
When the Bathroom Becomes a Battlefield
You've counted the days since their last bowel movement. You've watched them cross their legs, tiptoe around, hide in corners — anything but sit on that toilet. The cycle can be broken. That's what this page is for.
Chronic Constipation
Multi-Material Intervention
E-500

ACT I — RECOGNITION
The Recognition Moment
You Are Not Failing
You've tried more fiber. More water. Prune juice they hate. Stool softeners that help for a week and then stop. You've sat outside bathroom doors in tears. You've run out of underwear. You've run out of answers.
The pediatrician says "functional constipation" — there's nothing structurally wrong — but what you're living doesn't feel functional at all.
What This Page Does
Your child's body is caught in a self-reinforcing cycle that no amount of patience alone can break. But it can be broken. This page gives you the science and the tools to answer back.
You are not failing. Your child's nervous system and pain response are speaking. This page gives you the science and the tools to answer back.
🌸 Pinnacle Blooms Network® | OT · ABA · SLP · NeuroDev · Pediatric GI · SpEd
WHO Nurturing Care Framework (2018): Early identification and informed parental action directly impacts long-term developmental outcomes.

You Are Not Alone: The Numbers
Families from Hyderabad to Houston, Mumbai to Melbourne are navigating this same daily battle tonight. This is medical. This is real. And this is solvable.
30–70%
GI Issues in Autism
Of children with autism experience GI issues including constipation — one of the most common medical comorbidities in neurodevelopmental populations
1 in 3
Functional Constipation
Children develop functional constipation at some point — the majority between ages 2–6 during toilet training and school transitions
~40%
Develop Encopresis
Of children with chronic constipation develop encopresis (soiling) if the underlying pain-fear-withholding cycle is not systematically addressed
In India alone, an estimated 12–15 million children are affected by chronic functional constipation at any given time. NASPGHAN identifies functional constipation as one of the most common pediatric GI presentations — accounting for 3–5% of all pediatric outpatient visits and up to 25% of pediatric gastroenterology referrals.
The child who holds in stool is not defiant. They are afraid. The child who has accidents is not lazy. Their rectal sensation has been altered by chronic stretching. The child who refuses the toilet is not manipulating you. Their nervous system has learned that toilet = pain.

The Pain-Fear-Withholding Cycle
Why "Just Sit On The Toilet" Doesn't Work
Plain English: What's Happening
A single painful bowel movement can set this entire cycle in motion. Once the brain records "toilet = pain," the anxiety response fires every time the child feels the urge to go. They clench. They hold. The stool gets harder. When they finally pass it — days later, larger and drier — it hurts even more. The fear is confirmed. The cycle deepens.
Why Autism Complicates This
- They may not recognize the body signal until it's urgent or too late
- The bathroom environment itself triggers alarm before they even sit
- Communication barriers prevent them from expressing the fear
- Anxiety and rigidity amplify the response to any change
The rectum of a child with chronic constipation may become stretched over time (acquired megacolon), reducing sensation so that they genuinely cannot feel the urge until stool is already leaking. This is physiology, not defiance.
ACT I — CONTEXT
Where This Sits in Development
Chronic Constipation: A Waypoint, Not a Dead End
Age 1–2
Toilet training begins · bowel awareness emerging
Age 2–4 🔶
COMMON ONSET — toilet training transitions, first painful stools
Age 4–6
School entry → bathroom anxiety, withholding at school intensifies
Age 6–10 🔶
ACTIVE ZONE — encopresis peaks, social shame compounds
Age 10–15
With intervention: independent bowel management achievable
Why Children with Autism Are at Higher Risk
- Dietary selectivity → low fiber → harder stool
- Sensory sensitivity to bathroom environment → avoidance
- Interoceptive awareness differences → miss early signals
- Anxiety and routine rigidity → resistance to toilet training
- GI conditions are 3–4× more common in autistic children
Common Comorbidities
- Toileting anxiety and sensory processing differences
- Feeding selectivity and enuresis (daytime wetting)
- Sleep disruption and behavioral dysregulation
- School avoidance from chronic discomfort
Your child is at a critical intervention window. The cycle can be interrupted. Starting now matters.

ACT I — TRUST
The Evidence Behind This Approach
Clinically Validated. Home-Applicable. Parent-Proven.
🛡️ LEVEL I Evidence
Systematic Review + Clinical Guidelines + RCT
1
NASPGHAN/ESPGHAN (2014)
International clinical guidelines confirm combined dietary + behavioral + medical management is the standard of care. Single-intervention approaches are significantly less effective.
2
Sensory OT Evidence — PMC11506176 (2024)
Systematic review of 16 studies confirms sensory integration intervention is an evidence-based practice for children with ASD — directly applicable to sensory-based toileting avoidance.
3
Cuvo & Riva (1980), JABA
Behavioral training demonstrates that learned fear responses (toilet avoidance) can be systematically modified through structured intervention — the scientific foundation for toileting behavior programs.
4
Interoception Training (Emerging)
Body awareness training supports improvement in internal signal recognition in autistic children — directly relevant to bowel signal awareness.
95%
Physical Positioning + Diet
95%
Behavioral Routine + Reward
90%
Sensory Environment Mods
75%
Interoception Training
Clinically validated. Home-applicable. 20M+ sessions of real-world evidence from Pinnacle Blooms Network® across India.

ACT II — KNOWLEDGE TRANSFER
The Technique: What It Is
The Cycle-Breaker Framework
Formal Name: Multi-Component Constipation Intervention: 9-Material Approach
Chronic functional constipation is not simply a dietary problem — it is a self-reinforcing cycle of pain, fear, and avoidance that gradually alters bowel physiology.
The 9-Material approach addresses every component of that cycle simultaneously: physical positioning, routine structure, dietary optimization, sensory environment modification, fear reduction, body signal awareness, nervous system calming, motivation maintenance, and professional coordination.
No single material addresses the whole cycle. Together, they break it.
Domain & Setting
Domain E: GI Health / Toileting
Chronic Constipation
Encopresis
Toileting Resistance
- 🕐Age Range: 2–15 years
- 🏠Setting: Home · School · Therapy · Medical
- 📅Frequency: Daily routine integration (minimum 2× daily scheduled sits)
- ⏱️Duration: 8–12 weeks minimum for cycle interruption; ongoing maintenance thereafter
Canon Material Components
- Reinforcement Menus · Visual Schedules
- Sensory Modification Tools
- Interoception Materials · Social Stories
Who Uses This Technique
This Challenge Requires a Consortium. Here's Who's On Your Team.
Occupational Therapist (Primary Lead)
Sensory factors in toileting avoidance · Positioning assessment · Interoception awareness training · Environmental modification · Daily living skills framework
ABA Therapist / BCBA
Stool withholding behavior · Toilet avoidance/refusal · Reward system design · Systematic desensitization · Schedule compliance · Data-driven tracking
Pediatric NeuroDev / GI Doctor
Medical management of impaction · Stool softener protocols · Clean-out procedures · Monitoring for complications · Ruling out organic causes
Speech-Language Pathologist
Social story development · Communication supports · Vocabulary for body sensations · AAC programming for non-verbal children
Special Educator
School toileting plan · Teacher communication · Transition supports · Visual supports across settings · IEP/504 accommodation planning
This challenge crosses therapy boundaries because the bowel doesn't organize by therapy type. The Pinnacle Consortium addresses all five dimensions simultaneously through FusionModule™.
📞 FREE National Helpline: 9100 181 181 — speak to our GI + OT + Behavioral team in your language

