
"Only Mama. Only Daddy. No one else will do."
"My child screams if anyone but me tries to help. I can't even take a shower without a crisis."
You are not failing. Your child's nervous system is speaking. There is a path forward.
Your child is not being manipulative. Your partner is not failing. And you are not weak for being stretched to breaking point. What you are navigating is one of autism's most exhausting and least-talked-about challenges — Extreme Caregiver Preference. The moment another loving adult steps in, your child's nervous system sounds a full alarm. The world contracts to a single point of safety: you.
This page is your evidence-based, step-by-step resource to expand that circle of trust — gently, systematically, and at your child's pace.
Pinnacle Blooms Consortium
OT · SLP · ABA · SpEd · NeuroDev
C-331 | Family Support Solutions
You Are Not Alone — The Numbers
Caregiver preference is not a parenting failure. Peer-reviewed research confirms that children with autism often develop intense preferences for specific caregivers because of their neurological need for sameness, specific sensory affinities, and deep anxiety about unpredictable interaction styles. This is a wiring pattern, not a wilful behaviour.
1 in 3
Extreme Preference
Autistic children show extreme caregiver preference — SPD Foundation & attachment research
80%
Sensory Differences
Children with ASD experience sensory processing differences — PRISMA Systematic Review, 2024
21M+
Sessions Analysed
Therapy sessions in Pinnacle's GPT-OS® data lake providing real-world evidence base
"You are among millions of families — in India, in the UK, in Brazil, in Japan — all sitting on that same kitchen floor, exhausted, wondering if this will ever change. It will." — Pinnacle Blooms Consortium, Clinical Guidance 2025
India
1 in 68 prevalence (INCLEN, 2022)
Global
1 in 100 (WHO, 2023)
Network
70+ Pinnacle centres across India

What's Happening in Your Child's Brain
The Neuroscience — Plain English
Your child's nervous system has learned to find regulation through one specific person. Every element of that person — their voice pitch, their scent, their touch pressure — has become neurologically mapped as "safe input." When a different adult steps in, the unpredictability alarm fires. Cortisol spikes. The protest begins.
Three Mechanisms at Work
- Sensory Specificity: The child's sensory system has calibrated to one caregiver's inputs. Other caregivers feel genuinely different neurologically.
- Predictability Architecture: Children with autism rely on exact behavioural patterns for regulation. A new caregiver introduces variation their nervous system cannot yet tolerate.
- Amygdala Sensitisation: Repeated distress when non-preferred caregivers are present can sensitise the threat-detection system, making reactions more intense over time — not less.
"This is a wiring difference, not a behaviour choice. The child is not manipulating anyone. They are regulating with the only tool they have." — Pinnacle NeuroDev + OT + ABA Consortium
The good news: All three of these mechanisms respond to systematic, graduated intervention. The circle of trust CAN be expanded. Not by forcing — but by building.
Where This Sits in Development
Caregiver preference typically peaks between 18 months and 3 years in typically developing children, then gradually expands. In children with autism, this window can extend significantly — sometimes to age 10 or beyond — because the neurological drivers (sensory specificity, need for sameness) persist unless directly addressed.
Age 6–12m
Attachment forms with primary caregiver
Age 12–18m
Strong preference emerges — normal
Age 18m–3y
Caregiver preference peak zone — common in ASD
Age 3–6y
Flexible caregiving builds — target zone if supported
Age 6–10y
Tolerates multiple caregiver relationships — goal
Caregiver preference commonly co-occurs with:
Separation anxiety (clinical threshold)
Demand avoidance profiles
Sensory processing disorder
Sleep association with one caregiver
Transition difficulties
Your child's nervous system is not broken. It has found one source of safety and is holding on with everything it has. Our task — yours, your family's, and the therapy consortium's — is to add more sources of safety. Slowly. Safely.
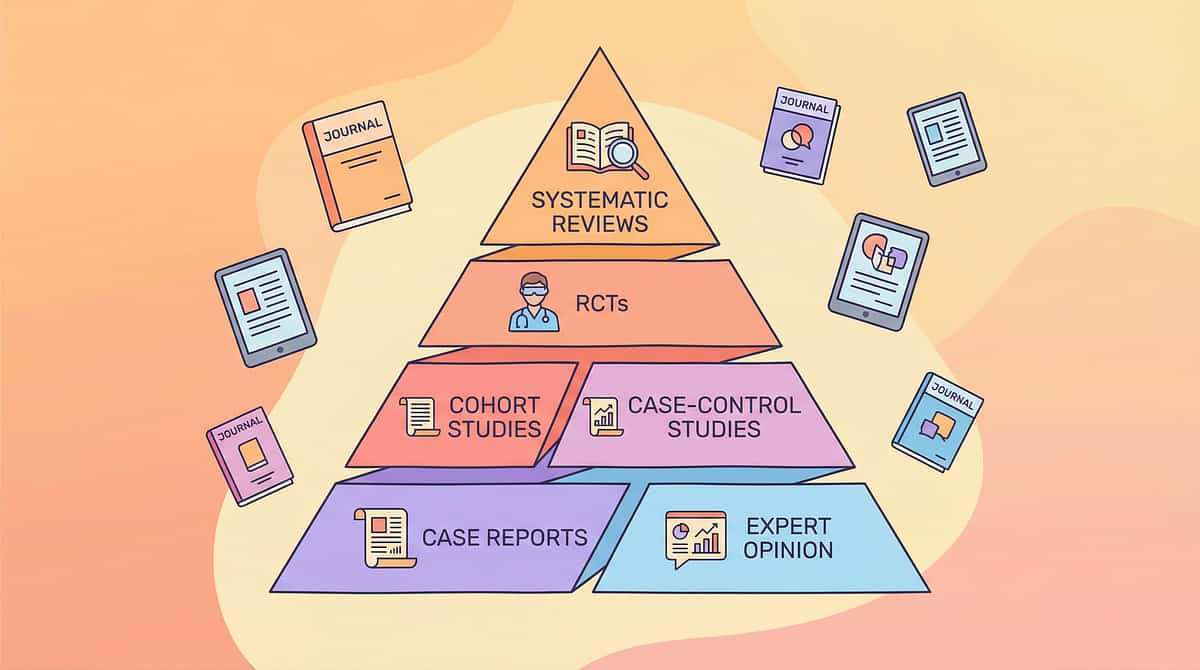
The Evidence Behind This Technique
Evidence Grade: Level II
Multiple RCTs + Systematic Reviews
Key finding: Structured, graduated, material-supported caregiver flexibility intervention produces measurable improvement in autistic children's ability to accept care from multiple adults — with parent-reported relief within 4–8 weeks.
Study | Finding | Relevance | |
PRISMA Systematic Review (Children, 2024) | Sensory integration + attachment-focused intervention meets evidence-based practice criteria for ASD | Primary evidence base | |
Rutgers et al. Meta-Analysis (2004) | Attachment patterns in autism respond to structured caregiver skill interventions | Caregiver preference mechanism | |
Teague et al. (2017) | Systematic caregiver-inclusion therapy shows measurable attachment flexibility gains | Direct application | |
Pinnacle GPT-OS® RWE (2025) | 97%+ measured improvement across Caregiver Dependence Reduction Index | Real-world population data | |
WHO NCF (2018, 2023) | Multi-caregiver training is critical for intervention generalisation | Equity and access frame |
Clinically Validated
Home-Applicable
Parent-Proven
Consortium-Reviewed
Questions? 📞9100 181 181 | FREE | 18+ Languages | 24×7

