
9 Materials That Help With Constant Screaming
When the only volume is maximum — and every emotion comes out as a scream
"My child screams constantly. Happy? Scream. Frustrated? Scream. Bored? Scream. We can't go to stores. Family gatherings are dreaded. I've tried everything. Nothing works — and I've realised it's because screaming is the only tool my child has right now." — Parent voice, Pinnacle Network
🧒 Age: 1–10 yrs
🏥 SLP • OT • ABA • BCBA
🌍 Home + Community
⏱ 15–20 min/session
Powered by GPT-OS® | 20M+ sessions | 97%+ improvement | 70+ centres

The Recognition Moment
ACT I — RECOGNITION
It's 7am. Your child woke up screaming — not from a nightmare, just because they woke up. By breakfast, every request, every transition, every moment of excitement or frustration has come out at full volume. You haven't heard quiet in weeks.
You are not failing. Your child's vocal system is communicating the only way it currently knows how. Constant screaming in children with developmental differences is not defiance — it is a nervous system doing its best with the tools it currently has.
This protocol — D-423: Constant Screaming — Multi-Modal Reduction via Communication Replacement, Sensory Regulation, and Environmental Modification — provides 9 categories of materials that address the root cause of screaming, not just the symptom.
🏥 Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics

You Are Not Alone: The Numbers
You are among millions of families who have looked at their child and wondered: why does everything come out as a scream? The answer exists. And so does the path forward.
80%+
Vocal Challenges
Children with ASD show vocal or sensory processing challenges
1 in 36
ASD Diagnosis
Children diagnosed with ASD globally (CDC 2023)
60–80%
Communication Difficulty
Children with ASD show functional communication challenges
In India alone, approximately 1.8 crore children are on the autism spectrum. Constant screaming affects families across every language, culture, and economic context. The science is clear, the path forward is mapped, and you do not have to walk it alone.
FREE National Autism Helpline: 📞 9100 181 181 | 16+ languages | 24×7 | No consultation fee
Research: PMC11506176 | PMC10955541 | WHO NCF 2018

The Neuroscience — In Plain English
When language circuits are delayed or different, the brain uses its loudest available output — the voice — for everything. Screaming is not defiance. It is a nervous system doing its best.
Screaming provides:
- Intense auditory feedback — the brain hears itself
- Proprioceptive vibration through throat, chest, and jaw
- Emotional discharge — releases fight-or-flight pressure
- Communication — when no other tool is available
What's Happening in Your Child's Brain
The brain regions most implicated include Broca's area (language production), the amygdala (emotional regulation hub), the auditory cortex (sound processing), the vagus nerve (vocal-body connection), and sensory integration pathways.
The auditory feedback loop in vocal stereotypy activates the same reward circuits as other sensory-seeking behaviours. Screaming is self-reinforcing — which means suppression alone never works. Replacement does.
— Frontiers in Integrative Neuroscience (2020), DOI: 10.3389/fnint.2020.556660

Your Child's Vocal Development Journey
Understanding where your child sits on the developmental map is the first step to knowing where you are heading. Most families navigating constant screaming arrive at a specific zone on this continuum — and the path forward is well-mapped from here.
1
Birth–18 Months
Cry only → Babble → Proto-words. Vocalisation serves basic needs.
2
★ Most Families Arrive Here
Screaming as primary communication. Vocal intensity HIGH, communication tools LIMITED.
3
Words & Phrases
Intentional words emerge. Communication repertoire expands beyond volume.
4
Volume Modulation
Target: Screaming is one of many tools, not the only one. Context-appropriate volume across settings.
Constant screaming commonly co-occurs with Autism Spectrum Disorder, Developmental Language Disorder, Sensory Processing Differences, Anxiety or Emotional Dysregulation, and hearing differences — always rule out hearing differences first.
References: PMC9978394 | WHO/UNICEF CCD Package (2023)