6 Interconnected Targets. One Integrated Plan.
1
Bowel Regularity
Goal: Bowel movement every 1–2 days
Baseline: Once weekly or less, hard/pellet stools, pain during passage
2
Fear Extinction
Goal: Child sits on toilet at scheduled times without distress
Baseline: Refusal, crying, running, hiding when bathroom suggested
3
Stool Consistency
Goal: Soft, formed, painless stools (Bristol Stool Scale Type 3–4)
Baseline: Type 1 (hard lumps) or Type 2 (lumpy sausage)
4
Interoceptive Awareness
Goal: Child recognizes bowel signal before urgency/leaking
Baseline: No awareness until too late, or no awareness at all
5
Encopresis Elimination
Goal: Zero fecal soiling incidents
Baseline: Variable — from rare overflow to multiple daily incidents
6
Toileting Independence
Goal: Child manages own toileting routine with minimal prompting
Baseline: Fully adult-dependent; high family burden
These 6 targets are monitored within GPT-OS® under the Toileting Independence Readiness Index, Interoceptive Awareness Readiness Index, and Self-Care Readiness Index — giving families and clinicians a standardized, measurable progression system.

The 9 Materials: Overview Map
9 Materials. 9 Components of the Cycle. One Complete Approach.
1. Toilet Footstool
Bowel regularity, stool consistency
2. Visual Toileting Schedules
Fear extinction, regularity
3. Fiber & Dietary Tools
Stool consistency, bowel regularity
4. Sensory Comfort Modifications
Fear extinction, relaxation
5. Toileting Social Stories
Fear extinction, interoceptive awareness
6. Interoception Training
Interoceptive awareness
7. Relaxation & Breathing Tools
Fear extinction, pelvic floor release
8. Reward Systems & Charts
Fear extinction, compliance, motivation
9. Professional Support
All targets (coordinating layer)
Fiber alone won't break the cycle if fear is running it. Rewards alone won't work if the stool is too hard to pass without pain. All 9 components work together. Using 3 or 4 in isolation produces partial results. The full protocol produces lasting change.

Safety First: Before You Start
Before You Use Any of These Materials — Read This First
🔴 Seek Immediate Medical Attention If:
- Blood in stool (beyond small amount from anal fissure)
- Severe abdominal pain or distension, or vomiting with constipation
- No bowel movement for 7+ days
- Signs of fecal impaction (leaking stool despite no voluntary BM)
- Constipation present from birth or first weeks of life
- Child is under 2 years of age (always medical evaluation first)
🟡 Schedule Medical Evaluation Within 2 Weeks If:
- Constipation present for more than 2 weeks despite home intervention
- Encopresis (soiling) is occurring — this is a medical sign, not a behavior problem
- Standard dietary interventions have not produced improvement
- Child is on medications that can cause constipation
🟢 Home Intervention Appropriate When:
- Pediatrician has confirmed functional constipation with no organic cause
- Medical management (stool softeners if prescribed) is in place
- No signs of acute complications listed above
- Child is medically stable and able to participate
CRITICAL — ENCOPRESIS: Fecal soiling in the context of constipation is NOT a behavioral choice. It occurs because the rectum has become stretched, reducing sensation. NEVER punish soiling. This response increases shame, worsens withholding, and intensifies the cycle.
Medication Note: Many children with established constipation need stool softeners (PEG/Polyethylene Glycol is most evidence-supported) as the medical foundation before behavioral intervention can succeed. Ask your pediatrician about maintenance stool softener protocols.
📞 Not sure where your child falls? Call 9100 181 181 — FREE consultation with our Pediatric GI + OT team.
Setting Up Your Home Protocol
Your Pre-Session Setup: Creating Conditions for Success
🚽 Bathroom Readiness
- Toilet footstool in position (knees above hips when seated) ← Material 1
- Padded or softened toilet seat cover in place ← Material 4
- Sound machine or white noise if auditory sensitivity ← Material 4
- Soft lighting (nightlight or dimmer) if visual sensitivity ← Material 4
- Preferred distraction item (book, tablet, bubbles) inside bathroom ← Material 7
📅 Schedule Readiness
- Visual toileting schedule posted where child can see it ← Material 2
- Timer or visual timer available for sit duration ← Material 2
- Reward chart visible and stickers ready ← Material 8
- Scheduled times confirmed: After breakfast + After dinner ← Material 2
🥦 Dietary Readiness
- Fiber-rich foods available in today's meals ← Material 3
- Water intake tracking visible ← Material 3
- Stool softener given if prescribed (30–60 min before typical BM time) ← Material 9
⏰ Daily Timing Guide
Morning (Primary): 6:30 AM — Wake + stool softener if prescribed. 7:00 AM — Breakfast (fiber-rich). 7:20 AM — Gastrocolic reflex window → Toilet sit 5–10 minutes → Reward for sitting regardless of outcome.
Evening (Secondary): 6:00 PM — Dinner (fiber-rich). 6:20 PM — Second sit opportunity → Toilet sit 5–10 minutes → Reward for sitting.
Calm caregiver = calmer child. Check your own stress level before every session.

