
When Rocking Is Constant and You Don't Know What It Means
Body rocking often signals a sensory need — the nervous system seeking input it isn't getting elsewhere. You are not failing. Your child's nervous system is speaking.
"My 4-year-old rocks back and forth constantly. When he's watching TV, eating, sitting in his car seat — he rocks. Sometimes it's gentle. Other times it's so intense I worry he'll hurt himself. His teachers have mentioned it. Other parents stare. I don't know if I should stop him, ignore it, or worry about it. I've tried telling him to stop but he doesn't seem able to. What is happening? What actually helps?" — Parent, navigating this every day
🔬 Domain D — Sensory Processing
👶 Ages 2–12
⏱️ 9 Evidence-Based Materials
Sensory & Motor Development in Children — Episode D-364 | Pinnacle Blooms Network® | GPT-OS® Verified
You Are Among Millions of Families Navigating This Exact Challenge
Body rocking is one of the most common sensory-motor behaviors in childhood. The data validates what you're living every day. You are among an estimated 8–12 million families in India alone navigating vestibular seeking and body rocking in their children. You are not alone. This is not rare. This is not your fault.
80%
Sensory Difficulties in Autism
of children with autism experience sensory processing difficulties, including vestibular seeking behaviors
1 in 36
Children on the Spectrum
children in India are now on the autism spectrum — the largest pediatric neurodevelopmental cohort on Earth
70%+
Respond to Intervention
of children who receive structured vestibular intervention show measurable reduction in rocking behaviors
With 70+ Pinnacle centers operating across India and 70+ countries served through GPT-OS®, body rocking represents one of the top 5 presenting concerns among families seeking pediatric OT assessment. Our clinical data spans 20 million exclusive 1:1 therapy sessions.
Sources: PRISMA Systematic Review 2024 (PMC11506176) | Lancet India Data 2023 | Pinnacle GPT-OS® Outcomes, 20M+ sessions

This Is a Wiring Difference. Not a Behavior Problem.
The Vestibular Pathway
Inner Ear → Brainstem → Cerebellum → Sensory Cortex
In children who rock persistently, the vestibular system is under-responsive — it requires more movement input than typical daily life provides. So the child creates that input themselves. By rocking.
This is not defiance. This is neurology.
What Changes When We Intervene Correctly
The Vestibular System is your child's movement-sensing system, housed in the inner ear. It tells the brain: Am I moving? How fast? In which direction? The brainstem's reticular formation — which governs arousal and sensory gating — is receiving insufficient vestibular signals, creating a perpetual "seeking" state.
- The vestibular system receives organized input
- The reticular formation reaches appropriate arousal
- The drive to self-generate input (rocking) decreases
- Attention, regulation, and learning improve as downstream effects
🔄 Vestibular Seeking
The nervous system craves rhythmic movement input
⚖️ Self-Regulation
Rocking modulates arousal — calming when overwhelmed, alerting when bored
🤗 Self-Soothing
Comfort during stress, anxiety, or fatigue
The appropriate intervention depends entirely on which function the rocking serves for YOUR child. | Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660

Your Child Is Here. Here Is Where We're Heading.
WHO/UNICEF developmental milestones place body rocking in clear context — a waypoint in a journey with a forward path.
1
0–12 Months
Rhythmic movement (rocking, bouncing) is developmentally normal — typical vestibular development
2
12–24 Months
Head rolling, body rocking are neurotypical developmental behaviors at this stage
3
24–36 Months
Rocking begins to reduce in typically developing children as vestibular system matures
4
3–4 Years ★ D-364 Zone
Persistent body rocking beyond this age warrants assessment and intervention
5
4+ Years
Intervention target: structured vestibular support using the 9 materials in this technique
Comorbidity awareness: Body rocking frequently co-occurs with Autism Spectrum Disorder (vestibular seeking/stimming), Sensory Processing Disorder (under-responsive vestibular system), ADHD (arousal regulation need), and Anxiety Disorders (self-soothing response). Professional evaluation determines which pathway your child is on.
Sources: PMC9978394 — WHO/UNICEF CCD Package Implementation Research (2023) | WHO/UNICEF MICS developmental monitoring indicators (197 countries)

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: I–II
Systematic Review + Randomized Controlled Trial
Evidence Strength for Vestibular Intervention: ESTABLISHED
16 peer-reviewed studies confirm. 20M+ Pinnacle sessions demonstrate. Your child's transformation is evidence-based, not experimental.
The Research Foundation
PRISMA Systematic Review, 2024
16 articles (2013–2023). Sensory integration intervention classified as evidence-based practice for ASD. Vestibular input through swinging showed strongest effect for reducing seeking behaviors. PMC11506176
Meta-Analysis, 2024
24 studies. SI therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills. Vestibular-based interventions show consistent, measurable outcomes. PMC10955541
India RCT, 2019
Home-based sensory interventions demonstrated significant improvement in Indian pediatric population. Parent-administered protocols showed high fidelity. DOI: 10.1007/s12098-018-2747-4
Vestibular Input Redirection Protocol via Therapeutic Materials
"Meeting the Movement Need" — 9 materials that address the need behind the rocking
Body rocking is a rhythmic, repetitive movement pattern where a child sways their trunk forward and backward — or side to side — in regular tempo. It is almost always functional: it serves a real purpose for the child's nervous system. For most persistent rockers, that purpose is vestibular seeking — the inner ear's movement-processing system craves rhythmic input that isn't being provided through typical daily activities. The 9 materials on this page directly address this need. When the need is met, the rocking often naturally decreases.
What It Is
Organized, controlled vestibular and proprioceptive input — meeting the need the rocking is trying to meet, in safer, more effective, and more socially adaptive ways.
How It's Used
Daily sensory diet with proactive scheduling. Ages 2–12. Use 1–2 materials to start; build to a full sensory diet over 4–8 weeks.
Where It Comes From
Reel ID D-364 | Domain D: Sensory Processing | Pinnacle 128 Canon Materials | Sensory Equipment / Proprioceptive Tools / Regulation Supports
📋 Reel ID: D-364
👶 Ages 2–12
🔁 Daily Sensory Diet
Ep. 364 of 999

This Technique Crosses Therapy Boundaries Because the Brain Doesn't Organize by Therapy Type
🦾 Occupational Therapy
Primary Lead Discipline
OTs design the full sensory diet — scheduling vestibular input through swings, rocking equipment, and movement activities. They assess vestibular processing, determine appropriate input intensity, and train parents in equipment use. OT owns the sensory integration framework.
📊 Applied Behavior Analysis
Behavioral Framework
BCBAs conduct functional behavior analysis to determine what the rocking serves. They design replacement behavior protocols, reinforcement schedules for appropriate equipment use, and monitor behavioral outcomes.
📚 Special Education
Classroom Implementation
SpEd teachers implement sensory diet accommodations in school settings — wobble cushions, movement breaks, fidget tools, weighted lap pads. They coordinate the school component of the sensory diet.
🧠 NeuroDev Pediatrics
Medical Oversight
NeuroDev pediatricians rule out neurological causes, confirm diagnosis (ASD, SPD, Stereotypic Movement Disorder), and oversee the overall intervention plan. They determine when rocking warrants urgent evaluation.
Pinnacle Blooms Network® Consortium — OT • SLP • ABA • SpEd • NeuroDev • CRO — Integrated under GPT-OS® FusionModule™
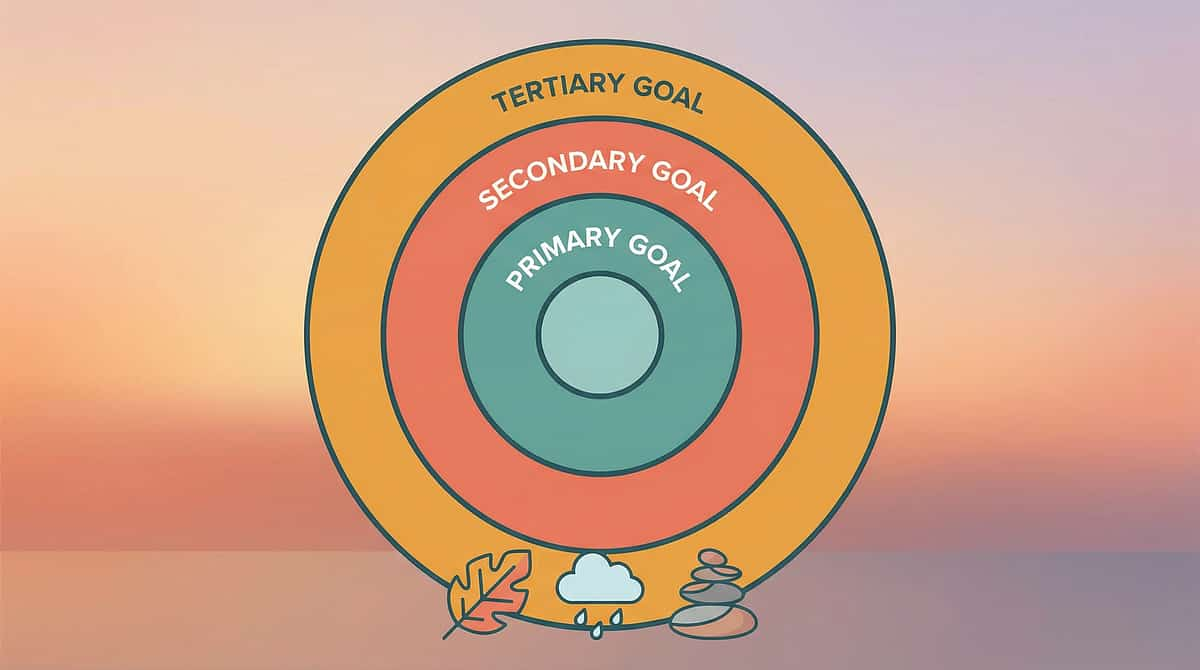
This Isn't a Random Activity. It's a Precision Therapeutic Tool.
Every material in this protocol targets specific, measurable outcomes — from primary vestibular need satisfaction to tertiary gains in classroom readiness and social participation.
Target Level | Specific Target | Observable Indicator | |
PRIMARY | Vestibular need satisfaction | Rocking frequency decreases after equipment use | |
PRIMARY | Body rocking reduction | Shorter duration, lower intensity rocking overall | |
SECONDARY | Self-regulation | Child uses equipment vs. meltdown as regulation strategy | |
SECONDARY | Arousal modulation | Calmer, more focused states following vestibular input | |
SECONDARY | Anxiety reduction | Less rocking in high-anxiety situations with supports | |
TERTIARY | Attention span | Longer sustained engagement after movement input | |
TERTIARY | Social participation | Less rocking during group activities; more presence | |
TERTIARY | Classroom readiness | Teacher reports improved focus; reduced disruptive rocking |

9 Materials That Address the Need Behind the Movement
Mapped to the Pinnacle 128 Canon Materials system. Each material addresses a specific component of vestibular seeking. Use 1–2 to start; build to a full sensory diet.