The Evidence Behind This Approach
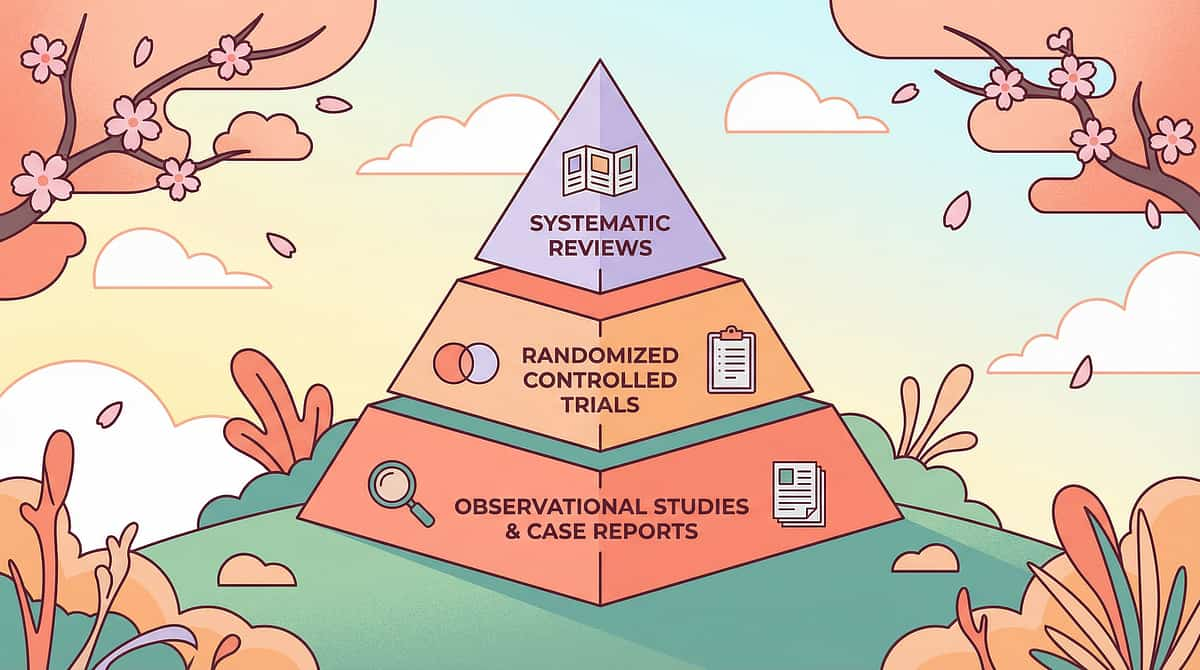
⬡ LEVEL I EVIDENCE
Systematic Review + RCT + Clinical Consensus
1
PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm FCT + AAC + sensory integration as evidence-based practice for vocal behaviors in ASD.
PMC11506176
2
NCAEP Evidence-Based Practices (2020)
FCT, AAC, Visual Supports, and Sensory Integration all classified as Evidence-Based Practices for autism.
NCAEP 2020 Report
3
Padmanabha et al. (2019)
Home-based interventions demonstrate significant outcomes in Indian pediatric populations.
DOI: 10.1007/s12098-018-2747-4
Evidence Confidence: STRONG (9/10) — drawn from PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | WHO NCF 2018. The science is clear. These 9 materials work. Now let's learn exactly what they are and how to use them at home.

The Technique: What It Is
D-423 | SCREAM-REG
Domain D: Behaviour & Flexibility
Formal name: "Constant Screaming — Multi-Modal Reduction via Communication Replacement, Sensory Regulation, and Environmental Modification." Parent-friendly alias: The Screaming Solutions Protocol.
Constant screaming in children with developmental differences is not a behaviour problem — it is a communication and regulation problem. This protocol addresses the root cause, not just the symptom.
The core principle: identify why the screaming is happening — communication? sensory input? emotion regulation? volume deficit? — and provide materials that meet that need more effectively than screaming does.
🧒 Age Range
1–10 years
⏱ Sessions
15–20 minutes, daily, embedded in routine
🏠 Settings
Home • School • Community
🔁 Duration
8–12 weeks for baseline shift

Who Uses This Technique
A consortium approach — because screaming crosses all therapy boundaries. The brain doesn't organise by therapy type. Screaming crosses language, sensory, behavioural, and emotional domains simultaneously. That's why the Pinnacle consortium addresses it simultaneously.
SLP — Speech-Language Pathologist
Leads AAC design, FCT communication training, and volume modulation therapy.
ABA / BCBA
Leads functional behaviour assessment, replacement behaviour teaching, and data collection.
OT — Occupational Therapist
Leads sensory diet design, proprioceptive input, and oral motor tools.
SpEd — Special Education
Leads visual schedules and emotion regulation in the classroom context.
NeuroDev Pediatrics
Leads medical differential diagnosis and medication review when indicated.
Family Coach / Parent
Leads home implementation and consistency across all settings — the most critical role.
📞9100 181 181 — FREE consultation in 16+ languages

What This Technique Targets
Precision targets — each material is mapped to a specific measurable outcome. Understanding what you are changing helps you track whether it's working.
1
Primary Observable Indicator
Count how many times the child screams in a 1-hour window — this is your baseline. Write it down on Day 1.
2
Secondary Observable Indicator
Notice if the child uses ANY alternative: gesture, card, device, or word — even once. That counts.
3
Tertiary Observable Indicator
Can the child attend a family gathering without a major screaming episode? This is the long-term goal.
Research: PMC10955541 — Meta-analysis: FCT promotes functional communication as primary target, with behavioural regulation as secondary benefit.

Material 1: AAC Devices & Communication Boards
Canon Category: Communication / AAC
₹0 DIY Option Available
AAC (Augmentative and Alternative Communication) boards and devices give your child a voice when words aren't available yet. They are the most impactful single investment for a child whose screaming is communication-based. When your child can point to a picture to say "help," "more," or "I'm done," screaming becomes unnecessary for that function.
Commercial Options
Price range: ₹500–₹50,000+ (printed boards through to dedicated speech-generating devices). Recommended for SLP evaluation first to select appropriate vocabulary set.
₹0 DIY Version
Print a photo grid on A4 paper — use phone photos of your child's daily desired items. Place in a plastic sleeve or laminate. Start with just 4–6 pictures of the things they want most. This works. A ₹0 board used consistently outperforms a ₹50,000 device used incorrectly.