Space & Child Readiness Check
The Best Toileting Session Is One That Starts Right
🟢 GO — All Systems Ready
- Child is calm (no active meltdown or distress)
- Recent meal was consumed (gastrocolic reflex active)
- Scheduled time has arrived (routine is set)
- Child is not acutely ill or feverish
- Bathroom environment is prepared and comfortable
- Caregiver is regulated and calm
🟡 MODIFY — Adjust the Approach
- Child is mildly resistant → Offer choice: "Would you like the bubbles or the book today?"
- Child seems uncomfortable → Reduce sit time to 3 minutes
- Unexpected bathroom issue → Address it before proceeding
- Child had a very bad BM recently → Consider sitting near toilet, not on it
🔴 POSTPONE — Not Today
- Child is in active meltdown or acute distress
- Child is acutely ill with vomiting or fever
- Child visibly in pain suggesting possible impaction → medical evaluation
- Caregiver is dysregulated and unable to remain calm
Never force a child to sit on the toilet. A forced sit creates a traumatic association that deepens the fear-avoidance cycle. Even tolerance without production is success. Your job is to create conditions for success, not to control outcomes.

ACT III — EXECUTION
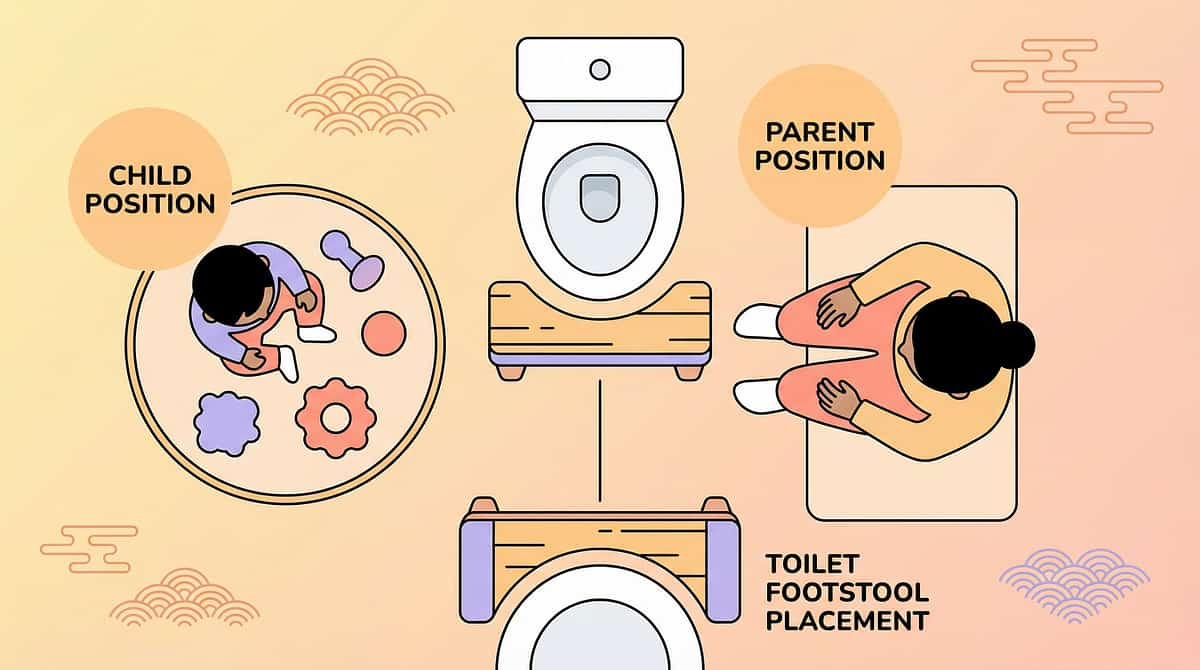
🚽 Material 1 of 9
Physical Positioning
Toilet Footstool
Optimal positioning for easier evacuation
The Science (OT Voice)
The human body was designed to squat, not sit at 90 degrees. A standard toilet positions children with their hips at 90 degrees — which actually constricts the puborectalis muscle that wraps around the rectum. This constriction means the anorectal angle remains closed, making evacuation require significant straining.
A toilet footstool raises the knees above the hips, creating a 35-degree position that straightens the anorectal angle — the position the body needs to allow stool to pass with minimal effort.
For children, whose feet often dangle in the air, the footstool provides two benefits: the physiological positioning benefit AND grounding security. An unstable nervous system cannot relax the pelvic floor. Stability enables relaxation. Relaxation enables evacuation.
In Practice
Place the footstool directly in front of the toilet. When the child sits, knees should be at or above hip level. Feet should be flat on the stool surface. The child should feel stable and grounded — encourage a slight forward lean from the hips to further optimize the angle.
Key Insight
The difference between straining for 10 minutes and a comfortable 2-minute bowel movement can be the 35-degree hip angle a footstool creates.
DIY Option (₹0)
Use any sturdy step stool that elevates feet so knees rise above hip level. A toilet seat reducer ring also eliminates fear of falling in. Test stability — no sliding.
Price Range: ₹0 (DIY) — ₹2,000 (commercial)

📅 Material 2 of 9
Behavioral Structure + Routine
Visual Toileting Schedules
Predictable routine works with the body
The Science (ABA + OT Voice)
The gastrocolic reflex — the body's natural signal to have a bowel movement — is strongest 20–30 minutes after eating, particularly after breakfast. Scheduled toilet sits at this time harness the body's natural physiology rather than fighting it. Consistency creates a new learned association: after breakfast → sit on toilet → this is normal. Over weeks, the bowel begins to respond on schedule.
For children who avoid the toilet, scheduled sits serve a second purpose: desensitization. Each sit that ends without pain is a new data point telling the brain "toilet is safe." Over dozens of neutral or positive sits, the fear association weakens. This is systematic desensitization occurring naturally through routine.
Schedule Structure
01
After Breakfast (7:00–7:30 AM)
Visual cue: picture card showing "eat → toilet → sticker" · Sit 5–10 min · Distraction item · Immediate reward for sitting
02
After Dinner (Evening)
Same routine, second opportunity · Same reward structure
03
Optional: After Lunch
For school-age children, if school bathroom anxiety is manageable and school team is aligned
KEY PRINCIPLE: REWARD SITTING, NOT PRODUCING. A child who sits for 5 minutes without producing stool has succeeded. Rewarding sitting reduces pressure. Pressure increases withholding. The goal is a relaxed sit — not a forced outcome.
DIY Option (₹0–200): Draw or print pictures showing the after-meal toilet routine. Laminate with packing tape. Use a simple calendar with sticker spaces for each successful sit.
Canon Product: 1800+ Reward Stickers — amzn.in/d/01wrHJWX — ₹299 | Price Range: ₹0 (DIY) — ₹600