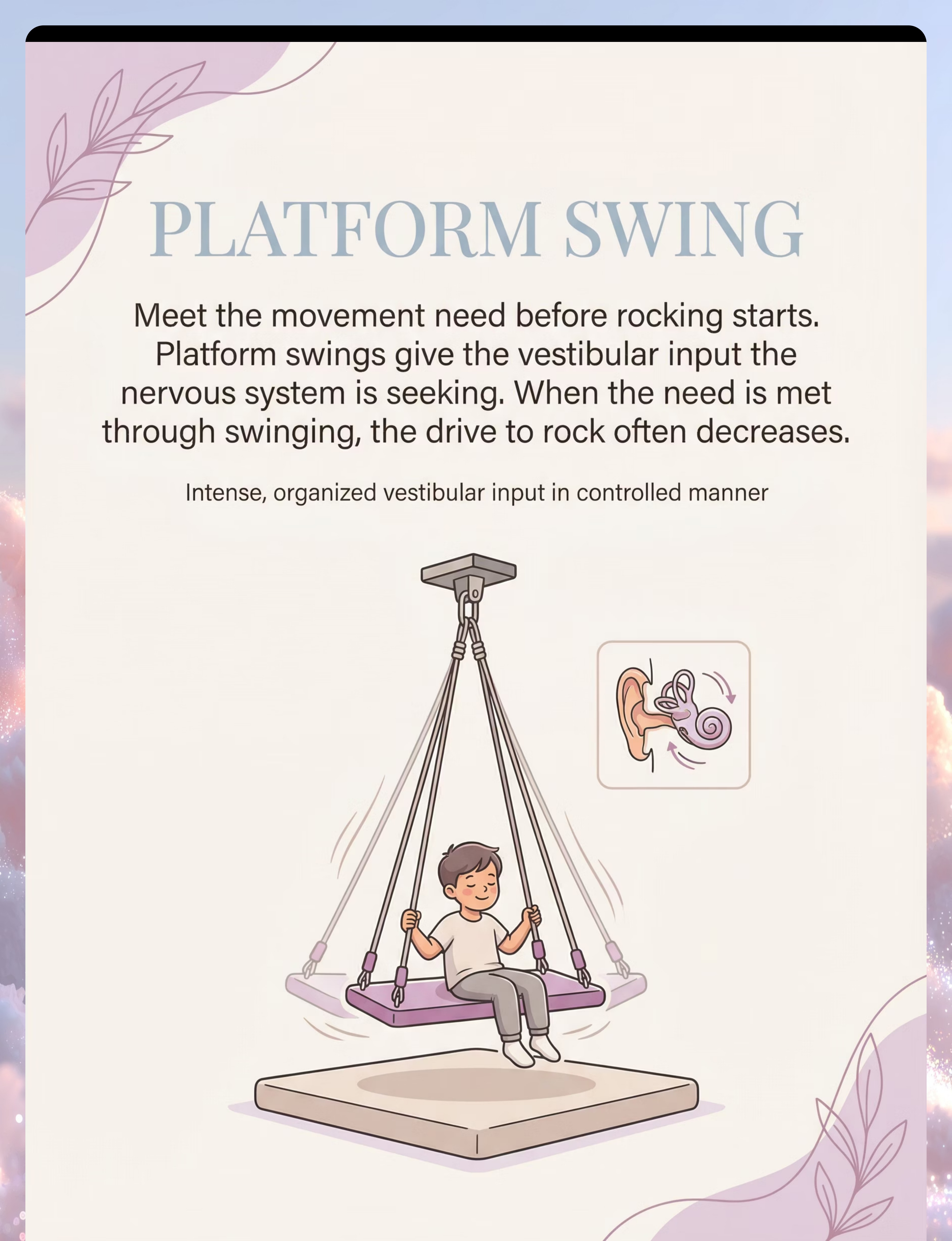
🔄 Material 1 — Platform Swing / Bolster Swing
Canon: Sensory Swings & Vestibular Equipment
The highest-impact vestibular input tool. Provides intense, organized rhythmic movement that directly meets the vestibular need driving rocking. When a child receives sufficient swing input, the drive to self-generate through rocking often decreases significantly. Vestibular type: Linear + rotary | Intensity: ●●●●○ High | Price: ₹3,000–12,000

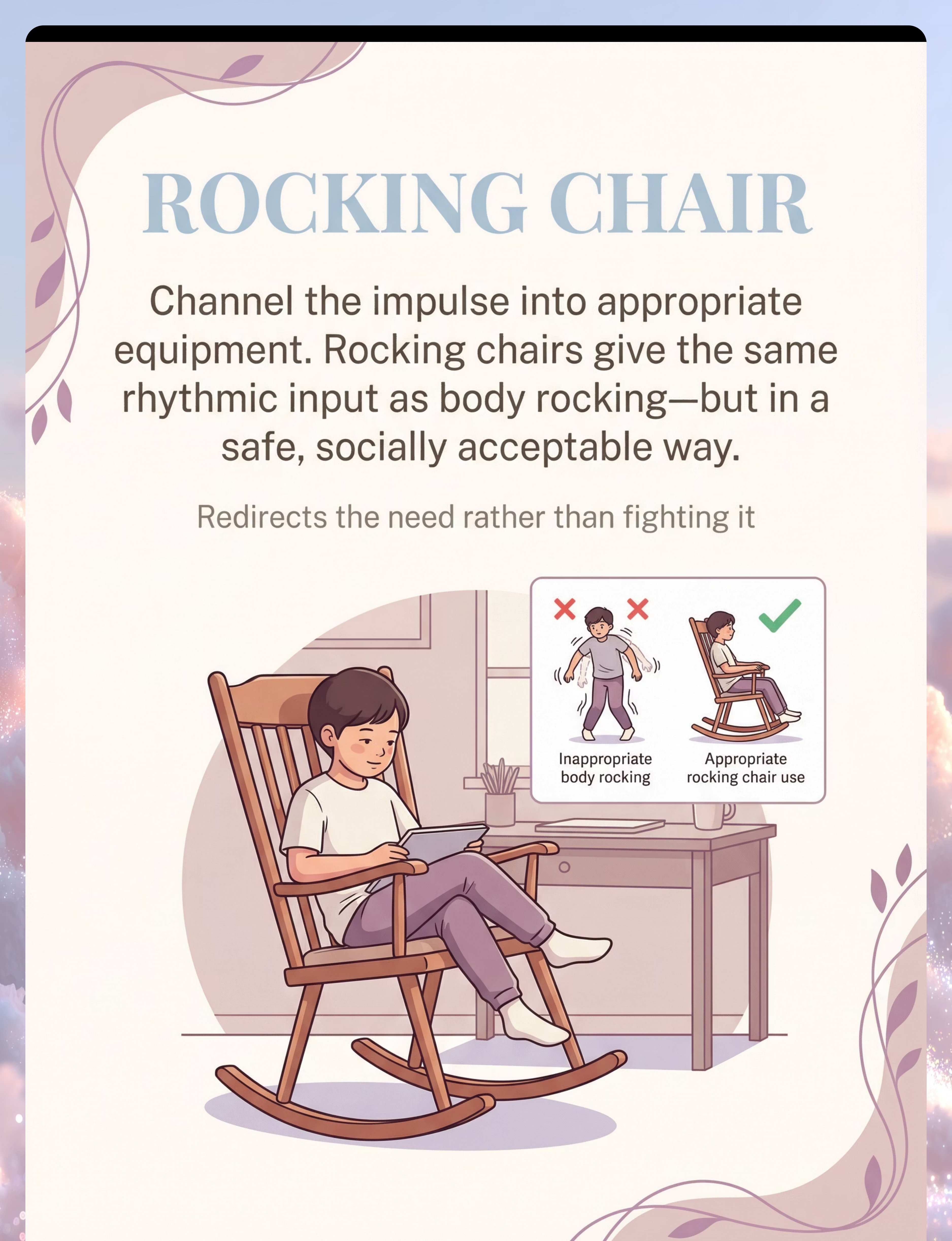
🪑 Material 2 — Therapy Rocking Chair / Glider
Canon: Sensory Furniture / Regulation Seating
Channels the rocking impulse into appropriate equipment. Same rhythmic vestibular input as body rocking — but in a safe, socially acceptable form. Critical for homework, mealtimes, and any seated activity where rocking is disruptive. Vestibular type: Linear rhythmic | Intensity: ●●○○○ Low-Medium | Price: ₹2,500–10,000

