"My child will do anything to avoid going. Crossing their legs. Clenching. Hiding behind the sofa. Days go by. Then the pain comes."
If you've counted the days — 3, 4, 5 — watching your child hold what their body desperately needs to release, searching their face for the pain they're hiding, feeling helpless in a battle that makes no sense… this page was written for you.
Bowel Movement Withholding Intervention
9 Evidence-Based Materials
Home-Executable
GPT-OS® Designed
"You are not failing. Your child is not defiant. Their body is caught in a fear cycle — and that cycle can be broken." — Pinnacle Blooms Consortium | Pediatric OT + Behavioral Pediatrics + ABA
Pediatric OT
ABA/BCBA
Developmental Pediatrics
NeuroDev
GPT-OS® Validated
WHO Nurturing Care Framework (2018): Early identification of functional challenges and parental awareness directly determines intervention outcomes. nurturing-care.org
🆓 FREE National Helpline | 9100 181 181 | 16+ Languages | 24×7 | pinnacleblooms.org

You Are Among Millions of Families Navigating This Exact Cycle
Bowel movement withholding is among the most common — and most distressing — self-care challenges in childhood. In children with neurodevelopmental differences, including autism, ADHD, and sensory processing differences, the prevalence is significantly higher. It is not a parenting failure. It is a fear-driven physiological cycle that requires targeted, simultaneous physical and psychological intervention.
1/3
Children Affected
Experience functional constipation or withholding at some point in childhood
5
Average Duration
Average withholding duration reported by parents in clinical surveys before seeking help
84%
Autism + GI
Of children with autism experience GI-related challenges including constipation and withholding, per systematic review (2024)
India-Specific Note: Constipation affects an estimated 10–20% of the Indian paediatric population. Among children attending Pinnacle Blooms centres, toileting challenges including withholding represent one of the top 5 presenting self-care concerns across all age groups 2–10.
NASPGHAN Clinical Guidelines on Functional Constipation | Rajindrajith S, et al., Pediatric Gastroenterology Systematic Review | PMC11506176 (2024 PRISMA Review — GI prevalence in ASD)
📞 Helpline: 9100 181 181

This Is Not Stubbornness. It's a Fear Cycle That Rewires How the Body Functions.
The physiological and psychological mechanisms behind withholding are deeply intertwined — wiring meets fear in a self-reinforcing loop. Understanding this cycle is the first step to breaking it.
The cycle above shows exactly how a single painful experience can trigger months — or years — of withholding. Both entry points must be addressed simultaneously: keep stool soft so passage is never painful, and reduce fear so the body stops interpreting "going" as danger.
1
The Fear Entry Point
A single painful bowel movement teaches the nervous system that "going" means pain. The amygdala flags the urge to defecate as a threat signal.
2
The Body's Response
The pelvic floor muscles clench, the anal sphincter tightens, and the child assumes characteristic postures: crossing legs, rising on tiptoes, hiding. These are active prevention, not attempts to go.
3
The Physical Cascade
Retained stool accumulates. Water is reabsorbed over days, making it larger, harder, and more painful. The rectal wall stretches, reducing sensation. When the hold fails, the passage is agonising.
4
The Breaking Strategy
Both entry points must be attacked simultaneously: keep stool soft (so passage is never painful) AND reduce fear (so the body stops interpreting "going" as danger).
Science Note: The puborectalis muscle creates a natural kink in the rectum when sitting at 90°. Raising the knees above the hips (squatting position) straightens this angle — this is anatomy, not behaviour.
Loening-Baucke V, Pediatrics (2004) | Frontiers in Integrative Neuroscience (2020): DOI 10.3389/fnint.2020.556660 | NASPGHAN Guidelines 2006/2014
Your Child Is Here. Here Is Where We're Heading.
Bowel movement withholding most commonly emerges between ages 2–6, often triggered by a single painful event, toilet training pressure, or a sensory sensitivity. Without intervention, the cycle can persist through age 10 and beyond, leading to chronic constipation, encopresis (overflow incontinence), and significant psychological distress.
Age 18m
Nappy use
Age 2
Potty intro begins
Age 3
Daytime control emerges
Age 4–5
Full toileting expected
Age 6–8
School toileting confident
Age 10+
Mastery and independence
⚠️Withholding most commonly peaks between ages 2–6. This is also the highest-leverage window for intervention. The protocol on this page is your tool.
Autism (ASD)
Sensory Processing Differences
Anxiety Disorders
ADHD
Post-training Regression
A message to you: Your child is not "behind." They are at a waypoint where targeted intervention produces the most rapid change. The window is open. The materials on this page are your tools.
WHO CCD Package (2023) | UNICEF MICS developmental indicators | PMC9978394 | Hyman PE et al., J Pediatr Gastroenterol Nutr (2006)
Not Anecdotal. Not Internet Advice. Evidence-Based, Clinically Validated, and Home-Applicable.
🛡️ LEVEL I–II EVIDENCE
Systematic Reviews + RCTs + Clinical Consensus Guidelines
Every material and step in this protocol is grounded in peer-reviewed research from leading paediatric gastroenterology, occupational therapy, and behavioural science bodies. Here is the evidence behind what you are about to begin.