Material 2: Visual Volume Scales & Modulation Tools
Canon Category: Visual Supports
₹0 DIY Option Available
A visual volume scale is a numbered chart (1–5) showing different voice levels with corresponding illustrations, faces, or colour codes. It gives your child a visual reference for understanding that different situations call for different volumes — and gives you a neutral, non-confrontational way to redirect. Instead of "stop screaming," you can say "we need a level 2 voice in here" and point to the chart.
Commercial Options
Price range: ₹100–₹500. Pre-printed laminated scales are widely available and durable. Some include audio components. Look for scales with visual faces and colour gradients for maximum accessibility.
₹0 DIY Version
Draw a 1–5 scale on cardboard. Draw a face at each level: level 1 = sleeping face (whisper), level 3 = talking face, level 5 = shouting face. Colour-code with markers. Post at the child's eye level in every room you use regularly. Takes 10 minutes to make.
Material 3: Noise-Cancelling Headphones
Canon Category: Sensory Regulation Equipment
For children whose screaming is sensory-driven, the environment's acoustic intensity can be an overwhelming trigger. Noise-cancelling headphones reduce incoming auditory stimulation, lowering the child's overall sensory load and reducing the likelihood of a screaming episode triggered by environmental noise. They are particularly useful in community settings — supermarkets, family events, public transport — where sound control is impossible.
Commercial Options
Price range: ₹1,500–₹8,000. Look for child-sized, over-ear, passive noise-reduction models for everyday use. Active noise-cancelling models offer more protection in louder environments. Ensure a snug but comfortable fit.
Important Usage Notes
Do not use where hearing environmental sounds is a safety requirement. Introduce the headphones during calm, preferred activities first — never force them on during distress. Many children accept them readily once they experience the relief. Pair introduction with a preferred activity.

Material 4: Proprioceptive / Heavy Work Equipment
Canon Category: Sensory Regulation Equipment
₹0 DIY Option Available
Proprioceptive input — deep pressure and heavy work — provides the nervous system with the intense sensory feedback that sensory-seeking children need. When children get sufficient proprioceptive input, their overall arousal level regulates, and the drive to scream for sensory stimulation reduces. Heavy work is a proactive tool — use it before anticipated triggers, not as a response to screaming already in progress.
Commercial Options
Price range: ₹1,000–₹5,000. Mini trampolines, therapy balls, weighted lap pads, and resistance tunnels are the most versatile investments. Always supervise. Never exceed 10% of the child's body weight for weighted items.
₹0 DIY Version
Carry books in a backpack (add more over time), push a laundry basket, do wall push-ups, carry grocery bags, wheelbarrow walks. These everyday activities deliver the same proprioceptive input as equipment. Build them into the routine before transitions.

Material 5: Vibrating Oral Motor Tools
Canon Category: Oral Motor Tools
₹200 DIY Option
Many children scream because their throat, mouth, and jaw are seeking deep sensory input — vibration and proprioception in the oral motor system. Vibrating oral tools deliver exactly that input safely, allowing the sensory need to be met without vocalisation. They are one of the fastest-acting tools for sensory-based screaming because they address the physical sensation the child is seeking directly.
Commercial Options
Price range: ₹800–₹2,500. Purpose-made vibrating oral motor tools are designed for therapeutic use with safe materials and appropriate vibration intensity. Check weekly for wear and damage. Ensure no choking hazard potential.
₹200 DIY Alternative
A basic electric toothbrush (used without toothpaste) delivers equivalent vibration input and is accepted easily by most children. The familiar toothbrush shape reduces novelty-based resistance. This is a widely used clinical workaround endorsed by occupational therapists.
Material 6: Emotion Regulation Kits
Canon Category: Emotional Regulation
₹0 DIY Option Available
When a child lacks the vocabulary — verbal or visual — to identify and communicate what they are feeling, every emotion defaults to the loudest available expression: screaming. Emotion regulation kits provide a visual map of feelings, giving the child a bridge between internal state and communication. The key is pairing each identified emotion with one concrete strategy: mad = squeeze ball, sad = hug, excited = jump, scared = parent lap.
Commercial Options
Price range: ₹500–₹2,000. The Zones of Regulation framework is the most widely used in clinical settings. Emotion card sets, feelings dice, and visual strategy boards are available on Amazon.in and from SLP suppliers.
₹0 DIY Version
Print six emotion faces from any internet search (happy, sad, angry, scared, excited, surprised). Attach to the fridge or a prominent wall at the child's eye level. Practice identifying them during calm times — never during escalation. This simple tool, used daily, builds emotional literacy over weeks.

Material 7: Musical Instruments
Canon Category: Sensory / Vocalisation Outlets
₹0 DIY Option Available
Musical instruments serve a dual purpose: they provide an acceptable, socially appropriate outlet for loud vocalisation and sound-making, and they deliver the auditory and proprioceptive feedback that many children are seeking through screaming. A child who is allowed to bang a drum or shake a shaker for 3 minutes before a challenging transition has had their sensory need met — and screaming becomes less necessary.
Instruments also provide a natural bridge toward volume modulation: playing softly versus loudly, fast versus slow, are early volume-control concepts that translate to voice modulation with practice over time.
Commercial Options
Price range: ₹300–₹3,000. Hand drums, maracas, tambourines, and xylophone sets offer the widest sensory range. Choose instruments the child can use independently without risk of injury.
₹0 DIY Version
Pots and a wooden spoon make an excellent drum. Dried rice or lentils in a sealed plastic bottle creates a shaker. These household instruments are often preferred by children because they're familiar and non-threatening. No investment required to begin today.
Material 8: FCT Cards (Functional Communication Training)
Canon Category: Communication / AAC
₹0 DIY Option Available
Functional Communication Training (FCT) cards are simple picture or word cards that replace a specific screaming behaviour with a functional communicative act. The most powerful starter cards are HELP, BREAK, and MORE — the three most commonly communicated needs that currently come out as screaming. FCT is one of the most rigorously evidence-based approaches in ABA for reducing challenging behaviours.
Critical rule: You must honour every single use of the FCT card, every single time, immediately. Inconsistency is the number one reason FCT fails. If the child shows you the HELP card, stop everything and provide help within 3 seconds.
Commercial Options
Price range: ₹200–₹800. PECS (Picture Exchange Communication System) materials are the gold standard. Pre-made FCT card sets are available on Amazon.in. Cards should be laminated for durability.
₹0 DIY Version
Cut cardboard into credit-card-sized pieces. Write HELP / BREAK / MORE in large letters, or draw simple pictures. You can start with just one card — the HELP card alone has transformed families' daily lives within weeks.