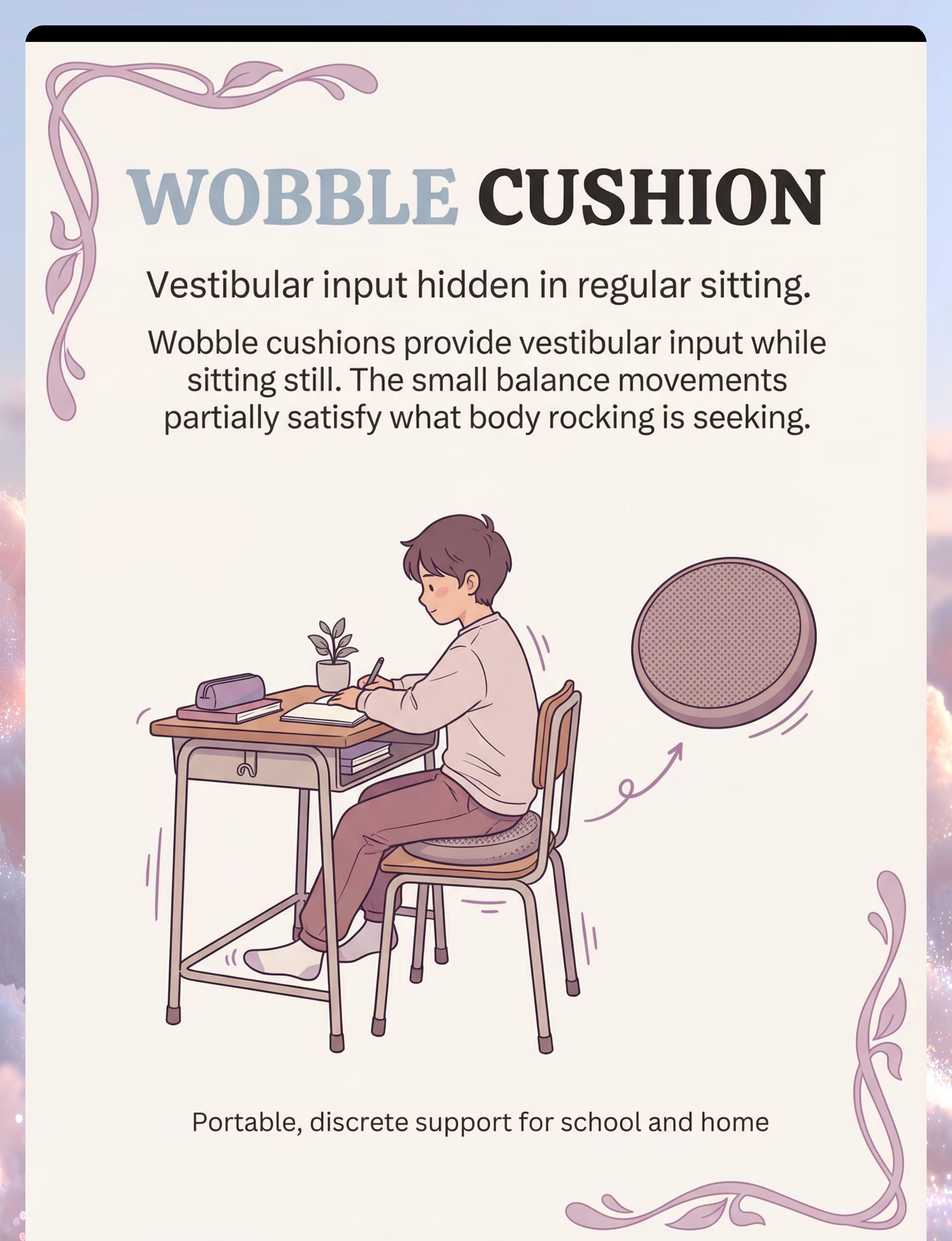
🟣 Material 3 — Wobble Cushion / Inflatable Seat Disc
Canon: Proprioceptive / Balance Equipment
Provides continuous low-level vestibular and proprioceptive input while appearing to sit normally. Critical for classroom settings. Portable, affordable, and invisible to others. The seated child receives constant micro-vestibular input that reduces the drive to rock. Vestibular type: Micro-vestibular + proprioceptive | Intensity: ●○○○○ Low | Price: ₹400–1,200

🛌 Material 4 — Weighted Blanket / Weighted Lap Pad
Canon: Deep Pressure / Proprioceptive Inputs
Addresses the self-soothing and calming function of rocking. Deep pressure activates the parasympathetic nervous system, promoting regulation without movement. Essential for sleep-related rocking and anxiety-driven rocking. System targeted: Proprioceptive + parasympathetic | Intensity: ●●●○○ Medium | Price: ₹1,500–10,000

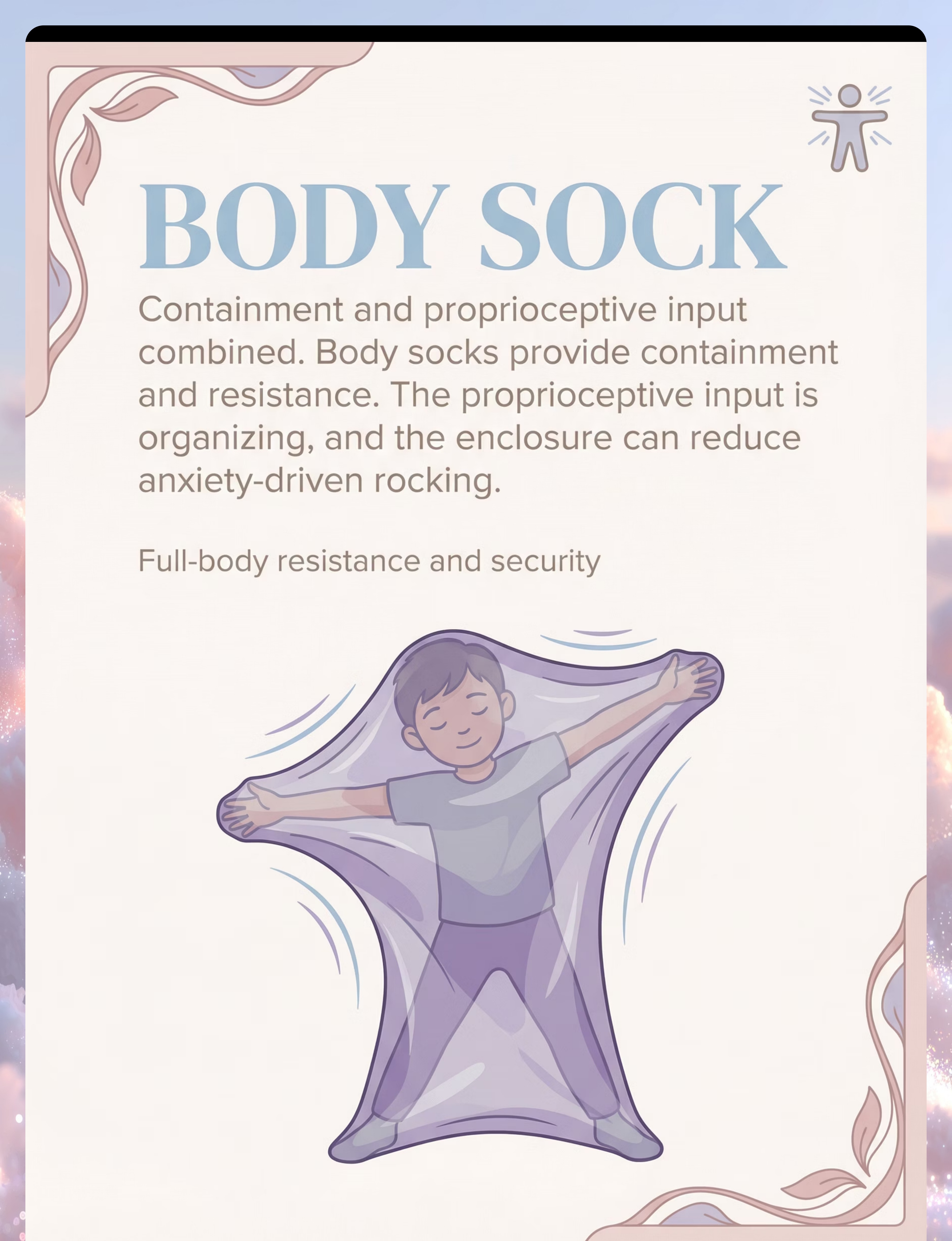
🧶 Material 5 — Body Sock / Lycra Compression Wrap
Canon: Compression / Containment Equipment
Provides full-body proprioceptive feedback and containment. The resistance to movement reduces rocking while the enclosed feeling addresses anxiety-driven rocking. Used as "heavy work" before challenging situations. System targeted: Proprioceptive + containment | Intensity: ●●●○○ Medium | Price: ₹800–2,500

⚽ Material 6 — Therapy Ball / Peanut Ball
Canon: Proprioceptive / Vestibular Equipment
Provides vestibular and proprioceptive input through bouncing and rolling. Structured bouncing sessions can proactively satisfy vestibular seeking, reducing rocking throughout the day. Peanut ball shape adds stability for beginners. Vestibular type: Bouncing/oscillating | Intensity: ●●●○○ Medium-High | Price: ₹600–2,000

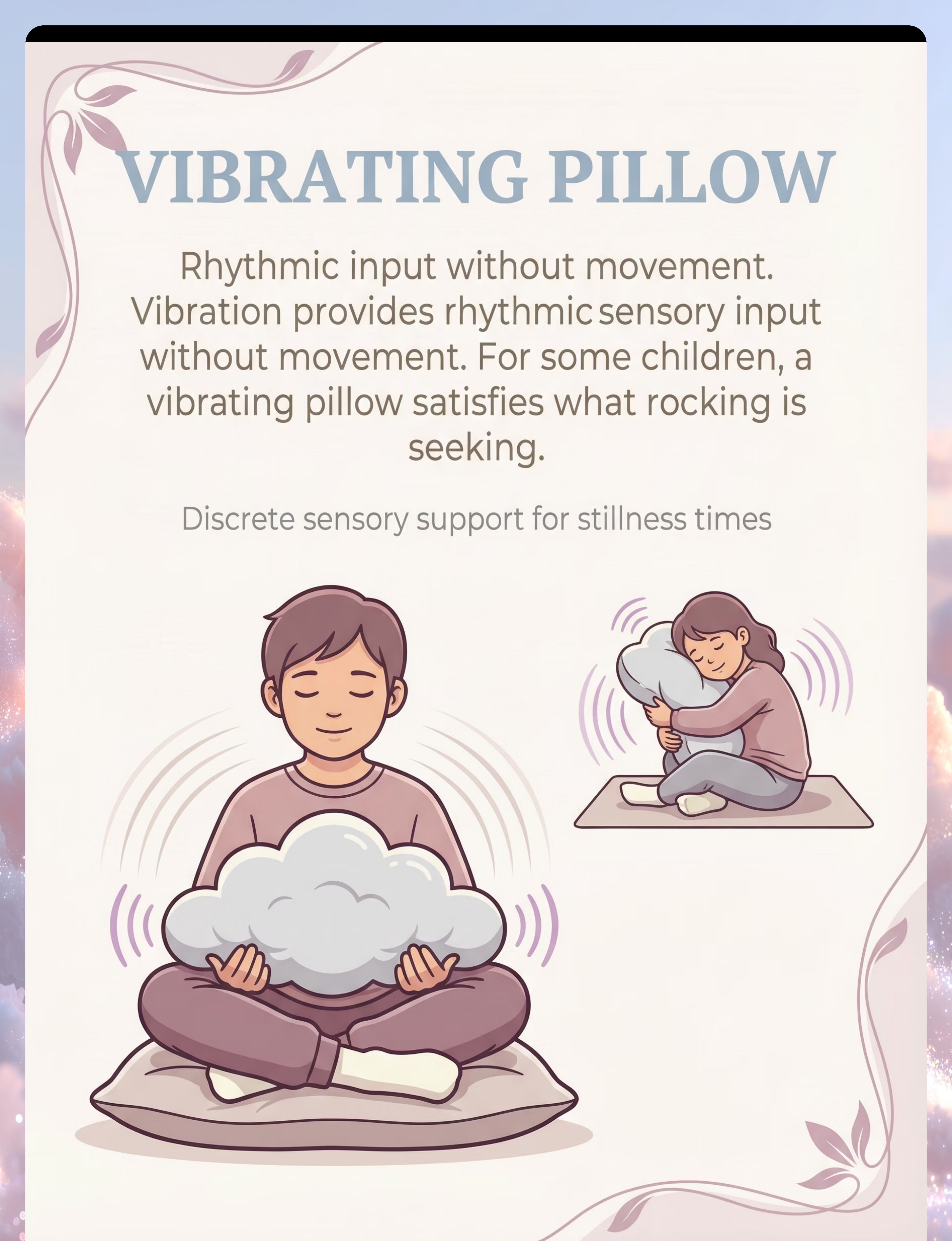
📳 Material 7 — Vibrating Pillow / Vibration Tools
Canon: Tactile / Vibratory Sensory Tools
Delivers rhythmic sensory input without requiring movement. For children who rock for rhythmic input (not just vestibular), vibration can satisfy the need while sitting completely still. Discrete and usable in any setting. System targeted: Tactile + proprioceptive (rhythmic) | Intensity: ●●○○○ Low-Medium | Price: ₹500–2,000
🪢 Material 8 — Cocoon Swing / Sensory Hammock
Canon: Sensory Swings & Vestibular Equipment
Combines vestibular input WITH deep pressure containment — addressing multiple sensory needs simultaneously. Often the most powerfully regulating single piece of equipment for body rockers who seek both movement AND security. Children frequently self-regulate in cocoon swings for 20–30+ minutes. Vestibular type: Oscillating + deep pressure | Intensity: ●●●●○ High | Price: ₹2,500–8,000 | Top Recommendation ✓

