journey — anonymously or openly. Your story is the evidence that moves another parent to start."

Your Need | Who to See at Pinnacle | |
Overall coordination assessment | Occupational Therapist + Physical Therapist | |
Balance and vestibular concerns | PT + Sensory Integration OT | |
Handwriting and fine motor | OT with VMI specialization | |
DCD/dyspraxia diagnosis | NeuroDev Pediatrician + OT | |
Behavior/engagement with therapy | BCBA + OT combination |

From Your Living Room to the Intelligence Layer
What GPT-OS® Learns from F-571 Data Which of the 9 materials produces the fastest coordination progress for different child profiles Which material combination is most effective for sensory-seeking vs. sensory-avoiding profiles At what session number most children break through to each skill milestone What parent behaviors correlate with best outcomes 🛡️ Privacy Assurance Child data is anonymized before entering aggregate models Your family's specific data is never shared without consent GPT-OS® is governed by India's DPDP Act and Pinnacle's data ethics framework "Your data helps every child like yours. 1,000 families tracking F-571 makes the AI a better therapist for the 1,001st family."

- 📖 Text + science → This page
- 🎬 Visual demonstration → The reel
- 👐 Hands-on practice → Cards 13–22 protocol
- 📊 Progress tracking → Card 20 tracker
- 📥 F-571 Family Guide — 1-Page PDF: The protocol simplified to one page. For grandparents, aunties, and anyone who looks after your child. Contents: 9 materials overview | 5-minute session guide | What to say and what not to say | When to call 9100 181 181
- 📥 Teacher Communication Template: Ready-to-send email to your child's PE teacher or class teacher. "Dear [Teacher], our child is working with a Pinnacle OT on motor coordination. Here are 3 things that help in the classroom..."
"Your grandchild is not clumsy on purpose. Their brain is learning to coordinate their body parts. We are practicing with special toys and activities. The most helpful thing you can do is: (1) Be patient when they drop things. (2) Let them try — don't rush to help. (3) Say 'Good try!' when they attempt something hard."
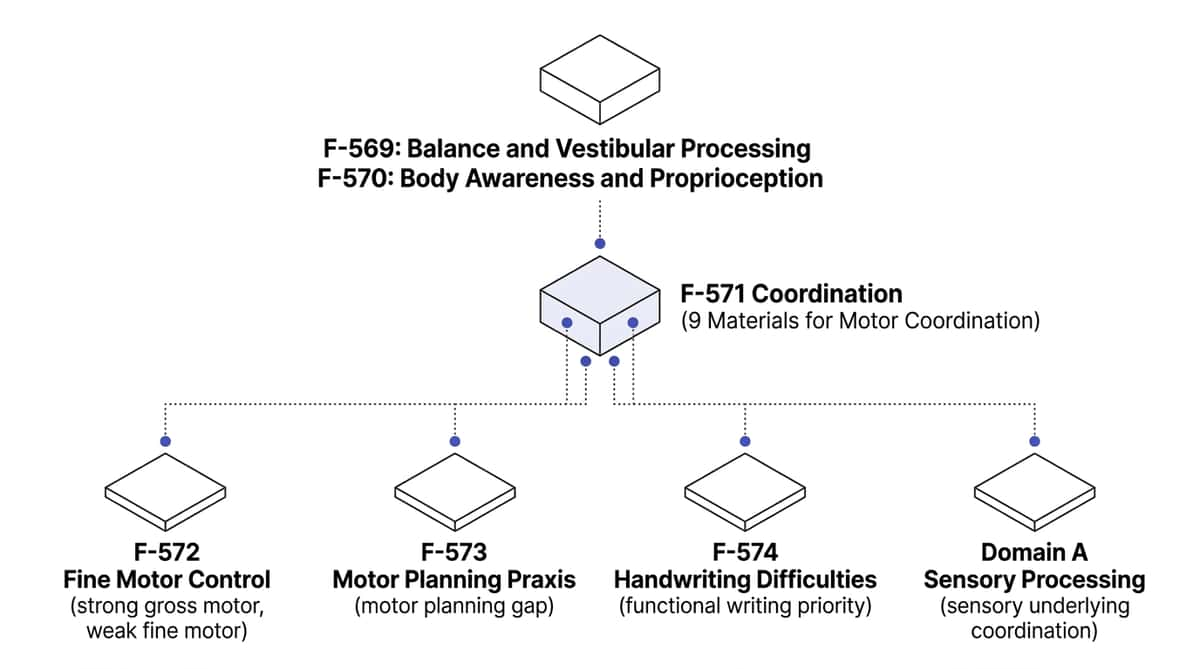
Preview of 9 materials that help with coordination Therapy Material
Below is a visual preview of 9 materials that help with coordination therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