Study | Finding | Source | |
NASPGHAN/ESPGHAN Joint Guidelines | Combined behavioural + dietary intervention is first-line treatment for functional constipation with withholding | JPGN 2014 | |
Systematic Review (2024) | 84% of ASD children experience GI issues; behavioural + medical integration produces best outcomes | PMC11506176 | |
Cochrane Review (2011) | Behavioural interventions for fecal withholding show significant improvement vs. laxatives alone | Cochrane Library | |
Indian J Pediatr (2019) | Home-based behavioural interventions with parental training show significant outcomes in Indian paediatric population | DOI:10.1007/s12098-018-2747-4 | |
WHO NCF (2018) | Caregiver-delivered interventions in home environments are the highest-leverage point for child development outcomes | nurturing-care.org |
✅Clinically validated. Home-applicable. Parent-proven. Consortium-reviewed.
PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | DOI:10.1007/s12098-018-2747-4 | NASPGHAN 2014
PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | DOI:10.1007/s12098-018-2747-4 | NASPGHAN 2014
📞 Speak to a specialist free of charge: 9100 181 181
The Technique: Bowel Movement Withholding Intervention
Parent-friendly alias: "Breaking the Fear Cycle — The 9-Material Protocol"
A multi-component, home-executable therapeutic approach that simultaneously addresses the physiological and psychological drivers of stool withholding in children aged 2–10. It uses 9 evidence-selected materials across physical positioning, dietary management, cognitive understanding, relaxation, behavioural routine, engagement, reinforcement, graduated exposure, and progress tracking — deployed as a coordinated system, not isolated tools.
Specification Badges
- Age Range: 2–10 years
- Session Duration: 5–15 minutes per sitting (3× daily preferred)
- Frequency: Daily, after meals
- Setting: Home bathroom
- Lead Discipline: Paediatric OT + ABA/BCBA
- Medical Integration: Required (paediatrician/GI for stool softener protocol)
Domain Badges
Self-Care & Daily Living
Toileting Independence
Paediatric OT
Behavioural Pediatrics
Gastroenterology-Integrated
Canon Material Badges
Toileting Visual Supports
Reinforcement Menus
Behaviour Support Materials
📱Companion reel: E-499 — 9 Materials That Help With Bowel Movement Withholding | Series: Self-Care & Daily Living Skills | Episode 499

This Technique Crosses Therapy Boundaries — Because Fear and the Bowel Don't Organise by Therapy Type
Five disciplines work together on the Pinnacle withholding protocol. Each brings a distinct lens. Together they address every dimension of the cycle.
🟣 Paediatric OT (Primary Lead)
Addresses positioning, sensory aspects of toileting, pelvic floor awareness, bathroom environment setup, and equipment selection. OTs design the physical protocol — stool height, seating adaptation, bathroom sensory modification.
🔵 ABA / BCBA (Co-Lead)
Designs the behavioural reinforcement architecture: scheduled sitting, token economies, gradual exposure hierarchy, consequence management. The ABA layer is what makes the behavioural cycle shift.
🟢 Developmental Paediatrics / NeuroDev
Coordinates with gastroenterology for stool softener protocols. Monitors medical progress. Rules out organic causes (Hirschsprung, hypothyroidism). Integrates medical and behavioural management.
🟡 SLP (Supporting)
Creates visual social stories explaining the bowel movement process in child-friendly, non-scary language. Supports comprehension of body functions for children with communication differences.
⚪ Special Education (Supporting)
Integrates toileting goals into the child's IEP/educational plan. Ensures school consistency mirrors home protocol. Trains school staff on the exposure hierarchy and reinforcement system.
At Pinnacle Blooms Network®, all 5 disciplines review and align on each child's withholding protocol through the FusionModule™ — ensuring no single intervention creates contradictory signals across settings.