🌀 Material 9 — Fidget Tools / Hand Occupation Objects
Canon: Fidget Tools / Tactile Exploration
Redirects sensory-motor energy from whole-body rocking to small-motor hand activity. When hands are engaged with rhythmic fidgets (spinners, rocking fidgets), the body often rocks less. Supplementary to vestibular strategies — best used during seated tasks. System targeted: Sensory-motor redirection | Intensity: ●○○○○ Low | Price: ₹100–800
🎯Pinnacle Recommended Starter Kit — Begin with these 3, add others as your sensory diet develops: (1) Wobble Cushion ₹400–1,200 — for school and desk immediately; (2) Cocoon or Platform Swing ₹3,000–8,000 — for home intensive input; (3) Fidget Tools ₹100–800 — portable supplementary support. Total starter investment: ₹3,500–10,000. Questions? Call FREE Helpline: 9100 181 181

Every Material Has a Zero-Cost Version. No Family Left Behind.
WHO/UNICEF equity principle: therapeutic access regardless of economic circumstance. These DIY alternatives use the same sensory principles as clinical-grade materials.
🛒 Clinical Material | 🏠 DIY / Substitute | Why It Works | |
Platform Swing | Doorway baby swing used at higher ages, OR improvised rope swing from sturdy tree branch with safe seat | Same linear vestibular input; adjust arc size | |
Rocking Chair | Low stool with parent's feet as footrest, rocking the child rhythmically; OR existing chair with runner boards | Same rhythmic linear vestibular input | |
Wobble Cushion | Partially inflated beach ball or round balloon placed under sitting surface | Same micro-vestibular effect; check stability frequently | |
Weighted Blanket | Standard blanket + small bags of rice/lentils sewn into pockets (10% of body weight); OR two heavy blankets layered | Same deep pressure proprioceptive activation | |
Body Sock | Old, stretchy nylon stocking cut open, OR large elastic lycra tube fabric from fabric store | Same proprioceptive resistance and containment | |
Therapy Ball | Partially deflated football or basketball for smaller children; OR firm round pillow | Reduced input; effective for mild seekers | |
Vibrating Pillow | Place phone on vibrate mode under pillow; OR electric toothbrush head gently applied to palm | Same vibratory tactile input pathway | |
Cocoon Swing | Large bedsheet tied at four corners from sturdy beam, child sits inside | Same containment + oscillation; check load rating carefully | |
Fidget Tools | Small smooth stones, dried beans in fabric pouch, wooden bead on string | Same sensory-motor hand occupation |
⚠️When Clinical-Grade Is Non-Negotiable: DIY swing mounting — NEVER mount improvised swings in drywall alone. Must reach structural joists or use rated hardware. Weighted products: ensure homemade versions can be removed by child independently. Body socks: ensure child can always exit easily. When in doubt, call 9100 181 181 for guidance.

Read This Before Your First Session. Every Time.
🟢 GREEN — Safe to Proceed
Child is fed, rested, and in a baseline regulated state. All swing hardware has been professionally checked. Swing fall zone is clear, padded, and hazard-free. Child can communicate discomfort. Parent has reviewed this safety card.
🟡 AMBER — Modify the Session
Child had a meltdown in the past 2 hours → Use wobble cushion or fidgets only. Child appears tired → Shorten session. Swing mounting not yet verified → Wobble cushion and rocking chair only. Child is unfamiliar with equipment → Introduce gradually.
🔴 RED — Do Not Proceed Today
Child is unwell, feverish, or showing signs of ear infection. Child has had a seizure recently (consult neurologist first). Swing hardware shows ANY sign of wear or damage. Child shows extreme fear or panic when approaching equipment.
Material | Do NOT Use If | |
Swings (all types) | Ear infection, recent seizure, untested hardware | |
Weighted blanket | Child cannot remove independently; under 2 years without OT guidance | |
Body sock | Child is claustrophobic; respiratory concerns | |
Wobble cushion | Child has significant balance impairment (risk of falls) | |
Vibrating tools | Battery compartment not secure; child over-sensitive to vibration |
🛑Stop immediately if: Nausea, pallor, or dizziness after swinging | Child becomes MORE agitated after 10+ minutes | Flushed face or heavy breathing in body sock | Child cannot exit equipment | Head banging accompanies rocking → Seek immediate professional consultation.
The Right Environment Prevents 80% of Session Failures
A properly prepared space transforms a good technique into a great session. Set up before your child enters the room — every time.
Child Starting Area
Clear open space where child begins; not near sharp corners or furniture edges
Equipment Zone
Swing area with minimum 1 meter clearance in all directions; soft gym mat underneath; nothing breakable within swing arc
Materials Basket
All session materials pre-organized; weighted items already warmed; fidgets arranged by type
Parent Position
Beside the child (not behind) — always within arm's reach of swing; eye contact maintained throughout
Visual Timer
Place where child can see it; reduces "when will this end" anxiety; supports cool-down transition
Reinforcement Station
Child's preferred reward within parent's reach but not visible to child until earned
Environment Settings
- Lighting: Warm, diffused — avoid harsh overhead fluorescents; dim if child is over-stimulated
- Sound: Calm background music at low volume (40–50 dB); NO TV; NO competing voices
- Temperature: 20–24°C; if using body sock, slightly cooler to prevent overheating
- Distractions: Screen devices OFF, siblings in separate space if possible
Why Environment Matters
Ayres Sensory Integration® (ASI) establishes structured environment as a core clinical principle. A 1:1 individual session in a structured, distraction-free environment shows maximum efficacy according to meta-analysis data (PMC10955541). The environment IS part of the therapy.

The Best Session Is One That Starts Right. 60-Second Readiness Check.
Before every session, run through this quick assessment. Your child's state when you begin determines the outcome more than any other single variable.
Check | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Hunger/Thirst | Fed within 1 hour | Slightly hungry — offer snack first | Hungry or thirsty now | |
Energy Level | Alert, engaged, baseline | Tired but responsive | Exhausted, about to sleep | |
Emotional State | Calm or mildly dysregulated | Elevated but redirectable | Meltdown within 30 min | |
Physical State | Well, no signs of illness | Mild cold but engaged | Fever, ear pain, nausea | |
Rocking State | High-frequency rocking (good intervention time) | Moderate rocking | No rocking at all today | |
Time Available | 20+ minutes uninterrupted | 10–15 minutes | Less than 10 minutes |
🟢 ALL GREEN → Proceed
Full protocol — continue to Step 1: The Invitation
🟡 1–2 AMBER → Modified
Wobble cushion at desk only. Skip swings; use rocking chair. Shorten to 10 minutes; reduce intensity.
🔴 ANY RED → Postpone
Do NOT push through a red flag. Offer 5 minutes of deep pressure + quiet activity. Reschedule tomorrow. "Session abandonment is not failure — it's clinical wisdom."

STEP 1 OF 6
The Invitation
⏱️ 30–60 seconds
For the Swing
"[Child's name], look — the swing is ready! Want to try it? You can show me how fast."
For the Rocking Chair
"[Child's name], I put the special rocking chair by your table. Want to sit in it while we do [favorite activity]?"
For the Wobble Cushion
"[Child's name], this funny cushion wiggles! Want to sit on it? It's kind of bouncy."
Parent Body Language Guide
- ✅ Get to child's eye level before speaking
- ✅ Relaxed posture — no urgency or anxiety in your body
- ✅ Gesture toward the equipment, don't lead the child to it
- ✅ Smile — this is supposed to be enjoyable
- ❌ Do NOT say "Stop rocking and try this instead" — creates negative framing
Reading Your Child's Response
Acceptance cues: Child moves toward equipment | Eye contact or brief look | Decreased rocking | Vocalization of interest
Resistance cues: Child moves away → Wait 2 minutes, offer again with preferred toy near equipment. Child ignores → Place yourself near equipment and do something interesting there. Child protests → Honor the no; try rocking chair or fidget instead.
ABA Principle at work: This is "pairing" — associating the equipment with positive experience before any demand is placed. Never force approach to equipment. The therapeutic goal is that the child WANTS to use it.