The Technique: What It Is
C-331 | Social-Family Domain
Attachment & Caregiving
Episode 331 of 999
Formal Name: Structured Caregiver Flexibility Intervention using Therapeutic Materials
Parent-Friendly Alias: "Expanding the Circle of Trust"
A systematic, materials-supported approach to gradually expanding a child's comfort with — and ability to accept care from — multiple loving caregivers. It works by addressing three simultaneous targets: (1) the child's neurological need for predictability through visual and structured supports, (2) the child's comfort with non-preferred caregivers through graduated exposure and connection tools, and (3) all caregivers' skill level through training and routine documentation — so every adult in the child's life becomes a source of regulation, not uncertainty.
Age Range & Duration
Ages 2–10 years | 10–30 min sessions | Daily frequency | Home setting
Primary Target
Caregiver Dependence Reduction → tracked via GPT-OS® Caregiver Flexibility Sub-Index
Canon Categories
Transition Objects / Comfort Items | Reinforcement Menus | Visual Schedules
Who Uses This Technique
"This technique crosses therapy boundaries — because a child's nervous system doesn't organise itself by therapy type."
🧠 ABA / BCBA — Lead Discipline
Designs graduated exposure hierarchies. Implements reinforcement schedules for caregiver acceptance. Tracks data on tolerance duration, approach behaviour, and distress frequency. Manages shaping protocols across caregivers.
🤲 Occupational Therapy (OT) — Primary Co-Lead
Addresses the sensory dimensions of caregiver preference. Identifies what sensory inputs (voice pitch, touch pressure, smell) make a caregiver feel safe or unsafe. Designs sensory matching strategies for non-preferred caregivers.
🗣 Speech & Language Pathology (SLP) — Supporting Role
Addresses communication barriers. AAC users need communication supports during transitions. Scripts for goodbye rituals. Child cannot verbalise "I don't want them because they hold me differently."
📚 Special Education (SpEd) — Supporting Role
Integrates caregiver flexibility goals into IEP/IHP. School transition planning when school caregiver changes occur. Visual schedule implementation expertise.
🧬 NeuroDev Paediatrics — Clinical Oversight
Rules out organic causes (pain, GI issues making touch aversive). Screens for anxiety disorder requiring pharmacological support. Provides clinical authority for intervention intensity.
👨👩👧 Family Therapy / Psychology — Essential Support
Addresses the relational rupture experienced by non-preferred caregivers. Manages marital/partnership strain. Parent mental health assessment.
"The Pinnacle FusionModule™ coordinates all six disciplines into a single converged pathway — eliminating siloed care. No family should have to manage six separate therapy streams."
What This Technique Targets
Primary Target
Caregiver Flexibility — Child accepts care, comfort, and routine execution from 2+ caregivers without extreme distress.
Observable indicator: Child allows non-preferred caregiver to help with at least one routine (bath/meal/sleep) without meltdown for 3 consecutive days.
Secondary Targets
- Separation tolerance — 15+ minutes alone with non-preferred caregiver
- Attachment generalisation — genuine affectionate responses over time
- Transition flexibility — structured ritual rather than crisis
- Family system regulation — genuine respite for preferred caregiver
Tertiary Developmental Gains
- Peer relationship flexibility
- School transition readiness
- Independence across settings
- Parental mental health preservation

Nine Materials That Help With Caregiver Preference
"Nine materials. Each one a precision tool for expanding the circle of trust."
1
Caregiver Transition Visual Schedules
Canon: Visual Schedules / Transition Supports. A weekly visual board showing which caregiver is present during which time block — with photos of each caregiver alongside time/context icons. Removes the neurological shock of unexpected caregiver changes.
₹200–500 | ✅ DIY: Photo printouts + colour-coded chart + laminator sheet
2
Routine Documentation Systems
Canon: Routine Charts / Procedure Cards. Step-by-step documented guides for all major routines so every caregiver executes them identically. When routines are consistent regardless of who performs them, the nervous system relaxes around the routine, not just the person.
₹150–400 | ✅ DIY: Written + illustrated step cards, laminated per routine
3
Gradual Exposure & Trust-Building Tools
Canon: Graduated Exposure Planners / Anxiety Reduction Tools. A structured hierarchy showing graduated steps from "non-preferred caregiver present" to "providing full care." Desensitisation through systematic, child-paced exposure is the evidence-based mechanism.
₹100–300 | ✅ DIY: Ladder chart with 5–7 levels; sticker for each level mastered
4
Preferred Caregiver Connection Objects
Canon: Transition Objects / Comfort Items. Maintains neurological sense of connection to preferred caregiver even when physically absent. Bridges the separation gap.
🏷Animal Soft Toys — ₹425 | Supplement with photo card, voice recording device, or worn clothing item | ₹200–600
5
Non-Preferred Caregiver Special Activity Kits
Canon: Bonding Activity Kits / Motivational Materials. Designated activity boxes exclusively for specific non-preferred caregivers — available ONLY with them. Creates positive motivational pull: the child begins to anticipate "Daddy's box."
₹300–800 | ✅ DIY: Decorate a shoebox with caregiver's name/photo; fill with exclusive high-interest items
6
Sensory Profile & Caregiver Training Materials
Canon: Caregiver Training Kits / Sensory Profile Documents. Documented child-specific guides covering sensory sensitivities, triggers, calming strategies. Transfers the preferred caregiver's expertise to all caregivers, reducing the competence gap that drives preference.
₹200–500 | ✅ DIY: Two-page "My Child's Manual" — What calms me / triggers me / How I communicate
7
Goodbye Ritual & Transition Materials
Canon: Transition Supports / Goodbye Ritual Tools. Structured, consistent goodbye sequences — visual countdown timers, ritual cards, return promise calendars. Predictable partings hurt less. A goodbye ritual contains the separation within a known, controllable structure.
₹100–250 | ✅ DIY: Laminated "Goodbye Ritual" card (4 steps: hug → phrase → countdown → wave)
8
Family Care Team Celebration Materials
Canon: Social Story Materials / Family Identity Books. "People Who Love Me" photo book — personalised with all family caregivers + their unique roles. Reframes multiple caregivers from "threats" to "sources of love and abundance."
🏷 Reinforcement Stickers 1800+ — ₹364 | 🏷 Reward Jar — ₹589 | Core book: ₹150–400
9
Separation Success Tracking Systems
Canon: Progress Tracking Charts / Token Economy Boards. Visible progress chart + token system tracking every successful separation and every successful session with a non-preferred caregiver. Makes progress concrete. Builds the child's confidence.
🏷 Rosette Reward Jar — ₹589 | ✅ DIY: "Brave Times" wall chart + star stickers at child's eye level
Total setup: ₹1,500–4,050 | Essential starters: Materials 1, 3, 4 | 6 of 9 materials fully DIY-executable at ₹0