📞9100 181 181
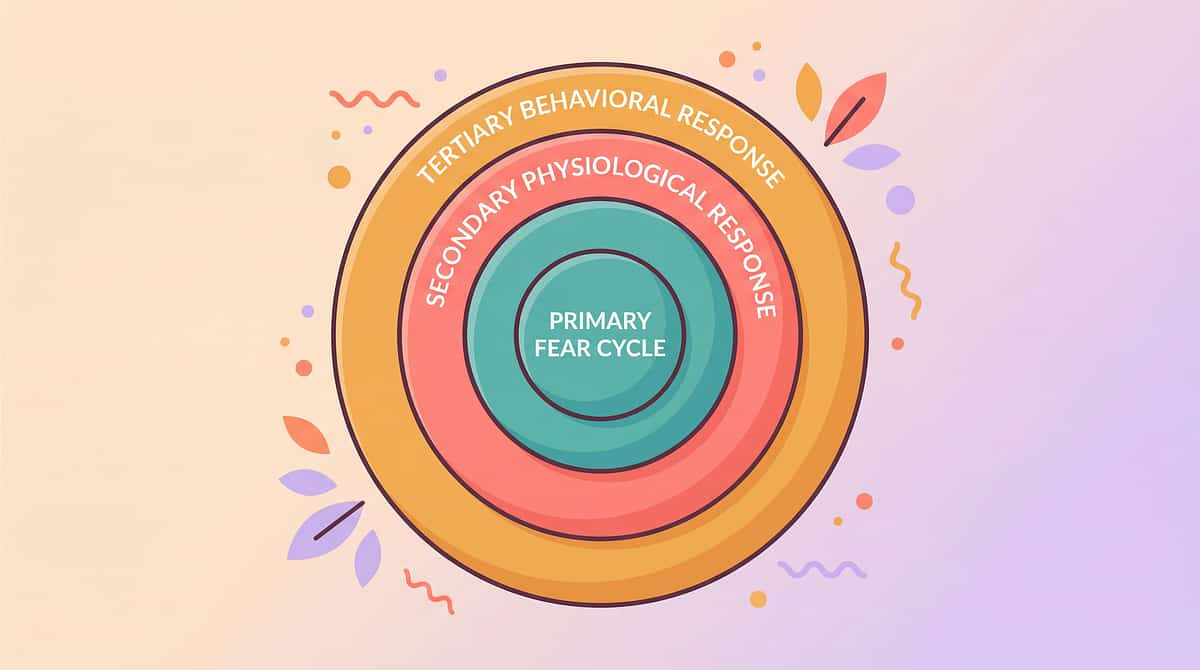
Three Rings of Impact. One Intervention System.
The E-499 protocol targets three concentric rings of impact, ensuring we address more than just the surface behaviour.
Ring 1 — INNERMOST: The Fear-Pain Cycle
The physiological core: a single painful bowel movement creates a fear memory. The child withholds to avoid pain, which causes harder stools and leads to more pain, deepening the cycle.
Protocol targets: Stool softening (dietary + osmotic), parasympathetic activation (breathing, warmth), and correct positioning (squatting angle via footstool) to physically interrupt the pain loop.
Ring 2 — MIDDLE: The Behavioural Avoidance Pattern
The psychological layer: avoidance becomes a learned behaviour. The child develops escape strategies—hiding, clenching, distraction—which are reinforced every time withholding "works" to delay the event.
Protocol targets: ABA-designed exposure hierarchy, scheduled sitting (not demand-based), token economy reinforcement, and an engagement kit to replace avoidance with approach behaviour.
Ring 3 — OUTER: The Environmental & Sensory Triggers
The contextual layer: bathroom lighting, toilet height, sound, smell, and caregiver tone all act as conditioned triggers that activate the fear response before the child even sits down.
Protocol targets: Sensory environment modification, caregiver script training, visual social stories, and consistent routine anchoring across home and school settings.
Every material in the 9-material toolkit maps to at least one ring. Most map to two. The footstool, for example, targets Ring 1 (positioning) and Ring 3 (sensory comfort). This is precision intervention — not a collection of activities.

9 Materials. Two Jobs: Soften the Body's Fear, Soften the Stool.
Some you may already own. Some cost ₹0 to make. All are evidence-selected. Here is your complete toolkit at a glance.
🚽 Squatty Potty / Toilet Stool
Canon: Toileting Visual Supports | Positioning Equipment
Cost: ₹500–2,000 | Search on Amazon.in →
Straightens the anorectal angle for easier, less painful passage
Cost: ₹500–2,000 | Search on Amazon.in →
Straightens the anorectal angle for easier, less painful passage
💊 Fibre Supplement System
Canon: Dietary Supplements (Medical)
Cost: ₹200–800/month | Paediatrician guidance required | Search on Amazon.in →
Keeps stool consistently soft — removes painful reinforcement from the fear cycle
Cost: ₹200–800/month | Paediatrician guidance required | Search on Amazon.in →
Keeps stool consistently soft — removes painful reinforcement from the fear cycle
📖 Visual Social Story for Bowel Movements
Canon: Toileting Visual Supports | Social Stories
Cost: ₹200–800 | DIY available | Search on Amazon.in →
Replaces fear of the unknown with body understanding
Cost: ₹200–800 | DIY available | Search on Amazon.in →
Replaces fear of the unknown with body understanding
🌬️ Relaxation & Deep Breathing Tools
Canon: Sensory Regulation Tools
Cost: ₹100–500 | Search on Amazon.in →
Activates parasympathetic nervous system — physiologically enables pelvic floor release
Cost: ₹100–500 | Search on Amazon.in →
Activates parasympathetic nervous system — physiologically enables pelvic floor release
⌚ Potty Watch / Scheduled Timer
Canon: Visual Timers / Schedules
Cost: ₹800–2,500 | Search on Amazon.in →
Interrupts avoidance patterns — provides non-confrontational prompting
Cost: ₹800–2,500 | Search on Amazon.in →
Interrupts avoidance patterns — provides non-confrontational prompting
📦 Toilet-Time Engagement Kit
Canon: Engagement / Distraction Materials
Cost: ₹300–2,000 | DIY available | Search on Amazon.in →
Redirects attention from fear — allows body to relax while mind is occupied
Cost: ₹300–2,000 | DIY available | Search on Amazon.in →
Redirects attention from fear — allows body to relax while mind is occupied
⭐ Reward & Reinforcement System
Canon: Reinforcement Menus ✅[Active Canon Product Available]
Cost: ₹200–1,000 | The Rosette Imprint Reward Jar ₹589 → | 1800+ Reward Stickers ₹364 →