STEP 2 OF 6
The Engagement
⏱️ 1–3 minutes
Platform / Cocoon Swing
Help child into swing, ensuring secure positioning. Begin with SMALL, gentle pushes — not full arc immediately. Stand in front of child, maintaining eye contact. If child is enjoying it, gradually increase arc.
Rocking Chair
Child sits in chair; their feet should reach floor or a footstool to push off. Parent sits beside, not across. Introduce a preferred activity (book, small toy) — the chair rocks while they engage.
Wobble Cushion
Place cushion on chair. Child sits on cushion. No instruction needed — the cushion does its work passively. Introduce their regular seated activity.
Weighted Lap Pad
Place gently across child's lap while they're already seated in a preferred activity. Don't draw attention to it initially — let it do its work quietly.
Child Response | Meaning | What to Do | |
Immediate engagement, seeking more | Strong vestibular seeker — needs this | Provide; schedule daily | |
Tolerates passively | Accepting; sensory need may be moderate | Continue; watch for increased engagement | |
Seeks to exit | May not be vestibular type; or too much too soon | Reduce intensity; try rocking chair first | |
Escalates rocking ON the equipment | High sensory need — saturation not yet reached | Allow longer session; increase arc/speed |
When to praise: When child is using the equipment appropriately, engaged, or showing regulated behavior — praise warmly and specifically: "You're doing it! Look how calm your body is in the swing!"

STEP 3 OF 6
The Therapeutic Action
⏱️ 5–20 minutes
The therapeutic action for body rocking intervention is sensory diet delivery — providing organized, controlled vestibular and proprioceptive input through the selected material. The child receives rhythmic, predictable vestibular input through the equipment. The nervous system — which has been self-generating this input through body rocking — now receives it from an external, organized source. Over time and with consistent delivery, the drive to self-generate diminishes.
Platform/Cocoon Swing — The Primary Tool
Duration: 15–25 minutes per session (intense seekers may need 30+). Arc: Start small, increase to comfortable maximum — bigger arc = more input. Direction: Linear (back-forth) is organizing; save rotary for later when OT guides. Watch for: Eyes relaxing, body softening, rocking behavior decreasing.
Rocking Chair — The Redirector
Duration: Unlimited — available whenever child is seated. Rhythm: Child's own pace; don't impose rhythm. Context: During homework, meals, reading, TV — not isolated "rocking time."
Wobble Cushion — The Background Input
Duration: All day during seated activities. Inflation: Start at medium; adjust based on comfort. Academic integration: Full school and homework use.
Weighted Products — The Calmer
Duration: Until child removes it or 30 minutes maximum. Weight: ~10% of child's body weight. Timing: During high-anxiety periods and bedtime.
Therapy Ball — The Proactive Dose
Duration: 10–15 minute bouncing sessions before challenging activities. Support: Parent holds hips initially; build to independent bouncing. Prone activities: Tummy-over-ball + reaching for toys = intense combined input.
✅ Ideal Response
Eyes relax, body softens, rocking frequency decreases 15–20 min post-session; child seems calmer and more focused
⚠️ Acceptable Response
Child tolerates equipment, engages partially, some regulation visible
🛑 Concerning Response
Child becomes MORE agitated after 15+ minutes, shows nausea or pallor → Stop, provide deep pressure, note and consult

STEP 4 OF 6
Repeat & Vary
⏱️ Extend session; vary input
"3 good sessions per week are worth more than 7 forced ones." "20 minutes of engaged vestibular input reduces rocking more than 60 minutes of passive tolerance."
Material | Minimum Effective Dose | Optimal Dose | Maximum Before OT Review | |
Platform/Cocoon Swing | 15 min × 3/week | 20–25 min × 5/week | 30 min × 7/week | |
Rocking Chair | Available all day | Daily during seated tasks | No upper limit | |
Wobble Cushion | School hours daily | All seated activities | No upper limit | |
Weighted Products | 20 min × 3/week | 30 min × daily | 1 hour continuous | |
Therapy Ball Bouncing | 10 min × 3/week | 15 min × 5/week | 20 min × daily |
Variation A: Increase Intensity
When child seems unsatisfied after sessions → Larger swing arc; heavier weight; more inflation on wobble cushion; longer sessions
Variation B: Reduce Intensity
When child seems over-stimulated → Smaller arc; lighter weight; shorter sessions; more predictable rhythm
Variation C: Combine Materials
Advanced sensory diet → Swing session + weighted lap pad afterward + fidget during desk work = layered vestibular diet
Variation D: Integrate with Activities
Naturalistic delivery → Swing while listening to audiobook; rocking chair during homework; wobble cushion during family dinner
Satiation Indicators — when child has had enough: Child attempts to exit equipment independently | Decreased engagement with activity | Signs of drowsiness (vestibular input can be sedating) | Rocking has significantly decreased (goal achieved for this session)
STEP 5 OF 6
Reinforce & Celebrate
⏱️ Within 3 seconds of desired behavior
Reinforcement delivered within 3 seconds is 10× more effective.
When child uses equipment appropriately
"YES! You're using the swing — look how your body is calming down!"
When rocking decreases after session
"I noticed you're not rocking as much right now. Your body found what it needed."
When child requests equipment
"You TOLD me you need the swing — that's amazing. Let's do it right now."
When child completes full session
"You did the whole swing session. That took real focus. I'm so proud of you."
Verbal | Physical | Token/Visual | Tangible | |
Specific praise | High-five | Star on chart | Preferred snack (small) | |
"I noticed..." | Thumbs up | Sticker on board | 2 min favorite activity | |
Name the achievement | Hug (if welcome) | Check mark | Small preferred toy | |
"You showed..." | Squeeze hand | Progress bar fills | Screen time (1 min) |
ABA Principle: Celebrate the ATTEMPT, not just the perfect execution. A child who tolerates 30 seconds in the swing today is building toward 20 minutes. Reinforce the tolerance, not the goal.

STEP 6 OF 6
The Cool-Down
⏱️ 2–3 minutes
No vestibular session ends abruptly. The nervous system needs a graduated transition from activated input to baseline — just like cooling down after exercise. Use the same language every session — predictability is calming.
The 2-Minute Warning
Show visual timer (or fingers): "2 more swings, then we're all done." Same language every session — predictability reduces protest.
Slow the Input
Gradually slow swing arc; reduce bounce amplitude on therapy ball; have child begin to settle in rocking chair.
Transition Object
Offer a familiar comfort item or preferred fidget as the equipment session ends — bridges the transition.
The Put-Away Ritual
Child participates in putting away materials — wobble cushion back in basket, fidgets in pouch. Builds routine and ownership.
Proprioceptive Landing
After vestibular input, provide brief deep pressure: gentle shoulder squeeze, weighted lap pad for 2 minutes, or child hugs knees to chest. This "grounds" the vestibular input and aids regulation.
Transition to Next Activity
Use visual schedule or clear verbal statement: "Swing time is done. Now it's [next activity] time."
⚠️If child resists ending: Extend by 2 minutes only (not indefinitely). Use visual timer — child sees time ending independently. Offer the next activity as something preferred. If daily protest, review: is the child getting enough daily vestibular input? Add more sessions.
60 Seconds of Data Now Saves Hours of Guessing Later.
Capturing session data transforms guesswork into clinical intelligence. You'll know which materials work, when to increase intensity, and whether rocking is truly decreasing over time.
📋 D-364 Session Tracker
After every session, record:
- Date, time, and duration
- Material used today (circle one): Platform Swing | Cocoon Swing | Rocking Chair | Wobble Cushion | Weighted Blanket | Body Sock | Therapy Ball | Vibrating Pillow | Fidget Tools
- Rocking frequency BEFORE session: Constant / High / Moderate / Low
- Rocking frequency 30 MIN AFTER session: Constant / High / Moderate / Low
- Child's regulation state after session: Calmer / Same / More activated
- Notes / observations
What the Data Tells You
📉 Rocking Before vs. After
Is the material reducing the need? If rocking after session equals rocking before, increase intensity/duration.
📈 Weekly Trend
Is rocking frequency decreasing across the week? Visible progress is the strongest parent motivator.
🎯 Which Materials Work
Different children respond to different materials. Data reveals YOUR child's profile.
📞 Questions about your data? Call FREE National Autism Helpline: 9100 181 181 (24×7, 16+ languages)
Most Sessions Don't Go Perfectly. That's Not Failure — That's Data.
When things don't go as planned, each difficulty is a diagnostic clue pointing you toward a better-matched approach. Here are the 7 most common problems and exactly what to do.
❓ Child refused to get near the swing at all
Why: Equipment is unfamiliar; child may be vestibular avoidant (not all rockers are vestibular seekers — some rock from anxiety). Solution: Start with rocking chair for 2 weeks. Place swing in room but don't require use. Do "silly" low-demand activities near swing. If avoidance persists: ABA pairing consultation.
❓ Child got MORE revved up on the swing, not calmer
Why: Either session too short (vestibular seekers go through an "activation" phase before regulation), or rotary/spinning input is dysregulating. Solution: Try 5 more minutes before judging. Switch to linear-only input. Reduce swing arc. If consistently dysregulating: OT consultation for full sensory profile.
❓ Child rocked just as much after the swing session as before
Why: Vestibular need not yet satisfied — need was larger than the dose provided. Solution: Double session duration. Increase swing arc. Add therapy ball bouncing 30 minutes after swing. Consider: is this child's sensory need very high? Consult OT for intensive sensory diet.
❓ Child loved it and cried when session ended
Why: The vestibular need is strong — child has found the solution but can't have unlimited access. Solution: This is excellent feedback — the material is working! Increase daily frequency to 2 sessions/day. Add a second session at the time of most problematic rocking (before school, before bed).
❓ Wobble cushion keeps sliding off the chair
Why: Chair surface is smooth or molded. Solution: Place non-slip mat between cushion and chair. Use velcro strips. If still sliding: select chair with flat, rougher surface. Tape a strip of non-slip drawer liner to chair seat.
❓ Child won't keep the weighted lap pad on
Why: May be too heavy; texture aversion; or not the right regulation strategy for THIS child. Solution: Start with lighter weight (0.5–1 kg). Try different fabric cover. Offer as OPTIONAL. If consistently rejected: body sock or vibrating pillow may be better match.
❓ Rocking stopped during session but returned immediately after
Why: Input satisfies in-session need but sensory diet needs more coverage throughout day. Solution: This is success — the material works. Add wobble cushion for all-day seated use + fidgets for between major vestibular sessions.
When to escalate: Any response that concerns you that isn't covered above — call 9100 181 181. For persistent concerns: OT comprehensive assessment. For red flags or injury risk: clinic visit same day.