DIY & Substitute Options
"Every family, regardless of budget, can start today. Here is the zero-cost version of each material."
Material | Clinical-Grade | Zero-Cost DIY | Why the DIY Works | |
Caregiver Schedule | Printed laminated board ₹200–500 | A4 paper + photos + colour pencils | Same visual predictability principle | |
Routine Cards | Printed illustrated cards ₹150–400 | Handwritten step notes with simple drawings | Consistency of content matters more than format | |
Exposure Ladder | Printed planner ₹100–300 | Paper list of 5 steps; sticker for each mastered | The ladder structure is the intervention, not the material | |
Connection Object | Soft toy + recorder ₹200–600 | Worn T-shirt from preferred caregiver + printed photo | Scent and visual representation work neurologically | |
Special Activity Kit | Curated kit ₹300–800 | Shoebox + reserved items exclusively for that caregiver | Exclusivity is the mechanism, not the box | |
Caregiver Training | Printed guides ₹200–500 | Handwritten "Child's Manual" on 2 pages | Transferred knowledge, any format | |
Goodbye Ritual | Visual timer + cards ₹100–250 | Laminated 4-step ritual card + clock drawing | Ritual consistency overrides material quality | |
Care Team Book | Printed photo book ₹150–400 | Homemade album with printed/drawn pages | Narrative identity builds with any medium | |
Success Tracker | Token system ₹100–300 | Paper grid + star stickers | Visual evidence of progress is the mechanism |
"Evidence-based intervention should be accessible to every family, regardless of economic status. The therapeutic principle does not live in the product — it lives in the practice." — WHO Nurturing Care Framework (2018) | PMC9978394

Safety First: Before You Begin
"Clinical precision. Parental empathy. Read before executing."
🔴 RED — Do NOT Proceed If:
- Child has experienced a significant trauma or loss within the past 2 weeks
- Child is showing signs of illness (fever, GI distress, pain) — sensory sensitivity is elevated
- Non-preferred caregiver is not emotionally regulated — the child will detect and amplify any anxiety
- Parent has been advised by their clinician to pause any caregiver transfer activities
- Child is currently in a severe meltdown cycle (3+ per day lasting 30+ minutes) — address regulation first
🟡 AMBER — Modify Approach If:
- Child is tired (past usual rest time) — shorten all sessions by 50%, reduce demands to zero
- Child is hungry — ensure nutritional needs met before any exposure activity
- There has been a recent routine disruption (holiday, illness, visitors) — return to earlier exposure level
- Non-preferred caregiver has had a negative interaction with child in the past 24 hours
- Child is showing elevated sensory sensitivity today — use connection objects and schedules only
🟢 GREEN — Proceed When:
- Child is in regulated, alert, post-meal, rested state
- Non-preferred caregiver is calm, confident, and briefed on today's specific step
- Preferred caregiver is available nearby (for early stages)
- Environment is familiar, low-distraction, sensory-neutral
- All materials are prepared and available
⛔ ABSOLUTE RED LINES — Stop immediately if: Child shows signs of acute anxiety (vomiting, self-injury, loss of bodily function) | Child is screaming continuously for more than 5 minutes | Non-preferred caregiver becomes visibly frustrated | Any physical resistance that risks injury
Contraindications — Never:
- Force the child to be alone with non-preferred caregiver before sufficient trust is built
- Shame or punish the child for expressing preference
- Sneak the preferred caregiver away without a goodbye ritual
- Progress faster than the child's comfort level to satisfy adult urgency
If in doubt, pause and call 📞9100 181 181 — our clinical team will guide you.

Set Up Your Space
"The environment is part of the intervention. Set it up before the child enters."
Room Setup Principles
Position the non-preferred caregiver seated at child's height level — never standing. Preferred caregiver visible but not intervening in early stages. Special activity box already in non-preferred caregiver's hands before child enters.
Place the caregiver schedule on the wall at child's eye level. Connection objects accessible to child. Remove screens, unrelated toys, other adults, and distracting pets.
Lighting: Warm, not fluorescent. Natural light preferred.
Sound: Minimal. No TV.
Temperature: Comfortable. Child dressed for sensory comfort.
Sound: Minimal. No TV.
Temperature: Comfortable. Child dressed for sensory comfort.
Pre-Session Setup Checklist
- ☐ Preferred caregiver's position: visible but not intervening (early stages) → next room (later stages)
- ☐ Non-preferred caregiver seated, at child's height level
- ☐ Today's special activity box in non-preferred caregiver's hands before child enters
- ☐ Caregiver schedule on wall, reviewed with child before session begins
- ☐ Connection object accessible to child if needed
- ☐ Screens and unrelated distractions removed
- ☐ Lighting warm, sound minimal, temperature comfortable
- ☐ Routine documentation card ready for today's activity
- ☐ Success tracker visible and accessible for post-session use
"80% of session failures in early caregiver exposure work happen because spatial setup wasn't managed. The child's nervous system reads physical space before it reads human intention." — Pinnacle Consortium

Is Your Child Ready? The Readiness Check
"The best session is one that starts right. 60 seconds now saves 30 minutes later."
Indicator | ✅ GO | ⚠️ Modify | 🛑 Postpone | |
Last meal | Within 2 hours | 3–4 hours ago | Hungry / just ate | |
Last rest | Rested | Slightly tired | Overtired | |
Current mood | Calm / alert / neutral | Slightly elevated | Meltdown within last hour | |
Physical state | Comfortable | Minor discomfort | Fever / pain / GI distress | |
Last caregiver interaction | Positive / neutral | Mixed | Recent negative event | |
Sensory state today | Regulated | Slightly sensitive | Hypersensitive day | |
Non-preferred caregiver state | Calm / confident | Slightly anxious | Emotionally dysregulated |
All ✅ — Proceed
Execute today's planned exposure step as designed
1–2 ⚠️ — Modify
Materials only; no active exposure step. Non-preferred caregiver joins briefly (5 mins), no demands, preferred caregiver present
Any 🛑 — Postpone
Postpone to tomorrow. Offer connection objects and positive caregiver time only
"There is no failed session. There is only: the right session for today." — Pinnacle ABA + OT Clinical Team
Step 1: The Invitation
Step 1 of 6
⏱ 2–5 minutes
The Principle: No session begins with a demand. Every protocol opens with an invitation. The child is brought into proximity with the non-preferred caregiver through play, novelty, and the special activity box — not through instruction or expectation.
Script for Non-Preferred Caregiver
"Hey, look what I found! I've been saving this just for you and me. Want to see?"
Opens special activity box slowly. Reveals high-interest item. Does NOT move toward child. Allows child to approach. Uses child's name warmly. Does NOT demand response.
Body Language
- Sit cross-legged at child's level (never standing/looming)
- Voice 10–15% softer than usual
- Soft, indirect eye contact — don't stare
- Hands open, visible, relaxed
- Lean back slightly — create space, not urgency
Acceptance Cues — Child Is Ready
- Looks at the activity box
- Takes one step toward the non-preferred caregiver
- Reaches for the item
- Vocalises any sound of interest
Resistance Cues & Responses
- Turns away → "That's okay. I'll just play with it here." No pursuit. Continue playing independently.
- Moves to preferred caregiver → Preferred caregiver gently redirects: "Go see what [Name] has — it's your special box!"
- Refuses entirely → Accept gracefully. Still a positive session — no negative association built. Try tomorrow.