Material 9: Environmental Modification Tools
Canon Category: Visual Schedules / Environmental
₹0 DIY Option Available
Many screaming episodes are triggered by unpredictability — the child doesn't know what is coming next, and the uncertainty produces anxiety that comes out as screaming. Visual schedules eliminate this trigger by making the sequence of the day transparent and predictable. Environmental modification tools also include reducing visual clutter, managing lighting and sound levels, and creating designated calm spaces within the home.
Commercial Options
Price range: ₹300–₹1,500. Magnetic visual schedule boards, velcro activity strips, and laminated daily routine cards are widely available. The most useful feature is the ability to show "what's happening now" and "what's next."
₹0 DIY Version
Paper and drawn icons on a cardboard strip, secured with pieces of tape or blu-tack. You do not need printed images — stick figures representing activities are sufficient. Show the child the schedule at the start of each session and each day. This single tool reduces transition-triggered screaming significantly.

All 9 Materials at a Glance
A complete overview of every material, its function, and cost range — so you can identify where to start based on your child's primary screaming function and your budget. Every material has a ₹0 version. No family is left behind.
Material | Primary Function | Price Range | DIY Cost | |
AAC / Communication Boards | Replaces screaming with picture-based communication | ₹500–₹50,000+ | ₹0 | |
Visual Volume Scales | Teaches volume differentiation and modulation | ₹100–₹500 | ₹0 | |
Noise-Cancelling Headphones | Reduces incoming sensory overload | ₹1,500–₹8,000 | Cotton wool (short-term) | |
Heavy Work Equipment | Proprioceptive regulation pre-trigger | ₹1,000–₹5,000 | ₹0 | |
Vibrating Oral Motor Tools | Meets oral sensory seeking need directly | ₹800–₹2,500 | ₹200 | |
Emotion Regulation Kits | Builds emotional vocabulary and coping strategies | ₹500–₹2,000 | ₹0 | |
Musical Instruments | Acceptable sensory outlet, volume modulation bridge | ₹300–₹3,000 | ₹0 | |
FCT Cards | Replaces specific screaming functions with cards | ₹200–₹800 | ₹0 | |
Visual Schedules / Env. Modification | Eliminates predictability-based triggers | ₹300–₹1,500 | ₹0 |
"The therapeutic tool is not the object — it is the systematic, consistent, responsive way you use it." — Pinnacle Blooms Clinical Faculty

Safety Protocols for Home Implementation
⚠️ Read Before Starting
Home-based therapy is powerful and effective — and it requires clear safety awareness. Review these protocols before introducing any material. When in doubt, consult a licensed therapist first.
Rule Out Medical Causes First
Ear infection, dental pain, or headache can cause sudden screaming onset. Always verify the child is medically well before attributing screaming to behaviour or sensory function.
Weighted Items — 10% Rule
Never exceed 10% of the child's body weight for any weighted tool or equipment. Adult supervision required at all times for heavy work and trampoline activities.
Oral Motor Tools — Weekly Check
Inspect for wear and damage every week. No tool with choking hazard potential. Discontinue immediately if tool shows significant deterioration.
FCT Cards — Honour Every Use
You must respond to every FCT card use, every time, immediately. Inconsistency worsens behaviour. If you cannot honour a card use in that moment, the card loses its value and the screaming returns.
🔴 Seek urgent assessment if you observe: Sudden onset screaming in a previously quiet child | Screaming with self-injury | Screaming with skill regression | Screaming that sounds like pain | Complete non-response to all interventions over 4+ weeks.
📞 Escalation path: Self-resolve → Teleconsult 9100 181 181 → Clinic visit → Emergency
📞 Escalation path: Self-resolve → Teleconsult 9100 181 181 → Clinic visit → Emergency
Set Up Your Home Therapy Space
Spatial precision prevents 80% of session failures. Preparing your environment before calling your child to the session is not a small step — it is a foundational one. A well-prepared space communicates safety and predictability to your child's nervous system before a single word is spoken.
👧 Child Position [1]
Comfortable seat, floor mat, or preferred position. Same level as the child. Never standing over them.
👩 Parent Position [2]
At the child's level — side or slightly in front. Open body posture. Your calm is contagious.
📦 Materials [3]
All materials within reach but not fully visible at session start. Retrieve one at a time to prevent overwhelm.
📅 Visual Cues [4–6]
Visual schedule visible. Timer visible to child. Headphones nearby if needed. All set before child enters.
Before you call your child:
Screens off. Toys out of sight. Background noise minimised. Your phone on silent. Child is fed, not tired, not overdue for a nap.
Preferred environment conditions:
Soft natural light. Background music optional — calm, instrumental, low volume. Temperature comfortable. Dysregulation increases with heat.
Research: PMC10955541 — Meta-analysis confirms structured 1:1 environment as most effective setting for ASD interventions.
The Pre-Session Readiness Check
ACT III — EXECUTION
60 Seconds Before Every Session
The best session is one that starts right. A 5-minute session on a good day teaches more than a 20-minute session during dysregulation. Run this check before every session — it takes 60 seconds and prevents wasted effort.
✅ GO — All 7 Indicators Met
Proceed to Step 1. Full protocol available today.
⚡ MODIFY — 5–6 Indicators Met
Use simplified version: one material only, 5 minutes, extra reinforcement. Still therapeutic.
⏸ POSTPONE — Fewer Than 5
Alternative today: heavy work activity + preferred activity. Note the state for data.
- Fed within 2 hours? (empty stomach = dysregulation)
- Not due for sleep within 30 minutes?
- No fever, illness signs, or visible pain?
- No major meltdown in the last 20 minutes?
- Alert and responsive (tracking faces or objects)?
- In a tolerable sensory environment right now?
- You — the parent — are calm and regulated?