Makes trying more rewarding than withholding — shifts behavioural contingency
Cost: ₹200–1,000 | The Rosette Imprint Reward Jar ₹589 → | 1800+ Reward Stickers ₹364 →
Makes trying more rewarding than withholding — shifts behavioural contingency
🪜 Gradual Exposure Hierarchy Chart
Canon: Visual Schedules / Progress Charts
Cost: ₹200–600 | DIY available | Search on Amazon.in →
Breaks the impossible into achievable — each step reduces anxiety before the next
Cost: ₹200–600 | DIY available | Search on Amazon.in →
Breaks the impossible into achievable — each step reduces anxiety before the next
📊 Bowel Movement Tracking Chart
Canon: Data Tracking / Progress Monitoring
Cost: ₹100–400 | DIY available | Search on Amazon.in →
Transforms invisible struggle into visible progress — essential for medical management
Cost: ₹100–400 | DIY available | Search on Amazon.in →
Transforms invisible struggle into visible progress — essential for medical management
💰Total Investment Range: ₹2,600–10,100 for complete system (plus ongoing fibre supplements) | ✅ Consortium Clinically Reviewed

You Don't Need to Wait for Amazon Delivery. Start Today With What You Have.
Every principle in this protocol can be executed with household materials. The clinical principle — correct positioning, soft stool, body understanding, parasympathetic activation, routine prompting, fear distraction, behavioural contingency, graduated exposure, and data visibility — produces the outcome. The principle, not the product.
Material | Buy This | Make This Today (₹0) | |
Toilet Stool | Squatty Potty ₹500–2,000 | Sturdy wooden box, stacked thick books, or inverted basin — knees must be above hips | |
Fibre System | Isabgol/psyllium husk ₹200/month | Increase fruits (papaya, prune), vegetables, whole grains — same fibre, slower dose | |
Social Story | Published potty book ₹200–800 | Draw 6 pictures with your child: food → tummy → poop feeling → toilet → sit → better! Laminate with tape | |
Breathing Tools | Pinwheel/bubble wand ₹100–500 | Blow tissue paper taped to a string, blow a feather, blow warm breath on mirror to make fog | |
Potty Timer | Potty watch ₹800–2,500 | Phone alarm set for 20 mins after each meal — labelled "Toilet Sitting Time" | |
Engagement Kit | Special toys/tablet ₹300–2,000 | One special toy or book that ONLY comes out during toilet sitting — immediately returned after | |
Reward System | Token jar/stickers ₹200–1,000 | Dried beans in a jar = tokens. 5 beans = a hug from a favourite person. Free. Powerful. | |
Exposure Chart | Printed poster ₹200–600 | Draw a ladder on A4 paper, 10 rungs, write each step, move a star sticker up each day | |
Tracking Chart | Printed chart ₹100–400 | Calendar on wall, sticker for each toilet sitting attempt, circle for successful BM |
⚠️ One non-negotiable: The fibre supplement and stool softener protocol requires medical supervision. A paediatrician or paediatric GI specialist must determine the appropriate agent, dose, and duration. This is the one component that cannot be safely improvised without professional guidance.
WHO Nurturing Care Framework (2018): Context-specific, equity-focused interventions. CCD Package across 54 LMICs: household-material-based intervention efficacy confirmed. PMC9978394
📞9100 181 181

🛑 Read This Before Beginning. Your Child's Safety Is the First Protocol.
1
🔴 RED: DO NOT PROCEED — Seek Medical Evaluation First
- Child has never passed stool without enema/suppository
- Withholding present from birth or first months of life (possible Hirschsprung disease)
- Abdominal distension (visibly bloated belly)
- Vomiting associated with withholding
- Failure to thrive or weight loss
- Blood in stool beyond minor anal fissure
- Withholding completely unresponsive to dietary intervention for 4+ weeks
- Suspected faecal impaction (palpable hard mass in abdomen)
RED LINE BEHAVIOURS during session — STOP IMMEDIATELY: Child shows signs of severe pain, vomiting, or complete distress beyond normal anxiety. Different from fear — this is physical distress.