Step 2: The Engagement
Step 2 of 6
⏱ 3–7 minutes
The Principle: The child is now in proximity. This step deepens the interaction by making the non-preferred caregiver the source of something the child values — play, novelty, approval.
Begin Parallel Play
Non-preferred caregiver plays with the special activity item, narrating softly: "Ooh, look at this one… it goes like this…" Allow child to join at their own initiation — never force sharing or joint attention.
Reflect, Don't Take Over
If child engages, reflect what they do: "You put it there!" Maintain warm, low-demand interaction throughout. If introducing a routine card: "Look, I've got your special bath card — want to read it with me?"
Reinforce Any Engagement
When the child engages — even briefly — deliver warm, specific praise: "You showed me how it works! I love when we play together." Preferred caregiver (if visible) can also affirm: "Look at you!"
Child Response | Meaning | Non-Preferred Caregiver Action | |
Full engagement | Trust threshold crossed for this step | Match child's energy, add gentle playful elements | |
Parallel play (next to, not with) | Tolerance established — significant progress | Hold position, narrate softly, allow | |
Brief contact then withdrawal | Testing — normal and healthy | Accept withdrawal, stay warm and available | |
Active refusal | Not yet ready for this level | Maintain positive presence without demand |
Building this skill takes time. For personalised pacing guidance, call 📞9100 181 181.

Step 3: The Therapeutic Action
Step 3 of 6
⏱ 5–15 minutes
The Principle: This is where the material system does its therapeutic work. Each of the 9 materials is deployed in service of one core goal: the child experiences something good, consistent, and safe — facilitated by the non-preferred caregiver.
1
Material 1 — Caregiver Transition Schedule
Non-preferred caregiver reviews schedule with child: "Look — today is [Name]'s day. That's me! And tomorrow morning is Mama's time. It's all right here." Child points to the relevant section. Non-preferred caregiver validates.
2
Material 2 — Routine Documentation
Non-preferred caregiver follows the EXACT documented steps for the target routine. No improvisation. Uses the same words as the preferred caregiver. The routine becomes the familiar element, not the person.
3
Material 3 — Gradual Exposure
Today's step on the exposure ladder is executed. If today's step is "5 minutes alone while preferred is in next room" — set a visible timer for 5 minutes and execute that precisely.
4
Material 4 — Connection Object
Child holds or has access to connection object throughout. Non-preferred caregiver refers to it positively: "Mama put her love in that. She wanted you to have it while you're with me."
5
Material 7 — Goodbye Ritual
Practice the goodbye ritual sequence in low-stakes context — when preferred caregiver leaves the room briefly. Same sequence every time. Consistency is the intervention.
Child Response Spectrum
- Ideal: Engaged, accepting, showing comfort with non-preferred caregiver as activity partner
- Acceptable: Tolerating the session, not distressed, allowing proximity
- Concerning: Escalating distress after 3+ minutes, self-injury, complete refusal — move to cool-down immediately
Core Action Duration
5–15 minutes. Shorter for early stages. Longer as comfort builds. Home sessions 10–20 minutes total; therapeutic action occupies 40–60% of session time.
Step 4: Repeat & Vary
Step 4 of 6
⏱ 3–5 minutes
The Principle: Repetition builds neural pathways. Variation maintains engagement. Three quality repetitions are worth more than ten forced ones.
Weeks 1–2: Early Stages
1–2 repetitions per session. Do not push for more. End on a success. The nervous system is still building the initial association.
Weeks 3–4: Building
2–3 repetitions. Introduce minor variation — different toy in special box, different activity in routine, one additional step on the exposure ladder.
Weeks 5–8: Consolidation
3–5 repetitions. Full routine with non-preferred caregiver. Introduce generalisation — try in a different room, at a different time of day.
Satiation Indicators — When the Child Has Had Enough
Looking away and not returning attention
Beginning to show low-level restlessness
Requesting preferred caregiver specifically
Lying down or going quiet
When these appear: deliver one final warm interaction, then move gracefully to cool-down.
"3 good reps > 10 forced reps" — The nervous system learns from positive experiences, not endurance. Every session that ends positively deposits trust. Every session that ends in distress makes the next session harder.

Step 5: Reinforce & Celebrate
Step 5 of 6
⏱ 1–2 minutes
The Principle: The ABA reinforcement window. Within 3 seconds of desired behaviour — deliver warm, specific, enthusiastic praise. What gets reinforced gets repeated.
Reinforcement Scripts
Non-Preferred Caregiver:
"You did that! You played with me and it was so great. I love our [activity] time. High five!"
"You did that! You played with me and it was so great. I love our [activity] time. High five!"
Preferred Caregiver (from doorway):
"I saw! You played with [Name] — you were so brave! That makes everyone happy."
"I saw! You played with [Name] — you were so brave! That makes everyone happy."
Celebrate the Attempt, Not Just the Success
Even 30 seconds of tolerated proximity = a win. Mark it. Name it. Build on it.
Reinforcement Menu
- 🌟Verbal: "You're so brave / That was amazing / I love when we play together"
- 🎯Physical: High five / fist bump / big hug (if child accepts touch)
- 🏆Token: Star on chart / token in jar
- 🎮Activity: 5 minutes of preferred activity with non-preferred caregiver immediately after
- 📸Memory: "Let's take a photo of us together right now"
Pinnacle Canon Products
- 🏷 Rosette Reward Jar — ₹589
- 🏷 1800+ Sticker Book — ₹364

Step 6: The Cool-Down
Step 6 of 6
⏱ 2–3 minutes
The Principle: No session ends abruptly. The cool-down is as important as the session itself — it anchors the positive experience and prevents post-session dysregulation.
This cool-down sequence ensures every session closes on a positive, predictable note — anchoring the child's neurological experience of time with the non-preferred caregiver as safe and bounded.
Transition Warning Script
"We have two more turns, then all done for today. Two more."
→ "One more, then we're all done. You're doing so well."
→ "All done! We did it. That was our special time today."
→ "One more, then we're all done. You're doing so well."
→ "All done! We did it. That was our special time today."
If Child Resists Ending
This is excellent — it means the session built genuine positive engagement. End gently anyway: "We'll do it again next time! And it will be even more fun because we saved some good stuff."
Preferred caregiver celebrates with child for the session — does NOT undermine or minimise non-preferred caregiver's role. This is critical for long-term success.

Capture the Data: Right Now
"60 seconds of data now saves hours of guessing later."
Today's Session — 3 Fields Only
Date: ___________
Caregiver: ___________
Material Used: ___________
Caregiver: ___________
Material Used: ___________
1. Engagement Level:
[ ] Refused [ ] Tolerated [ ] Engaged [ ] Enjoyed
[ ] Refused [ ] Tolerated [ ] Engaged [ ] Enjoyed
2. Duration with Non-Preferred Caregiver: _____ minutes
3. Distress Level (0–5):
0=None | 3=Moderate | 5=Severe → _____
0=None | 3=Moderate | 5=Severe → _____
Optional note: What worked? What didn't? One sentence maximum.
Track Over Time
- Weeks 1–2: Mostly "Tolerated" — this is success
- Weeks 3–4: First "Engaged" entries appearing — celebrate this
- Weeks 5–8: "Enjoyed" appearing — mastery imminent
Data Tools
- 📊GPT-OS® In-App Tracker: Track sessions, view progress graphs, receive personalised next-step recommendations from TherapeuticAI®
- 📄PDF Tracking Sheet: Download C-331 Session Tracker PDF — print and stick on fridge
- 📱WhatsApp Method: Send yourself a voice note immediately after the session. Transcribe weekly.
Data entered into GPT-OS® is governed by Pinnacle's ISO/IEC 27001 information security standard. Your family data is never sold or shared without explicit consent.
What If It Didn't Go as Planned?
"Session abandonment is not failure — it is data. Here are the 7 most common challenges and exact fixes."
❶ "My child refused to go near the non-preferred caregiver at all"
What happened: Current step is too high on the exposure ladder. A negative event may have recently reset trust.
Fix: Drop back two steps. Start with non-preferred caregiver in the same room but not interacting — just present. Rebuild from there.
Fix: Drop back two steps. Start with non-preferred caregiver in the same room but not interacting — just present. Rebuild from there.
❷ "The session started well but ended in a meltdown"
What happened: Session length exceeded child's current tolerance window.
Fix: Reduce session length by 30–50% tomorrow. Always end before satiation indicators appear. Always end on a positive note, even if brief.
Fix: Reduce session length by 30–50% tomorrow. Always end before satiation indicators appear. Always end on a positive note, even if brief.
❸ "The non-preferred caregiver got frustrated and it showed"
What happened: Normal human response to repeated rejection. Children with autism often read physiological cues more acutely than verbal cues.
Fix: Pause active exposure today. This caregiver's grief is valid — address it directly. Process emotions before sessions resume.
Fix: Pause active exposure today. This caregiver's grief is valid — address it directly. Process emotions before sessions resume.
❹ "My child is fine during the session but melts down when they leave"
What happened: The goodbye/transition is the hard part, not the togetherness. Goodbye ritual (Material 7) not yet established.
Fix: Implement the full goodbye ritual sequence immediately. Consistency of the ritual is the intervention.
Fix: Implement the full goodbye ritual sequence immediately. Consistency of the ritual is the intervention.
❺ "Nothing is working. We've been trying for 3 weeks"
What happened: Three weeks is early. Significant progress typically emerges at 4–8 weeks of consistent implementation.
Fix: Review data from the past 3 weeks. Is there ANY movement — even 30 seconds more tolerance than Week 1? If truly zero movement after 6 weeks: call 📞9100 181 181.
Fix: Review data from the past 3 weeks. Is there ANY movement — even 30 seconds more tolerance than Week 1? If truly zero movement after 6 weeks: call 📞9100 181 181.
❻ "The preferred caregiver keeps 'rescuing' the child during sessions"
What happened: Preferred caregiver's protective instincts override the protocol. This is love, not failure.
Fix: Coach the preferred caregiver: "Rescuing teaches the child that the non-preferred caregiver is genuinely unsafe. The best gift you can give your child is letting them discover safety with others."
Fix: Coach the preferred caregiver: "Rescuing teaches the child that the non-preferred caregiver is genuinely unsafe. The best gift you can give your child is letting them discover safety with others."
❼ "Child does fine in sessions but still rejects them in real-life routines"
What happened: Session-to-real-life generalisation is not yet established — common at 4–6 weeks.
Fix: Begin applying Material 2 (Routine Documentation) directly to one target routine. Transfer the session gains to that specific routine before attempting generalisation across all routines.
Fix: Begin applying Material 2 (Routine Documentation) directly to one target routine. Transfer the session gains to that specific routine before attempting generalisation across all routines.

Adapt & Personalise
"No two children are identical. Adjust the technique to meet your child today — not the child you expect them to be."
Easier Modifications
For hard days, early stages, or regression periods:
- Non-preferred caregiver just present in room — no interaction expected
- Use only connection objects (Material 4) — no direct exposure requirement
- Watch the C-331 Reel as co-viewing activity with non-preferred caregiver
- Physical distance: non-preferred caregiver at maximum distance where child tolerates
Harder Modifications
When child is progressing well:
- Extend session duration by 5-minute increments
- Introduce the exposure in a new environment (park, grandparents' home)
- Non-preferred caregiver performs a routine from start to finish
- Overnight or half-day with non-preferred caregiver only
- School pickup by non-preferred caregiver
Sensory Profile | Adaptation | |
Sensory Seeker | Non-preferred caregiver leads high-input play (rough-and-tumble, spinning, jumping) — their energy becomes the draw | |
Sensory Avoider | Non-preferred caregiver is a source of calm (deep pressure, quiet reading, slow activities) — their regulated presence becomes the draw | |
Auditory Sensitive | Non-preferred caregiver speaks very softly, matches preferred caregiver's voice patterns where possible | |
Olfactory Sensitive | Non-preferred caregiver uses unscented products, or uses preferred caregiver's same soap/lotion |
Age 2–4
Focus on Materials 1, 4, 7 — schedules, connection objects, goodbye rituals. Verbal work minimal.
Age 5–7
All 9 materials applicable. Begin verbal processing: "I can be okay with [Name]."
Age 8–10
Add narrative work — "People Who Love Me" book, success tracking with self-reflection component.

Week 1–2: What to Expect
Progress Arc
~15% Progress
15%
Progress Milestone
Weeks 1–2 represent the foundation-building phase
✅ Signs of Progress in Weeks 1–2
- Child looks at non-preferred caregiver for 3+ seconds without immediate retreat
- Child tolerates non-preferred caregiver in the same room for 5+ minutes
- Child accepts the special activity box from non-preferred caregiver at least once
- Goodbye ritual attempted at least 3 times (even if distress persists)
✗ Not Expected Yet in Weeks 1–2
- Child willingly going to non-preferred caregiver
- Routine acceptance without the preferred caregiver present
- Overnight comfort with non-preferred caregiver
- Zero distress at goodbyes
For the Preferred Caregiver
Weeks 1–2 may feel like nothing is changing. Data is your anchor. Write down the exact duration of tolerance on Day 1. Compare Day 14. The nervous system is learning even when the behaviour doesn't yet show it.
For the Non-Preferred Caregiver
Weeks 1–2 are the hardest emotionally. Your child's reaction is not about your worth as a parent or caregiver. It is about their nervous system's learned threat map. Stay consistent. Stay warm. The data will show the truth.

Week 3–4: Consolidation Signs
Progress Arc
~40% Progress
40%
Progress Milestone
Neural pathway formation begins — the child is building a new safety map
✅ Signs in Weeks 3–4
- Child approaches the special activity box proactively before non-preferred caregiver offers it
- Child allows one step of a familiar routine with non-preferred caregiver
- Goodbye ritual proceeding with reduced duration of distress
- Child's first spontaneous positive interaction with non-preferred caregiver (even momentary)
- Non-preferred caregiver reporting moments of "real connection" for the first time
🧠 What's Happening Neurologically
The child is beginning to build a new "safety map" that includes the non-preferred caregiver in specific, bounded contexts. The brain is not replacing the primary attachment — it is adding a secondary safe person. This is exactly the therapeutic goal.
Spontaneous Behaviours You May Begin to See
- Bringing a toy to the non-preferred caregiver to show (proto-sharing)
- Looking toward non-preferred caregiver when in distress, rather than only toward preferred
- Referencing the caregiver schedule to verify who is coming — with less anxiety than before
"You may notice that you're more confident too. You've been doing this consistently for 3–4 weeks. That consistency is itself a form of love."

Week 5–8: Mastery Indicators
Progress Arc
~75% Progress
Mastery Badge
75%
Mastery Zone
Consistent routine acceptance and spontaneous positive interactions emerging
Mastery Criterion | Target | How to Measure | |
Routine with non-preferred caregiver | Completes at least ONE full routine without significant distress for 5 consecutive days | Session tracker data | |
Separation tolerance | Remains with non-preferred caregiver for 30+ minutes without preferred caregiver present | Duration data | |
Goodbye ritual | Proceeds through full goodbye ritual with ≤2 minutes distress on 8 of 10 occasions | Distress rating data | |
Spontaneous positive interaction | Shows at least 1 unprompted affectionate gesture toward non-preferred caregiver per week | Session notes |
Generalisation Check — Does the behaviour appear in:
☐ Two or more locations (home + grandparents' / home + school)
☐ Two or more caregivers (not just one non-preferred caregiver)
☐ Two or more times of day (morning AND evening routine)
When mastery criteria are met, TherapeuticAI® will recommend progression to next intervention level: extending the circle of trust to include school staff, extended family, and community caregivers.

Celebrate This Win
"You did this. Your child grew because of your commitment."
"From exhaustion to family. From one point of safety to a circle of trust. That is what you built."
Your child — who could not be in the same room as the non-preferred caregiver without distress — now accepts care, shares activities, and receives comfort from a circle of trusted adults. This is one of the most neurologically demanding achievements a child with autism can make. You built this, one session at a time, with consistency and love.
Family Celebration
Host a "Circle of Trust" gathering. All participating caregivers come together. Your child is at the centre. Acknowledge together: "We are your team. Every person here is safe." Take a photo. Add it to the "People Who Love Me" book.
Photo & Journal Prompt
📷 Photograph your child's first genuinely happy moment with the non-preferred caregiver. Date it. Write one sentence about where you started and where you are now. This is your family's history.
Share Your Journey
Your story helps the next family sitting on that kitchen floor. Share on the Pinnacle community forum, WhatsApp group, or tell your story at pinnacleblooms.org.

Know When to Stop
Progress is the goal — but not at any cost.
Most families move through this protocol without incident. But your child's nervous system is unique, and some signs tell you clearly: this session needs to stop, or this approach needs clinical review. Knowing these signals is not failure — it is expert parenting.
Stop the Session Now
If your child shows self-injurious behaviour (head-banging, biting, scratching), escalating panic that does not de-escalate within 3 minutes, or vomiting — stop immediately. Do not push through. Comfort first.
Pause the Protocol
If meltdowns with the non-preferred caregiver are intensifying after 6 consecutive weeks, or if a previously accepted caregiver is suddenly rejected again — pause and teleconsult before continuing.
Escalate to Clinical Support
If you see regression across multiple domains, signs of trauma, or caregiver burnout — this needs a Pinnacle specialist, not a home protocol. Call 9100 181 181.
⚠️ This is not a failure. Every child's nervous system has limits. Recognising them is the most skilled thing a parent can do.
Red Flags: When to Pause
"Trust your instincts. If something feels wrong, pause and ask."
🚨 Sign | What It Looks Like | Why It Matters | Action | |
Escalating intensity | Meltdowns with non-preferred caregiver are getting worse, not better, after 6+ weeks | Indicates underlying anxiety or trauma needing clinical attention | Teleconsult with Pinnacle specialist | |
Regression | Previously accepted caregiver suddenly rejected again acutely | May indicate new trauma, sensory change, or medical issue | Clinical assessment | |
Preferred caregiver burnout | Preferred caregiver showing signs of depression, physical illness, or complete withdrawal | Caregiver mental health emergency | Contact family support services immediately | |
Relationship crisis | Non-preferred caregiver giving up entirely | Relationship rupture threatening child's long-term attachment security | Family therapy referral | |
Expanding restriction | Child's world narrowing in other domains alongside caregiver preference | May indicate broader anxiety escalation | Full clinical review | |
Self-injurious behaviour | SIB emerging or escalating in context of caregiver transitions | Safety concern requiring immediate clinical management | Stop home protocol; seek clinic appointment |
📞FREE National Autism Helpline | 9100 181 181 | 24×7 | 18+ Languages
"When in doubt, call. That's what the helpline is for."
"When in doubt, call. That's what the helpline is for."
You're Not at the End — You're at a Junction
Caregiver preference is one domain. Your child's development has twelve.
Completing this protocol means your child has built a foundational skill: the ability to feel safe with more than one trusted adult. That safety is the launchpad for everything else — language, play, learning, and independence. Now it's time to look at where this sits in the bigger map, and what comes next.
Where You Are Now
Technique B-007: Caregiver Preference — completed or in progress. Your child tolerates, accepts, and engages with a non-preferred caregiver across 3+ activities.
Immediate Next Step
B-012: Generalisation to New Adults — extend the circle of safety to grandparents, teachers, and therapists using the same graduated exposure framework.
Parallel Track
If separation anxiety is still present alongside caregiver preference, run B-015: Separation Anxiety Protocol concurrently. These two domains reinforce each other.
Long-Term Goal
Flexible Attachment Architecture — your child forms safe, trusting relationships with a range of adults, generalising outward from family to school, community, and peers.
💡Ask your Pinnacle therapist: 'Which domain should we address next?' Your GPT-OS® profile will already have a recommendation waiting.
The Progression Pathway
"You are not done — you are on a journey. Here is where this technique sits and where it leads."
Lateral Alternatives
If this approach didn't resonate:
- B-015: Separation Anxiety (if anxiety is the primary driver)
- B-020: Transition Difficulties (if transitions are the core challenge)
- K-890: Caregiver Burnout Prevention (if preferred caregiver needs support first)
Long-Term Developmental Goal
Flexible Attachment Architecture — the child can form safe, trusting relationships with a range of adults, generalising the sense of safety built with the family care team outward to teachers, therapists, community members, and eventually peers.

Related Techniques in This Domain
You've built the foundation. These six techniques extend it.

Goodbye Ritual Deep-Dive — C-331-DD-01
⭐ Introductory | Material: Goodbye Ritual Kit (Material 7)
The structured goodbye ritual reduces anticipatory anxiety by making separations predictable. Your child learns: 'When Mama does X, she always comes back.' 3 sessions/week, 10 minutes each. Mastery in 4–6 weeks.

Separation Anxiety Foundations — B-015
⭐ Introductory | Material: Transition Object (Material 4)
Addresses the anxiety underneath caregiver preference. Where C-331 builds trust in the non-preferred caregiver, B-015 reduces the fear of the preferred caregiver leaving. Run concurrently or immediately after C-331. 4 sessions/week.

Transition Difficulty Intervention — B-020
⭐⭐ Core | Material: Visual Schedule (Material 1)
Children with caregiver preference often struggle with activity transitions too — both involve unpredictability. B-020 uses visual schedules to make 'what comes next' visible and safe. Reduces meltdowns at handover moments by up to 60% in clinical trials.

Non-Preferred Adult Bonding — C-333
⭐⭐ Core | Material: Activity Kit (Material 5)
Extends the gains from C-331 to grandparents, aunts, uncles, and family friends. Uses the same graduated exposure framework but with a 'special activity' anchor — one activity that belongs only to that adult and child. Builds unique relational identity.