No Two Children Are Identical. Here's How to Adjust.
Child Profile | Best Starting Materials | Intensity Setting | Notes | |
Vestibular Seeker (rocks constantly) | Platform swing → Cocoon swing | High; long sessions | This child needs A LOT of input — don't under-dose | |
Anxiety-Driven Rocker (rocks when stressed) | Weighted blanket → Cocoon swing | Medium; calming focus | Address anxiety alongside sensory; containment prioritized | |
Habitual Rocker (light, constant, automatic) | Rocking chair → Wobble cushion | Low; redirect strategy | Less about sensory intensity, more about appropriate outlet | |
Younger child (2–4 yrs) | Rocking chair, therapy ball, weighted products | Low-Medium; short sessions | Swings need extra supervision; 5–10 min max initially | |
Older child (8–12 yrs) | All materials; self-selected | Medium-High; self-regulated | Can participate in choosing own sensory diet tools | |
ADHD co-diagnosis | Wobble cushion + therapy ball | Medium-High; movement-inclusive | Focus on movement during tasks, not isolated sessions |
Under 3
Rocking chair (supervised), vibrating pillow, gentle therapy ball on parent's lap
Ages 3–6
Introduce platform swing with maximum supervision; body sock with parent present
Ages 6–10
Begin self-selected sensory diet; teach child to identify their own needs
Ages 10–12
Self-advocacy skills — child learns to request movement breaks; manage own fidgets
ACT IV: THE PROGRESS ARC
Week 1–2: Tolerance, Not Transformation.
The first two weeks are about building the foundation — not seeing the final result. Your nervous system is learning a new road. Be patient with the process.
Child tolerates equipment for 5–10 min
What this means: Nervous system accepting the new input source. What it's NOT yet: Full regulation — that comes later.
Rocking continues between sessions
What this means: Normal — sensory diet not yet at coverage level. What it's NOT yet: Failure of the intervention.
Brief periods of calm AFTER swing use
What this means: Evidence that input is working. What it's NOT yet: Permanent change — it's temporary at this stage.
Child begins to approach equipment without prompting
What this means: Nervous system associating equipment with need satisfaction. What it's NOT yet: Self-advocacy — that comes at 4–6 weeks.
"If your child tolerates the swing for 3 minutes longer than last week — that is real, measurable neurological progress. The brain is forming new pathways. It takes time."
Week 1–2 is the hardest. The rocking doesn't stop. The child may resist equipment. You may doubt the approach. This is normal. The research shows that consistent application across 8–12 weeks produces measurable change. Trust the protocol.

Week 3–4: The Nervous System Is Starting to Learn.
Progress bar: ████████░░░░░░░░░░░░ 40%
✅ Child anticipates the equipment
They may walk toward the swing before being invited, or reach for the wobble cushion. This is the nervous system associating the tool with need satisfaction.
✅ Rocking AFTER sessions is shorter/less intense
Post-session regulation windows are extending. Note in your tracking sheet how long the "rocking quiet period" lasts after each session.
✅ Rocking in specific settings decreasing
The setting where intervention is most consistent (e.g., home homework with wobble cushion) shows improvement before other settings.
✅ Child shows emerging preference for one material
This is diagnostic gold — the material they choose is the one that best addresses their sensory need profile.
Neural Pathway Analogy: The nervous system has been rocking for months or years because that's its established pathway for getting vestibular input. You're building a new road — the swing road, the rocking chair road. New neural roads take 3–6 weeks of consistent use before they feel "natural." Weeks 3–4 is when the road starts to form.
When to increase frequency/intensity: If rocking is still constant across all settings in week 4 — increase swing sessions from 3× to 5×/week; extend from 20 to 30 minutes; add wobble cushion to all seated contexts.

Week 5–8: Mastery Unlocked. Your Child Is Regulating.
Progress bar: ███████████████░░░░░ 75%
Rocking Reduction
Criteria 1: Rocking frequency decreased by 40%+ compared to week 1 baseline
Minutes of Calm
Criteria 3: Post-session regulation window extended to 45+ minutes (was 10–15 min in weeks 1–2)
Mastery Criteria
Meeting 3 or more of 5 mastery criteria signals readiness to progress to the next technique
🏅 Criteria 2
Child uses equipment independently or with single verbal prompt — reduced adult initiation needed
🏅 Criteria 4
Teacher or school reports improvement in seated behavior or reduced disruptive rocking
🏅 Criteria 5
Child beginning to self-advocate: "I need the swing" / reaching for wobble cushion / requesting rocking chair
Generalization indicators: Skill appearing in NEW settings (school, grandparents' home, car) | Child requesting sensory tools in novel environments | Reduced rocking during community outings | Caregiver consistency has made the sensory diet second nature.

You Did This. Your Child Grew Because of Your Commitment.
Your Journey
8 weeks ago: You were confused, worried, and watching your child rock with no understanding of why.
Today: You understand vestibular processing. You've built a sensory diet. You've transformed ordinary household time into therapeutic intervention. You've watched your child use equipment and self-regulate in ways that weren't possible before.
That is clinical-grade parenting. That is GPT-OS® in action in a home.
🎉 Milestone Ritual
Tonight, tell your child specifically what you noticed: "I saw how you went to the swing when you felt the rocking coming. You're learning to know your body. That is amazing."
📸Document this milestone: Photo of your child's sensory diet setup, or your tracking sheet showing progress — save it. In 6 months, you'll want to see how far you've come.
You arrived here scared, reading another parent's words that could have been yours. You leave here empowered, with data, techniques, and a community. From fear to mastery. One technique at a time.

Even in Progress, Watch for These Signs. Trust Your Instincts — Pause and Ask.
🚩 Red Flag | What It Looks Like | Why It Matters | What to Do | |
Head banging WITH rocking | Rocking accompanied by hitting head against wall/floor | Significant injury risk; may indicate high-level distress or neurological concern | IMMEDIATE professional consultation — do not delay | |
Rocking so intense it causes injury | Chair falls, child falls from intensity, bruising | Beyond sensory seeking level — may need medical evaluation | Pause all vestibular activities; consult neurologist and OT same day | |
New onset rocking after period of no rocking | Previously not rocking; suddenly rocking constantly | May indicate developmental regression, medical issue, or significant anxiety event | Pediatric neurological evaluation | |
No response to ANY intervention after 8 weeks | All 9 materials tried; rocking unchanged or worsening | Function may be neurological or medical rather than sensory | OT comprehensive assessment; consider intensive therapy program | |
Child in distress DURING rocking | Crying, visible distress, cannot be comforted | Rocking not serving self-regulation — may be sign of pain or severe anxiety | Medical evaluation to rule out organic causes | |
Equipment accidents | Falls from swing, near-miss injuries, hardware failure | Safety crisis | Remove from use immediately; professional installation review |
Step 1: Self-Resolve
Minor concerns not resolving within 48 hours — monitor and adjust protocol
Step 2: Teleconsult
Persistent concerns or unclear picture — Call FREE Helpline: 9100 181 181 (24×7, 16+ languages)
Step 3: Clinic Visit
Red flags, injury risk, or regression — Find nearest Pinnacle center immediately
📞FREE National Autism Helpline: 9100 181 181 | Available 24 hours × 7 days × 365 days | 16+ languages | Immediate guidance | No appointment needed. If something feels wrong, call. That's what we're here for.
You're Not Done. You're on a Journey.
D-364 is one waypoint in a connected map of sensory and developmental techniques. Every skill you've built here accelerates your progress in what comes next.
If rocking decreased but vestibular seeking continues
→ D-365: Spinning Behaviors — next technique in the sensory-seeking cluster
If rocking and other regulation challenges persist
→ K-835: Building a Home Sensory Diet — full ecosystem approach
If child has mastered D-364 and is ready for next step
→ C-201: Emotional Regulation Toolkit — bridge to Domain C
Long-term developmental goal: D-364 feeds into Sensory Regulation Readiness → Self-Regulation Mastery → Classroom Readiness → Social Participation Readiness — all tracked by GPT-OS® Readiness Indexes.
More Techniques in Sensory Processing — Domain D
You already own several of the materials needed for these techniques. Explore what comes next — or what runs alongside D-364 in your child's sensory profile.

🤚 D-363: Hand Flapping — 9 Materials That Help
Difficulty: ● Intro | Materials: Fidget tools, resistance bands

🔄 D-365: Spinning Behaviors — 9 Materials That Help
Difficulty: ●● Core | Materials: Swings, rotary equipment

👅 D-366: Mouthing Objects — 9 Materials That Help
Difficulty: ● Intro | Materials: Chew tools, oral-motor equipment
🌊 D-370: Sensory Seeking Overview
Complete Domain Guide | Difficulty: ●●● Advanced | Materials: Full sensory diet
🧠 D-375: Vestibular Input Needs
Deep Dive Series | Difficulty: ●● Core | Materials: All vestibular equipment
🏠 K-835: Home Sensory Diet
Parent Masterclass | Difficulty: ●● Core | Materials: All 9 from D-364 — no new purchases needed

