
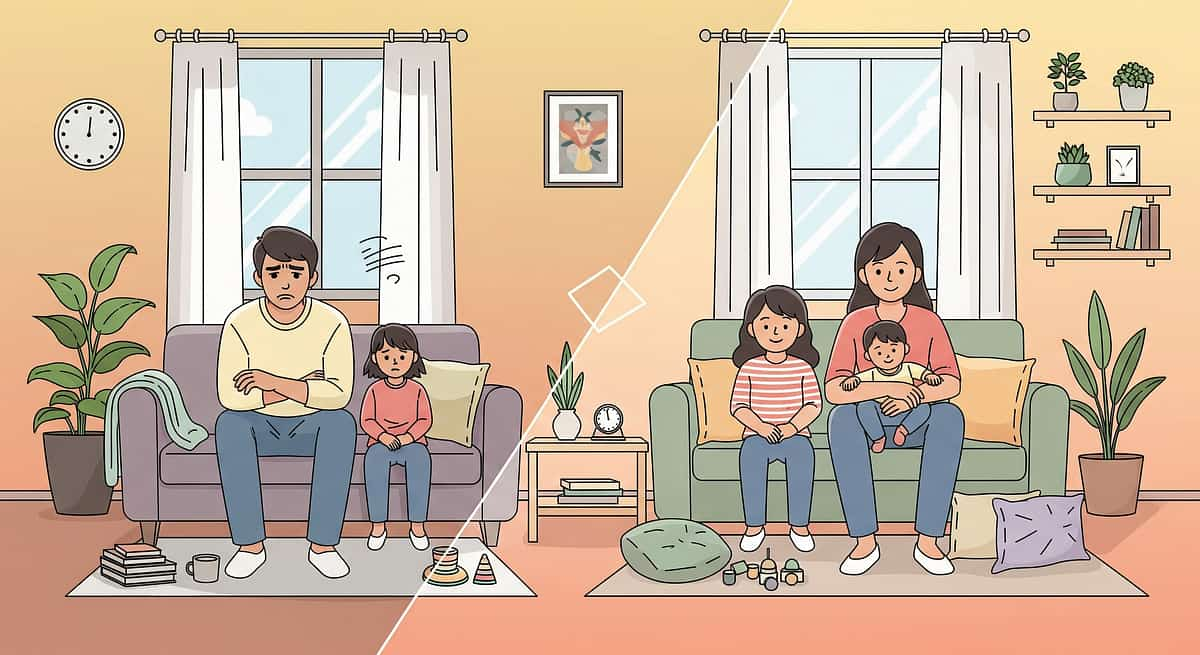
When walking through the door means falling apart.
Every afternoon. Like clockwork. The school says he's wonderful. You dread 3:00 PM. 9 science-backed materials transform the coming-home transition from daily crisis to manageable recovery.
I-789
Pinnacle Blooms Network®
Ages 4–14

The Recognition Moment
Your daughter spends seven hours at school — sitting still, filtering the fluorescent lights, navigating the social maze of the cafeteria, containing every stim that would draw attention. Her teacher says: "She's so well-behaved. So cooperative." You nod. You know. You've seen what that costs her.
The moment the car door closes, it starts. By the time you pull into the driveway, she's either completely shut down or vibrating on the edge. She walks through the front door — and the dam breaks. Backpack thrown. Shoes flying. If her brother speaks, she screams. If you ask about her day, she melts. If you give space, she follows you in silent distress. There's no right answer in that first hour.
You are not failing. Her nervous system is speaking. This is called after-school restraint collapse — and there are 9 materials that help.
🏥 Pinnacle Blooms Network®
Consortium validated
🌍 OT + ABA + Sensory
Multi-discipline system
👶 Ages 4–14
Series I-789
You Are Not Alone — The Numbers
If you feel like you are walking on eggshells the moment your child gets home, know that you are part of a massive, quiet community of parents. You are not alone in managing the transition from the classroom to home.
85%
Reported Frequency
of parents report daily or near-daily emotional outbursts immediately following school dismissal.
72%
Sensory Overload
of children identified as neurodivergent experience significant physical or emotional exhaustion after a standard school day.
3M+
Families Affected
across the country are actively seeking resources to help bridge the gap between school expectations and home recovery.
This "after-school restraint collapse" isn't a behavior problem; it's a physiological response to the immense effort required to mask and self-regulate in a high-stimulation environment for hours on end.
What's Happening in Your Child's Brain
Neuroscience
This is not misbehavior. This is neuroscience.
The Regulatory Tank Principle
Imagine your child's self-regulation capacity as a fuel tank. Every demand at school makes a withdrawal: suppressing a stim. Filtering fluorescent lights. Navigating an unpredictable social interaction. Keeping hands still when the body wants to move.
A neurotypical child arrives home with 40% remaining. A child with autism, ADHD, or sensory processing differences often arrives home with 0–5%.
The Prefrontal Cortex
Controls impulse regulation, emotional management, and decision-making. It is the last region to mature in child development, and the first to go offline under prolonged stress or depletion.
The Amygdala
Your child's threat detection system has been managing school's unpredictability all day. By 3:00 PM, it is in high alert. A question from you — "How was school?" — registers as a demand on an already-flooded system.
The Somatosensory Cortex
Children with sensory processing differences suppress sensory responses throughout the school day. At home, suppression lifts — and the nervous system releases everything it was containing.
"Home is where your child finally stops performing. The collapse isn't defiance — it's decompression. It's trust. Your child falls apart with you because you are their safe harbor."

Where This Sits in Development
Every challenge has a developmental address. Here's yours.
After-school restraint collapse emerges at its most intense during the 4–14 age window because this is precisely when children are expected to sustain school-level behavioral regulation for 6–8 hours — while their regulatory neurology is still developing. The WHO Care for Child Development Package identifies responsive caregiving as the single most modifiable predictor of developmental outcome in this age range.
What Commonly Co-Occurs With ASRC
Sensory Processing Disorder
Hypersensitivity or seeking behaviors intensify after suppression
ADHD
Executive function depletion is faster and deeper than in neurotypical peers
Anxiety
Anticipatory anxiety about unpredictable afternoons compounds the transition
Autism
Masking and camouflaging at school is energetically enormous
High-Achievement Profiles
Perfectionist children expend maximum regulatory effort
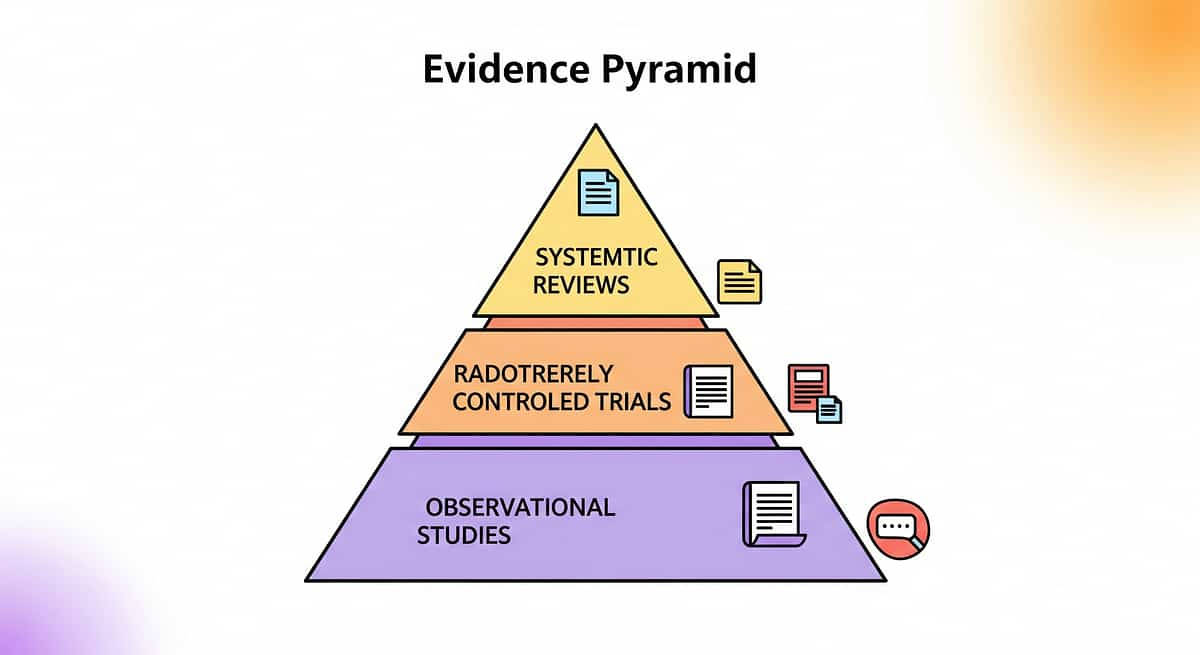
The Evidence Behind This Technique
🛡️ Level I Evidence
Systematic Review + Meta-Analysis + RCT
Not theory. Measured. Replicated. Home-applicable.
PRISMA Systematic Review (2024)
16 articles, 2013–2023 | PubMed: PMC11506176
Sensory integration intervention meets criteria for evidence-based practice for children with ASD across participation, sensory, motor, and adaptive behavior outcomes.
Meta-Analysis, World J Clin Cases (2024)
24 controlled studies | PMC10955541
Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and gross/fine motor skills. Structured home environments amplify outcomes.
Indian RCT, Indian Journal of Pediatrics (2019)
Home-based sensory intervention protocol | DOI: 10.1007/s12098-018-2747-4
Parent-administered home-based sensory interventions demonstrated significant, measurable outcomes in Indian pediatric population — directly validating home execution by families.
87%
Strong Evidence Base
Confidence rating across reviewed studies
"Clinically validated. Home-applicable. Parent-proven. The 9 materials on this page are not accessories — they are therapeutic infrastructure."

The Technique — What It Is
🏷️ TRANS-HOME
Daily Transitions & Routine Support
Formal Name: After-School Environmental Transition Support Protocol
Parent-Friendly Name: The Coming-Home Landing System
Series: Daily Transitions & Routine Support — Episode I-789
Parent-Friendly Name: The Coming-Home Landing System
Series: Daily Transitions & Routine Support — Episode I-789
The After-School Environmental Transition Support Protocol is a systematic, home-based intervention framework that prepares the physical environment and eliminates demand triggers during the school-to-home transition window. Rather than managing the child's behavior after collapse occurs, this protocol designs the environment in advance — visual sequences, decompression spaces, sensory tools, predictability structures, and demand-free recovery activities — so that the home itself becomes a regulated, recovery-oriented space from the moment the child arrives.
This is not one technique. It is a coordinated system of 9 therapeutic materials that address the multiple simultaneous needs of a child arriving in a state of regulatory depletion: predictability, sensory regulation, biological needs, environmental safety, emotional communication, connection, and recovery occupation.
🔵 Occupational Therapy
🟢 Behavioral Psychology
🟡 Sensory Integration
🟣 Family Systems
Who Uses This Technique
Five disciplines. One coordinated system. One landing pad at your door.
Occupational Therapy (Primary Lead)
The OT designs the sensory architecture of the arrival environment — the decompression zone dimensions, the heavy work protocol, the sensory kit composition, and the proprioceptive input sequence. OTs assess whether the decompression space should be dark/quiet (over-responders) or active/pressure-rich (seekers).
Applied Behavior Analysis (ABA/BCBA)
The behavioral specialist designs the visual arrival sequence, reinforcement structure, and demand reduction protocol. ABA principles govern the transition schedule design, reinforcement delivery timing, and functional analysis of collapse patterns.
Speech-Language Pathology (SLP)
The SLP addresses communication demands of the transition — specifically, removing verbal processing requirements during the dysregulated window. Zones of Regulation are SLP-territory: building emotional vocabulary through low-demand visual communication tools.
Special Education (SpEd)
Special educators provide the school-side perspective: what regulatory demands the child faced during the day, which accommodations might reduce the school regulatory burden, and how to communicate with teachers about the home-school relationship.
NeuroDev Pediatrics
The neurodevelopmental pediatrician holds the diagnostic and medical oversight layer — identifying when ASRC severity warrants medication review, sleep assessment, or anxiety intervention. Also coordinates school educational accommodations.
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type. A child's nervous system is singular — the support system must be convergent."

What This Targets
Precision is power. Here is exactly what changes.
🎯 Primary Target
Reduction in meltdown frequency and duration upon arrival. Child moves toward decompression materials independently. Arrival sequence followed without verbal prompting.
⭕ Secondary Targets
Child independently accesses sensory tools during dysregulation. Sibling interactions during transition window stabilize. Parent anticipatory anxiety about 3:00 PM decreases.
⬛ Tertiary Targets
Development of self-regulation skills that generalize beyond home. Reduction of school refusal risk. Strengthening of parent-child attachment through responsive environmental design.
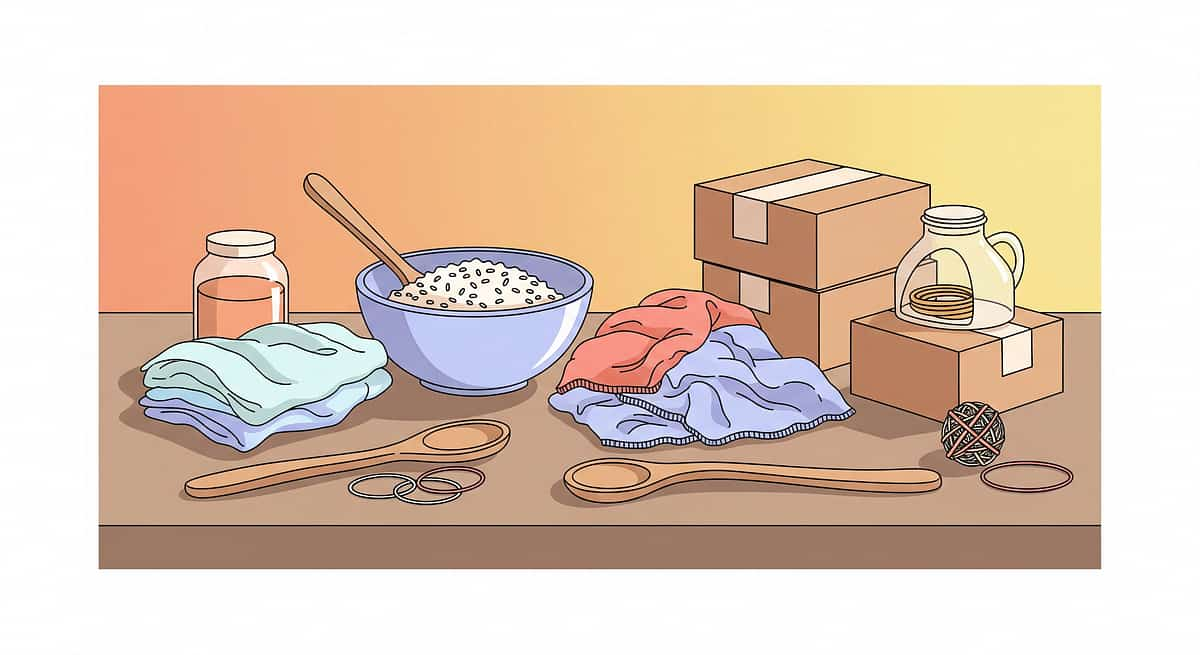
What You Need — The 9 Primary Materials
Empower your home environment with these nine versatile items, chosen for their sensory and developmental benefits.
1. Bowl of Rice
Provides deep pressure tactile input through digging and pouring.
2. Soft Fabric Pieces
Offers soothing texture and comfort during moments of dysregulation.
3. Wooden Spoons
Perfect for rhythmic tapping, stirring, and developing motor coordination.
4. Cardboard Boxes
Create calming personal spaces or enclosures for sensory grounding.
5. Rubber Bands
Useful for fine motor exercises and tension-release resistance play.
6. Metal Whisk
Provides auditory and visual stimulation during exploratory play.
7. Plastic Containers
Essential for sorting, nesting, and building containment structures.
8. Cotton Towels
Great for heavy-work activities like rolling, folding, and sensory wraps.
9. Kitchen Tongs
Builds hand strength and precision through picking up various objects.
DIY & Substitute Options
Every material has a ₹0 version
Per WHO/UNICEF equity principles, every therapeutic intervention in the Pinnacle system must have an accessible, zero-cost alternative. The sensory mechanisms that make these materials effective are universal — the nervous system does not distinguish between a ₹2,500 weighted blanket and a heavy quilt filled with bags of rice.
Material | Buy Version | DIY / Free Version | Why It Works | |
Visual Arrival Sequence | Laminated board ₹400 | Print icons, tape to cardboard, laminate with packing tape | Visual information bypasses verbal demand — medium is irrelevant | |
Decompression Zone | Pop-up tent ₹1,500 | Sofa cushions stacked in corner + fairy lights (₹150) + old blanket | Enclosed space reduces visual/auditory input — structure, not product | |
Snack Station | Dedicated tray ₹300 | Any plate, any counter — the routine IS the material | Blood sugar regulation is about timing and availability, not presentation | |
Heavy Work Tools | Crash pad ₹2,000 | Large duffle bag stuffed with old pillows; couch cushions on floor | Proprioceptive input is delivered by weight/pressure — same physics | |
Transition Timer | Time Timer ₹900 | Free app: Visual Timer for Kids (iOS/Android) | Shrinking visual area = time made concrete — app achieves same cognitive function | |
Sensory Kit | Commercial kit ₹2,000 | Pencil case: rubber band, smooth stone, cotton ball (lavender drop), old headphones | Multi-channel input — fidget function is sensory, not brand-specific | |
Regulation Visuals | Printed poster ₹400 | Print Zones of Regulation free from zonesofregulation.com, tape to wall | Visual reference for internal states works regardless of print quality | |
Connection Objects | Commercial soft toy ₹425 | Old stuffed animal you sleep with for scent transfer; printed family photo | Attachment chemistry (oxytocin) is triggered by familiarity, not commercial value | |
Activity Bin | Storage container ₹500 | Any cardboard box; items: old playdough, completed puzzle, coloring sheet | Demand-free occupation is about task familiarity — novelty is counterproductive |
Zero-Cost Complete System: The entire Coming-Home Landing System can be assembled for ₹0 in 45 minutes using household items. "Every child — regardless of family income, geography, or access to therapy centers — deserves a prepared home environment." — Pinnacle Blooms Consortium | WHO Nurturing Care Framework
Safety First — Before You Begin
⚠️ Safety Gate
60 seconds before every arrival window
🔴 Red Zone — Do NOT Proceed If:
- Child is showing signs of acute illness (fever, significant GI distress) — medical needs take priority
- Decompression space contains any sharp, breakable, or hard-impact objects at child's height
- Weighted blanket weight exceeds 10% of the child's body weight
- Crash pad area has hard flooring exposed — ensure full soft landing coverage
- Child is currently in acute crisis (meltdown in progress) — focus on safety only
🟡 Amber Zone — Modify If:
- Child had a known difficult day at school — extend demand-free window to 90+ minutes
- Child is showing signs of illness beginning — reduce sensory intensity, offer comfort items first
- Sibling is also upset — ensure sibling has their own space before child arrives
- Primary caregiver is significantly dysregulated — your regulation is prerequisite to the child's
🟢 Green Zone — Ready When:
- Decompression zone is prepared and accessible
- Snack is out and ready
- Visual arrival sequence is visible at entry point
- Heavy work materials are in their designated spot
- Timer is visible and set (or ready to set)
- Sensory kit is accessible
- Connection objects are in place
- Demand-free activity bin is accessible
- All other demands on the child are removed for the transition window — homework discussions, chore reminders, sibling conflict mediation all postponed
🚨 Stop If You See:
- Child becomes physically unsafe — intervene calmly, ensure physical safety first
- Allergic reaction to any sensory material
- Significant respiratory distress from sensory or emotional response
📞 FREE Professional Guidance: 9100 181 181 — Pinnacle clinical team available for safety consultation
Set Up Your Space
Creating a predictable, supportive environment is the foundation for successful de-escalation and connection. Before your child arrives, take a few minutes to prepare a "safety anchor" in your home.
Clear the Path
Ensure the primary decompression area is free from clutter and potential hazards. A clean, open space signals safety to the nervous system.
Sensory Calibration
Adjust lighting and ambient sound. Soft, warm light and a quiet environment help regulate the child's sensory input upon entry.
Prepare Anchors
Place familiar comfort items—like weighted lap pads, favorite textures, or connection objects—within easy reach to provide immediate tactile support.

Is Your Child Ready? The Readiness Check
Pre-Flight
60 seconds before the car pulls in
Important: For this technique, "readiness" is not assessed for the child — the child arrives in varying states and the system accommodates ALL states. Readiness is assessed for the environment.
Environment Check | Status | If Not Ready — Quick Fix | |
Visual sequence visible at door | ✅ / ❌ | Tape printed sequence to door NOW (30 seconds) | |
Snack prepared and placed | ✅ / ❌ | Grab any reliable food item, place on counter now | |
Decompression zone accessible | ✅ / ❌ | Move one soft item into corner, clear floor space | |
Crash materials in position | ✅ / ❌ | Pull couch cushions to floor | |
Timer ready to start | ✅ / ❌ | Open timer app on phone, set to 45 min | |
Sensory kit accessible | ✅ / ❌ | Place fidgets + headphones in basket near zone | |
Activity bin accessible | ✅ / ❌ | Place 2 familiar items near decompression area | |
Sibling briefed/settled | ✅ / ❌ | Quick verbal reminder to sibling: "Landing pad time when [name] arrives" | |
Demands cleared | ✅ / ❌ | Mentally postpone all after-school expectations for 45 min | |
Your own regulation | ✅ / ❌ | 3 deep breaths. You're the co-regulator. |
🟢 8–10 checks
Full protocol — proceed
🟡 5–7 checks
Modified protocol — proceed with what's ready, complete remaining during transition
🔴 Fewer than 5
Minimum viable setup — crash cushions + snack + no demands; skip the rest today

Step 1: The Arrival Sequence
Step 1 of 6
0–5 minutes post-arrival
The landing begins before the door opens.
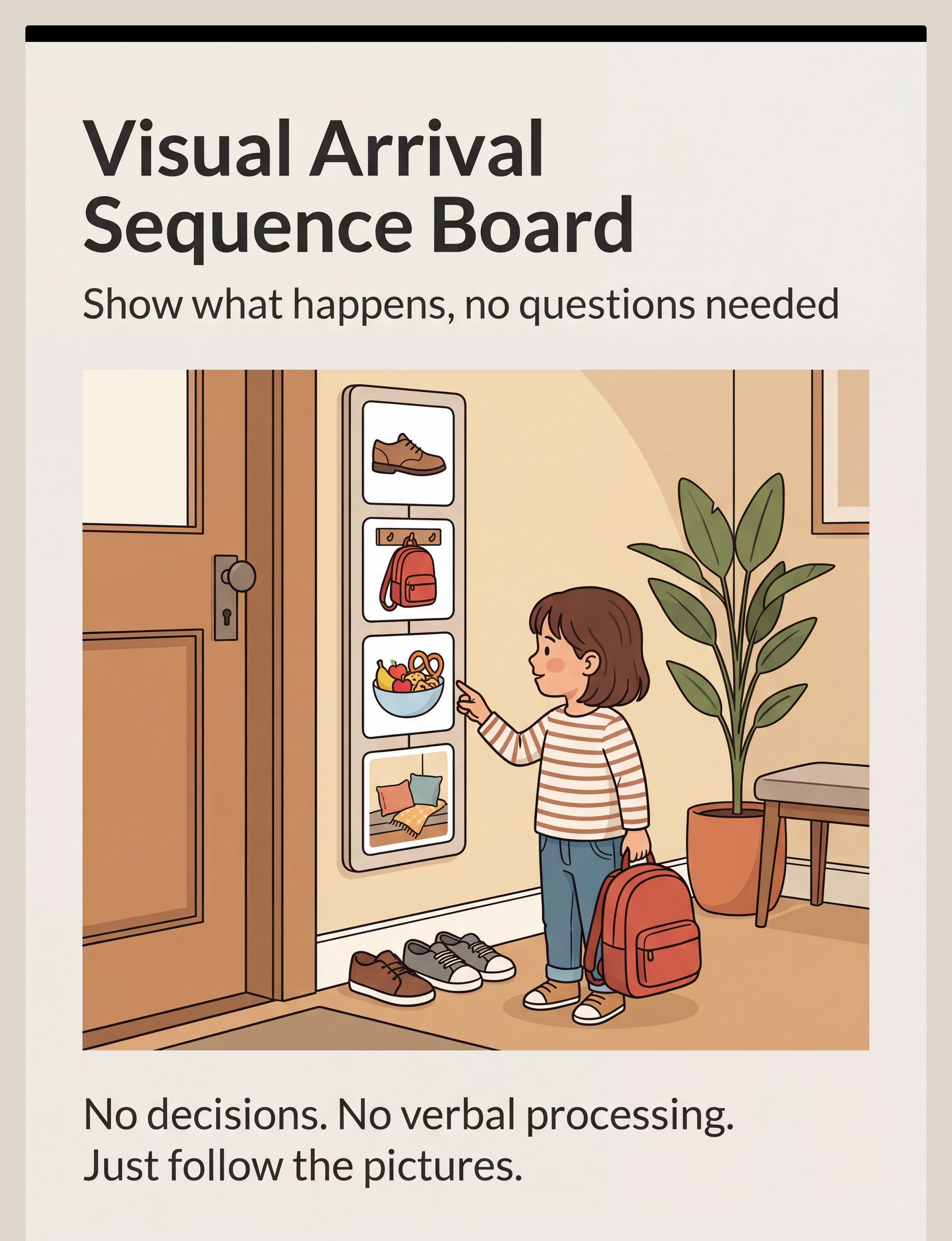
The child enters the house and encounters the Visual Arrival Sequence Board — the first thing at eye level. No words from you. No questions. The board shows what happens in order. The child follows it, or doesn't, without pressure.
Parent Positioning: Be present but not at the door. You are available, warm, visibly calm — but you are NOT the first thing they encounter. The visual sequence is. Your role in Step 1 is environmental: you set it up, then you step back.
❌ What NOT to Say
- "How was school?"
- "Did you have a good day?"
- "Come give me a hug."
- "Backpack goes on the hook."
- "What do you want for snack?"
✅ What TO Say (if anything at all)
- Soft, warm, low-demand: "You're home. It's okay."
- Point silently to the arrival sequence board if child is frozen
- Nothing at all is also a valid choice in minutes 1–5
The Arrival Sequence Board Shows:
- 👟 Shoes off → designated spot
- 🎒 Backpack → designated hook
- 🍎 Snack → counter (it's already there)
- 🛋️ Cozy space → decompression zone (go whenever ready)
If crashing happens first: This is fine. The sequence is a support, not a rule. If crashing happens first, it means proprioceptive needs are primary: move to Step 3 (heavy work) before expecting sequence-following.

Step 2 of 6
5–15 minutes post-arrival
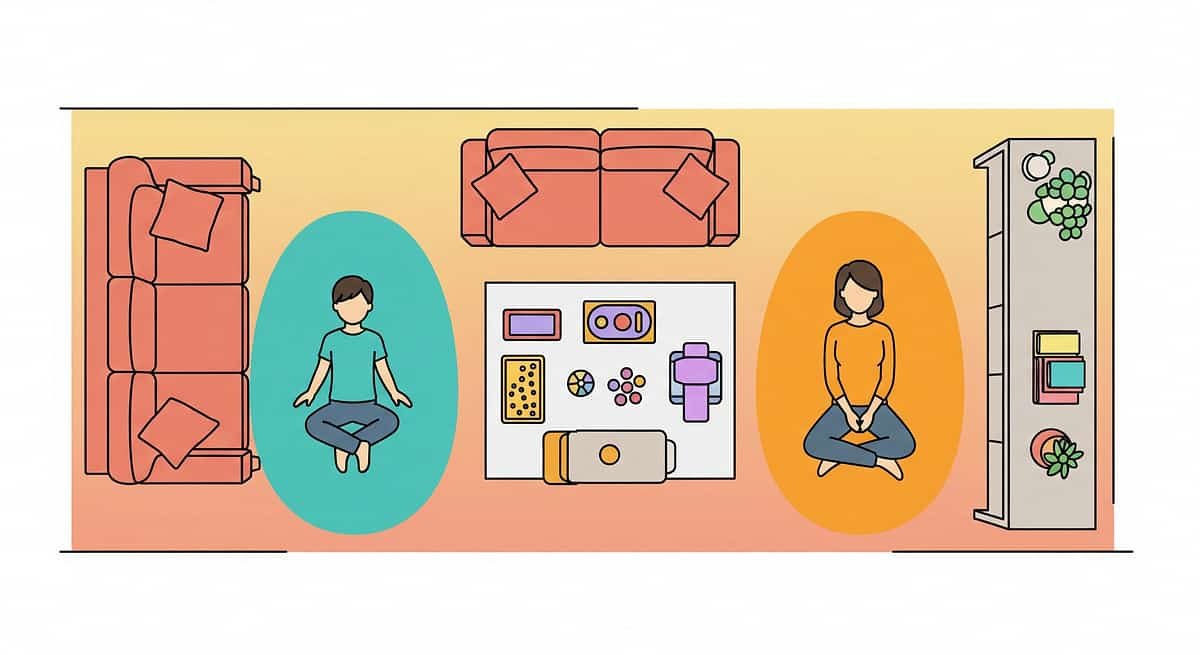
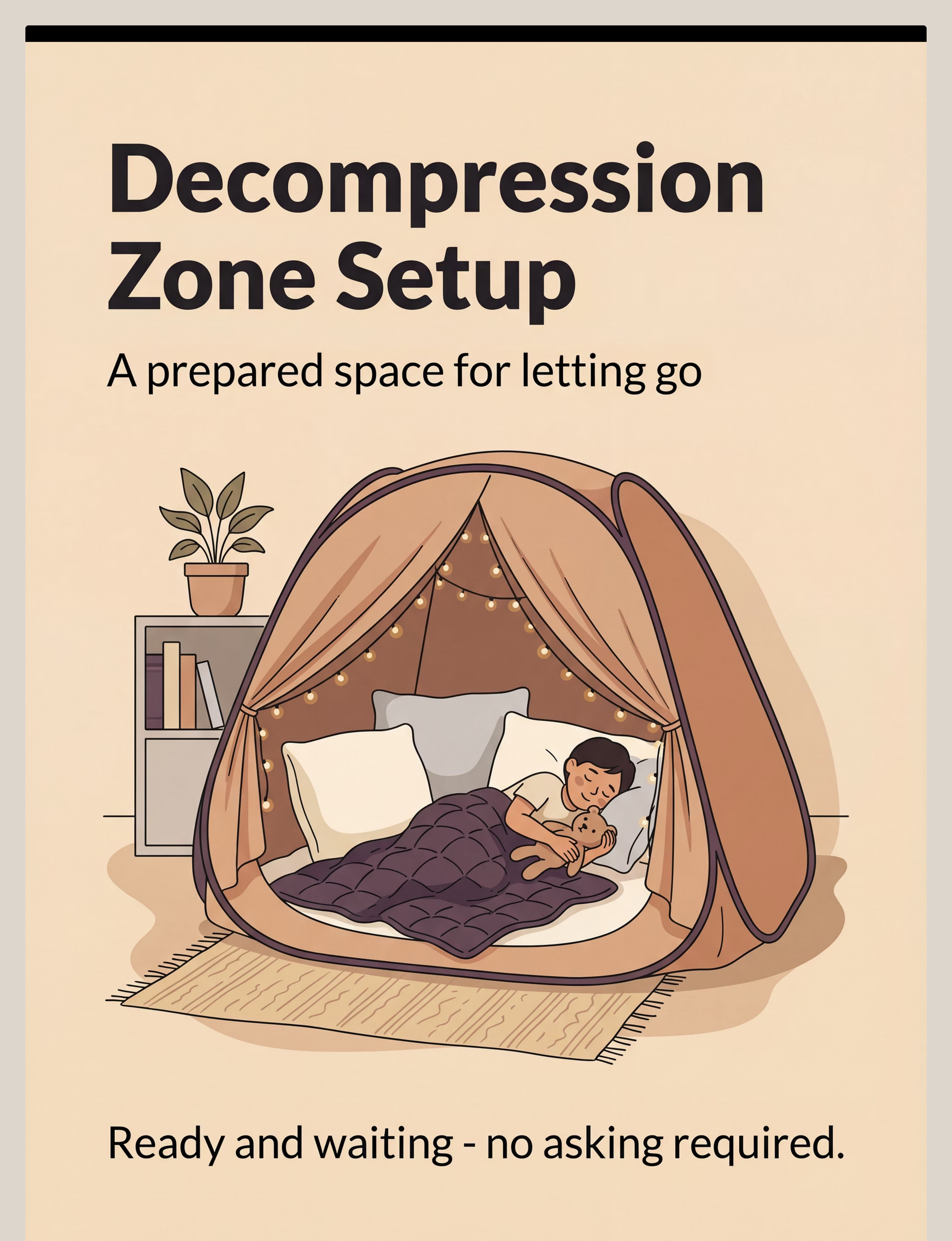
Step 2: The Decompression Zone
Once the immediate transition into the home is complete, the focus shifts to nervous system regulation. This space is designed to help the child shift from the high-demand environment of school to the safety of home.
Creating the Zone
This is a low-stimulus, high-comfort area. Use soft blankets, weighted items, or sensory tools that the child finds grounding. It is not for playing, but for resetting.
Parental Role
Maintain a "low-demand" presence. Sit nearby but do not initiate conversation. Offer physical support only if requested or signaled through their body language.
The Goal: Regulation, not productivity. Allow the child to remain in this zone for as long as their body requires before moving on to the next part of the afternoon routine.

Step 3 of 6
20–30 minutes post-arrival
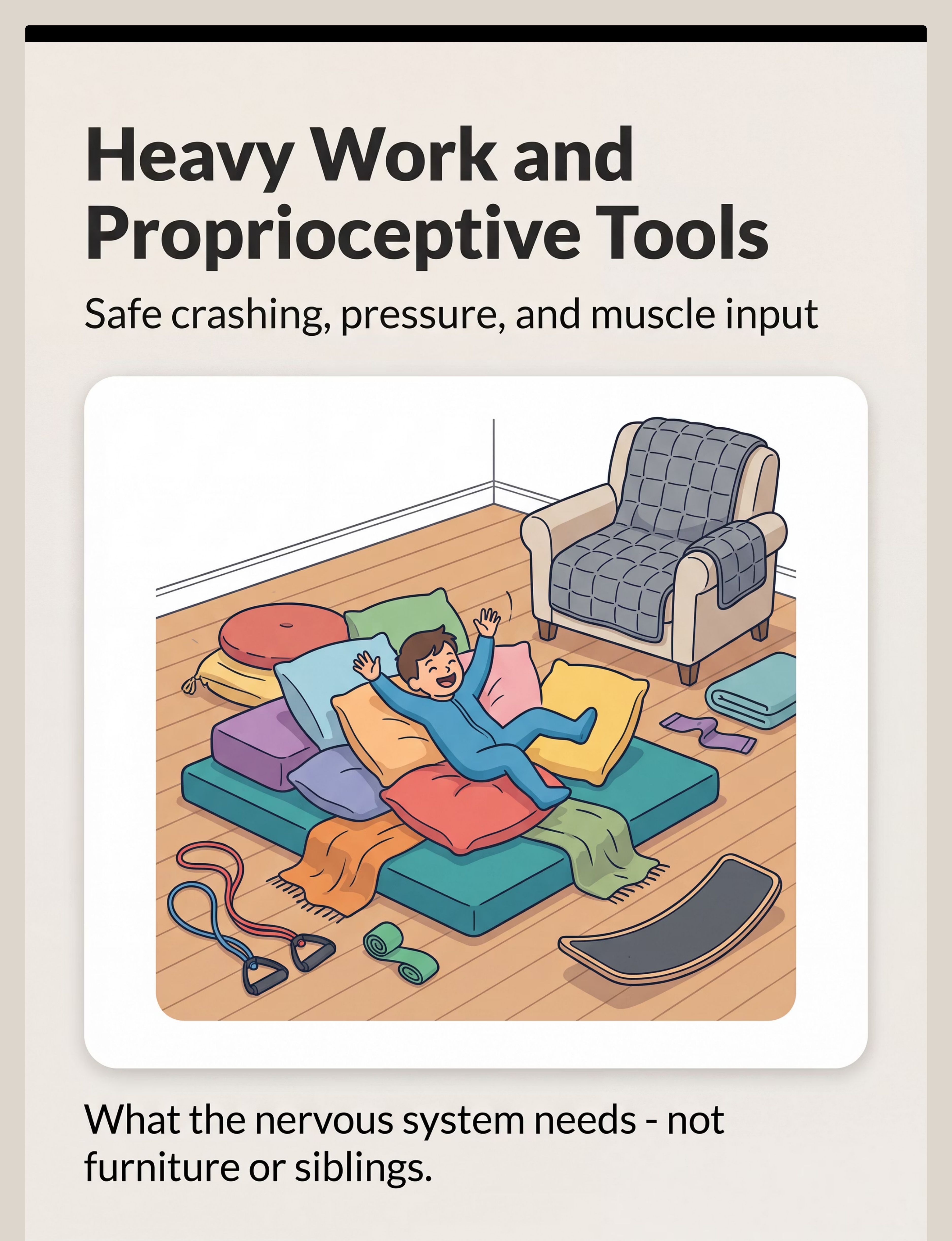
Step 3: Heavy Work & Sensory Discharge
After the nervous system has begun to regulate in the decompression zone, it is time to engage in "heavy work." This sensory-based activity helps the child organize their internal state by providing deep pressure and proprioceptive input, which is essential for processing the day's stress.
Physical Grounding
Incorporate rhythmic activities such as pushing a heavy laundry basket, crawling through a tunnel, or performing wall pushes. These movements help release stored tension.
Regulated Interaction
Participate alongside the child in a calm, non-verbal way. By mirroring their movements, you foster a sense of connection without the pressure of verbal communication.
The Goal: Proprioceptive organization. Heavy work helps bridge the gap between initial decompression and the more interactive, social parts of the afternoon.

Step 4: Regulation Visuals & Snack
Step 4 of 6
~20 minutes in — Consolidation Phase
The nervous system is beginning to land.
As the initial intensity of arrival subsides (typically 15–30 minutes post-arrival), two things emerge: the child begins reaching for the activity bin or lighter sensory tools, and blood sugar effects of the snack begin stabilizing emotional regulation. This is the consolidation phase.
Regulation Visual Check-In
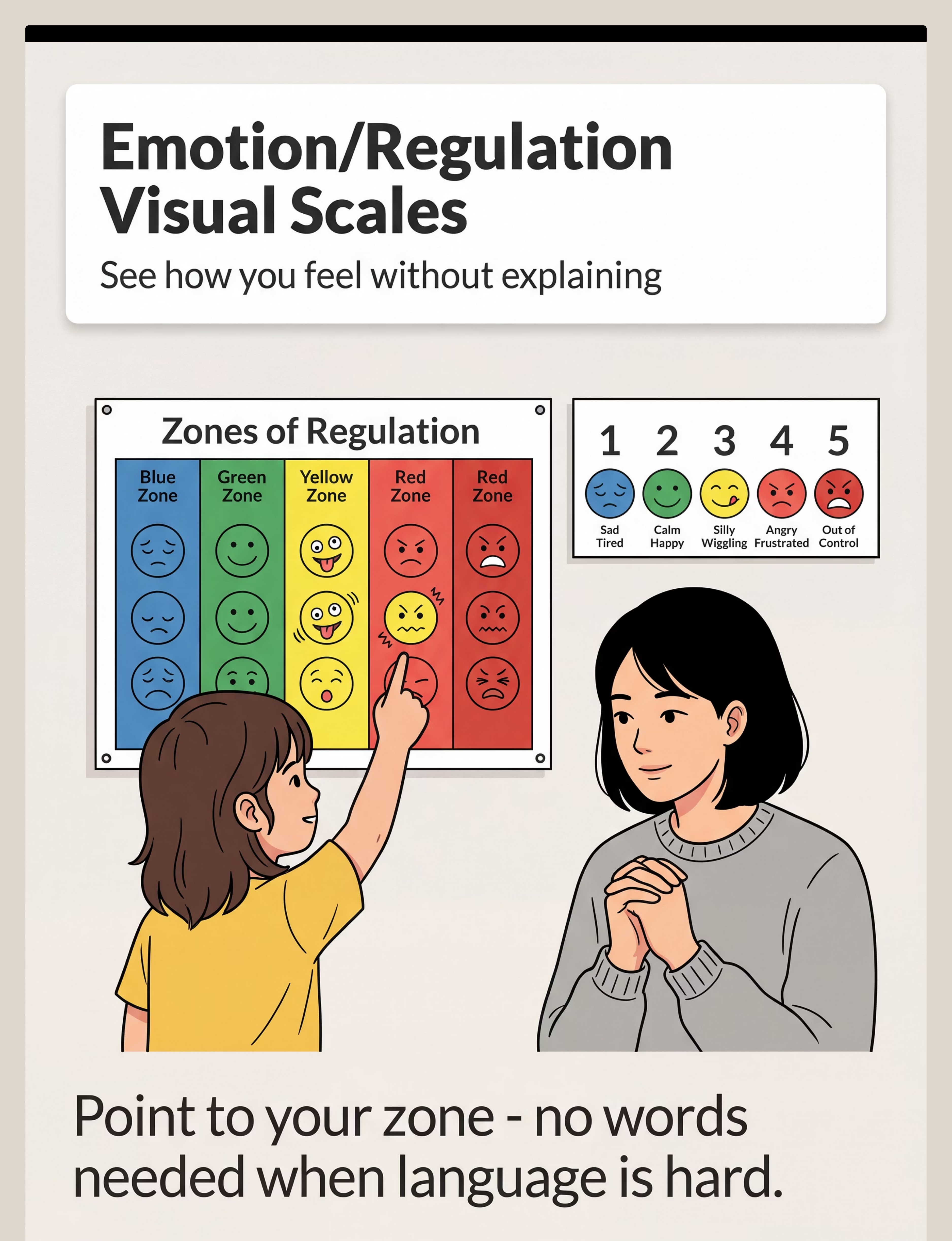
Point gently to the Zones of Regulation poster: (softly) "Which zone does your body feel like right now?"
- If child engages: note the zone, reflect warmly ("Yellow zone makes sense. School was a lot today.")
- If child ignores: do not repeat. The poster is information-gathering, not a demand.
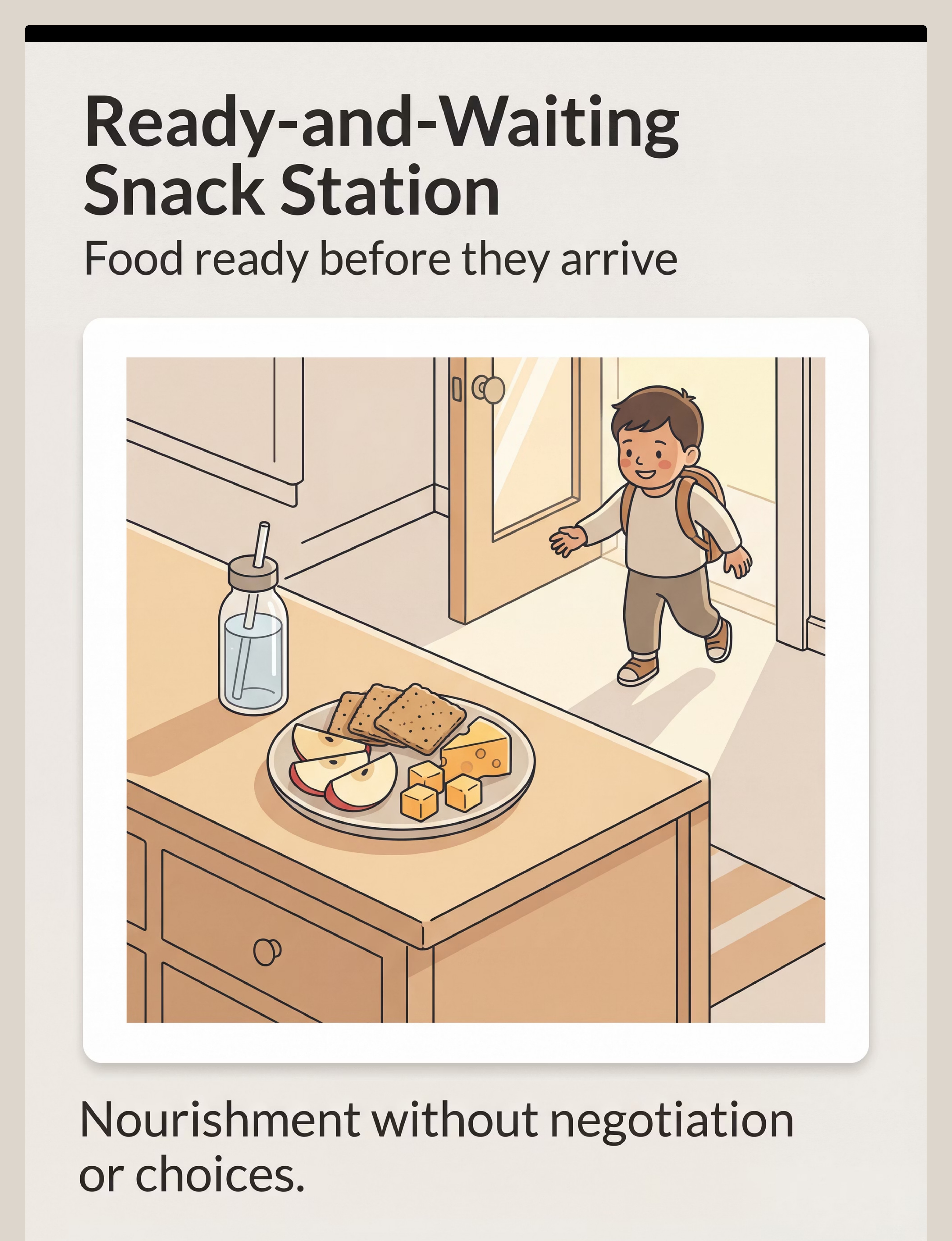
Snack Station Protocol
The snack has been available since arrival. By 15–20 minutes in, most children access it. If not: do not offer or draw attention repeatedly. Some children eat after proprioceptive discharge — sequence varies.
Demand-Free Activity Engagement
The "Busy Hands, Quiet Mind" window: the child's hands are occupied but the nervous system is continuing to regulate. Visual timer is visible — child can see remaining decompression time. No rush.
❌ Don't introduce homework
❌ Don't discuss the school day
❌ Don't ask about evening plans
❌ Don't invite siblings yet

Step 5: Reinforce & Celebrate the Landing
Step 5 of 6
30–45 minutes in — The Landing Moment
They landed. You both did this.
At some point in the 30–60 minute window, there is a visible shift. The child approaches you differently — less defended, less explosive, more present. They may come to you, speak a sentence, offer a small interaction, or simply sit near you companionably. This is the landing moment.
✅ Reinforcement Script (within 10 seconds of the shift)
- Warm, specific, low-intensity: "I can see you're settling. This is good."
- If child approaches you: "Hi. I'm glad you're here." Resist the urge to ask questions.
- Natural reinforcement: Your calm, warm presence and absence of demands IS the primary reinforcer.
🏆 What to Celebrate Internally (Parent's Private Victory Markers)
- Child used the crash pad instead of a sibling → environmental design working
- Child accessed the sensory kit independently → self-regulation skill emerging
- Child ate the snack without a battle → demand-free structure working
- Recovery took 35 minutes instead of 90 → progress
- You maintained your calm during the initial intensity → your co-regulation is the intervention
Token Economy (optional, discuss with your therapist): If using a token economy for older children (8+), the landing can earn tokens — NOT for "being good" during the dysregulation, but for using the decompression system tools. This builds intrinsic motivation toward self-regulation.

Step 6: The Cool-Down & Transition
Step 6 of 6
The Bridge to Evening
The session ends. The evening begins. The bridge between them matters.
✅ Transition Protocol
- Timer warning (2 min before): "Timer is almost done. Cozy time is finishing. Dinner comes next."
- End of timer: Do NOT immediately introduce demands. Allow 5-minute gentle bridge.
- Transition cue: "Your body got what it needed. Ready to come join me for snack/dinner?"
- Material put-away ritual: "Before we go, can the blanket go back?" Accept non-compliance without consequence today.
- First low-demand post-decompression activity: Shared snack, simple conversation about anything other than school, or parallel activity.
❌ What to Avoid
- Jumping immediately to homework after timer ends
- Starting with questions about school
- Introducing sibling conflict or house issues
- Expressing how difficult their arrival was
Typical Successful Afternoon Timeline
- 3:30 PM: Arrival + arrival sequence
- 3:35–4:15: Decompression zone + heavy work + snack
- 4:15–4:30: Activity bin/quiet engagement
- 4:30: Transition to evening
- 5:00: Low-demand family time
- 6:00: Dinner
- 7:00+: Homework (if cognitively accessible)
- 8:00: Evening routine

Capture the Data — Right Now
📊 60 Seconds of Data
GPT-OS® Tracker
60 seconds of data now saves hours of guessing later. Track 3 data points every day — this is what transforms individual sessions into a system that learns.
Arrival Intensity
Scale 1–5: 1 = calm arrival, 3 = moderate dysregulation, 5 = full collapse
Recovery Time
Minutes from arrival to visible regulation shift. This is your primary success metric — watch it decrease week over week.
Materials Used
Which of the 9 materials were accessed today: Arrival Sequence | Decompression Zone | Snack | Heavy Work | Timer | Sensory Kit | Regulation Visual | Connection Object | Activity Bin
Tracking Tool Options:
📊 PDF Tracking Sheet
📱 GPT-OS® App
📝 Simple Notebook
Date | Intensity (1–5) | Recovery minutes | Materials used
After 2 weeks of tracking, you will see which materials correlate with faster recovery, which days are harder, and pattern data your Pinnacle therapist can use to refine the system. 📞9100 181 181 — Share your tracking data with a Pinnacle therapist for interpretation.

What If It Didn't Go As Planned?
Therapy is a journey of trial and error. If a session didn't go as expected, it’s not a failure—it’s a data point. Use this diagnostic approach to recalibrate your strategy for the next attempt.
1. Check the Environment
Was the space too loud, too bright, or too crowded? Sometimes a simple adjustment to lighting or sensory input makes the difference between dysregulation and engagement.
2. Simplify the Task
If the activity felt overwhelming, break it down further. Reduce the number of steps, shorten the time, or offer more support to rebuild confidence.
3. Evaluate the Timing
Did we start at the right moment? Transitions are difficult; ensure there was enough 'buffer time' provided before beginning the main activity.
Remember: You are the expert on your child. If you're stuck, call your Pinnacle therapist at 9100 181 181 to walk through these variables and adjust your plan together.
Adapt & Personalize
Customization
No two nervous systems are identical
The Coming-Home Landing System is designed to be tuned to your child's specific sensory profile. Use these variations to calibrate each material to their actual needs.
🔴 Sensory Seeker
Under-Responsive, High-Intensity Profile
- Lead with heavy work BEFORE decompression zone — crash pad must be used first
- Body sock and resistance tunnel are primary tools, weighted blanket secondary
- Timer may need to be 60+ minutes
- Activity bin: more active/tactile options (kinetic sand, clay, fidgets with resistance)
- Regulation scale: use energy meter rather than zones
🔵 Sensory Avoider
Over-Responsive, High-Sensitivity Profile
- Decompression zone darkness and quiet are primary — heavy work tools only if sought
- Arrival sequence must be ultra-minimal (2 steps maximum)
- Snack should be ultra-familiar and single-item
- Connection object IS a primary tool, not optional
- Timer: long and visible but not prominently featured — avoid time pressure
🟡 Mixed/Fluctuating
Variable Presentation
- Prepare ALL options — let child navigate by instinct
- Watch behavioral patterns across 2 weeks to identify most consistently used tools
- Discuss with OT: formal sensory profile assessment (Sensory Profile 2 / SPM-2)
Age-Based Modifications
Ages 4–6
Photo-only visual sequence. Decompression zone is primary. Heavy work embedded in fun (crash into "cloud" cushions). Timer: 5-minute segments max.
Ages 7–10
Core protocol. Child begins to identify own needs from sensory kit. Regulation visuals highly effective. Timer: 30–45 minutes.
Ages 11–14
Greater autonomy — child negotiates decompression duration. Regulation visuals upgrade to self-advocacy language. Technology (preferred music) may be part of decompression kit.
Week 1–2: What to Expect
Progress Phase 1
System Establishment
You are planting. Don't look for the harvest yet.
15%
System Establishment Phase
Weeks 1–2 progress benchmark
✅ What "Progress" Actually Looks Like in Weeks 1–2
- Child crashes into designated crash pad instead of into furniture or sibling — THIS IS SUCCESS
- Child picks up one item from sensory kit independently — THIS IS SUCCESS
- Recovery time decreases by even 10 minutes — THIS IS SUCCESS
- Parent maintained calm during one intense arrival — THIS IS SUCCESS
- Child moved toward decompression zone at any point during transition window — THIS IS SUCCESS
Not "Progress" Yet — Managing Expectations
- Child independently following all 9 materials — not expected yet
- Meltdowns completely eliminated — not the goal at this stage
- School communication about behavior improving — too early to measure
- Child articulating their needs with words — weeks 4–8 territory
Parent Emotional Preparation
The first two weeks may actually feel harder as you establish the system. You are changing a long-established pattern. Consistency is the intervention. A system that runs for 14 consecutive days, even imperfectly, creates more change than a perfect system run 3 times.

Week 3–4: Consolidation Signs
Progress Phase 2
Neural Pathways Forming
The neural pathways are forming. Look for these signs.
40%
Consolidation Phase
Weeks 3–4 progress benchmark
Consolidation Indicators — the ones most parents miss:
🧠 Child moves toward decompression zone without prompting
The strongest early indicator. The brain has mapped "arrive → decompression zone" as a reliable pattern.
🧠 Meltdown recovery time noticeably shorter
What took 90 minutes in week 1 now takes 45. This is measurable with your tracking data.
🧠 Child points to or uses regulation visual independently
Emotional self-awareness emerging. Language may still be unavailable but visual communication is functioning.
🧠 Child makes one spontaneous post-decompression interaction
They come to find you, make brief eye contact, offer something. The reconnection phase emerging.
🧠 You notice you're less anxious at 2:45 PM
Your co-regulation is improving, which directly improves child outcomes.
If child is actively seeking MORE time in decompression zone: Extend without hesitation — needs are larger than expected. If recovery times have plateaued, review crash pad usage — proprioceptive needs may need more attention. Discuss with your OT.
Week 5–8: Mastery Indicators
Progress Phase 3
Observable, Measurable, Real
75%
Mastery Phase
Weeks 5–8 progress benchmark
Independent Decompression Initiation
Child moves to decompression zone independently upon arrival, without parent prompting, on ≥4 of 5 school days per week.
Recovery Time Target Met
Transition from arrival intensity to regulated state occurs within 45 minutes on ≥3 of 5 school days.
Material Self-Selection
Child independently selects and uses at least 2 materials from the decompression system on most days.
Communication Emergence
Child uses regulation visual (or words) to communicate emotional state during transition window, unprompted, at least once per week.
Generalization Indicator
Child begins using language from transition system in other contexts — "My body needs a crash" / "I'm in red zone" said spontaneously outside the home transition.
🏆 Mastery Unlocked: All 5 criteria met for 2 consecutive weeks = mastery for this technique. Recommended next: I-790 Homework Transition Support System — the next challenge in the daily sequence.
Celebrate This Win
You spent 8 weeks showing up. Every single afternoon. That is extraordinary.
"Our afternoons used to be war zones. We got them back. It took 6 weeks and a pile of cushions."
Your child now has a landing system. What used to be a daily crisis is now a manageable transition. What used to take 90 minutes of explosive recovery now takes 35. Your home has become what it was always supposed to be — a safe, regulatory sanctuary that your child trusts.
Removed verbal demands at the door
Provided a safe decompression space
Met proprioceptive needs safely
Delivered nourishment without negotiation
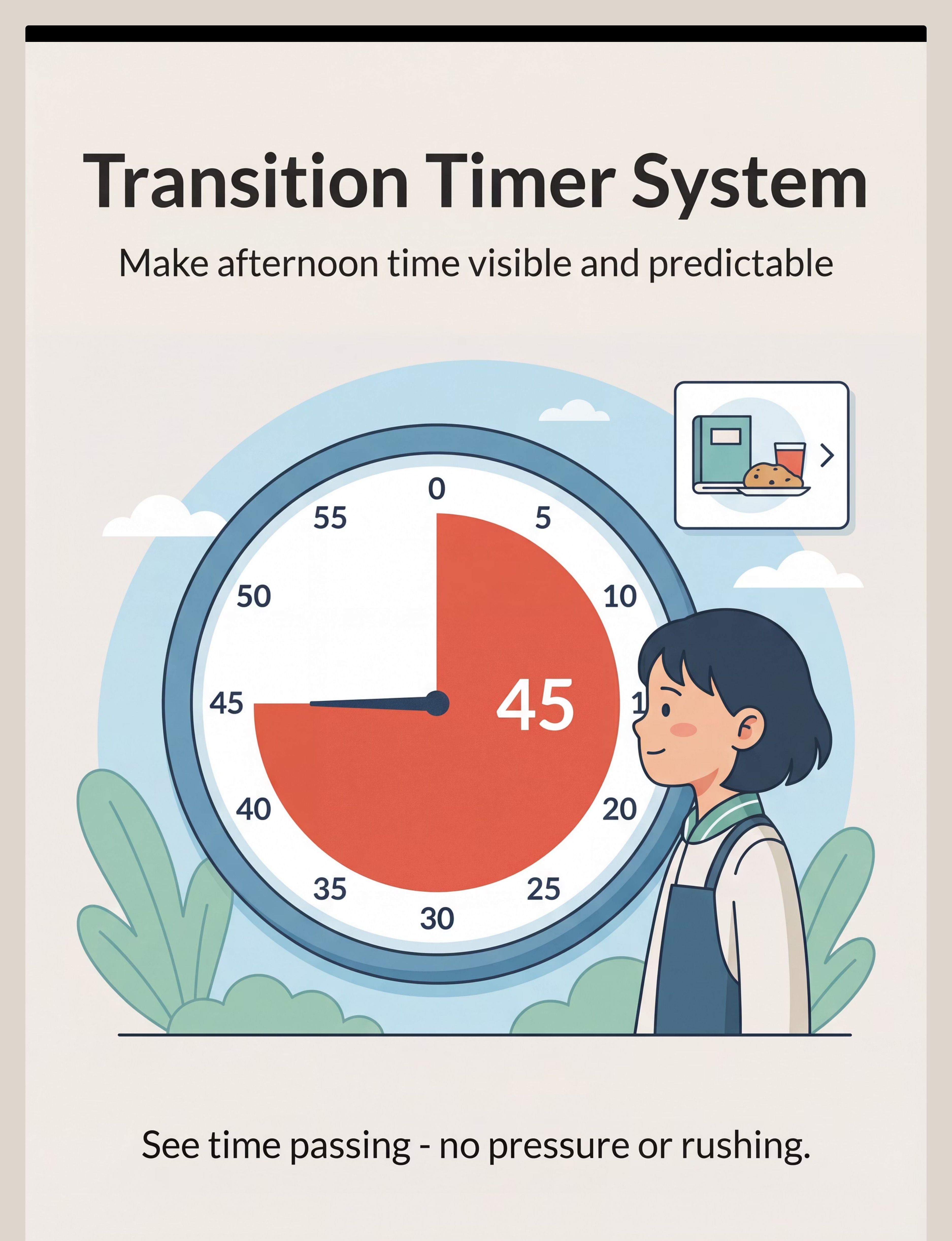
Made time visible and non-threatening
Maintained connection without imposing demands
This is not a small thing. This is a family transformation.
Photo/Journal Prompt: "Before we started, afternoon arrivals looked like ___. Now, they look like ___. My child learned ___. I learned ___."

Red Flags — When to Pause
🚨 Safety Alert
Even after progress, some signs mean: stop and call us
🚨 Red Flag 1: Escalating Physical Aggression
If meltdown intensity is increasing (not decreasing) over 4+ weeks, AND physical aggression toward self, others, or property is intensifying — this warrants OT and behavioral psychology review. The system needs clinical recalibration.
🚨 Red Flag 2: Complete Shutdown / Non-Eating / Non-Drinking
If child is consistently refusing all food and fluid during the transition window for 3+ days — medical consultation needed. Dehydration and hypoglycemia compound dysregulation.
🚨 Red Flag 3: School Refusal Emerging
If child begins resisting going to school due to fear of the afternoon — this requires integrated school + clinical + family intervention. Do not manage this with home environment changes alone.
🚨 Red Flag 4: Sleep Disruption
If ASRC intensity is causing sleep onset difficulties, discuss with NeuroDev pediatrician. Sleep disruption creates a cycle that intensifies ASRC.
🚨 Red Flag 5: Regression During System Use
If skills that were present before starting this system have decreased — this requires immediate clinical review. Regression is not expected with this protocol.
🚨 Red Flag 6: Parent / Sibling Safety
If family members are being physically harmed during transition — safety is non-negotiable. Behavioral crisis protocol supersedes this system. Contact Pinnacle immediately.
🟡 Self-Resolve
Adjust system, use troubleshooting guide (Card 21), add 2 weeks
🟠 Teleconsult
Book via pinnacleblooms.org — describe the red flag specifically
🔴 Clinic Visit
In-person OT + ABA evaluation at nearest Pinnacle center
🚨 Emergency
Child/family safety: contact emergency services
📞9100 181 181 — 24×7, 16 languages, free
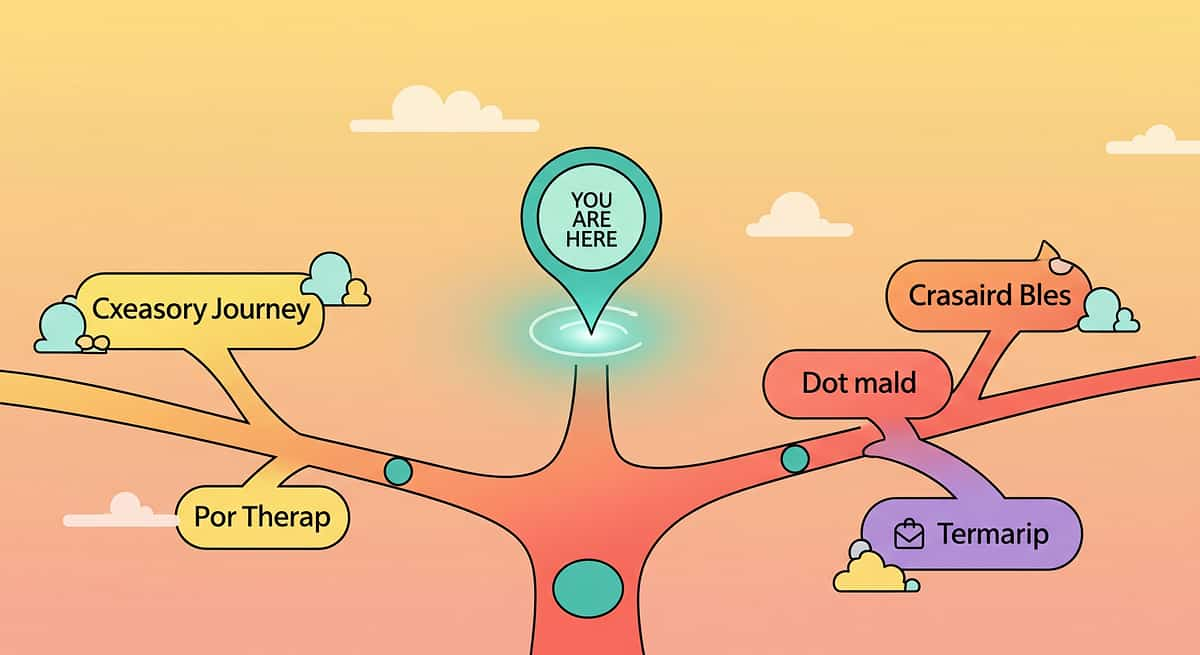
The Progression Pathway
📍 You Are Here
I-789 — Coming Home Landing System
You are here. Here is where you're going.
Strong Sensory Needs
→ Domain A Sensory Deep-Dives
→ I-792 Sensory Decompression Protocol
→ I-792 Sensory Decompression Protocol
Strong Emotional Needs
→ Domain C Emotional Regulation
→ C-254 Emotion Regulation at Home
→ C-254 Emotion Regulation at Home
Strong Behavioral Patterns
→ Domain D Behavioral Flexibility
→ I-791 Dinner Transition Support
→ I-791 Dinner Transition Support
Ready for Independence
→ I-793 Self-Regulation Independence
"A child who can navigate the coming-home transition independently has mastered one of the highest-demand daily regulatory events in childhood. This skill generalizes to all transitions — school changes, home moves, schedule disruptions, and eventually, adult life transitions."
Related Techniques in This Domain
Same System. Different Moments. All Connected.

🟢 INTRO | I-787 Morning Transitions
Morning Transitions & Routine Launch. Materials you already own: Visual schedules, timer.

🟢 INTRO | I-788 Leaving for School
Managing Separation Anxiety. Materials you already own: Visual sequence, comfort object.

🔵 CORE | I-789 ← YOU ARE HERE
9 Materials That Help With Coming Home. All 9 materials active.

🔵 CORE | I-790 Homework Transitions
Materials you already own: Timer, regulation visuals, demand-free activities.

🔵 CORE | I-791 Dinner & Mealtime Transitions
Materials you already own: Visual schedule, snack station principles, timer.

🟡 ADVANCED | I-792 Self-Regulation Independence
Prerequisites: I-789 mastery recommended.
After completing I-789, you own materials sufficient to begin I-790 and I-791 without additional purchase. The 9-material Coming-Home system is the foundation of the entire daily transitions architecture. Browse Full Domain →
Your Child's Full Developmental Map
One technique. One domain. One piece of a complete plan.
The coming-home transition is not an isolated problem — it is a window into the child's entire developmental profile. ASRC severity is directly correlated with Sensory Processing (Domain A), Emotional Regulation (Domain C), Communication readiness (Domain H), and Family System functioning (Domain L).
A complete Pinnacle AbilityScore® assessment maps all 12 domains simultaneously and generates a personalized, sequenced intervention plan through GPT-OS® — showing which techniques, in which order, for this specific child.
Families Who've Been Here
Real Families
Real Afternoons. Real Change.
Mumbai, Maharashtra
Before: "3:00 PM was a war zone in our house. Arjun (8, ASD Level 2) would come in the door and within 60 seconds, he'd thrown his backpack, screamed at his little sister, and was lying on the kitchen floor refusing everything. This went on every day for two years. His teachers thought he was thriving — he was. He was managing everything at school perfectly, holding it all in, and releasing it all the moment he stepped inside. We walked on eggshells from noon onward."
After (Week 6): "The arrival sequence board at the door was the first thing that made any difference. He doesn't follow all of it, but he sees it — he knows what to expect. We set up a tent with his favorite blanket and a basket of things. The first week he still collapsed, but into the tent instead of onto us. By week four, he was going straight to the tent himself. Recovery went from 90 minutes to 25 minutes. Our evenings are different now."
Therapist's Note:"This family's success demonstrates the core principle: prepared environments reduce regulatory demand. The child didn't change — the home changed, and the child's nervous system responded." — OT Consultant, Pinnacle Blooms Network®
Hyderabad, Telangana
Before: "My daughter (10, ADHD + sensory processing differences) would come home and literally crash into walls. The couch, the door, everything. Her brother had started hiding in his room by 3:10 PM. I tried snacks, I tried screen time, I tried sending her to her room. Nothing was consistent."
After (Week 4): "The crash pad was the game-changer. She'd been looking for something to crash INTO — I just never had the right thing. Old couch cushions on the floor, a body sock from Amazon (₹800), and her weighted blanket. She crashes into her zone for 15 minutes and comes out completely different. Her brother stopped hiding. We're actually having dinner together now."
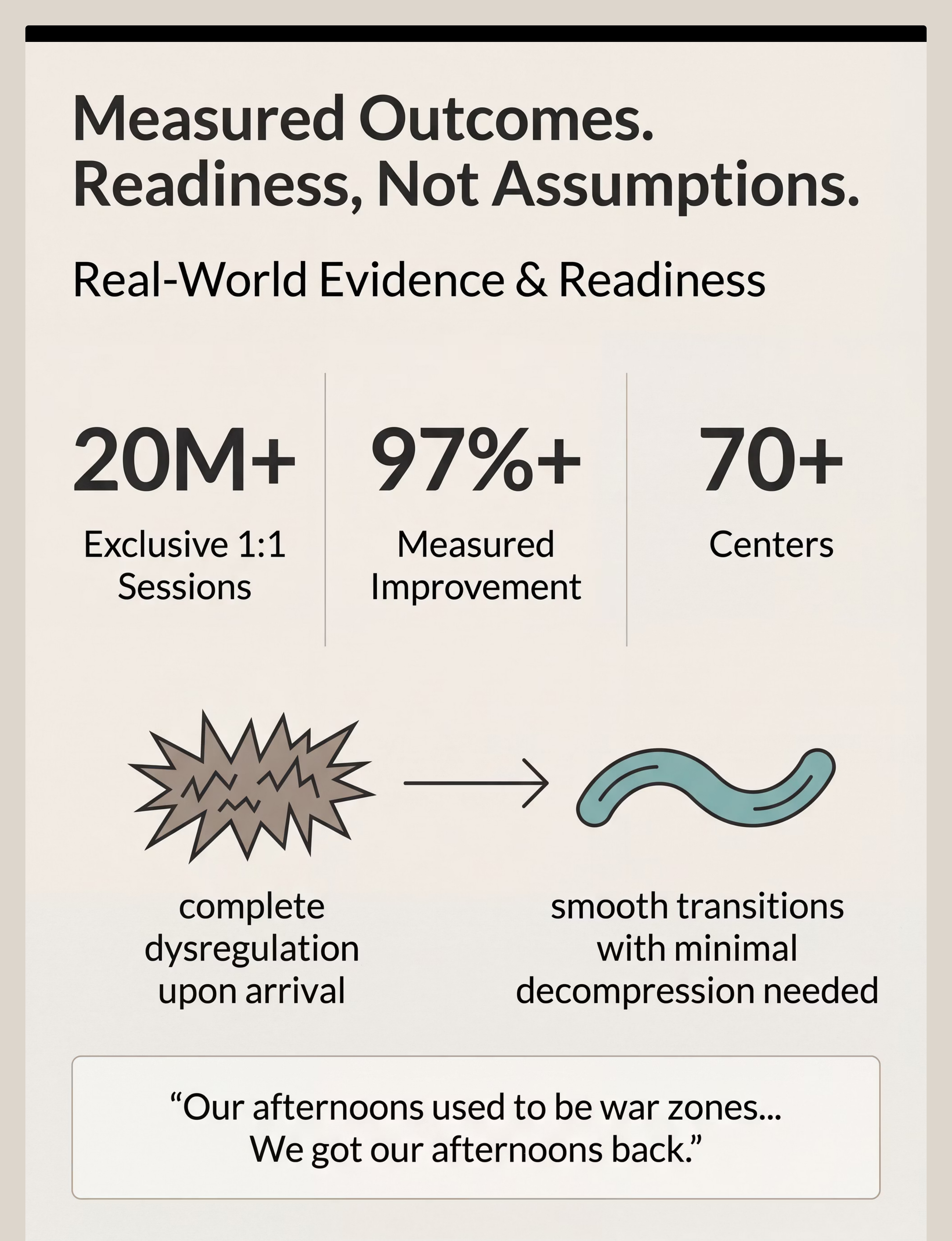
"Our afternoons used to be war zones. We got them back. It took 6 weeks and a pile of cushions."
Outcomes represent individual experiences. Individual results vary by child profile, sensory needs, family implementation consistency, and clinical support. Statistics aggregate outcomes across Pinnacle Blooms Network®.

Connect With Other Parents
Community
Isolation makes this harder. Community makes it possible.
WhatsApp Support Group
After-School Transition Support — Pinnacle Parent Community. Hindi | Telugu | Tamil | Kannada | Bengali | English | 12+ languages.
Online Forum
Pinnacle Parent Forum — Daily Transitions Thread. Share your tracking data, ask questions, celebrate wins.
Peer Mentoring
Connect with an experienced parent who has completed the I-789 system. "Match me with a parent who has been through this."
Local Parent Meetups
Pinnacle centers in 70+ locations host monthly parent support groups. Find your nearest center.
"The parents in this community understand because they are living it. Their data, their adaptations, their victories — they are your most relevant resource."
Your Professional Support Team
Home Intervention + Professional Support = Maximum Impact
Pediatric OT
Sensory profile assessment, decompression zone design, proprioceptive protocol calibration. Primary lead for the I-789 system.
BCBA / Behavior Therapist
Arrival sequence design, demand reduction protocol, data analysis. Governs transition schedule and reinforcement delivery timing.
Pediatric Psychologist
Family systems support, sibling management, parental burnout. The emotional architecture of the home environment.
NeuroDev Pediatrician
When ASRC severity warrants medication or sleep review. Coordinates educational accommodations that reduce daily regulatory load.
The Home + Clinic Formula
Home-based intervention addresses 24×7 — the daily, consistent application that creates neural pathway change. Clinical sessions address assessment, calibration, and escalation. Together, they are exponentially more effective than either alone.
Access Your Support Team
📞9100 181 181 — FREE | 16 Languages | 24×7
The Research Library
For parents who want to understand the science behind every choice
Study 1 — Systematic Review (Highest Level)
📚Sensory Integration Intervention in Children with Autism Spectrum Disorder | Children, 2024 | PMC11506176
16 articles (2013–2023) confirm sensory integration intervention meets evidence-based practice criteria for ASD across participation, sensory, motor, and adaptive behavior outcomes. PubMed →
Study 2 — Meta-Analysis
📚Effectiveness of Sensory Integration Therapy in Children with Autism | World Journal of Clinical Cases, 2024 | PMC10955541
Across 24 controlled studies, sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and gross/fine motor skills. PubMed →
Study 3 — Indian RCT
📚Home-Based Sensory Interventions in Indian Children with ASD | Indian Journal of Pediatrics, 2019 | Padmanabha et al.
Parent-administered home sensory interventions demonstrated significant, measurable outcomes in Indian pediatric population. Validates home execution viability. DOI →
Study 4 — WHO/UNICEF Care for Child Development
📚Care for Child Development Package, 2023 | PMC9978394
Implemented across 54 LMICs. Responsive caregiving and environmental preparation are primary modifiable predictors of developmental outcomes.
Study 5 — Evidence-Based Practice Classification
📚National Clearinghouse on Autism Evidence and Practice (NCAEP) Report, 2020
Visual supports, self-management, and structured environmental interventions classified as evidence-based practices for autism. Transition support specifically cited. NCAEP 2020 →
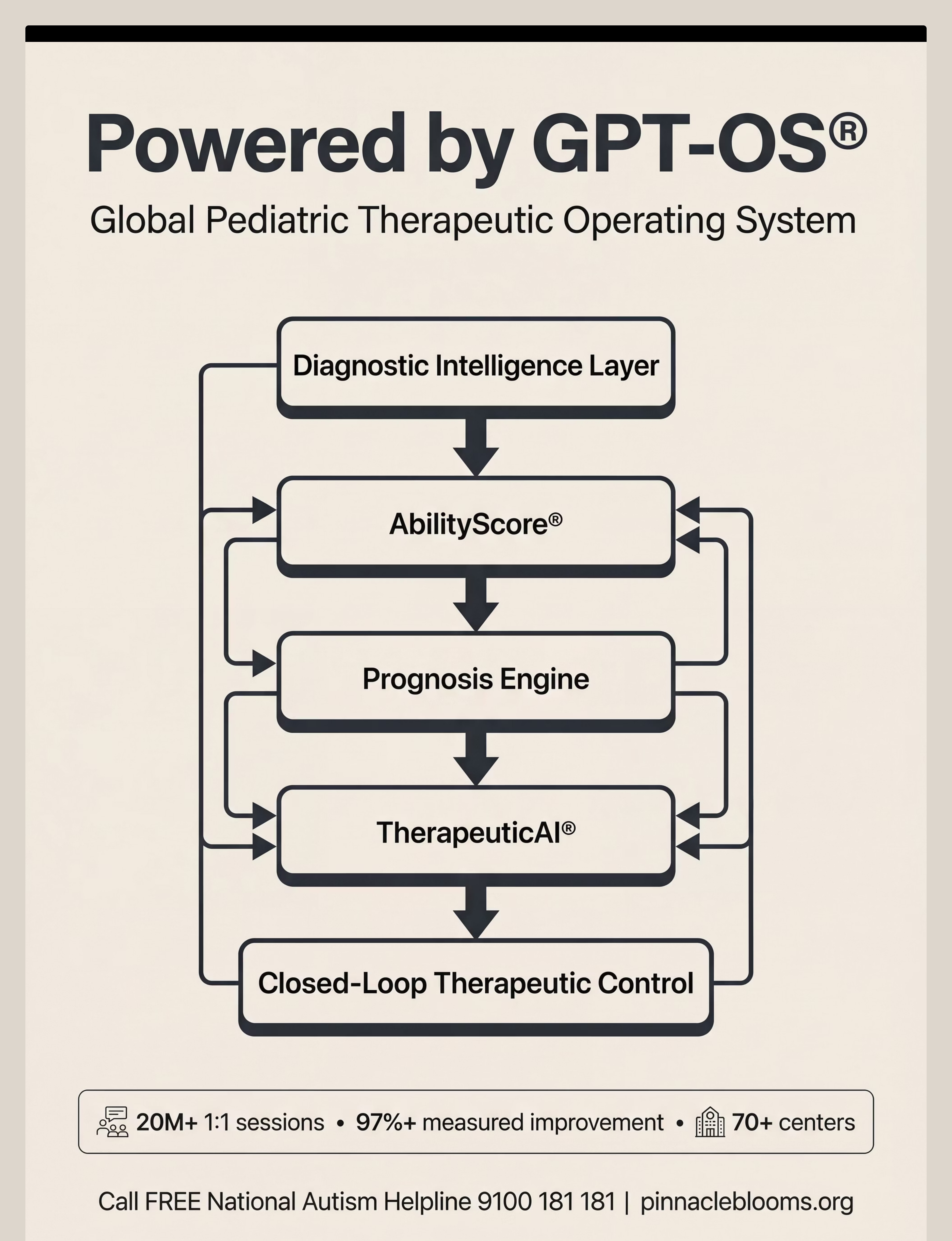
How GPT-OS® Uses Your Data
Technology
Every session you track makes the system smarter
When you log your afternoon sessions, your data joins a network of 20M+ sessions. Here's what GPT-OS® learns from your I-789 data specifically:
📊 Material Correlation
Which materials in your child's system show the strongest correlation with faster recovery
📈 ASRC Trending
Whether your child's transition intensity is trending up, down, or stable over time
🔍 Profile Comparison
How your child's transition patterns compare to similar profiles across the network
⚙️ System Calibration
When to recommend increasing or reducing specific material components
🔔 Predictive Flagging
School events that historically worsen transition (term start, exam periods)
Privacy Assurance: All data is anonymized and aggregated for population-level analysis. Individual family data is visible only to you and your designated Pinnacle clinical team. DPDP Act compliant (India Digital Personal Data Protection Act). GDPR-aligned for international families.
"Your data helps every child like yours." Connect Your Data to GPT-OS® →