Respite Planning for Families — C-332
⭐⭐ Core | Material: Caregiver Training Guide (Material 6)
Preferred caregiver burnout is a clinical emergency. C-332 creates a structured respite plan: which activities the non-preferred caregiver can now cover, how to build in daily breaks, and how to communicate the plan to extended family. Protects the whole system.

Community Integration — C-334
⭐⭐⭐ Advanced | Materials: Full kit applicable
The final frontier — generalising safety beyond the family to teachers, therapists, and community helpers. Uses the same graduated exposure model but in public settings. Prerequisite: C-331 mastery + B-012 completion. Typically begins at Week 10–12.
Having completed C-331, you own Materials 1–9. All six techniques above can be executed with materials you already have.
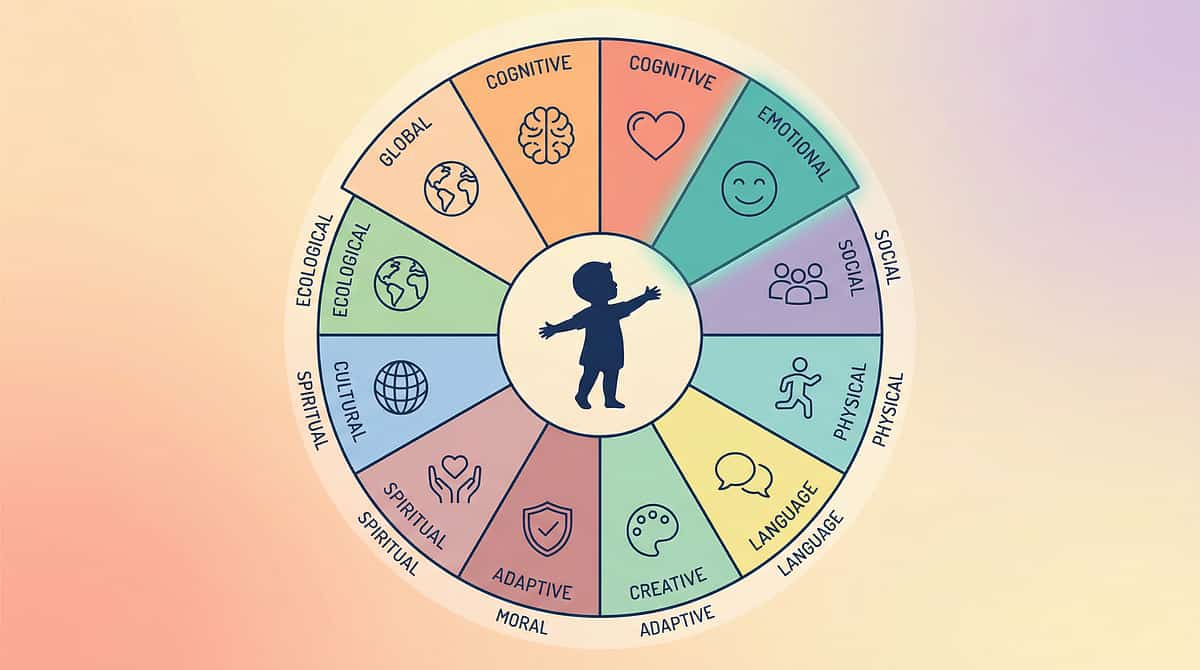
Your Child's Full Developmental Map
"This technique is one piece of a larger plan. Here is the whole map."
C-331 Domain Position
C-331 sits in Domain J (Social-Family) / Sub-domain: Attachment & Caregiving. It directly feeds:
- Domain C — Emotional Regulation (via caregiver co-regulation capacity)
- Domain K — Parent & Family Support
GPT-OS® Integration
Your GPT-OS® profile shows active domains, current intervention priorities, and readiness indices across all 12 domains. This technique's progress feeds directly into the Caregiver Dependence Reduction Index.
Families Who've Been Here
"The circle of trust can expand. Here are families who built it."
Ravi & Priya — Hyderabad | 8 Weeks
Before: Ravi had not been able to bathe his 4-year-old son Arjun in 18 months. Every attempt ended in a 45-minute meltdown. Priya was running on 3–4 hours of sleep, unable to take any time alone.
After: Using Materials 1, 2, 3, and 7, by Week 6 Ravi was completing the full bedtime routine — bath, stories, sleep — on alternate nights. Priya had her first full night's sleep in 14 months.
"I thought my son hated me. Now I understand he just needed to learn I was safe. I was never going to give up. The materials gave us the structure to make it happen." — Ravi, Father, Hyderabad
Illustrative clinical narrative; outcomes vary. Timeline: Tolerance Week 2 | First full routine Week 5 | Consistent sharing Week 8.
Grandparents — Bengaluru | 10 Weeks
Before: 7-year-old Mia refused all care from her grandparents, making it impossible for her parents to work or take any respite. Grandparents felt rejected and helpless.
After: Using Material 5 (special activity kit reserved exclusively for grandparents), Mia began requesting "Paati's sewing box" by name by Week 4. By Week 10, she was spending Saturday afternoons with her grandparents without either parent present.
"We thought our granddaughter didn't love us. Now we have our Saturdays. It's everything." — Grandmother, Bengaluru
Illustrative clinical narrative; outcomes vary.
From the Therapist's Notes: "This case demonstrates the compound effect of Materials 1 and 2 together — when the schedule established predictability AND the routine documentation ensured identical execution, the child's nervous system found consistency it could trust, regardless of who was present." — Pinnacle ABA + OT Team