2
🟡 AMBER: PROCEED WITH CAUTION — Modify Approach
- Child is currently in a withholding episode (actively holding) — do not attempt forced toilet sitting; use relaxation tools only
- Child is ill, feverish, or recently had a traumatic experience — postpone protocol for 24–48 hours
- Child has overflow soiling/encopresis — medical disimpaction may be required before behavioural intervention
- Child is extremely resistant — begin with exposure hierarchy Step 1 only, not full toilet sitting
3
🟢 GREEN: PROCEED — Standard Safety Guidelines
- Toilet stool must be stable, non-slip, and weight-appropriate
- Reduced toilet seat required for small children (prevent feeling of falling in)
- Fibre supplements: paediatrician-guided dose only — too much fibre without water worsens constipation
- Bubble solution: non-toxic only
- Never use force, anger, or punishment during toilet time — this increases fear and extends the cycle
Environmental Safety Checklist
Bathroom floor non-slip / mat in place
Toilet stool stable and non-tipping
Toilet reducer seat fitted (if needed for small child)
Temperature comfortable (cold bathrooms increase anxiety)
Lighting calm (not harsh/fluorescent if child is light-sensitive)
Indian Journal of Pediatrics (2019): Home-based behavioural intervention safety protocols DOI:10.1007/s12098-018-2747-4 | NASPGHAN 2014: Medical red flags for organic constipation | AAP: When to refer to paediatric GI
📞 Medical concerns? Call free: 9100 181 181
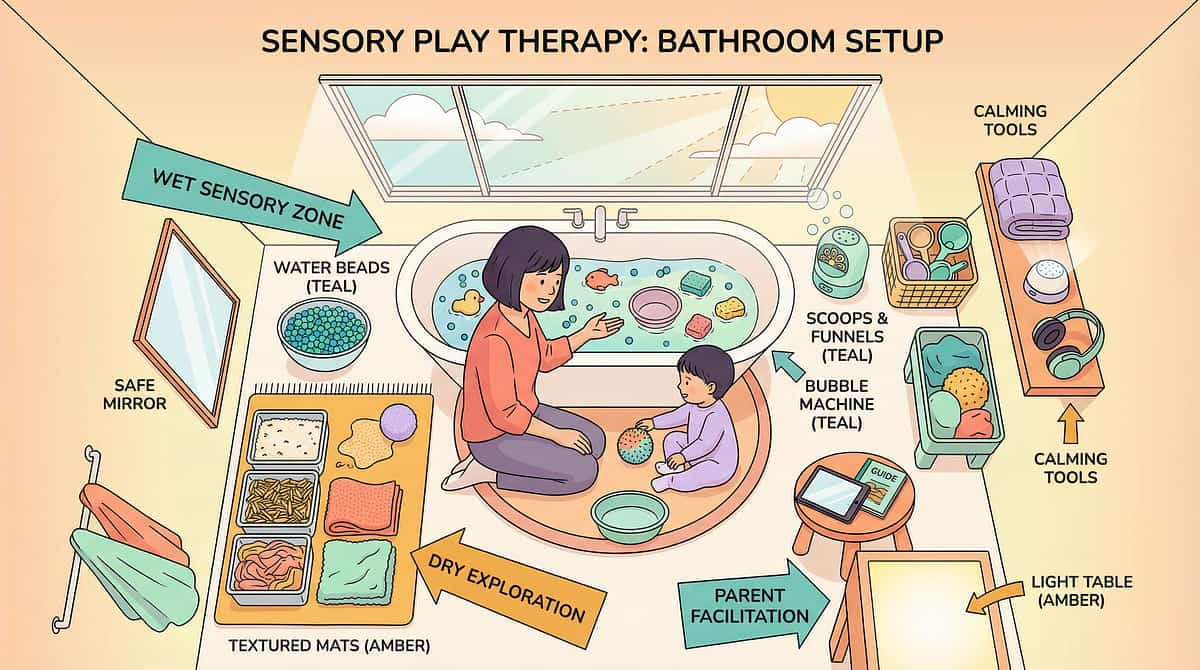
Before Your Child Sits Down — the Environment Must Be Ready
A child in a fear state is hyper-attuned to their environment. The wrong lighting, a cold seat, or a rushed caregiver can activate the threat response before the session even begins. Set the stage once. Set it right. Spatial and sensory preparation prevents 80% of session failures; the environment must be set BEFORE the child enters — not adjusted mid-session.
1. The Footstool — Position
Height: child's feet must rest flat, knees at or above hip level (approx. 90–110° hip angle). Material: non-slip surface, stable under weight. Correct squatting angle relaxes the puborectalis muscle, reducing physical effort by up to 30%. DIY: a stack of firm books wrapped in a non-slip mat works identically.
2. The Seat — Temperature & Comfort
Cold toilet seats trigger a startle/withdrawal reflex in sensory-sensitive children. Solution: warm the seat with a warm (not hot) damp cloth 60 seconds before the session, or use a padded toilet seat insert. The insert also reduces the "falling in" fear common in children aged 2–6.
3. The Lighting — Sensory Regulation
Bright overhead fluorescent lighting activates the sympathetic nervous system. Use a warm-toned nightlight or dim the main light to 40–60% brightness. Consistent lighting across sessions becomes a parasympathetic anchor — the body learns "this light = safe time."
4. The Sound — Auditory Environment
Running a white noise machine or soft instrumental music at 50–60 dB masks toilet sounds that can startle or embarrass the child. Avoid silence, as it amplifies body awareness and anxiety. Recommended: nature sounds, soft rain, or the child's preferred calming music.
5. The Engagement Kit — Pre-Positioned
The engagement kit must be visible but not yet accessible when the child enters. Visibility creates anticipation and approach motivation — the child walks toward something, not away from something. Never reveal the kit before the child is seated.