🥦 Material 3 of 9
Dietary Foundation
Fiber-Rich Foods & Dietary Tools
Soft stool starts with what goes in
The Science (Pediatric GI + Nutrition Voice)
Dietary fiber adds bulk and water content to stool — making it softer, easier to form, and far less painful to pass. When stool is soft, the pain-fear cycle has less to reinforce itself.
Critically: fiber without water makes constipation worse. Fiber absorbs water — if the child is not drinking enough, fiber draws water from the stool rather than adding it. The target is fiber AND fluid together.
Fiber Calculation Guide
Target: Child's age + 5–10 = grams of fiber per day
- Age 5: 10–15g/day
- Age 8: 13–18g/day
- Age 12: 17–22g/day
Increase fiber by 2–3g per week, not all at once. Sudden increases cause gas and discomfort. Pair every fiber increase with a proportional water increase.
High-Fiber Foods Children Often Accept
Food | Fiber | Notes | |
Popcorn (plain) | 3.5g / 3 cups | Often accepted by sensory eaters | |
Berries (strawberry, blueberry) | 3–4g / cup | Sweet, commonly accepted | |
Whole grain bread | 2g / slice | Replace white bread | |
Oatmeal | 4g / ½ cup | Mix with preferred flavors | |
Green peas | 4g / ½ cup | Try frozen thawed | |
Beans / lentils | 8g / ½ cup | Mix into preferred foods | |
Banana | 3g / medium | Often accepted |
Fiber Supplements: PEG (Polyethylene Glycol / MiraLax) is the most evidence-supported stool softener for pediatric constipation. Always consult pediatrician before starting supplements.
Price Range: ₹200–1,500 | Amazon.in: fiber-rich snacks children →
🛁 Material 4 of 9
Sensory Environment
Sensory Comfort Modifications
Make the bathroom a place the body can relax
For children with sensory processing differences — extremely common in autism, ADHD, and SPD — the bathroom can be a multi-sensory assault. An alarmed nervous system cannot relax the pelvic floor. A clenched pelvic floor cannot allow evacuation. Sensory modifications are a physiological prerequisite for successful evacuation, not comfort for comfort's sake.
👆 Tactile (Touch)
- Cold toilet seat → padded seat cover or toilet seat warmer
- Scratchy toilet paper → ultra-soft brands or flushable wet wipes
- Cold floor → warm non-slip bath mat underfoot
👂 Auditory (Sound)
- Echo + flushing noise → white noise machine or soft music player
- Flush after child exits — not while seated — for children who fear the sound
- Soft furnishings (towel on floor, soft mat) absorb bathroom echo
👁️ Visual (Light)
- Bright overhead light → install dimmer or use a plug-in nightlight
- Harsh shadows → warm-toned nightlight rather than cool LED
👃 Olfactory (Smell)
- Bathroom odors → preferred scent diffuser (lavender works for many)
- Unscented products if child is scent-averse
- "Poo-Pourri" type products that neutralize odor before it forms
🦵 Proprioceptive (Body Position)
- Dangling feet → footstool (Material 1)
- Fear of falling in → toilet seat reducer ring
- Need for containment → child-sized seat with side handles
DIY Option (₹0–500): Fabric toilet seat cover from old towel or fleece. White noise from phone speaker. Dimmer from local hardware. All significant impact for near-zero cost. | Price Range: ₹500–3,000

📖 Material 5 of 9
Fear Reduction + Understanding
Toileting Social Stories
Understanding reduces the fear that drives withholding
The Science (SLP + ABA Voice)
Social stories, developed by Carol Gray, are short, personalized narratives that explain a situation from the child's perspective. For toileting, they address the two drivers of the pain-fear-withholding cycle accessible through language: understanding and prediction.
A child who understands that poop is waste their body makes, that the toilet won't hurt them, and who can predict exactly what will happen in the bathroom routine — experiences less anticipatory anxiety. Familiarity reduces the "unknown" component of fear.
Social stories should be read during calm times — not when the child is already resisting. Repetition during low-stress moments builds familiarity.
Age-Appropriate Cycle Explanation
"When we hold poop inside, it gets bigger and harder. Bigger, harder poop hurts more. Letting it out before it gets too big means it doesn't hurt. The more we practice letting it out at toilet time, the easier it gets."
Sample Social Story: "When My Tummy Needs to Go"
01
Slide 1
"Sometimes my tummy makes poop. Poop is waste that my body doesn't need. All bodies make poop."
02
Slide 2
"When my tummy feels full or uncomfortable, that might be my body saying 'time to go to the toilet.'"
03
Slide 3
"My toilet has a footstool so my feet are cozy and safe."
04
Slide 4
"I sit for 5 minutes. I can read my book or blow bubbles."
05
Slide 5
"If poop comes out, great. If not, that's okay too. I still get my sticker for sitting."
Personalization Tip: Use photos of your child's actual bathroom, their actual toilet, their actual footstool. Personalization transforms an abstract story into a preview of a known, safe experience.
DIY Option: Create with PowerPoint or Google Slides using bathroom photos. Print and laminate. ₹0–300 | Commercial: ₹800

🧠 Material 6 of 9
Body Signal Awareness
Interoception Training Materials
Recognize body signals before urgency becomes crisis
The Science (OT + NeuroDev Voice)
Interoception is the eighth sensory system — our perception of the internal state of the body. It encompasses awareness of hunger, thirst, temperature, heartbeat, and critically: the sensation that the bowel needs to empty.
Children with autism, sensory processing differences, and ADHD often have atypical interoceptive awareness. They may not notice the signal that their bowel is full until it is overwhelming — or not at all, if chronic rectal stretch has reduced rectal sensation. This is not stubbornness. Their internal signaling system is not reliably delivering clear messages.
Interoception training teaches children to attend to body signals through structured practice — starting with easier-to-recognize signals (hunger, thirst) and progressively moving to subtler ones (bowel fullness).
📞 Interoception training is most effective when guided by an OT. Our team can build a personalized program. Call 9100 181 181
Training Sequence
Week 1–2: Easier Signals
"Let's be body detectives! What does hungry feel like? Where do you feel it? What does thirsty feel like?"
Week 3–4: Moving to Bowel Signals
"Let's check in with your belly. Scan from head to toe. What do you notice in your belly right now?" — Use body map with stickers.
Week 5–6: Connecting Signals to Actions
"When you feel this kind of pressure here, that might be your body saying 'time to try the toilet.'"
Week 7+: Spontaneous Self-Monitoring
Child begins doing body checks independently or with minimal prompting: "Check in with your body — what's it saying?"
Body Map Activity: Print body outline. During check-ins, child uses colored stickers to mark where they feel sensations: red = strong, yellow = medium, green = quiet.
DIY Option: ₹0 — print body outline, use any stickers. Consistency is the ingredient. | Commercial: ₹1,500
Canon Product: Rosette Reward Jar — amzn.in/d/02C5R9Jn