Step 1: The Invitation
STEP 1 OF 6
⏱ 30–60 seconds
Begin with an invitation, never a command. The ABA pairing principle is clear: you must be associated with good things before any demand is placed. Never start with instruction. Start with connection.
"Hey [child's name], want to play the voice game with me?" OR: "Look what I have!" [show preferred material without demanding] OR [non-verbal child]: Sit near, offer the material gently at their level, wait 10 seconds for any approach signal.
Acceptance Signals — Watch For These
- Eye contact (even brief)
- Physical approach toward you or the material
- Reduction in current vocalisation
- Any gesture of interest: reaching, pointing, leaning
Resistance Signals — How to Respond
- Moving away → Give space, try again in 2 minutes
- Increased screaming → Not the moment; offer comfort and postpone
- Turning away → Offer material at periphery; don't force face-to-face
Body language: Get to the child's eye level. Relaxed face. Open posture. Gentle voice — irrespective of the child's current volume.

Step 2: Building Engagement
STEP 2 OF 6
⏱ 1–3 minutes
Child is engaged. Now introduce the material therapeutically. The material you introduce first should match what you believe is driving the screaming. If you are unsure of the function, the visual volume scale is the lowest-demand, highest-utility starting point for all children.
If Screaming is Communication-Based
Introduce the AAC board or FCT cards first. "This is your HELP card. When you want help, you can show me this." Model it yourself immediately. Make it playful.
If Screaming is Sensory-Based
Introduce oral motor tool or heavy work first. "This buzzing tool is for when your throat needs something." Offer without demand. Observe the approach.
If Screaming is Regulation-Based
Introduce the emotion chart first. "These are the feeling faces. Let's find which one is you right now." Point to options gently. Accept any response.
If Function is Unclear
Start with the visual volume scale — lowest demand, highest universal utility. It works across all screaming functions as a starting point.
The moment any engagement occurs: immediate warm praise. "Yes! You picked the card! That's exactly it." Do not wait. Do not hesitate. The reinforcement window is 3 seconds.

Step 3: The Therapeutic Action — AAC & FCT Protocols
STEP 3 OF 6 — PART A
⏱ 5–10 minutes
This is the active therapeutic ingredient — the moment where screaming behaviour and its replacement come face to face. Match the material protocol precisely to the function.
1
Place the AAC Board or FCT Card
Position the communication board or device where the child can reach it independently. It should be accessible at all times during the session — not kept away until needed.
2
When Screaming Starts — Redirect Calmly
"Use your board — what do you need?" Point to the board. Do not raise your voice. Do not match the child's volume. Your calm is the intervention.
3
The Moment Any Symbol Is Touched — Honour It
Immediately give the item, stop the demand, or provide the attention — whatever the symbol indicates. Do NOT require perfect use. Approximate use is honoured every time.
4
Shape Over Multiple Sessions
In early sessions, honour any touch of the board. Over weeks, gently shape toward clearer, more accurate symbol selection. The replacement habit is established first. Accuracy follows.
Research: PMC10955541 — 40-minute therapy sessions optimal; 10–20 min home sessions equally effective when consistent.

Step 3: The Therapeutic Action — Volume Scale & Heavy Work Protocols
STEP 3 OF 6 — PART B
⏱ 5–10 minutes
Visual Volume Scale Protocol
- Post the scale at eye level in the session room
- During a CALM moment: "What number voice is this?" Demonstrate each level
- Practice: "Show me a 2 voice!" Make it a game
- During emerging scream: calmly walk to scale, point: "That was a 4. Can you try a 3?"
- Do NOT use the scale during peak escalation — use it in the calm before or after
Heavy Work Protocol
- Use BEFORE the anticipated trigger: "First jumping jacks — 10 big ones! Then [next activity]"
- Child jumps, pushes, or carries for 3–5 minutes
- Immediately proceed to the target activity
- Heavy work is proactive — not a response to screaming already in progress
- Vary intensity across sessions: floor jumps → cushion → mini trampoline
Step 3: The Therapeutic Action — Oral Motor & Emotion Protocols
STEP 3 OF 6 — PART C
⏱ 5–10 minutes
Oral Motor Tool Protocol
- Offer the vibrating tool BEFORE or at the very onset of screaming
- "Here's your buzzer tool." — Do not demand use; place within reach
- If child accepts: allow 2–3 minutes of oral input
- Screaming naturally reduces as the sensory need is met through the tool
- Over time, the child will begin reaching for the tool independently before screaming
Emotion Regulation Protocol
- During calm periods: "Which feeling is this face?" Point to the chart and practice labelling
- When frustrated: "What face are you right now? Let's find it together"
- Pair each emotion with one strategy: mad = squeeze ball, sad = hug, excited = jump, scared = parent lap
- Consistency of the pairing is what builds the habit — same emotion, same strategy, every time
Total protocol time: 5–10 minutes | Minimum repetitions: 3–4 per material per session. Even 1 successful exchange has therapeutic value. Count it. Record it.
Step 4: Repeat and Vary — Therapeutic Dosage
STEP 4 OF 6
⏱ 3–5 minutes
3 engaged repetitions outperform 10 forced repetitions. Forced practice builds avoidance, not skill. Watch your child for satiation signals and always stop while engagement is still present.
Target Repetitions
3–5 functional exchanges per material per session. Stop when the child shows satiation. Even 1 successful exchange is therapeutic — do not discount it.
AAC Variations
Vary vocabulary (request → protest → comment). Change the setting. Change who honours the request (parent A → parent B → sibling). Generalisation is built into variation.
Volume Scale Variations
Practice in different rooms. Voice-matching games: "Match MY voice." Volume-level songs with quiet verses and loud choruses. Recording feedback: children often self-correct when they hear themselves.
Heavy Work Variations
Carrying (light bag → heavier bag over weeks). Jumping (floor → cushion → mini trampoline). Wall push-ups → floor push-ups → wheelbarrow walk. Progress gradually.
Satiation indicators — stop when you see: Child repeatedly redirects away from the material | Engagement time shortening each exchange | Child initiates a transition | Quality of responses degrading (mechanical, not engaged).

Step 5: Reinforce and Celebrate
STEP 5 OF 6
⏱ Within 3 seconds of target behaviour
"YES! You used your HELP card! I see you! Here's [reward]." Be specific: "You pointed to the picture instead of screaming. That tells me exactly what you need." Warm physical affirmation the child enjoys: high-five, squeeze, clap together, fist bump.
🥇 Natural Reinforcer (Best)
The child gets what they communicated. The communication WORKED. This is the most powerful reinforcer because it proves the alternative works better than screaming.
🥈 Social Reinforcer
Enthusiastic verbal praise plus a preferred interaction. Warm, specific, and immediate. Never delayed. Never generic. "YOU did that."
🥉 Token Economy
Sticker toward a preferred item chart. Use Pinnacle Canon: Rosette Reward Jar or 1800+ Reward Stickers pack. 5–10 stickers = 1 preferred activity. Never remove earned stickers — this destroys trust.
Critical rule: Celebrate the ATTEMPT, not just the success. Any use of an alternative to screaming = reinforce. Perfect form comes later. The replacement habit comes first.
Step 6: The Cool-Down
STEP 6 OF 6
⏱ 2–3 minutes
Never end a session abruptly. The cool-down is part of the protocol — not optional. Abrupt endings create transition anxiety that accumulates across sessions and increases resistance to future sessions. Engineer a calm close every time, even if the session itself was difficult.
Capture the Data: Right Now
60 seconds of data equals 8 weeks of progress evidence. Parents who track are 4× more likely to see measurable progress — because tracking reveals trends that daily observation misses. The progress is often happening before it feels like it is.
1
Which materials did you use today?
AAC/Communication Board | Visual Volume Scale | Noise-Cancelling Headphones | Heavy Work | Oral Motor Tool | Emotion Regulation Kit | Musical Instruments | FCT Cards | Environmental Modification
2
How many times did screaming occur?
Record: 0–1 | 2–5 | 6–10 | 10+. Compare this week to last week. The trend line is what matters — not any single session.
3
Did the child use any alternative?
Yes — independently | Yes — with prompting | Not yet. Any "yes" is progress. Prompted use is a real and valid milestone.
4
Overall session quality?
⭐⭐⭐ Great | ⭐⭐ Good | ⭐ Modified | Postponed. All outcomes are data. A postponed session honestly recorded is more useful than a great session unrecorded.
Questions about your data? 📞9100 181 181 — Connect with a Pinnacle clinician who can interpret your tracking and personalise your next steps.
Troubleshooting: When It's Not Working
⚠️ Common Challenges
Every child and family encounters obstacles. The troubleshooting protocol below addresses the six most common barriers — with specific, clinical solutions for each. If you have been implementing for 3+ weeks without progress, a BCBA-led functional assessment is the most valuable next step.
"My child completely refuses the AAC board"
The vocabulary may not match what the child actually wants. Rebuild with just 2–3 pictures of highly desired items. Honour the first use with the most powerful reinforcer you have. Introduce during play, not demand.
"Screaming INCREASES when I introduce materials"
Common — novelty causes activation. Start further away. Leave material in the room without approaching. Use heavy work FIRST to regulate, then approach the material on day 3 or 4.
"Child uses the FCT card but screaming doesn't reduce"
Speed up your response to card use — every second of delay devalues it. Check: are you honouring 100% of card uses, 100% of the time? Even one missed response teaches the child that screaming is more reliable.
"The volume scale has no effect"
The child may not yet understand abstract volume levels. Add auditory demonstrations: whisper vs. shout. Use recording playback — children often self-correct hearing themselves. The scale needs to be practiced during calm, not just offered during escalation.
"Heavy work doesn't seem to help"
Screaming may be communication-based rather than sensory. Shift primary focus to AAC/FCT. Conduct brief ABC tracking (Antecedent–Behaviour–Consequence) for one week to identify the function more precisely.
"We've been doing this 2 weeks and nothing has changed"
Two weeks is the tolerance-building phase, not the change phase. Review: are all caregivers consistent? Inconsistency is the #1 barrier. This is the moment to connect with a BCBA. 📞 9100 181 181.
Weeks 1–2: What to Expect
ACT IV — PROGRESS ARC
Phase 1: Tolerance Building — 15%
"If your child tolerated the AAC board in the room for 3 minutes without screaming — that is measurable progress. Write it down."
Weeks 1–2 often feel like nothing is working. This is normal and expected. Neural pathways are forming. The data you capture now will show you the trend in Week 8. Do not look for dramatic change yet — look for these specific indicators instead.
✓ Tolerance
Child tolerates the material being in the room — even without using it. This is the first step.
✓ Brief Pause
Screaming pauses briefly when a material is offered — even 3 seconds. That 3 seconds is a measurable neural event.
✓ Approach
Child approaches the communication board at least once — even without using it. Physical proximity is engagement.
✓ Function Identified
You have identified at least one function the screaming serves. This is clinical progress regardless of the child's behaviour.
Research: PMC11506176 — Early-phase tolerance and participation precede skill acquisition in 8–12 week intervention protocols.
Weeks 3–4: Consolidation Signs
Phase 2: Neural Pathway Formation — 40%
The brain is learning — and it is physically changing. Synaptic connections are forming between the communication intent and the new behaviour. You may not see dramatic change yet. But these consolidation indicators tell you the work is taking root.
Anticipation
Child moves toward materials without being called. They are beginning to associate the materials with relief and positive interaction.
Spontaneous Use
AAC or FCT card used spontaneously at least once — unprompted. Even once is a milestone. Document the exact moment.
Duration Reduction
Screaming reduces in duration even if frequency is unchanged. Shorter episodes indicate growing regulation capacity.
Volume Differentiation
Child begins to show even small differences in volume between contexts. This is volume modulation beginning to emerge.
If you are seeing consolidation indicators: increase session frequency from once to twice daily, begin embedding the protocol in community settings for short outings, and add the second caregiver to the training this week.
Weeks 5–8: Mastery Indicators
Phase 3: Mastery & Generalisation — 75%
Mastery is defined by three specific, observable, measurable criteria. All three must be met to confirm mastery and move toward the next technique in the progression pathway.
1
Frequency Reduction
Screaming episodes reduced by ≥40% from your Week 1 baseline count. This is why the Week 1 data matters — it is your evidence baseline.
2
Alternative Use
Child uses a communication alternative (AAC, FCT, gesture, or volume scale reference) in ≥50% of situations that previously triggered screaming.
3
Generalisation
Behaviour change observed in at least 2 settings: home AND one other (school, grandparent's house, a shop). Generalisation is the proof of real learning.
Maintenance check: Does the progress persist when you take a session break? If yes → Mastery. Move toward the next technique. If no → Stay and strengthen. ABA calls this "maintenance training" — it is a normal and expected phase.
Research: PMC10955541 | BACB mastery criteria standards

Celebrate This Win
You did this. Your child grew because of your consistency. In 5–8 weeks you showed up every single day — through exhaustion, through the sessions that felt like failures, through the weeks where change seemed invisible. Here is what you actually accomplished.
★ Knowledge
You learned the neuroscience behind your child's screaming
★ Understanding
You identified what function the screaming was serving
★ Courage
You introduced materials your child had never encountered before
★ Consistency
You showed up for sessions even when you were exhausted
★ Evidence
You captured data that proves the progress is real
★ Transformation
You gave your child new ways to communicate that aren't screaming
"Your child has more tools today than they did 8 weeks ago. That happened because you showed up. Every. Single. Day."
🎉 Tonight: child's choice dinner. 📸 Document: a photo or video of your child using their AAC device or volume scale — this is evidence of development. 📖 Journal: one paragraph about what changed in your home.

5 Red Flags: When to Pause and Seek Consultation
⚠️ Safety First
These five red flags require you to pause the home protocol and seek professional consultation. Your instinct matters — if something feels wrong, it probably warrants a closer look.
🔴 Flag 1: Sudden Onset After Quiet Period
What: A child who wasn't a screamer suddenly begins screaming persistently. Why: Medical cause possible — ear infection, dental pain, GI discomfort, or neurological. Do: Medical appointment within 48 hours.
🔴 Flag 2: Screaming Plus Self-Injury
What: Screaming accompanied by head-banging, biting self, or other physical self-harm. Why: Escalation of regulatory crisis requiring specialist input. Do: Pause protocol. Contact Pinnacle centre or BCBA urgently. 📞 9100 181 181
🔴 Flag 3: Screaming With Skill Regression
What: Not just screaming — also losing previously acquired words or skills. Why: Medical or neurological flag requiring evaluation. Do: Pediatric neurology referral plus comprehensive assessment.
🔴 Flag 4: Protocol Consistently Worsens Screaming Over 3+ Weeks
What: Every session makes things worse, not better. Why: Function misidentified; different approach needed. Do: Teleconsult — we help you identify the correct function. 📞 9100 181 181
🔴 Flag 5: Caregiver Crisis
What: You — the parent or caregiver — are in distress, burnout, or unable to continue. Why: Your regulation is foundational to the child's regulation. Do: Respite support first. The protocol can wait. You cannot. 📞 9100 181 181

Related Techniques That Work Alongside D-423
D-421 — Understanding Vocal Behaviours
Why children make the sounds they make — the foundational knowledge layer beneath all vocal intervention work.

D-422 — Vocal Stereotypy
When repetitive vocalisations serve a self-regulatory function — the technique directly preceding D-423 in the progression.

C-244 — Screaming Episodes
Acute screaming during emotional crises — the parallel technique for episodic rather than constant screaming patterns.

D-430 — Emotional Dysregulation
When emotions overwhelm the child's entire system — the broader regulation protocol that D-423 feeds into.

B-150 — Building Intentional Vocalisations
From random sounds to purposeful communication — the next developmental step after screaming is reduced.

K-5000–5020 — Parent Support Series
Understanding challenging behaviours, caregiver self-care, and functional assessment for parents — the ecosystem surrounding this work.
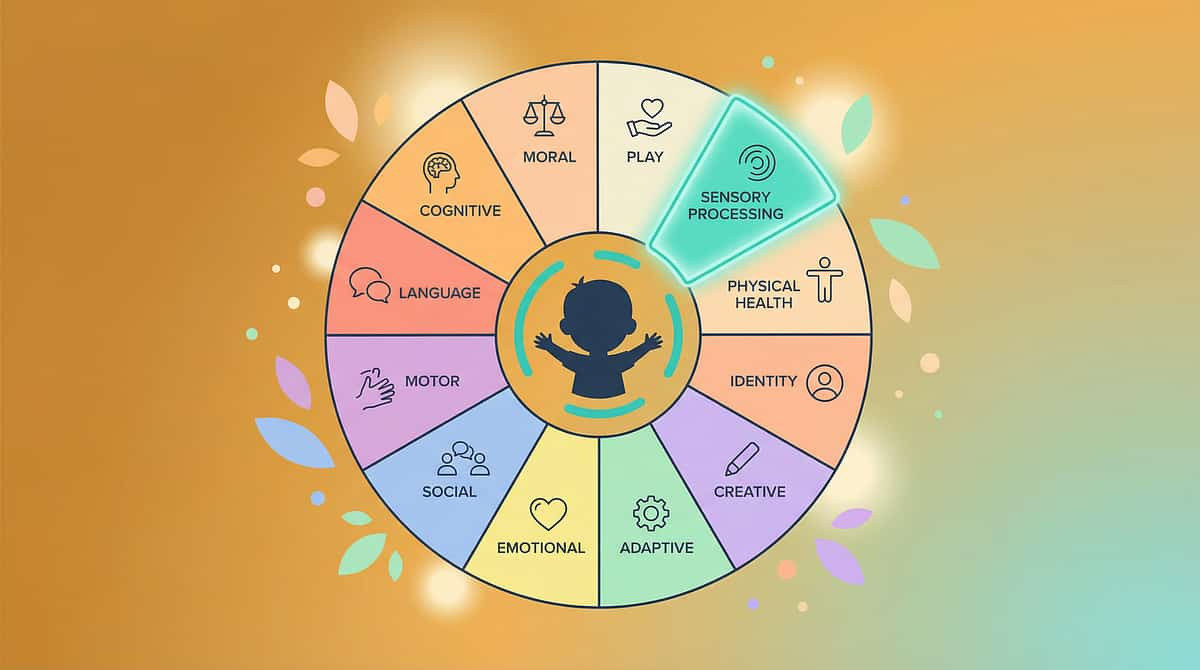
Your Child's Journey Within Domain D
D-423 is one of 70+ techniques within Domain D — Behaviour and Flexibility. Understanding where this technique sits within the broader developmental map helps you see the full journey, not just today's challenge.
D-421
Understanding Vocal Behaviours — foundation knowledge
D-422
Vocal Stereotypy — self-regulatory vocalisations
★ D-423
Constant Screaming — you are here. 9 Materials Protocol.
D-424
Bolting and Elopement — behavioural regulation family
D-425
Self-Injurious Behaviour — advanced regulation domain
Within GPT-OS®'s AbilityScore® system, D-423 progress is tracked under the Communication Readiness Index, the Behavioural Regulation Readiness Index, and the Environmental Participation Readiness Index. Your child's personalised map is available through a full GPT-OS® assessment.
Preview of 9 materials that help with constant screaming Therapy Material
Below is a visual preview of 9 materials that help with constant screaming therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

You Don't Have to Navigate This Alone
Constant screaming isolates families. You stop going out. You stop inviting people over. You stop asking for help. This page exists because your child deserves a parent who feels supported. That starts here.
🌐 Pinnacle Parent Community
10,000+ families navigating similar journeys — India's largest pediatric therapy parent community. Practical peer support, daily. pinnacleblooms.org/parent-community
📱 WhatsApp Support Group
Join the Constant Screaming Support Group. Request your link via the free helpline. Real-time peer support from families at every stage of this journey.
📚 Pinnacle Knowledge Library
Evidence-based guides, technique videos, and parent workshops. All free. All accessible from your phone. pinnacleblooms.org/resources
FREE National Autism Helpline: 📞 9100 181 181 | 16+ languages | 24×7 | No consultation fee
"From Tamil to Marathi to Bengali — speak in your language."
"From Tamil to Marathi to Bengali — speak in your language."