6. The Caregiver — Tone & Posture
The most powerful environmental variable is you. Regulated caregiver = regulated child. If you are tense, rushed, or visibly anxious, the child's nervous system mirrors it within 8 seconds. Script for entry: "Hey, it's [child's name]'s special box time. Let's go check what's in there today." — neutral, curious, no mention of toileting.
⏱️Total setup time: under 3 minutes. Do it before you call your child. Never adjust the environment while they are watching — it signals unpredictability.
60-Second Check Before Every Session. Non-Negotiable.
The best session is one that starts right. Run through this pre-flight checklist every time — it takes under a minute and prevents the most common session failures.
Check | ✅ Go | ⚠️ Modify | 🛑 Postpone | |
Fed within the last 30 min? (gastrocolic reflex active) | Yes | Partially | No | |
Calm baseline state? (not mid-meltdown) | Regulated | Slightly elevated | Dysregulated | |
No fever or physical illness? | Well | Mild | Sick | |
No recent traumatic event in last 2 hours? | Settled | Recovering | Recent trauma | |
Currently holding (active withholding postures)? | Not posturing | Mild posturing | Active clenching | |
Has at least 1 preferred item for engagement kit? | Yes | Alternate available | Nothing preferred | |
Parent calm and not rushed? | Calm | Slight pressure | Stressed/rushing |
🟢 3+ Green = GO
Proceed to Step 1 — The Invitation. Full protocol.
🟡 2+ Amber = MODIFY
Use relaxation tools only. No sitting expectation. Just calm time in bathroom. 3 minutes maximum.
🔴 1+ Red = POSTPONE
Alternative calming activity away from bathroom. Try in 2–3 hours or at next meal time. Never force. Forcing increases the fear cycle.
Key Principle: Missed sessions don't fail the protocol. Forced sessions do.
ABA Principles: Antecedent manipulation determines intervention effectiveness. Setting events are core to session readiness protocols.

STEP 1 OF 6
The Invitation
Every protocol begins with an invitation, not a command. ABA pairing principle meets OT's just-right challenge. Your tone at this moment sets the emotional trajectory for the entire session.
"Hey [Child's Name] — it's toilet sitting time! Let's go check your special [Engagement Kit Box Name]. I wonder what we'll play with today…"
What You're Doing
You are using the engagement kit as the positive cue — the toilet is associated with the exciting box, not with performance pressure. The child is being invited to the activity, not commanded to produce a result.
Parent Body Language
- Casual, light tone — like announcing a snack, not a task
- Move toward bathroom naturally, box in hand
- Don't look back repeatedly to check if they're following
- Light touch on shoulder only if child accepts touch
Acceptance Cues (Green)
Child follows, looks at box, asks about box, says "okay," or moves toward bathroom — ANY of these is acceptance.
Resistance Cues and Response
- Mild resistance: "We'll just check the box for two minutes, then you're done" — lower the demand
- Active resistance: Skip to modified version (Readiness Check Modify path)
- Bolting/shutting down: End completely. Not today. Note in tracking chart.
Timing
30–60 seconds
ABA Pairing Procedures: Establishing motivating operations before demand placement. OT "Just-Right Challenge" principle: matching task demand to current capacity.
📞9100 181 181

STEP 2 OF 6
The Engagement
Child is now seated. Engagement kit revealed. Anxiety redirected. The session deepens. This phase is about building the association: toilet time = exciting box time. Nothing more.
"Okay, let's blow some bubbles / look at this book / spin this toy… [Whatever child chose]" — No mention of bowel movement. No asking "are you going?" No watching, waiting, or subtle pressure.
The Breathing Pivot (30 seconds after seated)
Casually introduce the breathing tool: "Want to try spinning the pinwheel? Watch — slow breath out, like this…" Demonstrate slow exhale. Child attempts. No pressure. Simply normalised as part of toilet time.
Child Response | Meaning | Action | |
Engages with activity and breathing | Ideal | Maintain, don't interrupt | |
Tolerates sitting, minimal engagement | Acceptable | Gentle continuation, no demands | |
Restless but seated | Watch | Allow movement, keep session brief | |
Wants to leave immediately | Resistance signal | Offer 2-minute countdown, honour it |
After 2 minutes of calm sitting — praise immediately: "You're doing so well sitting! I'm proud of you." (Praise sitting, not producing.)
Timing: 1–3 minutes of this phase
PMC11506176: Structured material introduction in OT meets evidence-based practice criteria. ABA reinforcement scheduling: immediate, specific praise within 3 seconds.

STEP 3 OF 6
The Therapeutic Action: This Is Where the Cycle Actually Breaks
The core therapeutic event. This is where the 9 materials converge into a single session experience. Let the body do what it knows.
1
Physical Foundation (always present)
Child seated on toilet. Knees above hips via toilet stool. Feet flat on stool. Slight forward lean — elbows on knees. This position creates the squatting angle that allows the puborectalis muscle to relax, straightening the anorectal angle. You don't need to explain this to the child. Just ensure the position.