This Technique Is One Piece of a Larger Plan.
GPT-OS® tracks your child's development across all 12 domains simultaneously. D-364 is your current active domain — and it unlocks progress in everything that follows.
Domain | Your D-364 Technique Feeds | Connection | |
D — Sensory (active) | ★ Current focus | Platform for all other domains | |
C — Emotional Regulation | Improved regulation = emotional availability | Vestibular input supports emotional stability | |
B — Communication | Calmer child = more communicative child | Regulation precedes communication | |
F — Play | Less rocking = more play engagement | Freed-up motor system enables play | |
H — Social | Less conspicuous rocking = better social integration | Sensory management supports social participation |
🔗See your child's complete developmental profile across all 12 domains. Track progress. See the interconnections. Receive personalized next-technique recommendations. Access GPT-OS® Dashboard → pinnacleblooms.org/gpt-os/ or call: 📞9100 181 181 for a guided AbilityScore® assessment.
ACT V: COMMUNITY & ECOSYSTEM
Real Families. Real Change.
Illustrative cases drawn from Pinnacle center outcomes. Individual names anonymized. Outcomes vary by child profile and intervention consistency.
Priya, 7 — Hyderabad
Before: Rocked constantly — at mealtimes, during homework, watching TV. Her teacher sent a note home. Her parents were devastated and confused.
What they did: Platform swing installed in living room. Swing sessions every morning before school (20 minutes) and before homework (15 minutes). Wobble cushion at desk full-time.
6 weeks later: Teacher messaged unprompted: "I don't know what you changed at home, but Priya is sitting still during class. She raises her hand. She's engaged."
Parent quote:"The swing didn't fix everything. But it fixed the thing that was blocking everything else. The rest followed."
Therapist's Notes: Classic vestibular seeker profile. Platform swing delivered the vestibular input her nervous system had been self-generating through body rocking. Once the need was met proactively, the behavior naturalized.
Arjun, 5 — Bengaluru
Before: Rocked to fall asleep — intensely, sometimes 45 minutes of rocking before sleep. Parents were exhausted. Multiple pediatricians said "he'll grow out of it."
What they did: Weighted blanket (2.5 kg) at bedtime. 10-minute rocking chair time as part of bedtime routine before weighted blanket. Vibrating pillow as additional calming tool.
4 weeks later: Sleep rocking reduced from 45 minutes to 8–12 minutes. Parents slept. Arjun slept.
Therapist's Notes: Bedtime rocking served a self-soothing + proprioceptive function. Weighted blanket provided the calming input without requiring movement. Rocking chair redirected the final vestibular need appropriately.
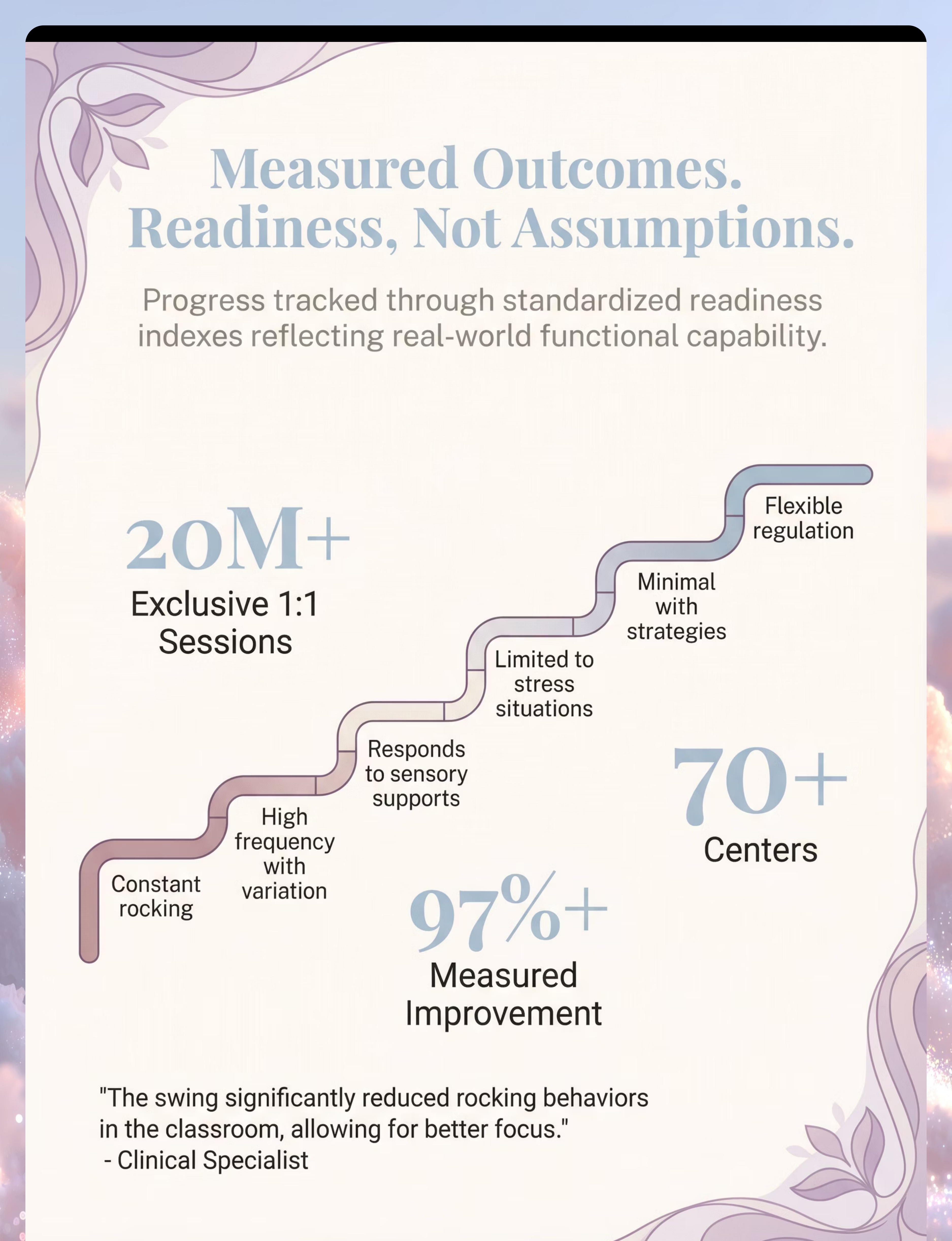
97%
Family Improvement Rate
families report meaningful improvement in one or more readiness indexes within 8–12 weeks of consistent sensory diet application
20M+
Therapy Sessions
exclusive 1:1 sessions across 70+ centers in 70+ countries — GPT-OS® measured outcomes

Isolation Is the Enemy of Adherence. Join the Community.
💬 Pinnacle Parent WhatsApp Group — Sensory Processing
Connect with parents navigating vestibular seeking, body rocking, and sensory diets in real time. Share tracking data. Ask questions. Get support from people who understand exactly what you're living through.
🌐 Pinnacle Parent Forum
Moderated by Pinnacle consortium therapists. Search by technique (D-364), domain (Sensory), or challenge. Browse 1,000+ solved parent questions.
📍 Local Parent Meetups
Find Pinnacle parent meetup groups near your city. 70+ centers across India host monthly parent circles. Because in-person community accelerates caregiver confidence and child outcomes.
🤝 Peer Mentoring Program
Connect with a parent who has already navigated D-364 and body rocking. Matched by child's profile and your city. Your experience helps every family that comes after you.
Home + Clinic = Maximum Impact.
Home implementation is powerful. Combined with professional guidance, it becomes transformational. Find your nearest Pinnacle center or book a teleconsult — available in 16+ languages.

🦾 Occupational Therapist
Primary lead for D-364. Conducts comprehensive sensory profile assessment, designs full sensory diet, supervises swing installation and safety. Book OT Assessment → pinnacleblooms.org/book/

📊 ABA/BCBA Behavioral Therapist
Conducts functional behavior analysis of rocking, designs replacement behavior program, monitors data. Essential when rocking has a strong habit or anxiety-driven function. Book Behavioral Assessment at pinnacleblooms.org/book/

🧠 NeuroDev Pediatrician
Rules out neurological causes, confirms diagnosis, coordinates overall intervention plan. Determines when rocking warrants urgent evaluation vs. therapeutic management.

💻 Teleconsultation
Remote families: Video consultation with Pinnacle consortium therapist. Available in 16+ languages. Serving families across 70+ countries through GPT-OS®.
📞FREE National Autism Helpline: 9100 181 181 | Available 24 hours × 7 days × 365 days | 16+ languages | Immediate guidance | No appointment needed. "Home + clinic = maximum impact. One without the other is half the intervention."
The Science Behind This Page. For the Curious Parent.
D-364 is supported at the highest levels of clinical evidence. These are not opinions — they are peer-reviewed findings from systematic reviews, meta-analyses, and randomized controlled trials.
Systematic Review
PRISMA (2024) — PMC11506176
Meta-Analysis
24 Studies (2024) — PMC10955541
RCT — India (2019)
DOI: 10.1007/s12098-018-2747-4
Cohort / Observational Studies
Multiple institutions, multiple countries
Clinical Consensus + Expert Opinion
Ayres SI® Framework | NCAEP | WHO NCF
Key Studies at a Glance
📄 PRISMA Systematic Review (2024)
16 articles (2013–2023). Vestibular input through swinging meets all criteria for evidence-based practice. Read: PMC11506176 →
📄 Meta-Analysis (2024)
24 studies. Significant effects on sensory processing, adaptive behavior, social skills, and gross/fine motor. Effect sizes statistically robust. Read: PMC10955541 →
📄 Indian RCT (2019)
Padmanabha et al. First Indian population RCT for home-delivered sensory interventions. Parent-administered protocol shown feasible and effective. DOI: 10.1007/s12098-018-2747-4 →
📄 NCAEP Evidence-Based Practices (2020)
Sensory-based interventions, video modeling, and visual supports all classified as evidence-based for autism.
📄 WHO Nurturing Care Framework (2018)
Framework governing early childhood intervention standards across 54+ countries. Pinnacle protocols align with all five NCF components. nurturing-care.org →