Watch the Reel
🎬 Reel I-789
75–85 seconds | 16 languages
See it in motion. The reel that brought you here.
The I-789 Reel features a Pinnacle OT specialist demonstrating all 9 materials in a real home environment. Each material is shown in action — not in a clinic, not in a therapy room, but in the kind of home your child actually comes back to.
Visual Arrival Sequence Board in use at door
Decompression Zone — child entering and settling
Ready Snack Station — food available, no interaction required
Heavy Work Tools — crash pad, body sock, proprioceptive input
Transition Timer — visual timer running in decompression zone
Sensory Regulation Kit — child self-selecting tools
Emotion/Regulation Visuals — Zones of Regulation in use
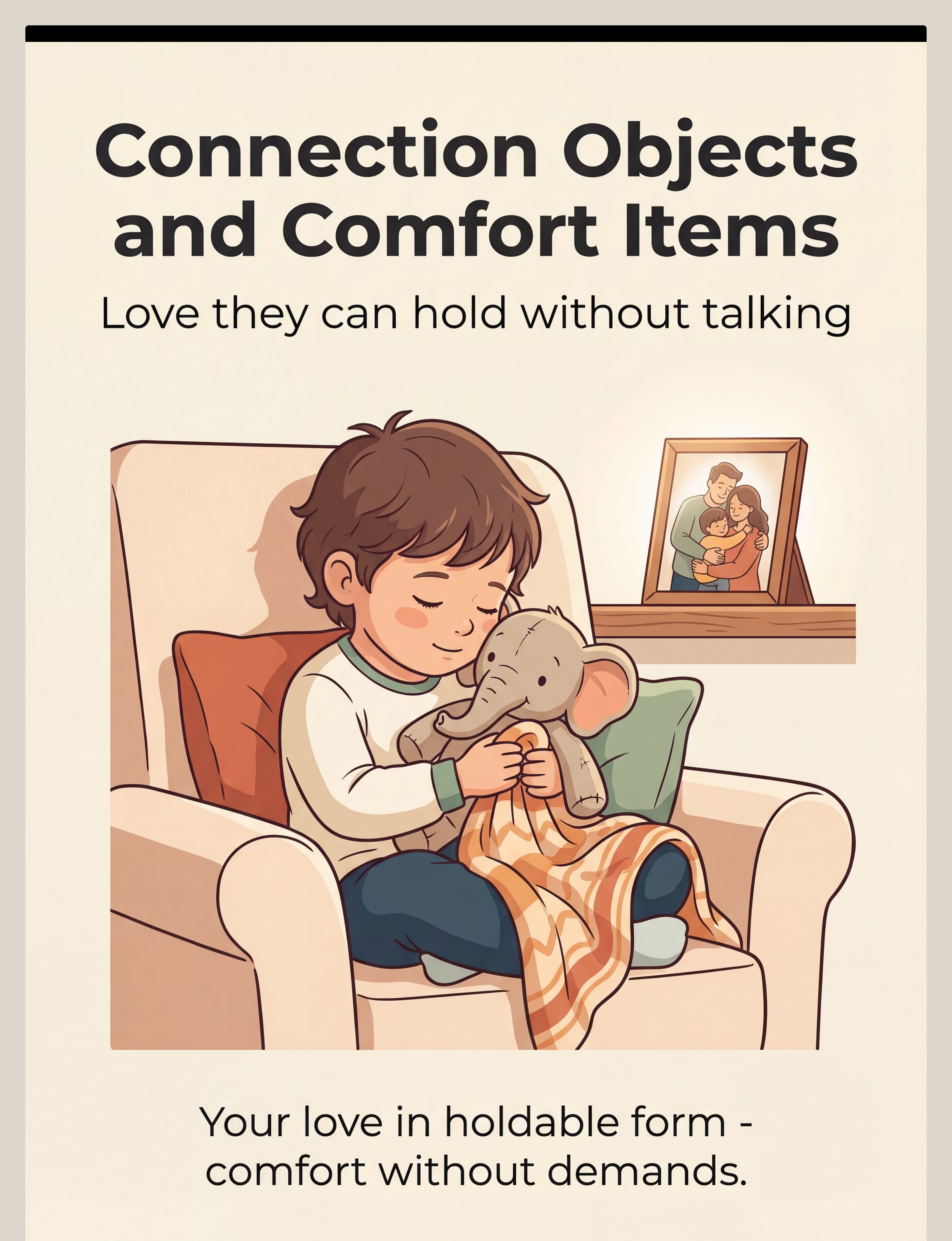
Connection Objects — comfort item providing regulation
Demand-Free Activity Bin — quiet occupation
"After-school restraint collapse is one of the most misunderstood daily experiences in families with neurodevelopmental differences. The child who holds it together all day deserves a home prepared to receive them — not another set of demands. These 9 materials build that receiving system."
— Pinnacle Blooms OT Specialist
Frequently Asked Questions
The questions every parent asks
Answers from 20 million sessions
Q1: My child's teacher says they're perfectly fine at school. Why is home so different?
This is the defining feature of after-school restraint collapse — not a contradiction of it. Children who appear to function well at school are often operating at maximum regulatory capacity to do so. Home is where the regulation releases. A child who is "perfectly fine at school" and explosive at home is not a parenting problem — it is a regulatory resource problem. School consumes every reserve. Home is where those reserves are replenished. The goal of this system is to optimize the replenishment process.
Q2: How long should the demand-free window be?
Begin at 45–60 minutes regardless of your schedule. This may feel inconvenient — it is necessary. As recovery time decreases, you can observe whether a shorter window maintains the same outcome. For children with high-intensity ASRC profiles, the window may need to be 90 minutes. The window is determined by the child's recovery time, not the adult's schedule preferences.
Q3: Should I talk about what happened at school during the transition window?
Not during the transition window. The question "How was school?" is a verbal demand on a system with zero verbal processing reserves. Wait until the child is demonstrably regulated — typically 45–90 minutes post-arrival. Many children with autism never fully process and verbalize their school experience. Alternative connection approaches (asking about one specific, concrete thing; showing interest in their current activity; parallel play) are more effective and less demanding.
Q4: My child uses the decompression zone but then still won't do homework. Help.
The goal of this system is not to make homework possible immediately after arrival. Homework capacity returns on its own timeline — typically 60–120 minutes post-arrival for children with high ASRC intensity. If homework is required earlier, consult with your child's school about (a) reducing homework load, (b) shifting homework expectations to the next morning, or (c) providing in-school completion time. Forcing homework during the regulatory recovery window creates a negative association that worsens long-term compliance.
Q5: Can this system be used for children without an autism diagnosis?
Absolutely. After-school restraint collapse occurs across the full neurodevelopmental spectrum and in neurotypical children with high-demand profiles, anxiety, perfectionism, or sensory sensitivities. The system is diagnostic-agnostic — it is designed for any child whose regulatory resources are consistently depleted by the school day. If in doubt, an AbilityScore® assessment can clarify the specific profile and calibrate the system accordingly.
Q6: How do I handle siblings during the transition window?
Siblings need: (1) An age-appropriate explanation: "When [child's name] gets home, they need quiet time in their space. This is their medicine time." (2) Their own space and activity for the transition window. (3) Validation of their experience — their feelings about the difficult afternoons are real. (4) Clear safety boundaries: ASRC decompression needs are valid; physical harm to siblings is not.
Q7: Is this system suitable for children who attend therapy centers?
Yes — and in fact, this system is most effective when integrated with clinic-based therapy. The 9 materials operate in the home environment 24×7, complementing clinic sessions which occur 2–5 times per week. Your Pinnacle OT can customize the specific materials and sequencing based on what they observe clinically. Call 9100 181 181 to connect your home system to clinical support.
Q8: What if we have more than one child with ASRC?
This occurs in approximately 30% of Pinnacle families with multiple children with neurodevelopmental profiles. Solution: staggered arrival times where possible; individual decompression zones (clearly demarcated, different materials based on each child's sensory profile); clear sibling decompression boundaries. The demand-free window applies to both children simultaneously — caregiver support is not optional in these families.

Your child doesn't need a perfect parent. They need a prepared home. Start today.
Everything on this page — the science, the system, the 9 materials — comes down to one simple truth: a prepared environment is the most powerful intervention available to you right now, today, before you spend a single rupee or book a single appointment.
🔵 OT
🟢 ABA/BCBA
🟡 SLP
🔴 SpEd
🟣 NeuroDev Pediatrics
📞 FREE National Autism Helpline: 9100 181 181 | 16 Languages | 24×7 | No appointment needed
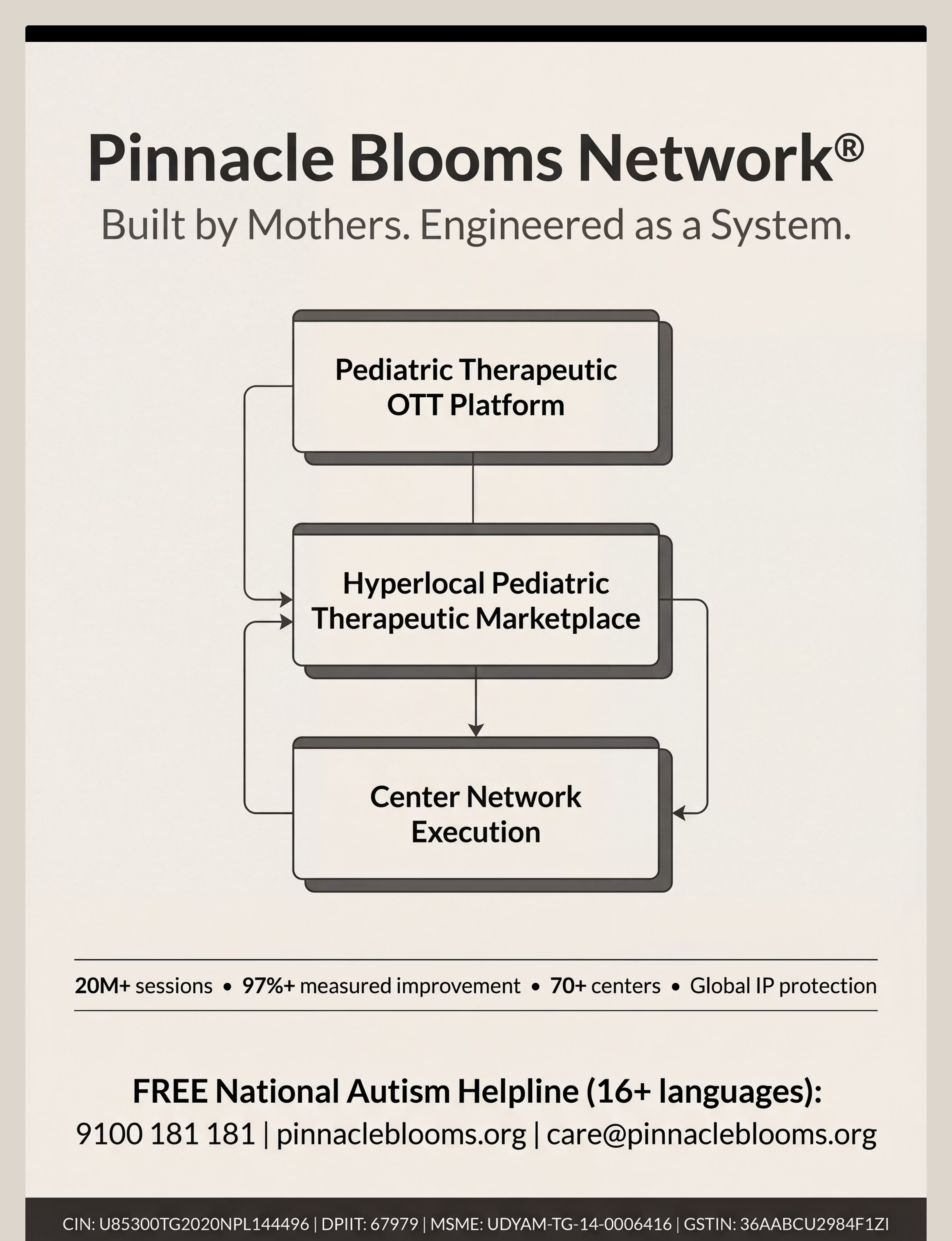
⬟ Validated by the Pinnacle Blooms Consortium | Pinnacle Blooms Network® | Built by Mothers. Engineered as a System.
⬟ Validated by the Pinnacle Blooms Consortium | Pinnacle Blooms Network® | Built by Mothers. Engineered as a System.
Preview of 9 materials that help with coming home Therapy Material
Below is a visual preview of 9 materials that help with coming home therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
The Pinnacle Promise
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
"From fear to mastery. One technique at a time."
— The Pinnacle Blooms Consortium | GPT-OS® Therapeutic Infrastructure
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
70+
Countries Served
This content is educational and informational. The 9 materials and intervention strategies described on this page are general therapeutic guidelines and do not constitute individualized medical, psychological, or occupational therapy advice. Transition support needs vary significantly between children based on sensory profiles, neurodevelopmental diagnoses, developmental factors, and family circumstances. Consult with qualified occupational therapists, behavioral specialists, speech-language pathologists, or other credentialed professionals for individualized assessment, diagnosis, and recommendations. These materials and strategies support but do not replace professional clinical guidance. After-school restraint collapse presentations vary in severity — some require clinical intervention beyond home environmental supports. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2026 Pinnacle Blooms Network® | Unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS® is a registered trademark. AbilityScore® is a registered trademark. EverydayTherapyProgramme™, FusionModule™, TherapeuticAI® are proprietary systems of Pinnacle Blooms Network®. Technique code I-789.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
📞 Helpline: 9100 181 181 | This page: techniques.pinnacleblooms.org/transitions/coming-home-after-school-I-789 | Previous: I-788 Leaving for School | Next: I-790 Homework Transitions