2
The Breathing Layer (active throughout)
Every 60–90 seconds, gently prompt: "Want to blow the pinwheel? Make it spin slowly…" Slow exhalation → diaphragm drops → abdominal pressure increases slightly → pelvic floor relaxes → the body is positioned to let go. Slow breath = parasympathetic activation = relaxation of sphincters.
3
The Engagement Layer (continuous)
Child engaged with activity from kit. Mind occupied. Body in correct position. Breathing periodically prompted. The child is NOT focused on whether a bowel movement will happen. This is precisely the goal — a distracted body is a relaxed body.
4
The Social Story Layer (2–3 times per week)
At a calm moment: "Can I read you a quick story about how our tummies work?" Read 2–3 pages of the bowel movement social story. Keep it light, matter-of-fact, positive. "See — the poop comes out and then your tummy feels so much better!"
Common Execution Errors
❌ Asking "Are you pooping?" every 2 minutes — increases anxiety
❌ Hovering and watching the child intently — increases self-consciousness
❌ Ending the session the moment you think they're done — they may not be done
❌ Reacting with large visible emotion to any output — keep all responses measured and warm
Duration: 5–10 minutes total therapeutic sitting. After meals = gastrocolic reflex window. NASPGHAN: Scheduled sitting after meals exploits gastrocolic reflex.
STEP 4 OF 6
Repeat and Vary
Therapeutic dosage matters as much as technique quality. Frequency, variation, and knowing the satiation point are the three levers of this step.
Target Schedule: 3× daily — after each meal (breakfast, lunch, dinner). Gastrocolic reflex is strongest 20–30 minutes after eating — this is your highest-probability window. Minimum: 1× daily (after the largest meal).
Variation Menu (to prevent boredom and maintain engagement)
Vary the Engagement Kit Item
Rotate through 5–7 items across the week. Same box, different "treasure" each sitting. Keep novelty high.
Vary the Breathing Tool
Monday = pinwheel. Tuesday = bubbles. Wednesday = feather. Thursday = counting breaths. Friday = humming.
Vary the Story Timing
Social story 3× per week, not every session. Keep it a special element.
Vary the Session Duration
Some days 5 minutes. Days when child is particularly calm and engaged — extend naturally. The child extending naturally is a positive signal.
Satiation Indicators (when to end)
- Fidgeting shifts from calm to agitated
- Asks to leave more than twice
- Engages with nothing in the kit
- Breathing exercises are refused
"3 calm, relaxed sessions are worth more than 10 forced, anxious ones."
Consistency principle: Every missed meal-time session is a missed gastrocolic reflex window. The schedule matters more than any individual session outcome.
SI dosage research: 2–3 sessions/week × 8–12 weeks for clinical protocols. Home protocols: daily frequency with shorter sessions.

STEP 5 OF 6
Reinforce and Celebrate: When Fear Makes Withholding Feel Safer — Make Trying Feel MORE Rewarding
1
Phase 1: Reinforce SITTING (Week 1–2)
Every toilet sitting attempt = immediate reinforcement, regardless of outcome. "Wonderful sitting! Here's your token/sticker!" No bowel movement required. Sitting alone is the win.
2
Phase 2: Reinforce SITTING + RELAXING (Week 3–4)
Toilet sitting + demonstrated attempt at breathing/relaxation = reinforcement. "Amazing! You sat AND blew the pinwheel. That's two tokens today!"
3
Phase 3: Reinforce BOWEL MOVEMENT (Week 5+)
When successful BMs begin occurring — add larger, special reinforcement for BM. Maintain Phase 1 reinforcement for sitting (don't remove the floor). "You did it! Big reward coming! AND your regular sitting token too!"
✅ Reinforcement Rules
- Within 3 seconds of desired behaviour
- Specific: "I love how you sat and relaxed" — not just "good job"
- Enthusiastic but not overwhelming
- Consistent — every sitting, every time, in Phase 1
❌ Never Do These
- Never remove earned tokens as punishment
- Never make the goal "BM only" in early phases
Active Canon Products
🛒The Rosette Imprint Reward Jar — ₹589 → — Canon: Reinforcement Menus
🛒1800+ Reward Stickers Book — ₹364 → — Canon: Reinforcement Menus
ABA Reinforcement Principles: Immediate, specific reinforcement increases behaviour. Token economies: strong evidence across multiple systematic reviews for autism. BACB ethical guidelines.
📞9100 181 181

STEP 6 OF 6
The Cool-Down: No Session Ends Abruptly
Transitions prevent post-session dysregulation. A thoughtful cool-down is the final therapeutic act of every session — and it takes only 90 seconds.
"Two more minutes and then we're all done for now. You did AMAZING today."
1
Verbal Warning
"2 more minutes" — stated calmly, without urgency
2
Child Begins Packing Away
Child participates in closure by putting away kit item — this gives them agency and ritual
3
Child Stands and Wipes
If needed. Flush if comfortable — do not force flush if child is flush-fearful
4
Hand Washing
Normalise as part of the ritual — consistent closure cue every session
5
Move Together to Next Positive Activity
Have something pleasant lined up immediately after: snack, preferred activity, outdoor time. The bathroom → reward chain should be frictionless.