🫁 Material 7 of 9
Nervous System Regulation
Relaxation & Breathing Tools
A calm body is the prerequisite for evacuation
The Science (OT + Physiotherapy Voice)
Bowel evacuation requires the pelvic floor to relax. In children who are anxious, afraid of pain, or in sensory alarm, these muscles remain in high-tone contraction. No amount of straining will overcome a clenched pelvic floor.
Deep, slow breathing — particularly slow exhalation — activates the parasympathetic nervous system ("rest and digest"), which directly reduces pelvic floor muscle tone. This is why blowing bubbles or practicing "belly breathing" during toilet sits is not just distraction: it is a physiological release mechanism.
The body cannot be in fight-or-flight (sympathetic) and evacuation mode (parasympathetic) simultaneously. Relaxation is not optional — it is a clinical intervention.
Tool Guide
🫧 Bubbles (Recommended #1)
Slow exhalation required · Activates parasympathetic NS · Provides distraction · 2–3 minutes before and during sit · Cost: ₹50–100
🌀 Pinwheel / Party Blower
Same exhalation mechanics · Visual feedback · Child's "special toilet toy" · Cost: ₹30–100
🤲 Belly Breathing Script
"Put hands on tummy. Big breath in — feel tummy push out like a balloon. Blow out slowly. Feel tummy fall. Let's do 3 together." Practice outside bathroom first.
💆 Abdominal Massage (I Love U)
Down right side → across bottom → up left side → across top. Firm, clockwise pressure. 3–5 minutes before toilet sit. Evidence supports intestinal motility effects. Cost: ₹0
Calming Music: Specific playlist for bathroom sits only — becomes a Pavlovian relaxation cue. Child learns: this music = relaxed time = toilet time = safe.
Price Range: ₹200–800

⭐ Material 8 of 9
Positive Reinforcement + Motivation
Reward Systems & Motivational Charts
Replace fear associations with positive ones — one sit at a time
The Science (ABA Voice)
Children who have experienced repeated painful bowel movements have a conditioned aversive response to toileting. Reward systems create a new positive association that competes with the fear response. Over repeated pairings of "sit on toilet → immediate reward → positive experience," the toilet's association in the brain gradually shifts from "danger" to "reward opportunity."
Critical Principle: Reward the behavior you want MORE OF, which is SITTING — not the outcome (producing stool). Rewarding only bowel movements creates performance pressure → anxiety → pelvic floor clenching → no bowel movements. Deliver the reward within 3 seconds of the child sitting.
Verbal Reinforcement Script
"I am so proud of you. That took real bravery. You sat on the toilet and you stayed for the whole time. That is amazing."
Reward System Design
Sticker Chart (Primary)
One sticker per completed sit regardless of output · Visible chart in bathroom · Child places own sticker · Every 5 stickers: small reward · Every 20 stickers: larger reward
Reward Menu
Preferred screen time (15 min) · Preferred snack · Special game with parent · Sticker book · Small toy from reward box. Child's choice increases motivation.
Things to NEVER Do
- Never express disappointment about lack of bowel movement
- Never say "you didn't even try" or "nothing happened again"
- Never remove a sticker that was earned for sitting
- Never use toileting as a punishment
Canon Products: 1800+ Reward Stickers — amzn.in/d/01wrHJWX ₹299 | Rosette Reward Jar — amzn.in/d/02C5R9Jn
Price Range: ₹200–800
🩺 Material 9 of 9
The Coordinating Layer
Professional Medical & Therapeutic Support
Home-based intervention works best when professionally coordinated
For most children with established functional constipation, home intervention alone is insufficient. Stool that has been impacted for weeks or months often requires medical clean-out before a behavioral program can succeed. Medical management must come first — clearing the physical problem — so that behavioral, sensory, and educational interventions can work on top of a clean physiological slate.

Pediatrician / Pediatric GI
Confirm functional constipation (rule out Hirschsprung's, hypothyroidism, food allergy) · Clean-out protocol if impaction is present · Maintenance stool softener prescription (PEG first-line) · Monitor for complications · Guide medication tapering

Occupational Therapist
Sensory profile assessment · Positioning assessment · Interoception training program · Sensory diet for nervous system regulation · Daily living skills progression

Behavioral Therapist / BCBA
Functional behavior assessment of toileting avoidance · Systematic desensitization hierarchy · Individualized reinforcement system · Data collection and protocol adjustment

Speech-Language Pathologist
Social story creation at child's comprehension level · AAC programming for non-verbal children · Communication supports for expressing toileting needs
📞FREE National Helpline: 9100 181 181 — 16+ languages — 24x7 available. "Tell us your child's age, primary challenges, and location. We'll connect you with the right specialist." | Price Range: ₹1,500–8,000 per consultation

Adapt the Protocol to Your Child
No Two Children's Constipation Is Identical
High Sensory Sensitivity (Autism, SPD)
- Prioritize: Sensory modifications (Card 16) FIRST — environment must be safe before behavior can change
- Extend: Allow longer adjustment periods to bathroom modifications
- Reduce: Sit duration to 3 minutes initially — tolerance is the target
- Add: Sensory diet before toilet sit (proprioceptive input — jumping, wall push-ups)
Severe Anxiety / Phobia
- Prioritize: Systematic desensitization (start far from bathroom, work closer over weeks)
- Add: Professional behavioral assessment before any forced exposure
- Consult: Pediatric psychologist if toileting anxiety is severe
- Do NOT: Force proximity to toilet until desensitization has progressed
Significant Encopresis
- Medical management FIRST: Consult pediatric GI before any behavioral program
- Do NOT: Begin sticker chart until medical clean-out has occurred — the child cannot feel or control soiling
- Explain: The soiling is not the child's fault — separate the shame before any behavioral intervention
Non-Verbal / Minimally Verbal Child
- Prioritize: Visual supports across all materials
- Add: AAC programming with SLP (symbols for "toilet," "I need to go," "it hurts")
- Track: Non-verbal behavioral indicators — posture, facial expression, withholding gestures
Older Child (10–15 Years)
- Prioritize: Dignity — involve them in every decision about materials and modifications
- Frame: Through health, not behavior: "This is how we keep your body healthy"
- Add: Age-appropriate psychoeducation about the constipation cycle
- Professional: Adolescent-appropriate OT and GI referral

ACT IV — THE PROGRESS ARC
Weeks 1–2: Building the Foundation
15%
Foundation Phase
You are planting the seeds of a new pattern, not expecting dramatic change yet
🟢 Positive Indicators (These Are Wins!)
- Child sits on toilet at scheduled time once (even briefly) with less resistance than before
- Child allows the footstool to be placed and used
- Child tolerates the bathroom with modifications better than without
- Social story being read daily during calm times
- Parent feeling more organized and purposeful about the approach
🟡 What Is Not Progress Yet (Normal at This Stage)
- Daily regular bowel movements — this comes much later
- Child requesting to use the toilet — this comes much later
- Soiling stopping — resolves with physical regularity, which takes weeks
- Complete fear elimination — this is a 6–12 week process
"In week 2, you may feel like nothing is working. The bowel movements may still be hard and infrequent. The soiling may continue. This is normal. You are rewiring a cycle that took months or years to develop. Progress at this stage is measured in tolerances, not outputs."
Week 1–2 Tracking Targets: Scheduled sits: Target 2/day, measure % compliance · Distress level: Target 20% reduction from baseline · Stool frequency and soiling: Baseline documentation only
NASPGHAN guidelines note that bowel retraining programs typically require 4–6 months of consistent implementation before full normalization. 2 weeks is foundation only.

Weeks 3–4: The Routine Is Taking Hold
35%
Consolidation Phase
Neural pathways governing habit formation are strengthening
What's Happening in the Brain
By weeks 3–4, the routine of after-breakfast → toilet sit is beginning to feel predictable rather than threatening. The bathroom modifications that were new in week 1 are now familiar. The footstool is expected. The distraction item is anticipated. Familiar = less threatening.
Consolidation Indicators
- 🟢 Child goes to bathroom with less resistance (or same resistance but shorter duration)
- 🟢 Sit duration increasing (staying 5 minutes more consistently)
- 🟢 Stool consistency may be improving (Bristol Scale moving toward Type 3–4)
- 🟢 Parent feeling more confident executing the protocol
- 🟢 Child anticipating the reward — asking about the sticker
Behavioral Generalization Seeds
Watch for these spontaneous behaviors as signals that neural pathways are forming:
- Child goes near the bathroom on their own between scheduled sits
- Child references the social story: "poop goes in the toilet"
- Child shows awareness of abdominal sensations ("my tummy feels funny")
When to Increase Intensity
If week 3–4 shows solid compliance (70%+ of scheduled sits completed), consider:
- Adding a third daily sit opportunity (mid-day)
- Increasing sit duration target from 5 to 8–10 minutes
- Beginning to fade some environmental supports if child is self-settling

Weeks 5–8: The Cycle Is Breaking
60%
Active Change Phase
With consistent implementation, the pain-fear-withholding cycle should be showing signs of interruption
Physical Progress Indicators
- Stool consistency improving (Bristol Type 3–4 appearing more regularly)
- Bowel movement frequency increasing (approaching every 1–2 days)
- Pain during bowel movements decreasing or absent for softer stools
- Soiling incidents decreasing in frequency
Behavioral Progress Indicators
- Resistance to toilet sits has decreased (no longer crisis-level)
- Child completes scheduled sits with distraction but less obvious distress
- Beginning of spontaneous toileting attempts outside scheduled times
- Child beginning to identify "full" or "pressure" sensations in lower belly
Pelvic Floor Release Signs
- Bowel movements becoming more complete (less large-mass episodes)
- Less straining reported or observed
- Child using breathing tools during sits voluntarily
Medical Management Review at 6–8 Weeks: Review stool softener dosing with pediatrician. If stool is now consistently Type 3–4, dose may be appropriate to maintain. Do NOT stop stool softeners prematurely — recurrence risk is high.
Celebrate Every Milestone
Every Single Win Deserves Recognition — By You and Your Child
First Sit Without Screaming
The first neural rewiring — this was the hardest one
First Soft Bowel Movement
The dietary + medical combination worked
First Breathing Tool Used
They learned the self-regulation skill — that's huge
First "I Need to Go"
Interoceptive awareness is waking up — the cycle is breaking
First Week Without Soiling
The physical cycle is breaking at its deepest level
30 Days of Scheduled Sits
Routine has been built — the habit is now structural
You have held this program together through weeks of resistance, soiled underwear, bathroom battles, and exhaustion. Every sit that ended with a sticker instead of a meltdown was your work. Every soft bowel movement was partly the result of your quiet persistence. Every time you responded to soiling with calm instead of frustration, you broke the shame cycle for your child. That is not small. That is everything.
📞 Reached a milestone? Our team at 9100 181 181 would love to hear your child's progress and help you plan the next phase.
Red Flags: Know When to Escalate
🔴 Escalate Immediately
- Blood in stool beyond minor fissure
- Severe abdominal pain, distension, or vomiting
- No bowel movement for 7+ days
- Signs of megacolon (grossly distended abdomen)
- Child is in acute and worsening distress
🟡 Schedule Medical Review
- No improvement in stool frequency after 4–6 weeks of medical management + full program
- Soiling increasing rather than decreasing
- New behavioral regression (was improving, now worse)
- Weight loss or appetite significantly decreased
- Child reporting increased pain despite softened stool
🟡 Schedule Behavioral/OT Review
- Protocol compliance dropping below 40%
- Child's anxiety around toileting increasing despite desensitization efforts
- No change in interoception indicators after 8 weeks
- Family exhaustion reaching breaking point
📞9100 181 181 — When the home program isn't moving forward, our clinical team can assess what's missing and build the next layer of support. Don't struggle alone.
The GPT-OS® Clinical Pathway
From Severe Withholding to Independent Bowel Health
Each stage builds on the last with coordinated medical, behavioral, sensory, and educational interventions working in parallel. GPT-OS® tracks progress across the Toileting Independence Readiness Index, Interoceptive Awareness Readiness Index, Self-Care Readiness Index, and Sensory Regulation Readiness Index — giving families and clinicians a standardized, measurable view of where the child stands and what's next.

Related Techniques: Building the Complete Framework
← Before This Technique
E-498: Understanding the Pain-Fear-Withholding Cycle
The neuroscience of why children withhold. One painful bowel movement can rewire the brain's threat response and make toileting feel unsafe. Essential reading before starting any behavioral protocol.
E-499: Disimpaction & Medical Clearance
Working with your pediatric GI to clear the backlog. Behavioral intervention without medical clearance often fails. Learn how to know when your child is truly ready to begin.
→ After This Technique
E-501: Encopresis & Soiling
When accidents become daily and shame starts to settle in. The 7-material protocol for children who soil despite awareness.
E-502: Toilet Training for Children with Autism & SPD
The full sensory-first toilet training protocol for children who have never been trained or who have regressed. Builds on the sensory modifications in E-500.
E-503: Bladder & Bowel Co-Regulation
When urinary urgency and bowel dysfunction occur together. The dual-system approach used by Pinnacle's pediatric urology and GI teams.
Where E-500 Sits in the Domain E Sequence
E-497 — GI Anatomy for Parents
E-498 — The Pain-Fear Cycle
E-499 — Medical Clearance
E-500 — 9 Materials
CURRENT
E-501 — Encopresis
E-502 — Toilet Training (ASD/SPD)
E-503 — Bladder-Bowel Co-Regulation
Each technique in the Domain E series builds on the last. Families who complete E-497 through E-500 in sequence report 40% faster resolution than those who begin at E-500 alone. — Pinnacle Blooms Network® Internal Outcomes Data, 2024
Chronic Constipation in Context: Your Child's Full Developmental Picture
Chronic constipation does not exist in isolation. Domain A (Sensory) drives bathroom avoidance. Domain C (Emotional) anxiety amplifies the pain-fear-withholding cycle. Domain D (Behavior) — stool withholding is a learned avoidance behavior. Domain J (Self-Care) — toileting independence is a core ADL milestone. Domain K (Medical) — GI health impacts appetite, sleep, mood, and behavior. GPT-OS® tracks all 12 domains simultaneously. Improvements in GI health often produce improvements in behavior, mood, and participation within 4–6 weeks.

ACT V — COMMUNITY & ECOSYSTEM
Families Who've Been Here
They Started Where You Are
Priya, Mother of 7-Year-Old with ASD, Hyderabad
Before: "My son hadn't had a proper bowel movement in a week. The soiling was happening 3–4 times a day. He had no awareness of it — he'd come home from school and not even know. He was being bullied. I was in tears every day."
After (4 months of full protocol): "He now goes every day or every other day. The soiling stopped at month 3. He told me last week, 'Amma, my tummy says I need to go.' That sentence. I cannot describe what that sentence meant to me."
Timeline: Month 1 — Medical clean-out + softeners · Month 2 — Behavioral protocol added · Month 3 — Soiling ended · Month 4 — Self-initiation beginning
Rajesh, Father of 5-Year-Old, Bangalore
Before: "My daughter would scream for an hour every time we suggested the toilet. She would hide under her bed. She had a look of absolute terror. We thought something was very wrong with her psychologically."
After (3 months — sensory modifications + social stories): "The terror is gone. It didn't happen overnight — it happened sticker by sticker. She now walks to the bathroom herself sometimes. The padded seat was the biggest single change — I had no idea the cold was triggering her that much."
"The cases that progress fastest share one feature: parents who understand that they are rewiring a fear response, not correcting a behavior problem. Once parents stop interpreting avoidance as defiance and start seeing it as fear, their entire approach shifts. And children feel that shift." — OT Specialist, Pinnacle Blooms Network®, Hyderabad
These are illustrative narratives representing composite outcomes from Pinnacle Network families. Individual results vary by severity, age, and contributing factors.

Connect with Other Parents
You Are Not Navigating This Alone
📱 Pinnacle GI & Toileting Parent WhatsApp Group
Join families navigating chronic constipation, encopresis, and toileting challenges. Share what's working. Ask what isn't. Join via pinnacleblooms.org/community
💬 Online Forum
Pinnacle Parent Community — technique-specific discussion threads, therapist-moderated, multilingual. pinnacleblooms.org/forum
🤝 Peer Mentoring
Connect with a parent who has been through this exact program and emerged on the other side. Request a peer mentor at pinnacleblooms.org/peer-mentor
🏥 Local Support
Pinnacle Blooms® operates 70+ centers across India. Most run monthly parent support groups for GI & toileting challenges. Find your center →
📞9100 181 181 — Available 24x7 in 16+ languages. When you need to talk to a person, not read a page.
Home + Clinic = Maximum Impact
Your Professional Support Team Across India
Your Need | Specialist | Pinnacle Module | |
Medical management | Pediatric NeuroDev Doctor / GI referral | Medical Coordination | |
Sensory bathroom issues | Pediatric Occupational Therapist | OT Track | |
Behavioral avoidance | BCBA / Behavioral Therapist | ABA Track | |
Social stories / AAC | Speech-Language Pathologist | SLP Track | |
School plan | Special Educator | SpEd Track |
In-Person Centers
70+ Pinnacle Blooms® centers across India with GI/Toileting specialists, OT, Behavioral, and SLP teams. Filter by specialty and location at pinnacleblooms.org/centers
Teleconsultation
Can't reach a center? Our teleconsultation service connects you with Pinnacle specialists from anywhere in India or internationally.
📞9100 181 181 — FREE · 16+ languages · 24x7
The Research Library
The Science Behind These 9 Materials
NASPGHAN/ESPGHAN Guidelines (Tabbers et al., 2014)
Standard of care for pediatric functional constipation. Confirms multi-modal intervention as evidence standard. J Pediatr Gastroenterol Nutr. 2014;58(2):258-274.
PMC11506176 — Children (2024)
Systematic review: Sensory integration intervention is an evidence-based practice for children with ASD. 16 studies, 2013–2023 confirmed.
Cuvo & Riva (1980) — Journal of Applied Behavior Analysis 13(2):315-331
Behavioral training with structured generalization — foundation for toileting behavior programs.
NCAEP Evidence-Based Practices Report (2020)
Social Narratives, Visual Supports, and Reinforcement-based strategies confirmed as evidence-based practices for autism.
Padmanabha et al. (2019) — Indian Journal of Pediatrics
Indian RCT: Home-based structured interventions for pediatric developmental challenges show significant outcomes. DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework (2018)
Global standard for early childhood development. Bowel health embedded in self-care and daily living skills domains. Implemented in 54+ countries.
All citations searchable at: pubmed.ncbi.nlm.nih.gov
How GPT-OS® Uses Your Data
Your Data. Your Child. The System That Learns.
What GPT-OS® Learns from E-500 Data
- Whether the 9-material framework is producing bowel frequency change in expected timelines
- Which materials produce the fastest behavioral compliance gains for this child's profile
- Whether interoception training is producing self-initiation signals
- When to recommend transitioning from high support to fading
GPT-OS® Stack
AbilityScore® → TherapeuticAI® → FusionModule™ → EverydayTherapyProgramme™ → Outcomes Re-measurement
Proof Strip
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centers · Patents filed across 160+ countries
Privacy
All data governed by data protection standards. CIN U74999TG2016PTC113063 | GSTIN 36AAGCB9722P1Z2
Watch the Reel: E-500
9 Materials That Help With Chronic Constipation — In 60 Seconds
Reel ID: E-500
Domain E — GI & Toileting
Episode 500
When the bathroom becomes a battlefield. 9 materials that break the pain-fear-withholding cycle — demonstrated in a real home environment by our OT specialist.
In this reel, see correct use of the toilet footstool, the visual schedule, and the breathing technique — giving you the visual model your text reading can't fully provide.
NCAEP Note: Video modeling is an evidence-based practice for autism (NCAEP, 2020). Watching the Reel and reading this page together increases parent skill acquisition significantly compared to either alone.
Share the Reel
If this Reel reached you and you know another family in the same battle — share it. Every family that finds this information one month earlier is potentially months of their child's discomfort prevented.