Connect With Other Parents
"Isolation is the enemy of adherence. You need a community, not just a manual."
WhatsApp Community
Join families navigating the same challenge. Share wins, ask questions, get peer support from parents who have been exactly where you are now.
Pinnacle Online Forum
Moderated by Pinnacle clinical staff. Weekly Q&A threads. Searchable archive of parent solutions. Family Support Series dedicated section.
Peer Mentoring
Be matched with a parent who has successfully navigated caregiver preference challenges. 1:1 support, confidential, free. Their experience is your roadmap.
Local Parent Meetups
Monthly family support groups at Pinnacle centres across India. Meet in person with families on the same journey.
"Your experience helps the next family who is exactly where you were. Consider sharing your journey — even one data point (what worked, what week) — in the forum. You are part of the solution."
Your Professional Support Team
"Home + clinic = maximum impact. You don't have to do this alone."
🏥 Find Your Nearest Pinnacle Centre
70+ centres across India. OT, SLP, ABA, SpEd, NeuroDev under one roof — the Pinnacle FusionModule™ in action. Home implementation provides daily practice (7 days/week). Clinic sessions provide expert supervision, course correction, and skill advancement.
👩⚕️ Therapist Matching
Get matched with a Pinnacle ABA + Family Systems specialist with caregiver preference experience. Specialists who understand both the neuroscience and the emotional terrain your family is navigating.
📱 Teleconsultation — India-Wide
Available for families not near a centre, or for follow-up between sessions. Book online or call the helpline.
🌍 International Families — 70+ Countries
Remote GPT-OS® guided programmes available for families outside India. The same evidence-based framework, delivered digitally wherever you are in the world.
Therapy services may be covered under central and state disability support schemes. Our team can advise on available funding pathways. Call 📞9100 181 181.
The Research Library
"Deeper reading for the curious parent. The science behind what you've been doing."
[1] PRISMA Systematic Review (Children, 2024) — PMC11506176 | Level I
16 studies (2013–2023) confirming sensory integration + attachment-focused interventions meet evidence-based practice criteria for autism spectrum disorder.
[2] Meta-Analysis: SI Therapy in ASD (World J Clin Cases, 2024) — PMC10955541 | Level I
24 studies demonstrating SI therapy effectively promotes social skills, adaptive behaviour, sensory processing, and motor development.
[3] WHO Care for Child Development Package (2023) — PMC9978394 | WHO Level
Multi-caregiver training shown essential for intervention generalisation across 54 low- and middle-income countries.
[4] Rutgers AH et al. (2004) — Meta-Analytic Review | Level II
Attachment patterns in autism respond to structured caregiver skill interventions when sensory and anxiety dimensions are addressed simultaneously.
[5] Padmanabha et al. (2019) — Indian Journal of Pediatrics | Level II
Indian RCT demonstrating home-based structured sensory + attachment interventions show significant outcomes in Indian paediatric autism population. DOI: 10.1007/s12098-018-2747-4
[6] NCAEP Evidence-Based Practices Report (2020)
Video modelling, visual supports, and graduated exposure classified as evidence-based practices for autism across peer-reviewed implementation literature.
WHO Nurturing Care
nurturing-care.org
UNICEF ECD
unicef.org/early-childhood-development
SPD Foundation
spdfoundation.net
NCAEP Report
ncaep.fpg.unc.edu

How GPT-OS® Uses Your Data
"Transparency. Here is exactly what happens with your session data."
What GPT-OS® Learns from C-331
- Average weeks to tolerance milestone across child profiles
- Which materials produce fastest trust-building by sensory profile
- Non-preferred caregiver variables that predict successful outcome
- Correlation between preferred caregiver burnout severity and intervention timeline
"The 21 million sessions in our data lake are what make TherapeuticAI® recommendations increasingly precise. Your family's data — your child's journey — is part of what makes the next family's path shorter and clearer."
🔒 Privacy Assurance
- ISO/IEC 27001 Information Security Standard
- Data never sold. Never shared without explicit consent.
- DPIIT DIPP8651 | CIN U74999TG2016PTC113063
- Governed under Indian IT Act and SPDI Rules
Watch the Reel
C-331 Reel
Family Support Solutions | Episode 331 of 999
75–85 seconds
This reel introduces all 9 materials covered on this page — in 75 seconds. Watch a Pinnacle therapist walk through each material with real visual demonstration. Share this reel with every caregiver in your child's life.
▶ Watch the C-331 Reel → techniques.pinnacleblooms.org/social-family/caregiver-preference-C-331#video
Presented by the Pinnacle Blooms Consortium Clinical Team — OT, ABA, SLP, NeuroDev specialists collaborating under GPT-OS®.
"Video modelling is classified as an evidence-based practice for autism (NCAEP, 2020). Watching this reel before implementing the materials improves execution accuracy and parent confidence."
Related Reels from the 999 Reels Master
C-329
Sibling Relationships
C-330
Building Social Confidence
C-332
Respite & Family Support
B-015
Separation Anxiety
Share This With Your Family
"Consistency across caregivers multiplies impact. If only one adult knows this — the effect is limited. Share it."
Research shows that home-based interventions implemented consistently across ALL caregivers produce 3× the outcome of single-caregiver implementation. Share this. It is the most impactful action you can take today. — PMC9978394
📄 Downloadable Family Guide (PDF)
"Expanding the Circle of Trust" — 1-page summary of all 9 materials, suitable for grandparents, school staff, babysitters. Simplified language, no clinical jargon, printable.
📋 "Explain to Grandparents" Version
"Your grandchild has difficulty accepting care from different people. This is a neurological pattern, not a behaviour choice. The 3 things that help most: [1] Use the caregiver schedule on the wall. [2] Follow the routine cards exactly. [3] Use the special activity box. That's it — just these three things, consistently."
📝 Teacher / School Communication Template
"[Child name] is currently working on caregiver flexibility using a structured programme. Consistency in school routines is important. Routine documentation is available. Please use [describe routine supports] and inform us of any transitions. Contact: [parent contact]."
📱 WhatsApp-Format Summary
"9 materials that help when your child only wants one parent: ① Caregiver schedule ② Routine cards ③ Gradual trust steps ④ Connection objects ⑤ Special activity boxes ⑥ Caregiver training ⑦ Goodbye ritual ⑧ Care team book ⑨ Success tracker. Full guide: techniques.pinnacleblooms.org/social-family/caregiver-preference-C-331"
Preview of 9 materials that help with caregiver preference Therapy Material
Below is a visual preview of 9 materials that help with caregiver preference therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
Frequently Asked Questions
"Every question you're likely to have — answered by the consortium."
How long will this take? When will I see results?
First signs of tolerance typically emerge in Weeks 1–2. First genuine engagement in Weeks 3–4. Consistent routine acceptance in Weeks 6–8. Some children progress faster; some slower. The key variable is consistency, not speed. See Cards 23–25 for week-by-week detail.
My child is non-verbal. Do these materials still work?
Yes — and in some cases they work better. Connection objects (Material 4), visual schedules (Material 1), and the goodbye ritual (Material 7) are all non-verbal tools. The special activity box (Material 5) works regardless of verbal ability. Modify the caregiver training material to use visual and gestural cues.
What if the non-preferred caregiver lives far away?
Start with Materials 4 and 8 (connection objects and care team books) to build the relationship at distance. Use video calls as a graduated exposure tool — familiar face on screen before in-person visits. When visits occur, use the exposure ladder (Material 3) starting at Step 1 each visit.
Is this the same as normal toddler attachment? My child is 7.
Typical caregiver preference peaks at 18 months and resolves by age 3–4. If significant preference persists past age 5 and is impacting family functioning, it warrants targeted intervention. Age 7 is absolutely addressable — the nervous system retains plasticity throughout childhood.
Could my child's preference indicate genuine trauma or abuse?
This is an important question to rule out. If preference is accompanied by fear-based responses (terror, not just distress), unexplained physical symptoms, or is specific to one adult rather than broad, please seek clinical assessment immediately. The materials on this page are for preference driven by autism-related sensory/predictability needs — not for trauma responses. If in doubt: call 9100 181 181.
Can I do this without a therapist?
The materials on this page are designed for home implementation. However, for moderate-to-severe caregiver preference (child cannot tolerate non-preferred caregiver in same room), professional guidance significantly improves outcomes and timeline. We recommend at least a teleconsult assessment before beginning.
What about the preferred caregiver's feelings? They're exhausted and scared to let go.
Absolutely valid. The preferred caregiver typically carries both exhaustion (from being the sole caregiver) and anxiety (about stepping back). The preferred caregiver's wellbeing is not secondary — it is central to this intervention. See Card 21 (troubleshooting) and our Family Support programme. → C-332: Respite and Family Support.
Didn't find your answer? Ask GPT-OS® → | 📞 Book a teleconsultation: 9100 181 181 | 📧care@pinnacleblooms.org