If child resists ending (having a good time): A child who wants to STAY on the toilet during toilet time is a therapeutic success. Never abruptly end a session that's going well. If they've been sitting 15+ minutes comfortably, the 2-minute warning is still appropriate — but honour their engagement first.
Visual supports and transition cues: NCAEP Evidence-Based Practices Report (2020): Visual supports classified as evidence-based for autism. Transition warning research: reduces post-session dysregulation.

60 Seconds. 3 Data Points. This Is How Progress Becomes Visible.
Within 60 seconds of session end, capture these 3 data points. This data drives clinical decisions — for you, for your paediatrician, and for the progression arc of the protocol.
The 3-Field Tracker
SESSION DATE: ___________ TIME: ___________
[1] SITTING TOLERANCE
○ Refused to sit ○ Sat 1–3 min ○ Sat 3–5 min ○ Sat 5–10 min ○ Sat 10+ min
○ Refused to sit ○ Sat 1–3 min ○ Sat 3–5 min ○ Sat 5–10 min ○ Sat 10+ min
[2] BOWEL MOVEMENT
○ No BM ○ BM in nappy/pull-up ○ Partial release ○ Full BM on toilet
Stool quality: ○ Hard ○ Formed-soft ○ Soft ○ Loose
○ No BM ○ BM in nappy/pull-up ○ Partial release ○ Full BM on toilet
Stool quality: ○ Hard ○ Formed-soft ○ Soft ○ Loose
[3] ANXIETY LEVEL
○ High (refused, crying, posturing) ○ Moderate (reluctant but sat) ○ Low (cooperative, calm) ○ Relaxed (engaged, self-directed)
○ High (refused, crying, posturing) ○ Moderate (reluctant but sat) ○ Low (cooperative, calm) ○ Relaxed (engaged, self-directed)
NOTES (optional): _______________________
Why This Data Matters
- For YOU: You'll see the pattern you can't see day-to-day. Sitting tolerance almost always improves before BMs improve.
- For your paediatrician: They need BM frequency and quality data to adjust stool softener dosing.
- For the progression: Your data from Week 1 vs. Week 4 will show change that feels invisible in the moment.
Download & Track
📥 Download E-499 Tracking Chart PDF
📱 Track in GPT-OS® App
Data-based decision making: Core to ABA practice and evidence-based OT. Medical management of withholding requires frequency/quality data (NASPGHAN). PMC11506176: Outcome measurement in paediatric behavioural intervention.
📞9100 181 181

The Session Didn't Go as Planned. Here's What to Do.
Every common obstacle has a specific solution. This is not a reason to abandon the protocol — it's an invitation to adapt it.
1
🔴 "My child refuses to sit at all"
Return to the exposure hierarchy. Start at the step BELOW where resistance occurs. Sitting on closed lid. Standing in bathroom. Talking about the toilet. Wherever there's zero resistance — that's your current rung. Daily practice happens there.
2
🟡 "My child sits but is clearly holding the whole time"
This is normal for weeks 1–4. The sitting itself is therapeutic. Focus on breathing tools. Do NOT comment on whether they're holding. Add a particularly engaging item to the kit.
3
🟡 "We had a successful BM last week but nothing this week"
Regression is part of the pattern. The fear cycle has memory. Maintain the protocol exactly. Review fibre supplement compliance. Check if stool has hardened (track in chart).
4
🟡 "My child only poops in the nappy — won't consider toilet"
Completely normal as a starting point. Fibre + toilet stool + engagement kit for sitting in nappy first. The nappy can be loosened over sessions, then opened, then removed. Graduated exposure works even here.
5
🟡 "The reward system stopped working"
Rewards lose power when the item becomes too familiar. Refresh the reward menu monthly. Survey the child: what's motivating NOW? Different at 3 vs. 7 years old.
6
🟡 "I'm too exhausted and frustrated to stay calm"
This is the most common and most serious challenge. Your emotional state directly affects the child's anxiety. On difficult days: abbreviated 3-minute session only. Tag-team with partner. Reach out to a Pinnacle specialist via the helpline.
7
🔵 "It's been 8 weeks and no improvement"
Time for professional evaluation. The cycle may be entrenched enough to require medical disimpaction, psychological intervention (anxiety-focused), or ABA-designed intensive behavioural protocol. Call 9100 181 181.
NASPGHAN: Lack of response to combined behavioural + dietary intervention = escalation criteria. ABA troubleshooting: behavioural function analysis guides modification.

The Protocol Bends to Fit Your Child. Not the Other Way Around.
Use the exposure hierarchy as a personalised ladder — create it with your child, decorate it together, and find the rung where daily practice happens comfortably. Move up only when the current rung is completely comfortable.
1
Rung 1
Talking about poop with stories, looking at books ○
2
Rung 2
Being in the bathroom, sitting on closed lid ○
3
Rung 3
Standing in front of toilet, touching it, playing near it ○
4
Rung 4–5
Sitting on toilet briefly then 5+ min with nappy on ⭐