Share This With Your Family
Consistency Across Caregivers Multiplies Impact
Why Sharing Matters
If one parent follows the footstool + visual schedule protocol at home but the other parent still allows sitting without the footstool, the inconsistency confuses the child's nervous system and slows progress. If grandparents don't know about the sticker chart, their well-meaning responses ("just push it out!") undermine months of fear extinction work.
Consistent application across ALL caregivers — both parents, grandparents, teachers, nannies — is one of the strongest predictors of successful outcomes. The WHO CCD Package emphasizes multi-caregiver training as critical for intervention generalization.
Share Options
- 📱WhatsApp: Share this page to your family group
- 📧Email: Forward to co-parents, grandparents, teachers
- 🔗Copy Link: techniques.pinnacleblooms.org/gastrointestinal/chronic-constipation-materials-E-500
📥 Downloadable Materials
- Family Guide (1-page PDF) — Simplified overview of all 9 materials for secondary caregivers
- Toileting Routine Card — Visual schedule for grandparents and school
- Sticker Chart Template — Print and use at home
Teacher Communication Template
"My child is on a bowel health program that includes scheduled toilet sits after meals. Could they have bathroom access 20 minutes after lunch? They have a visual schedule. Please respond neutrally to any accidents — shame worsens the underlying condition. Thank you."
ACT VI — CLOSE & LOOP
Frequently Asked Questions
Q: My child has been constipated for 3 months. Do I start the behavioral program now?
Not without medical evaluation first. Three months of constipation may involve impaction that requires medical clean-out before any behavioral program can succeed. Start with your pediatrician, get medical management in place, and then add behavioral and sensory interventions on top of that foundation.
Q: My child has soiling accidents. Is that constipation or something else?
Paradoxically, most soiling (encopresis) in children is caused by constipation, not diarrhea. When stool is impacted, liquid stool leaks around the blockage. This is a medical sign — see your pediatrician. The soiling will stop when the impaction resolves and the bowel regains normal function.
Q: How long before I see results?
Physical results (softer stool) may appear within 1–2 weeks of dietary and medical changes. Behavioral results (reduced resistance) typically emerge at 3–6 weeks. Bowel regularity typically normalizes at 6–12 weeks. Soiling elimination often happens at 8–12 weeks. Full toileting independence may take 6–18 months depending on severity.
Q: My child absolutely refuses to sit on the toilet. Where do I start?
Start with desensitization, not compliance. Week 1: walk past the bathroom without distress? Week 2: stand in the doorway? Week 3: touch the toilet? Week 4: sit on the toilet fully clothed for 30 seconds? Progress up the hierarchy slowly. Do not jump to extended toilet sits when severe avoidance is present.
Q: Should I use a potty chair instead of the toilet?
For younger children (2–4 years) or children with significant toilet anxiety, a child-sized potty chair can reduce fear and gives more floor contact. When comfortable with the potty, transition to the toilet with a seat reducer and footstool. The potty is a valid intermediate step.
Q: My pediatrician says just use Miralax. Is the behavioral program really necessary?
Miralax (PEG) should be the medical foundation. However, if the pain-fear-withholding behavior cycle is not addressed, constipation will return when softeners are stopped. The behavioral program addresses the cycle; the medication addresses the current impaction. Both are needed for durable resolution.
Q: How do I talk to my child about this without creating shame?
Body-neutral, factual language: "Poop is waste that everyone's body makes. It needs to come out to keep our body healthy. When we hold it in, it gets harder." Never suggest the child is wrong, bad, or choosing to cause problems. The soiling is not chosen. The fear is not chosen. The body is doing the best it can.
Q: My child is 12. Is this protocol still appropriate?
Yes, with age-appropriate modifications. Older children deserve to be involved in every decision — which materials to use, which rewards they choose. Frame everything through health autonomy: "We're helping your body work the way it should." Professional support (adolescent OT + GI) is especially important at this age.
Didn't find your answer? Ask GPT-OS® → | Book teleconsultation → 9100 181 181
Preview of 9 materials that help with chronic constipation Therapy Material
Below is a visual preview of 9 materials that help with chronic constipation therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Promise
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
CRO · Pediatric OT · Pediatric ABA/BCBA · Pediatric SLP · Pediatric NeuroDev · Pediatric GI · SpEd · WHO/UNICEF-aligned · 70+ Centers · India
Every technique on this platform was developed through millions of real clinical encounters with real children and their families — across 70+ centers, distilled into tools that work at home.
Chronic constipation has stolen routines, sleep, school days, and confidence from thousands of children who didn't have to suffer this long. You found this page. Your child's outcome changes from this moment.
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centers · Patents filed in 160+ countries · AbilityScore® · TherapeuticAI® · FusionModule™ · EverydayTherapyProgramme™
→ Next in the GI & Toileting Series
E-501: Encopresis and Soiling
When accidents become daily. When shame is settling in. When the stool is coming out but not where it should.
This content is educational. It does not replace individualized assessment and intervention planning with licensed medical professionals, pediatric gastroenterologists, and therapists. Chronic constipation may require medical evaluation and treatment. Seek professional help for persistent symptoms. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. techniques.pinnacleblooms.org/gastrointestinal/chronic-constipation-materials-E-500