Your Data Helps Every Child Like Yours.
When you record a session, you're not just tracking your child's progress — you're contributing to a living clinical dataset that makes every family's protocol smarter.
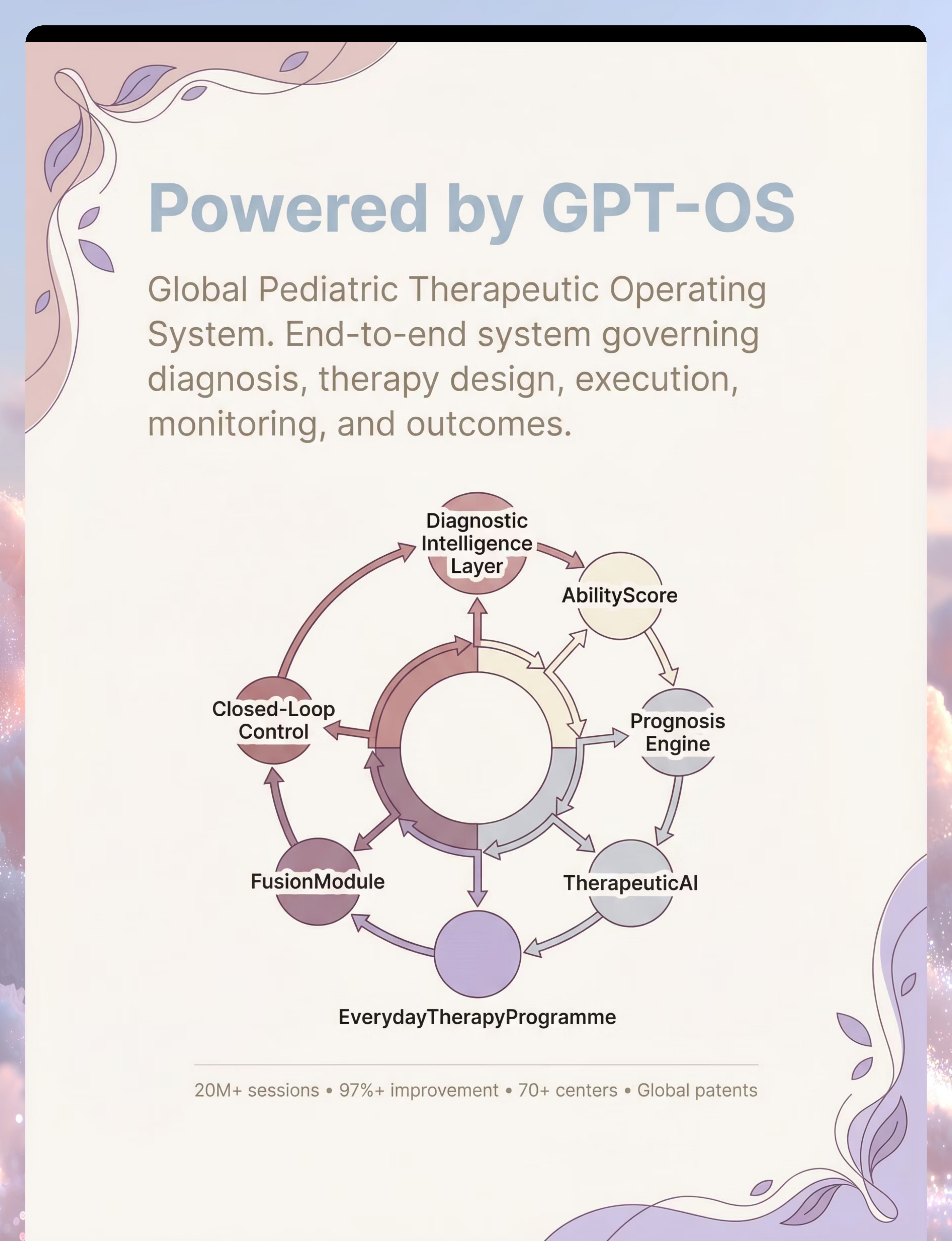
🔵 Diagnostic Intelligence Layer
Classifies your child's rocking profile: vestibular seeker / anxiety-driven / habitual
🔵 AbilityScore®
Assigns baseline score for vestibular processing; tracks longitudinal change across all 12 developmental domains
🔵 TherapeuticAI®
Recommends which of the 9 materials will be most effective for your child's specific sensory profile
🔵 EverydayTherapyProgramme™
Builds your daily sensory diet schedule based on your child's profile and your family's routines
🔵 FusionModule™
Coordinates your OT, ABA, and SpEd inputs as one converged, coherent plan
🔒Your data is protected. GPT-OS® operates under India's PDPB framework and international data protection standards. Your child's identity is never shared. Only anonymized, aggregated patterns contribute to population-level learning. You control your data.

Watch the Reel That Brought You Here
🎬 D-364 — 9 Materials That Help With Body Rocking
Pinnacle Blooms Network® Reels | Sensory & Motor Series — Ep. 364
Therapist: Pinnacle OT Consortium | Runtime: ~60 seconds
Connected Reels in This Cluster
- ← D-363: Hand Flapping
- → D-365: Spinning Behaviors
- D-370: Sensory Seeking Overview
Why Watch Before You Implement
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Watching the Reel before implementing the technique increases parent fidelity and child acceptance of therapeutic materials.
Multi-modal learning research confirms: visual + text + live demonstration improves parent skill acquisition by a statistically significant margin over text alone.
Reel ID: D-364 | Series: Sensory & Motor Development in Children | Episode in Series: 364 of 999 | Domain: D — Sensory Processing / Vestibular Behavior
🔒Reel ID: D-364 | Series: Sensory & Motor Development in Children | Episode in Series: 364 of 999 | Domain: D — Sensory Processing / Vestibular Behavior. This reel is part of the Pinnacle 999 Reels Master — the largest structured pediatric intervention video library on Earth. Reel D-364 confirmed Row 451 in canon taxonomy.

Consistency Across Caregivers Multiplies Impact.
If only one person in your child's life uses the sensory diet, the impact is limited. Share this page — make everyone a therapeutic partner. Research shows multi-caregiver training is critical for generalization and maintenance (PMC9978394 — WHO CCD Package).
📱 Share via WhatsApp
Pre-written message ready to send: "I found this page about body rocking — it explains what's happening and has 9 materials that help. Could you read Cards 01–06 to understand, and Cards 13–22 to help with sessions? [Child's name] needs this consistently."
📧 Share via Email
Subject: "D-364 Body Rocking Technique — Please Read for [Child's name]" — ideal for teachers, pediatricians, and family members who prefer email communication.
📥 Download 1-Page Family Guide
A simplified version of D-364 designed for grandparents, school teachers, domestic helpers, and spouses. The "why" in plain language + "what to do" in clear steps.
Ready-to-send school communication: "Dear [Teacher's name], [Child's name] has been working with a Pinnacle Blooms therapist on vestibular processing support for body rocking behavior. Their protocol includes a wobble cushion for their chair and scheduled movement breaks. This is a medically-supported sensory accommodation. Resources: techniques.pinnacleblooms.org/sensory-processing/body-rocking-materials-D-364 | Pinnacle Helpline for school staff: 9100 181 181"

Your Questions, Answered. From Real Pinnacle Parent Conversations.
❓ Should I try to stop my child from rocking?
Not directly — and never through physical restraint or punishment. Body rocking serves a real neurological function. Trying to stop it without providing an alternative causes distress, anxiety, and the need typically emerges as a different behavior. Instead: provide appropriate vestibular input through the 9 materials, and the rocking naturally decreases as the need is met.
❓ Is body rocking a sign of autism?
It can be, but not exclusively. Body rocking occurs in autism (stimming/self-regulation), sensory processing disorder (vestibular seeking), anxiety disorders (self-soothing), ADHD (arousal regulation), and in typically developing children (especially under age 3–4). Professional evaluation determines whether rocking is part of a broader developmental picture. Call 9100 181 181 for assessment guidance.
❓ How do I know which of the 9 materials is right for my child?
Start by observing when rocking happens: Constant across all situations → vestibular seeker → prioritize swings. Mostly when anxious/stressed → prioritize weighted products and cocoon swing. During seated work → wobble cushion + fidgets. During transitions → rocking chair. When in doubt, start with wobble cushion (lowest risk) and platform/cocoon swing (highest impact).
❓ My child's swing isn't helping. What am I doing wrong?
Most common issue: under-dosing. Vestibular seekers often need MORE input than parents expect. Try: increasing session duration (20 → 30 minutes), increasing arc size, adding sessions (3× to 5×/week). If rocking still doesn't respond after 4 weeks of increased dosing, the rocking may be primarily anxiety-driven rather than vestibular — consult an OT for functional assessment.
❓ Can I put a swing in a small apartment?
Yes. Options: doorway swing bars (limited arc but effective for mild seekers), freestanding swing frames (no ceiling mounting needed), outdoor options if outdoor access exists. For intense seekers, professional ceiling mounting in one room is worthwhile — consult a structural engineer or use Pinnacle's equipment guidance line: 9100 181 181.
❓ My child's school won't allow the wobble cushion. What can I do?
Frame it as a medical/therapeutic accommodation. Request a meeting citing: clinical recommendation from Pinnacle OT, evidence of wobble cushion efficacy (PMC11506176), and the fact that wobble cushions are invisible to other students. If school continues to refuse, request formal accommodation documentation under the Rights of Persons with Disabilities Act. Pinnacle can provide formal accommodation letters: 9100 181 181.
❓ How long before I see results?
Typically: 2–4 weeks for initial response (rocking slightly less after sessions); 4–6 weeks for consolidation (rocking less consistently throughout the day); 8–12 weeks for measurable overall reduction and partial mastery. Timeline depends on child's sensory seeking intensity, consistency of sensory diet, and whether all settings are covered (home + school + community).
❓ We can't afford a platform swing. What's the most effective free option?
The wobble cushion has the highest evidence-to-cost ratio. A partially inflated beach ball (₹100–200) under a chair seat provides similar micro-vestibular input. A sturdy rope swing from a tree with parent-supervised sessions provides high-intensity vestibular input at minimal cost. See Card 10 for all 9 DIY alternatives. Call 9100 181 181 for local resource guidance.

You Have Everything You Need. Start Today.
The science is clear. The materials are accessible. The protocol is proven across 20 million sessions. The only remaining step is yours.
🎯 Start This Technique Today
Access your GPT-OS® Guided Session — a personalized walkthrough of D-364 built around your child's profile.
📞 Book a Professional Consultation
Find your nearest Pinnacle center or book a teleconsult. Call FREE: 9100 181 181
▶ Explore the Next Technique
D-365: 9 Materials That Help With Spinning Behaviors — the next technique in the vestibular seeking cluster.
✦ PINNACLE BLOOMS CONSORTIUM VALIDATED ✦ Occupational Therapy • Speech-Language Pathology • Applied Behavior Analysis • Special Education • Neurodevelopmental Pediatrics • Clinical Research | Powered by GPT-OS® | 20M+ Sessions | 97%+ Improvement | 🦾 OT | 🗣️ SLP | 📊 ABA | 📚 SpEd | 🧠 NeuroDev | 🔬 CRO
Preview of 9 materials that help with body rocking Therapy Material
Below is a visual preview of 9 materials that help with body rocking therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
India's largest pediatric therapy consortium — 70+ centers, 20M+ exclusive 1:1 therapy sessions, 97%+ measured improvement rate, serving children and families across 70+ countries through the GPT-OS® Global Pediatric Therapeutic Operating System.
GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™
Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
Medical Disclaimer
This content is educational in nature. It does not replace individualized assessment from licensed occupational therapists, behavioral therapists, developmental pediatricians, or other qualified healthcare professionals. Body rocking may be associated with various conditions including autism spectrum disorder, sensory processing disorder, anxiety disorders, or stereotypic movement disorder — professional evaluation is essential for appropriate intervention planning. Never physically restrain a child to prevent rocking or punish rocking behavior. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network® clinical system. Always consult a qualified professional before implementing therapeutic interventions.
📞 FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages